with ca-7, a fibrinolytic enzyme from aspergillus orysae
TRANSCRIPT
762 Perry: CA-7: A Fibrinolytic Enzyme Canad. Med. Ass. J.April 20,1968, vol. 98
Treatment of Clotting in Arterial Hemodialysis Cannulaewith CA-7, a Fibrinolytic Enzyme from Aspergillus orysae
A. W. PERRY, M.D., F.R.C.P.[C], Victoria. B.C.
CLOTTING in cannulae used for chronichemodialysis seriously interferes with the
usefulness of this procedure. Unfortunately thiscomplication is all too common.1, 2 If detectedearly enough it is usually easy to aspirate theclot. Straight cannulae will allow the use ofFogarty catheters, but this type lacks the safetyfactor of stepped curved cannulae. Concomitantanticoagulant therapy is a useful preventivemeasure but adds a hazard in the patient withuncontrolled hypertension. During the past fewyears a new thrombolytic enzyme, CA-7, derivedfrom Aspergillus oryzae, has been developed atthe Connaught Medical Research Laboratories,University of Toronto. It has been reported ofpossible value in the management of venousthrombosis.3 This communication outlines itsusefulness, when used locally, in cases of oc¬clusion in the arterial side of the arteriovenouscannula.
Case 1..Mrs. S., aged 34, was undergoing re¬
peated hemodialysis for chronic renal failure due tochronic pyelonephritis. A standard curved Scribnerarteriovenous shunt was being used. The flows hadbeen satisfactory, averaging 166.5 ml. per minute.Flow rates were estimated from observation of themovement of a bubble of air in the venous line be¬tween the dialyzer and the drip chamber. On theevening of October 25, 1967, the patient noticedthat her arm felt different, but she did not reportthis until she arrived for hemodialysis at 10 a.m.on the following morning. Both the arterial andvenous sides of the shunt were found occluded withclot. Ready aspiration of the clot was not possible.Fifty milligrams of heparin was injected intra¬venously in the opposite arm to prevent furtherclotting beyond the cannulae. With a tourniquet on
the arm the venous cannula was repeatedly flushedwith a solution containing 150 ml. of saline, 2 ml.of heparin (1000 units per ml.) and one ml. of 1%procaine. With the additional help of aspirationusing an Intramedic tubing Pe 90-15* it was finallypossible to dislodge a firm clot from the venouscannula. The same procedure was followed with thearterial cannula, but the attempt to re-establishpatency was unsuccessful. The curve of the can¬nula prevented passage of a Fogarty catheter. Asolution of CA-7 was prepared by adding 50 ml. ofsaline to a vial containing 46,000 C2 units. The
From the Renal Unit, Royal Jubilee Hospital, Victoria,British Columbia.?Clay-Adams.Reprint requests to: Dr. A. W. Perry, 316-645 Fort Street,Victoria, British Columbia.
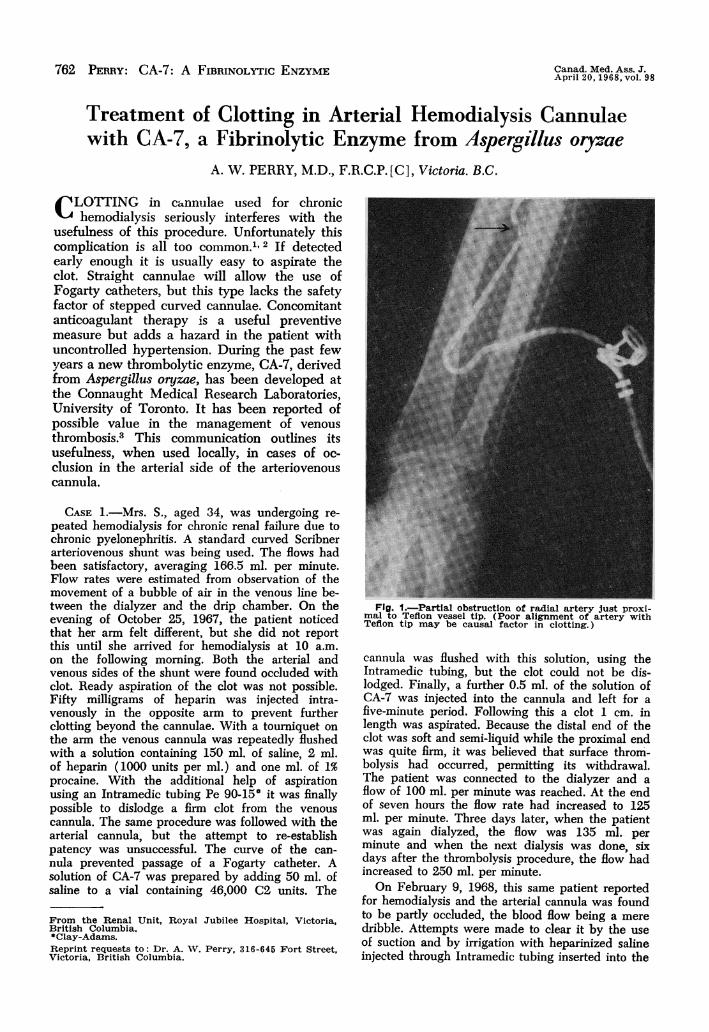
Fig. 1..Partial obstruction of radial artery just proxi¬mal to Teflon vessel tip. (Poor alignment of artery withTeflon tip may be causal factor in clotting.)
cannula was flushed with this solution, using theIntramedic tubing, but the clot could not be dis-lodged. Finally, a further 0.5 ml. of the solution ofCA-7 was injected into the cannula and left for afive-minute period. Following this a clot 1 cm. inlength was aspirated. Because the distal end of theclot was soft and semi-liquid while the proximal endwas quite firm, it was believed that surface throm-bolysis had occurred, permitting its withdrawal.The patient was connected to the dialyzer and aflow of 100 ml. per minute was reached. At the endof seven hours the flow rate had increased to 125ml. per minute. Three days later, when the patientwas again dialyzed, the flow was 135 ml. perminute and when the next dialysis was done, sixdays after the thrombolysis procedure, the flow hadincreased to 250 ml. per minute.On February 9, 1968, this same patient reported
for hemodialysis and the arterial cannula was foundto be partly occluded, the blood flow being a meredribble. Attempts were made to clear it by the useof suction and by irrigation with heparinized salineinjected through Intramedic tubing inserted into the
Canad. Med. Ass. J.April 20, 1968, vol. 98 Perry: CA-7: A Fibrinolytic Enzyme J@3
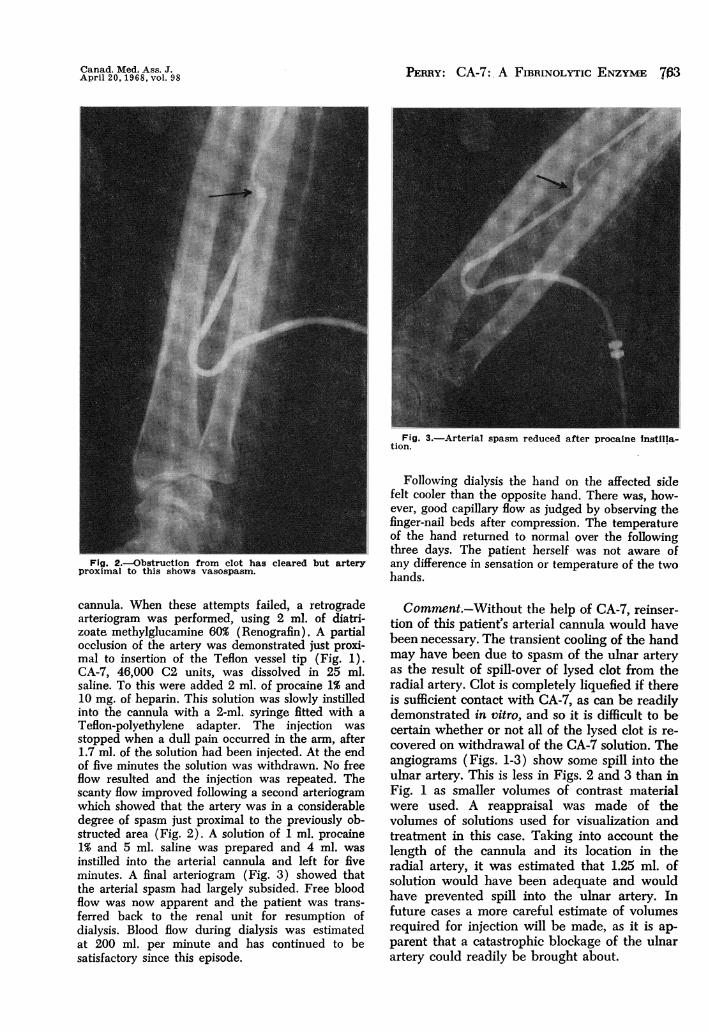
Fig. 2..Obstruction from clot has cleared but arteryproximal to this shows vasospasm.
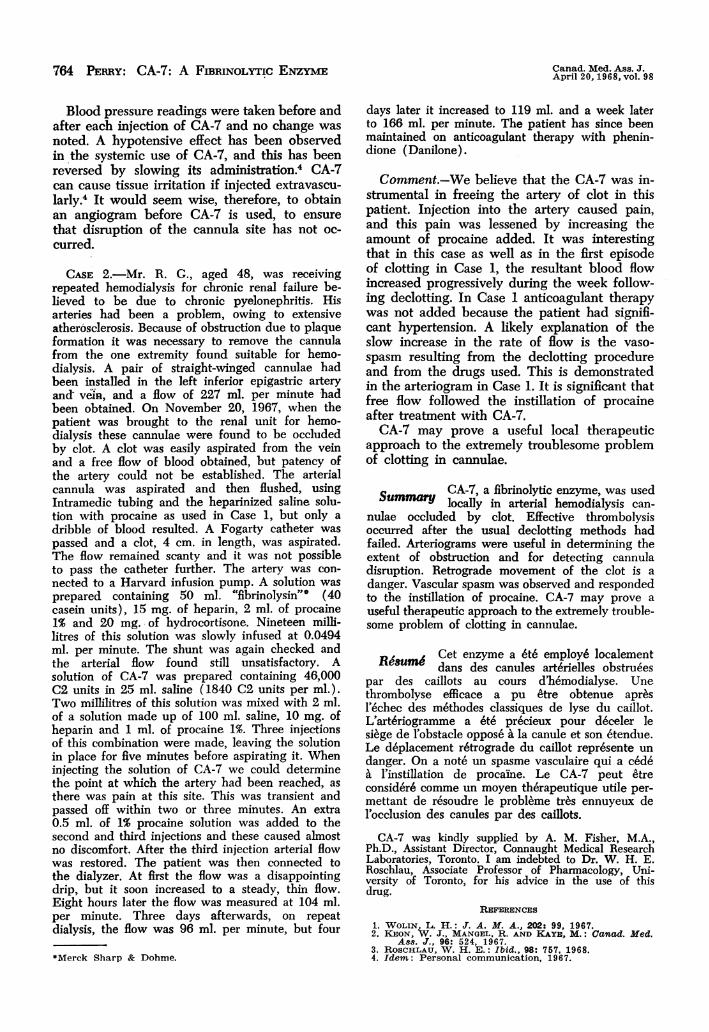
Fig. 3..Arterial spasm reduced after procaine instilla-tion.
Following dialysis the hand on the affected sidefelt cooler than the opposite hand. There was, how¬ever, good capillary flow as judged by observing thefinger-nail beds after compression. The temperatureof the hand returned to normal over the followingthree days. The patient herself was not aware ofany difference in sensation or temperature of the twohands.
cannula. When these attempts failed, a retrogradearteriogram was performed, using 2 ml. of diatri-zoate methylglucamine 60% (Renografin). A partialocclusion of the artery was demonstrated just proxi¬mal to insertion of the Teflon vessel tip (Fig. 1).CA-7, 46,000 C2 units, was dissolved in 25 ml.saline. To this were added 2 ml. of procaine 1% and10 mg. of heparin. This solution was slowly instilledinto the cannula with a 2-ml. syringe fitted with a
Teflon-polyethylene adapter. The injection was
stopped when a dull pain occurred in the arm, after1.7 ml. of the solution had been injected. At the endof five minutes the solution was withdrawn. No freeflow resulted and the injection was repeated. Thescanty flow improved following a second arteriogramwhich showed that the artery was in a considerabledegree of spasm just proximal to the previously ob¬structed area (Fig. 2). A solution of 1 ml. procaine1% and 5 ml. saline was prepared and 4 ml. was
instilled into the arterial cannula and left for fiveminutes. A final arteriogram (Fig. 3) showed thatthe arterial spasm had largely subsided. Free bloodflow was now apparent and the patient was trans¬ferred back to the renal unit for resumption ofdialysis. Blood flow during dialysis was estimatedat 200 ml. per minute and has continued to besatisfactory since this episode.
Comment..Without the help of CA-7, reinser-tion of this patient's arterial cannula would havebeen necessary. The transient cooling of the handmay have been due to spasm of the ulnar arteryas the result of spill-over of lysed clot from theradial artery. Clot is completely liquefied if thereis sufficient contact with CA-7, as can be readilydemonstrated in vitro, and so it is difficult to becertain whether or not all of the lysed clot is re¬covered on withdrawal of the CA-7 solution. Theangiograms (Figs. 1-3) show some spill into theulnar artery. This is less in Figs. 2 and 3 than inFig. 1 as smaller volumes of contrast materialwere used. A reappraisal was made of thevolumes of solutions used for visualization andtreatment in this case. Taking into account thelength of the cannula and its location in theradial artery, it was estimated that 1.25 ml. ofsolution would have been adequate and wouldhave prevented spill into the ulnar artery. Infuture cases a more careful estimate of volumesrequired for injection will be made, as it is ap¬parent that a catastrophic blockage of the ulnarartery could readily be brought about.
8764 PEImY: CA-7: A FiBRINoLYTic ENzymE~ Canad. Med. Ass. J.April 20. 1968, vol. 98
Blood pressure readings were taken before andafter each injection of CA-7 and no change wasnoted. A hypotensive effect has been observedin the systemic use of CA-7, and this has beenreversed by slowing its administration.4 CA-7can cause tissue irritation if injected extravascu-larly.4 It would seem wise, therefore, to obtainan angiogram before CA-7 is used, to ensurethat disruption of the cannula site has not oc-curred.
CASE 2.-Mr. R. G., aged 48, was receivingrepeated hemodialysis for chronic renal failure be-lieved to be due to chronic pyelonephritis. Hisarteries had been a problem, owing to extensiveatherosclerosis. Because of obstruction due to plaqueformation it was necessary to remove the cannulafrom the one extremity found suitable for hemo-dialysis. A pair of straight-winged cannulae hadbeen installed in the left inferior epigastric arteryand vein, and a flow of 227 ml. per minute hadbeen obtained. On November 20, 1967, when thepatient was brought to the renal unit for hemo-dialysis these cannulae were found to be occludedby clot. A clot was easily aspirated from the veinand a free flow of blood obtained, but patency ofthe artery could not be established. The arterialcannula was aspirated and then flushed, usingIntramedic tubing and the heparinized saline solu-tion with procaine as used in Case 1, but only adribble of blood resulted. A Fogarty catheter waspassed and a clot, 4 cm. in length, was aspirated.The flow remained scanty and it was not possibleto pass the catheter further. The artery was con-nected to a Harvard infusion pump. A solution wasprepared containing 50 ml. "fibrinolysin"* (40casein units), 15 mg. of heparin, 2 ml. of procaine1% and 20 mg. of hydrocortisone. Nineteen milli-litres of this solution was slowly infused at 0.0494ml. per minute. The shunt was again checked andthe arterial flow found still unsatisfactory. Asolution of CA-7 was prepared containing 46,000C2 units in 25 ml. saline (1840 C2 units per ml.).Two millilitres of this solution was mixed with 2 ml.of a solution made up of 100 ml. saline, 10 mg. ofheparin and 1 ml. of procaine 1%. Three injectionsof this combination were made, leaving the solutionin place for five minutes before aspirating it. Wheninjecting the solution of CA-7 we could determinethe point at which the artery had been reached, asthere was pain at this site. This was transient andpassed off within two or three minutes. An extra0.5 ml. of 1% procaine solution was added to thesecond and third injections and these caused almostno discomfort. After the third injection arterial flowwas restored. The patient was then connected tothe dialyzer. At first the flow was a disappointingdrip, but it soon increased to a steady, thin flow.Eight hours later the flow was measured at 104 ml.per minute. Three days afterwards, on repeatdialysis, the flow was 96 ml. per minute, but four
*Merck Sharp & Dohme.
days later it increased to 119 ml. and a week laterto 166 ml. per minute. The patient has since beenmaintained on anticoagulant therapy with phenin-dione (Danilone).
Comment.-We believe that the CA-7 was in-strumental in freeing the artery of clot in thispatient. Injection into the artery caused pain,and this pain was lessened by increasing theamount of procaine added. It was interestingthat in this case as well as in the first episodeof clotting in Case 1, the resultant blood flowincreased progressively during the week follow-ing declotting. In Case 1 anticoagulant therapywas not added because the patient had signifi-cant hypertension. A likely explanation of theslow increase in the rate of flow is the vaso-spasm resulting from the declotting procedureand from the drugs used. This is demonstratedin the arteriogram in Case 1. It is significant thatfree flow followed the instillation of procaineafter treatment with CA-7.CA-7 may prove a useful local therapeutic
approach to the extremely troublesome problemof clotting in cannulae.
CA-7, a fibrinolytic enzyme, was usedSumnmary locally in arterial hemodialysis can-
nulae occluded by clot. Effective thrombolysisoccurred after the usual declotting methods hadfailed. Arteriograms were useful in determining theextent of obstruction and for detecting cannuladisruption. Retrograde movement of the clot is adanger. Vascular spasm was observed and respondedto the instillation of procaine. CA-7 may prove auseful therapeutic approach to the extremely trouble-some problem of clotting in cannulae.
ReMsu6 Cet enzyme a &t6 employ6 localementdans des canules art6rielles obstruees
par des caillots au cours d'ehmodialyse. Unethrombolyse efficace a pu etre obtenue apresl'6chec des m6thodes classiques de lyse du caillot.L'art6riogramme a 6te pr6cieux pour deceler lesiege de l'obstacle oppose a la canule et son etendue.Le deplacement r6trograde du caillot repr6sente undanger. On a note un spasme vasculaire qui a cedea l'instillation de procaine. Le CA-7 peut etreconsider6 comme un moyen therapeutique utile per-mettant de resoudre le probleme tres ennuyeux del'occlusion des canules par des caillots.
CA-7 was kindly supplied by A. M. Fisher, M.A.,Ph.D., Assistant Director, Connaught Medical ResearchLaboratories, Toronto. I am indebted to Dr. W. H. E.Roschlau, Associate Professor of Pharmacology, Uni-versity of Toronto, for his advice in the use of thisdrug.
REFERENCES
1. WOLIN, L. H.: J. A. M. A., 202: 99, 1967.2. KEON, W. J., MANGEL, R. AND KAYE, M.: Canad. Med.
A88. J., 96: 524, 1967.3. ROScHLAU, W. H. E.: Ibid., 98: 757, 1968.4. Idem: Personal communication, 1967.