utility of morphometry in the study of donor and protocol biopsies d. serón servicio de nefrología...
Post on 19-Dec-2015
219 views
TRANSCRIPT
Utility of morphometry in the study of donor and protocol
biopsies
D. SerónServicio de Nefrología Hospital BellvitgeBarcelona
Morphometry
DisadvantagesAdvantages
When is morphometry redundant?
When may it be useful?
When is it necessary?
TopicsRedundant
Morphometry applied to the study of donor biopsies
Potential utilityMophometric evaluation of protocol biopsies in clinical trials
NecessaryGlomerular adaptation after renal transplantation
TopicsRedundant
Morphometry applied to the study of donor biopsies
Potential utilityMophometric evaluation of protocol biopsies in clinical trials
NecessaryGlomerular adaptation after renal transplantation
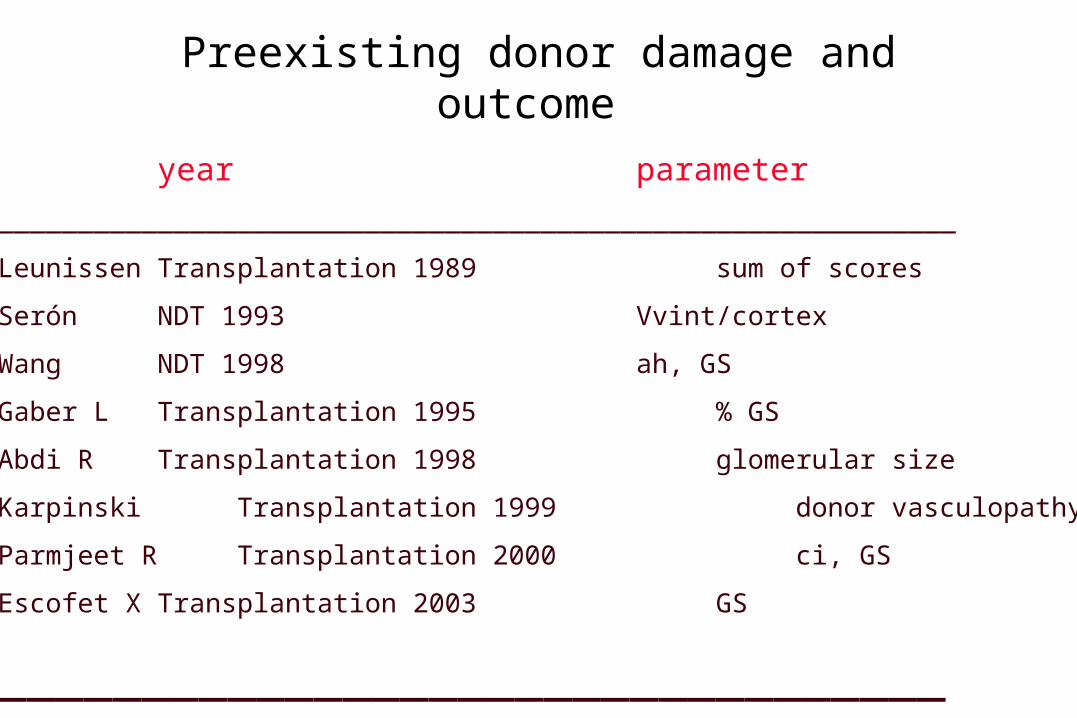
Preexisting donor damage and outcome
year parameter
____________________________________________________________
Leunissen Transplantation 1989 sum of scores
Serón NDT 1993 Vvint/cortex
Wang NDT 1998 ah, GS
Gaber L Transplantation 1995 % GS
Abdi R Transplantation 1998 glomerular size
Karpinski Transplantation 1999 donor vasculopathy
Parmjeet R Transplantation 2000 ci, GS
Escofet X Transplantation 2003 GS
_________________________________

Is there any advantage in the morphometric evaluation of
donor biopsies?

Evaluation of donor biopsies (June 2000-Dec 2001, N = 77 (10 glom, 1 art)
Banff criteria
cgcictcvahmm
Quantitative parameters
% glomerulosclerosis
Vvint/c (%)Vvglom/c (%)Vg x 106 3
Vvintima/artery
Lopes JA et al. Kidney Int 2005; 67: 1595

Results (1)
0
20
40
60
80
100
120
140
-5 0 5 10 15 20 25 30 35 40 45 50
Glomerulosclerosis (%)
CrCl at 3 m (mL/min)
R=0.52P<0.001

Results (2)
0
20
40
60
80
100
120
140
0 1 2
ci
CrCl at 3 m (mL/min)
Rho = 0.41P = 0.005
0
20
40
60
80
100
120
140
-,25 0 1 2
ct
Rho = 0.38P = 0.0014
CrCl at 3 m (mL/min)
0
20
40
60
80
100
120
140
0 1 2
cv
CrCl at 3 m (mL/min)
Rho = 0.48P < 0.001
0
20
40
60
80
100
120
140
0 1 2 3 4 5 6
ci+ct+cv
CrCl at 3 m (mL/min)
Rho = 0.51P < 0.001
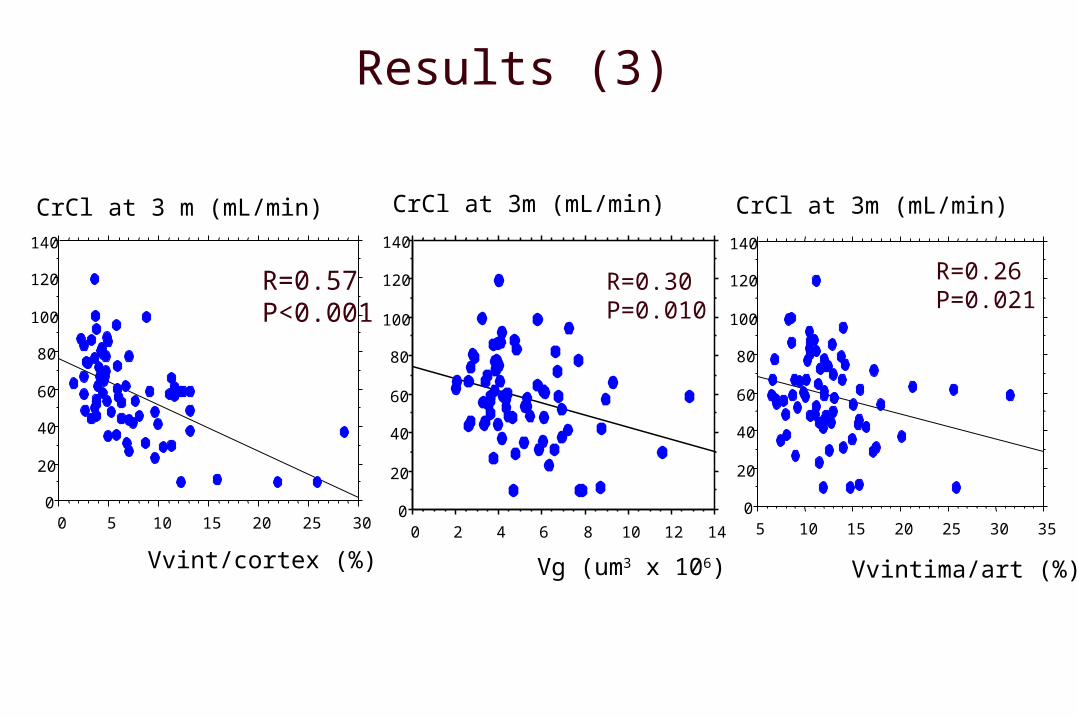
Results (3)
0
20
40
60
80
100
120
140
0 2 4 6 8 10 12 14
Vg (um3 x 106)
CrCl at 3m (mL/min)
R=0.30P=0.010
0
20
40
60
80
100
120
140
CrCl at 3 m (mL/min)
0 5 10 15 20 25 30
Vvint/cortex (%)
R=0.57P<0.001
CrCl at 3m (mL/min)
0
20
40
60
80
100
120
140
5 10 15 20 25 30 35
Vvintima/art (%)
R=0.26P=0.021
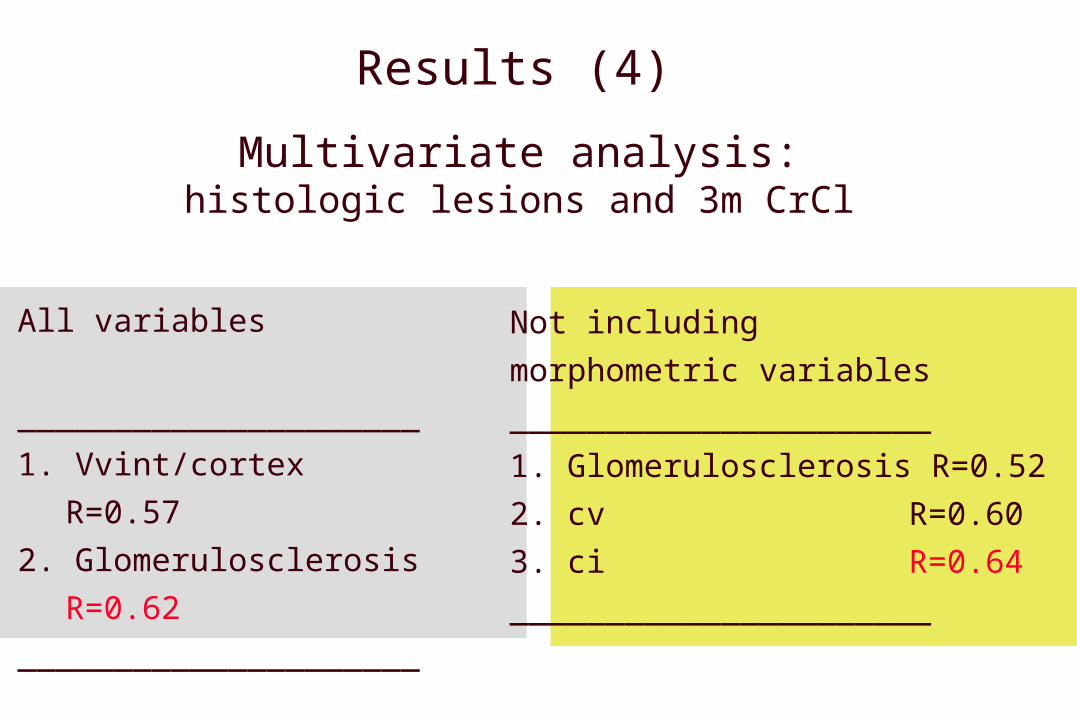
Results (4)
Multivariate analysis:histologic lesions and 3m CrCl
All variables
_____________________
1. Vvint/cortex
R=0.57
2. Glomerulosclerosis
R=0.62
_____________________
Not including
morphometric variables
______________________
1. Glomerulosclerosis R=0.52
2. cv R=0.60
3. ci R=0.64
______________________

Conclusions
Morphometric evaluation of donor biopsies does not improve the prediction of outcome

TopicsRedundant
Morphometry applied to the study of donor biopsies
Potential utilityMophometric evaluation of protocol biopsies in clinical trials
NecessaryGlomerular adaptation after renal transplantation

CAN and sequential protocol biopsies
Donor biopsies 15%4th month protocol bx 42 %1st year protocol bx 52%
% CAN
0 3 6 9 12 m
50
25
0
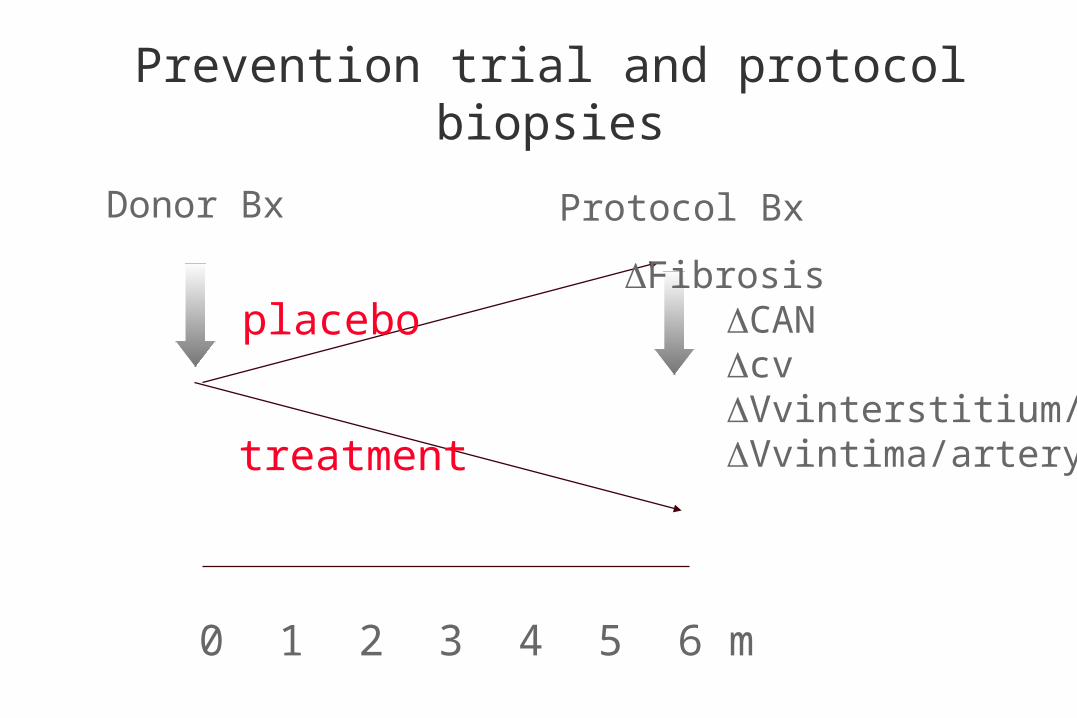
Prevention trial and protocol biopsies
0 1 2 3 4 5 6 m
Donor Bx Protocol Bx
placebo
treatment
Fibrosis CAN cv Vvinterstitium/c Vvintima/artery
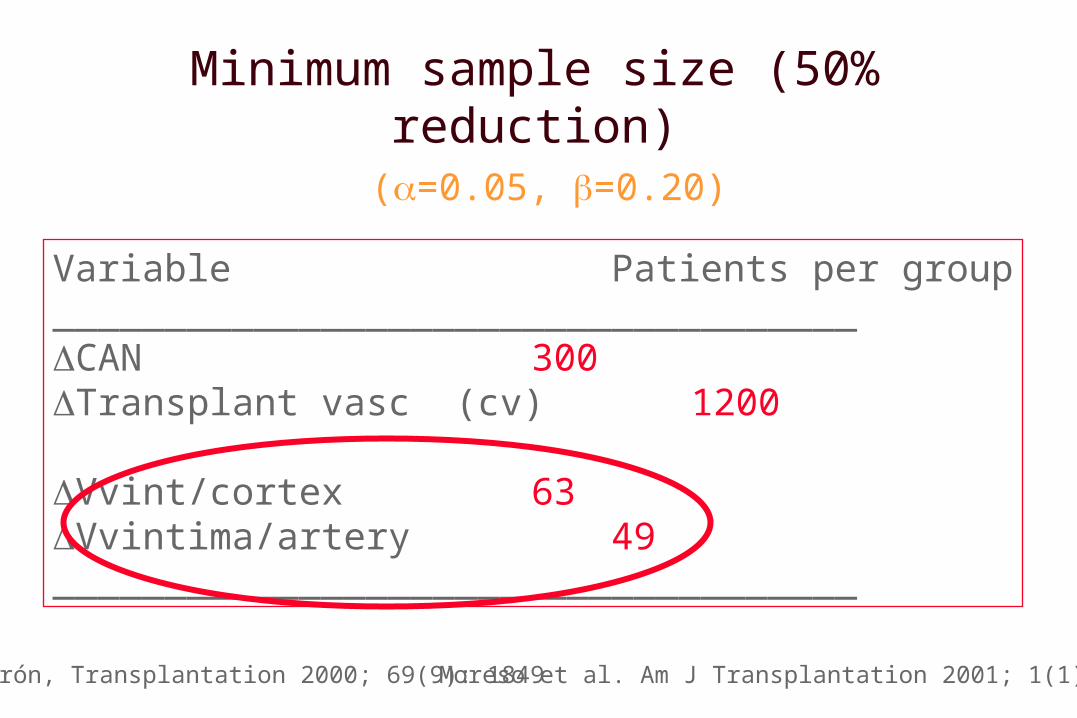
Minimum sample size (50% reduction) (=0.05, =0.20)
Variable Patients per group____________________________________CAN 300Transplant vasc (cv) 1200
Vvint/cortex 63Vvintima/artery 49____________________________________
Serón, Transplantation 2000; 69(9): 1849Moreso et al. Am J Transplantation 2001; 1(1): 82
Conclusions
Morphometric evaluation of protocol biopsies in trials aimed to prevent CAN may allow to reduce
minimum sample size

TopicsRedundant
Morphometry applied to the study of donor biopsies
Potential utilityMophometric evaluation of protocol biopsies in clinical trials
NecessaryGlomerular adaptation after renal transplantation
Glomerular number (Ng)Disector /fraccionator (n=56)
0.23-1.82 x 106
Hughson M et al Kidney Int 2003; 63: 2113

Ng and Vg in humans
Ng/Vg/BSA
Hoy WE et al, Kidney Int Suppl 2003; 83, S31
Renal adaptation after transplantation
adaptation
Ng
Vg

Ng
RadiologyHistology
Morfometry
New parameters
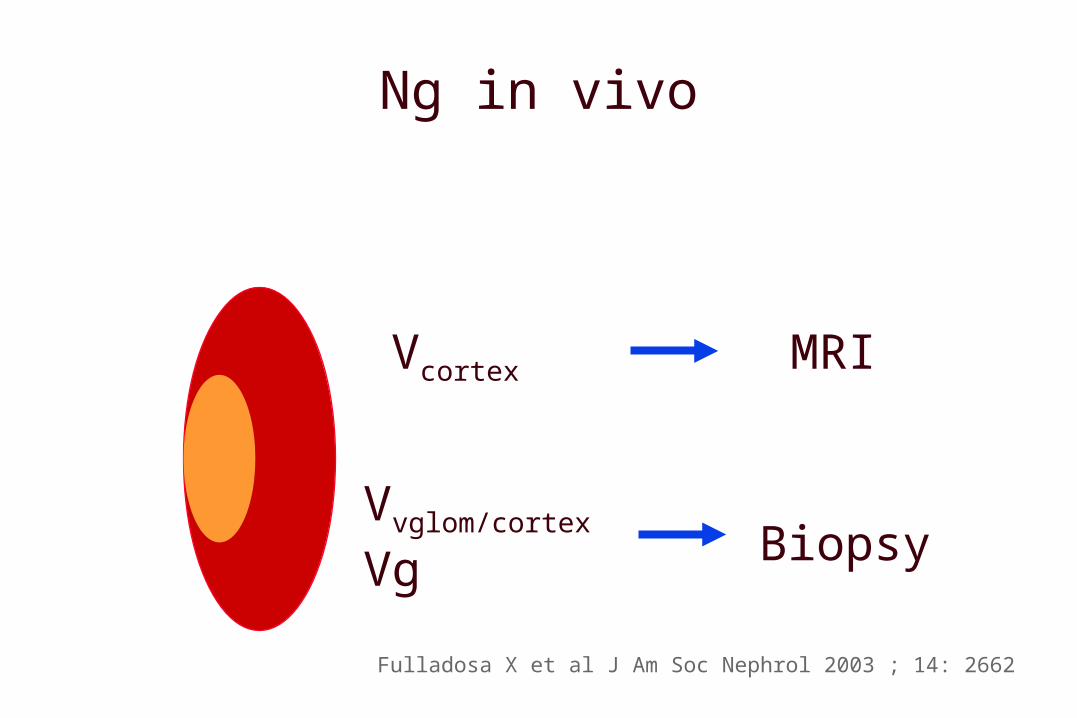
Ng in vivo
Vcortex MRI
Vvglom/cortex Vg Biopsy
Fulladosa X et al J Am Soc Nephrol 2003 ; 14: 2662
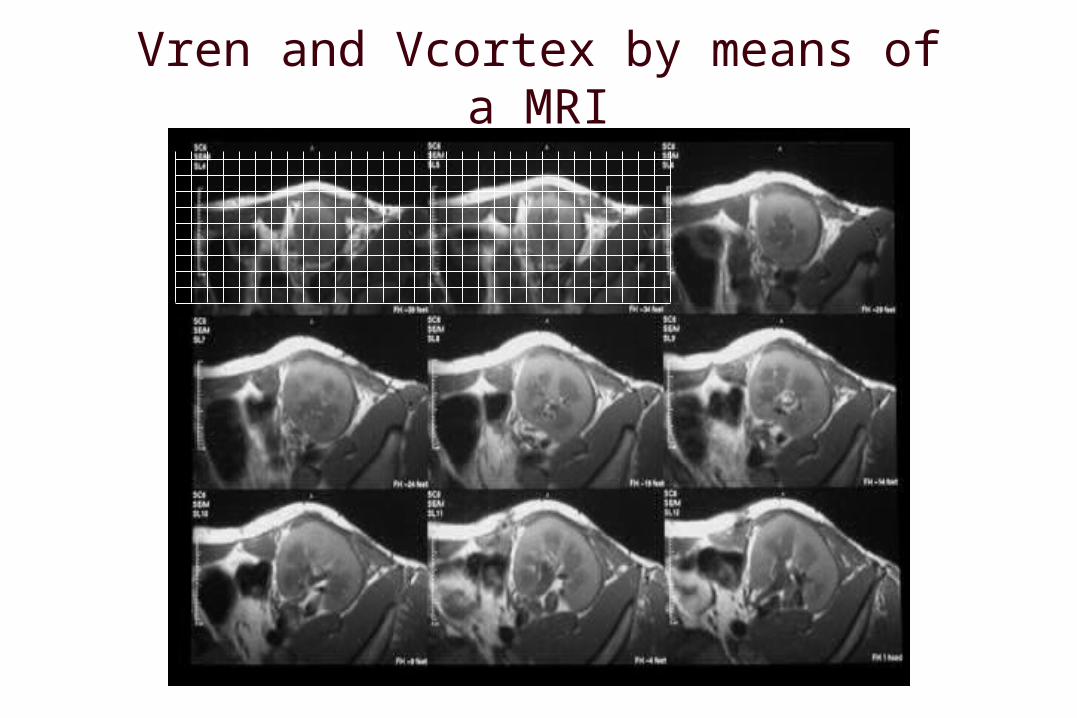
Vren and Vcortex by means of a MRI

Volumen renal VrenVolumen cortical Vcort
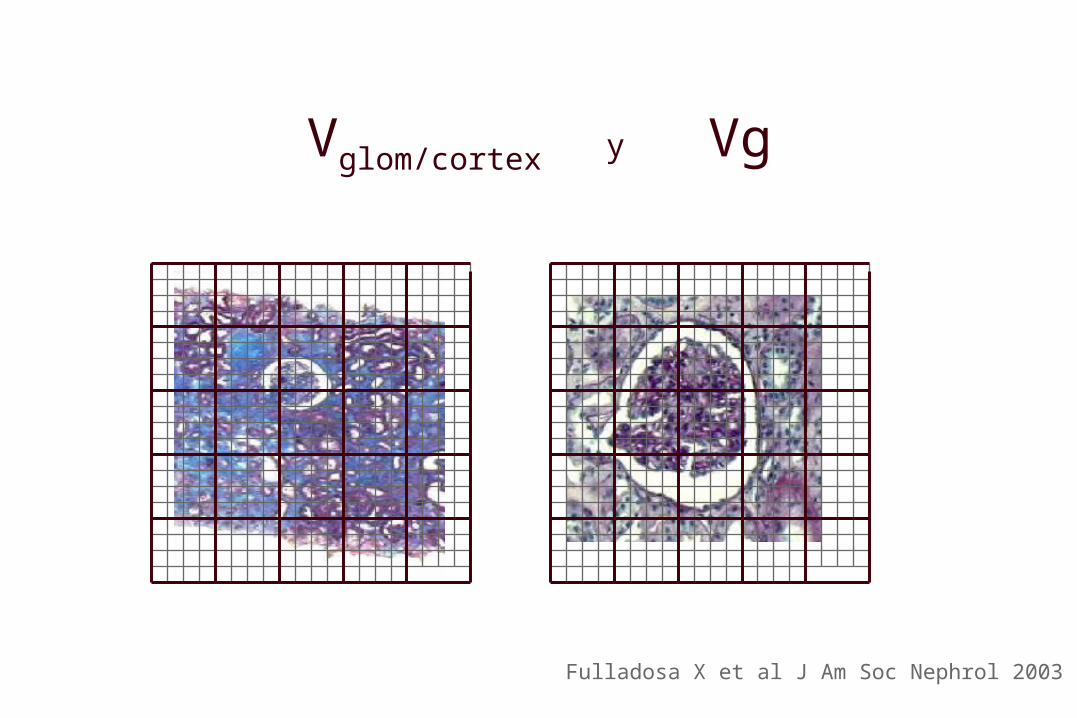
Vglom/cortex y Vg
Fulladosa X et al J Am Soc Nephrol 2003
Estimación del número de
Vcortex * Vvglom/cortex Ng = __________________
Vg

Characteristics of patientsSCr < 200 mmol/l and proteinuria < 1g/24h
4m protocol biopsy (n=39)Mean SD ______________________________________ N 39 Donor age 38 18Donor sex (male / female) 26 / 13Recipient age 46 14Recipient sex (male / female) 24 / 15Recipient BSAa (sqm) 1.74 0.19Cold ischemia time (hours) 20 5 Delayed graft function (no / yes) 37 / 2Serum Creatinine (mol/l) 12330Proteinuria g/day 0.38 0.47______________________________________
Fulladosa X et al J Am Soc Nephrol 2003; 14: 2662

Relationship between Ng and GFR
0
20
40
60
80
100
120
0 0.4 0.8 1.2 1.6
Ng-W&G (x 106)6
GFR
(m
l/m
in)
Fulladosa X et al J Am Soc Nephrol 2003; 51: 310
Ng is a major determinant of GFR
2GFR = 9 Ng

Glomerular enlargement after transplantation
(n=41)
Donor biopsy Recipient biopsyVg
0 4
Alperovich G et al, AJT 2004; 4 : 650

Vg after transplantationVg
Donor Biopsy Recipient Biopsy p_______________________________________________Ah 0.150.42 0.290.56 NScg 0.100.30 0.15 0.36 NSci 0.190.45 0.49 0.64 0.0006ct 0.15 0.42 0.49 0.67 0.0002cv 0.02 0.16 0.19 0.60 0.087Vg 4.1 1.4 5.1 2.40.021_______________________________________________
Alperovich G et al, AJT 2004; 4 : 650
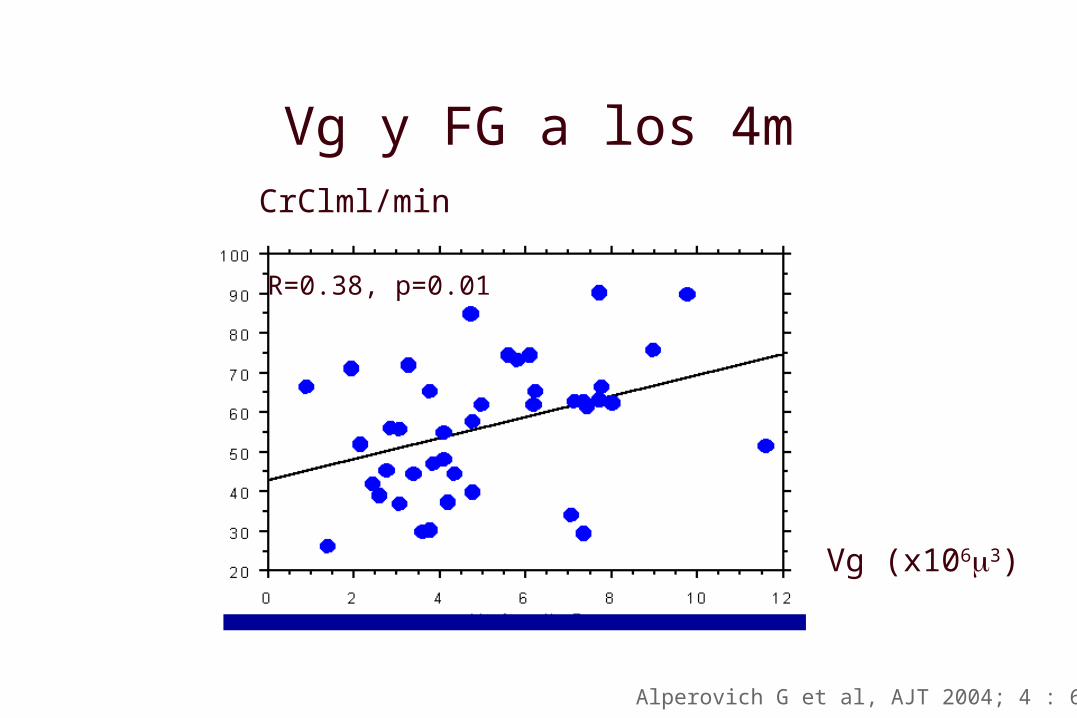
Vg y FG a los 4mCrClml/min
Vg (x1063)
Alperovich G et al, AJT 2004; 4 : 650
R=0.38, p=0.01

Glomerular enlargement may be
a necessary condition to achieve
a good renal function
Epidemiological paradox
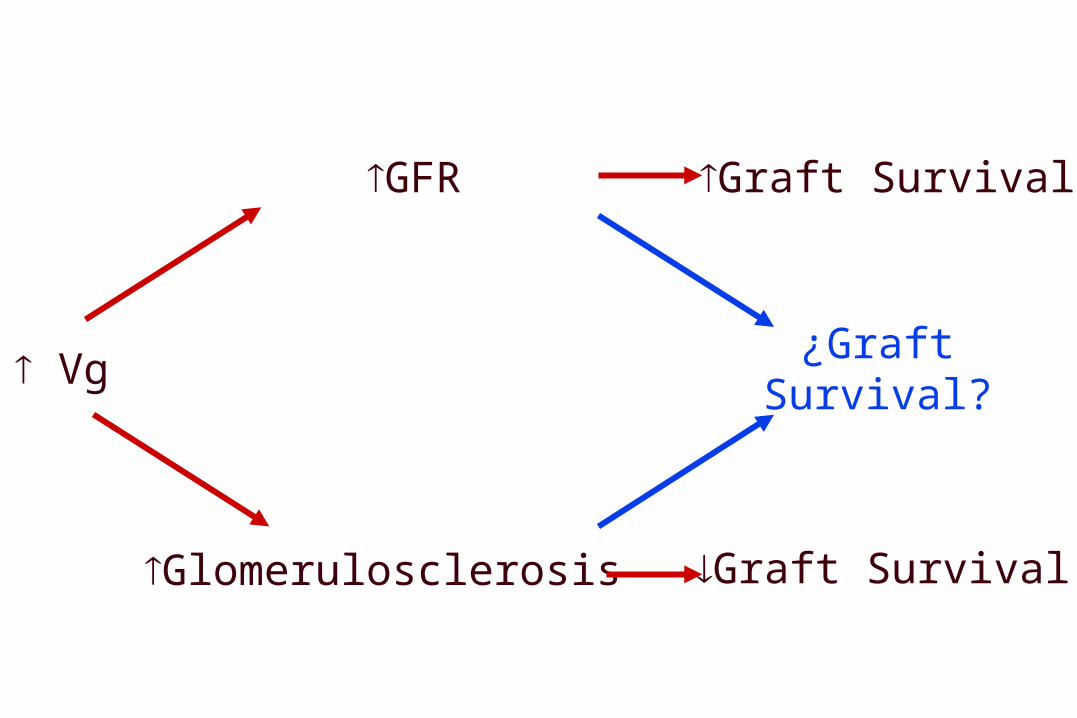
Vg
GFR Graft Survival
Glomerulosclerosis Graft Survival
¿Graft Survival?
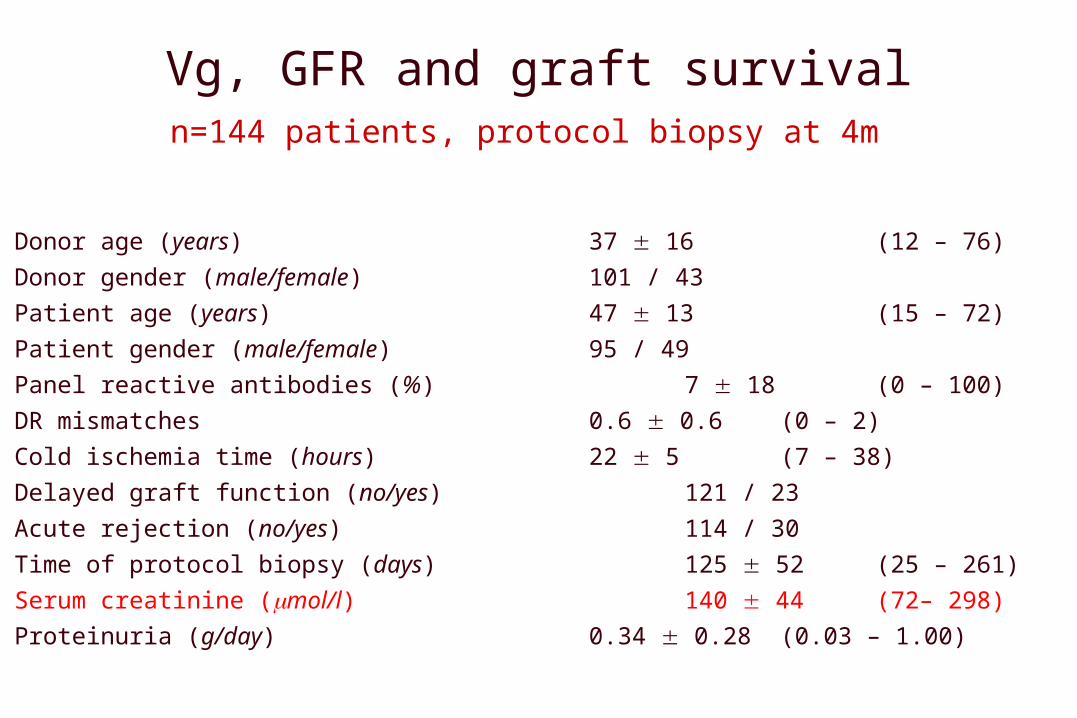
Vg, GFR and graft survivaln=144 patients, protocol biopsy at 4m
Donor age (years) 37 16 (12 – 76)
Donor gender (male/female) 101 / 43
Patient age (years) 47 13 (15 – 72)
Patient gender (male/female) 95 / 49
Panel reactive antibodies (%) 7 18 (0 – 100)
DR mismatches 0.6 0.6 (0 – 2)
Cold ischemia time (hours) 22 5 (7 – 38)
Delayed graft function (no/yes) 121 / 23
Acute rejection (no/yes) 114 / 30
Time of protocol biopsy (days) 125 52 (25 – 261)
Serum creatinine (mol/l) 140 44 (72– 298)
Proteinuria (g/day) 0.34 0.28 (0.03 – 1.00)
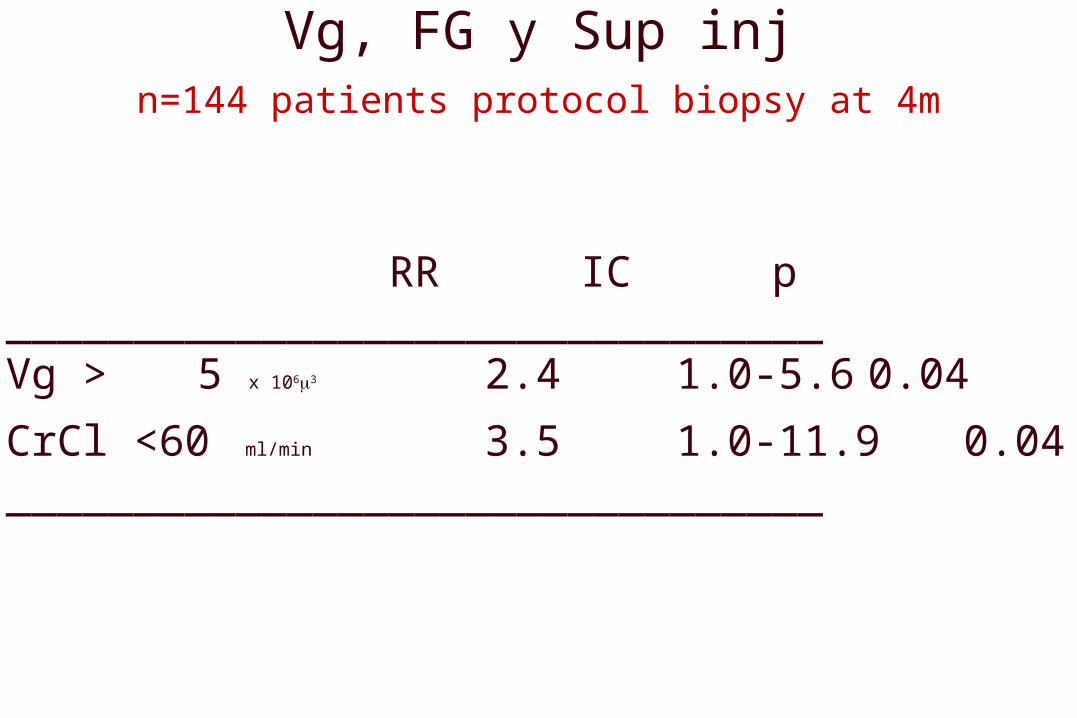
Vg, FG y Sup injn=144 patients protocol biopsy at 4m
RR IC p________________________________Vg > 5 x 1063 2.4 1.0-5.6 0.04
CrCl <60 ml/min 3.5 1.0-11.9 0.04________________________________
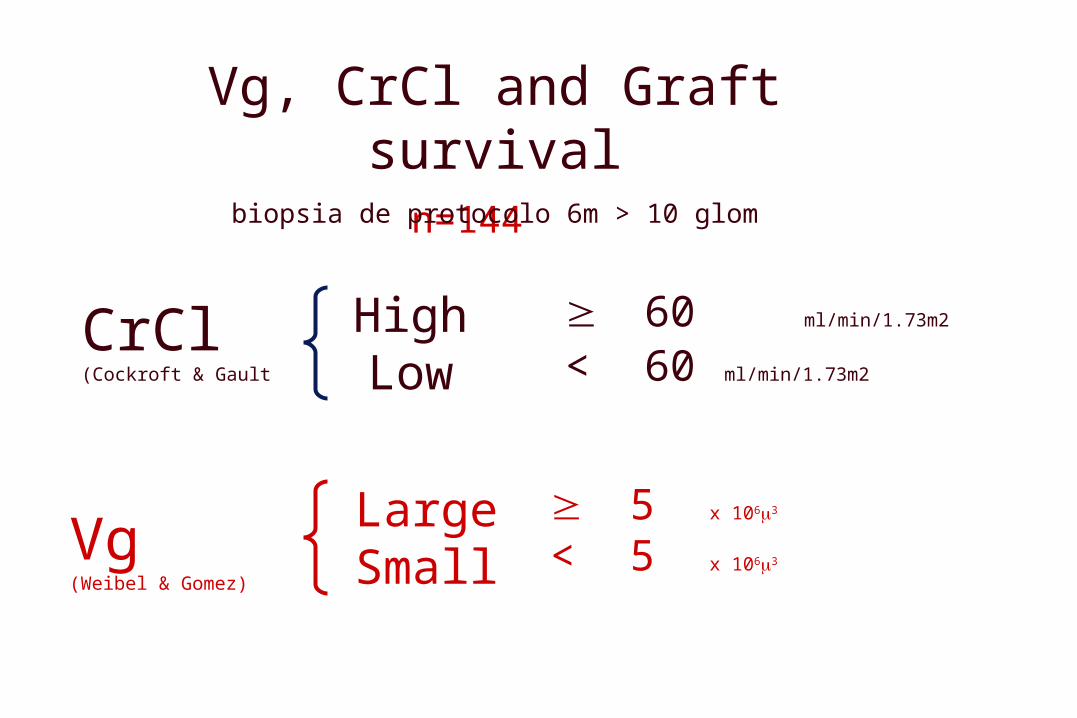
Vg, CrCl and Graft survivaln=144
biopsia de protocolo 6m > 10 glom
CrCl (Cockroft & Gault
60 ml/min/1.73m2
< 60 ml/min/1.73m2
HighLow
5 x 1063
< 5 x 1063 LargeSmallVg
(Weibel & Gomez)

Vg, FG, GS
0
,2
,4
,6
,8
1
Cum. Survival
0 25 50 75 100 125 150 175 200 Time (months)
Vg > 5 & GFR > 60 GS 73%
Vg < 5 & GFR > 60 GS 95%
Vg > 5 & GFR < 60 GS 45%
Vg < 5 & GFR < 60 GS 78%

Conclusion
Glomerular volume and renal function are independent predictors of graft survival
Summary

Acknoledgements
Francesc MoresoXavier FulladosaMiguel HuesoJosé Antonio LopesMeritxell IbernonGabriela AlperovichMontserrat GomàMarta CarreraJosep Maria CruzadoSalvador Gil-VernetJosep Maria Grinyó

Vg small CrCl high n=24 (17%)
Vg small CrCl low n=60 (42%)
Vg large CrCl high n=20 (20%)
Vg large CrCl low n=31 (21%)