using tcga data to inform on precision medicine in late ... · pdf fileusing tcga data to...
TRANSCRIPT
Using TCGA data to inform on precision medicine in late-stage cancer settings
Andrew J. Mungall, Ph.D. British Columbia Cancer Agency, Genome Sciences Centre [email protected]
3rd TCGA Symposium, Natcher Conference Center, NIH Campus, Bethesda, MD 12th May 2014
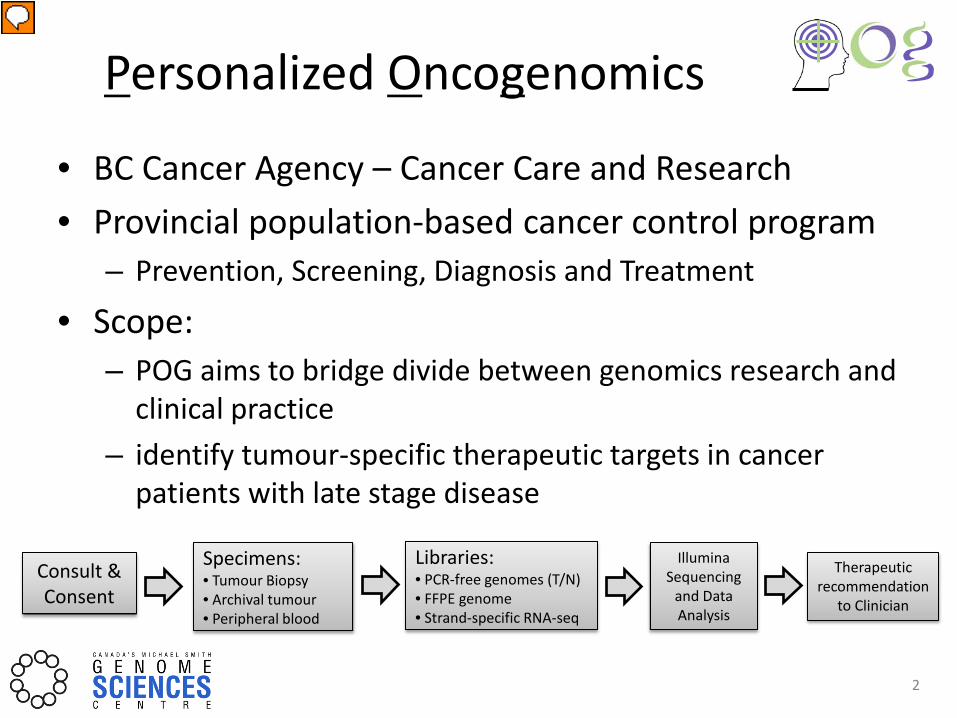
Personalized Oncogenomics
• BC Cancer Agency – Cancer Care and Research • Provincial population-based cancer control program
– Prevention, Screening, Diagnosis and Treatment
• Scope: – POG aims to bridge divide between genomics research and
clinical practice – identify tumour-specific therapeutic targets in cancer
patients with late stage disease
2
Consult & Consent
Specimens: • Tumour Biopsy • Archival tumour • Peripheral blood
Libraries: • PCR-free genomes (T/N) • FFPE genome • Strand-specific RNA-seq
Illumina Sequencing
and Data Analysis
Therapeutic recommendation
to Clinician
Gene coverage + QC
Assembly
Trans-Abyss
Assembly
Trans-Abyss
Paired calling
Concatenate fastqs
Tumour-Normal Fold change
Genome validator
CNV/LOH
Comparison to expression database
Pathway Analysis
Mining of drug databases and literature
Merge bams
Preliminary Report
Clonal Heterogeneity
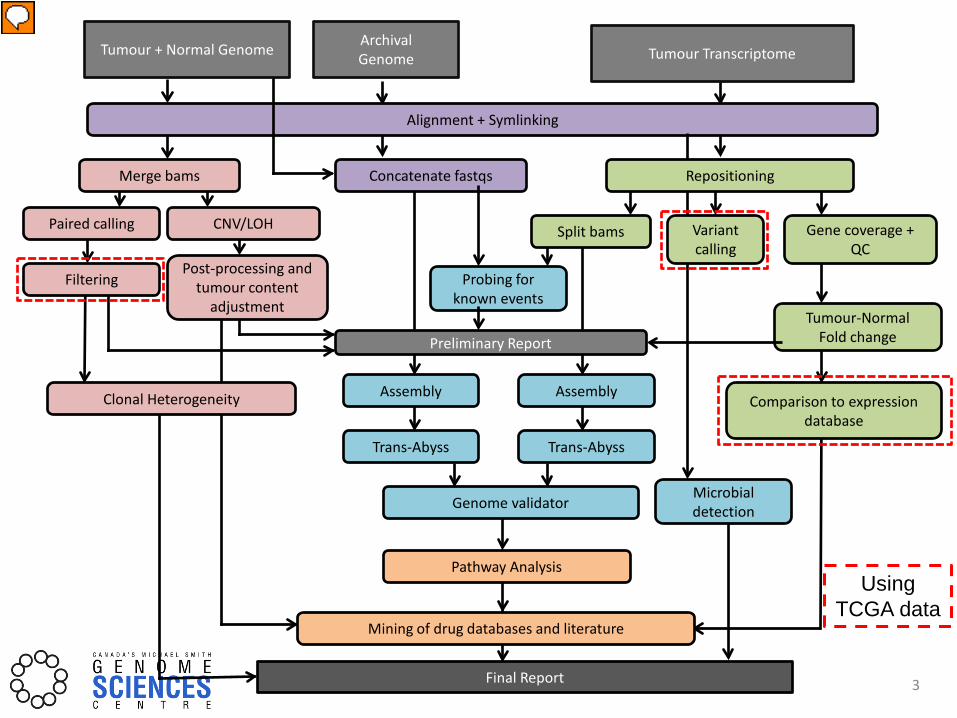
Alignment + Symlinking
Probing for known events
Split bams
Tumour + Normal Genome Archival Genome Tumour Transcriptome
Microbial detection
Variant calling
Repositioning
Filtering Post-processing and
tumour content adjustment
Final Report
Using TCGA data
3

Patients enrolled and data generated
0
5
10
15
20
25
30
Num
ber o
f pat
ient
s
Patients enrolled since July 2012 (pediatric) 83 (8)
Biopsies performed 69
Tumour types 28
Metastasis tumour genome coverage 93x
Matched normal genome coverage 46x
Archival tumour genome coverage 46x
Average tumour RNA-seq reads 306M
Analysis reported (in progress) 50 (19)
Average time from biopsy to report 38 days
4
How POG guides treatment decision making
1) Providing directed cytotoxic chemotherapy choices & targeted therapeutic options
2) Complemented/corrected clinical tests 3) Changed diagnosis 4) Identifying primary tumour sites when
previously unknown
5

1) Case POG 003 – SCC Provided targeted therapeutic options
6
2007 2008 2009 2010 2011 2012 2013 2014
“red rash” on chest Developed bleeding ulcerations Diagnosed with Squamous cell carcinoma
Three lines of chemotherapy and multiple rounds of radiotherapy started in 2007
• Jan 2012 – new preauricular node • Jun – Aug 2012 node and chest mass growing (pain and hearing loss) • Sep 2012, preauricular and chest lesions biopsied for POG
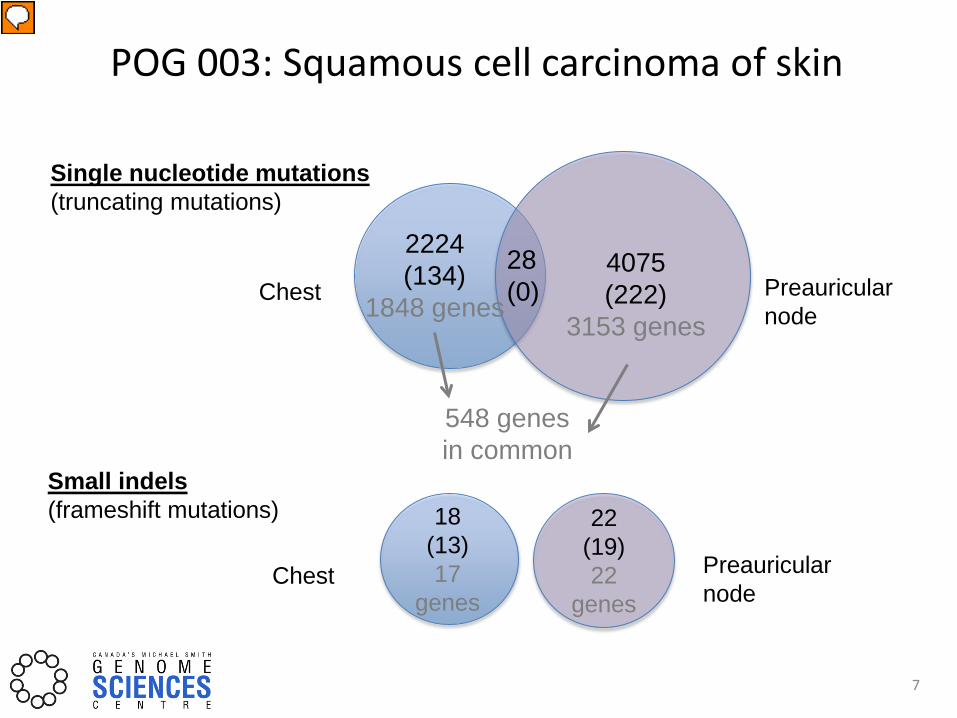
POG 003: Squamous cell carcinoma of skin
7
2224 (134)
1848 genes
4075 (222)
3153 genes
28 (0)
18 (13) 17
genes Chest
Preauricular node
Preauricular node
Single nucleotide mutations (truncating mutations)
Small indels (frameshift mutations)
Chest
22 (19) 22
genes
548 genes in common

POG 003 – Copy number variants
Gain Loss
Chest Preauricular node
8
Chest Preauricular node chr16 chr16
• Samples almost completely distinct • Very few common breakpoints

Pathway summary
9
SHC1
GRB2
SOS1
TGFBR2
SMAD2
SMAD3
SMAD4
CDKN2A CDKN1C
CCND1
CDK4/6
CCNA1
CDK2
cell proliferation
overexpressed compared to normal skin & compendium
X activating mutation
X mutation copy number gain copy number loss
TP53
activation interaction inhibition interaction indirect activation
X inactivating mutation
GAB1
PI3K
AKT1
mTOR BAD
p70S6Kb BCL2
evading apoptosis
protein synthesis
MMPs
MMP1 MMP9
Chest tumour
Laminins LAMC2 LAMB3
PTEN
TGFB1
TGFBR3 EGFR PDGFR
TGFA
ATM
SRC
FAK
endothelial cell mitogenesis migration
angiogenesis
Integrins ITGA3 ITGA6
TYMP o
VEGFs MMPs IL8
BCR
CDC42 RAC3
PAK7
AXIN1
microtubule stabilization
& organization
PDGFA
X
cell cycle progression
CHK2 CHK1 CRKL
RAS
CDKN2C
Double strand DNA repair
PARP1
Single strand DNA repair
GPCR signaling
X
NF1 X
X X X
X X X
X
X
X ATR
FANCM
cell cycle checkpoints
X X X
DNA repair defects, PTEN loss, AKT1 gain
Under-expressed compared to normal skin & compendium
SHC1
GRB2
SOS1
TGFBR2
SMAD2
SMAD3
SMAD4
CDKN2A CDKN1C
CCND1
CDK4/6
CCNA1
CDK2
cell proliferation
TP53
GAB1
PI3K
AKT1
mTOR BAD
p70S6Kb BCL2
evading apoptosis
protein synthesis
MMPs
MMP1 MMP9
Pre-auricular tumour
Laminins LAMC2 LAMB3
PTEN
TGFB1
TGFBR3 EGFR PDGFR
TGFA
ATM
SRC
FAK
endothelial cell mitogenesis migration
angiogenesis
Integrins ITGA3 ITGA6
TYMP o
VEGFs MMPs IL8
BCR
CDC42 RAC3
PAK7
AXIN1
microtubule stabilization
& organization
PDGFA
cell cycle progression
ATR
CHK2 CHK1 CRKL
RAS
CDKN2C
Double strand DNA repair
PARP1
Single strand DNA repair
GPCR signaling
X
X
NF1 X
X
X
X X
FANCM
cell cycle checkpoints
X X
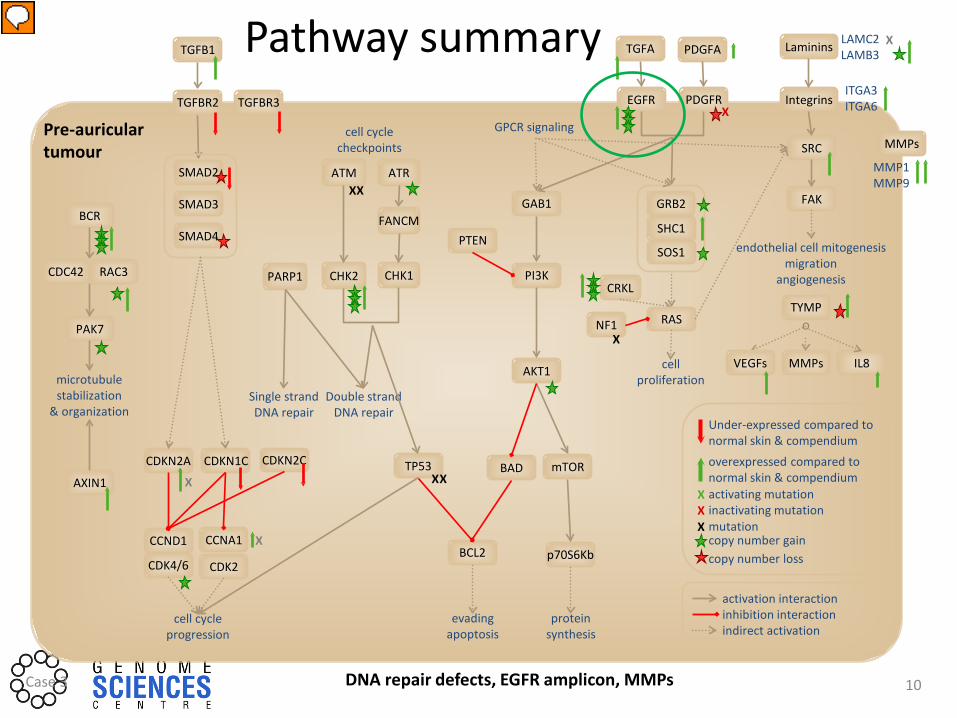
DNA repair defects, EGFR amplicon, MMPs Case 3
Pathway summary
10
Under-expressed compared to normal skin & compendium
overexpressed compared to normal skin & compendium activating mutation
mutation copy number gain copy number loss
inactivating mutation X
X X
activation interaction inhibition interaction indirect activation
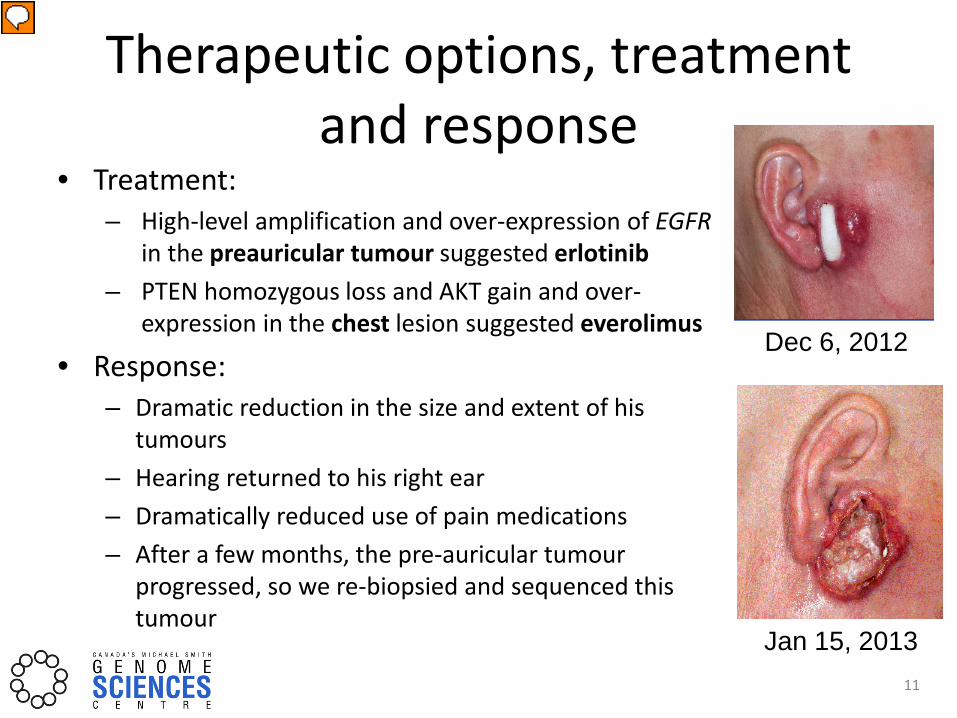
Therapeutic options, treatment and response
• Treatment: – High-level amplification and over-expression of EGFR
in the preauricular tumour suggested erlotinib – PTEN homozygous loss and AKT gain and over-
expression in the chest lesion suggested everolimus
• Response: – Dramatic reduction in the size and extent of his
tumours – Hearing returned to his right ear – Dramatically reduced use of pain medications – After a few months, the pre-auricular tumour
progressed, so we re-biopsied and sequenced this tumour
Dec 6, 2012
Jan 15, 2013 11
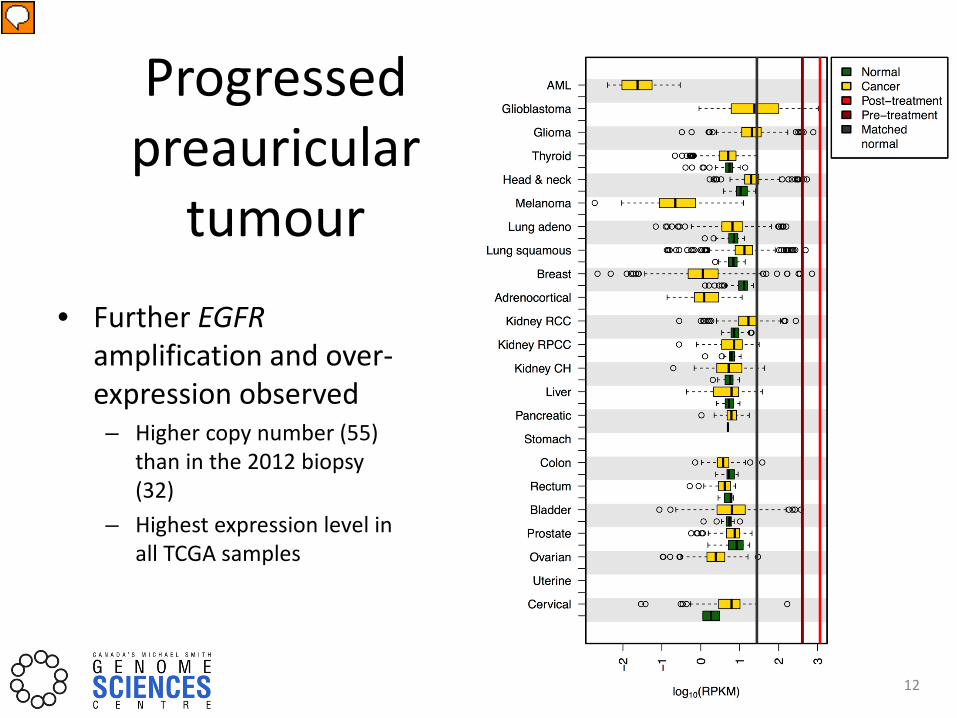
Progressed preauricular
tumour • Further EGFR
amplification and over-expression observed – Higher copy number (55)
than in the 2012 biopsy (32)
– Highest expression level in all TCGA samples
12

2) Case POG 030 - NSCLC Complemented/corrected clinical tests
• 68 yo male lifelong never smoker diagnosed with non-small-cell lung adenocarcinoma
Jan Feb 2013
Mar Apr May Jun Jul Aug
Confirmed Non-small cell lung adenocarcinoma, metastasis in lymph node
FNA of right supraclavicular node - EGFR and ALK tests negative
Radiation and three lines of chemo between March and July 2013 but rapid progression
Biopsied same node for POG
13
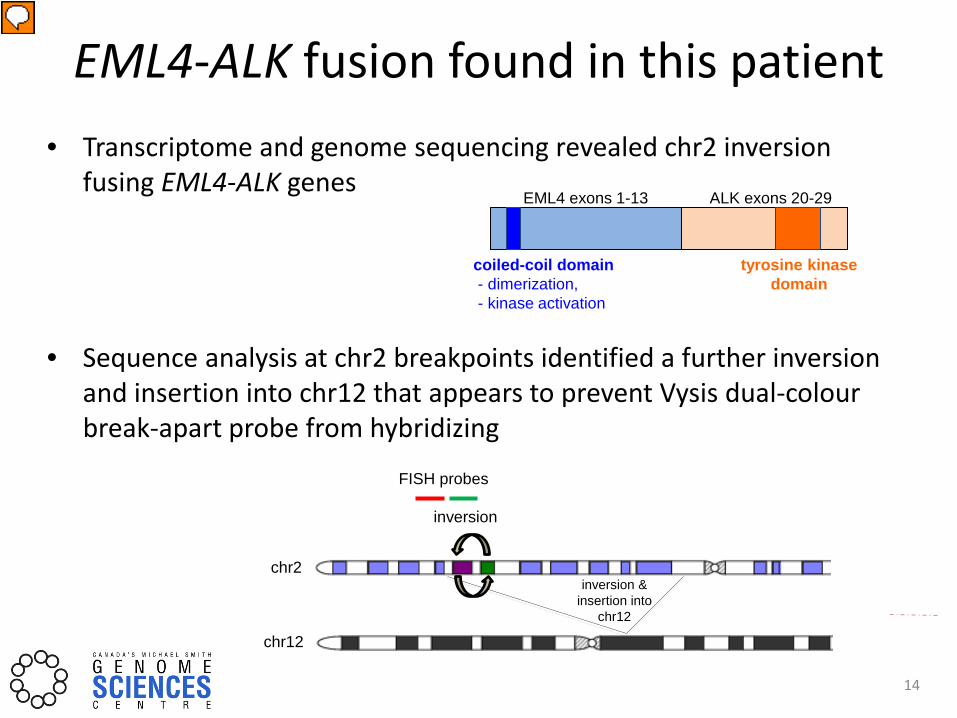
• Transcriptome and genome sequencing revealed chr2 inversion fusing EML4-ALK genes
• Sequence analysis at chr2 breakpoints identified a further inversion and insertion into chr12 that appears to prevent Vysis dual-colour break-apart probe from hybridizing
EML4 exons 1-13 ALK exons 20-29
coiled-coil domain - dimerization, - kinase activation
tyrosine kinase domain
EML4-ALK fusion found in this patient
14
inversion
inversion & insertion into
chr12
chr2
chr12
FISH probes
POG30
POG21 POG9
POG25
POG24
POG30 POG9
POG25 POG21 POG24
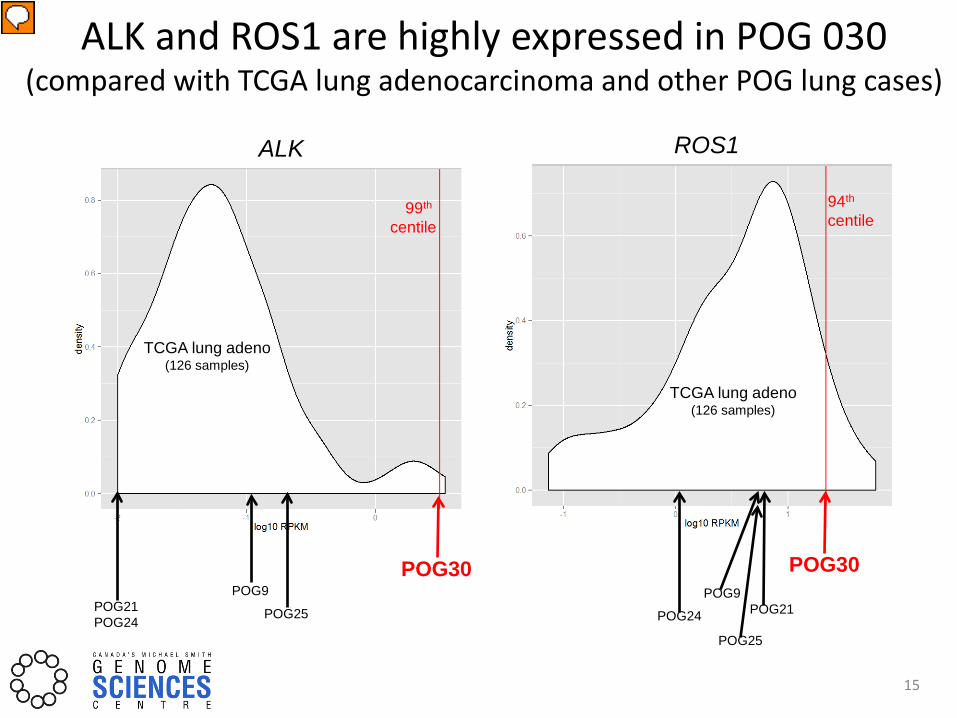
ALK ROS1
TCGA lung adeno (126 samples)
TCGA lung adeno (126 samples)
99th centile
94th centile
ALK and ROS1 are highly expressed in POG 030 (compared with TCGA lung adenocarcinoma and other POG lung cases)
15

Response to ALK inhibition (Crizotinib)
• EML4-ALK fusion, with high overall expression of ALK together with ROS1 over-expression
• TKI Crizotinib was immediately administered
• The tumour responded dramatically
16
Sept 4 2013 – before Crizotinib Crizotinib started Sept 25 Scan from Dec 12, 2013
17
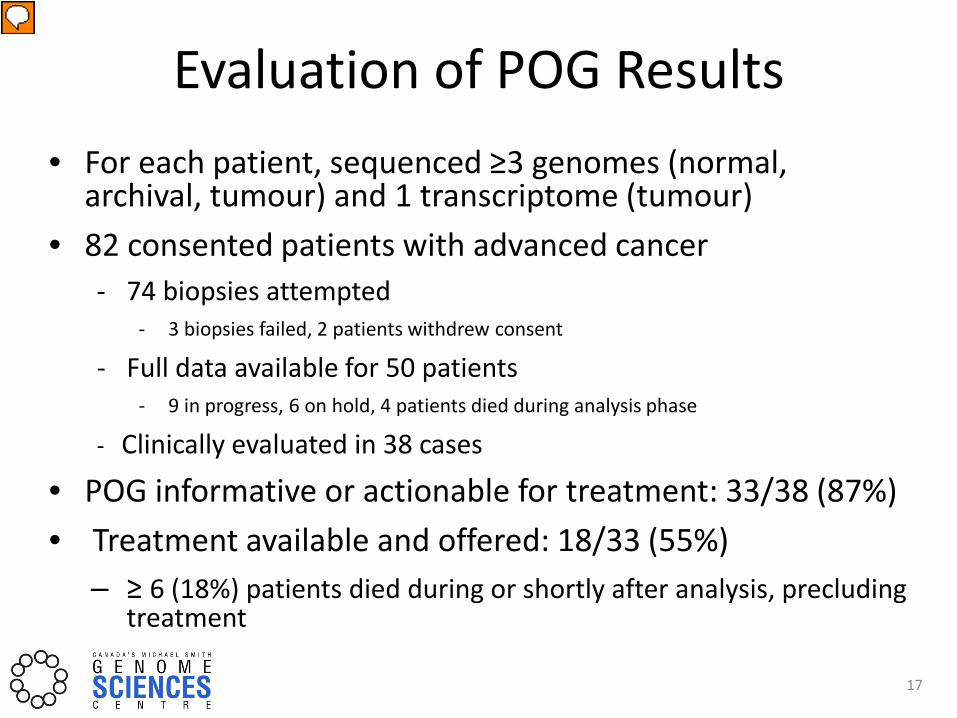
• For each patient, sequenced ≥3 genomes (normal, archival, tumour) and 1 transcriptome (tumour)
• 82 consented patients with advanced cancer - 74 biopsies attempted
- 3 biopsies failed, 2 patients withdrew consent
- Full data available for 50 patients - 9 in progress, 6 on hold, 4 patients died during analysis phase
- Clinically evaluated in 38 cases
• POG informative or actionable for treatment: 33/38 (87%) • Treatment available and offered: 18/33 (55%)
– ≥ 6 (18%) patients died during or shortly after analysis, precluding treatment
Evaluation of POG Results
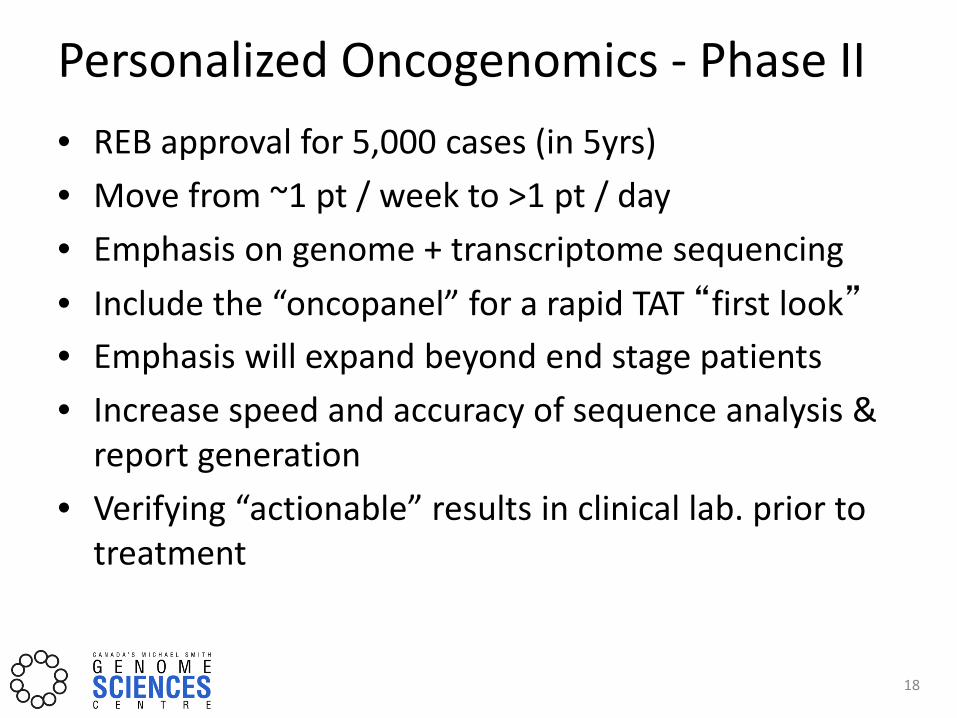
Personalized Oncogenomics - Phase II • REB approval for 5,000 cases (in 5yrs) • Move from ~1 pt / week to >1 pt / day • Emphasis on genome + transcriptome sequencing • Include the “oncopanel” for a rapid TAT “first look” • Emphasis will expand beyond end stage patients • Increase speed and accuracy of sequence analysis &
report generation • Verifying “actionable” results in clinical lab. prior to
treatment
18
Acknowledgements Janessa Laskin and Marco Marra
Co-Project Leaders Care Research
BCCA Francois Benard Kim Chi Stephan Chia Karen Gelmon Cheryl Ho Farzad Jamshidi Aly Karsan Christian
Kollmannsberger Howie Lim Caroline Lohrisch Martin Monty Torsten Nielsen Dan Renouf Tamara Shenkier Sophie Sun Anna Tinker Youwen Zhou
Yussanne Ma Richard Ma Simon Haile Merhu Helen McDonald Michelle Moksa Richard Moore Andy Mungall Karen Mungall Pawan Pandoh Erin Pleasance Robyn Roscoe Jacquie Schein Yaoqing Shen Young Song Nina Thiessen
VGH David Schaeffer Tony Ng
CTAG David Huntsman Julie Ho Julie Lorette Amy Lum Sarah Padilla Peggy Tsang Stephen Yip
Molecular Oncology
Sam Aparicio Sohrab Shah Peter Eirew
BCCH Rod Rassekh Rebecca Deyell Anna Lee Coleen Jantzen Coleen
Fitzgerald
GSC Steven Jones Jianghong An Carolyn Ch’ng Robin Coope Richard Corbett Katty Cruz Nisa Dar Alexandra Fok Jasleen Grewal An He Katayoon Kasaian Heather Kirk Sreeja Leelakumari Yvonne Li William Long
SFU Peter Chow-White
We gratefully acknowledge the participation of our patients and families and the generous support of the BC Cancer Foundation.
Tina Wong Natasja Wye Yongjun Zhao Kelsey Zhu
19
Poster #10

THANK YOU!