value based care: the top of the population health...
TRANSCRIPT

11/25/2014
1
©2014 MFMER | slide-1
©2014 MFMER | slide-1
Value Based Care: The Top of the Population
Health Pyramid
Robert Albright, Jr., DO; Michelle Hedin, RN; and Kathryn Zavaleta, FACHE26th Annual National Forum on Quality Improvement in Health Care
Session: C22December 9, 2014
These presenters have nothing to disclose
©2014 MFMER | slide-2
Objectives
• Explore how to meet the needs of the patients at the “top” of the population health pyramid, utilizing a value-based framework
• Illustrate the gap and opportunity to redesign care delivery for patients with complex needs
• Draw action-oriented conclusions
• Provide a take-away tool that can used tomorrow
The presenters have no relevant financial relationships or commercial interests to disclose.

11/25/2014
2
©2014 MFMER | slide-3
©2012 MFMER | 3186021-3
On any given Friday at 4:55 PM…
• 42-year-old with DM 2, HTN, obesity, OSA, hyperlipidemia and CKD Stage 3 (Cr. 3.2) presents with malaise, fatigue, nausea, shaking chills and purulent drainage from a chronically infected leg wound…
• Temp 39, BP 90/60, p 110, no urine for the pastday or so
• Chest: No rales, no rub
• Lower extremities: Purple, massive, an indurated weeping wound L shin, pulses absent
• Labs: HCO3 8, Cr. 8 mg/dL, Hgb 8 g/dL,glyco Hb 8%, K…
©2014 MFMER | slide-4
©2012 MFMER | 3186021-4
I II III aVR aVL aVF
V1 V2 V3 V4 V5 V6

11/25/2014
3
©2014 MFMER | slide-5
©2012 MFMER | 3186021-5
What is His K?
A. 8 mEq/L
B. 8 mEq/L
C. 8 mEq/L
D. 8 mEq/L
E. All of the above
©2014 MFMER | slide-6
©2012 MFMER | 3186021-6
Emergently placed on dialysis…
11/25/2014
4
©2014 MFMER | slide-7
©2012 MFMER | 3186021-7
A little history…
• He has seen Nephrology twice in the past4 years, both times creat “stable“ at 3.0,3.2 mg/dL
• He had a cough with his ACEi and stopped it
• His diuretics led to cramps, so he stopped them
• He recalls his kidneys were “bad” but does not recall any other discussions
©2014 MFMER | slide-8
©2012 MFMER | 3186021-8
Chart Review
• BP: 160s systolic “despite 4 agents” (nl< 140/90)
• Glucose: A1C is suboptimal at 9.8% (nl <8%)
• Lipids: Above target despite statin at “maximal dose”
• Lifestyle issues: Smoking a little, no time for exercise
• Education about transplant and dialysis options could not be found
11/25/2014
5
©2014 MFMER | slide-9
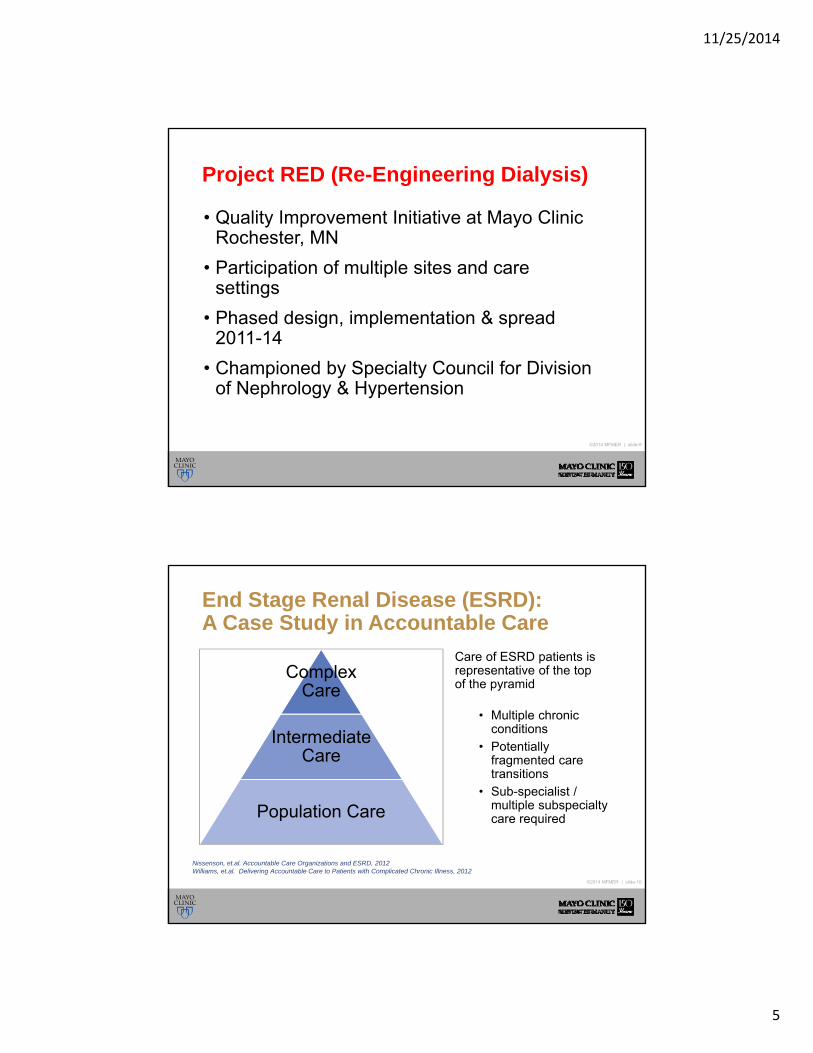
Project RED (Re-Engineering Dialysis)
• Quality Improvement Initiative at Mayo Clinic Rochester, MN
• Participation of multiple sites and care settings
• Phased design, implementation & spread 2011-14
• Championed by Specialty Council for Division of Nephrology & Hypertension
©2014 MFMER | slide-10
End Stage Renal Disease (ESRD):A Case Study in Accountable Care
Care of ESRD patients is representative of the top of the pyramid
• Multiple chronic conditions
• Potentially fragmented care transitions
• Sub-specialist / multiple subspecialty care required
Complex Care
Intermediate Care
Population Care
Nissenson, et.al. Accountable Care Organizations and ESRD, 2012Williams, et.al. Delivering Accountable Care to Patients with Complicated Chronic Illness, 2012
11/25/2014
6
©2014 MFMER | slide-11
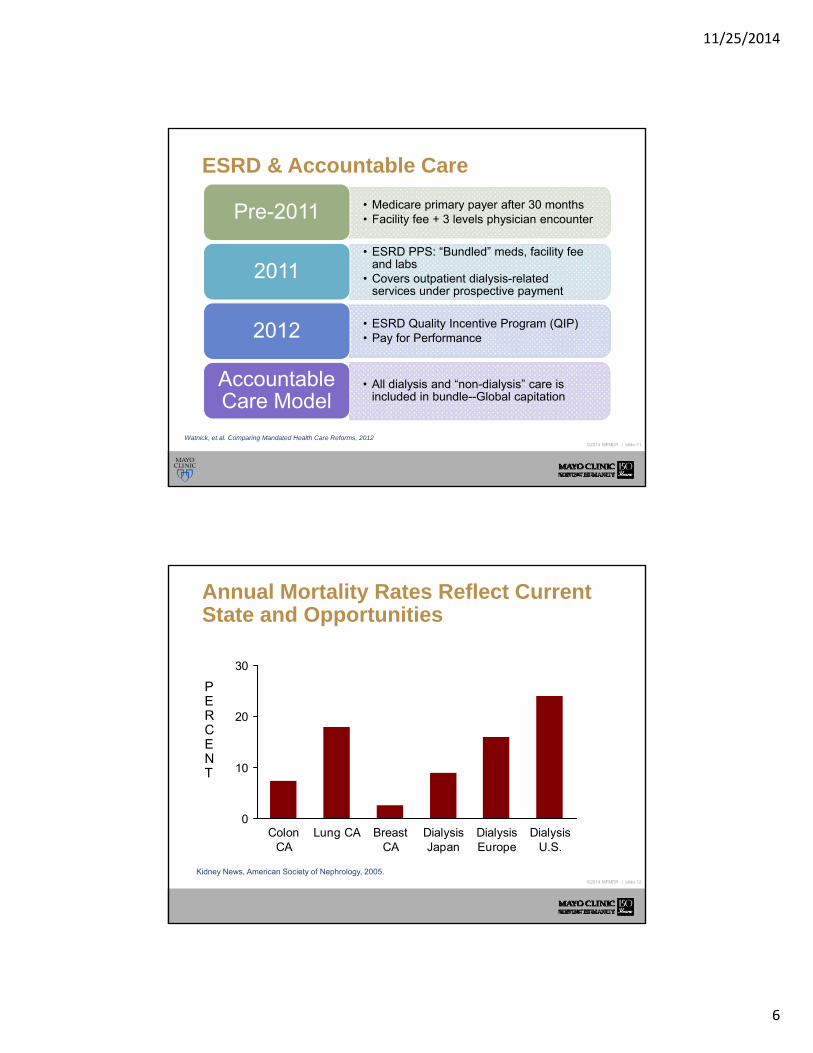
• Medicare primary payer after 30 months• Facility fee + 3 levels physician encounterPre-2011
• ESRD PPS: “Bundled” meds, facility fee and labs
• Covers outpatient dialysis-related services under prospective payment
2011
• ESRD Quality Incentive Program (QIP)• Pay for Performance2012
• All dialysis and “non-dialysis” care is included in bundle--Global capitation
Accountable Care Model
ESRD & Accountable Care
Watnick, et.al. Comparing Mandated Health Care Reforms, 2012
©2014 MFMER | slide-12
Annual Mortality Rates Reflect Current State and Opportunities
0
10
20
30
ColonCA
Lung CA BreastCA
DialysisJapan
DialysisEurope
DialysisU.S.
PERCENT
Kidney News, American Society of Nephrology, 2005.
11/25/2014
7
©2014 MFMER | slide-13
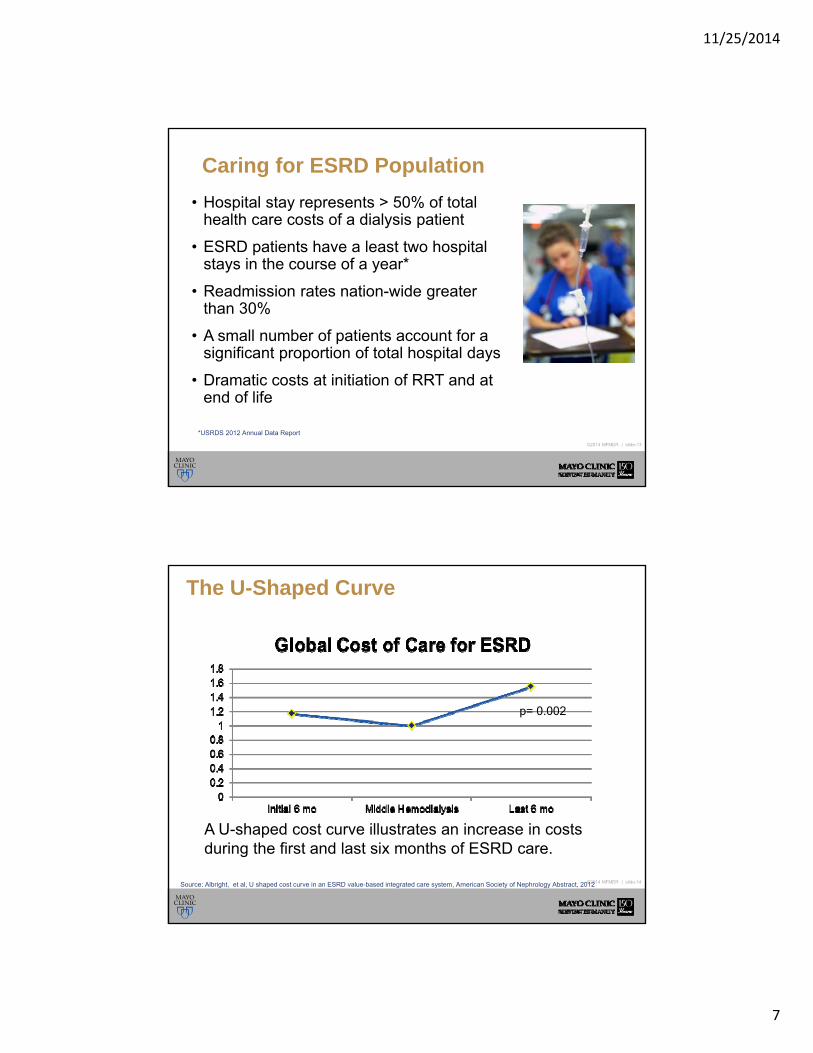
Caring for ESRD Population
• Hospital stay represents > 50% of total health care costs of a dialysis patient
• ESRD patients have a least two hospital stays in the course of a year*
• Readmission rates nation-wide greater than 30%
• A small number of patients account for a significant proportion of total hospital days
• Dramatic costs at initiation of RRT and at end of life
*USRDS 2012 Annual Data Report
©2014 MFMER | slide-14
The U-Shaped Curve
A U-shaped cost curve illustrates an increase in costs during the first and last six months of ESRD care.
Source: Albright, et al, U shaped cost curve in an ESRD value-based integrated care system, American Society of Nephrology Abstract, 2012
p= 0.002

11/25/2014
8
©2014 MFMER | slide-15
Meeting the Needs of ESRD PatientsRequires Quality Care at Each Level
Management of CKD & Patient-Centered Discussion
On-going dialysis care,management of ESRD and other acute / chronic needs
From chronic kidney disease (Stage III & IV) to End-Stage Renal Disease (Stage V)
Complex Care
Intermediate Care
Population CareManagement of Chronic Conditions & Appropriate Referral
©2014 MFMER | slide-16
Improvement Work for Each GroupStarts with the Patient’s Perspective
Understand Patients’ Perspective
Envision Ideal Care
Implement & Standardize
Diffuse & Spread

11/25/2014
9
©2014 MFMER | slide-17
©2012 MFMER | 3186021-17
Design Requirements:What Matters to Patients
• Shared Decision-MakingNon-paternalistic discussion
• Collaboration & EmpowermentEffectively exchanging information
• Open & Honest CommunicationTransparency of cost, data, modalities, and delivery of care
• Improved Education Intervals and InterpretationReal-time information that has a tighter feedback loops
• Clarified RelationshipsMutual understanding of team member roles and activities
Source: Mayo Center for Innovation
©2014 MFMER | slide-18
Decision-Making:Patients Think in Goals and Values
Patients want to be in conversation even when it is hard
With a care team they know and with whom they have an established relationship
Who can help them:o Understand the trajectory of the disease o Map uncertaintyo Create an effective self-management plan
Enabling proactive discussions allow them tomake quick decisions if required
11/25/2014
10
©2014 MFMER | slide-19
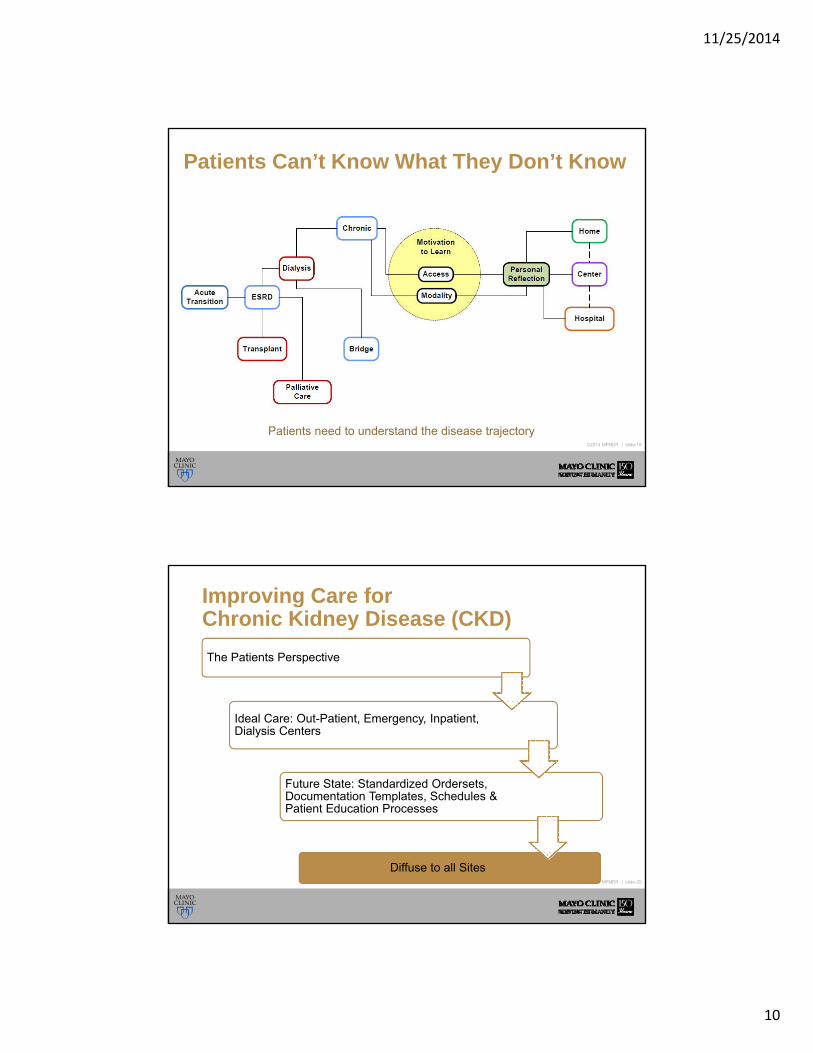
Patients Can’t Know What They Don’t Know
Patients need to understand the disease trajectory
©2014 MFMER | slide-20
Improving Care for Chronic Kidney Disease (CKD)
The Patients Perspective
Ideal Care: Out-Patient, Emergency, Inpatient, Dialysis Centers
Future State: Standardized Ordersets, Documentation Templates, Schedules & Patient Education Processes
Diffuse to all Sites

11/25/2014
11
©2014 MFMER | slide-21
The Burden of DiseaseThe Burden of Care
“I started in the Diabetic Nephropathy Clinic a couple years ago. I hadn’t retired the last time I saw him, but I think my doctor will be happy with my appointment today. I’ve been taking better care of my health now that I have more time to spend on exercising
I never thought my health would get this bad. I had never really been sick all of my life. Now I know what it’s like to have to take care of myself. I like coming to the clinic because they give me points when I come here. My other doctors don’t give me that feedback.
I just wish they had better training plans. I’m doing better with exercise but my diet is still the same as before. I don’t know if it’s better to have smaller portions or completely change what I eat”.
“I have a new career. My health is my new career.”
Source: Persona Descriptions (composite of interviews and observations)Mayo Clinic Center for Innovation
NANCY (F) with daughterAGE 60CKD PTRECENT RETIREEHAS KIDS AND GRANDKIDS
©2014 MFMER | slide-22
Improvement Target: Reduce in-hospital initiation of chronic dialysis from 65% to 20%.
Design focus: - Chronic Kidney Disease
Management Program
- Framing End of Life Discussions
Envisioning Ideal Care Chronic Kidney Disease Stage III & IV
Care Managers Toolbox/ Patient Education Processes
Acute TransitionCKD Stage III & IV CKD Stage V (ESRD)

11/25/2014
12
©2014 MFMER | slide-23
Minimally Invasive Medicine
• Capacity vs. Demand (Burden of Illness + Burden of Treatment)
IHI Chronic Disease Model:
• Self-Management Support
• Delivery System Design
• Decision Support
• Clinical Information Systems
• Organization of Health Care
• Community
Envision Ideal State:Drawing on Best Practices
CKD ESRDInpatientCare
May C, Montori VM, Mair FS. We need minimally disruptive medicine. BMJ 2009 andhttp://www.ihi.org/resources/Pages/AudioandVideo/WIHIMinimallyDisruptiveMedicine.aspxSee also: http://www.ihi.org/topics/ChronicCare/Pages/default.aspx
©2014 MFMER | slide-24
Process MapsTranslate Ideal Delivery to Standard Work
Objective: Decrease number of patients with CKD who enter dialysis as a result of an acute episode during an chronic inpatient hospital stay

11/25/2014
13
©2014 MFMER | slide-25
Testing the Future State — The CKD Clinic
Change Concepts• Electronic cue for primary care for
nephrology consult • Care process algorithms standardized
for primary care• Care standardization with dashboard,
auto template note• Nurse-physician /NP/PA model (PDSA)
CKD ESRDInpatientCare
©2014 MFMER | slide-26
Designing & Implementing Solutions -Small Tests of Change
What can we do by next Tuesday?
• Test Group Education
• Trial processes to trigger Annual Nutrition Consult for CKD Stage III & IV
• Test Scheduling RN Patient Education Follow-up
A P
S D
PA
S D

11/25/2014
14
©2014 MFMER | slide-27
Improvement Target: Better decisions related to initiation and transitions of dialysis
Design focus: Care Processes in the acute setting supporting patient / family decision-making & preparations for dialysis. Smoothing transitions
Envision Ideal Inpatient Care
Care Managers Toolbox/ Patient Education Processes
Acute TransitionCKD Stage III & IV CKD Stage V (ESRD)
©2014 MFMER | slide-28
Start with Patient’s PerspectiveKey Decisions & Care Transitions
Victoria (the daughter):
“My mother died years ago, and I try to get to see my dad when I can, but I can’t manage it all on top of my personal responsibilities.”
“I got a call from the hospital that he was admitted. He’s not very conscious or awake. I’m not sure if he knows where he is right now. Now I have to make all these decisions myself. The care team told me he would die if he didn’t start dialysis right away. I don’t know what other options I have.”
“Is this really the best thing for him?”
65% of patients start dialysis in the hospital setting.
Source: Persona Descriptions (composite of interviews and observations)Mayo Clinic Center for Innovation
Victoria's father is GEORGE (M)AGE 87ACUTE ESRD (CATHETER)RETIREDWIDOWER

11/25/2014
15
©2014 MFMER | slide-29
Results: Better Management of CKDPercentage of ESRD Patients Initiating Dialysis in Inpatient Setting
0%
10%
20%
30%
40%
50%
60%
70%
80%
2011 2012 2013
2011 vs 2013 p = 0.042
Percentage of ESRD Patients Initiating Dialysis in Inpatient Setting
73.2%
62.6%58.4%
©2014 MFMER | slide-30
Hospital Management

11/25/2014
16
©2014 MFMER | slide-31
Inpatient Care Change Concepts
• Standardized inpatient care order sets
• Co-location of medical patients when possible
• Improved transitions to renal replacement therapy or supportive care
• Template for team hand-offs
• Teleconferenced “huddle” between inpatient team and dialysis center team
MetricsCKD ESRD
InpatientCare
©2014 MFMER | slide-32
Leveraging Huddles for Transitions:“We all start the day on the same page.”
Discussion Items• Who has been hospitalized:
• Patient goals & concerns• New patients needing dialysis• Scheduling issues• Vascular access issues• Rounds & orders• Medication changes for established patients• Transition planning
• Expected discharge date• Expected discharge location

11/25/2014
17
©2014 MFMER | slide-33
Improvement Target: Reduce avoidable utilization of emergency & inpatient services by 20%
Design focus: Team-Based Chronic Disease Management for ESRD
Envision Ideal Care in the Dialysis Center
Care Managers Toolbox/ Patient Education Processes
Acute TransitionsCKD Stage III & IV CKD Stage V (ESRD)
©2014 MFMER | slide-34
“I started dialysis in the hospital. I thought I was getting sick a couple months ago, but I didn’t have a primary care doctor. To be honest, I was afraid of the cost and never imagined getting so sick so quickly.
Now I have a lot of hospital bills to pay, and I’m trying to organize my Medicare all at once. It’s so confusing. I need to find a primary doctor that I like. I’m just now starting to understand the process. Sometimes I have to skip dialysis, because of my work schedule. I know that it messes up my schedule, and that scares me. I don’t have a choice though. I have to put food on the table for my young kids.
My wife is already doing most of the work. To pay for all of these pills and diabetes appointments, I have to work extra shifts when I can. Then on top of this, the care team wants me to exercise and diet. I have so much stress that I can’t imagine where I will find the time. I want to be a dad too.”
“I’ll CROSS THAT BRIDGE LATER.”
JOHN (M) AGE 42
ACUTE ESRD (GRAFT)
HAD TO QUIT WORKING
MARRIED WITH KIDS
The Patient’s Perspective
Source: Persona Descriptions (composite of interviews and observations)Mayo Clinic Center for Innovation

11/25/2014
18
©2014 MFMER | slide-35
An Opportunity for ImprovementMedication Management
Baseline
• N = sample of 29 patients
• Mean = 18 medications
• Mean = 25 doses/day
• Mean AWP drug cost = $thousands of dollars/month
CKD ESRDInpatientCare
©2014 MFMER | slide-36
Common Drug Therapy Problems* & Associated Conditions
• Nonadherence – blood pressure lowering
• Nonadherence – hyperphoshatemia
• Nonadherence – nutritional supplements
• Nonadherence – aspirin use
• Dose too low – hyperphosphatemia
• Unecessary therapy – nutritional supplements
* The above were identified 10 or more times in 62 patients

11/25/2014
19
©2014 MFMER | slide-37
Redesigning Pharmacist Role
• Medication review with patient
• Adherence assessment and monitoring
• Drug information to staff and patients
• Round with consultants in dialysis center
• Group visits for home dialysis
• Med review after hospital dismissal (previously not ordered for all)
• Med review for new patients
©2014 MFMER | slide-38
Results: Medication Management
As a result of pharmacist identification and resolution of medication related problems
• Pharmacist service resulted in medication cost savings of 8.8% patient/year
• Cost avoidance of unnecessary lab testing, avoidance of additional clinic visits, selection of cost effective drug therapy, avoidance of serious adverse drug reactions
CKD ESRDInpatientCare

11/25/2014
20
©2014 MFMER | slide-39
Redesigning Patient Education
Standardized Resources• CKD• CKD Diet• Access• Treatment Options• Inpatient New Dialysis• Chronic Hemodialysis
Admission• Chronic Hemodialysis
Ongoing• Dialysis Diet
©2014 MFMER | slide-40
Providing Patient-Centered Education
• Consistent Across All Care Settings
• Used by all members of team: Physician, RN, Pharmacist, Dietician, Social Worker
• Standardized for all Sites
• Provides Individualized Care−Core documents that every patient will need−Expanded materials most patients will need−Supportive materials/ patient-specific
CKD ESRDInpatientCare
Patient Education
11/25/2014
21
©2014 MFMER | slide-41
Huddles Across the SystemDialysis Center (AM):
• NP/PA, Social Worker, Dietitian, Charge Nurse and Scheduler, access coordinator, pharmacist
• Team issues and / or concerns (i.e., access problems, exceptional patients, hypertension, fever, etc.)
• Plan-for-the-Day (goals, procedures, tests, priorities)
• Patient / Family coping and/or concerns
Dialysis Center (Shift): Huddle among RN and Tech staff
Between inpatient and outpatient teams (PM): • Hospital NP/PA and Liaison, Center NP/PA , Social
Worker, Dietitian, Charge Nurse and Scheduler
©2014 MFMER | slide-42
Results of Instituting Huddles:
“We all start the day on the same page.”
• Top 3 Improvements Staff Attributed to Team Huddles:
• 37% survey respondents reported improved communication
• 30% reported improvement in addressing patient issues
• 18.6% highlighted improved focus of team / unit
CKD ESRDInpatientCare

11/25/2014
22
©2014 MFMER | slide-43
• Shared Decision-Making: Expanded patient education toolkit for all settings
• Population Health Management:Best practice processes for Kidney Disease Stage 3 or 4
• Multi-disciplinary team management in specialty setting
• Redesigned support for patients facing initiation of dialysis
• Enhanced care and support at transitions:
o Improved discharge processes
o Early post-discharge follow-up
Summary of Interventions
Patient EducationMetrics
CKD ESRDInpatientCare
©2014 MFMER | slide-44
Multi-faceted Approach Across the Continuum• Pharmacist-directed medication therapy
management safer and more cost-effective
• Addressing therapy adherence: A business case for care managers for the very highest risk patients
• Team approach to Palliative Care and symptom management
Patient EducationCKD ESRD
InpatientCare

11/25/2014
23
©2014 MFMER | slide-45
Value Based Care
©2014 MFMER | slide-46
Results: Reduction in Hospitalizationof ESRD Patients
2011 2012 2013%
ChangeP value(Mood median)
Global costs/day* 100.0 83.23 78.44 ‐21.6 0.004
Inpatient
costs/day (*)
100.0 71.74 78.75 ‐21.5 0.014
Outpatient
costs/day (*)
100.0 105.91 88.45 ‐11.6 0.024
n hospitalized (%) 129 (67.5) 108 (59.7) 100 (54.9) ‐22 0.04
(Fisher
exact)
*Adjusted for inflation: costs stated as % of 2011 costs
Albright, et.al., J Am Soc Nephrol 25: 2014, Supplement, 2014

11/25/2014
24
©2014 MFMER | slide-47
Sustaining the Gains:
• Specialty Councils provide guidance
• Multi-disciplinary workgroups charged with continued improvement
• Dashboard of key performance metrics
• Diffusion matrix tracks extent specific processes in place
DiffusePatient EducationCKD ESRD
InpatientCare
Note: Template for multi-site spread included in hand-outs as a take-away
©2014 MFMER | slide-48
Lessons LearnedDrivers of Cost-Effective of Care
• Standardized care of the patient stage III or IV to slow or prevent progression
• Shared Decision-Making: -Dialysis vs. No Dialysis-In-Center Dialysis vs. Home Dialysis
• Reduce Utilization of In-patient Servicesthrough Enhanced Access
• Palliative Care Training for All Staff provided
additional support for the very Highest Risk Patient

11/25/2014
25
©2014 MFMER | slide-49
Other Considerations
• Delivering Patient-Centered Care:In order to put the needs of the patient first, one must understand the patient’s perspective
• Diffusion:IT Resources an important enabler but not a show-stopper
• Measurement: Data Warehousing / patient registries key
• Structure for Improvement Team: Project Executive Team with Working Groups provided traction
• Integration: Process-redesign supports integration and vice-versa
©2014 MFMER | slide-50
Future Directions
• Models of population mgmt. for ESRD population:Primary Care Physician vs. Nephrologist asprimary
• Integration of care managers
• Hospital / out-patient rule–based approaches to identify high risk patient

11/25/2014
26
©2014 MFMER | slide-51©2014 MFMER | slide-51
Questions & Discussion
©2014 MFMER | slide-52©2014 MFMER | slide-52