xavier forns, md liver unit, hospital clínic idibaps and cibrehd barcelona, octubre 2013...
TRANSCRIPT
Xavier Forns, MDLiver Unit , Hospital ClínicIDIBAPS and CIBREHD
Barcelona, Octubre 2013
Tratamiento de poblaciones especialesTratamiento de poblaciones especiales
Curso de Residentes AEEHCurso de Residentes AEEH

Patient survival in HCV-positive and HCV-negative individuals. ONT/ RETH (1991-2011)
Patient survival in HCV-positive and HCV-negative individuals. ONT/ RETH (1991-2011)
Hepatitis C recurrence after liver transplantation
• 65-year old patient with HCV-related liver cirrhosis
• An US examination reveals 2 HCC (3,5+1 cm diameter)
• After extensive evaluation the patient is included in the waiting list for liver transplantation.
Treatment of hepatitis C in the waiting list of liver transplantation
• Genotype 1b IL28 CT; Viral load 830.000 IU/mL
• Previous therapy with PegIFN and RBV in 2008: partial responder (> 2 log decrease in VL at week 12).

• Should we treat this patient in the waiting list?
• Bilirubin 1 mg/dL, albumin 39 g/dL, platelets 119.000
No ascites, transient elastography 19 kPa.
• What treatment would you propose?
a) PegIFN + RBV
b) PegIFN+RBV+PI (telaprevir/boceprevir)
Treatment of hepatitis C in the waiting list of liver transplantation
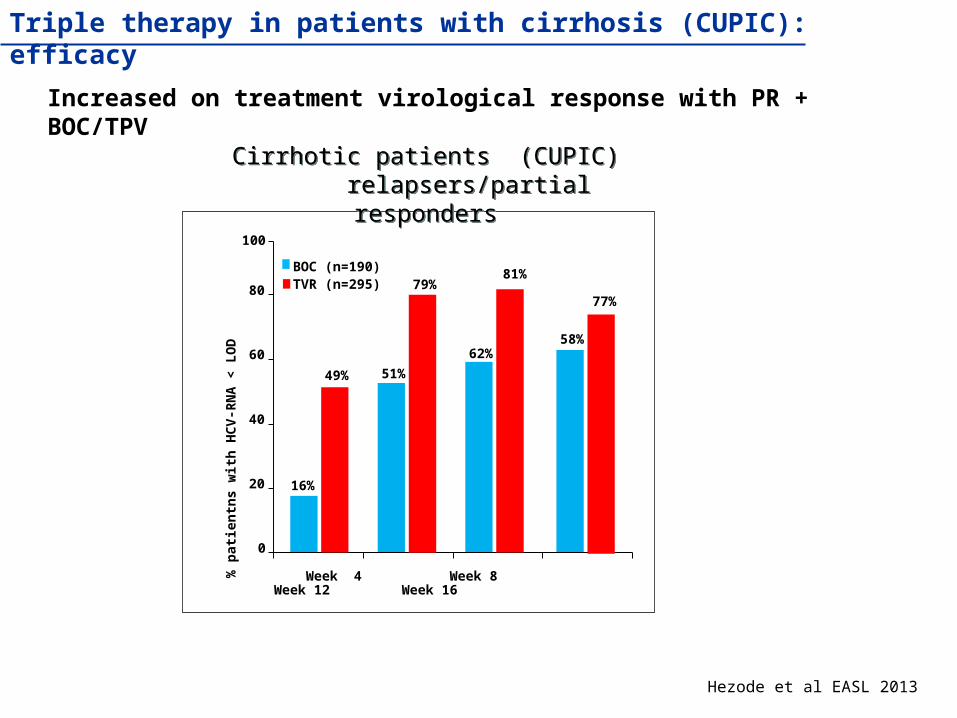
Triple therapy in patients with cirrhosis (CUPIC): efficacy
Increased on treatment virological response with PR + BOC/TPV
Hezode et al EASL 2013
0
20
40
60
80
% p
atie
ntn
s w
ith
HC
V-R
NA
< L
OD
49%
51%
62%
81%
77%
58%
BOC (n=190)TVR (n=295)
100
79%
16%
Cirrhotic patients (CUPIC) relapsers/partial responders
Cirrhotic patients (CUPIC) relapsers/partial responders
Week 4 Week 8 Week 12 Week 16

Pro
bab
ility
of
bac
teri
al in
fect
ion
s
0 60 120 180 240 3000,0
0,2
0,4
0,6
0,8
1,0P < 0.01
Control (n = 51)
Peg-IFN + RBV (n = 51)
Time (days)P
rob
abili
ty o
f b
acte
rial
infe
ctio
ns
0 60 120 180 240 3000,0
0,2
0,4
0,6
0,8
1,0P < 0.01
Child B–C(n = 57)
Child A (n = 45)
Time (days)
Risk of life-threatening side effects: bacterial infections (SBP, SB)
Carrion JA ,et al. J Hepatol. 2009
Safety of antiviral therapy in patients awaiting liver transplantation
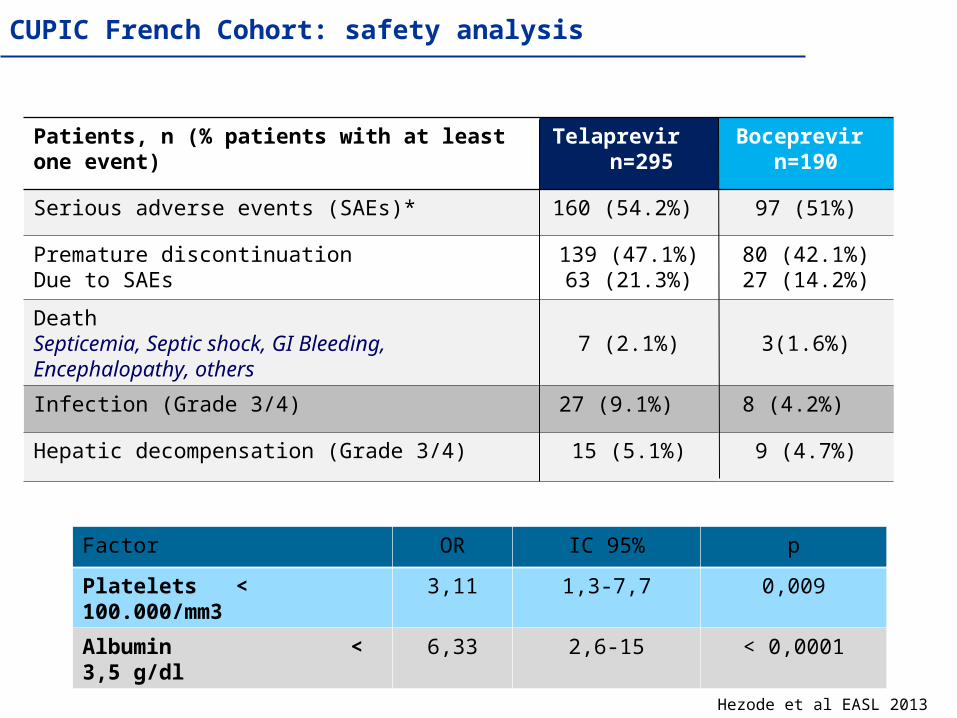
Patients, n (% patients with at least one event) Telaprevir n=295
Serious adverse events (SAEs)* 160 (54.2%)
Premature discontinuationDue to SAEs
139 (47.1%)63 (21.3%)
DeathSepticemia, Septic shock, GI Bleeding, Encephalopathy, others
7 (2.1%)
Infection (Grade 3/4) 27 (9.1%)
Hepatic decompensation (Grade 3/4) 15 (5.1%)
Boceprevir n=190
97 (51%)
80 (42.1%)27 (14.2%)
3(1.6%)
8 (4.2%)
9 (4.7%)
CUPIC French Cohort: safety analysis
Hezode et al EASL 2013
Factor OR IC 95% p
Platelets < 100.000/mm3 3,11 1,3-7,7 0,009
Albumin < 3,5 g/dl 6,33 2,6-15 < 0,0001
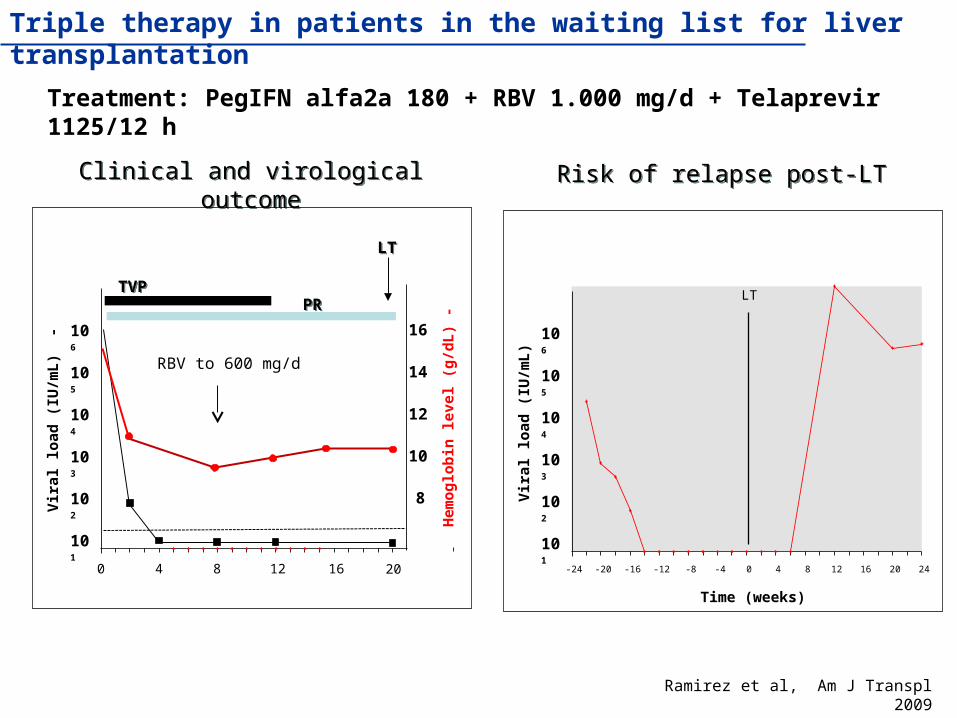
Triple therapy in patients in the waiting list for liver transplantation
Treatment: PegIFN alfa2a 180 + RBV 1.000 mg/d + Telaprevir 1125/12 h
-24 -20 -16 -12 -8 -4 0 4 8 12 16 20 24
LT
Vir
al l
oad
(IU
/mL
)
Time (weeks)
101
102
103
104
105
106
Ramirez et al, Am J Transpl 2009
Risk of relapse post-LTRisk of relapse post-LTClinical and virological outcomeClinical and virological outcome
0 4 8 12 16
Vir
al l
oad
(IU
/mL
) -
101
102
103
104
105
106
Hem
og
lob
in l
evel
(g
/dL
) -
20
8
10
12
14
16
RBV to 600 mg/d
TVPTVPPRPR
LTLT

Treatment in patients awaiting LT: risk of resistance
Years after end of therapy
0 0.5 1.0 1.5 2.0
91%
71%
62%59%
100
80
60
40
20
0
V36MT54S
R155KAny mutation
Cum
ula
tive
rat
e of
re
vers
ion
to w
ild-t
ype
(%
)
Weeks after end of therapy
Vierling et al EASL 2010
Selection of PIs resistance strains may compromise treatment after LT in case of severe hepatitis C recurrence
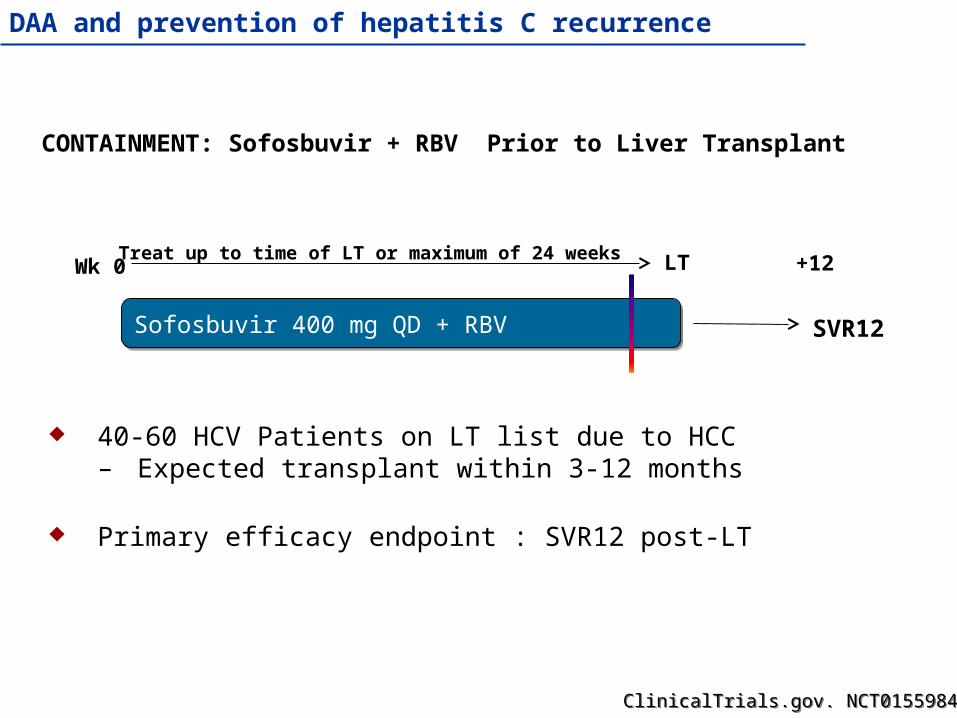
Wk 0 +12
Sofosbuvir 400 mg QD + RBVSofosbuvir 400 mg QD + RBV SVR12
CONTAINMENT: Sofosbuvir + RBV Prior to Liver Transplant
40-60 HCV Patients on LT list due to HCC– Expected transplant within 3-12 months
Primary efficacy endpoint : SVR12 post-LT
LTTreat up to time of LT or maximum of 24 weeks
ClinicalTrials.gov. NCT01559844 ClinicalTrials.gov. NCT01559844
DAA and prevention of hepatitis C recurrence

• 66-year old patient with hepatitis C recurrence after LT
• Transient elastography (12 months after LT) 10 kPa.
• Liver biopsy: F3
Treatment of hepatitis C in the liver transplant setting
Should we treat the patient? How?
1) PegIFN-RBV
2) PegIFN-RBV + PI
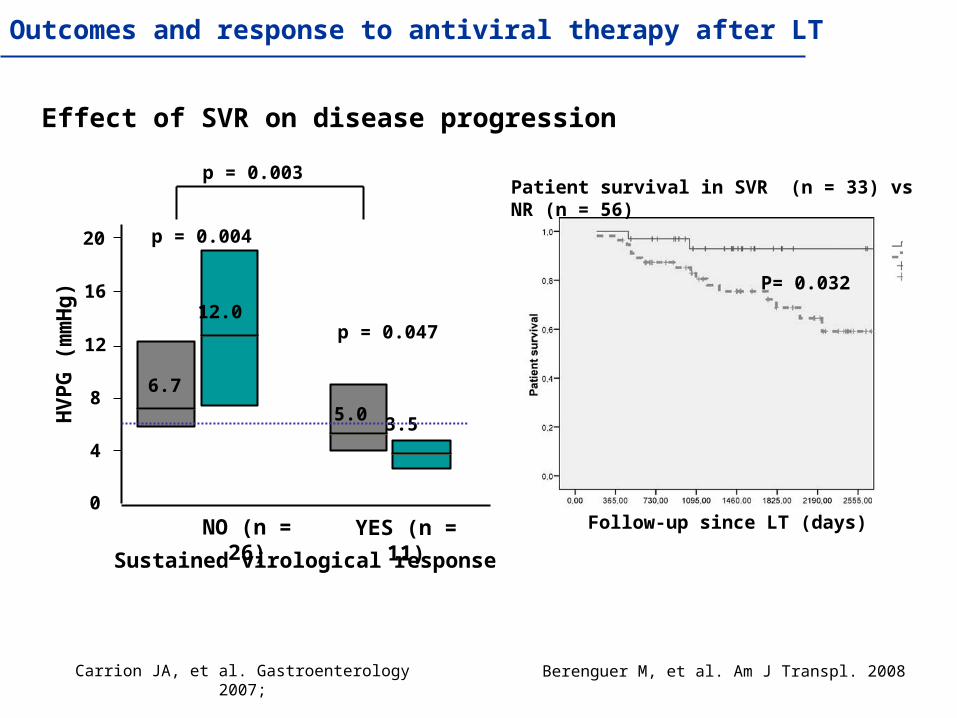
Carrion JA, et al. Gastroenterology 2007;
Effect of SVR on disease progression
4
8
12
16
20
HV
PG
(m
mH
g)
0
12.0
6.7
5.0 3.5
p = 0.047
p = 0.004
p = 0.003
NO (n = 26) YES (n = 11)
Sustained virological response
Berenguer M, et al. Am J Transpl. 2008
Patient survival in SVR (n = 33) vs NR (n = 56)
P= 0.032
Follow-up since LT (days)
Outcomes and response to antiviral therapy after LT

• Immunosuppression: tacrolimus 2 mg/d (levels 7 ng/mL)
Treatment of hepatitis C in the liver transplant setting
• Bilirubin 1 mg/dL, AST 243 IU/L, GGT 323 IU/L, Br 1,6 mg/dL, Hb 12,6 g/L, platelets 121.000, neutrophils 2300
• If we use a PI, use telaprevir or boceprevir?
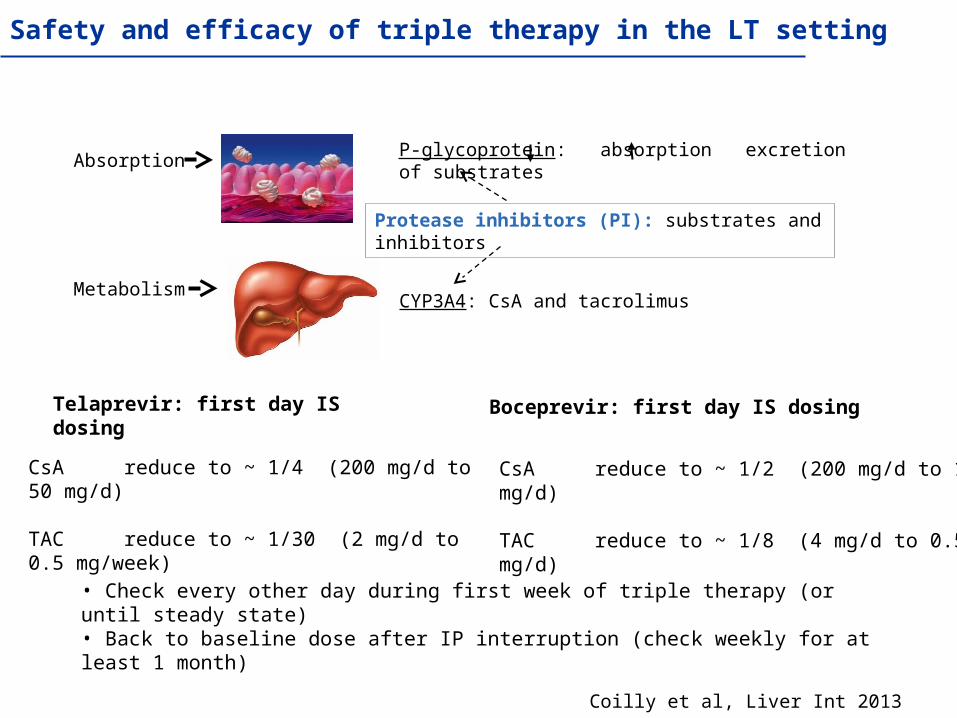
Absorption
Metabolism
P-glycoprotein: absorption excretion of substrates
CYP3A4: CsA and tacrolimus
Protease inhibitors (PI): substrates and inhibitors
CsA reduce to ~ 1/4 (200 mg/d to 50 mg/d)
TAC reduce to ~ 1/30 (2 mg/d to 0.5 mg/week)
Telaprevir: first day IS dosing
CsA reduce to ~ 1/2 (200 mg/d to 100 mg/d)
TAC reduce to ~ 1/8 (4 mg/d to 0.5 mg/d)
Boceprevir: first day IS dosing
• Check every other day during first week of triple therapy (or until steady state)• Back to baseline dose after IP interruption (check weekly for at least 1 month)
Coilly et al, Liver Int 2013
Safety and efficacy of triple therapy in the LT setting

0 8 12 24 48
Vir
al l
oad
(IU
/mL
)
101
102
103
104
105
106
Hem
og
lob
in l
evel
(g
/dL
)
12
8
10
12
14
16
RBV 600 mg/d
Transfusion and EPO
4
Fs 10 kPaFs 10 kPa Fs 6,3 kPaFs 6,3 kPa
Treatment of hepatitis C in the liver transplant setting
RBV 400 mg/d
Tarcolimus 2 mg/d a 0,4 mg/d Tarcolimus 0,4 mg/d a 2,5 mg/d
PRPR PR+ BOCPR+ BOC
Coilly et al EASL 2013; Verna et al EASL 2013
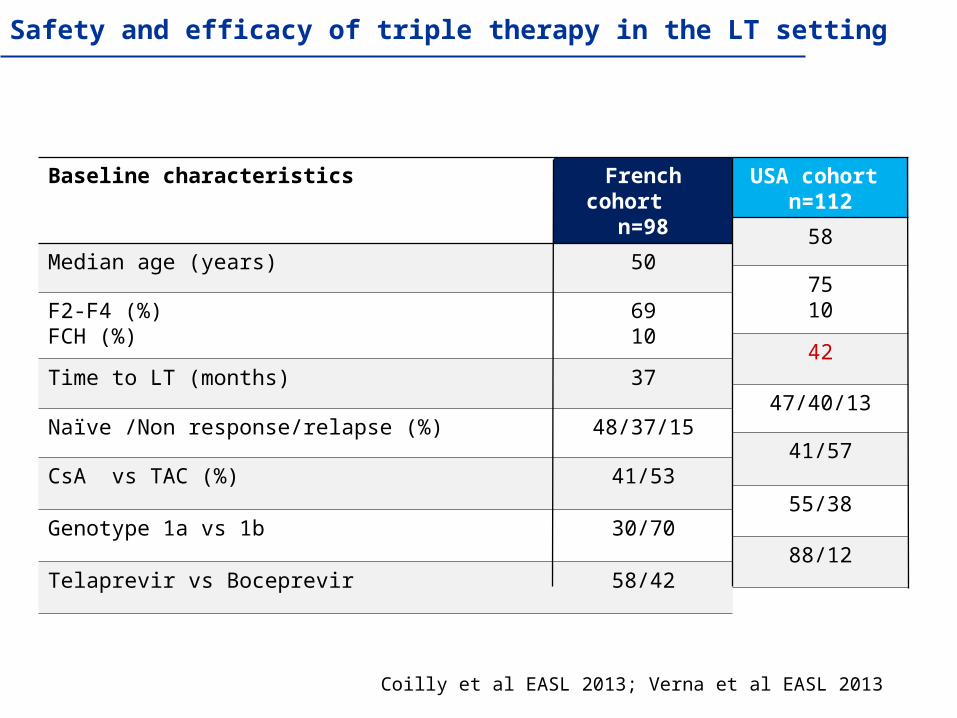
Safety and efficacy of triple therapy in the LT setting
Baseline characteristics French cohort n=98
Median age (years) 50
F2-F4 (%)FCH (%)
6910
Time to LT (months) 37
Naïve /Non response/relapse (%) 48/37/15
CsA vs TAC (%) 41/53
Genotype 1a vs 1b 30/70
Telaprevir vs Boceprevir 58/42
USA cohort n=112
58
7510
42
47/40/13
41/57
55/38
88/12
Coilly et al EASL 2013
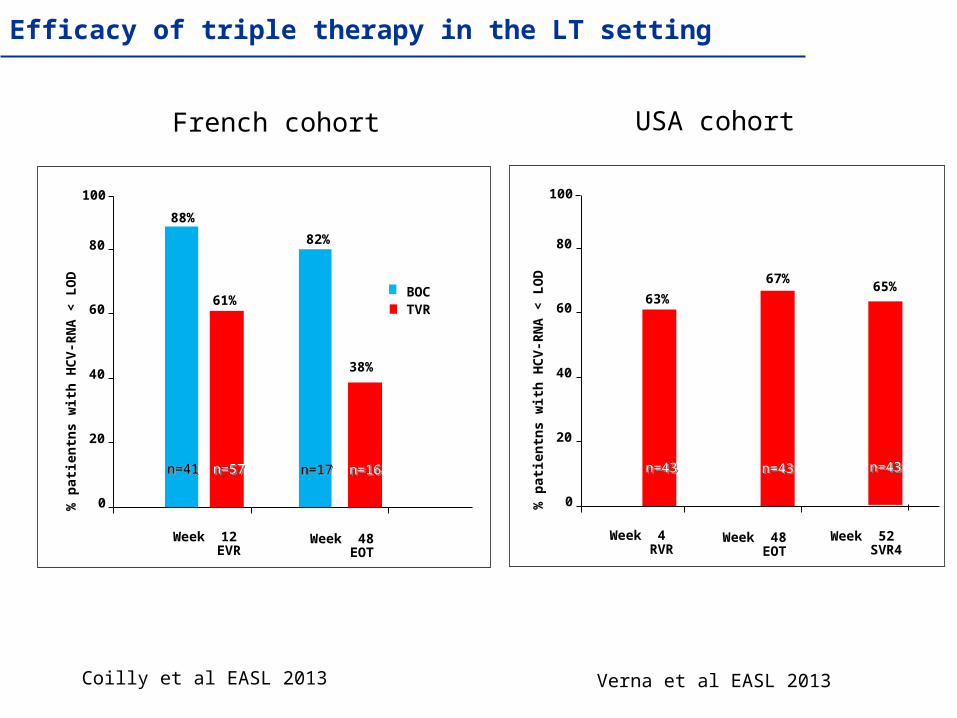
French cohort
Efficacy of triple therapy in the LT setting
Week 12 EVR
0
20
40
60
80
% p
atie
ntn
s w
ith
HC
V-R
NA
< L
OD
61%
82%
BOC TVR
100
38%
88%
Week 48 EOT
n=41n=41 n=57n=57 n=17n=17 n=16n=16
USA cohort
Week 4 RVR
0
20
40
60
80
% p
atie
ntn
s w
ith
HC
V-R
NA
< L
OD
63%
100
67%
Week 48 EOT
n=43n=43 n=43n=43
Verna et al EASL 2013
65%
Week 52 SVR4
n=43n=43
Coilly et al EASL 2013; Verna et al EASL 2013
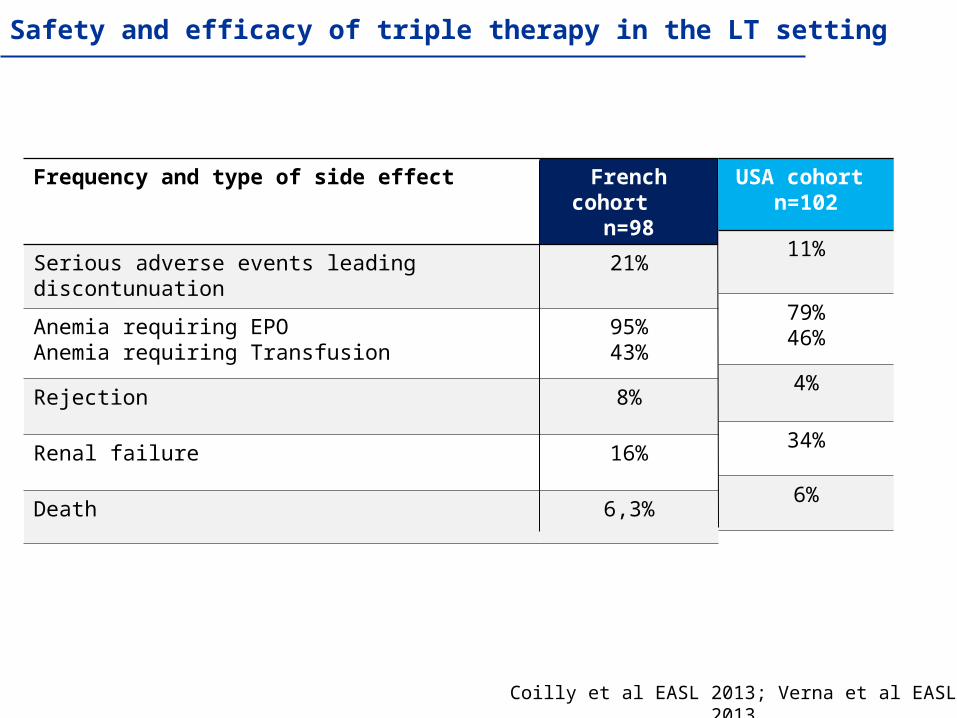
Safety and efficacy of triple therapy in the LT setting
Frequency and type of side effect French cohort n=98
Serious adverse events leading discontunuation 21%
Anemia requiring EPOAnemia requiring Transfusion
95%43%
Rejection 8%
Renal failure 16%
Death 6,3%
USA cohort n=102
11%
79%46%
4%
34%
6%
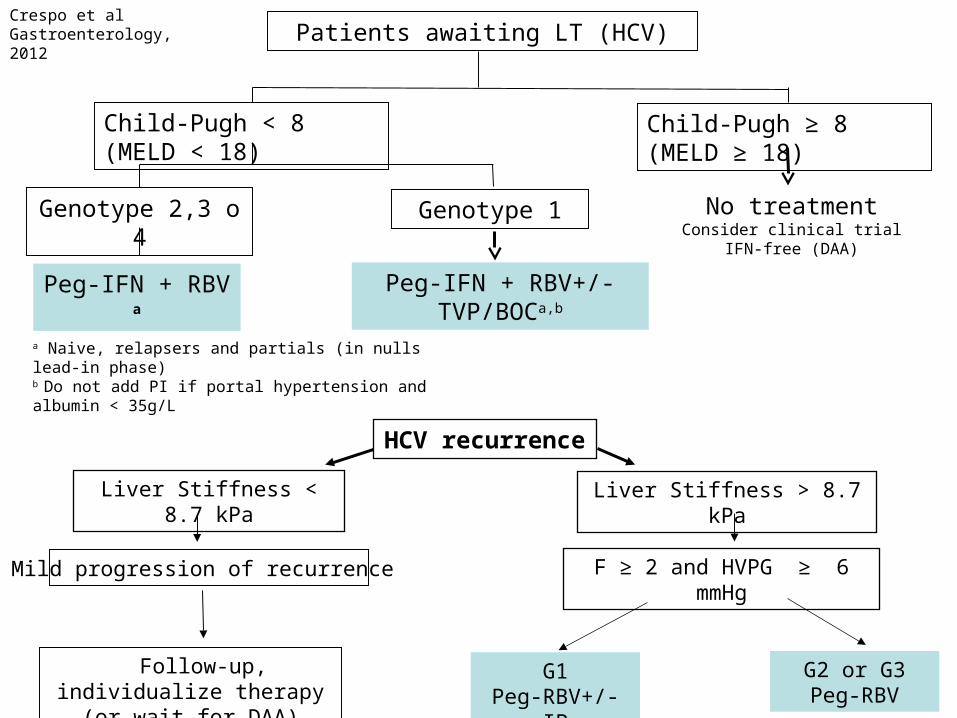
Patients awaiting LT (HCV)
Child-Pugh < 8 (MELD < 18)
Genotype 2,3 o 4
Peg-IFN + RBV a
Genotype 1
Peg-IFN + RBV+/- TVP/BOCa,b
Child-Pugh ≥ 8 (MELD ≥ 18)
No treatmentConsider clinical trial IFN-free (DAA)
a Naive, relapsers and partials (in nulls lead-in phase)b Do not add PI if portal hypertension and albumin < 35g/L
HCV recurrence
Follow-up, individualize therapy (or wait for DAA)
Mild progression of recurrence
Liver Stiffness < 8.7 kPa
F ≥ 2 and HVPG ≥ 6 mmHg
Liver Stiffness > 8.7 kPa
G2 or G3Peg-RBV
G1Peg-RBV+/- IP
Crespo et al Gastroenterology, 2012
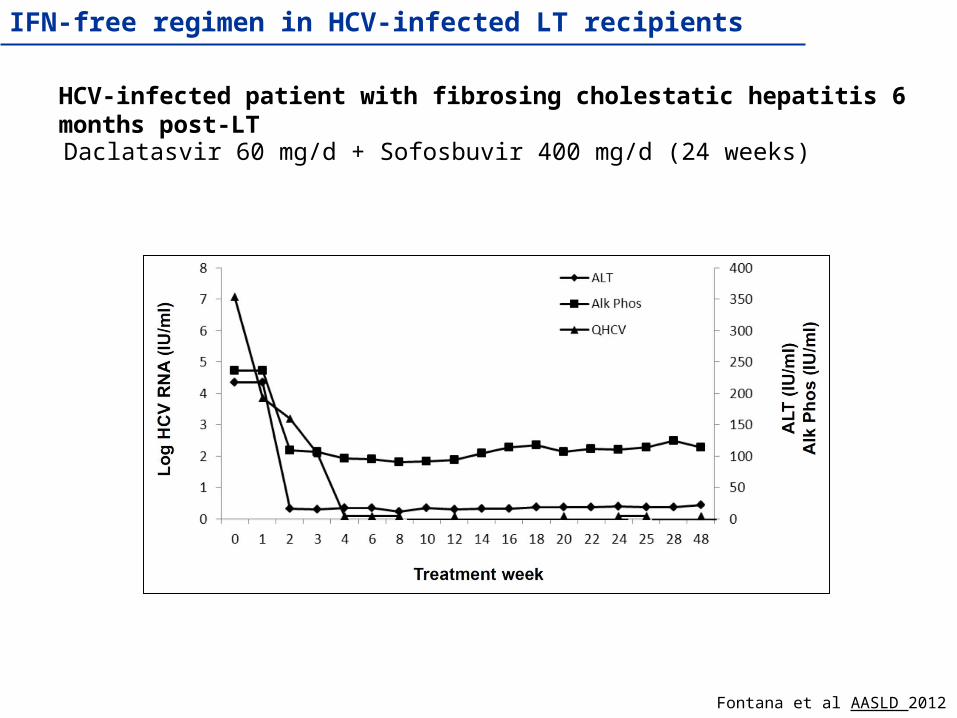
HCV-infected patient with fibrosing cholestatic hepatitis 6 months post-LT
Daclatasvir 60 mg/d + Sofosbuvir 400 mg/d (24 weeks)
Fontana et al AASLD 2012
IFN-free regimen in HCV-infected LT recipients
Viral Hepatitis UnitViral Hepatitis Unit
Liver Transplantation UnitLiver Transplantation Unit