world class hospice - hospice & homecare consulting · world class hospice ... before it is too...
TRANSCRIPT

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 220 of 370
World Class Hospice There is a new class of hospice that is “blowing away” the competition. They are not doing it through any trickery or deception. They are doing it by simply being a superior hospice! What a novel idea! These hospices are growing by hundreds of percent a year…and they are challenging the way hospice is done. The problem with the typical hospice is that change comes slowly. The World Class Hospice comes into a service area like a speed board. It embraces and implements great ideas quickly, as contrasted with the typical community-based hospice which changes course like a freighter…slow. Before the typical hospice can change course, half the census has eroded away and the World Class Hospice is implementing even more dynamic and innovative ideas. The point is, hospice can be improved not by a few percent BUT BY HUNDREDS OF PERCENT! This presentation is not about becoming a World Class Hospice. However, here are some points.
World Class Checklist If you don’t know the answer to a question, your answer is no. As a leader, if you’re unsure about an operational point, how can your staff know? Question Yes No
a. Does your hospice MEASURE and place value on measurement? (Clinical and Financial)
b. Would you describe your hospice as a speed boat? (Would you describe your hospice as a freighter (slow to implement planned change)?
c. Does your hospice think in terms of PRODUCTS and services? If you think in product terms, list them:
d. Does each team member receive at least 4 hours of phone skills training?
e. Do patients and families intentionally select the services they receive?
f.. Does your hospice have at least a 10% operational margin? (No fundraising or support dollars)

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 221 of 370
Question Yes No g. Does over 25% of your labor come from volunteers? h. Is your volunteer program so impressive with WOW presenters
that people are willing to pay $200 to attend?
i. Does your hospice provide in-home monitoring devices? j. Does your hospice call patients daily, as a service option? k. Does your hospice promote and provide a high level of
homemaker services?
l. Does your hospice see its clinicians as providers of care rather than teachers? (Nurse Mary gives good care!)
m. Does your hospice see clinicians as teachers rather than providers of care? (Nurse Mary is an excellent teacher of care!)
n. Does your hospice provide LifeDisk recordings? o. Does your hospice provide a menu AND explain the Pros and
Cons of each selection?
p. Does your hospice clearly explain why it is different than other hospices?
q. Does your hospice allow patients and families the chance to choose the level of service they receive?
r. Does your hospice provide caregiver education tools that will make a caregiver 80% more confident in 15 minutes?
s. Does your hospice take more than 28 days to train an RN? t. Does your hospice have only one Volunteer training program? u. Does your hospice have a standardized way of doing visits for
each discipline?
v. Does your hospice re-align its core ideologies with media? w. Does your hospice use an answering service? This list is not intended to demean any hospice, but to CHALLENGE us to be more. Again, hospices can be improved HUNDREDS OF PERCENT.
Examples of World Class Organizations
• Disney • Ritz Carlton • MD Anderson Cancer Center • The Boston Celtics (1960s)

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 222 of 370
Ideas and applications:
• On-Stage/Off-Stage in a hospice Inpatient Unit • Touching the inscription on the brass above the door as you leave to care for your
patients • Leaders are like PRODUCERS directing a movie, getting the best performance
possible out of the Stars • Hiring Gritty, dive on the floor-type players who know how to work HARD • 20 Points of Customer Service • The Journey – A photographic story of a life of a person…for patients? For the
hospice staff….to reinforce meaning and purpose. Artistic black and white photos? • Easy and non-threatening way for people to provide honest and immediate
feedback on the services and products they are receiving…before it is too late. • A dramatic end to orientation, one performed by inspiring WOW people.
Examples of Products
• Deluxe Acknowledgement Tracking Logs • Glossy Medication Tracking Sheets • Caregiver Education
o Quick Guides o Diagnosis Guides
• LifeDisk Recordings/Units • Monitoring Units/Devices
Examples of Services
• The Perfect Nursing Visit • The Perfect CNA Visit (Most Valued Service) • The Perfect Social Work Visit • Bereavement Services • Volunteer Services • Homemaker Services • Lawn Care Services • LifeDisk Recordings • Inpatient Care • Crisis Care • Respite Care • Future Notes/Milestone Messages

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 223 of 370
The Hospice Menu – Giving Patients & Families CONTR OL of the Experience
• Choice to Die in My Own Bed (Pros & Cons are presented) • Choice to Die only with My Family • Choice of Services • Choice of CNA Level • Homemaker Services • Daily Monitoring Calls • Resource Coordinator (SW) Plays Greater Role
o Insurance Review o Checking Balancing o Funeral Planning o Coordination of Needed Assistance o Not Hung Up on Counseling
• Integration of Volunteers like in beginning of Hospice Movement • LifeDisk or Life Review Digitally Recorded • Future Notes/Milestone Messages • Critter Care • Superior Caregiver Education • Bereavement Follow-up by SW or Specialist
Challenging Ideas about Clinical Practice Most clinical managers do work based on tradition and what they have been taught in school or by healthcare organizations. Though this training and indoctrination is important, it must not get in the way of getting RESULTS for your organization. We should not be so concerned with tradition and the “way it is normally done” as with results. Dare to be different and be more interesting! For example:
• Why can’t SWs do 4 or 5 visits a day? • Why not measure productivity by Average Daily Caseload rather than visits? • What if we poured tons of effort into really making the CNA role something radically
different through more education and visit design? • What if we restructured the Case Manager role in such a way that productivity in
terms of visits was not measured, but the happiness & satisfaction of a vastly increased caseload?

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 224 of 370
• Why not ELIMINATE the use of PRN at your hospice? PRN often leads to sloppy clinical practice and poor management.
Notice that we are addressing you in this program as a Leader and NOT a Manager. There is a huge difference! A manager is more of a maintenance position…a person who makes sure that things are going along according to plan. On the other hand, a Hospice Leader is a person who is taking people somewhere. They are leading…
How do you start the transition to World Class? First, you find someone who is motivated to do this…you! Next, I suggest that your organization develop a Hospice Menu specific to your hospice. The elements on the menu should come from a “Patient/Family” Walkthrough of services. That is, what do patients and families really want? What would make their experience better? What could be added that would provide patients and families an experience better than anything they could imagine? Equally important, what services need to be eliminated or diminished?

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 225 of 370
Select the Items Pros/Cons
Explained
Communication � Daily Monitoring Calls (normally from 9:00am to 10:00am) �
Pain & Symptom Relief � Medication Level � � No or minimal medication � � Some pain, but able to interact � � As little pain as possible, but conscious � � Knock me out! � � Physician Therapy � � Respiratory Therapy � � Massage � � Relaxation Exercises � � Breathing Exercises � � Prayer � � Yoga � � Guided Imagery or Visualization � � Music Type: ________________________ �

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 226 of 370
House Calls � Would you like a house call from a physician? � � Nurse As needed � � CNA (Personal Care) 1x wk 2x wk 3x
wk �
� Homemaker 1x wk � � Social Worker � � Spiritual Support (Chaplain) � � Bereavement � � Volunteer � � Dietary Consultant �
Medical Equipment & Supplies � Do you want to stay in your own bed? � � Would you like a hospice person with you when the
time comes?
�
� Would you like the standard array of medical
equipment (wheelchair, etc.)
�
Personal & Practical Support � Personal Care – Bathing, laundry, changing bed
linens, etc.
�
� Transportation to and from medical or other
appointments
�
� Volunteer companionship � � Help with shopping and other errands � � Yard care � � Critter Care Services �
Specialty Items � Hospice Inpatient Care � � Crisis Care � � Short-Term Respite Care � � Dreams � � Travel � � Parties � � Special Events � � Hair Care (styling, trims, shampoo, etc.) � � Would you like a Health Buddy? � � Future Notes/Milestone Messages � � Other ________________________________ �
Spiritual Care

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 227 of 370
� Discuss spiritual matters � � Read spiritual materials to you � � Pray with you � � Work with family clergy � � Contact spiritual leaders for support � � Digital recording of a family member � � Life Review � � Assistance with funeral planning � � Assistance Balancing the checkbook � � Review insurance policies � � Other ________________________________ �
Emotional Support � Coping with depression, anxiety, anger, nervousness � � Help resolve family conflicts & stresses � � Assistance with Medicare/Medicaid � � Help with legal documents such as Advance
Directives, Wills, Powers of Attorney, “Do Not
Resuscitate” Orders
�
� Help children cope with fears, grief, or problems � � Identify community resources that can help � � Grief Workshops, Seminars, Camps, and Other
Activities
�
� One-time grief workshop � � Summer grief camp for kids � � On-going counseling � � Group counseling �
The Volunteer Department – A Wasted Opportunity Here is an opportunity for very low cost labor that could save a hospice a bundle, yet is almost ignored. The Volunteer Department is one of the most underdeveloped areas in most hospices. They are often led by the weakest leaders in the organization, people who couldn’t cut it elsewhere and eventually get “relocated” to Volunteer Coordinator.
“The reason most Hospice Volunteer Programs are so anemic is that Leadership doesn’t place high enough emphasis on it.” AR
What are other reasons Volunteer Departments do not perform well?

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 228 of 370
• Hospices do not have well thought-out opportunities for volunteers. Most hospices
“limit” how volunteers can serve. • Highly educated volunteers are often assigned menial tasks well below their skill
levels. • Training takes too long. • There is not specialized training for each class of volunteer. • Training is boring. The presenters are bad (this could be you!) WOW! Presenters
are needed. • Volunteer training is infrequent. • Volunteers are trained and then are infrequently or never used. • Unimaginative people are in Volunteer Coordinator positions.
The Volunteer Coordinator needs to be one of the mo st skilled and powerful leaders in a hospice since they can easily have the largest number of people to lead. You can’t have a person with a low Lid in the Volunteer Coordinator position. They must be among the most capable, organized and inspiring leaders in a hospice. The Law of the Lid holds true again. A hospice should (or could) have thousands of volunteers…representatives from every organization, church and business in the community. Volunteers are your eyes and ears. They are your feedback mechanism from the community. They are your spokespeople, your spies, your groundskeepers, your nursing home program secret weapon, your leverage instruments…they can be a lot of important things…if we value them. There is an MVI audio interview with Rita Burch that offers much insight into the Volunteer area. The audio CD is titled Volunteer Focus.
Volunteer Best Practice – Almost like E-Harmony.com ! Those who have been in hospice for a long time and were users of HMS+ will remember that the system had a feature that allowed volunteers to be matched with patients based on common interests and backgrounds. Hospices that used this feature would gather information about the patient’s hobbies, interests, educational background, profession, hometown, favorite books, etc. This would be input into the computer system. Then, a query would be run and the closest matches for volunteer assignment would be displayed. Somehow this Best Practice has been lost by too many hospices. But it can be resurrected!

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 229 of 370
Phone Skills Dial 7 if You’re in Pain… Have you ever considered how much care is provided over the phone? A tremendous amount of care and comfort comes to patients and families as we reassure, instruct and give guidance. Yet, how much attention does the average hospice give to increasing phone skills? Not much if anything. The first thing that needs to be addressed is the way calls are handled. Does your hospice use an automated system? This is NOT a good experience for patients and families. NOBODY enjoys automated systems when dealing with hospice. My advice: get rid of them immediately. Do we believe that people are just “naturally” good on the phone? Do we leave it to chance? There is a marked difference in the organization that sets standards and trains staff “how” to effectively use the phone. Consider the anxiety issues that can be effectively addressed over the phone. This is a huge aspect of care. If a hospice wants to differentiate its services from other hospices (Part of the 12 Point Training System), it would be impressive if your hospice could say, “Everybody at Sunny Day Hospice undergoes a half-day of phone skills training”.
“Digging” Phone Skills Focusing on the Situation When a call comes to a hospice, it is important that we understand that no one calls hospice just for fun . There is always a reason. It is important that we learn to dig! This means we not only answer questions and get the call to the correct person or department, but that we DIG…that is, we probe to find out the real needs and concerns, even the unspoken ones. We must FOCUS on the caller and express genuine interest in their situation. It is not just about telling people about OUR services, but about engaging the caller in conversation about WHY they are calling today. What we want is a proactive mindset and not a passive relaying of information so common in so many hospices. A progressive hospice will implement a “Mystery Caller Program” where quality of the call experience will be graded and evaluated (See details in the following pages). Here are the things to keep in mind when receiving a call at Sunny Day Hospice:

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 230 of 370
1. Sunny Day Hospice, this is _______________ (first name)! Tone: HAPPY! In these
few words, much is communicated. a. You have dialed the right place! Sunny Day Hospice b. Who I am speaking with…YOU! c. And that I am HAPPY to be here! This is the importance of TONE.
2. FOCUS on the Caller and their situation…even unspoken needs. Listen carefully.
a. Write down the name of the caller. b. If the request or question is regarding something…ensure, recommended
DME vendor, medication question, DIG! “Oh, is someone ill? Perhaps we could help!”
3. If the caller is inquiring about hospice or you perceive this is a new relationship, ask
how they heard about Sunny Day Hospice, what is the patient’s name, what is the diagnosis, and where they live.
4. The goal of each inquiry or referral call is to MAKE A SAME DAY VISIT.
5. If you are going to transfer the call, tell them “I’m going to transfer you now. In the
rare event that anything happens during the transfer, please call me back. I want to make sure you are taken care of.
6. If a potential patient, offer to contact the doctor on their behalf.
7. If a potential patient, offer to schedule a visit to discuss needs.
Bottom-line: People want to know that we care and that we can do something to help them.
The Goal: A Same Day Visit Question or Concern Answer
When can you come? When would be convenient for you? We could do it today!
I’m not ready yet. We understand your concern, but we can help. We can have someone visit today and we can sort through your options.
How much does it cost? Most of our patients are completely covered by Medicare or Medicare. Also all major insurance companies work with us. We

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 231 of 370
could set this up today! The person does not think they need hospice.
Hospice is not only for the one that is ill. It is also for you, the caregiver. There are probably many things that would benefit you as well. Could we have someone stop by today to explore your options?
“Digging” Scenarios Question or Concern Answer
Where can I get some Ensure? Is someone ill? Maybe we can help! Can you tell me where to go for DME? Is someone ill? Maybe we can help! Can you recommend where I could get a wheelchair?
Is someone ill? Maybe we can help!
We heard about hospice and what to know more.
Is someone ill? Maybe we can help! Get information and then explain the Capital Way.
I’m a doctor and need to speak with someone about a patient?
Is this a current patient of ours or a potential patient that could benefit from our services?
I have a problem! Tell me your situation and let’s see if I can help or get you to someone that can.
The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 232 of 370
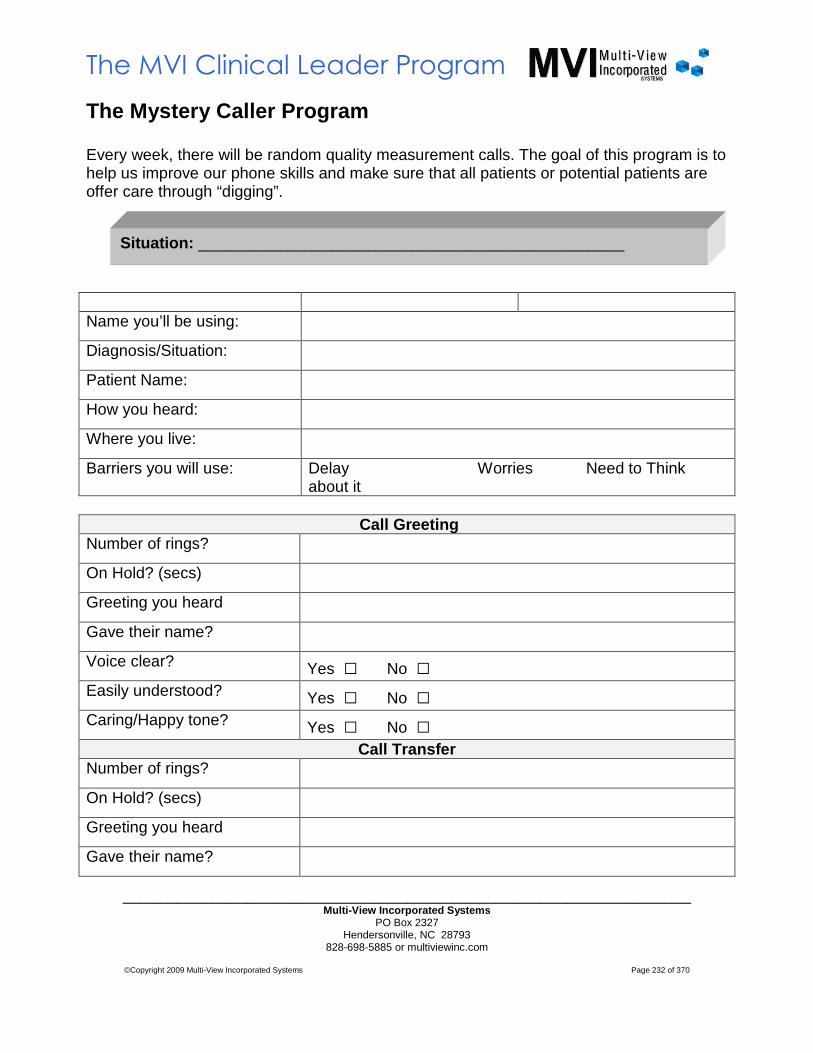
The Mystery Caller Program Every week, there will be random quality measurement calls. The goal of this program is to help us improve our phone skills and make sure that all patients or potential patients are offer care through “digging”. Name you’ll be using:
Diagnosis/Situation:
Patient Name:
How you heard:
Where you live:
Barriers you will use: Delay Worries Need to Think about it
Call Greeting
Number of rings?
On Hold? (secs)
Greeting you heard
Gave their name?
Voice clear? Yes □ No □ Easily understood? Yes □ No □ Caring/Happy tone? Yes □ No □
Call Transfer Number of rings?
On Hold? (secs)
Greeting you heard
Gave their name?
Situation: ________________________________________________

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 233 of 370
Voice clear? Yes □ No □ Easily understood? Yes □ No □ Caring/Happy tone? Yes □ No □
Call Rating Did not seem rushed or distracted
Yes □ No □ ? □ Difficult □
Cared about you, focused on needs and feelings
Yes □ No □ ? □ Difficult □
Communicated at your level of understanding
Yes □ No □ ? □ Difficult □
Effectively handled your barriers and roadblocks
Yes □ No □ ? □ Difficult □
Offered follow-up call/said what follow-up would be
Yes □ No □ ? □ Urged you to call back at any time
Yes □ No □ ? □ Gave you a sense of help and reassurance
Yes □ No □ ? □ Tried to get your name Yes □ No □ ? □ Asked how you heard about us
Yes □ No □ ? □ Asked about your situation/why calling today
Yes □ No □ ? □ Offered to contact the doctor on your behalf
Yes □ No □ ? □ Offered to schedule a visit to discuss needs
Yes □ No □ ? □ Urged and directed you to schedule a visit
Yes □ No □ ? □ You would call again if you needed help
Yes □ No □ ? □

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 234 of 370
Hold Music? As we “walk-through” the patient/family experience and review the phone area, “Hold Music” or the “Hold Message” must be examined. Is it cheesy? Is it unpleasant? Is it ordinary? Is it so bad that people hang up! Is it good enough that people want to be placed back on hold! A hospice can have a “play-list” of music that would make the “hold experience” actually pleasant. The songs must be appropriate to the target demographic. Suggestions? Positive and slightly upbeat tunes…but not too peppy, like… What a Wonderful World – Louie Armstrong Message: “Thank you for calling Sunny Day Hospice. Your call is important. We will be with you momentarily.”
Saturday in the Park – Chicago Message: “Thank you for calling Sunny Day Hospice. Your call is important. We will be with you momentarily.”
You’re My Best Friend – Queen Message: “Thank you for calling Sunny Day Hospice. Your call is important. We will be with you momentarily.”
Only Yesterday – The Carpenters Message: “Thank you for calling Sunny Day Hospice. Your call is important. We will be with you momentarily.”
Blackbird – The Beatles Message: “Thank you for calling Sunny Day Hospice. Your call is important. We will be with you momentarily.”
OK…some of these may not be your taste, but you get the idea! Make it a contest at your hospice. This can be something that is fun!
How Do You Start the Transition to World Class? Some hospices call it the “Great Transformation.” Seriously! The hospice functions along a certain path for many years and then WHAMO! Someone gets a fire in their gut that starts the change. That is how it usually happens, unless the person is starting a new hospice. Here are the steps:
• Passion and Fire in the Gut - Find someone who is motivated to do this…you! • Capture Your Organization’s Ideas. Take the Strategic Planning Document that
was mentioned previously and start to list all the things that you want your hospice to be and do. (Do you have to BE before you can DO or can you DO and then BE?). When filling in your Strategic Planning Document, I suggest you perform these exercises:
o Walk Through the Patient/Family Experience . See your services through their eyes and not yours. Remember when you had hospice services. What did you most value? What could have been offered that would have delighted you?

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 235 of 370
o Develop a Hospice Menu Specific to Your Way. The elements on the menu should come from a “Patient/Family” Walkthrough of services as well as anything your minds can imagine that would make their experience better. What could be added that would provide patients and families an experience better than anything they could imagine? Equally important, what services need to be eliminated or diminished?
• Ride the Plan! This is the tough part. You must be able to assign tasks, deadlines and hold people accountable. State your expectations very clearly…along with the consequences of non-performance. Look for quick wins to help you build momentum.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 236 of 370
Growing Your Hospice
Growing a hospice is always a concern as it impacts everything. There are a lot of formulas and recipes. However, in my mind, the major things that need to happen are clear, at least for now…they have changed over the years. There are tons of specific practices to embellish each major point, but let’s focus on the big guys. If we were to categorize these points, they might be classified as internal and external…both of which are impacted by what WE DO or DON’T DO. You will note in the following list that most things pertaining to a hospice’s growth are INTERNAL, not EXTERNAL.
1. INTERNAL Increase LOS – LOS is self-determined by a hospice. It is a product of a mindset that has been created by our behavior. We have trained referral sources and the community over years by the patients we have admitted or have not admitted. All hospices’ can intentionally increase LOS. The complaint in hospice for so many years was “if only we can get patients sooner”. While this is true in many cases, it points to the external world as the problem rather than pointing to ourselves. “How” to measure LOS is a big question. I think you need to measure it based on Average LOS for Terminated patients AND Median LOS for Living Patients. Both are required as ALSO (Terminated) can lead a hospice into Hospice Hell (CAP problems) and MLOS (Living) will keep a hospice out of the netherworld. I have not found a single measure of central tendency that will do the job…yet! Look at your UR process? What is your goals for Patient Mix > 365 Days? Of course, your documentation needs to substantiate the patient’s continuance in the program, but isn’t it better to have patients longer and not be providing ‘brink of death” hospice?
2. INTERNAL The Leader of Admissions – The profile of top Admissions leaders are characterized by high energy, can-do attitudes, admissions boards cleared daily, might drive a red sports car… you get the idea. These are clearly “sparkplug” personalities. You want this type of individual because their example will be transferred to the entire Admissions team. I call this the Principle of Replication. Leaders can only reproduce what they are. A slow, low-energy leader will reproduce a slow, low-energy team. In Admissions, we want a sense of urgency! Speed is the name of the game in a competitive hospice environment. Understand that the speed of the leader is the speed of the team. Evaluate the person running Admissions. We have seen hospice’s double census with this one move.
3. INTERNAL Develop Phone Skills & “Digging” – How do we handle calls at our hospice? Does everyone that could use our services get in? It is estimated that most hospice miss 10-15% of potential patients through misinterpreted phone calls. That is, a typical hospice could increase its census IF it learned to “dig” into calls. Nobody calls hospice without a reason. People call hospice because there is a need. In the Model workbooks (currently in development) this area is covered. It is a mistake to assume that people are just “good” on the phones. This is an area that

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 237 of 370
needs special attention. The tone of voice, message, training at meeting the unspoken need (digging), and even the hold music or message needs careful evaluation. You hospice could have its own “play list”!
4. INTERNAL Your VALUE Proposition – This is normally known as the “pitch”. What is being said? What image is being communicated? Have your marketing staff give their pitch – cold. Don’t give them time to prepare. Have them come into your office individually…then sit and listen. Don’t critique. Don’t comment on the performance. After you have heard all of the marketers, evaluate. Would you choose this hospice? Is it really any different than other hospices? If the message is “we are the oldest and the largest” or “we care more” or you find some other worn-out, value-devoid message, its time work on your message. Perhaps you need to work on your hospice! In my mind, since so many hospices “do it the same” it is relatively easy to differentiate in a market. It is not always about doing more. Perhaps it is about doing less, but doing less extraordinarily well…so that marketers have CONFIDENCE in what they promise. The Value must be rich. People want to know that their loved ones got the Cadillac hospice service. People are very upset when they realize that they chose the “2nd string” hospice. Is there ‘evidence” behind your claims? Benchmarking will clearly help in this area as you develop your message. Message the data points where your hospice excels. Such as having high visits per patient or low indirect costs.
5. EXTERNAL Paper Routes and Feet on the Street – This is where most hospice’s start when trying to grow. But it is the wrong place. There should be defined territories, accounts, and frequencies of message. We need to have all of these things worked out so that the crafted, value-rich message is communicated. But this is really the last factor. Even with a well crafted message, marketing initiatives will fail without a trustworthy marketer. Choosing a good marketer is probably more art than science. I do know that the best marketers have absolute belief in what they are selling and there is a high integrity factor that is palpable. Trust is the basis or all great relationships.
All hospices should be growing. Growth is a sign of life and of advancement. The hospice that is not growing has problems. Its mission is not about patients. It is more about themselves. Here are some points about the concept of growing a hospice. Is the census your job as the Hospice Leader? Well, technically no, but it IS!!! If you are a leader who is worth his or her salt, you are concerned with growth. You ARE a factor. Use your personality, wit, personal magnetism to influence a growth mindset.
“High water covers a lot of stumps.” Norman McRae

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 238 of 370
Firing People to Grow the Hospice This may sound like a paradox, but you have to have the right people on board to grow a hospice. Having the “right” people on board may involve throwing the “wrong” people off the bus. Resisters of growth have to go. We want only true believers and people with confidence in themselves that they can get the job done. An evidence of real leadership is GROWTH! Real leaders grow WHATEVER they are handed. So firing people in order to grow is not such a wild idea. I can see the new books, “Fire Your Way to the Top!” and “Cutting Staff to Grow!” This is a true paradox.
The Two Kinds of Growth There are two types of organization growth that relate to increased patient volume: Natural Growth and Forced Growth. Both are needed. Natural Growth creates CAPACITY before it grows. This means that the organization hires, trains and adds infrastructure before growth happens. It is logical. Growth in a Natural model comes from providing great services, word of mouth and designed promotional efforts. Forced Growth is where an organization does promotional activities designed to increase business with much less regard for building the infrastructure to support the growth. An organization finds itself “working short” in a Forced Growth situation. Staff works very hard in periods of growth, but profitability is great. When growth slows, which all growth plateaus at some point, infrastructure that was not created “on the fly” is implemented. At first glance, one would think that Natural Growth is always the best. This is not the case. When margins are tight and there is little capital in reserve, Forced Growth is a very good thing. Most hospices have been built on Forced Growth. Many times, even when a hospice intentionally plans on using a Natural Growth model, it ends up being a Forced Growth model as the growth outpaces the hospice’s ability to attract, hire and train new personnel. Forced Growth is always the most profitable as long as products and services do not deteriorate too severely during the period of growth. Graphically this is what Natural and Forced Growth look like:

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 239 of 370
You will probably recognize that most organizations do not really grow like either model. Reality is that we are a combination of both models. However, as an organization, we should choose a growth model as a strategic guide. Many hospices are AFRAID of forced growth and “self-truncate” as the NFP mentality feels that it is “not right” to work staff hard. Hear this…nothing that is worth anything is easy. Hard work is good for us. Set your standards high…”Everyone at Sunny Day Hospice works hard”…it is just the way we do it around here!

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 240 of 370
The Role of Confidence in Selling Before we go too far down the marketing road, recognize that the WHO is the most critical factor. You have to have the right person and it is more art than science in selecting the right person. With that said, one characteristic of the superstar marketing person is that of confidence. Can your marketing people CONVINCE others that you have a superior hospice product? Do they believe it enough themselves? Have they made the sale to THEMSELVES yet? If you are a Hospice Leader you need to provide or help instill confidence in the marketers that you have superior hospice services. You have to sell the sellers of your services! Confidence comes from:
• Doing • Success • Historical Fulfillment of Promises • Adequate Preparation • Risk Taking with Success
Confidence in the organization will:
• Increase your ability to sell your hospice services • Increase your ability to attract and hire top talent • Help your hospice retain people
One best practice is to have your marketing people lay their “pitch” on the Hospice Leaders at least once a month. This will build congruency between the “promise” and the fulfillment of that promise. In most hospices, Clinical does not know what Marketing is saying…talk about a problem.
“Great marketing is the continual re-education of t he customer so that they can appreciate what and how we serve. Then, by clearly denominating our services, we
provide the customer a basis to discriminate on our behalf.” AR

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 241 of 370
Points on Growing a Hospice Here are some points to keep in mind about growth.
Stop Wasting Dollars on Media to Grow Census It doesn’t work. If it did, the largest hospices would be doing it. It has been tried. You will get some results, but not enough to justify the on-going dollars needed. We need to be open minded about this. Perhaps, someday, a hospice will have incredible sustained results from a media campaign or a “wonder” ad will be developed that shoots a hospice’s census up by a hundred. But, it hasn’t happened yet. Here are the proven facts on how hospice grow:
• Personal relationships and “feet on the street” • Speaking engagements-promoting a general awareness of hospice • Relationships with physicians, hospitals, nursing homes
Rework the Admissions Department Increase the census 15-20% by just converting the inquiry calls you already get!
• NO ONE ANSWERS THE PHONE WITHOUT THE MINDSET AND THE TOOLS! • Have responses for every objection or delay. • Define what “words” your hospice uses. For example: Marketing, OutReach,
Education etc. • The goal is to get a visit scheduled that same day. • Track all inquiry calls about anything – looking for 75% conversion rate. No
excuses in the numbers. • Do weekend admissions. • Just do the visit. THEN call the physician (check on New Regulations). • Adopt Open Access; Expand the picture of a hospice patient. Take some risks. Let
people in! • Make the pill small. • Fast easy admission. Not too much information. Not much time. • While you are processing, we’ll take care of Mom for a few days. • What do you have to lose? • We can help! Not just the patient, but the CAREGIVER as well.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 242 of 370
Look at Your Discharge and UR Process Your hospice may have a very limited view of what a hospice patient looks like. Is it too conservative? Look at who you have performing this function.
• Usually it is only a percentage or two. • Are you discharging due to poor documentation? Could you keep more patients if
your clinicians learned to document better? Your Clinical Educator could add to your bottom-line if they were doing a better job in this area.
Rework the Marketing & Outreach Department Be pushing to get 45-50% of ALL deaths.
• Look at your Image. Is it professional? Do your brochures and website look like they were created by a committee?
• Sell VALUE and not the PROGRAM. “How can you help THEIR problems?” • Do the paper routes – the key is consistency.
o Medical Community-Physician practices, Nursing Homes, Assisted Living, etc.
o Campers at the Hospitals o Watchman Volunteers o Beauty Shop Marketing o Consistent Message from the SAME trusted person
• Make hospice a small pill. Anyone can do anything for a short time. • Hospice is different today! • Use the Volunteer Area! Use volunteers in the nursing homes more. The Volunteer
area in a hospice is one of the most underutilized areas. What a waste! Usually the Volunteer Coordinators are the WEAKEST leaders when they really need to be the STRONGEST since they have the most people reporting to them!
• Dig a new well! If you want more referrals, you may need to tap different referral sources. Who are you NOT seeing?
Adopt Open Access • NO ends the dialogue with referral sources. • It’s a New Day for your hospice! We are NOT what we used to be! • Contract for discounts. Chemotherapists, Radiologists, Dialysis, etc. • “We are trying to prepare for the future. You are our partner and our patients need
BOTH of us. We want to take away the limitations.” Good language! • Become known as the “liberal” hospice. • Don’t let financial fear hold you back. Financial fear is why hospice does not adopt
Open Access.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 243 of 370
• Don’t make people have to “think too hard” about hospice. • ADRs = Almost Dead Really! Don’t be afraid. • Discharge rate may increase, but be conservative in discharging.
Increase Efforts in Nursing Homes & Assisted Livin g We recommend 50% of a hospice’s census come from facilities. The average hospice’s census is 20% patients who reside in facilities (Nursing Home, Assisted Living, etc.). 50% would be a good goal.
• Why? Three Reasons: o Fulfills mission o Is good financially o Creates a barrier of entry for the evil empire
• Need specialized teams that knows the “turf” issues of each facility • Focus on “assisting” the facility in EOL • Marketing person • Some hospices are sending people or tools to help Nursing Homes do the billing
Become World Class How are you really distinguishing yourself in the MIND of the referral source and patient/family? Are you really different or better? Look at your products and services HARD. To give our marketing staff something real to promote, we need to have a fantastic and compelling product. Let’s go through the World Class Hospice checklist:
• Hospice Menu; “Hold the Pickles and the Mayo” • Increased CNA Services • LifeDisks • 12 Point Training System
o People Development o Phone Skills
• Nurse Magnet? • Phone Monitoring Services • Homemaker Services • High Standards instead of Coddling Clinicians • Products • Hire Staff to GROW. Many times a hospice will not grow because clinical staff do
not believe that they can handle it. This lack of confidence in the ability to serve will impede growth.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 244 of 370
NEVER NEVER NEVER Say You Can’t Take Patients This is the worst and most short-sighted message a hospice can put out. “We are too busy to take patients now.” What does this say about who we are. We are basically saying, “This hospice is more about our staff needs and we are less interested in patients…even if they are in pain.” And the short-sighted nurse says, “But we won’t be able to serve these patients at our standards.” Well, suck it up! Let’s work a little harder, let’s get the patients in. In our experience, referral sources will remember this message for YEARS! They will remember it for at least 2 years, maybe more. Even if your hospice only uttered this terrible message for 3 days, you will not recover from it for years. Mark my advice here.
More Thoughts on Marketing… Consider the source… I realize that I am a lunatic CPA. However with that said, perhaps this proves to some extent, that anyone can be an effective marketer of hospice. There is hope for practically anyone! When you boil it down, it takes (1) passion about what you are doing that comes from the belief in the mission, (2) competence and (3) a likeable personality. These three points are the foundational elements. But to really put admissions on the board, it takes much more conscious effort, a plan, and discipline. The people factor can not be underestimated Only sold-out, bought-in, and true believers make much of a difference in this world…this point is especially true in outreach efforts. Your people selection processes is critical. Success in outreach, as well as in most any area of an enterprise, is materially effected by the “who”…the people doing the outreach as well as the leader of the initiative. If you have invested in people and are NOT getting good results (in a relatively short period of time) get new people. If your marketing people are content with typing newsletters and focusing on print advertising rather than being out of the office (Feet on the Street), you don’t have the right players… This outline gives the marketing/outreach staff a textual point of reference to help keep the important and many times “subtle” points in mind. The audio CD Marketing & OutReach (Revisited) contains much of this material and this outline should be used to supplement.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 245 of 370
Record ADC Levels All across the nation, hospices are setting census records. These record ADC levels are being achieved, especially in areas where there is competition. We see programs that have been in “cruise mode” until a new hospice opens up. Suddenly, there is a sense of urgency and people start to question their services and marketing. And in the course of this “threat”, the hospice increases significantly, even doubling in many cases. Though not appreciated at the time, competition keeps us on our toes and if we are good at providing hospice and run a tight ship, we should have few fears.
Work on “Self” First If your services are poor, you don’t have much to market. Therefore, before ANY outreach efforts, your services MUST BE good, even great. If you provide good or great hospice care, then you can start your outreach program. If your services are of poor quality, you will be found out quickly and no amount of marketing hype will save you.
1. Look at your Admission Practices and the People in the Department. You could be limiting or self-truncating your ADC. This is MUCH more common than one would think. We’ve seen hospices double and triple in size just from working on this area. Be great on the front end. There is a reason why many of the successful hospice chains really work on the front-end, the admissions area. People love rapid response! Clearly denominate the benefit in terms that people will remember (Example: We will admit within 4 hours). Some hospices are claiming 2. Give prospects a basis to discriminate on your behalf. Some hospices send a “signer” or clerk-type of person to make the initial contact and to get some of the education and forms signed. Patients and families don’t care so much as to “who” shows up as long as “someone” shows up quickly. For best results get the right “who” with the right message out within a defined (short/impressive) period of time.
2. Separate Admissions Staff from Regular Line Staff. If they are not separated,
there is a tendency to “self regulate” the census. During times of high census, marketing slacks off. During times of low census, marketing is increased.
3. Make the Process “Easy” for Referral Sources. Too many hospices are focused
on their own needs rather than needs of referral sources. Remove the barriers of entry.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 246 of 370
4. Commit to Excellence and Become Impressive. Let your excellence spill out “externally.” Is your hospice really committed to excellence? I’ve come up against a new breed of hospice and the operative word is “impressive.” Be impressive in what you do. It will create pride in staff that leads to a more effective presentation. Ideas to become impressive might include providing lots of CNA services, daily phone contact with patients/families, rapid response admissions, high quality patient/family education, defined training systems, etc.
5. Develop Congruency Between the Promise and Promise Fulfillment. How
many hospices consciously meet (say every two weeks) to discuss exactly what is being promised with what is actually being delivered? Not many. To get the proper synergy, a meeting of the minds is essential. IF your promise makers absolutely TRUSTED the people that would be fulfilling the promises, wouldn’t it add to the degree of conviction that the promise could be made? You bet it would! Meet frequently…every two weeks and have them give you their “pitch.”
6. Develop the “System.” This is where we identify specific referral sources and
methods. Work on your SPECIFIC language and the images that come from your words. Set schedules. Assign outreach staff to paper routes. Determine speaking points and tools to keep outreach staff on message. Arm them with the right “marketing ammunition” – testimonies and updates on referred patients. Teach them how to “listen” and how to be able to hear NO a thousand times and still continue to visit. Design your perfect contact. Have them use the “just give me one patient and see how wonderful our services are” type messages for hard cases. THE TRAINING SYSTEMS OF OUR HOSPICES SEPARATE THE GREAT FROM THE UNGREAT. Don’t make it up as you go.
7. All Methods Plateau at Some Point. All methods that we’ve seen plateau at some
time. But does this mean that we stop them? Absolutely not!!! It means that we add to them or innovate. All successful methods work on a certain level. It is the combined effect that we are after…when methods build upon each other. Too many organizations reach a certain level of outreach success and the jump (and drop) the method that got them to their current level of success. Don’t pitch what has worked in the past…add to it!
8. Modify Your Ideas about Billboards, Radio, TV, and other Media Ads for the
Purpose of Increasing Census . In most cases, we just haven’t seen it produce great results. There are some exceptions. However, most hospices do not have the budget of someone like Coke that can spend the money to keep its name in front of the public continuously. There are some great hospice ads out there and maybe the best ad has yet to be written. But I would still put my money on the building census through relationships. One hospice even took $1,000,000 out of the

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 247 of 370
bank and blanketed the city with promotions for a year only to get the most minimal and short-term increase in census. Guess what? They aren’t doing it anymore! If they would have taken $300,000 of it and put it into hiring great outreach people, they would have gotten a much bigger increase in census. It’s about Feet on the Street.
9. It’s ALL about relationships!!! Your ADC will be directly related to your ability to
build relationships. MVI calls it the “Big R.” Therefore, the effort you put into building true, lasting, and integrity-based relationships WILL result in an increased census. All marketers MUST be trained on relationships. Have them listen to the MVI CD Understanding the Big R .
10. Define a “Hospice Patient” – It is important to get clear about “what” a hospice
patient looks like in your program. I believe that many hospices complain about short length of stays but don’t realize that is exactly what they have trained the medical community to refer. Open Access , the concept of taking patients on more aggressive treatments, is a hot topic.
The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 248 of 370
Building the “System” - Three Specific Areas Attack Nursing Homes This is your quickest way to grow your hospice. The average MVI hospice has 23% of its census in Nursing Homes and the highest hospice we serve in Nursing Homes runs 92%. There are good reasons why many hospices focus on Nursing Homes. The main one is that it is usually the most profitable class of patients due to great efficiencies regarding staff visits and usually this class has a higher ALOS. I would suggest that two more reason:
1. By serving Nursing Homes, you make it much more difficult for competition to come into your market. It is a proactive and defensive posture. If you already have built the “Big R” then it makes the going tougher for the competitor.
2. Most importantly, it fulfills the mission for most hospices. Just because Nursing Homes are not always the most attractive places to work. However this is not a good reason not to serve them…especially if they are bad! Are we here to serve ourselves or are we here to serve the people that are dying in pain …regardless of where they live? In fact, the worse the Nursing Home, the more they need hospice!
Be prepared to face stiff competition in this area. What we are seeing is “impressive.” Here are some pointers:
1. The Contract . Many aggressive “rev-up and get ‘em” hospices can get in the doors of Nursing Homes with great presentations and bullet-point brochures of the things the Nursing Home leaders want to hear and get a contract. We have found that there is little critical assessment in the decision making process as the Nursing Home leaders are very busy people and are u sually willing to “try” the new hospice. After all, what have they to lose? Many hospices want exclusive contracts. However, a better card to play is to let Nursing Homes offer a choice of hospices, but what you want is to be the preferred provider. Just having a contract doesn’t mean anything if there are no patients attached to it. Instead of “hiding” behind a contract, take a page out of the MVI playbook. Put in your contract that the Nursing Home can terminate the contract at any time if you fail to deliver on what you promise. Seems fair to me.
2. Hire the “Right” People. Don’t try to convert clinicians that signed up to do Hospice Home Care into your specialized Nursing Home team. It will fail or at best, you will have a sorry Nursing Home program. Instead hire people that already like it and WANT to do it.
3. Train Staff as Nursing Home Specialists – These staff should understand the potential turf issues and be conscious of filling the special needs of the facility.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 249 of 370
4. We are Guests . The language or mindset of the Nursing Home specialist must view themselves as a “guest” in the Nursing Home. This means that we are not telling the Nursing Home what to do and that we are respectful of their culture.
5. Communicate Value. Provide them with a compelling reason “why” it would be to their self-interest to work with you. What does your hospice bring? There are things that you can say that will get their heads nodding in agreement. One clever method is to do an in-service for all staff and then tell them things they want to hear and things they desire (of course, you have to do what you promise). With everyone from CNAs to RNs nodding in agreement and all staff looking to the management with the facial expression of “we’re going to do this, right?” It is very hard for administrators not to get caught up in the moment and succumb to the peer pressure. When marketing, you must communicate value. “We’re the best” and “We provide quality care” just doesn’t cut it. In Nursing Homes, they “hear” that you (1) will help them by keeping hospice staff at their facility for large blocks of time, (2) that their documentation will improve as surveyors see that hospice is involved, (3) that you will provide outstanding training in-services, (4) that you will split Inpatient level of care reimbursement with the facility, (5) that the care of patients in need of hospice will receive high quality services, and I’m sure there are many other value factors. Point them out. Denominate them clearly so that your services can be appreciated.
6. The Need to Become Great at In-Services . Still…there are too many people and Nursing Homes that do not understand hospice. Therefore, educational experiences are in order. Use quality in-services to help the Nursing Home. These are NOT just marketing presentations, but have real content and value. Offer a menu of presentations by various great presenters in your organization or contract for them! If they don’t have a preference of in-services they want, have a program or sequence of in-services. “WOW” people that can give a great presentation. But the people with real knowledge and substance have staying power and gain respect. Have your presentation staff become not only good, but great. Usually a good presenter can become great with a few pointers from a great presenter. These in-services provide a platform to keep your top-of-mind awareness up. Create “Super Presenters.”
7. Learn to Build Relationships with ALL of the Staff at the Facilities . Indoctrinate them, get them on your side, make them your ambassadors, validate their work, make them feel special, go out of your way to help them…do this and they WILL love to see you. Be the sunshine of their day. Don’t just visit and leave. MAKE FRIENDS with the receptionist, charge nurse, office manager, etc.
8. Don’t feel that you can be slack with Nursing Home patients just because you rationalize that “there are clinical people around! ” Who is the specialist in pain management? Every day, people are surrounded by healthcare professionals and suffer in pain. If nurses have this “slack” mindset, it must be overcome.
9. Put them on the Paper Route System . (see the next section)

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 250 of 370
10. Do not recruit their staff. If you want to end the relationship, go ahead and recruit. Some hospices have policies where a person that leaves a Nursing Home for Hospice must be separated from the Nursing Home for at least six months. This can be tough in small markets. Another considerate policy would be for the Hospice to call the Nursing Home BEFORE they hire the person to let them know that you think enough of the relationship that you would not risk it for the sake of hiring a person. The BEST idea is to communicate and get agreement on how you will handle this situation BEFORE it occurs.
To get in the door, you may have to beg…yes I mean “beg” for a single patient. “Just give me one patient and let us show you what we can do!” is your cry. Then you better perform. If you have already tarnished your reputation with a facility due to unfulfilled promises or poor service, you will have work to do. Your word may not be good anymore. It will take action in this case. It may take a visit from the CEO… If you’ve blown it before, admit it…ask to start fresh with one patient! Then provide some “impressive” care. You only get so many swings…
Paper Routes There is incredible power in a “systemic” approach to visiting referral sources and building relationships. Paper routes are predictable and absolutely consistent. Forgetting to deliver the morning paper to Mr. Jones will result in a phone call. I’ll guarantee it! Why? Mr. Jones has an “expectation” that the paper will be delivered at a “specific” time. You can take this same human phenomena and “program” an expectation in the minds of referral sources. Visit at the same time, on the same day, by the same staff…EVERY TWO WEEKS. It seems to us, that the two-week visit cycle outperforms all others. You can have someone brought to tears with a great story, but in 14 days they will have forgotten about the experience. Your visit brings top-of-mind awareness back to 100%. Here are some points regarding paper routes:
1. Divide Your Area into Geographical or Specialty Pap er Routes. Logical routes based on logistical considerations are wise. However, some people are gifted with specific referral sources. Special routes can be created for this situation. Hospital liaisons are a form of a specialized paper route.
2. Assign Staff – I would judge outreach people on their ability to create positive relationships and represent the image you’re trying to communicate. What is the first impress they made on you? How do they make you feel? Are they perceived as intelligent, creditable, and honest with a huge heart for hospice? This is basic but often the most overlooked stuff. Flashy people will only get you so far… People of substance prevail in the long-run.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 251 of 370
3. Create your “Good Things that Happen” or other Mark eting Ammo Forms. Have the regular visit staff record great events or patient information for the purpose of outreach. File by referral source. When its time to go on route “A” take your “route A” files. Read them before you enter the referral source. That is, load the information in your mind! It gives outreach staff something to talk about and lets the referral source know that you know what’s going on… It creates confidence as well.
4. Measure Results. Compare routes, people, and methods. Incorporate effective innovations into the standard call. Delete ineffective methods.
5. Provide Tools & Aids and NOT Trinkets & Candy. “If they have the money for this, then…” is the thought that goes through people’s minds. We feel that trinkets and candy are counter-productive and cheapen the image of your hospice. If you like to be grouped with pharmaceutical reps, then go for it! On the other hand, valuable tools that help referral sources know that we don’t just serve cancer patients and how to make an intelligent referral are viewed favorably. Home made goodies work well too. I am not opposed to pens and a few utility hand-out items, but don’t over do it! It’s nice to have a great functioning pen with your phone number on it!
By visiting on a consistent basis, it shows belief and commitment to the organization and mission. Make sure that you visit ALL potential referral sources, even hard cases. Eventually, hard cases will crack. Condition your outreach staff to be able to hear “no” a thousand times. Have them picture themselves as “reaching the lost” like a zealot! It makes the rejection easier to take (it is truly amazing how the way we picture things effects our behavior). The best outreach specialists view the paper routes as their favorite duty because “its time to go visit my friends!” When taking vacations, let your route know so they will not be disappointed when you don’t show up…manage the expectation. Marketers and Outreach staff are “account managers.” Each physician, Nursing Home, or other referral source is literally a stream of revenue when one looks at it over the long-term. Loss of a single referral source could be cutting off $250,000 of revenue over the course of a year. When the CEO, clinician or someone in accounts payable offends a referral source, it is a big loss. Seeing it in perspective of “how much” gives us new energy to put forth the effort to repair the relationship.
Increase Average Length of Stay (ALOS) Increasing ALOS obviously increases ADC as people are on the program longer. This area demands much more attention than it gets. Here are some observations:
1. Deep Penetration in the Community . Here we are talking about getting referrals directly from the community. The hospices with the highest ALOS have a

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 252 of 370
disproportionate percentage of referrals from the community. How do they do it? 4 of the top 5 hospices that we work with the highest ALOS are ones with deep community ties. They seem to be very spiritual organizations and their communities know it and apparently appreciate it. Several of them have the Watchman Program or hit upon an approach that works. The key is to know your communities, know what they value, and develop deep inroads with key organizations and people. What we like about the Watchman Program is that it creates a new class of volunteer and effectively can set 1,000 more sets of eyes on the community. They are trained to in what to look for and “how” to best present the hospice option in a comfortable and friendly way. Other hospices with a high ALOS find other ways to connect to their communities. If you have large manufacturing plants that employ thousands of workers, find ways so that every employee knows about hospice. What do they do with their time? How could you plug into their world so that they will remember hospice when there is a need?
2. Filling in Knowledge Gaps . Recently, my mother was diagnosed with cancer of the brain. As we were talking one evening, I discovered that she did not know that hospice could help her NOW, even though she has 6-9 months to live. Even with my work in hospice for more than a decade, I had not done a good job at educating her on the subject. She believed that hospice was to be called “near the end.” It shocked me…and I knew that there is a ton of education work still to be done… Don’t take for granted that people really understand and know about the benefits of hospice…they don’t.
3. Define Your Language Regarding Length of Stay . As part of your standard outreach language, you must CONTINUALLY speak about the need for patients to get signed up sooner. Use testimonies of people that have said “if only we would have known about hospice sooner” and messages like this… Over time and through repetition, it works. Most of the time we just don’t say it enough.
4. Open Access . By expanding the paradigm of what a hospice looks like, usually ALOS will increase. Many hospices take patients that are seeking non-tradition hospice treatments and therapies. One result of this practice is that patients will sign up for hospice earlier in the disease process, thus increasing length of stay (LOS). For more information, request the audio CD Open Access, an Interview with Carolyn Cassin or Open Access II with Malene Davis.
The words and images we use are powerful. They shape behavior. When someone is promoted to “manager” suddenly they start to think differently. Almost like magic. In the case of marketing, many people view it distastefully. So change it! Use a term that is more likeable or better yet, one that people will get fired up about! I like OutReach. You may prefer Education. Give it some attention because it WILL shape the results you get.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 253 of 370
Speaking Points for General Referral Sources Hospices need defined language in order to deliver a consistent message. Use defined language to make sure all value points are covered. Clearly denominate the value in specific terms. Avoid generalities. Speak with absolute conviction. Speak in terms of assurance to avoid anxiety issues and concerns. Manage the expectations by clear denomination. Vagueness leads to expectation failure, anxiety, wondering imaginations, confusion, and results in a poor customer experience. Above all NEVER promise what you can’t deliver. If you can’t do it, you have no thing to market! Speaking Point Purpose
1. We offer CNA services 5 days a week if you want it.
“We sure could use some help!” Mom will look better, feel better, feel better about herself, and the caregivers feel better. What a great service! The idea is that a daily weekday visit is helpful for patients and families. Usually, during weekends, there are families around. The quantity of service is up to your ideals of care…BUT YOU MUST DENOMINTE THE VALUE IN SPECIFIC TERMS!!!
2. We give you a “Hospice Menu” so you can have control over the care you receive.
“Hold the pickles and the mayo!” How many times in our lives do we get to have control over our health care? With our hospice you can choose how often a CNA will visit. You can choose to die in your own bed and not an electric hospital bed. How do you want your hospice care? Do you want to be left in peace when the sacred moment comes?
3. We send admission staff within 4 hours of a referral or as soon as you are ready.
“How quickly will you respond to our needs?” Never say within 24 hours or as soon as possible. State the number of hours. It doesn’t matter WHO shows up. It’s important that someone shows up!
4. We do not discriminate against patients that are in need of hospice care just because they are seeking more aggressive treatment than other hospice patients. We will cover these therapies “for a period of time.”
“You take the tough and costly patients?” We JUST SAY YES! If we say NO, we end the dialogue. If we say YES, we continue the dialogue. We can have the “weaning” conversations with the patient, family,

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 254 of 370
Speaking Point Purpose and physician. We can help them
emotionally accept the end of futile care.
5. We check on all patients daily. We have contact with patients and families everyday.
“We are proactive about our care.” Every day we call to see how our patients and families are doing. We visit if it will give the patient/family a better experience. We do not just “respond” to crisis. We stay on top of the situation and monitor our patients and families.
6. Patients often live longer when Hospice care is involved as they feel secure, comforted and taken care of….the stress of aggressive treatment will take its toll.
“I will live longer!” The longer a facility can keep a patient in their care system, the more they can bill.
7. Our staff receive specialized training unlike any other hospice in the region. We have a 12 point program and a special way of selecting people for this work. Not everyone gets to work at Sunny Day!
“They are pros at what they do!” This is a point of distinction that separates your hospice from others. DO NOT use this point if this specialized training does not exist! Be prepared to elaborate on your “12 point” system.
8. The Hospice Medicare Benefits pays the high cost of your medications and covers ALL the costs associated with the life threatening illness.
“Hey, this is a good deal from a financial standpoint.” Too often we overlook the great value of the Medicare Hospice Benefit. Let’s talk about it more.
Behind the Scenes
It is the work that goes on behind the scenes that ultimately makes a hospice World Class. Hiring Profiles Determine the “right” people to work in
the hospice. We are a special breed. Look for candidates that WANT to serve or have a heart for people. If you already have a great clinician, then interview them and find out what makes them tick.
• What attracts them to Hospice?

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 255 of 370
• What type of ad did they respond to when they were hired?
• What is their personality type? • What is their energy level? • Where did they work before? • What do they do in their spare
time? • RESOURCES: Training or Lip
Service? CD; Marketing & OutReach (Revisited) CD; People Selection Process CD; World Class Hospice CD
Specialized Training Systems 12 Points of Relationship Building Skills We are Guests
• Seeing the World from THEIR Perspective
• Weaning Conversations • Getting Connected with the Staff • The Sunny Day Hospice Perfect
Visit • Problem Resolution • Use DVDs, audio CDs,
laminated hand-outs, knowledge systems, guidelines
• RESOURCES: Training or Lip Service? CD; Marketing & OutReach (Revisited) CD; People Selection Process CD; World Class Hospice CD
Create Tools for Great Caregiver Education
• Make a caregiver 80% better in 15 minutes with a super tool.
• Diagnostic Indicators • “How to Bill” colored laminated
guide. • Presentation Program • RESOURCES: Training or Lip
Service? CD; Marketing & OutReach (Revisited) CD; World Class Hospice CD
Create a WOW! Presentation • Excellent Wound Care

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 256 of 370
Program • Grieving Over the Loss of a Favorite Patient
• Managing Stress • Why Our Work is Important • RESOURCES: Marketing &
OutReach (Revisited) CD; World Class Hospice CD
Design OutReach Paper Routes • Create proposed paper routes based on geographic location.
• Test drive routes. • Create marketing ammunition
filing system • RESOURCES: Marketing &
OutReach (Revisited) CD Follow-Up Monitoring System • Track in Patient Management or
Donor System • Create codes • Log all calls and contacts. • RESOURCES: World Class
Hospice CD Reporting • Referral and Admission Report
by Person and Paper Route • Conversion Ratio • RESOURCES: The Quantified
Hospice Doc

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 257 of 370
Speaking Points for Nursing Homes/ALFs Speaking Point Purpose
1. If you let us serve “enough” patients in your facility, we will have our staff in your facility almost constantly.
“You’re going to help us with our short staffing problems?” Without crossing the lines of fraud and inducement, you indicate that the facility will benefit from hospice staff being available.
2. Staff that understand billing and reimbursement “hand deliver” checks within 14 days after we receive your invoice. They can answer questions about financial matters.
“How are we going to get paid?” Communication of specifics is critical to add comfort to the purchase decision. Having a person that is knowledgeable about reimbursement see the billing staff of the facility on a regular basis will reduce billing/payment problems and increase their comfort level working with Hospice.
3. We send admission staff within 4 hours of a referral.
“How quickly will you respond to our needs?” Never say within 24 hours or as soon as possible. State the number of hours.
4. We offer an incredible menu of in-service programs for your staff. You can select specific topics OR use our program sequence.
We want WOW! presentations. Not just good presentations, but GREAT presentations that are content rich and substantive. These are NOT about promoting our hospice. They will know that inherently. Give a meaningful presentation.
5. If your facility has 24-hour RN coverage, you can let your patients remain in your facility that need acute hospice care. Hospice will pay your facility $250 per day for this level of care.
“We can make some money?” This value point makes the facility aware that they can keep highly acute patients within their care system and benefit simultaneously from the higher reimbursement from Hospice.
6. Your facility will be able to keep patients longer with Hospice involved. This applies especially for Assisted Living.
“We can make more money!” The longer a facility can keep a patient in their care system, the more they can bill.
7. Our staff receive specialized training to work in your facility. We are guests in your facility. It is important for our staff to understand your specific needs and blend
“They are pros at what they do!” This is a point of distinction that separates your hospice from others. DO NOT use this point if this specialized training does not exist!

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 258 of 370
Speaking Point Purpose with your model of care….adding to and not taking away.
Be prepared to elaborate on your “21 point” system.
8. Hospice care in facilities is great for patients and families. The Medicare benefit covers the costs of medications, medical supplies and clinical care relating to the terminal illness.
“Hey, this is a good deal from a financial and a care standpoint.” Too bad this point is near the bottom of the list, but this point probably is best left as the “icing on the cake.” You surely should indicate this in the beginning of your pitch, but it is the best closer to the end.
9. State chart auditors will view your charting more favorably when they see that Hospice is involved.
“My charts will be better?” If a state auditor sees that the medical chart contains weight loss or other decline, but also sees that Hospice is involved, they will view it more positively. This point should be represented tactfully as it could be perceived as crossing into their turf and “harvesting patients.”

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 259 of 370
Community Support and Fundraising Many people wonder why there is little reference to community support or fundraising in this program. The reason is that too many hospices become “dependent” upon community dollars. As mentioned in the Communicating the Need to Balance the Ideas of Purpose and Profit section, a hospice that is dependent upon community dollars is only 1 public relations disaster from being extinct. It is a very unhealthy state for a hospice. On the other hand, if a hospice is strong and can operating on earned revenue, then community support becomes a competitive edge. These funds can be funneled into valued-added products and services. They can be used to build large reserves in a short period of time. Community support is a good thing and we encourage hospices to garner it and be excellent stewards. However, it should NEVER be relied upon. Knowing that community dollars are available can make a hospice undisciplined and wasteful. The point is “Operate your hospice as if you receive ZERO suppor t from the community.” If you are able generate community support, here are some ideas:
• Thrift or Resale Shops – The average shops has a 51% margin and communities value them. A well managed shop will produce a higher and more consistent return that most other community support options. Call MVI for the CD on Resale Shops.
• Bequests – Hospices that master this area build reserves faster than any other community support option as large gifts are received by the hospice. The size of the gifts range from a few thousand dollars to millions. To be excellent at this takes work in the form of a cultivation process. Keys are having people (or a person) that have absolute integrity and the ability to clearly articulate the need. Above all, they must be trusted.
• Seasonal Signature Events – Galas, Taste of the Town, Celebrity Auctions, Tree of Lights, Golf Tournaments, Bike Rides, etc. are all examples of events that can be systemized. If possible, volunteers should do the majority of the work. If staff members are doing most of the work, perhaps you do not have the right leader of the volunteer area.
Casual versus Event-Driven Support At MVI, we classify community support into two categories, casual and event-driven. Casual support is composed of contributions and memorials. They are not linked or tied to a specific event or action. The Development Department receives credit for this support in our book as they can influence the volume to some degree.

The MVI Clinical Leader Program
________________________________________________________________ Multi-View Incorporated Systems
PO Box 2327 Hendersonville, NC 28793
828-698-5885 or multiviewinc.com
©Copyright 2009 Multi-View Incorporated Systems Page 260 of 370
Event-Driven support is linked or associated with some event or activity. In each case an Income and an Expense account should be added to the General Ledger to track the return on the investment. If a hospices has a large volume of small events, they can be grouped into several specific accounts and used perpetually It is important to segregate community support into specific classifications in the General Ledge and Donor System so that each item can be monitored and measured.
Activity Logs & Time Tracking As the Clinical Leader, the Activities Logs of your area or team are your responsibility. Late logs put unnecessary burden on Payroll, Billing and other areas. If a hospice wants to see a drastic improvement in the timeliness of Activity Logs, just link them to compensation. No logs, no pay. Time tracking is always an issue and most hospices spend entirely too much time on the subject. Laptops and remote field devices have helped. However, there still needs to be standards and clear expectations for this area. The following is an example for a “paper process” which incorporates some of the best ideas we have seen. Many of the concepts of this “paper process” are translatable to a electronic documentation environment. Simple is always best. Clear definitions are needed. Activity logs need to be easy to complete. Goals & Explanations:
• To reduce the time needed to complete the form by staff. Many hospices spend literally tens of thousands of dollars of staff time on Activity Logs. It should take less than 5 minutes to complete an Activity Log.
• There should be an economy of Activity Codes. Too many codes inherently
increase the probability of errors. Plus, we have never witnessed a single hospice that really utilized the information from an anal-retentive coding system. If you create STANDARDS (productivity, visit expectations, etc.) and you are monitoring them on a consistent basis, then does it really matter how much time is spent doing non-direct things? If our hospice needs an average of 4 visits a day for RNs, then measure actual performance against the standard. The other time is not critical to track in detail. Here are our recommended standards for clinical staff: Nursing – 4 visits per day, CNA – 4.5 to 5 visits per day, SW – 3 visits per day, PCs (Chaplains) – 5 visits per day.