building bridges for success: healthcare integration strategies for case management presented by...
TRANSCRIPT

© BHM Healthcare Solutions 2014
Building Bridges for Success: Healthcare Integration Strategies for Case Management
Presented by Mark Rosenberg MD PhD,
President BHM Healthcare Solutions

© BHM Healthcare Solutions 2014
Learning Objectives
LO 1
• Attendees will gain an intrinsic appreciation of the link between primary care conditions and behavioral health conditions, with an emphasis on depression.
LO 2
• Participants will become familiar with strategies which are utilized to incorporate meaningful integration between behavioral health and primary care services from the Case Management perspective.
LO 3
• Attendees will become familiar with the integrated case management model and learn ways to incorporate elements of the model into their practice.

© BHM Healthcare Solutions 2014
Presentation Overview
Case Management: Traditional Views and Emerging Perspectives
Healthcare Integration: The Integrated Case Management Model
Facilitating the Change: Impactful Strategies for Integrated Case Management
Practice Example: Depression, the Mind-Body Connection
Integration Strategies to Address Depression

© BHM Healthcare Solutions 2014
CASE MANAGEMENT: TRADITIONAL VIEWS AND
EMERGING PERSPECTIVES

© BHM Healthcare Solutions 2014
The Healthcare Silo
• In the current healthcare system, physical disease and mental health/substance abuse (behavioral health) issues are typically treated separately.
• The carve out of behavioral health issues from physical disease often leads to separation of treatment (15% of all patients) or lack of treatment (85% of patients).
• The carve out of behavioral health has furthermore resulted in the two arenas of healthcare being separated into distinct areas, commonly known as the silo effect
• Currently behavioral health and physical disease issues are separated according to treatment strategies, diagnostic techniques, clinical access and atmosphere, as well as funding
Kathol, Roger G., Rebecca Perez, and Janice S. Cohen. The Integrated Case Management Manual. Manual, New York: Springer Publishing Company, 2010.

© BHM Healthcare Solutions 2014
The Healthcare Silo
85% of behavioral health patients are seen in the physical health sector
65% receive no behavioral health
treatment
70% of all behavioral health treatment is
provided by primary care physicians (PCPs)
Only 13% of patients treated by PCPs get evidence-based care
Only 3% of behavioral health providers work in
the general medical sector
80% of expenses for patients with mental conditions are from
medical benefits, half of which are for physical
health services
Kathol, Roger G., Rebecca Perez, and Janice S. Cohen. The Integrated Case Management Manual. Manual, New York: Springer Publishing Company, 2010.

© BHM Healthcare Solutions 2014
The Development of Case Management
• Case Management was originally developed as a means to efficiently use limited health care resources and falls within the broader scope of Care Management
• With the average physician visit lasting 9 minutes, care management was implemented in order to assist in achieving optimal treatment outcomes and navigating the fractured health system
• This 2-5% of the population utilizes a third to a half of health care resources
Case managers usually work
with the 2%-5%
Kathol, Roger G., Rebecca Perez, and Janice S. Cohen. The Integrated Case Management Manual. Manual, New York: Springer Publishing Company, 2010.

© BHM Healthcare Solutions 2014
The Development of Case Management
70%
20%
10%
HEALTHY VERSUS CHRONIC DISEASE
HEALTHY OR HAVE READILY TREATABLE DISEASEINTEGRATED DISEASE MANAGEMENTINTEGRATED CASE MANAGEMENT
Kathol, Roger G., Rebecca Perez, and Janice S. Cohen. The Integrated Case Management Manual. Manual, New York: Springer Publishing Company, 2010.

© BHM Healthcare Solutions 2014
Case Management The Traditional View
Medical Case Management
• Medical case managers are often nurses or other clinicians
• Assistance is provided to patients who have a higher level of severity/acuity than expected
Behavioral Case Management
• Behavioral Case Management is often conducted by social workers, psychologist, and substance abuse counselors in addition to nurses

© BHM Healthcare Solutions 2014
Case Management The Traditional View
Medical Case Management
• Background in management and general medical care
• Concentration on biological factors that contribute to poor physical health
• Rarely focus on access to care, personal behaviors, or client ability to pay
Behavioral Case Management
• Background in mental health and substance abuse
• Concentration on diagnosis and treatment of mental health conditions and behaviors that predict poor outcomes

© BHM Healthcare Solutions 2014
Case Management The Traditional View
• Just as healthcare has experienced a fracture between the treatment and approaches to Mental Health and Behavioral Health, there is a corresponding divergence between the approach of Medical Case Management and Behavioral Case Management
Medical
Case Management
Behavioral
Case Management

© BHM Healthcare Solutions 2014
Emerging Perspectives: Healthcare Integration
Medical
Behavioral
Integrated Care: A Holistic
Approach
• There is currently a movement toward integrated care, which has been shown to improve overall outcomes by combining physical and behavioral health treatment while reducing total healthcare cost

© BHM Healthcare Solutions 2014
Emerging Perspectives: Healthcare Utilization
Top 5% of Patients Using 50% of Healthcare Resources
60-80% have co-morbid mental
conditions
70-85% receive no
mental health
treatment
80-90% with a mental
health condition see no mental health
specialist
5-15% get mental health
treatment that would
be expected to improve outcomes
Kathol, Roger G., Rebecca Perez, and Janice S. Cohen. The Integrated Case Management Manual. Manual, New York: Springer Publishing Company, 2010.

© BHM Healthcare Solutions 2014
Emerging Perspectives: Healthcare Integration
Mental Condition Co-Morbidity in Physically IllCondition Prevalence
Neurological 37.5%
Heart Disease 34.6%
Chronic Obstructive Pulmonary Disease
30.9%
Cancer 30.3%
Arthritis 25.3%
Diabetes 25.0%
Hypertension 22.4%
Physical Condition Co-Morbidity in Mentally IllCondition Prevalence
Pulmonary 31%
Heart Disease 22%
Gastrointestinal Disease
25%
Skin and Connective Tissue
19%
Metabolic 15%
Diabetes 12%
Any medical illness
75%
Kathol, Roger G., Rebecca Perez, and Janice S. Cohen. The Integrated Case Management Manual. Manual, New York: Springer Publishing Company, 2010.

© BHM Healthcare Solutions 2014
Emerging Perspectives: Healthcare Integration
• A high percentage of a few patients with health complexity use the majority of healthcare resources
• These patients have concurrent physical and behavioral issues which contribute to poor outcomes
• Integrated Case Management, and a better understanding in the mind body connection in complex cases is critical in bridging the gap between physical and behavioral healthcare
Medical
Case Management
Behavioral
Case Management
Integrated Case
Management

© BHM Healthcare Solutions 2014
HEALTHCARE INTEGRATION AND THE INTEGRATED CASE
MANAGEMENT MODEL

© BHM Healthcare Solutions 2014
Making the Case for BH/PC Integration
• Mental health issues are frequently unrecognized and, even when diagnosed, are not treated adequately.
• Recognition and treatment of mental illness are significant issues for primary care physicians who provide the majority of health care.
• In a recent national survey, 18% of the surveyed population with a DSM-IV diagnosis of a mental health disorder sought treatment, with 52% of those visits occurring in the general medical sector.
• Estimates are that 11% to 36% of primary care patients have a psychiatric disorder.
AAFP. www.aafp.org. Nov. 3, 2010. http://www.aafp.org/online/en/home/policy/policies/mentalhealthcare (accessed April 4, 2012).

© BHM Healthcare Solutions 2014
BH/PC: The Treatment Gap
• Surveys show that 40% of patients with major depression do not want, or perceive the need, for treatment.
• Only 20%-30% of patients with mental health disorders report them to a primary care physician.
• 33% of patients presenting in the ER with acute chest pain are suffering from either panic disorder or depression.
• 80% of patients with depression initially present with physical symptoms such as fatigue or chronic aches.

© BHM Healthcare Solutions 2014
BH/PC: The Treatment Gap
“There are analogous problems of under-recognition and under-treatment of medical problems for persons with
mental conditions.”• Symptoms of mental illness may reduce a patient’s
ability to initiate and follow through with treatmentPatients
• PC providers may feel uncomfortable treating patients with mental illnessPC Providers
• May lack knowledge or expertise to provide medical care for their patientsBH Providers
• Fragmentation between BH and PC can result in patients receiving inadequate or uncoordinated careSystem Gap
Druss, Benjamin G., and Elizabeth Reisinger-Walker. Mental Disorders and Medical Comorbidity. Research Synthesis Report

© BHM Healthcare Solutions 2014
Four Concepts Common in BH/PC Integration Models
Medical Home
Health Care Team
Stepped Care
Approach
Four Quadrant Clinical
Integration

© BHM Healthcare Solutions 2014
Medical Home
• Practice-based care coordination within the medical home is a direct, family/patient-centered, team oriented, outcomes focused process designed to: • Facilitate the provision of comprehensive health promotion and �
chronic condition care; • Ensure a locus of ongoing, proactive, planned care activities; �• Build and use effective communication strategies among family, �
the medical home, schools, specialists, and community professionals and community connections; and
• Help improve, measure, monitor and sustain quality outcomes �(clinical, functional, satisfaction and cost)
© BHM Healthcare Solutions 2014
Health Care Team
Health Care Team - In this approach the doctor-patient relationship is replaced with a team-patient relationship.
• Members of healthcare team share responsibility for a patient’s care.
• A visit is coordinated between various members of a team.
• The healthcare team has full knowledge of what the other team members are doing regarding patient care.

© BHM Healthcare Solutions 2014
Stepped Care Approach
Stepped Care Approach - healthcare providers should offer care that is the LEAST:• Disruptive for patient• Extensive needed for
results• Intensive needed for
results• Expensive needed for
results• Expensive in regard to
staff training required to provide service

© BHM Healthcare Solutions 2014
Four Quadrant Clinical Integration
Quad II• Patients with high BH and low
physical needs• Served in PC and specialty MH
setting• E.g., patients with bipolar disorder
and chronic pain
Quad IV• Patients with high BH and high
physical needs• Served in PC and specialty MH
setting• E.g., patients with schizophrenia
and hepatitis C
Quad I• Patients with low BH and low
physical needs• Served in PC setting• E.g., patients with moderate alcohol
abuse and fibromyalgia
Quad III• Patients with low BH and high
physical needs• Served in PC setting• E.g., patients with moderate
depression and uncontrolled diabetes

© BHM Healthcare Solutions 2014
Practice Models of Integration
• Effective Primary Care Behavioral Health collaboration models are dependent upon a number of variables, but should aim toward the following care goals:• Lessen the stigma of accessing care• Improve use of MD time and availability• Increase referrals to BH providers that PC physicians
actually know• Help patients with chronic illness manage disease• Identify patients with depression and other chronic
illness• Increase cost efficiency of treatment• Increase treatment adherence

© BHM Healthcare Solutions 2014
Practice Models of Integration
• Developing an effective model of integration is dependent upon many community/facility limitations, including:
• Array and capacity of services in the community• Trained workforce – do behavioral health providers and PC
physicians have the right skills to deliver services on-site?• Organizational support in providing service – do managers
provide encouragement/support for collaborative initiative?• Reimbursement factors – do payers support collaborative
care and make it easy for PC and BH providers to work together?
• Organizational impact – what is the organizational impact on documentation, billing, risk management, etc.?

© BHM Healthcare Solutions 2014
Practice Models of Integration
Coordinated
Routine screening for BH problems conducted in
PC setting
Referral relationship between PC and BH
settings
Routine exchange of information between treatment settings
Co-Located
Medical services and BH services located in same
facility
Referral process for medical cases to be seen
by BH specialist
Enhanced informal communication between
PC and BH providers due to proximity
Integrated
Medical services and BH services located in same
facility, or separate locations
One treatment plan with BH and medical
elements
Typically, a team working together to deliver care,
using formal protocol

© BHM Healthcare Solutions 2014
FACILITATING THE CHANGE: IMPACTFUL STRATEGIES FOR
INTEGRATED CASE MANAGEMENT

© BHM Healthcare Solutions 2014
Integration 101: Utilizing Case Management
Case Management May Include:
Coordination of Care
Assisting members accessing community
based resources
Providing disease specific
education
Any other options aimed at improving
quality of life, functionality of members, and
efficiently using
healthcare resources
© BHM Healthcare Solutions 2014
Integrated Case Management
• Case Management occupies a unique position in improving member health and reducing health care costs
• Core concepts for effective case management include targeted programs across the care continuum, including but not limited to:• Targeted prevention health• Disease management• Behavioral health management• Pharmacological management• Wellness incentives and reimbursements• Community resources• Healthcare access

© BHM Healthcare Solutions 2014
Integrated Case Management
• The goal of Integrated Case Management should be to break down complexity-based health barriers across multiple domains in order to appropriately address and treat patients from a holistic perspective
Biological Psychological
Social Health System
© BHM Healthcare Solutions 2014
Integrated Case Management
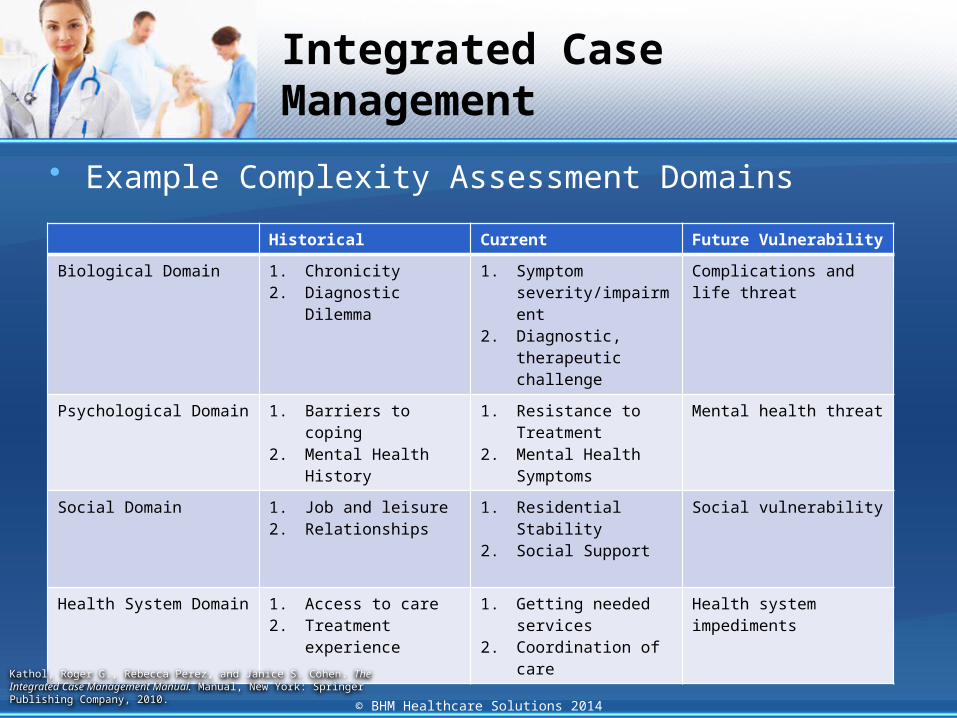
• Example Complexity Assessment Domains
Historical Current Future Vulnerability
Biological Domain 1. Chronicity2. Diagnostic Dilemma
1. Symptom severity/impairment
2. Diagnostic, therapeutic challenge
Complications and life threat
Psychological Domain 1. Barriers to coping2. Mental Health History
1. Resistance to Treatment
2. Mental Health Symptoms
Mental health threat
Social Domain 1. Job and leisure2. Relationships
1. Residential Stability2. Social Support
Social vulnerability
Health System Domain 1. Access to care2. Treatment experience
1. Getting needed services
2. Coordination of care
Health system impediments
Kathol, Roger G., Rebecca Perez, and Janice S. Cohen. The Integrated Case Management Manual. Manual, New York: Springer Publishing Company, 2010.

© BHM Healthcare Solutions 2014
Integrated Case Management
• Integrated Case Management should be grounded in a relationship based approach to interaction with patients• Develop and carry out a plan collaboratively with the patient• Incorporate the patient’s family• Incorporate the primary care provider and facilitate collaboration
with other care providers• Examine the situation from the payer perspective and the
community perspective to take advantage of programs that can optimize health, quality of life, appropriate use of services, and conservation of healthcare resources

Integrated Case Management
Patient Responsibilities• Willingness to form a relationship with the case manager
and maintain trust• Participate and be willing to learn about illness recovery• Initiate agreed upon treatments and recommendations• Participate actively in the improvement process• Provide timely feedback regarding treatment success, failure,
and roadblocks
Case Manager Responsibilities• Build a positive collaborative relationship with the patient• Provide educational resources along with an adequate
understanding of the illness• Identify and reverse barriers to improvement• Facilitate interventions and be willing to serve as a patient
advocate• Confirm improvement and adjust treatment based on efficacy
© BHM Healthcare Solutions 2014Kathol, Roger G., Rebecca Perez, and Janice S. Cohen. The Integrated Case Management Manual. Manual, New York: Springer Publishing Company, 2010.

© BHM Healthcare Solutions 2014
Integrated Case Management: Strategies for Change
• Include comprehensive patient assessments which evaluate both physical health and behavioral health issues into your case management strategy
• Do not ignore social factors; find out if there are any social factors which negatively impact treatment outcomes such as lack of housing or transportation and level of family involvement
• Actively encourage family and community involvement and support
• Assist and facilitate patient education at every opportunity• Provide a collaborative link between Primary Care and
Mental Health providers and ensure that there is open communication across provider channels

© BHM Healthcare Solutions 2014
Integrated Case Management: Strategies for Change
• Actively assist the patient in navigating the healthcare system, whether from a provider or a payer perspective
• Address any financial barriers to care and assist in finding workable alternatives
• Ensure that you, the Case Manager, receive ongoing education about both primary care and behavioral health issues

INTEGRATION STRATEGIES TO ADDRESS DEPRESSION
© BHM Healthcare Solutions 2014

© BHM Healthcare Solutions 2014
Integration 101: First Steps to Making it Work
• Utilization of appropriate screening tools in primary care for BH diagnosis
Screening Tools For Primary Care
• Building relationships with BH providers and facilitating communication
Relationships & Communication
• Effectively using technology to overcome obstacles
Technology

© BHM Healthcare Solutions 2014
Integration 101: Screening Tools Additional Resources
• What factors to consider when determining which screening tools to incorporate in your practice:• Method of screening delivery - interview/pre-screen• Proprietary Tools - are the tools free and readily available?• Reliability - is the tool proven to provide reliable results?• Sensitivity - is the tool accurate in identifying a problem?• Specificity - is the tool accurate in identifying those who do not
have a problem?• Patient population - is the tool age specific, and are there any
cultural considerations to take into account?
• For a comprehensive list of mental health screening tools for utilization in a primary care setting please visit:
https://www2.aap.org/commpeds/dochs/mentalhealth/docs/MH-ScreeningChart.pdf

© BHM Healthcare Solutions 2014
Integration 101: Relationships and Communication
• After deciding what screening criteria will be utilized, decide what metrics will be used to determine if a patient will be treated in primary care, or referred to a behavioral health specialist
• Develop a referral network• Develop a relationship with area behavioral health
specialists who will be a part of your referral network• Ensure that your network covers a range of services • Work to cultivate these relationships and refer patients to
providers who you actually know

© BHM Healthcare Solutions 2014
Integration 101: Communication and Relationships
• Appreciate the differences between Primary Care and Behavioral Health Treatment and Environments:
Primary Care Behavioral Health
Pace 15 minute appointment 50 minute session
Setting An exam room An office setting
Language Diagnosis, medical terminology, complaints
Assessment, mental health terminology, issues
Hierarchy Physician is in charge Diffused hierarchy that differs widely by provider
Flow Flexible patient flow Scheduled client flow

© BHM Healthcare Solutions 2014
Integration 101: Utilizing Case Management
• The goal of the Case Management Solutions Program is to provide high quality, integrated, culturally-competent case management services to members assessed as having high medical and/or non-medical case management needs.
• The Program meets this goal by doing the following:• Utilizing qualified staff to collaboratively identify and assess the physical,
behavioral, cognitive, functional, and social needs of members for case management services
• Developing a comprehensive case management plan with input from the member and caregiver
• Working with the member and caregiver to complete a planned and prioritized set of goals and interventions tailored to the individual needs of the member, caregiver and their family/support system
• Program staff encourages members to take action to improve their overall quality of life, functional status, and health outcomes, and strive to ensure the delivery of services in the most cost-effective manner.

© BHM Healthcare Solutions 2014
Integration 101: Realizing Opportunities
• Mental and physical health problems are interwoven.
• Integrated primary care helps to ensure that people are treated in a holistic manner, meeting the mental health needs of people with physical disorders, as well as the physical health needs of people with mental disorders.
Collins, Chris, Denise Levis-Hewson, Richard Munger, and Torlen Wade. Evolving Models of Behavioral Health Integration in Primary Care. New Yort: Millibank Memorial Fund, 2012.

© BHM Healthcare Solutions 2014
Integration 101: Realizing Opportunities
• The treatment gap for mental disorders is enormous.
• In all countries, there is a significant gap between the prevalence of mental disorders and the number of people receiving treatment and care.
• Coordinating primary care and mental health helps to close this divide.
Collins, Chris, Denise Levis-Hewson, Richard Munger, and Torlen Wade. Evolving Models of Behavioral Health Integration in Primary Care. New Yort: Millibank Memorial Fund, 2012.

© BHM Healthcare Solutions 2014
Integration 101: Realizing Opportunities
• Primary care settings for mental health services enhance access, but when this is not available Case Managers provide a vital link between the two health systems
Collins, Chris, Denise Levis-Hewson, Richard Munger, and Torlen Wade. Evolving Models of Behavioral Health Integration in Primary Care. New Yort: Millibank Memorial Fund, 2012.

Integration 101: Realizing Opportunities
• Integrated Depression/Medical Case Management Clinical Outcomes
Condition Intake Discharge Outcome
Depression 79% 44% 35% drop in depression
Energy level 49% 75% 26% increase in energy
Work limitations 63% 29% 34% drop in work limitations
Social limitations 71% 41% 30% drop in social limitations
Condition Intake Discharge Outcome
General health 5% 9% 4% increase in general health
Work limitations 61% 48% 13% drop in work limitations
Does less work 64% 45% 19% increase in work
Bodily Pain 12% 5% 7% decrease in bodily pain
Mental Health Survey
Physical Health Survey
Aetna-www.academyhealth.org/2006/Tuesday/611/unh.ppt© BHM Healthcare Solutions 2014

© BHM Healthcare Solutions 2014
Question and Answer Session
Website: www.bhmpc.comEmail: [email protected]: @BHM Healthcare
Phone Number: 1-888-831-1171Fax Number: 1-888-818-2425