1 transfusion medicine everything a medical oncologist should know about blood jeannie callum, md,...
TRANSCRIPT

1
Transfusion Medicine
Everything a Medical Oncologist should know about blood
Jeannie Callum, MD, FRCPC, CTBSDirector Of Transfusion MedicineAssociate Professor, University of Toronto

Which of the following is true about premedication?
A. Results in a 50% reduction in FNHTRB. Results in a 50% reduction in urticarial
reactionsC. Only prevents reactions from platelet
transfusionsD. Is of no value in preventing both FNHTR
and urticarial reactionsE. Should be administered to all patients
after the first transfusion reaction
2

Which of the following are true regarding platelet transfusions?A. Administered as pools of 5 unitsB. The total volume per pool of
platelets is 200 mLC. All apheresis donors are maleD. ABO compatibility is not important
for platelet transfusionsE. Indicated for prophylaxis if the
platelet count is below 20
3

Which of the following is an appropriate indication for plasma?A. A non-bleeding patient with an INR of
13 from warfarinB. A patient booked for lymph node
biopsy with an INR of 1.57C. A patient with a GI bleed and an INR
of 1.4D. A patient needing emergency
surgery for ICH on warfarin INR 3.2E. None of the above
4
5
The Medical School Basics
What you should already know
This should be a review

6
ABO and Rh D Grouping
There are four major ABO blood groups: O, A, B and AB
All recipients are also tested for Rh D: Rh D Positive or Rh D Negative

7
O
AB
BA
RBC Compatibility
Universal Donor
Universal Recipient

8
O
AB
BA
Plasma Compatibility
Universal Donor
Universal Recipient

Platelets
There is no such thing as a universal donor
We try for ABO-identical always but 30% of the time we can’t due to supply issues
Platelet incompatibility for A or B results in poorer increments and reduced plt survival
Plasma incompatibility can RARELY cause life-threatening ABO mediated hemolysis
9

10
Blood Grouping
Rh D not detectedA & B not detected Anti-A & Anti-Bpresent
11
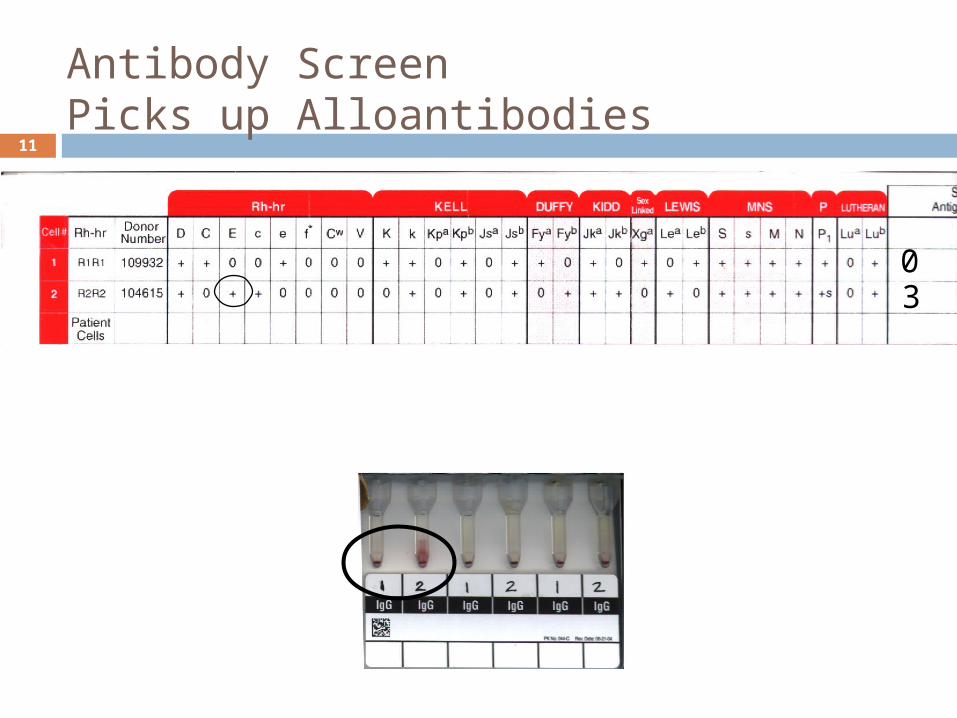
Antibody ScreenPicks up Alloantibodies
03

12
RBC Panel – Identify the antibody(s)
00400400000

13
RBC Panel – Identify the antibody(s)
00400400000

14
Crossmatch - 3 kinds
Electronic Crossmatch: 2 minutes patient blood group tested twice, unit ABO retested,
and antibody screen negative the computer does the final ABO check only
Immediate Spin: 10 minutes patient plasma and donor red cells mixed for final ABO
check only
Full antiglobulin Crossmatch: 45 min patient plasma, donor red cells, and anti-IgG checks for compatibility for all red cell antigens only used for patients with red cell alloantibodies

15
What are we going to cover?Hemovigilance dataInfectious risk updateNon-viral transfusion complications
Indications for components RBC, PLT, FFP

2001-2009Serious Reactions (n = 142 including 14 deaths)
15
3
46
34
6 6
16
2 1
13
05
101520253035404550
[1]
[10]
[1] [1]
[1]

17
HIVHIV
HCVHCV

18
Transfusion Transmitted Injury Surveillance System (TTISS) Canada’s National hemovigilance system Modeled on the French system You must report every transfusion
reaction to the hospital blood bank, including: Minor – including urticarial/febrile reactions Serious - obviously Circulatory overload

19
What are we going to cover?Hemovigilance dataInfectious risk updateNon-viral transfusion complications
Indications for components RBC, PLT, FFP

20
CBS disease prevention strategy HIV Ab, HIV NAT (minipool) HCV Ab, HCV NAT (minipool) HBsAg, HBcAb, HBV NAT (minipool) Syphilis HTLV-1/2 Ab WNV NAT (minipool) CMV Ab (selective inventory) Bacterial culture Parvovirus B19 (Fractionated products only) Leukoreduction Diversion pouch/arm cleaning Chagas’ testing Deferral of all female apheresis donors

21
HIV 1 in 7.8 million
Hepatitis C 1 in 2.3 million
Hepatitis B 1 in 153,000
HTLV 1 in 4.3 million
O’Brien et al. Transfusion 2007;47:316-325.
Residual viral risks

22
Year Emerging Pathogen
1995 HGV
1996 vCJD
1997 TTV
1999 WNV
2001 Monkeypox
2002 Chagas
2003 SARS
2004 Avian Flu
2005 Simian Foamy Virus
2006 Chikungunya
2007 HHV-8
2008 Dengue virus
2009 Plasmodium knowlesi
2010 XMRV

23
What are we going to cover?Hemovigilance dataInfectious risk updateNon-viral transfusion complications
Indications for components RBC, PLT, FFP

LitigationLitigation
PreventabPreventablele
MeasuraMeasurableble
HAZARDS OF TRANSFUSION
ARDSARDS
MOFMOF
ThrombosThrombosisis
TRIMTRIMCMVCMV
FeveFeverr
Allergic Allergic ReactionsReactions
AnaphylactAnaphylactoid oid
ReactionsReactions TRALITRALI
Transfusion Transfusion 1:1 Causation1:1 Causation
Transfusion Transfusion as risk factoras risk factor
Transfusion 1:1 Transfusion 1:1 Causation + other Causation + other
factor/sfactor/s
GVHDGVHD
CompatibilityCompatibility
HIVHIV
HepatitiHepatitissEndotoxaemiEndotoxaemi
a a
Technical Technical errorerror
UNIFACTORIALUNIFACTORIAL
DefiniteDefiniteOLIGOFACTORIAOLIGOFACTORIA
LL
ProbableProbable
MULTIFACTORIAMULTIFACTORIALL
PossiblePossible

Minor reactions to expect
Most common cause ofdeath from transfusion
Sepsis
Most common causeof morbidity
Other infectious risks(Risk of vCJD if patient expected to live >15-30 years)
26
Case
37F, healthy, G3P3 MVC head on collison – 78/50 on scene ER
CT abdo revealed active liver bleed 2 units of blood in ER -> 114/80, P84
OR laparotomy: splenic lac, liver lac, IM nail Rt
femur 6 RBCs, 4 FFP
27
ER CXR

28
Post-op
CRCU on admission, extubated 98/64, P98, SaO2 100% 2L nasal prongs Hgb 116, Plt 95, WBC 9.6, INR 1.33
POD 1 uneventful with plan to d/c to floor Hgb 93, Plt 68, INR 1.2, not bleeding 5 units platelets that afternoon 2 hours post transfusion develops dry
cough by 2400 intubation required for hypoxia

29
Post-transfusion

30
TRALI - Presentation
All ages – premature neonates to elderly Dyspnea Cough Hypoxia Fever Hypertension/Hypotension Leukopenia ++ secretions from the endotracheal
tube Normal BNP (pre to post correlation)

31
Leukopenia
0
2
4
6
8
10
12
14
16
0 1 2 3 4 5 6 7 8 9 10 11 12
Time (Days)
x10^9/L
WBC count
Neutrophils
Lymphocytes
Monocytes
RBC
Total white cell and differential counts.

32
TRALI - Presentation
Popovsky & Moore - Transfusion 1985 First case series of 36 patients from the Mayo
Clinic with TRALI over a 2 year period 72% required mechanical ventilation All <6 hours from end of transfusion Bilateral infiltrates in all patients Rapid resolution <96 hours in 81% Mortality 6% No long-term sequelae

33
Definition - Probable TRALITRALI Consensus Conference No prior acute
lung injury &
New ALI within 6 hours of transfusion &
No other risk factors for ALI
Acute lung injury = Acute onset PaO2/FiO2 <300 or
saturation <90% on room air
Bilateral lung infiltrates
No evidence of circulatory overload
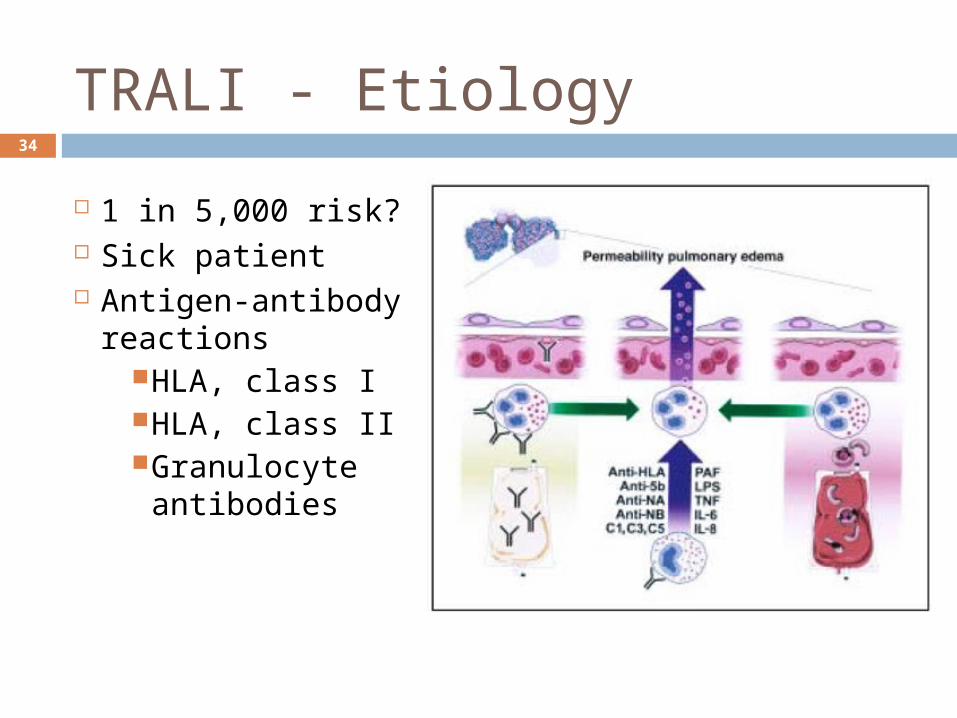
34
1 in 5,000 risk? Sick patient Antigen-
antibody reactions
HLA, class IHLA, class IIGranulocyte antibodies
TRALI - Etiology

35
Kopko et al., JAMA 2002; 287: 1968-71 Female donor implicated in a fatal TRALI
case (anti-5b) 290 donations in a 10 year period Lookback investigation on 36 of 50
transfusions (14 charts unavailable) over 2 year period
15 were associated with hypoxic transfusion reactions, and of these 8 were severe enough to require mechanical ventilation
Transfusion Related Acute Lung Injury Under-recognition & Under-reporting

36
TRALI - Management
MANAGEMENT Supportive care 80% recover in <4 days (compares to 50-60%
mortality from ARDS)
PREVENTION Reporting & donor deferral Female-free plasma products RBCs 2 mL plasma Apheresis platelet/plasma donors = male only

37
TRALI FatalitiesHolness et al. TMR 2004; July
TRALI fatalities reported to FDA (USA) Jan 1997 - Jul 2002 - 58 TRALI of 416
(14%) fatalities in USA FFP most frequently implicated
product (>RBC>PLT>cryoprecipitate) 83% positive for anti-HLA or anti-PMN
antibodies 75% of donors female

38
Ladies first, what next?Wright SE, et al. CCM 2008; 36: 1796-802
211 patients undergoing open repair of a ruptured abdominal aortic aneurysm between 1998 and 2006
Less ALI following the change to male fresh frozen plasma (36% before vs. 21% after, p = .04)
At 6 hrs after surgery, fewer patients were hypoxic (87% before vs. 62% after, p < .01)
Change to male plasma was associated with a decreased risk of developing ALI (odds ratio 0.39; 95% CI, 0.16-0.90)

39
TRIM – Transfusion-related immunomodulationReal or imagined? Retrospective series have found an
association of transfusion with many bad outcomes: Pneumonia Blood stream infections Multiorgan failure Death Thrombosis Tumour recurrence

Death and TransfusionMarik & Corwin. CCM 2008; 36: 2667-74.

ARDS and TransfusionMarik & Corwin. CCM 2008; 36: 2667-74.

Infection and TransfusionMarik & Corwin. CCM 2008; 36: 2667-74.

43
How / why might transfusions cause harm?
2,3 DPG depletion RBC deformity and
deformability loss aberrant RBC –
endothelial cell adhesivity
NO scavenging vasoconstriction,
platelet aggregation supernatant changes
inflammatory mediators

44
Nitric Oxide Binding & SNO-Hb
free Hb scavenges NO
SNO-Hb-depletion reduces delivery of NO from RBCs under hypoxic conditions

45
CaseCase
37 year woman with cervical cancer Presents to a peripheral hospital ER with SOBOE Hemoglobin 67 g/L She is transfused 4 RBC over 4 hours At the end of the fourth unit the patient
develops light headedness, back pain and has hematuria
Patient told that ‘red urine’ is common after transfusion and is sent home
Feels very unwell at home and family brings patient to Sunnybrook ER

46
Transfusion error ratesTransfusion Error Reporting System
Location Rate Denominator
Operating room 1 in 32 18,203
Emergency 1 in 46 6,829
Intensive care 1 in 71 30,546
Medical/surgical ward 1 in 99 36,546
Out patients 1 in 134 669
Out patient procedures
1 in 341 32,690
Obstetrics 1 in 1,369 1,369

47
What causes acute hemolytic transfusion reactions? ABO mistake
Usually group O patient given non group O
anti-A and anti-B are naturally occurring antibodies and hemolysis is immediate
Non-ABO antibody Either due to the use of emergency
‘uncrossmatched’ blood or antibody not detected on antibody screen

48
CaseCase
39 year old man AML, platelet count 9 x 109/L, tongue edema NYD, for ‘elective’ intubation in OR transfused with 5 units of platelets over 10 minutes
immediately before intubation within minutes - sBP <70 mmHg, HR 150, ST
depression Taken post-op to CRCU – temp 41C Blood cultures taken 1 hr, 4 hrs, 8 hrs post-op Serratia
marcescens despite iv cipro & tobramycin Patient expires at 18 hrs of septic shock 20 days later severe ‘febrile’ reaction to red blood
cells at a peripheral hospital – all other components recalled – including 1/5 above PLT

49
Platelets - Beware

50
BACTERIALCONTAMINATION
INCIDENCE Risk of septic shock:
1 in 10,000 PLT pools 1 in 100,000 RBC
Risk of death from septic shock: 1 in 40,000 PLT pools 1in 1,000,000 RBC
Key Message – Run PLT slowly for the first 15 minutes

51
BACTERIAL CONTAMINATIONETIOLOGY donor bacteremia, skin plug, processing Most common organisms
Yersinia enterocolitica Serratia marcescens/liquefaciens Staph aureus/epidermidis
PRESENTATION fever, rigors, hypotension, renal failure,
DIC PLT more common; RBC more severe

52

53
Bacterial Sepsis Prevention - Canada Donor history Donor vitals Optimal skin cleaning with 2
agents (timed) 40 mL diversion pouch Bacterial culture of all platelets Refrigeration Don’t leave RBCs out of the
fridge!
54

55
What are we going to cover?Hemovigilance dataInfectious risk updateNon-viral transfusion complications
Indications for components RBC, PLT, FFP

Basics
RBCs in non-bleeding, non-urgent situations are ordered 1 at a time 2 units okay if topping up for d/c for chronically
transfused to buy time till they need an outpt transfusion appt
PLT are ordered as POOLS There are no longer any sets of 5 or 6
FFP should be ordered as 15 ml/kg 2 units FFP is a completely inappropriate order
NEVER order pre-medication unless at least 2 episodes of FNHTR or urticaria
56
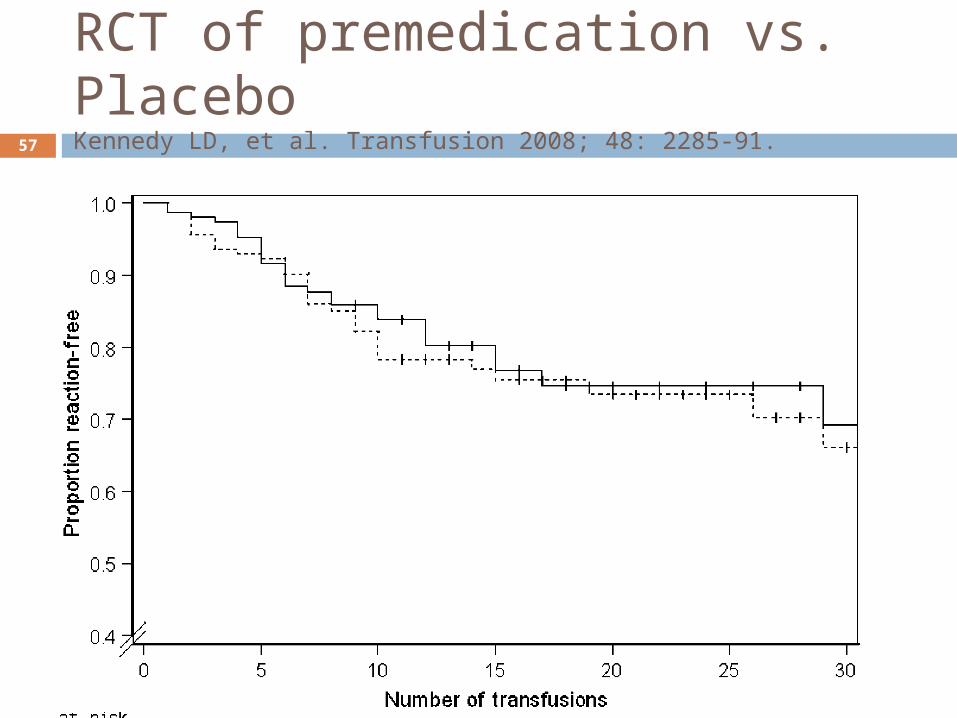
RCT of premedication vs. PlaceboKennedy LD, et al. Transfusion 2008; 48: 2285-91.57

58
RBC - TRICC Study
NEJM 1999; 340:409-17 - Hebert et al n=838 non-bleeding, ICU patients, Hb <90 g/L RCT - transfusion Hb <70 vs 100 Stratified by APACHE 2 score Those who were not enrolled were:
Older (mean age, 58 vs. 59) Less cardiac disease (26 vs. 20%)
Groups equal with respect to baseline characteristics Classic patient: 58 year old male, with 1-2 organ
failure, mechanically vented, admitted to the ICU from the OR
59
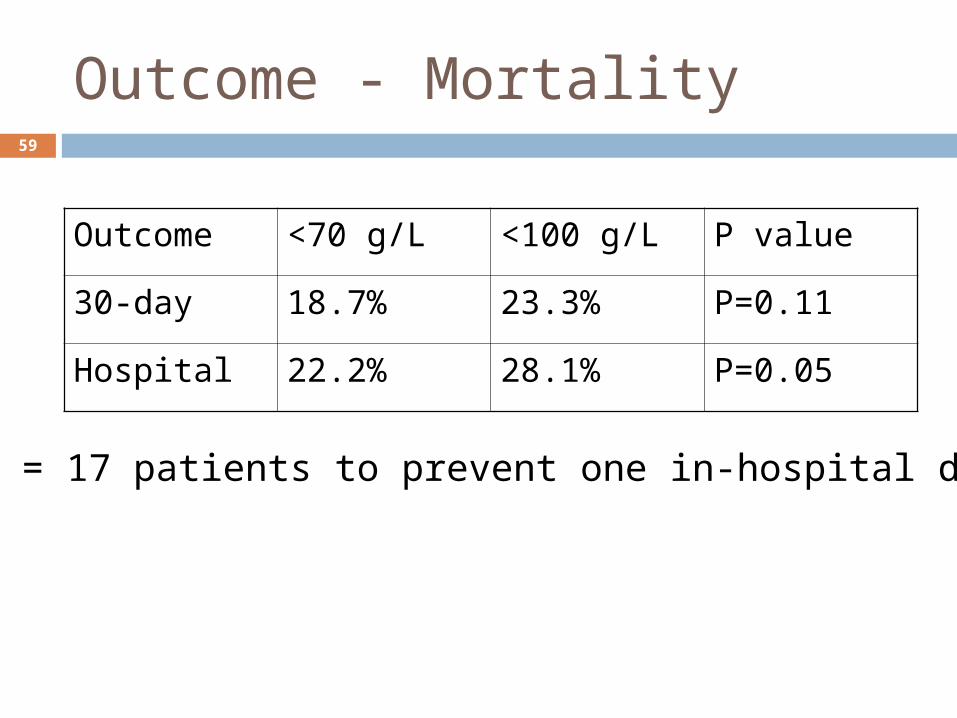
Outcome - Mortality
Outcome <70 g/L <100 g/L P value
30-day 18.7% 23.3% P=0.11
Hospital 22.2% 28.1% P=0.05
NNT = 17 patients to prevent one in-hospital death

60
What seemed to harm the patients in the liberal transfusion group?
Complication <70 <100 P value
Cardiac (all) 13% 21% <0.01
MI 0.7% 2.9% 0.02
CHF 5.3% 10.7% <0.01
ARDS 7.7% 11.4% 0.06

61
Survival to 30 days – All patients

62
All ‘cardiovascular’ patients (n=357)

63
FOCUS Study
1300 Fractured hip patients, over age 50 (median age 82 years)
Hemoglobin <100 g/L Randomized to 1 unit for <100
vs <80 g/L Primary outcome:
Ability to walk 10 feet at 60 days Secondary outcomes:
MI/stroke, death, functional status at 30 & 60 days
NO DIFFERENCES FOUND!
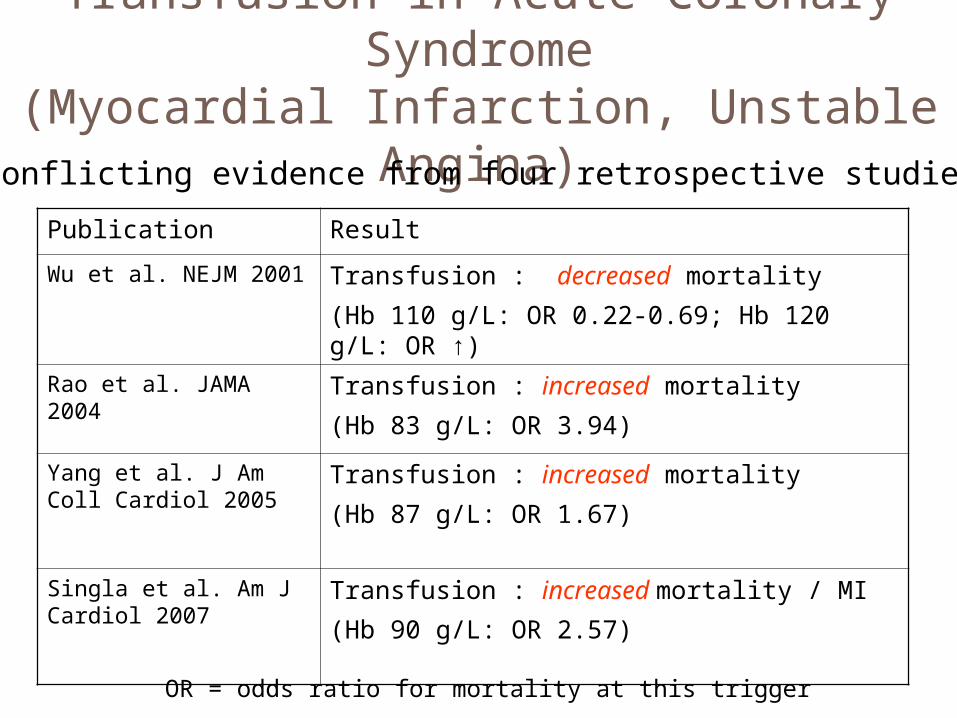
Transfusion in Acute Coronary Syndrome
(Myocardial Infarction, Unstable Angina)
Publication Result
Wu et al. NEJM 2001 Transfusion : decreased mortality
(Hb 110 g/L: OR 0.22-0.69; Hb 120 g/L: OR ↑)
Rao et al. JAMA 2004 Transfusion : increased mortality
(Hb 83 g/L: OR 3.94)
Yang et al. J Am Coll Cardiol 2005
Transfusion : increased mortality
(Hb 87 g/L: OR 1.67)
Singla et al. Am J Cardiol 2007
Transfusion : increased mortality / MI
(Hb 90 g/L: OR 2.57)
Conflicting evidence from four retrospective studies…
OR = odds ratio for mortality at this trigger

Keep in mind it might be bleeding that kills you and not the bloodCirculation. 2006;114:774-782

66
Bottom line for ACS/AMI patients We don’t know when to transfuse Probably ok with hemoglobin <80 g/L Hemodynamic instability is part of the
problem Don’t use an arbitrary hemoglobin level Stop transfusing when the patient is no
longer symptomatic (ie. no chest pain, no tachycardia) even if hemoglobin less than 100 g/L
Transfuse to a maximum of 100 g/L

67
FFPAmerican Society of Anesthesiologists Task Force on Blood Component Therapy. Anesthesiology 1996; 84: 732-47.
The dose is: 15 ml/kg (approximately 3-5 U per adult patient)
Indications: Significant bleeding with PT/PTT
more than 1.5 times normal Microvascular bleeding, massive
transfusion, AND patient’s clinical status precludes waiting for laboratory test results

68
Penalty AvoidanceDon’t do this...
Bleeding and INR <1.5 Procedure and INR <1.5 Massive transfusion and
you’re caught not knowing what the INR/PTT is
INR>1.5 but the patient is not actively bleeding
Warfarin reversal Heparin/LMWH reversal “2 units” = 33 kg patient Elevated PTT alone

69
An INR of 1.5 is indistinguishable from 1.7
A physician is very comfortable doing a renal biopsy an INR of 1.49 but requires plasma for an INR of 1.51
This is utter insanity! The INR can not have such a strict cut-off
I will show you why There has to be some thought built into
the interpretation of the INR

70
% coagulation Factors
50 %
30 %
100 %
INR 1 1.7 2.0 2.2 3.01.3
zone of normalhemostasis
zone of anticoagulation
15 ml/kg FFP
60 ml/kg FFP = 4 L FFP

71
Pre-FFP INR 1.3-1.8
Abdel-Wahab OI, et al. Transfusion 2006; 46: 1279-85
The INR of FFP is 1.2-1.4

72
iv vitamin K works much faster than oral
Gentle nudge back to 2-32 mg po
Emergency10 mg iv
Door #1 Door #2

73
RCT iv vs. poArch Intern Med. 2003 Nov 10;163(20):2469-73
• INR of 6-10 (n = 47) received either 0.5 mg iv or 2.5 mg oral
• IV more rapid at 6 hrs (11/24 vs 0/23) & at 12 hrs (16/24 vs 8/23)
• Patients in the intravenous group tended to be more often overcorrected (INR<2)

74
Oral Vitamin K for emergency reversalA common error that results in
delay in cessation of bleeding and getting a patient to a necessary
procedure
Note: If you have a patient with an elevated INR/PTT – you must figure
out why!
75
Prothrombin complex concentrates2,7,9,10 & Protein C/S
INR <3 = 1,000 IUINR >3 (or >90 kg) = 2,000 IU
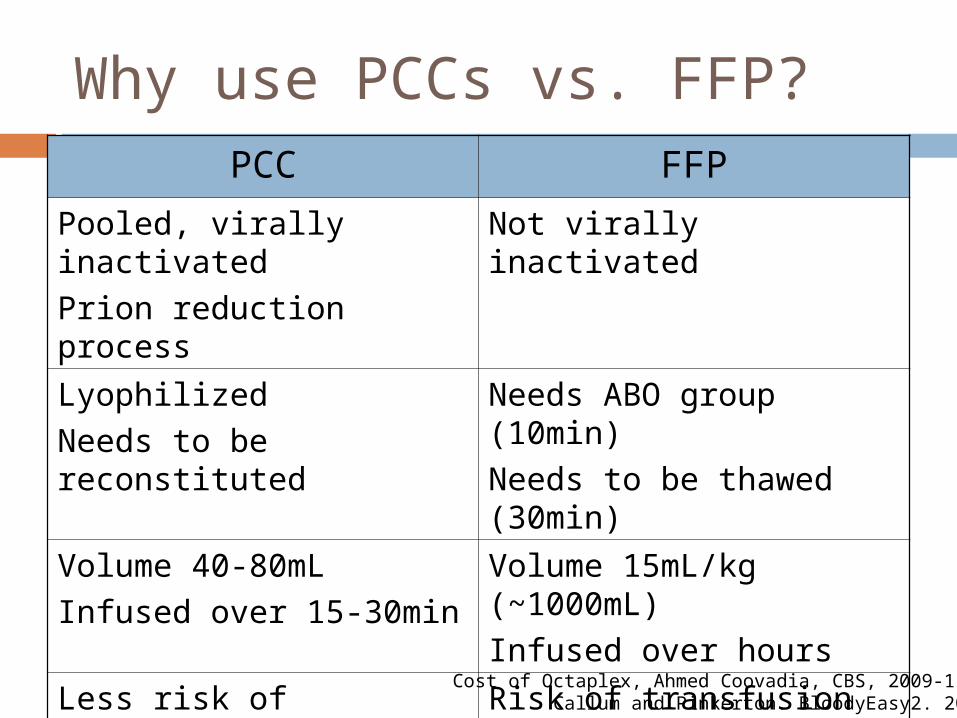
Why use PCCs vs. FFP?PCC FFP
Pooled, virally inactivated
Prion reduction process
Not virally inactivated
Lyophilized
Needs to be reconstituted
Needs ABO group (10min)
Needs to be thawed (30min)
Volume 40-80mL
Infused over 15-30min
Volume 15mL/kg (~1000mL)
Infused over hours
Less risk of transfusion rxns Risk of transfusion rxns: TRALI, TACO, anaphylaxis
$1150 for 1000 units1 $1050 for 6 units plasma2
Cost of Octaplex, Ahmed Coovadia, CBS, 2009-11-16Callum and Pinkerton. BloodyEasy2. 2005.

Why use PCCs vs. FFP?PCC FFP
Pooled, virally inactivated
Prion reduction process
Not virally inactivated
Lyophilized
Needs to be reconstituted
Needs ABO group (10min)
Needs to be thawed (30min)
Volume 40-80mL
Infused over 15-30min
Volume 15mL/kg (~1000mL)
Infused over hours
Less risk of transfusion rxns Risk of transfusion rxns: TRALI, TACO, anaphylaxis
$1150 for 1000 units $1050 for 6 units plasma
Only lasts 6-8 hours

78
The European ExperienceJ Thromb Haemost 2008; 6: 622-31

79
Platelets

80
XY
Buffy coat platelet pool
XY or XX

81
PLT CLINICAL SETTING SUGGEST<10 Immune thrombocytopenia Transfuse only with serious
bleeding<10 Thrombocytopenia (e.g. bone marrow
failure)Transfuse 1 pool
<50 Vaginal delivery or procedures notassociated with significant blood loss
1 pool of platelets on hold,transfuse only if seriousbleeding
<50 Periprocedure massive bleeding, majorsurgery, or pre invasive procedure
Transfuse 1 poolimmediately beforeprocedure
<100 Peri-neurosurgery Transfuse 1 pool<100 Head trauma Transfuse 1 poolAny Platelet dysfunction and marked bleeding
(e.g. post cardiopulmonary bypass,aspirin, antiplatelet agents)
Transfuse 1 pool
Platelet Indications

RCT – 20 vs. 10Rubella et al. NEJM 1997; 337:1870-5
82

Pre-transfusion triggersB Cameron et al, Transfusion 2007; 47: 206-11
83

84

Platelet Refractoriness1 hour post platelet count is <15 Is it non-immune refractoriness?
Hypersplenism Drug-related Fever DIC Infection
Is it immune refractoriness? ABO antibodies - match HLA antibodies - screen HPA antibodies - screen
85

You do not need to remember anything!
86

87
Thank You
Donate blood q56 days
Register for Stem cells