using virtual care and remote monitoring to engage people
TRANSCRIPT

Using Virtual Care and Remote Monitoring to Engage People With
DiabetesDawn Noe, RDN, LD, CDCES;
Diana Isaacs, PharmD, BCPS, BC-ADM, BCACP, CDCES, FADCES, FCCP

Dawn NoeRDN, LD, CDCESFormer Remote Monitoring Program Coordinator at Cleveland Clinic Diabetes Center
Diana Isaacs PharmD, BCPS, BC-ADM, BCACP, CDCESCGM and Remote Monitoring Program Coordinator Clinical Pharmacy Specialist Cleveland Clinic Diabetes Center

Disclosure to Participants• Dawn Noe, RDN, CDCES – No COI/Financial Relationship to disclose • Diana Isaacs, PharmD, CDCES-Speaker’s Bureau/consultant: Medtronic, Dexcom, Abbott,
Lifescan, Novo Nordisk, Xeris, Insulet
Objectives•Describe how remote technology is used to optimize care for people with diabetes
•Discuss different types of connected devices and platforms for remote technology
•Demonstrate how different members of the diabetes team utilize remote monitoring and virtual care

Remote Technology and Diabetes Care
• Technology is enabling us to connect with PWD in new ways
• PWD are asked to keep track of health data
• Remote diabetes services could include:
• Virtual Visits/Telehealth • Remote Physiologic Monitoring • Chronic Care Management Diabetes related education/coaching/support can be offered as part of these services

Patient Generated Health Data and Diabetes Care: Is it effective?
To Improve A1C:
• Communication• Patient-generated health data• Education• Feedback
Greenwood, D. A., Gee, P. M., Fatkin, K. J., & Peeples, M. (2017). A Systematic Review of Reviews Evaluating Technology‐Enabled Diabetes Self‐Management Education and Support. Journal of Diabetes Science and Technology, 11(5), 1015–1027.

Virtual Diabetes Care • Individual Appointments or Group Visits
• Observe living conditions• Do they live alone?• Can they afford medications?• Do they have access to enough food?• Meet family members, caretakers and even
pets
• Builds a strong rapport by letting you see more of their daily life

Virtual Diabetes Care Examples of HIPAA Compliant Virtual Platforms
• Skype for Business / Microsoft Teams• Updox• VSee• Zoom for Healthcare• Doxy.me• Google G Suite Hangouts Meet• Cisco Webex Meetings / Webex Teams• Amazon Chime• GoToMeeting• Spruce Health Care Messenger• American Well • Beam Health
UpdoxBeam Health
https://www.hhs.gov/hipaa/for-professionals/special-topics/emergency-preparedness/notification-enforcement-discretion-telehealth/index.html•Accessed: 06-07-2020

MedStar Diabetes Boot Camp Example • Smart Meter (cellular enabled)• PWD were seen in person for 2 visits to learn meter
and basic DSMES• Transitioned to virtual clinic
• Daily BG review• Virtual visits• Rx intensification & management • Ongoing DSMES
• CDCES (RD, RN, PharmD, NP) participated in medication management based on an approved medication algorithm
Magee MF, Baker KM, Fernandez S, Huang C‐C, Mete, M; Montero AR, Nassar CM, Sack PA, Smith KM, Youssef G, Evans SR. Redesigning Ambulatory Care Management for Uncontrolled Type 2 Diabetes: A Prospective Cohort Study of the Impact of a Boot Camp Model onOutcomes. BMJ Open Diabetes Research & Care Nov 2019, 7 (1) e000731; DOI: 10.1136/bmjdrc‐2019‐000731

MedStar Health Diabetes Pathway Boot Camp
Discharge to Primary Care
Visits 1 and 2‐ In person ”human engagement”‐ DM assessment‐ DSMES/MNT‐ DM Rxs management‐ Realtime BG meter
‐ Daily BG review‐ Virtual visits‐ Rx intensification & mngt‐ DSME
‐ Care integration.
DiabetesHigh Risk –High Cost :A1C > 9
Virtual Clinic Visits
Provider support
PCP referral
Timely
Magee MF, Baker KM, Fernandez S, Huang C‐C, Mete, M; Montero AR, Nassar CM, Sack PA, Smith KM, Youssef G, Evans SR. Redesigning Ambulatory Care Management for Uncontrolled Type 2 Diabetes: A Prospective Cohort Study of the Impact of a Boot Camp Model on Outcomes. BMJ Open Diabetes Research & Care Nov 2019, 7 (1) e000731; DOI: 10.1136/bmjdrc‐2019‐000731

MedStar Diabetes Population and Results • Adults with T2DM• A1C >9%• 79% African American• 63% Female • 59% Medicare or Medicaid insured• Mean age: 56 years • PCP/Endo approval for program • Willing and able to participate in program• Established patient in the healthcare
system
Magee MF, Baker KM, Fernandez S, Huang C‐C, Mete, M; Montero AR, Nassar CM, Sack PA, Smith KM, Youssef G, Evans SR. Redesigning Ambulatory Care Management for Uncontrolled Type 2 Diabetes: A Prospective Cohort Study of the Impact of a Boot CampModel on Outcomes. BMJ Open Diabetes Research & Care Nov 2019, 7 (1) e000731; DOI: 10.1136/bmjdrc‐2019‐000731
90 Day

Team Based Virtual Diabetes Care:Pharmacist• Virtual home visit to see:
• How patients are storing medications• If they have duplicates medications in
the house or varying dosages • How they carry their medication
• Virtually observe medication injection technique
• Analyze and adjust medications between physician visits using practice agreement
• Remote monitoring: glucose, BP, review pump and smart pen uploads for missed insulin doses
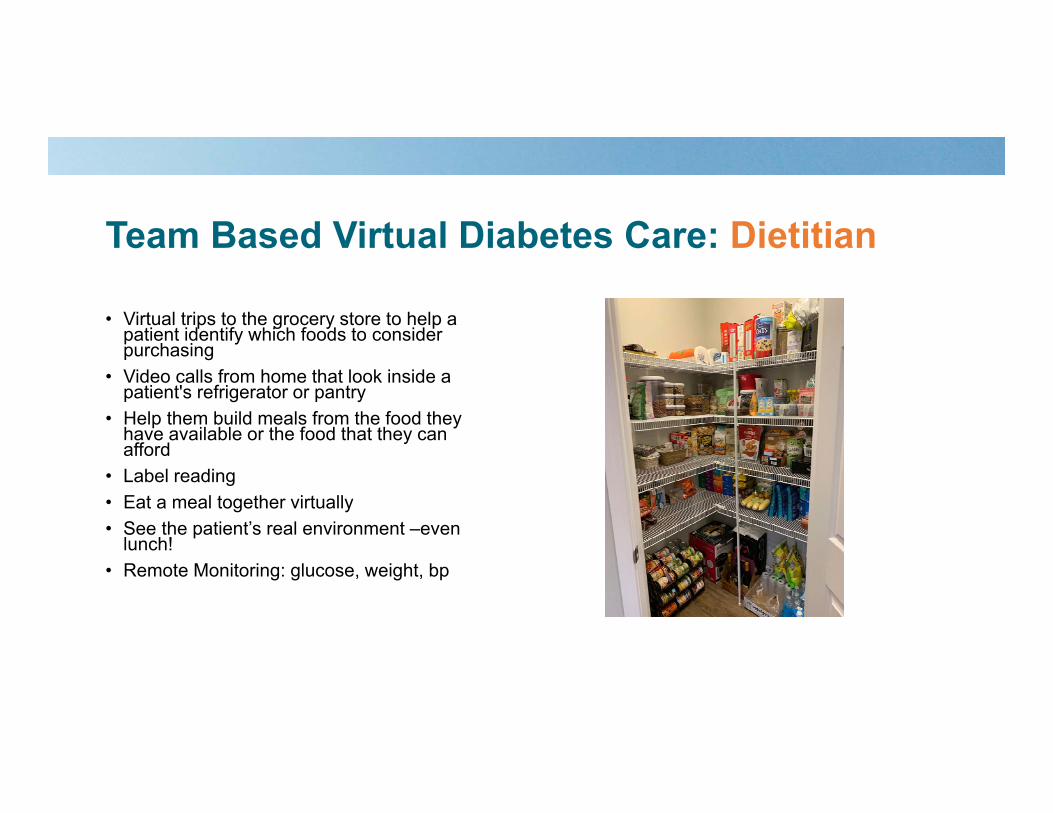
Team Based Virtual Diabetes Care: Dietitian
• Virtual trips to the grocery store to help a patient identify which foods to consider purchasing
• Video calls from home that look inside a patient's refrigerator or pantry
• Help them build meals from the food they have available or the food that they can afford
• Label reading • Eat a meal together virtually• See the patient’s real environment –even
lunch! • Remote Monitoring: glucose, weight, bp

Team based Approach to Virtual Care: Diabetes Care and Education Specialist • Diabetes Education Group Classes:
• Share the screen, view reports, use PowerPoint • Monitoring:
• Virtually review blood sugar patterns• Can’t forget the meter at home - No longer a
problem!• Check a blood sugar during the visit
• Problem solving: • Pump or CGM sites• Observing what items they keep around the house
to treat hypoglycemia – and where (downstairs versus next to the bed, etc.)
• Healthy Eating: • Food label reading with foods from the pantry
• Remote Monitoring: glucose, weight, bp
Photo Credit: Janet Zappe and Elizabeth Snyder from Ohio State University Medical Center

Team based Approach to Virtual Care: Exercise Physiologist• Create exercise prescriptions for
homebound patients • Virtual group fitness classes• Virtual personal training• Observe areas in patients home to
perform exercise.• Stairs• Chairs• Slippery surfaces vs. stable flooring
• Home exercises and equipment• Soup cans or other “weights”
• Remote monitoring: tracking steps/activity

Team based Approach to Virtual Care: Psychologist• Depression and diabetes
distress • Changing health behaviors• Relationship challenges• Teach/practice mental health
wellness • Stress management• Deep breathing • Positive thinking
• Online option may make this service more approachable!

Technology for Education, Coaching, and Support
• In traditional health care, people are told what to do (lose weight, eat healthier, check their blood sugar 3 times per day, etc.)
• However, they don’t have the assistance along the way.
• Coaches ASK questions (similar to Motivational Interviewing), ENCOURAGE and SUPPORT
• Technology increases potential access to this behavioral support ‐ even if it is telephonic or text support
• Minimum “dose” of coaching required to continue progress after intervention and the potential for technology to provide effective ongoing automated reinforcement of behavior change.
Young HM, Miyamoto S, Dharmar M, Tang-Feldman Y. Nurse Coaching and Mobile Health Compared With Usual Care to Improve Diabetes Self-Efficacy for Persons With Type 2 Diabetes: Randomized Controlled Trial. JMIR Mhealth Uhealth. 2020;8(3):e16665. Published 2020 Mar 2. doi:10.2196/16665

Virtual Shared Medical Appointments (VSMA)
•What is it?• Virtual group appointment aimed to help and support people with diabetes
•Who is involved?• Physician •Members of the multidisciplinary team • People with diabetes!

Virtual Shared Medical Appointments (VSMA)
• “Zoom fatigue”• Anxiety or fear of being on
camera• Technical difficulties• Health disparities
• Group support• All-in-one visit• Multidisciplinary team at
each visit• Convenience • Time
Advantages Challenges

Remote Physiologic Monitoring• Monitoring patient’s treatment plan remotely
• FDA-defined digital device
• Allows patient’s physiological data to be both collected and wirelessly transmitted to provider
• Provider virtually furnishing these “designated care management services” based on data received to beneficiary outside of in office visit.
•Sources: www.cms.gov•https://codingintel.com/remote-physiologic-monitoring-treatment-management-services-remote-monitoring/

Remote Physiologic Monitoring – Medicare Billing Codes Codes/Service National
non‐facility payment
National facility payment
Billing Providers Rendering Providers Diagnoses
99453
99454
99457
99458
$18.77
$62.44
$51.61
$42.22
$18.77
$62.44
$32.84
$32.84
MD, DO, NP, PA, CNS, Clinical nurse midwife
• MD, DO, NP, PA, CNS, Clinical nurse midwife
• Clinical staff employed by billing provider (as incident to physician’s services)
Ex: RNs, RDs, MAs, etc.(subject to scope of practice and state licensure law)
Chronic diseases: CVD, COPD,Depression, Diabetes, HTN, etc.
Important Notes:
• Only 1 Condition Needed
• Order from Provider
• Informed consent required!
www.cms.govhttps://codingintel.com/remote-physiologic-monitoring-treatment-management-services-remote-monitoring/

Remote Physiologic Monitoring:Medicare Billing Codes
• 99453 ‐ initial set‐up and patient education on use of equipment
• 99454 – equipment: “expense” related to practice purchasing RPM device
2020 wRVUNational
non‐facility paymentNational facility payment
0.00 $18.77 $18.77
2020 wRVUNational
non‐facility paymentNational facility payment
0.00 $62.44 $62.44
Sources: www.cms.govhttps://codingintel.com/remote-physiologic-monitoring-treatment-management-services-remote-monitoring/Mary Ann Hodorowicz: Certified Endocrinology Coder https://bit.ly/HowToBillForRPMLikeAPro

Remote Physiologic Monitoring: Medicare Billing Codes
99457
2020 wRVUNational
non‐facility paymentNational facility payment
0.61 $51.61 $32.84
• 20 minutes or more of clinical staff, physician, and/or other qualified healthcare professional time in a calendar month requiring interactive communication with the patient or caregiver during a month
• 1 x per each calendar month regardless of number of parameters monitored
• Do not bill with code 99091• Do not bill with CGM code 95249,95250 or
95251• Obtain order and beneficiary's written,
signed consent and document in medical record
• For “Incident to Physician Services” billing:
Change from provider’s direct supervision to general supervision (GS)
Sources: www.cms.govhttps://codingintel.com/remote-physiologic-monitoring-treatment-management-services-remote-monitoring/Mary Ann Hodorowicz: Certified Endocrinology Coder https://bit.ly/HowToBillForRPMLikeAPro

Remote Physiologic Monitoring:Medicare Billing Codes
994582020 wRVU
National
non‐facility paymentNational facility payment
0.61 $42.22 $32.84
New Code in 2020 Remote physiologic monitoring treatment management services, clinical staff/physician/other qualified health care professional time in a calendar month requiring interactive communication with the patient/caregiver during month
additional 20 minutes*
2 x per each calendar month regardless of number of parameters monitored
•Sources: www.cms.gov•https://codingintel.com/remote‐physiologic‐monitoring‐treatment‐management‐services‐remote‐monitoring/•Mary Ann Hodorowicz: Certified Endocrinology Coder https://bit.ly/HowToBillForRPMLikeAPro
Diabetes Related Health Data
BGM/CGM Blood Pressure Weight
Insulin Pumps and Smart Insulin
Pens
StepCounters/Activity
Trackers

Remote Glucose Monitoring • Glooko • Tidepool • DarioHealth• Map4Health• OneDrop• iGlucose• Livongo• CGM• Pumps/Smart
Pens • And more…
Questions to ask!Glucose:
More than one meter CGM
Education Component Coaching Features
Texting/Video/Automatic Reminders to the patient
Goal Setting and Tracking Meal SharingPeer Forums/Community Population Health Data/Alerts/Analytics EHR Integration Require Smart Phone Use/AppCost

Technology for Remote MonitoringSmart Meters – No app required!
• Livongo• iGlucose• Telcare

Glooko
#ADCES20
• Automatically sinks some meter, smart pen and CGM data
• Compatible with fitness trackers: ex, Fitbit, Strava, iHealth, runkeeper
• Track medication use, set reminders• Automatically shared with clinic via
online portal• Requires a subscription by individual
patient or through the clinic• Possible integration with EMR• Variety of cost structures depending
on services

Tidepool• Compatible with most insulin
pumps and CGM except Eversense
• Compatible with many glucose meters
• Data uploaded on Mac or PC and can be shared with the clinic
• Tidepool mobile app• Track meals, exercise, daily events
Free

Data Management Systems for Glucose MonitoringSystem Website What it DownloadsGlooko www.glooko.com Omnipod, Tandem, Dexcom, Eversense, MANY glucose
meters
Dexcom Clarity https://clarity.dexcom.com Dexcom
LibreView www.libreview.com Freestyle Libre
T:Connect https://tconnecthcp.tandemdiabetes.com/hcp_account
Tandem insulin pumps including basal IQ (dexcom data included)
Carelink https://carelink.medtronic.com/ Medtronic insulin pumps and Medtronic CGM
Tidepool https://tidepool.org/ All insulin pumps, Libre, Dexcom, Guardian CGM, many glucose meters
Eversense Data Management System
https://www.eversensedms.com/ Eversense
In Pen Insights Report
NA (InPen App) InPen, DexCom , Guardian Connect

Weight Management: Bluetooth Smart Scale

Getting Data Into Your EMR

Remote Monitoring Case Study • Referral for remote glucose monitoring
program from provider.
• Attempted connected meter – but patient preferred to write down blood sugars
Communication through EMR:
“Hi Tom, Thank you for checking and sending your blood sugars!
Here is the chart that we discussed and how we saw patterns today. Let me know what questions you have. I’ll check in next week!”
Dawn Noe, CDCES

Remote Monitoring Case Study
Scanning blood sugars 6‐8 times per day with flash CGM
Ate 2 Eggs and 1 piece of toast for breakfast
Afternoon snacks
Decided to take a walk before dinner

Remote Monitoring Case Study Near real time communication with diabetes care team to maximize care for diabetes.
April 6: Hi Dawn,
Can I take insulin before bed when my blood
sugars are high? They are all over 250 even though
I walk after dinner.
April 6: Hi Tom. You theoretically
could, but I'm worried about you taking it right before bed and having your blood sugar go too low when you are sleeping. The doctor would like you to increase your
mealtime insulin dose with dinner. Please start taking 5 units with dinner. Great job
on the walking! April 9: Hi Dawn,
I’ve been trying 5 units with dinner and it has been working well.
April 9: Hi Tom.
Awesome, Glad to hear it!

A Connected Pen Case
•Ana is a 24 year old female diagnosed with type 1 DM 1 year ago. She wears rtCGM and uses a connected pen
•DM1 doses• Insulin glargine 6 units daily • Insulin aspart 1-4 units at meals (7 units/day avg)
• She worries a lot about hypoglycemia• She’s afraid to move out and live on her own because of it

Ana’s Glooko Report

CGM and Insulin Pen Data

Plan•Discuss fear of hypoglycemia
• Past events? Ensure glucagon prescription• Increase insulin glargine to 7 units•Track carbohydrates, work toward IC ratio and correction factor
•Pre-bolus•Continue remote monitoring, follow-up virtual visit in 2 weeks

Patient Case: Hospital Discharge• George is a 54-year-old male who presents to the ED with
hyperglycemia. He experienced increased thirst and frequent urination over the past 2 weeks. Glucose was checked and was 578. He was admitted for hospital for 3 days.
• Diagnosed with new onset type 2 diabetes• In the hospital, he received diabetes education• Started on metformin, glimepiride• Consult to endocrinology• A1C=9.6%• 305lbs, BMI=36.4kg/m2

Endocrinology Telehealth Visit• Endocrinology via Telehealth• 2 days post-discharge• The patient's current meal plan
• Breakfast - eggs, pancakes, hash brown potato• Lunch - burger, no bread, baked chips • Dinner - steak, brussels sprouts
• Stopped sodas and Gatorade• Enjoys sweets - but cut down• Has a sedentary job • Walks 2-3 miles a day

Endocrinology Telehealth Visit• Frequency of glucose monitoring: 2 x daily • BG Values: 300-450
Plan: • Start Insulin glargine 12 units daily • Insulin aspart 4 units TID a.c. • Continue metformin 500mg twice daily • Stop glimepiride• Consults placed: diabetes education, pharmacy• Antibody testing

Next Day Diabetes Education Telehealth Visit• Patient picked up insulin from the pharmacy• Met with diabetes care and education specialist for insulin injection technique
and discussion of injection sites


1 Week Later: Pharmacist Visit• Frequency of Glucose Monitoring: Two times a Day• BG Values: all in the 200-300 range• Labs not done yet
• “Is there a way to monitor my sugars without poking my fingers all the time?”
Plan:-Increase insulin glargine to 14 units daily -Increase insulin aspart to 6 units at meals-Rx to pharmacy for CGM

Starting CGM

Linking to the Clinic’s Remote Platform• Smart phone app downloaded• Synced with clinic’s platform through share code• Data automatically available for virtual visits and/or remote monitoring

Pharmacist Telehealth Follow-Up: 2 Weeks

Follow Up: Continued• George has made a ton of lifestyle changes
• Lost 8 lbs since diagnosis• Antibodies were normal, diagnosis of type 2 DM confirmed• Plan:
• Titrate up metformin• Transition to non‐insulin medications• Continue DCES follow‐up
• And all of this was done remotely!

Key TakeAways• Remote monitoring provides diabetes monitoring, care, education, and
support to people with diabetes when they need it
• Uses tools to monitor and support patient progress and communicate via text, email or video
• The person with diabetes should be at the center of everything
• A successful program should have analytics and notifications to identify and address problematic trends with proactive and population health approaches