vascular(gra(infec/ons( - amazon s3 · vascular(gra(infec/ons(pranav(somaiya...
TRANSCRIPT

Vascular Gra* Infec/ons
Pranav Somaiya Ins/tute for Transla/onal
Research(IfTR)
#IPP-‐BI

Defini/ons
• difficult
• however there are well developed systems of classifica/on of prosthe/c vascular gra* infec/ons (PVGIs)
• for the purposes of today’s talk I will be focusing on Samson Groups 3-‐5
#IPP-‐BI

classifica/ons Szilagyi Definition of infection Samson Definition of infection
Group 1 dermis only Group 1
no deeper than dermis
Group 2 extends to subcut tissues, doesnt invade implant
Group 2
involve subcut tissue, not come into contact with graft
Group 3 arterial implant involved Group 3
involve body of graft but not anastomosis
based on level of: • anatomic invasion • gra* involvement
Group 4
surrounds exposed anastomosis, no bacteramia/bleeding
Group 5
involve graft-to-artery anastomosis, associated with septiceamia/bleeding

Diagnosis – Exis/ng tools
• Microbiology based techniques: -‐ culture -‐ PCR and sonica/on techniques • Imaging techniques -‐ CT scans -‐ PET scans
#IPP-‐BI

CT scans
#IPP-‐BI

CT scans

Diagnosis -‐ Microbiology
• Standard microbiology based techniques are woefully inadequate
• No standards are set na/onally on methods for microbiology based diagnos/cs for clinical laboratories to follow
• No guidelines are agreed on /ssue handling of PVGI explants
#IPP-‐BI

Treatment – Medical Management
• non-‐surgical treatment is reserved for pa/ents who are surgically deemed unfit for surgery due to associated co-‐morbidi/es
• the standard treatment is long term oral an/bio/c administra/on
#IPP-‐BI

Treatment – Surgical Management
To explant or not to explant is the ques/on? P Somaiya – circa 2012
#IPP-‐BI

Treatment – Surgical Management
• Samson group 3 PVGIs respond best to gra* salvage and muscle flaps for /ssue cover (Zetrenne et al, 2006) with be[er limb salvage rates and lower mortality
• microbiology plays a major role in the salvage of these gra*s and certain organisms like MRSA are thought to be associated with higher limb loss
#IPP-‐BI
Treatment – Surgical Management
• Data on explan/ng of Samson group 4 and 5 is patchy and there is clear management strategy for pa/ents, although explanta/on of the gra* is carried out in a majority of the situa/ons
• microbiology plays a rela/vely minor role in management of these pa/ents
#IPP-‐BI

Treatment – Surgical Management
How now? Anatomic or extra anatomic? Dead…
P Somaiya – circa 2012
#IPP-‐BI

Treatment – Surgical Management
• Extra – Anatomic By pass a*er explan/ng of original gra*

Treatment – Surgical Management
• Anatomic By pass a*er explan/ng of original gra*
#IPP-‐BI

Case studies
#IPP-‐BI

Case 1
#IPP-‐BI

History
• MS • 67yr old Asian man • seen in clinic – pulsatile groin swelling of a
couple of weeks duration • no h/o trauma • no h/o systemic infection
#IPP-‐BI

Background
Comorbidities IHD CABG 1999, then 2010 Hypothyroid HTN PVD Aorto-bifem graft Fem-Pop x2 Decreased Ex Tolerance Independent of ADLs
Regular Medications Nicorandil 10mg OD Levothyroxine 125mcg OM Atorvastatin 40mg ON Fluoxetine 20mg OD Amlodipine 5mg OD Atenolol 50mg OD Lisinopril 10mg OD Pregabalin 300mg BD Omeprazole 20mg OD Warfarin 4mg OD
#IPP-‐BI

Appearance
#IPP-‐BI

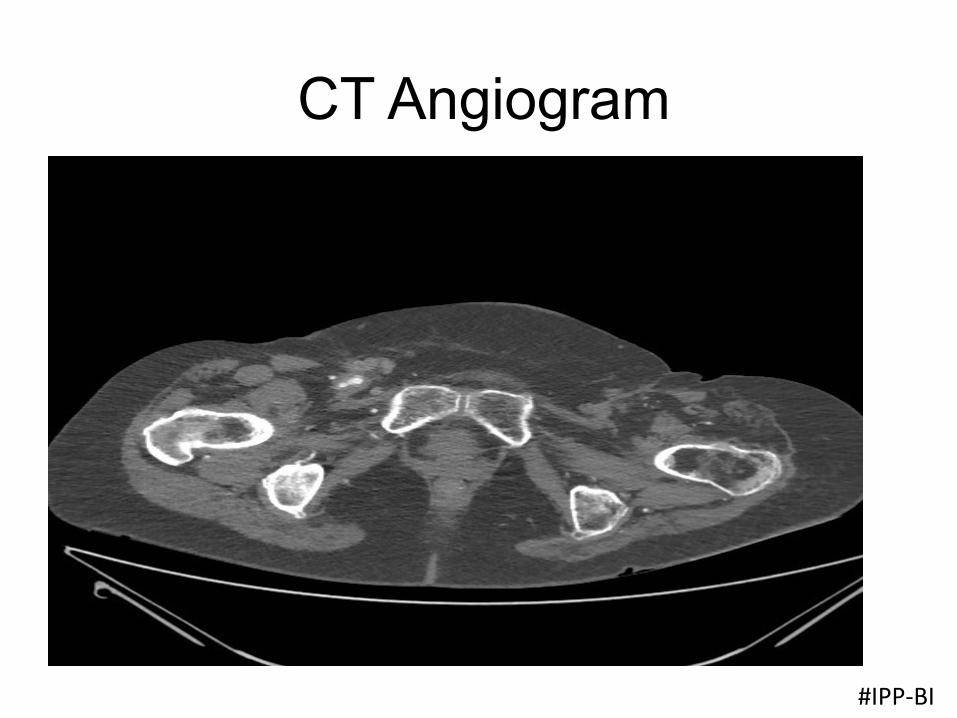
CT Angiogram
#IPP-‐BI

CT Angiogram
#IPP-‐BI

CT Angiogram
#IPP-‐BI

CT Angiogram
#IPP-‐BI

Complicated anatomy....

Case 2
#IPP-‐BI

History
• CS • 64yr old lady • presented to A&E with a critically
ischaemic LL • previous amputee • no h/o systemic infection
#IPP-‐BI

Background
L to R fem-‐fem cross over gra*
Aorto-‐bifem bypass gra*
L fem-‐pop followed by L SFA pop
L fem-‐distal followed by L above knee amputa/on
R fem-‐pop
R fem-‐pop(below knee)
R profundaplasty and stent
R fem-‐distal(we did this)
#IPP-‐BI
CT Angiogram
#IPP-‐BI

CT Angiogram
#IPP-‐BI

Appearance
#IPP-‐BI

CT Angiogram
#IPP-‐BI

CT Angiogram
#IPP-‐BI

Acknowledgements clinical colleagues and bosses from the years gone by at East Kent University Hospital Whipps Cross University Hospitals NHS Trust Queens Hospital, Romford Princess Alexandra Hospital, Harlow Mr J Refson(PAH) – friend and guide Mr S Jacob(QH) – mentor Mr J Coker(QH) – friend and guide Mr O Agu(UCLH/RFH) – clinical tutor and guide and most importantly my juniors who listen to me whiQle on for hrs and my scrub staff who give me ‘what I need not what I ask for’….without you all I would not be here!
#IPP-‐BI