vital and health statistics, series 1, no. 37. 10/97 center for health statistics edward j. sondik,...
TRANSCRIPT

Series 1No. 37
Plan and Operation of theNational Survey of AmbulatorySurgery
October 1997
Vital andHealth StatisticsFrom the CENTERS FOR DISEASE CONTROL AND PREVENTION /National Center for Health Statistics
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICESCenters for Disease Control and Prevention
National Center for Health Statistics

Copyright information
All material appearing in this report is in the public domain and may bereproduced or copied without permission; citation as to source, however, isappreciated.
Suggested Citation
McLemore T, Lawrence L. Plan and operation of the National Survey ofAmbulatory Survey. National Center for Health Statistics. Vital Health Stat 1(37).1997.
Library of Congress Catalog Card Number
McLemore, Thomas.Plan and operation of the National Survey of Ambulatory Surgery (NSAS).p. cm. — (Vital and health statistics. Ser. 1, Programs and collection
procedures ; no. 37) (DHHS publication ; no. (PHS) 98-1313)By Thomas McLemore and Linda Lawrence.Includes bibliographical references.ISBN 0-8406-0532-31. National Survey of Ambulatory Surgery (U.S.) 2. Ambulatory
surgery—Research—United States—Methodology. 3. Medical caresurveys—United States. I. Lawrence, Linda, 1948- II. National Center for HealthStatistics (U.S.) III. Title. IV. Series. V. Series: DHHS publication ; no (PHS)98-1313.
[DNLM: 1. National Survey of Ambulatory Surgery (U.S.) 2. AmbulatoryCare. 3. Data Collection—methods. 4. Health Surveys—United States. 5.Research Design. W2 A N148va no. 37 1997]RA409.U44 no. 37[RD27.42]362.1'07'23 s—dc21[617'.007'23]DNLM/DLC 97-36605for Library of Congress CIP
For sale by the U.S. Government Printing OfficeSuperintendent of DocumentsMail Stop: SSOPWashington, DC 20402-9328Printed on acid-free paper.

Plan and Operation of theNational Survey of AmbulatorySurgery
Series 1:Programs and Collection ProceduresNo. 37
Hyattsville, MarylandOctober 1997DHHS Publication No. (PHS) 98-1313
Vital andHealth Statistics
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICESCenters for Disease Control and PreventionNational Center for Health Statistics

National Center for Health Statistics
Edward J. Sondik, Ph.D.,Director
Jack R. Anderson,Deputy Director
Jack R. Anderson,Acting Associate Director forInternational Statistics
Lester R. Curtin, Ph.D.,Acting Associate Director forResearch and Methodology
Jacob J. Feldman, Ph.D.,Associate Director for Analysis,Epidemiology, and Health Promotion
Gail F. Fisher, Ph.D.,Associate Director for Data Standards,Program Development, and Extramural Programs
Edward L. Hunter,Associate Director for Planning, Budget,and Legislation
Jennifer H. Madans, Ph.D.,Acting Associate Director forVital and Health Statistics Systems
Stephen E. Nieberding,Associate Director forManagement
Charles J. Rothwell,Associate Director for DataProcessing and Services
Division of Health Care Statistics
W. Edward Bacon, Ph.D.,Director
Thomas McLemore,Deputy Director
Robert Pokras,Chief, Hospital Care Statistics Branch
Contents
Abstract. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Introduction. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Background. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1
Feasibility Study. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Purpose. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 2Design and Methods. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 3Recommendations. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
Pretest. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Sampling Frame and Sample Selection. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Data Collection Methods. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5Results. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7
The 1994 National Survey of Ambulatory Surgery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Sample Design. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 7Data Collection Procedures. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10Data Processing. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Estimation Procedures. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Reliability of Estimates. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14Data Dissemination. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16
References. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 17
Appendix I . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Legislative Authorization. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18
Appendix II. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 18Members of the Technical Advisory Panel for the Feasibility Study of the National Survey of Ambulatory Surgery. . . . . 18
Appendix III . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19Letters and Data Collection Instruments for the Feasibility Study of the National Survey of Ambulatory Surgery. . . . . . . 19
Appendix IV. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 69Letters and Data Collection Instruments for the Pretest of the National Survey of Ambulatory Surgery. . . . . . . . . . . . . . . 69
Appendix V. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92Definitions of Terms Used in the Survey. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 92
Appendix VI . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93Data Collection Forms Used in the 1994 NSAS. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 93
Appendix VII . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 117Introductory Letter. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 117
Appendix VIII . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118Endorsement Letters. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 118
Appendix IX. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123Definition of Terms Relating to the Medical Abstract Form. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 123
iii
Text Tables
A. Data elements collected in the Feasibility Study field test and recommended for use in the national survey. . . . . . . . . . . 4B. Number of hospitals and freestanding ambulatory surgery centers by facility specialty and region: National Survey of
Ambulatory Surgery, 1993. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 8C. List of types of service to classify hospitals in the 1994 National Survey of Ambulatory Surgery. . . . . . . . . . . . . . . . . . . 9D. List of specialties used to classify the freestanding ambulatory surgery centers in the 1994 National Survey of
Ambulatory Surgery. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 9E. Number of facilities in the 1994 National Survey of Ambulatory Surgery sample, number and percent of in-scope
facilities, and response rates by type of facility. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12F. Parameters for use in the relative standard error formulae for the National Survey of Ambulatory Surgery by selected
characteristics: United States, 1994. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 15
iv

Plan and Operation of theNational Survey of AmbulatorySurgeryby Thomas McLemore, M.S.P.H., and Linda Lawrence, Division ofHealth Care Statistics
e
Introduction
I n April 1994, the National Centerfor Health Statistics (NCHS)initiated the National Survey of
Ambulatory Surgery (NSAS) to gatherand disseminate information aboutambulatory surgery occurring inhospitals and freestanding ambulatorysurgery centers. NCHS has authorityunder Section 306(b)(1)(F) of the PublicHealth Service Act (42 USC 242k) tocollect data concerning the public’s useof health care and services (seeappendix I). This report summarizes thebackground and development of theNSAS and provides the survey’s designand methodologies.
Background
Since 1965, NCHS has providedannual data on the Nation’s use oinpatient medical and surgical care
provided in non-Federal, short-stayhospitals. These data, collected throughthe National Hospital Discharge Survey(NHDS), have been extensively used inmonitoring changes and analyzing the
This report describes the development and methoSurgery (NSAS). The design and execution of a laccomplished without the participation of a large nNational Center for Health Statistics (NCHS), in pMethods Staff, Office of Research and MethodoloBranch), and many others outside NCHS, participcontractor, the Center for Health Policy Studies, cCensus conducted the pretest and data collectionfacilities and their staffs without whose support ancompleted. This report was peer reviewed by MarAnnette F. Holman of the Publications Branch, Di
f
types of surgical treatment provided forhospital inpatients. However, advancesin medical technology, such asendoscopic techniques and newanesthetic drugs that allow patients toregain consciousness more quicklyfollowing surgery, have increasinglyenabled many procedures to beperformed outside the hospital inpatientsetting (1).
In addition, concern about risinghealth care costs led to changes in theMedicare program that encouraged theuse of ambulatory surgery. In the early1980’s, the Medicare program wasexpanded to cover care in ambulatorysurgery centers, and a prospectivepayment system based ondiagnosis-related groups (DRG’s) wasadopted for hospital inpatient care thatcreated strong financial incentives forhospitals to shift less complex surgeryto outpatient settings. Many StateMedicaid plans and private insurersfollowed the lead of the Medicareprogram and adopted similar policies(2).
In settings that provide ambulatorysurgery, the patient enters the facility;receives care that includes at least onesurgical, diagnostic, or therapeuticprocedure; and (generally) leaves on th
The National Survey of AmbulatorySurgery (NSAS), a national probabilitysample survey of ambulatory surgeryvisits in hospitals and freestandingambulatory surgery centers, beganoperation in 1994. This report tracesthe development of the surveyinstruments and procedures, andpresents the survey methodology forthe NSAS.
Keywords : National Survey ofAmbulatory Surgery c procedures coutpatients c hospitals
Page 1
ds used in the 1994 National Survey of Ambulatoryarge survey such as NSAS could not have beenumber of people. Many members of the staff of thearticular, Iris Shimizu (Mathematical Statistician, Surveygy), Robert Pokras (Chief, Hospital Care Statisticsated in the development of the NSAS. A privateonducted the 1990 feasibility study. The Bureau of thefor the 1994 study. Lastly, we are indebted to the sampledd cooperation NSAS could not have been successfullyy Moien, edited by Klaudia Cox, and typeset byvision of Data Services.

e
e
Page 2 [ Series 1, No. 37
same day. Facilities providing this typeof care can be hospitals or freestandingambulatory surgery centers.
Ambulatory surgery settings providea wide variety of surgical proceduresincluding tonsillectomy, myringotomy,lens extraction (and insertion of anartificial lens), dilation and curettage ofuterus, repair of hernia, laparoscopictubal ligation, and arthroscopic surgery.Also included are diagnostic proceduresincluding biopsy and endoscopicexaminations and therapeutic proceduresuch as injection or infusion of cancerchemotherapeutic substances. Asmedical technology progresses,additional procedures will move toambulatory surgery settings.
The growth of freestandingambulatory surgery facilities has beendramatic. In 1983, there were 239freestanding surgery centers performingapproximately 377,000 surgicalprocedures (3). By 1993, there were1,862 facilities performing more than3.2 million procedures (4).
There has also been a rapid growthof ambulatory surgery in hospitals. Datafrom the SMG Marketing Groupindicate that in 1993, U.S. hospitalsperformed about 12.4 million outpatientsurgical procedures and that about52 percent of all surgery in hospitalswas ambulatory surgery (5). Together,these figures indicate that ambulatorysurgery accounted for approximately58 percent of all surgery in 1993.
The decline of selected procedures(e.g., cataract extraction) on an inpatienbasis has been documented by theNHDS (6). However, the concurrentgrowth of ambulatory surgery has notbeen documented, resulting in a seriousgap of information about surgical care.
Valid data about the medical andsurgical care provided in hospitals andfreestanding ambulatory surgery centersare necessary to make national and locadecisions for the allocation of resourcesand training of medical manpower, toaid efforts to control medical costs, andto plan for the provision of futuremedical and surgical care. This need formore complete surgery data isaccentuated by the rapidly agingpopulation and the introduction of newmedical technology. Therefore, theomission of ambulatory surgery from
s
t
l
the surgical care database has left asignificant gap in coverage and limitsthe utility of the current NHDS data.The NSAS was developed to fill thisdata gap and to respond to theincreasing demand for more completesurgery data.
The NSAS is one of the NCHSestablishment surveys, collectivelycalled the National Health Care Survey(NHCS). The NHCS was designed toprovide nationally representative data othe use of health care resources for themajor sectors of the health care deliverysystem and to address the dramaticchanges occurring in the health caredelivery system during the 1980’s. Atthe request of NCHS, the plan todevelop the NHCS was evaluated by apanel of experts convened by theNational Academy of Sciences and theInstitute of Medicine. In the final reportfrom the evaluation,Toward a NationalHealth Care Survey: A Data System forthe 21st Century,the panel stated that it‘‘endorses the center’s plan to extendcoverage of the health care providersurveys to include additional health caresettings that have emerged in recentyears.’’ The original NHCS planincluded the development of a survey ohospital-based and freestandingambulatory surgery centers (7).
The plan for NHCS included arestructuring of its ‘‘traditional’’ surveysof health care providers and anexpansion of coverage to other majorsectors of the health care system. Undethis plan, the ‘‘traditional’’ surveys—theNHDS, the National AmbulatoryMedical Care Survey (NAMCS), theNational Nursing Home Survey(NNHS), and the National MasterFacility Inventory (NMFI)—weremodified to form an integrated NHCS.Two new health care establishmentsurveys, in addition to the NSAS, weredeveloped and fielded during the early1990’s. These surveys included theNational Hospital Ambulatory MedicalCare Survey (NHAMCS), whichprovides data on the utilization ofservices in hospital emergency andoutpatient departments, and the NationaHome and Hospice Care Survey(NHHCS), which provides data on theservices and staff of home healthagencies and hospices and on the
n
f
r
l
personal and health characteristics ofcurrent and discharged patients (8).
One of the first steps in developingthe NHCS was to identify viablesampling frames or listings of healthcare providers and establishments. Theslistings could be based on availabledatabases and/or developed based on thNational Master Facility Inventory(NMFI) methodology. The NMFImethodology involved identifyingavailable facility files, compiling listingsby facility type, processing the lists tocreate an unduplicated file, andcollecting additional information oneach facility through a mail survey. In1986, an evaluation of the coverage ofthe health facilities in the NMFI wasconducted under contract with La JollaManagement Corporation (9). Resultsapplicable to the development of theNSAS indicated that complete andaccurate lists of ambulatory surgeryfacilities could be collected; however,the NMFI methodology could not beused exclusively for developing listingsof these facility types. Use of both theNMFI methodology and data from theSMG Marketing Group wasrecommended for inventorying thesefacilities. Study findings also included aproposed definition of ‘‘ambulatorysurgery center’’ and suggested criteriafor differentiating ambulatory surgeryfacilities from private physicianpractices (10).
Feasibility Study
The development of the NationalSurvey of Ambulatory Surgerybegan with a study initiated in
1989 under contract to the Center forHealth Policy Studies to assess thefeasibility of collecting ambulatorysurgery data from hospitals andfreestanding ambulatory surgery centers(11,12).
PurposeWith the NMFI evaluation study
providing the foundation, the objectivesof the feasibility study were to providedetailed recommendations concerningthe design of a national survey of

ambulatory surgery, including thedefinitions of the universe of facilitiesand of surgical visits within facilities tobe sampled, the data set to be collected,the methodology to be employed, andthe estimated costs for a national surveyA principal focus of the study was toassess the extent to which the methodsused for the National Hospital DischargeSurvey (NHDS) could be adapted to anational survey of ambulatory surgery.Alternative methodologies were alsoinvestigated.
An expert advisory panel consistingof representatives of professional andtrade associations provided advice ontechnical issues throughout thefeasibility study. The panel reviewed thedesign and findings from the field testand assisted in formulatingrecommendations for a national survey.Members of the feasibility studytechnical advisory panel are listed inappendix II.
Design and MethodsThe feasibility study was conducted
in two phases. During Phase I, methodsand practices for collecting dataregarding ambulatory surgery andambulatory surgery facilities wereinvestigated. These activities included acomprehensive literature review; anevaluation of the number andcharacteristics of hospital-based andfreestanding ambulatory surgery centers;an investigation of the definition of theuniverse of ambulatory surgical facilities(hospital-based and freestanding) and ofpotential sampling frames; an evaluationof the accessibility and cost of selectingsamples and collecting data from thesesites, including an investigation of thesource, availability, and content ofcomputerized files for ambulatorysurgery centers; and an evaluation of thecomprehensiveness, availability, andreliability of these data. A workingdefinition for identifying types ofambulatory surgery visits to be includedand/or excluded from the samplingframe within hospitals was alsodeveloped.
Based on this background research,it was hypothesized that a datacollection methodology similar to themethodology employed in the National
.
Hospital Discharge Survey (NHDS), aretrospective records review, could beused to conduct a national survey ofambulatory surgery. A preliminarydataset was identified and operationaldefinitions were developed, samplingframes and definitions were developed,and the NHDS methodology wasmodified to fit the data collection needsof an ambulatory surgery survey. Thedata collection plan consisted of adetailed outline of the field testmethodology that included all surveyinstruments, training materials, letters ointroduction, protocols, and samplingmethodologies.
During Phase II of the feasibilitystudy, a field test was conducted.Because freestanding ambulatorysurgery centers tended to be locatedprimarily in medium-to-large cities, thefield test was restricted to metropolitanstatistical areas (MSA’s). The selectionof MSA’s was made to providegeographic diversity, to provide asufficient pool of ambulatory surgerycenters, and to avoid MSA’s in whichthe NHDS was being conducted. Thefield test included two types of facilitiesin which ambulatory surgery wasperformed: hospitals and freestandingambulatory surgery centers (FSASC’s).Out-of-scope and nonrespondent samplfacilities were replaced in an attempt toinclude about 15 participating facilities,half hospitals and half FSASC’s, in eachof the MSA’s. However, the smallernumber of FSASC’s available in theseareas compared with the numbers ofhospitals and the slightly higher refusalrate among FSASC’s (particularlyamong small eye surgery centers)resulted in a final sample of 51participating hospitals and 33participating FSASC’s. The number offacilities inducted was slightly larger,but several facilities inducted did notprovide abstracts within the datacollection time period, and severalfacilities visited for inductionsubsequently refused to participate.
The facility induction and datacollection phase of the field testoccurred in the first 6 months of 1991.Appendix III contains selected formsand letters used during this phase of thefield test. Using the initial telephone callscript, the contractor’s staff telephoned
f
e
each of the selected facilities to identifyan appropriate contact as well as his/hermailing address and telephone number.After this initial contact, an informationpackage was sent to each sampledfacility that included a letter ofintroduction from NCHS, a descriptionof the feasibility study, letters ofendorsement from the Society forAmbulatory Anesthesia and theFederated Ambulatory SurgeryAssociation, and an NCHS fact sheet.Approximately 10 days later, eachfacility was recontacted by telephone toverify that the facility met the criteriafor inclusion in the feasibility study andto set up an appointment for aninduction interview (see‘‘Script forSecond Phone Call to Facilities’’inappendix III). Facilities identified duringthese screening calls that did not meetthe eligibility criteria were excludedfrom the study. During the inductioninterview, contractor staff met with theappropriate facility contact(s) to explainthe purpose of the study, to explain whatfacility participation involved, and toask for the facility’s cooperation. Once afacility agreed to participate, theremainder of the induction visitconsisted of collecting information onthe facility’s ambulatory surgeryactivities, lists of surgical patients, andmedical records contents.
Facilities that participated in thestudy were given the choice of havingtheir staff sample and abstract medicalrecords or having the contractor’s staffperform these tasks. Because thefeasibility study was testing themethodology for a national survey,extensive sampling and data abstractionwere not required. The sampling wasconducted for a continuous 2-monthperiod and data were abstracted for onemonth of the sampled visits(approximately 20 visits). If facility staffchose to perform the sampling andabstracting, training was provided bycontractor staff.
After data collection wascompleted, quality control visits(consisting of resampling andreabstracting all previously selectedsampled visits) were conducted in 18 ofthe participating facilities. Debriefingvisits occurred in an additional 13participating facilities in an effort to
Series 1, No. 37 [ Page 3

n
Table A. Data elements collected in theFeasibility Study field test andrecommended for use in the nationalsurvey
Facility data and visit identification
Unique facility numberSeparate unit (unique) number (if applicable)Medical record ID numberDate of surgeryZIP Code of patient’s customary residence
Patient characteristics
Date of birth or ageSexRaceExpected source of paymentStatus/disposition of patient
Surgical visit and medical data
Times (operating room, recovery room, anddischarge)Type of anesthesiaAnesthesia administered by (credentials)ASA (American Society of Anesthesiologists)classification of patient (if an anesthesiologist isinvolved)Surgical procedures performedDiagnoses
Page 4 [ Series 1, No. 37
determine what worked well and whatwas problematic with the studymethodology.
RecommendationsThis study demonstrated the
feasibility of collecting ambulatorysurgery data from hospitals andfreestanding ambulatory surgery centersusing the NHDS methodology. Inaddition to providing experience infacility induction and data collection, thefield test identified problem areas andprovided insights into how well theproposed model would work in anational survey. These insights, as wellas the advice of a technical advisorypanel, were used to develop detailedrecommendations to assist with thefuture design of a national survey.Among the major recommendationswere the following:
The survey should include twofacility components—hospitals andfreestanding ambulatory surgery centersFacilities licensed as hospitals offeringoutpatient surgery should represent thehospital portion of the universe.Ambulatory surgery centers licensed byStates and/or certified as ambulatorysurgery centers for Medicarereimbursement should represent theFSASC’s portion of the universe.
The hospital sampling frame shouldinclude noninstitutional hospitals,exclusive of Federal, military, andDepartment of Veterans Affairshospitals, located in the 50 states andthe District of Columbia. Onlyshort-stay hospitals (hospitals with anaverage length of stay for all patients offewer than 30 days) or those whosespecialty is general (medical or surgicalor children’s general should be includedThese hospitals should also have sixbeds or more staffed for patient use.This is the same sampling frame that isused for the NHDS. The sampling framefor the FSASC’s should be compiledthrough a combination of two existingregularly updated machine-readablefiles: the Freestanding OutpatientSurgery Center Database (sold by theSMG Marketing Group) and the HealthCare Financing Administration Providerof Services file. An annual update of thesampling frames was recommended.
.
).
Because of the need for a highparticipation rate, a number of methodsshould be used to encourage andenhance facility participation. Facilitiesshould be given the option ofconducting the sampling and abstractingthemselves, or of having trained dataabstractors do the sampling andabstracting for them. Facilities should becompensated for selecting the sampleand completing the abstracts whenfacility personnel perform these tasks,and for the effort of pulling and refilingrecords when contract staff do theabstracting. Extensive efforts should bemade to obtain letters of endorsementfrom organizations representing thefacilities and the medical recordsprofession.
Identification of ambulatory surgeryvisits within hospitals can be difficult,particularly since hospitals may useslightly different definitions of a surgicalvisit. Generally, but not always,hospitals base their definition ofambulatory surgery on the locationwhere the procedure is performed. Useof a definition that captures all surgeryvisits performed in certain specifiedtypes of special procedure units and inoperating suites is operationally easy toapply and will provide reliable nationalstatistics.
The dataset used in the field testshould be simplified. Some dataelements should be deleted, othersshould be redefined, and data collectortraining should be revised to reflect fieldtest findings.Table Ashows the list ofdata elements that were field tested andrecommended for implementation in thenational survey. Two additional dataitems, ‘‘Ethnicity’’ and ‘‘Total charges,’’although not recommended for theNSAS, were included in the pretest.Although both data items had very lowresponse rates for the feasibility study(4 percent and 57 percent), they wereincluded in the pretest dataset due totheir importance for health care policyand research. The data elements thatwere field tested but not recommendedfor implementation included ‘‘SSNabsent/present,’’ ‘‘Marital status,’’ ‘‘Wassurgery cancelled or terminated?,’’‘‘Place of service,’’ ‘‘Patient and visittypes,’’ ‘‘Post-op anesthesiaassessment,’’ ‘‘Assistants in surgery,’’
‘‘Other services provided as indicated inthe medical record,’’ and ‘‘Outcomefollowup.’’
The field test and the deliberationsof the project’s technical advisory panelprovided the basis for recommending anumber of refinements to the field testinstruments and training materials.Because of these refinements, a pretestwas recommended before implementinga national survey. The testing could bemore limited than was attempted in thefeasibility study, but simplified versionsof the facility induction interview forms,simplified instructions for sampling inhospitals with multiple lists of surgicalpatients, and the recommended changesto shorten the dataset and abstract formneeded to be tested before full surveyimplementation. These findings werealso needed to provide updatedestimates of time required to conductsampling and abstracting, to prepare thefull survey Office of Management andBudget (OMB) approval request, tosupport negotiations for reasonablefacility reimbursement and Bureau ofthe Census (the proposed data collectioagent for the national survey)interagency agreement funding levels,and to prepare data collector trainingmaterials.

Series 1, No. 37 [ Page 5
Pretest
The pretest for a National Surveyof Ambulatory Surgery wasconducted in 1993 by the U.S.
Bureau of the Census as the datacollection agent. The purpose of thepretest was to test and finalize allprocedures, manuals, forms, instructionstraining, and data collection methods forthe NSAS.
Sampling Frame andSample Selection
The sample for the NSAS pretestconsisted of 80 facilities in five primarysampling units (PSU’s): 45 hospitalsselected from the NHDS-eligiblehospitals listed in the 1991 SMGHospital Market Database (13) and 35freestanding ambulatory surgery centers(FSASC’s) selected from the 1991 SMGFreestanding Outpatient Surgery CenterDatabase (14) and/or the Medicare-certified FSASC’s listed in the HCFAProvider-of-Services (POS) file datedFebruary 1992 (15).
The five PSU’s were selected by thefollowing criteria: (a) at least one PSU wasselected from each of the four Censusregions (Northeast, Midwest, South, andWest); (b) selected PSU’s had largenumbers of FSASC’s relative to otherareas; and (c) to the extent possible, allcurrent NHDS PSU’s and areas used in theNSAS feasibility study were excluded.
FSASC’s specializing in eye carewere oversampled to investigatemethods to improve participation ratesin these facilities. Hospitals with higherambulatory surgery volume wereoversampled to maximize opportunitiesto test sampling procedures in facilitiesthat had ambulatory surgery in morethan one location. Additionally, to verifydata contained in the sampling frame, al60 nonsampled facilities in the fivePSU’s were contacted by telephone andasked to verify general informationabout the facility.
Data Collection MethodsMaterials and methodologies that
had been revised based on the feasibilit
,
l
y
study results were provided to the U.S.Bureau of the Census. Census staffdesigned and printed the various surveyforms and questionnaires. Census staffalso prepared the regional officeinstructions, the field representativemanual, the facility manual, the fieldrepresentative self-study, the inductionflashcard, the sampling table, thetraining guide, the training aids, and theregional office checklist.
Six site visits to ambulatory surgeryfacilities in the Washington, D.C., areawere conducted by NCHS and Censusheadquarters staff to help develop thedata collection procedures. During the‘‘dry run’’ training, all materials werereviewed and suggested changes wereincorporated into the final trainingmaterials.
Field training for the pretestincluded a one-half day supervisors’conference, a 4-hour field representativeself-study, and a 1½ day fieldrepresentative classroom trainingsession. During the supervisors’conference, the background of theNSAS was covered; the questionnaires,sample listing operation, and samplingand abstracting methods were reviewed;and the field and office procedures werediscussed. Staff from NCHS and theU.S. Bureau of the Census attended theconference. The self-study coveredinformation about the purposes andobjectives of the pretest, definedambulatory surgery, presented the NSASforms, and discussed the composition ofthe sample. The classroom trainingincluded mock interviews to completethe Telephone Screener Call to SampledFacilities and the InductionQuestionnaire, sampling exercises,abstracting exercises, and role-playingsituations where survey respondentquestions and/or concerns about thepretest were addressed.
The initial contact with each facilitywas a telephone call made by a Censusregional office clerk. Form NSAS-1(X),Initial Telephone Call To SampledFacilities, contains the script used forthis first call (seeappendix IV). Duringthis call, the clerk:
Verified the name and address ofthe facility
Gave a brief explanation of thesurvey
Asked to whom an introductoryletter and information packageshould be sent
Asked if the facility was a hospital,a licensed and/or Medicare-certifiedFSASC
The regional office staff then mailedan introductory letter and informationpackage to the designated official at thesample facility. This package included aletter from NCHS that provided legallyrequired information to the facility andinformed them that a U.S. Bureau of theCensus representative would soon becontacting them, a fact sheet that gaveadditional information about the pretest,six endorsement letters signed byhealth-related organizations to encouragethe facility’s participation in the pretest,the NCHS Staff Manual onConfidentiality, and the National Centerfor Health Statistics Organization andActivities brochure.
The Census field representative’sfirst contact with each facility was thetelephone screener call to the facility.Form NSAS-2A(X), Telephone ScreenerCall To Sampled Facilities, contains thescript used for this call (seeappendixIV). During this call, the fieldrepresentative:
Verified receipt of the introductoryletter and information package
Determined whether the facility wasin scope for the survey
Explained what type of informationwould be collected during theinduction visit
Gave a brief explanation of thesurvey
Requested an appointment for aninduction interview
The only contact with thenonsampled facilities (see previoussection,‘‘Sampling Frame and SampleSelection’’) was the telephone call to thefacility made by the field representative.Form NSAS-2B(X), Telephone Call ToNon-Sampled Facilities, contains thescript used for this call (seeappendixIV). During this call, the fieldrepresentative:
Page 6 [ Series 1, No. 37
Verified the name and address ofthe facility
Gave a brief explanation of thesurvey
Determined whether the facility wasin scope for the survey
Asked several questions about thefacility including how many patientsreceived ambulatory surgery duringthe past 12 months
The Induction Questionnaire,NSAS-3(X), is shown inappendix IV.During the induction interview, the fieldrepresentative:
Completed an in-depth interviewabout the facility with theadministrator or designated contactperson
Obtained information for each logthat contained the types ofambulatory surgery specified duringthe induction visit
Established the method ofparticipation
If necessary, trained designatedfacility staff to sample and/orabstract data
Gave a Thank You Letter to thefacility administrator
For each of the facilities that agreeto participate in the pretest, a 2-monthsample (October–November 1992) ofapproximately 20–25 ambulatorysurgery visits per month was selectedand recorded onto NSAS-4(X) forms,and medical record data were abstracteonto NSAS-5(X) forms for the firstmonth (October) of the sampled visits.Both forms are included inappendix IV.The Medical Abstract form, NSAS-5(X),included all data items recommended inthe feasibility study. Two additional dataitems were included: ethnicity and totalcharges.
In the pretest, two methods ofsampling surgery logs that containedboth inpatient and ambulatory patientswere tested. In one method, every visitwas counted regardless of whether itwas inpatient or ambulatory surgery. Foselected surgical visits that wereinpatient surgery, only the case numberand inpatient status indicator were
d
d
r
recorded on the Sample Listing Sheet,NSAS-4(X). No additional informationwas recorded that would allow themedical records to be pulled and data tobe abstracted. In the other method, onlyambulatory procedures were counted,that is, inpatients were skipped duringthe counting process.
There were two basic methods offacility participation: primary andalternate. In the primary method, facilitystaff pulled the medical records andabstracted medical record data for the20–25 ambulatory surgery visits selectedfor October. For the facilities that had asingle log or list of ambulatory surgeryvisits from which to sample, the facilitystaff also performed the sampling ofapproximately 20–25 ambulatorysurgery visits per month for October andNovember of 1992. For facilities thathad more than one log or list ofambulatory surgery visits from which tosample, the Census field representativeconducted the sampling. Although theNovember sampled visits were notabstracted, 2-month sampling wasnecessary to test sampling methodsacross months. For the primary method,the field representative trained thedesignated facility staff to abstract and,if necessary, to sample the data. Thistraining was conducted during theinduction visit if possible. If not, thefield representative scheduled anappointment to conduct the trainingwhen facility staff were available. Forprimary procedure facilities, the fieldrepresentative returned to the facilityafter the abstracting was completed andedited the forms before leaving.
In the alternate method ofparticipation, the Census fieldrepresentative conducted the 2-monthsampling and data abstracting for theOctober sampled visits. Using thismethod of participation, facilitypersonnel were only responsible forpulling and refiling the medical recordsfor the October sampled visits. Ifpossible, the field representative selectethe October sample during the inductionvisit so these sampled records could bepulled and available for data abstractingwhen they returned at the appointed dayand time to conduct the sampling forNovember.
d
After sampling and abstracting werecompleted for each facility, a Post DataCollection Questionnaire was completedand returned to NCHS. Form NSAS-7A(X) was used by facility staff whoperformed the abstracting (and sampling,if applicable) in primary procedurefacilities to evaluate the pretest. FormNSAS-7B(X) was completed by Censusfield representatives who did thesampling and abstracting in alternateprocedure facilities or the sampling forprimary facilities with multiple logs.These forms (seeappendix IV) wereuseful in determining methods formaximizing participation rates for thenational survey as well as providing anaccurate indication of the responseburden imposed on facility staff forparticipation in the pretest.
The field representatives notifiedtheir supervisors of any facilities thatinitially refused to participate in thepretest. The regional office supervisorsattempted to persuade the facility toparticipate. Procedures were available toprovide compensation for facilityparticipation if they would notparticipate without reimbursement.Although none of the facilities requestedreimbursement for their activities in thepretest, personnel at several facilitiesindicated that compensation would benecessary for participation in an ongoingnational survey.
NCHS selected 12 participatingfacilities for quality control visits thatwere conducted by Census programsupervisors. The quality controloperation included contacting the facilityto set up an appointment, resampling forOctober and November, andreabstracting 10 of the originallysampled medical records.
Although there was no formal editof the NSAS forms in the regionaloffice, their staff checked in andreviewed all completed materials,verified that they received the correctnumber of forms for each completedinduction questionnaire, and checked forcompletion of a few specific items. Theregional office staff sent shipments ofcompleted induction forms to NCHS (inHyattsville, Maryland) on a flow basisand sent completed sampling andabstracting forms to the NCHS dataprocessing facility in Research Triangle

Series 1, No. 37 [ Page 7
Park, North Carolina, where the dataelements were coded and keyed.
A debriefing conference was held inMay 1993 that was attended by regionaloffice supervisors and staff from NCHSand Census headquarters. The agendaincluded discussions of the pretesttraining, data collection activities, andthe forms used in the pretest. Theexperiences of the pretest and thedebriefing discussions formed the basisof the recommendations for the nationalstudy.
Results
Of the 80 sample facilities, 5 weredetermined to be out of scope. Of the 75in-scope facilities, 68 submitted abstractdata, an overall response rate of91 percent. Thirty-nine of the 42in-scope hospitals participated for a93 percent response rate; and 29 of the33 in-scope FSASC’s participated for aresponse rate of 88 percent. Of the 60nonsampled facilities, 12 weredetermined to be out of scope. Of the 48in-scope facilities, 46 provided data, aresponse rate of 96 percent.
Results of the field test of the twomethods for sampling from logs thatcontained both inpatient and outpatientprocedures were inconclusive. TheCensus field representatives did notindicate a preference for either method.Therefore, based on the expectation thatthe nonsampling error would be less, themethod in which every visit wascounted regardless of whether it was aninpatient or outpatient wasrecommended for the national survey.
No major changes wererecommended as a result of the pretestfor a National Survey of AmbulatorySurgery. Minor changes to the datacollection instruments and to theprocedures for the national survey wererecommended. They include:
Increase the classroom training timeby 1/2 day to allow more time forthe sampling exercises
Allow the field representatives(instead of the regional officeclerks) to make the initial contactwith the facility
Include more instructions in thefield representative manual
regarding the determination ofin-scope and out-of-scope facilities
Provide procedures for handlingfacilities that have merged or havebeen purchased
Create an Annual Update form thatincludes new ambulatory surgerylocations, dropped ambulatorysurgery locations, volume for allnew locations, and a new name ofthe CEO and/or medical recordcontact person
Change item 4 in the TelephoneScreener, NSAS-2A(X), to ‘‘In thissurvey we are excluding facilitiesthat are exclusively a familyplanning clinic, birthing center,podiatry center, dentistry center, orabortion clinic. Is (facility)exclusively one of these?’’ Movethe ‘‘abortion clinic’’ category to themiddle or end of the response list
Revise the Induction Questionnaire,NSAS-3(X), to accommodateadditional sets of section V forfacilities that have multiple logs
Delete the items that requestdetailed information on Medicarecertification and state licensure(items 5, 6, 8, 9, and 10) in theInduction Questionnaire,NSAS-3(X), because they wereconfusing and unnecessary. Also,clarify item 7, which requests thenames, addresses, and telephonenumbers of satellite or affiliatedfacilities to include only thosefacilities that perform ambulatorysurgery
Use a log identifier, such as thealpha designation for each log fromthe induction questionnaire (item11), to link the sample visits to aparticular log. A log identifier (listused) field should be added to theSample Listing Sheet, NSAS-4(X),and the Medical Abstract form,NSAS-5(X)
Add an ‘‘other’’ category to item15, type of anesthesia, on theNSAS-5(X)
The Pretest for a National Survey ofAmbulatory Surgery was completed inJune 1993. No major methodological
problems were encountered during thepretest. Based on the successfulcompletion of the pretest, preparationswere begun to finalize the designmethodology and field the NSAS in1994.
The 1994 NationalSurvey of AmbulatorySurgery
The NSAS was first fielded as anational survey in 1994. It wasanticipated that the design and
data collection activities for this surveywould remain constant for a number ofyears; therefore, as an example of theseactivities, the 1994 NSAS is describedbelow.
Sample DesignThe 1994 NSAS used a multistage
probability design with samples ofhospitals and freestanding ambulatorysurgery centers selected at the first orsecond stage and surgical visits selectedat the final stage. The NSAS wasdesigned to provide estimates ofambulatory surgery based on thefollowing priority of survey objectives:U.S., hospitals and freestandingambulatory surgery centers, and region(16). The sampling frames and thesample design are described in thefollowing text.
Sampling Frames
The universe of eligible facilitiesfor the 1994 NSAS consisted ofhospitals and freestanding ambulatorysurgery centers (FSASC’s). Thedetermination of whether an ambulatorysurgery facility was a hospital or afreestanding center was based on thesampling frame (SMG listing) fromwhich a facility was selected. Thehospital universe included allnoninstitutional, non-Federal hospitals inthe 50 states and the District ofColumbia that were either short-stay(had an average length of stay for allpatients of less than 30 days) or ageneral hospital (medical, surgical, or

Table B. Number of hospitals and freestanding ambulatory surgery centers by facilityspecialty and region: National Survey of Ambulatory Surgery, 1993
Facility specialty and regionNumber inuniverse
Number insample
Hospitals with Ambulatory Surgery
All specialties:All regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5,252 368Northeast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 794 73Midwest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,545 84South . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,958 146West . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 955 65
General:All regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 5,104 259Northeast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 763 48Midwest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,517 64South . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,894 104West . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 930 43
All other specialties1:All regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 148 109Northeast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 31 25Midwest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 28 20South . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 64 42West . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25 22
Hospitals without ambulatory surgery2
All regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,015 50Northeast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 125 6Midwest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 173 8South . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 455 24West . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 262 12
Freestanding ambulatory surgery centers
All specialties:All regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,732 333Northeast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 170 61Midwest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 304 64South . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 695 135West . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 563 73
General and multispecialty:All regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 1,184 153Northeast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101 29Midwest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 207 26South . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 478 63West . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 398 35
Ophthalmic:All regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 308 70Northeast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 49 15Midwest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 55 14South . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 101 24West . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 103 17
All other specialties3:All regions . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 240 110Northeast . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20 17Midwest . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 42 24South . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 116 48West . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 62 21
1Includes alcohol and other chemical dependency; children’s general; children’s orthopedic; children’s other specialty; children’spsychiatric; children’s rehabilitation; chronic disease; eye, ear, nose, and throat; institution for the mentally retarded; obstetricsand gynecology; orthopedic; other specialty; psychiatric; rehabilitation; and tuberculosis and other respiratory diseases.2This sample accounts for hospitals that create ambulatory surgery units and that had incorrect sampling frame data.3Includes ear, nose, and throat; gastrointestinal; gynecological; hernia repair; laparoscopy/endoscopy; neurosurgery; orthopedic;other; plastic; and urological.
Page 8 [ Series 1, No. 37
children’s) regardless of average lengthof stay. The hospital also had to havesix or more beds staffed for inpatientuse (seeappendix V). The hospitaleligibility definition is the same as that
used in the National Hospital DischargeSurvey and the National HospitalAmbulatory Medical Care Survey.
The sampling frame for the hospitauniverse was the April 1993 SMG
l
Hospital Market Data Base (17). Asshown intable B, the SMG HospitalMarket Data Base contained 6,267hospitals meeting the NSAS eligibilitycriteria. Of these hospitals, 5,252(84 percent) indicated that ambulatorysurgery was performed in the hospitaland 1,015 (16 percent) indicated that noambulatory surgery was performed inthe facility. Hospitals were defined asperforming ambulatory surgery if thehospital file indicated a nonzero numberof ambulatory surgeries.
The universe of freestandingfacilities consisted of freestandingambulatory surgery centers (FSASC’s)that were regulated by States or werecertified for Medicare by the HealthCare Financing Administration (HCFA).The sampling frame for the FSASCuniverse consisted of facilities listed inthe 1993 SMG Freestanding OutpatientSurgery Center Database (18) and/orMedicare-certified facilities listed inHCFA’s Provider-of-Services (POS) file(seeappendix V) (19). Facilitiesspecializing in dentistry, podiatry, painblock, abortion, family planning, orbirthing were excluded. Duplicates inthe combined list were removed prior tosampling. There were 1,732 eligiblefacilities on the FSASC sampling frame.
Each hospital was classified by itstype of service or specialty. Each facilityon the FSASC sampling frame wasassigned a facility specialty based on thespecialty data from the SMG or POSfile. If only one specialty was listed, thefacility was assigned that specialty. Iftwo or more specialties were listed, thefacility was designated as multispecialty.The 16 hospital types and 13 FSASCspecialty groups in the 1994 NSAS areindicated intables CandD, respectively.Ninety-eight percent of theNSAS-eligible hospitals were classifiedas general (including medical, surgical,or children’s). Sixty-eight percent of theNSAS-eligible FSASC’s were classifiedas general surgery or multispecialty and18 percent were ophthalmic surgery (seetable B).
Facility Selection
The NSAS facility sample wasselected independently within two strata:hospitals with ambulatory surgery and
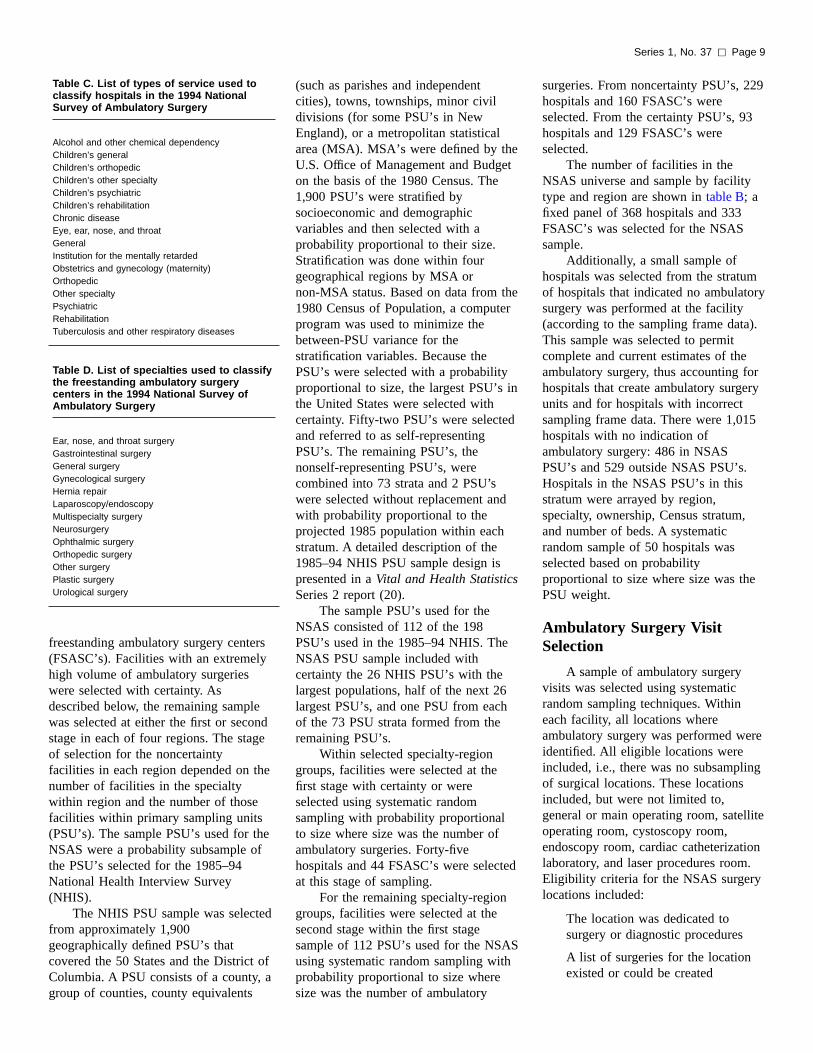
Table C. List of types of service used toclassify hospitals in the 1994 NationalSurvey of Ambulatory Surgery
Alcohol and other chemical dependencyChildren’s generalChildren’s orthopedicChildren’s other specialtyChildren’s psychiatricChildren’s rehabilitationChronic diseaseEye, ear, nose, and throatGeneralInstitution for the mentally retardedObstetrics and gynecology (maternity)OrthopedicOther specialtyPsychiatricRehabilitationTuberculosis and other respiratory diseases
Table D. List of specialties used to classifythe freestanding ambulatory surgerycenters in the 1994 National Survey ofAmbulatory Surgery
Ear, nose, and throat surgeryGastrointestinal surgeryGeneral surgeryGynecological surgeryHernia repairLaparoscopy/endoscopyMultispecialty surgeryNeurosurgeryOphthalmic surgeryOrthopedic surgeryOther surgeryPlastic surgeryUrological surgery
Series 1, No. 37 [ Page 9
freestanding ambulatory surgery centers(FSASC’s). Facilities with an extremelyhigh volume of ambulatory surgerieswere selected with certainty. Asdescribed below, the remaining samplewas selected at either the first or secondstage in each of four regions. The stageof selection for the noncertaintyfacilities in each region depended on thenumber of facilities in the specialtywithin region and the number of thosefacilities within primary sampling units(PSU’s). The sample PSU’s used for theNSAS were a probability subsample ofthe PSU’s selected for the 1985–94National Health Interview Survey(NHIS).
The NHIS PSU sample was selectedfrom approximately 1,900geographically defined PSU’s thatcovered the 50 States and the District oColumbia. A PSU consists of a county, agroup of counties, county equivalents
f
(such as parishes and independentcities), towns, townships, minor civildivisions (for some PSU’s in NewEngland), or a metropolitan statisticalarea (MSA). MSA’s were defined by theU.S. Office of Management and Budgeton the basis of the 1980 Census. The1,900 PSU’s were stratified bysocioeconomic and demographicvariables and then selected with aprobability proportional to their size.Stratification was done within fourgeographical regions by MSA ornon-MSA status. Based on data from the1980 Census of Population, a computerprogram was used to minimize thebetween-PSU variance for thestratification variables. Because thePSU’s were selected with a probabilityproportional to size, the largest PSU’s inthe United States were selected withcertainty. Fifty-two PSU’s were selectedand referred to as self-representingPSU’s. The remaining PSU’s, thenonself-representing PSU’s, werecombined into 73 strata and 2 PSU’swere selected without replacement andwith probability proportional to theprojected 1985 population within eachstratum. A detailed description of the1985–94 NHIS PSU sample design ispresented in aVital and Health StatisticsSeries 2 report (20).
The sample PSU’s used for theNSAS consisted of 112 of the 198PSU’s used in the 1985–94 NHIS. TheNSAS PSU sample included withcertainty the 26 NHIS PSU’s with thelargest populations, half of the next 26largest PSU’s, and one PSU from eachof the 73 PSU strata formed from theremaining PSU’s.
Within selected specialty-regiongroups, facilities were selected at thefirst stage with certainty or wereselected using systematic randomsampling with probability proportionalto size where size was the number ofambulatory surgeries. Forty-fivehospitals and 44 FSASC’s were selectedat this stage of sampling.
For the remaining specialty-regiongroups, facilities were selected at thesecond stage within the first stagesample of 112 PSU’s used for the NSASusing systematic random sampling withprobability proportional to size wheresize was the number of ambulatory
surgeries. From noncertainty PSU’s, 229hospitals and 160 FSASC’s wereselected. From the certainty PSU’s, 93hospitals and 129 FSASC’s wereselected.
The number of facilities in theNSAS universe and sample by facilitytype and region are shown intable B; afixed panel of 368 hospitals and 333FSASC’s was selected for the NSASsample.
Additionally, a small sample ofhospitals was selected from the stratumof hospitals that indicated no ambulatorysurgery was performed at the facility(according to the sampling frame data).This sample was selected to permitcomplete and current estimates of theambulatory surgery, thus accounting forhospitals that create ambulatory surgeryunits and for hospitals with incorrectsampling frame data. There were 1,015hospitals with no indication ofambulatory surgery: 486 in NSASPSU’s and 529 outside NSAS PSU’s.Hospitals in the NSAS PSU’s in thisstratum were arrayed by region,specialty, ownership, Census stratum,and number of beds. A systematicrandom sample of 50 hospitals wasselected based on probabilityproportional to size where size was thePSU weight.
Ambulatory Surgery VisitSelection
A sample of ambulatory surgeryvisits was selected using systematicrandom sampling techniques. Withineach facility, all locations whereambulatory surgery was performed wereidentified. All eligible locations wereincluded, i.e., there was no subsamplingof surgical locations. These locationsincluded, but were not limited to,general or main operating room, satelliteoperating room, cystoscopy room,endoscopy room, cardiac catheterizationlaboratory, and laser procedures room.Eligibility criteria for the NSAS surgerylocations included:
The location was dedicated tosurgery or diagnostic procedures
A list of surgeries for the locationexisted or could be created

a
l
to
s
Page 10 [ Series 1, No. 37
Ambulatory surgery, i.e., previouslyscheduled outpatient surgery, wasperformed
The location was not dedicatedexclusively to dentistry, podiatry,abortion, pain block, or smallprocedures
The location was recognized asdistinct from an outpatientdepartment (in hospitals).
For each location eligible for thesurvey, a systematic random sample ofambulatory surgery visits was selected.A list or log that could be used forsampling that location’s ambulatorysurgery visits was identified. The listcould be the operating room log for thelocation or another available list ofsurgery visits that included all theambulatory surgery performed at thatlocation. The list should also include themedical record number, date of surgeryinpatient or outpatient status (ifnecessary), and any other informationrequired to locate the sample medicalrecords.
A log could include the surgeriesperformed in more than one surgerylocation or each operating room couldhave a separate list. For example, onelist of surgeries could be available for asuite of operating rooms instead of aseparate list for each room.
For each facility, the approximatenumber of ambulatory surgery visits fora 12-month period for all survey-eligiblelocations was obtained from the facilitystaff. Based on this number, a singlesampling interval was determined whichif the facility-provided estimate ofannual ambulatory surgery volume wasaccurate, would yield a total sample of20–25 ambulatory surgery visits permonth for the entire facility. Arandom-start number less than or equalto the sampling interval was selected fothe first month of sampling for each logor list and, along with the samplinginterval, was used to select surgeryvisits from each designated log or list inthe facility. Although visit sampling wasdone monthly, quarterly, or on someother periodic interval at each facility,the sampling was continued across timefor each sampling list as though theentire sample from that list was selected
,
,
r
at one sampling session. That is, thesampling interval across samplingsessions was identical and the count foreach sampling session was continuedfrom where the count ended in the priorsession. This basic procedure wasadapted, as necessary, to the recordkeeping systems of the particularfacilities. In an effort to reduce thesampling error in surgery logs thatcontained both inpatient and ambulatoryprocedures, every visit was countedregardless of whether it was inpatient orambulatory surgery. For the sampledsurgery visits that were inpatientsurgery, only the case number andinpatient status indicator were recordedon the Sample Listing Sheet, NSAS-4.
After all survey-eligible locationswere identified and sampling was begunthere were three possible reasons for avisit to be designated out of scope forthe NSAS:
The patient was originally admittedas a hospital inpatient
The patient was admitted throughthe emergency room
The patient was a ‘‘no-show’’ or leftthe facility prior to the receipt ofanesthesia and/or thecommencement of the procedure.
Auxiliary information (e.g., numberof ambulatory surgery visits in thesampling frame for the month) neededfor estimation purposes was alsoobtained from each sampling list. Datafrom the medical record was abstractedfor each ambulatory surgery visit thusselected. During 1994, data for 117,861sample visits were included in the finalNSAS database.
Data Collection ProceduresThe Bureau of the Census was the
data collection agent for the 1994NSAS. Census headquarters staffdesigned and printed the surveyquestionnaires and telephone call scriptswhich are included inappendix VI.Census staff also prepared and printedthe regional office instruction manual,the field representative self-studymaterials, the field representativemanual, and the facility manual. Inaddition, Census headquarters staff
,
,
prepared all training materials, includingthe training guide and all training aids.
Field Training
Training for the 1994 NSAS wasconducted in March of 1994. Duringthis month, the Census fieldrepresentatives underwent extensivetraining in survey procedures, usingself-study materials and classroomtraining. In addition, each fieldrepresentative was given a manual thatcontained detailed instructions andinformation necessary to induct facilitiesinto the survey, conduct the samplingand abstracting, and edit and transmitcompleted forms. In selecting fieldrepresentatives for the NSAS, everyeffort was made to choose experiencedstaff who had also worked on theNational Hospital Discharge Survey orthe National Hospital AmbulatoryMedical Care Survey. These fieldrepresentatives were most familiar withworking with medical professionals andhad an understanding of medicalterminology and procedures.
Training for the NSAS wasconducted by the Census staff andconsisted of a supervisor’s conference,self-study session, and a classroomtraining session. The 1-day supervisor’sconference was held in Alexandria,Virginia, and attended by NSASsupervisors from the 12 Census regionaoffices. During the conference, NSASprocedures, sampling, and dataabstracting were described in detail.
NSAS field representative trainingincluded both self-study and classroomtraining. The self-study tookapproximately 4 hours to complete andwas used to introduce the fieldrepresentatives to NSAS concepts andgive a general overview of the NSASforms and procedures. The 2-dayclassroom training, attended by fieldrepresentatives and regional officeclerks, was held in four locations:Seattle, Dallas, Atlanta, andPhiladelphia. Each of these sessions waconducted by Census supervisors whohad attended the supervisor’sconference. To ensure uniformity oftraining, each supervisor followed awritten script that was prepared byCensus headquarters staff. The training

Series 1, No. 37 [ Page 11
covered the following topics: inductingfacilities; sampling procedures, includingdetermination of the random start and‘‘take every’’ numbers; data abstracting;training facility staff; and editingcompleted forms. In addition toproviding a detailed explanation andillustration of the forms and procedures,a major focus of the training was ongaining facility cooperation. The trainingutilized many interactive techniquessuch as role playing, practice interviewsand discussion groups. NHDS fieldrepresentatives attended many of thesessions to point out obstacles in dealinwith medical staff and to makesuggestions for overcoming them.
Facility Induction
Initial contact with the samplehospitals and freestanding ambulatorysurgery centers was made through atelephone call, using the telephonenumber provided in the 1993 listingfrom SMG Marketing, Inc. (16,17) orHCFA’s POS file (18). The call wasmade to identify to whom a letter aboutthe study should be sent and to validateinformation used to sample the facility.The script for this initial telephone callappears in the NSAS-1 (seeappendixVI).
Shortly after this initial telephonecall, a letter from the National Centerfor Health Statistics was sent to thedesignated official of the facility. Theletter (seeappendix VII) introduced thestudy and indicated that the facility hadbeen selected to participate in theNSAS. Included with the letter were asummary of NCHS activities, a generaldescription of the study, and letters ofendorsement for the study from theAmerican Hospital Association, theAmerican Academy of Ophthalmology,the American Health InformationManagement Association, the FederatedAmbulatory Surgery Association, andthe American College of Surgeons. Theletters endorsing the NSAS are shown inappendix VIII.
Approximately 10 days aftersending the letter, a telephone screenercall was made to the recipient of theletter. The NSAS-2 contains the scriptfor this call (seeappendix VI). Duringthis call, the field representative verified
,
g
receipt of the introductory letter andinformation package, determinedwhether the facility was in scope,answered any general questions aboutthe NSAS, and arranged an appointmenfor a facility induction interview.
The purposes of the inductioninterview were to:
Explain the study and urgeparticipation
Establish the method ofparticipation
Determine the locations in thefacility where ambulatory surgerywas performed
Implement an ambulatory surgerysampling plan
Determine the location of medicalrecords and other sources of neededata
Train the facility staff, if necessary
The length of time needed for theinduction interview varied by the sizeand complexity of the facility andwhether it was necessary to train facilitystaff. It generally took from ½ to 1½hours. Information about the samplefacility obtained by the Census fieldrepresentative was recorded on theinduction questionnaire, NSAS-3 (seeappendix VI). If, during the inductioninterview, it was determined that fewerthan 50 ambulatory surgery procedureswere conducted in the previous year, thfacility was deemed to be ineligible forthe 1994 NSAS.
During the induction process, themethod of participation for each facilitywas determined. There were twomethods of facility participation for theNSAS: primary and alternate. For theprimary method, facility staff agreed topull the medical records and abstractmedical record data onto the medicalabstract forms (NSAS-5, which is shownin appendix VI) for a sample ofapproximately 20–25 ambulatorysurgery visits per month, and to refilethe medical records. For facilities thathad a single log or list of ambulatorysurgery visits from which to sample,facility staff also performed thesampling. For facilities that had morethan one log or list from which tosample, the Census field representative
t
d
e
conducted the sampling because of thedifficulty and need for special training toperform this task.
The primary method of participationwas preferred for several reasons. First,the lack of standard medical recordforms or formats across facilities andthe individuality of the record keepingmade field representative trainingdifficult. Second, for confidentialityreasons some facilities did not want thefield representatives to review surgicallogs or see actual medical records.Third, facility staff knew the particularrecord-keeping systems of the facilityand were familiar with medical termsand coding.
For the primary method facilities,the field representative trained thedesignated facility staff to abstract and,if necessary, to sample the data. Thistraining was conducted during theinduction visit if at all possible. If not,the field representative scheduled anappointment to conduct the trainingwhen facility staff were available. AFacility Manual containing detailedsampling and abstracting instructionssimilar to those in the FieldRepresentative’s Manual provided thebasis for training facility staff and wasleft with the staff member(s) for futurereference. The field representativesmaintained communication with staff atprimary facilities to ensure that dataabstraction was on schedule and toanswer any questions that arose.
The alternate method ofparticipation was selected when facilitystaff were unwilling to perform thesampling and abstracting activities. Forthis method, the field representativeselected the sample of 20–25 visits permonth and performed the dataabstracting activities, thus reducingfacility staff responsibilities to pullingand refiling specified medical records. Ifpossible, the field representative selecteda 2-month sample of ambulatory surgeryvisits during the induction visit andmade an appointment to return to thefacility to perform the abstracting forthese sampled visits. For alternatemethod facilities, the field representativeattempted to visit the facility bimonthly,complete the abstract forms for therecords selected during the previousvisit, and select records for abstracting

f
n
r
Table E. Number of facilities in the 1994 National Survey of Ambulatory Surgery sample,number and percent of in-scope facilities, and response rates by type of facility
Type of facility SampleIn
scope Percent RespondentsResponse
rate
Hospitals1 . . . . . . . . . . . . . . . . . . . . . . . . . . . 368 333 90.5 293 88.0Hospitals2 . . . . . . . . . . . . . . . . . . . . . . . . . . . 50 3 6.0 3 100.0Freestanding ambulatory surgery centers . . . . . . . 333 281 84.4 198 70.5
1Hospitals selected from the stratum of hospitals that the sampling frame data indicated performed ambulatory surgery.2Hospitals selected from the stratum of hospitals that the sampling frame data indicated performed no ambulatory surgery.
Page 12 [ Series 1, No. 37
at the next visit. This process, which hasbeen used successfully for the NHDSfor many years, allowed time formedical records to be completed andpulled from the medical records roomprior to the visit.
Facilities still refusing to participateat this point in the induction processwere offered monetary compensation forparticipation. If compensation provednecessary, the field representativecompleted a Memorandum ofAgreement (NSAS-6, which is shown inappendix VI). This established theamount of reimbursement the facility orfacility staff would receive for themethod of participation selected. If theamount requested was higher than thefield representative was authorized toapprove, a call was placed to the Censuregional office to request authorizationfrom the NSAS supervisor. In 1994,approximately 40 percent of the samplefacilities requested compensation.
The number and percent of in-scopeand responding facilities in the 1994NSAS are presented intable E. Of the751 hospitals and freestandingambulatory surgery centers in the 1994sample, 134 were found to be out ofscope (ineligible) because they went outof business, performed less than 50ambulatory surgeries in the previousyear, or otherwise failed to meet thecriteria for the NSAS. Of the 617in-scope (eligible) facilities, 494responded to the survey. The responserate was 88 percent for the hospitals and70 percent for the freestanding facilities.
Data Collection
To initiate the actual data collectionprocess for the 1994 NSAS and, ifnecessary, to train facility staff, the fieldrepresentative requested the facility’sJanuary 1994 log(s) or list(s) that werespecified in item 7 of the NSAS-3,Induction Questionnaire (seeappendixVI). The determination of locations andambulatory surgery visits that wereeligible for the NSAS have beendiscussed in a previous section of thisreport entitled ‘‘Ambulatory SurgeryVisit Selection.’’ Within participatingfacilities, a systematic random samplingtechnique was used to select a sample oambulatory surgery visits. Using the
s
Sampling Table/Random Number Tables(seeappendix VI) and the estimate ofannual ambulatory surgery volumeprovided during the induction process,the field representative determined thesampling interval (‘‘Take Every’’) forthe facility and selected a random ‘‘StartWith’’ number for each NSAS-eligibleJanuary log.
The Sample Listing Sheet,(NSAS-4, which is shown inappendixVI) was used to list the monthly sampleselected from each operating room logor other acceptable list. A separateNSAS-4 was used for each monthsampled and for each log or listidentified during the induction process(see NSAS-3, item 7).
A medical abstract form (NSAS-5,which is shown inappendix VI) wascompleted for each in-scope samplevisit. Terms and definitions relating tothe medical abstract form are shown inappendix IX. The NSAS medicalabstract form is based on the medicalabstract used in the National HospitalDischarge Survey, which is based on theUniform Hospital Discharge Data Set,(UHDDS). Therefore, many of thevariables in these surveys are similar oridentical. Two of the UHDDS items(‘‘principal expected source of payment’’and ‘‘status/disposition of patient’’) havebeen slightly revised to make themapplicable to ambulatory surgery visits.
The remainder of the data items onthe abstract form were stronglyrecommended for inclusion by thefeasibility study technical advisory panelwith the exception of ‘‘total charges.’’Although this data item was not usuallyavailable in the medical record and thenonresponse rate for this item was highin the pretest (32 percent nonresponse),it was included in the NSAS because ofits importance for health care policyissues. With the exception of ‘‘total
charges,’’ all data items on the NSASabstract form were successfully tested ithe pretest with a response rate higherthan 70 percent. One data item, ‘‘ASAclassification,’’ which was recommendedby the technical advisory panel, wasexcluded from the NSAS due to anexceedingly high (56 percent)nonresponse rate in the pretest. As aresult of the pretest, minor revisions inthe data items were recommended bythe Bureau of the Census and wereincorporated into the NSAS MedicalAbstract form.
All completed Sample ListingSheets and Medical Abstract forms werereviewed by the field representatives atthe facility before being submitted on aflow basis to the regional offices.Attempts were made at that time toretrieve missing data or to correctinconsistent data. The NSAS-16,Transmittal Notice, (seeappendix VI)was used by the field representatives fotransmitting all completed work to theCensus regional offices. All forms werereviewed for completeness at theregional office. Forms that failed thispreliminary edit were returned to thefield representative for additionalinformation. All forms were transmittedon a flow basis to the NCHS dataprocessing center in Research TrianglePark, North Carolina, for data entry,medical coding, and editing.
1995 Data Collection Activities
Prior to beginning the 1995 NSASdata collection, field representativescontacted all of the 1994 participatingfacilities to update information on thelocations where ambulatory surgery wascurrently being performed to obtainestimated annual ambulatory surgeryvolumes of any new locations and toverify administrative information. TheAnnual Update Form (NSAS-7) was

Series 1, No. 37 [ Page 13
used to record this information (seeappendix VI). Due to the dynamicnature of ambulatory surgery, thisprocess was essential to ensure accurasampling of ambulatory surgery visitsfor the 1995 NSAS. In addition,facilities determined to be out of scopefor the 1994 NSAS were contacted prioto beginning the 1995 NSAS datacollection to determine whether theywere still ineligible for the study.Attempts were made to induct andcollect data from any of these facilitiesdetermined to be in scope for the 1995NSAS as well as from those facilitiesthat refused to participate in 1994.
Confidentiality
Assurance of confidentiality wasprovided to all facilities according toSection 308(d) of the Public HealthService Act (42 USC 242m), whichstates that:
‘‘No information, if an establishmentor person supplying the information ordescribed in it is identifiable, obtained inthe course of activities undertaken orsupported under section. . . 306, . . . may beused for any purpose other than thepurpose for which it was supplied unlesssuch establishment or person has consent(as determined under regulations of theSecretary) to its use for such other purposand (1) in the case of information obtainedin the course of health statistical orepidemiological activities under section. . . 306, such information may not bepublished or released in other form if theparticular establishment or personsupplying the information or described in itis identifiable unless such establishment operson has consented (as determined undregulations of the Secretary) to itspublication or release in other form, . . .’’
Strict procedures were utilized toprevent disclosure of NSAS data. Allinformation that could identify thefacilities was confidential, was seen onlby persons engaged in the NSAS, andwas not disclosed or released to othersfor any other purpose. As the datacollection agent for the NSAS, theBureau of the Census agreed to complywith NCHS laws while engaged directlyin survey activities.
Names or other identifyinginformation for individual patients were
te
r
ed
e
rer
y
not removed from the sample facility.To ensure patient confidentiality, thesampled facility kept the top copy of thecompleted 1994 Sample Listing Sheets,NSAS-4, which could have containedthe names of the patients or otherpersonal identifying information. Suchinformation did not appear on the othercopies of the NSAS-4’s that weretransmitted to NCHS.
Data ProcessingData from the NSAS medical
abstract forms were coded by trainedmedical coding personnel from theDivision of Data Processing at theNCHS Computer Facility in ResearchTriangle Park, North Carolina. TheInternational Classification of Diseases,9th Revision, Clinical Modification(ICD–9–CM) was used to code the finaldiagnoses (item 17) and the surgical andiagnostic procedures (item 18) on themedical abstract form (21). A maximumof seven diagnostic codes and sixsurgical or nonsurgical procedure codeswere assigned for each sample abstract
In addition to followups for missingand inconsistent data made by the fieldstaff, numerous clerical edits wereperformed on data received for centraldata processing. Detailed editinginstructions were provided to manuallyreview the medical abstract forms toreclassify or recode ‘‘other’’ entries, aswell as revising entries on the samplelisting sheets. Online keying edits forcode ranges and inconsistencies werealso performed.
All medical coding and keyingoperations were subject to qualitycontrol procedures. These proceduresutilized a two-way 10 percentindependent verification procedure inwhich abstracts were independentlyrecoded by a second coder, withdiscrepancies resolved by the chiefcoder. Error rates for 1994 NSAS datawere less than 5 percent for medicalcoding of diagnoses and procedures andless than 0.5 percent for the entry of thenonmedical data.
After medical coding and keyingwere completed, extensive computerediting was conducted to ensure that allresponses were accurate, consistent,logical, and complete. When necessary,
d
.
records were reviewed manually toresolve inconsistencies. Missing age andsex data were imputed using a hot deckprocedure. This imputation was requiredfor less than 2 percent of the 1994NSAS records and all imputed datawere identified as such on the data tapesto enable the analyst to distinguishbetween imputed and reported data.
Estimation ProceduresThe probability sample design of
the NSAS allows the sample data to beweighted to produce national estimatesfor the United States. Unweighted dataare not used for analysis becauseunweighted data ignore thedisproportionate sampling used inNSAS.
Statistics from the NSAS arederived by a multistage estimationprocedure that produces essentiallyunbiased national estimates for hospitalsand FSASC’s. The weight includes threebasic components: (a) inflation byreciprocals of the probabilities ofselection, (b) adjustment fornonresponse, and (c) ratio adjustment tofixed totals (22). Each component isbriefly described below.
Inflation by Reciprocals ofProbabilities of Selection
Because the survey utilized amultistage sample design, there wereseveral probabilities of selection. Theywere: (a) the probability of selecting thePSU, (b) the probability of selecting thefacility, and (c) the probability ofselecting the ambulatory surgery visitwithin the facility. The overallprobability of selection was the productof the probabilities at each stage. Theinverse of the overall selectionprobability was the basic inflationweight.
Adjustment for Nonresponse
Estimates from NSAS data wereadjusted to account for sample units thatwere in scope, but did not participate inthe study. These adjustments werecalculated to minimize the impact ofnonresponse on final estimates byimputing to nonresponding units the

Page 14 [ Series 1, No. 37
characteristics of similar respondingunits. As nonresponse may occur at eacstage of sampling, adjustments wereincluded for the month within log, logwithin facility-specialty strata, andfacility within specialty strata. A finaladjustment was included to account forsample facilities involved in mergers.
Ratio Adjustment
NSAS estimates includedpoststratification adjustments within 20strata defined by five facility-specialtygroups and four Census regions. Thefive groups, defined by facility type(hospital or freestanding surgery center)and the facility specialty (as designatedon the sampling frame), are:
Hospitals specializing in children’scare (general, orthopedic,psychiatric, rehabilitation, andother)
All other hospitals
Freestanding ambulatory surgerycenters with a single specialty inplastic surgery
Freestanding ambulatory surgerycenters with a single specialty ineye surgery
All other freestanding ambulatorysurgery centers
The ratio adjustment was amultiplication factor whose numeratorwas the total of annual numbers ofoutpatient surgeries in the samplingframe facilities in each stratum andwhose denominator was the estimatednumber of surgeries in that stratumbased on the sample facilities. Thenumerator for the hospitals was basedon figures from the SMG HospitalMarket Database and the numerator forthe freestanding ambulatory surgerycenters was based on figures from theSMG Freestanding Outpatient SurgeryCenters Database. These adjustmentratios are updated annually.
Smoothing of Weights
Procedures were used to reduceexcessively large weights whilemaintaining the total visit estimateswithin each of the 20 post-stratificationstrata. In each strata the weights were
hinflated to account for the reductions inexcess weights.
Reliability of EstimatesBecause statistics from the NSAS
are based on a sample, they may differsomewhat from the figures that wouldbe obtained if a complete census weretaken using the same forms, definitions,instructions, and procedures. However,the probability design of NSAS permitsthe calculation of sampling errors. Thestandard error is primarily a measure ofsampling variability that occurs bychance because only a sample ratherthan the entire population is surveyed.The standard error, as calculated for theNSAS, also reflects part of the variationthat arises in the measurement processbut does not include estimates of anysystematic biases that may be in thedata. The relative standard error (RSE)of an estimate is obtained by dividingthe standard error by the estimate itselfand is expressed as a percent of theestimate. Generally in NCHS publisheddata reports, an asterisk (*) indicatesany estimate with more than a30 percent relative standard error.
In repeated samples using the samforms and procedures, the chances areabout 68 of 100 that an estimate fromthe sample would differ from a completecensus by less than the standard error.The chances are about 95 of 100 thatthe difference would be less than twicethe standard error, and about 99 of 100that it would be less than 2 1/2 times aslarge.
Estimation of Standard Errors
Estimates of sampling variability forthe 1994 NSAS data presented in NCHpublications were computed using afirst-order Taylor Series approximationof the deviation of estimates from theirexpected values. The SUDAANsoftware was used to compute thestandard errors. A description of thissoftware and the approach it uses hasbeen published (23).
Standard Error Approximations
The SUDAAN procedure can beused to compute directly the standard
,
e
S
errors for NSAS estimates. However,this procedure is not practical or feasiblefor all users of the data. Therefore, ageneralized procedure for approximatingthe relative standard errors for theNSAS estimates was developed.
Relative standard errors werecomputed for a range of estimates.Regression techniques were used toproduce generalized variance equationsfrom which a relative standard error forany estimate may be approximated. Theparameters of the equations arepresented intable F. Rules explainingthe use of these equations are presentedin the section below.
To derive error estimates that wouldbe applicable to a wide variety ofstatistics and that could be prepared atmoderate cost, several approximationswere required. As a result, standarderrors computed using this procedureshould be interpreted as approximaterather than exact for any specificestimate.
Standard Error Applications
Estimates of Standard Errors forAggregate Estimates
The approximate standard errors forestimates of the number of ambulatorysurgery visits with a particularcharacteristic may be computed usingthe following formula, wherex is theaggregate estimate of interest, anda andb are the appropriate parameters fromtable F.
SE (x) =√ ax2 + bx
The approximate relative standarderror, expressed as a percent, for theestimated number of ambulatory surgeryvisits with a particular characteristic,may be computed as follows:
RSE (x) = 100√ a + b/x
Estimates of Rates Where theDenominator Is Assumed to haveNegligible Error
The approximate relative standarderror for a rate in which thedenominator is the total U.S. populationor one or more of the age-sex-racegroups of the total population isequivalent to the relative standard error

Table F. Parameters for use in the relative standard error formulae for the National Survey of Ambulatory Surgery by selected characteristics: Unite d States, 1994
Selected characteristic
Hospital Freestanding ambulatory surgery center
First-listed diagnoses All-listed procedures First-listed diagnoses All-listed procedures First-listed diagnoses All-listed procedures
a b a b a b a b a b a b
Total . . . . . . . . . . . . . . . 0.002996 936.205191 0.003143 1042.899257 0.003650 937.293644 0.003981 979.807673 0.018124 246.302178 0.014197 756.815317
Sex
Male . . . . . . . . . . . . . . . 0.005839 243.411027 0.005227 374.804666 0.007031 259.440811 0.006342 400.073897 0.019727 148.897701 0.023878 111.243531Female . . . . . . . . . . . . . 0.003221 744.535434 0.003760 617.095495 0.003961 765.853727 0.004677 609.191764 0.018401 194.160869 0.011996 581.791449
Age
Under 15 years . . . . . . . . 0.016112 65.117616 0.009705 221.957283 0.016933 94.811756 0.011514 232.068663 0.058636 9.701896 0.031078 86.17009815–44 years . . . . . . . . . . 0.004651 422.786841 0.004022 650.559674 0.005294 467.627182 0.004410 733.863531 0.019479 148.963379 0.019803 208.03592545–64 years . . . . . . . . . . 0.005557 376.824342 0.007491 168.934774 0.006899 395.110427 0.009749 118.058917 0.019775 133.575567 0.024660 131.18253965 years and over . . . . . . . 0.006409 406.831653 0.004337 572.576624 0.007944 425.446412 0.005884 577.976415 0.030411 111.597626 0.044043 1.418704
Region
Northeast . . . . . . . . . . . . 0.013512 985.293492 0.013715 857.242241 0.016358 999.602588 0.018943 737.602043 0.078174 58.884015 0.068619 58.777503Midwest . . . . . . . . . . . . . 0.010638 644.607350 0.012862 551.969910 0.010397 653.985309 0.012367 593.605658 0.091502 165.353131 0.095489 216.628667South . . . . . . . . . . . . . . 0.009821 404.799980 0.009781 527.582934 0.012810 346.621537 0.012582 522.614760 0.046815 90.105394 0.044594 114.414283West . . . . . . . . . . . . . . . 0.017904 457.195190 0.016911 649.373580 0.025218 411.895141 0.022593 618.081376 0.062637 174.678875 0.068295 256.659577
Source of payment
Worker’s Compensation . . . 0.038544 31.834535 0.039479 32.664023 0.051251 26.389558 0.050903 25.226753 0.098051 6.783712 0.086114 8.341723Medicare . . . . . . . . . . . . 0.009882 211.166190 0.009182 136.913855 0.012175 213.793529 0.011596 137.695464 0.033715 98.594817 0.047121 1.438590Medicaid . . . . . . . . . . . . 0.013403 250.110798 0.010870 344.151585 0.015120 260.182032 0.012655 348.099706 0.071604 66.821585 0.079337 36.770793Other government . . . . . . . 0.049033 157.029327 0.039332 226.739743 0.056480 173.181171 0.051979 215.742100 0.215697 1.579989 0.159833 23.475489Private insurance . . . . . . . 0.003355 777.159166 0.003298 1127.335798 0.003948 835.302005 0.003895 1209.832213 0.013969 252.712881 0.010695 605.398623Self-pay . . . . . . . . . . . . . 0.028160 151.933029 0.020759 293.084515 0.036721 129.202040 0.027805 246.162675 0.100330 35.442751 0.109715 39.262511No charge and/or other . . . 0.077170 145.424550 0.073571 149.427354 0.088636 123.675106 0.083409 154.663601 0.256708 0.770684 0.222136 0.791779Not stated . . . . . . . . . . . . 0.064640 318.862505 0.066747 381.219870 0.080030 325.472443 0.085397 297.598560 0.204803 56.398866 0.220737 115.011084
Series
1,No.37[
Page
15

f
e
Page 16 [ Series 1, No. 37
of the numerator that can be obtainedusing the relative standard error formulaabove and the appropriate coefficientsfrom table F. The standard error is thengiven by:
SE (r) = r c RSE(r)
The population figures used incomputing annual rates for the NSASare based on the July 1 estimates of thecivilian population, includinginstitutionalized persons, of the UnitedStates.
Estimates of Standard Errors ofPercents Where Both the Numeratorand Denominator are Estimated fromthe Same Sample and the NumeratorIs a Subclass of the Denominator
The approximate relative standarderrors, expressed as a percent, forestimates of percents may be computedusing the appropriate relative standarderrors for the aggregate statistics asfollows: Obtain the relative standarderror of the numerator and denominatorof the percent. Square each of therelative standard errors, subtract theresulting value for the denominator fromthe resulting value for the numerator,extract the square root, and multiply by100.
RSE (p) = RSE(x/y) = 100√ RSE2 (x) – RSE2(y)
Alternatively, if both numerator anddenominator are estimated from thesame sample, approximate relativestandard errors, expressed as a percent,for estimates of percents may becomputed using the following formula,wherep is the percent of interest andyis the denominator of the percent usingthe appropriate parameters.
RSE (p) = 100√ b(1–p)/py
For standard errors, the appropriateformula is:
SE (p) = √ bp(1–p)/y
The approximation of the absoluteor relative standard error is valid if therelative standard error of thedenominator is less than 0.05 (24) or ifthe relative standard errors of thenumerator and denominator are both lessthan 0.10 (25).
Estimates of Ratios (r = x/y) Wherethe Numerator Is not a Subclass ofthe Denominator
The standard error for a ratio maybe approximated by
SE~r! = r v RSE(r)
where
RSE (r) =RSE(x/y) =100 √RSE 2(x)+ RSE 2(y)
This approximation is valid if therelative standard error of thedenominator is less than 0.05 (24) or ifthe relative standard errors of thenumerator and denominator are both lesthan 0.10 (25).
Estimates of Differences Between TwoStatistics
The standard error of the differencebetween two statistics is approximatedby:
SE (x1 – x2) =√ SE2(x1) + SE2 (x2)
where SE(x1) and SE(x2) are computedusing the appropriate directions. Thisformulation represents the standard errofor the difference between separate anduncorrelated characteristics, although itis only a rough approximation in mostother cases.
Nonsampling Error
Estimates based on the 1994 NSASare subject to nonsampling as well assampling errors. Nonsampling errorsinclude reporting and processing errorsas well as biases due to nonresponse orincomplete response. Although themagnitude of the nonsampling errorscannot be computed, these errors arekept to a minimum by procedures builtinto the operation of the survey. Toeliminate ambiguities and encourageuniform reporting, careful attention wasgiven to the phrasing of questions,terms, and definitions. Also, extensivepretesting of most data items and surveyprocedures were performed. The stepstaken to reduce bias in the data arediscussed in the sections on datacollection and data processing. Qualitycontrol procedures and edit checksdiscussed in the data processing sectionreduced errors in data coding and
s
r
processing. Because survey results aresubject to sampling and nonsamplingerrors, the total error will be larger thanthe error due to sampling variabilityalone.
Data DisseminationThis report presents a description o
the NSAS through its first year ofoperation (1994). Summary data fromthe 1994 NSAS is available in anAdvance Data from Vital and HealthStatisticsreport entitledAmbulatorySurgery in the United States, 1994(26).A Vital and Health Statisticsreport thatcombines data on ambulatory surgeryand surgery performed on hospitalinpatients during 1994 is forthcoming.Additional descriptive, analytical, andmethodological reports will be publishedin Vital and Health Statistics,Series 1,2, and 13. Brief reports on topics ofspecial interest will be published inAdvance Data From Vital and HealthStatistics.Information will also bepresented in journal articles and inpapers presented at professionalmeetings. As resources permit, specialtabulations and analyses will beprovidedto both public and private datarequestors.
To obtain general information onpublished reports or to receiveTheCatalog of Publications, Catalog ofElectronic Data Products,andCatalogof Public-Use Data Tapes,contact:
Data Dissemination Branch (DDB)National Center for Health StatisticsCenters for Disease Control andPrevention6525 Belcrest Road, Room 1064Hyattsville, Maryland 20782(301) 436–8500E-mail: [email protected]:http://www.cdc.gov/nchswww/nchshome.htm
For each data year, a public-usedata tape and data tape documentationwill be prepared for distribution throughthe National Technical InformationService (NTIS). The public-use datatape for the 1994 NSAS is currentlyavailable. There are also plans to releasNSAS data on diskette and CD-ROMusing the Statistical Export and

Series 1, No. 37 [ Page 17
Tabulation System (SETS) databasesoftware. To purchase data tapes andother computer products, contact:
National Technical Information Service5285 Port Royal RoadSpringfield, VA 22161(703) 487–4650
References
1. New surgical technologies reshapehospital strategies. Hospitals66(9):30–36, 38, 40–42. 1992.
2. Leader S, Moon M. Medicare trends inambulatory surgery. Health AffairsSpring: 158–170. 1989.
3. Durant G. Ambulatory surgery centers:surviving, thriving into the 1990’s.Medical Group Management Journal36(2):16–18, 20. 1989.
4. SMG Marketing Group, Inc. Outpatientsurgery centers exceed three millioncases. SMG Market Letter 8(6). 1994.
5. SMG Marketing Group, Inc. U.S.hospitals performed 23.7 millionsurgical procedures in 1993. SMGMarket Letter 8(3). 1994.
6. Kozak LJ. Hospital inpatient surgery:United States, 1983–87. Advance datafrom vital and health statistics; no 169.Hyattsville, Maryland: National Centerfor Health Statistics. 1989.
7. Institute of Medicine. Toward aNational Health Care Survey: A DataSystem for the 21st Century.Washington. National Academy Press.1992.
8. McLemore T, Bacon WE.Establishment Surveys of the NationalCenter for Health Statistics.Proceedings of the InternationalConference on Establishment Surveys.Buffalo, New York. pp. 93–98. 1993.
9. Evaluation of the coverage of healthfacilities of the National Master FacilityInventory. Contract No. 282–86-0103.Columbia, Maryland. La JollaManagement Corporation. 1989.
10. Duggar, BC. Defining and findingambulatory surgery facilities. JAmbulatory Care Management. Vol. 13.No. 1. Jan. 1990.
11. Feasibility study of a national survey ofambulatory surgery. Contract No.200–89-8022. Columbia, Maryland.Center for Health Policy Studies. 1991.
12. Duggar BC, Balicki, B. The feasibilityof collecting data in a national surveyof ambulatory surgery. Proceedings of
the 1991 Public Health Conference onRecords and Statistics. pp. 48–53.Washington. 1992.
13. SMG Marketing Group, Inc. HospitalMarket Database. Chicago: HealthcareInformation Specialists. April 1991.
14. SMG Marketing Group, Inc.Freestanding Outpatient SurgeryCenters Database. Chicago: HealthcareInformation Specialists. 1991.
15. Health Care Financing Administration.Provider of Services Public Use File.Baltimore: 1992.
16. Shimizu, I. Specifications for selectingthe NSAS sample facilities.Unpublished document. 1993.
17. SMG Marketing Group, Inc. HospitalMarket Database. Chicago: HealthcareInformation Specialists. April 1993.
18. SMG Marketing Group, Inc.Freestanding Outpatient SurgeryCenters Database. Chicago: HealthcareInformation Specialists. 1993.
19. Health Care Financing Administration.Provider of Services Public Use File.Baltimore: 1993.
20. Massey JT, Moore TF, Parsons VL,Tadros W. Design and estimation forthe National Health Interview Survey,1985–94. National Center for HealthStatistics. Vital Health Stat 2(110).1989.
21. Public Health Service and Health CareFinancing Administration. InternationalClassification of Diseases, 9th Revision,Clinical Modification. Washington:Public Health Service. 4th ed. 1991.
22. Shimizu I. Estimators for NSAS.Unpublished document. 1995.
23. Shah BV, Barnwell BG, Biegler GS.SUDAAN User’s Manual: Software forAnalysis of Correlated Data, Release6.40. Research Triangle Park, NC:Research Triangle Institute. 1995.
24. Hansen MH, Hurwitz WN, MadowWG. Sample survey methods andtheory vol. 1. New York: John Wileyand Sons. Wiley Classics LibraryEdition, 1993.
25. Cochran WG. Sampling techniques.New York: John Wiley and Sons. 1953.
26. Kozak LJ, Hall MJ, Pokras R,Lawrence L. Ambulatory Surgery in theUnited States, 1994. Advance data fromvital and health statistics; no 283.Hyattsville, Maryland: National Centerfor Health Statistics. 1997.

e
s
d
Page 18 [ Series 1, No. 37
Appendix I
Legislative AuthorizationPublic Health Service ActSection 306(a) & (b)
NATIONAL CENTER FORHEALTH STATISTICS
Section 306. [242k](a) There isestablished in the Department of Healthand Human Services the National Centfor Health Statistics (hereinafter in thissection referred to as the ‘‘Center’’)which shall be under the direction of aDirector who shall be appointed by theSecretary and supervised by theAssistant Secretary for Health (or suchofficer of the Department as may bedesignated by the Secretary as theprincipal adviser to him for healthprograms).
(b) In carrying out section 304(a),the Secretary, acting through theCenter—
(1) shall collect statistics on—
(A) the extent and nature ofillness and disability of thepopulation of the United States(or any groupings of peopleincluded in the population),including life expectancy, theincidence of various acute andchronic illnesses, and infant andmaternal morbidity and mortality,
(B) the impact of illness anddisability of the population onthe economy of the United Stateand on other aspects of thewell-being of its population (orof such groupings),
(C) environmental, social, andother health hazards,
(D) determinants of health,
(E) health resources, includingphysicians, dentists, nurses, andother health professionals byspecialty and type of practice ansupply of services by hospitals,extended care facilities, homehealth agencies, and other healthinstitutions,
(F) utilization of health care,including utilization of (i)
r
ambulatory health services byspecialties and type of practice ofhealth professionals providingsuch service, and (ii) services ofhospitals, extended care facilities,home health agencies, and otherinstitutions,
(G) health care costs andfinancing, including the trends inhealth care prices and costs, thesources of payments for healthcare services, and Federal, State,and local governmentalexpenditures for health careservices, and
(H) family formation, growth,and dissolution;
(2) shall undertake and support(by grant or contract) research,demonstrations, and evaluationsrespecting new or improvedmethods for obtaining current dataon the matters referred to inparagraph (1);(3) may undertake and support
(by grant or contract) epidemiologicresearch, demonstrations, andevaluations on the matters referredto in paragraph (1); and(4) may collect, furnish, tabulate,
and analyze statistics, and preparestudies, on matters referred to inparagraph (1) upon request ofpublic and nonprofit private entitiesunder arrangements under whichthe entities will pay the cost of theservice provided.
Amounts appropriated to the Secretaryfrom payments made underarrangements made under paragraph (4shall be available to the Secretary forobligation until expended.
Appendix II
Members of the TechnicalAdvisory Panel for theFeasibility Study of aNational Survey ofAmbulatory SurgeryDr. James AquavellaClinical Director of Ophthalmology andDirector of the Cornea ResearchLaboratory
)
University of Rochester Medical CenterMedical DirectorRochester Ophthalmic AssociatesAmbulatory Surgery Center
Dr. Enzo DiGiacomoPresidentSociety for Ambulatory CareProfessionals of the American HospitalAssociationPast-PresidentMassachusetts Chapter of the AmericanCollege of Emergency Physicians
Ms. Irene FraserDirectorDivision of Ambulatory Care andEmergency ServicesAmerican Hospital Association
Mr. George GreenbergProgram AnalystDepartment of Health and HumanServicesOffice of the Assistant Secretary forPlanning and Evaluation
Mr. Allen D. HechtExecutive Vice PresidentMedical Management and DevelopmentCorporation
Dr. John HenleyPresidentFederated Ambulatory SurgeryAssociationAdministratorFayetteville Ambulatory Services, Inc.
Dr. Marie-Louise LevyAssociate Professor of AnesthesiaDirector of In-and-Out AnesthesiaGeorge Washington University Hospital
Mr. Ted Matson1
Senior Staff SpecialistDivision of Ambulatory Care andEmergency ServicesAmerican Hospital Association
Mr. Kurt Price1
Deputy DirectorMaryland Health Services Cost ReviewCommission
Ms. Jane RuseskiAssociate Director of MethodologyMaryland Health Services Cost ReviewCommission
1Mr. Kurt Price and Mr. Ted Matson were replacedby Ms. Jane Ruseski and Ms. Irene Fraser,respectively, between the first and second TAPmeetings.

Appendix III
Letters and Data Collection Instruments for theFeasibility Study of a National Survey ofAmbulatory Surgery
Series 1, No. 37 [ Page 19

Page 20 [ Series 1, No. 37

Series 1, No. 37 [ Page 21

Page 22 [ Series 1, No. 37

Series 1, No. 37 [ Page 23

Page 24 [ Series 1, No. 37

Series 1, No. 37 [ Page 25

Page 26 [ Series 1, No. 37

Series 1, No. 37 [ Page 27

Page 28 [ Series 1, No. 37

Series 1, No. 37 [ Page 29

Page 30 [ Series 1, No. 37

Series 1, No. 37 [ Page 31

Page 32 [ Series 1, No. 37

Series 1, No. 37 [ Page 33

Page 34 [ Series 1, No. 37

Series 1, No. 37 [ Page 35

Page 36 [ Series 1, No. 37

Series 1, No. 37 [ Page 37

Page 38 [ Series 1, No. 37

Series 1, No. 37 [ Page 39

Page 40 [ Series 1, No. 37

Series 1, No. 37 [ Page 41
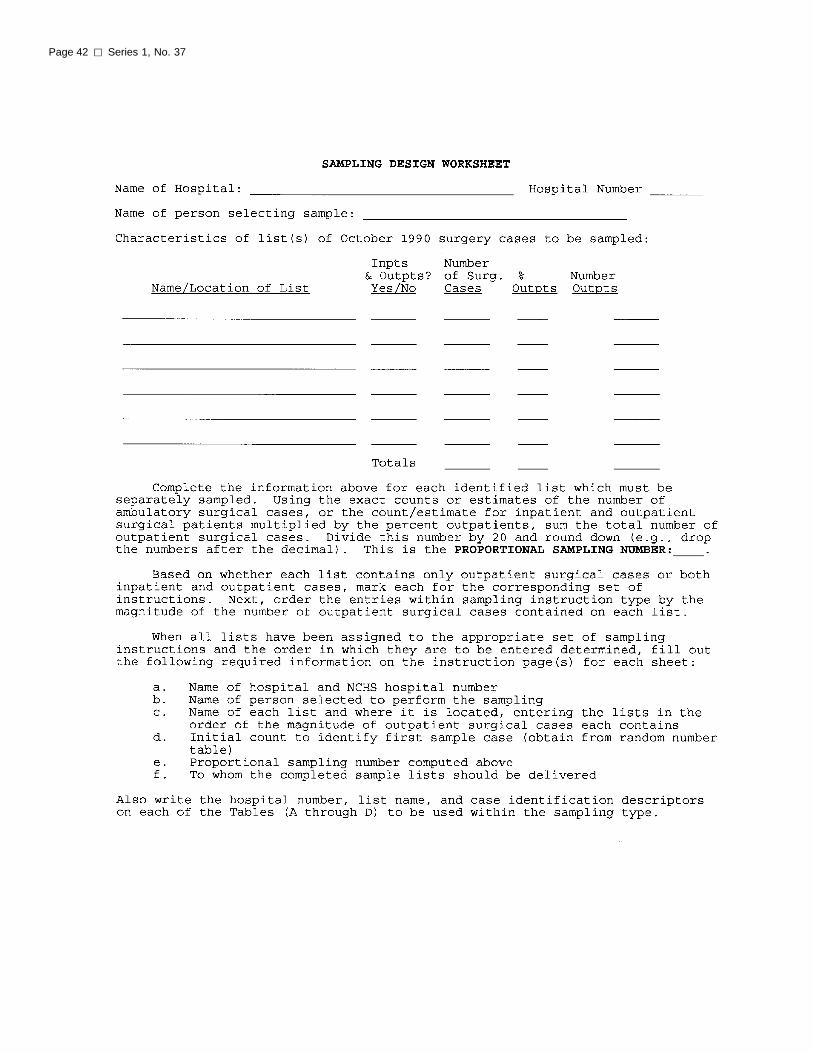
Page 42 [ Series 1, No. 37

Series 1, No. 37 [ Page 43
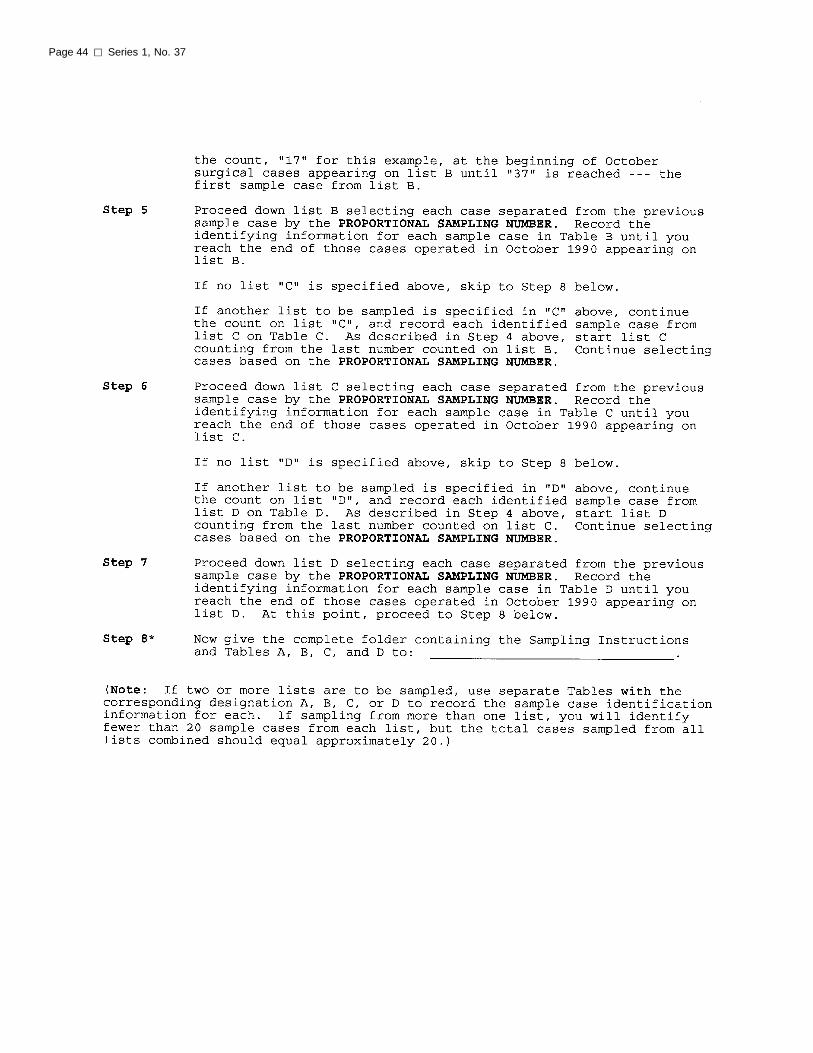
Page 44 [ Series 1, No. 37

Series 1, No. 37 [ Page 45

Page 46 [ Series 1, No. 37

Series 1, No. 37 [ Page 47
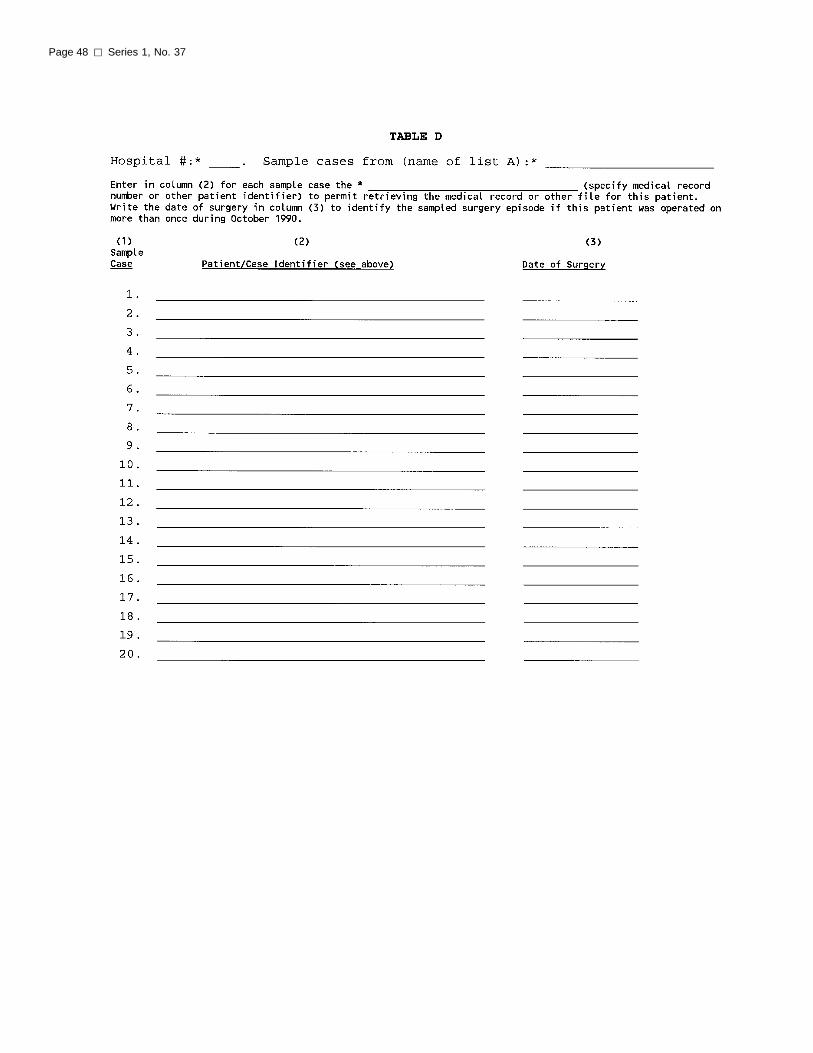
Page 48 [ Series 1, No. 37

Series 1, No. 37 [ Page 49

Page 50 [ Series 1, No. 37

Series 1, No. 37 [ Page 51

Page 52 [ Series 1, No. 37

Series 1, No. 37 [ Page 53

Page 54 [ Series 1, No. 37

Series 1, No. 37 [ Page 55

Page 56 [ Series 1, No. 37

Series 1, No. 37 [ Page 57

Page 58 [ Series 1, No. 37
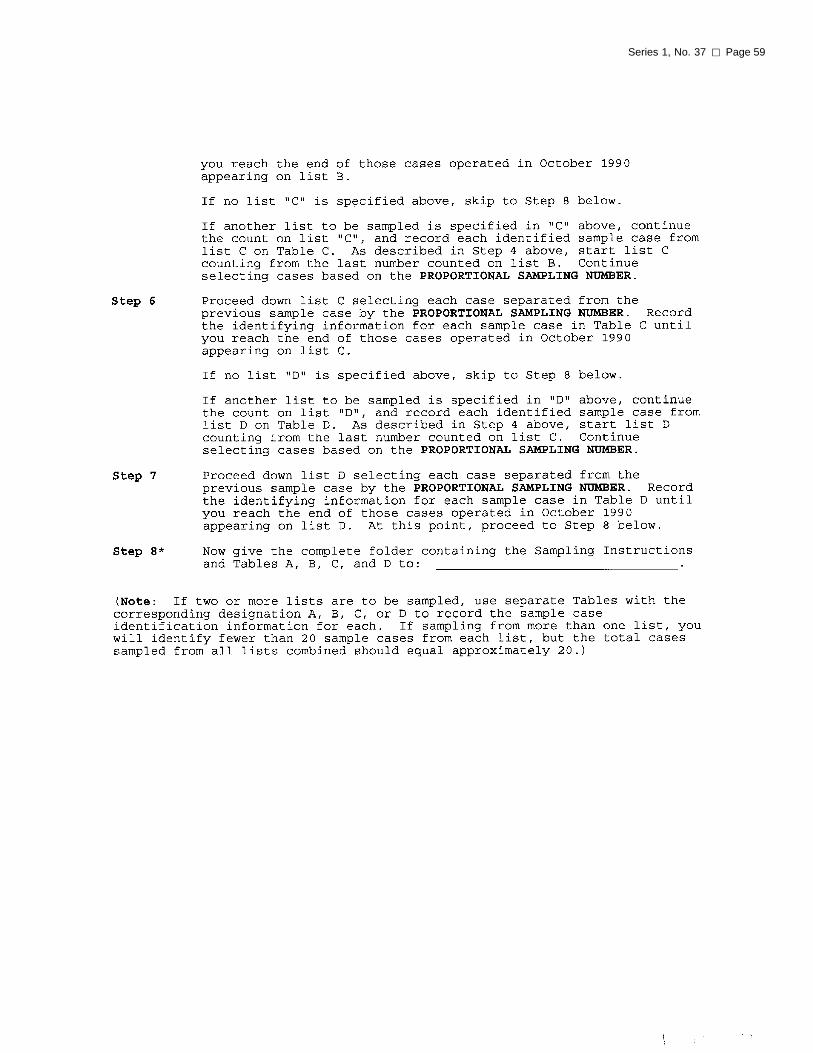
Series 1, No. 37 [ Page 59

Page 60 [ Series 1, No. 37
Series 1, No. 37 [ Page 61
Page 62 [ Series 1, No. 37
Series 1, No. 37 [ Page 63

Page 64 [ Series 1, No. 37
Series 1, No. 37 [ Page 65

Page 66 [ Series 1, No. 37
Series 1, No. 37 [ Page 67

Page 68 [ Series 1, No. 37

Appendix IV
Letters and Data CollectionInstruments for the Pretest ofthe National Survey ofAmbulatory Surgery
Series 1, No. 37 [ Page 69

Page 70 [ Series 1, No. 37

Series 1, No. 37 [ Page 71

Page 72 [ Series 1, No. 37

Series 1, No. 37 [ Page 73

Page 74 [ Series 1, No. 37

Series 1, No. 37 [ Page 75

Page 76 [ Series 1, No. 37

Series 1, No. 37 [ Page 77

Page 78 [ Series 1, No. 37

Series 1, No. 37 [ Page 79

Page 80 [ Series 1, No. 37

Series 1, No. 37 [ Page 81

Page 82 [ Series 1, No. 37

Series 1, No. 37 [ Page 83

Page 84 [ Series 1, No. 37

Series 1, No. 37 [ Page 85
Page 86 [ Series 1, No. 37

Series 1, No. 37 [ Page 87

Page 88 [ Series 1, No. 37

Series 1, No. 37 [ Page 89

Page 90 [ Series 1, No. 37

Series 1, No. 37 [ Page 91

Page 92 [ Series 1, No. 37
Appendix V
Definitions of Terms Usedin the SurveyAmbulatory surgery—Previouslyscheduled surgical and nonsurgicalprocedures performed on an outpatientbasis in a hospital or freestandingambulatory surgery center.
In scope—Ambulatory surgeryconducted in general or mainoperating rooms, satellite operatingrooms, cystoscopy rooms,endoscopy rooms, cardiaccatheterization labs, and laserprocedure rooms.
Out of scope—Ambulatory surgeryconducted in locations dedicatedexclusively to dentistry, podiatry,abortion, pain block, or smallprocedures (i.e., lump and bumpprocedure rooms).
Hospital—A hospital with an averagelength of stay for all patients of lessthan 30 days (short stay) or a hospitalwhose specialty is general (medical orsurgical) or children’s general, exceptFederal hospitals and hospital units ofinstitutions and hospitals with less thansix beds staffed for patient use.
Out of scope—Hospitals where lessthan 50 ambulatory surgeryprocedures were conducted in theprevious year.
Freestanding Ambulatory SurgeryCenter—A freestanding ambulatorysurgery facility that was regulated by aState or was certified for Medicare bythe Health Care FinancingAdministration (HCFA). For the 1994NSAS, a facility listed in the 1993 SMGFreestanding Outpatient Surgery CenteDatabase and/or a Medicare-certifiedfacility included in the Health CareFinancing Administration’s Provider ofServices (POS) file.
Out of scope—Facilities where lessthan 50 ambulatory surgeryprocedures were conducted in theprevious year as well as facilitiesspecializing in dentistry, podiatry,pain block, abortion, familyplanning, or birthing.
r
Ambulatory surgery visit—A visit by aperson to a hospital or freestandingambulatory surgery center to receivepreviously scheduled surgical ornonsurgical procedures on an outpatientbasis. Each appearance of an outpatientto a surgical location constitutes onevisit regardless of the number ofprocedures the patient receives.
Procedures—All surgical procedures(such as tonsillectomy), diagnosticprocedures (such as cystoscopy), andother therapeutic procedures (such asinjection or infusion of cancerchemotherapeutic substance) reported onthe patient’s medical record are includedin the NSAS. A maximum of sixprocedures per ambulatory surgery visitare coded.
Region—Facilities are classified bylocation in one of the four geographicregions of the United States thatcorrespond to those used by the U.S.Bureau of the Census.
Region States included
Northeast Connecticut, Maine,Massachusetts, NewHampshire, New Jersey, NewYork, Pennsylvania, RhodeIsland, and Vermont
Midwest Illinois, Indiana, Iowa,Kansas, Michigan, Minnesota,Missouri, Nebraska, NorthDakota, Ohio, South Dakota,and Wisconsin
South Alabama, Arkansas,Delaware, District ofColumbia, Florida, Georgia,Kentucky, Louisiana,Maryland, Mississippi, NorthCarolina, Oklahoma, SouthCarolina, Tennessee, Texas,Virginia, and West Virginia
West Alaska, Arizona, California,Colorado, Hawaii, Idaho,Montana, Nevada, NewMexico, Oregon, Utah,Washington, and Wyoming

Appendix VI
Data Collection Forms Used inthe 1994 NSAS
Series 1, No. 37 [ Page 93

Page 94 [ Series 1, No. 37

Series 1, No. 37 [ Page 95

Page 96 [ Series 1, No. 37
Series 1, No. 37 [ Page 97

Page 98 [ Series 1, No. 37

Series 1, No. 37 [ Page 99
Page 100 [ Series 1, No. 37

Series 1, No. 37 [ Page 101

Page 102 [ Series 1, No. 37

Series 1, No. 37 [ Page 103

Page 104 [ Series 1, No. 37

Series 1, No. 37 [ Page 105

Page 106 [ Series 1, No. 37

Series 1, No. 37 [ Page 107

Page 108 [ Series 1, No. 37

Series 1, No. 37 [ Page 109
Page 110 [ Series 1, No. 37

Series 1, No. 37 [ Page 111

Page 112 [ Series 1, No. 37

Series 1, No. 37 [ Page 113

Page 114 [ Series 1, No. 37

Series 1, No. 37 [ Page 115
Page 116 [ Series 1, No. 37

Appendix VII
Introductory Letter
Series 1, No. 37 [ Page 117
Appendix VIII
Endorsement Letters
Page 118 [ Series 1, No. 37

Series 1, No. 37 [ Page 119

Page 120 [ Series 1, No. 37

Series 1, No. 37 [ Page 121

Page 122 [ Series 1, No. 37

Series 1, No. 37 [ Page 123
Appendix IX
Definitions of TermsRelating to the MedicalAbstract Form
Facility number—The uniquelyassigned four-digit facility identificationnumber.
NSAS number and list used—Theuniquely assigned NSAS number for thesampled ambulatory surgery visit andthe alphabetic identifier for the log orlist used for sampling.
Medical record number—The uniquelyassigned number within a facility thatidentified the individual patient.
Date of surgery—The date on which thesampled ambulatory surgery visitoccurred, using two digits for the monthand day, and four digits for the year.
Residence ZIP code—The nine-digit orfive-digit U.S. Postal Service ZIP codethat designates the patient’s residence.
Date of birth—The patient’s date ofbirth, using two digits for the month andday, and four digits for the year.
Age—Entered on the medical abstractform only if the date of birth wasunavailable. The computed age thatappears in NSAS reports and data tapesis calculated from the date of birth andis the age at last birthday on the date ofsurgery.
Race—This item was completed basedon information recorded in the patient’smedical record.
White—Patient is white orCaucasian.
Black—Patient is Negro, black, orAfrican American.
American Indian/Eskimo/Aleut—Patient has American Indian originor is classified as Eskimo, Aleut, orany other Alaskan Native origin.
Asian/Pacific Islander—Patient hasorigins in the Far East, SoutheastAsia, the Indian subcontinent, or thePacific Islands. For example, thisarea includes China, India, Japan,
Korea, the Philippine Islands, andSamoa.
Other—Patient’s race does not fallinto a category described above.
Not stated—Patient’s race is notindicated.
Ethnicity—Refers to the national orcultural group from which the patient isdescended, i.e., the nationality or lineageof the patient’s ancestors. Race andethnicity are considered separatecharacteristics. The item was completedfrom factual information from themedical record and was not completedbased on the patient’s name orbirthplace.
Hispanic origin—Person is ofMexican, Puerto Rican, Cuban,Central or South American, or otherSpanish culture or origin, regardlessof race.
Non-Hispanic—All other persons.
Not stated—Patient’s ethnicity isnot indicated.
Status/disposition of patient—Thestatus/disposition of the patient upondischarge from the facility.
Routine discharge to customaryresidence—Patient was dischargedto return to his or her normal placeof residence, i.e., home, nursinghome, or prison.
Discharge to observationstatus—Patient was kept at thefacility for up to 72 hours for‘‘observation,’’ but was notconsidered an inpatient.
Discharge to recovery carecenter—Patient was discharged toan organized recovery care center.
Admitted to hospital asinpatient—Patient was admitted tothe hospital as an inpatient afterambulatory surgery was performed.
Surgery canceled orterminated—Patient was scheduledfor ambulatory surgery, appeared atthe designated time and receivedanesthesia and/or began theprocedure, but the procedure wasterminated prior to completion.
Other-Specify—Patient’s statusand/or disposition was somethingother than the above categories.
Status/disposition notstated—Patient’s status and/ordisposition was not indicated.
Expected source(s) of payment—Themethod of payment expected for theambulatory surgery visit. If only onepayment source was indicated in themedical record, only the ‘‘Principal’’column was marked and the ‘‘Otheradditional sources’’ column was leftblank. If two or more payment sourceswere indicated and one was designatedas the primary source, the ‘‘Principal’’column was marked for the primarysource and the ‘‘Other additionalsources’’ column was marked for theremaining indicated sources of payment.Only one source of payment wasmarked in the ‘‘Principal’’ column.
Worker’s Compensation—Expectedpayment is a state or municipaldisability insurance or industrialaccident insurance. This categorydoes not include company healthinsurance plans or direct paymentby an employer.
Medicare—Expected payment isunder the Health Care FinancingAdministration’s health insuranceprogram for the aged and disabled.This includes Medicare part Aand/or B and patients under therenal dialysis program. If Medicarebenefits are available, they areconsidered ‘‘Principal’’ unlessanother source of payment isspecifically stated as the principalsource.
Medicaid—Expected payment ismade under Title XIX of the SocialSecurity Act, which gives Federalassistance to states to provide healthcare for medically indigent patients.Medicaid may be known as publicaid, medical assistance, generalrelief, or some title specific to theState of residence, such as MediCalin California.
CHAMPUS—Expected payment ismade by the Civilian Health andMedical Program of the UniformedServices and is for military

a
Page 124 [ Series 1, No. 37
personnel and their families whouse civilian facilities.
Other governmentpayments—Expected payment underthe Title V Program, includingpayment under the State-fundedMaternal and Child Health Programand the State-funded CrippledChildren’s Program, or if theexpected payment cannot beclassified in one of the other fourgovernment categories.
Blue Cross/Blue Shield—Expectedpayment is made by a Blue Crossinsurance plan, Blue CrossAssociation, or Blue Shield plan.
HMO/PPO—Charges are includedunder a prepayment plan. Includeshealth maintenance organizations(HMO’s), independent practiceassociations (IPA’s), preferredprovider organizations (PPO’s), etc.
Other private or commercialinsurance—Expected payment ismade by any private insurance plannot included in the ‘‘BlueCross/Blue Shield’’ or ‘‘HMO/PPO’’categories.
Self-pay—Charges are paid in partor in full by the patient or thepatient’s family, which will not bereimbursed by a third party.Includes ‘‘co-payments’’ and‘‘insurance deductibles.’’
No charge—Visits for which no feeis charged.
Other—Any other source ofpayment not covered in thecategories above.
Billing Number—Needed on occasionto match medical record data to ‘‘totalcharge’’ information.
Total charges—Total charges asreported by the facility. In most cases,this amount was the facility fee chargedfor the procedure(s) performed thatexcluded any professional (e.g., surgeonfees. However, some charges may haveincluded professional fees if facilitieswere unable to separate them from anall-inclusive bill or ‘‘flat fee’’ chargedfor certain procedures.
)
Time—The appropriate clock time(including a.m. or p.m.) was recorded orthe ‘‘not available’’ box was checked foreach phase of the ambulatory surgeryvisit.
Type of anesthesia—All types ofanesthesia used during the ambulatorysurgery visit that were clearlydocumented in the medical recordwere included. If the type ofanesthesia was not clearly identified,‘‘other’’ was marked. If the type ofanesthesia was not given, ‘‘nonespecified’’ was marked.
Topical/local—Anesthesia thatnumbs only part of the body;feeling is numbed by temporarilyblocking nerves at or near the siteof the operation.
Regional—A special form of localanesthesia; anesthetics are injectedaround the main nerve to theaffected area. The anesthetics stopsensation in a wide region of thebody. Regional anesthesia can be ofthree types: epidural, spinal, andblock.
General—Anesthesia causing thewhole body to lose sensation. Thereare two ways that general anesthesican be administered: inhalation ofgas or vapor; and intravenous.
Anesthesia administered by—Thespecialty of the person(s) administeringthe anesthesia.
Final diagnoses—The ‘‘final,’’‘‘discharge,’’ ‘‘primary,’’ ‘‘secondary,’’‘‘associated,’’ ‘‘additional,’’ and ‘‘other’’diagnoses specifically identified andclearly summarized on the dischargesummary of the patient’s medical recordwas recorded. ‘‘Admitting,’’‘‘preliminary,’’ ‘‘working,’’ ‘‘tentative,’’or ‘‘provisional’’ diagnoses were notabstracted. If the final diagnoses werenot specifically identified and clearlysummarized on the discharge summary,the face sheet of the medical record wasused for abstracting the diagnosticinformation. If the physician did notspecify a principal diagnosis (thecondition established after study to bechiefly responsible for causing thepatient’s visit for ambulatory surgery),
the first final diagnosis listed on thepatient’s medical record was designatedon the medical abstract form asprincipal.
Surgical and diagnosticprocedures—The physician’s exactwording for each procedure as itappeared in the patient’s medical record.If a principal procedure was specified, itwas listed as ‘‘principal.’’ If a principalprocedure was not specified, the firstprocedure listed in the medical recordwas recorded as the principal procedureon the abstract form.

Vital and Health Statisticsseries descriptions
SERIES 1. Programs and Collection Procedures—These reports describethe data collection programs of the National Center for HealthStatistics. They include descriptions of the methods used tocollect and process the data, definitions, and other materialnecessary for understanding the data.
SERIES 2. Data Evaluation and Methods Research—These reports arestudies of new statistical methods and include analyticaltechniques, objective evaluations of reliability of collected data,and contributions to statistical theory. These studies also includeexperimental tests of new survey methods and comparisons ofU.S. methodology with those of other countries.
SERIES 3. Analytical and Epidemiological Studies—These reports presentanalytical or interpretive studies based on vital and healthstatistics. These reports carry the analyses further than theexpository types of reports in the other series.
SERIES 4. Documents and Committee Reports—These are final reports ofmajor committees concerned with vital and health statistics anddocuments such as recommended model vital registration lawsand revised birth and death certificates.
SERIES 5. International Vital and Health Statistics Reports—Thesereports are analytical or descriptive reports that compare U.S.vital and health statistics with those of other countries or presentother international data of relevance to the health statisticssystem of the United States.
SERIES 6. Cognition and Survey Measurement—These reports are fromthe National Laboratory for Collaborative Research in Cognitionand Survey Measurement. They use methods of cognitive scienceto design, evaluate, and test survey instruments.
SERIES 10. Data From the National Health Interview Survey—Thesereports contain statistics on illness; unintentional injuries;disability; use of hospital, medical, and other health services; anda wide range of special current health topics covering manyaspects of health behaviors, health status, and health careutilization. They are based on data collected in a continuingnational household interview survey.
SERIES 11. Data From the National Health Examination Survey, theNational Health and Nutrition Examination Surveys, and theHispanic Health and Nutrition Examination Survey—Datafrom direct examination, testing, and measurement onrepresentative samples of the civilian noninstitutionalizedpopulation provide the basis for (1) medically defined totalprevalence of specific diseases or conditions in the United Statesand the distributions of the population with respect to physical,physiological, and psychological characteristics, and (2) analysesof trends and relationships among various measurements andbetween survey periods.
SERIES 12. Data From the Institutionalized Population Surveys—Discontinued in 1975. Reports from these surveys are included inSeries 13.
SERIES 13. Data From the National Health Care Survey—These reportscontain statistics on health resources and the public’s use ofhealth care resources including ambulatory, hospital, andlong-term care services based on data collected directly fromhealth care providers and provider records.
SERIES 14. Data on Health Resources: Manpower and Facilities—Discontinued in 1990. Reports on the numbers, geographicdistribution, and characteristics of health resources are nowincluded in Series 13.
SERIES 15. Data From Special Surveys—These reports contain statistics onhealth and health-related topics collected in special surveys thatare not part of the continuing data systems of the NationalCenter for Health Statistics.
SERIES 16. Compilations of Advance Data From Vital and HealthStatistics—Advance Data Reports provide early release ofinformation from the National Center for Health Statistics’ healthand demographic surveys. They are compiled in the order inwhich they are published. Some of these releases may befollowed by detailed reports in Series 10–13.
SERIES 20. Data on Mortality—These reports contain statistics on mortalitythat are not included in regular, annual, or monthly reports.Special analyses by cause of death, age, other demographicvariables, and geographic and trend analyses are included.
SERIES 21. Data on Natality, Marriage, and Divorce—These reportscontain statistics on natality, marriage, and divorce that are notincluded in regular, annual, or monthly reports. Special analysesby health and demographic variables and geographic and trendanalyses are included.
SERIES 22. Data From the National Mortality and NatalitySurveys—Discontinued in 1975. Reports from these samplesurveys, based on vital records, are now published in Series 20or 21.
SERIES 23. Data From the National Survey of Family Growth—Thesereports contain statistics on factors that affect birth rates,including contraception, infertility, cohabitation, marriage,divorce, and remarriage; adoption; use of medical care for familyplanning and infertility; and related maternal and infant healthtopics. These statistics are based on national surveys of womenof childbearing age.
SERIES 24. Compilations of Data on Natality, Mortality, Marriage,Divorce, and Induced Terminations of Pregnancy—Theseinclude advance reports of births, deaths, marriages, and divorcesbased on final data from the National Vital Statistics System thatwere published as supplements to theMonthly Vital StatisticsReport(MVSR). These reports provide highlights and summariesof detailed data subsequently published inVital Statistics of theUnited States. Other supplements to the MVSR published hereprovide selected findings based on final data from the NationalVital Statistics System and may be followed by detailed reportsin Series 20 or 21.
For answers to questions about this report or for a list of reports published inthese series, contact:
Data Dissemination BranchNational Center for Health StatisticsCenters for Disease Control and Prevention6525 Belcrest Road, Room 1064Hyattsville, MD 20782-2003
(301) 436–8500E-mail: [email protected]:http://www.cdc.gov/nchswww/nchshome.htm

DEPARTMENT OFHEALTH & HUMAN SERVICES
Centers for Disease Control and PreventionNational Center for Health Statistics6525 Belcrest RoadHyattsville, Maryland 20782-2003
OFFICIAL BUSINESSPENALTY FOR PRIVATE USE, $300
DHHS Publication No. (PHS) 98-1313, Series 1, No. 377-0673 (10/97)
STANDARD MAIL (B)POSTAGE & FEES PAID
PHS/NCHSPERMIT NO. G-281
FOLD FOLDSPINE
COVER 4PRINTER: ADJUST SPINE TO FIT
PRINTER:
POSITIVE ART FOR BACK COVER (cover 4): PRINT SOLID PMS
NEGATIVE ART FOR FRONT COVER (cover 1): PRINT SOLID PMS