when stomach is not available - duke university · pdf filethe gastric conduit is standard of...
TRANSCRIPT
©2014 MFMER | slide-1
When Stomach is Not Available… Shanda Blackmon, M.D., M.P.H., FACS Associate Professor, Thoracic Surgery, Mayo Clinic

©2014 MFMER | slide-2
Objectives
• To review options for long-segment esophageal replacement
• To review equipment and techniques
• To share our outcomes and experience

©2014 MFMER | slide-3
Background
• 1st successful resection of the thoracic esophagus for carcinoma was performed by Torek near the turn of the century in a patient with esophageal carcinoma1

©2014 MFMER | slide-4
Background
• Gastrointestinal continuity was established using an external "rubber tube" between a cervical esophagostomy and gastrostomy
• The patient survived for 13 yrs and was able to swallow liquified food

©2014 MFMER | slide-5
Background
• Immediate reconstruction of the gastrointestinal tract after an esophagectomy with an esophago-gastrostomy did not occur until the mid 1930s
©2014 MFMER | slide-6
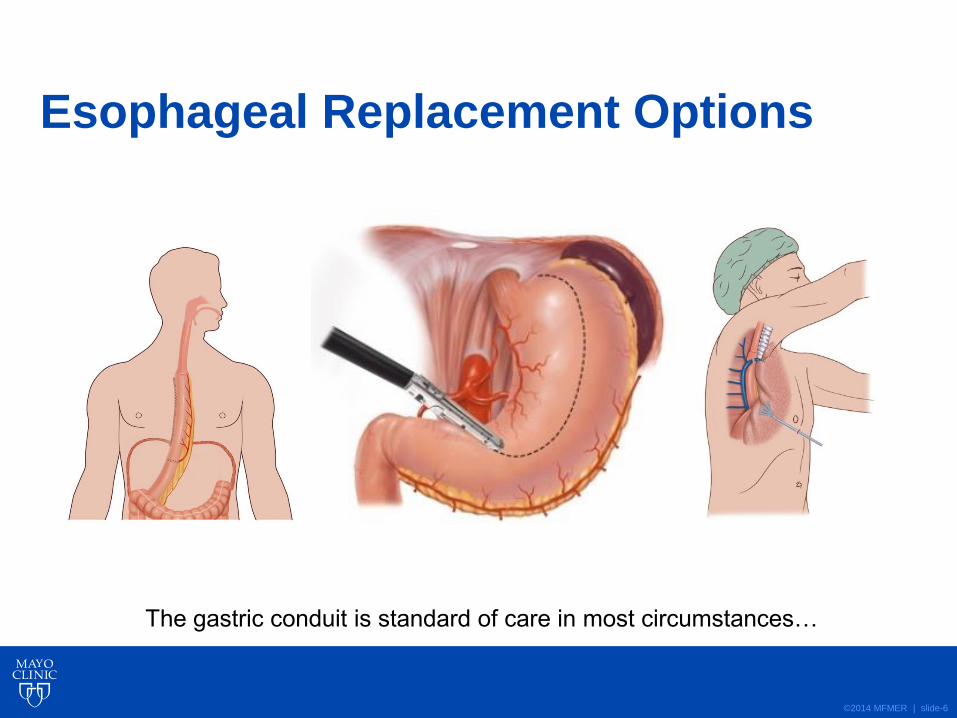
Esophageal Replacement Options
The gastric conduit is standard of care in most circumstances…
©2014 MFMER | slide-7
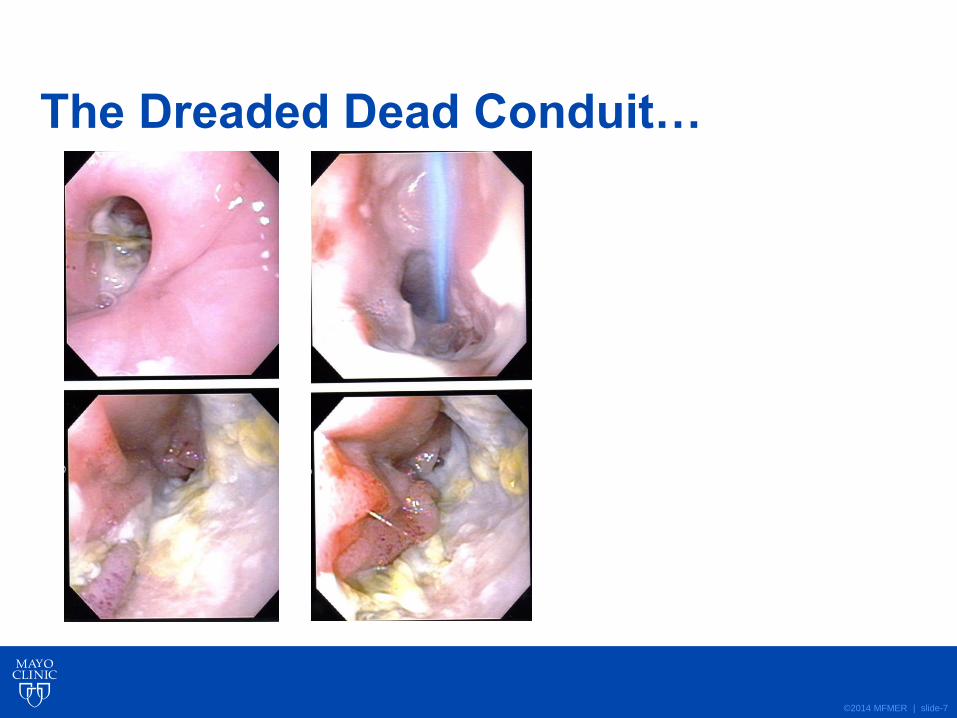
The Dreaded Dead Conduit…

©2014 MFMER | slide-8
Indications for Alternate Conduits:
• Dead gastric conduit
• Injury to GE Vessel
• Cancer extending Into eso & stomach
• Recurrence of esophageal tumor1, 2
1. Schipper PH, Cassivi SD, Deschamps C, Rice DC, Nichols FC 3rd, Allen
MS, Pairolero PC. Locally recurrent esophageal carcinoma: when is re-
resection indicated? Ann Thorac Surg. 2005 Sep;80(3):1001-5; discussion
1005-6.
2. Kim MP, Brown KN, Schwartz MR, Blackmon SH. Advanced esophageal
cancer in patients who underwent radiofrequency ablation for barrett
esophagus with high grade dysplasia. Innovations (Phila). 2013 Jan-
Feb;8(1):17-22.
©2014 MFMER | slide-9
Esophageal Replacement Options
• Colon
• Jejunum
©2014 MFMER | slide-10
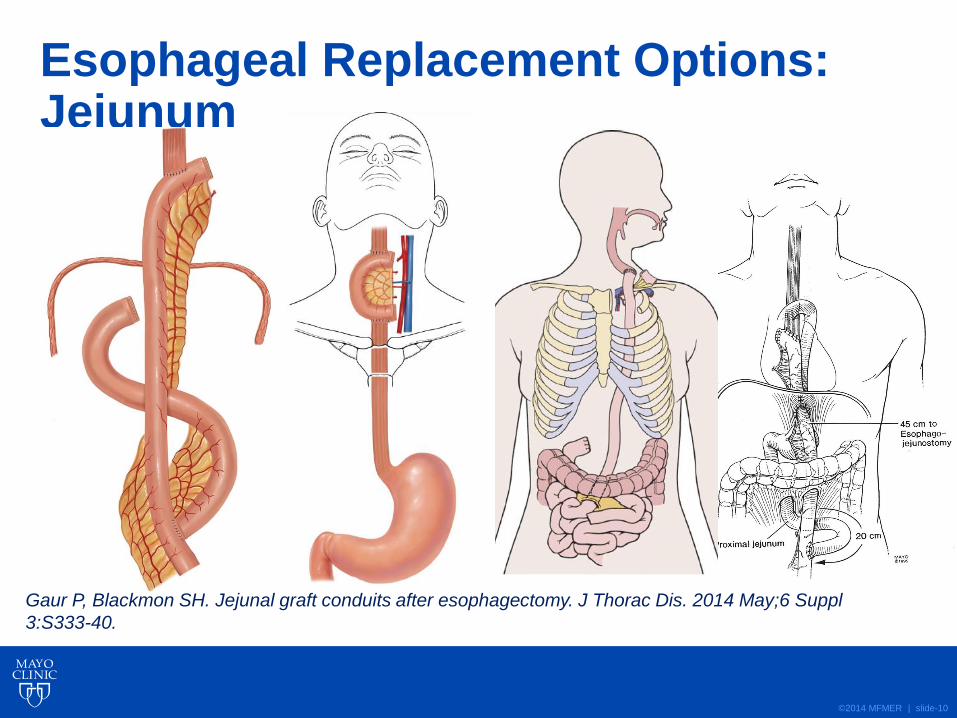
Esophageal Replacement Options: Jejunum
Gaur P, Blackmon SH. Jejunal graft conduits after esophagectomy. J Thorac Dis. 2014 May;6 Suppl
3:S333-40.
©2014 MFMER | slide-11
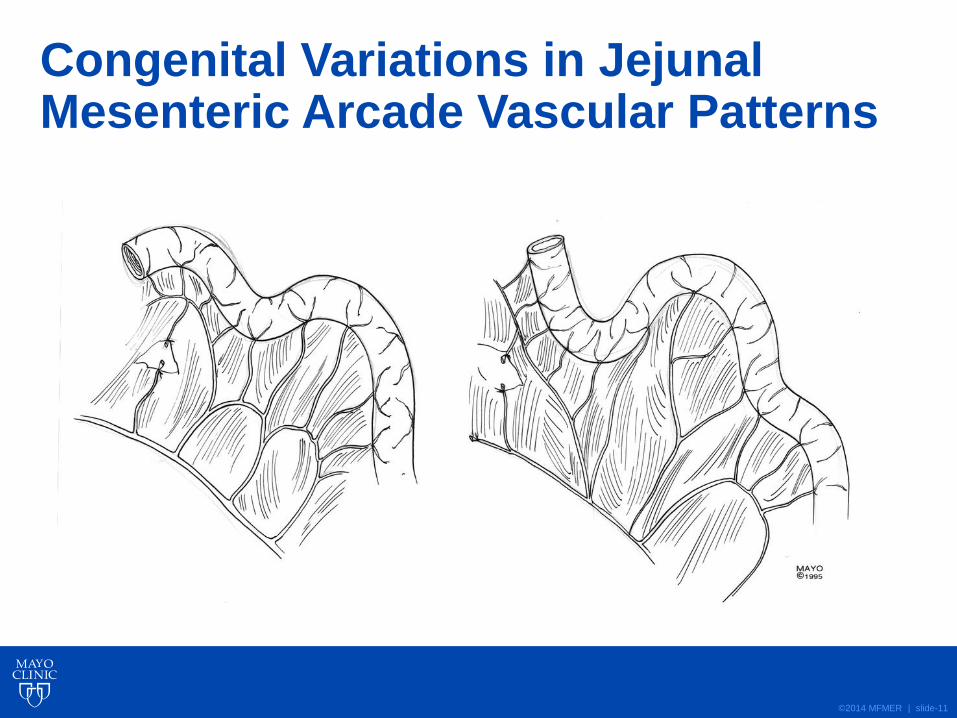
Congenital Variations in Jejunal Mesenteric Arcade Vascular Patterns
©2014 MFMER | slide-12
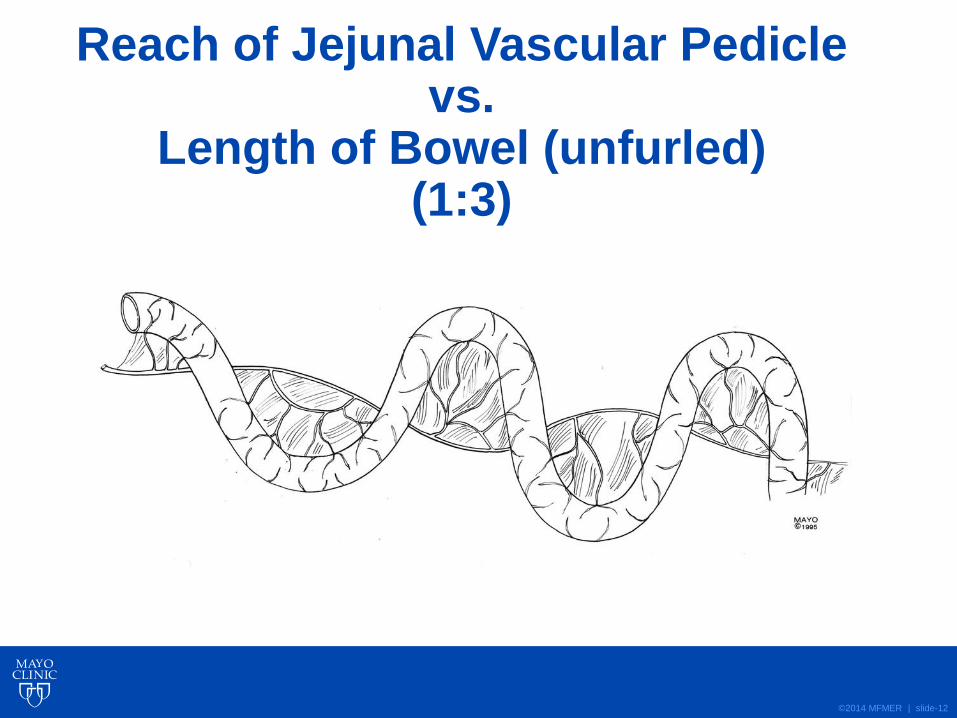
Reach of Jejunal Vascular Pedicle vs.
Length of Bowel (unfurled) (1:3)

©2014 MFMER | slide-13
Dividing the Mesentery for a Long Jejunal Graft

©2014 MFMER | slide-14
Dividing the Bowel for a Long Jejunal Graft
©2014 MFMER | slide-15
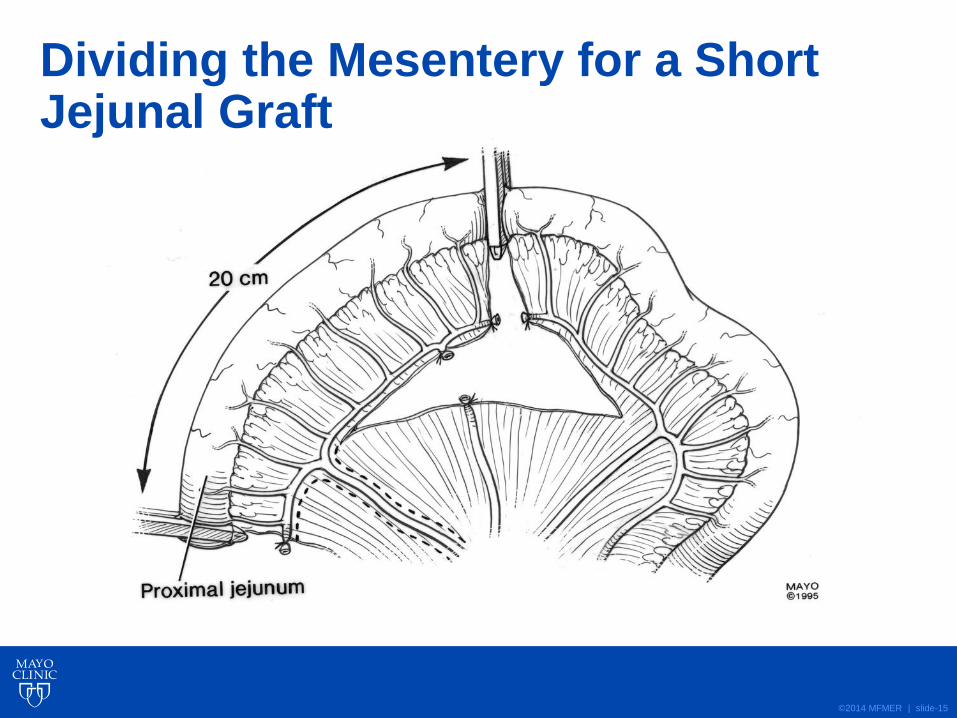
Dividing the Mesentery for a Short Jejunal Graft
©2014 MFMER | slide-16
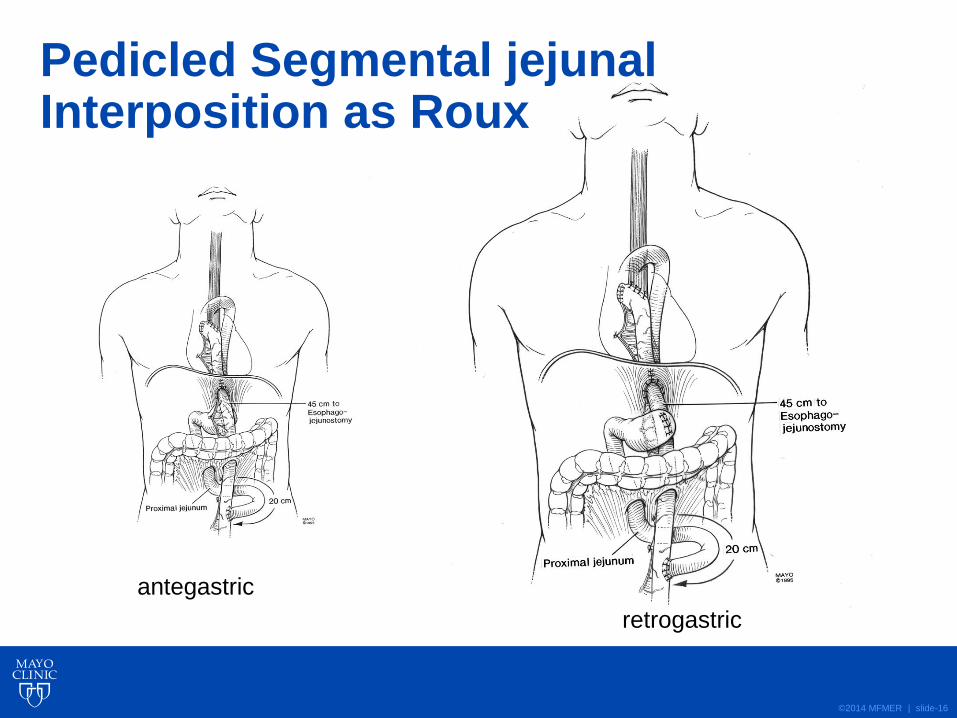
Pedicled Segmental jejunal Interposition as Roux
antegastric
retrogastric
©2014 MFMER | slide-17
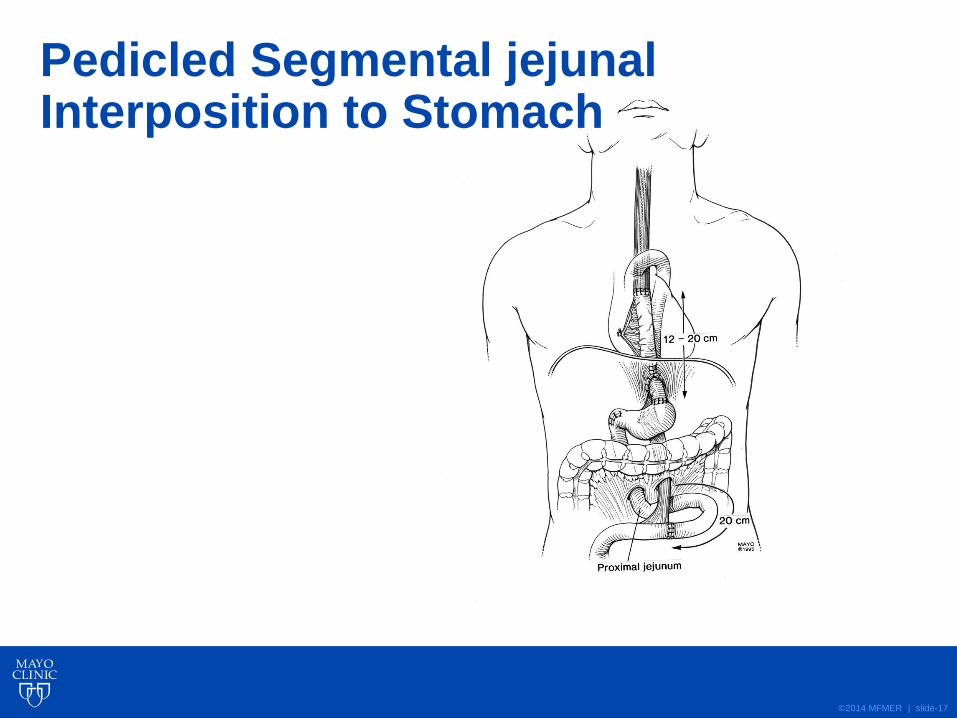
Pedicled Segmental jejunal Interposition to Stomach

©2014 MFMER | slide-18
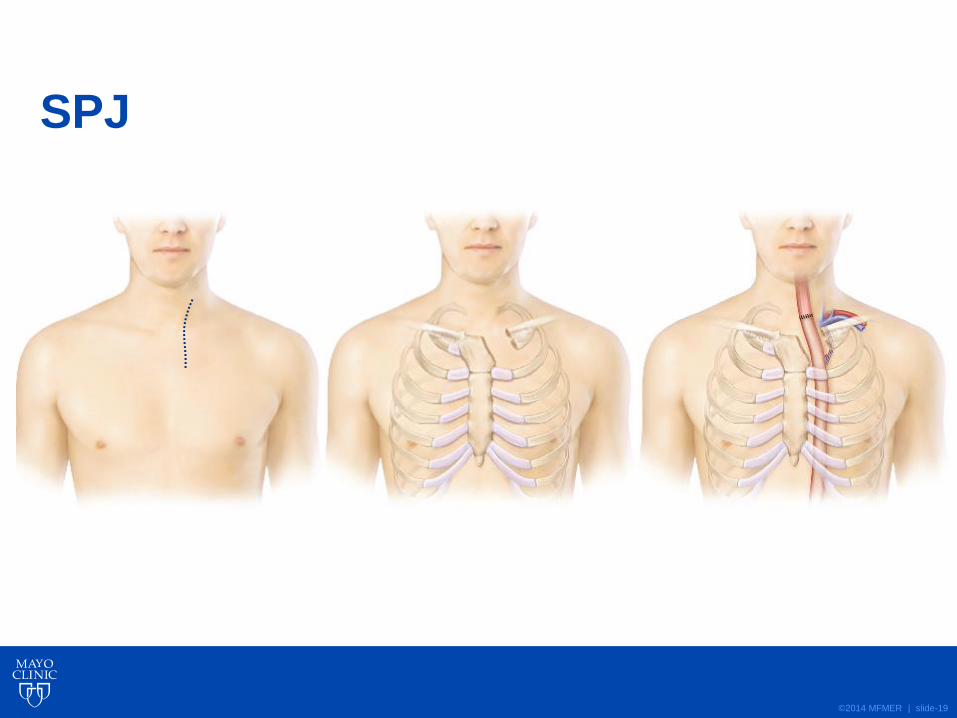
SPJ
©2014 MFMER | slide-19
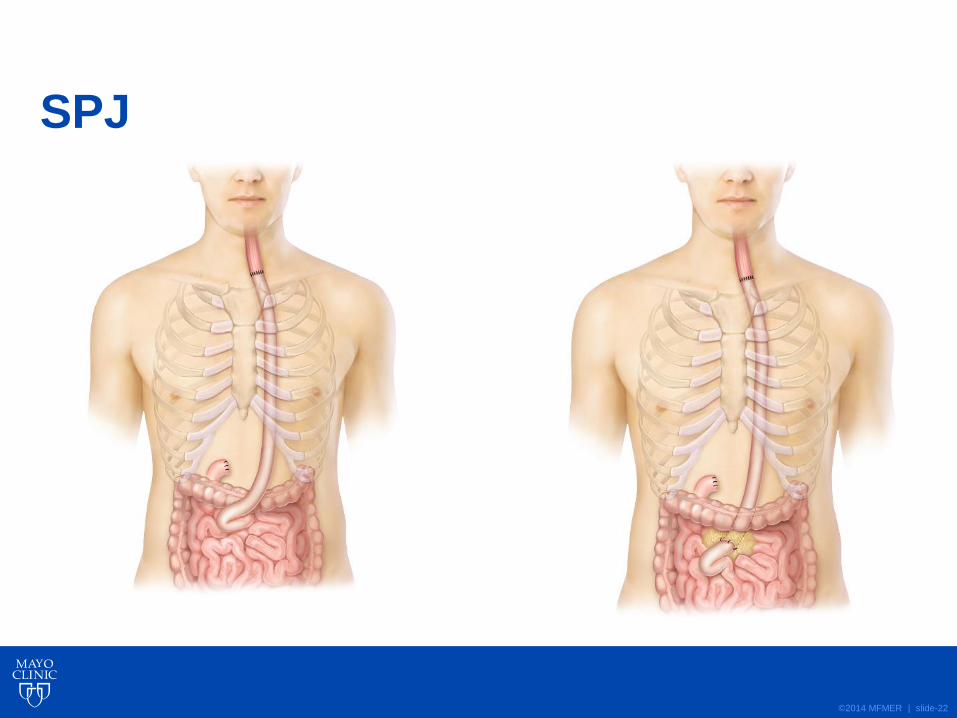
SPJ

©2014 MFMER | slide-20
SPJ

©2014 MFMER | slide-21
©2014 MFMER | slide-22
SPJ
©2014 MFMER | slide-23

©2014 MFMER | slide-24
©2014 MFMER | slide-25
Indications
• To replace segmental esophagus (cervical)
• To reach the pharynx
• To replace entire length of esophagus when a gastric conduit is not available
Blackmon SH, Correa AM, Skoracki R, Chevray PM, Kim MP, Mehran RJ, Rice DC, Roth JA, Swisher SG,
Vaporciyan AA, Yu P, Walsh GL, Hofstetter WL. Supercharged pedicled jejunal interposition for esophageal
replacement: A 10 year experience.Ann Thorac Surg. 2012 Oct;94(4):1104-11; discussion 1111-3.

©2014 MFMER | slide-26
Experience
• From June 2000 to December 2010,
• 60 consecutive patients underwent SPJ
• 50 patients from MDACC (2000-2010)
• 10 patients from HMH (2006-2010)
• A database was created to evaluate patient characteristics, operative technique, and outcomes
Blackmon SH, Correa AM, Skoracki R, Chevray PM, Kim MP, Mehran RJ, Rice DC, Roth JA, Swisher SG,
Vaporciyan AA, Yu P, Walsh GL, Hofstetter WL. Supercharged pedicled jejunal interposition for esophageal
replacement: A 10 year experience.Ann Thorac Surg. 2012 Oct;94(4):1104-11; discussion 1111-3.

©2014 MFMER | slide-27
Results
male Age female
44 (73%) 28---------------->76 16(27%)
LOS
7----------------->575 19
57
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.
©2014 MFMER | slide-28
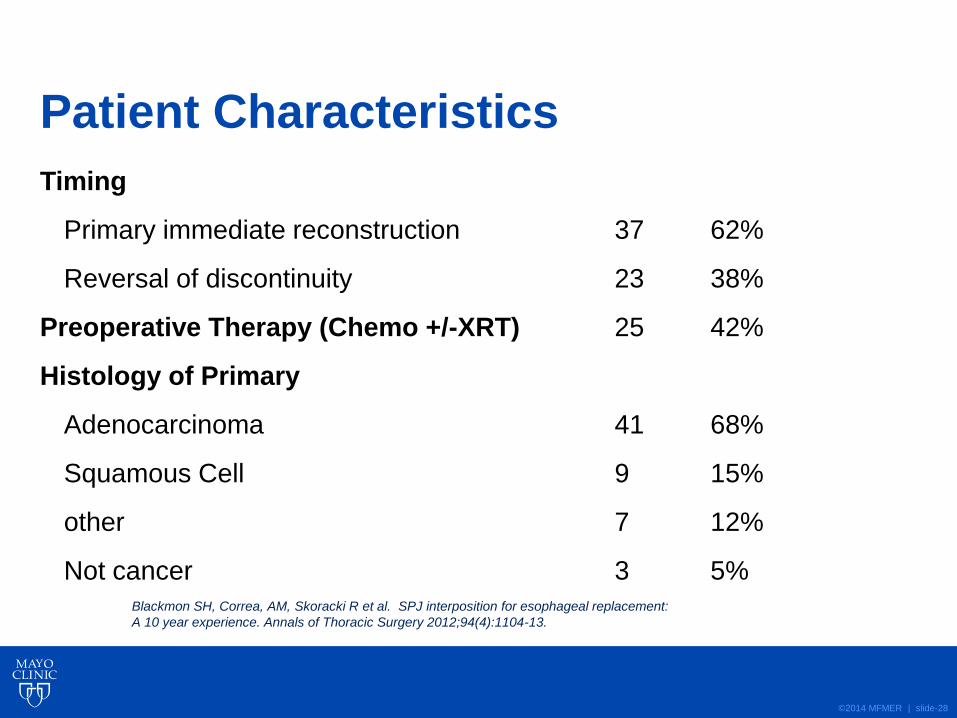
Patient Characteristics
Timing
Primary immediate reconstruction 37 62%
Reversal of discontinuity 23 38%
Preoperative Therapy (Chemo +/-XRT) 25 42%
Histology of Primary
Adenocarcinoma 41 68%
Squamous Cell 9 15%
other 7 12%
Not cancer 3 5% Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.

©2014 MFMER | slide-29
Jejunal Route
Operative Detail n %
Posterior 21 35%
mediastinum
Retrosternal 39 65%
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal
replacement: A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.
©2014 MFMER | slide-30
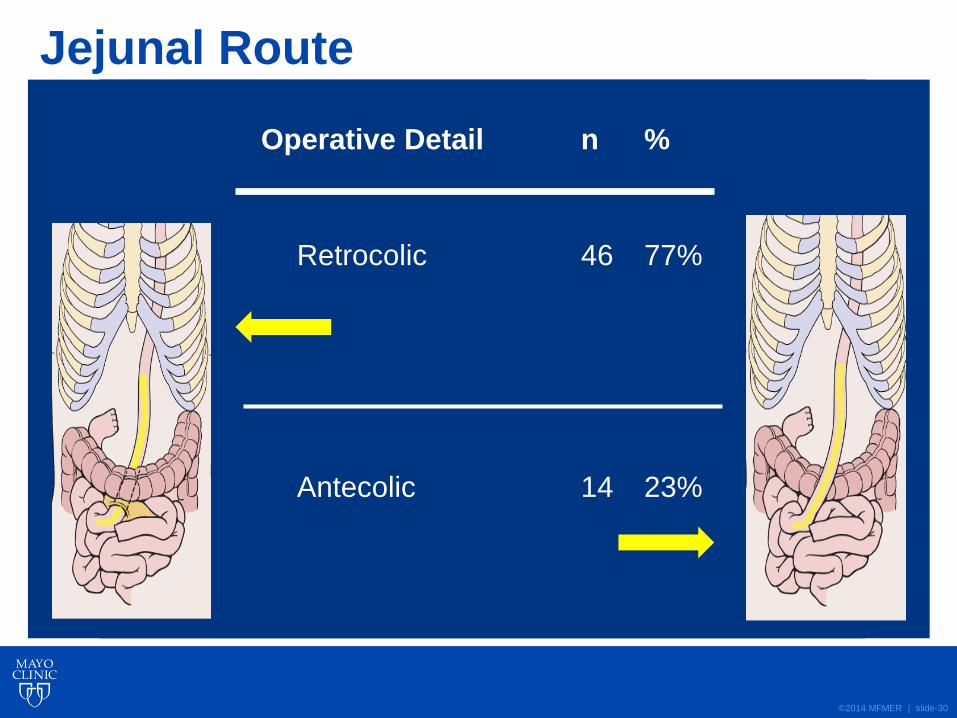
Jejunal Route
Operative Detail n %
Retrocolic 46 77%
Antecolic 14 23%

©2014 MFMER | slide-31
Results: Anastomosis
Operative Detail n %
Neck Anastomosis
Hand-sewn 51 85%
Stapled side-to-side 8 13%
Circular-stapled 1 2%
Distal Connection
Jejunum to stomach remnant 29 48%
Jejunum to jejunum (Roux) 31 52%
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.

©2014 MFMER | slide-32
Results: Graft Loss
Operative Detail n %
Intra-operative vascular revision 16 27%
Intra-operative Graft loss 1 2%
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.
©2014 MFMER | slide-33
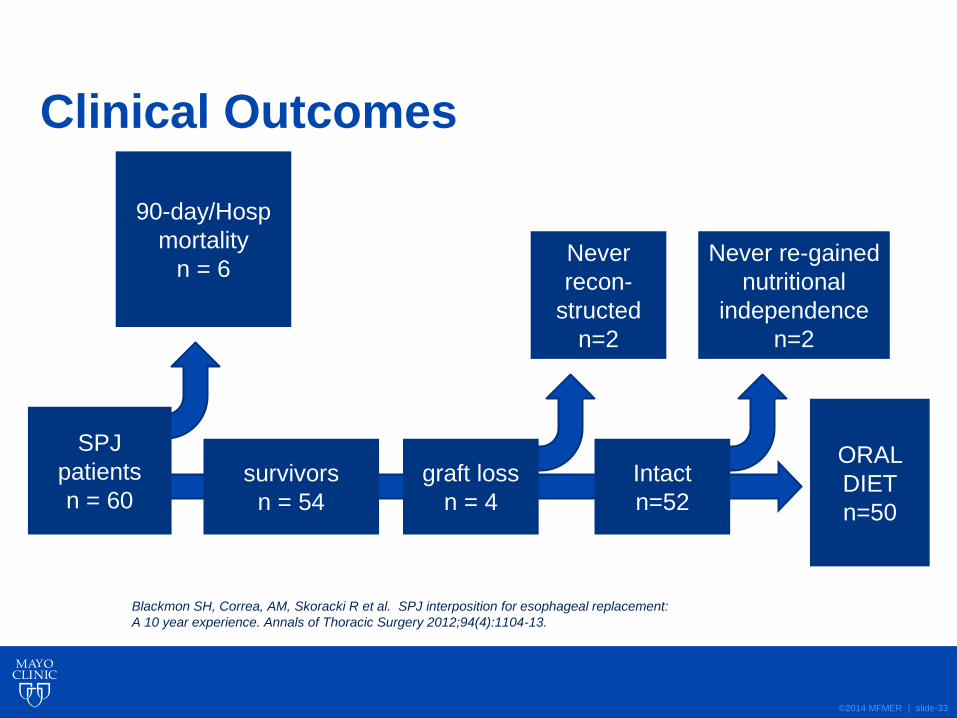
Clinical Outcomes
SPJ
patients
n = 60
90-day/Hosp
mortality
n = 6
survivors
n = 54
Intact
n=52
Never
recon-
structed
n=2
ORAL
DIET
n=50
graft loss
n = 4
Never re-gained
nutritional
independence
n=2
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.

©2014 MFMER | slide-34
Results: Operative Events
Early Event n %
Morbidity:
Leak 19 32%
Grade I 1
Grade II 9
Grade III 4
Grade IV 5
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.

©2014 MFMER | slide-35
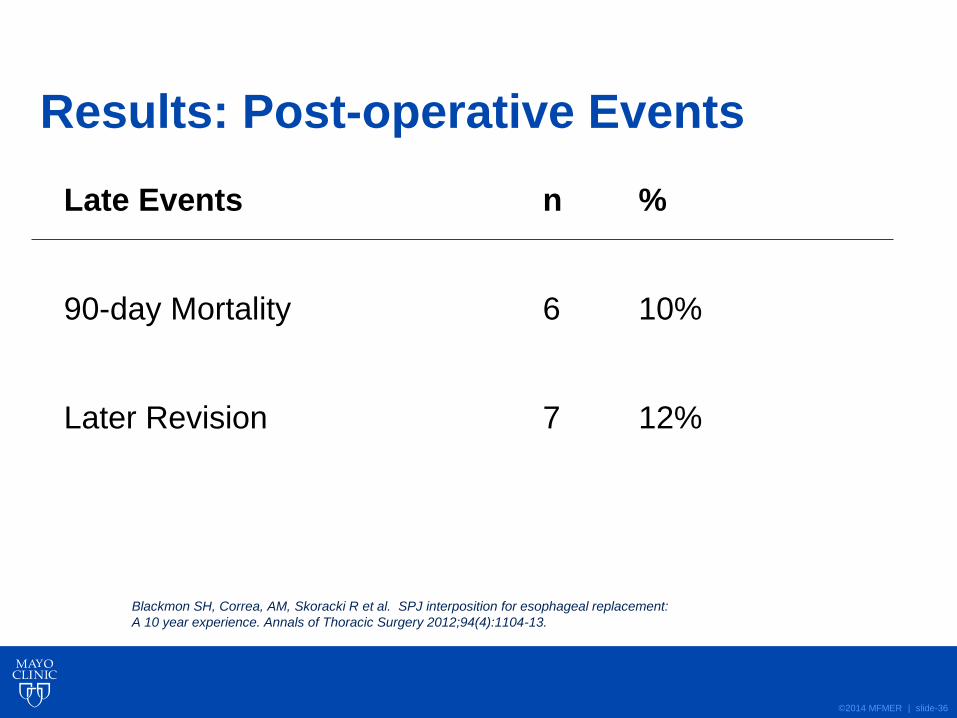
Results: Post-operative Events
Early Event n %
Morbidity:
Pneumonia 18 30%
RLN Injury 10 17%
NOMI 4 7%
Jejunal Graft loss/diversion 5 8%
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.
©2014 MFMER | slide-36
Results: Post-operative Events
Late Events n %
90-day Mortality 6 10%
Later Revision 7 12%
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.
©2014 MFMER | slide-37
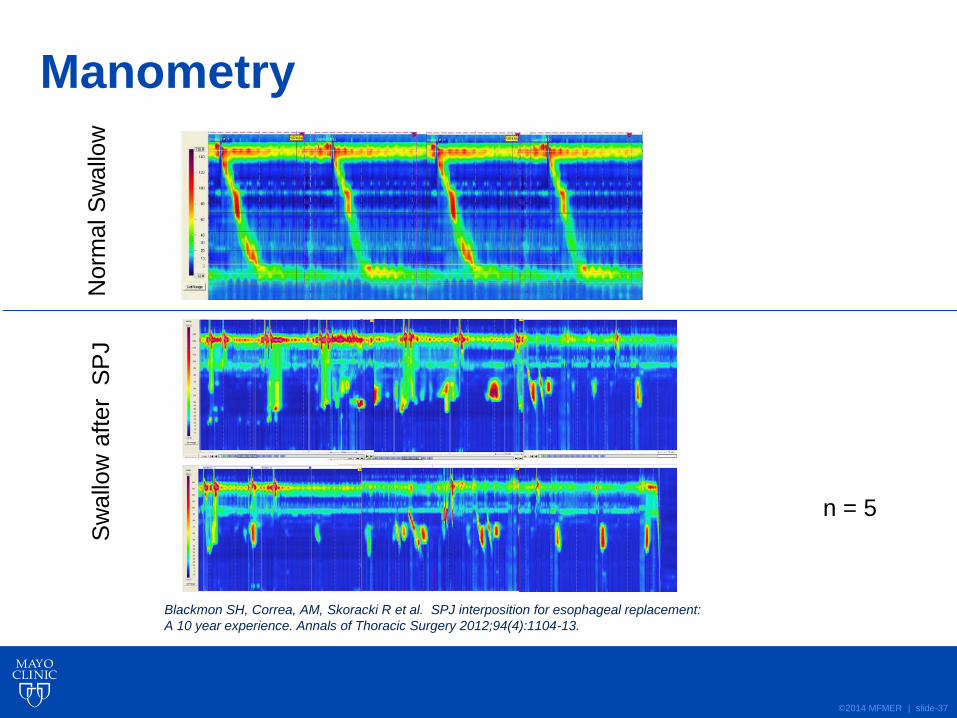
Manometry N
orm
al S
wallo
w
Sw
allo
w a
fter
SP
J
n = 5
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.
©2014 MFMER | slide-38
Conclusions
• SPJ can establish nutritional independence in a high-risk patient population when stomach is unavailable
• This is my preferred alternative for reconstruction when stomach is unavailable
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.

©2014 MFMER | slide-39
Blackmon SH, Correa, AM, Skoracki R et al. SPJ interposition for esophageal replacement:
A 10 year experience. Annals of Thoracic Surgery 2012;94(4):1104-13.
©2014 MFMER | slide-40
How does the SPJ compare to a Gastric Conduit?

©2014 MFMER | slide-41
Super-Charged Pedicled Jejunal Interposition Performance Compares Favorably to a Gastric Conduit After Esophagectomy
Stephens EH,1 Gaur P,2 Hotze KO,2 Correa AM,3 Kim MP,2 Blackmon SH4
1Cardiothoracic Surgery, Columbia University, New York; 2Thoracic Surgery, The Methodist Hospital, Houston; 3MD Anderson, Houston; 4Thoracic Surgery, Mayo Clinic, Rochester
©2014 MFMER | slide-42
Background
• Long segment esophageal reconstruction can be accomplished with “super-charged” jejunum (SPJ), colon, or stomach
• In patients in whom a gastric conduit is not possible, SPJ has advantages:
• Does not require formal preparation
• Usually free of disease
• Similar in diameter to esophagus
• Intrinsic segmental peristalsis
• May not undergo senescent lengthening
• Challenges with SPJ: micro-anastomoses
• Previous studies have examined peri-operative and long-term outcomes of SPJ, but its functionality has not been previously assessed.
• Objective: Assess the functionality of SPJ in comparison to gastric conduits

©2014 MFMER | slide-43
Methods
• A conduit functionality questionnaire was
developed evaluating: • Reflux • Dumping • Dysphagia • Stricture • Zubrod score (functional status) • Post-op pain • Conduit emptying (radiography)
• Preoperative/demographic, intraoperative, and
postoperative data were prospectively collected on
the 94 living patients who underwent esophageal
reconstruction 2009-2013 at HMH.
©2014 MFMER | slide-44
Methods
• 45 of the 94 (48%) patients answered the
questionnaire >1 month after surgery. For
patients who completed multiple
questionnaires, the worst score for each
category was used.
• Statistical analysis was performed using SPSS
(SPSS, Chicago, IL) and included Mann-
Whitney u-test and Fisher’s Exact Test for cross
tabs with statistical significance defined as
p<0.05.
©2014 MFMER | slide-45
Development/Validation of Conduit Assessment Tool
• Tool was developed using three methods to establish content validity:
• 720 patient encounter records during focus groups held over a 5 year period
• formal presentations and review in multidisciplinary GI conference
• formal presentations and review in multidisciplinary esophagus tumor board meetings

©2014 MFMER | slide-46
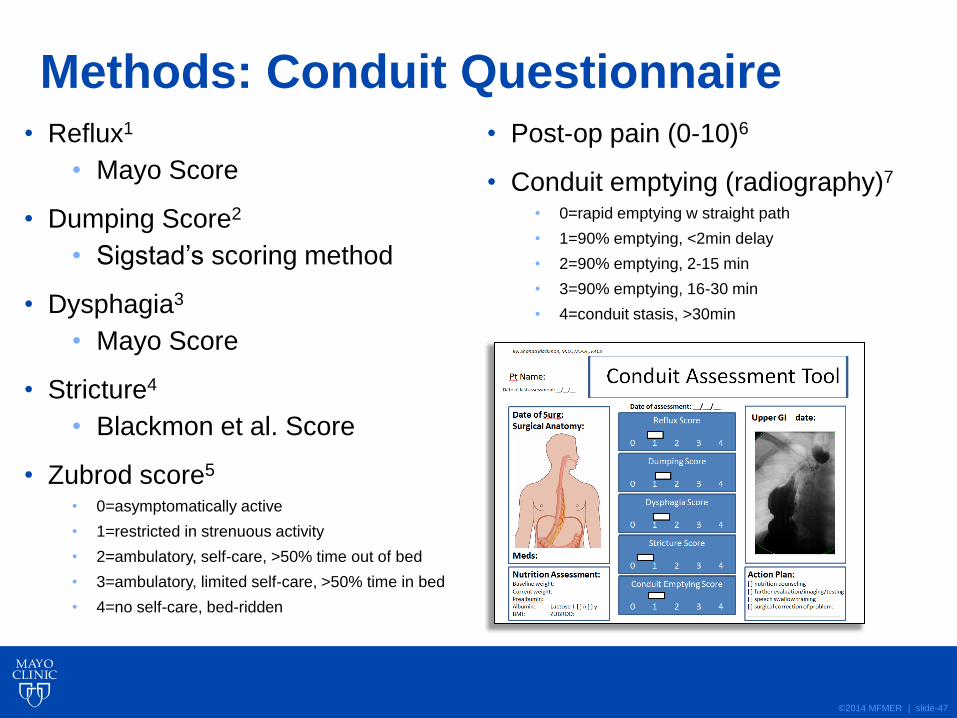
Methods: Conduit Questionnaire
©2014 MFMER | slide-47
Methods: Conduit Questionnaire • Reflux1
• Mayo Score
• Dumping Score2
• Sigstad’s scoring method
• Dysphagia3
• Mayo Score
• Stricture4
• Blackmon et al. Score
• Zubrod score5 • 0=asymptomatically active
• 1=restricted in strenuous activity
• 2=ambulatory, self-care, >50% time out of bed
• 3=ambulatory, limited self-care, >50% time in bed
• 4=no self-care, bed-ridden
• Post-op pain (0-10)6
• Conduit emptying (radiography)7
• 0=rapid emptying w straight path
• 1=90% emptying, <2min delay
• 2=90% emptying, 2-15 min
• 3=90% emptying, 16-30 min
• 4=conduit stasis, >30min
©2014 MFMER | slide-48
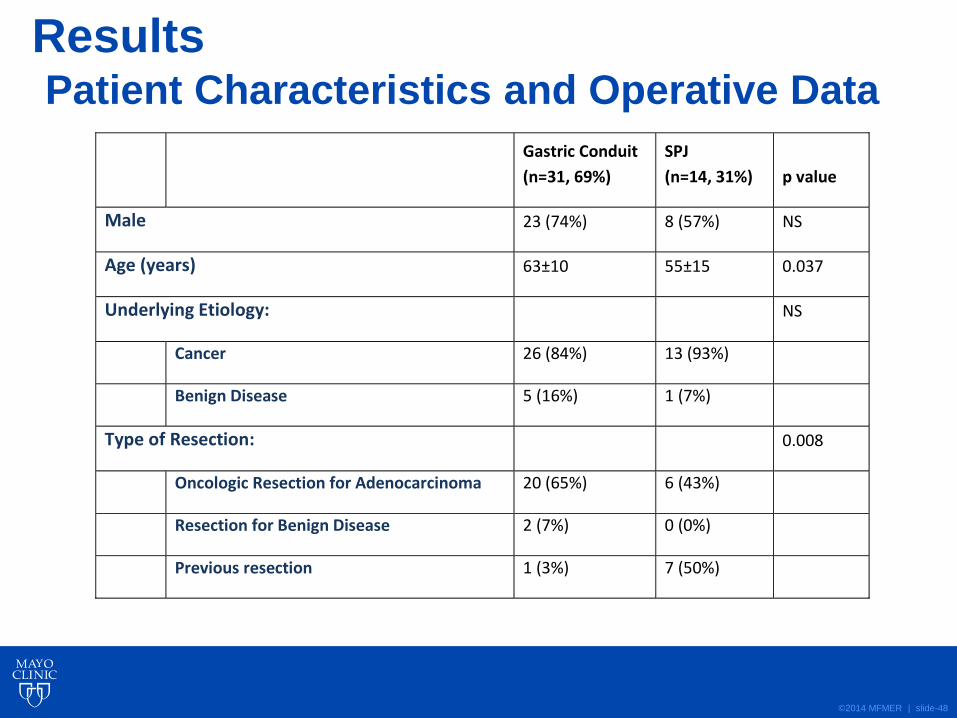
Results Patient Characteristics and Operative Data
Gastric Conduit
(n=31, 69%)
SPJ
(n=14, 31%) p value
Male 23 (74%) 8 (57%) NS
Age (years) 63±10 55±15 0.037
Underlying Etiology: NS
Cancer 26 (84%) 13 (93%)
Benign Disease 5 (16%) 1 (7%)
Type of Resection: 0.008
Oncologic Resection for Adenocarcinoma 20 (65%) 6 (43%)
Resection for Benign Disease 2 (7%) 0 (0%)
Previous resection 1 (3%) 7 (50%)
©2014 MFMER | slide-49
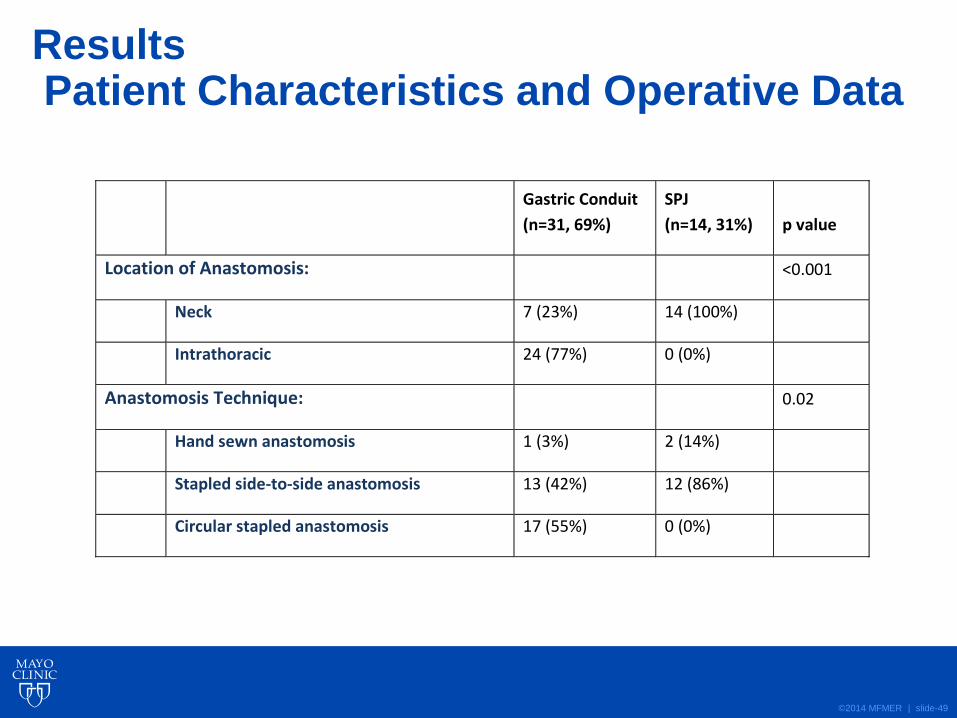
Results Patient Characteristics and Operative Data
Gastric Conduit
(n=31, 69%)
SPJ
(n=14, 31%) p value
Location of Anastomosis: <0.001
Neck 7 (23%) 14 (100%)
Intrathoracic 24 (77%) 0 (0%)
Anastomosis Technique: 0.02
Hand sewn anastomosis 1 (3%) 2 (14%)
Stapled side-to-side anastomosis 13 (42%) 12 (86%)
Circular stapled anastomosis 17 (55%) 0 (0%)

©2014 MFMER | slide-50
Results Post-Operative Complications
Gastric Conduit
(n=31, 69%)
SPJ
(n=14, 31%) p value
Surgical Complications: 15 (48%) 7 (50%) NS
Pneumonia 7 (23%) 3 (21%)
Afib 4 (13%) 1 (7%)
Renal failure 1 (3%) 1 (7%)
Respiratory failure 3 (10%) 1 (7%)
UTI 1 (3%) 0 (0%)
DVT 1 (3%) 1 (7%)
Length of stay (days) 10±4 17±15 0.04
30 day mortality 0 (0%) 0 (0%) NS
Leak within 60 days 7 (23%) 4 (29%) NS
Reoperation 3 (10%) 1 (7%) NS
Afib=atrial fibrillation, NS=not statistically significant, UTI=urinary tract infection, DVT=deep vein thrombosis.

©2014 MFMER | slide-51
Results: Clinical Follow-Up
Gastric Conduit (n=31, 69%)
SPJ (n=14, 31%) p value
Death at last follow-up 2 (7%) 2 (14%) NS
Length of follow-up 14±11 22±14 NS

©2014 MFMER | slide-52
Results: Conduit Function
0
1
2
3
4
5
6
7
Gastric
SPJ
P=0.04
©2014 MFMER | slide-53
Discussion
• SPJ compares favorably to gastric conduit for
esophageal reconstruction in terms of
functionality.
• The groups differed significantly with SPJ
patients more likely to have had prior resection.
• Operative outcomes and peri-operative
complications were not significantly different
between groups except longer length of stay
for SPJ patients and more post-operative pain.
©2014 MFMER | slide-54
Discussion
• The conduit assessment is a useful tool to
compare reconstruction techniques, as well as
assess patients’ recovery and need for further
interventions.
©2014 MFMER | slide-55
Discussion
• Future studies involve:
• Validation of the conduit assessment tool at
other institutions
• Application of the tool to compare the outcomes
of other reconstruction techniques (ie Ivor
Lewis vs. transhiatal +/- pyloroplasty) in terms
of physiologic outcomes
• Establish expected ranges at each post-
operative time point for a given surgery,
enabling identification of patients who deviate
and may need further intervention

©2014 MFMER | slide-56
Limitations
• Small sample size at a single institution.
• Inherent differences in baseline characteristics of patients.
• Did not specifically examine role of conduit assessment tool in subsequent interventions and improvements in symptoms.

©2014 MFMER | slide-57
Jejunal Interposition Results: ROL

©2014 MFMER | slide-58
Colon Conduits
©2014 MFMER | slide-59
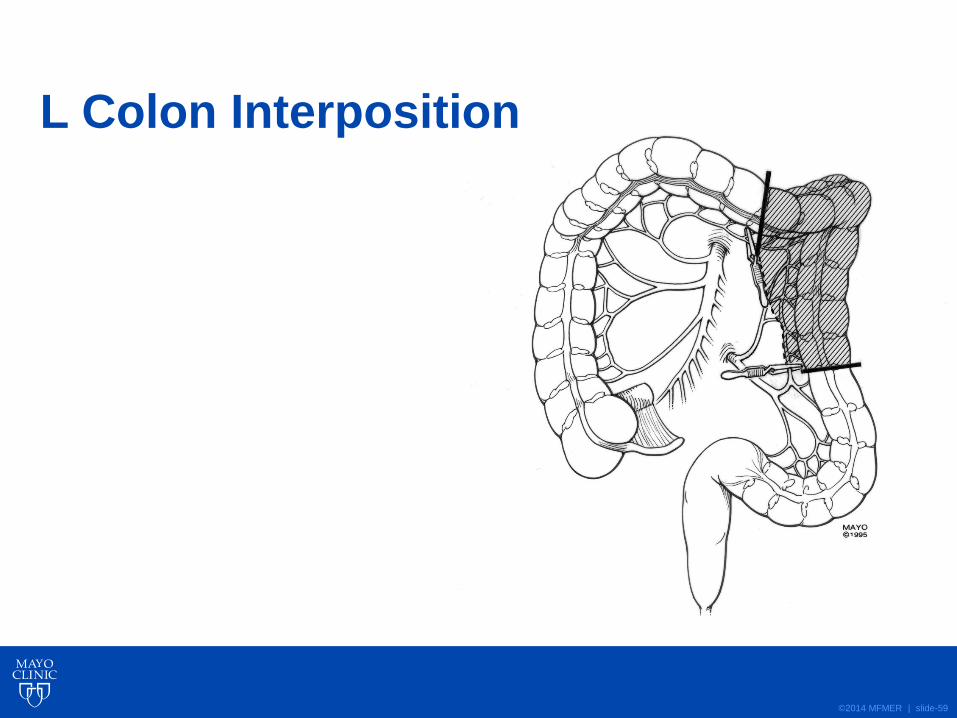
L Colon Interposition

©2014 MFMER | slide-60
Transverse Colon Interposition
©2014 MFMER | slide-61
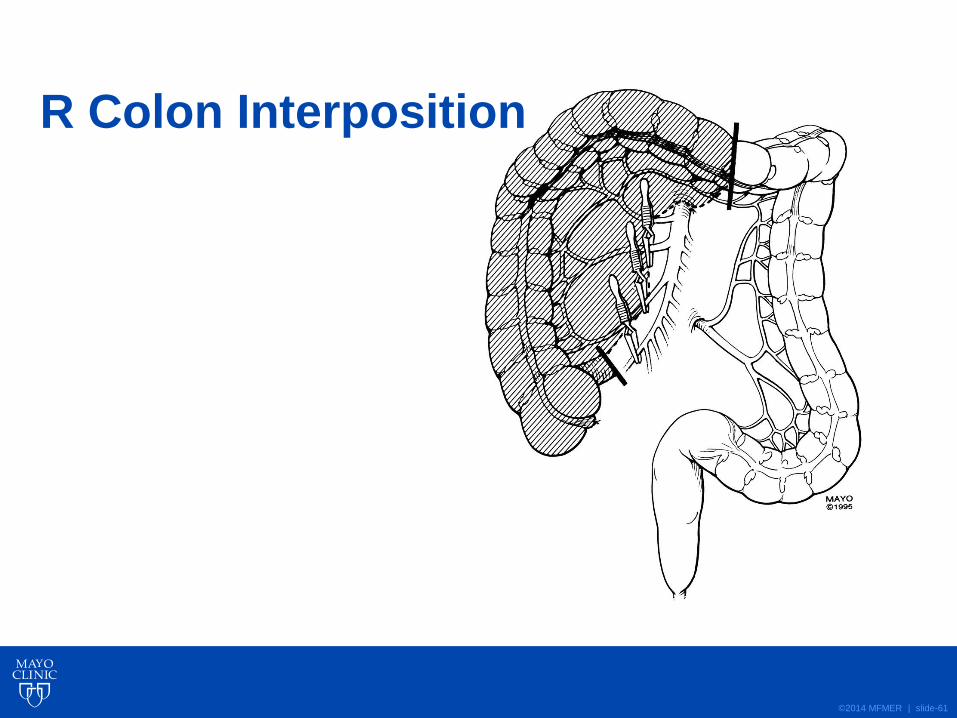
R Colon Interposition

©2014 MFMER | slide-62
Selecting and Measuring the Colon Interposition
©2014 MFMER | slide-63
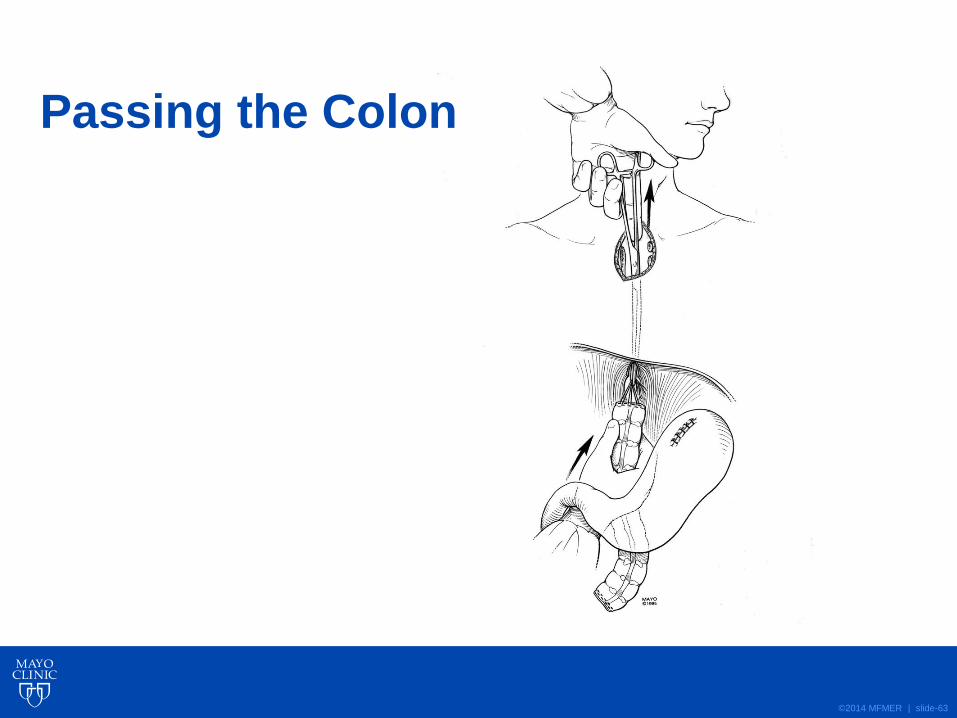
Passing the Colon
©2014 MFMER | slide-64
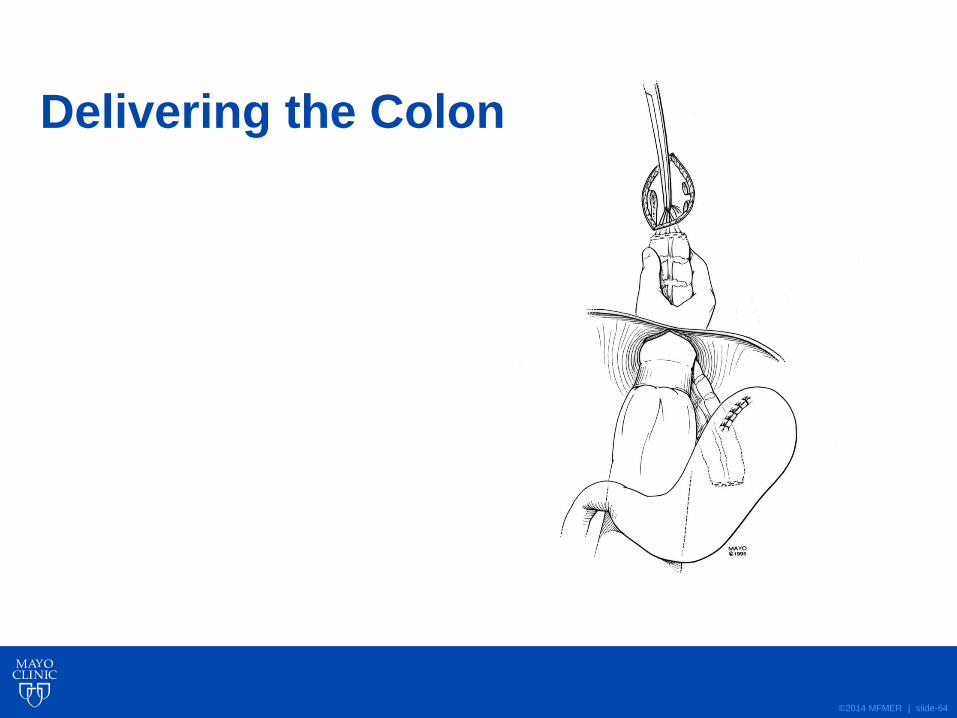
Delivering the Colon

©2014 MFMER | slide-65
Esophago-colonic anastomosis
©2014 MFMER | slide-66
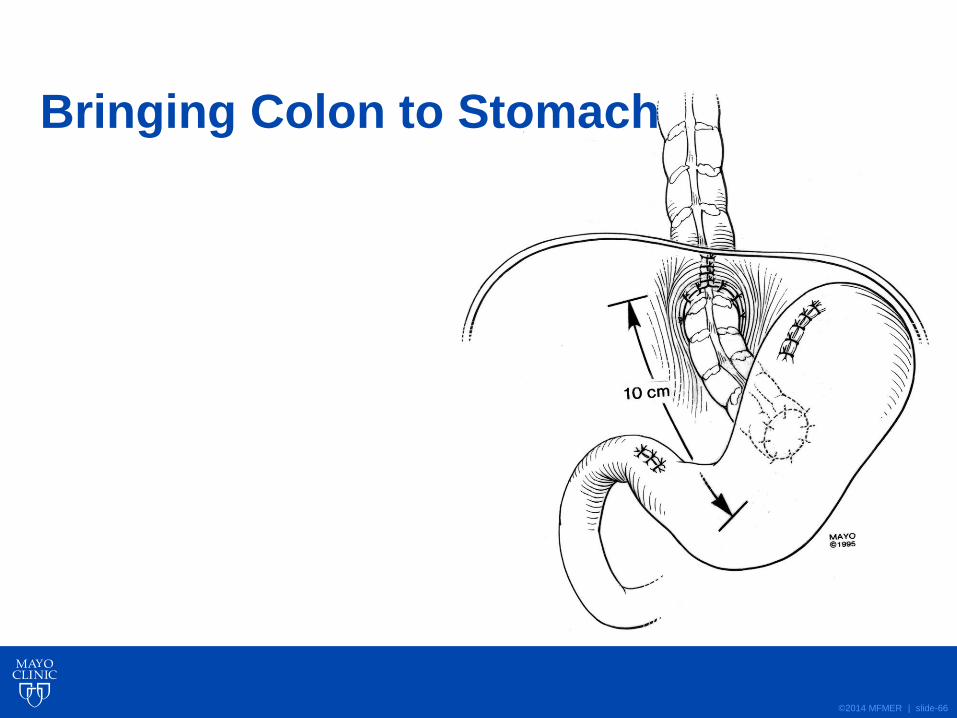
Bringing Colon to Stomach
©2014 MFMER | slide-67
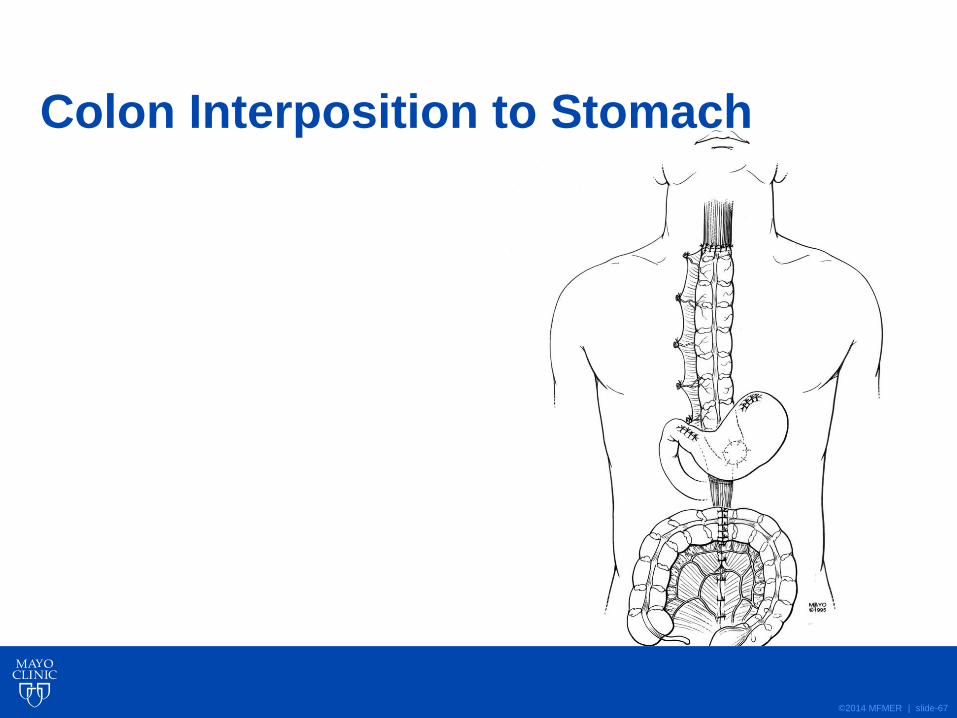
Colon Interposition to Stomach

©2014 MFMER | slide-68
Colon Interposition
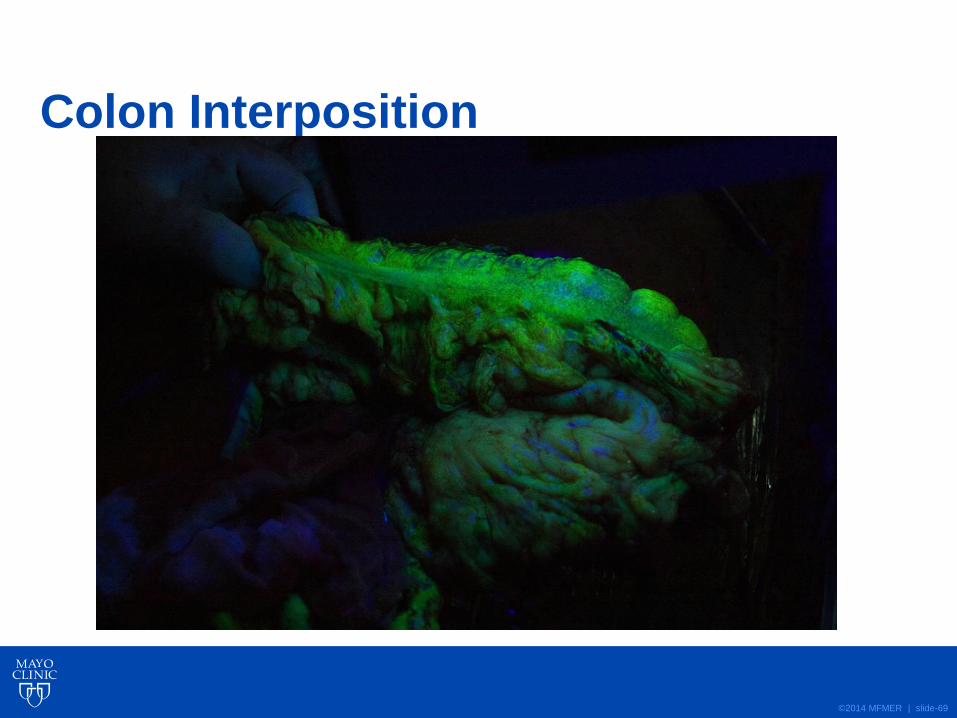
©2014 MFMER | slide-69
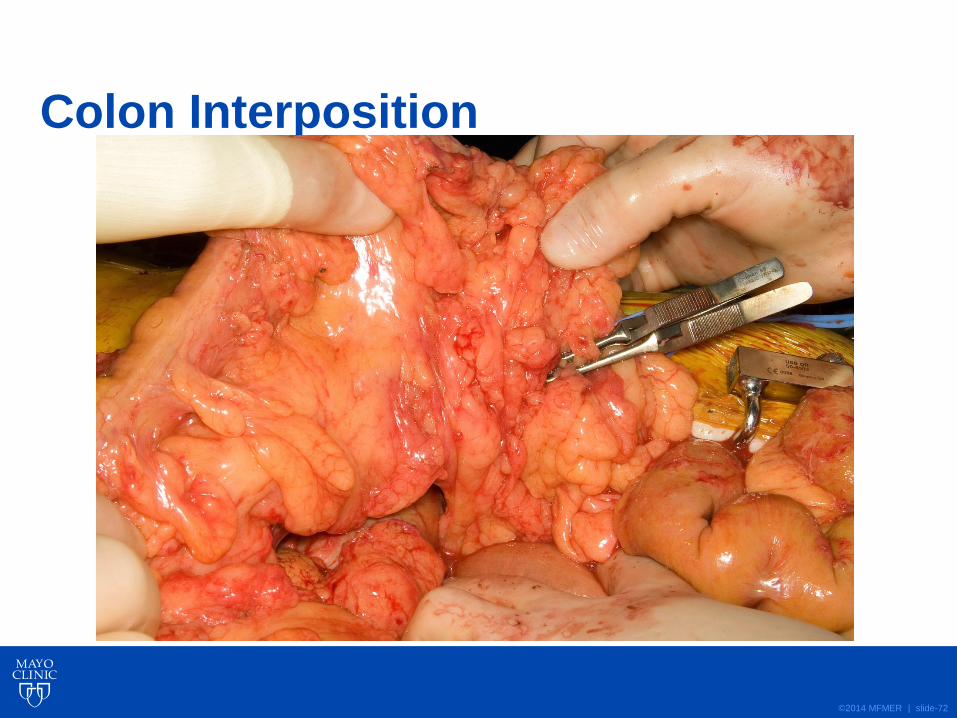
Colon Interposition

©2014 MFMER | slide-70
Colon Interposition

©2014 MFMER | slide-71
©2014 MFMER | slide-72
Colon Interposition
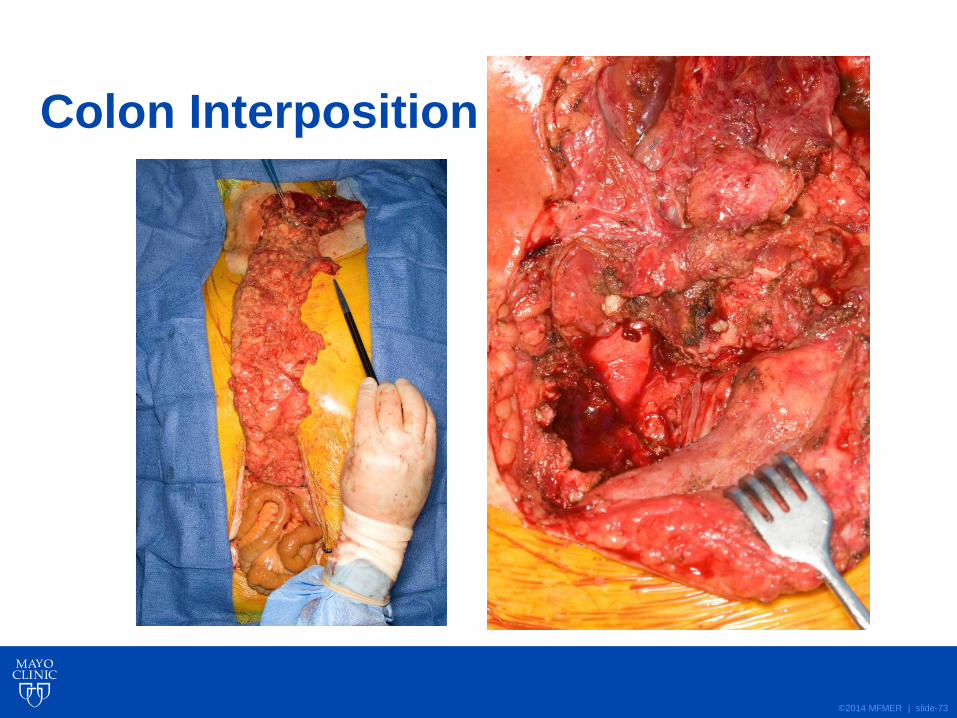
©2014 MFMER | slide-73
Colon Interposition
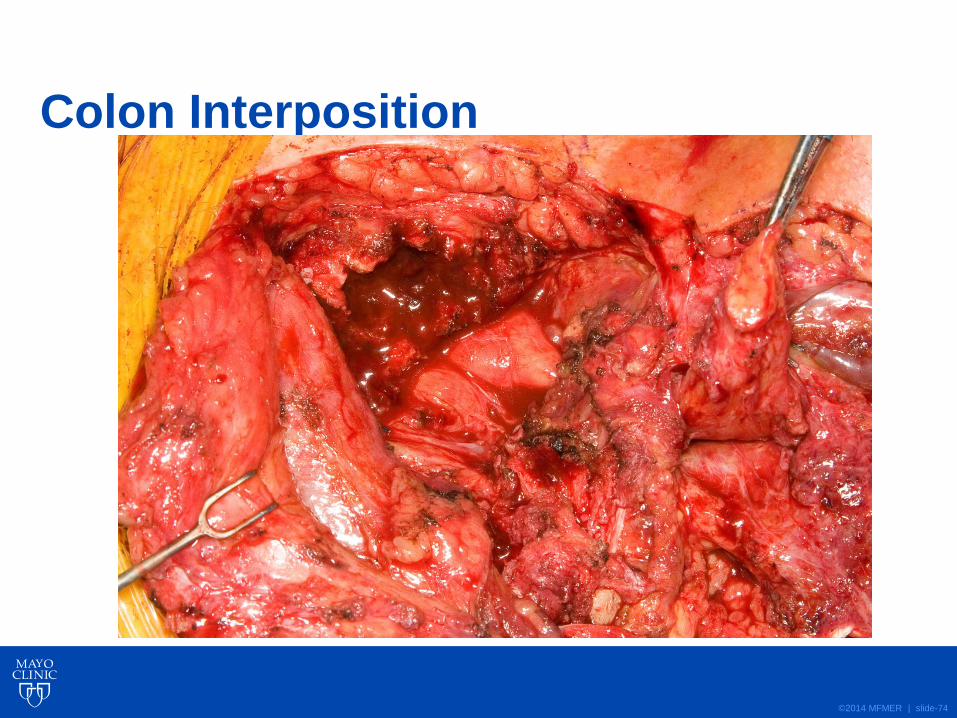
©2014 MFMER | slide-74
Colon Interposition

©2014 MFMER | slide-75
Colon Interposition
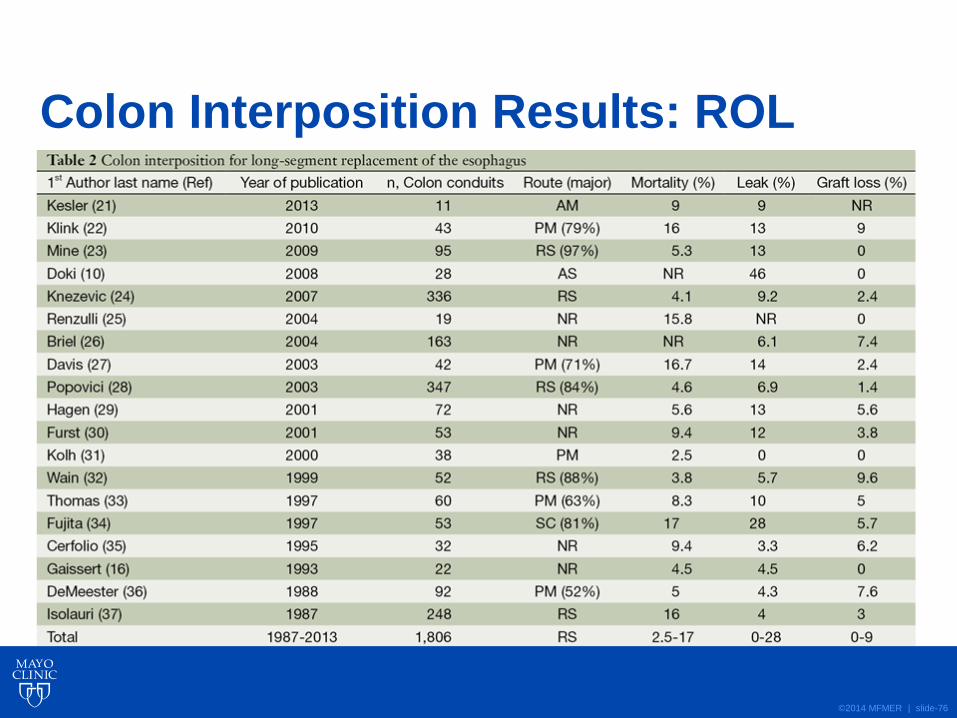
©2014 MFMER | slide-76
Colon Interposition Results: ROL
©2014 MFMER | slide-77
Esophageal Replacement
• Patients who have acquired long segment esophageal discontinuity and lack stomach as a viable replacement conduit primarily have two options for reconstruction:
• jejunum
• colon
©2014 MFMER | slide-78
Esophageal Replacement
• On the contrary, shorter esophageal segmental replacement has many other options:
• free pedicled forearm skin tubes
• folded myocutaneous flaps
• Short jejunal segment
©2014 MFMER | slide-79
Esophageal Replacement
• The future may hold many other options:
• Tissue-engineered 3-dimensional scaffolds repopulated with stem cells have already been used to replace the trachea
• Esophageal stents have now given us the ability to bridge a disconnected segment of bowel and allow for regrowth of tissue and establish new continuity
©2014 MFMER | slide-80
Esophageal Replacement
• Our group has successfully reconnected a distal esophagus to jejunum with a 2 cm separation with the use of stenting alone
• The addition of antibiotics, stem cells, chemo-attractants, and other materials may enhance healing and re-growth of healthy tissue over the stent matrix
©2014 MFMER | slide-81
Question 1
• The “super-charged” jejunal interposition typically bases the blood supply to the superior arcade upon:
a) The axillary artery and vein
b) The internal mammary artery and vein
c) A vein loop graft off the aorta to the left subclavian vein
d) The carotid artery and jugular vein
©2014 MFMER | slide-82
Question 1
• The “super-charged” jejunal interposition typically bases the blood supply to the superior arcade upon:
a) The axillary artery and vein
b) The internal mammary artery and vein
c) A vein loop graft off the aorta to the left subclavian vein
d) The carotid artery and jugular vein
©2014 MFMER | slide-83
Question 2
• The typical blood supply to the abdominal jejunal includes which purpose for each branch:
a) 1-SMA 2-LIMA 3-bridge 4-SMA
b) 1-SMA 2-SMA 3-bridge 4-SMA
c) 1-SMA 2-LIMA 3-SMA 4-SMA
d) 1-SMA 2-bridge 3-bridge 4-SMA
©2014 MFMER | slide-84
Question 2
• The typical blood supply to the abdominal jejunal includes which purpose for each branch:
a) 1-SMA 2-LIMA 3-bridge 4-SMA
b) 1-SMA 2-SMA 3-bridge 4-SMA
c) 1-SMA 2-LIMA 3-SMA 4-SMA
d) 1-SMA 2-bridge 3-bridge 4-SMA
©2014 MFMER | slide-85
Question 3
• When stomach is not available for esophageal conduit, which one of the following is not an option:
a) colon
b) jejunum
c) pleura
d) skin
©2014 MFMER | slide-86
Question 3
• When stomach is not available for esophageal conduit, which one of the following is not an option:
a) colon
b) jejunum
c) pleura
d) skin

©2014 MFMER | slide-87

©2014 MFMER | slide-88
Thank you for your attention.
©2014 MFMER | slide-89
Case
• CC: cough due to aspiration
• HPI: A 17 year old woman presented with a complicated history of congenital TEF repair, chronic esophageal stricture, multiple foregut procedures, and an inability to swallow- she has been fed by a G tube for the majority of her life…

©2014 MFMER | slide-90
History
4/25/94
birth
TEF repair
3 m:
Nissen
&
G Tube
3 y:
Re-do
Nissen
&
G Tube
3.3 y:
Repair
Of
Vascular
ring
Dx
w
Tracheo-
malasia
Aspiration, G-tube feeding, serial dilations (>30-40)
9 y:
LLL
for
Bronch-
iectasis
13 y:
Started
propulsid
17 y.o.

©2014 MFMER | slide-91
She had a type C TEF:

©2014 MFMER | slide-92
What would you do?
• She needs entire length of esophagus replaced
• Her stomach has had previous surgeries (fundo/G tube), and one of these resulted in the G tube going through the GE vessel
• Options:
• Colon interposition
• Jejunum