1 using root cause analysis to reduce hospital readmissions jennifer wieckowski, msg health services...
TRANSCRIPT

1
Using Root Cause Analysis to Reduce Hospital Readmissions
Jennifer Wieckowski, MSG
Health Services Advisory Group of California, Inc.
(HSAG-California)
2
Purpose of the Root Cause Analysis (RCA)
Identify the “root” cause of readmissions at your hospital.
Identify patterns of readmissions specific to your community and its providers.
Use RCA results to guide targeting criteria and intervention selection.

3
Community Based Care Transitions Program (CCTP) Application
Describe the results of the RCA that was performed.
Describe how the results informed the selection of the proposed intervention and target population.
Describe your implementation strategy.

4
National Coordinating Center http://www.cfmc.org/caretransitions/toolkit.htm

5
Common Application Errors
The community-specific RCA is missing. The community-specific RCA is present, but
not explicitly tied to the methodology for targeting high-risk beneficiaries and the proposed interventions.

6
Using RCA to Drive Intervention Selection—Good Example

7
Using RCA to Drive Intervention Selection—Poor Example

8
Using RCA to Drive Intervention Selection—Good Example

9
Variety of RCA Tools
Patient/family interviews Care coordinator interviews Medical record reviews Process mapping Cause-and-effect diagrams “5 Whys”

10
Patient/Family Interviews
Semi-structured telephone or face-to-face interviews with patients who were readmitted
Helps to identify opportunities for improvement from the patient’s perspective

11
Care Coordinator Interviews
Conduct individual and/or group interviews with care coordinators.
Identify patterns, trends, and opportunities for improvement from the staff member’s perspective.
Formulate groups across settings or within provider teams, organizations, or specialties.

12
Medical Record Reviews
Review randomly sampled hospital discharges and 30-day readmissions.
Common finding: – Patient education is completed and
documented, but patients need more in-depth understanding to be compliant.
13
Process Mapping
Observe discharge and admission processes directly, interview process owners, and map the processes.
Elicit staff perceptions about where communication issues and gaps may occur.
Clarify specific roles and contributions of those involved in the process.

14
Cause-and-Effect Diagram(Fishbone Diagram)
Visually illustrates potential causes of high readmissions
15
“5 Whys”
This is simple and easy to complete without statistical analysis.
Start with asking why readmissions occur at your hospital and record the answer. If the answer provided does not directly identify the root cause of your readmissions problem, ask why again and record the answer.
Continue this process until your team agrees the problem’s root cause has been identified.

16
“5 Whys” Example
17
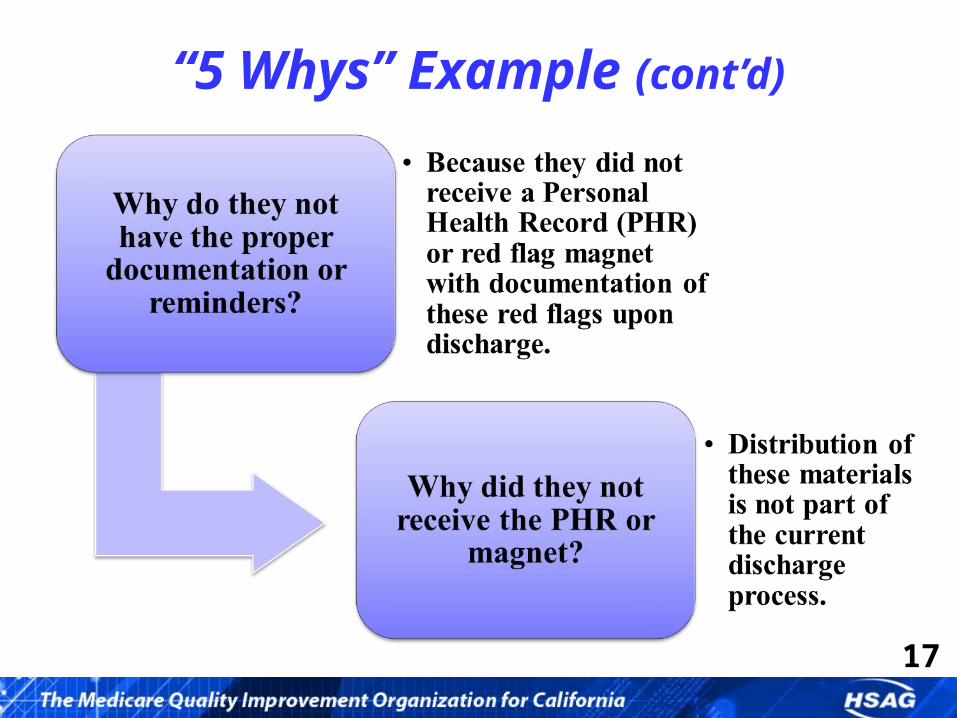
“5 Whys” Example (cont’d)

18
Results from Previous Care Transition RCAs
“Rocket science is helpful, but not required.”
19
Results from Previous Care Transition RCAs (cont’d)
RCAs revealed remarkably consistent results. Patients experienced readmissions because of:
– Unmanaged worsening of their conditions.– The use of suboptimal medication regimens.– Returning to emergency departments instead of
accessing a different type of medical service.

20
Three Basic System Gaps
Lack of engagement or activation of patients and families
Lack of standard processes among providers for transferring patients– No medical responsibility
Ineffective or unreliable sharing of relevant clinical information

21
RCA Conclusion
Many of the evidence-based interventions to improve transitional care are directed at one or more of these gaps, but require cooperative activity by more than one provider.
All communities must build cross-setting or multi-provider relationships to deploy, measure, and revise implementation strategies.
Community building is the necessary groundwork to enable improvement.

22
For More Information
Mary Fermazin, MD, MPAChief Medical Officer, HSAG-California
Jennifer Wieckowski, MSGProgram Director, Care Transitions, HSAG-California
700 North Brand Blvd., Suite 370
Glendale, CA 91203
818-265-4650

23
www.hsag.comThis material was prepared by Health Services Advisory Group of California, Inc., the Medicare Quality
Improvement Organization for California, under contract with the Centers for Medicare & Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not
necessarily reflect CMS policy. Publication No. CA-10SOW-8.0-101311-01
We convene providers, practitioners, and patients to build and share knowledge, spread best practices, and achieve rapid, wide-scale
improvements in patient care; increases in population health; and decreases in health care
costs for all Americans.