© bhm healthcare solutions 2014 understanding the mind/body connection and the treatment of...
TRANSCRIPT
© BHM Healthcare Solutions 2014
Understanding the Mind/Body Connection and the Treatment of Depression
Presented by Mark Rosenberg, MD, Ph.D.
CEO, BHM Healthcare Solutions
© BHM Healthcare Solutions 2014
Learning Objectives
To gain a General Understanding of Major Depressive Disorder (MDD)
To Understand the Economic Burden of MDD from multiple perspectives
To Provide a Comprehensive Review of Diagnosis Strategies Based on the Diagnostic and Statistical Manual of Mental Disorders
To Discuss and Understand Traditional Pharmacologic Treatment, and Gain an Appreciation of Treatment from the Mind-Body Perspective
To Discuss Initial Treatment of MDD and Treatment after Therapeutic Failure as Recommended by the APA Guidelines
To Identify Follow-up Tools and Communication Strategies to Improve Management of MDD
© BHM Healthcare Solutions 2014
Presentation OverviewDisease Overview
Costs of MDD
Diagnosis Strategies for MDD
Pharmacologic Treatment and Gaining a Mind-Body Perspective
Improving the Outcome

© BHM Healthcare Solutions 2014
DISEASE OVERVIEW

© BHM Healthcare Solutions 2014
Prevalence of the MDD
• In any given year 14.8 million American adults, or 6.7% of the US population, suffer from major depressive disorders
• Depression is the leading cause of disability in the US
• By 2020 it is projected that depression will be the leading cause of disability worldwide
• Average age of onset = 32
http://www.nimh.nih.gov/health/publications/the-numbers-count-mental-disorders-in-america/index.shtml#Intro

© BHM Healthcare Solutions 2014
Prevalence of MDD
http://www.cdc.gov/features/dsdepression/
© BHM Healthcare Solutions 2014
Prevalence of MDD
• High rate of occurrence – 17% lifetime prevalence, this prevalence corresponds to a national population projection of 32.69 to 35.1 million US adults with lifetime MDD and 13.1 to 14.2 million US adults with a 12 month prevalence of MDD
• Episodes of long duration- 33% of patients have episodes > 2 years’ duration
• >50% rate of recurrence within 2-3 years of recovery (8 weeks of minimal depressive symptoms)
• Morbidity comparable to angina and advanced coronary artery disease
• High mortality (15%) from suicide in depressed patients hospitalized once for depression
Keller MB. J. Clin Psychiatry. 1999; 50(suppl 17):41-45Kessler RC, et al. Arch Gen Psychiatry. 1994:51:9-19Laveril PW, et al. Int J Meth Psychiatry Res. 1994;4:211-229Meuller 11, et al. Amer J Psychiatry. 1999;156:1000-1006Wells KB, et al. JAMA. 1989;262:914-919
Aben L, et al. Stroke. 2002;33:2391-2395Barefoot JC, et al. Circulation. 1996;93:1976-1996.Aben L, et al. J Neurol Neurosurg Psychiatry. 2003; 74:581-585Keller MB, et al. Arch Gen Psychiatry. 1992;49:809-816
© BHM Healthcare Solutions 2014© BHM Healthcare Solutions 2014
BH/PC: The Treatment Gap
• Surveys show that 40% of patients with major depression do not want, or perceive the need, for treatment.
• Only 20%-30% of patients with mental health disorders report them to a primary care physician.
• 33% of patients presenting in the ER with acute chest pain are suffering from either panic disorder or depression.
• 80% of patients with depression initially present with physical symptoms such as fatigue or chronic aches.
© BHM Healthcare Solutions 2014
Major Depression Disorder (MDD): Urgency to Treat
• MDD has become a major public health concern and is responsible for significant social impairment, including deterioration of family and interpersonal relationships, lost work productivity, and general suffering
• MDD is the most common psychiatric disorder in the United States
• Few patients receive adequate treatment• Depression is frequently associated with, and may negatively
impact other medical disorders• Inadequately treated depression may have progressive course
and may be associated with functional and structural changes in the brain
Murray CJ, et al. Science. 1996;274:740-743Greenberg PE, et al. J Clin Psychiatry 2003;64:1465-1475Kessler RC, et al. JAMA. 2003;289:3095-3105Everson SA, et al. Arch Intern Med. 1998;158:1138

© BHM Healthcare Solutions 2014
MDD: Progression to Disorder and Recovery
1
Nonadherence,4
Treatment Phases
up to 50% up to 70%
Acute Continuation/MaintenanceRemission Delay Time to
Major Depressive EpisodeTreatment Goals
> 12 wks10-12 wksTime
Response
Remission Recovery
Seve
rity
Safety & Tolerability
Effic
acy
Symptoms
Euthymia
Syndrome
Progression
to Disorder1. Kupfer DJ. J Clin Psychiatry.1991;52(5 suppl):28-34.2. APA. Am J Psychiatry.2000;157(4 suppl):1-45.3. Lin EH, et al. Med Care.1995;33(1):67-74.4. Simon GE, et al. Gen Hosp Psychiatry. 1993;1:399 -408.
5. AHCPR Depression Guideline Panel. 1993.6. VHA/DoD Major Depressive Disorder Working Group. 2000 (ModuleA).1-35.
Kupfer DJ. J Clin Psychiatry. 1991;52(suppl):28-34APA. Am J Psychiatry. 2000;157(4 suppl):1-45Lin EH, et al. Med Care. 1995;33(1):67-74Simon GE, et al. Gen Hosp Psyciatry. 1993;15:399-408
AHCPR Depression Guideline Panel 1993.VHA/DoD Major Depressive Disorder Working Group 2000 (Module A). 1-35

© BHM Healthcare Solutions 2014
Progression of Depression: Adverse Effects of each Successive Episode
© BHM Healthcare Solutions 2014
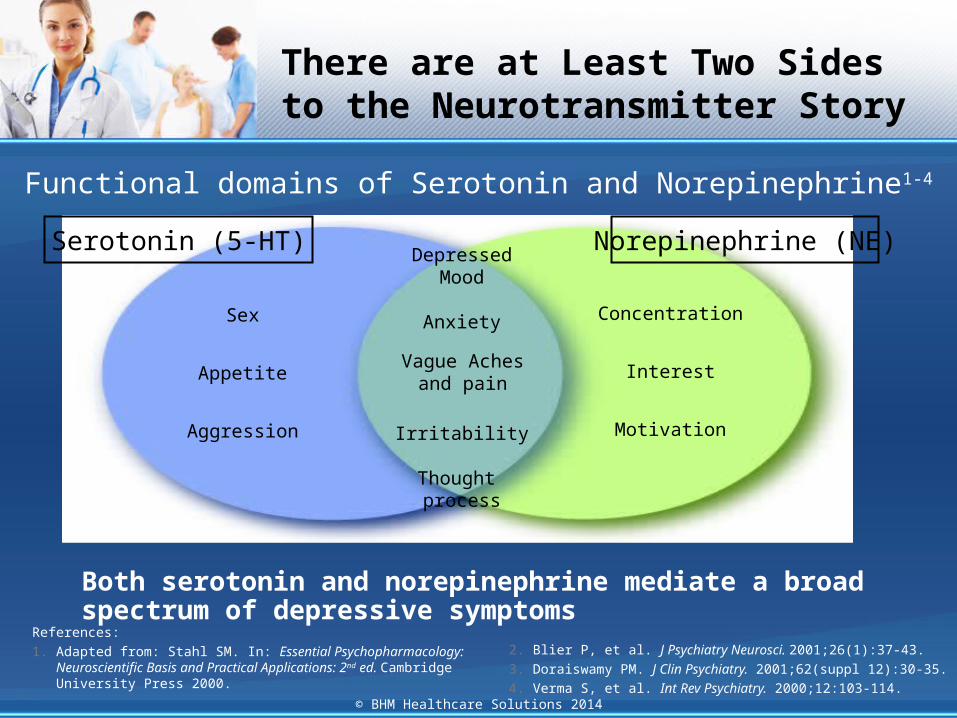
There are at Least Two Sides to the Neurotransmitter Story
Sex
Appetite
Aggression
Concentration
Interest
Motivation
Depressed Mood
Anxiety
Irritability
Thought process
References:
1. Adapted from: Stahl SM. In: Essential Psychopharmacology: Neuroscientific Basis and Practical Applications: 2nd ed. Cambridge University Press 2000.
2. Blier P, et al. J Psychiatry Neurosci. 2001;26(1):37-43.
3. Doraiswamy PM. J Clin Psychiatry. 2001;62(suppl 12):30-35.
4. Verma S, et al. Int Rev Psychiatry. 2000;12:103-114.
Norepinephrine (NE)
Both serotonin and norepinephrine mediate a broad spectrum of depressive symptoms
Serotonin (5-HT)
Vague Aches and pain
Functional domains of Serotonin and Norepinephrine1-4
© BHM Healthcare Solutions 2014
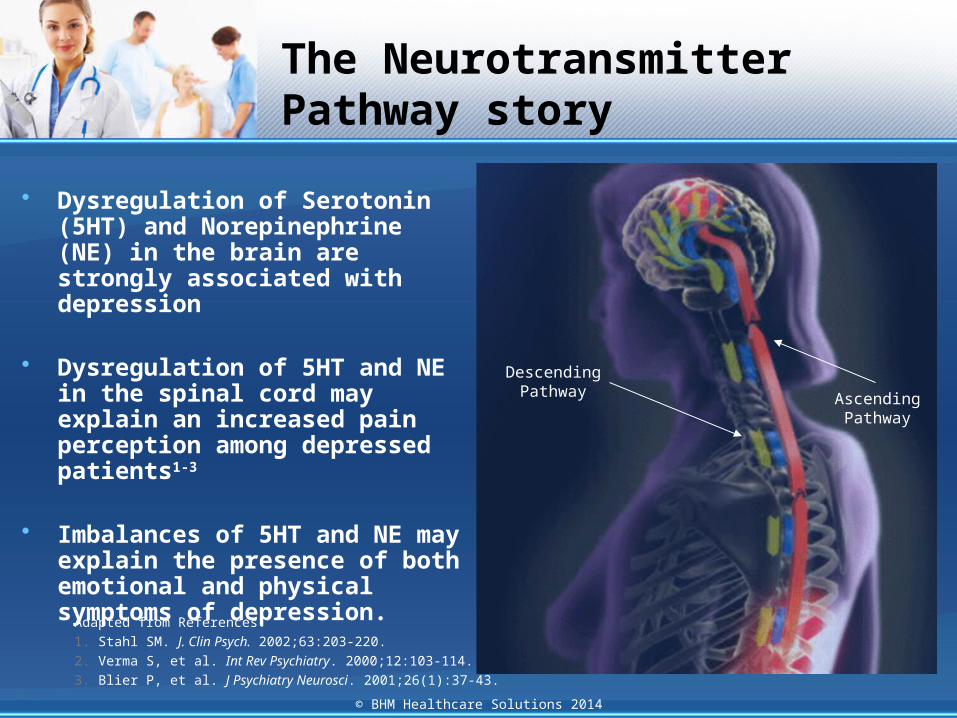
The Neurotransmitter Pathway story
Adapted from References:
1. Stahl SM. J. Clin Psych. 2002;63:203-220.
2. Verma S, et al. Int Rev Psychiatry. 2000;12:103-114.
3. Blier P, et al. J Psychiatry Neurosci. 2001;26(1):37-43.
• Dysregulation of Serotonin (5HT) and Norepinephrine (NE) in the brain are strongly associated with depression
• Dysregulation of 5HT and NE in the spinal cord may explain an increased pain perception among depressed patients1-3
• Imbalances of 5HT and NE may explain the presence of both emotional and physical symptoms of depression.
Descending Pathway
Ascending Pathway
AscendingPathway
DescendingPathway
© BHM Healthcare Solutions 2014
THE COSTS OF MAJOR DEPRESSIVE DISORDER

© BHM Healthcare Solutions 2014
MDD is Disabling and an Economic Burden
Rank 1990 2020 (est.)
1. Lower respiratory infections
Ischemic heart disease
2. Peri-natal conditions
Major Depressive Disorder
3. HIV/Aids Road Traffic Accidents
4. Major Depressive Disorder
Cerebro-vascular disease
5. Diarrheal diseases
Chronic obstructive pulmonary disease Total Costs of $83.1
Billion (2000)
31%
7%
62%
The High Cost of MDD
Direct MedicalSuicide RelatedWorkplace
Murray CJ, et al. Science. 1996;274:740-743Greenberg PE, et al. J Clin Psychiatry. 2003;64:1465-1475
Disability Rank

© BHM Healthcare Solutions 2014
Workplace Burden: Impact of Depression on Absenteeism
http://www.gallup.com/poll/163619/depression-costs-workplaces-billion-absenteeism.aspx

© BHM Healthcare Solutions 2014
MDD and Healthcare Costs
• Depression is one of the top ten conditions driving medical costs, ranking 7th in a national survey of employers• The greatest cause of productivity loss among workers
• Depression is an important factor in morbidity and mortality of co-existing diseases
• The presence of type 2 diabetes nearly doubles an individual’s risk of depression and an estimated 28.5% of diabetic patients meet criteria for clinical depression
• Back/neck and other chronic pain also have a
significant depression/SA component
Jaeckels, Nancy “Improving the Value of Health Care Through a Successful Collaborative Care Model.” Ppnt. 2nd Annual Lifespan Psychiatry Quality Conference. 22 Oct. 2010

© BHM Healthcare Solutions 2014
Impact on Healthcare Costs
• High costs of unmet Behavioral Health needs and other unsuccessful chronic disease management due to the BH needs
• High costs of fragmented and uncoordinated care from PC to BH and inpatient settings• BH disorders account for half as many disability days as “all” physical conditions• Annual medical expenses--chronic medical & behavioral health conditions
combined cost 46% more than those with only a chronic medical condition• Top five conditions driving overall health cost (work related productivity + medical +
pharmacy cost)• Depression • Obesity• Arthritis • Back/Neck Pain• Anxiety
Jaeckels, Nancy “Improving the Value of Health Care Through a Successful Collaborative Care Model.” Ppnt. 2nd Annual Lifespan Psychiatry Quality Conference. 22 Oct. 2010
© BHM Healthcare Solutions 2014
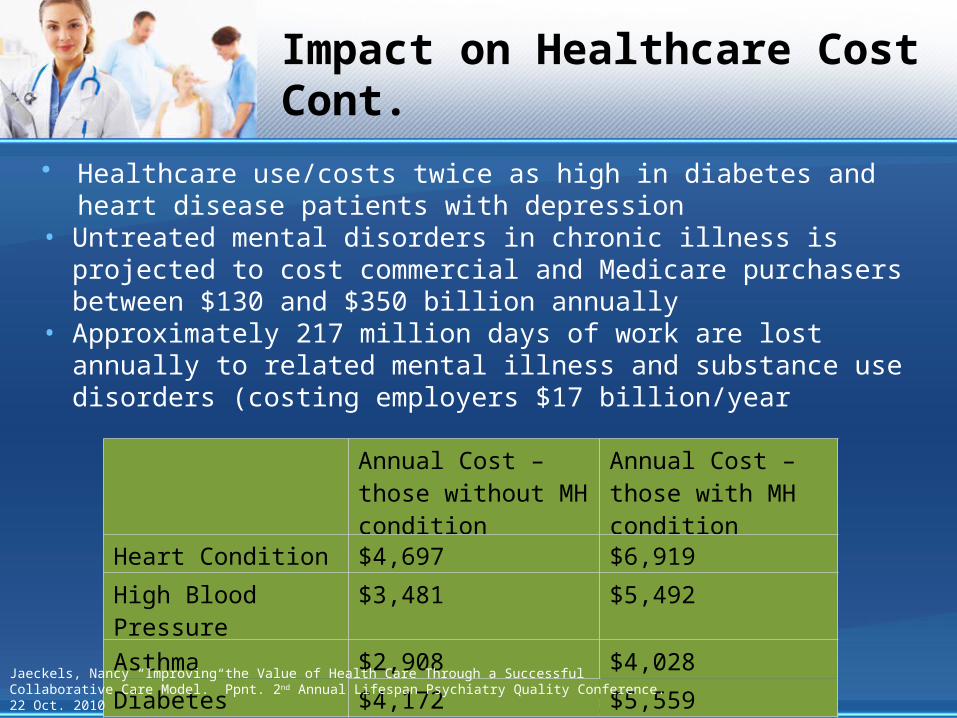
Annual Cost – those without MH condition
Annual Cost – those with MH condition
Heart Condition $4,697 $6,919
High Blood Pressure $3,481 $5,492
Asthma $2,908 $4,028
Diabetes $4,172 $5,559
Impact on Healthcare Cost Cont.
• Healthcare use/costs twice as high in diabetes and heart disease patients with depression
• Untreated mental disorders in chronic illness is projected to cost commercial and Medicare purchasers between $130 and $350 billion annually
• Approximately 217 million days of work are lost annually to related mental illness and substance use disorders (costing employers $17 billion/year
Jaeckels, Nancy “Improving the Value of Health Care Through a Successful Collaborative Care Model.” Ppnt. 2nd Annual Lifespan Psychiatry Quality Conference. 22 Oct. 2010

© BHM Healthcare Solutions 2014
DIAGNOSIS STRATEGIES FOR MAJOR DEPRESSIVE
DISORDER
© BHM Healthcare Solutions 2014
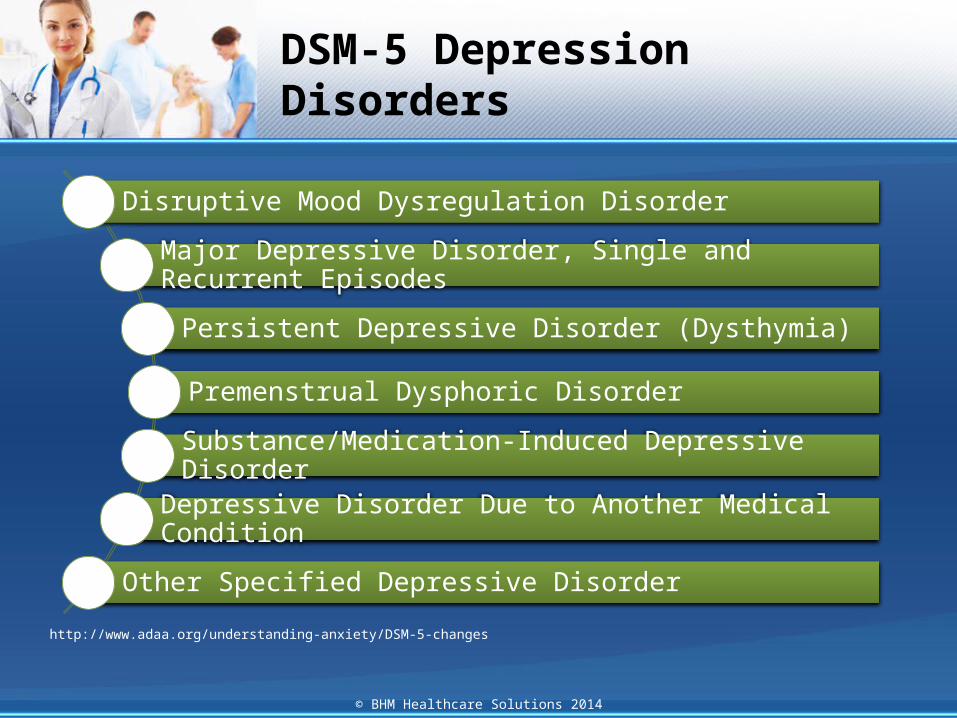
DSM-5 Depression Disorders
http://www.adaa.org/understanding-anxiety/DSM-5-changes
Disruptive Mood Dysregulation Disorder
Major Depressive Disorder, Single and Recurrent Episodes
Persistent Depressive Disorder (Dysthymia)
Premenstrual Dysphoric Disorder
Substance/Medication-Induced Depressive Disorder
Depressive Disorder Due to Another Medical Condition
Other Specified Depressive Disorder
© BHM Healthcare Solutions 2014
Comparison of DSM-IV to DSM-5 for Depressive Disorders
• DSM-5 contains new depressive disorders:
http://pro.psychcentral.com/dsm-5-changes-depression-depressive-disorders/004259.html
Disruptive Mood
Dysregulation Disorder
Premenstrual Dysphoric Disorder
© BHM Healthcare Solutions 2014
What’s new in DSM-5?
Major Depressive
Disorder
Bereavement Exclusion
Specifiers for Depressive Disorders

© BHM Healthcare Solutions 2014
Comparison of DSM-IV to DSM-5 for Depressive Disorders
• Major Depressive Disorder – No changes to the core criteria or symptoms for major depression, nor the prerequisite 2 week time period needed before it can be diagnosed. The coexistence within a major depressive episode of at least three manic symptoms is now acknowledged by the specifier “with mixed features”.
http://pro.psychcentral.com/dsm-5-changes-depression-depressive-disorders/004259.html
© BHM Healthcare Solutions 2014
Comparison of DSM-IV to DSM-5 for Depressive Disorders
• Bereavement Exclusion – removed in DSM-5:• To change the misperception that bereavement is temporary,
generally only lasting about 2 months. In actuality, bereavement can last up to 2 years.
• Bereavement is recognized as having a causal effect on major depressive episode(s) in vulnerable individual, which may begin to surface soon after the loss. When major depressive disorder occurs in the context of bereavement, an additional layer of risk may be added for suffering, feelings of worthlessness, suicidal ideation, poorer somatic health, worse interpersonal and work functioning, and an increased risk for persistent complex bereavement disorder.
http://pro.psychcentral.com/dsm-5-changes-depression-depressive-disorders/004259.html

© BHM Healthcare Solutions 2014
Comparison of DSM-IV to DSM-5 for Depressive Disorders
• Bereavement Exclusion cont. • Bereavement-related major depression is most likely to occur in
individuals with past personal and family histories of major depressive episodes. It is genetically influenced and is associated with similar personality characteristics, patterns of comorbidity, and risks of chronicity and/or recurrence as non–bereavement-related major depressive episodes.
• The depressive symptoms associated with bereavement-related depression respond to the same psychosocial and medication treatments as non–bereavement-related depression. In the criteria for major depressive disorder, a detailed footnote has replaced the more simplistic DSM-IV exclusion to aid clinicians in making the critical distinction be-tween the symptoms characteristic of bereavement and those of a major depressive episode.
http://pro.psychcentral.com/dsm-5-changes-depression-depressive-disorders/004259.html
© BHM Healthcare Solutions 2014
Comparison of DSM-IV to DSM-5 for Depressive Disorders
• Specifiers for Depressive Disorders – a new specifier was added to indicate the presence of mixed symptoms across both bipolar and depressive disorders, allowing the possibility of manic features in individuals with a diagnosis of bipolar depression.
http://pro.psychcentral.com/dsm-5-changes-depression-depressive-disorders/004259.html
© BHM Healthcare Solutions 2014
DSM-5 Characteristics of MDD
• 5+ of following symptoms present during the same 2-week period and represent change from previous functioning. At least 1 of the symptoms is either (1) depressed mood or (2) loss of interest in pleasure.
http://csmh.umaryland.edu/Conferences/ship/SHIPArchives/1.DSM5.%20SHIP%20CarltonMunson.pdf
Depressed mood most of the day, nearly everyday, as he indicated by subjective report or observation made by others (Note: In children and adolescents can be irritable mood).
Markedly diminished interest or pleasure in all or almost all, activities most of the day, nearly every day.
Significant weight loss when not dieting or weight gain (note: In children,… failure expected weight gain)
Insomnia or hypersomnia nearly every day.

© BHM Healthcare Solutions 2014
DSM-5 Characteristics of MDD cont.
http://csmh.umaryland.edu/Conferences/ship/SHIPArchives/1.DSM5.%20SHIP%20CarltonMunson.pdf
Psychomotor agitation or retardation nearly every day.
Fatigue or loss of energy nearly every day.
Feelings of worthlessness or excessive or inappropriate guilt.
Diminished ability to think or concentrate, or indecisiveness, nearly every day.
Recurrent thoughts of death (not just fear of dying), recurrent suicidal ideation without a specific plan, or a suicide attempt or a specific plan for committing suicide.

© BHM Healthcare Solutions 2014
DSM-5 Diagnostic Criteria for MDD
• According to the DSM-5 Criteria, a person who suffers from MDD must either have a depressed mood or a loss of interest or pleasure in daily activities consistently for at least two week period and represent change from previous functioning
© BHM Healthcare Solutions 2014
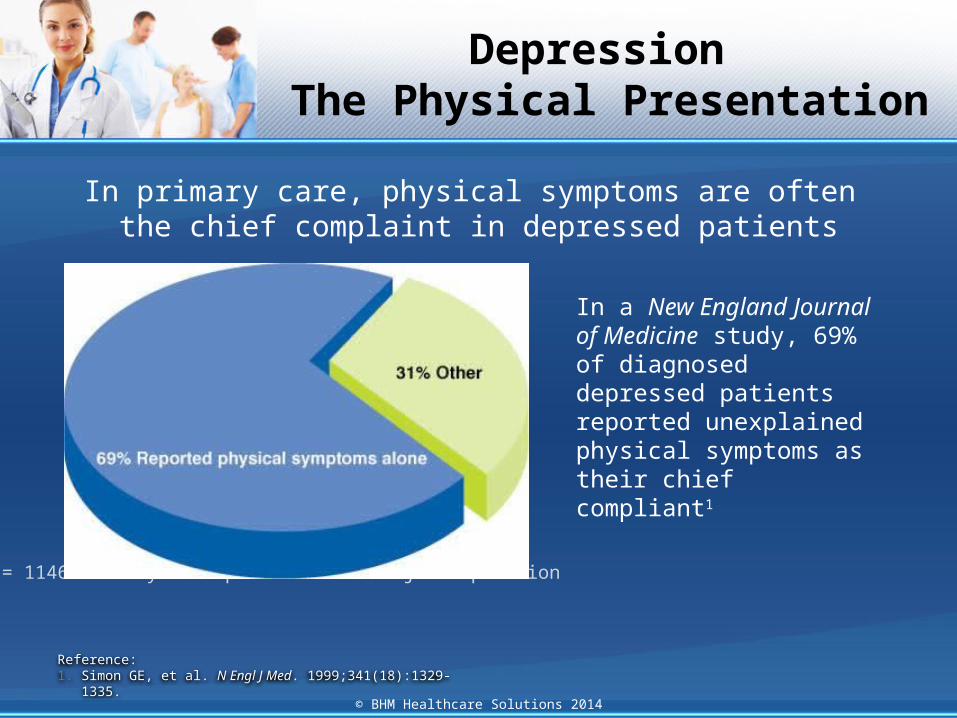
Reference:1. Simon GE, et al. N Engl J Med. 1999;341(18):1329-1335.
Depression The Physical Presentation
In primary care, physical symptoms are often the chief complaint in depressed patients
N = 1146 Primary care patients with major depression
In a New England Journal of Medicine study, 69% of diagnosed depressed patients reported unexplained physical symptoms as their chief compliant1

© BHM Healthcare Solutions 2014
Depression Screening Tools
Tool Cost ReferenceHamilton Depression Rating Scale Free http://img.medscape.com/pi/emed/ckb/psychiatry/79926-1889862-1859039-212
4408.pdf
Beck Depression Inventory Cost http://psychcorp.pearsonassessments.com/HAIWEB/Cultures/en-us/Productdetail.htm?Pid=015-8018-370&Mode=summary
Patient Health Questionnaire (PHQ-9) Free http://img.medscape.com/pi/emed/ckb/psychiatry/79926-1889862-1859039-2128912.pdf
Major Depression Inventory Free http://img.medscape.com/pi/emed/ckb/psychiatry/79926-1889862-1859039-2129923.pdf
Center for Epidemiologic Studies Depression Scale
Free http://img.medscape.com/pi/emed/ckb/psychiatry/285911-1335297-1859039-1859099.pdf
Zung Self-Rated Depression Scale Free http://img.medscape.com/pi/emed/ckb/psychiatry/79926-1889862-1859039-2129979.pdf
Geriatric Depression Scale Free http://img.medscape.com/pi/emed/ckb/psychiatry/285911-1335297-1859039-1859094.pdf
Cornell Scale for Depression in Dementia
Free http://www.scalesandmeasures.net/files/files/The%20Cornell%20Scale%20for%20Depression%20in%20Dementia.pdf
http://emedicine.medscape.com/article/1859039-overview#showall
© BHM Healthcare Solutions 2014
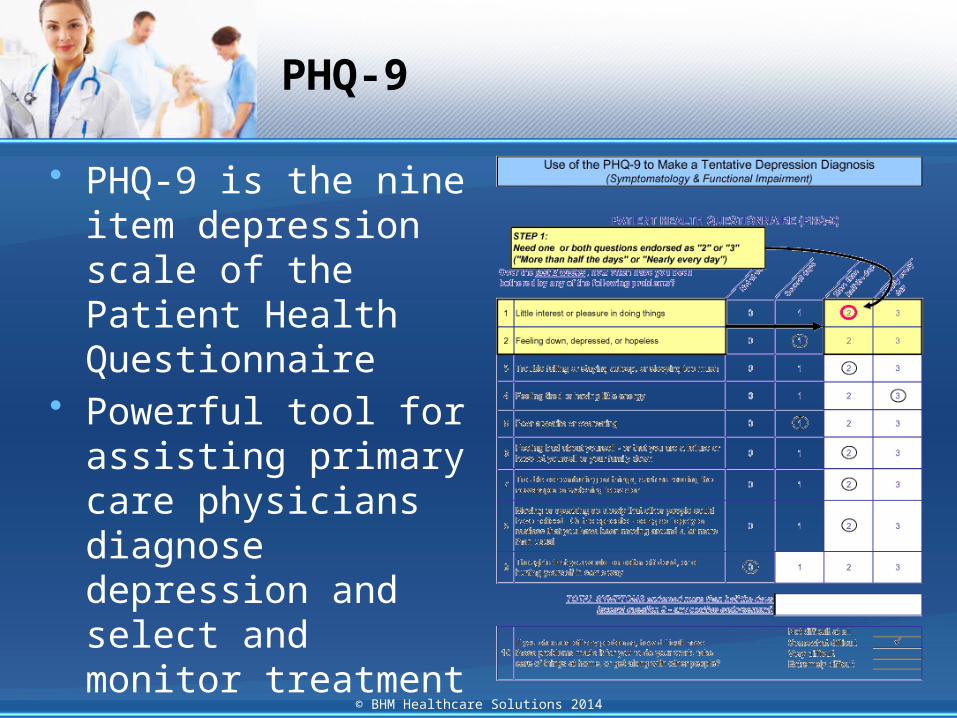
PHQ-9
• PHQ-9 is the nine item depression scale of the Patient Health Questionnaire
• Powerful tool for assisting primary care physicians diagnose depression and select and monitor treatment

© BHM Healthcare Solutions 2014
PHARMACOLOGIC TREATMENT, AND GAINING A
MIND-BODY PERSPECTIVE

© BHM Healthcare Solutions 2014
Per
cen
t R
em
issi
on
45.5
27.6
39.3
22.2
50.0
28.0
17.6
45.539.8 39.1
52.2
7.7
0
20
60
40
Medication Psychotherapy Combination
Medication(n=33)
Psychotherapy(n=53)
Combination(n=255)
None(n=88)
Preferred Treatment
In 429 patients with MDD who participated in a large multisite study ofnefazodone vs Cognitive Behavioral Analysis System of Psychotherapy
vs a combination of both modalities, patient preference strongly predicted outcomes over 12 weeks of treatment. Patients did better when they were randomly assigned to the treatment they would have preferred if given a choice.
Kocsis JH et al. J Clin Psychiatry. 2009;70(3):354-361.
Patient Treatment Preference Predicts Outcome
© BHM Healthcare Solutions 2014
Depression: Current treatment outcomes
• In any given year, between 13.1 million and 14.2 million U.S. citizens will experience an episode of major depressive disorder (MDD).
• Although approximately half of these people seek help for this condition, only 20 percent—10 percent of the total population with MDD—receive adequate treatment.
• Even then, only 30 percent of those who receive adequate treatment reach the treatment goal of remission.
• The remaining 70 percent will either have a response without remission (about 20 percent) or not respond at all (50 percent).
http://www.guideline.gov/expert/expert-commentary.aspx?id=36835

© BHM Healthcare Solutions 2014
Treatment Options
Pharmacologic Options• Serotonin Selective Reuptake
Inhibitors (SSRIS)
• Serotonin Norepinephrine Reuptake Inhibitors (SNRIs)
• Tricyclic Antidepressants
• Monoamine Oxidase Inhibitors
• Adjunct Therapies▫ Atypical Antipsychotics▫ Mood Stabilizers▫ Anxiolytics
Psychotherapy• Cognitive Behavioral
Therapy
• Interpersonal Therapy
• Problem-Solving Therapy
• Supportive Therapy
• Group Therapy

© BHM Healthcare Solutions 2014
SalivaryCortisol(µg/dL) Beforethe4weekprogram Afterthe4weekprogram t P
Forestgroup 0.113(0.053) 0.082(0.044) 2.97 0.008
Hospitalgroup 0.125(0.052) 0.132(0.057) -1.62 0.121
Controls 0.137(0.100) 0.148(0.106) -1.31 0.206
Montgom
ery-Asberg
Rating Scale
Score
Mean (SD), paired t-test
Kim W et al. Psychiatry Investig. 2009;6(4):245-254.
30
25
15
10
5
0Week 1 Week 2 Week 3 Week 4
25.3725.24
23.7
25.0524.3822.31
24.53
22.48
16.87
11.83
23.33
20.32
***
* P<0.007;**P<0.048.
ControlsHospital
Forest
MDD Remission Rates:CBT in Forest = 61%
CBT in Hospital = 21%
Controls = 5%
Beauty in Nature and the Impact on Depression

© BHM Healthcare Solutions 2014
Cardiovascular Fitness and Depression Correlation
Low
Mod
erat
eHigh
0
4
8
12
16
Men
Linear trend P<0.0001
Cardiorespiratory Fitness Level
Cu
mu
lati
ve I
nci
den
ce R
ate,
%
Low
Mod
erat
eHigh
0
4
8
12
16
Women
Linear Trend P<0.001
Cardiorespiratory Fitness Level
Cu
mu
lati
ve I
nci
den
ce R
ate,
%
Objectively assessed cardiorespiratory fitness independently predicted development of clinical depression over a 12-year follow-up period in 11,258 men and 3,085 women Sui X et al. J Psychiatr Res. 2009;43(5):546-552
© BHM Healthcare Solutions 2014
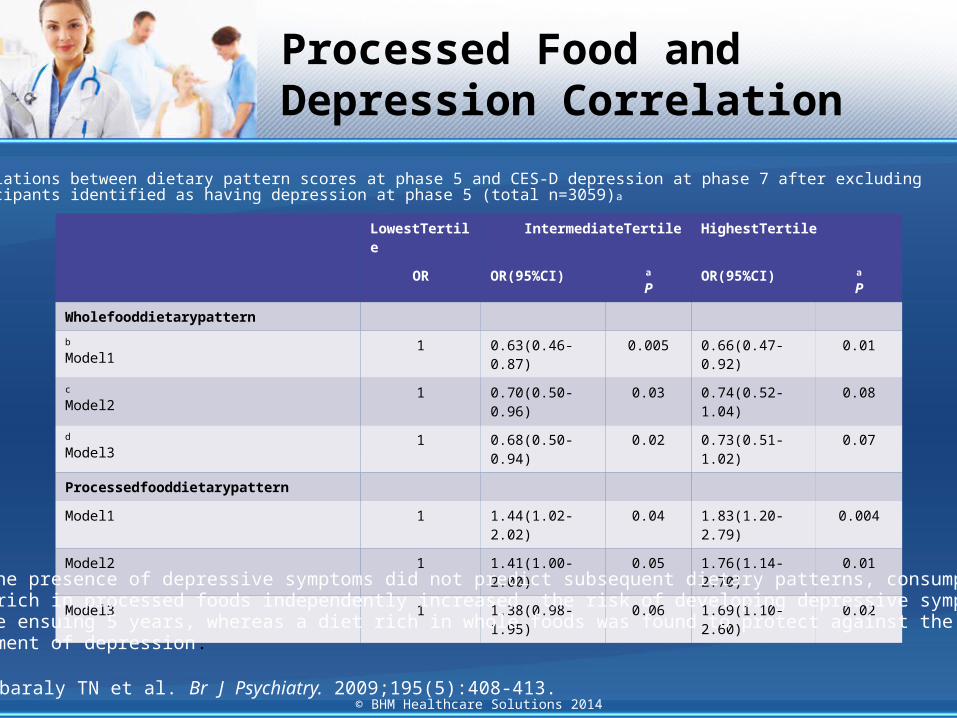
LowestTertile IntermediateTertile HighestTertile
OR OR(95%CI) a
POR(95%CI) a
P
Wholefooddietarypattern
b
Model11 0.63(0.46-0.87) 0.005 0.66(0.47-0.92) 0.01
c
Model21 0.70(0.50-0.96) 0.03 0.74(0.52-1.04) 0.08
d
Model31 0.68(0.50-0.94) 0.02 0.73(0.51-1.02) 0.07
Processedfooddietarypattern
Model1 1 1.44(1.02-2.02) 0.04 1.83(1.20-2.79) 0.004
Model2 1 1.41(1.00-2.00) 0.05 1.76(1.14-2.70) 0.01
Model3 1 1.38(0.98-1.95) 0.06 1.69(1.10-2.60) 0.02
While the presence of depressive symptoms did not predict subsequent dietary patterns, consumption ofa diet rich in processed foods independently increased the risk of developing depressive symptomsover the ensuing 5 years, whereas a diet rich in whole foods was found to protect against thedevelopment of depression.
Akbaraly TN et al. Br J Psychiatry. 2009;195(5):408-413.
Associations between dietary pattern scores at phase 5 and CES-D depression at phase 7 after excludingparticipants identified as having depression at phase 5 (total n=3059)a
Processed Food and Depression Correlation
© BHM Healthcare Solutions 2014
IMPROVING THE OUTCOME: FOLLOW-UP TOOLS AND
COMMUNICATION STRATEGIES
© BHM Healthcare Solutions 2014
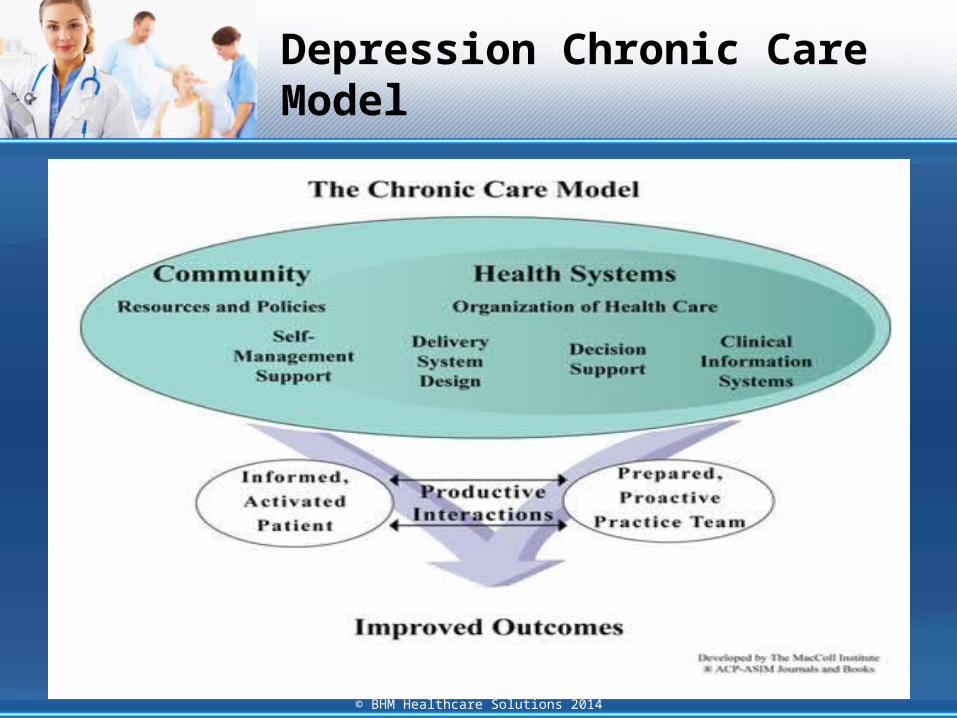
Depression Chronic Care Model
© BHM Healthcare Solutions 2014
Common Issues Regarding Antidepressant Therapy
• Non-compliance is an important reason for suboptimal treatment outcomes.
• Patients frequently report the following:• Read up on it on the internet and didn’t like side
effects.• Took it for a week then stopped.• Only take it when I feel bad.• Once I felt better I stopped the medication.
• 75 % of antidepressants are discontinued by month 4

© BHM Healthcare Solutions 2014
Interventions to Reduce Non-Compliance
Educate patients
regarding the disease and
treatment options.
Discuss common side effects of the
antidepressant medication openly with
patients.
Reassure patients that
other medication
options will be explored in case of side
effects.

© BHM Healthcare Solutions 2014
Interventions to Reduce Non-Compliance
Emphasis that these
medications need to be taken on a daily basis to be effective.
Reassure patients that
Antidepressant medications are not addictive.
Explain to patients that
continued treatment with antidepressant
medication has a neuro protective
effect.

© BHM Healthcare Solutions 2014
Behavioral Modifications
• Understanding the Mind-Body Connection in Depression can inform a variety of treatment methods to provide optimal patient care. For Instance:• Encourage physical activity which increases Brain
Drive Neurotropic Factor• Encourage a healthy diet and limitation of
processed foods• Let the patient preference inform treatment• Engage patients in support groups, and if possible
conduct support groups outdoors or in aesthetically pleasing environments

© BHM Healthcare Solutions 2014
Behavioral Modifications cont.
• Let the patient’s preference inform treatment• Engage patient in support groups, and if possible
conduct support groups outdoors or in aesthetically pleasing environments
• Educate patient on importance of structure in daily life, need to continue with ADLs and avoid spending increase time in bed.

© BHM Healthcare Solutions 2014
Behavioral Modifications cont.
• Patient needs to adhere to regular sleep and wake times.
• Involve family members early in treatment. Educate them regarding the disease process. They can provide extra support and help implement recommendations, monitor medication compliance, and provide better feedback on patient’s functioning.

© BHM Healthcare Solutions 2014
Management of Patients who are not Responding to Treatment
• Identify mind body treatment approaches
• Reconsider diagnosis• Refer to Psychiatrist• Implement case
management • Monitor med
compliance through the pharmacy services
• Consider more aggressive Pharmacotherapy

© BHM Healthcare Solutions 2014
Question and Answer Session
Website: www.bhmpc.comEmail: [email protected]
Phone Number: 1-888-831-1171Fax Number: 1-888-818-2425