welcome to w.t. moore elementary school · *bus riders- bus schedules are published in the...
TRANSCRIPT

1706 DEMPSEY MAYO ROAD
TALLAHASSEE, FL 32308
PHONE (850)488-2858 FAX (850)922-6658
Kerri Anderson Ben Threadgill
Principal Assistant Principal
“The Leon County School District does not discriminate against any person on the basis of sex (including transgender status,
gender nonconforming, and gender identity), race, age, color, ethnicity, national origin, religion, pregnancy, marital status,
disability, sexual orientation, or genetic information.”
WELCOME TO W.T. MOORE ELEMENTARY SCHOOL Registration Requirements
Pre-K and VPK students are registered through the LCS Pre-K office. Please call 922-2099 for more information. Pre-K students will also need a passport from the Pre-K Office in order to register.
New to Leon County Schools:
Parents registering a new student to Leon County Schools must present the following documentation for their child
and fill out our school’s registration packet along with:
-withdrawal form from prior school
-last report card and transfer grades for the current 9 weeks.
-copy of the standardized test scores
-copy of certified birth certificate
-certificate of immunization – (Florida Shots form 680) or Florida exemption certificate
-certificate of medical examination performed on or after 8-1-17 (school health entry exam)
-social security card or number
-copy of your driver’s license (for verification purposes only, not used as a proof of residency)
-2 proofs of address: Current Bills only:
The first proof must be one of the following:
-Lease, Rental, Mortgage Statement, Property Tax or Homestead Exemption.
The second proof may include:
-City Utility Bill/ Electric Bill/commit for services receipt.
-Insurance Bill/Phone Bill
-Contract, building permit and letter from builder with occupancy date within the school year.
-Construction loan, letter from builder with occupancy date within the school year.
A Copy of the “Reassignment Approval Letter” if applicable, along with the above listed residency documentation.
Students Transferring within Leon County:
If you are transferring from another Leon County public school, you will need to submit the 2 proofs of address as
listed above and fill out our school’s registration packet. We will request the student’s records from the previous
school.
Residing with another Family: The same two required proof of residency as listed above from the
homeowner/renter. The Affidavit of Residency and Homeowner’s/Renter’s Acknowledgement sheets notarized.
Also the following: Two documents mailed to the address in the parent/guardian’s name.
Guardians: Leon County Schools does not accept notarized letters regarding guardianship, please provide one the
following: Copy of the Court Order Granting Guardianship.
Letter from the Clerk of the Court or attorney affirming that guardianship has been filed for (an
update must be given to the school every 60 days.)
Foster care/shelter letter from DCF verifying placement.
Pre-K-5th
1706 Dempsey Mayo Road
Tallahassee, FL 32308
Phone :( 850)488-2858 Fax :( 850)922-6658
Kerri Anderson Ben Threadgill Principal Assistant Principal
Welcome to W. T. Moore Elementary School! Here is some important Information for you: Times: School Hours are 8:30am to 2:50pm. First bell rings at 8:25am; instruction begins at 8:30am. Supervision is available from 7:45am-3:20pm. Before school program begins at 7:00am-8:00am for a fee. (PreK-5th) After school program starts at 2:50pm and ends at 6:00pm for a fee. (PreK-5th) Visiting: Parents are always welcome. Please sign in at the front office. Please have your driver’s license ready to scan into our Raptor System. Arrival and dismissal: School bus Car pick-up Day Care Vans Transportation changes must be in writing. Lunch: Come eat with your child during their lunch time. Bring in food items for your child only. No Sharing food with friends due to food allergies. Choose two friends to eat with you and your child. Volunteers: Lots of opportunities to come and volunteer. Complete a volunteer application on-line at www.leonschools.net Log your hours in the front office. Example: Classroom, book fair, carnival, field trips, etc. Registration: Packets will be available May 1st. Immunizations must be up to date. School health entry exam must have a date on or after 8/1/17.

KINDERGARTEN - LEARN MORE ABOUT MOORE!!!
Parents
Please join us for Kindergarten Parent Orientation, Tuesday, August 7th – 6:30 to 7:30 p.m. You will meet our teachers and learn about the kindergarten program. This presentation is for Adults Only. We will be collecting a student activity fee of $50.00. This will cover a Kindergarten class T-Shirt, Weekly Readers, tie-dye t-shirt, monthly themed journals, fieldtrip costs, end of the year activities, in-school presentations and celebrations and some activity supplies.
Students
We look forward to meeting the children on Thursday, August 9th from 1:30p.m. to 3:00p.m. You may bring your supplies at this time if you wish. Our parent organization, PTM, will have various items for sale in the cafeteria. You may also enroll your child in before and after school care.
KINDERGARTEN Supply List
(To be collected and shared):
- 4 boxes of 24-count Crayola crayons
- 2 packages of #2 pencils (Ticonderoga or Papermate preferred)
- 1 box of large Crayola Classic Colors markers
- 4 - large glue sticks
- 1 pair of small school rounded-tip scissors
- 1 package of Expo markers
(Write name inside of):
- 1 plastic pencil/crayon box
- 1 backpack (NO WHEELS, NO EXCEPTIONS! They do not fit in the cubbies.)

Dear Kindergarten Parents,
Welcome To W. T. Moore! We're happy to be sharing this special kindergarten year with you and your child.
We want the first days to be as happy and smooth as possible, so we have tried to think of questions you may have or
information that might be helpful as you prepare for the first week of school. If you have other questions or
concerns, please let us know.
*BACKPACK- Each child needs a regular size backpack WITHOUT WHEELS. Check this bag daily for the
homework folder and notes from school.
*LABEL EVERYTHING- All personal items need to have your child's name written on them.
*NO TOYS- Toys should be left at home.
*LUNCH- Children may bring a lunch from home or get a lunch at school.
*SNACKS- Send fruit, crackers, or some other healthy snack and a drink each day.
*CLOTHING-Children need to wear clothing and shoes that will allow them to play easily and safely. Children must
wear closed toe shoes instead of sandals or flip-flops.
*ACCIDENTS HAPPEN- Send a change of clothes in a ziplock bag with your child's name on it.
*SCHOOL HOURS- School starts at 8:30 a.m. and dismisses at 2:50 p.m.
Supervision is available from 7:45am-3:20pm.
*CAR RIDERS- Have your child here by 8:25 a.m. so that we may begin our work promptly at 8:30 a.m. For those
who bring their children to school, we ask you to prepare your child to say good-bye at the center door. We will take
loving care of your child.
*BUS RIDERS- Bus schedules are published in the Tallahassee Democrat in August. Pin the bus number to your
child the first few days of school. If your child is going to ride the bus, please allow them to start the first day of
school. This helps them learn the routine and avoids confusion later on. Students will be given a plastic, waterproof
bracelet to identify which bus they are to ride home. Please allow your child to wear this for the first week of school. It
makes for a much smoother dismissal. At the end of the day teachers will walk the students to the bus ramp and
make sure they are waiting in the correct bus line.
*DAY-CARE VANS- Teachers will walk van riders to the area where daycares pick up.
*PARENT PICK-UP- A teacher will walk with the children to the front of the school where they will wait for their
ride. Tell your child to be sure to wait with the teacher until you pull up to the sidewalk and stop. Pick your child
up on time as little ones become very anxious when they see everyone else leaving. Children must be picked up by
3:20p.m.
Do not ask older children to pick up your kindergartner in the classroom. Tell older brothers, sisters, or friends to look
for them at the bus or car areas.
Once again, Welcome to W.T. Moore and the beginning of a very special year for your child! We look forward to
working closely with you this year.
Sincerely, The Kindergarten Teachers

KINDERGARTEN Questionnaire Sheet from Parent/Guardian:
STUDENT NAME _____________________________ TEACHER __________________________
1. How well does your child play with others? Circle one
very well needs some direction needs frequent adult intervention
2. Can your child take turns, share, follow rules and play fair? Circle one
always sometimes rarely
3. Can your child use the restroom without any help? ________________________________
4. Which of the following tasks can your child do? Circle all that apply
fasten zippers tie shoes button clothes
5. How many lower case letters does your child recognize? ____________________________
6. How many upper case letters does your child recognize? ____________________________
7. Can your child write his/her name? yes no
8. How long can your child sit quietly and listen to a story? Circle one
0-5 min 5-10 min 10-20 min at least 30 min
9. How well can your child re-tell the story he/she just heard? Circle one
can re-tell most of the story can tell some can tell very little
10. Does your child recognize all of the numbers 1-10? yes no
11. Can your child count up to 10 objects? yes no
12. Can your child draw a picture and tell about it? yes no
13. Is your child able to attend to a task for at least 10 min? yes no
14. Is your child able to follow multi-part directions, such as, go to your room, put
on your pajamas and then bring a story book to me? yes no
15. Does your child separate easily from you when you have to leave? yes no
_____________________________________________ ___________________________________
Parent/Guardian signature Date

KINDERGARTEN
STUDENT NAME _____________________________ TEACHER __________________________
Did your child attend pre-school? YES NO
Which pre-school? __________________________________________________________________
Did your child’s pre-school teacher make any recommendations regarding this coming school
year?
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
If the recommendation was made in writing, may we have a copy? _______________________
Does your child have any medical conditions the teacher should be aware of?
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
Is there other information about your child that you wish for us to know?
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
_____________________________________________________________________________________
____________________________________________ __________________________________
Parent/Guardian Signature Date

LCS Student Registration Form
FOR SCHOOL USE ONLY
LCS Student #_____________________ School: ________________________
Date: ___________________________ Birth Verification: ________________
To be completed by the parent/legal guardian
1. Student’s Full Legal Name
First: ____________________________ Last ________________________________
Middle: ________________________ Gender: (check one) Female Male
Date of Birth: _______________________ *Social Security#: _____________________
2. Student lives at the following residence:
______ ___________________ ____ _______________ ____ __________ House # Street Name Apt # City ST Zip Code
Mailing address if different from residence address: (If Yes, PO Box only- Contact Registrar)
______ ___________________ ____ _______________ ____ __________ House # Street Name Apt # City ST Zip Code
Student lives with: Both parents’ Father Mother Guardian Other _______
**Home phone: ______________ Pref # **Parent Cell phone:___________ Pref #
**=Automated voice messages from Leon County Schools will be sent to the phone # marked as preferred. If it is a cell phone number, you are agreeing to receive these messages using this cell phone number.
3. Grade: ________
4. Last school attended (Name): ____________________________________________
School address: __________________________ County: _____________________
Has this child ever been enrolled in a Leon County School? Yes No
If Yes, School Name: ___________________________
5. Has this student had any previous expulsions, felony arrests resulting in a charge, orjuvenile justice actions? Yes No (If Yes, complete follow-up with AP)
6. Generation (Suffix): ___________ Nickname (Preferred Name): ____________________
7. Ethnicity: (check one) No, not Hispanic/Latino Yes, Hispanic/Latino
8. Race: (check all that apply) Black/African American White Asian
American Indian/Alaska Native Native Hawaiian/Pacific Islander Other
9. Student Survey: Was this student in special education (with an IEP), served as gifted,or have a 504 plan? Yes No If Yes, which program? _______________
10. Did the student have a first language other than English?
Yes No If Yes, which language? _______________________ (Native Lang)
• Is a language other than English used in the HOME?Yes No If Yes, which language? _________________ (Parent/Guardian Lang)
• Does the student most frequently speak a language other than English?Yes No If Yes, which language? _______________ (Student Primary Lang)
• Was the student in ELL at the previous school? Yes No 11. Is this child an immigrant student? Yes No
Birth City: ___________ Birth State: ____________ Birth Country: ____________ Multi Birth (twins/triplets/etc.): Yes No
If Birth Country is not “U.S.”, has the student attended school in the US for more than three years? Yes No Date entered US School: ___________
12. This student is a child of an active military family. Yes No
13. Is there a shared-custody or parenting plan in effect Yes No
If yes, plan must be on file with the school for enforcement.
• Is there a restraining order in effect? Yes No If yes, legal papers must be on file with the school for enforcement.
14. Restraining order is against: Mother Father Other
15. Parent/Guardian Information: The adult male and/or female with who the student lives.
• Last Name: ______________________ First Name: ______________________
Relationship: _____________________ Home phone: ______________________
Work phone: ________________ ext. _____ Cell phone: ______________________
Legal Custody/Guardian Yes No Permission to pick up? Yes No
Email address ________________________________________________________
• Last Name: ______________________ First Name: ______________________
Relationship: _____________________ Home phone: ______________________
Work phone: ________________ ext. _____ Cell phone: ______________________
Legal Custody/Guardian Yes No Permission to pick up? Yes No
Email address ________________________________________________________
LCS Student Registration Form
FOR SCHOOL USE ONLY
LCS Student #_____________________ School: ________________________
Date: ___________________________ Birth Verification: ________________
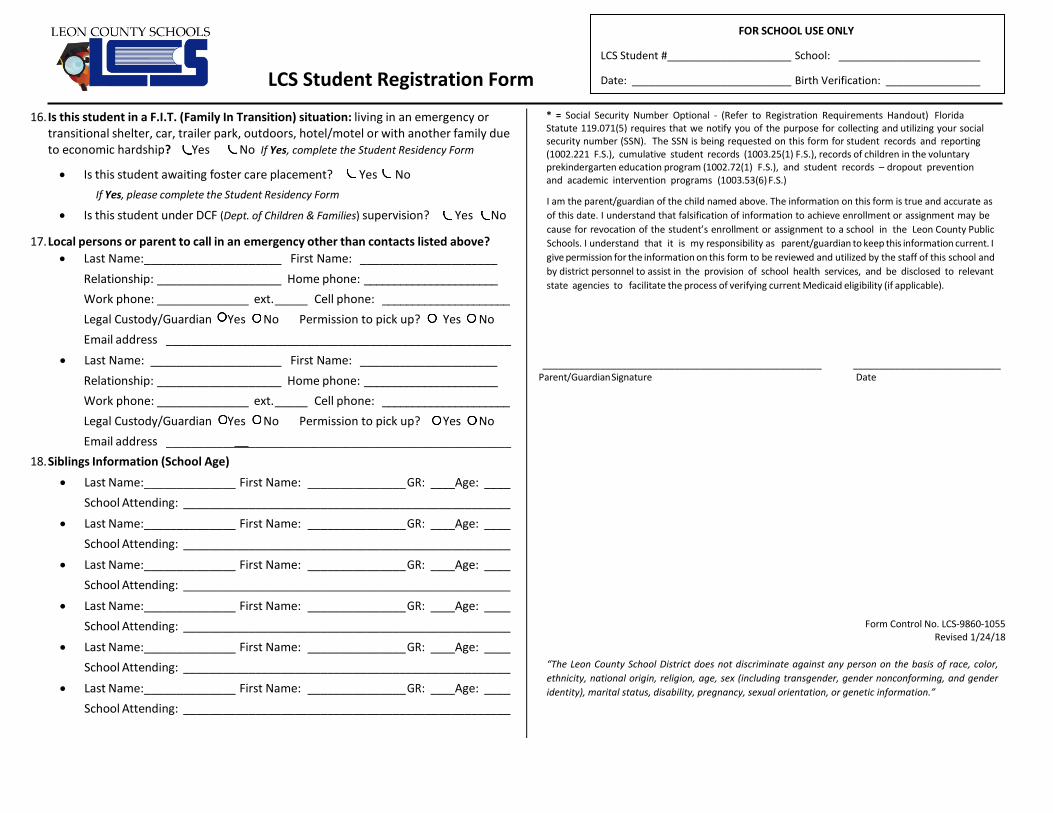
16. Is this student in a F.I.T. (Family In Transition) situation: living in an emergency ortransitional shelter, car, trailer park, outdoors, hotel/motel or with another family dueto economic hardship? Yes No If Yes, complete the Student Residency Form
• Is this student awaiting foster care placement? Yes NoIf Yes, please complete the Student Residency Form
• Is this student under DCF (Dept. of Children & Families) supervision? Yes No
17. Local persons or parent to call in an emergency other than contacts listed above?• Last Name: _____________________ First Name: _____________________
Relationship: ___________________ Home phone: ______________________ Work phone: ______________ ext. _____ Cell phone: _____________________ Legal Custody/Guardian Yes No Permission to pick up? Yes NoEmail address ______________________________________________________
• Last Name: ____________________ First Name: _____________________Relationship: ___________________ Home phone: ______________________ Work phone: ______________ ext. _____ Cell phone: _____________________ Legal Custody/Guardian Yes No Permission to pick up? Yes NoEmail address ______________________________________________________
18. Siblings Information (School Age)• Last Name: ______________ First Name: _______________ GR: ____Age: ____
School Attending: __________________________________________________• Last Name: ______________ First Name: _______________ GR: ____Age: ____
School Attending: __________________________________________________• Last Name: ______________ First Name: _______________ GR: ____Age: ____
School Attending: __________________________________________________• Last Name: ______________ First Name: _______________ GR: ____Age: ____
School Attending: __________________________________________________• Last Name: ______________ First Name: _______________ GR: ____Age: ____
School Attending: __________________________________________________• Last Name: ______________ First Name: _______________ GR: ____Age: ____
School Attending: __________________________________________________
* = Social Security Number Optional - (Refer to Registration Requirements Handout) Florida Statute 119.071(5) requires that we notify you of the purpose for collecting and utilizing your social security number (SSN). The SSN is being requested on this form for student records and reporting (1002.221 F.S.), cumulative student records (1003.25(1) F.S.), records of children in the voluntary prekindergarten education program (1002.72(1) F.S.), and student records – dropout prevention and academic intervention programs (1003.53(6) F.S.)
I am the parent/guardian of the child named above. The information on this form is true and accurate as of this date. I understand that falsification of information to achieve enrollment or assignment may be cause for revocation of the student’s enrollment or assignment to a school in the Leon County Public Schools. I understand that it is my responsibility as parent/guardian to keep this information current. I give permission for the information on this form to be reviewed and utilized by the staff of this school and by district personnel to assist in the provision of school health services, and be disclosed to relevant state agencies to facilitate the process of verifying current Medicaid eligibility (if applicable).
_____________________________________________________ ____________________________ Parent/Guardian Signature Date
Form Control No. LCS-9860-1055 Revised 1/24/18
“The Leon County School District does not discriminate against any person on the basis of race, color, ethnicity, national origin, religion, age, sex (including transgender, gender nonconforming, and gender identity), marital status, disability, pregnancy, sexual orientation, or genetic information.”
LCS Student Registration Form
FOR SCHOOL USE ONLY
LCS Student #_____________________ School: ________________________
Date: ___________________________ Birth Verification: ________________
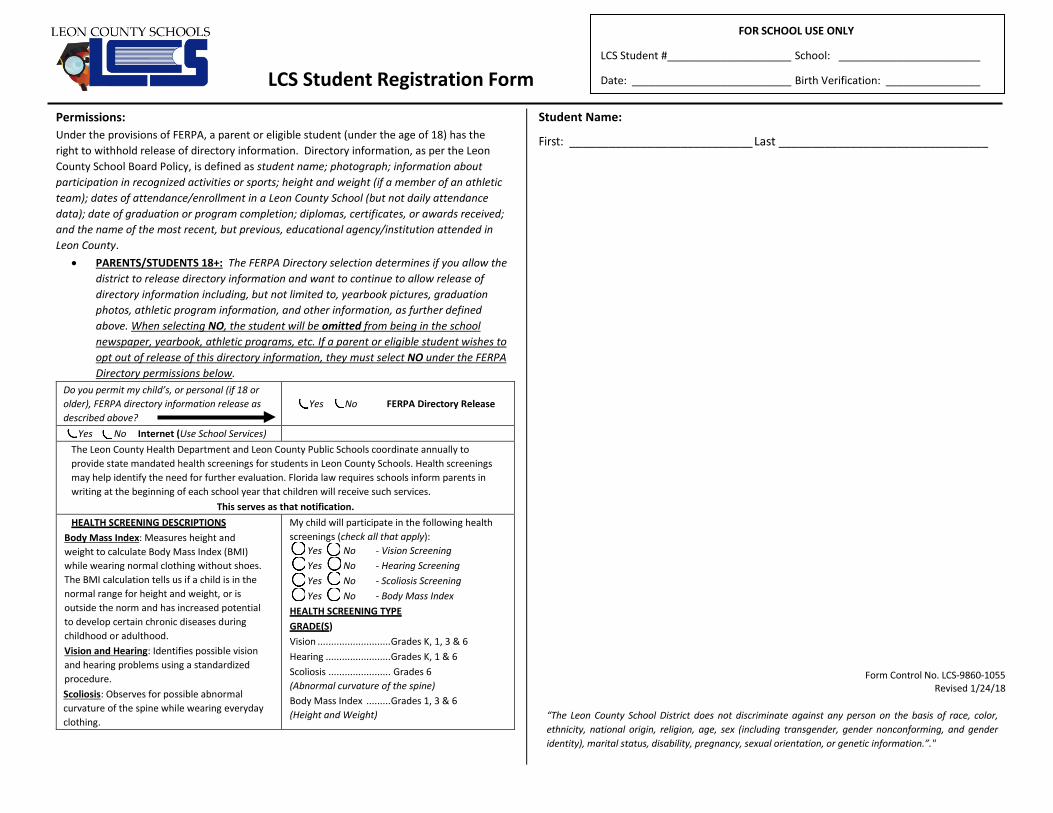
Permissions: Under the provisions of FERPA, a parent or eligible student (under the age of 18) has the right to withhold release of directory information. Directory information, as per the Leon County School Board Policy, is defined as student name; photograph; information about participation in recognized activities or sports; height and weight (if a member of an athletic team); dates of attendance/enrollment in a Leon County School (but not daily attendance data); date of graduation or program completion; diplomas, certificates, or awards received; and the name of the most recent, but previous, educational agency/institution attended in Leon County.
• PARENTS/STUDENTS 18+: The FERPA Directory selection determines if you allow thedistrict to release directory information and want to continue to allow release ofdirectory information including, but not limited to, yearbook pictures, graduationphotos, athletic program information, and other information, as further definedabove. When selecting NO, the student will be omitted from being in the schoolnewspaper, yearbook, athletic programs, etc. If a parent or eligible student wishes to opt out of release of this directory information, they must select NO under the FERPA Directory permissions below.
Do you permit my child’s, or personal (if 18 or older), FERPA directory information release as described above?
Yes No FERPA Directory Release
Yes No Internet (Use School Services) The Leon County Health Department and Leon County Public Schools coordinate annually to provide state mandated health screenings for students in Leon County Schools. Health screenings may help identify the need for further evaluation. Florida law requires schools inform parents in writing at the beginning of each school year that children will receive such services.
This serves as that notification. HEALTH SCREENING DESCRIPTIONS
Body Mass Index: Measures height and weight to calculate Body Mass Index (BMI) while wearing normal clothing without shoes. The BMI calculation tells us if a child is in the normal range for height and weight, or is outside the norm and has increased potential to develop certain chronic diseases during childhood or adulthood. Vision and Hearing: Identifies possible vision and hearing problems using a standardized procedure. Scoliosis: Observes for possible abnormal curvature of the spine while wearing everyday clothing.
My child will participate in the following health screenings (check all that apply):
Yes No - Vision Screening Yes No - Hearing Screening Yes No - Scoliosis Screening Yes No - Body Mass Index
HEALTH SCREENING TYPE GRADE(S) Vision ........................... Grades K, 1, 3 & 6 Hearing ........................ Grades K, 1 & 6 Scoliosis ....................... Grades 6 (Abnormal curvature of the spine) Body Mass Index ......... Grades 1, 3 & 6 (Height and Weight)
Student Name:
First: ____________________________ Last ________________________________
Form Control No. LCS-9860-1055 Revised 1/24/18
“The Leon County School District does not discriminate against any person on the basis of race, color, ethnicity, national origin, religion, age, sex (including transgender, gender nonconforming, and gender identity), marital status, disability, pregnancy, sexual orientation, or genetic information.”."

STUDENT'S
NAME______________________________GRADE_____TEACHER_________________________
1st-5th Grade Students - ACADEMIC INFORMATION from Parent/Guardian:
Welcome to W. T. Moore Elementary School.
* Please complete the following items and feel free to add additional information about your child on the back.
READING PROGRESS-Mark the item that best describes your child's reading progress.
___Excellent reader; was reading in above grade level materials
___Enjoys reading as leisure activity
___Good reader; completed the reading material for his/her grade level
___Had problems with reading
(Please describe)____________________________________________________________________________
MATH PROGRESS-Mark the item that best describes your child's math progress.
___Excellent progress; was working in above grade level materials
___Satisfactory progress; completed grade level materials
___Had problems with math
(Please describe)____________________________________________________________________________
WORK/STUDY HABITS-Mark the area that best describes your child's ability to work independently and
complete assignments.
___Excellent work/study habits
___Satisfactory work/study habits
___Needs to improve in work/study habits
(Please describe)____________________________________________________________________________
BEHAVIOR-Mark the item that best describes your child's behavior at school.
___Excellent ______Satisfactory ___Needs to improve
(Please describe)____________________________________________________________________________
SPECIAL PROGRAMS-Mark any programs in which your child was enrolled (if any)
___Chapter I Reading ___SLD ___Gifted ___Speech ___Other
(Please describe)___________________________________________________________________________
LIST BELOW OTHER STRENGTHS/PROBLEMS/CONCERNS YOU WOULD LIKE TO SHARE WITH US
WHICH WOULD AID IN MAKING THE MOST APPROPRIATE CLASS ASSIGNMENT FOR YOUR
CHILD:
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
__________________________________________________________________________________________
This form completed by (circle one) mother father guardian Name: ________________________________
Signature: _________________________________________________________________________________
Date: _____________________________________________________________________________________


Leon County Schools 2018-2019 EMERGENCY & MEDICAL INFORMATION
STUDENT INFORMATION To be completed by Parent/Guardian only. Use pen.
School__________________________________________
______________________________ __________________________ _______ ______________ ____/___/____ ________ Student’s Legal Last Name Student’s Legal First Name MI Nickname Birth Date Age ________ __________________________ _____________ ________________________ Grade Homeroom Teacher/First Period Sex/Race Student Social Security Number ______________________________________________________________________________________ Address/City/State/Zip ______________________________________________________________________________________ Mailing Address (If different from residence address above)
PARENT/GUARDIAN INFORMATION
_________________________________ _____________________ (h)_________________(w)________________(c)_____________ Mother’s Name Place of Employment Phone numbers
_________________________________ _____________________ (h)_________________(w)________________(c)_____________ Father’s Name Place of Employment Phone numbers
_________________________________ _____________________ (h)_________________(w)________________(c)_____________ Guardian’s Name (if applicable) Place of Employment Phone numbers
STUDENT LIVES WITH: Both Parents (same address) Mother Father Other _____________________ CUSTODY: ____________________________________________________________________________________________________________ (List any special custody arrangements. Appropriate legal documentation must be on file in a student’s cumulative folder) Siblings at this school: ________________________________________________________________________________________________
DOCTOR AND INSURANCE INFORMATION It is important that you provide information regarding your child’s
health conditions and health insurance to assist us in the case of an emergency.
_____________________________________ _____________________________________ _____________________ Doctor’s Name Address Telephone Number
_____________________________________ _____________________________________ _____________________ Specialist Doctor’s Name Address Telephone Number
HEALTH INSURANCE: Healthy Kids Acct#____________________________ Medicaid ID #__________________________
Other Insurance _____________________________________ Policy #____________________________
Children’s Medical Services Name of case manager: __________________________________________
None at this time.
HEALTH CONDITIONS (Diagnosed by a healthcare provider)
ALLERGIES (specify severity below) ASTHMA SEIZURES/EPILEPSY DIABETES ADD Medication Required?
insects medicine Mild Date of last seizure Type 1 Pump Home School food other_________ Moderate ______________ Pen
Requires EpiPen Severe ADHD Medication Required? Requires Benadryl/antihistamine Requires medication/inhaler Requires Diastat Type 2 Home School
available at school
Anemia Hearing Impairment Nosebleeds Transplant (specify below) Arthritis Hemophilia Physical Impairment Urological Conditions Cancer (specify below) Heart Disease/Murmur (specify below) Pregnancy Other (specify below) Cerebral Palsy High Blood Pressure Psychological Disorder (specify below) Religious Restrictions Cystic Fibrosis Hypoglycemia Scoliosis ESE (specify below) Ear Infections (repeated) Kidney Disease Sickle Cell Disease (exceptional student education) Emotional Difficulties (specify below) Leukemia Sickle Cell Trait Gastrointestinal Condition Muscular Dystrophy Skin Condition (specify below) None Known Headaches (specify below) Motor Impairment Speech Impairment
Religious restrictions (specify):_____________________________________________________________________________________________ Specify severity of health conditions/Specify restrictions on activity and any accommodations needed while at school: _________________________________________________________________________________________________________________________________ __________________________________________________________________________________________________________________________
List all medications (prescription and non-prescription, including “as needed” and emergency meds) that student takes
AT HOME:_________________________________________________________________________________________________________________
AT SCHOOL:_______________________________________________________________________________________________________________
****TURN FORM OVER TO COMPLETE – Signatures Needed on Back**** Rev. 2/18
Transportation from School After School Care Car Pick Up Van Carpool Walk’s With _____________ Bike Drive Bus # _________ Day Care Name_______________
L
as
t Na
me
, F
irst N
am
e
Fo
r Office U
se On
ly.

The Leon County Health Department and Leon County Public Schools coordinate annually to provide state mandated health screenings for students in Leon County Schools. Health screenings may help identify the need for further evaluation. Florida law requires that parents be informed in writing at the beginning of each school year that children will receive such services. This serves as that notification.
If no box is checked, your child will be screened.
HEALTH SCREENING DESCRIPTIONS Vision and Hearing: Identifies possible vision and hearing problems using a standardized procedure. Scoliosis: Observes for possible abnormal curvature of the spine while wearing everyday clothing. Body Mass Index: Measures height and weight to calculate Body Mass Index (BMI) while wearing normal clothing without shoes. The BMI calculation tells us if a child is in the normal range for height and weight, or is outside the norm and has increased potential to develop certain chronic diseases during childhood or adulthood.
HEALTH SCREENING TYPE GRADE(S) Vision Grades K, 1, 3 & 6 Hearing Grades K, 1 & 6 Scoliosis (Abnormal curvature of the spine) Grades 6 Body Mass Index (Height and Weight) Grades 1, 3 & 6
I do not want my child to participate in the following health screenings (check all that apply):
Vision Screening Hearing Screening Scoliosis Screening Body Mass Index
___________________________________________ _____________________
Parent Signature Date
EMERGENCY CONTACTS and PARENTAL CONSENT
Child Pickup/Emergencies: Should my child become ill or injured during the school day and the school is unable to contact me, I hereby give the school permission to contact one or more of the following persons to pick up my child at school and care for my child during my absence. (Must be at least 18 years of age.)
1._______________________/_______________________/_____________ 3._______________________/_______________________/____________ Name Relationship Telephone Name Relationship Telephone 2._______________________/_______________________/_____________ 4.______________________/_______________________/_____________ Name Relationship Telephone Name Relationship Telephone
In case of accident or serious illness during the school day, I request that the school contact me. In case of an emergency, I hereby give the school permission for my child to be transported by Emergency Medical Services to the hospital and given the necessary treatment. All students will receive care for injuries and emergencies. I understand that I will be responsible for any and all related charges. I understand that it is the parent’s/guardian’s responsibility to notify the school of any change in this information throughout the school year.
_____________________________________________ _____________
Parent/Guardian Signature Date Leon County Schools relies on Medicaid reimbursements to support the delivery of health care services in clinics throughout the school district. By signing below you are giving Leon County Schools permission to utilize information contained on this form that is required by the Agency for Health Care Administration in order to verify Medicaid eligibility. In addition, you are giving permission for Leon County Schools to access your child’s public benefits to pay a share of the cost for services provided as referenced in the child’s Individual Educational Plan (if applicable). At no time will you be required to incur out of pocket expenses for these services regardless of your child’s Medicaid eligibility status. Any personally identifiable information about your child will not be disclosed to any other organization for any purpose except what has been noted above.
______________________________________________ _____________ Parent/Guardian Signature Date
Rev. 2/18
HEALTH SCREENINGS
La
st N
am
e,
F
irst N
am
e
Fo
r Offic
e U
se
On
ly
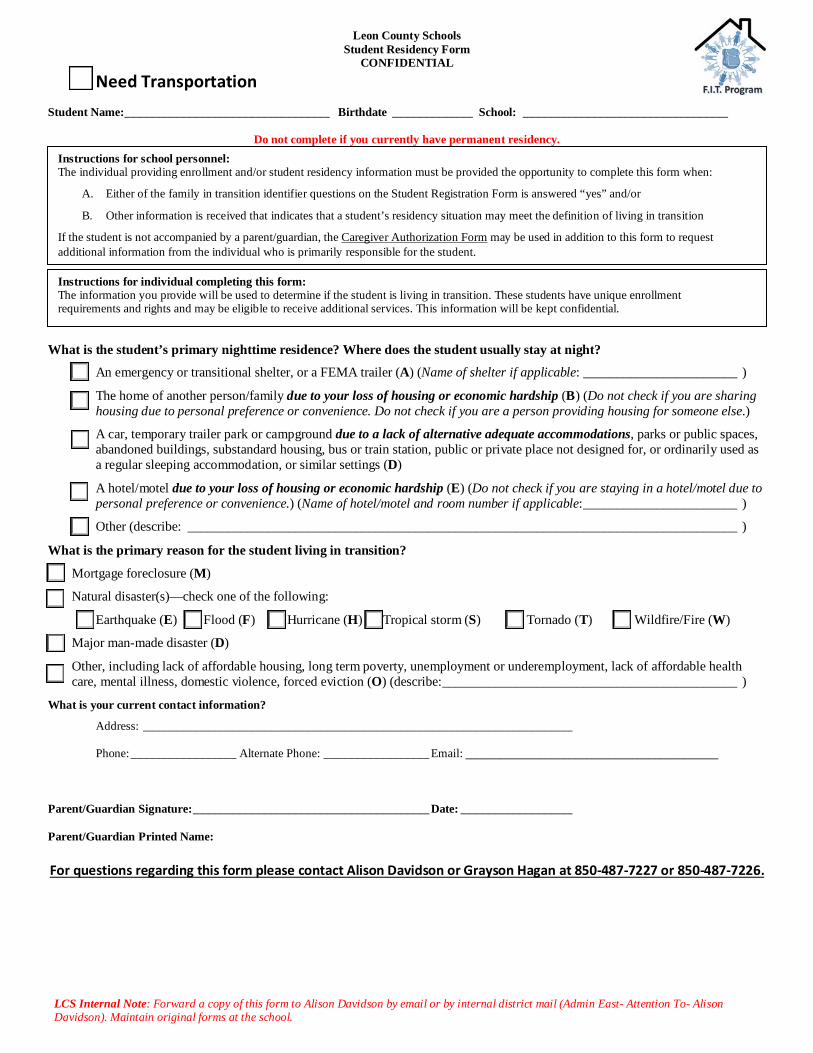
Leon County Schools Student Residency Form
CONFIDENTIAL
LCS Internal Note: Forward a copy of this form to Alison Davidson by email or by internal district mail (Admin East- Attention To- Alison Davidson). Maintain original forms at the school.
Need Transportation Student Name:_________________________________ Birthdate _____________ School: _________________________________
Do not complete if you currently have permanent residency.
What is the student’s primary nighttime residence? Where does the student usually stay at night?
An emergency or transitional shelter, or a FEMA trailer (A) (Name of shelter if applicable: _______________________ )
The home of another person/family due to your loss of housing or economic hardship (B) (Do not check if you are sharing housing due to personal preference or convenience. Do not check if you are a person providing housing for someone else.)
A car, temporary trailer park or campground due to a lack of alternative adequate accommodations, parks or public spaces, abandoned buildings, substandard housing, bus or train station, public or private place not designed for, or ordinarily used as a regular sleeping accommodation, or similar settings (D)
A hotel/motel due to your loss of housing or economic hardship (E) (Do not check if you are staying in a hotel/motel due to personal preference or convenience.) (Name of hotel/motel and room number if applicable: _______________________ )
Other (describe: __________________________________________________________________________________ )
What is the primary reason for the student living in transition?
Mortgage foreclosure (M)
Natural disaster(s)—check one of the following:
Earthquake (E) Flood (F) Hurricane (H) Tropical storm (S) Tornado (T) Wildfire/Fire (W)
Major man-made disaster (D)
Other, including lack of affordable housing, long term poverty, unemployment or underemployment, lack of affordable health care, mental illness, domestic violence, forced eviction (O) (describe: ____________________________________________ )
What is your current contact information?
Address: _____________________________________________________________________ Phone: _________________ Alternate Phone: _________________ Email: ____________________________________________ Parent/Guardian Signature: ______________________________________ Date: __________________ Parent/Guardian Printed Name: For questions regarding this form please contact Alison Davidson or Grayson Hagan at 850-487-7227 or 850-487-7226.
Instructions for school personnel: The individual providing enrollment and/or student residency information must be provided the opportunity to complete this form when:
A. Either of the family in transition identifier questions on the Student Registration Form is answered “yes” and/or
B. Other information is received that indicates that a student’s residency situation may meet the definition of living in transition
If the student is not accompanied by a parent/guardian, the Caregiver Authorization Form may be used in addition to this form to request additional information from the individual who is primarily responsible for the student.
Instructions for individual completing this form: The information you provide will be used to determine if the student is living in transition. These students have unique enrollment requirements and rights and may be eligible to receive additional services. This information will be kept confidential.
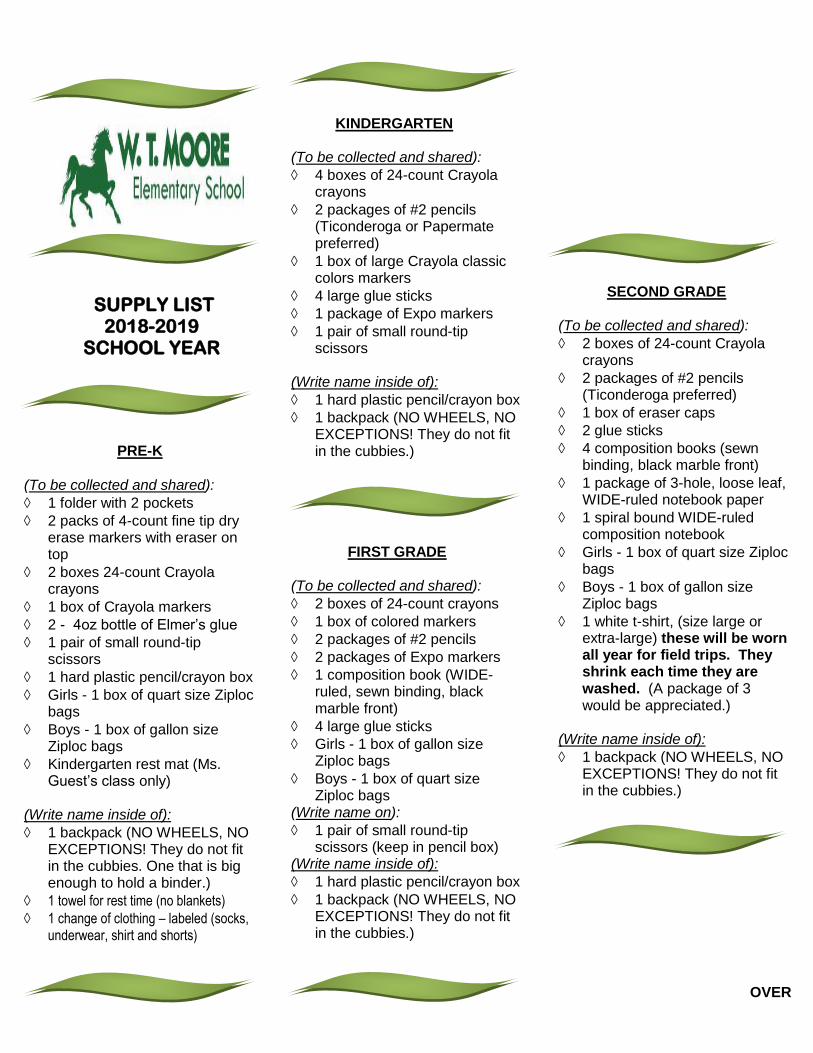
SUPPLY LIST 2018-2019
SCHOOL YEAR
PRE-K
(To be collected and shared):
1 folder with 2 pockets
2 packs of 4-count fine tip dry erase markers with eraser on top
2 boxes 24-count Crayola crayons
1 box of Crayola markers
2 - 4oz bottle of Elmer’s glue
1 pair of small round-tip scissors
1 hard plastic pencil/crayon box
Girls - 1 box of quart size Ziploc bags
Boys - 1 box of gallon size Ziploc bags
Kindergarten rest mat (Ms. Guest’s class only)
(Write name inside of):
1 backpack (NO WHEELS, NO EXCEPTIONS! They do not fit in the cubbies. One that is big enough to hold a binder.)
1 towel for rest time (no blankets)
1 change of clothing – labeled (socks, underwear, shirt and shorts)
KINDERGARTEN
(To be collected and shared):
4 boxes of 24-count Crayola crayons
2 packages of #2 pencils (Ticonderoga or Papermate preferred)
1 box of large Crayola classic colors markers
4 large glue sticks
1 package of Expo markers
1 pair of small round-tip scissors
(Write name inside of):
1 hard plastic pencil/crayon box
1 backpack (NO WHEELS, NO EXCEPTIONS! They do not fit in the cubbies.) FIRST GRADE
(To be collected and shared):
2 boxes of 24-count crayons
1 box of colored markers
2 packages of #2 pencils
2 packages of Expo markers
1 composition book (WIDE-ruled, sewn binding, black marble front)
4 large glue sticks
Girls - 1 box of gallon size Ziploc bags
Boys - 1 box of quart size Ziploc bags
(Write name on):
1 pair of small round-tip scissors (keep in pencil box)
(Write name inside of):
1 hard plastic pencil/crayon box
1 backpack (NO WHEELS, NO EXCEPTIONS! They do not fit in the cubbies.)
SECOND GRADE
(To be collected and shared):
2 boxes of 24-count Crayola crayons
2 packages of #2 pencils (Ticonderoga preferred)
1 box of eraser caps
2 glue sticks
4 composition books (sewn binding, black marble front)
1 package of 3-hole, loose leaf, WIDE-ruled notebook paper
1 spiral bound WIDE-ruled composition notebook
Girls - 1 box of quart size Ziploc bags
Boys - 1 box of gallon size Ziploc bags
1 white t-shirt, (size large or extra-large) these will be worn all year for field trips. They shrink each time they are washed. (A package of 3 would be appreciated.)
(Write name inside of):
1 backpack (NO WHEELS, NO EXCEPTIONS! They do not fit in the cubbies.) OVER

THIRD GRADE
(To be collected and shared):
4 package of #2 pencils
1 package of 3-hole, loose leaf, WIDE-ruled notebook paper
2 glue sticks
2 dry erase markers
1 ream of copy paper
Girls - 1 box of quart size Ziploc bags
Boys - 1 box of gallon size Ziploc bags
(Write name on outside of):
1 box of 24-count crayons or
1 box of 12-count pre-sharpened color pencils
1 one-inch 3-ring binder
2 composition books (sewn binding, black marble front)
scissors (keep in pencil case)
3 PLAIN 2-pocket, 3 prong folders, one each: red, blue, green
(Write name inside of):
1 hard plastic pencil box
1 backpack (NO WHEELS, NO EXCEPTIONS! They do not fit in the cubbies.)
FOURTH GRADE
(To be collected and shared):
1 box of 24-count crayons
48 (or more) #2 pencils with erasers, pre-sharpened, if possible
1 box of 12-count pre-sharpened color pencils
2 - 4-pack of fine tip dry erase markers
5 composition books (sewn binding, black marble front)
1 package of 3-hole, loose leaf, notebook paper
1 box of gallon size Ziploc bags
5 – 3-prong folders with pockets (Blue, Green, Red, Yellow and Purple)
1 pack of pencil erasers (Write name inside of):
1 backpack (NO WHEELS, NO EXCEPTIONS! They do not fit in the cubbies.)
FIFTH GRADE
(To be collected and shared):
1 box of 12-count pre-sharpened color pencils
4 packages of #2 pencils (Ticonderoga preferred)
scissors
2 boxes of eraser caps
4 glue sticks
Expo markers
4 composition notebooks (sewn binding, black marble front)
1 pack of plastic dividers with pockets
Girls - 1 box of quart size Ziploc bags
Boys - 1 box of gallon size Ziploc bags
(Write name inside of):
1 - 2-inch Heavy Duty 3 Ring View Binder (no fabric or zipper binders)
zippered SOFT binder pencil case with clear view window (no boxes)
1 backpack (NO WHEELS, NO EXCEPTIONS! They do not fit in the cubbies.)