vanderbilt sports medicine seacsm clinical conference i lt. shoulder pain out of proportion to the...
TRANSCRIPT

Vanderbilt Sports Medicine
SEACSM Clinical ConferenceI
Lt. Shoulder Pain Out of Proportion to the Stimulus
David G. Liddle, MDVanderbilt Sports Medicine
February 11, 2012

Vanderbilt Sports Medicine
History• 18-year-old right-hand-dominant high school student who plays
football and baseball with left shoulder pain
• Began 2 months prior to presentation without specific injury– Football season had finished
– Not working out or doing anything differently
– Present intermittently since it began
• Able to snow ski in Gatlinburg without injury 10 days prior to eval
• No h/o prior shoulder injury

Vanderbilt Sports Medicine
History• Pain worse over 4 days prior to presentation; particularly
around the posterior aspect of his shoulder• Pain at rest and worse with any movement • No paresthesias or vascular symptoms• No known fever but endorses a drenching sweat the night
before presenting to clinic• Naproxen, ice, and Lortab provide little relief• Only PMH is a recent Rt. Knee MRSA cellulitis; Tx w/ Bactrim• Otherwise healthy

Vanderbilt Sports Medicine
Physical Exam• Appears fatigued, ill, & in obvious pain
• Holds his arm still at his side
• No warmth, erythema, or rash and no swelling in BUE
• PROM in any plane of motion causes significant pain around the posterior aspect of his shoulder
• TTP over the posterior aspect of his shoulder with pain out of proportion to the stimulus– No tenderness around the medial edge of the scapula
• Pain worst with resisted internal > external rotation – No pain with biceps strength testing
• Normal sensation and pulses
Vanderbilt Sports Medicine
Questions
Vanderbilt Sports Medicine
Differential Diagnoses
Vanderbilt Sports Medicine
Data
• Labs– CBC – WBC 18.4 w/ 88% PMN but o/w NL
– CMP – WNL x/ non-fasting glucose 130
– ESR – 48
– CRP – 264

Vanderbilt Sports Medicine
Shoulder XRays

Vanderbilt Sports Medicine
MRI

Vanderbilt Sports Medicine
Diagnosis and Treatment• Admission Diagnosis– Myositis of Subscapularis and Infraspinatus
complicated by SIRS
• Management– Referred to ED for evaluation & admission
– Found febrile & septic; Started IVF and Abx• Obtained Blood Cx x 2 & started Vancomycin in ED
– Admit to Internal Medicine w/ Ortho Consult

Vanderbilt Sports Medicine
Treatment• Initial blood cultures grew MRSA• Hospital Day 4– Transferred to the ICU for hypoxic respiratory
distress

Vanderbilt Sports Medicine
Chest XRay

Vanderbilt Sports Medicine
Chest CT

Vanderbilt Sports Medicine
Treatment• Transthoracic echocardiogram – No infective endocarditis

Vanderbilt Sports Medicine
Treatment
Vanderbilt Sports Medicine
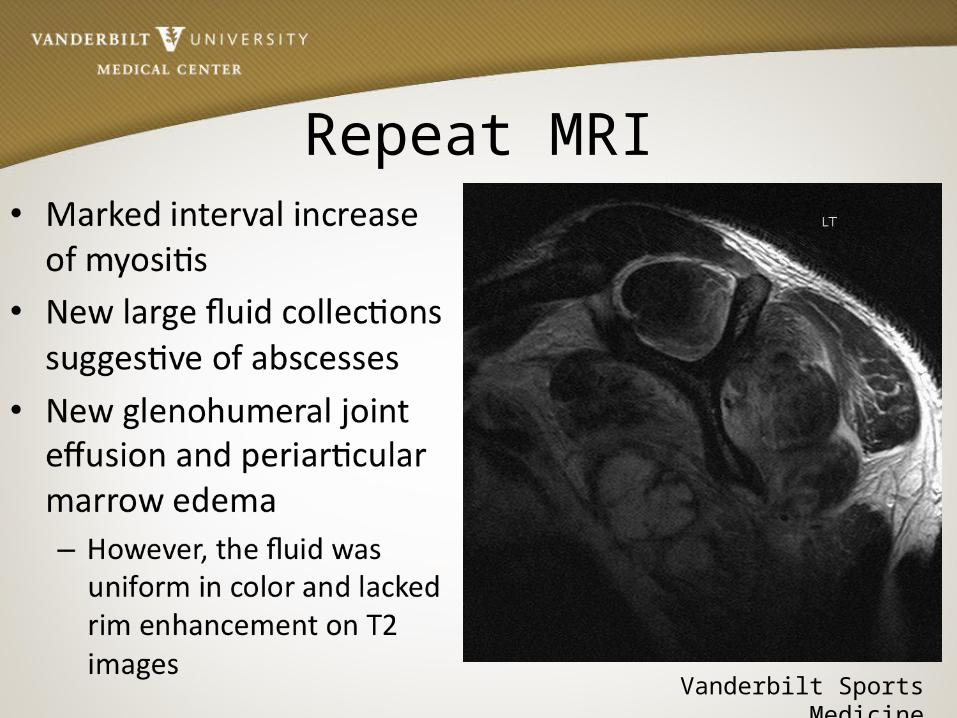
Repeat MRI

Vanderbilt Sports Medicine
Treatment• Shoulder explored on HD7 given continued pain and
fever and increased inflammatory markers• Operative Report– “no purulent material”– “myositis that was swollen as a result of the fascial bands
in the subscapularis appearing to be walled off, but in fact there was no abscess.”
– “irrigated his shoulder” & “put in a gram of vancomycin to put on some local antibiotic coverage.”

Vanderbilt Sports Medicine
Final Diagnoses• Lt. Subscapularis & Infraspinatus Myositis– No septic arthritis or osteomyelitis
• Sepsis with MRSA Bacteremia– No e/o endocarditis or infective thrombophlebitis
• TEE not obtained due to respiratory distress and likely no change in Abx therapy given no e/o IE on TTE and resolved bacteremia
– Presumed source from Rt. Knee furuncle/cellulitis
• Hypoxic respiratory distress• Septic pulmonary emboli

Vanderbilt Sports Medicine
Outcome• Pain resolved by POD1• WBC peaked at 18 after initial improvement to 12; 16 at discharge• CRP 260 on admit, Peak 442, 260 prior to d/c• Respiratory distress & hypoxia resolved• Discharged on HD11 with PICC line to continue Vancomycin for a
total of 6 weeks – Changed to Bactrim for 2 weeks followed by MRSA decolonization therapy
• No pain and normal ROM in Orthopedic clinic on post-HD5• Chest XRay 6 weeks after admission showed near resolution of
septic emboli• Returned to play baseball that spring

Vanderbilt Sports Medicine
Questions or Comments

Vanderbilt Sports Medicine
Thank You