updates in the treatment and management of relapsed ... mm.pdfcurrent recommendations and treatment...
TRANSCRIPT

1
Rachid Baz, MD
Associate Professor, Departments of Oncologic Sciences and Medicine
University of South Florida
Associate Member, Myeloma Section Head and Director of Clinical Research
Department of Malignant Hematology
H. Lee Moffitt Cancer Center and Research Institute
Updates in the Treatment and Management of Relapsed/Refractory
Multiple Myeloma
Disclosures
Research Funding:
– Celgene
– Millennium
– Sanofi
– Bristol Myers Squibb
– Karyopharm Therapeutic
2
Overview
Selecting Therapy Based on Specific Patient and Disease Features
Current Recommendations and Treatment Options for Relapsed/Refractory Myeloma
Future Directions in the Salvage Setting
Management of Adverse Events
Selecting Therapy for Myeloma Based on Specific Patient and
Disease Features

3
When to Consider Retreatment
Need to consider biochemical vs symptomatic relapse
– Patients with asymptomatic rise in M-protein can be observed to determine the rate of rise and nature of relapse
– Caveat: Patients with known aggressive or high-risk disease should be considered for salvage, even in the setting of biochemical relapse
Factors in Selecting Treatment For Relapsed/Refractory Myeloma Disease-related factors
– Duration of response to initial therapy
Treatment-related factors
– Previous therapy exposure (relapsed or refractory)
– Toxicity of regimen (combination vs single agent)
– Mode of administration (eg, oral or intravenous)
4
How do We Synthesize These Variables?
Does the patient NEED therapy?
– Defined by presence of symptoms similar to initial treatment
– Not all patients with biochemical relapse need therapy
– Aggressiveness of previous relapse, risk of organ damage, and magnitude of M-protein increase all play into this decision
Relapsed/Refractory Myeloma: Preferred Regimens NCCN Category 1
– Bortezomib
– SC vs IV administration
– Bortezomib/PLD
– Carfilzomib/lenalidomide/ dexamethasone
– Panobinostat/bortezomib/ dexamethasone
– Lenalidomide/dexamethasone
NCCN Category 2A
– Repeat primary induction therapy if relapse at > 6 mos
– Bortezomib combinations
– With dex; len/dex; thalidomide
– Carfilzomib
– Cyclophosphamide
– High-dose or with bort/dex or len/dex
– Pomalidomide/dexamethasone
– Thalidomide/dexamethasone
– DCEP, DT-PACE, or VTD-PACE
NCCN clinical practice guidelines in oncology: multiple myeloma: v.2.2015. www.nccn.org

5
Treating Indolent, Slow-Growing Myeloma in First Relapse
• Initial treatment with bortezomib
• May consider single agent without dexamethasone
• Underlying PN
IMiD-Based Salvage PI-Based Salvage Transplant-Based Salvage
• Initial treatment with IMiD
• Previous bortezomib therapy but good or long response
• Renal dysfunction
• Transplant not part of initial therapy
• Long remission post transplant
Treating Relapsed/Refractory Myeloma
Carfilzomib-Based Salvage
Pomalidomide-Based Salvage
Other Salvage
• Intolerance to bortezomib
• Dexamethasone-sparing treatment as part of a combination
• Intolerance to IMiDs
• Lenalidomiderefractory
• Refractory to standard-dose PI
• Pts with del(17p)?
• Refractory to pomalidomide and carfilzomib
• Monoclonal antibody candidate
• Clinical trials
6
Treating Aggressive Myeloma With Rapid, Multiple Relapses
• DCEP vs DT-PACE
• Oral vs IV chemo
• Performance status of patient plays important role
Chemotherapy-Based Salvage
Likely Combination TherapyDo Not Wait for Symptomatic Relapse
Chemotherapy + Novel Agent
Transplant-Based Salvage
• Combinations of lenalidomide/ bortezomib and other chemotherapy agents
• Likely to be short lived
• Rapid disease control
• Reconstitute marrow
Current Recommendations and Treatment Options for
Relapsed/Refractory Myeloma

7
Summary of Combination Therapy in RR MM
60 65
31
6555
87
70
95
67 64
85
71
0
20
40
60
80
100
IMiD-Based PI-Based
11
4
9
4
26
10 10 119
30
1316
20
NR
NR
30 29
0
5
10
15
20
25
30
35
IMiD-Based PI-Based
1. Dimopoulos M, et al. N Engl J Med. 2007;357:2123-2132. 2. Morgan JG, et al. Br J Haematol. 2007;137:268-269. 3. San Miguel J, et al. Lancet Oncol. 2013;14:1055-1066. 4. Baz R, et al. ASH 2014. Abstract 303. 5. Lendvai N, et al. Blood. 2014;124:899-906. 6. Stewart AK, et al. ASH 2014. Abstract 79. 7. Shah JJ, et al. ASH 2013. Abstract 690. 8. Bringhen S, et al. Blood. 2014;124:63-69. 9. Mikhael JR, et al. Br J Haematol. 2009;144:169-175. 10. Richardson PG, et al. Blood. 2014;123:1461-1469. 11. Lacy MQ, et al. ASH 2014. Abstract 304. 12. Monge J, et al. ASCO 2014. Abstract 8586.
Rd[
1] *
CyR
d[2
]
Pom
D[3
] *C
yPom
D[4
]
CD
[5]
CR
d[6
] *C
Pom
D[7
]
CyC
D[8
]
VD
[9] *
VR
d[1
0] *
VP
omD
[11
]
CyB
orD
[12
]
Rd[
1] *
Pom
D[3
] *
CyP
omD
[4]
CD
[5]
CR
d[6
] *
CP
omD
[7]
VR
d[1
0] *
VP
omD
[11
]
CyB
orD
[12
]
OR
R,
%
Sur
viva
l, m
onth
s*Data from phase III trials, all others from phase I or II trials
ORR PFS OS
Summary of IMiD Combination Therapy Regimen Phase N Outcomes
Len/dex vs dex[1] III 351 OS: NR vs 20.6 moTTP: 11.3 mo vs 4.7 mo
ORR: 60.2% vs 24%
Len/cyclo/dex [2] II 21 ORR: 65%
Pom/dex II[3]
III[4]
221
302
OS: 16.5 mo vs 13. 6 moPFS: 4.2 mo vs 2.7 mo
ORR: 33% vs 18%PFS: 4.0 mo vs 1.9 mo
Pom/cyclo/dex vs pom/dex[5] II 70 OS: 16.4 mo vs 10.5 moPFS: 9.2 mo vs 4.4 mo
ORR: 65% vs 39%
1. Dimopoulos M, et al. N Engl J Med. 2007;357:2123-2132. 2. Morgan JG, et al. Br J Haematol. 2007;137:268-269. 3. Richardson PG, et al. Blood. 2014;123:1826-1832. 4. San Miguel J, et al. Lancet Oncol. 2013;14:1055-1066. 5. Baz R, et al. ASH 2014. Abstract 303.

8
Summary of Proteasome Inhibitor Combination Therapy Regimen Phase N Outcomes
Carfilzomib ± dex[1] II 44 OS: 20.3 moPFS: 4.1 moORR: 55%
Carfilzomib/len/dexvs len/dex[2]
III 792 PFS: 26.3 mo vs 17.6ORR: 87.1% vs 66.7%
(Interim 24-mo OS: 73.3% vs 65.0%)
Carfilzomib/pom/dex[3] I/II 79 PFS: 9.7 moORR: 70%
Carfilzomib/cyclo/dex[4] II 58 2-yr OS: 87%2-yr PFS: 76%
ORR: 95%
1. Lendvai N, et al. Blood. 2014;124:899-906. 2. Stewart AK, et al. ASH 2014. Abstract 79. 3. Shah JJ, et al. ASH 2013. Abstract 690. 4. Bringhen S, et al. Blood. 2014;124:63-69.
Summary of Proteasome Inhibitor Combination Therapy Regimen Phase N Outcomes
Bortezomib ± dex[1] IIIb 638 ORR: 67%
Bortezomib/len/dex[2] II 64 OS: 30 moPFS: 9.5 moORR: 64%
Bortezomib/pom/dex[3] I/II 47 PFS: 10.7 moORR: 85%
Bortezomib/cyclo/dex[4] II 55 OS: 29 moPFS: 9.2 moORR: 71%
1. Mikhael JR, et al. Br J Haematol. 2009;144:169-175. 2. Richardson PG, et al. Blood. 2014;123:1461-1469. 3. Lacy MQ, et al. ASH 2014. Abstract 304. 4. Monge J, et al. ASCO 2014. Abstract 8586.

9
Phase III ASPIRE: Len/Dexamethasone ±Carfilzomib in RR MM Randomized, open-label, multicenter phase III trial
KRdCarfilzomib* 27 mg/m2 IV
Days 1, 2, 8, 9, 15, 16 (20 mg/m2 days 1, 2, cycle 1 only)Lenalidomide 25 mg Days 1–21
Dexamethasone 40 mg Days 1, 8, 15, 22(n = 396)
RdLenalidomide 25 mg Days 1–21
Dexamethasone 40 mg Days 1, 8, 15, 22(n = 396)
Stratified by: β2-microglobulin, prior bortezomib, and prior lenalidomide
*After cycle 12, carfilzomib given on days 1, 2, 15, 16. After cycle 18, carfilzomib discontinued. Stewart AK, et al. ASH 2014. Abstract 79.
Pts with symptomatic RR MM after 1-3 prior treatments with ≥ PR to ≥ 1 prior regimen
(N = 792)
Len/Dexamethasone ± Carfilzomib in RR MM (ASPIRE): PFS (ITT)
KRd Rd(n = 396) (n = 396)
Median PFS, mo 26.3 17.6HR (KRd/Rd) (95% CI) 0.69 (0.57–0.83)P value (one-sided) < .0001
1.0
0.8
0.6
0.4
0.2
0.0
Pro
po
rtio
n S
urv
ivin
gW
ith
ou
t P
rog
ress
ion
KRdRd
0 6 12 18 24 30 36 42 48Months Since Randomization
Stewart AK, et al. ASH 2014. Abstract 79. Reproduced with permission.
Risk Group by FISH
KRd (n = 396) Rd (n = 396) HR P Value
n Median PFS, mo n Median PFS, mo
High 48 23.1 52 13.9 0.70 .083
Standard 147 29.6 170 19.5 0.66 .004
10
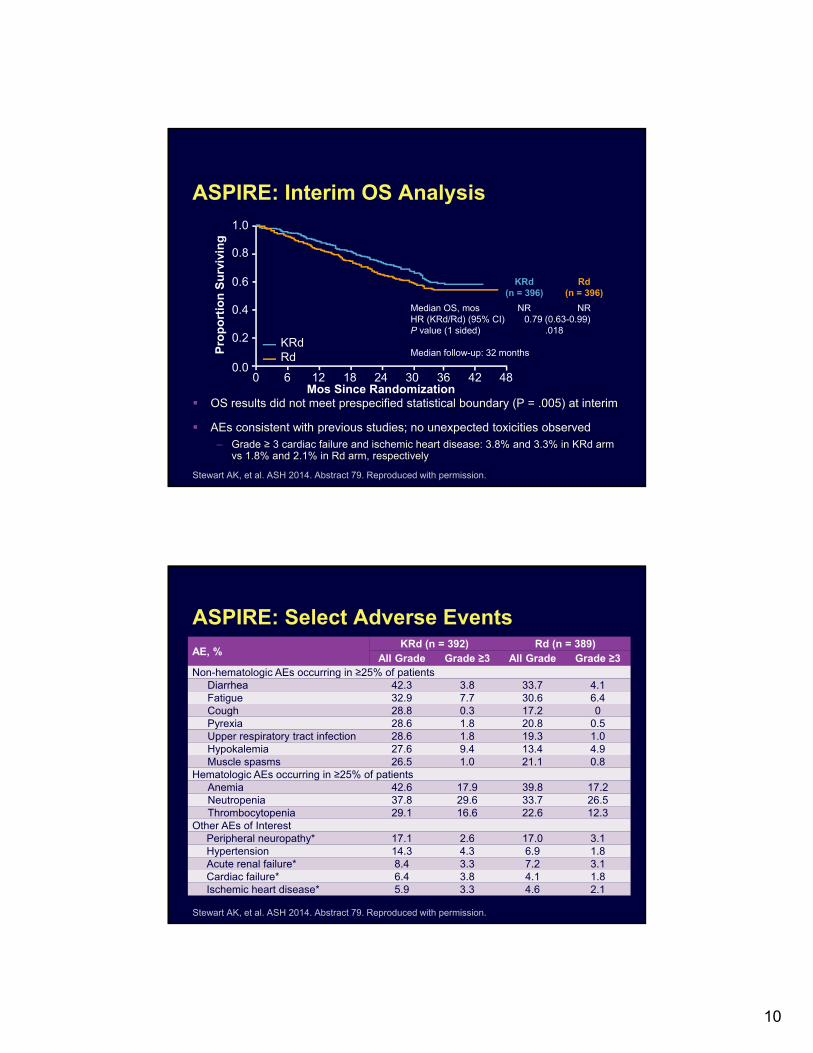
ASPIRE: Interim OS Analysis
OS results did not meet prespecified statistical boundary (P = .005) at interim
AEs consistent with previous studies; no unexpected toxicities observed– Grade ≥ 3 cardiac failure and ischemic heart disease: 3.8% and 3.3% in KRd arm
vs 1.8% and 2.1% in Rd arm, respectively
KRd Rd(n = 396) (n = 396)
Median OS, mos NR NRHR (KRd/Rd) (95% CI) 0.79 (0.63-0.99)P value (1 sided) .018
Median follow-up: 32 months
1.0
0.8
0.6
0.4
0.2
0.0
Pro
po
rtio
n S
urv
ivin
g
KRdRd
0 6 12 18 24 30 36 42 48Mos Since Randomization
Stewart AK, et al. ASH 2014. Abstract 79. Reproduced with permission.
ASPIRE: Select Adverse Events
AE, %KRd (n = 392) Rd (n = 389)
All Grade Grade ≥3 All Grade Grade ≥3Non-hematologic AEs occurring in ≥25% of patients
Diarrhea 42.3 3.8 33.7 4.1Fatigue 32.9 7.7 30.6 6.4Cough 28.8 0.3 17.2 0Pyrexia 28.6 1.8 20.8 0.5Upper respiratory tract infection 28.6 1.8 19.3 1.0Hypokalemia 27.6 9.4 13.4 4.9Muscle spasms 26.5 1.0 21.1 0.8
Hematologic AEs occurring in ≥25% of patients Anemia 42.6 17.9 39.8 17.2Neutropenia 37.8 29.6 33.7 26.5Thrombocytopenia 29.1 16.6 22.6 12.3
Other AEs of InterestPeripheral neuropathy* 17.1 2.6 17.0 3.1Hypertension 14.3 4.3 6.9 1.8Acute renal failure* 8.4 3.3 7.2 3.1Cardiac failure* 6.4 3.8 4.1 1.8Ischemic heart disease* 5.9 3.3 4.6 2.1
Stewart AK, et al. ASH 2014. Abstract 79. Reproduced with permission.

11
Phase III PANORAMA 1: Bort/Dex ±Panobinostat in RR Myeloma Randomized, double-blind trial
Panobinostat 20 mg (3x/wk)Bortezomib 1.3 mg/m2 IV (d1,4,8,11)
Dexamethasone 20 mg(d1,2,4,5,8,9,11,12)
(n = 387)
Placebo (3x/wk)Bortezomib 1.3 mg/m2 IV (d1,4,8,11)
Dexamethasone 20 mg(d1,2,4,5,8,9,11,12)
(n = 381)
Stratified by prior lines of therapy, and prior bortezomib
Richardson P, et al. ASCO 2014. Abstract 8510^.
Pts with symptomatic RR MM after 1-3 prior
treatments (bortezomib-refractory excluded)
(N = 768)
Panobinostat 20 mg (3x/wk)Bortezomib* 1.3 mg/m2 IVDexamethasone* 20 mg
*reduced frequency
Placebo (3x/wk)Bortezomib* 1.3 mg/m2 IVDexamethasone* 20 mg
*reduced frequency
Treatment Phase I:Eight 21-d cycles (24 wks)
Treatment Phase II:Four 42-d cycles (24 wks)
Patients with ≥ SD in tx phase I can proceed to tx phase II
Bort/Dex ± Panobinostat in RR Myeloma (PANORAMA 1): PFS Primary endpoint reached: median PFS ↑ by 3.9 months
Richardson P, et al. ASCO 2014. Abstract 8510^.
GK6
k17

Slide 22
GK6 Design: For the PFS and OS slides, change to Pan/bort/dex and placebo/bort/dex both here and in legend. Also, hyphenate CI ranges. Change PFS column header to "Median PFS, mo (95% CI)"Gordon Kelley, 3/19/2015
k17 Creative, please redrawkrosenthal, 3/31/2015
12
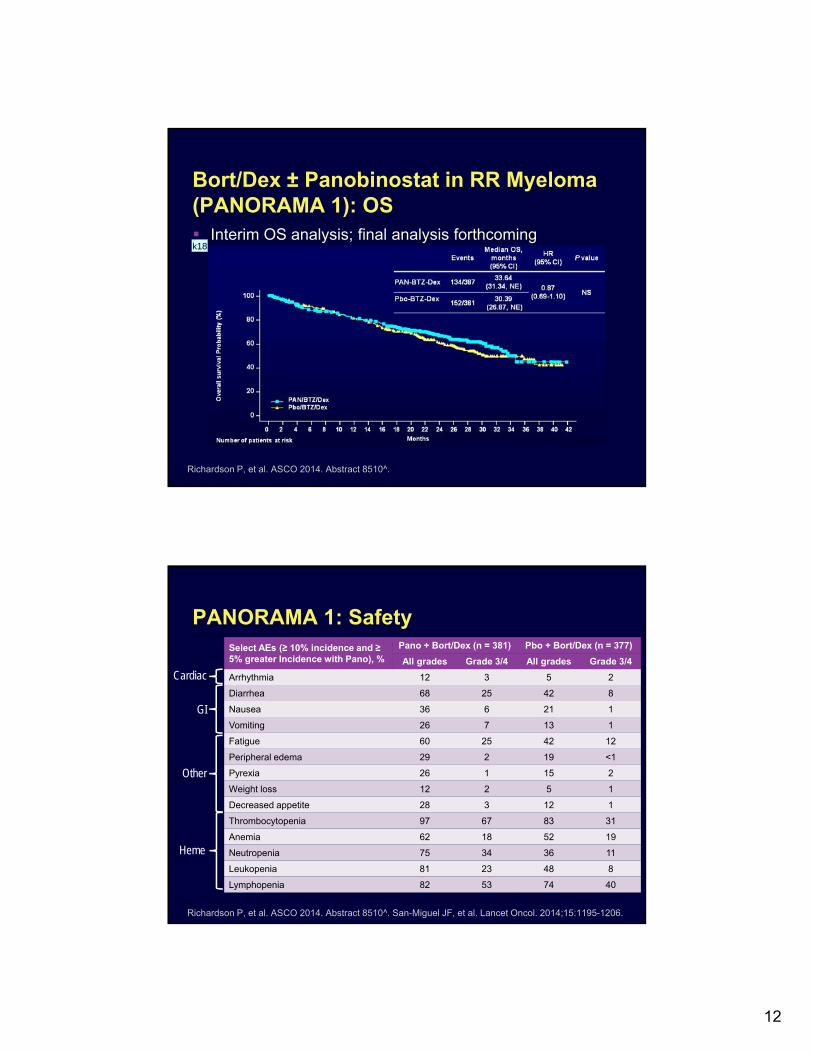
Bort/Dex ± Panobinostat in RR Myeloma (PANORAMA 1): OS Interim OS analysis; final analysis forthcoming
Richardson P, et al. ASCO 2014. Abstract 8510^.
k18
PANORAMA 1: Safety
Richardson P, et al. ASCO 2014. Abstract 8510^. San-Miguel JF, et al. Lancet Oncol. 2014;15:1195-1206.
Select AEs (≥ 10% incidence and ≥ 5% greater Incidence with Pano), %
Pano + Bort/Dex (n = 381) Pbo + Bort/Dex (n = 377)
All grades Grade 3/4 All grades Grade 3/4
Arrhythmia 12 3 5 2
Diarrhea 68 25 42 8
Nausea 36 6 21 1
Vomiting 26 7 13 1
Fatigue 60 25 42 12
Peripheral edema 29 2 19 <1
Pyrexia 26 1 15 2
Weight loss 12 2 5 1
Decreased appetite 28 3 12 1
Thrombocytopenia 97 67 83 31
Anemia 62 18 52 19
Neutropenia 75 34 36 11
Leukopenia 81 23 48 8
Lymphopenia 82 53 74 40
Cardiac
GI
Other
Heme

Slide 23
k18 Creative, please redrawkrosenthal, 3/31/2015
13
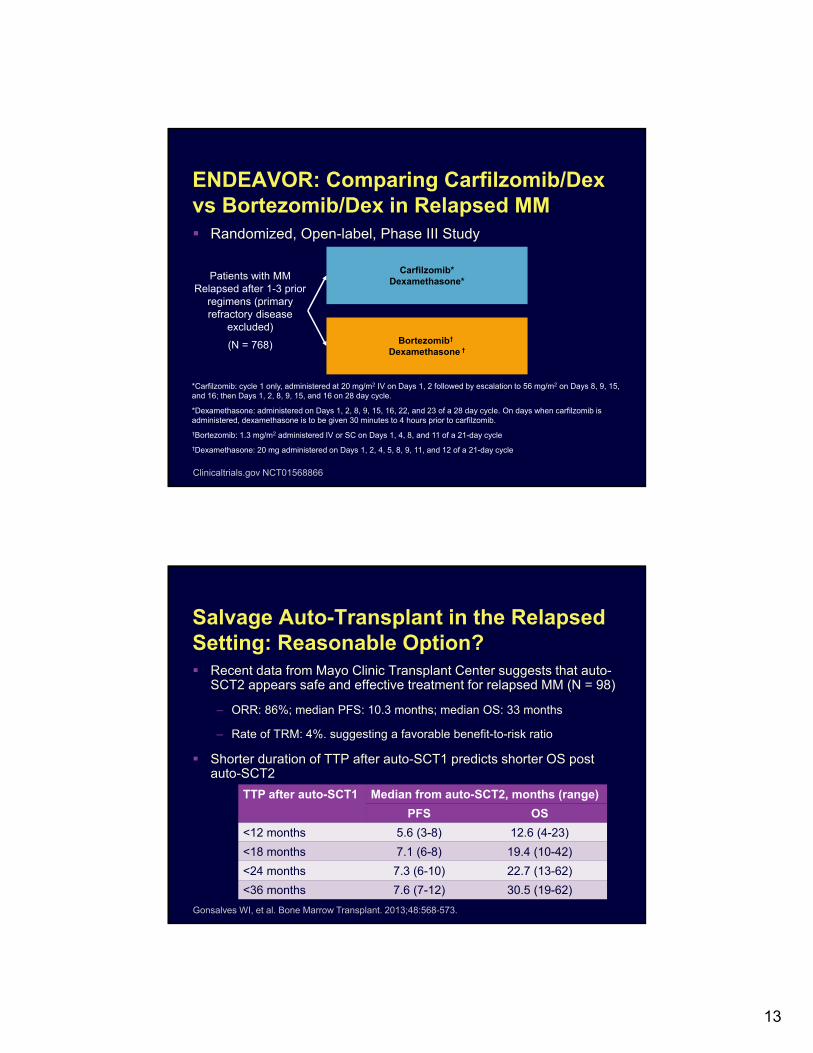
ENDEAVOR: Comparing Carfilzomib/Dex vs Bortezomib/Dex in Relapsed MM Randomized, Open-label, Phase III Study
Carfilzomib*Dexamethasone*
Bortezomib†
Dexamethasone †
Patients with MM Relapsed after 1-3 prior
regimens (primary refractory disease
excluded)
(N = 768)
*Carfilzomib: cycle 1 only, administered at 20 mg/m2 IV on Days 1, 2 followed by escalation to 56 mg/m2 on Days 8, 9, 15, and 16; then Days 1, 2, 8, 9, 15, and 16 on 28 day cycle.
*Dexamethasone: administered on Days 1, 2, 8, 9, 15, 16, 22, and 23 of a 28 day cycle. On days when carfilzomib is administered, dexamethasone is to be given 30 minutes to 4 hours prior to carfilzomib.
†Bortezomib: 1.3 mg/m2 administered IV or SC on Days 1, 4, 8, and 11 of a 21-day cycle
†Dexamethasone: 20 mg administered on Days 1, 2, 4, 5, 8, 9, 11, and 12 of a 21-day cycle
Clinicaltrials.gov NCT01568866
Salvage Auto-Transplant in the Relapsed Setting: Reasonable Option? Recent data from Mayo Clinic Transplant Center suggests that auto-
SCT2 appears safe and effective treatment for relapsed MM (N = 98)
– ORR: 86%; median PFS: 10.3 months; median OS: 33 months
– Rate of TRM: 4%. suggesting a favorable benefit-to-risk ratio
Shorter duration of TTP after auto-SCT1 predicts shorter OS post auto-SCT2
TTP after auto-SCT1 Median from auto-SCT2, months (range)
PFS OS
<12 months 5.6 (3-8) 12.6 (4-23)
<18 months 7.1 (6-8) 19.4 (10-42)
<24 months 7.3 (6-10) 22.7 (13-62)
<36 months 7.6 (7-12) 30.5 (19-62)
Gonsalves WI, et al. Bone Marrow Transplant. 2013;48:568-573.

14
Future Directions in the Salvage Setting
Ixazomib (MLN9708): Phase I Studies in Relapsed/Refractory Myeloma N = 50 evaluable
Dose: 0.24-2.97 mg/m2 on days 1,8,15 q28d
ORR: 9 pts (1 VGPR, 8 PR)
– MR: 1 pt
– SD: 15 pts
– Disease control up to 9 mos
Safety: generally well tolerated
– Heme, GI AEs manageable
– Low rate of discontinuation
– Infrequent PN; 1 grade 3 PN
PK profile supports wkly dosing
Kumar S, et al. Blood. 2014;124:1047-1055.

15
Primary Endpoint: PFS Secondary Endpoints: OS, OS and PFS in high-risk patients, response (ORR,
PR, VGPR, CR, DOR), safety, pain response, global health outcomes, PK analysis, association between response or resistance to ixazomib and cytogenetics
Patients with relapsed/refractory
MM; 1-3 prior therapies;
ECOG PS 0-2(Planned N = 703)
Treatment continued until
disease progression or unacceptable
toxicity
*Lenalidomide 25 mg PO Days 1-21; dexamethasone 40 mg PO Days 1,8,15,22
Ixazomib 4 mg PO D1,8,15 + RD*28-day cycles
Placebo PO D1,8,15 + RD*28-day cycles
Phase III TOURMALINE-MM1: IRD vs RD in Relapsed and/or Refractory MM
ClinicalTrials.gov. NCT01564537.
Single-Agent Oprozomib in RR MM: Summary of Efficacy
Response data not shown for step-up cohorts due to limited treatment exposure
2/7
Sch
edu
le5/
14 S
ched
ule
*ORR in 11 carfilzomib-refractory patients (phase II): 18.2%
Vij R, et al. ASH 2014. Abstract 34. Reproduced with permission.
0 50 100
Phase Ib150-330 mg/d
(n = 16)
Phase Ib + II150-270 mg/d
(n = 43)
PD SD MR PR VGPR CR
44 19 19 13
9 42 9 9 12 2
ORR: 31.3%
ORR: 23.3%*
CBR: 50.0%
CBR: 32.6%
16
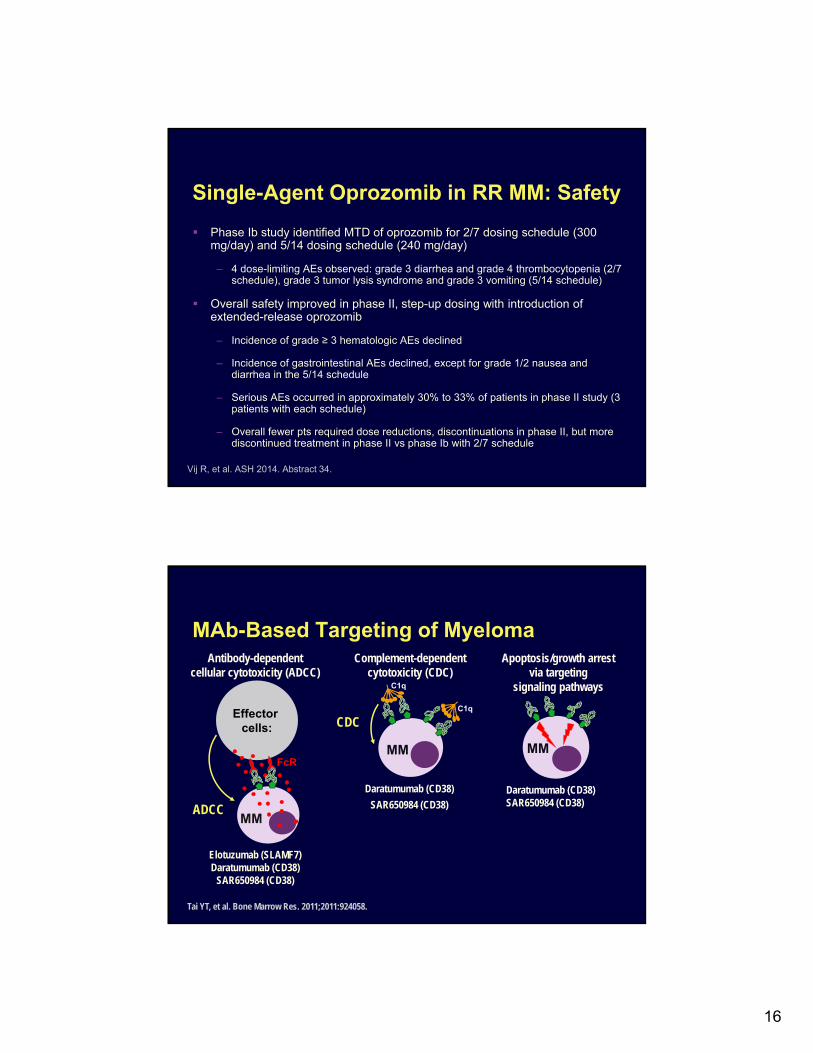
Single-Agent Oprozomib in RR MM: Safety
Phase Ib study identified MTD of oprozomib for 2/7 dosing schedule (300 mg/day) and 5/14 dosing schedule (240 mg/day)
– 4 dose-limiting AEs observed: grade 3 diarrhea and grade 4 thrombocytopenia (2/7 schedule), grade 3 tumor lysis syndrome and grade 3 vomiting (5/14 schedule)
Overall safety improved in phase II, step-up dosing with introduction of extended-release oprozomib
– Incidence of grade ≥ 3 hematologic AEs declined
– Incidence of gastrointestinal AEs declined, except for grade 1/2 nausea and diarrhea in the 5/14 schedule
– Serious AEs occurred in approximately 30% to 33% of patients in phase II study (3 patients with each schedule)
– Overall fewer pts required dose reductions, discontinuations in phase II, but more discontinued treatment in phase II vs phase Ib with 2/7 schedule
Vij R, et al. ASH 2014. Abstract 34.
Antibody-dependentcellular cytotoxicity (ADCC)
ADCC
Effector cells:
MM
FcR
Complement-dependentcytotoxicity (CDC)
CDC
MM
C1q
C1q
Apoptosis/growth arrest via targeting
signaling pathways
MM
Elotuzumab (SLAMF7)Daratumumab (CD38)
SAR650984 (CD38)
Daratumumab (CD38)
SAR650984 (CD38)
Tai YT, et al. Bone Marrow Res. 2011;2011:924058.
MAb-Based Targeting of Myeloma
Daratumumab (CD38)SAR650984 (CD38)

17
Phase Ib/II 1703 Trial: Elotuzumab in Combination with Len/Dex in RR MM Patients treated with elotuzumab 10 or 20 mg/kg +
lenalidomide/dexamethasone
– Approximately 60% of pts received previous treatment with bortezomib and/or thalidomide and 20% to 30% were refractory to previous treatment
Richardson PG, et al. ASH 2014. Abstract 302.
ORR92%
ORR76%
ORR84%
Per
cent
of
patie
nts,
%
34
Phase 2 efficacy: progression-free survival
363773
322759
292453
232144
191534
181331
161329
333265
302656
262147
211940
181533
181331
151227
151227
139
22
117
18
000
246
86
14
149
23
128
20
107
17
46
10
022
10 mg/kg20 mg/kg
Total
Numberat risk:
Median time to progression/death:
10 mg/kg (n=36): 32.49 mos
20 mg/kg (n=37): 25.00 mos
Total (n=73): 28.62 mos
0
10
20
30
40
50
60
70
80
90
100
0 4 8 12 16 20 24 28 32 36 48Time (months)
Prog
ress
ion-
free
pat
ient
s (%
)
44402 6 10 14 18 22 26 30 34 38 42 46

18
Elotuzumab in Combination with Len/Dex in RR MM (Phase Ib/II): Safety
Infusion reactions: if pts tolerated 2 mL/min, flow rate increased to 5 mL/min
– 33% of infusions were at 5 mL/min
– 11% experienced infusion reactions
– 7 at < 2 mL/min rate
– 1 at ≥ 2 mL/min rate
– Most common events included pyrexia (3), nausea (1), rash (3)
Richardson PG, et al. ASH 2014. Abstract 302.
Grade 3/4 AEs, n (%) Elo 10 mg/kg (n = 36)
Elo 20 mg/kg (n = 37)
Lymphopenia 10 (28) 5 (14)Diarrhea 5 (14) 2 (5)Neutropenia 7 (19) 7 (19)Thrombocytopenia 7 (19) 6 (16)Anemia 6 (17) 5 (14)Hyperglycemia 2 (6) 5 (14)Fatigue 3 (8) 2 (5)Back pain 3 (8) 1 (3)Dyspnea 3 (8) 1 (3)Muscle spasms 2 (6) 0Insomnia 0 2 (5)Asthenia 1 (3) 1 (3)URI 1 (3) 1 (3)Pyrexia 1 (3) 1 (3)Peripheral edema 0 1 (3)Nausea 0 1 (3)
Primary endpoints: PFS and ORR Secondary endpoints: OS, pain response Exploratory endpoints: Safety, time to response, DOR, time to subsequent
therapy, health-related QoL, PK and immunogenicity of elotuzumab
Patients with relapsed/refractory MM and 1-3 prior
therapies(Planned N = 640)
Treatment continued until
disease progression,
death, or withdrawal of
consent
Randomized 1:1
Elotuzumab + RD28-day cycles
RD28-day cycles
Phase III ELOQUENT-2: Len/Dex ±Elotuzumab in RR MM
Lonial S, et al. ASCO 2012. Abstract TPS8112; ClinicalTrials.gov. NCT01239797.
Elotuzumab 10 mg/kg IV weekly D1,8,15,22 (Cycles 1-2) and D1,15 (Cycles 3+); Lenalidomide 25 mg PO D1-21; Dexamethasone 40 mg D1,8,15,22 (8 mg IV + 28 mg PO during elotuzumab dosing)
19
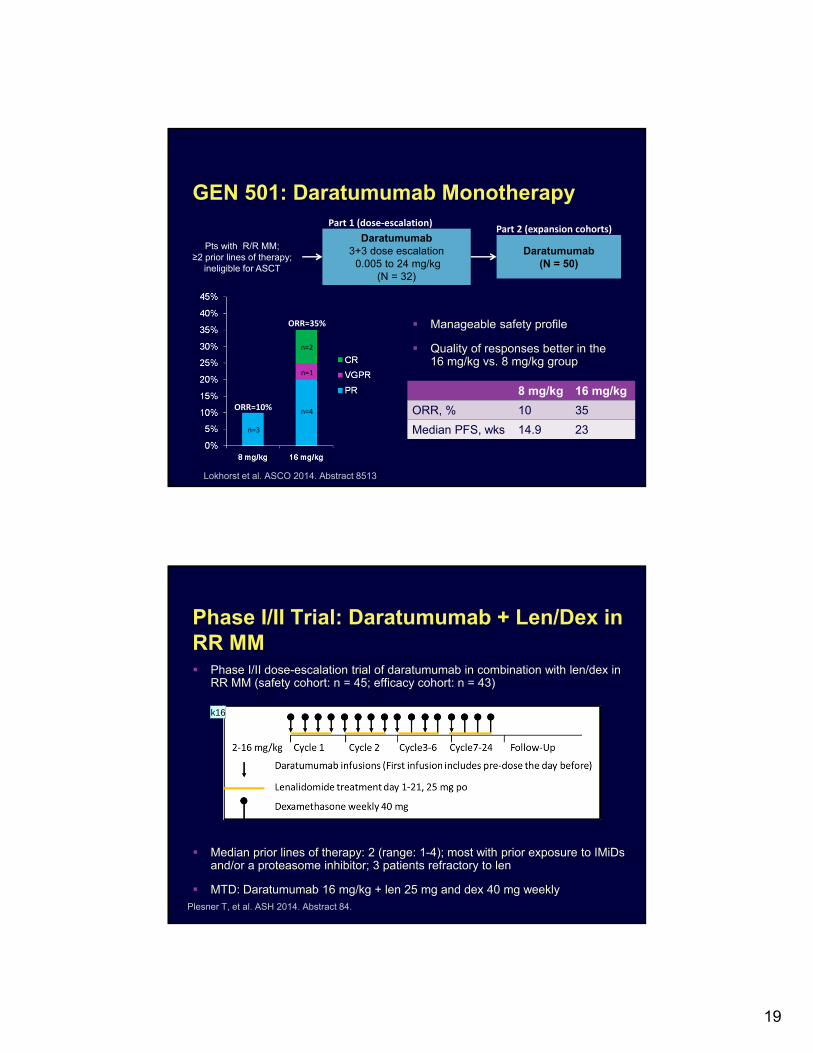
GEN 501: Daratumumab Monotherapy
Pts with R/R MM; ≥2 prior lines of therapy;
ineligible for ASCT
Daratumumab3+3 dose escalation
0.005 to 24 mg/kg(N = 32)
Daratumumab(N = 50)
Part 1 (dose‐escalation)Part 2 (expansion cohorts)
n=3
n=4
n=1
n=2
ORR=10%
ORR=35% Manageable safety profile
Quality of responses better in the 16 mg/kg vs. 8 mg/kg group
8 mg/kg 16 mg/kg
ORR, % 10 35
Median PFS, wks 14.9 23
Lokhorst et al. ASCO 2014. Abstract 8513
Phase I/II Trial: Daratumumab + Len/Dex in RR MM Phase I/II dose-escalation trial of daratumumab in combination with len/dex in
RR MM (safety cohort: n = 45; efficacy cohort: n = 43)
Median prior lines of therapy: 2 (range: 1-4); most with prior exposure to IMiDs and/or a proteasome inhibitor; 3 patients refractory to len
MTD: Daratumumab 16 mg/kg + len 25 mg and dex 40 mg weeklyPlesner T, et al. ASH 2014. Abstract 84.
k16

Slide 38
k16 Creative, please redrawkrosenthal, 3/31/2015
20
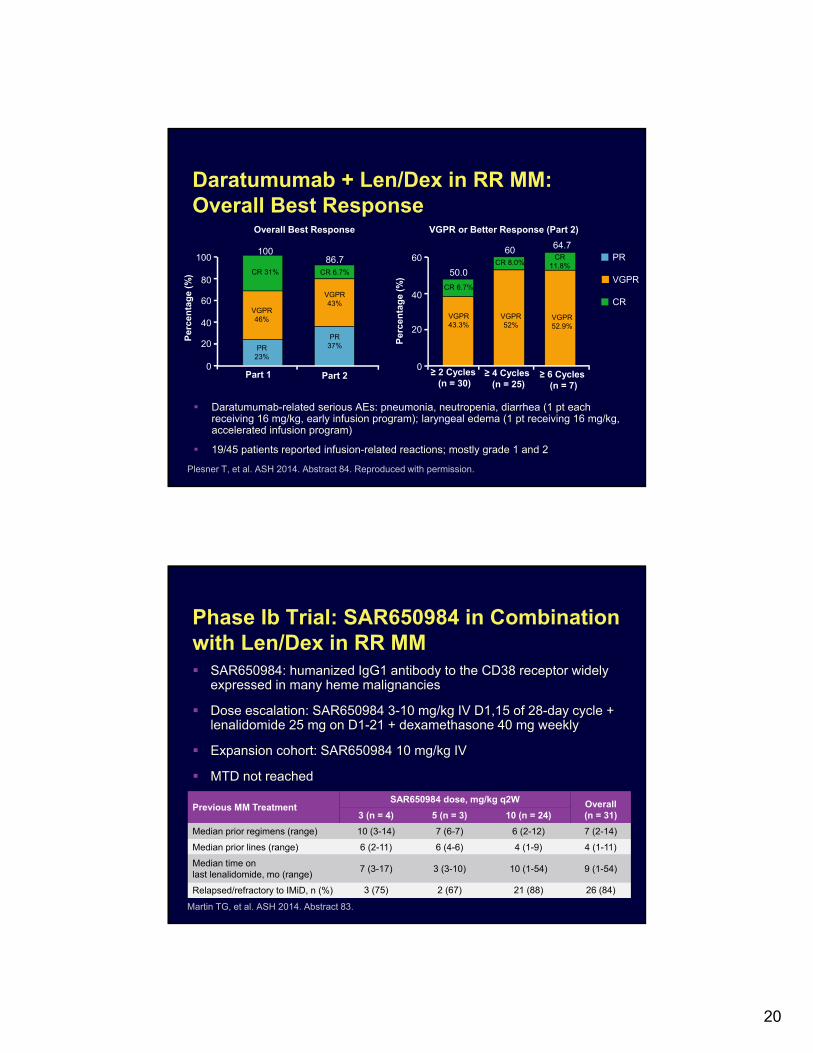
Daratumumab + Len/Dex in RR MM: Overall Best Response
Daratumumab-related serious AEs: pneumonia, neutropenia, diarrhea (1 pt each receiving 16 mg/kg, early infusion program); laryngeal edema (1 pt receiving 16 mg/kg, accelerated infusion program)
19/45 patients reported infusion-related reactions; mostly grade 1 and 2
CR 31% CR 6.7%
VGPR 46%
PR 23%
VGPR 43%
PR 37%
CR 6.7%
CR 8.0%CR
11.8%
VGPR 43.3%
VGPR 52%
VGPR 52.9%
Plesner T, et al. ASH 2014. Abstract 84. Reproduced with permission.
Part 10
20
40
60
80
100
Per
cen
tag
e (%
)
Overall Best Response
Part 2
PR
VGPR
CR
10086.7
50.0
60 64.7
0
20
40
60
Per
cen
tag
e (%
)
VGPR or Better Response (Part 2)
≥ 2 Cycles (n = 30)
≥ 4 Cycles (n = 25)
≥ 6 Cycles (n = 7)
Phase Ib Trial: SAR650984 in Combination with Len/Dex in RR MM SAR650984: humanized IgG1 antibody to the CD38 receptor widely
expressed in many heme malignancies
Dose escalation: SAR650984 3-10 mg/kg IV D1,15 of 28-day cycle + lenalidomide 25 mg on D1-21 + dexamethasone 40 mg weekly
Expansion cohort: SAR650984 10 mg/kg IV
MTD not reached
Martin TG, et al. ASH 2014. Abstract 83.
Previous MM TreatmentSAR650984 dose, mg/kg q2W Overall
(n = 31)3 (n = 4) 5 (n = 3) 10 (n = 24)
Median prior regimens (range) 10 (3-14) 7 (6-7) 6 (2-12) 7 (2-14)
Median prior lines (range) 6 (2-11) 6 (4-6) 4 (1-9) 4 (1-11)
Median time on last lenalidomide, mo (range)
7 (3-17) 3 (3-10) 10 (1-54) 9 (1-54)
Relapsed/refractory to IMiD, n (%) 3 (75) 2 (67) 21 (88) 26 (84)

21
SAR650984 in Combination with Len/Dex in RR MM (Phase Ib): Efficacy DoR: 9.13 mo (range: 1.2-15.2)
Martin TG, et al. ASH 2014. Abstract 83. Reproduced with permission.
Response, %Total
(N = 31)
ORR 58
sCR 6
VGPR 23
PR 29
CBR 65
MR 6
SD 19
PD 13P
atie
nts
, % ORR 25%
CBR 50%
ORR 67%CBR 67%
ORR 63%CBR 67%
ORR 58%CBR 65%
100
80
60
40
20
03 mg/kg(n = 4)
5 mg/kg(n = 3)
10 mg/kg(n = 24)
Overall(N = 31)
25
25
67
8
29
6
23
6
25 29
4
PR sCRVGPRMR
Most common treatment-related grade 3/4 AEs: neutropenia, anemia, thrombocytopenia, and febrile neutropenia
15 incidences of infusion reaction, all occurring in the first 2 cycles
JS10
Additional Agents Currently in DevelopmentAgent MOA Phase in Development
Ibrutinib Tyrosine kinase inhibitor (BTK, ERK1/2, others)
Phase I and II
Filanesib Kinesin spindle protein (KSP) inhibitor
Phase II
Indatuximab ravtansine CD138 antibody-drugconjugate
Phase I and II
Ricolinostat HDAC inhibitor Phase I and I/II
Selinexor (KPT-330) XPO1 nuclear transport inhibitor
Phase I and II

Slide 41
JS10 The relative size of the PR and VGPR bars in the "overall" column need to be adjusted.Jill Sakai, 3/18/2015

22
Management of Adverse Effects
Peripheral Neuropathy: Risk Factors and General ConsiderationsGeneral Considerations Endocrine disorders
– Hypothyroidism
– Diabetes
Nutritional disease Connective tissue disease Vascular disease Medications Herpes zoster Most common symptoms
– Sensory deficits
– Neuropathic pain
Disease- and Treatment-Related Factors Hyperviscosity syndrome Hypergammaglobulinemia Incidence of peripheral neuropathy
in untreated patients: 39% Incidence of grade 3/4 CIPN with
novel agents– Bortezomib: 26% to 44%
– ↓ with weekly vs twice weekly dosing
– ↓ with SC administration
– Thalidomide: 28% to 41%– ↑ with higher doses and prolonged
therapy
– Carfilzomib: overall 14% Gleason C, et al. J Natl Compr Cancer Netw. 2009;7:971-979. Palumbo A, et al. J Clin Oncol. 2014;32:587-600. Kurtin S, et al. J Adv Pract Oncol. 2013;4:307-321.
23
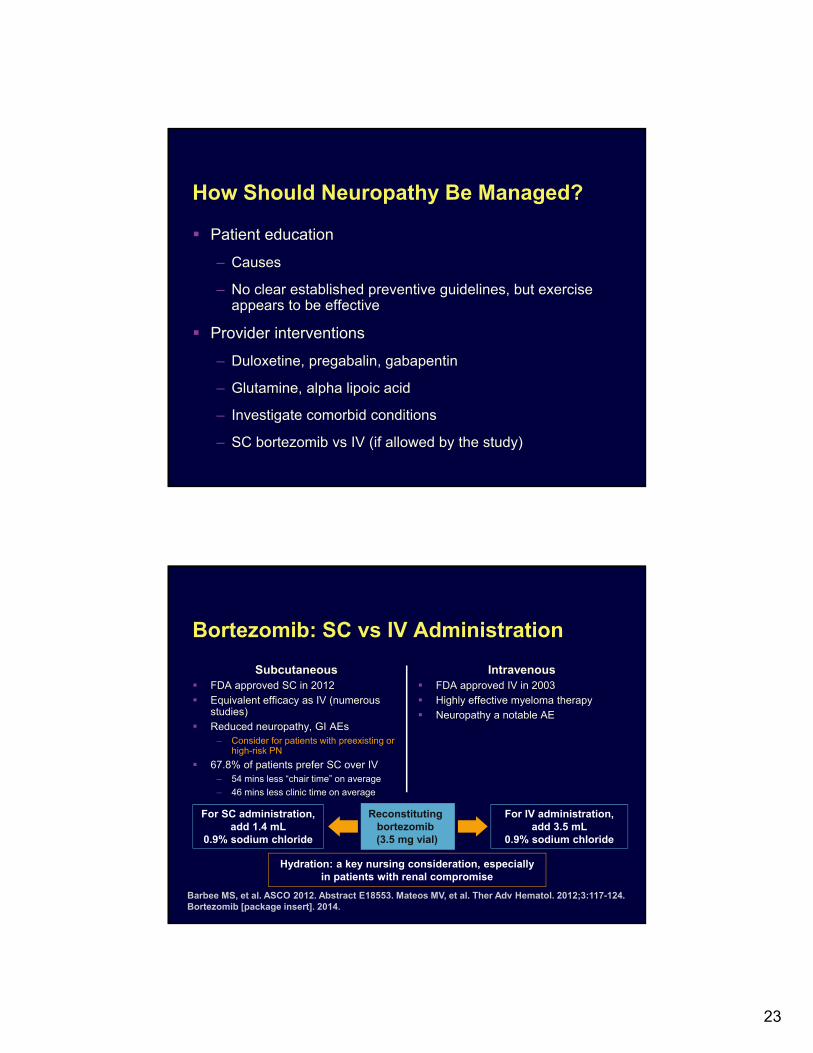
How Should Neuropathy Be Managed?
Patient education
– Causes
– No clear established preventive guidelines, but exercise appears to be effective
Provider interventions
– Duloxetine, pregabalin, gabapentin
– Glutamine, alpha lipoic acid
– Investigate comorbid conditions
– SC bortezomib vs IV (if allowed by the study)
Bortezomib: SC vs IV Administration
Subcutaneous FDA approved SC in 2012
Equivalent efficacy as IV (numerous studies)
Reduced neuropathy, GI AEs– Consider for patients with preexisting or
high-risk PN
67.8% of patients prefer SC over IV– 54 mins less “chair time” on average
– 46 mins less clinic time on average
Intravenous FDA approved IV in 2003
Highly effective myeloma therapy
Neuropathy a notable AE
Reconstituting bortezomib (3.5 mg vial)
For SC administration, add 1.4 mL
0.9% sodium chloride
Hydration: a key nursing consideration, especially in patients with renal compromise
For IV administration, add 3.5 mL
0.9% sodium chloride
Barbee MS, et al. ASCO 2012. Abstract E18553. Mateos MV, et al. Ther Adv Hematol. 2012;3:117-124. Bortezomib [package insert]. 2014.
24
Risk Assessment for VTEs in Patients Receiving Thalidomide or Lenalidomide VTE prophylaxis for individual risk factors (eg, age or obesity) or
myeloma-related risk factors (eg, immobilization or hyperviscosity)
– If ≤ 1 risk factor present: aspirin 81-325 mg/day
– If ≥ 2 risk factors present: LMWH (equivalent to enoxaparin 40 mg/day) or full-dose warfarin (target INR: 2-3)
VTE prophylaxis for myeloma therapy–related risk factors (eg, high-dose dexamethasone, IMiDs, doxorubicin, multiagentchemotherapy)
– LMWH (equivalent to enoxaparin 40 mg/day) or full-dose warfarin (target INR: 2-3)
Palumbo A, et al J Clin Oncol. 2014;32:587-600. Palumbo A, et al. Leukemia. 2008;22:414-423.
Myelosuppression and Infection
Myelosuppression is associated with both myeloma and the drugs used to treat it
– Risk of infection increased due to hypogammaglobulinemia
– Dose-modification guidelines are available in package inserts
Infection prophylaxis
– Patients should remain up-to-date on appropriate vaccinations
– VZV prophylaxis when receiving PIs
– Use of IVIG or prophylactic antibiotics is controversial, and should only be used when warranted
– Patient education emphasizing importance of alerting treating clinicians of potential infection can reduce unnecesary antibiotics
25
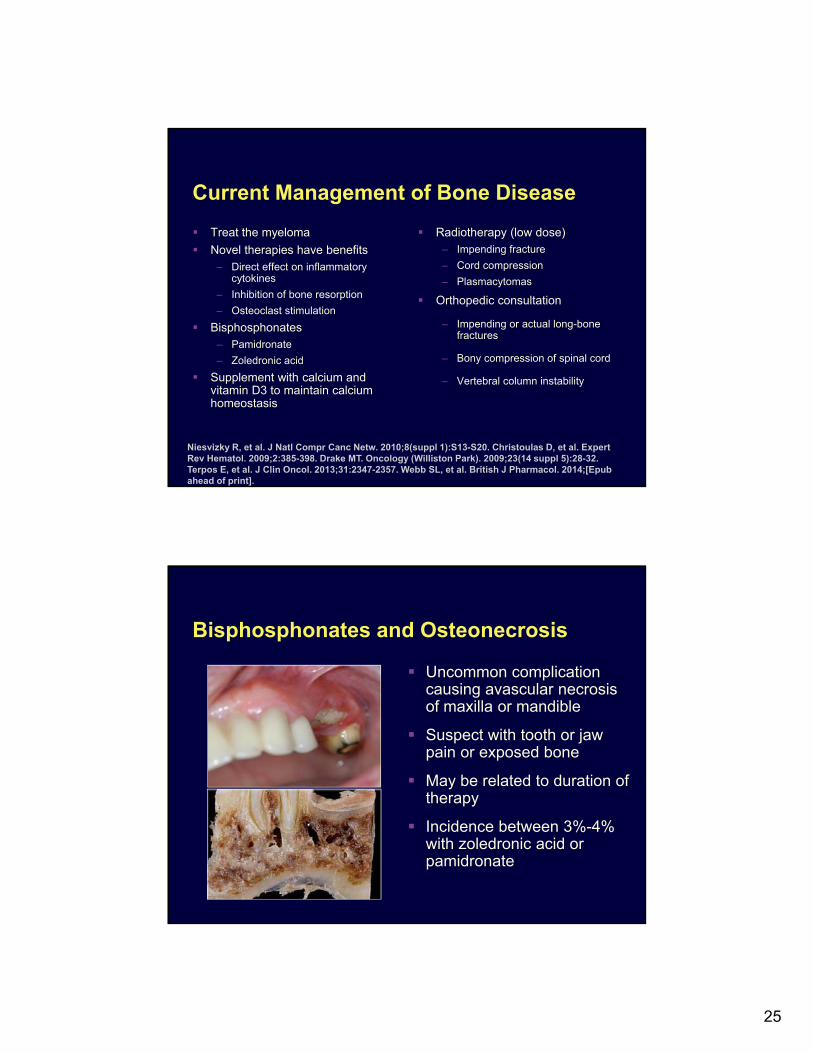
Current Management of Bone Disease
Treat the myeloma
Novel therapies have benefits– Direct effect on inflammatory
cytokines
– Inhibition of bone resorption
– Osteoclast stimulation
Bisphosphonates– Pamidronate
– Zoledronic acid
Supplement with calcium and vitamin D3 to maintain calcium homeostasis
Radiotherapy (low dose)– Impending fracture
– Cord compression
– Plasmacytomas
Orthopedic consultation
– Impending or actual long-bone fractures
– Bony compression of spinal cord
– Vertebral column instability
Niesvizky R, et al. J Natl Compr Canc Netw. 2010;8(suppl 1):S13-S20. Christoulas D, et al. Expert Rev Hematol. 2009;2:385-398. Drake MT. Oncology (Williston Park). 2009;23(14 suppl 5):28-32. Terpos E, et al. J Clin Oncol. 2013;31:2347-2357. Webb SL, et al. British J Pharmacol. 2014;[Epub ahead of print].
Bisphosphonates and Osteonecrosis
Uncommon complication causing avascular necrosis of maxilla or mandible
Suspect with tooth or jaw pain or exposed bone
May be related to duration of therapy
Incidence between 3%-4% with zoledronic acid or pamidronate
26
Overall Conclusions Doublet or triplet combination approaches should be considered
– Combination treatment with either bortezomib, carfilzomib, and/or pomalidomide with dexamethasone active and well tolerated
– Novel agents in combination can achieve prolonged responses even in relapsed disease
Optimal management approaches should emphasize improving QoL by identifying potential complications of therapy and minimizing long-term toxicity
New classes of agents and second-generation agents have activity and are of considerable interest