© national jewish health 2018
TRANSCRIPT
© National Jewish Health 2018

Thank You!
This activity is supported by an independent educational grant from Vertex Pharmaceuticals Incorporated.
Thank You!
You can access the slides and infographic for the program at www.njhealth.org/CFDenver2018Slides

Faculty Presenters
Disclosures
All CME/CE educational activities sponsored by National Jewish Health are reviewed to ensure a balanced and evidence-based presentation. Any potential conflict of interest among program faculty has been identified and resolved according to ACCME guidelines.
Faculty PresentersPamela L. Zeitlin, MD, MPhil, PhD discloses that she is an Investigator for Novartis and on an Advisory Board for Gilead Sciences and Proteostasis. Milene Saavedra, MD discloses that she is an investigator for Gilead SciencesRaj J. Shah, MD, FASGE, AGAF discloses that he is a Consultant for Cook, Olympus, and Boston Scientific and a Medical Advisory Board for Boston Scientific.
Program Planners and ReviewersStephanie Corder, ND, RN has no financial relationships to disclose.Andrea Harshman, MHA, CHCP, CMP-HC has no financial relationships to disclose.Esther Langmack, MD has no financial relationships to disclose.
Pamela L. Zeitlin, MD, MPhil, PhD Silverstein Chair, Department of Pediatrics
Professor of PediatricsNational Jewish Health
Program Chair

ARS Question
Meconium ileus in a newborn with CF is a consequence of:
a. Too much fat in breast milkb. Delayed administration of pancreatic enzymesc. Cholestasisd. Pancreatic insufficiency in utero
In a CF patient with pancreatic insufficiency, which of the following is missing?
a. Lactate dehydrogenase (LDH)
b. Lipase
c. Protease
d. Trypsin
ARS Question
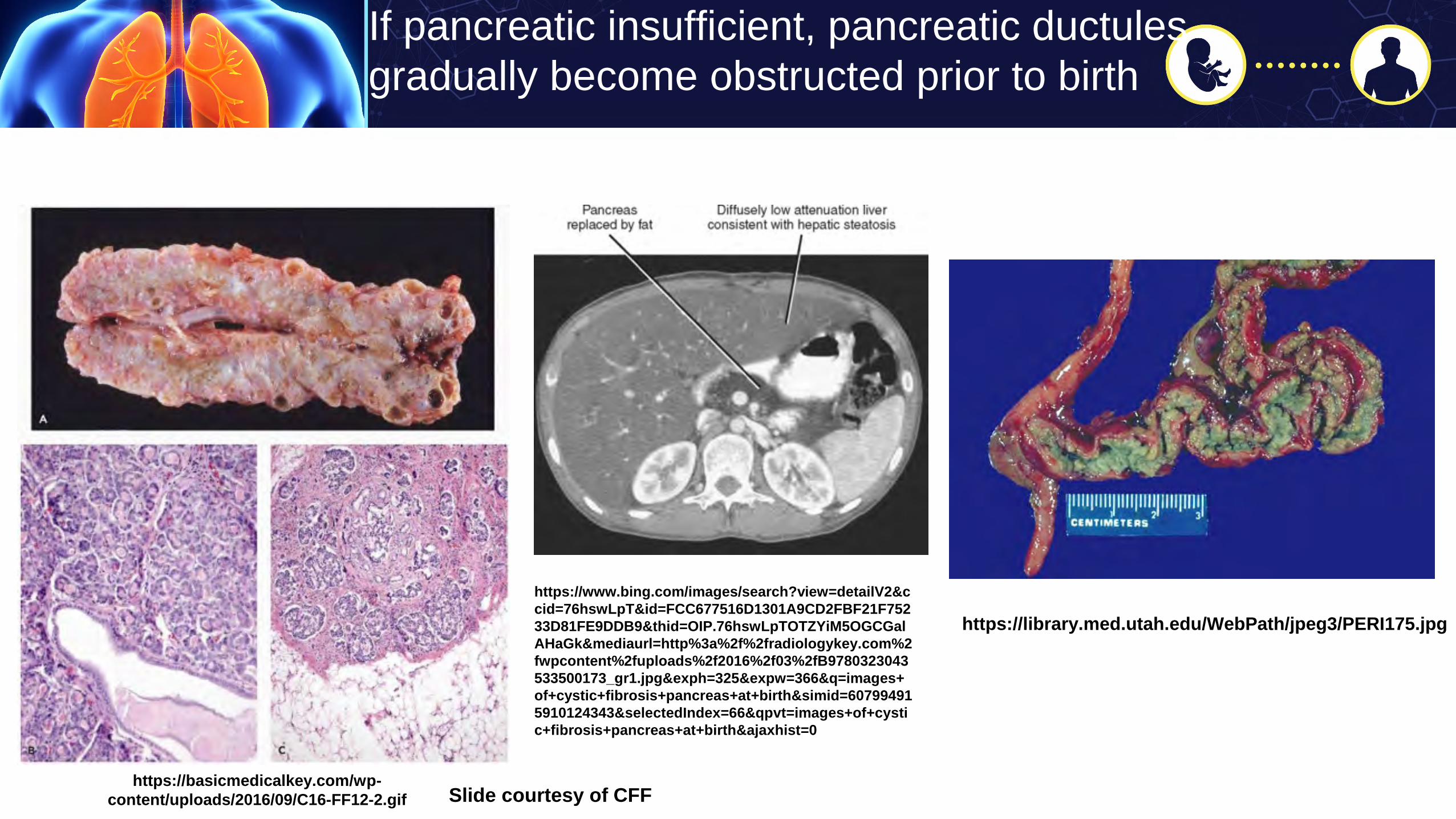
If pancreatic insufficient, pancreatic ductulesgradually become obstructed prior to birth
https://basicmedicalkey.com/wp-content/uploads/2016/09/C16-FF12-2.gif
https://library.med.utah.edu/WebPath/jpeg3/PERI175.jpg
https://www.bing.com/images/search?view=detailV2&ccid=76hswLpT&id=FCC677516D1301A9CD2FBF21F75233D81FE9DDB9&thid=OIP.76hswLpTOTZYiM5OGCGalAHaGk&mediaurl=http%3a%2f%2fradiologykey.com%2fwpcontent%2fuploads%2f2016%2f03%2fB9780323043533500173_gr1.jpg&exph=325&expw=366&q=images+of+cystic+fibrosis+pancreas+at+birth&simid=607994915910124343&selectedIndex=66&qpvt=images+of+cystic+fibrosis+pancreas+at+birth&ajaxhist=0
Slide courtesy of CFF

Challenges for the infant with CF at birth
• Malabsorption in infants with exocrine pancreatic insufficiency, fat-soluble vitamin deficiency
• Not all infants with CF are identified unequivocally by newborn screening
• Infants with meconium ileus may have false-negative newborn screening tests
• Nutritional status has a strong positive correlation with pulmonary function and survival
1) Infant Care Guidelines: Cystic Fibrosis F, Borowitz D, Robinson KA, et al. Cystic Fibrosis Foundation evidence-based guidelines for management of infants with cystic fibrosis. The Journal of pediatrics. 2009;155(6 Suppl):S73-93.
2) Preschool Guidelines: Lahiri T, Hempstead SE, Brady C, et al. Clinical Practice Guidelines From the Cystic Fibrosis Foundation for Preschoolers With Cystic Fibrosis. Pediatrics. 2016;137(4).
Clinical care guidelines for the management of both infants and preschoolers with cystic fibrosis have been published.(1, 2)
Guidelines


Infants with poor growth or failure to thrive
• Evaluate for triggers: weight loss, decline in weight or weight/length
• Insufficient intake, inadequate PERT, infections, hypercatabolic state from lung disease, vomiting/GERD, glycosuria
• Diabetes mellitus, CF liver disease

Early nutritional intervention
• Anticipatory guidance
• Oral supplemental calories, temporary nasogastric tube feeds
• Gastrostomy tube feeds
• Cyproheptadine is not used in newborns
Key Points
• Malabsorption, intestinal inflammation, small intestinal bacterial overgrowth, low bicarbonate output, impaired insulin secretion with variable degree of insulin resistance and impaired liver function contribute to energy losses
• Energy needs are high due to pancreatic insufficiency, lung inflammation and lung/airway infections
• If patient cannot consume enough calories to compensate or suffers meconium ileus equivalent, DIOS, GERD, or poor appetite, tube feedings are recommended
• Micronutrient supplementation is helpful

Infographic

Raj J. Shah, MD, FASGE, AGAFProfessor of Medicine
University of Colorado School of MedicineDirector, Pancreaticobiliary Endoscopy
University of Colorado Anschutz Medical Campus
CF and Pancreatitis: Management of pain
ARS Question
Which CF patients are more likely to develop recurrent acute pancreatitis (RAP)?
a. Panc insufficient patients
b. Panc sufficient patients
c. Patients with two severe CFTR mutations
d. Patients with chronic abdominal pain

CF and GI Manifestations
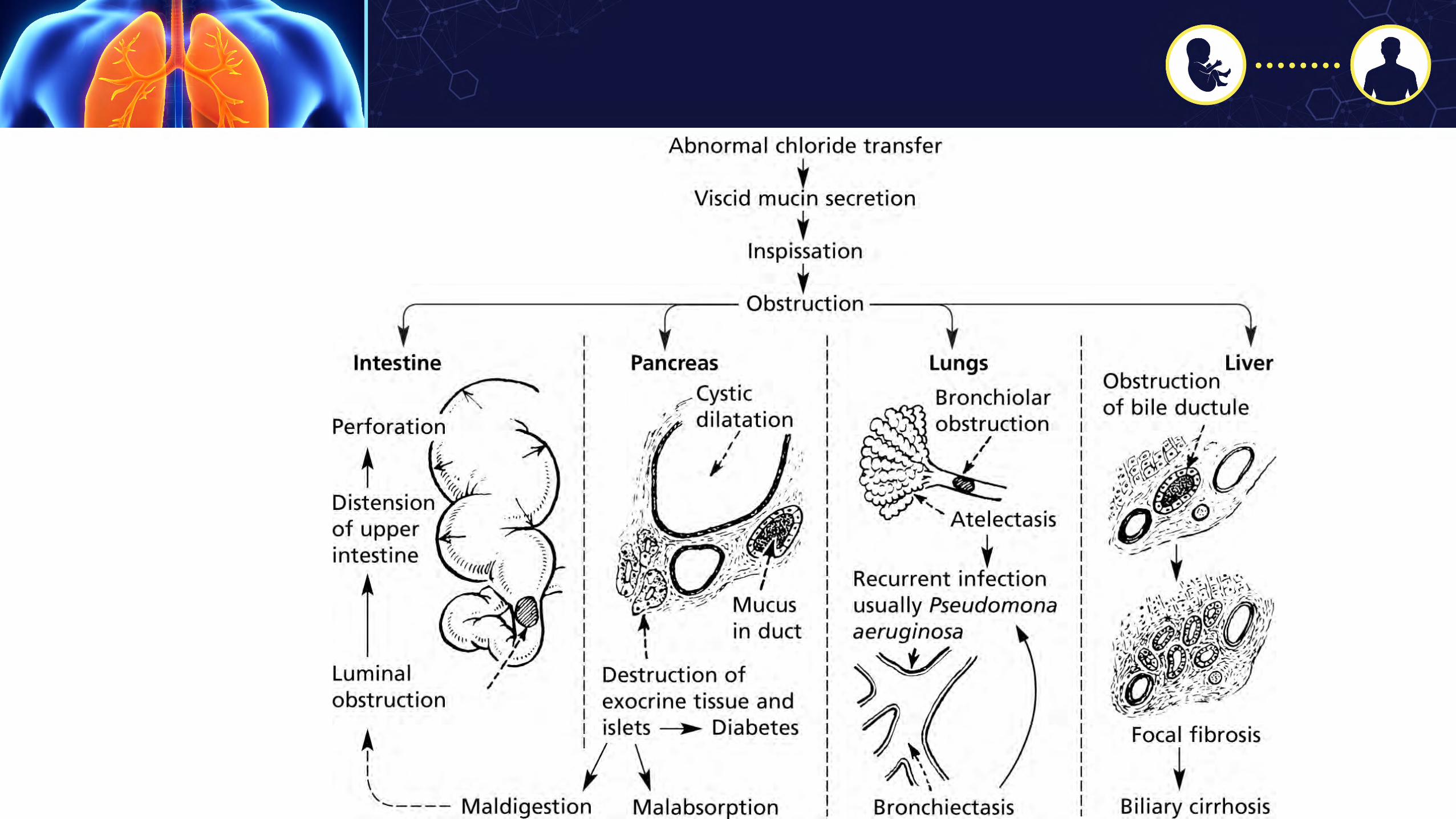
• Pathophysiology: inspissation of secretions in the hollow structures of the gastrointestinal tract
• Complications in GI lumen:–Distal intestinal obstruction syndrome (DIOS)–Meconium ileus–Intussusception–Constipation
• Complications in Biliary tract:–Cholelithiasis–Focal biliary cirrhosis–Biliary dilatation
Kelly and Buxbaum DDS 2015
CF and Pancreatitis
• 2 severe CFTR mutations – pancreas insufficiency at birth
- Loss or minimal ion transport eliminating pancreas function
- Abdominal pain more related to DIOS
• Only 20% who retain pancreas function at birth develop pancreatitis (0.5 - 1.8% of all CF pts)
Durno, et al. Gastro 2002Ooi and Durie. J Cyst Fibros 2012
Ahmet Gut 2003

Quantitative pancreatic acinar and ductular secretion following intravenous CCK/Secretin infusion (a percentage of mean control values)
N Ahmed et al. Gut 2003;52:1159-1164
Copyright © BMJ Publishing Group Ltd & British Society of Gastroenterology. All rights reserved.
Class I, II, III (‘severe’): complete loss of cAMPregulated Cl- channel
function

CF and Pancreatitis
• A single mutation (heterozygote) – increased risk for acute or chronic pancreatitis
• One allele: minimal ion transport and bicarbonate secretion in ductules leading to sluggish flow; premature trypsin activation - and recurrent acute pancreatitis (RAP) can and does progress
to chronic pancreatitis by pancreatography
Trikudanathan, et al. Gastroenterol Clin North Am 2012Ahmet Gut 2003
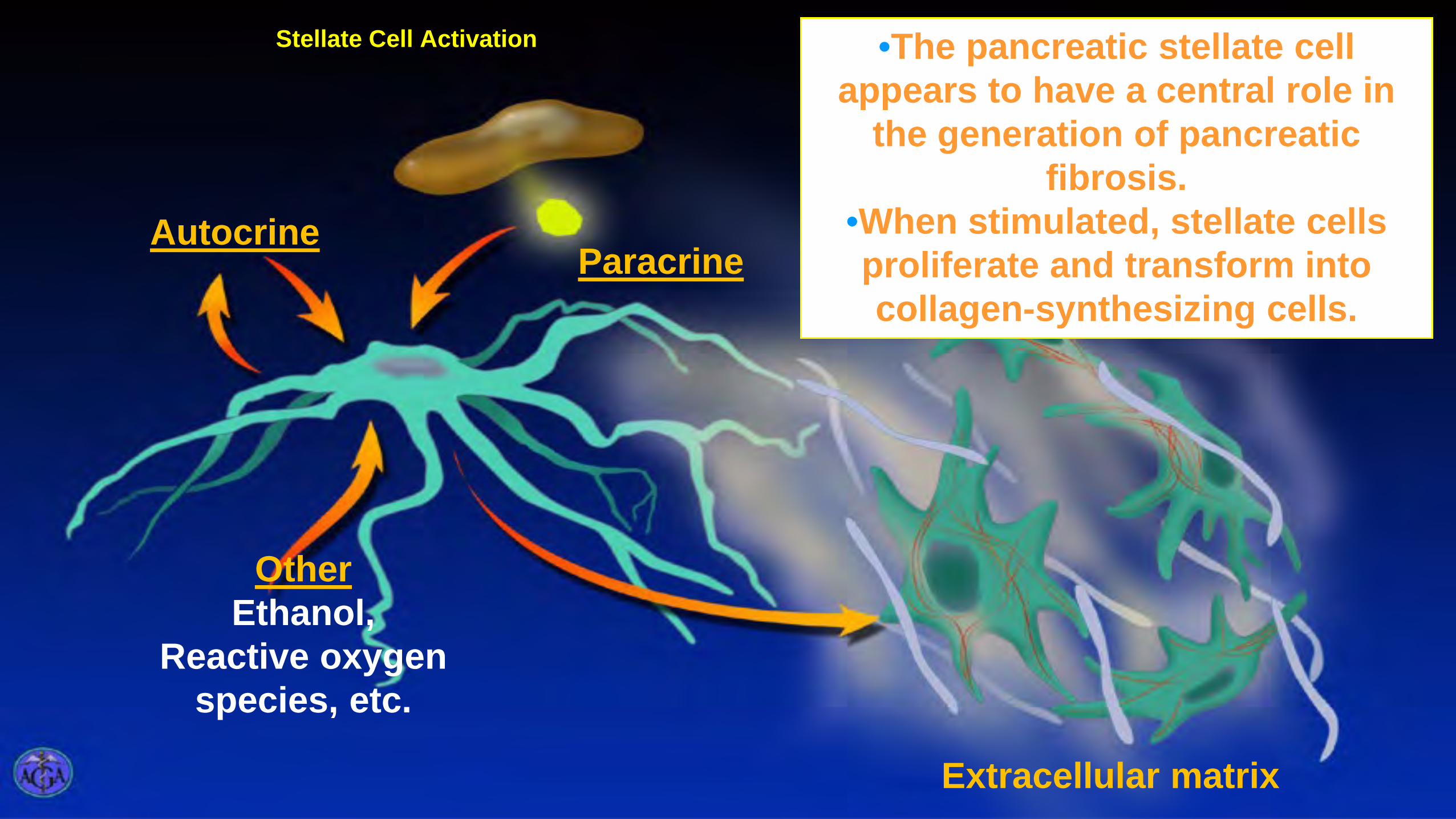
ParacrineAutocrine
OtherEthanol,
Reactive oxygen species, etc.
Extracellular matrix
Stellate Cell Activation •The pancreatic stellate cell appears to have a central role in
the generation of pancreatic fibrosis.
•When stimulated, stellate cells proliferate and transform into collagen-synthesizing cells.

ARS Question
What is best evaluation choice for determining management plan for a CF patient with chronic pancreatitis and constant epigastric pain that radiates to the back?
a. Endoscopic ultrasound and Celiac plexus block
b. CT or MRCP to evaluate panc duct anatomy
c. Evaluation by chronic pain service
d. Enzyme supplement trial
e. ERCP and possible pancreas duct stenting

Clinical Example
• 43 yo with RAP and IRDM seen initially at UCH in 2008 for pseudocyst management
• TG’s 500, no GB stones, meds, and weekend alcohol moderate and none year prior to referral
• In 2000 – R117H carrier and 5T variant copy (86 mutations checked)
• FMH two siblings with chronic pancreatitis but not in parents
• Hospitalizations were six in prior one year and associated 15 pound weight loss

EUS-guided pseudocyst drainage
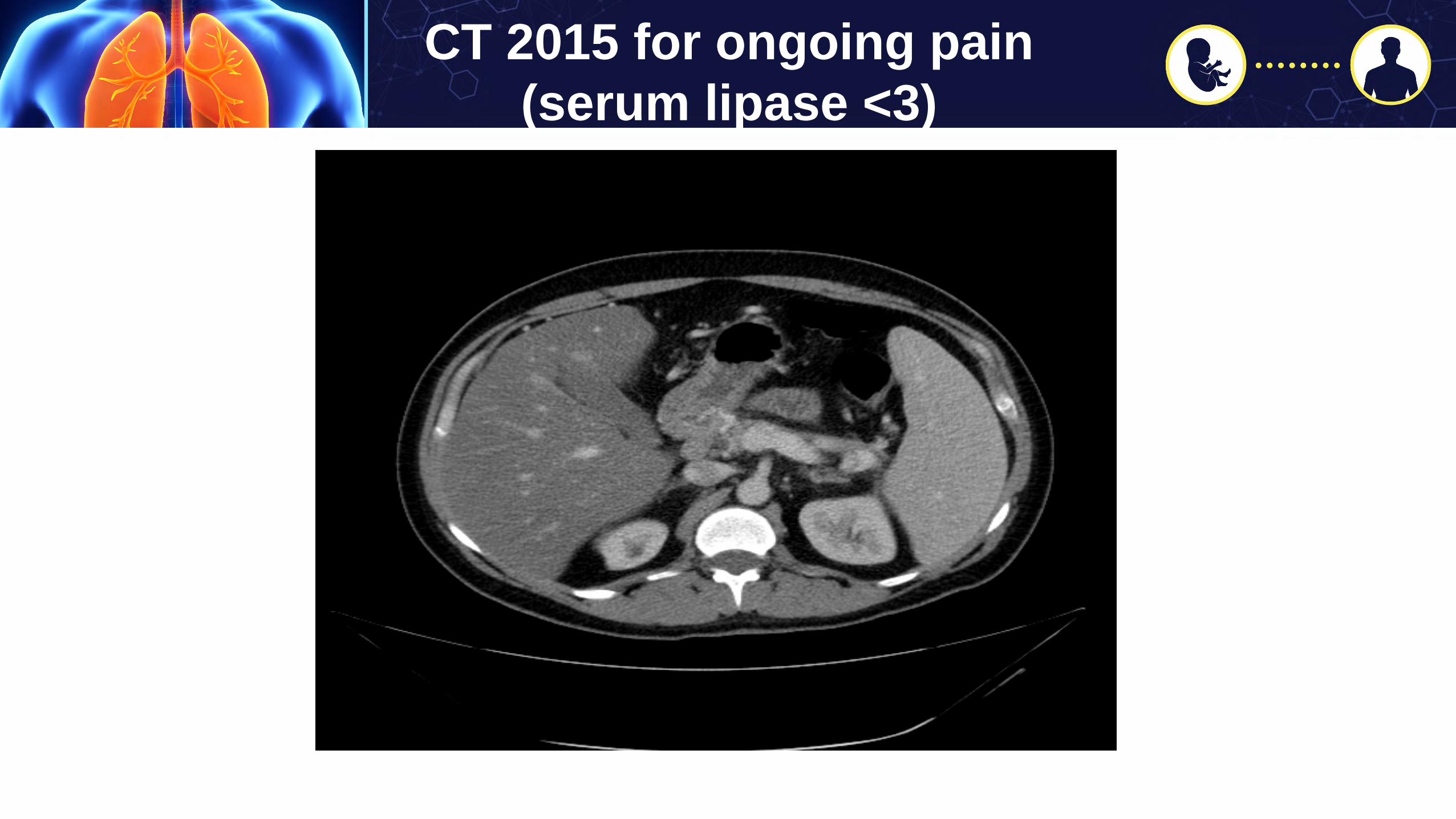
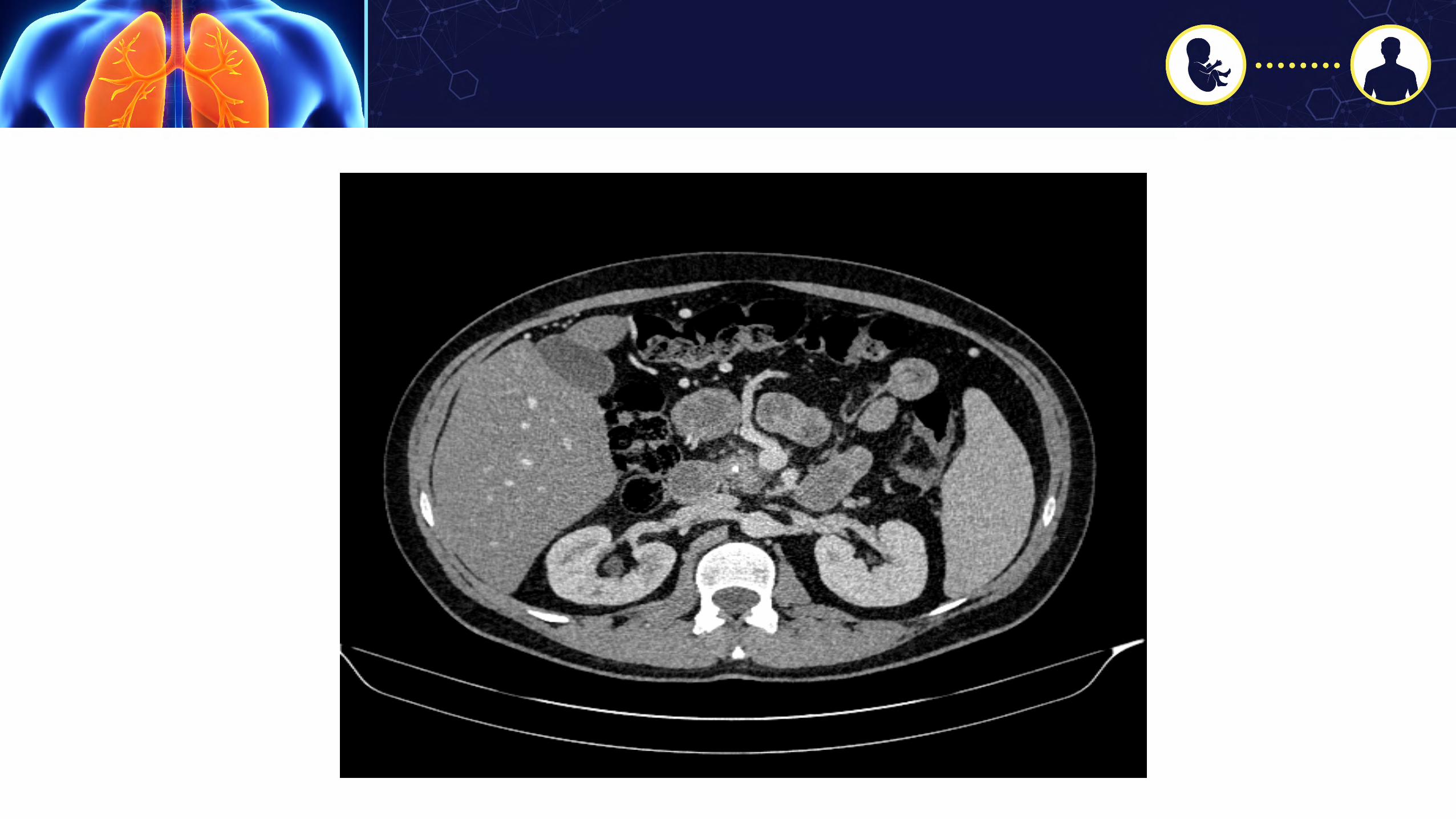
CT 2015 for ongoing pain (serum lipase <3)


Further f/u
• Repeat referral 2015 and EUS-guided CPB performed – no effect then six percutaneous CPB’s – not very effective
• Repeat referral in 2018 for chronic RUQ abdominal pain thought to be related to chronic pancreatitis (last ED visit 2016)
• Meds:
• 30mg oxycodone and acetaminophen (Percocet) daily, hydromorphone hydrochloride (Dilaudid) prn to avoid ED visits
• duloxetine and amitriptyline
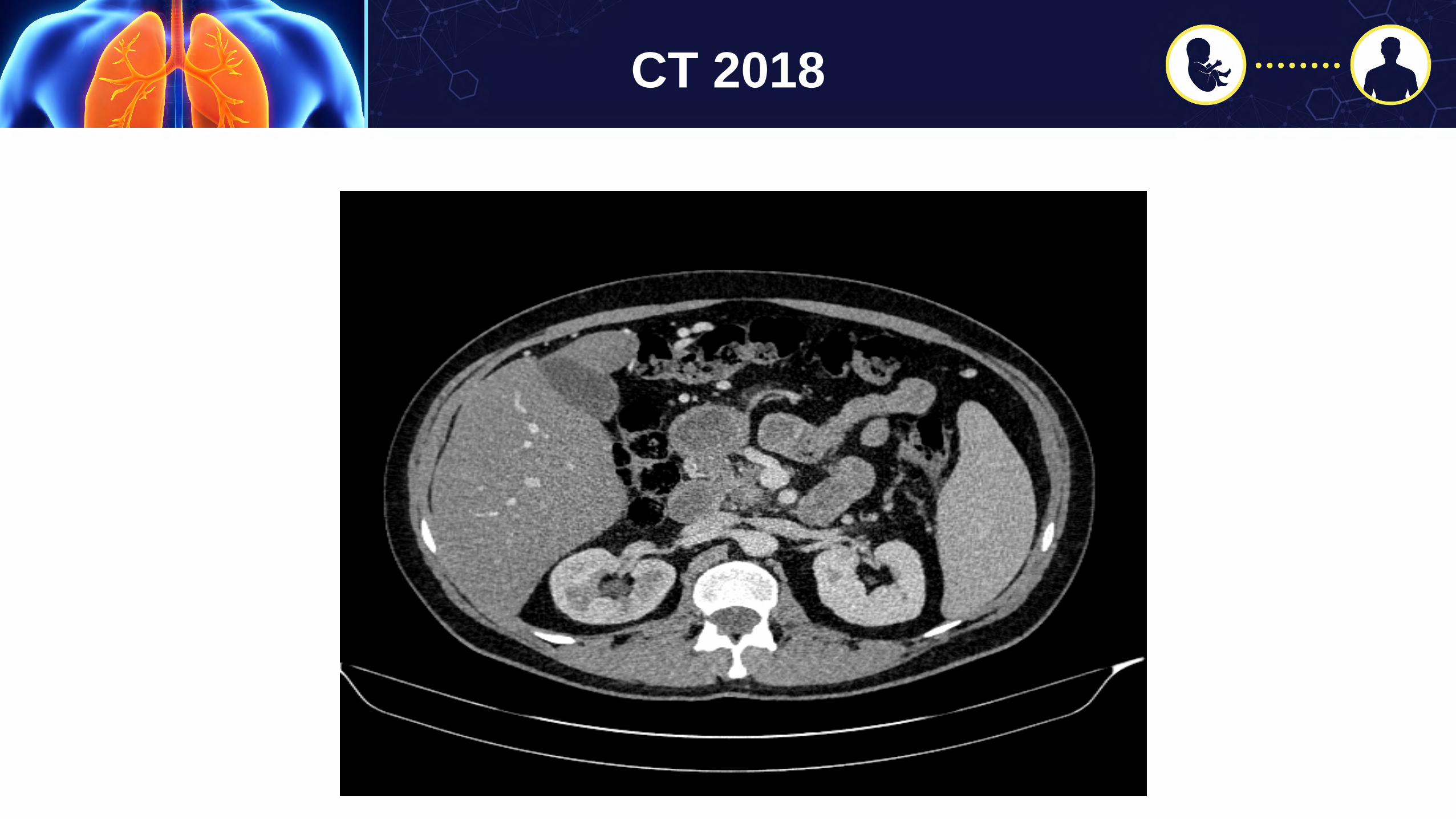
CT 2018



ERCP 2018
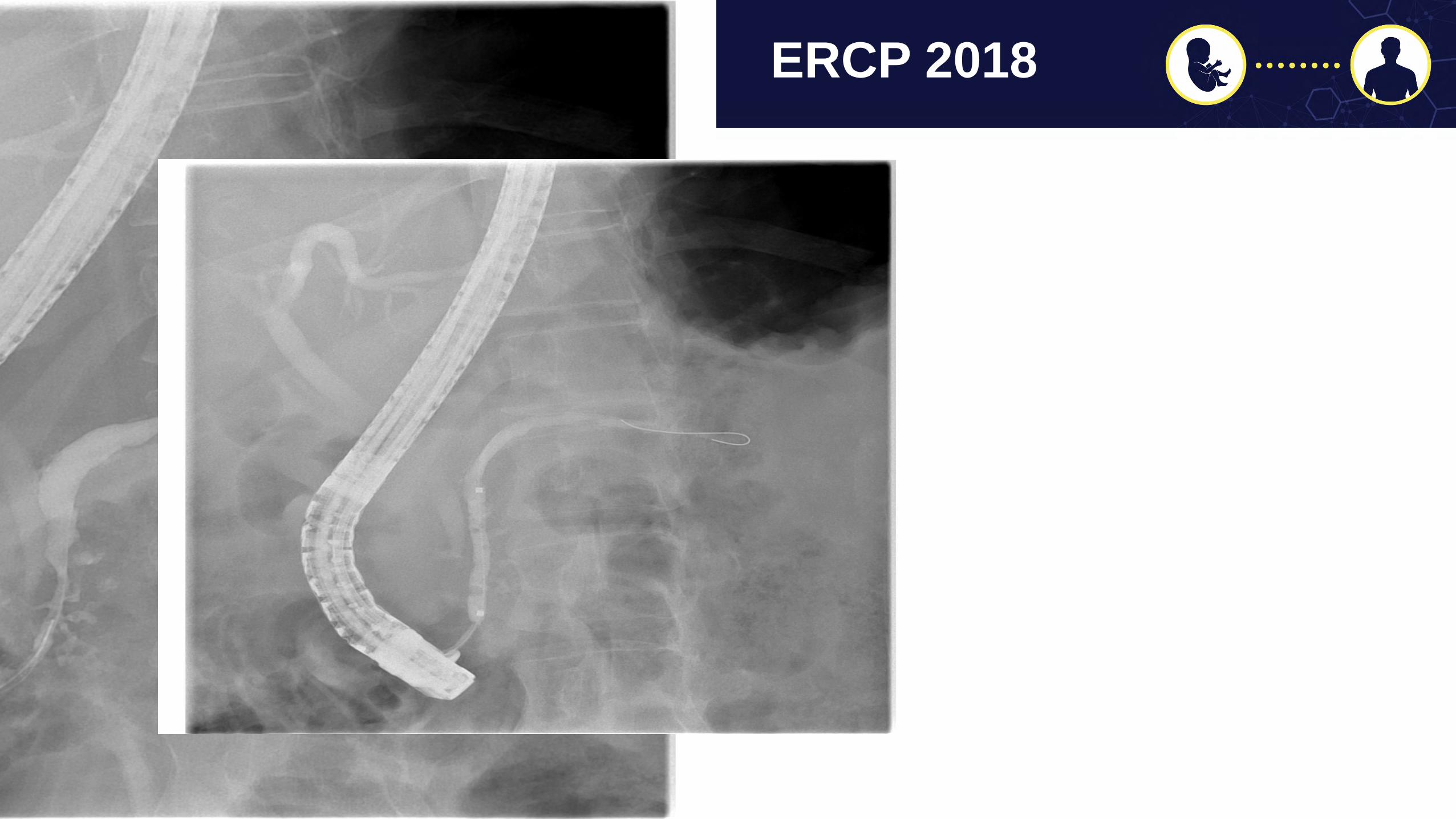
ERCP 2018
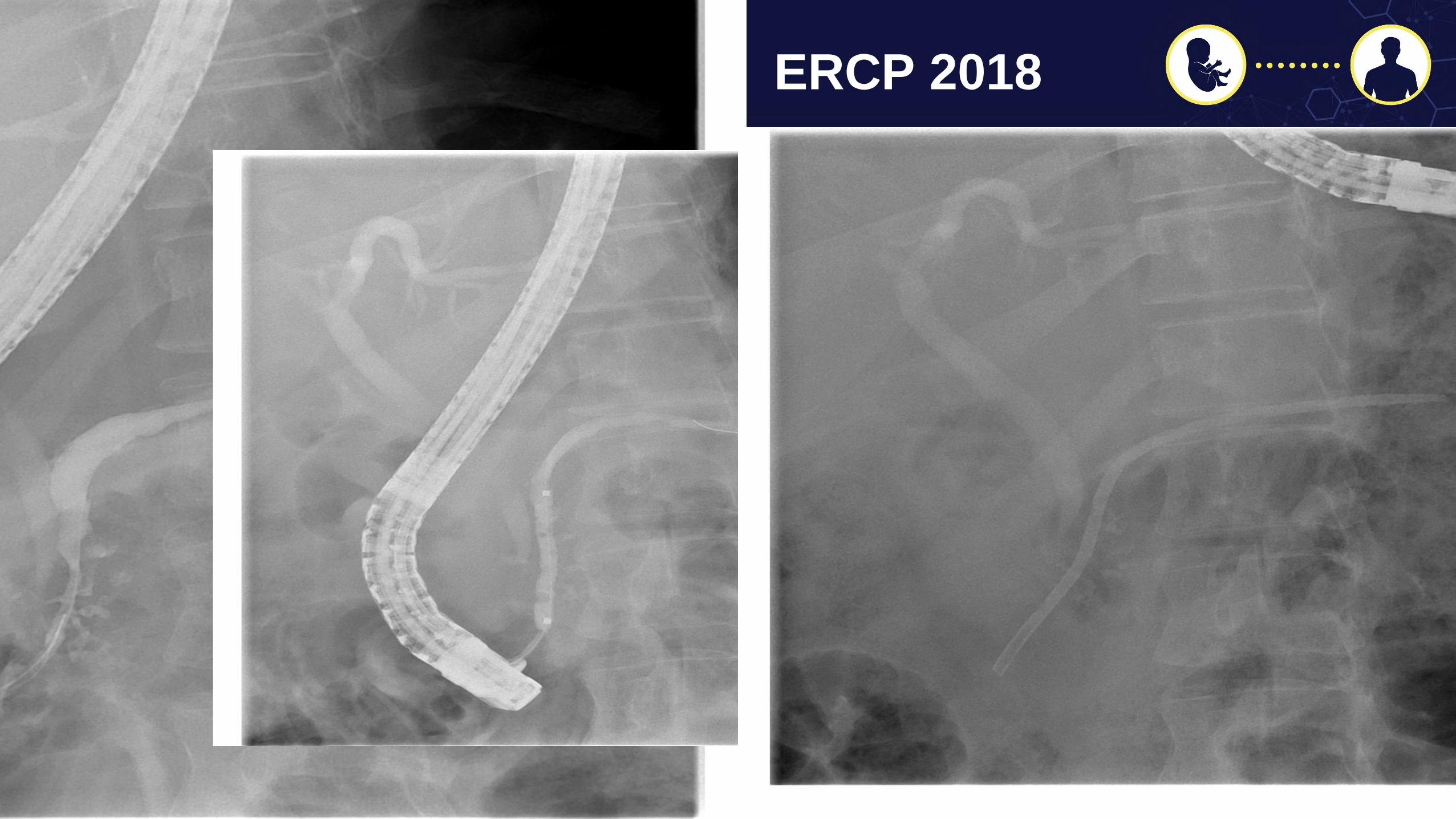
ERCP 2018
Further f/u
• Suboptimal response to stenting and I repeated EUS-CPB mid September 2018.
• From EPIC 9/27/18 related to chronic pain svc referral to consider dorsal column nerve stimulator
- ‘You know I'm good for now. If the pain gets worse I'll reach out. Thanks for your time!’

Treatment Options for Chronic Pancreatitis
• Analgesics, low-fat small frequent meals, pancreatic enzyme supplements, antioxidant therapy, celiac nerve blocks, pancreatic endotherapy
• Surgery if medical therapy fails
Trikudanathan, et al. Gastroenterol Clin North Am 2012Ahmet Gut 2003
Diagnosis of Chronic Pancreatitis
• Do best to determine that chronic pancreatitis is the actual etiology of the pain
• Serum pancreatic enzymes often normal
• Stool fat – need to lose over 90% of exocrine pancreas
• Low fecal elastase
• Imaging

A. PseudocystsB. CalcificationsC. Dilated ductsD. Parenchymal atrophyE. Dilated CBDF. Splenic vein thrombosisG. Gastric varices
CT
Etemad, Whitcomb 2001
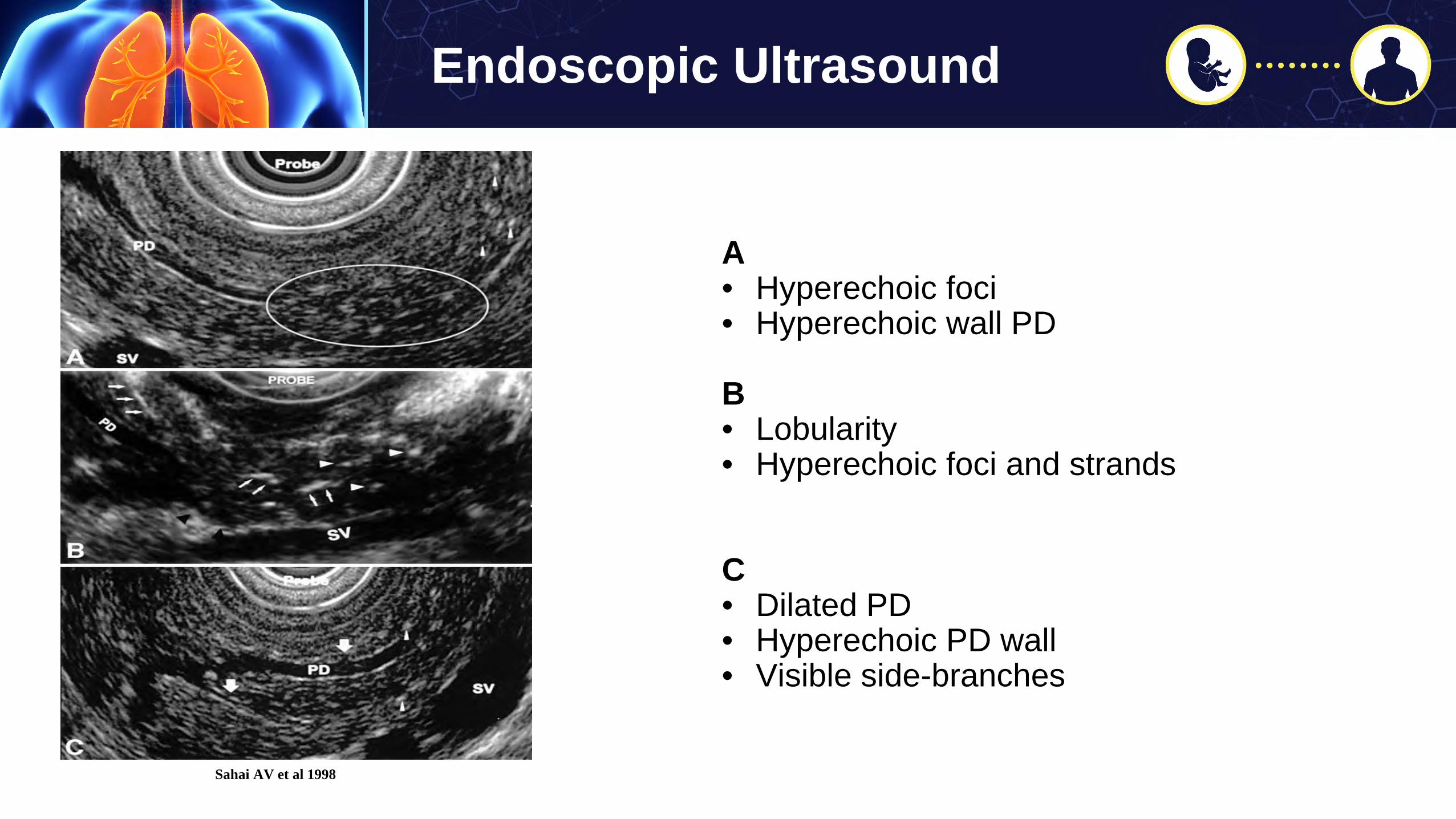
Endoscopic Ultrasound
Sahai AV et al 1998
A• Hyperechoic foci • Hyperechoic wall PD
B• Lobularity• Hyperechoic foci and strands
C• Dilated PD • Hyperechoic PD wall• Visible side-branches

Simple Analgesics
• Limit NSAID use due to GI toxicity but I do use it in adult patients motivated to be off or to minimize narcotics
- Can alternate with Acetaminophen
• Anti-spasmodics, anxiolytics, anti-depressants, anti-convulsants
• Opioids - Try tramadol
• Behavioral and Multi-disciplinary treatment important especially in children and caregivers
Drewes, et al. Pancreatology 2017Guidelines to manage pain in CP
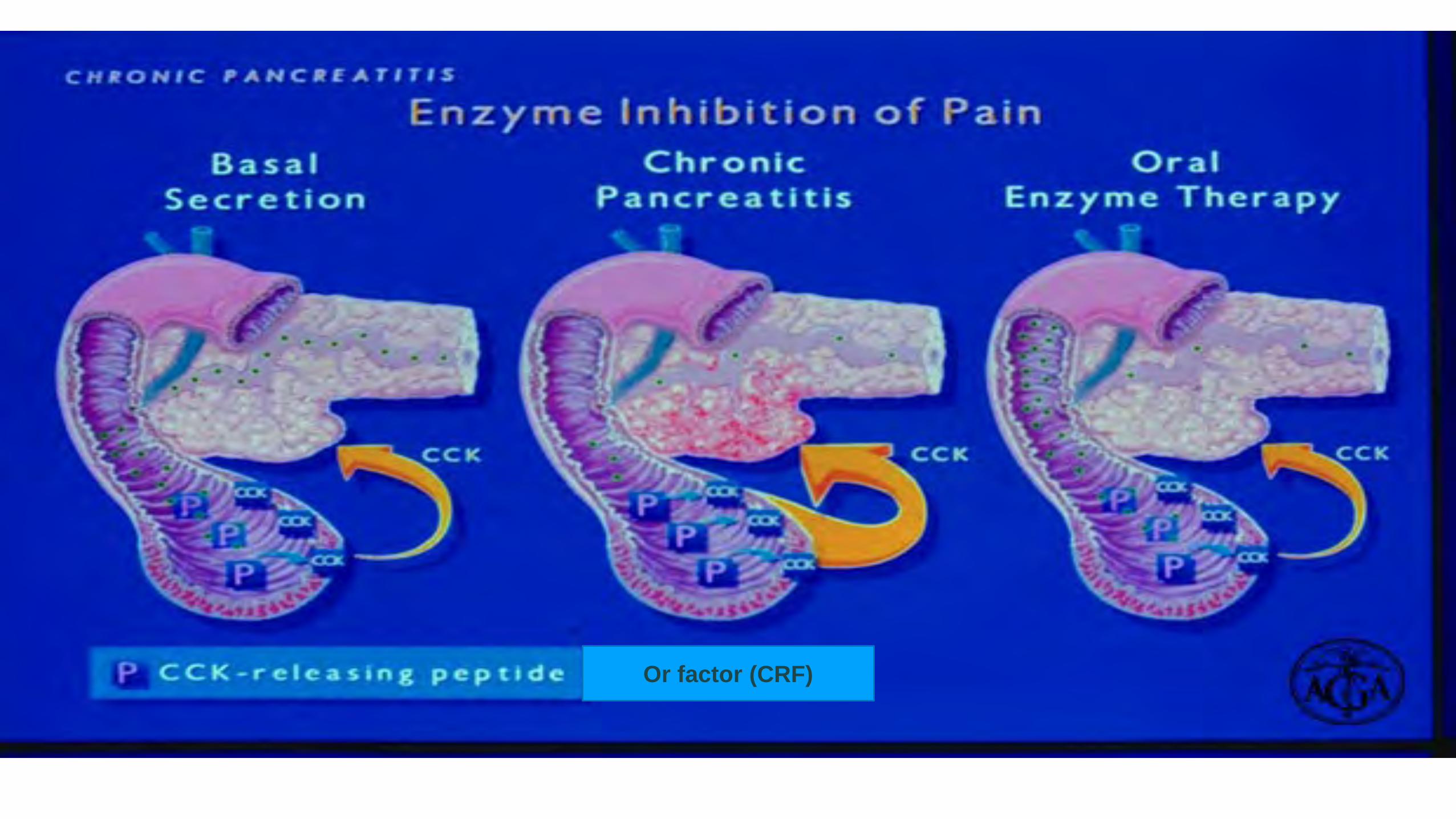
Or factor (CRF)
Enzymes for pain
• Cochrane review 2009
- Review of 10 RCT’s (361 pts) some compared enzymes to placebo, encapsulated vs. non-encap, types of PERT and impact on pain, steatorrhea and
weight loss
- No consistent benefit in pain (but most studies used encapsulated formulations)
- Only consistent benefit is in improving fecal fat (NS changes in weight)
Shafiq, et al. Cochrane 2009

Enzymes and Anti-oxidants for pain
• Panc enzyme rx with high protease content- Data mixed but used encapsulated formulations- Try ‘immediate release’ break capsules, sprinkle granules or use pancrelipase tablets,
powder (Viokase)- Requires concomitant PPI therapy- Two week trial sufficient
• Combined with antioxidants- b-carotene, vit C, vit E, selenium, and methionine- Consider use in combo with serotonin and norepinephrine reuptake inhibitors (SNRI)
or Gabapentinoid
Ahmed, et al. Cochrane 2014Talukdar, Pancreatology 2015

Endoscopic Therapy
• Treat pancreatic duct strictures associated with upstream ductal dilatation ‘obstructive’ pancreatic pain
• Treat PD stones (don’t typically see this in CF patients)
• EUS-guided celiac plexus block for neuropathic pain
• Or percutaneous CPB
Drewes, et al. Pancreatology 2017Guidelines to manage pain in CP
EUS-Guided Celiac Plexus Block for Neuropathic CP PainKaufman et al. J Clin Gastroenterol 2010
• Meta-analysis 6 studies
• 221 patients
• Technique and follow-up varied
• Pros: 51.46% reduction in chronic abdominal pain
• Cons: Transient

Drewes, et al. Pancreatology 2017Guidelines to manage pain in CP
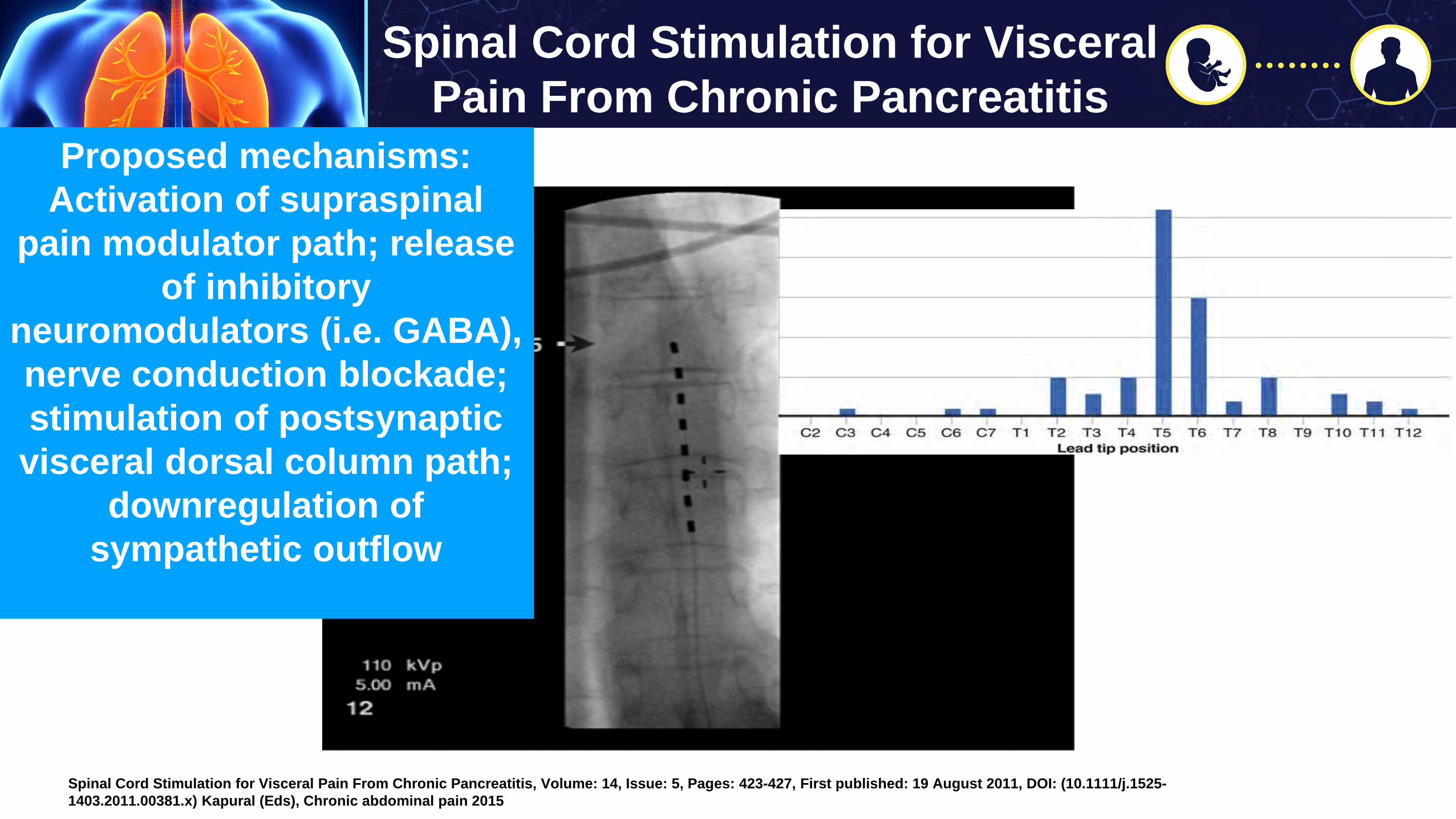
Spinal Cord Stimulation for Visceral Pain From Chronic Pancreatitis
Spinal Cord Stimulation for Visceral Pain From Chronic Pancreatitis, Volume: 14, Issue: 5, Pages: 423-427, First published: 19 August 2011, DOI: (10.1111/j.1525-1403.2011.00381.x) Kapural (Eds), Chronic abdominal pain 2015
Proposed mechanisms:Activation of supraspinal
pain modulator path; release of inhibitory
neuromodulators (i.e. GABA), nerve conduction blockade; stimulation of postsynaptic
visceral dorsal column path; downregulation of
sympathetic outflow

Spinal Cord Stimulation for Visceral Pain From Chronic Pancreatitis
Spinal Cord Stimulation for Visceral Pain From Chronic Pancreatitis, Volume: 14, Issue: 5, Pages: 423-427, First published: 19 August 2011, DOI: (10.1111/j.1525-1403.2011.00381.x)

Spinal Cord Stimulation for Visceral Pain From Chronic Pancreatitis
Spinal Cord Stimulation for Visceral Pain From Chronic Pancreatitis, Volume: 14, Issue: 5, Pages: 423-427, First published: 19 August 2011, DOI: (10.1111/j.1525-1403.2011.00381.x)
Total pancreatectomy for chronic pancreatitisI P Linehan, M A Lambert, D C Brown, A B Kurtz, P B Cotton, and R C G Russell
From the Departments of Surgery, Gastroenterology and Medicine, The Middlesex Hospital and Medical School, London
Summary• 29 patients• 80% had improvement in pain• 1 post-op death
Gut 1988
Total Pancreatectomy With Intraportal Islet Autotransplantation as a Treatment of Chronic Pancreatitis in Patients With CFTR Mutations
• U of Minn: TPIAT for CP w/CFTR vs. without CFTR• 12 year period (avg age mid-20’s; 80-100% daily narcotic usage)
- 20 CFTR homozygotes- 19 CFTR hetero- 20 age-gender matched w/o CFTR
• 1 yr f/u- No Insulin
• 40% CF• 22% hetero• 35% controls
- Off narcotics (variable f/u):• 80% of CF patients• 52% of carriers • 45% of controls Colling, et al. Pancreas 2018 Feb

© 2018 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology,. Published by Lippincott Williams & Wilkins, Inc.
2
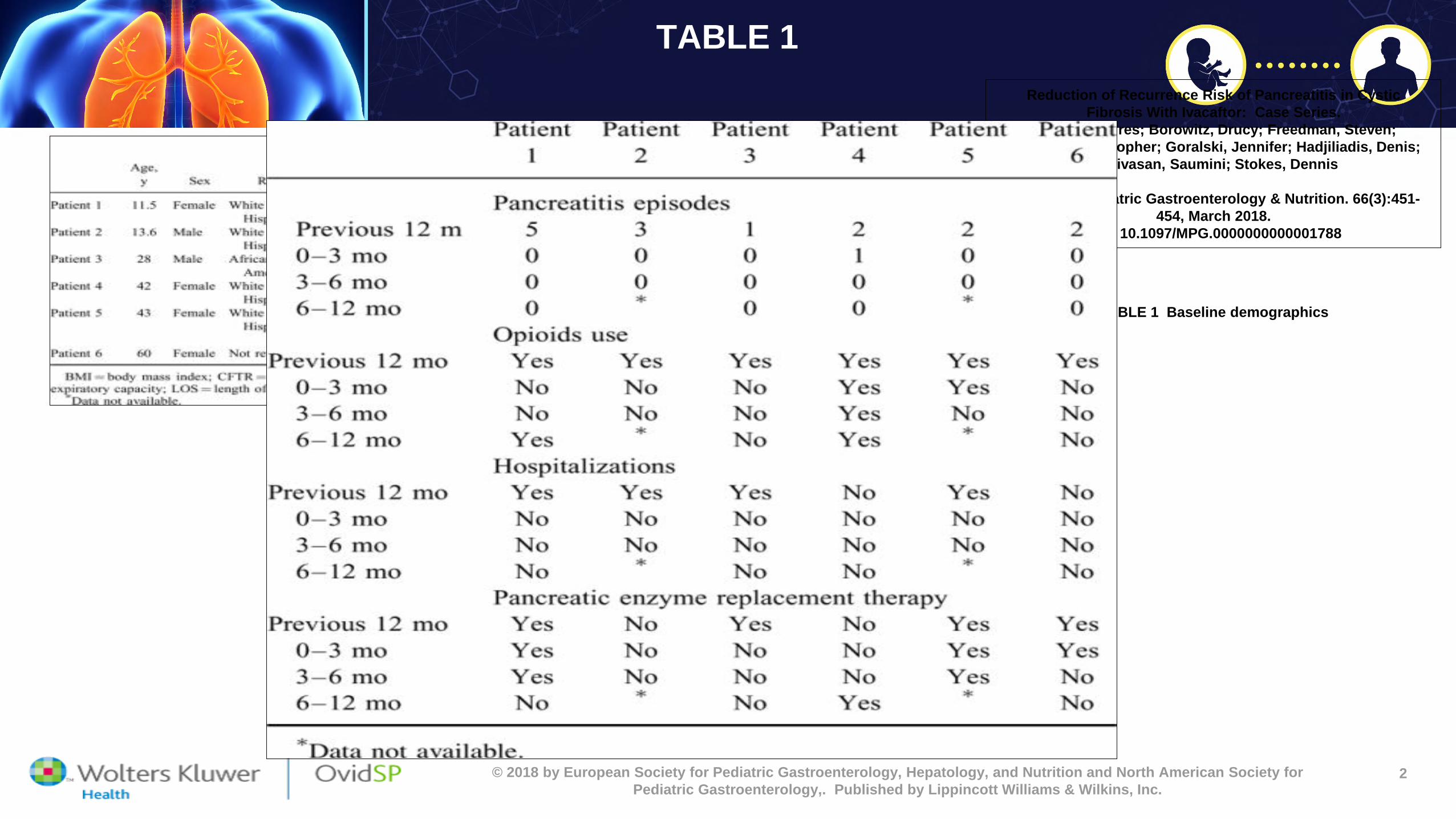
Reduction of Recurrent Pancreatitis in CF with Ivacaftor: Retro multi-center
Reduction of Recurrence Risk of Pancreatitis in Cystic Fibrosis With Ivacaftor: Case Series.
Carrion, Andres; Borowitz, Drucy; Freedman, Steven; Siracusa, Christopher; Goralski, Jennifer; Hadjiliadis, Denis;
Srinivasan, Saumini; Stokes, Dennis
Journal of Pediatric Gastroenterology & Nutrition. 66(3):451-454, March 2018.
DOI: 10.1097/MPG.0000000000001788
TABLE 1 Baseline demographics
Ivacaftor increases duodenal pH and bicarbonate secretion;
At least one CFTR mutation responsive to med;Median 2 prior AP episodes to rx
© 2018 by European Society for Pediatric Gastroenterology, Hepatology, and Nutrition and North American Society for Pediatric Gastroenterology,. Published by Lippincott Williams & Wilkins, Inc.
2
TABLE 1Reduction of Recurrence Risk of Pancreatitis in Cystic
Fibrosis With Ivacaftor: Case Series.Carrion, Andres; Borowitz, Drucy; Freedman, Steven;
Siracusa, Christopher; Goralski, Jennifer; Hadjiliadis, Denis; Srinivasan, Saumini; Stokes, Dennis
Journal of Pediatric Gastroenterology & Nutrition. 66(3):451-454, March 2018.
DOI: 10.1097/MPG.0000000000001788
TABLE 1 Baseline demographics

Pamela L. Zeitlin, MD, MPhil, PhD Silverstein Chair, Department of Pediatrics
Professor of PediatricsNational Jewish Health
Program Chair
Prevention is aimed at:
• Dehydrated, viscous pulmonary mucus
• Multiply drug resistant bacterial infections
• Impaired cough and mucociliary clearance due to viscous abnormal secretions
• Allergic fungal conditions
• Hemoptysis
• Hypoxic and hypercapneic respiratory failure

Infants with CF are usually born with normal lungs because:
a. CFTR gene is not expressed until after birth
b. Submucosal glands develop after birth
c. Other ion channels compensate for CFTR dysfunction
d. mucociliary clearance is unimportant until after birth
ARS Question
Origin of CF lung disease
• In Utero: CFTR is expressed in future airways and future submucosal glands
• Other non CFTR-dependent anion channels are co-expressed and compensate in the developing fetus with CF

Lung Development
http://www.embryology.ch/anglais/rrespiratory/phasen01.html

https://www.google.com/search?q=images+of+CFTR&tbm=isch&tbo=u&source=univ&sa=X&ved=2ahUKEwisxu3s_NPdAhWL5IMKHY9CUcQ7Al6BAgGEB0&biw=1668&bih=1249#imgrc=fz5z7BMqgI-edM:
CFTR
ENaC

Which of the following structure in the lungs is affected by CF?
a. Submucosal glands
b. Alveoli
c. Lymphatics
d. Vasculature
ARS Question

Perinatal origins of CF lung disease
• Prior to birth, ENaC (sodium) channels in alveolar epithelia up regulate expression and chloride channels in airways down-regulate function to prepare to reabsorb fetal lung fluid
• Absence of CFTR after birth leads to progressive dehydration of airway luminal fluid and viscous mucus because all the epithelial chloride channels decrease chloride secretion to facilitate air-breathing.

Thia LP, et al. Thorax 2014;69:320–327. doi:10.1136/thoraxjnl-2013-204176
Early Intervention
Intervene Earlier
• Target CF lung disease before symptoms occur
• Target genetics to optimize pulmonary and nutritional status
• Prevent bronchiectasis and loss of lung function
• Promote good nutrition
Develop Comprehensive Treatment Plan (CTP)
from Early Age
• Address comorbidities• Add exercise to CTP• Address adherence• Plan transition to adult care
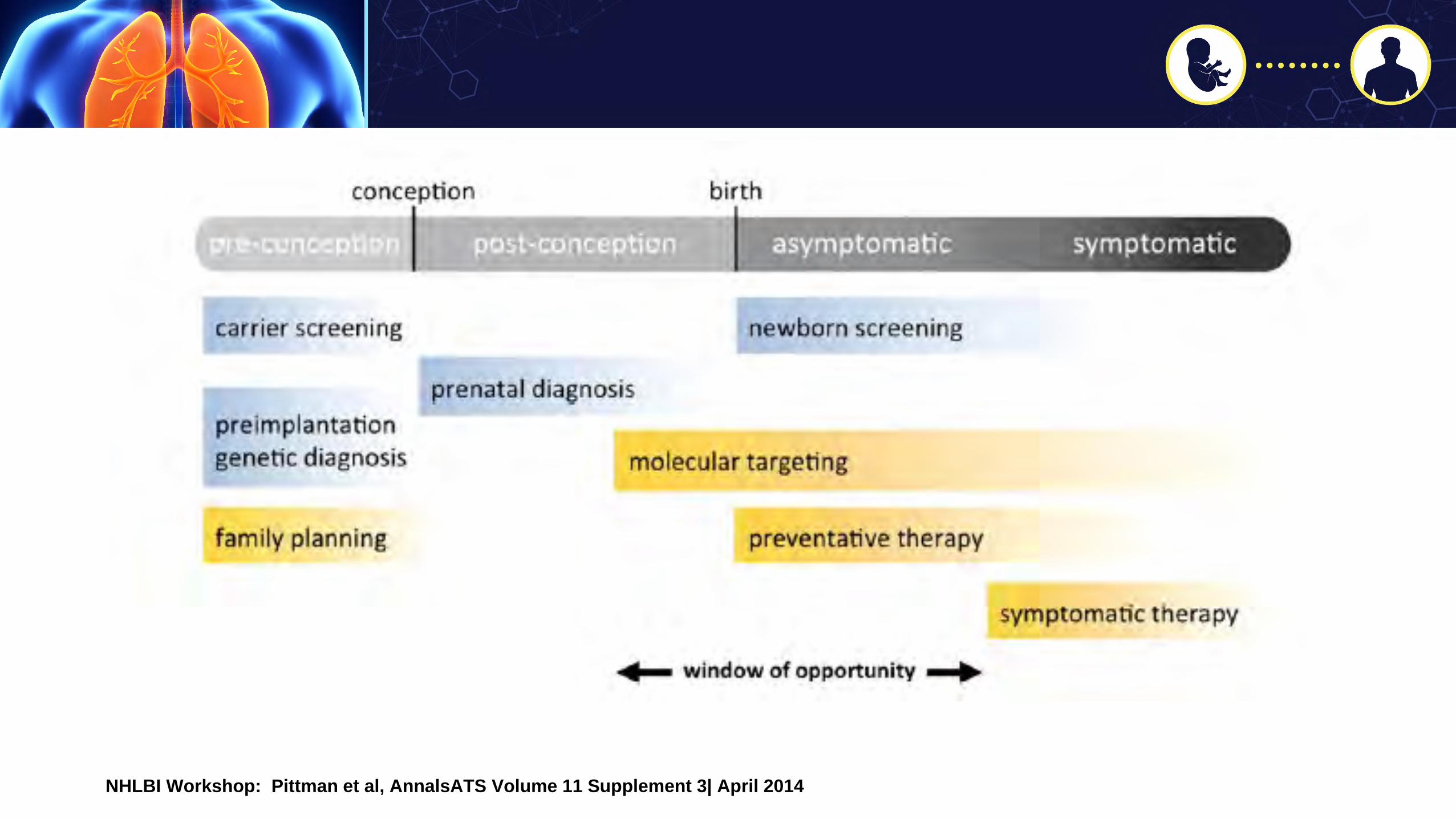
NHLBI Workshop: Pittman et al, AnnalsATS Volume 11 Supplement 3| April 2014
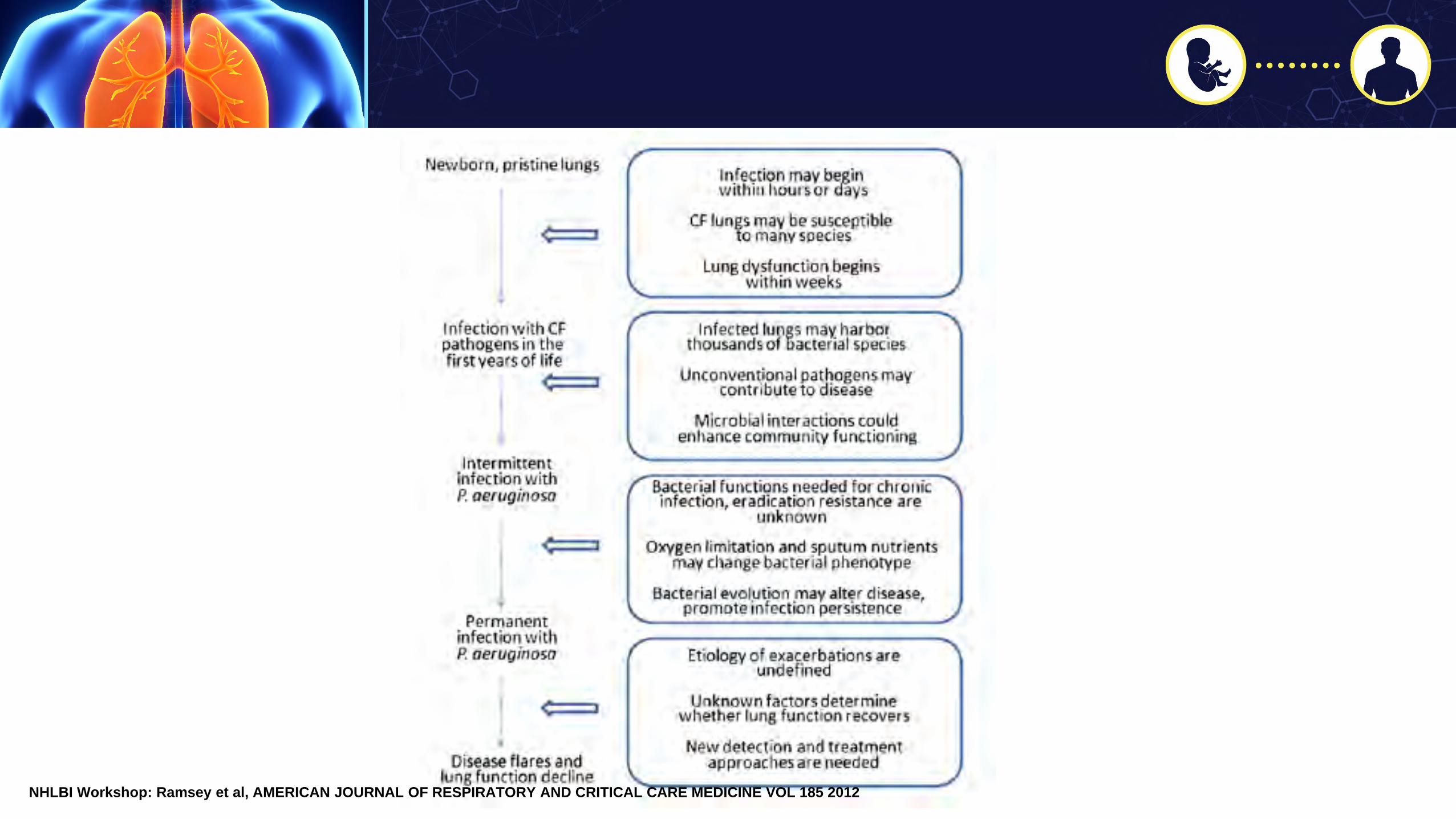
NHLBI Workshop: Ramsey et al, AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE VOL 185 2012
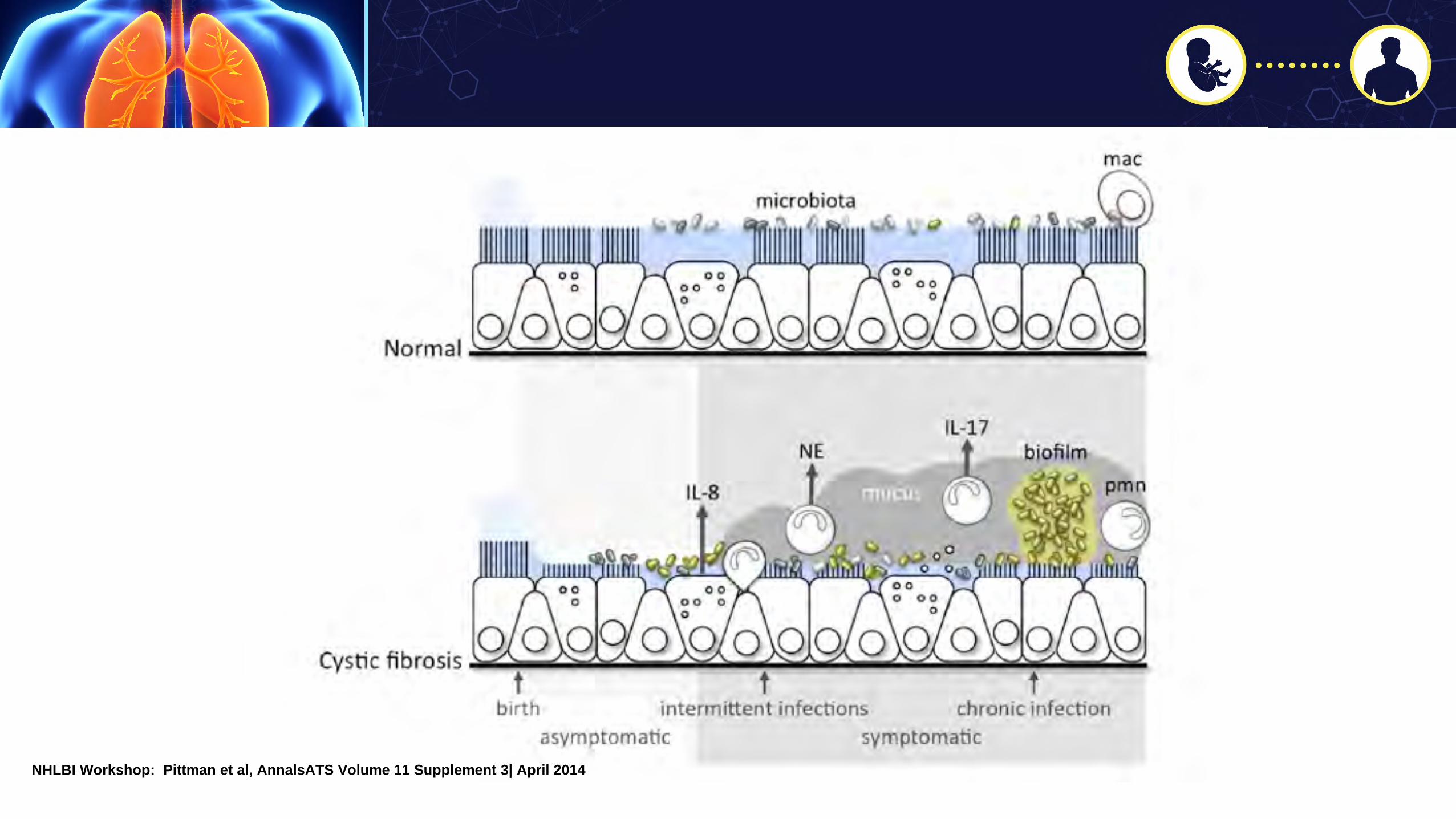
NHLBI Workshop: Pittman et al, AnnalsATS Volume 11 Supplement 3| April 2014
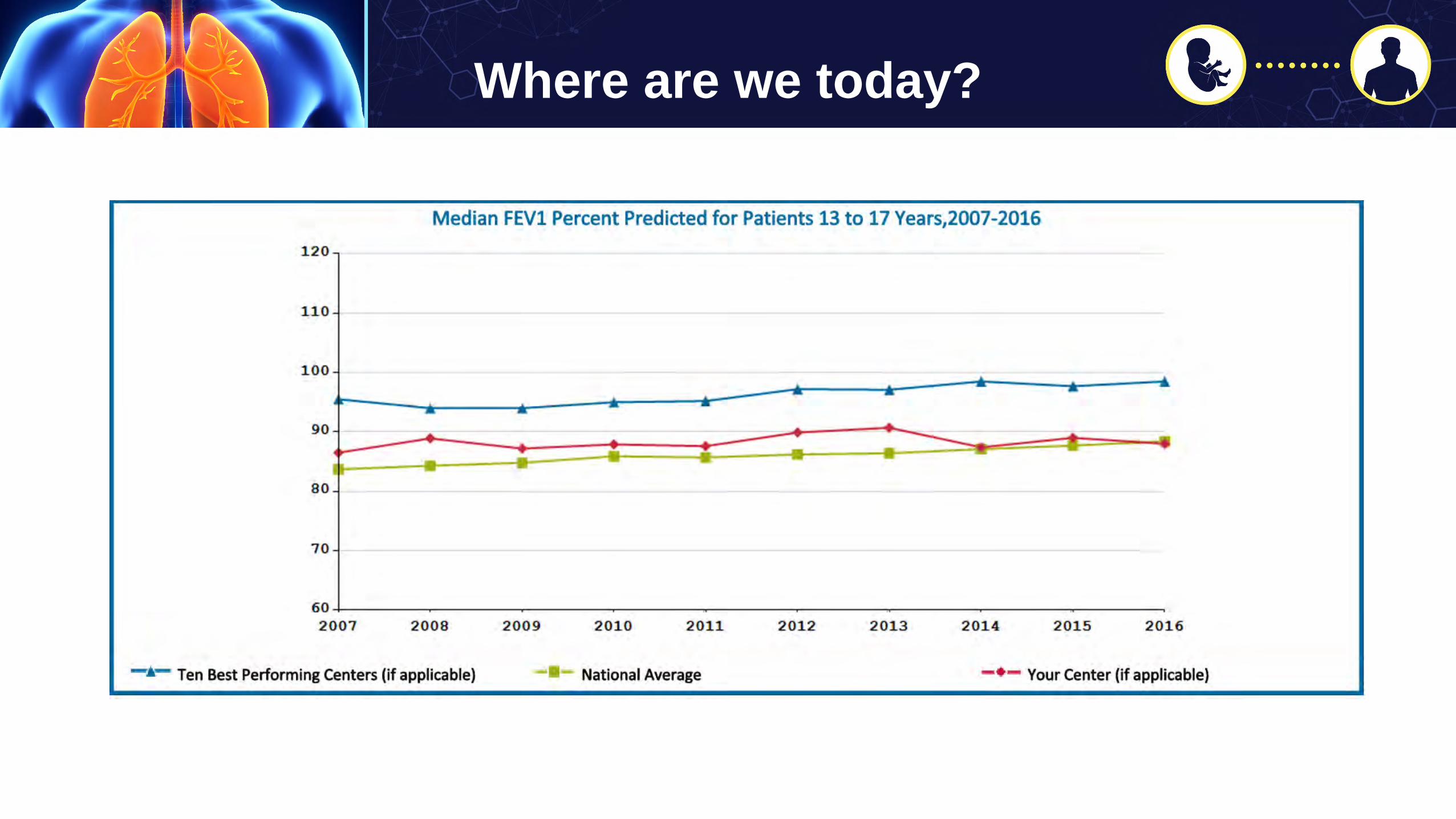
Where are we today?

Where are we today?
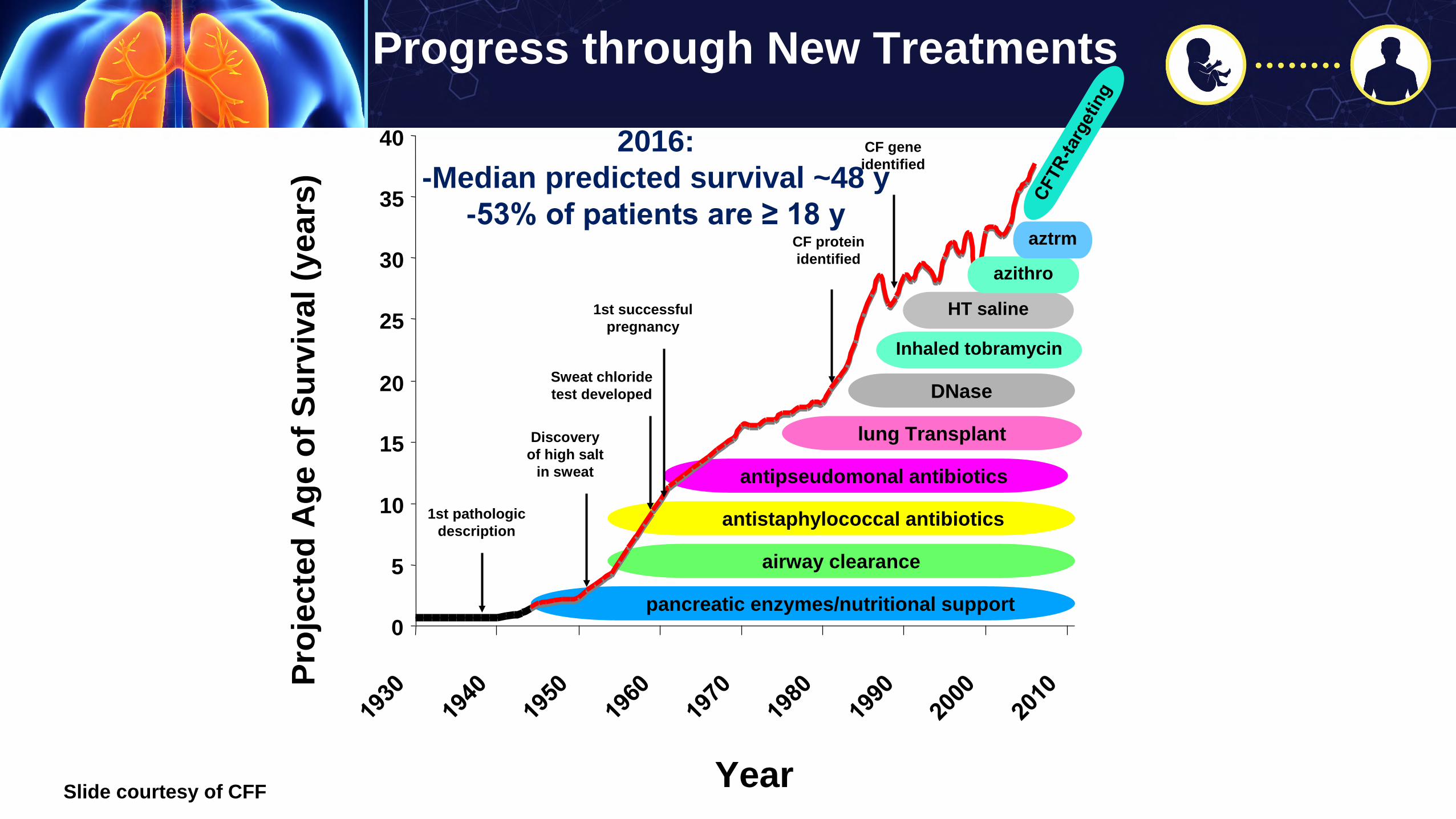
Progress through New Treatments
pancreatic enzymes/nutritional support
antistaphylococcal antibiotics
lung Transplant
antipseudomonal antibiotics
DNase
Inhaled tobramycin
airway clearance
0
5
10
15
20
25
30
35
40
Year
Proj
ecte
d A
ge o
f Sur
viva
l (ye
ars)
1st pathologicdescription
CF geneidentified
Discoveryof high salt
in sweat
Sweat chloridetest developed
1st successfulpregnancy
CF proteinidentified
HT saline
azithro
aztrm
2016:-Median predicted survival ~48 y
-53% of patients are ≥ 18 y
Slide courtesy of CFF
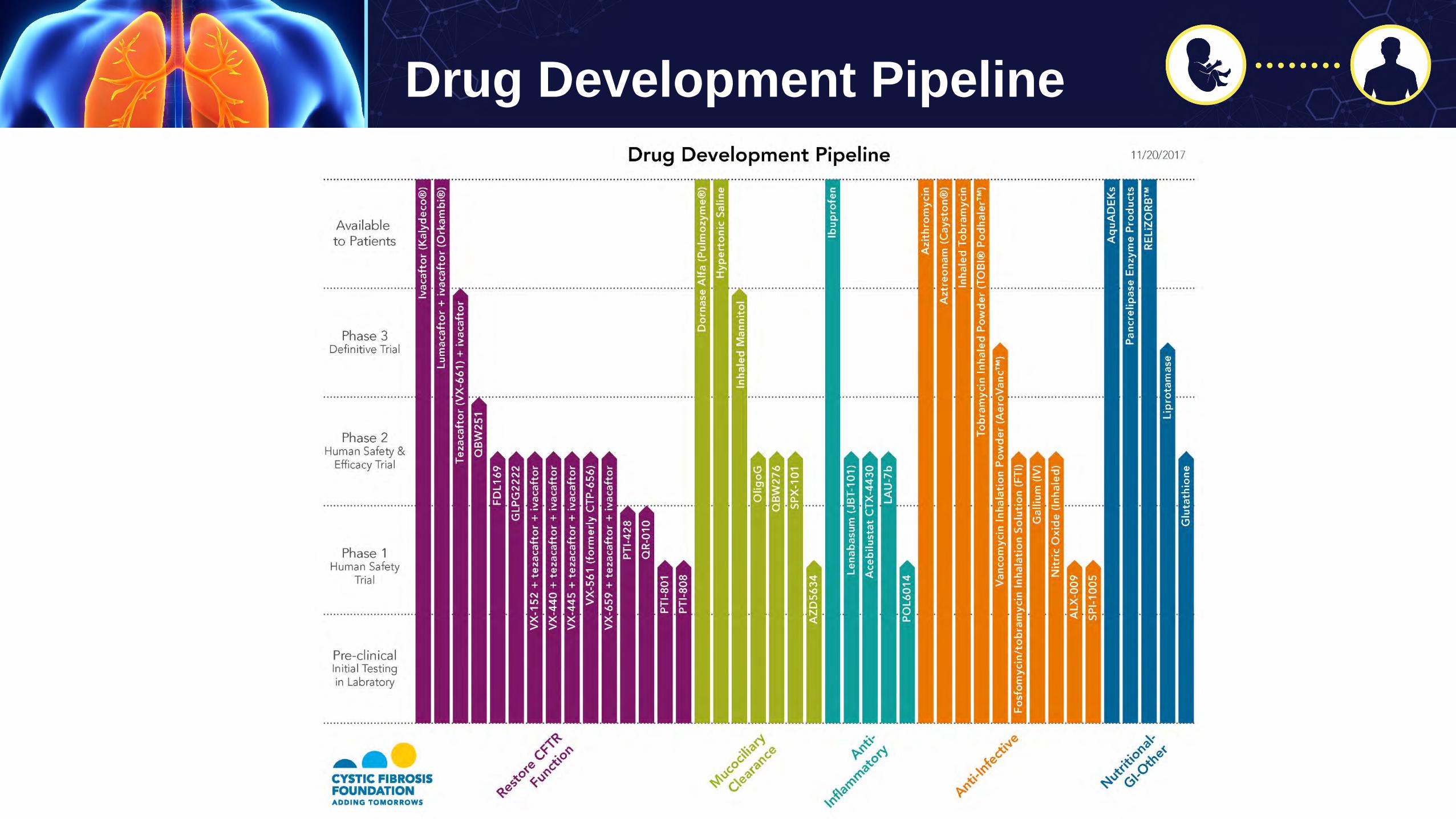
Drug Development Pipeline
Milene Saavedra, MD
Adult CF Program, National Jewish Health
October 18, 2018
Cystic Fibrosis: Maintaining Health into Adulthood
Milene Saavedra, MDAssociate Professor
Department of MedicineDivision of Pulmonary, Critical Care & Sleep Medicine
National Jewish Health

Cystic Fibrosis
https://www.cff.org/Our-Research/CF-Patient-Registry/2015-Patient-Registry-Annual-Data-Report.pdf. Accessed February 21, 2017.

Reprinted from Knowles MR, Durie PR. N Eng J Med. 2002;347:439-442.
Classic CF(Childhood Diagnosis)
Non-Classic CF(Adult Diagnosis)
Knowles MR, Durie PR. N Eng J Med. 2002

• 57 yo with h/o chronic rhinosinusitis, asthma, bronchiectasis,and ABPA seen in ENT clinic
• Genetic sequencing for CF sent
• Mutations: dF508/R117H/5T
• Future treatment: ivacaftor
Case

Genetic Testing Helps Identify Non-Classic Groups
Nick, J. A. et al, 2010. Effects of Gender and Age of Diagnosis on DiseaseProgression in Long-term Cystic Fibrosis Survivors. Am J Respir Crit CareMed. 182:614-626.
Nick J.A, et al. 2005. Manifestations of cystic fibrosis diagnosed inadulthood. Cur Opin Pulm Med 11:513-18.
Rodman, D. M. et al. Am J Respir Crit Care Med 171:621.
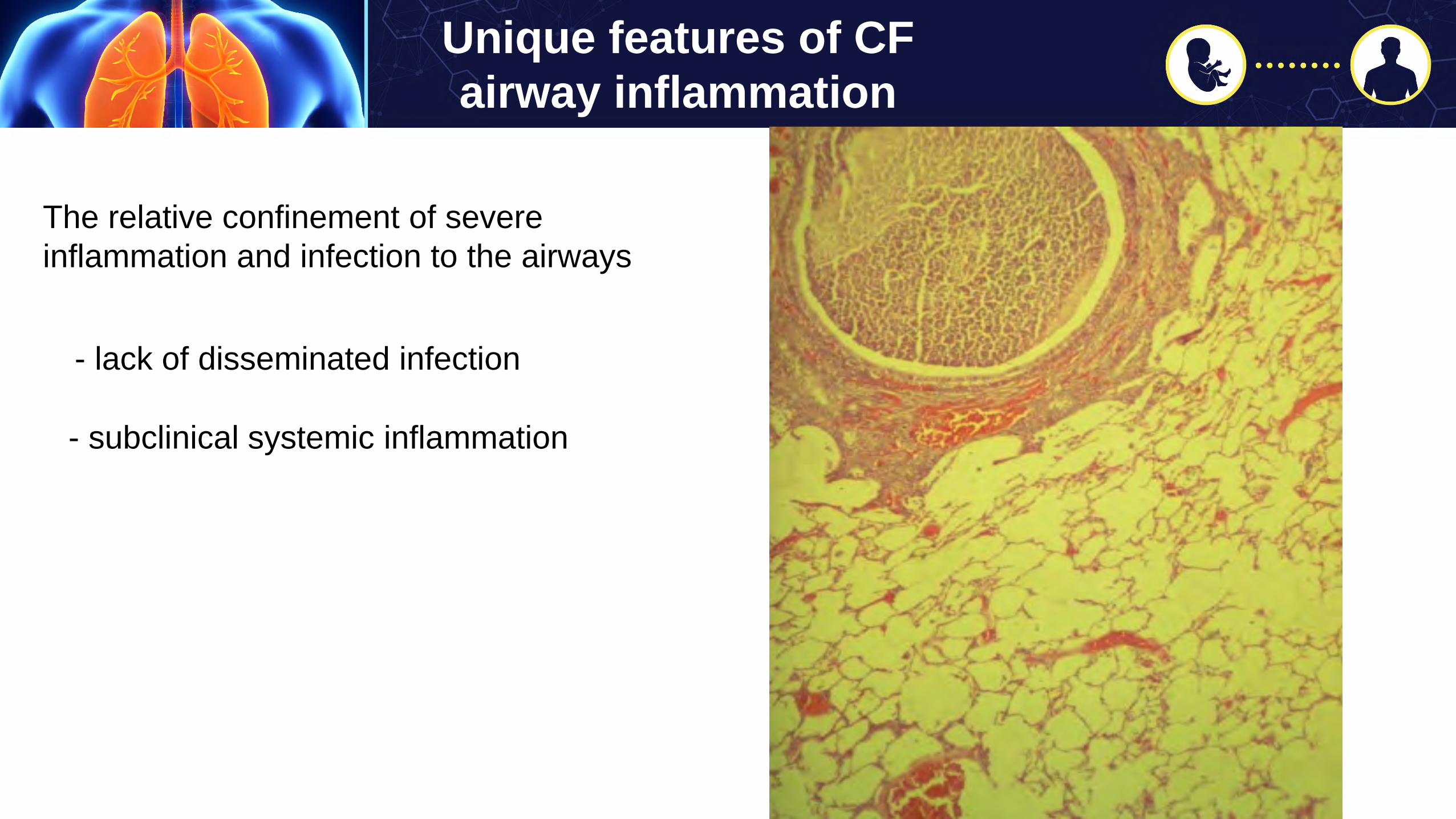
Unique features of CF airway inflammation
The relative confinement of severe inflammation and infection to the airways
- lack of disseminated infection
- subclinical systemic inflammation
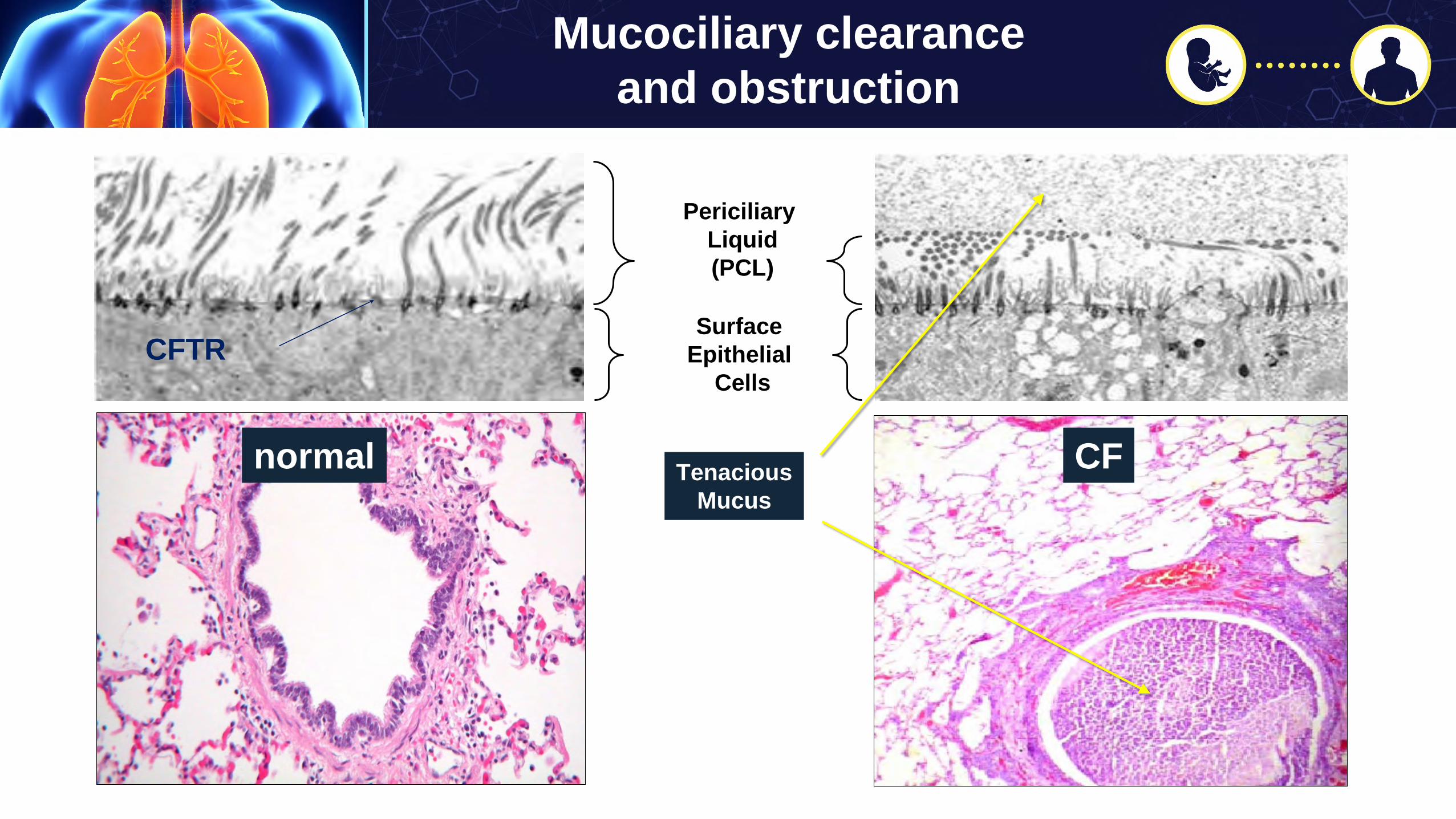
Mucociliary clearance and obstruction
TenaciousMucus
PericiliaryLiquid(PCL)
Surface Epithelial
Cells
normal CF
CFTR

Stoltz D A et al. Sci Transl Med 2010;2:29ra31-29ra31Wine J J Sci Transl Med 2010;2:29ps20-29ps20
Mucus accumulation – CF Pig
Lung Defense: Bacterial Eradication
Mucus plugging –CF Human and Pig
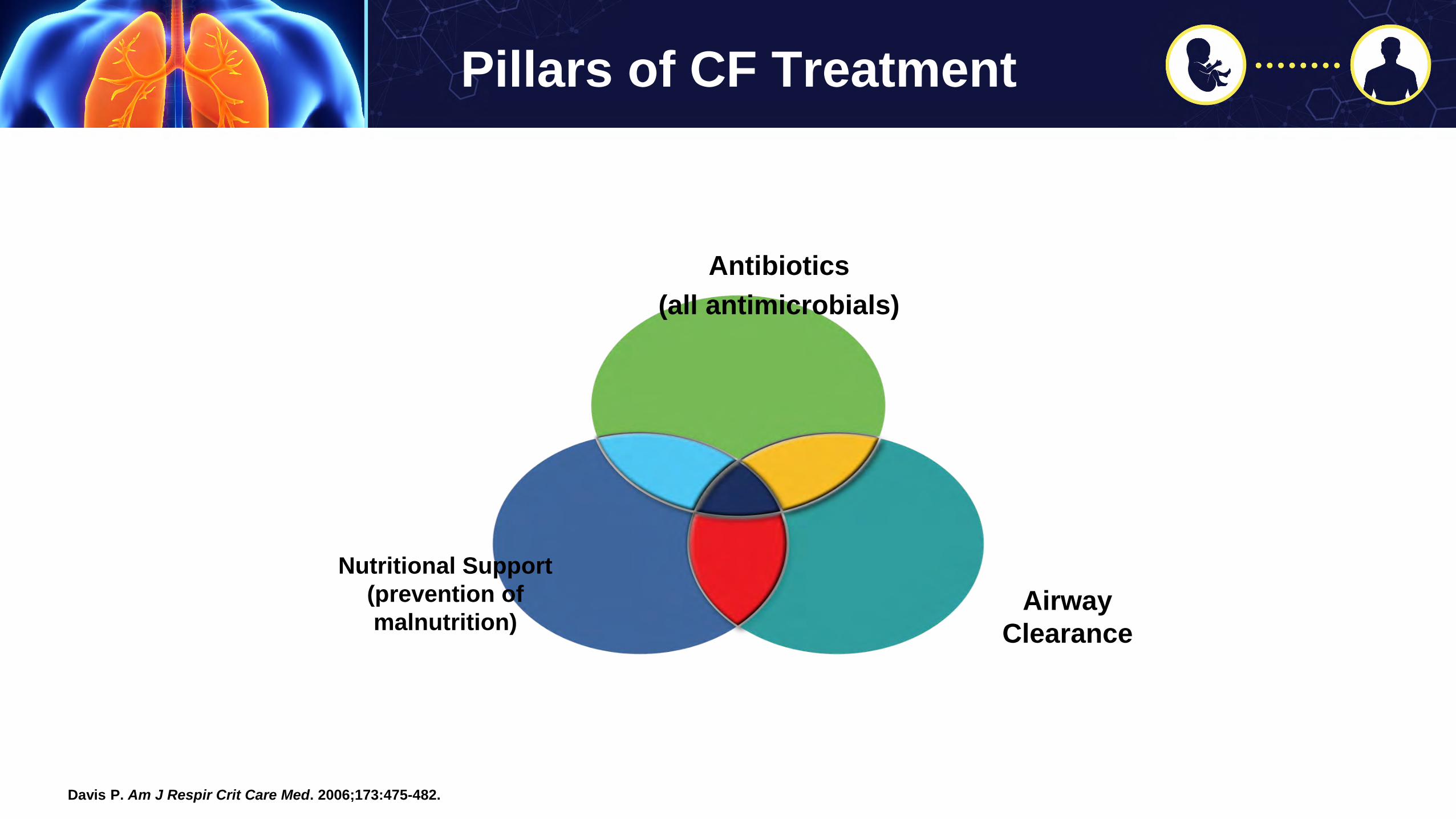
Pillars of CF Treatment
Antibiotics(all antimicrobials)
AirwayClearance
Nutritional Support(prevention ofmalnutrition)
Davis P. Am J Respir Crit Care Med. 2006;173:475-482.

Case #1: Pseudomonas
J is a 32 yo female with h/o severe CF pulmonary involvement (F508del homozygous)• Colonization with MSSA and Pseudomonas• Pancreatic insufficiency• CFRD• Hospital admissions are frequent approximately
every 3 months
CC: increased SOB and darker sputumSpirometry: FEV1 40% (from baseline FEV1 55% predicted)
Combination antibiotics are standard of care

Acute pulmonary exacerbation: most serious events in CF disease course
Sixty percent of patients DO NOT return to baseline lung function JCF 2017
PICC lineIntravenous antibiotics (14-21 days)Intensified chest physiotherapyDiabetes controlNutrition
Airway occlusion Arterial occlusion



How do we decide when PExis occurring?CFF guidelines
Clinical Practice Guidelines for Cystic Fibrosis. Cystic Fibrosis Foundation, 1997, Appendix VIII, Table 7

CFF Pulmonary exacerbation treatment guidelines
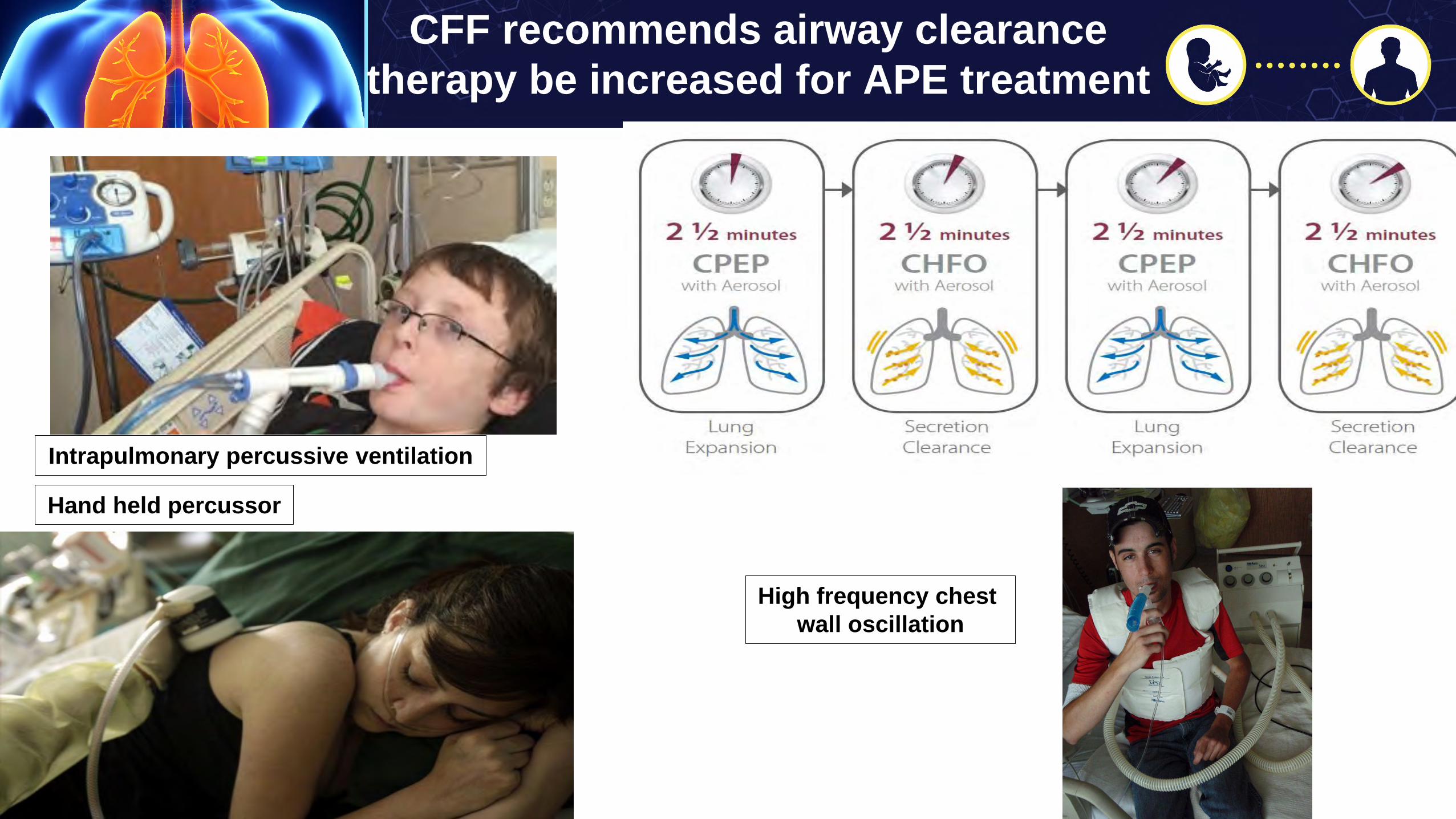
CFF recommends airway clearance therapy be increased for APE treatment
Intrapulmonary percussive ventilation
Hand held percussor
High frequency chest wall oscillation

Number of antibiotics used to treat P. aeruginosa
Standard of care for severe cases or inpatient treatment
• 2 anti-pseudomonal drugs to enhance activity and reduce selection resistant organisms.
Cell wall agentsCeftazidime 2 gm q 8 hrsMeropenem 2 gm q 8 hrsAztreonam 2 gm q 6 or 8 hrsPiperacillin/Tazobactam 4.5 gm q 6 hrs
+AminoglycosideTobramycin (8-10 mg/kg/d)

Treatment Pitfalls: Pathogen Complexity
• Multiple pathogens• Treatment of acute infection on a background of chronic infection (NTM infections)• Increased pathogens means more antibiotics- treatment not only of infection but cumulative
toxicities of antibiotics (harder to interpret results of tx)• Non infectious inflammation?• No coordinated approach to antibiotic antagonism or interactions when treating pathogens

CF Pulmonary Guidelines. 2013 AJRCCM
Guidelines for chronic care
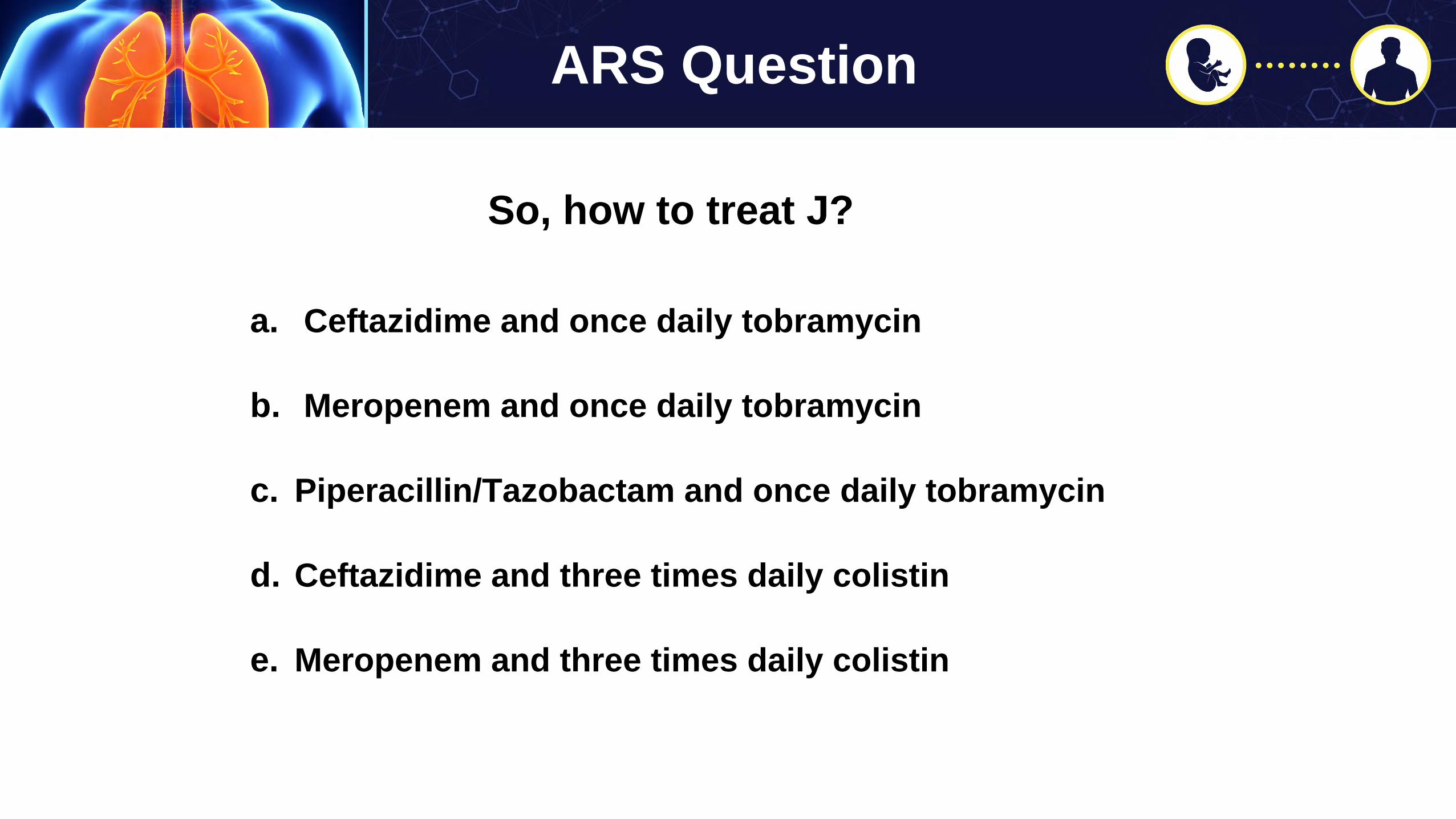
So, how to treat J?
a. Ceftazidime and once daily tobramycin
b. Meropenem and once daily tobramycin
c. Piperacillin/Tazobactam and once daily tobramycin
d. Ceftazidime and three times daily colistin
e. Meropenem and three times daily colistin
ARS Question

Case #2: Treatment of Burkholderiacepacia complex
L is a 38 yo with h/o severe CF lung disease, B cepacia subspecies B multivorans, PI, CFRD who presents with - temperatures to 100.6- increased chest tightness- CXR reveals no new infiltrates- FEV1 down to 28% from 36% baseline

• Reference lab at University of Michigan– send all first isolates, then once yearly• Identification of subspecies and transmissible strains• Genomovar III or B cenocepacia – more aggressive and poor prognosis with lung
transplantation• B cenocepacia clones can be transmissible between patients• Will follow patients longitudinally, as they move from Center to Center• Intrinsically markedly resistant, meaning requires a minimum of 3 drugs to treat
Burkholderia cepacia- identification and treatment

Aaron, AJRCCM, 2000
Dales, Eur J Clin Inf Dis, 2009
Sensitivities of planktonic vs biofilm grown isolates

Hemoptysis guidelines
When should the patient with hemoptysis be treated with antimicrobials?Panel: with all episodes > 5 mls
Should the patient with hemoptysis stop airway clearance therapies?Panel: No, for scant hemoptysis. Yes, for massive hemoptysis.
And nebulized therapies?Panel: No, for scant hemoptysis. Yes, stop nebulized hypertonic saline for massive.
Which studies should be performed in patients before BAE?Panel: The patient with massive hemoptysis should not undergo Bronchoscopy before BAE. Panel with low enthusiasm for CT chest (but may yield useful info).
Flume et al, Cystic Fibrosis Pulmonary Guidelines, AJRCCM,2010

DIOS: Distal intestinal obstructive syndrome
1. Providers need to actively inquire if pts with symptoms
2. Implementation of a step-up bowel regimen is important
Treatment: osmotic laxatives (PEG), gastrografin enema,endoscopic approaches and finally in rare cases, surgery

CFTR Essential Functions: Intestine
• CFTR = bicarbonate and chloride secretion
• Abundant CFTR expression in small intestinal enterocytes

Human CF Intestine
CLINICAL MANIFESTATIONS
Inflammation, Mucosal Injury
Small Intestinal Bacterial Overgrowth
Mucus retention
Altered ion transport

NTM in cystic fibrosis
• Prevalence of NTM-positive culture rates in US from CFF registry data: 12%(with variation from 0-28% between individual states)
• Most common species identified are Mycobacterium avium complex and therapidly growing Mycobacterium abscessus complex.
• Acquisition associated with age: 10% in children <10 and 30% in adults >40
• A single NTM culture is not clinically significant; 1/3rd do not recur
Martiniano et al, AnnalsATS, 2014

Primary Objective:• Develop user-friendly, evidence-based protocols for NTM disease diagnosis and
treatment to be used for all CF patients in the US.
Secondary Objectives:• Define an expected rate of development of NTM disease for patients with positive
cultures. • Identify clinical features associated with the development of disease.• Define the expected rate of response to treatment using the current CFF/ECFS NTM
guidelines, independent of expert consultation or specialized facilities.• Define the rate of side effects or toxicities requiring alternate drug combinations.• Facilitate molecular analysis of NTM isolates from CF patients.
Colorado PREDICT and PATIENCE Trials
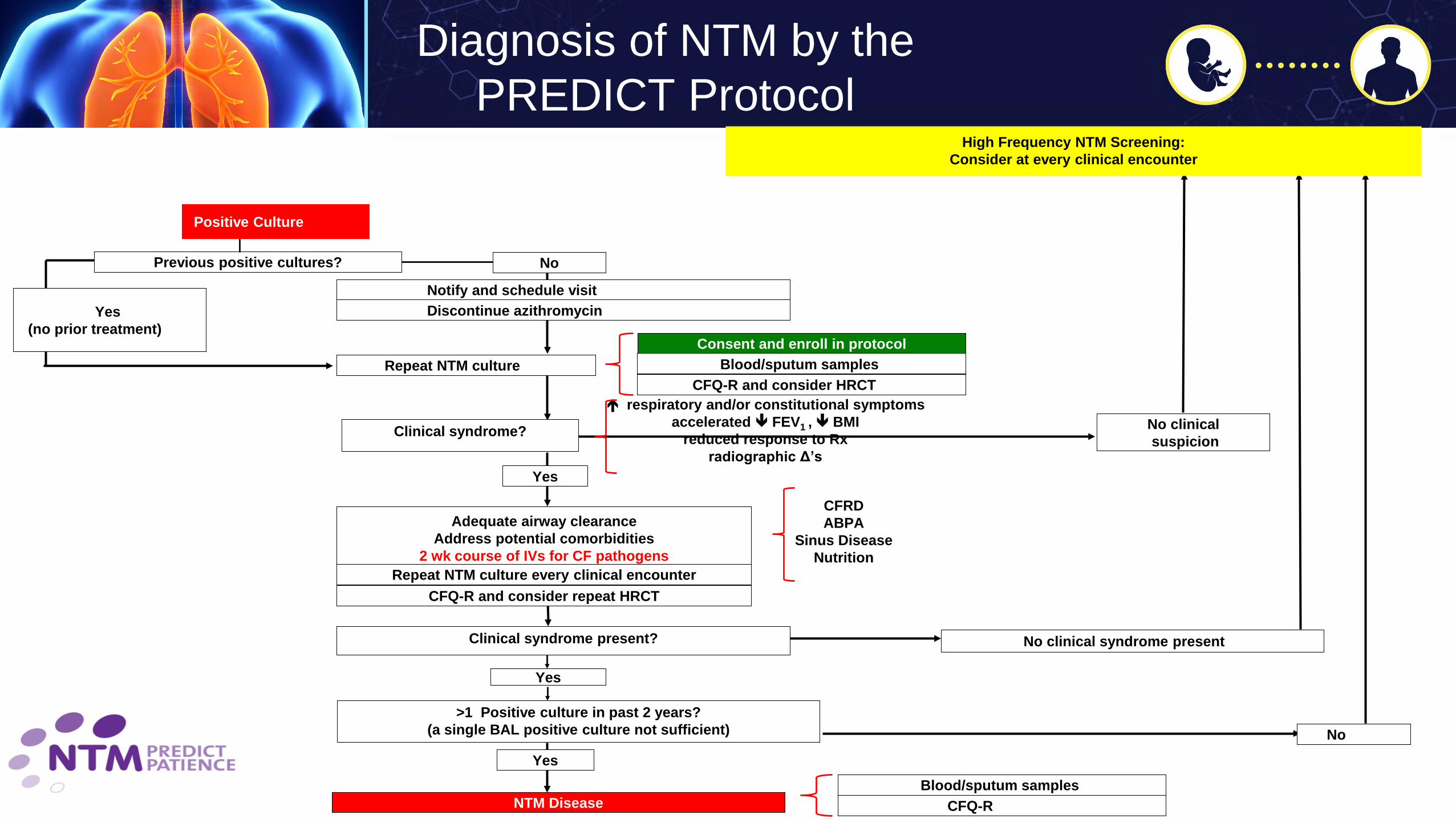
NoPrevious positive cultures?
Yes (no prior treatment)
Clinical syndrome? No clinicalsuspicion
Clinical syndrome present? No clinical syndrome present
No
Yes
Adequate airway clearanceAddress potential comorbidities
2 wk course of IVs for CF pathogensRepeat NTM culture every clinical encounter
Repeat NTM culture
>1 Positive culture in past 2 years?(a single BAL positive culture not sufficient)
Yes
Yes
NTM Disease
Positive Culture
High Frequency NTM Screening:Consider at every clinical encounter
respiratory and/or constitutional symptomsaccelerated FEV1 , BMI
reduced response to Rxradiographic Δ’s
Consent and enroll in protocolBlood/sputum samples
CFQ-R and consider HRCT
CFRDABPA
Sinus DiseaseNutrition
Blood/sputum samples CFQ-R
Discontinue azithromycinNotify and schedule visit
CFQ-R and consider repeat HRCT
Diagnosis of NTM by the PREDICT Protocol


2Intensive IV Alternates:Cefoxitin
Tigecycline
Azithromycin
Yes
M. abscessus or M. bolletii
ImipenemAmikacin
AzithromycinLinezolid
Amikacin (neb)Moxifloxacin
Linezolid 3ContinuationAlternates:
MoxifloxacinClofazimineMinocycline
PATIENCE Treatment Protocols
1 Severe Disease:•Smear positive +/or•Cavitary infection
radiographically +/or•Systemically ill
M. avium complex
Additional alternates:
Amikacin (neb)ClofazimineMoxifloxicin
M. abscessus complex
No
M. massiliense
12 wksImipenemAmikacin
Azithromycin
AzithromycinAmikacin (neb)
Linezolid
Functionalerm gene
IntensivePhase2
ContinuationPhase3
Macrolide sensitiveYes
Severe1?
No
RifampinAzithromycin
Ethambutol
Yes
No
Amikacin IV (12 wks)
AzithromycinRifampin
Ethambutol
Preliminary Conclusions
• Use of an NTM Treatment Protocol within a CF care center setting is feasible• 80% of subjects have tolerated first line treatment• Initiating a standardized, first-line treatment for MAC and MABSC pulmonary
disease may result in:– Good culture conversion to negative rates• 10/12 subjects with > 6 months on therapy have converted to negative cultures
(12/12 MAC, 2/4 MABSC)• 7/12 have > 12 months of negative cultures
– Stabilization of FEV1 percent predicted decline• Improved culture conversion rates (compared to historic rates) may in part be due
to optimizing CF care first (PREDICT)• Emergence of dual infection was common (33%)• Delayed response or failure to clear NTM after >6 months of treatment was often
associated with dual infections
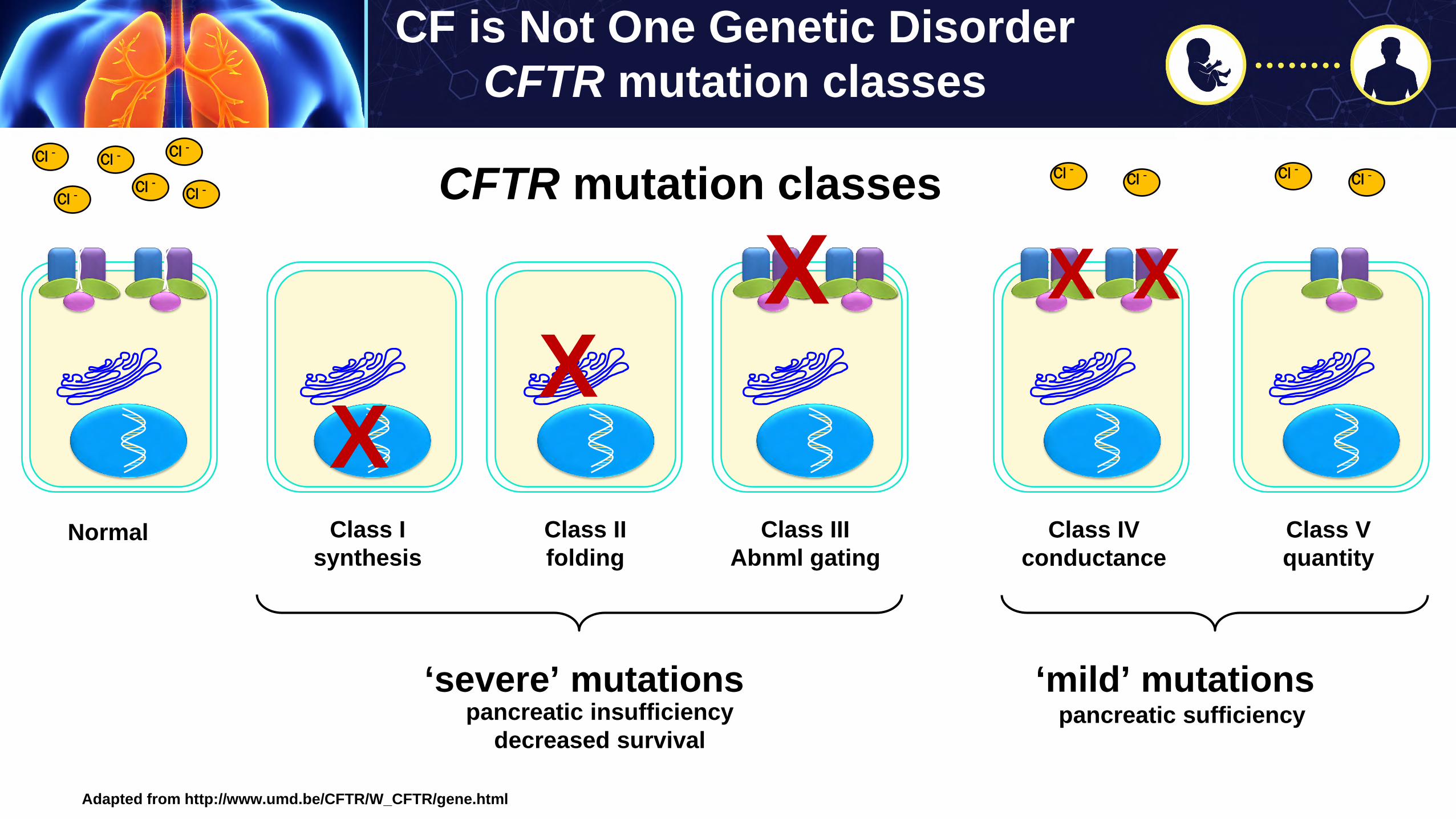
CF is Not One Genetic DisorderCFTR mutation classes
Adapted from http://www.umd.be/CFTR/W_CFTR/gene.html
Cl -Cl -
Cl -
Cl -
Cl - Cl -
Normal
XClass I
synthesis
XClass IIfolding
X
Class IIIAbnml gating
XCl -Cl -
X
Class IVconductance
Cl -Cl -
Class Vquantity
‘severe’ mutationspancreatic insufficiency
decreased survival
‘mild’ mutationspancreatic sufficiency
CFTR mutation classes
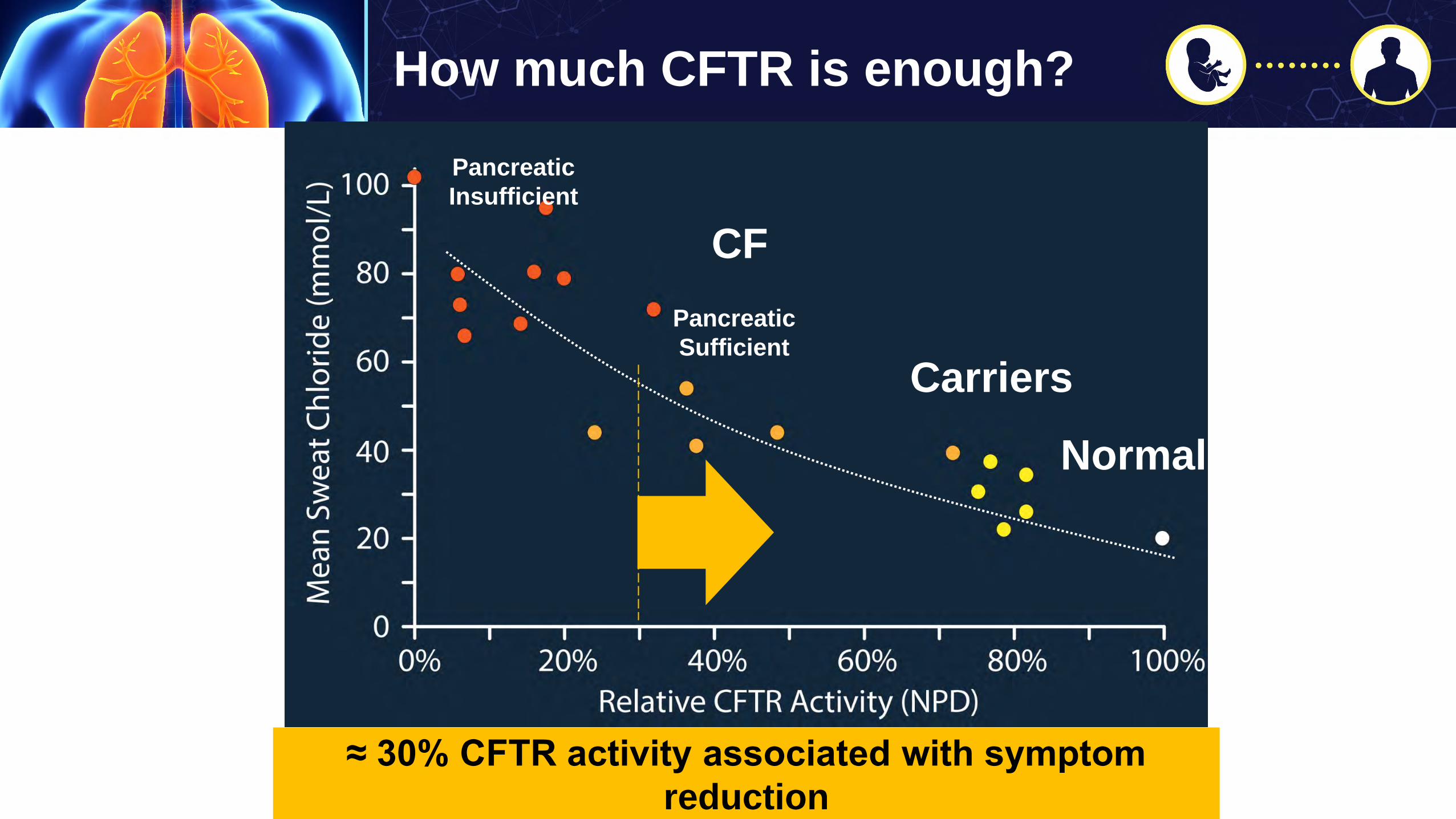
Carriers
Adapted from Accurso et al JCF 2013
Normal
CF
Pancreatic Insufficient
Pancreatic Sufficient
≈ 30% CFTR activity associated with symptom reduction
How much CFTR is enough?
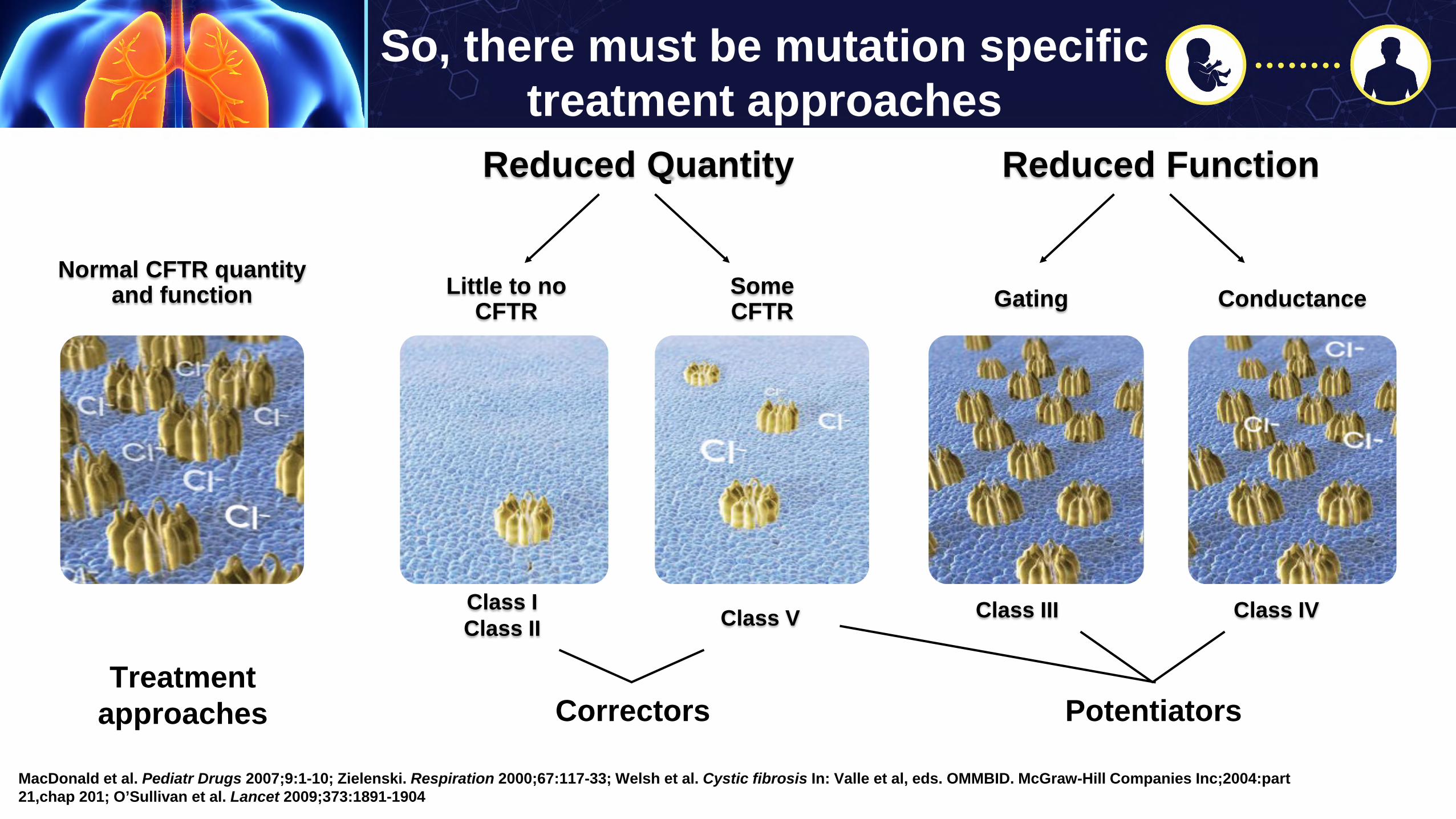
So, there must be mutation specific treatment approaches
Reduced Quantity Reduced Function
MacDonald et al. Pediatr Drugs 2007;9:1-10; Zielenski. Respiration 2000;67:117-33; Welsh et al. Cystic fibrosis In: Valle et al, eds. OMMBID. McGraw-Hill Companies Inc;2004:part 21,chap 201; O’Sullivan et al. Lancet 2009;373:1891-1904
Class I Class II Class V Class III Class IV
Little to noCFTR GatingSome
CFTR ConductanceNormal CFTR quantity
and function
Correctors PotentiatorsTreatment
approaches
ARS Question
Once a patient is on the appropriate CFTR modulator, the following treatments may be discontinued:
a. Pancreatic enzymes
b. CF vitamins
c. Chest physical therapy
d. All of the above
e. None of the above
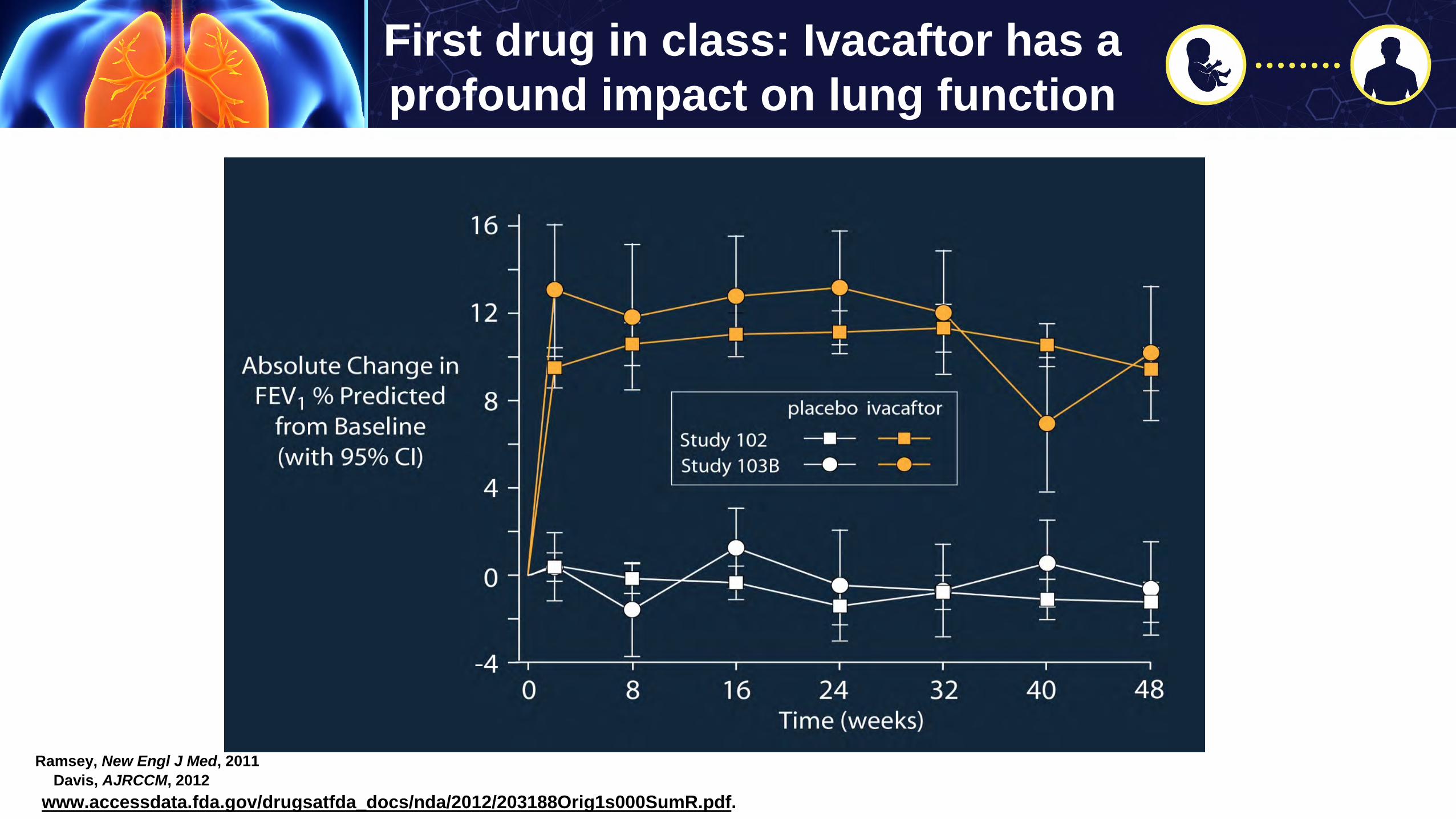
First drug in class: Ivacaftor has a profound impact on lung function
ttp://www.accessdata.fda.gov/drugsatfda_docs/nda/2012/203188Orig1s000SumR.pdf.
Ramsey, New Engl J Med, 2011J Davis, AJRCCM, 2012
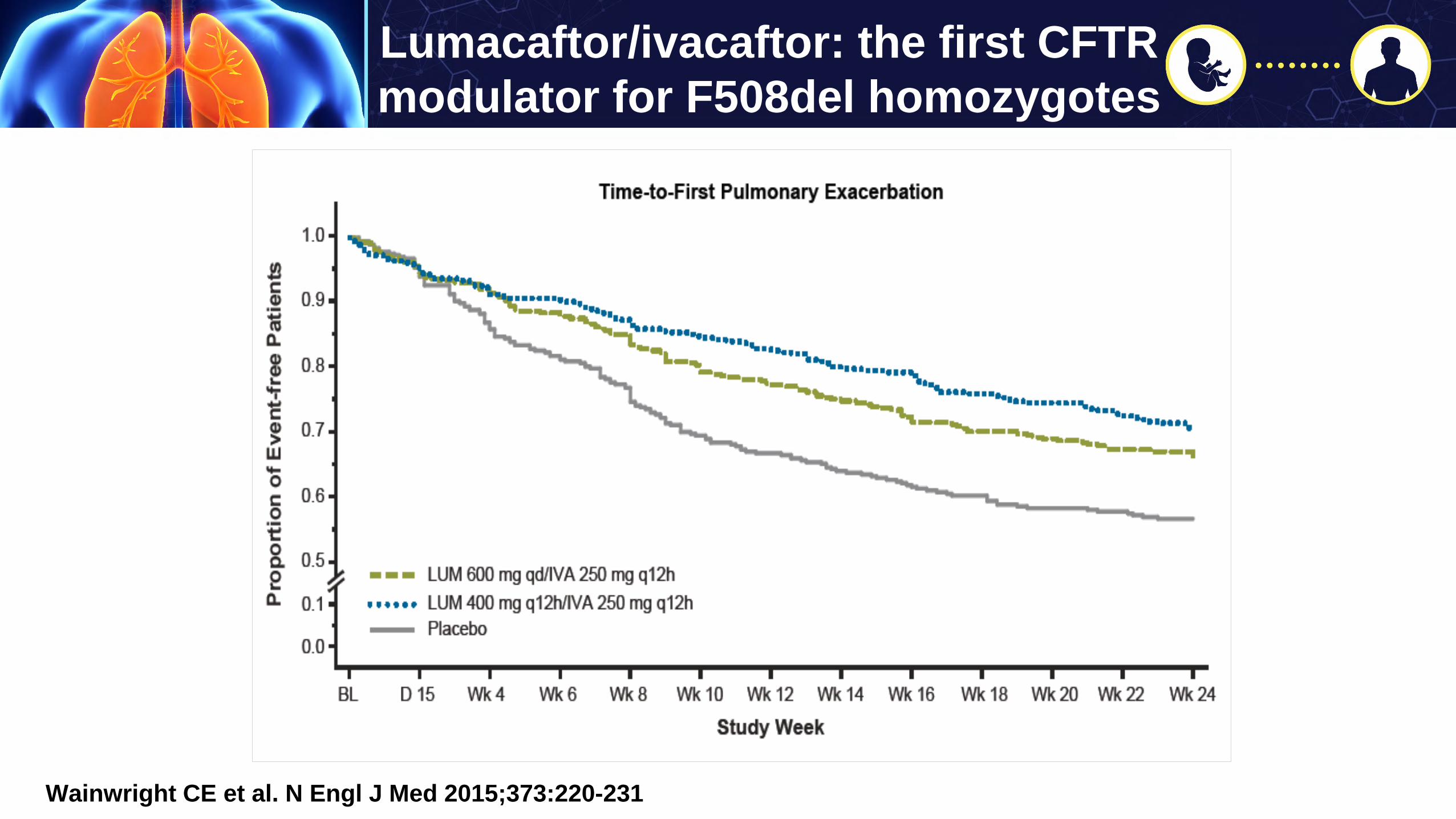
Lumacaftor/ivacaftor: the first CFTR modulator for F508del homozygotes
Wainwright CE et al. N Engl J Med 2015;373:220-231
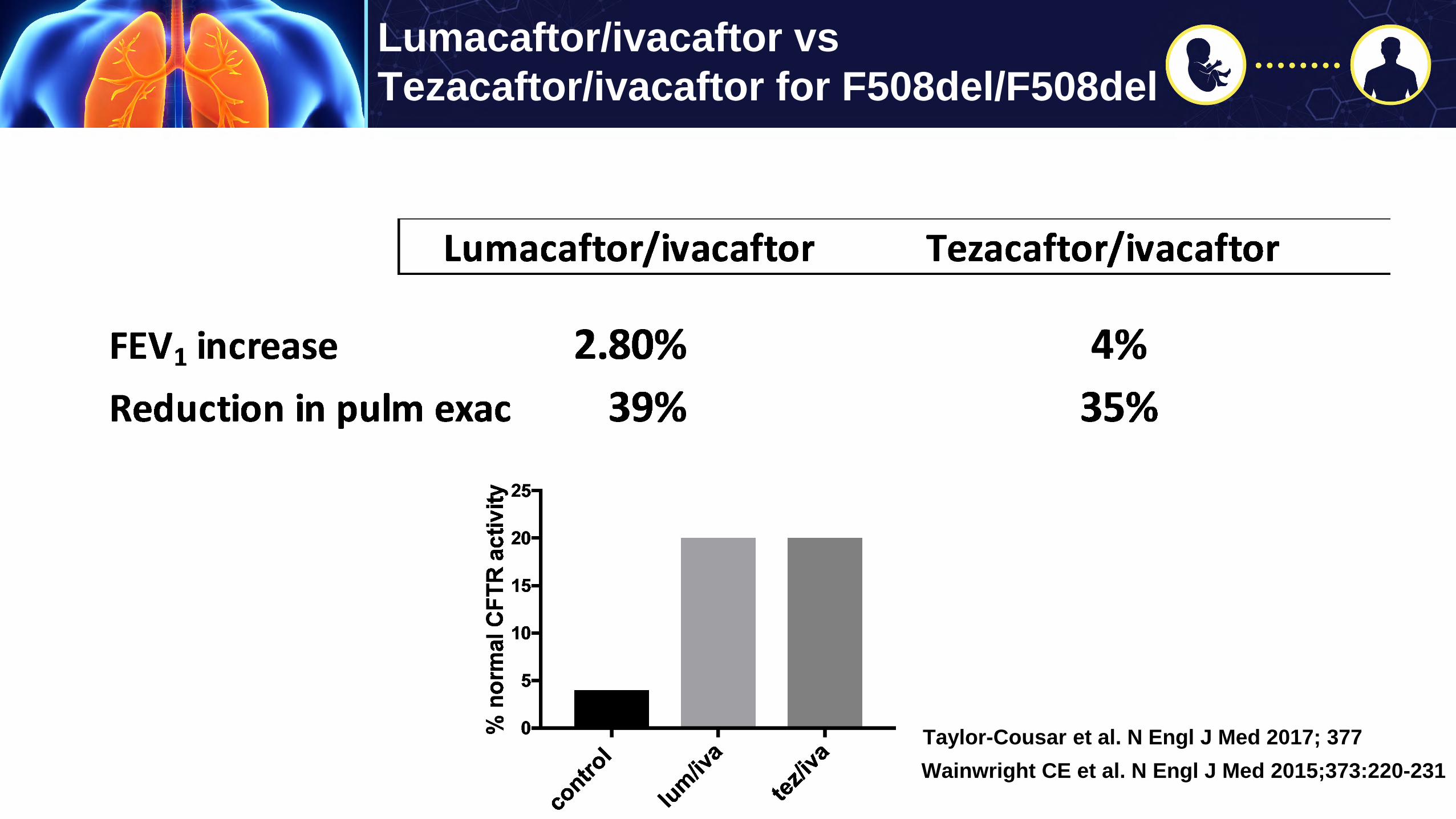
Lumacaftor/ivacaftor vsTezacaftor/ivacaftor for F508del/F508del
Wainwright CE et al. N Engl J Med 2015;373:220-231Taylor-Cousar et al. N Engl J Med 2017; 377

Are there other patients with CF who may benefit from CFTR correction?

38 Mutations approved for treatment with Ivacaftor
Ivacaftor
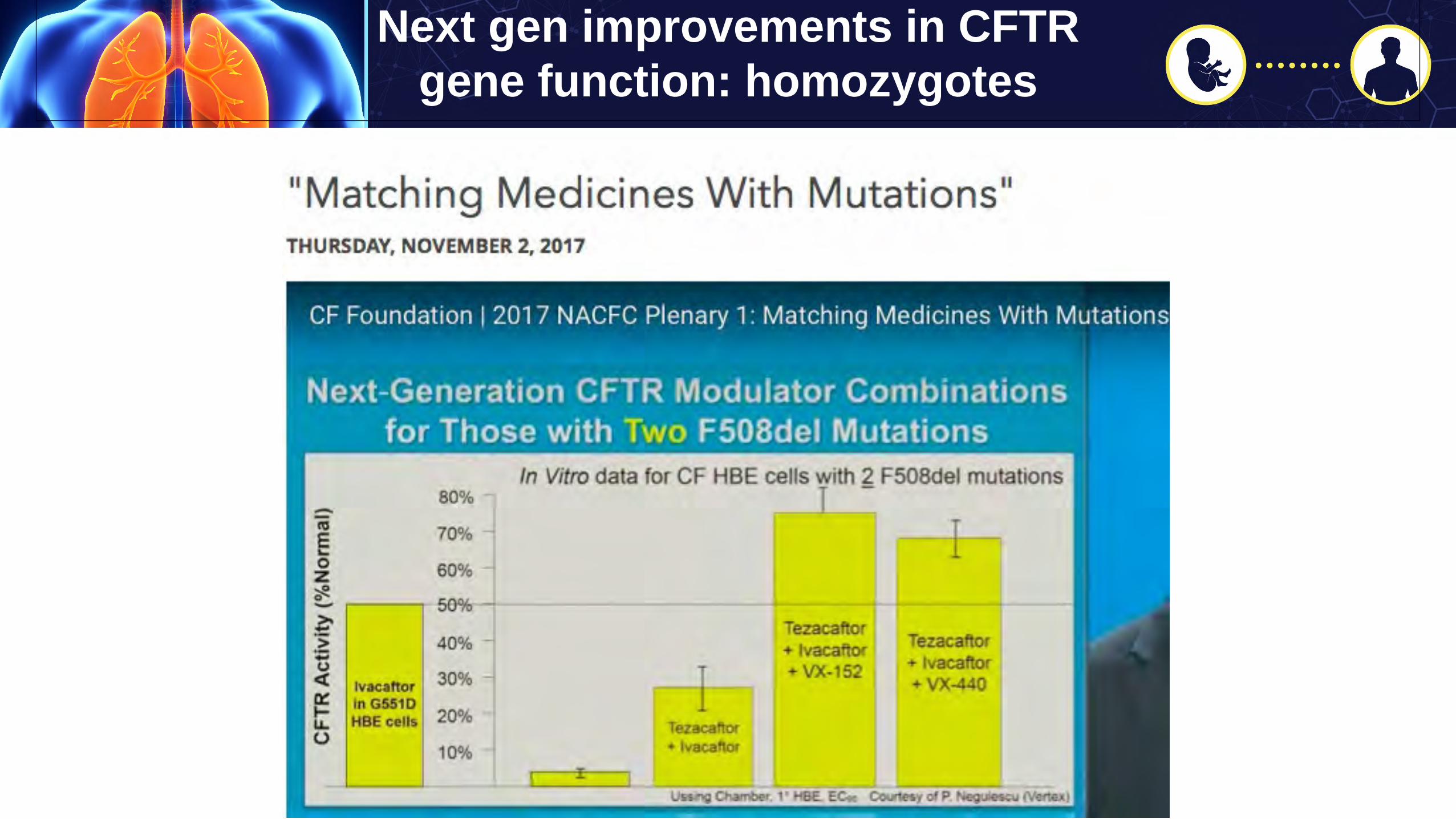
Next gen improvements in CFTR gene function: homozygotes

Next gen improvements in CFTR gene function: het min

93% of CF patients will be on treatment with highly effective
modulatory therapy
By 2020