well woman care: overview and updates well woman.pdf · menopause – may include complementary...
TRANSCRIPT

WELL WOMAN CARE:
OVERVIEW AND UPDATES
© 2015 PLEASE NOTE THAT THESE SLIDES ARE POSTED ONLY FOR REFERENCE BY WORKSHOP
PARTICIPANTS. ANY ADDITIONAL USE IS PROHIBITED UNLESS EXPLICIT PERMISSION IS OBTAINED.
Workshop presenter:
Hilary Schlinger, CNM, MS

WHY MIDWIVES?
Applying the Midwifery Model to Women’s Health
Approach to Care:
Education focus
Individualized attention
Holistic
Integrative/complementary
Non-judgmental
Cultural sensitivity
“With Women” – Intimate with intimacy
Sensitivity to abuse issues

WELL EXAM
General Health Parameters
Vitals, Physical Exam
Laboratory Testing
Based on Symptoms, History, Age
Other Screening
Based on Symptoms, History, Family History, Age
and Personal Decision-making
Breast Exam

WELL EXAM
The Well-Woman Examination:
Choosing the proper speculum
&
Performing a bimanual exam

VAGINAL SPECULUMS
Graves: Wide, “duck-billed”
Pederson: Narrow, straight sides
Metal or plastic; reusable vs disposable
Multiple lengths and widths available
SELECTING A SPECULUM
Graves Postpartum
Multiparous woman
Known laxity of vaginal musculature
During procedure, such as IUD insertion
Pederson (medium width) Routine well-woman exam
Narrow Pederson Young woman; 1st exam; naïve to penetration
Post-menopausal woman

GRAVES SPECULA

PEDERSON SPECULA
VISUAL EXAMINATION
Examine the external genitalia for:
Warts
Other lesions
Visible prolapse
Discharge
Internal skin color
Hemorrhoids
Lichensclerosis
INSERTING THE SPECULUM
Tilt the handle to one side
Angle downward toward coccyx
Slowly rotate handle downward during insertion
Wait to feel a “give” when beyond the vaginal muscles
Slowly open by raising upper blade
Obtain desired specimen(s)
Remove by “reverse” of above

SUGGESTIONS FOR AN EASIER EXAM
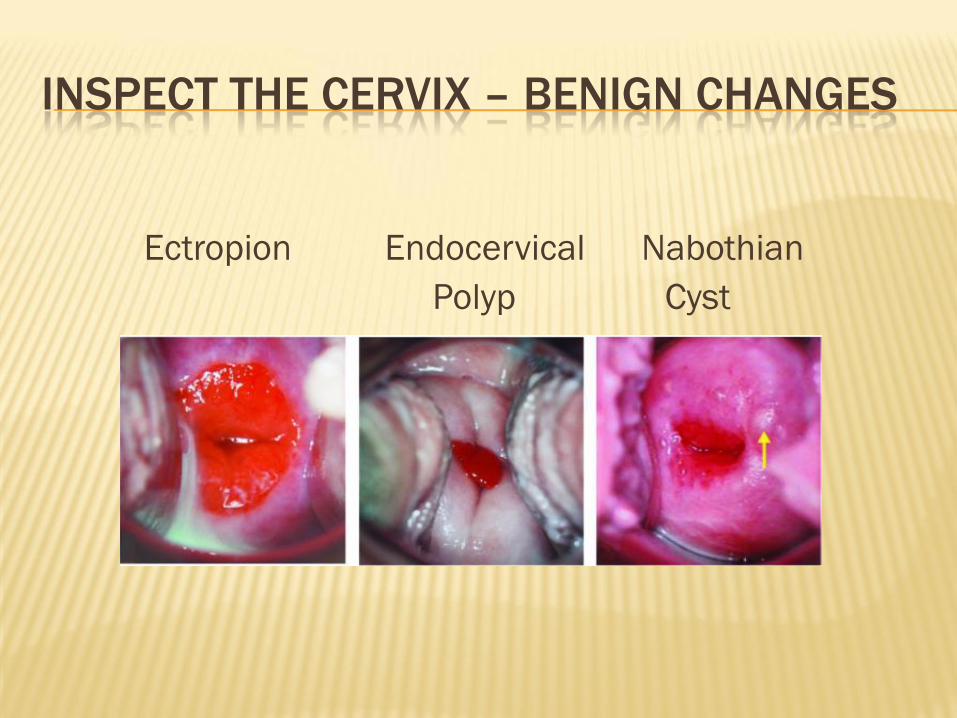
INSPECT THE CERVIX – BENIGN CHANGES
Ectropion Endocervical Nabothian
Polyp Cyst
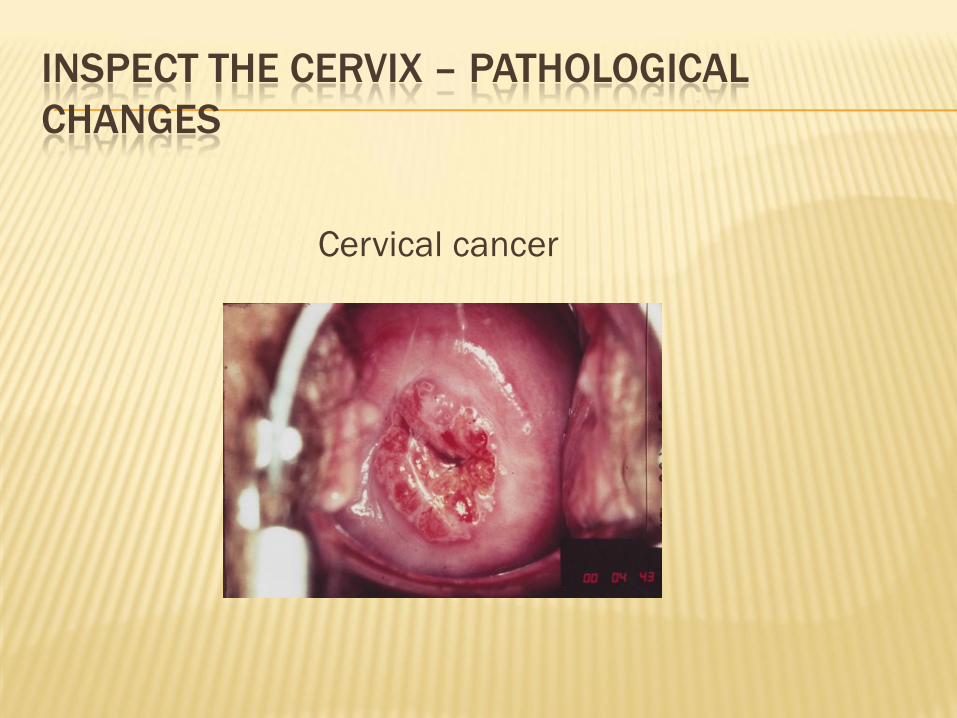
INSPECT THE CERVIX – PATHOLOGICAL
CHANGES
Cervical cancer

OBTAIN PAP AND CULTURES
Broom, spatula/brush, or broom/brush?
Broom alone adequate with pre-menopausal women
due to lower transformation zone
Some studies support broom/brush combination for
use in older women with higher TZ
ThinPrep or SurePath?
Either can be used for Pap, HPV, and/or CT/GC
ThinPrep: +Trichomonas
SurePath higher cell yield, so may be superior for
menopausal women with scant cellularity
Check with your lab for acceptable lubricants

BIMANUAL EXAMINATION
Use two lubricated, gloved fingers
Place fingertips behind cervix
Place external hand above pubic bone
Gently lift cervix
Palpate uterus “between” hands
Assess for position, size, shape, firmness,
mobility, tenderness or pain on palpation

BIMANUAL EXAMINATION
Palpating the uterus

UTERINE POSITION
Anteverted – majority of women

UTERINE POSITION
Anteflexed

UTERINE POSITION
Retroverted

UTERINE POSITION
Retroflexed

PALPATE THE OVARIES
Move your internal fingertips to one side, into the adnexal area
Using your external hand, push gently downward
Sweep hands toward pubic bone
Ovary will “slip” between your fingertips; the ovary is palpated by the internal fingers
Repeat on the other side

PALPATING THE OVARIES
Position of the ovaries:
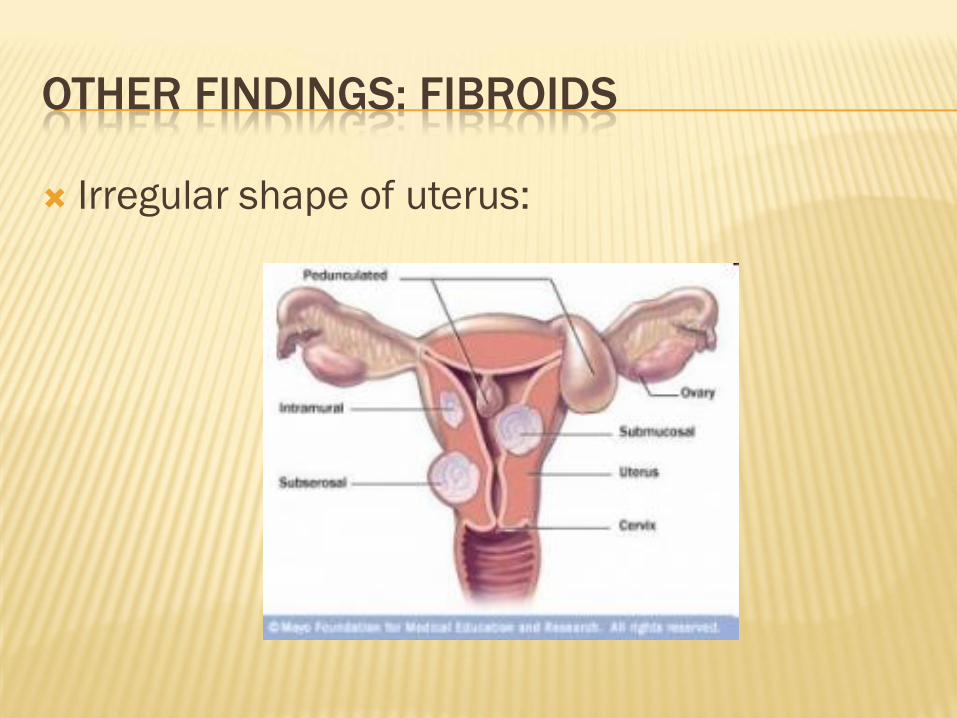
OTHER FINDINGS: FIBROIDS
Irregular shape of uterus:

OTHER FINDINGS: PID
Tenderness or Pain on Palpation
Discharge
Causative organisms
Most Common: Chlamydia or Gonorrhea
Mycoplasma
BV may contribute
Treatment
IM + PO outpatient vs in-hospital txt
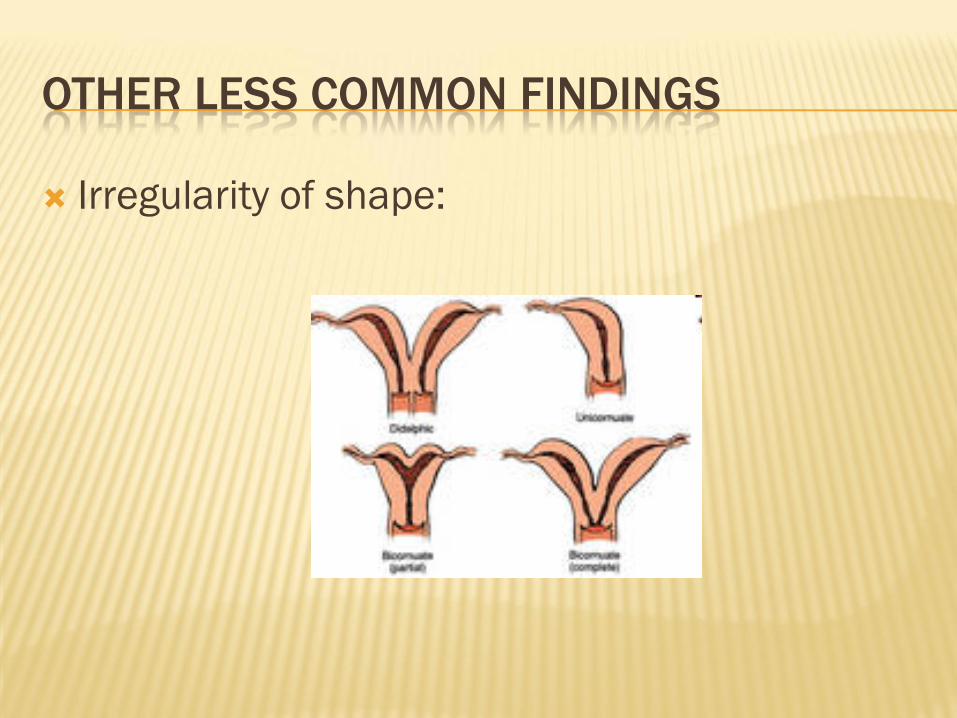
OTHER LESS COMMON FINDINGS
Irregularity of shape:

PAP – THE NEXT GENERATION OF GUIDELINES
Pap Smears
Interpretation and Action
PAP SMEAR – CERVICAL CYTOLOGY
Screening for cervical cell changes Cancerous changes; abnormal cells
Inflammation
Infection
Bethesda System for reporting of results
Performed via speculum exam; brush & spatula OR broom OR broom & brush
Liquid-Based Cytology:
Not proven to be more accurate, however
can also be used for HPV + other STIs

BETHESDA SYSTEM
Satisfactory or Unsatisfactory?
Endocervical component present?
No cell abnormalities:
Reported as Negative for Intraepithelial Lesion
or Malignancy
SQUAMOUS CELLS
Thin, flat cells that form the surface of the
cervix
Squamous cell abnormalities
ASC-US – most common abnormal pap result
LSIL
HSIL
ASC-H
Squamous cell carcinoma
SQUAMOUS CELL ABNORMALITIES
Dysplasia and Cervical Intraepithelial Neoplasm
(CIN) – describe the actual cell changes
CIN 1 – mild dysplasia
Usually resolves on its own
CIN 2 – moderate dysplasia
CIN 3 – severe dysplasia

GLANDULAR CELLS
Mucus-producing cells found in the endocervical canal
Glandular cell abnormalities:
AGC—atypical glandular cells
AIS—endocervical adenocarcinoma in situ
Adenocarcinoma
Glandular cell abnormalities much less common than squamous cell abnormalities
PAP SMEAR
Speculum exam and pap are performed prior to
a bimanual exam
Best time for a pap:
Day 10-20 of cycle;
When not menstruating;
Has not douched, used vaginal creams or
spermicides for 48 hours;
Has not had a tampon in for 48 hours

WHO SHOULD HAVE A PAP?
ASCCP Updated Guidelines of 2012:
First pap at age 21 – Women younger than 21 should not be screened regardless of risk factors
Age 21 - 29:
Screening pap every 3 years; reflex AS-CUS to HPV
Age 30 - 65 with no history of CIN
Screening pap + HPV-HR “Co-testing” every 5 years (preferred ) – fewer colposcopies/sl. lower cancer rate
OR Screening pap every 3 years
PAP SMEAR TIMING
Not “Annual” Anymore:
Annual screening for low-risk groups result in twice the rate of colposcopies with only slightly greater cancer risk reduction
More intensive or alternative screening for:
Women with HIV
Women with immunosuppression
DES-daughters
Women with a history of CIN 2, CIN 3 or cervical cell carcinoma
WHO CAN STOP HAVING PAPS?
Women whom have had a hysterectomy for
non-cancerous reasons
Women aged 65 or more with:
At least 3 consecutive negative Paps
OR 2 consecutive cotests in the past 10 years
And adequate screening with no history of CIN 2+
for past 20 years
With most recent screening within past 5 years

CIN 2, CIN 3 OR CANCER DIAGNOSIS
These women remain at risk for persistent or
recurrent disease for at least 20 years
Screening for 20 years, even in the event of
hysterectomy or beyond age 65

HPV
HPV: a group of >150 viruses
Some types cause warts, including genital warts – although those which cause genital warts are NOT those associated with cervical cancer
Approximately 15 types are referred to as “high-risk”: i.e. they are more likely to cause cancerous changes in cervical cells

HPV TESTING
Age 21-30: reflex testing for ASC-US
Age >30: offer HPV-HR cotesting
regardless of diagnosis every 5 years
OR reflex testing, either for ASC-US or any
abnormality on pap, with pap every 3 yrs
Decision-making will be determined by
both pap and HPV result

NEGATIVE HPV DNA TEST
Offers better predictive value after 6 years
than a negative pap does after 3 years
Rates of CIN 3+ with neg HPV vs neg Pap:
Pap: 3 yrs: 0.51%; 4 yrs: 0.69%; 5 yrs: 0.83%;
6 yrs: 0.97%
HPV: 3 yrs: 0.12%; 4 yrs: 0.19%; 5 yrs:0.25%;
6 yrs: 0.27%

HPV GENOTYPE-SPECIFIC TESTING
Why do typing?
Assessing risk
HPV 16 – Highest risk of CIN 3+ of any HR type
HPV 18 – Associated with adenocarcinomas
HPV High-Risk Other – lower risk of future
CIN3+ than 16 or 18

PAP, HPV, OR PAP + HPV?
20,810 Women followed for up to 10
years
Negative Predictive Value for CIN 3 after
45 months:
Pap alone 99.47
HPV DNA 99.76
Pap + HPV 99.84
NEGATIVE PAP WITH POSITIVE HPV
Occurred in 4% of cases overall
Cumulative incidence of CIN 3+ 3% after 39 months
5% after 120 months
Selected group of HPV 16/18 positive 12% CIN 3+ after 39 months
21% CIN 3+ after 10 years if HPV 16+
17% CIN 3+ after 10 years if HPV 18+
2% CIN 3+ after 10 years non 16/18+

NEGATIVE PAP WITH POSITIVE HPV
Management options include:
Repeat pap and HPV in 1 year; OR
Immediate HPV 16/18 assay, if available
Cotesting in one year:
If positive on either test: Refer for colposcopy
If negative: Return to routine screening
16/18 genotyping
If 16/18 positive: refer for colposcopy
If 16/18 negative: Repeat pap + HPV in 1 year

NEGATIVE PAP WITH POSITIVE HPV
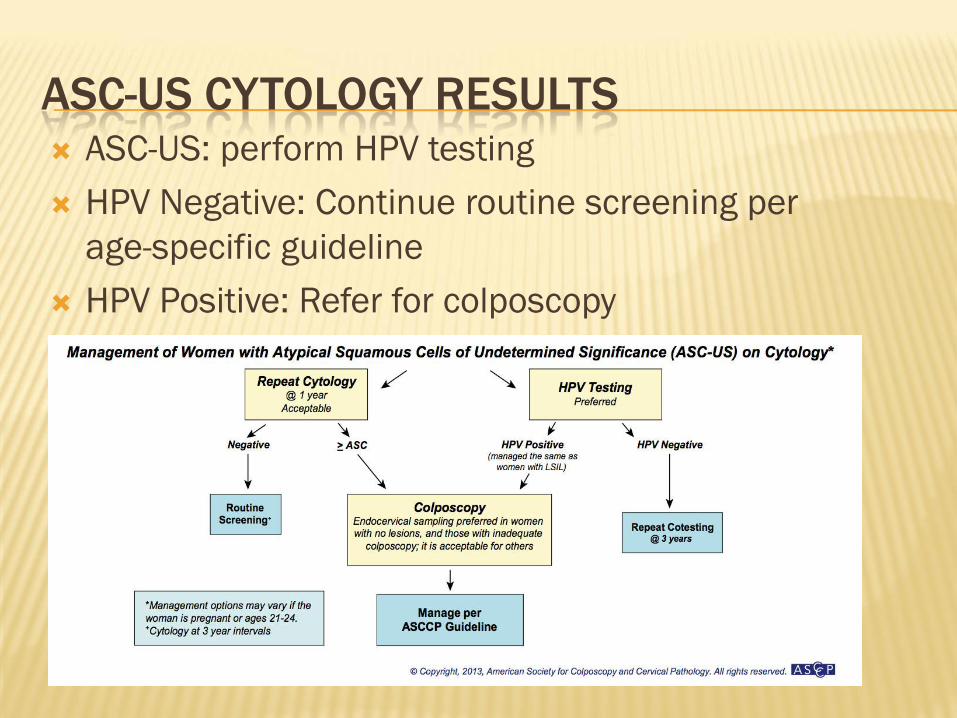
ASC-US CYTOLOGY RESULTS ASC-US: perform HPV testing
HPV Negative: Continue routine screening per
age-specific guideline
HPV Positive: Refer for colposcopy

YOUNG WOMEN AND HPV
2007 survey: 24.5% of those aged 14-19 were
positive for HPV, and 17.6% positive for high-
risk HPV
44.8% of women aged 20-24 tested positive for
HPV; 28% positive for high-risk HPV
Conclusion: adolescents and young women
acquire HPV efficiently

YOUNG WOMEN AND HPV
Young women are also very efficient at clearing
the infection
Median duration of HPV infection in one study
was 8 months
70% no longer infected by 12 months
81% no longer infected by 24 months
0.1% rate of cervical cancer in adolescents
(~1/1,000,000)

YOUNG WOMEN
Young women (age 21-24) with ASC-US or LSIL:
Reflex HPV for ASC-US only; OR
Repeat cytology in 12 months (preferred)
If negative, ASC-US or LSIL, repeat pap again in 12
months
If negative, return to routine screening
If ASC-US or higher, rec. colposcopy
If HSIL, recommend colposcopy

YOUNG WOMEN 21-24

DECISION-MAKING TREE
ASC-H: Recommend colposcopy
No CIN 2 or 3: repeat pap @ 6 & 12 mo OR
HPV DNA testing at 12 months
If any pap abnormality or + HPV, repeat
colposcopy
If negative, return to routine screening

DECISION-MAKING TREE
LSIL: Recommend colposcopy
No CIN 2 or 3: repeat pap @ 6 & 12 mo OR HPV
DNA testing at 12 months
If any pap abnormality or + HPV, repeat colposcopy
If negative, return to routine screening
CIN 2 or 3: Diagnostic excisional procedure

DECISION-MAKING TREE
HSIL:
Immediate Loop Electrosurgical Excision (LEEP) or
Colposcopy with endocervical assessment
If no CIN 2 or 3, either observation with
colposcopy and pap at 6 & 12 months OR
diagnostic excisional procedure

ABNORMAL PAP IN PREGNANCY
ASC-US & HPV+ or LSIL – 2 options: Colposcopy without endocervical sample
No CIN 2 or 3: Postpartum follow-up
CIN 2 or 3: consider least-invasive excisional procedure
Defer colposcopy until at least 6 wks postpartum
HSIL or ASC-H: Colposcopy without endocervical sample
(as above)
DIAGNOSTIC PROCEDURES
Biopsy
Endocervical Sampling
Endometrial Sampling
LEEP – Loop Electrosurgical Excision Procedure
Cone Biopsy
Cryotherapy (freezing)
Laser treatment
Differential Diagnosis of Vaginal Infections

VAGINITIS
Inflammation of the vagina
A change in microbial balance:
Use of antibiotics
Change in hormones due to pregnancy, breastfeeding or menopause
Douching
Spermicide or lubricant use
Sexual intercourse
Infection

COMMON VAGINAL INFECTIONS
Yeast - Candida
Bacterial Vaginosis (BV)
Trichomonas
Less common:
Ureaplasma or Mycoplasma infection

DIAGNOSIS OF VAGINAL INFECTIONS
Discharge – appearance Normal: White, creamy
Yeast: White, curdy
BV: Thin, white/gray, adherent
Trich: yellow/green, frothy
pH Normal: 3.8-4.2
Yeast: <4.5
BV & Trich: >4.5
DIAGNOSIS OF VAGINAL INFECTIONS
Amine Odor (KOH “whiff test”) Normal: absent
Yeast: absent
BV & Trich: fishy
Microscopy Normal: epithelial cells, lactobacilli
BV: clue cells; no WBCs & no lactobacilli
Trich: trichomonads; WBCs
Yeast: w/KOH: hyphae, buds
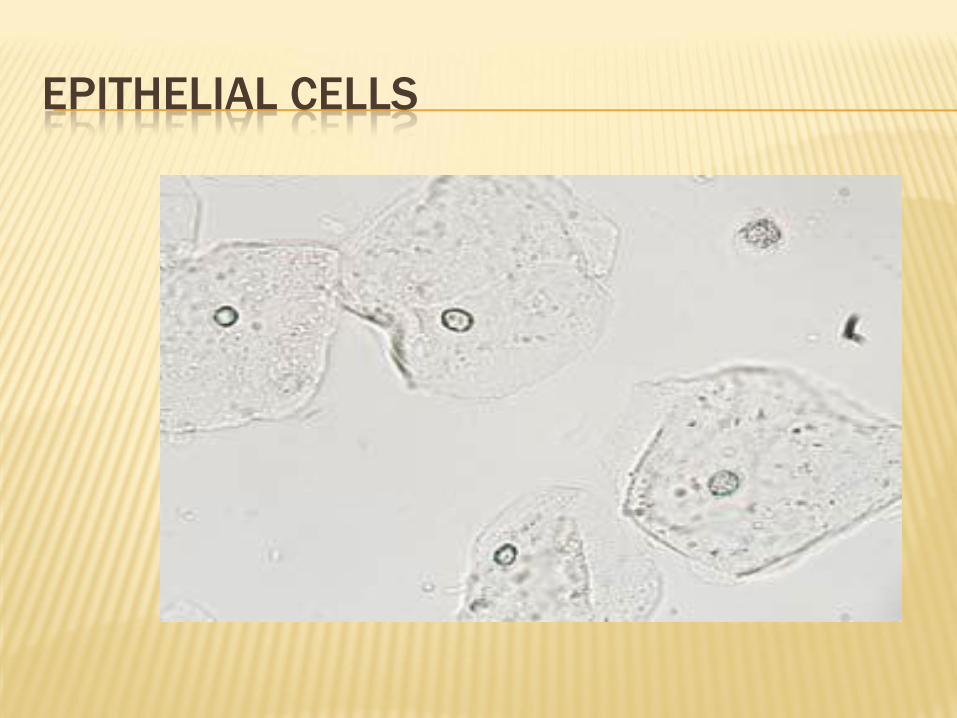
EPITHELIAL CELLS
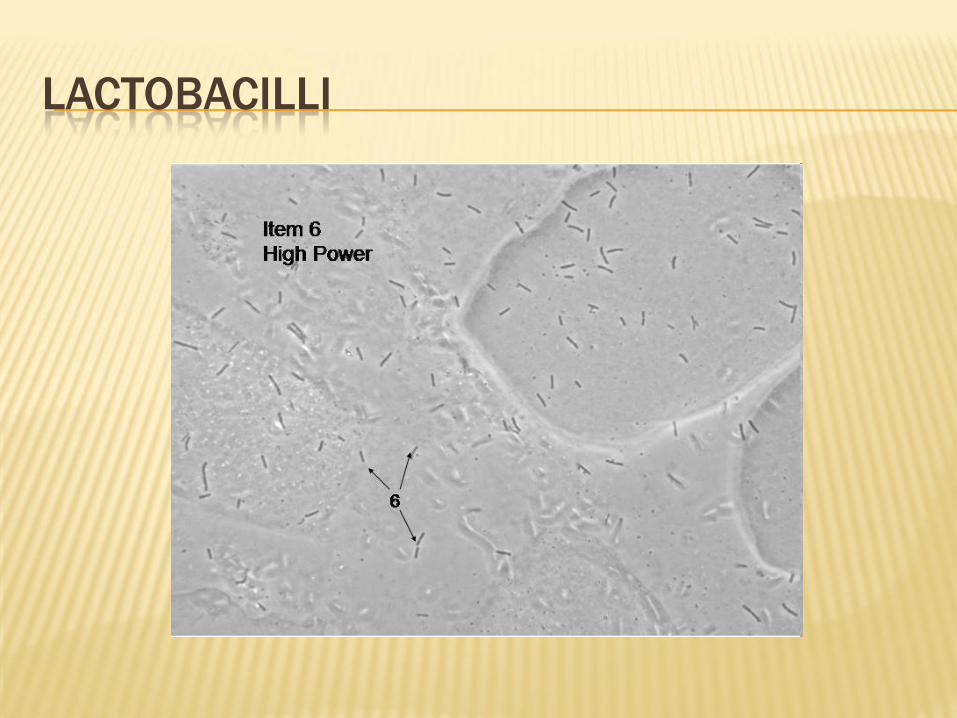
LACTOBACILLI

RED AND WHITE BLOOD CELLS

YEAST

YEAST

BV – CLUE CELL

BV – CLUE CELL

TRICHOMONAS
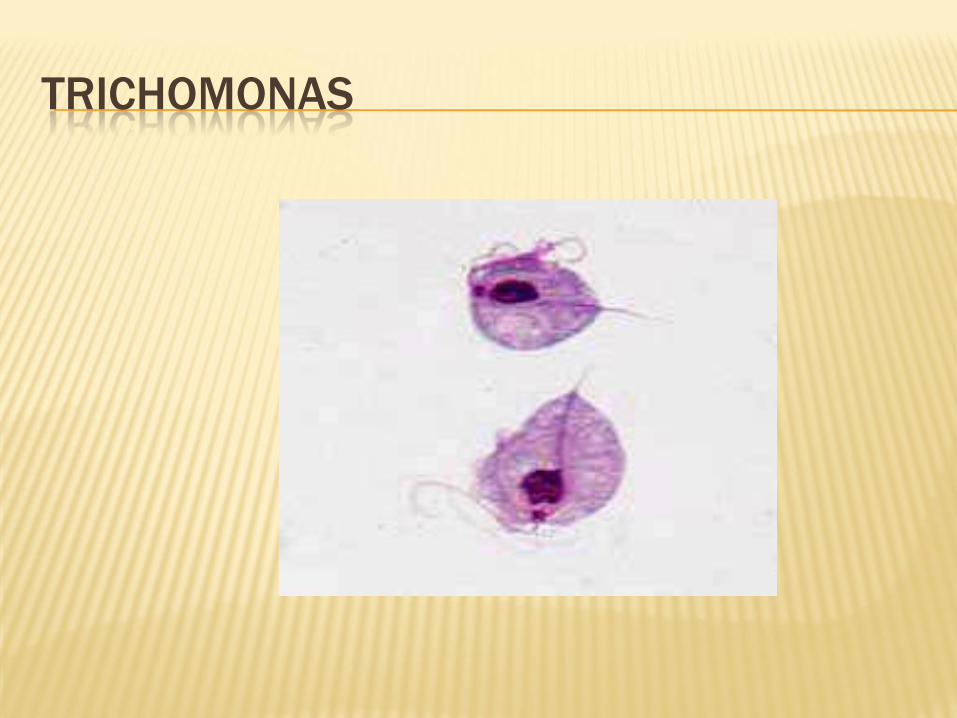
TRICHOMONAS

OVERVIEW
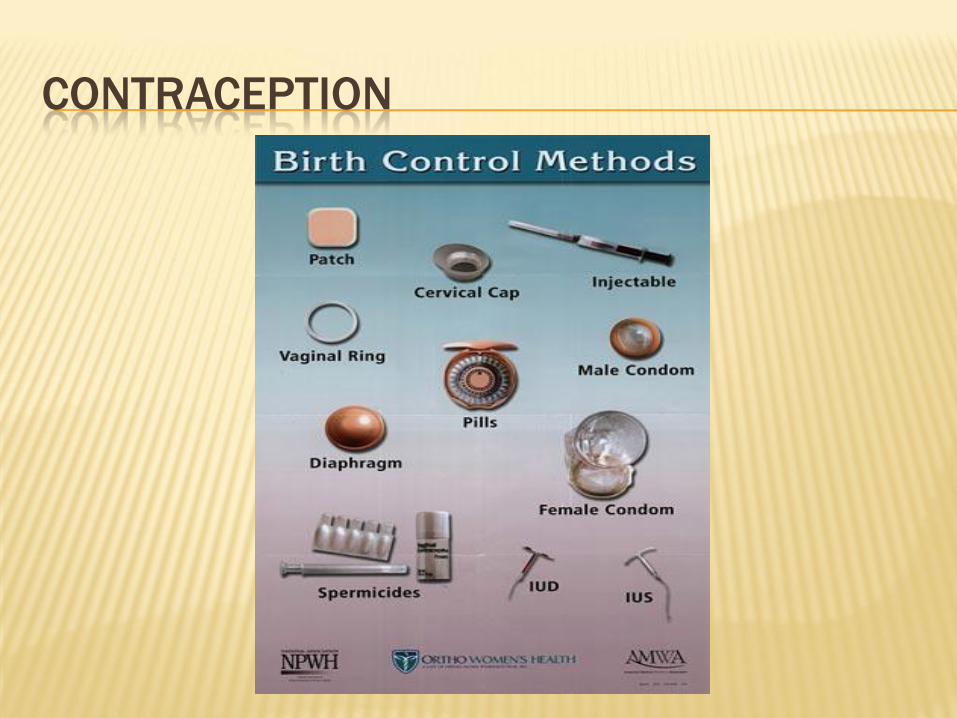
CONTRACEPTION

CONTRACEPTION
Hormonal Contraceptives:
Progestin-only:
Implantable – Mirena & Skyla IUD, Nexplanon
Injectable – DepoProvera
POP - “Mini Pill”
Combined Estrogen & Progestin:
COC – “The Pill”
Nuva Ring
Evra Patch
CONTRACEPTION
Non-Hormonal:
Barrier Methods:
Diaphragm
FemCap
Condoms – Male and Female
Withdrawl
Spermicides
Copper IUD (Paragard)
Natural Family Planning
Lactation Amenorrhea

“MORNING AFTER”
Progestin-only
Plan B
RX vs pharmacist-prescribed vs OTC
Progesterone Receptor Modulator
Ulipristal: ella
Limited availability at this time
Paragard (copper IUD) insertion
Highest efficacy – within 5 days of sexual intercourse

CONTRACEPTIVE EFFECTIVENESS
BRANCHING OUT – AREAS OF EXPERTISE
Menopause – may include complementary
therapies or Bio-HRT
Transgender care – may include hormone
therapy
Herbal consultations for specific health issues
Adrenal fatigue, Hypothyroidism, Chronic fatigue
Adolescent and teen health