vol 31 no 1 – march 2012 - acnem
TRANSCRIPT

Vol 31 No 1 – March 2012
ACNEMJournal
Biochemical Individuality; Assessment of the Chronic Refractory (or Complex) patient part 2
Co-infusing Glutathione and Vitamin C during cancer treatment: a reply
Determining an anti-inflammatory diet based on post-prandial research findings
ACNEM Online (Distance) Learning: Behind the interface
the journal of the australasian college of nutritional and environmental medicine
AUSTRALIA POST PRINT POST PUBLICATIONNo. PP327230/0008 ISSN 1328-8040
about acnem
The Australasian College of Nutritional and Environmental Medicine (ACNEM) Inc, is a not-for-profit medical college established in 1982, offering postgraduate training for doctors and other graduate healthcare professionals in Nutritional and Environmental Medicine, membership, Fellowship and a popular find-a-practitioner service for members of the public.
what is nem?
Nutritional and Environmental Medicine (NEM) is concerned with the interaction of nutritional and environmental factors with human biochemistry and the resulting physiological and psychological symptoms and pathology. NEM is evidence-based, drawing on the latest biomedical science, research and clinical application to develop new treatment approaches to illness and disease, for primary prevention and to promote optimal health and well-being.
Nutritional deficiencies or imbalances, or the presence of environmental toxins in the body can result in cellular dysfunction, illness or disease. Treatment is aimed at correcting underlying causes as well as providing symptomatic relief. This may involve removal of certain foods from the diet or toxins from the patient’s environment, or prescription of supplements such as vitamins, minerals, trace elements and essential fatty acids where diet and lifestyle alone cannot rectify physiological imbalances.
acnem membership
Full Membership of the College is open to doctors and dentists. Associate Membership is available to other suitably qualified and affiliated healthcare professionals. Membership benefits include the quarterly ACNEM Journal, a weekly email newsletter, and discounts on education and training. Members of the public are also invited to become Friends of ACNEM to support the work of the College.
acnem training
ACNEM training is regarded as unique in the world. The training programs are designed by the expert ACNEM Faculty for practitioners wanting to learn more effective ways of treating their patients. Content is strongly referenced and presented by some of Australia and New Zealand’s leading clinicians. The emphasis is always on ‘putting it into practice’, with guidelines and practical tools to aid implementation. Training is held throughout the year at locations around Australia and New Zealand, and also by distance (online) learning.
cpd/cme points
ACNEM is an accredited RACGP QI&CPD training provider for the 2011-2013 Triennium with 40 Category 1 points allocated to most training programs. ACRRM, RNZCGP and CPD/CME points from other professional organisations may also be available.
Continued on back page...
R A C G P Q A & C P D A
PP
RO
VE
D RACGP QA&CPD
AP
PR
OV
ED
A C C R E D I T E D
P R O V I D E R
membership of acnem
If you wish to apply for membership of the College to receive this Journal, please complete and return this expression of interest form.
Name:
Address: State: Postcode:
Phone (work): ( ) Phone (home): ( )
Fax: ( ) Mobile:
Email:
Occupation: Qualifications:
Post to: Or fax to: ACNEM (03) 9597 0383 PO Box 298 Sandringham Vic 3191 Australia
✃
ACNEM Journal Vol 31 No 1 – March 2012
Contents
The College, Journal, and its Editorial Board do not take responsibility for or necessarily agree with opinions or claims of authors or advertisers. All reasonable care is taken to select responsible and well-researched material for the Journal. Guidelines for authors are available on request and may also be viewed at www.acnem.org. The Editorial Board reserves the right to accept or reject content or advertising material without giving reasons for any decisions made.
This Journal is copyright of ACNEM. All rights reserved. The College’s written permission must be obtained prior to using or reprinting any part of this Journal. The ACNEM logo is a registered trademark of the Australasian College of Nutritional and Environmental Medicine Inc, and all parts of the logo are protected, including its graphic elements and the word ‘ACNEM’. ACNEM Inc. is an incorporated association under the laws of Victoria, Australia. Reg: A0022218W. ABN: 18 776 847 535.
From the Editor 2
Biochemical Individuality; Assessment of theChronic Refractory (or Complex) Patient Part 2 3Joanna Harnett
Co-infusing Glutathione and Vitamin C during cancer treatment: a reply 8Ian Dettman, Cliff Meakin, Rob Allen
Determining an anti-inflammatory diet based on post-prandial research findings 12Garry Egger
ACNEM Online (Distance) Learning: Behind the interface 15Adrian Hekel
In The News 22Shirley Schurmann
In Memoriam - Chris Reading 23
In Memoriam - Archie Kalokerinos 24
Your College 25
Featured Books 26
Letters to the Editor 28
Journal of the Australasian College of Nutritional and Environmental Medicine Inc (ACNEM) PO Box 298, Sandringham, VIC, 3191, Australia Phone: (03) 9597 0363 Fax: (03) 9597 0383 Email: [email protected] Web: www.acnem.org
Editorial Board Oscar Serrallach, MBChB, FRACGP (Editor) Stephen Penman, M AppSc (H Sc)(R), GC Tert Teach Learn Jimena Acevedo ( Journal Production) BSc, BAppSci
Board of ManagementDr Karel Hromek (President)A. Prof Eugen Molodysky (Vice President)Dr Jennie McKern (Secretary)Dr Tony Bartone (Treasurer)Dr Anjana ArunachalamDr Ron EhrlichDr Debbie FewtrellDr Timothy HallDr Braham RabinovDr Oscar SerrallachDr Matthew SheltonDr Michelle Woolhouse
The Expert Teaching Faculty includes Dr Denis Rebic, MBBS, ABAAM, Dip ACNEM, Cert NEM,FACNEMAnn-Mary Hromek, RN, ND, MATMSDr Peter Baratosy, MBBS, PhD, Dip Acu, Dip Clin Hyp, FACNEMDr Debbie Fewtrell, MB ChB, Dip Obst, FACNEM, FRNZCGPDr Kerry Harris, BMBS, FRACGP, BSc(Hons), FACNEMDr Karel Hromek, BMed, BSc, FACNEM, FACRRMDr Carole Hungerford, BA, MBBS, FACNEMDr James Read, MBBS, Dip RANZCOG, FRACGP, FACNEMDr Matthew Shelton, MBChB, MRCGP, DRCOG, FCAnaes DA,FACNEMProf Melvyn Sydney-Smith, KGSJ, MBBS, PhD, MHMS(prov), GradDip Clin Nut., Grad Dip Gestalt Ther., Grad
Personnel Stephen Penman (CEO)Jimena Acevedo (Executive Officer)Michelle Bradford (Training and Events Manager)Ann-Mary Hromek (Education Co-ordinator)Kathryn Silver (Administration and Membership)Max Wang (Technical Manager)Sean Hubbard (Website & Graphic Design)
ACNEM Journal Vol 31 No 1 – March 2012
2
To the Members and Friends of ACNEM,
As the new editor of the ACNEM journal, I welcome you all to this latest issue. It is with great honour and a sense of pride that I embark on this role in what is a key part of communication between our college and the greater community.
Many patients ask me, “Why is none of this nutrition stuff taught in medical school and why isn’t it part of mainstream practice?” My reply to them is, “There is a lot of science in medicine… and even more that isn’t!” It is in this spirit that I will endeavour to provide articles that:
1. Review core aspects of nutritional biochemistry, such as Joanna Harnett’s article series on Urinary Organic Acids
2. Give sound expert opinion, such as Ian Dettman’s reply to the Chen et al. article
3. Introduce new concepts and further our horizons, such as Garry Egger’s article discussing the concept of ‘metaflammation’.
No individual can be an expert at everything (contrary to what some Google-holics might think!) but many of us are experts in select areas of the vast realm of nutritional and environmental
medicine. With this in mind I invite all our colleagues in their busy lives to pass on a pearl of their wisdom by writing an article for the Journal. Your efforts will be greatly appreciated, and will help to keep our community inspired, informed and up-to-date.
I recall an article I read in the ACNEM Journal ( June 2011) by Dr Jim Bartley regarding Exorphins and Food Hypersensitivity. This article explained how stress could lead to CRF release, which in turn would increase intestinal permeability. This well referenced article for me was one such pearl that explained a key link in the Body-Mind-Gut paradigm, and was neither an opinion nor an hypothesis, but indeed, a fact! I am so grateful for these morsels on the path to understanding, and I am excited about what yet remains unseen.
In this issue we also pay deep respect to two pioneers of nutritional medicine whom have recently passed away, Dr Chris Reading and Dr Archie Kalokerinos. May we be thankful that we are still able to stand on the shoulders of such giants.
Sincerely,
Dr Oscar Serrallach
From the EditorDr Oscar Serrallach, MBChB, FRACGP
3
ACNEM Journal Vol 31 No 1 – March 2012
preface
One of the central premises of Nutritional Environmental Medicine (NEM) assessment is the consideration of the unique biochemistry of the patient. Chronic illness of unexplained aetiology is a good example of a patient population that may benefit from an individualised nutritional biochemical assessment1. This technical article is part two of three articles looking at different subgroups of urinary organic acid markers and their potential clinical use in patients with chronic refractory symptoms. Part one of this series covered an introduction to urinary organic acids and their use in the assessment of fatty acid, carbohydrate and citric acid cycle metabolism2. In this publication, we will consider specifically the metabolites of gastrointestinal microbiota.
introduction
The recognition of the role of gastrointestinal microbiota in health and disease is not new and dates back to 400BC, with Hippocrates stating that “bad digestion is the root of all evil and that death begins in the colon”3. In more recent years, our quest to understand the complexity of the composition and function of gastrointestinal microbiota in health and disease has gained considerable momentum. This momentum is reflected in a four-fold increase in publications dedicated to the topic4. It is estimated that the human microbiota contains as many as 10¹⁴ bacterial cells, a number that is ten times greater than the number of human cells in our body. Of these 10¹⁴ microbial cells, 70% are found in the gastrointestinal tract which has a surface area the size of a tennis court5. Recent analysis has estimated that the collective commensal microbiota is composed of over 35,000
bacterial species6. Throughout history much of our attention has focused on identifying and understanding pathogenic bacteriology, mycology and parasitology, however, the growing body of research has turned its attention to understanding the predominant or commensal microecology7. This new knowledge supports the infamous deathbed remark by Pasteur where he belied the notion that germs could tell the whole story. It was the tacit acknowledgement to Claude Bernard, who advocated that health was due to the equilibrium in the “milieu interieur” and “maintained by a continuous and delicate compensation, established as the most sensitive of balances” that would be the travailing line of inquiry 117 years later8.
main functions of gut flora
Metabolic Fermentation of non-digestible dietary residue and endogenous mucus; salvage of energy as short chain fatty acids; production of thiamine, riboflavin, B12, Biotin and vitamin K, absorption of ions9
Trophic Control of epithelial cell proliferation and differentiation; development of homeostasis9
Protective Protection against pathogens9
Immunomodulation Modulation of immune response to self and foreign proteins10,12
Biochemical Individuality; Assessment of the Chronic Refractory (or Complex) patientPart Two: Urinary metabolites originating from intestinal Microbiota Joanna Harnett, MHSc, BHSc, PhD scholar (Southern Cross University)
continued next page
ACNEM Journal Vol 31 No 1 – March 2012
4
metabolomics and the gastrointestinal tract
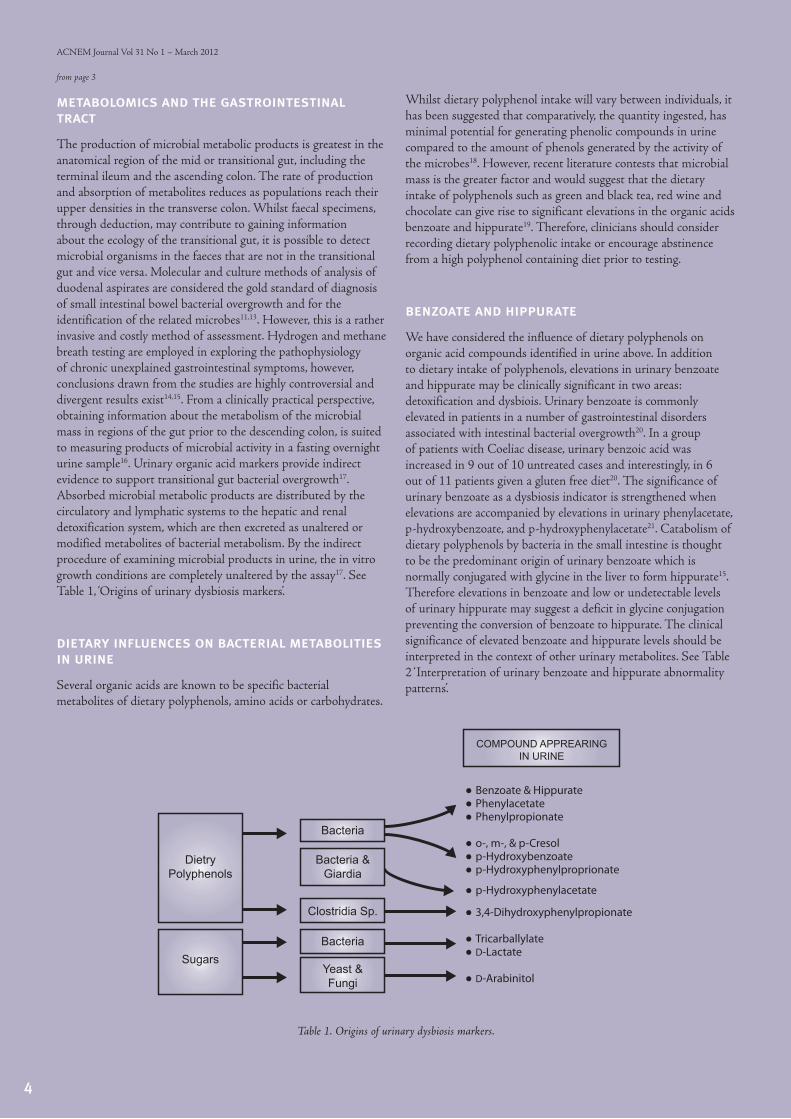
The production of microbial metabolic products is greatest in the anatomical region of the mid or transitional gut, including the terminal ileum and the ascending colon. The rate of production and absorption of metabolites reduces as populations reach their upper densities in the transverse colon. Whilst faecal specimens, through deduction, may contribute to gaining information about the ecology of the transitional gut, it is possible to detect microbial organisms in the faeces that are not in the transitional gut and vice versa. Molecular and culture methods of analysis of duodenal aspirates are considered the gold standard of diagnosis of small intestinal bowel bacterial overgrowth and for the identification of the related microbes11,13. However, this is a rather invasive and costly method of assessment. Hydrogen and methane breath testing are employed in exploring the pathophysiology of chronic unexplained gastrointestinal symptoms, however, conclusions drawn from the studies are highly controversial and divergent results exist14,15. From a clinically practical perspective, obtaining information about the metabolism of the microbial mass in regions of the gut prior to the descending colon, is suited to measuring products of microbial activity in a fasting overnight urine sample16. Urinary organic acid markers provide indirect evidence to support transitional gut bacterial overgrowth17. Absorbed microbial metabolic products are distributed by the circulatory and lymphatic systems to the hepatic and renal detoxification system, which are then excreted as unaltered or modified metabolites of bacterial metabolism. By the indirect procedure of examining microbial products in urine, the in vitro growth conditions are completely unaltered by the assay17. See Table 1, ‘Origins of urinary dysbiosis markers’.
dietary influences on bacterial metabolities in urine
Several organic acids are known to be specific bacterial metabolites of dietary polyphenols, amino acids or carbohydrates.
Whilst dietary polyphenol intake will vary between individuals, it has been suggested that comparatively, the quantity ingested, has minimal potential for generating phenolic compounds in urine compared to the amount of phenols generated by the activity of the microbes18. However, recent literature contests that microbial mass is the greater factor and would suggest that the dietary intake of polyphenols such as green and black tea, red wine and chocolate can give rise to significant elevations in the organic acids benzoate and hippurate19. Therefore, clinicians should consider recording dietary polyphenolic intake or encourage abstinence from a high polyphenol containing diet prior to testing.
benzoate and hippurate
We have considered the influence of dietary polyphenols on organic acid compounds identified in urine above. In addition to dietary intake of polyphenols, elevations in urinary benzoate and hippurate may be clinically significant in two areas: detoxification and dysbiois. Urinary benzoate is commonly elevated in patients in a number of gastrointestinal disorders associated with intestinal bacterial overgrowth20. In a group of patients with Coeliac disease, urinary benzoic acid was increased in 9 out of 10 untreated cases and interestingly, in 6 out of 11 patients given a gluten free diet20. The significance of urinary benzoate as a dysbiosis indicator is strengthened when elevations are accompanied by elevations in urinary phenylacetate, p-hydroxybenzoate, and p-hydroxyphenylacetate21. Catabolism of dietary polyphenols by bacteria in the small intestine is thought to be the predominant origin of urinary benzoate which is normally conjugated with glycine in the liver to form hippurate15. Therefore elevations in benzoate and low or undetectable levels of urinary hippurate may suggest a deficit in glycine conjugation preventing the conversion of benzoate to hippurate. The clinical significance of elevated benzoate and hippurate levels should be interpreted in the context of other urinary metabolites. See Table 2 ‘Interpretation of urinary benzoate and hippurate abnormality patterns’.
from page 3
● Benzoate & Hippurate● Phenylacetate● Phenylpropionate
● o-, m-, & p-Cresol● p-Hydroxybenzoate● p-Hydroxyphenylproprionate
● p-Hydroxyphenylacetate
● 3,4-Dihydroxyphenylpropionate
● Tricarballylate● D-Lactate
● D-Arabinitol
DietryPolyphenols
Sugars
Bacteria & Giardia
Yeast & Fungi
Bacteria
Clostridia Sp.
Bacteria
COMPOUND APPREARING IN URINE
Table 1. Origins of urinary dysbiosis markers.

5
ACNEM Journal Vol 31 No 1 – March 2012
phenylacetate and hydroxyphenylacetate
Intestinal bacterial metabolism on dietary polyphenols may also result in the appearance of phenylacetic acid (PAA) in the urine. However, urinary PAA is also the product of unidentified, specific strains of bacteria22. Urinary phenylacetate may be elevated in small intestinal bacterial overgrowth (SIBO)22.
Enteric bacteria that possess L-ammonia acid decarboxylase produce hydroxyphenylacetic (HPA) acid from dietary tyrosine. Increased excretion has been demonstrated in both children and adults with small bowel disease or bacterial overgrowth syndrome23. In 360 unselected acutely ill infants and children, urinary 4-hydroxyphenyl acetic acid was measured as a potential screening tool for small bowel disease and bacterial overgrowth. No false negative results and only 2% false positive results were observed. Among the 10 patients whose urinary excretion of the analyte was considered to be abnormal were patients with giardia lamblia infestation, ileal resection with blind loop and other small intestinal disease associated with bacterial overgrowth23.
hydroxyphenylproprionate
Dietary intake of polyphenols such as caffeic acid from coffee, catechins from green tea and the proanthocyanidins found in grapes, can increase the excretion of hydroxyphenylproprionate (HPPA) in the urine of healthy patients. High levels of HPAA, may also indicate increased bacterial metabolism of dietary polyphenols23. A dietary loading of catechins and caffeic acid resulted in a significant increase in HPPA excretion in rat urine to 200 mcg/24 hours. However when a combination of the antibiotics sulfathiozide and auromycin were administered the level of HPPA dropped to 10 mcg/ml24. These results suggest that dietary polyphenol intake and the individuals’ microbial mass play a role in the variations observed in HPPA
excretion. Furthermore, Khan et al demonstrated that the urinary metabolites, p-hydroxybenzoate, p-hydroxyphenylacetate, phenylproprionate, phenyllactate and phenylpyruvate are specifically products of the bacterial action on HPPA, not protozoal action25.
Indican is a product of bacterial action on the amino acid tryptophan. An elevated level of urinary indican has been demonstrated as a possible marker of SIBO26. Patients with small bowel disease are at a greater risk of SIBO. In a systematic review of the diagnosis of small intestinal bowel overgrowth urinary indican was considered to be a valid indicator of SIBO27. As with the interpretation of all urinary organic acids, dietary factors must be considered. Impaired protein digestion may be a cause of high excretion of urinary indican by increasing the available tryptophan for bacterial action. Therefore in the absence of any other urinary metabolites of bacterial metabolism, the clinician should consider protein digestion capacity. To this end, urinary indican has been used to assess enteric protein loss in patients with cirrhosis of the liver and malabsorption of protein in the elderly in conjunction with plasma amino acid levels28.
tricarballylate
Tricarballylate is a product of aerobic bacterial metabolism with a significant mineral chelating capacity. The clinical implication of tricarballylate producing bacterial overgrowth is principally nutrient deficiencies of magnesium, zinc and calcium29. In ruminant studies, the wheat grass feed fermented to form high levels of tricarballylate, resulting in loss of appetite, tetanic convulsions and death30. Thus a laboratory finding of high urinary tricarballylate indicates the need to assess the patient for mineral deficiencies.
continued next page
Low Low
LowHigh
Low High
High High
Benzoate Hippurate Other Bacterial Markers Interpretation
No elevations
Multiple elevations
No elevations
No elevations
No elevations
Multiple elevations
Multiple elevations
Multiple elevations
Low intake of benzoate and precursors, plus normal or low dietary polyphenol conversion by intestinal microbes
Low intake of benzoate and precursors with intestinalmicrobial overgrowth of species that do not metabolize dietarypolyphenols (very rare)
Glycine conjugation de�cit (possibly genetic polymorphic phenotype if hippurate is very low); dietary benzoate or precursor intake
Glycine conjugation de�cit; presume benzoate is at least partiallyfrom intestinal microbial action on dietary polyphenols
Normal hippurate production via active glycine conjugation; Noindication of microbial overgrowth
Normal hippurate production via active glycine conjugation;Presume hippurate is at least partially derived from intestinalmicrobial action on dietary polyphenols
Very high dietary benzoate or precursor intake with partial conversion to hippurate
Very high benzoate load, some, or all, or which is contributed byintestinal microbial action on dietary polyphenols
Table 2. Interpretation of urinary benzoate and hippurate abnormality patterns
ACNEM Journal Vol 31 No 1 – March 2012
6
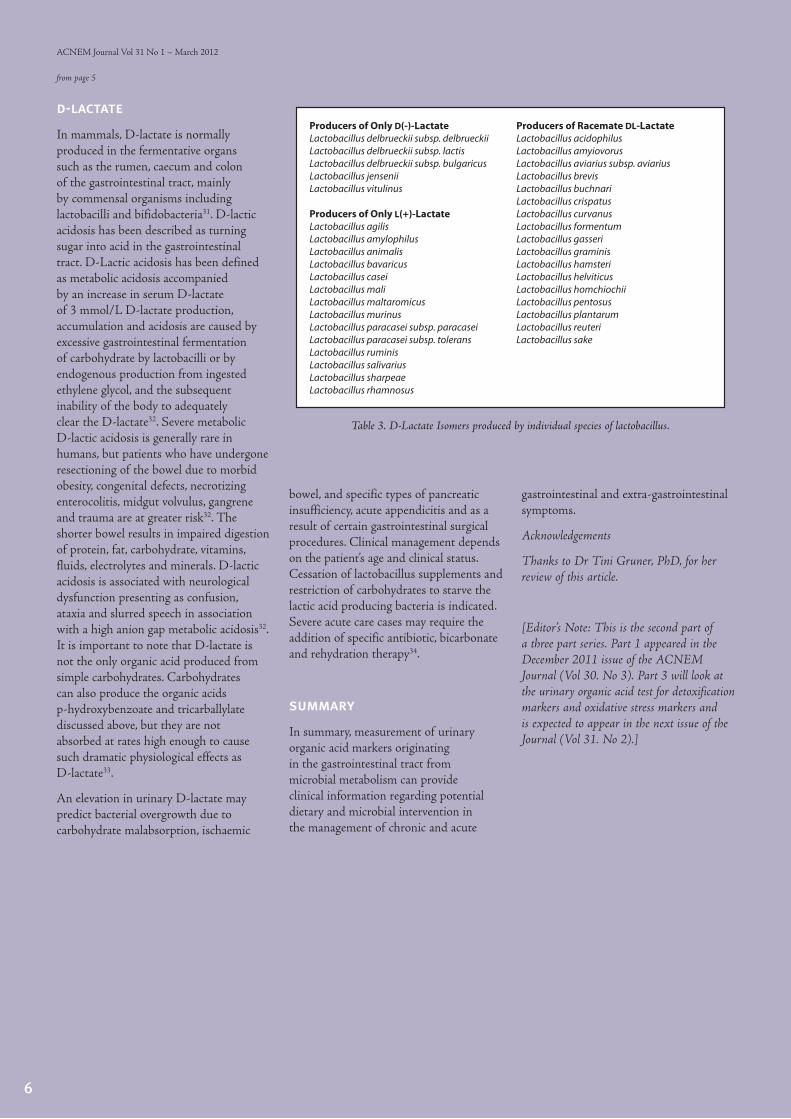
d-lactate
In mammals, D-lactate is normally produced in the fermentative organs such as the rumen, caecum and colon of the gastrointestinal tract, mainly by commensal organisms including lactobacilli and bifidobacteria31. D-lactic acidosis has been described as turning sugar into acid in the gastrointestinal tract. D-Lactic acidosis has been defined as metabolic acidosis accompanied by an increase in serum D-lactate of 3 mmol/L D-lactate production, accumulation and acidosis are caused by excessive gastrointestinal fermentation of carbohydrate by lactobacilli or by endogenous production from ingested ethylene glycol, and the subsequent inability of the body to adequately clear the D-lactate32. Severe metabolic D-lactic acidosis is generally rare in humans, but patients who have undergone resectioning of the bowel due to morbid obesity, congenital defects, necrotizing enterocolitis, midgut volvulus, gangrene and trauma are at greater risk32. The shorter bowel results in impaired digestion of protein, fat, carbohydrate, vitamins, fluids, electrolytes and minerals. D-lactic acidosis is associated with neurological dysfunction presenting as confusion, ataxia and slurred speech in association with a high anion gap metabolic acidosis32. It is important to note that D-lactate is not the only organic acid produced from simple carbohydrates. Carbohydrates can also produce the organic acids p-hydroxybenzoate and tricarballylate discussed above, but they are not absorbed at rates high enough to cause such dramatic physiological effects as D-lactate33.
An elevation in urinary D-lactate may predict bacterial overgrowth due to carbohydrate malabsorption, ischaemic
Producers of Only D(-)-LactateLactobacillus delbrueckii subsp. delbrueckiiLactobacillus delbrueckii subsp. lactisLactobacillus delbrueckii subsp. bulgaricusLactobacillus jenseniiLactobacillus vitulinus
Producers of Only L(+)-LactateLactobacillus agilisLactobacillus amylophilus Lactobacillus animalisLactobacillus bavaricusLactobacillus caseiLactobacillus maliLactobacillus maltaromicusLactobacillus murinusLactobacillus paracasei subsp. paracaseiLactobacillus paracasei subsp. toleransLactobacillus ruminisLactobacillus salivariusLactobacillus sharpeaeLactobacillus rhamnosus
Producers of Racemate DL-LactateLactobacillus acidophilusLactobacillus amyiovorusLactobacillus aviarius subsp. aviariusLactobacillus brevisLactobacillus buchnariLactobacillus crispatusLactobacillus curvanusLactobacillus formentumLactobacillus gasseriLactobacillus graminisLactobacillus hamsteriLactobacillus helviticusLactobacillus homchiochiiLactobacillus pentosusLactobacillus plantarumLactobacillus reuteriLactobacillus sake
Table 3. D-Lactate Isomers produced by individual species of lactobacillus.
from page 5
bowel, and specific types of pancreatic insufficiency, acute appendicitis and as a result of certain gastrointestinal surgical procedures. Clinical management depends on the patient’s age and clinical status. Cessation of lactobacillus supplements and restriction of carbohydrates to starve the lactic acid producing bacteria is indicated. Severe acute care cases may require the addition of specific antibiotic, bicarbonate and rehydration therapy34.
summary
In summary, measurement of urinary organic acid markers originating in the gastrointestinal tract from microbial metabolism can provide clinical information regarding potential dietary and microbial intervention in the management of chronic and acute
gastrointestinal and extra-gastrointestinal symptoms.
Acknowledgements
Thanks to Dr Tini Gruner, PhD, for her review of this article.
[Editor’s Note: This is the second part of a three part series. Part 1 appeared in the December 2011 issue of the ACNEM Journal (Vol 30. No 3). Part 3 will look at the urinary organic acid test for detoxification markers and oxidative stress markers and is expected to appear in the next issue of the Journal (Vol 31. No 2).]
7
ACNEM Journal Vol 31 No 1 – March 2012
Referencees:
1. Genius SJ. “Medical practice and community health care in the 21st century: A time of change” Public Health 11:671-680, 2008
2. Harnett J. “Biochemical Individuality: Assessment of the chronic or refractory or complex patient” ACNEM Journal 30:3;8-13, 2011
3. Hawrelak J A, Myers SP. “The causes of intestinal dysbiosis a review”. Altern Med Rev 9: 180-197, 2004
4. http:www.ncbi.nlm.nih.gov/pubmed/
5. Sekirov et al. “Gut Microbiota in Health and Disease” Physiol Rev 90:859-904, 2009
6. Frank DN et al. “Molecular-phylogenetic characterization of microbial community imbalances in human inflammatory bowel diseases.” Proc Natl Acad Sci USA 104:13780-13785, 2007
7. http:www.ncbi.nlm.nih.gov/pubmed/
8. Tracey K. “Physiology and immunology of the cholinergic anti-inflammatory pathway.” J Clin Invest 117(2):289-296, 2007
9. Guarner F, Malagelada JR. “Gut flora in health and disease” The Lancet 361:9356;512-519, 2002
10. Guarner F, Malagelada JR. “Gut flora in health and disease” The Lancet 361:9356;512-519, 2002
11. Guarner F, Malagelada JR. “Gut flora in health and disease” The Lancet 361:9356;512-519, 2002
12. Kelly D et al. “Commensal gut bacteria: mechanisms of immune modulation” Trends in Immunology 26(6):326-333, 2005
13. Choung R S. “Clinical predictors of small intestinal bacterial overgrowth by duodenal aspirate culture” Aliment Pharmacol Ther 33:1059-1067, 2011
14. Simren et al. “Use and abuse of hydrogen breathe tests” GUT 55:297-303, 2006
15. Lord R S, Bralley J A. “Clinical applications of urinary organic acids, Part 2: Dysbiosis Markers” Altern Med Rev 13:(4)292-306, 2008
16. J.B. Ewaschuk et al. “Metabolic acidosis: separation methods and biological relevance of organic acids and lactic acid entiomers” J. Chromatogr. 781: 39–56, 2002
17. Lord & Bralley. “Laboratory Evaluations for Integrative and Functional Medicine” 2nd edn. 2008
18. Lord R S, Bralley J A. “Clinical applications of urinary organic acids, Part 2: Dysbiosis Markers” Altern Med Rev 13:(4)292-306, 2008
19. Gonthier M P et al. “Chlorogenic acid bioavailability depends on its metabolism by gut microflora in rats” J Nutr 133:1853-1859, 2005
20. Van der Heiden et al. “Gas Chromatographic analysis of urinary tyrosine and phenylalanine metabolites in patients with gastrointestinal disorders” Clin.Chim.Acta 34:289-296, 1971
21. Goodwin et al. “Gut flora and the origin of some urinary aromatic phenolic compounds “Biochem Pharmacol. 47:2294-2297, 1994
22. Chalmers RA, Valman HB, Liberman MM. “Measurement of 4-hydroxyphenylacetic aciduria as a screening test for small bowel disease” Clin Chem. 25(10):1791-4, 1979
23. Chalmers RA, Valman HB, Liberman MM. “Measurement of 4-hydroxyphenylacetic aciduria as a screening test for small bowel disease” Clin Chem. 25(10):1791-4, 1979
24. Griffiths L.A. “Studies on flavanoid metabolism. Identification of the metabolites of (t) –catechinin rat urine. Biochem J 92:173-79, 1964
25. Khan RI et al. “Aromatic amino acid biosynthesis and production of related compounds from p-hydroxyphenylpyruvic acid by rumen bacteria, protozoa and their mixture.” Amino Acids 22:167-77, 2002
26. Powell-Jackson PR et al. “Intestinal bacterial metabolism of protein and bile acids: role in pathogenesis of hepatic disease after jejuno-ileal bypass surgery” Br J Surg 66:772-775, 1979
27. Khoshini et al. “A systematic review of diagnostic tests for small intestinal bacterial overgrowth” Dig Dis Sci 53:1443-1454, 2008
28. Mayer PJ et al. “The role of urinary indican as a predictor of bacterial colonization in the human jejunum. Am J Dig Dis 20:1003-1009, 1975
29. Schwartz R et al. “Effect of tricarballylic acid, a non-metabolizable rumen fermentation product of trans-aconitic acid, on Mg, Ca and Zn utilization in rats” J Nutr 118:183-188, 1988
30. Russell JB. “Production of tricarballylic acid by rumen microorganisms and its potential toxicity in ruminant tissue metabolism.” British Journal of Nutrition 56:153-162
31. Ewaschuk J et al. “D-Lactate in Human Ruminant Metabolism” J Nutr 135:1619-1625, 2005
32. Peterson C. “D-Lactic Acidosis “Nutr Clin Pract 20:6 634, 2005
33. Uribarri J et al. “D-Lactic acidosis” Medicine 77:73-82, 1998
34. Bongaerts GP et al. “Lactobacilli and acidosis in children with small short bowel” J PaedGastroenterol Nutr. 30:288-293, 2000

[Editor’s note: This article is in reply to “Chen P, Stone J, Sullivan G, Drisko JA, Chen Q. Anti-cancer effect of pharmacologic ascorbate and its interaction with supplementary parenteral glutathione in preclinical cancer models. Free Radic Biol Med. 2011 Aug 1;51(3):681-7. Epub 2011 May 30., available for purchase from http://www.sciencedirect.com/science/article/pii/S0891584911003479.]
Recently, a criticism has been raised by Chen et al. to avoid the administration of intravenous Vitamin C and Glutathione at the same time6. We acknowledge that the authors understand the benefits of high dose intravenous Vitamin C and that from their studies they have deduced that in cancer treatment the “simultaneous administration” of Glutathione (antioxidant effect by their definition) and Vitamin C (pro-oxidant by their definition) interferes with the cytotoxic effectiveness of the Vitamin C. Although from their results there is some suggestion of this interference by Glutathione, at this stage we remain unconvinced that the common practice of administering low levels of Glutathione (500mg to 1g) at the same time as high dose intravenous Vitamin C (30g to 100g) is not in the best interests of cancer patients who are usually under considerable systemic oxidative stress.
Of interest are the following observations
concerning the Chen trial:
1. The amounts of Vitamin C and Glutathione used in vivo were distinctly non-physiological compared to the in vitro studies, where it was claimed in the paper (correctly) that the in vitro concentration of Glutathione was clinically relevant (640µM). 640µM is approx equivalent to the infusion of 1.5 gram of Glutathione into an adult human, presuming 5 litres of blood. Instead, they have used the equivalent of 48 grams of Glutathione infused into a 60kg human. This was a massive overdose in terms of additional Glutathione but still there was some positive effect both on tumor reduction and mouse survival. It is hardly a relevant comparison with what is done in clinical practice and, therefore, potentially, not particularly meaningful in explaining the benefits or shortcomings of co-infusing Glutathione and Vitamin C.
2. The concentration of Vitamin C used in tissue culture was in fact quite low – let’s say 2mM, which is approx 40mg%. However, the amount injected into the mice was 4000mg/kg – equivalence for an adult human body is 240,000mg/60kg, which could potentially result in levels in the blood stream at least as high as 400 to
600mg%, which is far in excess of what was used in vitro. No investigation was done into Vitamin C levels achieved in the blood stream of the athymic mice, so there is no way of evaluating if these high levels of Vitamin C were achieved and maintained in the mice. Unless the Vitamin C levels were/are measured in the mice (in the blood stream or preferably in situ at the cancer cell site), it is very difficult to make a deduction about the correlation of their tissue culture studies and the in vivo studies.
3. Virtually all cell lines had a 100% kill rate by ascorbate concentrations between 1mM and 2mM – this is quite remarkable because 100% kill rate of cancer cells at such low Vitamin C concentrations has not been reported across such a large range of cancer cell types.
However, research by the Riordan Institute7 and by Mark Levine8 have reported 100% kill rates at ascorbate levels as high as 20mM, with a 50% kill rate reported at somewhat lower Vitamin C concentrations.
It is an interesting observation by Chen et al. that virtually all cell lines had a very similar 100% kill rate by the same low concentration of Vitamin C (1 to 2mM); an unusual phenomenon.
8
ACNEM Journal Vol 31 No 1 – March 2012
Co-infusing Glutathione and Vitamin C during cancer treatment: a replyIan Dettman PhD (Biochem), BSc Hon (Biochem), Cliff Meakin BHSc, Rob Allen MBBS
9
ACNEM Journal Vol 31 No 1 – March 2012
4. Despite the claim that Glutathione totally stopped the effect of the Vitamin C in vitro, this is not what the accompanying graphs show. In virtually all cases in vitro there has been a decrease in cell viability when the combination of Vitamin C and Glutathione has been used. Who knows what the effect on cell survival may have been if they had used the same absolute concentrations of Vitamin C and Glutathione in vitro that they ended up using in vivo.
5. It is interesting that more mice survived up to 30 days in the Vitamin C + Glutathione-treated group than the Vitamin C group or the Glutathione group. Is successful treatment measured only by tumor shrinkage or by survival? (Preferably both, of course, but survival is imperative.)
6. It is also interesting that the same number of mice survived to 30 days in the Vitamin C group and the Glutathione group. Toxicity levels would appear to be the same.
7. Despite the claim that there was no reduction in tumor volume in the Glutathione group or the Glutathione + Vitamin C group, in the graphs there was some reduction compared to the control and it was greater in the Glutathione + Vitamin C group compared to just the use of Glutathione. Who knows what would have ultimately happened if the experiment had been allowed to go to ‘natural death’, as the Glutathione + Vitamin C-treated mice were surviving in greater numbers.
8. Evidence is certainly accumulating that one of the mechanisms by which high-dose intravenous Vitamin C works is (indirectly) through the production of hydrogen peroxide. The addition of Glutathione in tissue culture in the absence of plasma, red cells and white cells, endothelial barriers, extracellular matrix barriers, systemic oxidative stress, liver uptake, brain uptake and metabolic catabolism, is hardly representative of an in vivo clinical situation of infusing a gram or two of Glutathione, especially when, because of pharmacokinetics, only a small amount of the infused Glutathione is likely to end up at the cancer cell site. So, it may well be that, in low concentration, Glutathione is a scavenger of reactive oxygen metabolites. However, the question could be and should reasonably be proposed that a small amount of co-infused Glutathione is far more likely to end up in multiple areas of the body – liver/brain/red cells/lungs – than suddenly concentrating in situ in a cancerous tissue. It is probable that these lower levels of Glutathione help protect the body from the systemic oxidative stress that exists in a person with cancer11,12.
9. This paper unfortunately alludes to that old concept of not giving an antioxidant at the same time as an oxidizing agent. The medical literature now abounds with papers demonstrating quite the opposite; that the co-administration of an antioxidant along with a cytotoxic drug decreases side effects and increases the effectiveness of the cytotoxic drug in vivo9,10. Once again we acknowledge that Chen et al. have mentioned that Glutathione is not uncommonly administered at the same time as platinum based cytotoxic drugs (pro-oxidant) where it has been demonstrated that the Glutathione (anti-oxidant) does not interfere with their activity and decreases their side effects. The purpose of the Chen paper was to see if this pro-oxidant (Vitamin C) and anti-oxidant (Glutathione) combination was equally valid. We repeat that a massive amount of Glutathione
(48 grams equiv to a 60kg person) was given to the athymic mice to achieve the Glutathione interference – other (not measured) physiological effects could well have occurred from such a massive amount unrelated to the ‘apparent’ anti-oxidant interference of Glutathione. Such levels of Glutathione (48g) have never before been documented or infused by doctors practicing nutritional medicine nor have they been used or documented in combination with platinum based cytotoxic drugs.
10. The etiology of cancer, and almost certainly the propagation of metastases, involves oxidative stress. There is much evidence to support the use of antioxidants to slow cancer progress and to prevent its propagation13,14,15,20.
11. Finally, like Vitamin C, if the right concentration of Glutathione can be found, it has been shown that even Glutathione can be cytotoxic and can produce hydrogen peroxide around cancer cells16,17. Alpha lipoic acid has also been found to be very useful in increasing the cytotoxic effect of chemotherapeutics whilst decreasing the side effects18. Additionally, alpha lipoic acid has been found to dramatically increase the cytotoxic effect of high-dose Vitamin C7.
Further observations on the Chen paper include the use of athymic mice, presumably on the basis that immune stimulation by the high-dose Vitamin C was being excluded. For what reason? Surely in humans we are not going to remove the thymus gland before we administer high-dose intravenous Vitamin C and Glutathione. Probably, there is an attempt to continue to postulate that the only way high-dose Vitamin C works is by stimulation of hydrogen peroxide production and that Glutathione will inhibit this action; well, who knows what effect the Glutathione would have if there was still an intact thymus gland – the case in most humans. It is abundantly clear from the medical and scientific literature that high-dose intravenous Vitamin C works in multiple ways, some of which are described by Frei2.
It is a misperception that megadose intravenous Vitamin C is acting as a pro-oxidant – it is quite the reverse. InjectableVitamin C is a reducing agent – it donates electrons; the oxidized form of Vitamin C, dehydroascorbate (its redox pair), accepts electrons and, of course, is an oxidizing agent.
continued next page

10
ACNEM Journal Vol 31 No 1 – March 2012
In the claim that the ‘pro-oxidant’ Vitamin C produces hydrogen peroxide, ascorbate would be accepting electrons. This is contrary to the proposed mechanism of how megadose Vitamin C works in cancer treatment. Adding dehydroascorbate to tissue culture (the oxidized form of ascorbate) does not result in the formation of hydrogen peroxide – the reduced form of ascorbate is required for hydrogen peroxide production.
Chen and Levine et al.1 propose that ascorbate donates an electron (reduction) to a metal ion, the identity of which is still to be determined but may be cupric (Cu++) or ferric (Fe+++), to produce cuprous (Cu+) or ferrous (Fe++). It is the oxidizing molecule of cuprous or ferrous which then potentially interacts with oxygen to produce superoxide O2
-, which in turn dismutates to produce hydrogen peroxide. Ascorbate does not directly produce hydrogen peroxide; in fact, ascorbate is a great scavenger of free radicals such as superoxide, so the concept of high doses of Vitamin C directly producing large amounts of superoxide free radical is contradictory. The addition of dehydroascorbate (the oxidized form of Vitamin C) by definition, according to the scheme outlined by Chen and Levine, would not result in the formation of hydrogen peroxide. So, if we follow Chen and Levine’s discourse1, Vitamin C acts as a reducing agent to indirectly produce hydrogen peroxide – this still suggests that in this instance Vitamin C is not directly pro-oxidant but is acting as a reducing agent, albeit with an ultimate oxidative effect.
Further indirect confirmation of the requirement for Vitamin C to be in the reduced form has recently been published by Heaney et al.21. They demonstrated that the in vitro addition of dehydroascorbate to myeloid leukemia and lymphoma cell lines inhibited the cytotoxic action of anti-cancer drugs rather than increasing their potency; a similar inhibitory effect on anti-cancer drugs occurred when dehydroascorbate was administered to mice with cancer xenografts. In general an increased cytotoxic action of anti-cancer drugs is observed when ascorbate (not dehydroascorbate) is used at the same time as anti-cancer drugs22,23,24,25,26. These papers add further confirmation to the importance of the anti-oxidant effect of megadose Vitamin C in cancer treatment adding a further conundrum to the pivotal points of Chen’s paper – that it is the anti-oxidant effect of glutathione which is interfering with the claimed pro-oxidant effect of the infused megadose Vitamin C.
Whatever the mechanism, high doses of the reduced form of Vitamin C appear to be involved with the production of significant amounts of hydrogen peroxide that have a pro-oxidant effect against cancer cells. Unfortunately, it has become axiomatic that this is how high-dose Vitamin C works in cancer treatment. There are undoubtedly many mechanisms by which high dose Vitamin C works2.
Whatever the ultimate mechanism of action against cancer cells, in vitro and in vivo, it involves cancer cell death. In vivo there are probably mechanisms, such as generalized immune stimulation, inhibition of angiogenesis, hyaluronidase inhibition, collagen growth (to contain tumors), that are not easily quantified in vitro. Researchers in the Vitamin C and cancer field have succumbed to the temptation to apply the orthodox reductionist singularity approach of hydrogen peroxide production being the only
mechanism by which high-dose Vitamin C works against cancer cells – most unfortunate, as so much excellent research is not being properly pursued and debated.
To date, cancer trials using high-dose Vitamin C have had mixed outcomes. Pauling and Cameron reported an increase in length and quality of life using just 10 grams of intravenous Vitamin C in patients whose immune systems had not been compromised by long-term cytotoxic therapy3. Although there are occasional successful case history studies of the use of intravenous Vitamin C in cancer19, more recently a Phase 1 clinical trial by Hoffer and Levine et al.4 did not find remarkable results using doses of Vitamin C as high as 100g. However, on careful reading of the Hoffer and Levine paper, for 2 out of the 24 patients their cancers became stable. Additionally, cancer patients who received intravenous Vitamin C at levels ≥ 0.6g/kg maintained their quality of life compared with patients who received a lower dose. All of these cancer patients were phase 4 and had exhausted other treatment methods, including surgery, radiotherapy and chemotherapy (compared with the patients described above by Pauling and Cameron3). This illustrates that there are many complicating factors involved in high-dose Vitamin C therapy above and beyond the apparent measured in vitro cytotoxic effects. Not the least of these is the overall systemic oxidative stress that cancer patients are under, including widespread inflammation, SIRS (systemic inflammatory response syndrome) and the sepsis that often accompanies terminal cancer patients5. Cancer patients are often malnourished, cachectic and immune-overloaded/depleted, which can be caused by the cancer, associated disease or the treatment, or all of the aforementioned. Every one of these areas needs to be addressed.
Although it is tempting to use a singular approach in cancer treatment, this is fundamentally ‘shortchanging’ the patient in terms of their requirements to best deal with their cancer. Of course, the aim should be to remove any rapidly growing and/or life-threatening cancer tissue, to use appropriate and preferably targeted cytotoxic/radio therapies as required (which can include high dose intravenous Vitamin C and other appropriate nutraceuticals administered in combination or separately as indicated), maximize the patient’s immune function, their nutritional status and their energy levels, diminish their toxic load (which may be contributing to their oxidative stress) and their depleted immune status, and to address their social and spiritual issues.
It has always been of interest that animals that are used to validate the effect of a known dose of Vitamin C manufacture their own Vitamin C – indeed mice were used that manufacture up to an equivalent of 17 grams per day based on a 60 kg human body weight. Of course, Glutathione is also manufactured by most mouse tissues, and tumor cells also manufacture abundant amounts of Glutathione. Without accounting for the Vitamin C and Glutathione levels in/around the mouse tumor before and after the administration of extra levels, it is not the easiest task to evaluate the real effect of loading extra Vitamin C and Glutathione. Also, how is this relevant to what happens in the human body, which starts off with very low levels of Vitamin C and unknown levels of glutathione in/around the tumor tissue?
In conclusion, the use of collateral antioxidants in the treatment of cancer has both clinical and scientific support. The Chen et al.
from page 9

11
ACNEM Journal Vol 31 No 1 – March 2012
experiment needs to be repeated to give more clinically meaningful results; to include physiologically relevant levels of the intervention drugs and treatment continued until survival or natural death for all animals in the cohorts. There may also be a distinct advantage to use animals that don’t make their own Vitamin C and have an intact thymus and coupled with more appropriate levels of Glutathione may result in different outcomes.
Until there is conclusive evidence against the simultaneous use of Glutathione and Vitamin C, it would not seem imprudent to continue such a protocol. It remains to be firmly established what is the best combination of antioxidants and other nutraceuticals (including Vitamin K3, Vitamin D3 and Selenium) for long-term survival and for use with orthodox cytotoxic therapy to increase its efficacy and decrease side effects. If at any stage it is clearly demonstrated that one or two grams of Glutathione and megadose Vitamin C (commonly 15g up to 100g) should not be administered at the same time, then naturally practitioners should cease this practice.
Author for contact: [email protected] Australasian College of Medical Nutrition, Braeside, 3195 Australia. www.nutritioncollege.org
Disclosure: The authors are associated with a company which manufactures Vitamin C for injection.
References:
1. Chen Q, Espey MG, Sun AY, Lee JH, Krishna MC, Shacter E, Choyke PL, Pooput C, Kirk KL, Buettner GR, Levine M. ‘Ascorbate in pharmacologic concentrations selectively generates ascorbate radical and hydrogen peroxide in extracellular fluid in vivo.’ Proc Natl Acad Sci USA. 2007 May 14.
2. Frei B, Lawson S. ‘Vitamin C and cancer revisited.’ Proc Natl Acad Sci USA. 2008 Aug 12;105(32):11037-8. Epub 2008 Aug 5.
3. Cameron E, Pauling L. ‘Supplemental ascorbate in the supportive treatment of cancer: Prolongation of survival times in terminal human cancer.’ Proc Natl Acad Sci USA. 1976 Oct;73(10):3685-9.
4. Hoffer LJ, Levine M, Assouline S, Melnychuk D, Padayatty SJ, Rosadiuk K, Rousseau C, Robitaille L, Miller WH Jr. ‘Phase I clinical trial of i.v. ascorbic acid in advanced malignancy.’ Ann Oncol. 2008 Jul 25.
5. Thomas E Ichim , Ron Hunninghake, Neil H Riordan et al. ‘Intravenous ascorbic acid to prevent and treat cancer-associated sepsis?’ Journal of Translational Medicine 2011, 9:25 doi:10.1186/1479-5876-9-25.
6. Ping Chen, Jennifer Stone, Garrett Sullivan, Jeanne A. Drisko, Qi Chen. ‘Anti-cancer effect of pharmacologic ascorbate and its interaction with supplementary parenteral glutathione in preclinical cancer models.’ Free Radical Biology & Medicine 51 (2011) 681–687.
7. JJ Casciari1, NH Riordan1, TL Schmidt1, XL Meng1, JA Jackson and HD Riordan. ‘Cytotoxicity of ascorbate, lipoic acid, and other antioxidants in hollow fibre in vitro tumours.’ British Journal of Cancer (2001) 84(11), 1544–1550.
8. Qi Chen, Michael Graham Espey, Andrew Y. Sun, Chaya Pooput, Kenneth L. Kirk, Murali C. Krishna, Deena Beneda Khosh, Jeanne Drisko and Mark Levine. ‘Pharmacologic doses of ascorbate act as a prooxidant and decrease growth of aggressive tumor xenografts in mice.’ PNAS August 12, 2008, vol. 105 no. 32, 11105–11109.
9. Stefano Cascinu, Vincenzo Catalano, Luigi Cordella, Roberto Labianca, Paolo Giordani, Anna Maria Baldelli, Giordano D Beretta, Emilio Ubiali, and Giuseppina Catalano. ‘Neuroprotective Effect of Reduced Glutathione on Oxaliplatin-Based Chemotherapy in Advanced Colorectal Cancer: A Randomized, Double-Blind, Placebo-Controlled Trial.’ J Clin Oncol 20:3478-3483. 2002.
10. Silvia Böhm, Saro Oriana, Gianbattista Spatti, Francesco Di Re, Gianluigi Breasciani, Carlo Pirovano, Ilaria Grosso, Cinzia Martini, Augusto Caraceni, Silvana Pilotti and Franco Zunino. ‘Dose Intensification of Platinum Compounds with Glutathione Protection as Induction Chemotherapy for Advanced Ovarian Carcinoma.’ Oncology 1999;57:115–120.
11. Dorota Ścibior, Michał Skrzycki, Małgorzata Podsiad, Hanna Czeczot. ‘Glutathione level and glutathione-dependent enzyme activities in blood serum of patients with gastrointestinal tract tumors.’ Clinical Biochemistry 41 (2008) 852–858.
12. JF Smyth, A Bowman, T Perren, P Wilkinson, RJ Prescott, KJ Quinn & M Tedeschi. ‘Glutathione reduces the toxicity and improves quality of life of women diagnosed with ovarian cancer treated with cisplatin: Results of a doubleblind, randomised trial.’ Annals of Oncology 8: 569-573, 1997.
13. Ewa Wybieralska, Monika Koza, Jolanta Sroka, Jarosław Czyż And Zbigniew Madeja. ‘Ascorbic Acid Inhibits the Migration of Walker 256 Carcinosarcoma Cells.’ Cellular & Molecular Biology Letters Volume 13 (2008) pp 103-111.
14. Mikirova N, Jackson J, Riordan N. ‘The Effect of High Dose IV Vitamin C on Plasma Antioxidant Capacity and Level of Oxidative Stress in Cancer Patients and Healthy Subjects.’ Orthomolecular Medicine, 2007, 22(3):153-160.
15. M Valko, CJ Rhodes, J Moncola, M. Izakovic, M. Mazura. ‘Free radicals, metals and antioxidants in oxidative stress-induced cancer.’ Chemico-Biological Interactions 160 (2006) 1–40
16. Paola Perego, Laura Gatti, Nives Carenini, Laura Dal Bo and Franco Zunino. ‘Apoptosis Induced by Extracellular Glutathione is Mediated by H2O2 Production and DNA Damage.’ Int. J. Cancer: 87, 343–348 (2000).
17. Barbara Donnerstag, Gerhard Ohlenschlogera, Jindrich Cinatlb, Michael Amrania, Dieter Hofmann, Sven Flindt, Gemot Treusch, Lothar Trlgera. ‘Reduced glutathione and S-acetylglutathione as selective apoptosis-inducing agents in cancer therapy.’ Cancer Letters 110 (1996) 63-70.
18. L Novotny1, P Rauko, C Cojocel. ‘Alpha α-Lipoic acid – the potential for use in cancer therapy.’ Minireview Neoplasma 55, 2, 2008 81.
19. Jeanne A Drisko, MD, Julia Chapman, MD and Verda J Hunter, MD. ‘The Use of Antioxidants with First-Line Chemotherapy in Two Cases of Ovarian Cancer.’ Journal of the American College of Nutrition, Vol. 22, No. 2, 118–123 (2003).
20. Masaki Shiota, Akira Yokomizo, Seiji Naito. ‘Oxidative stress and androgen receptor signaling in the development and progression of castration-resistant prostate cancer ’ Free Radical Biology & Medicine 51 (2011) 1320–1328.
21. Mark L. Heaney, Jeffrey R. Gardner, Nicos Karasavvas, David W. Golde, David A. Scheinberg, Emily A. Smith, and Owen A. O’Connor. ‘Vitamin C Antagonizes the Cytotoxic Effects of Antineoplastic Drugs’ Cancer Res 2008;68(19):8031–8.
22. Kurbacher CM, Wagner U, Kolster B, Andreotti PE, Krebs D, Bruckner HW. ‘Ascorbic acid (vitamin C) improves the antineoplastic activity of doxorubicin, cisplatin, and paclitaxel in human breast carcinoma cells in vitro.’ Cancer Lett. 1996 Jun 5;103(2):183-9.
23. Frömberg A, Gutsch D, Schulze D, Vollbracht C, Weiss G, Czubayko F, Aigner A. ‘Ascorbate exerts anti-proliferative effects through cell cycle inhibition and sensitizes tumor cells towards cytostatic drugs.’ Cancer Chemother Pharmacol. (2011) 67: 1157-1166.
24. Prasad SB, Rosangkima G, Nicol BM. ‘Cyclophosphamide and ascorbic acid-mediated ultrastructural and biochemical changes in Dalton’s lymphoma cells in vivo.’ Eur J Pharmacol. 2010 Oct 25;645(1-3):47-54.
25. Qazilbash MH, Saliba RM, Nieto Y, Parikh G, Pelosini M, Khan FB, Jones RB, Hosing C, Mendoza F, Weber DM, Wang M, Popat U, Alousi A, Anderlini P, Champlin RE, Giralt S. ‘Arsenic trioxide with ascorbic acid and high-dose melphalan: results of a phase II randomized trial.’ Biol Blood Marrow Transplant. 2008 Dec;14(12):1401-7.
26. Michael Graham Espey, Ping Chen, Brian Chalmers, Jeanne Drisko, Andrew Y. Sun, Mark Levine, Qi Chen. ‘Pharmacologic ascorbate synergizes with gemcitabine in preclinical models of pancreatic cancer.’ Free Radical Biology & Medicine 50 (2011) 1610–1619.
12
ACNEM Journal Vol 31 No 1 – March 2012
introduction
Decisions about good and bad foods, or healthy vs unhealthy diets, are often based on little objective information. This is often not aided by nutritional research, which isolates nutrients or food components from whole foods.
The discovery of a low-grade, chronic and systemic form of inflammation however (‘metaflammation’1), which has been found to be common to many chronic diseases, has changed this by offering relatively simple post-prandial blood tests of pro or anti-inflammatory inducers.
‘Metaflammation’ is a type of metabolically induced inflammation. It was discovered in the early 1990s and was originally thought to be caused by obesity2, hence possibly explaining the link between obesity and chronic disease.
Metaflammation differs from the classical form of inflammation associated with microbial infection and injury in that;
1. It is low grade and often only 3-4 fold normal, compared with ~100-fold in classical inflammation,
2. It is not localised but exists throughout the arteries and organs of the body,
3. It is chronic and appears to be associated with many forms of chronic disease and,
4. It has a lifestyle or environmental cause in contrast to microbial ‘antigen’3.
Determining an anti-inflammatory diet based on post-prandial research findingsProf Garry Egger, BA(Hons), MPH, PhD
● Breast milk● Eggs● MUFA meat● Fish● Fibre● Low EI/EE ratio● Activity● Fruit/Veg● Nuts/seeds/soy● Low N6/NS ratio
● animal milk
● Alcohol (moderate)● wine● Vinegar
● Olive oil● Cocoa
● Tea● Herbs/spices
● Mediterranean diet
● alcohol (excessive)● Co�ee
● Smoking● Fructose● SAFA meats● High EI/EE radio● Inactivity● Sleep deprivation
● Chronic stress● High N6/N3● “Fast foods”
● Obesity● Over-activity
Pro-
In�a
mm
ator
y
Ant
i-In�
amm
ator
y or
Neu
tral
TIMELINE
Pre-NeolithicNeolithicRevolution
AgrarianRevolution
IndustrialRevolution
GreenRevolution
10,000 BP 1,000 BP 200 BP 50BP Present
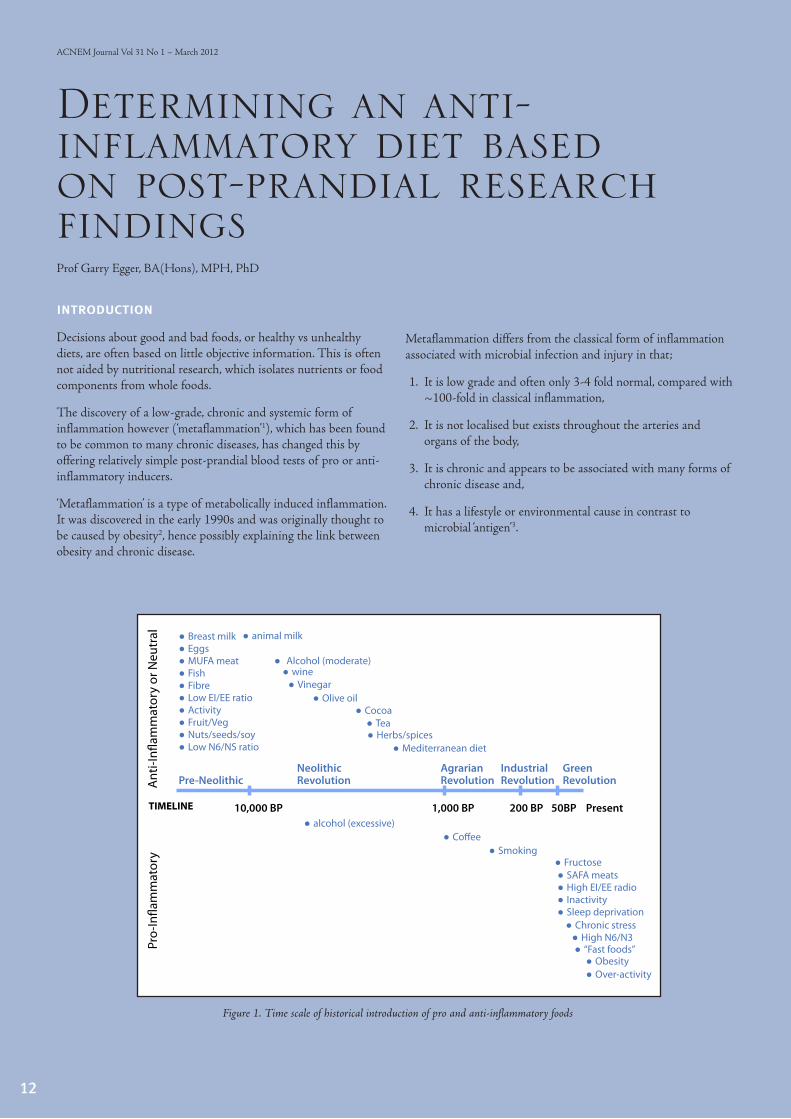
Figure 1. Time scale of historical introduction of pro and anti-inflammatory foods
13
ACNEM Journal Vol 31 No 1 – March 2012
Research over the past decade has allowed the accumulation of data categorising foods that are distinctly anti, or pro-inflammatory. Pro-inflammatory cytokines include the commonly known C-Reactive Protein (CRP) as well as less well known interlekins (Il-6; IL-10), TNF alpha, NFkB and many others. Anti-inflammatory indicators include adiponectin and HDL in particular4.
Blood assays can be taken before eating a particular type of meal and hourly or half hourly (depending on the research funding) for up to four hours after. And while these are acute measures, there is evidence to suggest that acute measures can be an indication of chronic inflammatory effects, with a potential link to a range of chronic diseases. Obviously not all good or bad foods can be determined on this one continuum. However the data available to date, is generally consistent with other nutritional measures of health.
food types and ‘metaflammation’
In a study completed at Sydney University and since published in the British Journal of Nutrition5, post-prandial bloods were compared within a small group of subjects after eating kangaroo (an ‘old’ form of low-fat meat) one week, alternated with wagyu beef (a ‘newer’ form of hybridised, but high fat meat) the next. There was little effect of the kangaroo, but blood levels of inflammatory markers rose significantly after the wagyu and stayed up for two hours.
The suggestion is that this is a result of an immune reaction to a form of fat (saturated) in the wagyu, with which humans have not evolved, thus causing an immune reaction, albeit lower grade than to standard pathogens.
From an analysis of research carried out over the last decade, we have been able to put together a list of specific foods that have been shown to have a pro- or anti-inflammatory reaction (or neutral in the case where an equivalent type of food is pro-inflammatory). This is shown in Table 1. While not labelling all foods, this gives an indication of the underlying factor(s)
continued next page
ANTI-INFLAMMATORY (OR NEUTRAL)
PRO-INFLAMMATORY
Generic Specific Category Foods/drinks
Alcohol (moderate)Red wine; white wine;
beer; non-alcoholic beerAlcohol (excessive)
High total intake;
Bingeing
Bulbs/roots Garlic; ginger; onions
Cocoa Dark chocolate
Dietary patterns
Low N6:N3 ratio;
Mediterranean;
polymeal; portfolio;
vegan
Dietary patterns
‘Fast foods; High
N6:N3 ratio; ‘Western’
style; High GI Load;
High fat diet; ‘cafeteria’
diet
Dressings/condiments Olive oil; vinegar
Eggs
Energy intake (total) RestrictedEnergy intake
(excessive)
Acute; chronic high
intake
Fat MUFA; some PUFA Fat Saturated; trans fats
Fibre (high intake) Fruits; vegetables; lignan GlucoseHigh GI (mainly
processed) foods;
Fruit
Greater variety (not
quantity); apples;
berries; bilberries;
blueberries; camu
camu (tropical fruit);
cherries; cranberries;
grapes; raisins;
raspberries strawberries
Pomegranate
Fruit juices
Apple; blackcurrent;
orange; pomegranate;
red grape
GrainsCereals; flaxeed flour;
wholegrain
Meat (neutral)Lean game meats;
kangarooMeat
Domesticated beef;
wagyu
MilkBreast milk; wild
animal; A2; soyStarvation Fasting
Nuts & Seeds
Almonds; hazelnuts;
macadamia; mixed nuts;
pistachio; walnuts
Sweetened drinksSugar/fructose
sweetened
SeafoodFish (salmon); Farmed
fish-fed fishRefined carbo-hydrates
Soy Beans; tofu; milk
Supplements
Black raspberry extract;
black current extract;
fish oil; garlic powder;
grape seed/skin/power
extract; Omega 3;
plant sterols; psyllium;
strawberry extract;
walnut extract
Tea Green; black
Vegetables Legumes; tomatoes
Veg. juices Beetroot; carrot; tomato
Table 1. Pro and anti-inflammatory foods and food categories based on published research

that may have such an effect.
A look at the historical timeline (Figure 1) for the introduction of pro and anti-inflammatory foods (and other environmental, and social stimuli jointly called ‘anthropogens’*) shows a clear distinction between pre- and post-industrial revolution stimuli. Those with evidence of anti-inflammatory action have generally been around for hundreds, or thousands of years, thus allowing the human immune system to develop a familiarity with them and no inflammatory reaction. Newly introduced foods on the other hand, or food-related products, often produce a pro-inflammatory postprandial response, suggesting a similar response (albeit lower grade) as that to a microbial pathogen or injury. A term that has been proposed to differentiate between these modern day stimulants and classical microbial ‘antigens’ is ‘inducers’ of metaflammation6.
Table 1 shows a listing of pro and anti-inflammatory foods identified in the literature, for which there is existing evidence. Figure 1 gives an idea of the historical context of the introduction of both types of foods into the human environment.
* Defined here as: “man-made environments, their bi-products, and lifestyles encouraged by those environments, some of which may be detrimental to human health”.
conclusion
There is a current shift in nutrition research from the specific effects of isolated nutrients in food to whole foods and whole meal patterns. The development of post-prandial measures of metaflammation has facilitated this and allowed the development of a portfolio of anti and pro inflammatory foods, which can be used often or sparingly by someone hoping to achieve a healthy nutritional intake without ‘going on a diet’. Many of these are shown in Table 1, although it should be recognised that the specific foods listed here are those for which there is currently available evidence of a pro or anti-inflammatory post-prandial response. It is most likely that the general categories
shown in Table 1, would reflect the same outcomes of the specific foods, thus widening the options for developing an ‘anti-inflammatory’ diet.
It’s not coincidental that all of the anti-inflammatory foods referred to in Table 1 have also generally been shown to assist weight loss, cardiovascular health and a range of other chronic disease problems, the effects on which are likely to be proportional to the degree to which these are utilised. A selection of foods based around these categories would be most likely to have a generally healthy effect, providing a healthy alternative to the current modern-type western eating plan.
summary of key points
• Low-level, systemic inflammation (also called ‘metaflammation’, para-flammation’, ‘smouldering inflammation’, or ‘homeostatic inflammation’) underlies many, if not most, chronic, lifestyle-related diseases (viz. CHD, Type 2 diabetes, many forms of cancer, PCOS, Alzheimer’s, Dementia, Depression, etc).
• Metaflammation is to chronic disease what classical inflammation is to infectious disease or injury.
• Modern nutrition is a significant ‘inducer’ (although not the only one) amongst a number of ‘anthropogens’ associated with ‘metaflammation’, and hence possibly much chronic disease is induced through this process.
References:
1. Hotamisligil GS. Inflammation and metabolic disease. Nature 2006;444:860-7.
2. Hotamisligil, GS, Shargill, NS.Spiegelman, BM. Adipose expression of tumor necrosis factor-alpha: direct role in obesity-linked insulin resistance. Science 1993;259:87-91.
3. Egger G, Swinburn B. Planet obesity: How we are eating ourselves and the planet to death. Allen and Unwin, Sydney, 2010.
4. Tilg H, Moschen AR. Inflammatory mechanisms in the regulation of insulin resistance. Mol Med 2008; 14: 222–231.
5. Arya F, Egger S, Colquhoun D, Sullivan D, Pal S, Egger G. Differences in post-prandial inflammatory responses to a ‘modern’ vs a traditional meat meal:A preliminary study. Br J Nutr 2010, 104:724-728.
6. Medzhitov R. Origin and physiological roles of inflammation. Nature 2008; 454: 428–435.
14
ACNEM Journal Vol 31 No 1 – March 2012
from page 13
15
ACNEM Journal Vol 31 No 1 – March 2012
the acnem primary course
The ACNEM Primary Course is a 4-day post-graduate training program for doctors and other healthcare professionals in Nutritional and Environmental Medicine (NEM). Course content is evidence-based, well-referenced and constantly updated. Apart from better understanding the nutritional biochemistry underlying disease and illness, and therefore for prevention and optimal health, the lectures and discussion sessions address symptoms and conditions commonly seen in primary care. Content and delivery is focused on clinical application, always with an emphasis on ‘how to’ in practice.
acnem online learning
The Primary Course has historically been delivered face-to-face at venues around Australia and New Zealand. However, in July 2010 an entirely online version of the Primary Course was launched, using the latest internet technology to allow participants to watch the lectures on their computer exactly as they were filmed at a recent course, synchronised with the lecturer’s Powerpoint presentation. Added to this were discussion forums, Powerpoint slide notes, lecture handouts, references and pre and post-reading and activities.
Despite the obvious benefits of face-to-face learning, we have been gratified by
hundreds of online learning enrolments, and high participant satisfaction with the ACNEM online learning experience. Numerous participants have cited the ability to watch the lectures in their ‘spare time’, along with the ability to pause and replay lectures for better note-taking and understanding, as being of real benefit. Others have reported re-watching lectures a number of times, or have benefited from presenting case histories to other doctors in the closed discussion forums.
Distance learning, of course addresses issues of accessibility, flexibility, cost-effectiveness and asynchronous time zones. Currently, there are practitioners enrolled from all over Australia, New Zealand, South East Asia and even the UK and USA. However there are drawbacks, especially as this form of learning requires motivation and discipline; to find the time to watch the lectures and to fully participate in the online activities. To assist with this, there are a raft of improvements being developed, all designed to enhance engagement and the experience of online learning, along with online assessment to further establish the extent to which the learning objectives have been met.
As you might expect, filming of fresh content is constantly taking place at face-to-face courses. A somewhat unexpected benefit of creating this online repository for Primary Course content is that each time a new lecture topic is filmed, or an existing topic is delivered by a different lecturer, subject to suitability and post-
production (a lengthy process), additional content is added to the online version of the course, resulting in over 40 hours of lectures online (currently) compared to 30 hours in the 4-day face-to-face course. This has required us to identify ‘core’ and ‘additional’ content, and as the lecture-base continues to grow, some of this additional content will become a separate course specifically designed to extend the initial knowledge base established in the Primary Course.
ACNEM Online Learning: Behind the interface
continued next page

16
ACNEM Journal Vol 31 No 1 – March 2012
16
acnem special training programs
Following the success of the online Primary Course, a number of shorter courses (equivalent to 1 or 2 days face-to-face) historically known as ‘Special Training Programs’ within ACNEM circles, have been launched in the same online format. These are also designed to extend Primary Course knowledge and understanding, through a more in-depth investigation of NEM approaches in specific systems. These include:
• Nature or Nurture? - Epigenetics & Nutrigenomics
• The GUT - including Gut Dysbiosis and Permeability
• Tired or Wired - Thyroid & Adrenal Conditions
And, for doctors and nurses only:
• Injectable Nutrients
• Heavy Metal Detoxification with optional Certification (pre-requisite: Injectable Nutrients)
feedback from online learning participants
Finally, whether face-to-face or online, one theme is common in the written feedback forms of all Primary Course participants; “I can’t believe we weren’t taught this before.” This is both inspiring in terms of enhancing the future clinical practice of participants, but also sobering. In the words of a recently retired GP at a recent face-to-face Primary Course, “I feel somehow cheated to have just completed my career without this knowledge.” Feedback commonly expresses frustration at working within a disease-management, short-consultation, pharmaceutical-driven system, while lifestyle and likely toxin-related illness and disease reach epidemic proportions. On a more positive note, feedback also commonly expresses renewed hope and excitement for practice, looking forward to better patient outcomes with a new ‘doctor’s bag’ of enhanced understanding and clinical tools.
pre-disposing and reflective activities
Clearly ACNEM’s mission is to make Nutritional and Environment Medicine available to all healthcare practitioners, and specifically through the medical undergraduate curriculum and during registrar training. It is with this in mind that we present the Pre-disposing and Reflective Activities of a GP registrar who recently completed the online Primary Course and who kindly agreed to allow publication of his reflections. To explain, all participants, whether face-to-face or online, are required to complete these ‘before’ and ‘after’ activities as part of the course requirements along with specific pre and post-reading.
The ACNEM Online Learning Team and Teaching Faculty
from page 15
17
ACNEM Journal Vol 31 No 1 – March 2012
Unfortunately my clinical experience is limited so I’m reluctant to offer a case history. However, the reading from Good Health in the 21st Century provided much food for thought and plenty for me to reflect upon prior to engaging in this course.
Firstly, having worked for about one year as a general practice trainee, I reflect that the patients I think about after a day’s work are the ones that keep on coming back with the same complaints and I feel resigned to thinking that I can’t really offer them much help. They have seen numerous specialists. They have had counselling. They have tried all kinds of diets. Many simply want a repeat of their antidepressant or pain medication, lacking confidence that anyone in the medical profession could really understand their struggle.
I think of one patient JA, for example, a long-term smoker with COPD and a host of other medical problems, with depression that failed to respond to ECT and home visits by a psychologist. And I can’t help but recollect that I never really asked about his diet in any detail, and his mouth contained a sea of amalgam fillings. Notwithstanding the tremendous good work that is done for many patients with chronic illness, patients such as JA beg the question; are we missing something? Could we inadvertently be reinforcing a state of learned helplessness in many patients? Perhaps, I think, NEM will help fill this gap.
Secondly, my experiences as a junior doctor, and also my own periods of ill health, have caused me to rethink my whole philosophy about health in general. Historically, it seems there was a point when modern medicine could have evolved in either of two directions. Through the work of Virchow and others, incredible insights were being gained into what makes cells healthy, while at the same time the disease management model gained widespread support with the work of Alexander Fleming and the ‘discovery’ of good hygiene. To translate these discoveries to the doctor’s clinic and hospitals, it seems we favoured the disease/germ model and this has carried over to almost every area of health care. It worked so well, and the Randomised Controlled Trials (RCTs) proved this to us.
But then, bam... depression, diabetes, heart disease, syndrome X, cancer, ADHD... all emerging as the new plague of the modern era. Yes, public health campaigns are out there; immunisations, screening for breast & colon cancer etc. But sadly they seem to miss the point that our overarching model for health care fails to support health at a grassroots level, but rather exists to diagnose and treat illness and disease.
The idea that the body is designed to win if we care and nourish it in the right way; with careful attention to vitamins and minerals that may be in short supply, a diet which provides all the raw materials we need, and avoids harmful toxins such as industrial chemicals and heavy metals, first came as a revelation to me. I used to think that if the baseline blood tests were all
‘normal’ and alarm symptoms were absent, ill health was all in the mind and cognitive therapy, along with exercise and a low-fat diet, could fix just about anything. Yet now after a few years of clinical experience, I reflect how naïve this view was - a bit like trying to grow a tree in soil that is hopelessly infertile, with only minimal rain and sunlight, relying on powerful fertilizers and pesticides to make it grow - while ignoring the delicate web of life surrounding it.
How the mind-body link works and the dynamic dance between nature and nurture are still big mysteries to me. Yet when it comes to understanding the deeper causes of chronic disease, I look forward with enthusiasm and humility to embracing what this course has to offer. I know the science is there, and I look forward to seeing how we can apply this to changing patients’ lives.
Adrian Hekel, BSc (Hons), BMBS, (GP Registrar)
online primary course: pre-disposing activity
After completing the pre-reading, please write a short case history (please ensure no identifying patient information is included) or an exploratory piece (500 words) based on any of your previous knowledge, experience or practice of nutritional and environmental medicine in relation to one or more of the learning objectives. Please post this in the online forum for review by the course coordinator and discussion by other participants.
continued next page

18
ACNEM Journal Vol 31 No 1 – March 2012
The ACNEM Primary Course has certainly met all my expectations, and has left a considerable impact on my views on medical practice, along with plans to establish my own ‘integrative practice’ sometime in the future. As someone whose knowledge about diet and environmental triggers for illness and disease was woefully lacking, I am very grateful to have been able to fill some of those gaps. It has been a steep learning curve for me (having been through a period of ill health which got me interested in the NEM approach on quite a personal level!), but also a very enjoyable and rewarding one. I will now reflect on three main points which have emerged from the course, and also in response to the post-course reading. After this I will comment on the case of Mr JA that I introduced in the Pre-disposing Activity.
1. the nem approach can seem complicated and time-consuming
But I feel that patients deserve this level of health care. In medical school we were introduced in the first week to the standard method of taking medical histories: history of presenting complaint, past history, medications, smoking, allergies, alcohol & other drugs, family history, review of systems and social history, with a few extras thrown in for a psychiatric assessment. This was supposed to give us 90% of the information we needed to formulate a working diagnosis, and we would confirm this with a physical exam and diagnostic tests. Then when I began GP training I was introduced to Murtagh’s brilliant framework: Is it common? Is it serious? Is it one of the fourteen masquerading illnesses? Or is the patient trying to tell me something else1?
Since commencing this ACNEM course, my understanding of ‘diagnosis’ has once again been turned upside-down. Although on the surface, the NEM diagnostic approach seems much more complicated than what I am used to, after some reflection I feel it is considerably more practical. At first I thought I’d have to add another column to my list of masqueraders; coeliac disease, under-methylation, magnesium and zinc deficiency, food intolerance, inadequate protein and fatty acid intake, heavy metal toxicity, hypochlorhydra, gut dysbiosis etc. Then I realised I was missing the point, as I would have to alter how I thought about diagnosis much more radically... based on interlinked systems and mechanisms, which give rise to disease when one or more components are out of balance (making the actual name of the illness/disease much less important).
To borrow the framework used in ‘functional medicine’ (the US
counterpart to NEM2), I would now try to consider:
1. Is nutrition optimal (especially intake of good fats, amino acids and nutrient-rich foods)?
2. Is immune imbalance and inflammation an issue (caused by food allergens, poor diet, chronic infections, etc.)?
3. Is hormone and neuro-endocrine function optimal (including thyroid, cortisol, insulin and sex hormones)?
4. Is digestion functioning well?
5. What is impeding the body’s detoxification systems?
6. Is energy metabolism functioning well or is it hindered by oxidative stress?
7. Are stress or poor lifestyle habits of concern?
Based on these mechanisms, we can ask about antecedents for a patient’s current presentation (e.g. did they ever have a history of dairy intolerance or symptoms which may represent an ‘allergic march’3?), or the nature of any food cravings - indicating hyperinsulanaemia or other sensitivities and deficiencies4,5). We can then explore immediate triggers, such as whether a patient’s symptoms coincide with exposure to a specific chemical, or particular life events or lifestyle changes such as staying indoors with a new job6. Then we are in a position to formulate a treatment plan based on one or several of these mediators, rather than act in a reflex manner to treat a specific ‘fixed name disease’7.
As far as treatment goes, I found Dr Karel Hromek’s analogy of a ‘ship with anchors’ particularly helpful (with allergies, food intolerances, chronic infections, heavy metals, etc, all adding up to lower a patient’s sensitivity threshold8). I look forward to developing treatment regimes that embrace these principles and to using the quality hand-outs on topics such as elimination diets and allergen management, as presented in this course. I would now also consider recommending to patients a good cookbook and perhaps a personalised ‘treatment plan’ handout to help ensure that they have access to correct information, and take responsibility for their own health; more as a ‘student of health’ rather than a patient waiting to be ‘fixed’.
Yes, this diagnostic and treatment approach may be more time consuming, but in the long run I feel it may be much quicker in leading to answers (or at least a workable treatment framework) and therefore more beneficial for most patients affected by
online primary course: reflective activity
After completing the post-reading, please review your pre-disposing activity case history or exploratory piece in view of what you have learned during the learning activity and write a reflective piece (1000-1500 words) indicating how this has influenced your understanding of nutritional and environmental medicine, in relation to one or more of the learning objectives above, with particular reference to any additional guidelines, management and treatment options available to you. Please ensure this is appropriately referenced. Please post this in the online forum for review by the course coordinator and discussion by other participants.
from page 19
ACNEM Journal Vol 31 No 1 – March 2012
19
chronic disease. Although it may be critiqued for seeming ‘alternative’ or lacking evidence, this type of integrative approach has in fact been described as ‘best practice’ rather than ‘alternative practice’9 Personally, I now feel ethically obliged to at least give patients the option of embarking upon such a comprehensive assessment and treatment plan.
2. evidence-based-medicine is not what i used to think it was
Throughout medical school I was a big fan of ‘evidence-based medicine’, and I thought it was so convenient that almost everything a doctor needs to know is neatly summarised in the Australian Medicines Handbook and Therapeutic Guidelines. Setting out to train in General Practice as I was, I thought, ‘What could possibly go wrong? The best available evidence is right there at my fingertips’.
How naïve I was! I soon discovered that clinical practice was more of an art than a science, and that evidence was much more about gaining confidence in one’s own clinical experience (a view supported by Lowe and Brewster10, who point out that ‘evidence’ is a synthesis of others’ experience with one’s own, i.e. what the RCTs say in relation to one’s own clinical experience). Furthermore, as pointed out by Dr Matthew Shelton and other lecturers in the course11, more often than not it is the combination of nutrients/anti-oxidants/doctor-patient interactions, etc. which make a treatment work, and this seldom equates to a double-blind RCT proving the effectiveness of single isolated factors.
Furthermore, it has been a rude awakening to delve into the questionable methodology of drug company sponsored trials, and I am especially saddened to learn how the oil, grain, dairy, sugarcane and processed food industries have had such an influence on the direction of research and health policy12,13.
However, rather than being critical of mainstream medicine, I believe that the lesson here applies to both mainstream medicine and NEM – that we should be careful to ensure that all available approaches and evidence are considered and evaluated in an unbiased, ethical and
cost-effective way. As far as following EBM from a NEM point of view, I feel there is a danger in taking on a ‘reductionist stance’, branching out into more and more specialised areas such as bio-identical HRT and indiscriminate use of supplements which may be expensive and make some people feel better temporarily, but fail to address the root of a problem. There is also a danger of being ‘bought’ by neutraceutical companies, especially if we are to dispense our own supplements.
Where do we draw the line as to what qualifies as EBM, which we can feel comfortable applying in clinical practice? This is a difficult question. I know of a dentist who has accumulated 20 years worth of data trialling different supplement combinations to help patients after amalgam removal, correlated with detailed pre and post-treatment biochemical analyses. I also know a traditional Tibetan doctor who has been trained in a completely different etiological model to Western medicine. Yet she treats many chronically unwell patients referred by her local GP… with consistently good results. Does this qualify as ‘evidence’?
3. ‘body-mind’ medicine seems equally, perhaps more important, than mind-body medicine
The final point I wish to discuss is a reflection on the eye-opening mental health lectures presented by Dr Kerry Harris14 (as well as the public lecture by Dr Bill Walsh15) – an area which I am
especially interested in.
Prior to my NEM journey, whenever I saw patients there was an invisible wall between mind and body. If there was nothing ‘physically wrong with them’ and all the blood tests were normal, it was time to help them function as best they could while treating any psychological or psychiatric conditions. I have generally appreciated the mind-body connection, as elegantly described by Dr Craig Hassed in ‘General Practice: An Integrative Approach’16. However, I have rarely considered the other side of the coin – the idea of nutritional and environmental factors having a profound effect on the brain and mind, let alone at the level of gene expression!
Functional Medicine practitioner Mark Hyman claims that ‘only about 10 percent of us are nutritionally, metabolically, and biochemically balanced enough to fully benefit from psychotherapy’17. The surprising conclusion is that the cure for mental disorders may not be in the mind or the brain, but rather outside the brain.
The culprits on my list of differentials for mental disorders now includes heavy metals, detox problems, gluten sensitivity, under/over-methylation, pyrroluria (caused by a nasty bi-product of the haem biosynthetic pathway), too little EFA’s, poor absorption of vitamins and minerals such zinc and B6 and inadequate dietary protein… in fact the very same mediators that were discussed above in point one, which in fact apply to just about all chronic diseases.
reflection on the case of mr ja
Now back to patient JA that I touched on in the Pre-disposing Activity; a man in his early 70s with chronic depression and fatigue (not responding to ECT or intensive psychotherapy), as well as long-standing COPD with frequent exacerbations treated with recurrent antibiotics, plus insomnia and bouts of intractable pruritis on his back.
When I last saw JA, his management simply involved juggling medications such as olanzopine (under his psychiatrist), weekly home visits by his psychologist, steroid creams/ antihistamines for his
continued next page

20
ACNEM Journal Vol 31 No 1 – March 2012
itchy back, and the usual inhaled steroid regime for COPD. At the time I didn’t take a diet history18, I didn’t enquire about food intolerances19, I didn’t look to see if he had amalgams in his mouth or ask about prior occupational exposure to heavy metals20. I didn’t bother to check if his digestive function could be improved21, or if he had a subclinical form of thyroid disease or adrenal issues22. I didn’t check to see if there was adequate protein, cholesterol or good fatty acids in his diet23. I didn’t screen for vitamin or mineral deficiencies24, and finally I didn’t check for impaired glucose tolerance or insulin response25 (reassured that his fasting BSL was in the normal range). And of course I had no idea about checking his methylation status or seeing if he was a pyrrole26... or for that matter coeliac27! Any one of these factors, but more likely some or all of them in combination, would have undeniably contributed to his problems.
Though I haven’t followed him up as I am not working in General Practice at the moment, in hindsight I would certainly do things differently. Although the temptation is there to begin with every possible blood test, hair mineral analysis, etc, I think it would be more beneficial and cost-effective to trial a number of things in a gradual, systematic way, emphasising thorough patient education and JA’s role as a ‘student of health’, ensuring he understands the ‘ship with anchors’ model.
From the NEM point of view, I would begin with Medicare-approved tests and a trial of the low stress diet (with sufficient protein), and possibly refer him to a nutritionist to help him implement the appropriate changes. I would ask in detail about his diet as well as his allergy history, as well as potential environmental triggers of his symptoms, along with the particular characteristics of his depression (as a clue to neurotransmitter imbalances, methylation status, etc), and questions that point to vitamin/mineral status – such as dream recall for B6 and taste for Zn.
My initial tests would probably include an MBA 20, vitamin D, FBE, coeliac screen, glucose tolerance test, B12 & folate, hs-CRP, cortisol and thyroid hormone levels, and perhaps also an ANA and lipids (as both low and high cholesterol
may contribute to depression, etc). Initially I might commence fish oil/cod liver oil, probiotics (given his history of frequent antibiotic use), zinc, B6, magnesium, vitamin D and rock salt. Reviewing how he goes on the new diet would give us a closer chance to look at his digestion (and perhaps order a Comprehensive Stool Analysis to check for yeast, blastocystis, etc or consider acid supplements). I would also treat any abnormalities indicated by the initial bloods and consider Walsh/Pfeiffer-style testing for pyrroles/methylation status. If improvement is minimal I might then investigate the possibility of heavy metal toxicity and test and treat as appropriate.
Would this approach be practical? At the time I was seeing JA every 2-3 weeks, often 30 minutes at a time in a counselling capacity, hearing him complain relentlessly about how nothing was ever improving. A psychologist was doing home visits but he wasn’t getting anywhere with this either. He also got sick several times with infective exacerbations of COPD and basically thought his life was little more than a burden to others. In my view, having completed this ACNEM course, there is a good possibility that his poor health may have improved dramatically with appropriate treatment. In the time I saw him I could have been moving forward with a clear plan of action, and I would anticipate considerable cost savings by getting this man better in the long run, not to mention improvement in his quality of life (and that of his wife!).
in summary
I look forward to the time when Medicare, the MBS and PBS will remove disincentives to GP’s and other doctors to embrace this kind of medicine, though I acknowledge this process won’t happen overnight - in fact as I write these words I am shown an article in the local rag saying that ‘Australia’s top doctors want university courses in acupuncture, chiropractic and naturopathy scrapped, claiming they are a misuse of public money and encourage quackery28’ It is sad and difficult that NEM (based on essential nutritional and environmental biochemistry) seems to be up against misinformed peers, misinformed politicians and policy makers, a misinformed media and a misinformed public.
The establishment of integrative medical clinics, I believe, is a good step forward29. However, is it enough? I believe ACNEM has a responsibility to develop clear and stringent guidelines for its member-practitioners, and to develop a cost-effective model for healthcare in the 21st century which will hopefully influence the way that all doctors are educated (rather than remaining a little-known sub-speciality within general practice).
I congratulate those good souls (including most of the lecturers) who choose to practice in the ACNEM way and advocate for change. Maybe one day I’ll be brave enough to become one of them!
Good luck to everyone on this ACNEM journey!
Adrian
Adrian Hekel, BSc (Hons), BMBS, (GP Registrar)
from page 19
21
ACNEM Journal Vol 31 No 1 – March 2012ACNEM Journal Vol 31 No 1 – March 2012
21
References and ACNEM online learning resources cited:
1. John Murtagh (2003). General Practice. 3rd ed. McGraw Hill
2. Sidney MacDonald Baker et al. (2005) Textbook of Functional Medicine. Johnson Printing
3. Mervyn Garrett (2010). Allergy in General Practice – Clinical Patterns and What They Mean. Presentation for ACNEM on-line course.
4. Peter Baratosy (2010). Metabolic Syndrome. Presentation for ACNEM on-line course.
5. Mel Sydney-Smith (2010). Nutritional Assessment. Presentation for ACNEM on-line course.
6. Karel Hromek (2010). The Sensitive Patient. Presentation for ACNEM on-line course.
7. Carole Hungerford (2008). Good Health in the 21st Century: a Family Doctor’s Unconventional Guide. Penguin.
8. ibid
9. Kerryn Phelps and Craig Hassed (2011). General Practice: The Integrative Approach. Elsevier.
10. M Lowe & DR Brewster (2003). Evidence-based medicine and clinical practice. Journal of Paediatrics and Child Health. Volume 39, Issue 2, pages 145–146.
11. Matt Shelton (2010). Safe Integration of NEM into Clinical Practice. Presentation for ACNEM on-line course.
12. Nora Gedgaudas (2011). Primal Body, Primal Mind: Beyond the Paleo Diet for Total Health and a Longer Life. Healing Arts Press.
13. Mary Enig (2001). Know Your Fats: The Complete Primer for Understanding the Nutrition of Fats, Oils and Cholesterol. Bethesda Press.
14. Kerry Harris (2010). Mental Health: A Nutritional Perspective. Presentation for ACNEM on-line course.
15. Bill Walsh. Epigenetics and Mental Health. ACNEM Public Lectures.
16. Kerryn Phelps and Craig Hassed (2011). General Practice: The Integrative Approach.
17. Mark Hyman (2009). The UltraMind Solution: Fix Your Broken Brain by Healing Your Body First. Scribner.
18. Mel Sydney-Smith (2010). Nutritional Assessment. Presentation for ACNEM on-line course.
19. Mervyn Garrett (2010). Allergy in General Practice – Clinical Patterns and What They Mean. Presentation for ACNEM on-line course.
20. Karel Hromek (2010). Heavy Metal Toxicity and Anti-oxidants. Presentation for ACNEM on-line course.
21. James Read (2010). Gastrointestinal Problems. Presentation for ACNEM on-line course.
22. Peter Baratosy (2010). Thyroid and Adrenal Disease. Presentation for ACNEM on-line course.
23. Kerry Harris (2010). Low Stress Diet in General Practice. Presentation for ACNEM on-line course.
24. Mel Sydney-Smith (2010). Nutritional Assessment. Presentation for ACNEM on-line course.
25. Peter Baratosy (2010). Metabolic Syndrome. Presentation for ACNEM on-line course.
26. Kerry Harris (2010). Mental Health: A Nutritional Perspective. Presentation for ACNEM on-line course.
27. Carole Hungerford (2010). Coeliac Disease. Presentation for ACNEM on-line course.
28. Natural Therapy Attack (Dec 2011) The Sunday Mail.
29. Jennifer Hunter (2008). Establishing an Integrative Practice. Complementary Medicine. pp23-26.

22
ACNEM Journal Vol 31 No 1 – March 2012
On ABC Radio National’s Life Matters, between 24 Jan and 7 February 2012, Karen Law in her three part series, ‘Sprinkle of Hope’, discussed coming to terms with her diagnosis of MS, in which she took control in the face of a debilitating and incurable illness. She undertook her own journey, combining conventional medical options and following advice from Phillip Day, she addressed her borderline vitamin D levels. She eliminated saturated fat including meat, dairy, as well as sugar and all processed food, to a diet based on raw and organic fruit and vegetables and found her symptoms modulating1.
Implementing the rigorous diet required may be difficult for many, but for Karen, compared with the loss of the use of her arms and legs for good it was easy. She was also able to identify a possible stressful triggering event.
Based on the work of neurologist, Ray Swank, a study of 144 patients published in the Lancet followed up for 34 years, found that of MS patients adhering to a low saturated fat diet (<20g per day) 31% died compared with approximately 80% of patients not sticking to the diet. Furthermore of the group who started with low level of disability only 5% died. Also, when those who died from non-MS diseases were excluded from the analysis, 95% survived and remained physically active2.
The dramatic results of this study were largely ignored by the medical community, perhaps because the great strength of the study, its 30+ years duration, may also have been its greatest weakness. It was commenced in 1949 with examination of participants’ dietary fat consumption in conjunction with a graded neurological disability scale. It was published in 1990 in the era of the randomized controlled trial as the benchmark for evidence.
An anonymous editorial in The Lancet stated that, “the role of lipids in MS must remain not proven,” and the dietary intervention was largely ignored, denying the potential benefits to the
MS community despite the size of the effect, its positive health benefits, and its enormous potential for the management and treatment of an incurable disease3.
Karen discovered the work of Prof George Jelinek, Professor of Emergency Medicine at Charles Gairdner Hospital Perth, also with a diagnosis of MS, in his book ‘Overcoming Multiple Sclerosis: An Evidence-based Guide to Recovery’, to be in line with her thinking on a holistic treatment program.
Lifestyle and complementary interventions found to have merit in treatment of MS as reviewed by Jelinek include very low animal and saturated fat, no dairy products, Vitamin D 3000-4000 IU per day, supplementation with omega 3 fatty acids, e.g.; fish or flax seed oil, minimal regular sunlight exposure (10-15 minutes exposure of most of body surface 2-3 times per week), positive mental and social health and coping strategies, and exercise4.
Despite accumulating evidence for these lifestyle factors they rarely form a major part of the management of MS. Management seems to rely on heavily promoted conventional medicine despite limited benefits, side effects, and methodological flaws in clinical trials. Side effects often have to be managed with a variety of other medications, each with their own side effects5.
This holistic approach to MS raises the issue of the important issue of lifestyle for treatment of chronic illness. Outstanding is the work of Dr Dean Ornish, whose patients with heart disease show sustained benefit from intensive lifestyle change. Results look promising for patients with prostate cancer following the same protocol. This approach is not to reject the conventional pharmacological and technological methods such as stem cell therapy, but a balanced approach using the best of every modality is required, each based on the best available evidence6.
Karen Law had undertaken her own search for a holistic treatment program. With the myriad, and at times conflicting,
information available she was empowered and took control rather than wait for the debilitating effects of the disease to take effect.
In a European study, 64% of German patients with MS were using complementary and alternative medicine (CAM) and in Australia the numbers can be assumed to be similar7. A balanced approach utilising the best of conventional and lifestyle medicine needs to be adopted. Specialists are best placed to promote these therapies. GPs or other suitably qualified health professionals may be better placed time-wise to implement the complementary and lifestyle strategies. MS support groups and the MS Society are valuable resources.
There is an urgent need for education and resources to be available to MS patients and those with other chronic illness to adopt a holistic treatment program.
References:
1. Day, Philip. Health Wars, Credence Publ 2001.
2. Swank RL and Dugan BB. The Lancet 1990: 336(8706):37-9.
3. Anonymous. The Lancet 1990 ; 336:25-6.
4. Jelinek GA and Hassed. CS 2008 discussion paper managing multiple sclerosis.
5. Ryan M and Piascik. P Journal American pharmaceutical Assoc 2002;42(5):753-66.
6. Ornish D et al. JAMA 1998;280:2001-
7. Winterholler M et al. Fortschritte der Neurologie-Psychiatrie 1997;65(12):555-61.
In The NewsShirley Schurmann, RN, B App Sci, Dip Nurs Ed, M Ed Studies, Grad Cert Health Sci(Nutr&EnviroMed)
ACNEM Journal Vol 31 No 1 – March 2012
23
In Memoriam:Chris Reading
For those of us whose lives were touched by Dr. Chris Reading (BSc, Dip Ag Sc, MBBS, FRANZCP, FACNEM), he will be remembered for his medical genius, his healing intent and his deep humanity. Dr Reading was a dynamic force in the international holistic health community, tirelessly caring for his many thousands of patients and helping hundreds of thousands of others through his writings. He was an original thinker, many of whose ideas were decades ahead of their time. Finally, Dr Reading was a courageous practitioner, who fought for the beliefs and values he championed in practising orthomolecular medicine/psychiatry, at its very inception and amidst much controversy in Australia.
In going through thousands of Dr Reading’s files in his newly formed archive, I have been amazed by the sheer mass of clinical care and detailed follow-up, personal correspondence and broad-ranging research that occupied Dr Reading’s days and nights. I have found
articles as diverse as the nutrition of dinosaurs and early mammals to a vast file on the genetic engineering of food crops among these papers. I have met only one other man in my entire lifetime who has attempted to distil so much information to create a cohesive framework for health and healing.
As well, I was deeply impressed by the sincere appreciation and gratitude written in thousands of cards and letters from Dr Reading’s patients. Among these were many whose health, careers, sanity and very lives were saved by Dr. Reading’s clinical and personal care. Thousands sent him their family health trees. And hundreds wrote letters of support when Dr Reading’s very livelihood was under assault from the medical establishment.
Dr Reading would undoubtably be grateful to know that his work and life is being honoured by many organisations to which he contributed, including ACNEM and the International Society
of Orthomolecular Medicine, who will induct him into their “Hall of Fame” this coming April.
For myself, I am grateful to have known Dr Reading and to have worked with him to re-publish his book, ‘Trace Your Genes to Health’, and two other books shortly before he passed on. Hopefully a new generation of readers will become acquainted with Dr. Reading’s work as we continue to publish articles and papers found in Dr. Reading’s files.
While I truly miss Dr Reading, I trust that his healing work will live on.
David Richard, Publisher
Vital Health Publishing/Enhancement Books
24
ACNEM Journal Vol 31 No 1 – March 2012
24
Many of you reading this will have known Archie, who passed away on 1st March 2012.
Archie was a rare person, able to use his training and profession (as a doctor) to improve the lives of many people beyond those he dealt with directly. His greatest legacy is the awareness he created of the prevalence of vitamin C deficiency in most Aboriginal children in outback NSW. He frequently witnessed them dying and was able to eventually reverse this through injections of vitamin C. His experience led him to write Every Second Child, which is both a condemnation of an uncaring (White) society and a testament to what one committed person can achieve. Later in his life Archie tried to alert the world to the likelihood that many babies who were thought to have been shaken to death were, in fact, suffering from subclinical scurvy.
Archie was multifaceted and spent some years in the middle of his professional career mining for opals in Cooper Pedy and wrote several acclaimed books about this gem.
Archie has been rightly honoured a number of times, including the Australian Medal of Honour for Outstanding Scientific Research (1978), ‘Greek Australian of the Century’ (2000) and the Annual ACNEM Award (2008). He was an ACNEM Fellow and for years lectured at ACNEM training events.
Archie Kalokerinos did not tolerate dishonesty, especially in medical practitioners, and in his confrontations seemed disinterested in his own reputation. We hope he will be remembered for his humanity and his honesty.
Dr Ian Dettman & Daan Spijer
For more information about Archie’s life and work:
http://kytheraismos.blogspot.com.au/2012/03/archie-kalokerinos-passed-away-on-march.html
In Memoriam:Archie Kalokerinos
25
Your CollegeExciting new trends in ACNEM training in 2012
ACNEM offers a more flexible training calendar this year to practitioners who wish to learn more about Nutritional and Environmental Medicine (NEM). Our traditional face-to-face training courses have in many cases been augmented by an online component, with a view to managing all course enrolments through our online interface before long.
Our aim is to give practitioners more flexibility when choosing the type of training which best suits their needs, such as having to take less time out of practice or away from family, saving on travel and accommodation costs, or still to enjoy the full immersion of the 4-day Primary Course in-person! To kick off 2012, we held a 4-day face-to-face training event in Auckland in March. This will be followed in July in Fremantle with a new ‘hybrid’ Primary Course of 2-days face-to-face plus the equivalent of another 2 days of lectures online (4 months access).
In September we will be in Sydney with a full 4-day event, and then, to cap off the year, a major 5-day event in Melbourne in November which will also serve as ACNEM’s 30th birthday celebration, with a large gathering of ACNEM members and Fellows for a gala dinner on the evening of Saturday 24th November.
2nd Nutrition in Medicine Conference
At the time of writing, the 2nd Nutrition in Medicine conference, convened by ACNEM in conjunction with the Nutrition Society of Australia and the Food and Nutritional Sciences division of CSIRO is looking to exceed all expectations set by last year’s sold-out inaugural event.
With a bigger venue, registrations have once again reached capacity and we are again gratified by the enormous goodwill and support for this event. We believe it reflects not only the belief of the convening organisations, but that of the speakers, delegates, sponsors and supporting organisations, that the intersection of science, nutrition and medicine is the future of healthcare, and in fact is our hope for the future of a society plagued by preventable, chronic and complex lifestyle-related illness and disease.
ACNEM’s 30th birthday celebrations
Members will soon be receiving information in the mail about a series of initiatives in 2012 designed not only to celebrate ACNEM’s first 30 years and to honour those who made the College what it is today, but to prepare ACNEM for the next 10 years, in line with the strategic planning process commenced by the Board last August. Members can expect to receive a detailed survey for completion, a range of special benefits of membership for the next 12 months, and to hear about a redesigned Fellowship program.
Warm regards from the ACNEM Team.
ACNEM Journal Vol 31 No 1 – March 2012

26
ACNEM Journal Vol 31 No 1 – March 2012
Featured BooksThe Panic Virus: Fear, Myth and the Vaccination Debate By Seth Mnookin
When dealing with large issues that have an impact both on society and the lives of the individuals in that society, it is important that we have available to us books
such as The Panic Virus, to assist us in navigating our way. Vaccination is a global phenomenon with almost global support from governments and the medical professions, from academics and the World Health Organisation. It also has its many opponents and detractors. There are powerful and emotional arguments on both sides of the debate.
Before undertaking to review this book, I need to declare that I am a sceptic on this topic, not convinced that universal vaccination is, on balance, a good thing; but willing to be convinced that it is, given enough credible evidence.
The Panic Virus is one of the rare books I have read that has helped to inform me on this vexed question. It sits on the pro-side of the fence while most of the other books I have read have been anti-vaccination. However, the author’s main aim seems to be to highlight the misinformation that has come into the public debate from many of the anti-vaccination groups and individuals, as well as from governments and government (health) departments;
and the far from helpful role played by many media outlets. He is scathing of the media.
One area that the author expands on is that of the MMR vaccine and the claim that it can cause autism. He is highly critical of groups and individuals who keep this possibility alive when the evidence seems to be overwhelmingly against it. His major criticism is that the continued lobbying for recognition of the MMR vaccine as a cause of autism is diverting limited resources from research that may uncover some of the actual causes of this increasingly prevalent condition. In the process, Seth Mnookin examines the role played by Andrew Wakefield and the questions around that doctor’s integrity and those who have collaborated with him.
The title of the book refers to Seth Mnookin’s claim that the way that governments and the media have dealt with questions of vaccine safety has led to panic reactions amongst parents, which in turn has led to large numbers of parents not having their children vaccinated.
The Panic Virus can help inform parents about some of the issues relating to mass vaccination, but I don’t believe that the book would offer them much beyond that, other than perhaps having them look elsewhere than vaccines as a cause of autism*. This is a book about politics and social commentary.
My only criticism of this book is the tone occasionally used by the author. He seems to be trying to be a dispassionate reporter of facts and opinions (Seth Mnookin is a journalist) but from time to time he is emotional in his comments. I found this
somewhat confusing and also felt that he was telling me what my attitude should be. I still think that this book offers the reader valuable insights into a difficult set of issues: whether to vaccinate children; the role of governments in mandating medical treatment; the manipulation of data (immunological and epidemiological); the role of special interest groups and lobby groups; the role of the media in reporting on medical and social issues and in leading debate; and the role of the courts in mediating conflicting interests.
Seth Mnookin has done us all a service by investigating some of the difficult questions surrounding mass vaccination and offering us his thoughts and insights in this valuable book.
* See for instance: Devil in the Milk, Keith Woodford, Craig Potton Publishing, NZ, 2007.
Reviewed by Daan Spijer, LLB www.thinking-allowed.com.au
This book is published by Black Inc ISBN: 9781863955188
26

27
ACNEM Journal Vol 31 No 1 – March 2012
Healthy Home Healthy Family By Nicole Bijlsma
This text covers all aspects of sources of environmental toxicity in our everyday lives, particularly in the home. It gives advice on what to avoid and minimise, and
suggestions for alternatives where available. It has an Australian focus but is relevant to any country.
Overall I found this to be a very informative, thorough and balanced book. It is of course applicable to any family, healthy or otherwise, but particularly pertinent to those planning a family, with children at home or those who are unwell.
Nicole is a naturopath who herself has undergone health issues which necessitated her increased awareness of toxins in her own environment. She has an easily understood writing style and often relates to her own experience. She asks questions of the reader to invite you to explore your personal situation and offers clear explanations of the issues. Her style is sensible and not alarmist. I like the fact that the book has plenty of practical tips for how to deal with issues such as mould in the home.
There is an interesting section on electromagnetic fields and radiation with good explanations and good advice on how to minimise exposure. All aspects
of the home are covered; from allergens to chemicals. There are many references and useful website resources in the book. I would have appreciated more references at times. They are collected alphabetically for each chapter however I feel numbering each chapter’s references would have been more user-friendly.
Overall, I highly recommend this book for any family or health practitioner as a valuable one-stop resource for healthier living.
Reviewed by Dr Debbie Fewtrell, MBChB, Dip Obst, FACNEM, FRNZCGP
This book is published by Joshua Books.ISBN: 9780980789812
28
re article by judy jacka: ‘the human energy field’, acnem journal vol30 no.3, dec 2011
A fascinating article; with insights into some key ideas and researchers in the area of 20th century work on the ‘human energy field’.
To extend the discussion to some complementary research, the Eastern bloc workers of Ignjatić1 and Sit’ko2 have connected modern Western physics and the human biology with extensive, comprehensive and largely unknown data.
Ignjatic, presented a review paper3 at the Symposium of Quantum-Informational Medicine QIM 2011, Belgrade, 23-25 September 2011, in a lecture entitled MICROWAVE RESONANCE THERAPY (MRT). His lecture describes the theoretical basis whereby tissues have dielectric properties that when changed will lead to a diseased state at the physical biochemical level. The physics of the electromagnetic fields in health and disease are presented and the significant feature they claim to have evidence for is the action of quantum field effects at the macroscopic level rather than simply the subatomic level.
Microwave resonance therapy (MRT) is based on the Russian-Ukrainian concept on quantum nature of the acupuncture system, as a dynamic structure joined at the locations of the maximum of de Broglie’s interferential three-dimensional standing waves. The changes in dielectric properties of tissues lead to a disease, deforming the structure of the EM MW standing waves and related acupuncture
system. Microwave resonance therapy (of extremely high frequency 42-100 GHz, athermic energy 10-4eV and extremely low intensity 10-21 W/Hz cm2) resonantly normalizes frequency responses in excited acupuncture system and an organism biochemically overcomes a disease via physiological-neurohumoral MW and self-regulatory acupuncture mechanisms.
Sit’ko in his 1996 patent application for a microwave resonance therapy (MRT) device indicates the possibility of managing functional health problems, which is confirmed by Ignjatic with his presentation of data of numerous health problems treated with MRT and positive results.
Another strand of investigation is that of biophotons and relationship to human health and disease states. It has been clearly shown that biological tissue emits photons, termed biophotons. The emissions vary depending upon health status. Beloussov et al in a 2007 publication4 combines reports from the principal investigators in the field and also utilises modern physics to explain the human energy field. They also confirm the possibilities of early diagnosis.
As Jacka correctly highlights, enhanced understanding of the human energy field would provide a tremendous boost to preventive approaches and also to early diagnosis with resulting improved prognosis. As the papers above indicate, treatment possibilities abound.
It is of great interest that Ignjatic1 highlights the results of their investigations of quantum physics and
energy fields of the human body correlate very closely, if not precisely, to acupuncture points and also to the Indian knowledge of prana and the ida, pingala, and sushumna energy channels.
This is of significance, in that modern physics seems to be confirming the two most comprehensive traditional health and medical systems have a functional understanding of the human energy fields.
That is Traditional Chinese Medicine and Ayurveda, including the Yoga system of self culture (with its detailed description of mind, body, energy relationships), have provided guidance on human energy fields for centuries, that are being confirmed by modern biophysics research.
When boiled down to the practical nitty gritty, the fundamental way we act in our daily lifestyle, and what and how we eat and the environment we work and live in, in relation to our inherited potentials, is what impacts the most on our energy, health and well being.
Dr Graeme Stringer, BDSc, MDSc, FRACDS
References:
1. Z.Jovanovic-Ignjatic & D.Racovic, Proceedings of the 4th All-Russian Workshop on Quantum Therapy 2005. Microwave Resonance Therapy: New Possibilities.
2. Sit’ko, United States Patent Application 5,507,791. April 16,1996. Microwave Resonance Therapy.
3. Zlata Jovanovic Ignjatić, Symposium of Quantum-Informational Medicine QIM 2011: Belgrade, 23-25 September 2011, Invited lecture : Microwave Resonance Therapy.
4. L.V. Beloussov, V.L. Voeikov and V.S. Martynyuk, Biophotonics and Coherent Systems in Biology. Springer 2007.
ACNEM Journal Vol 31 No 1 – March 2012
Letters to the Editor
28

2929
ACNEM Journal Vol 31 No 1 – March 2012
smart meters: do not place them on a bedroom wall
As part of the federal government’s National Energy Efficiency Initiative to tackle climate change and move to a low-carbon future, the May 2009 budget included a $100 million program to develop a commercial scale smart grid project in partnership with the electricity supply sector. This would in turn, be used as the model for a ubiquitous electricity smart grid network throughout Australia, and promoted as the electricity system of the future by improving the efficiency of power production, delivery and use.
At the heart of the smart grid is the smart meter which communicates with the utility wirelessly (radiofrequency and microwave –RF/MW) and eventually with a whole new generation of household appliances that will have in-built wireless interconnectivity. All these new wireless enabled appliances, besides being a $$$ boon for the energy and appliance industries in difficult economic times, will inevitably increase chronic RF/MW exposures in the home or office. As for safety standards to protect the public, unfortunately there are none, for the RF/MW exposure standards, conveniently set by industry, are limited to preventing acute immediate hazards (heating) but not chronic effects.
There are a number of valid unresolved problems with the technology, but there is one aspect which I find particularly concerning:
Apparently in Victoria, once 90% of all buildings in a region have a smart meter installed the system goes active, with an increase in 24/7 emissions from the smart meter. However, regardless of region, if you have solar panels on the roof feeding back into the grid your smart meter will already be active. One such meter, which I measured recently on a Bendigo home, was emitting (at 1 foot) three RF spikes every two minutes. Ambient power levels were .004 mW/m2 (okay) but spiking up to 67.4 mW/m2 (not good). This spike is significantly higher than what one would
be exposed to when having a DECT phone by the bedhead (about 1.2 mW/m2
at 1 foot).
It is not unusual to find in many Australian homes that the electrical meter box has been placed on a bedroom wall, with a bedhead hard up against that wall. As I have seen on numerous cases (and published papers about), in this situation the powerfrequency magnetic fields can cause insomnia and fatigue in some people. What will be the effects, however, once a smart meter has been installed and RF/MW is added as well? It is my understanding that the pineal gland may sense impinging electromagnetic fields as ‘light’ and suppress nocturnal melatonin release. If this be the case I suspect that those frequent smart meter spikes will have a deleterious effect on anybody trying to sleep nearby.
I conclude that medical practitioners trying to help patients with sleep and fatigue disorders must take into consideration what is in the bedroom (or on the wall). It can no longer be ignored in patient treatment.
Don Maisch, PhD
AUSTRALASIAN COLLEGE OF NUTRITIONAL & ENVIRONMENTAL MEDICINE INC.
■ Presented by medical and clinical experts■ Evidence-based and strongly referenced ■ Clinical tools for application in daily practice■ Supportive college atmosphere
■ Network of like-minded peers ■ Improved patient outcomes ■ Certificate & Diploma (coming soon) ■ Fellowship
■ Online (distance) learning■ RACGP, ACRRM, RNZCGP CPD/CME points
may apply
www.acnem.org +61 3 9597 0363 po box 298 sandringham vic 3191, australia [email protected]
training calendar
July 2012 Fremantle ■ Primary Course in NEM (28-29 July + online component)■ The GUT – Gastrointestinal Conditions (28 July + online
component)■ Allergy & Autoimmune Conditions (29 July + online component)
September 2012 Sydney ■ Primary Course in NEM (13-16 Sept) ■ Mood & Anxiety Disorders (13-14 Sept) ■ Metabolic Conditions, Diabetes and CVD (15-16 Sept)
November 2012 Melbourne ■ Primary Course in NEM (22-25 Nov)■ NEM in Dentistry (22 Nov) ■ Environmental Health (23 Nov) ■ A to Z of NEM - Putting it into Practice (24-25 Nov)■ Heavy Metal Detoxification (26 Nov + online component)
March 2013 Adelaide ■ Primary Course in NEM (23-24 Mar + online component)■ Childhood Conditions (23 Mar + online component)■ Mid-Life for Women & Men, Hormones & BHRT (24 Mar + online component)
ONLINE LEARNING
■ Primary Course in NEM 30+ hours, equivalent to 4 days face-to-face, 6 months access
■ Epigenetics & Nutrigenomics - Nature or Nurture?15 hours, equivalent to 2 days face-to-face, 3 months access
■ The GUT - Gastrointestinal Conditions including Gut Dysbiosis and Permeability 15 hours, equivalent. to 2 days face-to-face, 3 months access
■ Tired or Wired - Thyroid & Adrenal Conditions15 hours, equivalent to 2 days face-to-face, 3 months access
■ Injectable Nutrients 7 hours, equivalent to 1 day face-to-face + assessment, 2 months access
■ Heavy Metal Detoxification with optional Certification 15 hours, equivalent to 2 days face-to-face + assessment, 4 months access. Prerequisite: Injectable Nutrients (online)
the acnem primary course
The four-day (30 hour) ACNEM Primary Course provides foundation training in NEM, covering the key nutritional, environmental and biochemical factors in health and well-being, and treatment approaches to many of the conditions, illness and disease seen in primary care. The course is pitched at a post-graduate medical level, providing the nutritional biochemistry not taught at medical school or during registrar training, and the application of this knowledge in clinical practice. With practical tools to aid integration into daily practice, the Primary Course enables practitioners to immediately begin practising Nutritional and Environmental Medicine confidently and safely.
Topics covered in the Primary Course include:
• Introduction to NEM• Gastrointestinal conditions• Cardiovascular disease• Diabetes & metabolic conditions• Allergies and food sensitivities• Dietary history & the Low Stress Diet• Cancer• Mental health• Chronic fatigue syndrome• Coeliac disease• Vitamin C & antioxidants• Migraines & other headaches• Adrenal & thyroid conditions• Musculoskeletal conditions• Women’s health & menopause• Men’s health• Childhood conditions• Heavy metal toxicity• The sensitive patient• The dental perspective• Applications in pharmacy• Contraindications & interactions• Case histories• Interactive panel discussions
special training programs
The Primary Course is complemented by a range of shorter courses (usually two days) investigating particular subject areas in more detail, such as Gastrointestinal conditions, Thyroid & Adrenal conditions, Mental Health, and Allergy & Autoimmune, to name a few. Some of these programs are also available online. Prior completion of the Primary Course is recommended.
certificate, diploma & fellowship
ACNEM training optionally leads to nested Certificate and Diploma qualifications in NEM (coming soon) and the ACNEM Fellowship, providing greater recognition of training and specialty. The Certificate and Diploma qualifications are open to healthcare practitioners who meet Associate membership requirements while the Fellowship is open to Full members (doctors and dentists). The ACNEM Primary Course is the starting point for each of these qualifications.
online (distance) learning
ACNEM online learning is good news for those living in rural or remote areas, overseas, or who are otherwise unable to travel or to spend days away from family or practice to attend training in person. Online learning also reduces costs, such as travel and accommodation, and increases flexibility allowing you to learn at your own pace from your computer. The Primary Course and a growing selection of shorter courses are available online.