19550504 nu shape-ag2030-04-med-1010-55-log 1955 … · supkeme headquarters allied powhts europe...
TRANSCRIPT
iPV \L\i
-1010/55 L O G
: •••' - : .• • i • . ,
> I" /.v v .>• ••• -• —• . ' . .. :
E1"^..!... -V
••I I
il
^ ^ v. .V •,-'v; "S-V-Z* S--C • 7. .:--7, -, V \
= W X v.; - V"'- " > ' •• ' •
1955
l i lS lSi l i i i l iS f '^^ÄPfe- • ' W i ^ f -M EDjlCA L : :
I - . - . v . - . • -.-. , •• . . - •• - • ' - - .. : • ' ..
| - r- • ... . " .-- , i - .,.
- ' * • t ' T" t '.V , , , 1* -, . . " ». ' - , ' •
• -i. 1 ' - < ''V V'-V" t: •
'A
•, I
•ter ^
If ' • * T ' • •' -J'ï*'-'; f-"1 r^ ' '•' " • '.••"",' '-4.4/ >'.7 ,- vJ' '' "
V.
•'J. 1..U *. ' .77.*
' ;
. 7 .,* •
' NATO CONFIDENTIAL I-':v;. .•• •••. . ï : :
• . 1 ' *-, • •' ", . •-f '' -- Z'.'; J,
1'- -, '-... : •''-:.--./,.- ,'...;
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
SUPKEME HEADQUARTERS ALLIED POWHtS EUROPE PARIS FRAMCE
AG 2O3O.04/MED-1010/55 LOG i7 October 1955
SUBJECT : SHAPE Medical Conference, k thru 7 May 1955
TO J See Distribution List
1, Herewith Minutes of the SHAPE Medical Conference, held at SHAPE on 4, 5, 6 and 7 May 1955.
2, Sufficient copies are forwarded to enable distribution to be mad« to all delegates who attended the Conference.
FOR THE SUPREME ALLIED COMMANDER EUROPE:
F.S* BE5SQN, JR. Major General, U.S. Army ACofS Logistics
DISTRIBU TIOM Ehglish ÎX2&S&
Director General, Belgian MiUtary Medical Services 5 10 1 Belgian Corps ~ 2
Director General, Canadian Aimy Medical Services 3 Director General, Medical Services, Royal
Canadian Air Force 3 -Director General, Medical Services, Royal Canadian Navy 3 Director General, Canadian Dental Services 1 Defence Research Board, Canada k Canadian Army Medical Liaison Officer, London 1 Radian Forces Medical Council 2 Canadian Joint Staff, London 2 Director General, Danish Joint Medical Services Ö Director 'General, Central Directorate,
French Military Medical Services 1 25 Ist French Army - 1 Ist French Army Corps - 1 2nd French Araiy Corps - 1 lere C.A.T.A.C. - 2 Director General, Italian Army Medical Services 2 3 Director General, Italian Air Force Medical Services 2 3 Director General, Italian Naval Medical Services 2 3 Chief, Luxembourg Army Medical Services 2 3 Director General, Netherlands Army and Air Force
Medical Services 7 Director General, Netherlands Naval Medical Services 3 1 Netherlands Corps 2 Director General, Joint Medical Services, Norway 9 Director of the Portugese Army Medical Services 2 U Surgeon General to the Turkish General Staff 6 9 Director General, Army Medical Services, U.K. 15 Director General, Naval Medical Services, U.K. 6 Director General, Medical Services, R.A.F., U.K. 6 Principal Medical Officer, Ministry of Defence, U.K. 3
L
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
DISTRIBUTION ( Continued) EhgUaft French
D.M.S., Northern Artqy Group 2 D.D.M.S,, 1 (CB) Corps 1 Surgecai General, Department of the Amy, U.S. 9 Surgeon General, Department of the Air Force, U.S. 9 Surgetm General, Department of the Navy, U.S. 9 Assistant Secretary of Defence (Health & Medicine) U.S. 10 Headquarters, USAFS JV Headquarters, USAREUR 4 Headquarters, 12th U.S. Air Force 2 2nd Tactical Air Force 3 CINCNELM 2
' COMNAVCENT 1 Chief, Medical Branch, HQ ACLANT 4 DCS/LOG, HQ AFCENT 3 2 Chief, Medical Branch, HQ AFNORTH 5 Chief, Medical Branch, HQ AFSOUTH 10 6 Chief, Medical Advisory Staff, HQ AIRCHJT 5 4 Chief, Medical Branch, HQ LANDCENT 7 4 Chief, Medical Section, AIRSOUTH 2 2 Medical Adviser to CINCAFMED 4 Southeastern Army Group 2 2 HQ 1 Canadian Infantry Brigade 2 Office of the Air Attache, U.S. Etabassy, Paris 1
SHAPE
DCLA 1 1 - SECY 2 1 SHAPE CENTRAL RECORDS 1 1 LOG DIV 40 40
120
French translation to follow.
2
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

NATO CONFIDENTIAL
SUPREME HEADQUARTERS
ALLIED POWERS EUROPE
1955 SHAPE
MEDICAL CONFERENCE
MINUTES
4, 5, 6 a 7 MAY 1955
TABLE OF CONTENTS (
FART I LIST OF REPRESENTATIVES ( I )TO(VI I )
PART H INDEX (VIII) TO (XVI)
RfcRT HT MINUTES 1 - 1 7 7
NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

LIST OF REPRESENTATIVES OF NATO NATIONS AND HEADQUARTERS OF COMPONENT FORCES OF ALLIED OOMMAND EUROPE IN ATTEN-DANCE AT THE FOURTH SHAPE MEDICAL CONFERENCE AT SHAPE.
PARIS. FRANCE. 6. 7 MAY 1955
(Represnntatives are_listed alphabetically by Mations)
BELGIUM
BOURDEAUXi H.O.M.J.
EVRARD, E.E.O.J.G.
GEUENS, F.L.
MAGE, J.
Major
Major
Belgian Medical Services
Director, Air Force Medical Services
Lt. Colonel Director General, Belgian Medical Services
Colonel Inspector General, Belgian Medical Services
CANADA
BROSSEAU, D.T.M.
CORBETT, A.A.G.
CRAWFORD, J.N.
HAY, H.B.
HUNTER, K.A.
L££f
McCHARLES, C.W.
McFARLANE, J.A.
VttKSBOROUGH, E.H.
Lt. Colonel
Air Ccoimodore
Brigadier
Wing
Commander
Brigadier
Surgeon Commodore
Dr.
Dr.
Brigadier
Can Army Medical Liaison Officer, London
Director General, Air Force Medical Services
Executive Staff Officer, Can Forces Medical Comcil
SOMS, Can Joint Staff, London
Director General, Army Medical Servicen
Director Generaljl Naval Medical Services
Senior Staff Officer (Medical), Defence Research Board
Chairmans Can Fore«? Medical Council
Director General, Dental Sen-ices
DENMARK
BRUN-PEDERSEN, M.
FASTING-HANSEM, C.R.H.
HEMPEL-JORGEMSEN, J.
Surgeon Chief, Danish Royal Naval Captain Medical Services
Major Director General, Danish General Joint Medical Services
Colonel Deputy Director, Danish Array Medical Services
Colonel Chief, Danish Air Force Medical Services
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
FRANCE
COLLIN, G.A.P.C.
DUVAL, B.A.M.
GALIACÏ, J.
GARBIES, R.E.L.
LABABTHE, P.E.
HONNIN, Ai
REILINGER, A.J.
SANTINItl P.
SIMON. R0F,A.
Colonel
Colonel
Rear Admiral
Major
Assistant Director General, (Army), of Military Medical Services
Chief G-Z of Military Medical Services *
Deputy Director General o£ Military Medical Servie*« (Navy)
V
Chief, Amy Sectioh of G3 of Military Medical Ser-vices
Brigadier Assistant Director General General of Military Medical Services
(Air)
Lt, Colonel Chief of Air Section of G3 of Military Medical Services
Major Director General, Military General Medical Services
Lt. Colonel Medical 4th.Bureau, French Anny,Headquarters
Captain Chief G4 of Military Medical Service*
(Officers attending specific periods only);
CHASSENDE-BAfiROZ, K«J»PiHt Fo
DUCHESNE, B.
FAVRE, R.G.J.
GENAUD, P.E.M.
LABORIT, H.L.M.
LIEUX, L.A.A.J.
PETITDatANGE, C.A,
Lt. Colonel Central Establishment of El ectro-Rad iolôgy
Captain Val'.de Grace Hospital, PAH-IS
Colonel Professor at Val de Grace Hospital, PARIS
Colonel Technical Section for Studies and Reiearch <f Military Medical Services
Lt. Technical Section for Commander Studies and Research of
Military Medical Services
Brigadier director of Supply and General Fabrication for Military
Medical Services
Colonel
( i i )
NATO CONFIDENTIAL
Deputy Director of Supply and Fabrication for Ittlltary Medical Services
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
ITALY
FERRI, G.
PERA, G.
RUTOLI4 0.
LUXEMBOURG
FELTEN, P.
NETHERLANDS
BORGELD, W.A.
BROEKHOFF, P.C.
BROUWER, J.E.
KRIJNHJ, J.J.
NEUBERGERfc. J-W.
STADELMANtJ von ESCHOLZMATT, J.H.
VAN DER GIESSEN, H.J.
NORWAY
DALE, T.
GREVE-BRUN, J.
NYBY, 0.
UDJUS, L.
PORTUGAL
de BETTENCOURT
General
Lt. General
Major General
Major
Surgeon Captain
Surgeon Rear Admiral
Brigadier General
Surgeon Lt. Colonel
Doctor
Lt. Colonel
Major General
Major General
Surgeon Comnodore
Colonel
Colonel
Colonel
Director General, ;.nny Medical Services
Director General, Air' Force Medical Services
Vice Director General, Army Medical Services
Chief, Array Medical Services
Representing Royal Nether-lands Naval Medical Service
Director, Royal Netherlands Naval Medical Services
Director, Royal Netherlands Air Force Medical Service
Represaiting Royal Nether-lands Army Medical Service
Consultant to M.O.D.
Logistics Division, Royal , Netherlands Anny Medical Service
Director General, Netherlands Army & Air Force Medical Ser-vice
Director General, Joint Norwegian Naval Medieal Services
Director General, Royal Norwegian Naval Medical Services
Director General, Rcyal Norwegian Air Force Medical Service
Director, Medical Services, Norwegian Army-
Director, Medical Services, Portugese Army
( i l l )
NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
TURKEY
GOGEN, H.V.
JCUNTOL, R.
YAKAL, F.
UNITED KINGDOM
CLARK, G.A.
CROSSE, J.H.J.
CRITCHLEYi J.A.
HARRIS, Sir Frederick
HIDE, F.A.C.
INGLEBY-MACKENZIE Sir Alexander
KILPATRICK, Sir James
KNIGHTj G.A.M.
MARKS, R.L.
MEDLANDil A.J.
MENECES, A.N.
NICHOLSON, C.B.
WYNN-PARRY, C.B.
UNITED STATES
ARMSTRONG, G.E.
ARMSTRONG, H,G,
BEDWELL, ToC.
BLOUNT, R.
Major Surgeon General, Turkish Army-General
Rear Surgeon General, Turkish Navy Admiral
Colonel Divisional Surgeon, Turkish Air Force
Dr. Principal Medical Officer, Ministry of Health
Colonel The War Office (Army Medical Directorate)
Captain Field Training School, RAMC
Lt. General Director General, Army Medical Services
Captain Field Training School, RAMC
Surgeon Vice Admiral
Medical Director General, Royal Naval Medical Services
Air Marshal
Director General, Medical Services, R.A.F.
Group Captain
Air Ministry (Medical Directorate)
Lt. Colonel
Field Training School, RAMC
Major Field Training School, RAMC
Colonel Field Training Centre, RAMC
Surgeon Captain
The Admiralty, (Medical Directorate)
Squadron Leader
The Air Ministry
Major The Surgeon General,' General United States Army
Major The Surgeon, USAFE General
Colonel Office of the Surgeon General, U.S.A.F.
Colonel Office of the Air Attache, U.S. Etabassy, Paris
(iv)
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
NATO CONFIDENTIAL
UNITED STATES (Continuod)
BROWNTON, S.S.
CUSHBfG, E.H.
HÛGAN, B.W.
MOLLIS, T.L.
OGLE, D.C.
ROURKE, A.J.J.
WINGO, B.W.
Colonel Staff Director (OASD), (Health and Medicine)
Dr. Deputy Assistant Secretary of Defence (Health & Medicine)
Rear Surgeon General* U.S. Nayy Admiral
Lt. (JG) Aide to the Surgecn General, U.S. Navy
Major Surgeon General* U.S. General Air Force
Dr. Member of the Advisory Council, OASDj (Health and Medicine)
Captain Office of the Surgeon General, U.S. Amy
CINCKORTH
DOUGLAS, J.P.
TURNER, E.V.
CINCSOUTH
BACH, S.A.
GARGAN, N.
FELOSI, E.
TURKAN, K.
CINCAPMED
MAT, R.C.
CINCENT
DICKSON, J.
CARROL, F.S,
MOREAU, G.J.C.
CINCtJEIM
ROSE, H.W.
Colonel Senior Medical Officer, AFNORTH
Lt. Staff Surgeon, CINCNORTH Colonel
Lt. Chief, Medical Branch, AFSOUTH Colonel
Brigadier Turkish Army General
Lt. Italian Air Force Colonel
Colonel Turkish Army
Surgeon Medical Adviser, C3NCAFMED Rear Admiral
Lt. Medical Adviser, HQ ALFCE Colonel
Lt. Surgeon, 7th U.S. Corps Colonel
Major French Army
Captain District Medical Officer, CINCNELM
(v)
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

SACLANT
VAN FEENEN, H.J.
FOLEY, S.R.
AIRCEMT
CELLARS, R.J.
USAFE
BYRNES, V.
NIELSEN, G.L.
USARHJR
MARTIN, J.I .
SEELEYp S.F.
NORTHERN ARMY GROUP
HALL, E.H.
1 (GB) Corpa
RICHARDSON, F.L.
SOUTHEAST ARMY GROUP
MAZARELLA, A.
MENGAt S.
STAVROPOULOS, M.
COMLANDCEflT
WILSON, W.L.
Iat French Aimy
BOLZINGER, R.F.L.
Iat French Army Corps
PALEOLOGUE, J.E.M.f:,
2nd French Army Corpa
ICABtT, F.B.M.
Captain Representing Medical Branch, 'HQ ACLANT
Ccmunander Representing Medical Branch, HQ ACLANT
Group Chief, Medical Advisory Staff, Captain AAFCE
Colonel Deputy Surgeon, HQ USAFE
Major USAFE
Major General
Surgeon, USAREUR
Brigadier Deputy Surgeon, USAREUR General
Major Director of Medical Services, General Northern Army Group
Brigadier D.D.M.S., 1 (GB) Corpa
Major
Major General
Italian Army
Turkish Army
Lt, Greeik Army Colonel
Brigadier Surgeon, 7th U.S. Army General
Colonel D.D.M.S., Ist„French Army
Colonel D.M.S., Ist French Army Corps
Colonel D.M.S.„ 2nd French Army Corps
(vi)
NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
12th U.S. Air Force
STRICKLAND, 6.A.
Iere CATAC
SENEGAS, R.
1 BELGIAN OORPS
CASTERS
1 NETHERLANDS CORPS
KOTKE
1 CDN INFANTRY BRIGADE
FITCH
2nd TAF
COflBETT, L.M.
2 Group
REDFERN, C.H.
Ô? Group
BAKWOOD, A.J.
Colonel Surgeon, 12th U.S. Air Fcrce
Colonel D.M.S., 1er« CATAC
Colonel D.D.M.S., 1 Belgian Orps
Lt. D.D.M.3., 1 Netherlands Colonel Corps
Lt. S.M.O., 1 Cdn Inf Bde Colonel
Air P.M.O., 2nd TAF Cotanodore
Wing S.M.O., 2 Group Ctmmander
Wing S.M.O., 83 Group Commander
SHAPE MEDICAL BRANCH
AHERN, T.M.R.
BARKER, C.C.
HALL, W.F.
NELSON, H*B.
PARENT, M.L.K.
STONE, E.G., Jr.
Colonel
Group Captain
U.K. Aray
RoAoP»
Brigadier U.S.A.F. (MC) General
Colonel U.S.A.F. (MSC)
Colonel FVw Army (MS)
Commander MC U.S.N.
(v i i )
NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

TAKti-TC QP QQNTgITS
FOURTH ANNCTAL SHAIS MEDICAL COKFERMCE 1 THRP 7 MAT 1955
FIRST DAJj 4 MAT 1955
Page Rtmibgr
General &:™enther ... .,, Opening Address ,. 1
General Hall » , ,<,« Introdii^Vjo. 2
Canmande:? 3ton« , ... „.e ABC Df^&iœ gaining .. ... .., 3
Colonel Mage . . . . <><.. <..o Discussion <>... . . . . . . . . . , . . 8
GmeraS, Dale 0 0 0 . .„„ .„<, Discussion ..t>. ... ... ... ... S
General Ferri ... . 0. ..<, Dls^ussioa ..«».... «•• 8
GaieralHalI ,.. ... Discussion .,, ... .... ,., ... 10
General Gog«o. t»« o«. oo. Dis^aissiai ... ,,» .... .,. ... 11
G'W.eral. G 0E 0 ArmstroDg Treafaaent of Bunas in
Ancrai*; Disaster ,<, »<>.. ••• ••• 11
MajorFeH-^an . . . « c Discussicr. . . . . . . . . . . . . . IS
CaaaanderLatiorit .<>« « « . Disaissioc. ... .... ... ••• 18
General Hall <«•< ••• <><,<> Discission .,, ... .... ••• ... 20
S '/L Hpnn^Parry ,0 ot,0 „<• Etfaafcllit a!;* a* is. ths B.A.F...» 21
pen'i ... D<« Disaisaiati .. ... «... 25
SEOQKD D M , 5 MAÏ 1955
General Brisa,*; .. ,,n Opening Aâd-'.'sas .. .... ... ... 26
General a... o«» Discussion a a .... ••• 27
Lt. Colctiel Bynaes .. Retinal Affects of Atomic Flash 27 Colonel Bash ...» ,.1 Di s w l a aion ... 52 tfflnCti'&l fiftitk tooft ooo to)
C"?I<mel Faj.re .o. 10« ..« Shoclc - C3-«arlng and Treatment ccf Wouadadf Burned0 Radiated and Gassed Casualties , ,». 35
GT«q V»n dm 5 Giesa*®. , o,u Discussion ..., ,, .., 51
General S^sley au. Dlamsai-Cea. ,.,, ., ,,.. ,., ... * 51
CcnniaDder Läbor&t . D i s c u s s i o n , , , , . , . , , , , , . *•• 52
G«ner?al Hall'. ..os ... ..o Disjussicai ,, .... 53
Ma^or General H.G, Armstoong »... , .<. Reçor*; c» the KATO Medical
Canniiitee ,, ,,, ... 53
GaaerralHsXl »».. Discussion „,.. ,. .... ... ... 56
(TUi)
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Page KUnfcer
Colooel Meneoes . . . . . . . A Tale of Tno Cities . .* . . . . . . %
Lt* ColcnelMarks . ».» . Casualty Estimation ( 0 . ... ... 57
Caaiaander Stcaie » . . . . . . Rerport an SHAPE ABC Caaialty Hates conmittee .... ... ... ... 70
Major Qanaral pasting' ) Haistti )
Brigadier Richardson 1 Sp« Capta Cellars 1 Discussion. . . . . . . . . . . . . . . . . 83 lit« Colonel Bach J Lte Colonel Harks J General Hall )
THXRP DATfl 6 MAY 1955
GeaieralHarzds .<,. « Introductian to Avemus » . » . . . . 84
Lt. Colonel Msiis , , Exercise Setting . . . » . . . . . . . . . 86
Colonel Crosse .<.. . . . . JXIS (Army Surgean1 s) plan en
(26 September 1957) ». .»<> 90
(Playlet) ...» » t . g«. « Situation Report .... ... ... ... 103
General Harria . . . » Discussicn . . . . . .o« . . . . . . . . . . 105
Colonel Ueneoes . . . . plan for UCUS 3 Corps (Corps Surgeon) cti 1*9 (9 October 1957)« 106
Colonel cross« ) Flan far DDUS 2 Carps (carps Colmel Douglas)*" ' Surgeon) on Df9 (9 Octciber 1957). 110
GmeralHarris .... ... » Discusaicn ... ... ... ... ... ». U 5
Colonel Mazks ) Problems of AIMS 46 Civisdcn (Divi-captaincritcfaley) *
0 0 0 " sicaaal Suigean) at 16C0 hours an
IM-9 (9 October 1957) .«. — .. H 7
Gflneral Dale ) General Harris ) General Pasting Hans») Discussion ... ... .». ... ..» ». 123 A/M Kilpatricik ) Lt0 Colonel Dickson )
GeneralHarrls . . . «0. 0 TheEpilogue .... . . . . . . . . . . 124
Colonel Aiwrn . . . . . . . The Tactioal Setting . . . oa<> . . . . 126
GeneralHarris . . . . . . 0 Discussicti . . . . . . „.. . . . . . . . . 127
Notes (Si The Epilogue ... a . 129
Colonel Maxks . . . .<>. 00 Colmel Crosse . . . . . . . ^20 Years on", 1755 Colonel Douglas . .<>. . . ^ z t m rm c. „„ , 1QT7 ^ Captain Crltdiley . . . . . h o a r ^ q^ 6 ^ 1977 ** ' *** * " 0 1 3 k
FOTJRra P H ., 7 MAT 1955
General Bessan . . . . . . . Opening Address . . . 142
(1*)
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Paga Number
Colonel Nelsm . . . . « » . , Medical Materiel Report, 1955 *• 1½
General Hall « . . Discassioti 148
Captain Van Peanen . „ . . . Repart by BACLANT's Representative Itfl
National Report 152
Dr. HfasSFarlane o.» . . . . . National Report 156
Col4 Hetopel J/$rg«isen . . National Report 159
Naidonal Report 160
National Report - Italy 162
Major pelten . . . . . . . . . National Report -Luxsnbourg . . . 164
Maj Gen Tan der Giessen National Report - Netherlands *• 165
National Report 169
Col. de Bettenoourt <>•<><> National Rerport 170
GeneralGogen . . . . . . .n. National Rerport 171
A/M Kilpatricfc . . . . . . . . National Rerpocrt - United Kingdom 173
General G. Azmstrong *o* Naticnal Rerpart - T^iited States 175
Closing Remaxics 177
(x)
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Ser-
4 I
5
6
7
8
10
11
12
SHAPE MEDICAL CCWFHtEMCE
4, g, 6 and 7 MAY 19?ji
FIRST DAY
AGENDA FOR 4 MAY 1955
Time Item
1000-1015 Opening Addreaa
1015-1030 Introduction to Con-ference
IO3O-IIOO Intelligence Review
IIOO-II3O Interval
II3O-I2OO Military Operational Review
1205 Group Photograph
1210 Lunch
I33O-I4OO/ ABC Defence Training
I4OO-I43O / Discuaaion on Serial 8
Chairman: Brig. Gen. W.F, HALL
I43O-I515 ^Treatment Qfi Burns in Atonic Disaster
I515-I545 Interval
1545-1615^ Discussion on Serial IO
ChairmanÎ Brig. Gen. tf.F. HALL
Speaker
General A.M. GHUENTHEa s US Army Suprcote Allied Commander Europe
Brig. Gen. W.F. HaUf, USAF (MC) Chief Medical Officer, SHAPE
Brig. Gen. J.M. SCHWEITZEKr USAF Assistant Chief of Staff, Intelligence Divisicns SHAPE
Major Pierre RCiMANs Belgian Anny11 Plans Policy and Operationa Division,, SHAPE
1615-1650 XMedical Rehabilitation in the R.A.F.
Cdr. E.C. STONEa Jr. , MC USNs Medical Branch* SHAPE
Diacussion Leaders; a. Col J. MAGE11 Inspector General
Belgian Medical Services b. Maj Gen Te DALEfl Director-
Gmeralll Joint Medical Serviceat, Norway
c. Gen1 G. FIltRI1, Director General1 Italian Army Medical Services
Maj„ Gen. G.E. ARMSTRONG, Surgeon General* U.S. Arngr
Discussion Leaders; a. Maj Gen H.V. GOGEN1, Surgeon-
General., Turkish General Staff b. Maj P. FELTENs Kiief of Luxar-
bourg Army Medical Services c. Air Marshal Sir James Kilpatrick1,
Director General* Medical Ser-vices j R.A.F.
ä. Lt. Cdr. HOC.M. LABORIT j i Fr. Navy
Sqn. Ldr. C.B. WÏNN-PARRY* RAF, The Air Ministiyj, U.K.
(Jd)
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Ser-ia l
14
16
17
18
19
21
22
Time ftan
1650-=1700/7 Discuaaion on Serial 13
Chairnians
Brig. Gen. W.F. HALL
SECOND DAY ? H M 1???
Opening Address
Speakey
General G. PERAj Chief of Italian Air Force Medical Serri.ce Inspectorate
15 O9OO-O915
0915-0945 / Retinal Effects of Atomic Flash
Lt. Gen* Pierre BRISAC , Deputy Chief of Staff s Logistics and Administration
Col. Victor A. BÏRNES, USAF (MC)
0945-1000 Discussion on Serial 16 Cpen Discussion
Chairman: Brig. Gen. W.F. HALL
1000-1030 Interval
IO3O-III5/ Triage and Treatment of Shock
20 III5-II45/ Discussion on Serial 19
II45-I2O5 /
1205
Chairmani Brig. Gen. W.F. HALL
Report on the NATO Medical Ccnimittee
Col. R.G.J. FAVRE, Fr. Army
Djscuasiqn Leader; Maj. Gen. H.J. VAN DSl GIESSEN Surgeon General, Royal Netheiv lands Army and Air Forces
Major General H.G. ARMSTRONG, USAF(MC) Surgeon, US Air Forces, Ebrcpe
Lunefr
«ftHMHHHHBBHBHBBBBHBHHMBBB-HBHK M M B B IHHHHHHH8WH8BHHH< B H H B Wlf *
* BRITISH STUDY PERIOD * 5 MAY 1955
6 MAY 1 ? »
* # * # * * * « * * * * *
BB WMBHHBMBKHWHHtHHB WH W WBIHHHHHfrHHHXHBBIHHHHHHi Wt BBBHHBBIHHfr
* 1. Starts at 1330 hours, 5 May 1955* in the Con-* ference Rooiajl 4-C-13. # * *
* 2, On 6 May 1955 s the British Study Period contin-* ues In the Auditorium, Camp Voluceau, starting * at 0900 hours. *
* 3* For detail®j see separate programme, Serials * 23-49, (See pages xiv etc.)
50
FOURTH DAY 7 MAY 1955
0900-0915 QpCTiinp Address Maj Gen F.S. BESSON, JR., US Aimy ACofS Logistics, SHAPE
(xti)
NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Sér-i â t
51
52
53
54
55
Time Itm
0915-0945 Medical Materiel Report
0945-0955/Report fron SAOANT
0955 National Reportei on Ma.lor Medical Problems
0955-1005 1. Belgium IOO5-IOI5 2. Canada IOI5-IO25 3. Deanark IO25-IO35 4. France
IO35-IO5O Interval
1050-II00 1100-1110 1110-1120 II2O-II3O II3O-II4O II4O-II5O 1150-1200 1200-1210
5. Italy 6. Luxembourg 7. Netherlands 8. Norway 9. Portugal
10. Turkey 11. United Kingdom 12. United States
Speaker
Colonel H.B. NELSQN, USAF (MSC) Medical Branch, SHAPE
Captain H.J. TAN PEENENs MC USN Representing HQ ACLANT
Col. J. Mage Dr. McFarlane Col. J. Hempel-J^rgensen Maj. Gen. J.H. ReiUnger
Ceneral G. Ferri Maj. P. Feiten Maj. Gen. H.J. VAN DER GISSBl MaJ. Gen. T. Dale Col. J.N. de Bettencourt MaJ. Gen. H.V. Gogen Air Marshal Sir James Kilpatrick Maj. Gen. G. E. Armstrong
56 I2IO-123O Final Discussion Open Discussion
>*U U r ** MM** MMM KmH WHTT Wior BKfl
(JdLii)
NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
SHAPE MEDICAL CONFERBfCE - 1955
BRITISH SlUDY PERIOD
Locations a. PROLOGUE
b. Exercise 1AVERNUS1 and EPILOGUE
- 5 May 1955 - at the SHAPE Conference Room, 4-C-13
6 May 1955 - at the Auditorium, Camp Toluceau, SHAPE
Hlftl if JtAt iUUC If W W HVti H It H JUUL WW U frf.M H MJUL MKM HnK HTfTT Hnn H H M n n n NHfl TfFTTf lIv1M H TnlW
AVERNUS
A lake near Cumae and Naples, Close to it was the cave by which Aeneas descended to the nether world. The name was sometimes used for the nether world i t se l f . It was generally written in Greek "aomos", which was supposed to mean "without birds" and the lake was, in con-séquence« thought to be birdless, a feature which is often referred to.
4HH* ### frtt* ###
DIRECTING STAFF
Brigadier Gênerai Wllford F. IIALLjl USAF (MC) Chief Medical Officer* SHAPE
Colonel T.M.R. AHERNjl British Army, Medical Branch5 SHAPE
Lieutenant-General Sir Frederick HARRIS, Director General, British Army Medical Services
Colonel J.H.J. CROSSE* The War Office (Amy Medical Directorate), London.
M If If WAf M If W w HUT! JUOi u n M lt fit H If H him Mnn N n n n n n TTTTTT M M n Tnnr ?NNR BKn H K JT AM H
Sér-i â t
23
24
25
26
27
28
lies
1330-1345
1345-1450
1450-1520
1520-1545
1545-1620
1620=1650
29 I65O-I72O
PROLOGUE
THURSDAY. 5 MAY 1955
It s i
Opening Address
A Tale of Two Cities
Discussion
Interval
Casualty Estimation
Speaker
Brig. Gen. W.F. HALL
Colonel A.N.T. MMBCES
Lt. Colonel R.L. MARKS
Report, of SHAPE ABC Casuay Cdr. E.C. STONE, JR., MC USN ty Rates Canmittee
Discussion on Serials 27 and 28
(xiv)
NATO CONFIDENTIAL
Medical Branch, SHAPE
Discussion Leader? Maj Gen C.R.H. FASTING-HANSEN Director General, Joint Medical Services, Denmark
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

35
36
37
39
AO
a
42
A3
A4
45
46
47
40
EXERCISE 'AVENUS'
FRIDAY. 6 MAY 1?55
Ser-Ial
30
31
32
33
34
Time
0900-0915
0915-0945
0945-1045
1045-1100
1100-1145
Itefl
IntrodQCtlon
Exerclae Setting
DMS (Army Surgeon's) Plan on D-4. le. 26 Sep 57
Biterval
.Situation Report at 1400 hrs on D plus 8. i .e . . 8 October 1957
Speaker
Lt, General Sir F, Harris
Lt. Colonel R.L. Maries
Col. J.H.J. CROSSE
Colonel J.H.J. Colonel T.M.R. Colonel J. P. Lt. Col R. L. Captain F.A.C. Captain J. A. Major A. J,
CROSSE AHERN DOUGLAS MARKS HINE CRITCHLEY MEDLAND
1145-1210
1210-1345
I345-I4OO >, 3 Corps aE 38 I4OO-I415
1U5-1420
1420-1450
1450-1510
151O-1525
1525-I6O5
1605-1625
1625-1630
1630-1700
1700-1710
1710-1745
Djscussiqn_
Lunch
Plan of DDMS, .(.Corps Surgeon) at D plus .9. i . e . . 9 Oct 1957
How the plan worked: des-cribed at 0900 hrs D plus 15. I .e . 15 Oct 1957
Interval
Plan of DDMS (Corps Sur-
Colonel A.N.T. MENECES
Colonel A.N.T. MQIECES
geon) 2 Corps, at 0900 hrs on D pips 9. ie. 9 Oct 57
Discussion
Interval
The Problan of ADMS 46 Div
Colonel J.H.J. CROSSE Colonel J. P. DOUGLAS
(Divisional Surgeon 1 at 1600 hrs on D plus 9. ie. 9 "et 57
Discussion
Interval
EPILOGUE
jtntroductloyi
Interval
Twenty Ypars o n . M At 1755 hrs on 6 May 77
M
Lt. Col. R. L. MARKS Captain J. A. CRITCHLEY
Lt. General Sir F. HARRIS Colonel T. M. R. AHSlN
Colonel J.H.J. CROSSE Colonel J.P. DOUGLAS Lt j Col. R.L. MARKS Captain J.A. CRITCHLEY L/Cpl D.M. LEE
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Sér-i a ^ Time Item
49 1745-1750 Cloaiiig Retaarkfl
(xvi)
Speaker
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
SHAPE MEDICAL CONFERENCE - MAYa 1955
Minutes of the Meeting held at SHAPE, PARIS, Francs, 4 thru 7 May 1955* with representatives of NATO Nations and Headquarters of Component Forces of Allied Oomaand Earope in attendance
General Alfred M3 Gruenther, Suprane Allied Conmander Europe, opened the Conference at 1000 hours, 4 May 1955*
After welcoming the delegates to the Conference, General Gruenther described the changes in planning at SHAPE which had taken place since the 1954 Conference. He said it was bee coing evident that NATO so-called "conventional" forces could never reach the level that ' would give, a reasonable chance of being able to meet the strength of manpower of the Soviet Union. For that reason, what he described as the "atomic factor" was Introduced into oui; planning and policy. In any all-out war NATO would repel enemy attacjc with atomic weapons. This policy was approved by the North Atlantic Council in December 1954, and SACEUR was authorized to base his plans on this assumption, bearing in mind that the political authorities would always be the ones to make the decision for the use of atomic weapons. The other assumption;which must be f i l led before we could prepare a realistic defence- plan was that there should be an effective German contri-bution;* About two weeks from now, Gemany wil l become a manber of NATO. I t wi l l require 3-4 years before German forces are effective.
Thus, the free world had advocated* the use of atonic Weapons^liit certain circumstances; there waé W other alternative as far as the military situation was concerne^. Thebaslc objective of NATp iras to prevent war. I f war came, i t woiild be very horrible, but it wou Ld not be less horrible by virtue of a. set of pious resolutions to abrftafrrÏKxn certain actions, i f these resolutions had no chance of be-comingTeffective. The Soviets, in talking about prevention of atomic war, had«never allowed themselves to be part of an.inspection system that >fpdld make prevention effective*
Continuing, General Gruentheç said that the most recent Sovleti'methods were clever, in that they were vaccinating their own people against the fear of atomic war, and the new twist they gave to the situation was that atonic war would be f^tal» not to the Soviet Union but to",the decadent social system of the West. So the Soviets were doing everything they could to calm their people .about the dangers of atonic war, and at the same time doing everything they could to make the West thoroughly apprehensive about i t . Soviet claims that they had parity or superiority in the possession of atomic weapons and means of delivering them might not be well founded.
It was also significant that in this atonic age the Soviets in their public talk on May-Day, and also in Pravda, emphasized the ' prowess of the Soviet ArnQr. Some theorists have argued that in the atomic age, amies are useless, but it should be borne in mind that the Soviets have not found theirs useless yet, A very significant part of their re-sources were s t i l l going into building up their army.
Gttieral Gruenther concluded by stressing the importance of unity, which in the Soviet was achieved by a "gun-in-the-back" method, and which the West obtained by a system of collective security;
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

the latter had many Irritations, frustrations, and inherent dis-advantages, but i f the NATO Nations really had faith in the syst an of collective security, he was çertain that the mission of NATO must succeed.
4 BRIGADIER GENERAL HAU
Brigadier General Hall, the Chairman, made his in-troduction to the 1955 SHAPE Medical Conference as followss-
After welcoming the delegates to SHAPE, he said that the l i s t of invitations had been enlarged by including, for the f i rst time, the Surgeons of national land, air and naval forces assigned to Allied Conmand Europe.
This year's Conference had been built around a central theme—that of the problems, deployment and Ainction of medical ser-vices in the field in atomic warfare.
The Annual SHAPE Medical Conference was very important to SHAPE. Medical support, for the forces committed to NATO, was of course a national responsibility: i t would be as adequate or even luxurious, or as inadequate or even austere as the representative nations cared to make i t . He was certain that no surgeon general here present was entirely satisfied with the adequacy of his own service. There were many cogent reasons why our medical services could not attain perfection—manpower shortage, budget diff iculties, other military priorities, lack bf ptockpiles of materiel, to name some of them. It was the responsibility of the national medical representatives forcefully to represent the medical requirements of their own services and to make the medical support of troops comnitted to NATO as adequate as possible.
One of the missions of the SHAPE Medical Branch was to search out the medical implications and repercussions of SACEUR1S plans, and to attempt to interpret them and advise the NATO Nations accordingly* As an example, the work done in the Medical Branch on Casualty Rates in Atomic Warfare had a large influence on military planning.
This annual meeting gave an opportunity to present SHAPE information and thinking to the national military medical heads in person and collectively, to obtain national views and knowledge on these problems(, better to understand mutual problems and lay the foundation for their solution.
In facing the médical problems of unconventional war-fare, it was not possible to be sure, in advance, that even the best possible planning and provisioning would be adequate. Somç nations might require medical help, but a l l would be hard-pressed adequately to serve their own national forces under atomic warfare conditions; none was likely to have more medical support than it needed far its own troops.
The start of atonic war would be violent and devas-tating, with mass destruction and mass casualties. Thu»p the forces actually in being on M-DaJ Were all-important, and must be ccmbat-ready, essentially in their battle positions and with adequate
2
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
reserves of materiel. There would likely be l i t t le or no reinforce-ments of men or materiel to troops in Allied Command Europe for weeks, or months, after the start of war.
Finally, the mission of Allied Ccramand Europe was to produce a completely coordinated international defence effort. Medical support to this effort would be more vital to combat effectiveness in a future war then ever before.
The state of readiness of forces in being, was the vitally important factor. Peacetime building of international acquaintance, understanding, trust, solidity of purpose and the concept of mutually conceived broad policies was a necessary prerequisite to the maximum state of readiness on D-Dayt
Presentations were then given as followss
Brigadier Gmeral Schweizer; Military Intelligence Review
Major Pierre Roman J Military Operational Review
These presentations are classified as COSMIC TOP SECRET, and are not recorded for distribution.
The Chairman then introduced Coraniander Evan C* Stone, Jr., MC USN, of the Medical Branch, SHAPE, Kho proceeded to present a paper "ABC Defence Training."
COMMANDS! STONE.
Medical Passive Defence Training In ABC Warfare
This presentation has resulted from many requests for assistance and guidance to further medical passive defence training in ABC warfare among NATO Forces. Those in Subordinate Commands of SHAPE who are directly or indirectly concerned with this training, have in-dicated great concern over the lack of training in this f ield. Most of thess requests have been made through personal conversations, but a number of off icial letters have indicated dissatisfaction with progress in passive defence training, including the medical problems. Arqrthing that indicates insufficient training in any field is of interest to SHAPE, and that is where and why we enter the picture.. From a series of studies carried out following these reports and requests, we feel a practical way to accomplish this training, has been found. I wil l , for the sake of simplicity, call this plan a "Packaged Training Unit". This unit contains training manualss training films and film strips, maps, map overlays, instructors' guide, movie screen, chart rack, paper and pencils, and a box to hold a l l the above-listed items.
NATO was established in 1951, Most NATO countries feel that progress in certain fields of training has been too slow since then. Medical Passive Defence Training is one of these fields. We would like to see this training stepped up, so that a l l NATO forces
3
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
are a» well trained in this field as they are in the technical f ield of handling the latest armaments. When I f i rst arrived In SHAPE some 9 months ago, my f irst reactions and impulses for expanding the train-ing programme were to encourage SHAPE to issue additional training directives, I found later that such procedures would not produce the desired effect and really would not solve any of the existing problems.
Those who came in to discuss the problems would say, nIt wont do any good to issue further directives. We cannot even get com-pliance with existing directives," Subordinates would say "We do not have the staff specialists for the job5 thcmedical officers and the ABC experts required to Implement the programme," They would add, " I f we are going to do anything*» we need helps you will have to give us the working information—tell us what to teach, what material is required for teaching and where we can get i t . "
Before delving further into the subject, we should re-fresh our minds on what is meant by the phrase "Medical Passive De-fence Training," Sfca&wd in its simplest terms it means doing every-thing we can do3 by pre-planning and training to decrease the number of casualties, relieve their suffering and to decrease morbidity be-fore the actual emergency.
Why is this so Important? If ABC warfare is started, our medical job will be so overwhelming, our logistics requirements so great, that we would be helpless without prior training. It would produce a most difficult situation for the military commander. Training can, to a large extent^ correct this situation. Just writing into a plan« of what we intend to do in an emergency, is not enough; we must actually train,, actually test and practise our procedures and methods. Our position in this training programme is somewhat peculiar because i t is not primarily a NATO responsibility. My understanding of the training problem is that a l l forces assigned to NATO are theoretically fully trained prior to the rime of their assignment^ which left SACEUR with the job of accomplishing only that coordinating training required to complete his mission.
In addition.,, the responsibility to establish and supervise training, except for technical aspectss is a responsibility of training branches under line command er 6 j, not by medical units. We feel, however, that we should Isnd every assistance we can to further training programme of medical Importance.
I think SHAPE was correct when it assigned the responsibility for passive defence training to Subordinate Commanders. The responsibility for this type of training is and should remain a national responsibility. However,, the following specific questions have been asked of us which makes i t advlseable for us to offer assistance. These questions are:
What do we teach? What and where do we get teaching material and pamphlets? Where do we get qualified instructors? , Where can we have personnel trained to become instructors? What do we do when there is no ABC specialist on the staff? Where can we get training films and other training aids? Where do we get the money? What do we use for schools?
These and many others are hard questions to answer, es-pecially when the medical does not have direct responsibility for the job. Yet we cannot honestly or with a clear conscience toss the com-plete responsibility back to Subordinate Ccmmandars and say - "Worte i t out the best you can with what you have, without any help."
U
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
The foregoing questions make i t quite evident that Subordinate Commanders need assistance because they do not have the necessary personnel, equipment er knowledge. Any solution to the problem must be worked out within the framework and limitations noted by the foregoing questions.
For the benefit of the newer participants to this medical conference, let us review the assistance in medical passive defence training that has already been made by SHAPE.
First, SHAPE has made a number of national schools available for the instruction of NATO personnel. These schools in -elude an atomic warfare school at the NATO Special Weapons School in Oberatomergau, Germany; School of Chemical Warfare, Winterbourne Ginner, Ehglandi the Royal Naval Hedlcal School, Alverstokep England, and the Joint School of Chemical Warfare, Winterboume Gunnerj Qigland. Graduates from these schools are a potential source of instructors for the programme to be outlined today.
Second, SHAPE recently sent Subordinate Commanders a consolidated l i s t of ABC classified material cleared for NATO use.
Third, the ABC adviser to SACEUR in January, 1954, made a circuit trip throughout the NATO Nations to gl#* suggestions for organi-zation of training courses in ABC Defence.
Fourth, the SHAPE ABC Casualty Rates Conmittee has made data available on projected casualties to Subordinate Commanders for ^guidance.
Fifth, a l ist of training films was made available. *
We in SHAPE have spent Considerable, effort to search out -a practical means of accomplishing the essential passive defence training within Uie stated limitations. Our problem was always the need to scale down a too-ambitious project—in other words, i t was felt that i t was better to walk before learning'to run.
In looking for an answer, I believe we found the correct one quite by accident. The idea was not ours, we got i t from the USAFEt Wiesbaden. We therefore gratefully give credit to them for the plan we are now implementing. This is their method of solving the same problems we are trying to solve. AU we have done to the unit is to make a number of changes so i t would more adequately meet the needs of NATO forces.
At the end of this talk, you will have the opportunity to see and examine one of their training units. Che of their instructors will be happy to answer any questions you might have on the training unit.
This method of training is designed primarily to see that a l l troops get a certain amount of training In ABC warfare at a minimum of ex-pense and effort. With practically no change it is readily adaptable for use by the Army, Navy or Air Force. A change of emphasis of training due to locale is a l l that is needed. The fact that a l l troops will receive similar training wil l be of great help in an emergency. We in the Medical Branch of SHAPE are interested and concerned in that medical passive de» fence training reaches two different groups of personnel: one, to reach every military man in NATO; the other is a l l medical department personnel.
This packaged training unit is adaptable with slight changes for either purpose. It physically contains everything required to teach medical passive defence to a group of personnel. Placing every essential item in the packaged training unit removes the temptation to say the course cannot be given because I do not have this or that. The type and quantity of teaching material, instructor background, length of the course, ease of
• mobility fund cost were a l l taken into consideration in the design of the
5
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

unit. At this point I would like to describe and explain this packaged junit to you in some detail.
f
First9 the unit contains 12 different manuals on ABC passive defence training for a class of AO students. The l i s t of manuals will be made available to you for Ioani, upon of f ic ia l request.
Second^ the unit contains 3 35=mm films.
Thiixlf, there are two film strips.
Fourthx, the unit contains 2 area maps and 2 plastic
overlays,
Fifth9 the unit contains one instructor guide.
Sixthi, a course manual gives the outline of the course.
Seventh,, the unit also contains a folding chart rack. Eighth, the unit contains one movie screen for movie or
slide projector use.
Ninth3 pencils and paper.
Tenths the last item Ja the box designed to store a l l the above material.
I initially stated that this unit contained everything needed for the course. I wi l l have to correct that misstatement now. Two items are omitted because of cost. They are a projector for 35-nmi films and slide film projector.
The student hand^outs, which are included in the aet-up^you will see at the conclusion of this talk, are emitted from our proposal. Translating^, reprinting and reduplicating efforts are considered too ex-pensive for inclusion in our plan.
Our reason for inclusion of a l l material into a single packaged unit is simple. It removes a l l excuses for delays and procras-tinations in not accomplishing this training.
The subject of instructor needs merits further discussion. Success of the course will be to a large measure dependent on the init -iative and enthusiasm of the instructors. There are several ways in which the instructors may be obtained to run these training courses. Each will be discussed in some detail,
First5 the problem of obtaining sufficient instructors is simple if one or more officers with some training in ABC warfare are available on the staff. His ABC background and acquaintance with the training unit are sufficient for him to organise and conduct an Instruc-tor's course. The students of his instructors' course would.be the 'Xuture instructors for teaching passive defence training to the rest of the military personnels or to the medical department personnel, as the case may be. Packaged units would be assembled equal to the number of student instructors. Upon completion of the course a training unit would be given to each instructor for his continued use. The care of this unit would then be his responsibility.
Secondly, i f officers with an ABC background are not available in the Ccoiinandi, the procedure to get the needed instructors becomes a bit more complicated and eoqpensive.
6
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
The USAFE Headquarters in Wiesbaden has tentatively agreed to run one or two instructor courses to help us to get NATO courses started. In addition, graduates from one of the previously mentioned schools are also considered qualified to get this teaching programme-linkway.
An estimation of the proposed length of the course of instruction is considered important. It is estimated that it will take a minimum of 20 hours to cover the essential training points in the course for each individual; whereas a minimum of k0 hours wi l l be re -quired in the course for medical department personnel.
Now I would like to give you a rough idea of the number kf Xnstructors and units required to put this training course into operation. For this I think I can best explain the method of deter-mining requirements by using an example. Let us determine the re-quirements for Air Force with a total of 35,000 personnel strength distributed in 20 different« air bases. The air base strengths are assumed to vary from 600 to 3,000 personnel. I f an instructor has IiO students in each class, the course wil l have to be repealed 75 times to reach a l l the personnel in the largest base*. Aaaumijafc.20 hours instruction for each class, 2 classes or 00students can be taught per week. Approximately 36 weeks Instruction would be re-quired to reach a l l personnel. This time requirement is considered reasonable to reach a l l of the personnel. Using the same factor it would take only 7i weeks to instruct a l l of the personnel in the smallest base. It would not appear worthwhile in tenus of length of time of unit utilization, cost to establish the unit, and the effort involved to have an instructor and unit assigned to each of the smaller bases. A single instructor and unit could rotate through several of the smaller bases for instruction. Vftien a l l factors are taken into consideration i t would appear that approximately 8 instructors with Ö packaged units would be sufficient for this entire training programme in this air force. The programne would require even fewer instructors i f a year's time was considered sufficient to complete the training to a l l personnel.
The course for medical department personnel would be run along similar lines. Due to the limited number of personnel to be in-structed, the course would require very few instructors and packaged training units.
The foregoing discussion is in essence the brief outline and plan for the medical passive defence training course which wil l be ready for implementation soon«
Before closing, I would like to state that the course has one additional omission: i t lacks training aids, gas masks, protective clothing, dosimeters, chemical detector sets and related passive defence equipment. These »ere purposely omitted because of the cost of the ItVLSd In some instances these items have not been stockpiled for Aiture possible use, Xf any or a l l of these Items are. available for demonstration purposes, they should by a l l means be included in the training programme. Their inclusion wil l immeasurably enhance the value of the course. The instruction should not, however, be delayed or can~ celled because these items are not available.
The time interval from the concept of this training pro-gramme to its present state of development has been short. A number of details must s t i l l be worked .out before the programme can be placed in fu l l operation.
In conclusion, I would like to leave the following thoughts with you;
7
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Ones the primary responsibility for training lies with the training division of a staff . Ve in the medical department give what assistance we can to further training programmes of medical im-portance.
Twos a letter wi l l shortly be forwarded to Subordinate Ccmmanders and MODs explaining this programme, and availability of training aids«
Three*, that training;, including medical passive defence training, is a National responsibility. The responsibility to imple-ment the programme remains with than.
(After the presentation,, the packaged training kit was demonstrated by Major Nielsen. USAFc. He said that the project would be to develop a minimum SHAPE training standard in ABC Def «te® Training. He hoped that the training aids here demonstrated would eventually be made available to NATO Armed Forcess so that each Nation could duplicate the aids and prepare training progranmes,}
COLONEL IlAGE
Colonel Mage described the organization for ABC Defence Training in Belgium. He said that in Belgium i t was considered that indoctrination of the troops should be preceded by f i r s t aid instruc-tion begun in the schools at the secondary level. In order to render the programme readily acceptable to the population, any idea of its use in wartime should be exludèd from its presentation.
I t was important that the medical services should not be overwhelmed by masses of minor casualties and this should be clearly understood by commanders at a l l levels. He concluded by warning that, although mass indoctrination« begun in youth and continued throughout the soldier^ military seyriee was admittedly essential, this encroached on a f ield of activity as yet unexplored and requiring great experience and coordination.
GENERAL DALE
Contimiing the diseussion,, General Dale said that in Nor-way sane 80 instructors in ABC Defence methods had been trained, following init ia l training of a group of instructors in the UK, Military units had not been able to take f u l l advantage cf their instructors. ABC Defence Training had, to seme extent, been looked upon as a medical responsibility^ but this attitude was now changedj the problems were being studied by the General Staff , and more rapid progress was likely.
Saaller countries had dif f iculties in carrying out such training efficiently, Without the active help of SHAPE and the more powerful nations, i t was not easy to keep abreast of highly scientific and technical developments in the ABC f ie ld, Thusp the training and organization of the analler nations' forces would to some extent depend on help received from larger allied nations. This presentation just heard was a necessary prerequisite to military medical efficiency.
GENERAL FERRI
General Ferri gave an account of the history of ABC Defence Training in the Italian Armed Forces. The Amys Navy and Air Force each
8
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
had their own separate schools at which officers and officer cadets were trained in ABC Defence,
He added that in April 1953, a new school opened its doorss the ABC Defence School, which was set up by the Italian Armed Forces General Staff. It is a joint school and is located in Rome. It was created in an effort to extend to officers and NOOs of a l l the Italian Anned Forcess both combat forces and services, a basic lnstruo-tion in- ABC Defence and, in that way, to prepare ABC officers who would be highly specialized and widely experienced.
The ABC Defence School gives different courses for different purposes for example:
1. Courses of a tactical nature, with special empha-sis on atomic weapons, These courses are attended exclusively by high-ranking officers (generals and colonels) of the combat forces of the three services.
2. Special courses to train Regimental (or equivalent) ABC officers. These are 50-day courses of a high technical and mili-tary level and are attended Only by officers of the fighting aims.
3. Courses for medical and veterinary officers of the three armed services. They last for 25 days and deal mainly with biology and atomic medicine, physlopathology and therapy of -chemically caused lesions, and concepts of biological attack and defence capa-bi l it ies. A number of civilian doctors and veterinarians also attend these courses,
4. Courses for NCO radiometiy specialists* These are basically practical courses, the only purpose of which is to train NC0s> to measure radioactivity in the field and to use and maintain radiometric devices. There are also plans to have some of the Medical Corps NCOs attend these courses.
All of these courses are supplanented by individual pro-tection and first aid exercises, practical tests in the gas chamber and open-air démonstration.
The courses for military and civilian doctors and Veter-inarians are also supplemented by visits to civilian specialised institutes, such as the Advanced Institute of Public Health, the Cobalt Isotope Radiotherapy Centre at Rome, and the Radio Isotope Therapy Centre attached to the Ancoha Hospital.
Just after It opened, the ABC Defence School offered, three information courses to doctors and veterinarians, which were attended by 00 senior medical officers and 7 veterinary officers. The officers who took these courses then gave lectures on ABC defence in their units or in the military hospitals. These lectures were intended to extend the basic concepts of ABC defiance among the officers, NCOs and troops of the Medical and Veterinary Corps.
Training for medical orderlies can only be provided when there is a sufficient number of specialist instructors.
An Important detail regarding the operation of the Medical Service in war or in the event of ABC attack concerns the divi-sion of responsibilities between the Medical Oorps (including the Veterinary Corps) and the special ABC Defence Service.
9
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Xt has been decided that the detawt'on of ABC agents In the field (radiation^cd ^haaical cr bici^gisal agsofca) is the res-ponsibility-;, in principle j of the special wmdt<? of the ABC Defence Sendee,, the organisation of which is undei' study by the Armed Forces General Staff , where progress is bei'-ng mad* on the problem* Special-ist officers of the Amy Hedlcal Corps may be included as consultants.
The d «contamination of unwoundc fehd otherwise healthy men and arimale and of the terrair»P supple», water, aquipaent, etc, Is also the responsibility of the special rnits of the ABC Defwice Ser-vice.
Qn the other Itandn the M$&Lcal and Vatarinary Gorps are responsible for the d«eontaminatio& and treatment of the wounded and sidi men and animals wfcc- require therapy*
That is iriiy the ABC Defence Sarsic » mist be responsible for deciding the degree of danger involved In decontaminating personnel who do not require therapy and in deÜsntsminating equip" ment and the terrain.
Hcwevers the Medical Serjica muat b? responsible tor de-termining the dutgerousness and need for tht^apy of contaminated personnel sc well as fey dfttsoirfcamin&tiiig the ei«k and woonded.
Recently the subject of i-idioa^f/rs iMräjpe research has ïcitte under discussion. Htwe of this t^i'l öf ^»asi-cli is now being conducted ift the Italian Aimad Fan-as Institut®, but here again, ß'illaboration with the U.S. woald fca deßirsbl« and helpful.
Ansther sourse of InfoKnatiea to whi h medical officers have assess in this fisld ere the up-A,-date arti^.se in the Journal of Military Medicine (to wfcish they al l aubaesflbs) on the medical aspects cf atomic and bacteijic^gi.^al warfare. Tfc^es articles are written by Gatreral MastAj Ifca3*.an Msdlictf, Corp?, who is a professor at the University et Rcme and has mada a sp?^iai study of these questions.
AH of what I have said àe&ie that for srae time now we hairs been expending the knowledge of ABC d&ftanft'i aamg the Medical Service personnel of the Itallac Armed For-; es on ax? effort to pro-vide the Territorial Military Hospitale and the medical units in the field with peratmnel^ in the event of an eEWgcajr/, who ere trained in the methods to be used in caring for ABC saBualties.
We are s t i l l fa? froa our goal, but it is comforting to note that the InstPacti1Tn given ie b»»:Mihg mwo and more complete and that it is reaching an e^ecy-increaaing rcnaber of officers and NCOs of the Medical and Vefcwlnary Cor^.
GENERAL, HALL
The Chairman9 ir. Introducing ths next presentation, said that the aim of the Confei-ance was to consid?:* the functioning of medical services In atomic w&rfare, and not to discuss the details of surgical and medical conditions* The™a were, however, two major professional problems in atomic war:*ars whixh must bs considered, however briefly. These We^ejl the treatment of mass burn casualties and the treatment of mass shock casual le*.
10
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Before Major General George Amstrong 's presentation on the treatment of mass burn casualties,, Hajor General Gogen, of the Taticish Armys would speak on the general aspects of this subject.
MAJOR GENERAL H.V, GOGEN
Major General H.V. Gogen8 Surgeon General, Turkish General Staff, then addressed the' Conference. He gave an account of the his-tory of bum-producing weapons and their use in warfare, and drew attention to the changes that nuclear weapons would cause in this f ield. The great difference would be in the very large numbers of burn cases which would be created simultaneously.
He then traced the development of nuclear weapons and- re-ferred to the type of casualties caused by the 'atomic explosions at Hiroshima and Nagasaki.
General Gogen referred to the peaceful use of atomic energy and said that the known fearful effects of nuclear weapons were so terrible that they might act as a deterrent to any aggressor of the future, and so serve to avoid war.
HAJOR GENERAL G.E. ARMSTRONG
General Hall, and Gentlemen. First I should like to rwark that I miss on the front row the faces of two of our stalwarts; General WiDcens of the Netherlands and General Hugonot of France. Those of us who had the pleasure of attending the previous NATO Medical Conferences will understand what I mean when I say we not only miss their faces, bqt their very sound observations from time to time during the previous conferences *
Secondly, I should like to apologize to General Hall0 to General Gogen and to Major Feiten because of the lateness with which I furnished them copies of this particular paper. Vftten the decision had been made at these headquarters that this paper was to be part of this programne, and when it was assigned to us, we fe l t that we should come to this particular conference and present to you the very latest de-velopment«,, in the therapy of burns. When I got a l l together certain Experts in ttaia .field, both civil and military, they were unable to cane to a unanimous opinion relative to the present status of this therapy. TherefoJrep as you wil l note this afternoon, I present to you a compromise; and let 's consider i t more in the nature of a progress report.
Jreatmenj;, Cf ffitrna in Atqaic Disaster
Under conditions of mass disaster such as may be expected in nuclear warfare, thousands of casualties are produced. I t is esti-mated that as many as 65$ of the surviving casualties 'will have ex-perienced flash bums of varying extent and severity. Added to this large group wil l be those suffering burns produced by f ires ignited by the f i re bal l at the time of detonation or from broken gas and electric lines and overturned heating devices.
Burns are one of man's most frequent and serious injuries and annually account for many deaths and many more disabilities. The economic loss to any nation in terms of man-hours is highly si f f i i f ic-ant. Furthermore, i t is common experience that when only four or five seriously-burned patients are admitted to any hospital, an otherwise well equipped and well staffed organization finds itself severely taxed to properly meet the responsibility.
11
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Beeause of theo^ facts, research in this f ield is a continuing programne universally to develop better methods of medical management of burn wounds and reduce the undesirable morbidity and mortality rates.
When great numbers of bums occur, i t becomes apparent that i f the best care possible for the most injured Is the sound approach to the problem, certain compromises in therapy must be made and concentration on the ideal management of the few wi l l not meet the challenge in a satisfying manner.
In the approach to the problems involved in the medical managonent of thousands of bum casualties, on« logically reviews the current concepts of burn therapy and the studies being under-taken to perfect' better methods. The treatment of burns is con-sidered from two approachft«Î (1) the syst «aie care of the patient, and (2) the local care of the burn wound.
Systemic care takes precedence ov«r local care both as to time and importance, for i t is the deterioration of the body economy that k i l l s , rather than the loss of skin and subcutaneous tissue. Innediately following burn injury there is a diminution of blood volume with loss of fluid into the interstitial spaces, as well as from the wound surface. ï'hese losses of colloids and electrolytes eventually cause peripheral circulatory collapse unless they are adequately replaced. It Is now known that both blood and electrolyte solutions are required to re-establish a proper circulatory .volume s though the ea»«i rat Is? is yet to be determined. The best working guide should be the clinical response of the patient,.(Supported by repeated labci*&fcory studies. The vol-ume of input required Is determined by the urinary output which should be maintained at 3C~50 cc. per Iisur. A comparatively simple formula has been widely accepted in the United States and, though generally applicable, is subject to modification according to the clinical progress being made by the individual patient, (SLIDE.)
The per cent of body surface burned is rapidly estimated by the equally popular »rale of nin«»11'. (SLIDE)
The fluid requiranents for the s«cond 24.hours are about one-half the amount of colloids and electrolytes estimated for the f i r s t 24 hours,plus an additional 2 litres of glucose in water. After 48 hours, the Btoderate burn can usually be managed with an ad U b intake of water and food by mcuth and with blood transfusions as required. The more severely burned patient «ho maybe intolerant to oral feeding wil l require continued intravenous therapy.
Foreseeing the ne«d of a temporary substitute for blood which may not be Immediately available, several solutions have been studied and used as plasma volume expanders, the most popular being Dextran. Si an emergency they have been l i f e sustaining uatil whole blood is available.
In less severely bUrned patients the use of an oral electro-lyte solution is usually adequate. Such a solution is made by adding three grams of sodium chloride and one and one half grams of sodium bicarbonate to a l i t re of (tool water. This solution is usually well tolerated and provides sufficient replacement of electrolyte loss in patients of not Jnore than 25% of body surface burn.
In addition to replacement solutions, other supportive therapy includes narcotics for pain, antitetanus prophylaaie and antibiotics for
12
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

the prevention of secondary infection. PeriblUin and Streptcmycin are the antibiotics of choice, but à broad spectrum antibiotic may be required i f these prove to be ineffective.
Local care is carried out in one of two ways. For several years effective care has been obtained by covering the burned areas with petrolatum-impregnated, fine-mesh gauze supported by a bulky occlusive pressure dressing. More recently the open or exposed method has been re-introduced and proved to be acceptable. This latter method is particularly applicable for burns of the face, perineum, and when only one side of the body has been burned. The aim of both methods is to prevent the wound from invasive infection. In the latter instance this is accomplished by the dried coagulum which rapidly foxms on the wound surface« These methods may complement one another, parts of the body being covered with a dressing and other regions exposed to the air. For ease of application,, a bulky one-piece dressing has been devised . in two sizes, one of which f its the arm and a larger one suitable for the leg or torso. When employed, they are le f t in place for 5 to 7 days. Such dressings are now standard items in the United States Armed Fbrcws.
Ttte -Mposure method has two distinct disadvantages; (1) not a l l bums can b«r adequately exposed, such as large circumferential bums, and ¢2) moderate discomfort has been present during the f irst 46 hours or until the coagulum is well dried. Likewise, the dressing method has certain disadvantages; ( I ) the application of dressings is time-consuming and requires reasonable experienceP (2) they are com-paratively expensive, (3) they require changing at regular intervals. Such changes are frequently painful and may require general anaesthesia*
Begardless of the type of local care employedp less infection occurs i f the wound surface is cleansed IMtia l ly with soap and water, a l l blisters broken, and devitalized epithelium excised.
Early excision of the eschar of füll-thickness bums and the immediate covering of such denuded areas with split-thickness skin grafts is a genuine advancement made in the care of burn patients. Convalescence is thus speeded and in severe bums the degree of dis-abling irtsnition appreciably reduced. Easily mastered instruments for cutting* such grafts have been perfected and the problems relating to the use of homografts and banking of skin for future use have been thoroughly studied. The use of fresh cadaver akin is being carefully evaluated, for such a source may prove to be Important in the care of masses of casualties.
Much He^ been accomplished In studies concerning the nutrit-ional problems of eeverely-burned patl#ft£s. All eagerly await each new report of progress made.
i
The primary aim in the management of masses of casualties must be to accomplish the greatest good for the greatest .number. It is reasonable that during the f i rst few days a l l supporting medical personnel will be engaged to the uti*90t° It is mandatory, therefore, that the greatest effort be directed to those casualties who may be expected to survive. Admittedly there are calculated risks In establishing priorities for care, and penalties for delayed treatment caused by the heavy load. Certain intelligent compromises in optimal care wil l be required.
Unlike mechanical injuries, the barn injury lends itself to rapid estimation of the extent and severity. The severity of a burn wound is directly related to the volume of tissue burned. It is be-lieved that the majority of burns in atomic disaster will be of the second degree, though i t may be dif f icult in any individual case to deteimlne the exact extent of second and third degree burning.
13
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Furthermore, massy wi l l hava associate injuries. Thus, triage of patients becomes highly Important and for practical pur-poses four groups of burn casualties wi l l fc? considered! ( I ) self-care burn's, (2) moderate burns, (3) seves,** bum» and ¢4) overwhelming bums.
Self-care bums. This group comprises those with 10$ or less of body surface burned and, unless of hands or feet, wil l re-quire no immediate professional attention* Xt is believed that iuider conditions of atomic disaster a large percent of the flash . burns wil l f a l l within this grcip and naist for themselves or each other,
MofljWjàte bums. This gmip wi l l cxisiat yf those with 10 to 20% of body surface burned« many of whom wi l l also be required to care for th ans elves whereas other» wil l requis professional guid-ance and eventually medical ski l l .
These f i r s t two groups wil l not be «onside:fed for early hospitaliz-ation, for the hospital beds must be reserved for more urgent cases and life-saving measures.
Severe burns. Theds wi l l be thos« casualties with 20 to 40$ of body surface burned,, many of wheat wi l l be in need of intra-venous fluids arid intolsrftnt to fields by nwuth, Additional in-juries i f present may require priority in att.<<ntion and probably wi l l need hospital care. Sarly organization of bum centres or sections within the hospital wil l b$ desirable. Special di*essing rooms wil l be required; otherwise, within a few days such cases wi l l cause severe contamination of the entire faci l ity.
1 [
Qvejfyihelmin burr-?. The survival ^atio of burns greater than A0£ under ideal conditions be;:«iee progressively less with each increment of total area burned. Under conditions;.,producing thousands of burns with limited personnel and supplies available to care for them, the mortality ratio may prove to be appalling. In many in-stances, efforts to resuscitate may ¢3 fruitless, and at best only those measures which wi l l promote somferft wi l l be possible. The age -of the patient must be considered alsoj, for neither the very young nor the very old tolérât® bura injuries vetry well, Whereas none wi l l be abandoned, i t must be considered that many cafrualties wi l l be hope-lessly injured.! As unsatisfactory as i t may s<sens, this group wi l l of necessity receive a low priority in the sewtlngly endless chain of care.
Admittedly5 this rough classification is inadequate and fails to distinguish between soârad dögra« »iii thirä degree burns which are more serious injuries. Nevertheless, two important deductions may be drawn: (1) Because of the enormous medical load suddenly created, many casualties must care :?or fchemsjlTSS aad their neighbours who under normal conditions or in conventional warfare would be evacuated to hospitals, and (2) a smaller grosp fare ia^ured and a great percentage may not be expected to survive with the best care avail-able. This latter group grews with the Increase in volume <on the one hand, or the decrease in professional p^ioma«! and needed material on the other.
The f i r s t deduction points out the urgent necessity for ré-évaluation by a l l nations of their ti.'&inißg programmes in f i rst aid and snergency care for civilian personnel and ^oaprafessional military personnel. I f self-care and "buddy-sare" or neigtiboar^care, are expected to play such an important role ITI the earJ^ hours OF atomic disaster, -such could be more effective with pre-planning and a broad educational programne of instruction in the principles of anergeacy care.
U
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Their« are additional problans in need of solution i f a realistic attitude is assumed regarding, the total medical responsi- . bi l ity. These may be divided into two groups: (1) organization and administration, and (2) casualty/care. ^ v • - • i/ :.-
It must be accepted that there wil l be loàsés of profess* ional personnel In the disaster. Early mobilization of physicians from neighbouring units and.areas who, during the1 early hours of.posi-bcmbing, will guide and direct the activities of many less-trained individuals rather than actually performing the details thens elves, wi l l be indicated. . Sorting of casualties for priority in* care>ç ' ijitV evacuation, hospitalisation and surgical treatment-beeome^i-ia^^r^ portant responsibility and obligation. Leadership^ teaoworkand >. the ability to improvise under the imposed limitations and adverser conditions are but arfew;of the subjects to consider before., and^not/^, after the incident; : ^
' Under medical care, one must consider the problems of mobilisation ofpreserve .suppliesand the necessity for simplicity ;, ; in technical j ^ c e d u W required to provide care for the greater,..' " , number. Whether :or not the application of a bland ointment to a l l : burned surfaces'-jwith or without an incorporated antibiotic as a simple solution to a/difficult problem is in need of . review. Certainly many can be made; mor*1 comfortable by so doing. Whether or not hypoder-—'--;---aoclysis (shouldCbe used; in Ilea o t intravenous therapy: Is* another1- ^ • simple approach -to be considered. .The preparation of packets -of SalV1; and soda fipr*le«trolyterepl&cecient would not be di f f lcnlty ahd^ th'e ^ identification and general distribution of a broad spectrum antibiotic for oral use merit* iIifrrttigation; ' - • ' \ T ;V'-
.: •-•• ' . -:,-.-1. . . * . -V • -,
These are but a few of the problems considered .to be,ln;<r > • ttëed of early study and decision. This responsibility i a a imtual'one thai the recommendations made be generally accepted, and policies,^VY doctrines and techniques be the best for patient care whei ever, such care becomes necessary, . , : •-".
Ih conclusion, one may state thai themedicalproblems ' created by the Incidence of large numbers of burn casualties/presents difficulties in/Used, of thorough evaluation. The ,ourrent;feohc«pts of"' medical managent«it under ideal' conditions are a distinct ^rbveme^ft^ - . over the past, but also present genuine deficits* ' Lfcrge numbers of ^ Imrii patients o^r ly tax our best facilities and; recent advances in ' V therapy inadequately solve the problem. In aicmie warfare capable, of producing masses of burn casualties, some sacrifices must be made in desired therapy and individual care in order that the medical; effort may effectively serve the greatest oumberg considering:this workload . , and toted responsibility, attention must be divided among the, many, \ Therefore, many burns usually requiring professional attention be diverted temporarily to allow life-saving measures to others;'Soite seriously burned must be classified as, being fatally lnjured and re-ceivé^|upp»iriife care only, vhereaa others wil l be judged to be in need i f simple procedure» of f irsi*aid and returned to duty. A known, penalty in this approach to the total problem Is accepted. However, the success of the m«t±Vf£ effort wi l l be measured by the survival-rate and the capability of continuing the resistive* effort and do- / feat of the opposing forces,- Success in any military mission can be attained only by superiority in numbers of effective personnel capable of applying irresistible counter-measures*
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

BROOKE FLUID FORMULA (SLD)BDr."'
FDBT 24 HOURS .
Oolloida - 0.5cc/kg/sS Burn (blood, dextran,« plasma)
IO5O cc
Electrolytes - lr5ccA«/* Burt» (lactated - ringer, saline) ...
315O eo
Qlucose in Water, daily requirement - 2000 cc
: 1.. ,!V : •• •
- J^ - .- .-V .1.,-jr-
-V1 ".-!••> -.. ' •
' • -
-••Sffïfpil' ' ;
Ke1-SiSJigtto''
• , t .. :
'-•f
I . .i
6200 ce
70 Kg - • -H
:-.. • .-y
16
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

i, .1; (SLIDE 2)'
t. . •n.
î.
METHOD FOR
ESTIMATION
PERCENT OF BURN
& • •
11 RULE OF NINES"
• - 1
17
M
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

MAJOR FKLTHJ
(Discussion)
Any bum affecting 151¾ or more of the body surface must ; necessarily be treated in a hospital centre. .In giving correct treatment to a serious bum, i t must primarily be borne in mind that the bum creates general lliness affecting the whole of the body. Each of the three stages through which the bum casualty passes necessitates an adequate therapeutic. > ^
As soon as the casualty-has got over the primary,and • /.;*/ secondary shock, grafting must bs carried out as rapidly as possible.
One criticism is-that i t is insufficient' to know what must : ' be done and how it must be done, but one must also be able to do' it^ ; : -Here—I wil l not try to escape it—is the crucial point of the whole - r problem. What can be done in the case of a rush of thousand s/jorreven '/ tens of thousands of serious bum casualties? If a solution can be / J J found to this heartrending problem it tan only be sought at a-hlgh"^'" level after long préparation and in wide cooperation between the civil and military sectors. , ; Y V'V /3-n -.
Even in a war fought with conventional weapons, burn c&s- r j * ualtles constitute a .very grave problem for each medical service. • - / Consideration has been given to issuing boxes of bum dressings to , each unit. In particular, for armoured forces and air forces each vehicle or aircraft should' have boxes' of dressings for the crew. The\/-box should, contain big,padded dressings for the trunk and lotig dressings for the limbs. In addition, it Should contain 500cc flasks of dry . plasma and 500cc flasks of dextran. Howeverj i t seems to me that i t would be much more advantageous and productive of more efficient r e - r >> ' i suits i f "mobile burns teams** were set up, capable of rapid movement,v staffed with experienced personnel and fully eqûipped with materiel. I t is this last suggestion in particular that I would like to have 1
discussed.
AIR MARSHAL KILfATRICK ' / In the general discussion which followed, Air Marshal Kilpatrlck
pointed out the mistakes inherent in* assessing bums only by their / extent. The eventual effects of the bum on function was of consider^ . . able importance, especially of military importance. He supported General Armstrong's suggestions that f i rst aid methods, which burn/ cases could apply to themselves, be defined and developed. .In eases -such as bums of the hand, where function is affected disproportionately to the extent of the bum, a practical f i rst aid measure would do a-great' deal to preserve function, save ski l l and.manpower.
Naval Principal Medical Officer LABORIT • »
I have been greatly interested in the discussion «1 burns,.-, but I am not entirely in agreement on a number of points, and I feel that General Armstrong made a most interesting remark when he said - - -that, having gathered his colleagues around him and having asked them . their opinion on the current treatment of bums, none of them agreed*.
I consider in fact that this is a problem which is far from being solved, both on the:general plane of military tactics, which con-cerns us, and on the more special plane of the treatment of Individual /, bum casualties,
10
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Much bias been said, in particular, about; shock treatment* Personally I feel , on the contrary, that this treatment is just about solved* Our burn patients, even with severe and extensive bums, reaching ai times 05$ = are slow in dying. I remember, three years ago, a woman with this proportion of burns, who, because of the . explosion, was suffering also from pneumothorax and hemorrhagic pericarditis^ this woman did not die until the f i f th day and not ., . ; frcm shock. It is during the period from the 8th to IOth day that, v their condition becomes extremely serious and we cannot do much about i t . . r • ..,..
In the f i rst place,, I do not carry out transfusions as , ,. abundantly as has been recommended. We were told:that the liquids ' transudate, but in fact i t is in part to Intratissular transudation," the water, and the salt in particular, remaining in the tissues* Our "hibernated" turn casualties do not transude in large quantities outside the body, so that' on the 3rd and 4th day, when the, circulatory' equilibrium is re-established, there is a risk of acute. edema of the . 1 lung which carried off the patient relatively quickly, ; .Therefore,;,we . are on our guard against abundant transfusions, particularly,tealina i transfusionsj generally during the f irst 24 hours we do not give, more than 2 to 3 l itres. . ' V, . .. -J
You may say that 2 to 3 litres are insufficient to re-est-ablish blood pressure,. To that I reply that what is necessary in this, case is to prevent reactlohal phenomena and, inparticular^this trans-udation about *rtiich we have heard, this extrà-tissular and intra- - ' tissular transudation, which can be avo id edby, bio eking t the syst «>..- ,, „ ertlich originate i t , the vegetative and endocrine systems^ by pharmaco-logical methods. . v., -- :
' Actuallyf our burn casualties,are dry burn casualties., All those who have practised neuroplegia on burn patients =• severely ->!•' bumed patients - our colleagues in the Northern mines like Amoudru, like Lagrot aft ELgiers, and Thaleimer at Boucicaut,Hospital, in Paris, s agree in their observations that these burn cases do Wt transude and v
there is no edema because transudation is prevented., Inere is therefore no need for abundant trar» fusions. With two litres in the f i rst 24 hours - two litres of plasma or blood since hamo-concentrâtion,is not to be feared - i t is possible to maintain their blood pressure at a sufficient value for the kidneys to functionearly,.. and these burn ; ' patients urinate in the f i rst 24 hours from 200 to 500 cc.. ..The next',-, day they urinate in general from 8 0 0 to IJOOO cc, and the question of adrenocortical exclusion and anuria, which is a vasomotor problan, Is also, in ny opinion, resolved. .. " .'. .-.
The problan is therefore delayed and drlses, between the Sth • "and 15th days. It is à problem of exhaustion caused by- the. severe ,,. burn and basically i t is the only one which we have to deal with s ta serious burn is an aggression which continues; It is an aggression \ • whlçh lasts fpr poptt^. . . -. ^ . ci--..
I have at present at Boucicaut Hospital a 60% bum patient with wham I did not concern myself after the f irst month, as.,I. was quite happy about her general condition, and during the third month Ijwas toId that she was dying* It was necessary for me to rehibernate ,her, and .re-sume management df the case* At present .she is for the time being .coming along a l l right, but we are now in the f i fth month. A burn is thus a . long, drawn-out af fair , and, because of this, it may .'lead, to exhaustion particularly an adrenal exhaustion, raising the question of .the d i f f i - " culty of the later treatmentP which is , I feel san,essential question.
General Armstrong also stressed at length another point which seems to me to be very Important, and that is that in the case of a- , :
W
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
catastrophe on a national level, there would obviously be such a number of burn casualties that, they could not a l l be looked a f t e r ; / i and above burned body surface, in view of the.precariousness of our therapeutic possibilities, we can only prevent these doomed".' ' -j. casualties Aram suffering. The therapeutic which; we advocate di>ss' prevent suffering. The, casualty i s quite unconcerned and is unaware , of what Is happeningj he does not suffer and he does not complain, )
This is a very Important point ; '' ' Axiy ' l^rMiweii^'^'&l^ alleviate suffering by placing the patient In a state of indifference , without adversely affecting, the vita l prognosis of, the case should be cnq>lc^ed;r. On the other hand* any type ,of analgesia which .would r e - ( ' duce the patiéàt's chances df survival should not be employed.', ; ..
In any event, in this non-suffering condition, it s .much,^f easier to evacuate Ute casualty and that is Just about thé essential '^ fact I wanted to bring out. There are obviously many tithér thinjgs .' to do; i t is'ari extremely complex matter. I do not thlnk|thatvlocal/ j: treatment in particular i s Essential', 'whether i t Is treatment 'ly^eom-^ pressive dressing or by "open a ir " methods. I feelvthaV the ; l o c a l ^ ; 4 treatment is quite secondary; i t i s the biochemical treatment", in ^ general, for the nervous, and endocrine systems which is the dominating' factor. ' . , - . - '
• • • • ' " . ; .- . . . -- \ ' ' • . ' 1 . . • - V A Ï . . . • >-„" *;
: • •
i I have tided to sum up às simply as posslblê what I tK ink^ of the problem. I am sorry to have taken so long to do i t .
At présent, the general treatment that we give tô'àerious;/ burn cases is as follows? V' v- - / • , 1IjVi -ISp ^ ^ f? :,
First 24 or 40 hours't a r t i f ic ia l hibernation, lowering the body temperature to 32 or 34° Centigrade (89.6 ^ ^
Then neuroplegia (chlorprotoaaine pins promethaaine p i n ' s - , nembutal (pentobarbital sodium)) for ;'ilfveral weeks. ' " /'• ' ' / ^ f ^ V ' l
Frcm the 3rd or 4th day onwards i ; - V X ^rt i
Each Evening - pituitary somatotroph!^ 30'to 50 units DC'yI
Each Morning ~ A.C.T.H. 25 mg for 3 days, then Cortisone/ 25 mg for 3 days, ' . , ,, , .
This treatment seemstö us to be indi sp «ns ib i e^ t ö'c o®i>ansàt e parenchymatous endocrine exhaustion. . - ... ... -
Supply of K and Ca, based on the patlenttSTneuro-museular ,. excitability. In addition, insulin (10 to 20 units per day) i n ' 4 : l n - v jections plus hypertonic glucose (30 to 60 cc) and herapin pïùs ' l ipo-^ cad c (8 to 12 sublingual glossettes)^ which have seemed'to us: to act favourably on metabolic disorders of the l iver cells.
.•'.. • ••••- / '
GENERAL HAU. : ...>,.......- ... - 7 / , . ' „ . -
The Chairman then'stated that the papers that had ljeen, pre-, s anted would be provided in' detail when the minutés of the meeting were published, and when the controversies on the types of'treatment^lnZr., V various services could be settled.' The magnitude Of the problem .wis greater than generally realized,~and as could be appreciated^^afteri hearing General Armstrong's statement, even the arrival of four or f ive severe burn cases in any., good functioning hospital would practically disrupt the routine of thé institution. - ^
20
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
The Chaliman then Introduced the next speaker. Squadron • • Leader C.B. Kynn-Farry of the R.A.F., who was presenting a paper nHedical Rehabilitation in the Royal Air. Force." The presentation was opened by the showing of a film. ,:
SO) AKtON LEADER WMf=PARRY
I hope that this film has given you some idea of the work done- in these Centres and the tempo of rehabilitation. . I should */. like now to discUss briefly the advantages of such centres and the sort, of results obtained. -V ' ' ,
-V i. • i / , " V.
The aim of the rehabilitation units is to returrr an in-jured or sick patient to duty as quickly as possible, this goal is a functional one in that we aim to rehabilitate a patient"for his particular job. As soon as he is f itto do that job he returns to duty. I think there are six nain advantages of. a residential-re-i' -habilitation Centre. The patients get f i t quicker, they regain a.-'-hitler standard of fitness, they learn how to care for their disability and prevent future occurrences, a higher proportion are enabled to - - -return to service duties^ there is a quicker hospital turnover and r thus hospital waiting l ists are reduced and there is a better morale within the service as & whole, when it is known that whatever happens7
to à man there is a comprehensive rehabilitation scheme to get him f i t again, .. . : 1
Type of Patient ... ,,
Orthopaedic cases account for some 70$ of the patients at a rehabilitation centre,, these Include a l l typès of fractures and' dislocations, orthopaedic operations such as meniscectomies^-repaitfs^. for recurrent dislocations, arthroplasties, tendon transplants and . other reconstructive procedures 3 postural abnormalities; and spinal disorders. The sooner the patients are sent to . the centres'the quicker they wi l l become f i t for duty. In the case of fractures' for. example, the ideal time for such patients to be sent is as soon as the Aracture i s in good position and the Surgeon is satisfied with the plaster. Thus a patient" with a fracture of the Tibia should be at the Centre within four weeks after injury* In this way the Muscles can be pre-vented from wasting to any great extent, joint stiffness is minimal and bad posture and walking habits are avoided. The second group of patients are those with neurological disorders. These are of a l l - . types and in the main comprise patients with Polio and Peripheral -Nerve Injuries where f u l l time, treatment is so essential-for a good result. Many patients with medical disorders benefit from rehabi-litation and .the common cases we-see in this group are ehest: disorders such, as Bronchiectasis, unresolved pneumonia-and rhoumàtic-diseases particularly rheumatic fever and rheumatoid diseases. -Manypatienta-. after surgical operations such as appendicectcmy, hernia repairs and varicose veins are sent for a short course of muscle re-education,
FinaUys there are a group of patients who' are sent for a short period before operation either to build up muscle power t o f i t them for the operation to obtain fu l l passive movement in -joints be- -fore tendon repair». There are some patients in where a tentative • ' diagnosis of torn cartilege has been made-and in which there is not- • sufficient evidence to warrant operation. A short course of provoca-tive exercises at the Ceotre ^will establish whether such-patients re-quire operation or not, and .thus much time and chronie disability -can-/ be avoided.
21
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
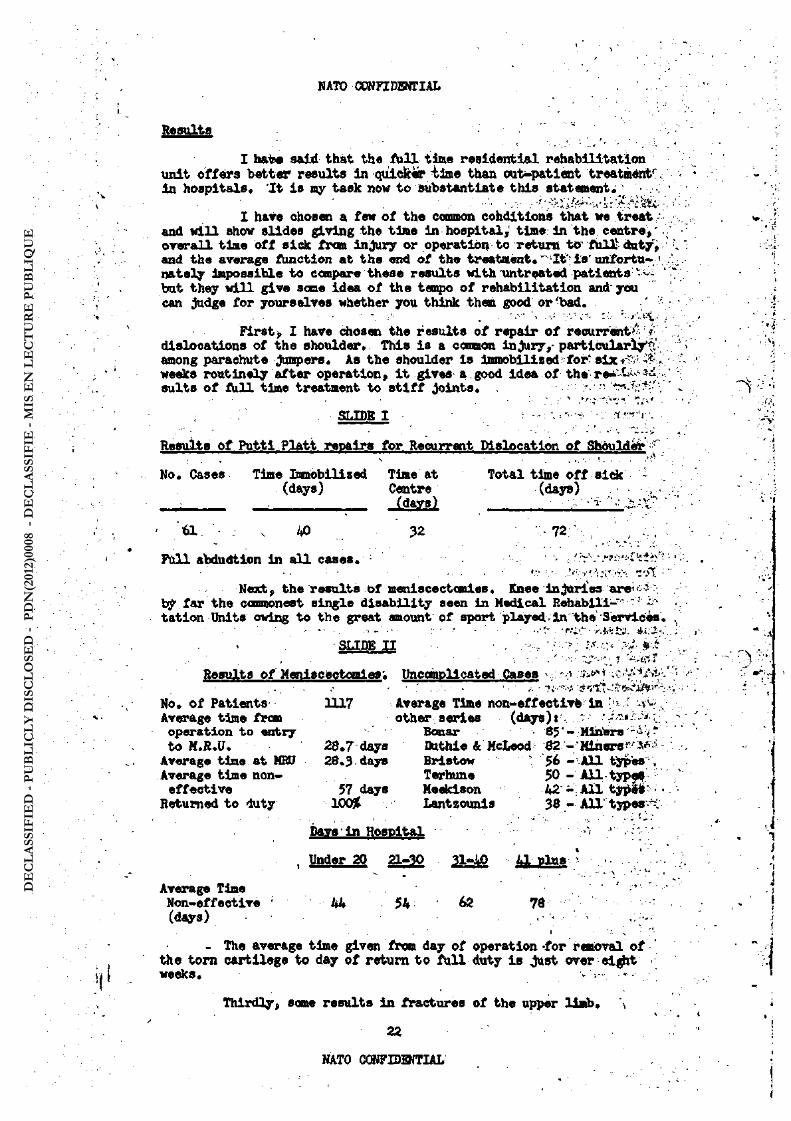
RftBttlta
I hat« said that the A i l l tine residential rehabilitation 1
unit offers better results in quicker tine than out-patient treatmént' in hospitals. 'Xt i s my task now to substantiate this statement; • •
I have chosen a few of the common conditions that we treat / and wi l l show slides giving the time in hospital, time: in the centre^ ". overall time off sick from injury or operation to return to' füll- duty, and the average Amotion at the end of the treatment. " I t is ' unfortu- 1
nately impossible to compare these results with untreated patients ' • -but they wi l l give some idea of the tempo of rehabilitation and'you can judge for yourselves whether you think them good or'bad.
First, I have chosen the results of repair of recurrent^ dislocations of the shoulder. This is a connon injury, particularly^' among parachute jumpers. As the shoulder is immobil! sedfor ' six • weeks routinely after operation, i t gives a good idea of t h e r e * - ^ 1 ^ suits of full time treatment to s t i f f joints. , • ••
SLIDE I - : • r r - r tt -
Results Of iPutti iPlatt repairs for Recurrent Dislocation of Shoulder •
No, Cases Time ünmobllized Tlme at Total time off side -(days) Centre (days)
: (da»s) • : ^--sT
< 61 AO 32 72 ' . ' /-./,
Full abdudtion In a l l cases. , , r
Neact, the results of meniscectanies. Knee injuries are<" by far the commonest single disability seen in Medical Rehabili-" ' tation Units owing to the great amount of sport played,in the'Services.
• • • - - • :- '.v.- .i.T v di i-. . SLIDE I I - -. ' ,
i •--:• / : '• -f-.r ResuJLts of Meniscectomies'. Uncomplicated Cases v.: - •> v^^.t- .
-... . .- - • ' ..--.- • , J V T V v ^ i ^
No. of Patients 1117 Average Time non-effectivè In * ; « / ^ .. Average time f r « other series (days): operation to entry Bonar • 65' - Miriers --< * to M.R.U. 28.7 days Duthie & McLeod $2 - MlnersJ r-V - -
Averagetlme at MBD 28.3 days Bristow 56 - A l l types*. Averagetlmenon- Terhune 50 - A l l types
effective 57 days Maekison 42 - A l l tjtf&r - • Returned to duty IOOJt Lantzounis 38 - A l l types /
-- - - '-.. "' ..-it-: Davs in Hospital •'<
, Under 20 21-30 31-JtO 41 Plus -
Average Time ' 1 ' Non-effective 44 54 62 78 (days) ,.- -• ' ' : ' ,
- The average time given from day of operation-for removal of • the torn cartllege to day of return to f u l l duty is Just over-eight weeks. -./-••.
Thirdly, some results in fractures of the upper limb. ^ , * 22
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
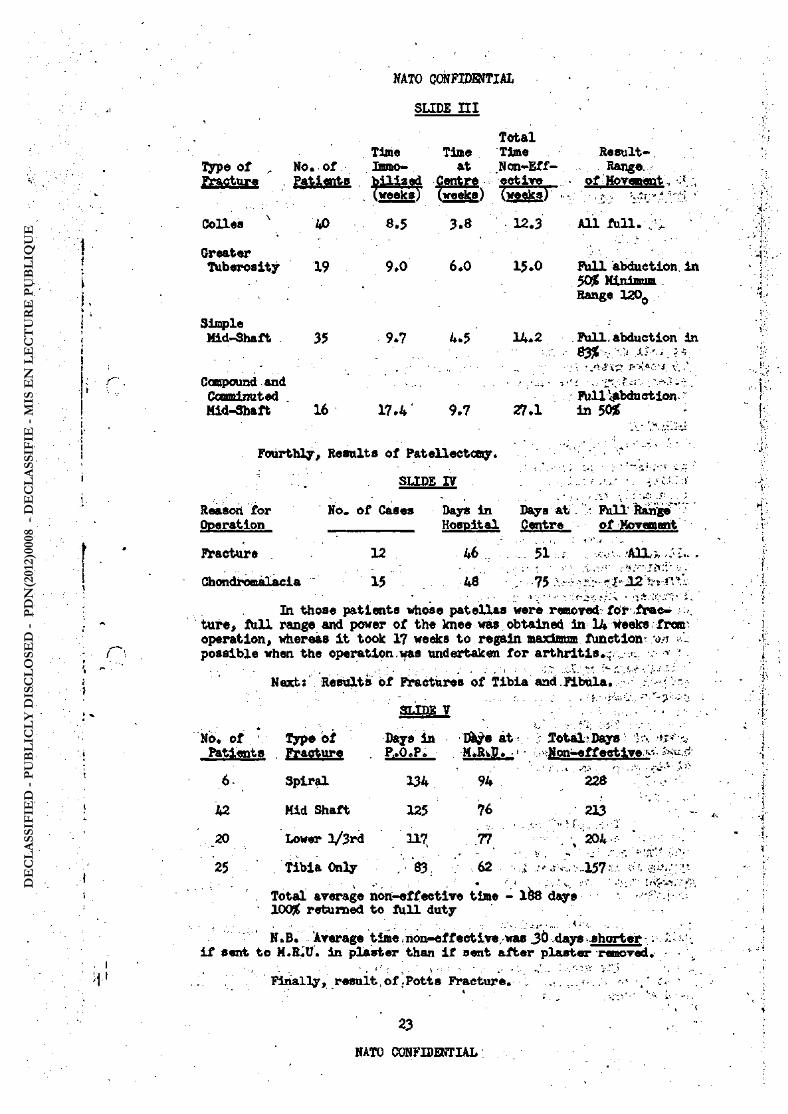
Type of
OoIles
Greater Tuberosity
Simple Hid-Shaft
Compound and Coomiinuted . Mid-Shaft
No. of
PftUflftg
AO
19
35
16
NATO ÇCWFIDSfTIAL
SLIDE n i
Total Time Time Time Lnmo- at Non-Eff-
Iaed Centré ectiTeL
<5 [weeks) (weeks) fwftsksV
8.5 3.8 12.3
9.0
9.7
17.4
6.0
4.5
9.7
15.0
14.2
27.1
Result-Range.
of Movement.
All fü l l . ; : .
FUll abduction, in 50^ Minimum . Range 120o
Full,abduction in 8y% . • s.;-.,
:'•: r- >!4: v.
Fulliabduction in 50$
Fourthly, Results of Patellectomy.
SLIDE IV
Reasoii for Operation
No. of Cases Days in Days at Hospital Centre
Full' Range" of Movement
Fracture .
Chondromalacia
12
15
46
48
51 -, AH ; . - : . .
75 * f J 2 Vt Î'."*.*.
In those patients whose patellae were removed för frac-ture, fu l l rangs and power of the knee was obtained in 14 weeks fran operation, whereas it took 17 weeks to regain maximum function ui --7 possible when the operation was undertaken for arthritis.;; ,.- .>:.. .•• '
Hexbt' Results of Fractures of Tibia and Fibula.
SUDE Y ' ! ^
No. of , v Type of Patients Fracture
6-
42
. 20
25
Spiral
Mid Shaft
Lower l/3rd
Tibia Only
Days in at v ;; 2otal>.Daysl lo. ^ = ^ P,.0.P. MtRiP. -iMoni-effeotive
134 94 228 TT —
125 76 213 ' ..... • ••...'.:•.. ''- f,;.. •
117 77 - ' . , 204 "'V/- ; • . $3 .62 - .i -.v,;.V..157
Total average non-effective time - 1Ö8 days 100$ returned to fu l l duty
N. B. Average time non-effective, was 30 days -shorter - : i f sent to M.B.Ü. in plaster than i f sent after plaster removed.
Finally, resuit of .Potts Fracture. : . . . •••« , '
23
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
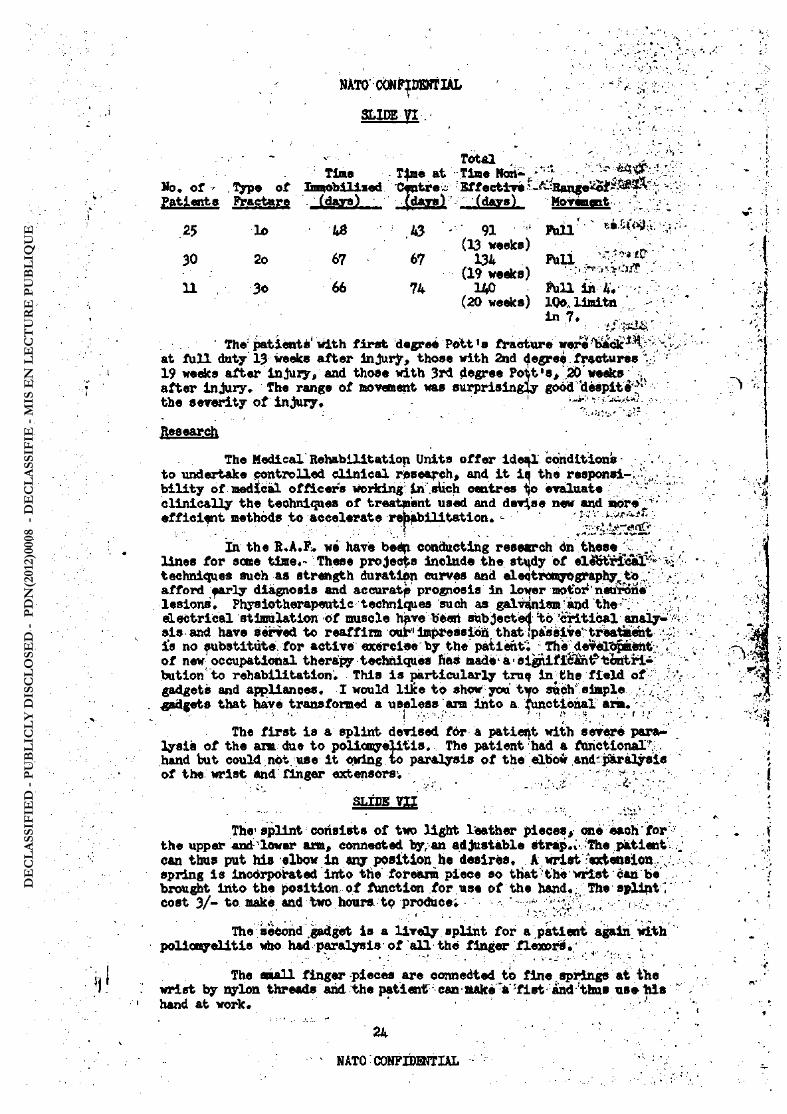
25 lo 48 A3 - 91 A3 (13 weeks)
30 2o 67 67 134
66 (19 weeks)
11 3o 66 74 140
...,- - v.. ' Total • _ , • Tin« TJme at Tiae Nan-./'';*- "
No. of ' TJfpe of Immobilised Centre Effective '-^'Range'^of PatifMts FTactmre (days) . . foj f l , (days) Morwient •
F W l ' '
R a i . '
FViU in 4. . (20 weeks) IOo.. Ilmitn
In 7. ... .
' The patient*'With f i rst degree Pott's fracture were at fu l l duty 13 weeks after InJurjr9 those with 2nd cfegreefractures. 19 weeks after injury, and those with 3rd degree Pott ,s, 20'weeks after injury. The range of movment was surprisingly good 'despite';'1
the severity of injury. 1
Research
The MedicalRehabilitatiop Units off er I de^ condltionb -to undertake controlled clinical research, and it iq the responsi-;^-bility of medical officers woridng In'.stich centres to evaluate clinically the techniques of treatment used and devise new and more',. ' ' ' efficient methods to accelerate rehabilitation. - '.:-'v wr
In the R.A.F» we have beéfi conducting rese«rch dn these lines for some time«- These projects lnolnde the stx;dy of elifctricai^ < techniques such as strength duration curves and eleotixwyography^to / ••. afford early diagnosis and aecuratp prognosis in lower mot'o: neurone lesions. Physiotherapeutic techniques such as galvanism and the •". electrical stimulation of muscle hpve been subjected to 'critical analy-sis and have served to reaffirm oui*1 Impression that fpàssiW treatment ; i's no substitute for active exercleebythepatient, The deveûLt pmènt; . of new occupational therapy techniques fias madea1 al0Üfi£^t?töiitri-butlon to rehabilitation. This i s particularly truq In^ the f ield of gadgets and appliances. I would like to show you tifo such'simple • .. ' gadgets that have transformed a useless arm into a functional arm. . , T •>'••, -S -.-.--. - --. •...'-(• V ••.<•• - • i • •
! • • , ' ' ; • 1 f * i, . T. •- \
The f i rst is a splint devised f6r a patient with severe para-lysis of the arm due to poliomyelitis. The patient had a fttrictionalv , hand but could not. use it owing to paralysis of the elbow and-paralysis of the wrist and: finger extensors, , * -.
• • • ' • . ••••v-"*, -.',-':-SLfDE v u .'
The'splint consists of two light ltother pieces, one each for the upper and lower arm« connected by, an adjustable strap.% The patient can thus put his elbow in any position he désirés. A wrist extension. v spring is incorporated into the forearm piece so that-the'Wrist can be brought into the position of function for use of the hand,; The splint] cost 3/- to make and two hours to produce. ' - : ,- - ,-,./.-
The second gadget is a lively splint for a patient again with poliomyelitis who had paralysis of a l l the finger flexors, ,
The n a i l finger -pieces are connected to fine. springs at the wrist by nylon threads and the patient can aake a 'f ist and thus use M s hand at work,
24
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Apart from research Into physical techniques and auxiliary aids to diagnosis, we are always concerned to improve -the- fac i l i t ies for resettlement of patients that are invalided from.the serriceUjv'B®-, settlement starts as early on in rehabilitation as possible and ré-; training goes hand in hand with physical treatment. Patients thus . ' have a definite goal to work for , and their recovery is hastened. A recent review of 113 patients invalided from one of the Medical Re^ :v habilitation Dnits showed that 107 were in f u l l time employment and their average wage was between.L 3 and 9 a week. . ,
Conclusions .. ••• • 'I ' .. V
. Watson Jones says-'with the right attitude,-of mind^a Surgeon can practice rehabilitation in a barn; without i t , he will. Ta l l In.the most lavishly equipped gymnasium. ' There is no need for complex appar- ' atus, or buildings of architectural beauty. V^ '
The success of rehabilitation depends primarily on the w i l l of the patient to get better quickly. I t is the dutyof a l l members;.': of the rehabilitation team to Inculcate this spirit byan attitude - of n optimism and confidence. I t i s essential that the doctor explains- *!<>•• ' carefully to-the patient and in simple terms exactly what is WronglSnd how he can get better.- The patient should work hard, playjhâi^and ; o thoroughly enjoy himself« The staff should make i t clear toMm that • . they are glad to see him come and glad .to see him -go; .> •:> .-.-Utv- . '
...},' • ..y- • -i.; < . >
Otherfactors of prime importance are the close liaison C- :" between the staff/of the rehabilitation centre and the hospital con-sultants, the transfer of patients to the Centre as early as possible^ and the Interest in each patient as an individual, ' 7 ^
.-. To anyone starting a rehabilitation centre with. only -limit ed- -
funds we, would say, site i t near enough.the hospital to beWithitf easy-reach of consultant opinion but far enough away for the'patient' to' f èe l he is- away frcn hospital} start with' one or two well tralned and enthusiastic physiotherapists and Physical Training Instructorei, and-iuse a » l l t t l e -apparatus and complex gadgets as possible. ,^vW-at^-J
The essence of rehabilitation is that the' patient by-his. exer-tions gets himself better, provided there Is skilled medical- care, an- in -centlve to get better,. and an atmosphere of -happiness, and hope, miracles" wi l l continue to be worked every day. /•'-*•• v
1 * ' r
GENERAL PffiA . -^--VV „ . . . , . • • ' • • . •; :.•- -..- -•> rt:.- . J.-.;,-/, .
General Peras in discussing the paper, said; that although^* • the Armed Forces in Italy had no rehabilitation centre of their own, their were many civilian centres of which perhaps the most famous was the new nOspitale Haggloren in Milan, directed by Professor Lapadari«
However, an Air Force Medical Centre was. shortly to be opened at Desenzaro on Lake Garda and in this centre great importance wi l l be placed on functional and occupational therapy. , --=.
General Pera further developed .a point made in the paper under discussion; that the success of réhabilitation depends primarily on the wi l l to recover of the patient. In the case of a pilot who" has suffered severe injury^ including perhaps the loss of a rlimb, I t i s the general attitude of the patient, determined by his strength of personal-ity which wi l l enable him through compensation or substitutiôn'of his ; re-maining bodily attributes, to.learn to f l y again. •-.-;• -
25 • • '. V : .;
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Medical proceedings are therefore designed to direct the personality and wil l of the patient, and encourage the wil l to over-come physical disability. It is the duty of a l l members of a re-habilitation team to inculcate such a spirit.
— SBOOWD DAY - 5 HAÏ 1955 —
The Chairmanjl General Hall, introduced Lt. Goieral Pierre Brisacj, French Army». Deputy Chief of Staff for Logistics and Adminis-tration, SHAPE,/who opened the second day of the conference as follows.
LT. GENERAL BRISAC
General Brisae said that his duties made him cognizant not only of logistics and medical questions, but he was also concerned with personnel matters. He expected the medical services to find remedies for the personnel losses which we were now attempting to forecast.
A stepping-stone in the study of the effects of nuclear weapons would be crossed at this Conference. During the British Study Period, under the direction of Lt. General Sir Frederick Harris, Exercise "AVERNUS" would be presented—a sinister name conjuring up the infernal manifestations which the future may hold in store*
This peri l 's unparallelled scale already occupied the atten-tion of a l l those who had to cope with i t , and as the delegates here were aware, last ottngfti . biologists of 18 nations met in Rome to study' the effects of radiation on living organisms. Furthermore, the concept of a "National Hedical Service'1 was being developed with the object of mobilizing and uniting within each country the civilian and military medical services, the watertight screens of which were fading before the magnitude of the task to be accomplished, and pooling their resources in personnel, installations, and equipment of a l l sorts.
This task of working out the appropriate methods f e l l to the NATO Medical Committee, which had been functioning since last November and the oreatian of which was a direct result of the wishes expressed by delegates at the 1953 Conference, and of the action taken by the Chaiman at that time, Brigadier General Kennard.
Naturally, this pooling ceased at the fringes of the Forward Zone, which remained under the exclusive responsibility of the military authoritiesi this task, albeit geographically restricted, nevertheless remained a considerable one„ owing to the several determining factors affecting i t : the rate, instantaneousness and simultaneity of casual-ties occurring, the techniques to be applied, as well as the new tac-tical. conditions to be considered owing to both the very extensive dis-persal Imposed by the nuclear threat, and the considerable. Increase in depth which the new "forward strategy" would entail—depth covering the staggering of the troops and increasing their mobility.
In addition to those technical problems, the definitions of which are the delegates alone, there are very many new perspectives opened up for consideration.
General Brlsac closed by depressing his confidence that so many competent hands, Imbued with the same ideal and devoted to the same cause, would initiate research, and would elaborate methods highly advantageous to the preservation of manpower*
26
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
GgfBIAL HALL
( The Chairaui introduced Colonel Victor A. Byrnes, USAF (MC), formerly,director of the Department of Ophthalmology at the •
^School of Aviation Medicine, Randolph Field, Texas, LT. COLONEL BIRMSS
1 Lt. colonel Byrnes pointed out that the t i t l e of his pre-sentation should read "Retinal Effects of Atonic Flash", and not as r was contained in the Agenda, ' '
i Hi proceeded?
The explosion of nuclear devices releases tremendous ' amounts of eh er g y p ï various types. These types IhelUde''the various emanations in different* portions of the electromagnetic energy spefr-trum, Sotte i>t these energies have a limited radius at, the .t iaeof .the detonation; however, the radiant energy in semé portions ofthe 'spéc-trtäf has & large effective radius. These radiations can involve eyes at great distances from a nuclear detonation i f the a i r i s ' elear. C; Retinal hums can be-produced as a result of a combination' of- physical factors. This combination results in the production of these eye V :
lesions at greater distances than any other primary harmful effect of nuclear weapons. The physical factors wi l l be discussed f i r s t and followed by a discussion on the type of lesions produced and, f inal ly of the possible protective measures which can be taken.
- • ' *
'Physical Factors
There are large amounts of ultraviolet, visible and infra--red light emitted at detonation. The effect these have on the retina depends upon their abil ity to penetrate the atmosphere to the eye, - -'their penetration of the eye tissues themselves ,, and the point "at'which HfceSe eaergWa are absorbed into the eye. - ^ v - ' ;
Ultfaviolets This is largely absorbed by the ozone surr-ounding the bombat detonation. The amount that does-get through-this ozone f i l t e r is absorbed as follows* Wavelengths shorter than320 -millimicrons are absorbed by the cornea; those between 320 and 395 millimicrons Are absored by the lens; thus, practieallyno ultraviolet can penetrate the retina. Following cataract extraction thére'would, be seme slight increase in the'hasard to the retina because of the re -moval of the lens, - N • " 'J *
Visible IAahtt Those wavelengths between 400 and 700 mi l l i -microns are transmitted well by the eye as follower
Millimicrons . Percent TVawnri -1¾
400 8.6: , 410 10.6 ; 420 16.0 -430 24.8, 440 31.8 -450 38.8 460 42.6 470 * 43.8 J
480 45.8, 490 48.1 500 49.5 520 52.5
27
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Mllliailcrona Percent Trayaaiagion
540 55.9 560 57.? 500 59.4 600 61.0 620 63.1 640 6/-.9 660 66.4 680 69.0 700 70.5
The average transmission for visible portions of the spectrum is 53.1$. The 46.9$ is absorbed by the cornea, aqueous, lens and vitreous. I t is to be noted that the longer wavelengths are transmitted sanewhat bftter than the shorter ones.
Infrared - Int *ired in the "near visibly", wavelengths is transmitted better tha j the longer wavelength infrared, as follows:
Millimlo i ns Percent Transmission
740 - 71.1 780 71.6 820 71.6 850 72.6 900 69.0 950 ; 53.0
1000 38.Q 1050 29.Q 1100 , 21.0 1150 18.Q 1200 12.0 1250 7.0 1300 4.0 1350 3.0 1400 2.0 1450 and above Less than 1
It can thus be seen that infrared wavelengths from 700 to 1200 millimicrons are of importance. The others penetrate the eye so poorly as to be no real retinal problon.
The wavelengths of radiant energy of Importance from the intraocular standpoint are thus essentially those from 400 4Io 1200 millimicrons .
Sierffir Absorptlmi - The effect of the light energies which reach the retina depends upon the manner of their absorption. Retinal structures are relatively transparent to visible light until the pig-ment layer is reached. At this point most of the light is ^absorbed. Since light is & form of energy, heat is produced in the tissue which absorbs this energy. It is nonspecific thermal effect whieh Is in-dependent of the wavelength of the light Involved. It is produced by the visible as well afl the infrared portion of the spectrum.
It is obvious j, then that the darker the plgnent&tion of the eye, the shorter wil l be the distance in which the energy will be absorbed. Therefore,- the temperature will be higher because the energy is absorbed in a smaller tissue volume. People with darker pigmented fund^ are, therefore, more susceptible to retinal buipis than those individuals with lighter coloured ftandl,
28
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
i .-,-...--.- . • • - . ,-- J - ' Burn threshold» - The total amount of energy required toburn
a retina depends to a large extent upon the length of time in .which i t is delivered. The higher the dose i»ate, the less total energy i s re - . <. quired because heat cannot be effectively dissipated by the retinal .cir -culation. The threshold in pigmented rabbits is 0.14 Gta. calories per square centimetre per second at the retina i f delivered In .less than 1/3^ second. , Slncethe atomic bomb delivers about 35$ 'bf the effective flight - ehergjr ? in the f i r s t 0,001 second, the figures found experimentally are applicable*
Effect.of pupillary diameter. - The total energy level on the rëWna is directly-proportional to the pupillary area. ' %A widely dilated pupil w i l l admit ..over 150 times as much light as a contracted pupil. I t is obvious that tpis factor results in a marked increase in susceptibility of Individuals at n ig l » . ' Since, the pupil constricts relatively slowly in comparison to the,dellvery of radiant energy from an atomic detonation, the pupillary reflex i s of very limited protective v a l u e . / / {<-. -
.-'•?'• i • • -. • • - . . ' • - -- .- r. -f-.': . -'..'...-tA.'-cr / Effect of blink reflex - Since the. average blink reflex-Occurs
in about 0.1 second, i t i s obvious that the protective value 'of this^ . . . physiological reflex is vèry limited. ; •.' '.-.' -. v -- ..
•• • " '.L . - ... ; • '-.- '.-i- ..
Effeçgwf tfie optical system of the eye - The optical syftiln of the eye i s largely responsible for the distribution of the eneTgy .over the surface of the retina I f we assume a normal length eyeball'with a normal optical system,'..since the sun i s always the same distances away, ^ its Image is always the same size on the retina.- The i n t e n s i t y . f l i g h t per unit image area, ^iven a constant pupillary Size j isd«pendent,only upon the absorption of, light in the atmosphere. The image'of an-atonic bomb has an additlonal^varlable factor in that i t may be detonated a t r rf different distaheés from an individual* The amount of light.'.falling;On .. the eye decreases'-Ih accordance with the inverse square law as the^in-dividual gets farther away. However, the area of the -retinal image de- r creases by an idehtiaX'.amonint* Thus, the energy per unit area ln-the, ••' retinal Image remiiins constant regardless of distance exceptfor^the-energy absorbed.in the lnterrening atnosphere. I t is .this optical factor which makes nucii^SfiftpW's such a long distance eye hasard, ^especially at night. ; ., - ,./-. -/, //.-.:¾ :w •.:*.>
.Effebfrof refractive errors ~ ReifVactive errore result in - , distributing the .light ; energy over an area slightly larger than -an'"^: ^ " euro etroplc
eye.'.,,Since.the.human eye has a total dioptric power öf,about. 58 diopters, a.refractive error of several diopterä-resultain.only a-: negligible increase in the size of the retinal image. ; • -
- •"• • "t Si-Ii1- -
v • •'
Experimental Chorioretinal Burn» in'»Rabbits »<i-. - ^ rS V .... : . . - - ..-• .••- ,. .. '
Computations were made on the b&sis of size and intensity of the f i rebal l and the above mentioned threshold, for retinal'bornsl ^They A indicated that -such -bums should be produced In the unprotected human -eye at night to a distance of AO' miles under clear air conditions.' It -was fe lt necessary-to Verify these predictions-'by-actual experimentation. For this reasori TOO pigmented rabbits were obtained. - These were a l l male rabbits weighing between 4 and 6 pounds. It was-essential to ua»jp>ig-mented rabbits because the pignent In their, fundi absorbs radiänt energy In the same manner as does that of a human. These-rabbits were exposed (one time each) during six.different atomic detonations.at the Nevada . Proving Grounds. They .were a l l detonated in the dark under -very clear atmospheric conditions» '
The rabbits, were placed in individual boxes whlfch limited V their head motion« They were aligned to that one visual axis was directed
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
at the approximate location of the detonation. Since a rabbit moves his eyes very l i t t le , no method of eye fixation was required. They were placed in groups at various distances from the detonation point starting at 2 miles and going back in one instance to miles. Alam clocks were set to awaken the rabbits just prior to detonation. In addition,, each group was photographed by the light of the bomb i t -sel f . This was done by a photo-electric timing device which snapped the picture during the f irst 21 milliseconds,, thus recording it be-fore the rabbits could blink. In this manner the animals with closed or shadowed eyes were eliminated from statistical consideration. The animals were examined ophthalmoscopically within the f i rst few hours after the detonation. Retinal burns were identified, described, and then photographed with a fundus camera. Scme animals were sacrificed at once in order to obtain the eyes for study; others were followed for longer periods to determine the subsequent course.
The typical fresh lesion in the rabbit eye as seen with the ophthalmoscope is almost perfectly round, sharply circumscribed and consists of a central and peripheral, zone. In animals exposed near the detonation flash (within approximately 6 miles) one sees a deep central hole with glistening white base which appears to be sclera. Elevated volcano-like margins border this area. There may or may not be hemorr-hage and/or coagulated debris exuding from the hole. Surrounding the CHitral hole is a "halo**-of dirty gray colour, often twice the diameter of the hole. At greater distances from the flash the central area no longer appears to be a hole but Is rather a yell<?wish-white plaque, while the "halo** also diminishes in size with increasing distance until at middle distance i t disappears completely, whereas the plaque per-sists s The remainder of the retina appears entirely normal. Not a l l distances were utilized on a l l shots, and a camera and photo-electric equipment were not available for each station« In addition the photo-electric device failed to trip the shutters at the 28 and 42 mile stations. Fifteen rabbits were located at each of the stations except the very close ones. The rabbits that were sho wiphotographically to have closed eyes at time of detonation were eliminated from statistical consideration» On at least one of thé shots chorioretinal burns were produced in 100$ of the animals at each of the following distances in miles: 4,5,6,7,8,9,10, 12, 13, 14 and 27 miles. At the 27 mile station 4 rabbits had closed eyes, and the other U had well defined chorio-retinal burns. At the 28 mile station, 8 out of 15 rabbits had retinal burns, but since the camera failed tit register i t it not known how many had opened eyes. At the 42.5 mile station, 3 out of 10 rabbits had retinal burns, but again the camera failed to operates so the real per-centage of exposed eyes is not known.
The extent of the microscopic changes in the choroid and re-tina of pigoanted rabbits exposed to atomic flash varied greatly, according to the amount of energy which had been absorbed by the tissues primarily the retinal pigment epithelium and. the choroidal chromato-phores. These histologically visible changes in choroidal and retinal tissues can be divided into two characteristic types?
%
1. Lesions characterized by coagulation necrosis with additional major tissue and cell destruction in retina and choroid. This major tissue destruction is probably produced by explosive intra-cellular and extracellular generation of steam and gaseous expansion.
2. Lesions characterized by coagulation necrosis without major tissue and cell destruction in the retina.
30
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
NAT1O CON FlDENT IAI.
RelatiOfighlp Between Experimental.ftespl&s:,, \ ., in Babbite and Thoae Expected in Humana . V^-VV''^V.
The relative opening of the eye differ« indifferent species. A rabbit eye with wide night pupil, about has about twice, the. re- . lative opening of a human «ye with wide pupil of ten (the nodal -point "is closer to the retina in the rabbit.) Since lrradiance on the retina is s proportional to the square of the relative opening of. the eye,a human eye, if absorption were equal; would require at the cornea, four.times, the lrradiance necessary for a rabbit at the cornea for the production of. a. chorioretinal burn.. . . . , , . , ' -4 '
Pbr the human the. time interval from explosion to 0.15aeconds was utilised in computations. Far the rabbit twice the relative ôpening " of the human eye and time interval fron explosion to 0.25.second was uti-Used because of the slower blink reflex in rabbits* Cto this basis a':20 ^ JCT weapon was computed to produce a retinal born at night under dear air conditions in humans to a distance of ZtO mil4s and in rabbits U9.miles. Since the rabbit figures were well verified in the above reported -experi- ;
, ments, it maybe assumed that the humanestiaatesare quite ac curst ealso, ,
Effect on Vision - The effect on vision will ordinarily, not Mje-'. severe unless the individual is relatively close to the dst«uttiön./,.Vnd«r these circumstances visual loss can be severe. • If the iaage^of theibcmb . falls «n the macular area, central vision will be lostandmaximumjacuity remaining will be 20/200 or that équivalent to peripheral vision.%'The probability that an individual at any reasonable distance, away would be looking directly at a nuclear fireball at the'instant of its detonation is not great* • > . ^ i ' j ^ Ä » -
If the image falls in the peripheral fields, it.will.produe* a peripheral scotoma, the sise d^>endingupon distance> siBe.of;weap9ns,'etc, If it is a s«vsre hurnf it will produce a sector defect by destruction' of , the nerve fibers -overlying the burned area* iv.'.
If'the image of the fireball falls on thei optic, nerveof. one eye (It cannot fall on both simultaneously unless the lftdividual-isi.oonvri'ging) and is severe, complete blindness of that eye may ensue. It is emphasised that it would require a very high intensity bum todo.this.sinoethe nerve head refleots a high percentage of light falling on it..- ^ ^
fyofreeti,?* Derlo-ss - This matter should be oonsldered under two separate headings, the daytime problem and the nighttime problem,.'because they are so different.
' / * r
in the daytime the human has a nail pupil béôùâsë of the hitfi light level. This may reduce the amount of light entering.?«»" sye to , 1/50 of that at night* This alone is a valuable protective device*. ;.&,* addition, if it is desired, the individual can wear rather dense filters and still sse sufficient^ to carry out most necessary tasks,- ; Such,filters . should exclude Infrared and. ultraviolet light entirely since these wave-' lengths are of no assistance in vision.. They can have,a neutral absorp- * tion over the whole visible spectrum or can be restrfctedto a.single / . -portion of the spectrum* If the latter Is considsred desin%le«f the^M ' - • portion selected should bé in the longer wavelengths-(red) i f this i r cam-patible with the-visual task being performed by the,individuAlv,-AThlB is true because of the higher Intensities in the shorter produced.by the very high colour temperature detonations.; ^v-v •
In addition, if the visual task will permit, the indirtdual cui occlude one eye. It is obvious that this san» solution Is applicable to the flash blindness prpblea.
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

The nighttime problem is a much greater one. TheIarger pupil renders the individual much mere susceptible to retinal burns, so the hazard is greater. Li addition, the individual usually cannot discharge his duties i f he wears a f i l ter of adequate density to pro-tect his eyes. If he can perfora adequately with one eye covered, he can at least assure himself of useful function of one eye. I f he can function with monochromatic light (for example, red lighted in-struments or panels) then a f i l te r can be worn to transmit rather high percentages of light in only a narrow spectral band with com-plete absorption of wavelengths. This will effectively decrease the total energy entering the eye in the event of nuclear detonation but may permit an individual to be!quite effective while the f i lters are worn. Again, this is an effective solution in the flash blind-ness problem, especially i f combined with available high intensity light source to be used to illuminate the visual task immediately after de-tonation .
Summary
1. Thermal bums of the retina and choroid can be produced by the radiant energy released by nuclear detonations. They are pro-duced by the visible and near infrared portion of the spectrum.
2» The primary site of the lesion is the pigment layer of the choroid and retina.
3. The diameter of the lesion depends upon the distance from the f irebal l . The severity of the lesion is much greater at near dis-tances because the fluids in the -tie«uea are converted to steam and produce an actual .explosion of the retina.
it, The energy is delivered so rapidly that pupillary and blink reflexes are too slow to prevent the lesion, Protedtive devices to be of any value must be in place before the eyes prior to detonation.
$. Pupillary diameter is very important? thus, the danger is much greater at night.
6. The optical system of the eye prevents the decrease of energy per unit area in the image which occurs elsewhere as a result of the inverse square law. For this reason these retinal burns can be produced farther away than any other primary harmful effect of nuc-lear detonation,
LT. COLONEL BACH * * * * * * * * * *
In the discussion which followed, Lt. Colonel Bach asked, in order to put this type of injury into perspective, how many sufferer» from this lesion were reported after the atomic explosions in Hiro-shima and Nagasaki. Lt. Colonel Byrnes said that as far as he knew, only one case 6f retinal burns was reported after Hiroshima* It was, however, a very small boub by modern standards, and was detonated in bright sunlight. At night, and with people looking in the direction of the banbj the Incidence might haire been considerable.
In replying to another question, Lt, Colonel Byrnes said that observers with unprotected eyes in "pre-dawn" explosions did not suffer burns. Bums in the individuals shown a l l occurred at night.
He said that tmpcrary blindness following the flash lasted only for a matter'of minutes, not longer than 15 minutes and much less as a rule,
32
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

The C airman askad Aether it was tho intœttçn to aupply all ; troops with protective coloured or,tinted glasses,.:/v -Z1Vil
Lt. Colraiel Byrnes replied that tliis. problem wae to be; attacked.-in the light,of the individual's military task. If the time,ôf-Jheieac-^. plosion is known in advance, closing of the eyeswould be sufficient,^, If he could cover one eye, he would be protected. Slncethedangeris1 worse at night, care must be: taken not to npr ot e et M.th e, individu al. so-. -.. much that he becomes a danger to himself and others. -.- -., /•; .-.- . -.
Lt, Colonel Byrnes said that there would te a publication.on this subject in the "Archives of Pphthalmologyn, United States,; within^Aj the. hext .few months. i ;.•,>,% Vi- :,--1¾. »y > fi.-'i?,
....-••. . . . > i ö,s:n.\ Uri GMERAL HALL •-; v~-T--v./'^^r-; I
The Chainiian then introduced Colonel R.G.J. Favre, of the^Ftench/. i Army, Professor of Surgeiy at the Val de Grace Hospital,. /Paris,-..; who -,t gave his presentation as follows j . , , ' V -. /1.- - '
- • ,. i ..-/-,,-.¾. "fr . 1 rf^ Vf
f-S? '
1 -•=' "j " •• •
J - •_•"... " - , ' - . ' . • * . --. •. v:. -. .. -.,--.--. • COLOM&. FAVHE . .< r - '
Shock- Clearing and. Treatment of Voundedi - V -/ Burned. Radiated apd Gassed Casualties^df -aa. À^cfeat
' A* BASIS OF TREATMENT -(THERAPEUT IC OOHCEPTj DIACWOSIS ANB PROGNOSIS) Two definitions,of Shock, Wfiich mutually complete>éâch.»others;.can.:
be offered: one an old but still valid. clinical definition»/. a more modern physiopathological definition.' ; • '•'. :: v'
-.,-. ,.. J . •'•-.- ---- . • • -..•.'/•••-•• •„-..'. • / . • V tJl -A,?!?;.' fi,-, V .. a. Cliiically, shock-Is a syndrome of violent, and serious.course-! »,
affecting an organism aftW> an injury. It is charaeterl*edAby<«';laitial [; decrease in .volume of blood' In circulation, accompanied by lower blood * pressure and faster hea&sat, and toy a state of prostration-., (adynaay). /-This Initial circulation deficiency is rapidly complicatedby anoxia -by, a toxic condition arid by multiple organic defieiencies, espeoially-of > the liver and kidneys. Any one of these factors alone may:oause;. death•,. > : within à few hours» " :..:. , .vx'-j'/ii-'-; //!
b. Fran the physiopathological viewpoint, shock,can/bé defined as : sin upsetting of the haneostatic balance essential to life between /two / .1 Opposing forces, one of which is due to the injury itself,and^the-other-to the defansive reactions of the organiaa struggling against the force« attacking it. The attack may be due to fluid loss, to t stre'ss/Ca' direct depressive effect on the nervous system), or to ap ost-traumat le ; toxico-sis. These factors, characteristic of the attadc itself^constltute.the-: lnlury syndrome. The fluctuating reaction after, the lnjuryj ythe normal defensive reaction of the Injured orgahi«j'alway* -Slmilari whatever the V -nature of the injury, is the reaction pyndrcme. Let us> examine success-ively these two phenomena, which are always assocated nd whose conditions of balance or unbalance will determine whether the -shock-is;'reversible or fatal. -. •••=. .- , .• . zô v,iï^-r .S.-"»- ' -'
. :.-, f! ' »jiM-Xi^ f '»: - ' ..- •
I. - Under the term "injury syndrome", we can group all -the causes-' and symptoms of the traumatic shock. We have said that theseycsnSes can be classified under three headings: .-..
,/---.- 1. Fluid losses -,- • ,,</ 2. Post traumatic toxicoses -. - -,1.-.¾^¾ ' 3. Stress acting directly on the nerve centres , ; . r.. •
- -o-- & J.33 f / ; ''V-';/ T
' NATO. CONFIDENTIAL- : . - ,
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

1. The causes of possible fluid deficiencies are numerous. The condition may be loss of whole blood by external or internal hemorrhage, or i t may be a loss of plasma. This plasma loss may be exclusively external, as in extensive scalding, internal only as in cases of crush injury, or combined as in burns, where the exhania causes exoserosis through the break in the skin and at the same time considerable edona under the burned area.
It has been suggested-that henmorhagic factors be excluded from the discussion of shock. We consider this a serious mistake. No one would, of course, bring up the question of shock in the presence of a massive and violent hemorrhage from a wound of the main carotid artery, since in this case death occurs within a few minutes from loss of blood and the evolutionary phenomenon of shock does not have time to run its course. On the other hand, a wound of the spleen with intra-peritoneal hemorrhage causes a real condition of shock due to the slower, but prolonged, loss of blood.
Honorrhagic shock acts in two ways; f i rst through the direct decrease in the volume of blood, and then by progressive anoxia with its effects on the visceral and organic cellular functions.
However, while blood or plasma fluid loss is one of the chief factors of shock, i t may sometimes be entirely non-existent. We must therefore admit also other« pathogenic theories for this syndrceie.
2. Post-traumatic toxicoses are of two principal types: shocks due to removal of a tourniquet and those due to the resorption of the products of proteolysis,
a. The theory of shock Induced by the removal of a tourniquet is of very long standing and was rejuvenated during the last war as a result of -fi* studies on shock following crush injury.
b. The resorption of the products of tissue proteolysis has been known to be a factor of delayed shock since Quern's reports in 1917. This proteolysis may be due to mechanical devitalization (crushing, , ischemia) or to infectious devitalization (myositis or cellulities caused by aerobic or anaerobic^germs).
* The release of the products of proteolysis into the blood stream after re=-establishment of circulation is the basic factor of shock arising frcm the removal of a tourniquet or the relief of a' crushed condition.
This old theory of toxicosis has recently been revived, but what was originally attributed to toxicosis is in reality due to the release of three types of nerve-centre depressing faetorss
1. Acidosis resulting from the acid products of anoxic proteo-lysis in the Krebs cycle
%
2. Hyperhistaminemia due to anoxia of Uie tissues. As a choli-nergic factor, hystamlnemla tends to produce a vasoplegia, hyperemia (hyper exudation) and infarction.
3. Hyperkalemia induced by cellular damage*
However, while vasoplegia or vasoparalysis and excessive capillary permeability due to the cholingeric effects of histamine, and proteolytic acidosis, are undoubtedly factors of shock, they are not constant. This toxic theory therefore doss not explain a l l cases of shock.
3U
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

3. This is one of the reasons for the present-tendency:to go back to the nerve theory of shocks Cannon's f irst theory has bean revived and bJiOught up to date by the recent research of Reilly on the part played by the sympathetic syst an In shock, and by Seyle and Laborlt on the' part played by the neuro-endocrine system. ' ' V- --«• • Oi; .
These factors of vasomotor balance are directly disturbed by'the depressive effect of the stress conducted to the dieneephalon and to-the . floor of the third ventricle by the sensitive centripetal fibers o f the sympathetic and parasympathetic nerve sys t « . Ve have already mentioned that the vital brain centres can be indirectly depressed by the reper- j
cussion of anoxia, fluid losses or toxic factors of tissue;destruction of traumatic or infectious origin on the neuro-endocrine system.-
Although the physiologists may be tod prone to distinguish between these different factors of shock, the clinical physician is . generally faced by an association of these three factors, acting êithèr successively or simultaneously. Btt fact, a wounded man is subject, to a l l three of these causes of shock within the space of a few hours'* At the onset, he undergoes the Initial shock due to the depressive attack on his sensorimotor system and of his psychosomatic .balance (nerve shock, initial shock or "sharp shock"). His injuries then cause-the shock due' to fluid loss and later, the anoxic proteolysis of the devitalised tissue of the wound also take effect (toxic or recurrent shock*) /
However, in spite of the fact that the factors involved in this injury syndrome are numerous and variable-, the reaction of thè organis» to the attack is always the same, whatever the cause of the disturbance ; may be. 'V-.' ' '*•'.
I I . The reaction syndrome of the injured Organism jIikealI-Iife phenomena, runs a sinusoid, or sine-wave course. This has been described' by Laborit under the term "fluctuating post-traumatic reaction" (in' French: "Reaction Oscillante Post-Aggressive", abbreviated to' ROPA, l iteral trans-lation: Post Aggressive Oscillating Reaction".) -i ^ ' . - : - % . .
1. Cannon ' s Hcmeoatatic Balance ' '*"•'•"'" J-'"':^
In its normal state, the organisé lives-in a lsohdition *6f hemeostatic balance, in accordance with Claude rBernard's great law df-the biological constancy of the inner organiem. This homeidstAsi8> so thoroughly studied by Cannon, was shown to be the result of the oscillating inter-action between two very distinct systems governing the l i f e of organisms, '' the organs of vegetative or autonomic l i f e and Uie organs of relation or related function.
The vegetative organs are those which ensure that the organiem continues to live in .the state of rest; They are-essentially the f i l l ing, covering and storing tissues, the organs of nutrition (liver, digestive tract, pancreas and thyroid gland) and of evacuation (kidneys). The vital balance is , as we know, a compromise between the phenomena of absorption * and storage, that is of anabolism, and the phenomena of combustion'and elimination, or of catabolism. These opposing phenomena are'kept in har-monious balance by a neuro-endocrlne control mechanism, the hypophyso-thyrsoi-àdrenocortical, acting through the balanced secretion' of glucocor-ticoid and mineralocorticoid, scmatropic and gonadic ahabollzlng hormones and ACTH and cortisone catabollzlng hormones*
The organs of the l i f e of relationship are those Which enable the organism to fight for its l i f e by struggling or retreating when attacked*' They are, essentially, the brain, themuseles^the heartand the lungs. Ih fact, in the-higher animals, this neuromotor complex utilises
35
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

a l l the energy created and st .racJ by the organs of relationship. This massive and powerful utilization i s accomplished by means of medullo-adrenal secretion. An example selected by Cannon to illustrate this theory is that of a cat confronted by a dog. When attacked, the cat mobilizes its adreno-sympathetic system, as evidenced by i ts pilomotor erection, i ts pupplllary-dilatation, i ts tachycardia and polynea. Trueta demonstrated by an ingenious and complex technique, in 1950, that a gmeralized vasoconstriction and an adrenocortical shift took place in the animal at that time - an entire mechanism set up in order to enable i t to escape or to fight the dog. But this intense u t i l i -zation of energy resources is a great strain on the organism. It Is a break in the homeostatic balance necessary for l i f e .
Let us examine a l i t t l e more closely hew this upset of balance = a factor of shock, takes p^ace.
2. The Upset of the Homeostatic Balance
a. The hrpophyso^t.hyyeo-adrenocqrt,ical shift
In cases of violent need of energy, priority of cata-bollsm over anaboHsm' is obtained by means of a hypophysc-thyreo-adreno-cortical shift (Slides 1 and 2) set in motion by adrenalin secretion in the vagus ttataugh a nicotinic effect on the suprarenal medulla. Prom that instant, the somatropi£ hormone and the gonad~atimulating hormones are no longer secreted, but, on the contrary, ACTH, cortisone and thyro-stimulin reach a peak': of hyper-s«cr«tion. These catabolizing hormones provide the locomotor syston with an additional mass Bupply of glucose. This cortisonic hyperglycemia is due to a triple factor; insulinlc glycogenosis, cortisonic neoglycogenesis and thyroid hyperglyconenolysis accompanied by an increase in basal metabolism,
b. Prefermtial irrigation of the neuromotor mechanism
At the same time as the adrenal-medulla secretes adrenalin (epineprhine) for neuroendocrine effect, i t also secretes noradrenalin (norepineprine or sympathin E) or vasoconstrictive effect* This vasocon-striction acts on the irrigation of a l l the elements of vegetative or trophic l i f e . But i t dees not affect the l i f e elements of relation. The brain,, heart, lnngs and mus^lts receive preferential irrigation at that time. It is d i f f icu lt , sometimes, not to go too far , but i t is evident that in this case nature puts a l l she has into the fight by the creation and vascular delivery of factors of energy, and this preferential circu-lation continues right up to the preagonic phase, as the organism stakes everything on the outcome of the struggle. It i s this tragic obstinacy in fighting which completes the upset of the homeostatic balance, because, during this entire countershock phase, the organs of vegetative l i f e suffer damage on the cellular plane and on the general plane.
On the cellular plans, a series of phe&cmetaa occur which repldly become serious! ancxia, acidosis by destruction of glucides and lipids in areas poorly supplied with oxygen, leading to the production of keto-genous and acidulous dér iva t i f s (hence the seriousness of the catabolism of the cycle of creation and destruction of gluclâe, or cycle of Krebs, in a state of anaerobiosis)s depolarization of the c«l lular membrane, which loses its selective role with a loss of potassium and overloading of the protoplasm with sodium and fluids causing edema; and a tendency toward the pre-agonic thermodynamic level by exhaustion of the bio~energetic re -serves of the cel ls .
Cn the general plsme.:, the establishment of unbalanced circu-lation, as shown in the diagrams of Chambers and Zweifach, and the adrenocortical cutoff of Trueta. The unbalanced hydroelectrolysis of the Intracellular f luid is manifested in the exfcasa cellular fluids by hyperkalemia, hyponatremia and acidosis. N«arc-hormonal exhaustion of the thyroadrenal countershock system and visceral exhaustion of the biological energy stocks gradually set in, with pre-agonic hypoglycemia
36
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
fpllowing the initial hyperglycemia of the reaction stage." '"
The cellular and visceral deficiericyis." aggravated in turn by the circulatory Insufficiency,creatihg'a vicious*cycle(Moon's cyOle) ^ from which the organism at bay can no' longer merge alive'. . . - !
It may therefore be said that there are two types of. hcmeo- . static unbalance:
a. The jha ponious reaction, with spontaneous return to • hcmeostatic balance when, the Or^nian is capabla'of footing the bill for the damage sustained in the struggle against .the attacki : This is compensated or reversible shock, and it is.benign. , , , / T :
b. The disharmonious reaction, ending iir death ;ty exhaustion of the organism in the unequal straggle. This is. uncompensated or irre-versible shock, and it is fatal. . . ' V . ^
(reu»1 - J1Sti-Ki '-Iiorn * . ^O "'S. ' "'_' '.'•• (Four slides were then shown, as follows t )
SUDE I .- ' V'--- . --1
v This shows the first phase of shock. At the top you' see the ; three kinds of attackt Sensory Shock, loss of fluids, and' lnfectldu^ ; toxicosis, (represented by lightning flashes). I have'âej ctW tfcfcm'Ç r acting directly on the cortex and also on the nuclei of the third-vveS^ tricle and of the medulla oblongata.. , , ^ • ' ,-
This 'StAss depression will cause two other phenomena. The first of.JUtese, which I have shown at the left, is a parasympathetic phenttaena frcn the floor of the third ventricle, causing hypothermia, hypoglycemia, metabolic failure and polyuria. '/-. ,,,-..- ..
. ' ' ' - ' • ' / /
At the same time you see vasodilation, plasmatic^exudation and cardiorespiratory depression appearing through the v&gal rcttte,. (marked, with an X). • ' ; ' - -"
'!•••/• ti. Fortuttateily for the attacked organism, however the!-Vagalirfe1J. : phenomenon will, by a rvärkable nicotinic effect, csuse a hypersecretion in the suprarenal »edulla, producing adrenalin (epineprhine), Idiich is the starting point of the oeunterahock reaction. - ,':1 : '
i ;
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
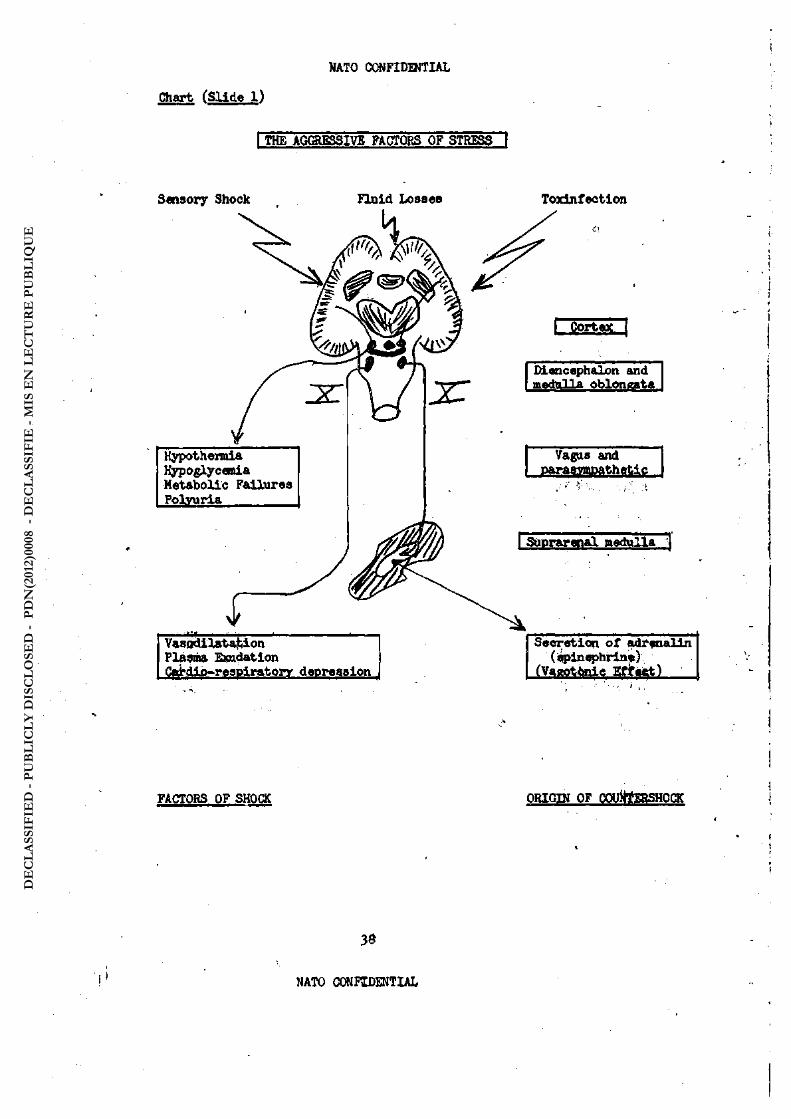
Chart (Slide 1)
I THE AGGRESSIVE FACTORS OF STRESS 1
Sensory Shock FInid Losses Toxinfection
Hypothermia Hypoglycemia Metabolic Failures Polyuria
Vasodilatation PlÀSma Exudation Cffictip-respiratory depression
I j
Diencephalon and itiart iift oblongata
Vagus and parasympathetic
i-' ' >;• ••
I Suprarenal medulla"^
Secretion of adrenalin (epinephrine)
(Vagotonic Effect)
FACTORS OF SHOCK ORIGIN OF OOtritfEBSHOCK
30
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

SLIDE I I
Here Is the counter shock reaction, which begins, ' a tthetop, with the adrenalin attack. It is now known that adrenalin i snot a single substance, but that there are two substances: noradrenalin and adrenalin , (or norepinephrine and spinsprine).o -Noradrenalin operates under 'the, / ort ho sympathetic system and, as a phenomenon of reaction, i t automatically causes vasoconstriction, stops the plasma exudation and decreases,-the . production of heparin, resulting in increased blood coagulation, greater " cardiopulmonary activity and contraction of .the spleen, as has now been known for quite some time.,
As for the adrenalin, i t has a neuroendocrine action (top „ i right*) - It operates upon the anterior pituitary lobe, which» aV;Ve"*v-J'--\ I saw'just now,-has either an anabolic, constructive secretionor a1'"cata-V , bo11c, destructive secretion in order to give the organism endugh !
glucides to make a fight* i, ... „...J : .... . . - 1
f • '.•-. -i " Thus, there is a shift phenomenon in shock. ' • j '
The pituitary completely stops the secretion of the anabolic-hormones, scmatotrophin and the gonad hormones, and reltas W > a " p e a k ° ) promotion of catabolic hormones In the form of thyrostiaulin.flThis acts upon the thyroid and automatically Increases the basal metabolism and .s: therefore combustion of glucides. ;i /' !".
•••'•''• • •• • • -• • - •-. - Y' ' • • Ey means of the adrenocorticotropic hormone (ACTH) f the pituit-
- ary acts upon the adrenal cortex, the souroe of cortisone, which pro-duces glucidal hypermetabolism. The countershock process therefore causes vasoconstriction to strengthen the falling circuletion.and also, gives the tissues additional glucides to enable .theorgani«*tà9,^figbt.,~v_ -
.. j . Is./ j/H/.WfOO'i«»
• . / . .' ..•' .. .-• i>. ;.;•-< i i
. : - - r •
W . -.-
. •' ï
^ F-i
39 DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
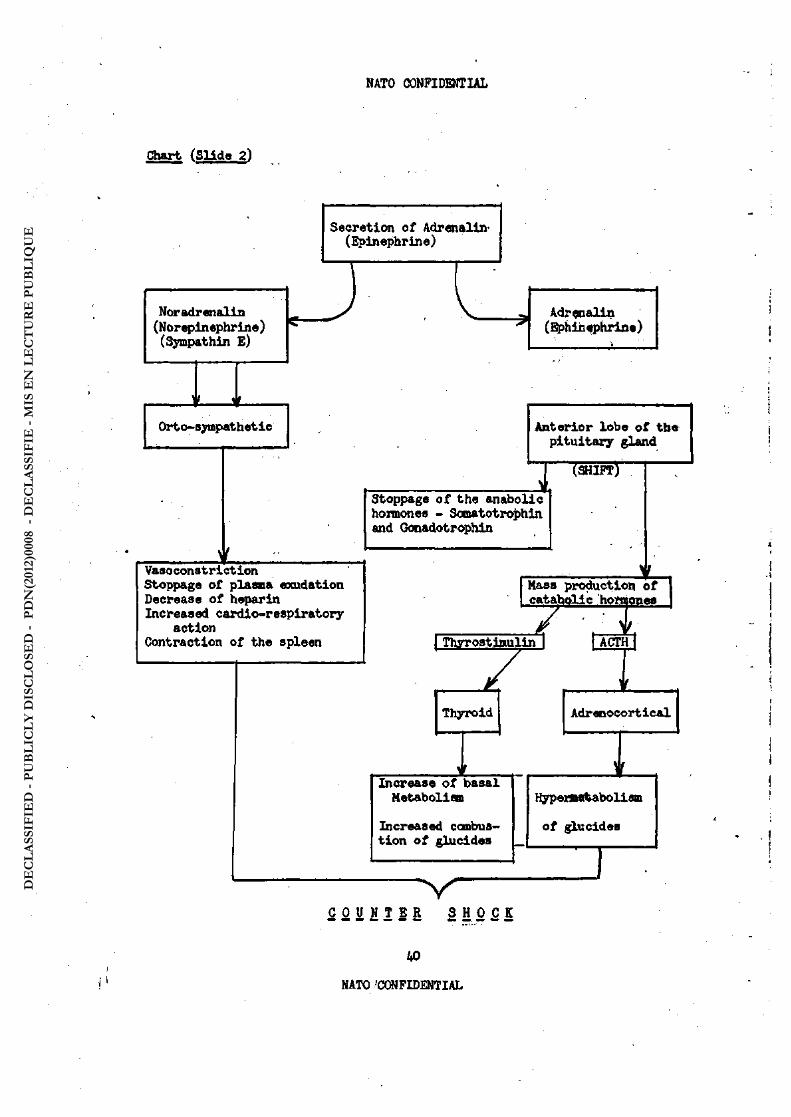
Chart (Slide 2)
Secretion of Adrenalin' (Epinephrine)
Noradrenalin (Norepinephrine) (Sympathin E)
t
Orto-sympathetic
Adrenalin (Bphinfphrine)
Anterior lobe of the pituitary gland
(SHIFT)
Stoppage of the anabolic hormones - Somatotrophin and Gonadotrophin
Vasoconstriction Stoppage of plasma exudation Decrease of heparin Increased cardio-resplratory
action Contraction of the spleen \ Thrrostiaulln I
Mass production of catabollc hormones /
Thyroid Adrenocortical
Increase of basal Metabolism
Increased combus-tion of glucides
Hypenwtabolism
of glucides
-sV "
C O U N T E R S H O C K
kO
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
SLIDE I I I
Here, fop example/is what occurs in a turned area. It is Interesting because, as I believe I have shown here, the phenomena occur In the vasomotor systaa. ^ ^
When there is a1thermal attack upon the tissues,' shown on the le f t , the burns are of the Ist , 2nd and 3rd degrees and th e under- .'• lying vasomotor, system is also affected. This is known as'the\,v • Chanbers-Trueta reaction. Tou will note that.owing to the adrenalin reaction,1 the entire arterial and arteriolary system as state, of ; ,..' . vasoconstriction. The metarterioles contract and, closed aid thereon»:', tractile capillary wall cells (Rouget cells) also close.j Thié caases ^i, stress in the' capillary ansa, and as. there is now no^ciwrnlatiw^l^ through the capillaries, it goes through the arteriovenous "shuri underneath. The blood therefore flows almost directly from .the « r - . .
teries Into the veina. At the same time, the capillary ansa,* wi l l .;.: suffer, as they ai'e no longer sufficiently supplied to maintain. their vascularity* This causes hyperhistamlneiia of the affectfed1 . ; . , :.. tissues and a resulting increase of plasmatic exudation'or eocoserosis. At this stage, as you see (top right), the lympatic^system.-is ;ccat-v, \ , pletely blocked, which is why. there is oedecaa. 'On théjpther .hand , ' . you see the lympatic system working again' in burn casesafters ix days. The arteriolarand capillary contraction' (vascullar spasm)^has-disappeared
• and the circulation Is how no longer through the arteriovenous ^shunts" • but Is beginning to take place normally .throu gh the capillaries. This
explains why large quantities of replacement fluid should no lotiger bê given in burn cases after the fourth'day, as not only has. the circulation returned to normal, with a cessation of exudation, but all [the edfcuas have also been reabsorbed. The electrolyte (sodium), diposit*, .1 » instance, are reabsorbed, and after the fourth day the*> drgânÏÂ^ saturated. That is why extreme caution In adadnisteririgllquidS-is nece-ssary, in burn casés after the fourth day, ; ? " 'if7' î *"
• " • ; . . . ' .• ••:•'.'':, --1 . L- . .i
' - - , y • ' •;•• ; : --/
1 / . ^ - ( . •
••tr" • '.S -, .-
I
1 . • • j
Al
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Chart fSlidto 3)
D.« E3EzäaV.cei phass
Opaâ Euraa
2. RESOKPTxCW IHASE
- '42
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
SLIDE IV
Gn this last sl id«, I have attempted to materialize the - .. area of homeostasis in which the human organisa can live. The centre line is the hcmeostatlc balance line between sxftbollsm and catabolism, and the hatched areas on each side of the homeostasis -strip are the fatal states of unbalance in which the patient dies.' -At the onset of the Injury to the organism, we see the initial vagal shock, which, i f too violent, crosses the outer limit of homeostasis and results in immediate death. But when the organism is capable of reacting, it checks the vagal descent by a- swift up- -ward swing to the catabolic side of the balance line. Here again,, i f this catabolism curve goes too far - Iiks an automobile driver ' -who Ijerks his steering *heel to far in 1Uie effort to keep 'out of the right hand ditch and meets with disaster on the le f t aide ofV ' the road - delayed but inevitable death may result, because the reaction was too strong, - r -
A third cause of death is when the organism; in its ob-stinate struggle against the aggression, has produced and continues to produce an enoîmous secretion of adrenalin.' After a certain per-iod of time, the organism exhausts a l l its reserves and the result i s fatal delayed shock, - death by exhaustion.. r;,-, . [ . -
However, when Uie fluctuation of the reaction shock syn-drome is within harmonious limits, after the phasê of defnnsive^ catabolism
comes a phase of anaboliam, as in a l l the sinusoidal : , reactions of living matter: the organism regains its hcÄeostatlc ;
balance and the shock is cured.
43
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Chart fSlide k)
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

.. - B. DIFFKKEMT TYP^ OF SHOCK AND CLEARING OF CASUALTIES V ...: f, : .1 - .. On'the basis of the above mentioned facts, it is possible to distinguish clinical foms of Shockfl differing in course and in . etiology* These.considerations will enable us to carry out the sur-g i t ^ clwapce afid.assorting of these different conditions of shock* .
• ;..•,. , Fbms Accordinft to Course
•'.'• r ^ . - v iPriataryj or Inoaediate Shock - is rarely encountered except at the place where the injury occurs. It is the shock incurred on the
; battlefield, the maximum form of traumatic shock. It is the shock of .. /ths;operating room, the classic form of operational shock. This shock,
owing to; the immediate seriousness of the injury syndrome, places the organism-in danger of immediate death. These cases are extremely urgent.,, > ,..-, . -. , ' , - , . '
f Compensated Shock - is the type with which the doctors and surgsons of the forward area have most to deal. It is the state of shock of tho wounded, who, at least'temporarily, are paying the cost of the fight against the injury and are making the adjustment more or less-satisfactorily, but this condition of countershock ,1s always
' liable to be an upset of balance. They are priority casualties.
, ' Uncompensated Shock - appears when, after a phase of efficient . reaction, ;the organism .reaches the end of its resources, in the terminal ' phase.of exhaustion. Another type of uncompensated shock is character- ,
ized ^ t h ë reappearance of the state of shock after phases of relaxation ; due 'to adequate treatment.' This recurrent shock 'is always extremely
serious. 'Because of the danger of lmnediate death, these uncompensated -• shock, casualties are emergency cases.
. . .,...- I I . Forms According to Origin V -UvS
i=Sf^-' V ^ V "
'irk v.-. v-Traqmatlc In.-tyfr shock i s th^ most common and best known-form -.
i,.of shock. -W^have already mentioned the three pathogenic types i shock ^toxic shock frcm release of tourniquet or crush or from
- toxi-infectioue proteolysis, and nerve shock by stress acting directly -on, the «dieneephalon. . From the clearance point of view, degrees of
; j»ri«rity "and emergency will be assigned according to the course fom of ^the shocik and . its state of compensation or unCompensationf or relative
• reversibility, as we have indicated before. ' V y-', ' - Bum shock presents some special characteristics. According to . "theiwursepf the Ieaionsi, we have a succession of shock factors.' After ' 6 to S hours, a state of shock due to plasma loss appears, the pathogenic effect.^appearing only after this free interval, and at the end of the first-or. beginning of the second day a delayed toxic shock appears. •'• V-. ^V" v.". • U . v . ' ! •• ^^ - However, in addition to these course types of shock, there are
^^ollnical a^ects' peculiar to each etiological type of bums : • In pure heat buyps. associated .lesions of the upper respiratory
.tract..will add the immediately and subsequently serious complications which lesions .of-the air way always cause. Spamn of the larnyx or edema and purulent mîcous hypersecretion in the nose, pharynx, trachea or bronchi may be an early source of asphyxia making neoessary broncho-aspiration or mnergency tracheotomy.
''' • In Chemical Burns, toxic phenomena frequently add to the lesions of the enveloping tissue. .While the chemical intoxication is delayed in
''-V- 45
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
the case of phosphorus burns, the same is not true in the case of napalm burns, where the carbon-monoxide poisoning must be urgently treated by bleeding with or without blood transfusiony mass administration of oxygen and oxygenocarbogenotherapy. In gassed cases, general treatment of toxi-cosis o r o f t h e upper respiratory tract Is also a factor of emergency.
In Atomic Bums0 hematological and reticuloendothelial lesions are not energency factors influencing clearance^ but they call for the routing of such radiated casualties to the specialized centre. On the .other hand, the actual condition of the wounds or burns i s a factor which must be immediately considered in the clearance of multiple-injury casual-t ies, who may be wounded, burned and radiated-at the suite time. Gwierally speaking, every nrrltiple-in Jured or multiple wounded casualty i s an emer-
'gency case. . ,
/ GasiShock includes a considerable variety of emergency types. Suffocation iä a factor of extreme emergency because of the danger of lniaediate death by severe lesionas of the lungs and fai lure of the right heart .associated with pulmonary edema. Baergency handling may be Justified by the injury i t se l f , or i t may depend on whether the toxicosis is of the quick-acting type (Trilon or Tabun) or delayed lacrlmators and lung i r r i -• tants.
• "'-C. TREATMENT OF SHOOC
:' -., ; • I . Therapeutic Methods and Results
r ; ' . In order4.not to be merely symptomatic and fatally Incomplete, shock treatment must have two objectives: treat the injury syndrcme and at the same time treat the reaction syndrome. These two objectives must be aimed at" simultaneously.
1. Treatment of the InlIury Syndrome
• ,\/- In treating the injury syndrome, the immediate causes of the 'shock,pust,first be attacked. Ccmbat hemorrhage by temporary hemostatic P^ocedtures ' such as a tourniquet, or f inal hemostasia - when possible at the outset - e.g. surgical honostasis. Combat pain by immobilizing the Injured ideas' and administering from the f u l l resources of pain-killers„ Combat the dangers of toxic resorption by avoiding sudden release of tourniquets, using pressure therapy in cases of crush Injury, or Allen 's local re-
"frlgeration method in cases of devitalized limbs. Combat stress propagation towards the diencephalic centres, either by stopping the centripetal nerve transmission by general sedatives, infiltration of novocain in the main nerve trunks and regional sympathetic centres, or by putting these centres at test by Astrakian's method of induced sleep (In which case barbiturates perform a function similar to that of Laborlt's hibernation therapy.)
In combatting the injury syndrome, i t I s not sufficient to e l i - . . ainate'the causes, Iwt the symptomatic manifestations must also be de-creased. Al l transfusion methods must be used to offset the deficit in circulating blood. You are perfectly familiar with the utilization, ad-vantages and disadvantages of the various replacement f luids:
- /'•'•"-'?• /Fresh, Whole booda and especially stored blood, i s almost constant in effectivenesss but i t i s di f f icult to maintain a large reserve stock,' and i t can only be preserved for a few days, in spite of numerous technical Improvements.'.-The' US Medical Service has devised remarkably equipped refrigerator tracks, at regiment level. - , ' . \ - ' , . , ' • b. Human plasma is easier to store, and a l l blood groups can contribute.~'Dried plasma can'easily be preserved for several years, but, unfortunately, its action is less complete than that of blood. Also, the
A6
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

recent occurrence of .epidemic viral jaundice bas cooled.down the en-thusiasm inspired by the f i r s t mass tests.
Ct Large-molecule plasma substitutes are more indicated. The , so-called physiological or isotonic saline solutions have not been used any more^for--Scme time.' An organism affect edby a severe loss of blood is In-
1 «apablsiof retaining these solutions andthey are also a factor of tissular edana. 'In order to obtain plasma substitutes which can be retained in iCir-culating blood, i t i s necessary to use maercuolecular fluids having a mole» cular weight similar to that of serum albumin. These large moeleules are leas^easily eliminated through the hi^ily permeable capillary walls. Serums containing large glucide or protein, molecules are now in general use. Al= though not as efficient as blootf Or plasma, these replacement products are undoubtedly-effective in re-eStabllshing the telnrne of blood in circulation. This is-the most Important thing In shock treatment. The body can l ive in a reduced -corpuscle comit (1 to 1½ million)., but i t cannot he so easily . tolerated in a "reduction of 'thê f luid volmtaé. These very effective methods are one-of the fing things learned in the medical f ie ld from the last "World War. But the re-establishment of the circulating blood volume i s not, enough* The other shock symptoms must also be fought. Anoxia must be countered by mass 'BdmlniBtration of oxygen. Acidosis must be countered by means of a l -kaline solutions.. SLectroIytic disorders must be remedied by the Introduction of solutions rich In sodium or chlorides. Cold must be combat ted by wanning with'care to avoid peripheral vaso-dilation of themio. origin. Low blood''' pressure must-be'remedied by acting upon the arterial tension regulating'centre by infiltration of novocain-in the cartoid sinus, as proposed by Wilmoth -and Leger,. _
« Al l these methods have amply proved their efficiency. . HoweversAo ,: brlhg^the-patieut successfully cut of the " infernal cycle" described by -Moon^in cases-of uncompensated or reversible shock, the treatment of the injury syndrome must be accompanied by therapeutics intended to offset the reaction: syndrome, the 'second element in the twofold menace of shock, ;-r.ci
2, treatment of the Reaction Syndrome
mythod: Strengthening the countershock reaction ---.-.-}. ^ir a." , ; - . ,--.,-,--- .
?.»«?.. • - "The reaction, syndrome is , as we.jaäve said, the struggle of-Jdigr. body it8elf again8t thèraggres8iona thespontaneous manifestations of cauintj^r-shock activity.' . I t would'then seem logical 'to support the organism in this reaction, to reinforce i t and puBh i t in the same reactional direction.
" Vaso—constriction is the process of compensation to Offsett^the decrease in'^he volme of blood In circulation, and, with i ts preferential circulations for the neuromotor system, i t is also a process favoring the coneervation of the' encephalic and cardlo-pulmonary centres. I t therefore appeared logical to try to increase this vasoconstriction. This Idea was
-responsible-for*thr custon of using vascular analeptics in shock treatment. Adrenalin, -advocated sci strongly by Levouf1, and more recently noradrenalin, adrenocortical -extracts'"and ascorbic acid. We also used these Yasoconatrifc= tors, as'did so many others, with unquestionsfi sucsess sometimes, and yet they can be dangerous, as we wi l l show.
•' '' -- Thefover-functioning of the hypoQhysodlencephalic centres is'-necessary *tO;bring into play the hypercata^plic shift . I t - i s therefore logloal~to-use-central analeptics, such as strychnine, reccnmended in strong doses -by Petlt-Äitalllis^ Lobeline answers the same purpose.
•*:.' Then the discovery of ACTH and cortisone, major cataboll2ing homones j had as a corollary their use in traumatic shock to produce maximum increase, at their endocrine scurces, in the hypermetabolic phenomena- of the
- ' ' -
47
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
hyperphysoadranocortical shift. Bat after a period of enthusiasm, almost a l l the authors began to apply the soft pedal* Among other ; drawbacks, which we wi l l mention later, cortisone greatly favors the processes of infection, which is an all-Important drawback in the case of war, casualties in imoinent danger of mass infection*
:.. -,S The chief objection which can be made to these methods of increasing the spontaneous defensive reaction of the organism is that, while they strengthen the beneficent side of the processes of correction, such as vasoconstriction, tending to reestablish the a l -tered- circulation, they, also increase the dangers by doing so. The disordered expenditures of the organism, tissular and visceral anoxia and adrenocortical exclusion, cannot be prolonged with impunity.
We have a l l had "triumphant resuscitations" - followed from four to six days later, by death from anuria due to anoxic neph-rosis of the kidneys. The effect of these methods can be compared to the stroke-of a whip.applied to horse which has fallen in exhaus-tion. He either{gets ùp in a last desperate effort, or he dies of com-plete exhaustion while making this last effort*
. ., b. New Method j Elimination of the Countershock Reaction
.- > .; -V > A different concept of treatmmt, simultaneous with ^ the action against .the injury syndrome, aims at the élimination of the-counter .reaction in order to avoid its dangerous consequences for the homeostatic balance* I refer to the hibernation therapy of Laborit and Huguenard*
, , , - • ^This -method i s based on the combined use of lytic drugs and of low«iigvthe patient's temperature. The drugs constitute a mixture of which.has-been applied the slang term ltIytic cocktail.1* This pharmaco-dynamic: coipcKund consists chiefly of euypatholytics, vagolytics and anti-histamines*., The total
suppresses a l l action of the chmical media of propogation of the nerve current. This offers a vast f ield of pharmaco-logical action.
Largactyl and phenergan have a cortical and mesencephalic hypnotic effect on the brain centres* These drugs also act on the dien-cephalon and the pituitary body giving a "vacation" to the system regu-lating thermogenesis and neuro -hormonal, hypophysothyreoadrenocortiçal homeostasis.
There is a three-way action on the vasomotor system. The sympatholytics suppress vasoconstriction, the vasolytics prevent init ial
. vasoparalysis inhibition, and the antihistamines avoid the closing of the cotttraetible capillary wall cells (Rouget oells) and also capillary hyper-permeability.
Ih i ts effect on the eel l , largactyl re-established the Btoobrane potential, which permits i t to recharge with potassium and the return to normal of the blood and cellular potassium content, with die-charge of water and sodium from the cells.
In other words, a l l the serious phenomena afflicting the autonomic or^vegetative :life system due to the post-aggressive reaction are eliminated. That is , of course, accomplished at the expense of the activity.of„the related l i f e system. Moreever, the suppression of the hypophyso-diemcephalis thermostat enables the body tmperature to be lowered without danger (to 30 or 32 degrees Centigrade, equivalent to S6° -89.6° Fahrenheit). This lower temperature decreases fcy that much the energy Amanda of basic metabolism and protects the energy stores of the organism thus placed in a state of rest.
48
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

' ' . tUiS . -. . ' .
,,:>,''„.«.••-..;>••••.•• This elimination of the body's entire defensive re-action is undoubtedly'an economy, but'it would be fatal i f not accom-panied'by the necessary corrections: the conservation of a 'vital balance-and remedial action against the injury syndrome which is the cause-of the-Strock. - The antishock therapist is taking over the
" patient's battle plus the responsibility to keep him going. That is a.difficult task, f i l led vrith serious consequences for the1non-initiated.
Lyt^c Drugs are Vasople^dc. Therefore, in order to avoid a disastrous drop in blood pressure, i t i s essential that a sufficient' circulating blood volume be re-established by appropriate transfusions or perfusions* • ..4;'"--'; - . , . . . . . .
à ' ; lytic drugs suppress the regulation of the anabolism 'to catabolism ratio. Therefore, in order to ensure the energy re-quirements, which are indispensable even to an organism in a state of hibernation, i t is necessary to control with precision the measured in-take and'ratlonal utilisation of proteins, glucides, electrolytes and water; .-•'«• / - . , - . - . - - . - -
' . We can then take advantage of this "vacation" of the in Jured. organism to fight in its place, medically and surgically, .,againstJ-the injury syndrome. Only after the victory has been assured . .over these pathogenic factors is & not exhausted organism'given back its independence and its own homeostatic balance. . .
V?.; : - , V. However, the refrigeration method or hiberno-therapy is s t i l l a new enterprise and i t requires precise management by quall-fiedl'-specialists, -careful nursing, hourly clinical control and a very ccmplex daily para-clinical control, Althcwgh its efficiency is certain, its5 complexity is considerable. Moreover, in war surgery, this method !
precludes the possibility of evacuation becauseof the likelihood of hemodynamic disturbances due to vaeoplegia,
•These statement? regarding both the efficiency and the complexity'of-the method are based on a large number of facts of exper-ience/both in' civilian and in war surgery, spread over several years -of experiment. The work of Chippaux in Indo-China is conclusive on this subjects I will, mention the exact indications calling for the application of refrigeration in war surgery in my next, and last chapter—devoted to the therapeutic Indications.
I I . Therapeutic Indications
:. 1 -..-.:,%. - These Indications must be considered In the light of two different factors?' the location of the casualty and the type of Injury oaualng ther shock. '
1. IiQ cation
In the Forward Area, i t wi l l be poasible to use only sim-ple:procedures, adaptable to a l l casualties and at a l l advanced or inter» mediate echelons of the Combat Zone Medical Service. These procedures must make possible, or not delay, the evacuation of the casualty.
' * f First of a l l , the-treatment will attack the Injury shock Syndroms. I t wil l therefore be aimed at eliminating or minimizing the causes ot shock. ' !
Against pain, analgesia should be administered in the form of morphine, the harmlessness of which is almost -universally recognized.
49
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
But overdoses should be carefully avoided, and every dose of morphine given must be shown on the casualty's f ield medical card. _ Heavy over-doses should especially be an object of great discretion in de-shocking* A wounded man suffering from shock with slow circulation resorbs poorly a substance injected into his muscles or under his skin. When circu-lation, has been re-established, the process of resorption is accelerated, and at that time, a patient who had previously received no benefit from repeated Injections of morphine may undergo a toxic stage from the sudden release lato the blood stream of the morphine Initially stored at the point of injection* This intravenous route avoids this danger of con-cafcntto?.
Ve wil l pass rapidly over the question of temporary hemostasis by installation of a tourniquet} the dangers of the abuse
' of tourniquets are only too well known. Traction on an injured limb is o f t ep sufficient to stop the bleeding and doesnot offer the same dangers of ischemious and devitalizing striction.'
...-...., The-immobilization of fractures, pressure therapy for crush injuriesp oxygen adainiatration and the clearance of theresplra-tory tract or "air way" are too essential and too well-known for i t to be necessary to discuss than her*.
. • * : • » - • - - - ( , .'j Al l these procedures, plus th? performance of transfusions
or perfusions for fluid replacement, form an integral part of the forward zone treatment of. shock.
To this treatment of the injury pyndrcme must be added therepsutics.intended for the reaction syndrome. We have referred to the tendwicy today .to discontinue tjtie use of vascular and central analeptics of tjw'adjwnalin or'strychnine type. ; At this echelons a simple check against, the post-traumatic reaction can be applied lya simple dis-connection, thanks to the use of the phenergan-dolosai mixture. However, even this prudent disconnection Should not be effected until after per-fusion of the fluids necessary to re-establish the blood pressure under medical control.
-. At the surgical echelons, the more complex and more . efficient procedures pan V« practised. The normal shock treatment, as we have outlined it,,rcanbe continued, in 9/10 of the cases, this thera-peutic is effective and therefore sufficient. But, in cases of uncompen-sated,or recurrent shock, In serious multiple-injury casualties (about
Of medical.battle casualties), only the low-pressure treatment or hibernation therapy wil l make it .possible to break Moon's "vicious circle" and pull these severe shock casés out of a fatal course. And the number of these cases to whom the treatment can be given will be inevitably reduced owing to thedifficulties of its application by specialized personnel in a surgical formation overcrowded by a mass influx of casualties. These are the conclusions reached by Laborit and Chippaux during thewar in Indo-China.
2. Btiologr of the Shode
' In the therapeutical management of shock conditions, a few essential differences must be taken into consideration.
A special method of treatment must be performed in shock cases having lung lesions, owing1 to thedanger of failure of the right heart (cases of pulmonary blast, gas, suffocation, burns of the upper respiratory tract, pleuropulmonary wounds). The shock treatment remains the same in principle, but i t must be conducted with special care not to overload the pulmonary circulation. Transfusions should be given by enoarterial route after exposure of the radial or brachial artery* A
50
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
vasoplegia induced by the hibernation Method wil l ease the right heart and is a good indication in such cases.
In turn casualties suffering from both toxic poisoning and.ehock,,the normal shock treatment must be accompanied by treatment ,against;toxicosls; the special treatment for toodcosis resulting from war gases,<or phosphorus or carbon monoxide poisoning*
SUrned and radiated casualties must receive, in addition ( to the normal shock treatment, the special therapeutics for radiation. Besides^the bdood traiisfUsions Vtich form the basis of-this particular treatment, largaotyl can be 'administered, as it appears to ensure considerable ^protection of the cells against radiation sickness. The possibility of increasing the tolerance to the heavy doses used with cancer patients ^undergoing radiotherapy has been shown by authors in the United States and in France, particularly by Baclesse, Harois and Casma* ' , .
* * * *
Ths above outline covers the main points in the present status offthe qpsstion^of traumatic shock. It is a vast subject s t i l l
,being-«developed ;and always 'subject to being studied all' over again from scratch* Aftw every war, a l l the conclusions previously acquired and considered as final are again aade subject to question, and new per-spectives appear.'
' •• t tu Z-y.!. • . . .
.. li. ' These différences and this continuous process of develop--ment :«4d to the "interest of this important subject—a subject which is ^of ertreuely^great i concent to a l l war surgeons. In fact, the war surgeon's f i rst precaution is to fight against traumatic shock, the most immediate and the most: serious of the dangers which threaten the lives of wounded men In time of war* That is why the surgeon has had to become a physio-logist and adapt himself to the new surgery of his times*
"y . • - * 'L •
1 - -
MUCR -tSMBRAL VAN DBt GIESSEN
...i-: v. Kajor .General H.J.' Tan der Glessen, Surgeon General, lBoyal Netherlands. Aimy and Air Forces, opened the discussion by giving a short description-of-the state of shock. He then classified "patients" into
- four categories ^according to Bescher, i . e . ! .
- ^ >r.--- a* Patiwrts shcrwlng-.no sign. cf shock - .' i..., b* Those showing a slight shock
, . o* -Those showinga serious shook j ^ > • • ' d. 'Those showing a perilous shock . . -
,'Qsneral Tan der Glesssn dealt with treatment of shock in the forward :areas, and 'polnted out that not a l l wounded men are in great pain. In fact, -administration of phénobarbital or nembutal in small doses, to relieve distress or anxiety, was often of more value than the administration of morphine. He spoke of the necessity for early surgery, as an additional means of ccmbatting wound-shook. He concluded by referring to the work done by the. French Medical Services in Indo-Chlna in art i f ic ia l hibernation and pre-hibernation. •
HftipADIEa GBllRAL. SEELEÏ
Brigadier General Seeley recalled that Colonel Favre and
51
, NATp CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

himself were two of the three surgeons responsible for writing the Surgical Handbook for NATO Armed Forces.
He said that the practical application of the treat-ment.of Shocks at the front, is dependent entirely upon the recognition of clinical signs of .shock. Once recognised, the only treatment avail-able to "us, ris replacement of blood volume. In his opinion, on the battlefield and particularly In the case of mass casualties, when the • estimated blood volume loss is 20£ or less, there wil l probably not be a sufficient amount'of material to treat them a l l , .
When.the blood volume loss-is between 20-40$, he would use dexbran - first./v Because of scarcity of whole blood he would give
,as much' as -six pints of dextran before resorting to whole blood. In Korea as much as 15.pints of dextran was given, lo**^*h"W»efc«tfeofrffcoiteading from 45 down 12, Fatients went through surgery and convalescence without blood transfusion, ; We must conserve whole blood, and work for a greater stockpiling of plasma expanders.
COMMANDER UBORIT !
J.:.''.;. .--f ; .In-the treatment, of shock . (burn casualties, wounded, etc) the, previous speaker had stressed the importance of transfusion .and of re-ejStablislanentof;theblood\volume.
Dr. Laborit considered this replacement of the normal blood volume insufficient, because transfusion only re-estabpished the normal .arterial pressure without correcting the circulation. At the same time:the peripheral vasometer reaction must, be suppressed. As. a matter of „fact , - ln treat ing stat es of shock i t has been noted that, in . sp.ite of. abundant transfusion alone, the patients died on the second or third, day frem disorders of the kidneys and liver, anuria in par-ticular,', ., ,.'.• ., •
One must choose the treatment to be «mployeds either the classical method (transfusion' and aàninlstration cardio-vascular analeptics and morphine), which aids vasoconstriction, the organism's natural method of defence, but which prevents any use of the hibernation method, or apply .from the outset a slight disconnection, that is to say, that,;-contrary^to\;the above method, the vasomotor reaction is lessened by the atainistratiop of phenèrgan, which is anti-histaminic, parasym-pathicilytic and has a strong central action, and dolosal. i .. . • . ' y* - , '
1
Dr.: Laborit also stressed the dangers of morphine, an extremely powerful respiratory inhibitor and an inhibitor of renal secretion. In cases of shock, the administration of morphine may en-ta i l respiratory stoppages by acting on the nerve centre^ of the medulla oblongata.
/ As opposed 'to this, he recommended the systonatic anploy-ment'of drugs such .as phenothiazine derivatives which give the surgeon freedom of.choice in later treatment, whilst lessening to a very great extent the fatigue and pain inherent, upon evacuation* '
•. -<,;.• , This disconnection must not be'confused with true hiber-nation, used only at the Base Hospital by we 11-equipped and extremely specialized personnel,
GENERAL HAIL
At the.conclusion of the discussion, the Chairman said
52
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

that the NATO Surgical Handbook to which Brigadier General Seeley referred, was coming along very well, and the preview he had of some chapters wasmost- encouraging.
< ' 'Heathen introduced Major General Harry Amstrong, Surgeon of the United States Air Forces in Europe, who.was to re-
'portlon the, NATO Medical Coiimtlttee.. Vi' - .Ü.'J J .. r< • r • .
. -, -, -, Since your last meeting here a year ago, a NATO Medical "' Conniittee 'has been organiz ed and its f i rst meeting was held on 22 November 1954. ï have been asked to outline briefly the factors which led to the formation of this committee, to state its terms of reference and to review the'work of the committee to date.
• •*!.'' Iou will recall that the Medical Branch of SHAPS was created.in ,the latter part of 1951 with Brigadier General Kennard as ' its "chief. At about the same time General Eisenhower, then the Supreme .Qommander, requested that an analysis be made of .the resources .whicb.were'ayailable within NATO or, which could be made available i f >rar rShould occur'. Y m attempting to carry out his responsibilities under this directive, General Kennard found that he was unable to com-pile the required information on the medical resources available in NATO due.to the fact that this information was lacking in most of the nations, concerned.
: î A few months later Colonel Howard Nelson was made available to SHAPE Headquarters and assigned the task of visiting the
.umber' nations of NATO for the purpose of making a survey of the existing situation. At your meeting last year you wil l no doubt re-
'cal l that Colonel.Nelson reported to you the results of his survey which .indicated that in many countries:
• ,./JV. n / 'V a. Estimates of national casualties were not available*. _ ;
.. . h* The total national requirements 4 r medical mater-
iel, ' facil ities and personnel had not been formulated. rJ, r,. c, Existing stocks of medical materiel were in-
adequate^* ; YV Y '-Y' -.
d. There was a largs degree of medical supply inter- '. v
dependency between a l l NATO oountrles in Europe and in many cases the " existence'of this interdependency was not recognized,
' • e. " There existed no formal basis for coordination among the NATO countries on a national basis.
„ i * ....-• ••••.' . . if
Y ' Y1 It was General Kennard's belief that the solution to . thesevarious problaas was dap aident primarily on the creation of a NATO Medical Coordinating Agency. 'Accordinglyy the SHAPE Medical Branch-prepared a staff study which recommended that the NATO -
Standing Ooup ' approve the ' establishment of a NATO Medical Canmittee which would:
Provide coordination internationally on problems of
Develop total requirements.
/ a. health resources,
. «•••' y V
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

. .c. . Assess national capabilities.
di RecciDDiend measures for alleviating deficiencies.
_ e. Formulate plans for the most efficient utilization of existing and planned resources, especially in wartime*
SHAPE Headquarters approved this staff study and on 11 August-1953 forwarded it to the Standing Group in Washington, D,C. for their, consideration along with a recommendation that a working party be established to develop the terms of reference for the proposed
• committee which would be acceptable to the NATO Council. These re-commendations were approved] the Terms of Reference were formulated and
' each of tKe ATO Nations appointed repres entAtives as members of the new ; c«isnitt'ee. '"
The first meeting of this Medical Committee was con-vened at the Palais de Chaillot, Paris, on Monday, 22 November 1954 at lO.JO^aVn^Mr.' P^ Anninos of the International Staff was made avail-able to: the'cqnoittee. as its'permanent secretary and in an opening state-ment' he explainedthe primary purpose of the Ccmnittee and pointed out ' that, in the future i t would probably be asked to assist other NATO CceadtteM on the medical aspects of problems which they might be con-' S i d e r i n g V • / : ' • • " '' « ''V.' . • 1 il * • r » - ' • j ^ ' . •
' " J1 f* ' ' ' '
. ' C ' As the f irst item of business at the meeting, Dr. C. Toftauark of Denmark was elected Chairman. Other countries represented were Belgium, France, Italy, Luxoabourg, the Netherlands, Norway, the United Kingdom,and. the United States. : Also in attendance were Sir John KodsoU.(Senior Civilian Deifence Advisor), Colonel R.T. Bennett (SGLO) and Gàieràl W.7.' Hall, Colonel Ahem and Colonel Nelson, representing SHAPE, ' . .. .:
The prepared agenda was next reviewed and after some dis-cussion i t was agreed that it should be followed without change. It was also decided"that at the initial meeting only the first section of the agenda would be acted upon since that section had to be completed before the remaining sections could be dealt with.
V . .. ; The f irst item of the Terms of Reference called upon the Committee to prepare*
^ lL. ' l ; A planning assessment of casualties both civil (to include refugees) and military for the first 60 days of war for each country within th e NATO areas.
-, /----- ? with'reference to this Item the Conmittee agreed:
, a. That a l l delegations should make an assessment of casualties as* outlined ;
,,.. ,. b. That those countries which did not possess practi-cal experience in heavy. bombardment should, in making their evaluation make use'of ^ i e ^werience gained by other countries.
. - . . -Ur i—; • rT-.' - : —• • : , • ••- - .
0V1 That'those countries which did not possess sufficient, information rto make a useful assessment should request through the Secretary such information from Sir John Hodsoll.
*
- : d. ThatV at the present stage, the question of refugees should be left out completely as it was the Ccmmittee9S understanding that the NATO Comnittee on Refugees and Evacuees had not yet completed
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
its studies and was not in a position to furnish information on the eventual numbers of refugees in certain NATO countries.
V ' .The second agenda item called upon the Ccmmittee to préparai :
2. An assessment of thestocks of medical materiel ^ow-heldTin each country together with an assessment of requirements.
.Withreference to this i t « , the committee agreed:
•"• ,- a. That SHAPE should provide the Secretary with copies of an existing report based on a questionnaire which SHAPE had circu-lated-, in- Ju^e 1952, concerning these matters, namely: (1) an assessment of- theastocks. of medical materiel' now held in? each country together - 1
.withanjaas.essBentofrequirraients, and (2) a review of • essentia! ex- -port' and import requirements of medical materiel in each country.
.. b.- That this-SHAPE report. should then be circulated to delegations/who in. turn would complete those parts affecting their res-• pectiyei countries • and inform the secretary o f such additions.
^r-j^i-if That-this information should then be collated by the secretary ,so that a complete picture would be available of the extent ' to which.countries are independent or are relying on other'meniber countries, for .important medical supplies.
/ " d. That when the results under c. above were available, a depipion could be taken as to whether any further action in the supply '! or'economic "planning f ields was required. 1
^ . . The third agenda item called upon the Committee to: ' -
* Jisirii'. rHeview present plans for wartime hospitalization and » popl ins - for alternative hospital accommodation should present urban1 , facilities*:be destroyed by enemy action.
.•'li'ii ' -A-« ^vBegarding this question the Committee agreed: -.. - , ' ' > • > .i
j a . That it would be d i f f icu l t , under the conditions contmaplated, to differentiate between militaryand civilian casualties for hospitalization* purposes and that there was great advantage, where nationalsor^other conditions permitted, to cover both requirements.
-. - b.- That delegations should prepare a short, broad out-line o£»theto.<<alsting hospitalisation plans..
The fourth agenda item called upon the Committee to:
-.+ :,.+2 - A .Review the medical- manpower for each country to dis- . close, i important deficiencies.
v :>s -ivC Regarding this: question the Committee agreed?
.,-vifi. '; '-V a . That delegations should prepare brief reports on the question. ' . .
b. That in addition to physician*, nurses (male aqd f e - ' male), anaesthetists, dentists and veterinary surgeons should be ty&uded.
Jïi^s >- In addition to the above, the CooiBittee was to study s . V ;.- :,...;' '•;•'.
5. A definition of the respective responsibilities of the civilian and military authorities with regard to Uie hospitalization and treatment of civilian and military casualties: < <
- " ' , • ' . , • ' ; ' • " : 55
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
a. in the zone of military operations
b. In ports and coastal areas
, c, along strategic lines of communication
d, In a l l other areas
After consideration of this item, the committee agreed:
' a. that-to attanpt to deal with this problem on the lines of the above« sub-divisions would prove unrealistic and impractical,
• and V - , ,-••.••.••.••• * - .
,, ^ -.-- - =-:--.- -:- b. that delegations should prepare a short report, on-as broad a. basis; as possible, on their national organization, to cover in-formation not already embodied in the report requested under item 3*
. above.
. - This completed the f i rst section of the agenda which was to be acted upon during the f irst meeting of the Committee. The Secretary requested.that the delegations submit their respective reports within two months and upon receipt of such reports that he would circu-late: them. either independently-or in combined form to the delegations one month: prior to the, next meeting of the committee. This second meeting was scheduled to be held on Thursday, 22 April this year,but due to the fact that many of the reports had not been received on schedule^, this meeting was postponed until ZU May.
-. .. «./: - ' >. '-• ' •• . ^ : In this second and other-subsequent meetings i t is anti-
cipated that the Committee will proceed to-take appropriate action on ' the remaining agenda items. Based on the data now being collected, the committee; will develop and recommend plans for medical materiel stock-piling, for providing adequate wartime facilities and equipment, for minimizing deficiencies in medical manpower and for establishing channels for the. exchange of medical information. Finally, the terms of reference call upon the committee to collect and disseminate medical information with reference to hydrogen and atomic weapons, biological warfare, chemical warfare, and such.other problems as may be approved by the NATO Comnittee on civil organization in time of war.
-'. It is my, personal opinion that the NATO Committee will serve as a very useful medium for the collection and dissemination of essential information upon which sound plans and decisions can be leased. However, the degree to which this is so wil l depend almost
V entirelyucn-the support-which each of the NATO Nations gives.the Committee and will determine whether i t will succeed or f a i l in its purpose. -
GENERAL HALL '
. Vvi^1J j -. . The Chairman referred back,' at this point, to the "Report on the NATO Medical Committee" presented by Major General H.G. Armstrong. He said that although the Medical Branch at SHAPE had taken the f i r s t steps towards : bringing-, this Committ ee into being, i t was in fact entirely a civilian committee the members of which were nominated by NATO Nations. The NATO Medical Committee reports to the Chaiiman of the NATO Committee for Civil Organization in Time of War, which sits at the Palais de Chaillot, in Paris.
The Chairman then introduced the British Study Period, which would occupy the next one and one-half days of the Conference.
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

This. would deal with the deployment and functioning of the medical services in the field In face of atomic warfare« Itwould comprlse three phases:, f irst ly, with prcerem infoiwtion and experience of the problem; and, arising from this, with a forecast of casualty rates^fo^.nudear weapons secondly, there would be a presentation of the- problem: of nuclear warfare, as a CP2; thirdly, there would be a:!»erystal gaze" into the future, in which new organizations of medical units »would be considered.
Y." Y v He said the Director General, British Army Medical ^Services, had graciously accepted the responsibility for this part -'of,,the Conference programne, and had contributed significantly in time, ' effort' and money to create the presentations and bring M s
' team toPtiris, a fine example of NATO cooperation. The Study period would:start with Colonel MeneceS' presentation, "A Tale of Two Cities.-"
OOLONEL MaiECES
• ,'••• v.*,?- - ^ Colonel A.N.T. Metieces, Commandant of the Field Training V Cent?e«r;BAMC> presented his serial,- "A Tale of Two Cities." He -showed
a series of. slidss illustrating the "physical and biological'effects of • the atomic weapons uaed against Hiroshima and Nagasaki, and also the 1
^ methods, employed by the atomic bomb .Casualty Commission in investigating rthe survivors of these two incidents,
• frt'i ColtQnel BACH *** *** *** * * *
Yln the discussion which followed, i t . Colonel Bach drew attention to a possible fallacy in-showing the scaling laws for heat -/effeots on-a chart. In the case of a small yield atcmic Weapon ( i . e . , up to^ *bout, 60; KT) a l l the heat was delivered in about 3/10 of one second. -For larger weapons"this period of time is much increased', and
-may bs <M* much as several seconds. Thus, the intensity of heat is ' different in.the two cases, and a large weapon might require several
-times tjie number of calories to produce the same effect on the skin as a small one would.
- iHHM Mm W if M W W if • ; ~ T T*iT7* JTTTn TiTIT HMH
LT. CCLONEL MARKS : .
Lt. Colonel S.L. Marks, the Field Training Centre, RAMC11 .Ù than--.PKjMnted his. paper on "Casualty Estimation", as follows:
•;-Y:. - "General
• One of the f irst things an officer must know when making a plan for a military operation at any level is his aim, or mission—in siii^le;-tenw—VWhat- is the task?" For the medical staff off leer or medical
: unit, commander much'of this boils down to "What is the ejected casualty . rate^how many .killed, how many seriously or slightly wounded?11
li: :'•> • V ; :-. . . .-'.'v.. - . . . . - " , • • • "• ; V Y- It is normally the responsibility of the General Staff to
give Medical Branch the anticipated casualty rate but they sometimes say . "Well, doctor,', -what do you think?" Ve have a very sound guide to-the : estimation of casualties from conventional warfare in statistics of the 1 ast. ,war,• but for: casualty estimation in Atomic Iforfare we must look
.-»-further. r', And we must be prepared to make our own estimates for any. -<-• specific incident because the General Staff branch wi l l be much too busy with the urgent operational problms.
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
- -In atomic warfare the estimates will vary considerably Anom incidents in built up areas on the Com Z and Base, in which mili-tary are involved/to incidents over well dispersed and well dug in troops in the divisional area.
; Now there are four main sources of information that we may consult) ' 1
a. The Civil Defence figures for build up areas
b. The NATO wastage figures
c. A simple template system
.i'M. h"" d. A form of ready reckoner which has been published in the U.' K. *
Civil Defence Figures
It would take too long to go.into details of Civil De-fence Casualties Estimation Just now—that would hiâu.a lecture in Itsel f . All l need W y ' i s that^they are estimated in accordance with certain fac-tor s / s u c h a s : ' - ' '
..- • i V ' a Population Density: which may vary between day and night.
b. ,^fteiEvacuation Policy; I . e . , percentage actually evacuated,
'-1W- 'c.^ Degree of Protection! e.g., population in houses or in ShelterSrtOf varlous>8tandards, depending of time of day, warning, etc.
. . * .-. ; . ... • • . -. -
-y d. . Characteristics of Buildings; wood, concrete, brick,
••> '. In fact, casualties in built up areas can also be estimated from the. Beady Becdconer which I'm going to deal with in a moment.
The NATO Figures \ •
The NATO figures which Ccnmander Stone, US Navy, is going to deal with in detail in the next serial are concerned mainly with over- . a l l manpower wastage and the resultant hospital and reinforcement require-ments. • '. .
The methods I am going to describe are those that might be of use to a medical ocraoander or staff officer at a headquarters In the field .that has no logistics division to do the calculations for him. They relate to specific incidents and, given certain basic data, can be worked out by any-offlcer of average, Intelligence—in fact, "simple SUBS for simple CHUMSAN
Let us therefore look at some of these figures in greater detail remembering that a l l these are estimates only. As we go through the factor involved you wil l see that there are so many variables that an accurate forecast is not possible. AU we can give is a reasonable approxi-mation of the order of casualties ejected.
Th« SffiW1Tffifttt gyrtfft
- This:is the simplest possible template and shows the effects on man and equipment assessed purely1 on their distance from ground zero and divided broadlyinto Severe, Moderate and Light damage or injury. These are defined as follows:
58 .
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
a. Severe: DuagaA seriously enough to render equip-ment useless and to make repair essentially impossible without removal to a awjor repaid facility. , v
•" ' V.' b. Moderate: Sufficient to prevent any military use -until repairs are effected.
c. Ljgtrti Can still be used but requires some repair to restore equipment completely.
These definitions though primarily applied to equipment, can equally be applied to casualties. • 4
. Ths particular template I am going te show you Ial Ubat of the 20 KS weapon, but they can be produced for weapons of any size 5 Et or 100 KT.
.,The burst height is taken as 2,000 ft. an a clear day. Jfo allowance is'made for protection by natural features.
Y The centre of the-diagram is GZ. Each concentric circle represents :1,000 yards. . The table below shows measurements from GZ of degrees of damage and Injury. The colours indicate:
. Red: Severe Yellow':Moderate Green: Slight
* ' " • • -
f •V A-''- .
' F- • ; W ' -. ) . ' j i j  1 Î L
• . f
59
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

"•' /2,,000 Ft. - Clear Day '• - ; . MEN IN SLfIT TEBJCflSS M© IN
• ' -, !BUILT-UP ••• V AfiEAS
MSN IK THE OPEN MEN Dt TANKS
BEDt Severe Injury ÏELLOWî Moderate. Injury CBEQlt Slight Injury
Subject Measurements in yard s fron G Z
Subject Severe Moderate - LlBht
Men in the Open Men in Qpen Slit Trenches
4 feet deep Men in. Built-Up -Areas Men lnTanks 7 .
0-1300
O- 500 O- 900 -0-1000
.1 00-2200 .
500- 900 9OO-I3OO
1000-1100
2300430Û0 t:
9OO-I3OO I3OO-35OO 1100-1200
60
; NATO CONFIDENTIAL U l - • -.,,-.-
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
The Raadr Reckoner
Description
This i s based on the template but i t goes further in that the template is applied to a particular map scale and can therefore be-applied to a specific deployment of troops. Also, by the use of certain tables we can arrive at not only A figure of total casualties but a breakdown into types of casualty. The purpose of the reckoner is to give the medical staff officer a quick guide to his problem as soon as possible after the incident. The data i t requires, in addition to the location'of Ground Zero, the height and power of the bomb, are a l l pieces of information that he would normally have available. The height of the detonation and the location of GZ wil l be computed prob-ably by the gunners, passed to G Branch and should be available very shortly, after the explosion. The medical staff officer is then in a position to make his calculation of anticipated casualties, and work out his lsnediate plan quickly and put i t into operation without delay,
Fötors
Again there are certain basic factors upon which the numbers wil l depend, such as:
a. The nature of the operation they support, e.g., defence, attack, river crossing, etc.
b. Density of troops on the ground - concentrated, dis-persed.
c. Degree of protection of troops - s l i t trenches or in the * open—difficult to assess at any given time.
d. Number and power of weapons used - 10 KT, 50 KT.
e. Height of detonation - 2,000 feet or lower.
f . Meteorological conditions - hase, effects of heat (thermal effects).
g. Protection afforded by ground.
Of course i t is obvious that estimated numbers can vary within wide limits but we can arrive at some sort of guide which wil l be a reasonable approximation.
The method I'm going to show you is based on the effects of the nominal bomb, i . e . p 20 KT burst at a height of 2,000 feet on a clear day. Let's have a look at the f i rst Chart (Chart 'A ' ) . Now this is re-lated to a specific map scale—in this instance In to 1 mile; only here we've enlarged i t to 1 foot to 1 mile.
You'll see that this target diagram refers to temperate, c l i -mate with men in battle dress. In a tropical climate with clear atmos-phere and men in tropical kit the effect is much greater.
Here i t gives the effects on:
Men in the open Men in built up areas Men in s i l t trenches
61
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

. W W -I I I-W I w v i m m M V I i w i *—* LAyiVlU V/ll I LJAiJV/IIHUU-
TEMPERATE CLIMATE M e N IN B A T T L E D R C S S CHARTA
CftEEN-
MEN IN SUT \
TRENCHES (WfTHOUT OVERHEAD V PROTECTION)
MEN IN THE OPEN
(Colours Indlestet HED t Serere Injury YELLOW : Moderate Injury GREEN : Slight Injury
MEN IN BUILT-UP AREAS BKS. T O W N S ctc.,
SCALE* t* I MILE
DATA BASED O N : 20KT B O M B . BURST HEIGHT : 2,000 FT.
CUAft VISIBILITY ( V S MILES APPflQX)
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Now will you look at this Chart (Chart 1B1). Thla-ha» columns , corresponding with the appropriate target : diagram and tabulates, as a per-centage of „the forces exposed.in Sadi section»'the likely distribution of casualties within these levels of Injury, classified as.:
- a. Total Casualties
b. IknediateDeatiis
^ e.- Casualties requiring Evacuation».;. Broken down Into:
1* Badlation - alone -.v.-nv '•><.-\ ; -v.* -. • pins severe blast,injury .
11« Burns - 2nd and 3rd degree ..-*' minor - 3rd degree with radiation injury
v.: - 3rd degree with severe blast injury
ill... Blast,. - alone - severe injury-- alone - minors-injury
' " . .'. Now this reckoner is used in thieway. Tou takeasituation. . map with -troops. disposition accurately marked on. an everlay. Having, ascertained G2 from. G Branch you nark that on your overlay, then slide. . the template underneath the overlay until the centre of the circles co-incides with the estimated GZ. Tou then trace the circles appropriate to the situation of the troops.
Then, applying the tables I've Just shown you, you do a rapid calculation using neither, logarithms nor slide rules, but this simple , proforma (Chart 1C'.)
Now, let me show you how X worked all this out - this chart (Chart D) shows a hypothetical deployment of an Infantry Battalim and one Field Regiment RA in an area which it is assumed they have recently
. occupied, ' * " " .
a 2ÛSÇT Bomb has been exploded at a height of 2000feet over the GZ marked on the chart and it is required to. estimate the probable numbers
• and types of casualties likely to result from the incident.
/ .
a. Height of Detonation - 2000 feet
b. Power of Weapon - 20 KT
. c* Meteorological conditions - Clear day - visibility 6 miles
d* Level of protection - both of infantry and the artillery have not been in the area long and it is therefore assumed that, whilst the infantry will have open slit trenches, the- artillery will still be digging slit Vsnches and gun pits. In view of the form of these pits and the fact that at this Aage they will have no overhead cover, they can afford'little protection to personnel from airbnrst atonic explosion. Therefore the levels of protection adopted for the purpose of the present calculations are:
Infantry i Men in open slit trenches
Artllleryt Men in the open
; , ' 63
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

NATO CONFIDENTIAL
e. Strengt!) of Units
Infantry BattaUon ,., 700 all ranks Flelcj Reglmsnt, R.A. 500 a l l ranks
Forces are assumed to be evenly distributed over the area occupied.
« appropriate target diagrams over the units as shown 'in Chart D.' ' r -, •
•V Estimate by .eye the fraction of each unit falling within the red, yellow and green areas and hence the numbers of men involved. The figures so dejrlveid are approximately:
v Strength £ed YeUow Green ;inf Bn 700 NegUgible 1/10- 70 men lTT^UO men
-, :Fd,Ha$t KA 500 2/5 - 300 man 3/5 - 300 men Nil
Applying the appropriate casualty analysis given in (Start B of-the'Seadr^ckoiaarcan calculate the number of casualties to be espected'using our proforàa. The figures so derived are given in the foUowlng ta ile, (Chart'1E'.)
w ^ i r *1 . . . . . . V,
' •. • i '
<n i. t: ' fcv-./i«.' •-:.-; ; '• • • . • ~ . . 1IiVijt' V: ; • •';•
1. ' -T.:. . .¾
•: . . ^-.4--., C hi • - : " ! • ' ' . . . 'ir-Ä' :;• M...,'!.: • " v. •• r .•
- r k- - y j - :
64
NATO CQNFIDiirriAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
CHABT iß«.
V
•M
I I t?
15
t f
Ü
' I H
t
in
o
s y ä « .
A l A - I i ^
| M 1 &
•3
* I g
i1 V
*
S .f
o
8
m
in
O ir\
8
CM
O OO
fo
ITl
m
I t
m
i i
i m
8
R tu
it g
t *
i i
4»
o »
m »A
KsI CM
î 'f
B -M
à]
'•«h
- t T « e I IS m o
çî P P * M
I l i m
tr»
65
«J
P itti
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
; ; SOQgEggH) CTpktBMA PSE IK 00MJPMCT3DH H T H "BEADY HECK3MSS" FOR
" .—7 " ~ CASUALTIES BEStJLTIMQ FBDM ATOMIC EmOSlON ' .. •..V V- vi- *. •. • .J .. ...——' . ..:.-,.. .. .•.,. • .
a
S £
Unit spd Strength >* :., :
' . ] ? t . ' 'è * • -*-4-- ' . . . . » ' TOTALS
XCaaualty Zones and Kimbars Exposed in Eaoh
•t J . , - Red .
.> 7-.. Yellow - , - - '
Green Red .. Yeliov Green
TOTAL CASUALTIES 1
- j. " . - - -
IMMEDIATE DEATHS . V- - ' -
BramK HniiRTO hstbtitwc wninraw » " ; lll j m
j
-«naimniiir op <mngg NEEDING TBEA3MEHT
PAnTtTTnnr Aloise ' . bT
a a a a u" Plus Severe Blast Injuiy
.... • . •i ; i
2nd a^d 3rd Degree — M i n o r
1 : ' Kl IKFIx *
3rd Degree plus Badiation 3rd Degree pins Severe Blast
Brinn Alone — Severe Alone - Minor
* - • • . - - . .1 =S
E
I 1
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Scale -1 : IOQOOO (I cm.-I km.)
INF. BN. GP.
CHAUT D
Temperate Climate
YELLOW-L /
V I v .
,
RED / J T A R G E T D I A G R A M F O R
GZ
FD. REGT. RA.
tEN
MEN IN SLIT TRENCHES TARGET DIAGRAM FOR
MEN IN THE OPEN
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
SUGGESTED HjQFOEMA FOR PSS IK CONJONCTION WCTH "BEADY RBOKOfW FOH CASOAUIEfi RBSIlLTItE FBDM ATOMIC EXPLOSIONS
M
UnitandStrength I Infantry Bn. 700 Fd. Eegt. RA 500 I0IU5
I Bed Casualty Zones and Ktanbers Exposed in Eaoh Il HIL
Yellow -
1/10 « 70
Green
1/5 = 140
Red
2/5 » 200
Yelloir
V5'» 300
Green
NIL
TOTAL CASUALTIES g -. .. w j f « . 2 0 0 ^ 2 0 0 - 622
B(US)IATB DEATHS | - 7 0 j tIOO
s NIL 2 0 0IOO=
1 5 0 10
3 ° ¾ ^ 30 - 215
HENCE NUMBER NEEDING- TREATMENT U — _ Ti ^ ^ 1 Ia 2 0
^ i =5 0 3 0 ( ^ 1 0 - 407
Breakdown of Those Needing TreatmKit I
RADIATION ^0 n e
c ^ T , 1 " Plus Severe Blast Injury U - ™ I
- - - -
2nd and 3rd Degree
BIII9TS Hiiur 3rd Degree plus Radiation 3xd Degree plus Severe Blast
-
- 7 0 ^ 3 5 2uoMsij2 2 0 0 ^ 5 0
300jg.90
3 0 ^ g = l Q 5
-
90
302
BLAST Alone - Severe . Alone - Miiwr
- — • — 3 0 0 ^ 15
S O O
C
*
6 -S M P
f
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

*0f course«'there are Iiaitations to this method.
ai '!Ibu must'know GZ, ' s ••••••
b, Iou must know the approximate distribution of troops.
1 •• c.;-You'must know their level of protection« and it might be :
very difficult to assess the ratio of protected to unprotected troops at any glyen'mcment. :
d. . The bomb is assumed to be 20 KT. ' -
' 1 ^ 1 Ze i There is no allowance for topography.
This ready reckoner is based ondata approved by the various scientiflc'and'Other interested authorities in-the United Kingdom but : May i I Oiphasise again what I said at the beginning - at our present state pf^knowledge a l l these estimates are approximations to assist in planningfor'&taïic incidente» .,:',* £,- ..--, - •; ' ' s •'••• ' • ;
-; -fZ '' " T h e Army Operational Research Group who produce the Ready -Redconer^have also produced a circular slide rule which will give total casualties for a number of weapons'burst at varying heights In varying degrees of visibility. I understand this slide rule has been discussed with officers at "SHAPE but its value for field use has not yet been determined."'- :
i V With particular reference to the divisional problem,, a care-' fUl^study 'has been 'carried out in the UK of the exploding of theoreti-cal" atomlcweapona over many specific military situations in the last war?" IV i s 'reckoned that over the well dispersed and well dug in'forward
^p^tions: :of'a well disciplined division* one atonic weapon of 20 KT wil l "'pi^uce:average''total-casualties.(including kllled) of the order of 1000, -It n ^ well'be that the enemy1 s aim will 'be'to produce 20$ - 25$ casual» \ies:'SndvWe^may'therefore expect 3-4 20 KT weapons or one 50 KT to be «Kploded^ovêr^the'division he is: going to attack, This will"give:us a ' total çMualty^.list'of "the order of 2500-3500 of when about half, say 13p0-130o; will"be for the medical services to deal with. Of these0 some~500-600;will'requireFurgent evacuatlon(1 i .e . » to be at the CoC.3. or Surgical Hospital within 6 hours. <
These figures bring the task somewhere within the competency of the divisional medical services - always remembering that Uiere will be/'ln addition« the casualties from conventional weapons to be dealt with as well. > - -,
; You. will-have noticed that throughout theBe calculations I have been referring nainly to the nominal bomb - that Is« the 20 KT weapon burst at a height of 2000 feet on a d e a r day. I have» In passing« referred to scaling laws relative to waaptfp of greater or less energy. This is obviously a case of chronic "nominaUtes**, In the early days for teaching purposes we had to have a'yardstick on which to base cur calculations « but . there is a great tendency to concentrate too much on ther'lM;KT wjwpop«'bttratt:alwsys at a height of 2f000 feet, and always on a clear .daylLet us consider for a moaent the three variables relative to the explosion - the sise or energy of the weapon« the height of the explosion and the visibility. - '
Firstlyp then* to get away from the nominal bonb« we must think of a family of weapons of varying sizes - but not lnfladtely variable - , perhapa 3 or 4 in the (atomic) Kiloton range and acne more in Uie (thermo-nuclear) megaton range. .The sise of the weapon will presumably bear some
69
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
relationship to the size and type of target and to the means' of de-livery. Perhaps 5 KT against a .battalion, 20 KT against a brigade (or.regiment) - the 50 KT against a division. No doubt, i f war comes. We sh&llquickly be able to assess the energy range of weapons that the enemy is using.
' The next factor for consideration is the height of the ex-plosion. It I^j interesting and perhaps obvious to not« that the low aircraft produces the maximum percentage of casualties amongst men in the open with the percentage falling slowly as the explosion height rises, fcut with men in open s l i t trenches the figure rises .»rapidly as the explosion height rises.
i Now visibility and its effect on the thermal or heat flash.
' I t was at f i rst Jthought that conditions limiting visibil ity would very materially reduce the effective area of the heat flash, TMs effect is now. believed to be much less marked than was originally estimated, FUrtheraore," .the phenomenon of the scatter of heat rays was not taken into considerationt In fact, Just as light rays and ganma rays are , scattered'by atmospheric particles so are heat rays, so that simple screening in a direct line between oneself and'the explosion may not give absolute.protection. Also, i t is estimated that in an explosion detonated below a low cloud base as much as U0% of the heat that nor-mally would go upwards may be reflected from the cloud base.
This might account for the scorched tree and telegraph poles that Colonel Meneces showed us some four miles from ground zero.
One last and perhaps reassuring thought that I 'd like to leave with you". Now that i t seems probable that both sides wil l have sufficient weapons for fair ly free tactical use it. may well be that we need not necossarily. conaider every weapon that is exploded as producing a mass
rof c^Bualties. Just as.in a conventional artillery barrage many shells 'fall;on^unocoupied: ground*so the enemy i f he has a mission.of sufficient taçticalcimiwrtanbe, ~»ay explode a series of weapons over ground he wishes .to.,occupy. or through which he wishes to pass irrespective of whether .there,are:sufficient men or weapons on that ground to make, what
• has'hitherto*bsen"considered"a worthwhile target.. In other words,'if i t "is vital for "him to take a piece of ground he may explode atomic weapons over the approaches to i t and over the piece of ground i tse l f , irrespective of whether i t is occupied or not.
Conclusion j • - *
v In conclusion I hope that I have been able to give you some idea of the possible methods of casualty estimation in nuclear war-fare in Ute field = with some thoughts on factors relating to casualty production, ranembering that what we really want is a good idea of the order of magnitude of the medical task in any given circumstance,
^Ql J t flW WW ^HT . •• •. . \ .. ...- , J • - V
CCMMANDEB STONE" / -
V' Oxraander Evan C. Stone, Jr., HC USN, Medical Branch, SHAPE, then presented his nBeport of SHAPE ABC Casualty Bates Canoittesp" as follows!,-"..".'"". ' , •
70
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

"CASUALTIES -FRCM ATCMC WARFARE
\ ; - . ,The casualty-rate, you wi l l see today, should have a most sobering effect ort a l l of us, Yetp in spits of these high rates, which result fron the destructive power of atomic and thermonuclear weapons, I take hope, because I believe we are slowly beginning to svolve'Kays ofcombatting the effect of these weapons. Undoubtedly many>>years: will'pass jpefore we begin to see much concrete evidence of our~paseive defensive efforts, Ultimat e l y l think we should be able to^cope with thisnew weapon in somewhat the same manner as our fore-fathers did-with the f i rst use of gunpowder.
JV ? To begin with, I believe we should review for a few minutes, a number of the basic factors and assumptions used in the Initial study to estimate atomic casualties, which were most ably and fully presented to you-by; Captain Coggins at this conference last year. These rates
• are sti l luseft i l andthey constitute an important segment of the casualty irates.;estimation,-Just completed, ;
^ U r d VM All of the basic factors which went into the initial study were.tborou^ily re-evaluated. Although a number of the assumptions which went into that study have been revised in conformance with changing mili-tary policies and plans and Intelligence reports, the technical aspects of:bomb damage are s t i l l considered entirely valid.
.(Slide) (See page 78) • _ srf i-.:- Ki i;'.:- . .
: ; -. arf v'i" Kl
* ao-i*: ^Tou : wi l l notice In thiB slide that casualties are reflected separately iforrtheraal burns,'radiation burns and blast injury, and-'; •
^hatfths-number -of casualties fraii eaoh-cause are related to the dis - ' tance frott ground zero. This pie-plate graph also shows the degree of protection offered by slit-trenches, tanks or wooded areas under f ield or battle conditions. These figures or percentages were re-confined during'Ithe vcurrent re-study of the problem. Our current atomic casualty estimation 'presents this1 same basic data in'a different way. inrIt 'is de-signed to indicate hospital bed requirements,, including the extent and length-of hospitalizing for Uie walking dead *s well as the injured; this study also indicates the extent of infirmary or field type bedcare for the less seriously injured and also the extent of medical care to be --provided to those requiring treatment, but not requiring bedcare. This data Willahs shown .to you later in a series of slides.
- The fu l l report of the init ial study, which was submitted to Subordinate .Commanders last November, stimulated many comments and re-commendations forimproving and projecting a more complete casualty
jtestimation picture. Thess reconmsndations were incorporated into the present study.
AU currant members of the SHAPE ABC Casualty Rates Committee, except one, are new to the Coomittee since.completion of the init ial
; study»'^They brought with them fresh ideas and new vigor to-solve the •problem.'^ALL' have contributed freely of their expert knowledge of ABC warfare to'the current study.' Ih order to reflect SHAPE thinking, ' Cqmsittee members were sheeted to represent each Division directly con-cerned with the atomic problem! that i s , the Intelligence, Personnel and Administration, Chemical, Training and Logistics Divisions, as well as the Air DeputyU Office, Through' thenthe ideas, and plaça of'SHAPE were cry-stallised« - ' The review and analysis of the latest military and atomic information, to develop valid answers to the present Studye has been an almost continuous procedure since completion of the initial report. Every bit of informatIons coming to the attention of the Ccnmittee, which might prove to be of value to the Conmittee in its Worici, was studied and
• 71
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
i • ' . ' * ' evaluated. This entailed a study of the many new concepts advanced
.for fighting wars in an'atomicage. Inclusion of these new concepts of warfare caused the Ccnnittee to change a number of assumptions a number of times,. to keep casualty estimations planning« current with the latest : approved thinking*
' a v.».'Please remember that the atomic casualty estimation figures whichi you. will see today do not'represent the-final answer; however, they do representcaaualty rates based on latest available assumptions and^planning guidance. That is« the estimations are based on the same type of „Infoimtiqn« on which we do a l l the rest of our war planning* nie same type of planning data on which NATO is «pending its money. Of ccurse^àddltional studies will be required in the future to keep our casualty factorsin line with changing scientific developments and modes of flatting wars.
..,. •; ;With that lntrodu et ion, let us now look more closely at some ^of^the^assunptlonsthatwent into the present study. These assumptions are subject to change in later studies, some slightly« others completely. The first assumptions we will look at, are those which are more or less
' coob^'^to^alll-Pfvtbe three military services: Army, Navy and Air Foree. ¢- . 17/.-4.,- A ? ...V •' ' . •'• - r1 - - • . '•• . Fjrst 4 - -.
The present study was tied to a specific date - July 1957. A definite date was considered necessary, to tie the estimation to an actual situation as well as to a specific troop strength. For example, planned changes Ih combat troop re-organization« which could not be accqpopUshed^by^this -date, due to time or economy, were excluded from thia^.a(tudy<.JiikewiseJ, proposed changes in the base structure of a ir -flei^a-^hich could-not he.accomplished by this date, were also excluded.
3qcond-«i--..-• ••> -..-Cr -'f,:.i.- • £»-,iTlih;ojr •«>*.. vjfis*. S-'ii-;' - ;
.- .vn^llocation of atcmic benbs, for use against various types of tàrgets were made in -accordance with best available intelligence infor-mation. fx s ••>..;• Iij..':.'
;r:.V ' : • . . - •
d c . - j--..: '.. ; ; '• • • • -- . • 1 . t • .- :
- / A^-preliainary study was accomplished to consolidate the very many sized atonic beobs into a few average sized bombs for use in this study, - Calculation of casualties for each possible sized bomb would lead:to endless .oathaaatic compilationP far beyond that which would serve:as(.a;Useful.purpose in this study, Ih addition« a time phasing fo ruseo f the^banbs was estimated* The assumption that 1/3 of the available bonhs.would not .be detonated over planned targets was carried forward from the initial study. Fourth .----. ' * V- v":- - •
- ^f^-Bomb detonation over planned targets took Into consideration the probability-of ne^r mlssps. Li other words, the bombs dropped over planned -targets,<-were not considered direct hits.' Fifth-.-- • t -..-.,: : K. .,; : -j • •,?si .r.l v- -t.? "-rT-tir '•' .- . '- '•' - . . - -
,-,,., ^ ;/Estimations of casualties were trended to reflect an average number, of, (Casualties i- not the minimum.' Planning for a minimum mmber
vvi . v'.'J.p * Iw.1,... . . I 72 . . - . - - -
' , ' < . NATO CONFIDENTIAL .
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
of casualties wil l only lead to gross under provision'of nodical care« While prwlgion of medical support for average numbers of ~ casualties will/meet local peak requirements, it wi l l in most Iim stances provide sufficient support until additional Ielp can arrive..
Sixth
The assmiption was made that the only time surprise attack wil l be the first one, the arrival of the f irst bomb. AHer the f i rst bomb, certain steps will be immediately taken by a l l military forces ;to construct shelters and slit trenches'and to disperse personnel, both on and off duty. This obviously wil l reduce the number of casualties oyer that sustained in the 'initial attack. In other words the only attack which would find us in the'same position as the Japanese, would be the f i rst explosion. This assumption of no true surprise attack, subsequent to the f i rst bomb, has raised a considerable content and . discussion« Perhaps i t wi l l stimulate the same comment with you.* However, what constitutes a surprise attack is an interesting question. Do w<mean;a "second", a "minute", an "hour", or what? Additional passive defence measures can be taken with each additional second oç ' minute of warning. There are so many variables connected with warning' that.lt was found essential to work with an average here.
Seventh
„ i :. »This study provides an answer onljf to the lmiediate number.. , of.casualties resulting from an exploded baoib. This assumption i s un- . doubtedlyrthei'mostYiiq>ortant me in the study« This estimation does~not,
"wpsat,;does not'consider the effects of radioactive f a l l - o u t . ^ I t ^ does notlncjufle the additional casualties which wil l occur because in -divlduals.'cannot get out of the damage area ^ themselves, or because^V
' evacuation assistance'does not reach than in tlne« Introducing these ? additional factors into the problok wil l require a whole new series of -formula to estimate casualties. It was therefore considered adviseable to f i r s t complete the estimate you see today and then in .a later study .include'the effects of radioactive fall-out. It is anticipated that the next^revision'of this study will'include an estimation of casualties due to radioactive fall-out.
Mahth ' ' '
This casualty estimation is for the f i rst 30 deys of war. The use of this time interval may cause some confusion whan figures of this work-up are compared with those of the init ial study. The casualty rates in the Initial estimation were based on thé f i rat„ « ) days of war.- not 30. The 30-day time interval was used to make this casualty estimation conform'with' other 3HAPE plans. Certain other studies must be completed
'before casualty estimations after the f i rst 30 days of war can be made..
Ninth'
- " That the assuniptions used for estimating Army casualties, in atomic warfare, is consistent and compatible with those used against the
' Navy and Air Force. Anottpgr facet of this same assumption is that the :. uss of atomic warfare is consistent with waging of other types of war- , fare. Atr fir?t^ikamlnat£on, 'this asaiaiption may appear superfluous, or
• innocubUSpi byV l t servep to keep the study on an even keel. When coiw siderlng 'ttv» offensive and'defensive aspects of atonic warfare alone, ' i t is quite easy to depart from the realm of reality and probabilities« Tiiis assumption helps to prevent these errors.
Tenth ' ' ' . . ..-, ». . i
/ *
An assumption was made as to the -average weather condition to prevail at the time of an atomic explosion. The clarity of weather has a very marked effect on the casualty radius for heat and radiation. A
1» AfWJ-V flMTf*Tni.*HllT M T
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
idiole Bertee of diagrams could be made on the number of casualties as related to weather alone^ with all the other assumptions remaining coistaat'.
SLshbUl' ' V
-That all detonations will be sir bursts. fc/kjp Ä'-T i,,' * 0 • UWU • uUu 'WflWI ^T ' r
v-JT- Now let us- Ipok at same pf the assumptions which more specifically apply.-to Just one servies.
t ...The following additional assumptions were used in calculating Airiy^çr -ground,forces personnel casualties s > First
"'y .. .That?ground forces personnel will be o dispersed that no more .than"one*battalion will find itself within'the personnel casualty area';;pf. a-'.single atcaaic kiloton burst.
Second
. That a Regimental Caabat Team with its adjacent logistic support force will be so dispersed that no more than one Regimental Cceibat Team wili receive casualtiee from a single thermo-nuclear megaton bttTet «*"' Of course , estimates of bombing target accuracy and "accuracy .of intelligence reports. were also .considered. A consolidation of ,these "varipus/facttjrs gave the same answer as though a,uniform density 'of troops was used'for calculating casualties. Thareforec the latter aethod of estimating casualties was used, In this study, for •ase 'of amputation.
That„;40# of all Army personnel will, be outside in the open rat ttte' tiiw^of the detonation of which 50 are intentionally or unin-' tantionaUy shielded by some type of object. The other 60JÈ of the personnel are under or inside some type of protection.
: Assunptions were made on thé .percentage of service support . "troops to be found in combat areas.-'. '''Zt "!"sAlMumber of specific assumptions were also made, to estimate atomic cas ialties.anong Air Force personnel. The Casualty Rates figures for 'AirrForce personnel as presented in the initial casualty rate study provoked much comment and recommendations for chaning the base complex to an Air Base. It appears that certain changes will eventually be accom-plished to alter the base complex so that- future estimates of Air Force caaualties Vill b« low*r<, However, we cannot see this change as being
'acccprçjlished'by the selected target date. Ibitll certain changes are made casualty rates for the Air Force will remain prohibitively high. The Air Force is working hard to find ways to reduce casualties and still carry outf its'mission. The assumptions on the number of Air Force personnel Who1WiU be in. the -open or those who,have some degree of protection, .were sij»ilar. to tho8e made for the Army,
The Navy recommended a number of changes to the initial ca»~ ua^y-estimation study. These recommended changes were incorporated into
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
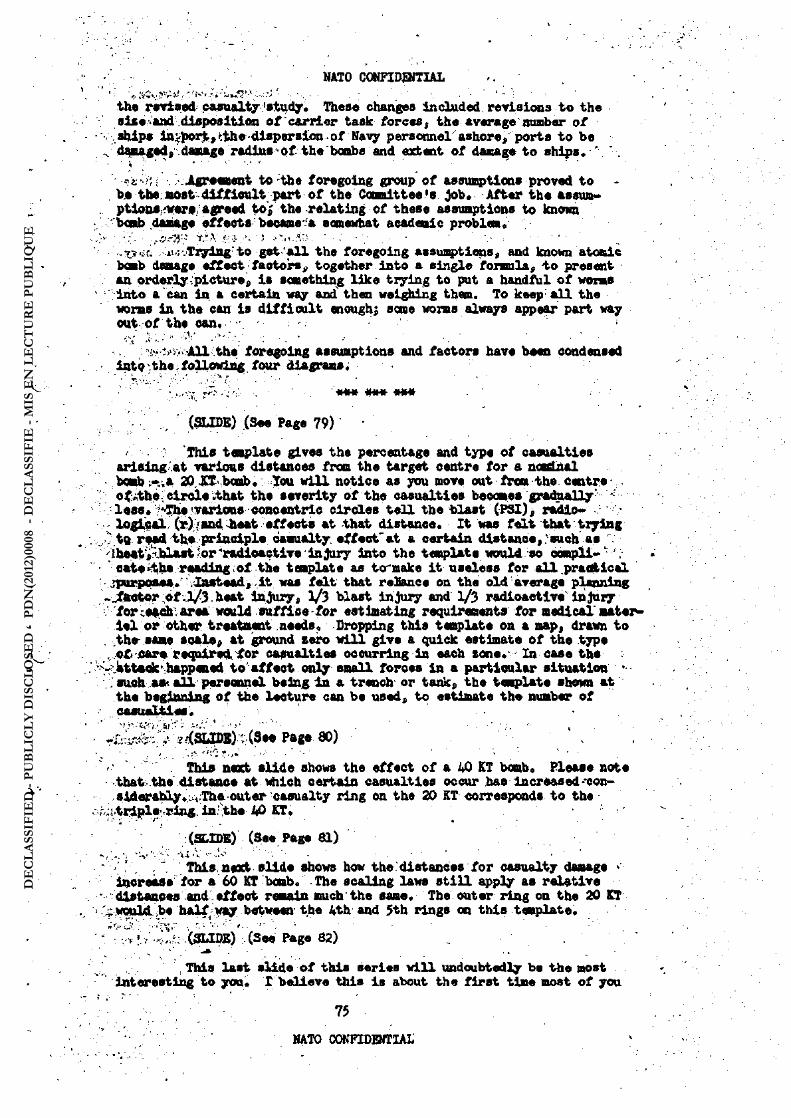
the rtrised cMualty 'study. These changes included revisions to the sise,Vend disposition of carrier task forces, the average number of ships inv]port,<;the-dispersionof Navy personnel'ashore, ports to be d^nagsd, daiuLge radi»s>of the bombs and extent of damage to ships« *
• .¾ "•?*•( .Agreement to the foregoing group of assumptions proved to -be tbs: most difficult, part of the Coonittee's Job. After the assum-ptions;fwere/agreed to; the relating of these assumptions to known 'Ixab damage effects' became a somewhat academic problem. .
-•o>:t. ii.:.Trying to get 'all the foregoing assunptions, and known atomic bomb damage effect factors, together into a single formula, to present an orderly picture, is something like trying to put a handful of worms into a can in. a certain way and then weighing them. To keep aU the worms in the can is difficult enough; seme worms always appear part way out of the can. .
'^--All thej foregoing assumptions and factors have been condensed i^QVthe,following, four diagrams; •
» • -K--T ••'>'. ' MttM MH M M i t 1,( . y * ^ • HHH HM H V|rn
, (SLIDE) (See Page 79)
••. This template gives the percentage and type of casualties ariaing at various distances from the target centre for a nosdnal bomb ;-.,a ZOiJTvbcmb.: Xou will notice as you move out from the centre offlthe. circleithat the severity of the casualties becomes gradually-lesst/^evarlousconcentrlc circles tell the blast (PSI), radio* -logical Or) ; and lieat effects at that distance. It was felt that trying
" to rf»d th,e principle casualty effectuât a certain distance, .-such as *".' theat^bl^ jor'radloactive injury into the template would so campli- ' . «ate^ha reading;of the template as to maks it useless for all practical ^purposes. Instead, it was felt that relance on the old-average planning jfaotor pf l/3,heat injury, 1/3 blast injury and 1/3 radioactive injury forcs^di.arsa waild suffice-for estimating requirements' for medical'matei Iel or other treatment .needs. Dropping this template on a map, drawn to rthe same soale, at ground zero will give a quick estimate of the type jQti J&t* requiredrfor casualties ocourring in each zone. In case the "MtMktIiappemsd to affect only small foroes in a particular situation > such aa< all personnel being In a trench- or tank, the template shorn at the beginning of the lecture can be used, to estimate the number of casualties.
UI - - -y.---y • . • • : . . - , - -
Page SO) .
. This next slide shows the effect of a 40 KT bomb* Please note that the distance at which certain casualties occur has increased--con-siderably ..Theout er casualty ring on the 20 KT corresponds to the
^tt^e^ring. in:;the 40 KT.
(SLIDE) (See Page 81) Ï .. - . J : „ -. \ - -s' . 'V ' .U ' l .1 - - , . - - - . - . '
Thls next slide shows how the dlstances for casualty damage increase' for a 60 KT bomb. - The scaling laws still apply as relative dlstances and eff ect remain much "the same. The outer ring on the 20 KT
: would, be halfway between the Ath and 5th rings on this tesplate. . ;V-jV Vr r- ,.. •<-'-..
-^r(SLIDE) (See Page 82)
' This last slide of this series will undoubtedly be the most . interesting to you. I believe this Is about the first time most of you
75
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
have, seeit a template for casualty damage from a thermonuclear weapon. This one happens to,be for a 5 megaton weapon. Note how changes In the scaling laws have modified the casualty picture as related to distances for radiation, blast and heat effect.. Note the dotted ring which re-presents the outer damage radius for 20 KT weapon.
.„.l . ' .The next step In the Committee's work was to translate these percentage figures into total casualties for selécted sized units of the military forces. This was done. The percent*of casualties was calculated for a battalion, a regimental Combat Team, total combat forces and total Army. Casualties are also shown for an Air Base, total Air Force, a carrier task force, navy port personnel, total navy, storage facilities and FQL faci l it ies, and finally a l l NATO forces. These same figures were regrouped to show the same data in terms of daily.rates.
The next series of four slides presents to you the casualty figures for the groups of personnel I have Just described. We wil l go through them rapidly without any thought of your trying to remember any of the figures. The fu l l report with these figures wil l be for-warded to Subordinate Commanders in the near future. After you have
' had a chance to study these figures« SHAFE would appreciate your CCCinents on the ful l report.
0fJDE$) (See Note on Page 77)
. A distinction is made between the words "hospital** and "Infinuryn..as/used,in this study. Hospital is tfsed to mean a medical facil ity where long term definitive medical care can be provided by an adequately equipped medical staff . The use of the iqoid "Infirmary" may.be a misnomer to many of you. It is meant to include short term bed pare in various types of field units or -other similar medical faci l it ies. :, •'These facil it ies are not as elaborately staffed or equipped as hospitals. Due to limited number of existing military hospitals, i t is considered essential that additional hospital construction be located away fraapotential atomic target areas In order that anticipated casual-ty loads-can be taken care of without loss of beds due to the atomic attack*
^ The ABC Casualty Rates Compiittee was not charged with the res-ponsibility, for developing conventional casualty rates. However, casual-ty estimations due to conventional warfare are Included for the sake of completeness and comparison.
Incidentally the personnel strength figures used in the study were so arranged that individuals could not be counted twice as a casual-ty—that is , both for conventional warfare and atqaic warfare.
• The conventional casualty rates for gronnd forces have been re-studied since,,the .Initial study. These rates were revised upwards from those reflected in the initial study. Conferenceswith Subordinate Commands on these rates have met with informal concurrence.
I t is anticipated that conventional rates for the Air Force and Navy will.be re-studied in the not too distant future.
' , , :A completed study indicates that approximately 11.$$ hospital beds will be required for hospital patients alone at the end of the f irst 30 days. About another 6$ beds will be required for infirmary type care* These figures will be further Increased when the effects of radioactive fall-out are included,
76
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
In summary, I would like to emphasize the following points in thiB study:
First t 11. SSE hospital beds and 6% infirmary beds will be required at the end of 30 days.
Seoond r Positive steps should be taken now at this time to provide for the beds, personnel and medical materiel required to care for the projected casualties.
Third* t The effects of radioactive fall-out were excluded frcm the study.
Fourth i Repeated studies should be carried out to keep the casualty estimations current with changes in war plans and scientific development.
HWW uk^u wuU uiijf MJlM ^nn* ^ K T
(NOTE! Due to the Security Classification of the slides mentioned on page 76, they cannot be reproduced here; however, they will be forwarded under separate cover in the near future).
77
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
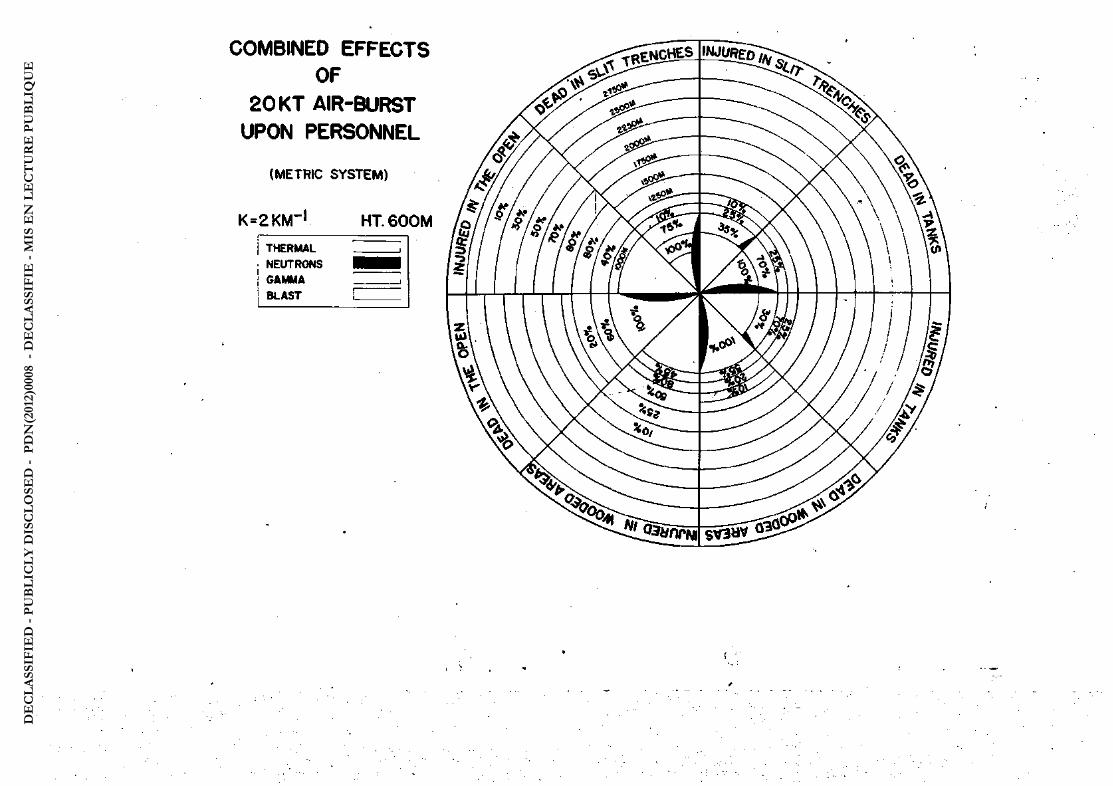
COMBINED EFFECTS OF
20 KT AIR-BURST UPON PERSONNEL
(METRIC SYSTEM)
K = 2 K M ~ ' H T . 6 0 0 M
TFERMAL NEUTRONS GAMMA BLAST
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
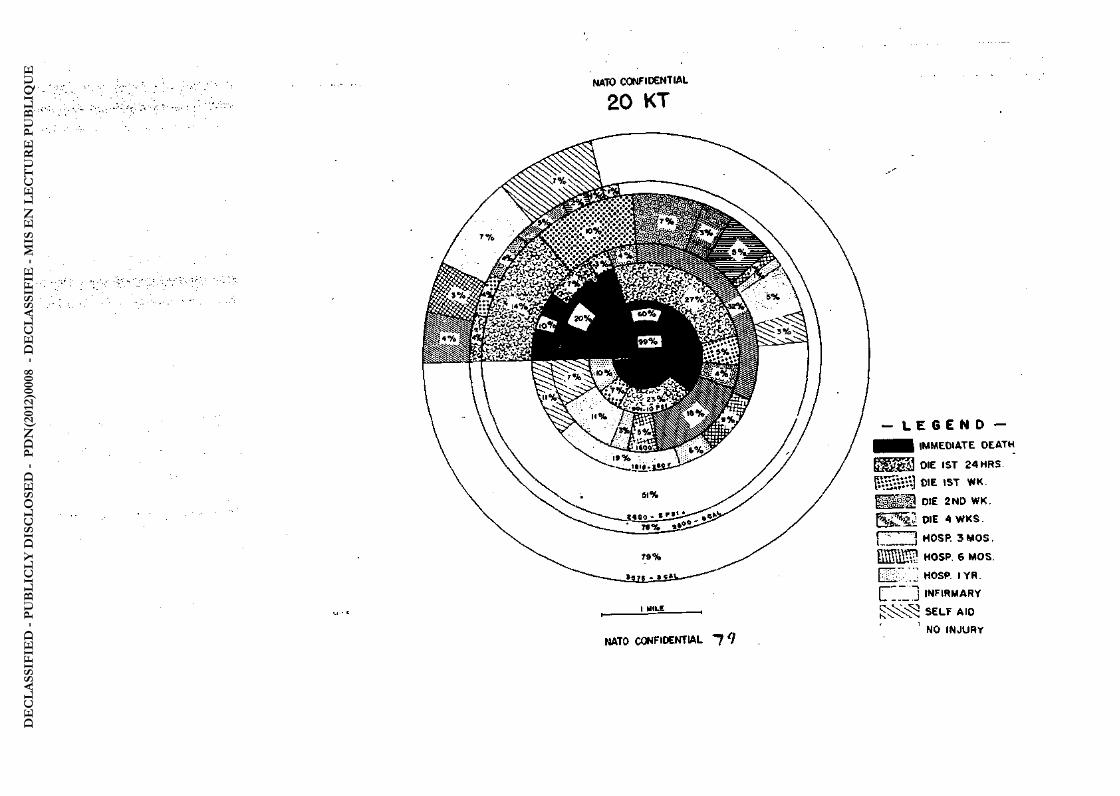
HATO CONFIDENTIAL
20 KT
- L E G E N D -• m IMMEDIATE D E A T H
E j g g ^ DIE IST 2 4 H R S ,
OIE IST W K .
f H H D DIE 2 N D W K .
{ 5 2 ¾ W E 4 W K S .
! \ j MOSP. 3 M O S .
Ë K S P H 0 S P . S M O S .
H i t ' . " HOSP I YR
CTZ'J I N F I R M A R Y
^ ¾ ¾ S E L F A t D 1 NO I N J U R Y
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
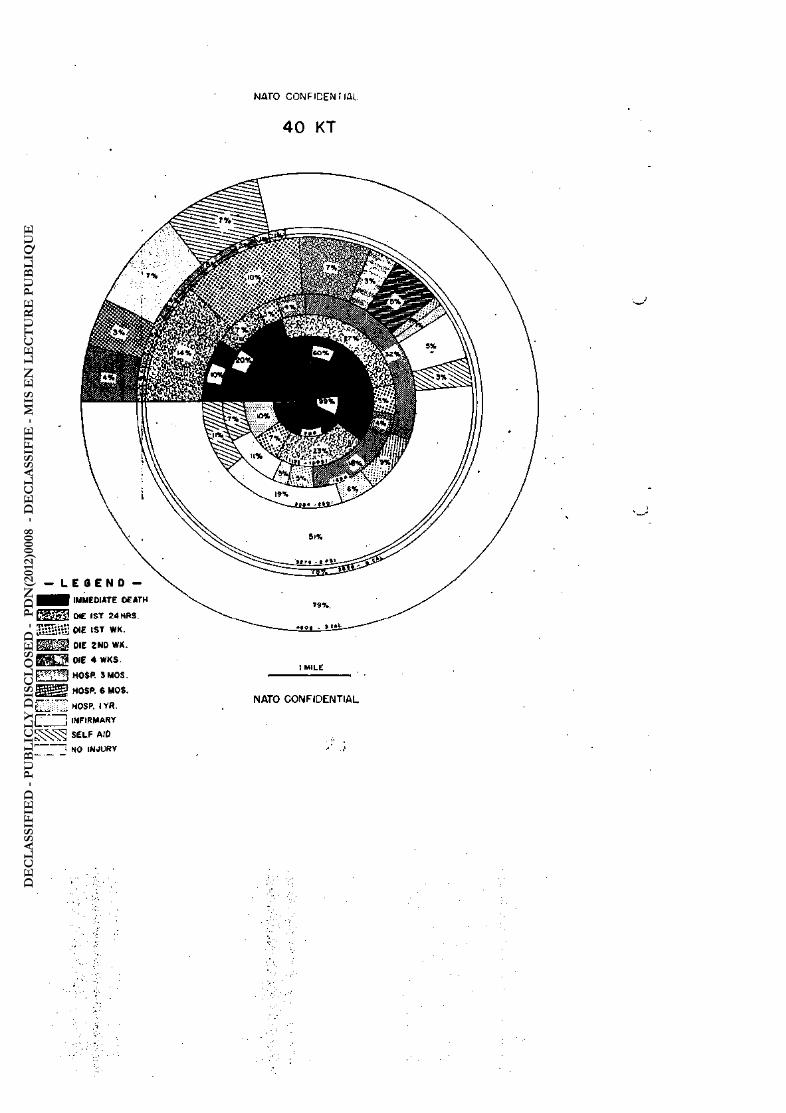
4 0 K T
- LEGEND -• • IMMEDIATE OEATH K g g f f S j OC IST £ 4 HRS. ffli:; w e IST WK. Ü H Ü DIE ZNO WK.
DIE 4 WKS. ' ^ j HOSP. SMOS,
g j j g g g HOSP. 6 MOS.
I MILE
^ HOSP. IVfl
(7 I INFIRMARY
SELF AID 1 : NO INJURV
NATO C O N F I D E N T I A L
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

WATO'WHh HJtN I WIT
60 KT
- L E S E N D — H ^ l IMMEOtATE OCATH E t ä Ü K J DIE IST 2 4 HRS. 1:¾¾1.¾ DIE IST WK. ü l g ü OIE 2ND WK. f r - v C v i DIE 4 WKS,
î I HOSP. 3 M O S . HOSP. « MOS.
r . . _ J HOSP. IYR 1
F INFIRMARY S£LF AID
' NO INJURY
.. m
SCALE I IM.t
NATO CONFIDENTIAL ) »
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
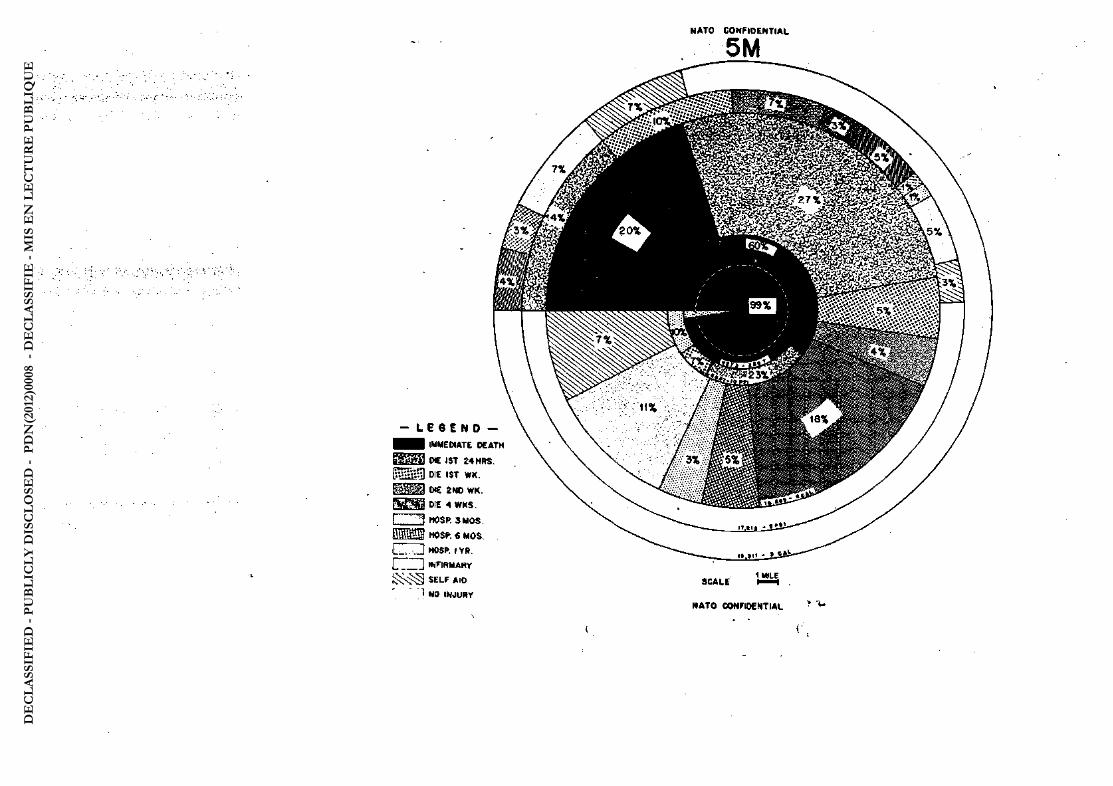
- L E G E N D -IMMEDIATE OEATH
S i S g ä OC IST Î 4 HRS. P S S i i D DIE IST WK. E j j j j DIE SNO W K . S s f o j f l PIE 4 W K S . i ' v I HOSP. 3 M O S . M S i W S * C MOS. . I L S . ; ; J HOSfc I Y R . 1 j WFIRMARy
i^sJS self AID 1 NO INJURY
N A T O C O N F I D E N T I A L
5M
M A T O CONFIDENTIAL y u
(
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
MAJOR GENERAL FASTING-HAHSEH
The discussion on the two pre ceding presentat ions was opened by Major General C.B.H. FASTING-HAlfSlWjl DirectorGeheralp JointMedlcal ServicesillDenmazfc. He gave.an account of tharcurriint state of medical -planning in the Danish Armed Forces, and saidthaV 16£ military hospi-tal beds were envisaged for the future. This percentage can be,increased by using stretchers to supplement the beds in military hospitals and in -auxiliary- hospitals. The real basis oc calCTlatlonivhcweverv-'lPst be- to compute the maxima» number of wounqed that- can becared>*for bjr;"the ,doc- . torsand nurses available. This is the real, limiting factor.
• He emphasised that if-preparations were-to-be of:Safcy wè»-*1^ -. -. they must be perfected in peacetiaf.. i c - I t - ^ -
BRISADIHt RICHARDSON ... ^ «ai? . V, : u ^ i . . - . - , : . . . - S J T ' ' «d- ..•••: ^ £ ¢ 0 ¾ ¾ ^ •
Brigadier Bichardson drer from his researches In-military-' -•• - -history to show that armies had survived very large ^casualtiesclnVthe^ past, and had not »llowed their huge (proportional) ; losses' to defanr •'.*'-. them. T . - - : - ' . . - • • • . v V
GROUP CAPTAIN HPf teS . . ' . .¾ ; jhl* • r "/•• -- - • -':... , -V *>.•••"'•-. . -::-5.- -..»-.*• .
* : Group Captain Cellars wa uncertain as to the value of- "ready reckoners" for atomic casualties, xhich merely indicated the' personnel losses for a given incident. He thought that a reconnaissance'of the bombed area mi it give earlier and more accurate^ information. v >
- ..-..,.- --.-..-.. • -. .- ,-. ' -- •,. Iff.' COLONEL BACH . . •. ,. ; : ' ""
Lto Colonel Bach8upport^thisview,rand'.sa±jd^haV» reconnaissance could quickly give all the information needsd.rV A v. ;> .
. .. , . .- -.--V ^r.;J'VV-Iff. COLONS, MfcBKS -.-- -vP-^- '
, . . Lt. Colonel Marks in reply said that, given certain data, e.g.
energy release of the-bomb'and ground sere, Uie estimated casualty rate, could be worked out very quickly for a given incident*'Apparatus?was> being developed which could provide all required data* on'the'-'batt lefleld .
• -. ' . . - . » . L r f A f - i ^ t - . . . ;; - . GHNlBALflALL V .- \ y . ' > > • . ' • >
In sunning up, the Chairman said that it would be mistaken to look on casualty estimates as an academic exercise. As ah instance, the SHAPE Casualty Bates Conmittes was made up by representatives from all the major Staff Divislwis^ and their findings would-undoubtedly affect future deployment of airfields and troops in the field. The medical -ser-vices also stand to gain valuable data—the proportion; of killed to . wounded, requirements for hospital beds,.etc. V -
. • . - . . . : • - . < • < _ • . . . '
These casualty estimates have a great influence on all types of SHAFS planning; for instance, the Air Forces could- not accept the seale of casualties that were,forecast, and therefore must plan solas' ' not to have so many casualties. In medical planhing VejistiU stand by. the planning figures for hospital beds which we have sent out to nations and to which General Fastlng-Hansen had, referred—thesef lgures are in. respect only of foroes: assigned to SACBOB. , - ' -
Figures showing the estimated number of days casualties of various kinds would.spend in hospital.would be-seut out to nations shortly. .-.-,••. ; /,-. ..•.,-•.• . 7. -"rv. -^yyt
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

INTRODUCTION BY : • (
LT GHI SIR FREDERICK HARRIS. DGffiS
TO EXERCISE "AVEHNUS"
For th« past year or so I have bee« considering, the suitability of oar, that i s , the British, f ie ld medical units for atomic warfare; and by this I mean atomic weapons used both strategically ( i . e . on' ports and large Industrial areas) and tactically ( i . e . on troops in the* CcmbatrZone)
To enable me to carry out this study I have staged three exer-cises in ertlich we have endeavoured to test our present field: medical or-ganization in certain situations which we thought might be reasonably pected to occur in all-out atomic war. I was privileged,to have Brigadier General Hall of the USAF HC as a spectator at one of these exercises and he suggested to me that i t might be'of general interest i f I were to stage this particular exercise at this Spring SHAFE-Study Period. Naturally, I willingly accepted, apd f e l t much honoured by his invi -tat Ion.
As a restât of our studies, we in the UK feel that our present . f ie ld medical units can deal adequately with such situation as may. be -. expected In atomic war; but we also feel that In many ways certain o f these units leave room for Improvement. In very general terms, what.we think is this: ! ,-
a. In the Divisional Area our medical units' ( i . e . , our f ie ld ambulance and f ie ld dressing station) provide for the requirements of atomic War an unnecessarily large collecting potential andtoo eas&U a treatment potential. Moreover their organization Is such that it i s . d i f f icult to provide s special reserve for atomic Incidents;'
b. . In the Corps Area the Casualty Clearing Station is neither' • large enough In holding and treatment potential nor flexibleenough.. for atomic war.
c. In the Communication Zone, and Base Area our hospitals - — ; adequately meet the situation, for treatment potential for both atonic
' and conventional war; but, owing to the fact that very large^niaibers of casualties are now l iable to occur in rearward areas, wi l l require . the assistance of a considerable collection potential which they 46 not require for conventional warfare.
In br ie f t -
_ a. Our Divisional Units need a greater treatment potential.
- b. Our rearward units need a greater collection potential. _
c. Our units between these two zones need greater f le idbi i i ty .
As a result, we have tentatively.devised three ney units j
a. Medical Clearing Unit. . , '
b. Medical Staging Unit.
c. Evacuation Hospital.
The f i r s t two are mainly for Use In the Divisional Area and . would replace our present f ie ld ambulances and f ie ld dressing station.'
04
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

NATO fcONFIDBTCIAL
Tou have been given a "hand-out** which shows a resuaeo f the i r , organization. The intention is that .each division Woold^beiallotted^ one each of these units. A certain number of the clwing„raiitsVand. ,7* a few staging units would also be a l lottedto the rearward areas'to- , -.-collect cases following an atomic in cid eritt here and, conyey^them ^ t o ^ i the nearest hospital. ' ' !' .
The evacuation hospital is intended to replace' our present 1
CCS. You have been given a "hand-out" showing the resume of. Its j .or- ., ganization. . , . , -, ' " : •
The Exercise which follows, and which I have christened /. ••AVERNUS", is divided into two parts?- ; . '
à. The main part of the Exercise, »Aich lasts from 0^30 . ' ., ' t i l l about 1700 hours. ^
b. An Epilogue which lasts from 1715 to 1800" hours. - • • I'-f S
In the main part of the Exercise we s hall, endeavour to show you by a series of playlets how I believe our prèsent . f ie ld .medical . units would work in a campaignin which atomic weapons: aré'hëïngVirtÂ..,-..• both strategically and tactically. We shall try and. show in. what respects these units have failed—and here I,hope^we'sha^M*®Jpoiirj1^i, criticisms in the discussions which follow certain of thé'sérials. ^ The unit a mainly involved ares • : ' - v ' P V T
a. Division Three Field Ambulances,,,;) , 'Per ,-.-,-. • , - ' ;;{ Infantry.'/.
One Fd Dressing Station") Division J ; ..• • • • . ... t -.. .- ' : i >.\'• b. Corps Three Casualty Cleailng.Stationa^; .
' c. Amr. Com Z and General Hospital^ at. (fitiieïiï,<mbulahee Base as required. Ten Field .Dreasing/yt j ;
Stations ., . . •
The size of the Force is an Army of three Corpscoaprising/ the equivalent of eleven Divisions, with f u l l logistic ^support jgLving in a l l a total of half a million persons. The head of^the ;medlMl^-c. 1. services for this Force is a Director of Medical Services with the rank of Hajor General. The head of the Medical Services of the Mniy . is a Deputy Director of Medical Services (DEHS) with the: rank, of / : Brigadier. The head of the medical services in the Communications . Zone Is a DIMS with the rank of Brigadier. The head of the m e d i c a l - -• services in each Corps is a DCHS with therank of Brigadier, while the medical heads in Divisions and Areas are. Assistant. ïklrectorsöf^Medical Services with the rank of Colonel. Uostilitleis are assumed, to have •'..."., broken out on 30 September 1957* In other words, 30 September 1957 is D-Dsy. "... . . t; ,:.,.-- •
. - • -, i - -i . j : - .^ . ,^ ,7 .-1-(. j1.-
a. In Serial J l you wi l l be' given the military background . to the Exercise. . . . , . , ' -'
b. In Serial 32 the Director of Medical Services, of "the..Torce will, t a i l you how and why he made his plan. Remember he only nasour. present standard f ield medical units at his disposal. , j . •. Zj .1,,,
c. In Serial 3U you wi l l see how his. plan copes with .the^^ situation in' the eight days, which follow the outbreak, of wir Von 30 Septmnber 1957. , ' . ~ / r ^ " •
85 -
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

NATO CONFIDENTIAL , • 1 ' .
d. Serial 35 allows three quarters of an hour for discussion} and, while I welcome criticism, I must point o<ut that a l l diseussiön ,v periods are strictly, limited to the time shown oft the progranaie so that I would suggest that every speaker limit his remarks to.5 minutés'In^this . f i rst discussion and to 3 minutes to subsequent discussions,
e. In Serial 37, the DBMS 3 Corps wil l explain his plan.to deal with the anticipated battle in 3 Corps which is expected to,starts on D plus $.
plan* f , Ai Serial i|0 the DCNS 2 Corps wil l similarly, explain his
g. While in Serial IS, you will see how his plan worked'.
h. Ih Serial A3, the AIMS 46 Division w m explain his plan to deal with the casualties expected in his division .in, the battle ex- t' 'pected to start on D pins 9. , v -
i . In 3erial 46 I shall try to explain the puirpose of Serial /»&. In this I shall be assisted by Colonel T,M»R. Ahem. " 'Tt . ' ^
J. In division, equipped battle' in which atomic weapons were used tactically* I would rmind you that in this serial these units ares
Serial wev shall endéavoùr -^ f în - în ï iS^ry sd with our new proposed field medical units, 'fared *in ,a
r> ' , i . 1 Our Medical Collecting Unit ) To the i i . One medical Staging Unit j Division. . ' , , .
One final word,, with one exception, Gfc. Captain Baricer, RAF, of SHAPlff1T a l l the officers taking part in Exercise ttAVroNUSw and in' its , S^ilogue are members of the BAMCs and their assistants,- .who put down'./ and rembve the various models, are other ranks (what our friends in the U.S.A.• CaU'' 'enlisted men1 ) of the BÀMC. Hay I say that I and a l l the . offloer*.fend other ranks are proud and gratified at having been given the signal honour of presenting this Exercise to you today. ,,-
: ' "i shall now ask Colonel Marks to give you the military' back»,-ground c>f the Exercise.
uub J^w «jtjâ; JUQt• nWn ^HfTV TT^tT Tnfn inn ï
LT. COLONEL MARKS (Exercise Setting (Serial 31)) • , i . ^ - - • . i ?..
It is September 1957. Following the implementation of the Paris1 Agreement of 195V55-, a defence force of twelve Gerinan.division's., has been organized by the Federal Republic as part of the NATO Forces-,,' in Europe. Taking advantage of the Western Powers pre-occupation'with ' the ever-expanding Ccnmunist Chinese advances into Indo-Chinaf Thailand, Burma and Tibet, and also the Chronic Israelis-Arab feuds, .in.the Middle East, the Fantasians have been building up their forces in'Eastern,,,..., Germany and the satt elite countries. As a result of the finalbrealc*' ' down of the Stockholm Disarmament Conference in July 1957r Fantasia and her satellites withdrew from the United Nations Organization. ^ A r , "blow upn of the cold war into a hot one now seems inevitable, /It i s " known that the Fantasian ground forces in Eastern Europe include a core of highly mobile armoured divisions with powerful self-propelled ., artillery covered and supported by the Fantasian Tactical-Air. F|orces* They also possess a number of atomic and thermonuclear bombs and atomic artillery, guided missiles with atomic warheads and are known to have' stocks of nerve gas. '..
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
The Bcitish force of one Amy, three Corps and eleven equivalent divisions,, say 500s000 men, is part of an Amy Group deployed against the Pantasiana and operating in IÇrthland, /which . is a friendly industrial nation whose fcfrces are part of-the Amy . Group. Therehas been a period off strategic preparation; and the . British force has been deployed fully in lfythland.
The Br^tish Puree Maintenance System is superimposed on Mythland's rearward industries andon which considerable reliance•.-•-'.:•!.••>^ has been placed for heavy workshop facilities^ etc, and the use of * MythlandtS ports which are about 36 hours sailing frcra the U.K.
Myth land is an industrial country and therefore has eoc- ., .r cellent road and ra i l ccotnmicat ions which i t is almost impossible to interdict* There are 6 modern airfields and a number, of smaller ones.
Civil Defence in Western Europe has been organized . - . o n - -NATO basis on the British model and Hythlahd has s small but effec-tive CivSl Defençe Organization. ,
I 1 - ^
The floor model represents the part.of Itythlahd..in which the British Expeditionary Force is deployed* It is some 200 miles ~ r
long by 12$ miles-wide at. the base. The country is generally feature- ' less and undulating, except for sope hilly ground in the.Upper Lethe , Valley., Thè Hiver Lethe itself forms, the eastern boundary, of Mythland with Fantasian occupied Europe, FhHher north the river turns.iwest •> -and forms a wide ^stuary at the north of the model*' Tou see some of -themain roads, railways and airfields marked: on the model., . , .
Megalopolis is the seat pf the Mythland government and has a population of about one million.' • . . •«.'
•The four principal ports of Mythland are Kohaiothezgreat „ v peart on the Lethe. Estuary, taking a l l ocean going vsssels^r.Susa,-a . smaller general purpose port taking vessels, up to 10,000 tons j -, . Scylla is a good port of the cross channel type and,will be used.in-the f irst Instance for personnel, reinforcements, leave parties,.'etc, ' and is the medical embarkation port. Charybdis l s in the south, and is another large port capable of handlingtanks,-vehicles ,ammunition and general stores. Petroleum'products wil l be handled primarily by the port of Susa which is the base of the pipeline but a l l ports have , seme POL landing faci l it ies. Between Scylla and Charybdis are two •• small-ports of Eleusis and Chalkis both taking vessels.up to 5,000-, tens and there are numerous good beaches to which reasonable road-approaches are available.
Apart from Megalopolis the two most Important towns in:the Com Z are Krokamnia In the north, and Myketia in the souths : each., with, a population of almost half a million, , Keos is a centre of communi-cations set back inland from the southern ports. -
The industrial area of Mythland is a broad,belt in the area between Mona-Memphi s-Megalopolis and Troy in front and SparC^Krokamnia-Myketla- and Charybdis behind. Oor forward base is in' the general area, •> M«phia-MegalopoIis-Krokamnia with base- Installations around the four main ports and a staging organization and same depots around Myketla. ' r-Installations are well dispersed and away from the towns. GHQ Anqy :. Group is located in the spa of Elysius and HQ Com Z is outside Krokannia
Now let us go to the forward areas. We are holding the line ; of the Hiver Lethe with three Corps. 1 Corps In the north is in an orthodox layout with Corps HQ and its Corps Maintenance Area 30 miles .
07 •
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
behind Arcady. 2 Corps is in the centre also in an orthodox Isyontf around Pelnsium. 3 Corps is in the south holding its front with a - ' forward main position or bastion of two infantry divisions and-an, -armoured division near Marathon. Main Corps HQ with-Corps?MaintsnaneeV^ Area i s some 40 miles back In the area of Tartarus;- Let us mark-the^ *-: intercorps boundaries and rear corps boundary. , / / .-^-.¾
Kw Aimy area extends back to its rear boundary east of Memphis-Hegalopolis-Trcy. Army Headquarters is in the vicinity of - , Olympus with its AMA and medical installations dispersed to. the '.west;"
AIR ••• ; - . .-'- • c»
General •! • .. <•'.. :v r • v ) 4 M .
The appreciation is that the Fantasians will-be able toi-i S „y.: v
exert air superiority from the outset. Air support, tactical, - .. ^¾¾^, strategical and transport for the British force is likely to be very' v ' limited for the f irst three months as the main air effort will be directed to defence of the UK and to offensive effort over Fantasian^A«,'. occupied Europe and Fantasia itself . •-,A^V-ij..
Casualty Evacuation . ' r > "
There wil l be no regular air evacuation,neither by^meditim: ')/., aircraft within the theatre nor by heavy aircraft to the U K. -Urgeht-^ ' pttoritystores will be flown in and forwarded and th es e àircrâft - Vili^îî be available for casualty evacuation on their return^ journey.^^ThereiC»^ will be normal light aircraft and helicopter availability fc^^urgent' LM casualty evacuation in the forward area. "lThirty sortiesper'corps, per^< day have been so allotted. . '„ - • ,sv
Movwtent' \ V
sWell dispersed road convoys wJJJ. be permitted by day be-hind CorpsMaintenance Areas and i t is proposed to. run certain trains.-p including Ambulance Trains by day up as far as OlympuSp but It mayv.T;X prove impossible to run trains forward of the Army Rear Boundaryf *f.f joS,-. except at night.. - • • j ,,.* > ^rxil »rtJ
-..-.- , - . « if.C hi'. • Operational and Logistical » -.
r . , .L.-i ts Vs^eiWS ^ ^ ^
Military Intelligence , consider that hostilities * are; prfcbatymî ? within1 a month of this time and that i f all-out war starts the Fan- V < v}4 tasians will not hesitate to use nuclear weapons, thouj^î"it'is^thouä^t ^ , that the Ifydrogen Boob will not be used tactically. Thsy believe tpat" ' it will be a case of "no holds barred** and that the enemy will* gor f o r ^ a quick victory by using almost a l l their atomic effort within the f i rst few wesks. The'-probability is that the following targets will be • ; attacked Ih this order in rapid succession* • >• .1 --'t y* iy'Vr,^ ;
.-,- - - i •' t s ... ,- -- k ' , • ' • . . • * ' ' ^ d.;"'^. " «
a. Capital Cities and main centres of population^ e.g.^;». J* ; London, Paris, Brussels, Megalopoliss followed bys , , ; ..-:
•v - •'-. • - -.-.-• •-"•-'rv .. ,/.«..;• b. Industrial centres such as Binainghaa1; Coventry, Liver-v
pool, Tjme and Teeslde in UK, Li l le, liege, Valenciennes, etc, on>the^',;' Continent. This phase might include attacks on atomic production^ though this would be unlikely to have inniediate' effect on our ability to re->-taliate because wefcave been stockpiling atcmic weapons for six'years.:
,•-•:••••.'•• . v - . i. / .-.- • '<i' O^v" •
c. Main ports and airfields, using perhaps "some underwater : ' •buret bombs for the former and perhaps ground burst bombs fori the latter.
---1 '-.'„V '.i V
1S
' . 88 • . ' • v
: • y.1 ; ;
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
He would make every attempt to interdict, ccmiuhieationsbertween the W and the Continent so that ports and airfields on^both sides of the ' Oumiuil would be attacked. ' - ' • - 'V " •.
td. Haying thus attnpted to disrupt centralized'{government, civilian morale, key industries ahd communications/ he wi l l turn his 4
attention to the sector he proposes to attack - Thaiftdi^tioris are :'v';* that he will mount his màin attack against the British seetor'br'albhg ' the Junction of British and American sectors to the south;-" ftI v'^vfr
s. Atomic attacks can' therefore be expected'©à'i&rtfcV'ai*4
fields, centres of communications, installations and headquarters in ,.
our Base and'Cms Z followed by attacks on the Armyx Maintenance Area and possibly Corps Maintenance Area. ' •'! '--J-s
f . Having produced a considerable degree of disorganization and chaos in the rear areas the culmination would be the,use of tac-tical bombs on the division or divisions through which' Ua intended to*1
break so that he could effect rapid' and deep penetratiofr 1^^-00^ dis-organised Com Z and Base and make the channel coast ln'vthe^idnlmm--'-;1 .
•time. •• !.••••;•'•*; - r ^^ - : ^^KW^
g. I t is believed that tteFaxrtasian rtockpile-bf atcmi^V . weapons is quite sufficient for theirpurpose both'-strategical''and'-'* :
tactical. Any worthwhile target Is likely to*be' attacked;-4' i
WLth these possibilities in vi«w Q (Movmfents) W v ^ äedüeiT' '; that i t is inadvisable to have exclusive commodity ports' rahd >ill/portfe: " must be prepared to accept a l l types of cargo within'-their Äpa&tJy/^ Installations are duplicated and are as yldely disperSedas'èff iciertt , handling permits. Only essential personne^ egp Port Reglmehtsy-ire^' '
' located in likely target areas. Alternative rai l and" roadroùtetf.'are' planned and the maximum flexibility in tjie system' bfkatoenajteê'is ** being carried out. ' ' , . / - a -y^»-. y.r>-- : • - - . . ' - . . . ..- • -r ':><-, rff - "-.'-?• •• - >
On the operational side, every' Base'Sul^Are^tthd »CSiptf®^-;-Cotnmandar has been ordered to organize mobile columns' bh Defence model from his own resources consisting of elmnents o'f^the»^ ; following arms; , ;
Infantry and Pioneers as general duty troops ;
Engineers -. .. • SuppUes and Transport .. .'v.. JZ>1 " Medical -.r;-"'
' / Provost • V .-::•-,• .:. - . i '•; • ••• ; : - , . .-: -.., '. . i. ' • «$.: ' ' .rr. i'V:-:,-:1,: • -Complete formations or even units are Unlikely to be^availiblV 'for^ ' t
this task; so the column will have to be ad hoc, pre-planned and •' **•' • rehearsed.1' - • ''•••• L t-
The role of these columns wil l be deal with* At col c Incidents' involving military Installations and for assistance to ciVil/deferice'. i f required. Their tasks are likely to be s , .- .
• • ' 1 . , • ' ' - 'r ' '' •' • " TV* ' ' S ^ i
a. Rescue and Debris Clearance ' ' ' » - ~.vl: . Wra^«^* .
b. Assistance to f i re services - -'• • 1 -.- < '
: • cv Treatment and evacuation of casualties arid- provision"bf' ;.BWdical-supplies. :-- :-"-. ; .,: .-. . •• , ;.v. :, v,;.!-;.-:.''-,'. . - . - ' t i t :. •...•.'.. " :-.. ..„A:.-:-.--;:^
d. Oontrol of refugees especially on military routes. .
69 '•'''"'!-:";'- i' '' • , - o - I a.-.-vS-.-.":.-''-', •
NATO CONFIDENTIAL .., ••*
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
e» -Transport-
f . Estergenoy feeding
g. Burial of Uie dead
' With regard to assistance to Civil Defence, the Mythland , : , ' authorities had been told that we cannot guarantee any help what- ,-i,\< ' ever. In the event of continued attack, however, i t is certain that-for humanitarian reasons, to sustain civilian morale and .to retain our large civi l labour force, we shall have to do so.
In the forward area, Army HQ itself has gone-almost cent- ; > pletely underground and the AMA is dispersed over an area of 50 ,, , ,-, square miles. One armoured division is held in Anqy reserve north of Olympus as a-counter attack force. , >
t As has already been said, the northern and central Corps ,^ » are deployed in a more or less orthodox layout, but are holding wide.-, a fronts. Bach Corps has one independent Minoured. brigade under command in a counter attack role. 3 Corps in the south is thought to be the „• ;: one most likely to be attacked. The Oorps Main position is a two-divisional bastion sited on good, tactical ground east of the cconrani-cations centre of Marathon, ^ain Corps HQ and its: installations^are^ ; if> miles to the west in the area of Tartarus. Ö Armdi Div is under /;, ctrnvand and Is sited at the western end of the gap between 3 Corps and 2 Corps. There is a similar gap between 3 Corps and 17 (OS) Corps to the south who also,have an armoured division in a similar position.-^ iz-yr'
Divisions are well dispersed down to battallon ieveiy /- " battalion being about 2,000 yards apart but occupying normal frontages. AU possible troops and installations arp dug down to as great a. degree as possible for maximum protection. ^ ^ ^ , ^ - - . 7 , ^ , - ,
The tG,' .estimate of casualties frcm the ground battle is -1,250 daily, <including sick or some 30,000 in the,- firstrmonth. , The wastage rates for both conventional and atomic warfare have_ b e e n . , worked out and were given to, you in a previous serial. -..,1.,-- - v ; ' "
ia^^l U^tu ^^^d «^nr ^^^^^ ^n^n ^^^^^ ^^HT ' i ' •' - " ' 7;. s
D.M.S. (Army Sura«*mt«)pi«m on DmfflaasV - , i . e . . 26 September'1957 (Serial 32) . r .,
».. v .\ • - . . • ' .
The EMS of the Expeditionary Force, Major General Hopeful, arrived at Force HQ some days ago, and, after numerous discussions with -the Chief of Staff, ha* made his plan ,to meet- the onset; of> hostilities -,-which is expected any day now. . > It is 26 September. 1957} and, although the IMS naturally .does not know this, i t is 4 days before the war breaks out. In other words, i t i s D-4. The IHS now presents his plan:
TYPE OF OPERATION ' ,,, -,7. ' • „-.-'o^'.
Jn making my plan for the medical arrangements for the BEF iii Mythland, the f i rst factor I considered wastheType of (Operation.
Initially, we expect a defensive battle in well prepared positions, but one in which the' atom bomb may well be used by both sides both on the front and rearward-areas.; : Our own offensive is unlikely to' take place for many months. (We
are told that the H bomb.is not likely to be used on Mythland, and therefore I am not considering'-lt in my plan
NATO CCWFIEEtiriAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

My plan therefore bad to eater for & defensive/ground battle with all the usual ingredients like conventional banbing and mining. At the sane time I must be in a position to cope with the eocbra casual- * ties resulting fron a number of atailc incidents not only In the Cai Z, and Base but also in the forward areas. This obviously required a. very*? flexible plan and in fact it has been stressed-repeatedly In planning • j that the whole administrative and maintenance syst m mist be flexible, j I did not want to do any major deployment specially designed to meet the : atomic threat. Hy aim was to use a more or less standard deployment j of J. medical units which would enable me to deal with the 'foreseeable problems plus giving me the flexibility to deal with any of the variations which i -would arise. \ < >; tef . • ' !
MATUBE O P TERRAIN AND CLIMATE / \ \ : * ^ ^ ' • V j
Naturallyjl I considered the terrain and climate, but,' apart'•'• i from the exceptionally good road and rail ccimmmications, which not only ,} extend right frcm the front to th« Channel ports, but which also are . -very well linked laterally by numerous cross-roads andrailways,the"' • features are not Important to our discussion today—so I shallileave ' th SB Out « /; ' • ' i -
, . ' • ; • : v • "., r, ,•„•:'•• '> •• EVAOUATION OP CASUALTIES TO THE UK '•'•"" J.1 /•'•'••'. •;*>.,)•
I would like to spend a little time In giving you the bae&- , ; ground of evacuation of casualties to the UK, together with "a word on; [r my meagre resources and a hint on how I feel about it all. V ' ^ Vj ' ; *
• ' ^ '.-••• ' .....' • ' r ' V .• » • j/
I have been allotted 6% hospital bed.cover ofthe strength of! the force in Uie theatre. -Fran conventional Varfare this should suffice to enable me to normally hold in the theatre all those caaualties^likely to be fully fit for duty within three months and evacuate the longer. ; tern eases back to the-U.K. where bed coverii^available for the BEP in Mythland. However, this is not conventional warfare and injthe opening stages It has been agreed that I keep ny hospital )beds'clear'by evacuating all but the most trivial cases, back to the U.K., i.e,, 80 , ^ '' Sfc • >> • j
FVooi this you can see the success of my plan must depend on • j two factors which are not-within-ay control: ,-.. '?• ,V ^ f .> J
t people to^Ä^'ftr'"^;»*'^?. n^U.K. port's. .. '
a. The ability of the Sea*Transport casualties across the Channel and land them in'
b. The ability of civlV&nd/or military hospitals in the U K ^ to take in and hold «y casualties right fran the start of operations.,'Ji J
:, .-. '... ..- * - K
I want to make it crystal clear franthe cutset that I feel , ! most uneaay about all this, , ^ . j
I am certain that the enmy could—in fact, can and will— '<• succeed in reducing or even stopping our sea traffic across the Channel • by means of atomic attack on the ports on both sides. Gveiu lf the entgtj only achieved a JOjK reduction of traffic for a week or 1IO days ny ? t ' situation could well become serious. The estinate of casualtieB ie >-.T |'. 1,250 per day for conventional means only, and alO day block is thus 12,500, exclusive of atomic casualties. Also, the event of ä total j cessation of traffic for even a week, coupled with atcaic incidents, '" • j would make things very difficult'. * •;:'-< .'-'' V- " ';
• . • " s "•
There is also the problem which Is bound to arise that the'flow of casualties within the theatre may—indeed, will—be severely inter- . -feredwith, ' -y 7, •- ,,.- . \
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

There Is a further possibility that the en «my might succeed '-> • in disorganizing, by means of atomic attack on the UK, thejcivil
medical services there to an extent which might well prevent my casual-ties y even if they got througi to the UK, being accepted by civil hospitals during the first month or so of war. . - . - !
What ga*;e me some anxiety,was the question-df 'collection in the Ccn Z and Base, The General Hospitals are hot designed to collect V and in any case will be fully occupied treating cases.' Hy mobile units are now up at the forward end • and I cannot rob the forward end since they will be fully occupied. I therefore asked for three Field Amtailancss as my atomic reserve and I don't think it's toomany...Wv • However, since we have as yeb no actual experience;of atomic warfare : , we can only wait and see. ^ . . : • , ;
•. • • • ' . ".• . •.'• •I ' ,-:-ATOMIC IMPLICATICTiS . ^ . /. , ...,:
I neoct considered the. implications of atcmic warfare/on .the, , ' medical services. I appreciated that there waslittlenew ln-.the -.-.y ,.-type of injury we should have to deal with—the burns, the;blast;j In-VV,. Jwy and radiation sickness, which is reasonably well understood. -,. .. . Though the problau of a severe compound fracture with a O fcurnj off .<-• the legs and trunk plus a probable dose of 200 r struck me as -being a pretty tricky surgical problem. I passed that one on„to my aur- •, gical consultant. ' 1V - ' ' ' - -
. -,, . . -.-: . • '.•;•••,••.• t v . - , - •
The main difficulty of atomic warfare was, of ,course, the- v-.* tremendous number of casualties occurring at one time and -occurring suddenly. In addition, the problem is increased by twö: other, major'v-: \ factors Î .--V -
" .. .- ••'• /. -i-rl-Hi.-<•:'. V a. Gross destruction at the scene of the incident whichî -.I- '.- >. »'r1---'; • ' :
1. Might wipe out the entire medical. units :'>- -)-,1- . i i . 1 Hinderevacuation ,-!.- . >-'.J i l l . Delay medical aid, and stores, getting onto ttfe
, scene of the incident* ;;,•-.-.>
b. The special nature of medical stores- required: - - : , .=--. * . . . . . . . . . . . .
i. Barn dressings v . -. • -.-' •-' i i . - Oilsd silk gloves -. ./.-/.::---^- . , I i i . • Penicillin- -: iv. . Blood, Blood Transfusion Equipment ;
Though my supply of 'blood was a colossal problem-in itself, (I passed that one on to ny DD Path to chew over), I was most con- .. earned/to know at what level, and at what time after woundingisthe/ optimum time to start transfusions for burns? I am still not certain : but shall certainly hope to know after this show is over—«y impression is-6 hours maximum. . '• .•-»••v--'. -
CASUALTY ESTIMATES - • ••-...•.•.- - --. - -: . • , •• C/- //V. -y-wr; S11 /
In. consultation with tG'> we estimate that casualt lesirecpilring treatment in medical units wiU. be 1,250 each d^'from conventional V : weapons including sick and Injured, and rmember I am evacuating 80$ , per thousand a day back to the U.K. , , - J . - : •
Casualties fraa atomic weapons were more difficult to esti- ' mate as they depend on so many varying factors: ' * '//
a. Number and power of bombs used.
93 ï ^
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
b» The height of the detonation. , ,'•
c. Meteorological conditions.
d, The nature of operations they support, eg, defence, / '^ s i attack, river crossing, etc. ' ! - ,^wf
~ "V • ..-.1
e* Thedfnslty oftroops onthe ground in relation to GZ, '.
f . The degree of protection of the troops. ' ^ r ^
Of course, it's obvious that the estimated casualties^can vary within very wide limit». Before I left London I found that threes-author itiesh&d issued guides as to the numbers of casualties which "•'•'. might be expected under certain given circumstances. The British had estimated and published tables showing the casualties which. be expected in built-up areas—this is obviously applicable to the Base-.'.-and Ccm Z. SHAPE had also prepared apd issued tables giving estimated 60 day wastage rates for troops in Theatre.7 Our own Ar»y Operational '^ v Research Gtroup (ACftO) had recently completed a study on the subJect^^^V Indeed, Dr6 Gadsby of AORG had devlsed'.a most ingenious and 'handy readyT? reckoner showingnot only numbers but types of casualties within .radii of varying length from GZ (Gadsby Gadget). The figures given bjrvAORG'fV are possibly more applicable to the medical problem, while the SHAPE ^VV figures are at the most valuable in calculating reinforcements.* :.-^..4
- .«'J'S iïïrÇ ÔV
Assuming that 20 KT atom weapons are used against well-dis- y ciplined, well dug in troops in a prepared position on a clear day and : " detonated at 2,000 feet, we arrive at the figure of ,sàne ;2> 500 -I itV t t^? casualties per division—these'would be produced by3 Ojri k atomle^^ 3¾^1
weapons.
If I assume, and ny 'G' says it is quite likely, that the.,. ' enemy will explode up to 8 atomic bombs on the Army front as a pre- .-Iude to his main attack, I therefore estimate that I might expect at the / height of the'battle to have to deal with 5,000-6,000 atomic casual-ties in additlon'to those resulting from conventional weapons, in a = •' Corps. These atomic figures are maximum rather than minimum. ; v: /
. , .... • .. ', •.%-*••:• v/ TOTAL CASUALTIES MJRIHQ FIRST 2 WEEKS ; * ^ ^ / ; ; , r ; 'V
Prom the above rough èstimatê 'of what might reasonably be the position regarding total casualties requiring treatment in medical units during the first two weeks.
f r , ' ! .
D to D PIXJS 7
This would be a period when the enenqr would be building up for his main attack and the enemy resources are sufficient to allow " <- ". heavy conventional fighting all along thé fronts At • 1,250 'casualties11
per day this adds up to seme 10,000 casualties for this phase'.' In \ ; ;, addition the enemy is expected to attack the Com Z and Base civilian -industry, communications and ports—this is mainly civilian and mili-tary casualties will be mixed'up witha much larger numiberofi civlUâiisïv How many army casualties there will be is almost Impossible to estimate, but I feel it cannot be less than 1,000,' while the SAP airfields are.bound to be attacked and a further 1,000 RAP casualties would be'a low*estimate.
Therefore D to D plus 7 is taken "as 12,000 casualties; '
D PUIS à to D pujs u • ••• -'• — A' ..-.-:
The main attack is likely in this phase and is taken for conventional casualties as in the first phase generally,'.plais ùp to Ö
' % ' • :• / - ; .•: ./.1:.:1.11-,
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
atonic weapons tactically on the forward area, which is estimated to give sane 4,000-6,000 casualties, though this.may vary considerably either upwards or possibly downwards. Irt addition],." the severe critical battle is estimated to produce a further 3,000—during the battle attrition D plus 11 to 14. This would give smethlng like 20,000 casualties to be dealt with in this phase when everything' • will be arcy larcy. -- .--.- -i . -
D to D PLtTS LL '
The total I expect, subject to the probability; of.wide v ',;«1, variations, is in the order of 32,000 casualties in the first 15 days which will be the care of the medical services, -
CIVILIAN CASUALTIES " ,
I would like to deal briefly with civilian . casualties.^ I was informed by the War Office that CD in Ifythland : is-: good, and that,, if atom bcmbs are dropped on their portB and citles,the. whole; medical; , side of their CD can be expected to put up quite a good show. At all/i^, events, I am making no preparation s—-and In fact I am unable to'do so-* . to deal with Kythland civilian casualties. .
MEDICAL ORDER OF BATTLE -.../ ^ ^ './..'
I think I have now considered the various factors and the--task, so I will now look at what I have been' given to deal with, it, i.e., Medorbet. Tou will see from this drop what the Ordert, of j Battii-is, generally a standard nSUSteritynOrbat. The important exceptions ^ are that I have three extra field ambulances. Tou will also note the -allotment of General Hoepital beds is 6 per 100 troops on à force of v half a million, which equals 30,000 beds,
I would like to remind you that bed cover should, deal with-conventional casualties most adequately^ plus folding those-,likely to, ;-prove useful in three months within the theatre. .1 have not asked for more beds—i.e., I have refrained from asjking for more medical manpower at the expense of combatant manpower in this battle for survival.. In- • stead,-! have arranged equipment to enable all General Hospitals to have 50£ crisis expansion to deal with an emergency. In other words, .this gi+es a 15c000 bed reserve for the atomic threat. I must add that I ' have obtained an allotment of labour of 50 per 1,200 bed General Hos-pital and 25 for each hospital snail er than 1,200 beds and for.each CCS* It will free RAMC tradesmen for their proper Jobs.. :. ; ; v ;
P L A N
CCTERAL PRINCIPLES
I think It would be profitable if I quickly went over the-. main principless
' •• ' . . ... - • • } / - ' • < . - . - . •• . : , - /
a. , I must have enougi hospital beds in the theatre to cope with considerable interference with evacuation to the UK and with . .. '•= potentially large influxes of atomic casualties plus conventional": casualties at the same time. As'you know, this is the present- ease-*-/ -: I have 6% beds which I have numerically raised to 9% by crisis expan- : sion with^ I believe, a not too great sacrifice of medical standards.
b. I must deploy my hospital so that;
1. They are not- in or near likely target areas. , i i . Alternative evacuation routes in the Com Z are.
. covered and as far as possible they; are, mutually * supporting.
.-- 95 : / <•/" -NATO CCNFDIENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Ii i . Thsgrare in a position to evacuate to ports • . - • ncr or beaches other than Scylla., ^ ¾
iv. Crisis expansion up to. 50% can take place. - • ..-•
c. Hobile medical cover on the Com Z - Scne form of mobile^ medical cover must be found for the Base or Com Z and this is provided O by the three reserve Field Ambulances.
d. Evacuation Routes to the Ports - Duplicate routes, both• _ by rail and road, must be planned from Corps to Amy Hedical Centre and thence to the Channel ports,
DEPLOYMENT OF MEDICAL UNITS :
General Ifoapj.tal ' ..V;"1- 1
a. At 6$ for £ million this ccmes to 30,000. These are allotted as nineteen 1,200 bed and twelve 600 bed Gsneral Hospitals ' « v ; and our standard ration of three 1,200 bed to two' 600 bed General t. Hospitals. ; sTY^iv.
i :-. •.' -.-1-. •• . ' . . ' • , • •• . b.. Tasks . , > ' Lc,••
I considered that each hôpital should, do four tasksjjl^C^:
• 1, . / • Staging of casualties on their respective *•' . , evacuation routes. - - -
i i . Holding casualties. . . V.'. . i i i . .. Medical eovar to -local troops.: -v- > • ; J .J'W^V ; .
: iv. Acting as "cushion" hospitals on: the CD -systas<.!3 p . . ' to c«itres ofmilitary population where r
. quired. . ••-/Ait^jf/^&f^
c. Location - ; - : •-=; .. - • , ' • - • - . • • ><::-<% v .
, I located my resturces as follows; •[<•••-*'•-•• .: •''••',-.•' . , - . - , . . • - -
1. KBOS - I grouped S x 1200 bed and one 600 bed v. , . General Hospitals
as qy main hôpital group Vell dispersed In this area and in a position evacuate SCYLLA,'. I did not follow the lapt-war*^
. method of grouping compactly around Scylli and v'Vy. the medical embarkation port, as I felt it • ' -better to lay back In a safer area and be pre-_ v.. : pared to evacuate to any port or beach between : Scylla and Charybdls.
i i . ELKHJM - MEGALOPOLIS - I had a forward hospitaly:. . group v of only 2 x 1,200 bed and 3 x 600 bed General Hospitals » These were on good road and rail communications well outside the -towns and . -were close up in support -of the Army Medical • Centre. In facte I visualise both'the AMA and ' ; this forward group of General Hospitals working ; • as one. .. • -.
i l l . SPABTA - MOMA - HMPHIS - j.,,
SPARTA - 2 x 1,200 General Hospitals and 1 x ! 600 General Hospital. •;•
MONA - I x 1,200 bed General Hospital MEMPHIS - 2 x 1,200 bed General Hospital
96
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
These would deal with'local, t^per^tiilh the forward'base and cover the northern evacuation route. In addition^ theysàct-;as <rtcT 8hions,l
for the main and advanced hospital-bases.
lv„ KIKETIA - CHABYBDIS - I simiÇôpïy'plkeetf Z x 1200 ' bed General Hospitals in the prea *6t each town to
, cover local troops and act' as'1*" cushion .to the . south plus coveting a southern evaluation route,
v, ABMY - I gave the Army three ¢00 bed General '"•' Hospitals, V - - tto .
vi. - RESERVE - I kept Ax 600 bed General Hospitals closed in reserve, I felt fujUyi-Jdstlfi^ik^i^; -doing this as hospitals can mpve and open very quickly,' especially with blocjc - priekttigj**' Is felt the three places they weremost Hkely to^be ' V ! needed were Sparta, where I pjji«etf^^i«ere";wé.£.'" had a lot of administrative troops and installa- -/
1 tions, andwherewe might neéd kdditionil '. Vv •;
holding capacity for evacuating by the northern , route via SUsa or adjacent beaches, 'I'placed ' ' two reserve hospitals at MIKETIA where they were well placed to move and help northwards or to go forward in support of 3 Corps; Further, if cir^ ; cumstaaces forced the use of ports in adjacent '•"-' military allied areas eouth of Charybdi s iT'ttw^^:-could give the necessary imediate medicalcover-age. The third place was EljMimJKttj Qbpolia . This was an importait piYbt 1BinWrIti was -Ttoth-a* -5
"cushion" to keep the AMA relat iv^ and'.;' for holding casualties if <iâÉâMÎ<âctâbQ tô;Xe6s were interrupted—in1 fact / ItWs^hWe est possible Interruption hospitals were on -sites «0 -GSViJtcff
' " I thihk with the given resources thla delpl^^^i'^^cwveiip ^ tional, plus observing the principles discussed, - Vheri jLJtal trööfes/" staging areas, port areas, etc,, are not.within easy reach-of hospitals, they are covered by the MKSs of the useful Field Medi'cal: Ccwipahiea, , These units will also provide staging and holding posta/för'ervacüa'tion.* -
• ; ••-- . • i- :•'." /."-.v.. • -I-.... -.'...««i .:AXn x i - 1 -CvW-A filial word on 600 bed General Hospitals-,? > AlthWgfi1 foâr âré -
made Into a specific reserve, all 600 bed General Hospiteils can be moved, «ice emptied of patients, in a very quicktime fchd they will be used if necessary to boost pointa.-1 ' * •"< - sr.c jFi ^ •
As I said, I gave the remaining 3 x 600 bed G^fsralTtoapitals ' to Army as I considered that a major assault on one or more Cdrps would require aectonmodation for -that far forward. Ï.- ->clï
•.•'.-:... • " -, ' . • . • »•«••::.>ß«tri» nj. -. DDKS Army tells me he has located his CCSs as^ollwé*:* \
-•'-."• • - •< •„;•; . • •• " ' srii-nr r. .-
. a. : 1 Corps was the least threatened^ They' Vere giventwb^ CCSs. '• • ' . •:>
' b. 2 Corps and 3 Corps, three CCSs
c. The raaalning two 'CCSs were kept Iii thief *Âxny Médical . Centre, one being earmarked for 3 Corps if required}, as they weta moït ' likely to bear the main brunt of the attack, r «£ '
.. .97 . . •. V'.' •
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
c. The AIKQT Medical Centre therefore consisted oft
Three x 600 Hospitals -Two CCSs One Convalescent Traihing Depot One FMH> , „ • The Anj Field Ambulance which was to be the DDMS
Araiy'a Mobile Reserve. -. 'J . • - '
Convalescent Training Depots
One at the «tall spa of Hippocrene near Elysium and one at the main group of hospitals it Keos.
Field Medical Companies • .: ;
. One to Arniy and three to Com Z in normal role.
Medical Eguiwwnt Depots ,
FMEDs One per Corps and one per Anqy at CMCs and AMC.
, SMEDs I have had to put one pear MWIA though I realized .. I risked losing it. Of the other two,' one was at* Keos and one with the forward group of hospitals .. near. Elysium. , . s
• ~ - '
Evacuation ,
^ Bearing in mini the principle that evacuation routes must be ' duplicated, I planned my evacuation as follows 2
a. Evacuation from 1 and 3 Corps will,be by Ambulance Trains harboured.well forward by day to run up to Arcady and Tartarus (or Mara-thon by night load and be out of the "no movement" by day area before morning.) Each of these Corps has an alternative route, 1 Corps direct to Hemp his and 3 Corps to Ifyketla if necessary. The DIMS Arny tells me he had allotted a platoon from the Army MACs for. evacuation of casual-ties front 1 and 3 Corps. , • ,. *.-• v: i..
b. 2 Corps will have to be evacuated entirely by MAC bot it?;* Is a short journey and should present no difficulty. ,1 and 3 Cdrps also' have their MACs which will augment the ambulance trains though in the case of 1 Corps, a staging post may be required. .;.: t
¢. : Of the four MACs allotted to KIQ and Ccm Z,- two will be l¢¢-given to DEMS Ccm Z and I will keep one under my hand at the forward >Vi
group of hospitals, and the other I will allot tanporarily to DIMS Army, giving him 2. • : • ;
:.1... •.'• .-.'•..••• - J .'.'ii'ifcf'- ,. .• xepiA "fii
The forward group of hospitals at Elysiun-Megalopolis will' work in conjunction with the AMC In addition to looking after local tXVops and will-act as buffer—ifthere are too many casualties, trains can run the short journey between Corps and the forward group of hos-pitals, and a second shuttle can run back to the Main Hospitals Base at Keos or alternativa "cushions". • ••>'•• /
Stretchers and Blankets
The reserve of stretchers forthetheatres was % (roughly 1000; per Bde) - 25,000, and blankets at 3 per stretcher - 75,000 . vS^ 0 blankets. .. ..- - •
Distribution of stretchers (each with 3 blankets)s
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Keos 5pOOO 3*000 Local Dmip and'2,000 distributsd between the 1,200^-. bed hospital.
Spar^f ? 4,000 2,000 at each place , ,., Memphis ) * -, • < - -• , •*'"••
Elysium 7,000 1,000 at each of two 1,200 ' bed General Hospitals ^ 2,000 at Ambulance Train Duap-v .. 3,000 at ADMS Duap
-, 11
• .- . ..-, .-,A •^J.y-PT Army 9,000 2,¢00 each- of threeCorps' • /
3,p00. DDHS: Amor reserve ,
These acs in addition to thoss held by General Hospitals for crisis expansion, i.e., 600 per 1,200 bed general "hb%pltal and ^ J
300 per 600 bed General Hospital - 15,000 in all... , ,• - •><*<• w • .. • .. . . - • • :>.-
Provision of Medical Stores -..-,- . v;.'--;- ;< .it
Blood
The BTU is deployed thus: -<•-.-•- .„•--; r ::-.
Keos - Base Mobile Blood Bank AMC - Any Mobile Blood Bank - ' Corps Med Centres- Forward Mobile Blood Bardes
Whole blood by air at 660 bottles per day - 50St above tjie last, war figure to be adjusted on experience. -
Dextran. and Crystalloids ,>
TMO bottles of each for 12JÉ estimated casualties, v' • '.' ~ r
SffR8 Pfti
ka
24 BD, 48 single gloves, 50 doses Pen. - 1,000 Casualties ;
200 packs per F Med * ) 330 packs par B Med ) Reserve .
ATOMIC ARRANGEMENTS ' •
TRAINING :
Gweral
The C-In-C put out a: directive on training and covered the following points; - . . - ,
a. SverymanmuStbe educated In the effects of atomic..... weapons so that he knows the sort of thing to expect and.-how to pro-tect himself. -
b. Everyman should be trained in elementary first.aid so that he instinctively knows «hat to do in the first few stunned minutes after, the explosion. (I think we have largely achieved this and it should be a great help when the "Mushroom" goes up.) : ' • •"<•-•'•.•'• v
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
o.' He defined good leadership aa one of the most luportant factors contributing to high morale which is now mot$ important than ever.
d. On unit training he emphasized the importance of camouflage and concealment and the1 necessity in the division for , speed in concentration and dispersion. #-
.. . ... .. . • V • 'V - -/-:.^7^.-
e. Lastly he stressed the paramount importance of digging ° for everybody. IjisB phrase was "dijj or die".
TECHNICAL ' ^ ' ! ;
a* Blood Transfusion Tephniciue ( '. .• ' 1 . T- 1 • /,,1-- ,--,.--
We have been training our best nursing orderlies (i.e., - ;. Number Is) to give transfusions, fart, of the NO III training how to set up the apparatus. ; All medical personnel have been-tralned^£, particularly in burn treatment. J
b. Team Training within Pnlta
For some time now we have been training'on the team basis in medical units. This Is done with the aim of detaching odd teams and scattering them about the countryside. This use of them v lacks cohesion, coordination and commands There is no specific . / ^ transport and no cooks, cooking equipment nor cover. The intention is that they should be used in this way; V - '.j*
; i . , The team consists of k men,j with perhaps' five* *:'1 ^ teams working under a medical officer. The Uv^i'. men ares , .. ; *,'..; .,:--
:• • ' ''''S-. • . * - • -'V One GDO to act as undresser and fetch and '
. carry man . -,
One NO to apply, dressing
• One NO to give morphine and penicillin : 1 ' .-" '' -
The best NO to supervise and give, a'trans- : fusion if ne ce s Sary1. under the eye-of the - -
. MO. - O-,.-
11. Team function;Withln the normal basic organi-zation of the unit, e.g., in the field ambulances, reception and minor treatment and major steht and evacuation might be quadrupled by /*'• adding the necessary teams.
i l l . They are able to be detached if necessary for attachment to other units. • ^ • : ' - •
iv. Or if only a few survivôrs of a medical unit, , itself the victim of an attack, can form the
nucleus of a treatment centre until other help> arrives.
c. I have been having sane trouble with ny consultant ^ J
geon. He will keep talking on technicalities of blood chemistry but I1
have told him I want this jargon interpreted into a' simple drill "for ; ''' -recognition and first aid treatment of mass burns in three categories, I stressed the need for simplicity.
100
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Ist - those burns which can be left to look after them-selves for a time. "'V
2nd « those who will die whatever we do, Vl •
3rd - those which are worth expending our efforts "on as*; they will recover if treated promptly,' " ' f Ä ' • '
i I am still awaiting his answer and I am getting a bit / Impatient.' • ' •
I also spoke to ay consultant psychiatrist who is a möst;
sensible chap and said to him that in the 1939-1945 war it'was ** generally found that if a man was subjected to 200 hours frightening ' 1 ' combat conditions — in faot frightened stiff for 200 hours — he ;..,, could be taken to have "had it" as a front' line soldier. \ •
What I wanted to know was *rtiat the position and time' fac-tor were for atomic or nuclear combat and even more important, what steps we could take to prevent or delay psychiatric breakdown and up-hold morale in this new scientific warfare. r ' • • - -,
Again I am still awaiting a reply. :;.if; 'V-. . :
UNIT ORGANIiiATIQN ' . I laid it down on Force Medical Standing Orders that just' C
as in peacetime every unit has its mobilization scheme so nowevery' unit must have its 'A* scheme with full plans as to how it"will; cope • with large numbers of casualties, who will do which job, hoir an ele-^-' ment will be thrown off if required, field ambulances andCCSswork^T on the production line basils, general hospitals on convoy reception-, drills only more so. Field Ambulances concentrate at full strength " plan to pass through 2,000 casualties in 24 hoursP FDSe with 1,5P0 j CCS holding to be up to the number of stretchers available; ;and ^ i; general hospitals to 50$ above capacity. ; 1 ' f' "
ORDNANCE STORES
In addition to the 50$ crisis expansion equipment ^eld' by^'^^ General Hospitals, there is a requiremsnts for additionsl stores \ ; . ;
particularly cooking equipment and' tentage. I asked Q for ar 5$ ill- . crease in ordnance holdings of these items, to be dispersed through! *
, Ordnance depots and up to Div Ord Field Parks. ,
TRANSPORT ,
Although our greatest contribution to an atomic incident will be In the treatment of casualties the trahsjportation of these " •• casualties and the movement of units will be a difficult problem.' First of all many routes may not be available to us because of the movement of essential reserve formations or units or of priority • stores, or because they are blocked by rubble or wecked vehicles; '' f * Secondly, transport columns may be most pressed just when we want v their help badly. Thirdly; vehicles are vulnerable to blast and f ' heat and so many may be lost. rGt have agreed that casualty " ' *' ;
evacuation will never be lower than third priority behind movement '' of essential fçraations and of ammunition,
A helicopter shuttle service should be of inestimable' * v value but production of helicopters is still so short of our needs " that they will only be fully available for casualty evacuation in the forward areas,
101
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

THR CCM Z PROBtJM . ,
With mr dispersed location of hospitals in the^Ck» 2, and . Base I feel that I have disposed of my resources of Doqdftg W s ^ ; : to the best advantage on the information I po<»ess. F r ^ f l a -1 to find medical cover for the mobile columns. I knew that SM •, v wore asking ?or more GT columns to cope with dispersal of Advancad t ; S C . AMA, etc, so I thought it a fair one to aekjor ^ ^ ^ f ' Mdical units for the atomic threat, and I obtained 3 Fi«Id ambu- ., , lances for Oom Z and Base to cover three Caa • - ^ eub-areas. These I aUotted to the Com Z areas, and sited thm near^ ^ , S^TWlce t i a and Elysium. The two base sub-areas 100 bed detachments from their «cushion« hospitals ^t Charybdis and Mona-Memphis. OsQ Field Medical Companies Deoots are detailed as coordinators for incidents under the ADsMSv r :
v . . _ ^•.••y'ri-m./:^
THE ARMY AREA PROBLEM Vv The EMS Aray has at his disposal these units: • J ^
Three X 600 General Hospitals .> / Two CCSs . . • ' • • • ' • < , The 'Army Field Ambulance : ' One'Conv Training Depot - ^ V i
One Field Medical Coy - , ^ He might, in addition, call on one of the Field Ambulaiices- ^ "
allotted to toe independent armoured brigades if necessary. . r , ;, V v
For an incident in the army area he has. one or two S ^ d ^ ambulances to work at the site of the i n c i d e n t backed by two CCSs 5 , ^d thwe general hospitals with his Convalescent Depot as ;a: b o n u ^ K , ^ .
- so he is sluing pretty. . • .> . . .< - - ^ t - W j : . • . . • . . - • . . . • • • , •• • / • . .ti.
Hie main problems will be to cover atomic attacks ou one or . ? more Corps aî S f s ï ï e tSe as, a major ground attack. |G« estimate^ S K S i s Bd^t produce 20,000 casualties including 6.0^ J t ^ c j O W
aperiod of 7 da^Ttaken'arbitrarily at i lying and \ sitting. . The problems are - clearing the area and where to put the
casualties. We feel that the first aim is to get the casualties con- ,. centrated away fror the incident and then clear thm on a priority -,, . ^ I S l T t S S S t pSt taking four to eight hours, the second as soon - . , as possible thereafter. ' - ' ••••'"• '•">••'•• -
I discussed: ./ . a. Each Division will always have one Field Ambulance
allotted in the atomic role and kept in potential^ ; • . , : (holdiS llght cases in rear of Div Adm Area). »
, 2 its owndivision, it will, be on ^ »pot to help ^ on another division, it can move in and help there. The BEHS of, corns will have to hand, therefore, an early holding capacity of, 3 S S S SbulSces which can pass 2,000 casualties through per S ^ S S c a l Centre, of three CCSs plus three FDSs^n « v i , « » and 1 Corps with two CCSs and .tw FDSs 3,500» and the AMC! ^ m I Z u t ^ o T TotS of some 17,000 excluding Field Ambulances,; for>he ,>., three Corps. . . \
b. Requirements for clearing, in an mergence a« ten lying.. .. or 20 sitting per lorry is some 450 journeys for at«ic-casualties^ alone The Lrries required will be dependent on turnover, ;e.g;^6 - ^ y S ^ ' t o S S s T c ^ s r o r say 1 hour to ADS. 3Q' have,been warned.,, . ,n?
• , ; . : ' .- •. ' tj .•Tit-' 102
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
that medical daoands would be 500 lorries and it was agreed that M H , the likely general line of evacuation might be: • • .. ..
i. The enaay will'attack following 1A' bomb; ; •.. : - • • • • ',!• . ... ,, .,y*- teri''^-*^
i i . We use infantry, armour and supporting arms-..:T. u .-to cope. >1--. -.
i i i . Infantry and anmunition will come up. in-GT. .M compani as and medical will us e r eturning «npty ; t y,- •: vehicles plus anything that canbe-aUotted/; W-V^yr specifically. The Corps MAC of • 90 Jmb>Cars. & .::-C and 30 TCVs will l ift AOO lying and 600 ».«*.'-,-. sitting. . * • -. i . - - , : . : ,
c. The DDMS Army will be able to concentrate resources "yV:. from less pressed Corps which would take the fornrof sending wholet uy; units or parts of units to work with existing units. , . y v.':;
. . - . • • • . • • :
d. DIMS Anqy will coordinate extra blankets j, stretchers,; '-.riii/ medical equipnent snd cooking equipment. y :.,,.V i^.
• . . • , • .V 4
-i'-'fl/liv Jsi^.,..:/
e. Evacuation will be by the normal means and thejplan^Vy vp. -decided when the time comes with the aim of cl earing all*. lcas eS i to ; ; > , Com Z and Base hospitals as early as possible. ,.'..1. :v
...... .. ),..-.- . ,-.-.-tV '•''•:•.'•
• This will include maximum working of aatwlancetrainsjuse-.i;.'.' y and emergency staffing of passenger trains,demands for a .speciall y air l ift of maximum size as near the Incident as possible* CCW CLUSICM
That, then, is my plan, gentlemen. The units are now de-ployed and the plan in operation. I can do little more than-sit* back and await events. ,'• - ••.-•<:- '/.-• • rxzr^'rx-vtl'.
U t l M U Ufci u u U i ^ i o t M l b ^ U U . . . J I ' It T WÏÏW www. wr ww innc t - . ""ijj ' /„ij, ^ ; * \ •
•••:•••• -.:,- !•'» :\u &.L ••" . . - . •-- 7. •.-•'. .• • - . - v ' c ? . •,. <
. SITUATION REPORT v . , -:4 «v-rUt.': ..- • (flavlet) • . .. . -t / o.• Z. . >j."1'.;' v •«
•..,•••• - • : ."..r* -^iV' yKi-?. r-r'i*
' The scene was set in the -Director of Medlcal Service 's ;*«^c (EHS's) office, at General Headquarters in Elysium. The timewas , 1400 hours on October 8 (D plus 8) 1957. Present Were ttt EKSJs - ' the Deputy Director of Medical Services (DEHS) to EMS,..DEBSisCosswtftl-' cations Zone, DlKS Amy, Assistant Directors of MedicalVSarviee»-,•-, (AIKSs) of Nos. 1 and 2 Ckpnunications Zone Area;, and AIMS Operations and Planning, GHQ. ; .;ï .-v.«. f£*. v:.-
• • • -. « V . ' ,. ; i ' * . ? , * .
Before the conference started, thsy-Ustsned'-.toVa-.brosd-«:.. ..(,-cast frcrn the United Kingdom (UK) to America of what had happened in: • England from D plus 5 to D plus 7, when for 3 days*the Fantasians -. had dropped atomic bombs on London and the major cities and ports. -••-
i' -.- .. ,-..-..•*-'-• --¾ .,- --s-".v <*•<•. • / The DMS (Major General Hopeful) • said that the situation in .v..
Ehgland and Mythland was now grave and critical. Reinforconents were minimal, re-supply of any commodity negligible. ,-InSeffect, the forces must now fight wLth the men and material they, had; in; Mythland. ,-
' Casualty evacuation to the UK was no longer possible, ; vM-.r....,. . . The DDMS GHQ (Chief Staff Officer to Major General. Hopeful) ,..
103 V-:
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

then gave si outline of events which had pc curbed to date*. Th« first, V,'" three days of warfare were conventional.' Information showed that ithe* •"•.'* enemy were building up for an attack opposite 2 and 3 Corps. Then on D plus 3 j in the evenings the'first atomic raid occurred, with two '• bombs plus high explosive (HS) and incendiaries on Mona, one an air-burst and the other an underwater burst.' Ota D plus 4 two bombs were "-t -dropped over Megalopolis. On the night of D plus 5 Susa and Chary- ; bdls were, attacked. On D plus 6 the malp; strategic air base at Krokamnia was destroyedj in the same raid the port facilities of ~ Scylla were wrecked, both from atomic -raids. The latest attack had •• been on D plus 8 with a 50 KT banb over the Advance Maintenance Area (AHA)p there was a low airburst which left 'a large area of residual -and Induced radioactivity. The Reinforcment Holding Unit and an ' •• < Anqy CCS were damaged, but outside the area of radioactivity.
In each incident, the military have been called In, the '< Hythland Civil Defence being unable to cope. • ^ . ^
The ADMSp Nol 1 Communications Zone Area then gave de-tails of the two bombs -in his Conniand. The Base Hedical Equipment ; Depot had been at Ground Zero of the airburst and was 'totally'dea-***^»v
troyed, and a Medical Reception Station (MRS).about 2,000 yard* :>V•/;';" 'I away burnt out» The Civil Defence asked for help and-the Sub-Area . Mobile Column was'sent. It took about four hours to arrive, the«' '>• medical element being a 100 bed detachment fron the -Memphia höe ' Né '3 pital. Of 15,000 troops in the vicinity, about 1-2,000 were un-accounted • for the next morning. " By the end of 2A hours , the Memphis ; hospitals were full and casualties were diverted to Spartar Inevl i^ tably military and civilian casualties were mixed up J OC-Field.. 1U.'; ' Medical Conqpany was given the task of finding the military casualties evacuated to the civilian hospitals. -¾¾¾¾^
Next, what had happened in Megalopolis was told by'the Area: " AIMSt Of the two incidents, , the military concentrated om. one'; and iyy the civilians on the other. It was estimated that, excluding-killed» ' outright, there were 14,000 casualties fron »ach bomb, of which 6,000 were in desperate need of hospital treatment. The mobile column had . been alerted at the Mona raid and so was fillip functioning within 2/ hours, A Field Dressing Station was the'medical cover. It worked ; * well and later was augnsited by 5 medical officers and 100 nursing ' orderlies, alao the reserve Motor Anibulance Company waa sent to help with the evacuation. A total of 3,500 casualties were evacuated in. ' .
' 36 hours." ' • -- .v ; ' • ' r -.; • K'" * •"".-.".: V . . --- ,>',.;.- .-:'•• .• •-V..-. '
The AEHS continued with the incident on the 3usa Petrol, - Oil"'"' -and Lubricants . (POL) installations, which was mainly a military/^ .f^*', affair. This being the case the Comminications Zone Aré& ïfobil'e^ColaBh'»" was called up', and worked much-as the Megalopolis column did ji'itöalso>£ÄI had an FES attached,, The total casualties here were 800, mainly: : r> T . ' flame burns <, Difficulty in evacuating cases was experienced owing to . shortage' of ambulance' transport; the second GHQ reserve Motor Amba- ; r-" lance Company was- at Elysium and could not be got up invtlm«;' ' s^ï ' :-4
The incidents on Charybdls and Stella were told by'the AHC -2 Caaminications Zone Areat Both of these were ports, and the pic- . ture was much' the same as at Mona.- : , . ' ' j . •
The Medical Specialist at the RAF Station Hospital n e a r * Krokamnia told what had happened
there;: and finally ths AHHSiAiMjrf' h' spoke. The bomb over the AMA had been a low air bur stands amongst* : other things, seme ammunition had been made radio-active.' Unfortu- x nately part of it had been Issued,1a search waa being 1Biade for it, and the people who had handled it,
104
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Hajor General Hopeflil then said that the main medical difficulty was in finding beds for the casualties, and that the greatest problans were in the Com Z and Base rather than in the Combat Zone. It was Important to screen casualties carefully before evacuation, to keep as many as possible with their own units, and to reduce the time of hospitalization to a minimum by early return of patients to convalescent depots or to their own units. (See Chart on Page 106*)
The salient points brought out in the playlet were:
a. The British Expeditionary Force had provided hospital beds in Mythland. Major General Hopeful had raised this number to 9% by a 50$ crisis expansion, i.e., creating extra beds perhaps by using stretchers, without ooplpying additional manpower. He also directed that hospitalization time be reduced to a minimum by the early return of patients to convalescent units or to duty*
b. That the disorganization of coumunications,.ports and airfields in the UK and in the Advanced Base were bound to Interrupt evacauation of casualties. Therefore the DMS plan should allow for a much smaller percentage than 80 to be evacuated to the UK.
c. That, whatever the state of preparedness of the Civil Defence Organization in Mythlahd5 military help wuld be required. In any case, in many incidents Civil and Military casualties were Inextricably mixed and early separation was not practicable.
d. That there was a definite requirement for mobile medical units in the Ccninunications Zone and Base to carry out collection, sorting and first aid treatment of casualties from an . atomic incident and to organize their evacuation to the General Hospitals.
*J U ht U t l M ^ " " " ** 1WHT Rfl R WlH H HHfl
GENHtAL HARRIS
In the discussion which followed, General Harris explained that the 600 bed General Hospitals did not have the organie trans-port required to move them. This would be obtained from the Quarter-master General's department as required, and when available. The medical services normally have a high priority in the allocation of transport under such circumstances.
In reply to a question from General Labarthe, Colonel Crosse said that the hospital area at Keos was chosen because our Intelligence report showed it to be an unlikely target for an atom bomb. The hos-pitals were well dispersed, and would have a very good chance of es-caping damage.
General Harris, in a discussion in which Admiral Galiacy and Admiral Ingleby-Mackenzie took part, pointed out that the ships carrying casualties from Hythland to the UK would not be employed as floating hospitals, but a means of transport only. In the situation envisaged for Averaus it would be extremely difficult to transport patients by sea', to the UK, because of lack of air superiority and of damage to harbours*
*** ««» 105
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Ë] §1 ¢5
Mj
g
§ r I * ï! ,1 ^ i s * * « î rf S 8
sI *
I j IriI W
s1 S
a1-3a 5s J1S i l t*-& J^jh
Illlsl m J é »
I i m I t i l l M SlIiJIiS $1! l!i IiiE
I M
J1-
iItiI Jsisi Illlia
i f? lla
I j
MS 4 P ii
S É 1 3 3 J s riS H
ITl £ il «
S t u l l
I
!»
m m l
î a* 31e H
h Ä J ï -rs s
t % J k
«îwfia:
4 n i
S m m J f
SIsi l 8 • »
i l l
En l u
4 s |rf£.
a mh k p ! R
8 • »
i l l
En l u
4 s |rf£. î%
tek s » »
i l l
En l u
4 s |rf£. I
! S » a
S S . 4
g S g"
S 8 »
§ ei N* !
ï
g I § "î rl % I H*
I *
rf I •
I W S a" 1 * B
î lg A + p Is td
1 « • « * § il i Sh CO 0(1-1
I 1 -J-. fi " P b a A S Ä
S S -JU f » SI II 3A sa Sn
Ii
§ *
1 * 1 i
iN S SA
I *
rf I •
I W S a" 1 * B
î lg A + p èe 33 1 1 &
S S -JU f » SI II 3A sa Sn
Ii
§ *
S I is § i
2
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
PLAN OF DIHS 3 OOHPS (CORPS SURGEON) AT D FHJS 9- I.e.. 9 OCTOBER 1957
. ••' •.•• -,-- ; •> 1--. r;r i >•
The DIMS 3 Corpsi, Brigadier Menecest following a conference. -with the DtHS Ö Anny, and in the light of various intelligence-reports, will present his .plan to you. It is. 0900 hours, on 9 October 1957 (i.e., D plus 9). fiftckpround - ,, ,, • '," -•
' . -V- v ,
Dqring October 1957 the rapid sequence of aerial atomic attacks on the Base posts, airfields and other installations,- followed by the-attack on Megalopolis and the AMA on D plns4»..suggested that - . after attempting to interdic-t cconunications inrsar of the Army-.area , . the Fantasians might be about to launch a violent assault by land.;
. .i- ". • . •• ' •• - ..*:.• .- tri -•
The Army commander was of the opinion that of the various j. • Corps in 1 (GB) Army, 3 Corps was the most vulnerable owing to poor • road communications and the,difficult terrain» ? - - ^
Following the reconnaissance the, Commandw Ofj' J jCorps-decided that a hilly feature nWialebonen approximately. 17. m i l e s M i s s , in the centre of the Corps area was to be defended at all costs,as .t'ccnmanded a wide area of surrounding country and was essentially .en«, oi,the keys.to the Whole defensive system. If the feature remained in Allied1 hands,it would serve as a base fran which to block the.FSntaslm^arnoaredjthrust;, to the west towards the coast. "1Ti" v . '
The Corps Cc»imander decided that the feature was-6 ;su< '|im-, portance as to Justify the location there of two; divisionsiihe,/- ^,/ accordingly ordersISO Div to occupy the eastern end or the rld^'and,^,, r> 2 Div the western end. 8 Armd Div was to be the. Ctorpsmobile^reserve -and would harbour in the hollow between the western end of.' the feature {; and a small hill due west. The Corps Conmanderc warned that*thsre£i;<>t -, rnigit be a possibility of heavy Fantasien attacks cutting the ccewoni-cations to the west of Marathon, in which case.the Corps would have to fight a defensive battle in an isolated position. . --
The Corps Commander hoped that by holding this natural ; obstacle in strength, by widely deployedinfantrysupportedby strong detachments of anti-tank guns/ aid covered by deep-mlnefields,> the Fantaslan attacking forces would have to pause and concentrate before launching an assault, preceded by breaching operations „.rHe. intended . to use 8 Axmd Dlv by concentrating it rapidly against any.,eneay who succeeded in penetrating the cruet. .,,-/=- v
Following the Corps, Commander's outline plan the,DAMtCHG called a conference of heads of all services and explained,that-the: Administrative Organization of 3 Corps was governed bytwofactorst
a. The unfavourable air situation causing not only: wide dispersion of units, but limiting adminstrative traffic tOMnovingby day in pairs at three minute intervals driving at . 20 mph,-iOr;in( greater numbers by night or during unfavourable feather.- .-.
b. The discontinuous front with gaps covered only by mine-fields.
He stressed the Importance of reducing forward transport to the minimum, also the danger of possible Interruption to coramunl- . cations of forward units would necessitate the latter holding stocks . and also being prepared to retain casualties until communications were
107 ' . ; ' " " v ; .
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
restored. He stated that air supply would be minimal and air evacu-ation of casualties correspondingly small* He promised to supply each Division with an extra wireless link to Hain Corps HQ expressly for the'AIMS and CRASC of eachDivision to ccnnrunicate wi h the DDKS and r
DDST. He stated that the maintenance and medical and recovery plans1 " for S (Armd) Divmight prove difficult. V '
Immediately after the conference the DDHS visited the DAfcQiG. to discuss the medical plan.
The DDKS pointed out that'in this type' ot terrain 'Aindi'battle^ and with the possibility of large numbers- of casualties sïRHenly occurring efficient medical care was vital for the maintenance Of morale. Ä '
In consultation with 'Gt Bretnch he estimated his daily casual* * ties as: • • • • • • • . vi.
• - - ' '.••; V J1-. iC : .p-.îj Daily sickand IhJured- . . . . . . . . . . . . . . . . . '45 v< '
Daily battle casualties as a result of con - 1 — ^ -ventional weapons (average) . . . . 150*
(During Severe fitting) ... 900 * ' ' /
Atomic Bcmb Casualties ;
5»000-6,000 total casualties of which 3,000-4,000 (sLL^itly more than half the total casualties) would require treatment; Approxi-mately one third of these would be so seriously injured as to require' evacuation as early as possible to undergo operation within 6- hours; A further third could wait somewhat longer before evacuation (asswdng 1
that trahsftasion has been Initiated); the remainder would'be'on'low' ' ' priority for evacuation. , ..>.. ^ ,
The DEMS gave details of his Medical Order of Battle as - '' ^ comprising: r"
3 Casualty Clearing Stations 1 Field Dressing Station t : " 3 Field Surgical Teams (1 attached to each CCS) 1 -/J ; 2 Field Transfusiwi Teams • 1 Field Hygiene Section ' ' ; ; 1J' 2 Mobile Dental Teams J. ISpecialTreatmentTeaa " 1 Ophthalmic Team • • -. ., . 1 Earj Hose and Throat Team 1 F. Med - • 1 Motor Ambulance Coanpany BASC (less 1 platoon)
He stated that there was a possibility of 3 Corps cnwmini-cations with its Main HQ, CMA ànd CMC at Tartarus being Interrupted,'' and he was proposing to supplement the Divisional medical resources covering the main defensive position with the following units:- '"v - ....
To 50 Divs 1 Field Dressing Station 1 Field Surgical Team
To 2 Divs (which was also the advanced base from which 8 Armd Div would operate):
1 Field Dressing Station 2 Field Surgical Teams
108
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
I Field TranafUd.cn Team ,-... V IMobileDentalTeam - -'•••• • v. '- .-'-• 1 Platoon of the Motor AmbMlanoe Coy RA3C . ;,
His decision to send forward one Field BTtosing-Station -1*— v each to 2 and 50 Divs would enable each of the Divisions tohave 1 Field Ambulance pre-loaded as a Divisional Atomic ReSarre. .
:, ' ! .-. . -- C -KA- - '
Later that afternoon the AIMS of 8 (Armd) Div and -2 and" .* ;
50 Divs met the DIMS to discuss their problems. ; . --. .-. > • -
AIMS 50 Div explained his layput with 149-and<150'Brigades?- deployed and 151 Bde as Divisional Reserve. r. : < / ¾.. »
. - .- « * i
In view of the fact that access to one single- ADS'froé more' than one brigade sector might be Impossible, he had allocated one con*:.' ' plete Field Ambulance to each of 149 and 150 Brigades; he wasJ.pro--' s . posing to utilize the FDS and FST which the DOfS has allotted to him, inside what might be tensed a Divisional Medical Area; this gave him ' his third Field Ambulance unconmitted as a Divisional*Reservej-which - J -he proposed to have pre-loaded on wbeelb ready to move.'He had- sent all unnecessary vehicles and personnel back to the tBl Schelon-inside the Corps area;'he has laid down a stock of plasma, burn dressings,' stretchers and blankets. He asked the DDMS how he could obtain whole blood if he required it. The DIMS advised him toobtainanybloodhe required from the FTT attached to 2 Division. . -V ' • v<-
. • • - . - ., . - -s . • r,.--: •"<
AIMS 2 Div stated that his Divisional Ccemandariproposed-to: deploy 3 and k Bdesp retaining 5 Bdep as Divisional Reserve. . He was providing inside his Divisional Administrative Area (onthe«xtr«e west of the feature);« a base fron which 8 Arad Div could operate, ,-,-t -..' either to the north ôr south of the feature. •• - , .v*; -y..-»-
The ADMS 2 Div stated that he had awanged rwithVthe vMMS'ßze --'' 8 Armd Div to take in any sick or casualties trm the two Field . -Ambulances of that Division. In view of his many ccwnitmentshe was proposing to locate one Complete Field Amibulance with each of J and-4 , Bdesj, and to establish an improvised Divisional Hedical Area ln the hollow ground near the Divisional Administrative Area. At, this looation he would haye the FDS which the DIHS Corps had allotted to him, also, two Field Surgical Teams, one Field Transfusion Team.(which;would have;to v1
hold blood for all.three Divisions), the Mobile DeabaX-Teaaiand'the'— platoon of the Motor Ambulance Coy RASC. This would give, him his third Field Ambulance uncommitted, which could act as Divisional Atcoic Re-serve. . -VvX - .
He has also laid In stocks of burn dressings,'--plasma,* *> • >.= stretchers and blankets, and returned all unnecessary vehicles and personnel to the Divisional 'B1 echelon near the CMC. :
ACHS 8 Armd Dlv stated that his Division might have to oper-ate either to the north or to the south of the feature, because Regi-ments were liable to operate on widely separated jcenti;e lines. He was proposing to leave one complete Field Ambulance with each Brigade; A. - '. Whenever possible casualties from either Brigade would be 'evacuated : • to the 2 Divisional Medical Area.- He would be in wireless communi-cation with the AEHS 2 Div at'all times. I '
NARRATIVE -
During the night of D plus 8 to D plus 9,* there was Iriglriii moonlight and the Fantaslan Air Force taking advantage of this bombed - : the western end of the feature with HE and incendiaries, causing -moderate casualties amongst the personnel of 2 Div , but unfortunately -
109 ; :. ' ..' -'/;- .'v.!". t,
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
NATO CO fIDHJTIAL
destroying a large amount of the reserve petrol of S Amid Dir.
On D plus 9 at 1750 hours an FOO with 149 Bde of 50 Div observed Fstntasian aircraft approaching from the direction of the Biver Lethe and Hying due west ovep-the main feature. ; , . ?
• . .-•• W ' . v.. t..-" At approximately lßOO hours two atomic bombs were exploded
by high air burst over the 3 Corps defensive positions; The ground zero of the first bomb was in the area of 150 Bde of 50 Div, causing i approximately 3,000 casualties, (12p0 dead and 600 wounded), unfortu-nately the casualties included a lajr^e number of personnel of the-Field Ambulance with 150 Bde (the Divisional Atomic Reserve). - The ^' second bomb exploded in the gap to the western end of the feature, -causing 3,000 casualties amongst personnel of both 8 Armd'and 2 Divisions, and tragically destroying the FTT stocks of blood, and wounding the O.C. ;
This aerial bombardment was followed by a furious long- r. > range rocket, guided-miss&e and artillery barrage on the area of ;;> I49 Bde of JO Div. Ae dusk was falling the Fantaslan amour could be seen carrying out a breaching operation through tty minefields : and endeavouring to thrust along the north side of the feature.'
When dawn broke on D plus 10, a Brigade of 8 Arind Div moved eastward to lnteroept and a Airious dog fight ensued In which both : sides lost numerous AFVs. D plus 11 was relatively quiet, but on D plus 12 wave after wave of Fantasian armour attacked both north and : south of the feature. Also, Fantasian infantry in APC over-ran the" area of 149 Brigade. - • \ -- '
By the dawn of D plus 13 the position was critical,and - * . the Fantasian armour was massing for. several thrusts in an attempt to . break through between 2 and 3 Corps.
At 081$ hours the Fantasian Air Force dropped an atoeti.c bcnb in the vicinity of Karathon, but caused only a minimum of damage ands very few casualties.
" ' "-V -viTk-1 By now the position inside the 3 Corps defensive position/was
critical; a proportion of casualties had been evacuated to .Tartarus up-to the evening of D plus U , but the 'casualties on D plus 12 and D plus 13'were as follows; . , - W--Jf:.;
Daz ££S t? f S^X 2_Diy ?0 Div Total
D plus 12 - Atomic 200 320 400 920 Conventional 150 170 190 510 . i
D plus 13 Atomic 150 316 390 656 Conventional 200 400 200 800
Thus in the 3 Corps defensive position a total of 1310 con-ventional wounded,'-and 656 atomic casualties were recieving attention* Of this total of 30S6 casualties, approximately 700 were serious*
Inside the Divisions, 50 Dlv had lost one Complete Field Ambulance; 2 Div had lost Its FTT and its stock of blood. 6 (Araid) '•>•: ; Dlv had had heavy casualties to personnel of both Its field ambulances. The DEWS was able to fly forward on D plus 13 by helicopter to the 2 Div Medical Area. -,
He found that in the 2 Div Medical Area the FDS and the serve Fledd Ambulance were endeavouring to treat approximately 900
110
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

casualties of whom 300 were serious. . j ,- Va- '
Jxi the 50 Div area, the FDS and ADS fron 151 Bde. were endeavouring to trexat 780 casualties of whom 260 were serious..,.,! .;.
All the stocks of whole blood had been destroyed*
Oti D plus 13 the Allied Air Force dropped four atomic bombs on the Fnitasian armour massed for further : attack«. 1 -Inmediately following this a vigorous counter-attack by 11 A ^ Div wtffcH~ttad ; moved up by night, stopped Wie Fantasian attack} drove:th«m bao1r and restored the situation. The successful counter-attack.byj11.AradnDiv enabled connminications to be re-established between the- CMA, the Corps , Medical Units to the west of the CMA, and the format ionsaround the^,t ; feature "Whalebone." -- : , -Jt- N -. h'.t.*
The EDMS, using all available motor ambulances and2TCVs, was able to evacuate 1,A00 casualties to the Çorps Medical Units, . v , leaving behind about 700 cases too i l l to be moved. l He arrangéd v ' helicopter sorties to fly forward blood and cryatalloidsandtrans-fusion apparatus. He also sent forward by road to 2 Diva^spare refrigerator van to replace that destroyed by the air attack.'
r: : • *' - .- -r-"*
M Irw J U L l t J U U f c J&JfcJl J h l t l t If fcflf It W tf M l7n JftJMt H T T H H n H H M TCHTT WTf I* Tl Ä H . T I n f 1 J T T n T . . t . . . , » ^ . . . , . . - -. . V • - - . , ••
FLAN OF DCMS (CORPS SUBflECTt) 2 CORPS /- ^ "tw AT 0900 HOUBS CM D PLUS 9. I.e.. 9 OCTOBER 1957 -
. ..•••;. ..• .. , ' s -vtii- t.-, •
The DEMS 2, Corps, Brigadier Cross e,following&; conference, ,,. with the DEHS 6 Amy, will present to you his plan to deal.-withthe.- , j major battle which is now. considered to be imminent on<his';0orps~,v. '«V.'i front. It is 0900 hours on 9 October 1957 (i. e., D plus, 9). ? ;-, V -. ,.. -.
Appreciation by the DDHS 2 Corps at CRQ (Elysium),-at 0900 hours on 9 October (D plus.9) 1957* :
• • • ' , ; • -• , \ W - X ' - ' - l1
AIM; The maintenance of morale and of manpower by the pre-servation of htalth, and by the speedy and efficient collection, evaluation, treatment' and éarly return to duty.of casualties.-.:
. , . .:, '•. v, ; v: L- - .-..«'• 11.} î - i a / FACTORS • •
The Naturei lQfl the Operation • ' ,¾^..1¾ ^^
, 2 Corps is prepared to fight a defensive battle in wèll-prepared positions, lasting over 7-10 days during which'the Fantasian forces may be expected to use not only conventional.but also atonie weapons. . As the 2 Corps front covers vital communications to.both : -Olympus and Megalopolis, the fighting may be very heavy, with corres-pondingly high casualty rates.
. » .• .j. . I estimate our casualties as followsj
Assuming the present- total strength of 2 Corps at 40,000,
• . -VJ ' 1 I ' ; . we »ay expects
Dailyi sick and InfIured t $0 daily.,' ,(•
Battle Caaualties from Con- : . ventlonal Weapons » Up to 1,200 daily ;
Casualties fron Atonic ï Up to 1,000 par ncminal bomb, Weapons s >t of which from 4OO-5OO would
WSL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Tbus the total casualties which might pass thAû'éh thë;' ; î i  ΠΠ2^ Medical Units of 2 Corps on any given day may vary from .1,200 up ' ^ to 2,700. This latter figure would occur if the-Fantasianswere to superimpose three atomic weapons (or their equivalent) on to L' 1^-' heavy attacks by conventional weapons.
* * * * * * * * * * - Mature of the Terrain
2 Corps covers a front of approximately 25 ailes^with depth of approximately 50 miles. Each of the three Infantrjr Divi-sions (48, 3 and 53 Dlvs ) covers a front of approximately - 7 miles 48 and 53 Divs occupy hilly ground; with 3 Dlv occupying the"low^ ^r-. ''f5
lying ground in between. • ' A K
The CMA is approximately 25 miles In rear'of Main HQ of fp — 3 Div, and about 7 mile's more from Main HQ of 48 and 53 Divs. ^ J-s
..-OJtjfti-VJ^j-
Ifoln HQ 2 Corps is to the east of Pelusium sbbut 10 miles" north of the CMA0 ^ ^
The country is hilly, mainly agricultural, with a good water supply? only farm-houses accommodation is available.
Coramunications inside the areas of 48 and 3 Dlvs are poor . . . and consists mainly of secondary, roads used by the farmers. t is more fortunate, as the arterial road.from Megalopolis - arid Ol^pu S^.-iA passes through the area of the CMA and through Pelusium down towards-/, the wftst ;bank of the River Lethe. This road is in excellent'cdn- // dition at present* There are no railways or water-ways near the 2'' Corps area. Ths only potentialairfields1 are' lielicopter'/and llgtft^ aircraft strips available near HQ 3 Div, HQ 2. Corps and the àrea^of > "itvs^ the CMA. . • -.
Transportation of casualties by vehicles is llkely to^be t^t very difficult insids the areas of 48 and 53 Divse but easiertfor 3 • • DiV.
L- • • • ' . . ' V.
' '•1 ' • - ' • . ..-
1. 'if
1 .-".yi^v-w
Evacuation of casualties to the rear of 48 and 3" WvS "will w ^ w
depend upon the single, fragile road through the hills to HQ 2 Corps;/, ^ Evacuation to the rear of 53 Dlv should be easier, making
use of the arterial road. . -. , 1 ' " '
Climate and Ettdenic Diseases ^ ^
It is not anticipated that this autumn willbenuidùlyëôldî" J
Intelligence reports State that no abnormal Sndaiiic foci of disease^ exist. ; ' ' ' " 'Y
• • •• • - - -. 1- . -i v Y r-.
•Courses Open *
The AlMSs of 48, 3 and 53 Divisions have told me that they are satisfied with their existing Medical Order"of Battled They in-tend establishing one CCP per Brigade-and one ADS per Division; near ' the main Divisional HQ or near the main administrative axis controlled < by the AWE, In each of the three Divisions, one-Field Ambulance-is being earmarked aa "atomic reserve.1* 1- '
• ',-••'.•."'• : : ' • '.- 1. vi."'}
The evaicuation of casualties from 53 Div to* the Corps Medi-cal Units presents no major problem, but the evacuation of casualties
- • > MH •
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
from the rear of 48 and 3 Diva over the hilly roads may be difficult especially if the Fantasians anploy atomic weapons on either of these two divisions.
The existing Medical Order of Battle of Copps Medical Units is in my opinion adequate.
The Corps Medical Units include the following;
FiaLd Dressing Stations . . , . . . .3 Field Hygiene Section ....1 Casualty Clearing Stations .3 . Field Surgical Teams .6 Field Transfusion Teams ..3 Ear, NoseandThroat Ophthalmic Team '•!.••'• Special Treatment Team ..1 Mobile Dental Team 3 Forward Medical Equipment Depot ,1
Iri addition, one Motor Ambulance Company RASC has been allotted to 2 Corps. ,
The deployment of these Corps Medical Units requires special consideration. W *
Administrative units Amotion better when concentrated. Thua If Corps Medical Units are focused into a Corps Medical Centre, the> ; ; drivers of motor ambulances can find their destination easier; the,re- . caption, classification and subsequent distribution of patients can be controlled at a central reception point (e.g., a Field Dressing Statlon acting as a f i lter ) , also the personnel of-the CCS and SurgicalVor other;< Teams can work on the shift system. <
t • ' • • 1 • . .
(At this stage, models of various units included in a Corps ' Medical Centre as in World War II are put down on- the<floor). :
Since 1945 studies of the various effects of atomic ex-plosions—especially the thermal effects—make it Imperative that attention should be paid to a reasonable degree of disperelon of Corps • Medical Units. „ i
- • M " • • " . ' ' '
On a fairly clear day exposure to thermal radiation from a nominal atonic bomb would cause serious burns at a distance of about _-10,000 feet, from Ground Zero. .Tent fabric nay bum at distances from 5,OOQ-6,000 feet, whilst Nylon will melt at 10,000 feet. ,
, * - ? ' These facts suggest that it would be extremely hazardous to
concentrate Corps Medical Units. One bomb with groind ,zero centrally located in a Corps Medical Oentre might cause great loss of l i fe through being set on fire, and imobile patients being caught in secondary fire.t
On the other hand, wide dispersion .of Corps'Medical Units 'will not only make it more difficult for mojtor ambulance car drivers,.to locate; each unit, but also make the reception and distribution of patients from a central point more complicated^ and Impose delay upon surgical aid being given to serious casualties. .
One solution would appear to be a reasonable dispersion of Corps Medical Units, using the headquarters of a Field Dressing Station; as a Control Point for reception and distribution of casualties, and . allotting one section of a Field Dressing Station to each of two Casualty ' Clearing Stations open to receive patients. The detailed layout will bè discussed in the plan.
m NATO CONFIDENTIAL
'Ï : ' / '
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
NATO CONFIDENTIAL , t
Evacuation of casualties frcm the Coips Medical Units to \ 'r the A H Q T Medical . Area west of Olympus will only he a short Journey • ; ; r> and Kill be carried out entirely by MAC and should present no majorvl;. tv r difficulty. Although potential helicopter and light aircraft strips exist near all three Main Divisional HQs and Corps HQ and the CMfc,, no organized air transportation of casualties is available as yet-* : ,
Medical and Ordnance equipment supply Is detailed^in the Plap.
As regards assistance to civilian casualties occurring in the Corps area, apart frcm Pelueium, only scattered farming canBRini-ties are. present In the area.
The Civil Affairs Liaison Officer with HQ 2 Corps has a ' •• small civilian hospital of 50 beds in Peluslum and is confident;1.that •'. his staff will be able to cope with any civilian casualties -In.the . Corps Area. .. •
Flan '
a. Maintenance of Health and Morale . > • • ^ r.-v
- AU ranks of all units in 2 - Oorps have been briefed ' ' concerning their tasks, and the fitting potentialities of the ene«y„ -. and his techniques and weapons, and of our measures to combat same* As a result, morale is high. All- units have been traineddnmeasures ' ' to preserve health; apart f om rickettsial infections, no1 undue^èdesd^ 'Lt diseases .are Ukely. The C onm anders of all format ions-, have . b e e n v i nr;-pressed with the necessity for the strictest discipline ,with:-watsr,stf^.H^ food and conservancy.The Medical Services may be extend edtovthe >full-i.-.' with battle,casualties and so the occurrence of preventable/.diseases^rj;^^ will be regarded by the Corps Ccnmander as indicative of poordiscip-*;- Vf. line in the unit or formation responsible. - , ,, ,
b. The. Deployment, of theOorps Medical Units: . . ...'-• . v. ••
The distance from Main HQ of each Divislon;to theCCorpsv
Maintenance Area is approximately 25 miles. The distance-from' thetCMfc .:¾¾ to the Amy Medical Centre is approximately 50 miles., MÜ1. i j,-.
Dispersion of Corps Medical Units will not be radial but' linear. The location of those units dispersed along one'axis,nis justified by the fact that this axis (the main Peiusium-Olympus.road) ^ is themain supply route to all the Units in 2 Corps and apart .from' • [^-:.0/ airborne attacks is the least likely of all the three Corps main ' v
supply routes to be cut. •' -
(At this stage, models.of the Corps Medical Units andrtheirv,-..-,-proposed deployment are laid down on the ground in turn.) ?•.••
• •. . . . • -..,..- .- -.-f. . i - ' .--.r Firstly, at a point near the main Peius ium-Olympu s jroad,
approximately three miles southwest of. the. {MA, a control point will . , " be established by the HQ of one-FDSj one mile beyond this point'near^ the MRS one CCS will be located accompanied bygone.section/of a FDS and.i-.S; with two surgical teams, one Field Transfusion Team and one Mobile . Dental Team attached. •,.••< /
Five miles further along the MSS a second CCS is established together with the second section of the FDS and two FST> one FTT and one Mobile-Dental TeamJ finally, approximately a fürther, three miles} -r -distant^ a complete Field Dressing Station -Is located to receive minors . surgical or medical cases; it has the Corps Psychiatrist and the ... Special Treatment Team attached*
114
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Th«-third.-CCSj th« third FDS, two JSTp One FTT and 1 Mobile Dentol Team, all- in reserve are dispersed within 2,000 yards of this: "' FDS ready to open up at short notice»
The EMT and the Ophthalmic Team are attached to the rearmost of the two open CCS,
Wie PMED is located on the MSR to on» side of the .open'FIS. "• This FMED serving 2 Corps, has been stocked with reserve turn dress-ings, gloves, antibiotics, and Blood Transfusitm Equipmentsufficient for a total up to 6,000 casualties,
The stock of Whole blood (approximately 200 pint bottles of blood per day) has been distributed among the three FTT to ensure the minimum incidental loss, DDOS 2 Corps has arranged for à reserve of 2,000 stretchers and 6,000 blankets to be distributed between the'threé' Divisions,
The field hygiene section has been located near Maihcorps' HQ',
DETAILS.OF COLLECTION. EVACUATION. ' DISTRIBUTION AND TBBATMENT OF CAS-
UALTIES a. Within Divisional areas existing transport is considered- '
adequate for the collection of casualties up to peak figures*
b. All casualties from Divisional ADS will be evacuatid't r 1
motor ambulance companies,to &>rps Medical Units. The total of 90 " - ''J motor ambulance cars, plus 30 troop carrying vehicles is'irafJflclent; to transport casualties up to peak figures (maximum on any'one day, ' 2,700) back to any of the.CCSs or the FDS allocatedifor inihor sick. '
c. All MAC ambulance cars upon arrival at'the '^ntrol ' ' ; ' point established.by the FDS HQj 3 miles southwest of the CMA, are-' --checked as to the nature of the casualties they are-transporting. (Spare ambulance cars and troop carrying-vehicles should; be located near this.control post.) Any minor cases can be transferred to these spare aabulance cars or vehicles and sent direct to the FDS for ' minor battes. This FDS is situated 10 miles-to the southwest'of the «A, . ' ;
The more serious casualties would be carried on in the ' 1
original motor ambulance cars to one of the two open CCS situated respectively -4 and 7 miles to the southwes't of the CMA.
Admissions to the different CCSs in the locatiittis mentioned can be alternated.either on a .time basis switching every 12 hours, or on the basis of the number of casualties admitted, depending on'the ' " flow of casualties, ••'•• : - -...,.: >.*,-(.!: .-•
' . . . . . - , . - : - - = - 1 - - .
The existing Medical /Wer of Battle Of 2 Corps of three -CCSs and three FDSs is. In iqy opinion,- adequate to: hold up to peak ' figures (900 in any gLven dayj, provided that the flow of casualties- 1
back to the group of hospitals at the Army -area near Elysium-Megalo-polis, is notumttly Interrupted. " c ; : - :
The distance from , the CCSs to the Ariqy Medical Centre is approximately only 45 miles and all evacuation over this route will have to be made by Mbtor Ambulance Company cars.
. Siimuft-ry ... .: - V
For the eocpected type of operations over the given terrain .
3U5 . .
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

and with existing road ccomuiiications, the existing 2 Corpff Medical Order .of Battle is adequate. .Transportation of casualties will be entirely by road. . ••
Corps-Medical'Units will be dispersed in line on either side of the MBS from the GMA to the AMA.
Medical Equipnent sufficient for both- conventional and atomic casualties has been located In the FMED. ^ <.:'„••••
«,.. No major Civil Affairs medical problems are envisaged • -- .. .. inside the Corps Area. • ;;
JMUt WMM IfVlI W MIf Juut . • • HHH HHH H.H. . H H H . n n n . . . . - . . „ . . . : -. ;. , - -, : ..- , ^ ' ^T j uJ
A discussion, between DBMS 2 Corps and Colonel Douglas ••'. r ^ made the following points: - • • • - : . ; . - • ; -. - CO..?
.,. .„s.U-.iv.:
a. The Corps Medical Centre was dispersed over an area 12 miles long. .•••.<'.-•': v: '
b. There was a distance of at least: 2,000 yards between medical units. ..-.-.-•... .
c. The imita providing surgical teams were not more than 5 miles apart*
d. The present British Casualty Clearing Station is too small for its task in atomic warfare. It should be possible to re-tain such cases as. light burn cases and treat , them in medical unite In the Combat. Zone. V^W
I ... .. . ' , ' , ^ - ...- . ' .....- • r.-iii-i'.1 < • •<..' À
e. The positioning of the advanced surgical centre de-- 1¾ pends upon availability of helicopters (if they are available the Centre can be placed, far back) and on the need to avoid an area likely to be fought over when engaging an enemy force which has "f- ; penetrated our-own-lines.- -.-• *<-•'.---- 1-.¾. 1.¾^
4UUfc If MU If iftl JUUt WWH JUUt-n h fi nnn • nun . nan innr h h a ) .
V - , DISCUSSION FOLLOWING SERIAL TiO ' '•• v - ^
Replying to a question by Air Marshal Kilpatrickj General Harris agreed that the present British CCS has become too small to deal with the casualties of a nuclear war. The grouping together of ; - '; Casualty Clearing Stations was wasteful of medical effort. • Brigadler-' - v
Hunter quoted his experience with the First Cahtulian Corps in Italy in 1944* Field Dressing Stations were all removed from'Divisional, control and placed under Corps command. They could be used in-various > , roles, for treating minor sick cases, for staging, for forming an ad- - 1
vanced surgical centre (with surgical and transfusion teams attach«!),' In a future war, and in face of nuclear weapons, he thou it the trend should.be, not to enlarge such unit* as Casualty Clearing Station's, but" _ to create larger numbers of more versatile units, in spite of the'essen-' tially uneconomical lmplicatioiii of such a plan. . . v i' •
In the Canadian Army, the Field Dressing Statlon'had never been so tied to the Casualty Clearing Station as seemed the British practice. - v . ' -: • " --... .
General Harris agreed that it would be un wie e to Increase the CCS in size unless the proviso (which her had made In his opening address) was accepted, I.e., that such an augnented unit was truly divisible into independent sections and was then dispersible.
- 116
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
. Brigadier Richirdson spoke of the practical, difficulties ; in providing shelter for casualties in the medical unit's. the, f,-:. • six days that precedsd the start of the enemy attack ^stdescribed, it might have been possible to reinforce the cellars ofamiy'avail- : ,"/' able houses, and then demolish the house on top of, the, cellar to/ • give overhead cover. Whether this would provide for large/ numbers- ^ l„ , of casualties was doubtful. In six or seven hours at field! aalmïaricé^/,^-(230 personnel) might dig out shelter for.40 to' 50 casualties,^iiod^ thai take some further hours to dig slit trenches for them8"eïvesî,/,+ ' " . ' Mechanised diggers may help, if they are not wantéd for Ai^er prioiy!, f •. Ity Jobs. . ; . • ^ ..., ^ / ¾ / ^ : ¾ ¾ ¾ ^
He quoted Napoleon as saying "If success in' battle could be ,j achieved without taking risks, then military glory would be at the . ' disposal of any mediocre personality,*—but you can take, risks Jif you are a Napoleon, not if you are a doctor. ^ -
Helicopters may provide the only hope, of survival for cas- * * "Z' ualties in a future war. Public, opinion shoulcSsee that a goveronent which will not lay out an adequate sufficiency of this method of air evacuation does not survive many weeks of war.
It was pointed out that the "digging in">problem^would:• ,¾1¾"V^ apply. equally to units such as general hospitals p Well"to the -reaj^-*-— -of the Combat Zone. Qulded missiles and long range artillery may ' penetrate 80 to 100 miles behind the fitting. -¾Z^3VcJ. **.;-..<
Général George Anastrong "corrected any impression wnich ' r - - n>-may have been created by an earlier speaker that the United a ta tes^^ ,^ / Amy. might site a surgical hospital close to the divisional area"as- '• • ' . / shown in the previous presentations,. If nuclear.
weapons were expected 1 ;. to be used. Surgery in the forward area, as was the practi^S^îûi^K^^L^^ Korea, - would be out1 of the question. He was in favour- of • sit'tojg "-the Field Dressing Stations well forward, for screening purposes,« • -was indicated by Brigadier Hunter and would Ilke1 to, place t^w ;CaSualty ' -Clearing Stations'50, to TO miles farther back than nad^folon^^C^ssie ' ' - f * < . ' •
; It might be necessary in the future to consider ,not{ only-' , • ; smaller medical unitss but also .smaller t a et ical Vnlts Tft e;tae<&cal,,^ policy would be to get rid of the serlou'sly in^rec^'as possible "and to get them as far back as "transport/ Bihdv gasoline.^ouldi-^^tZ allow. If air transport is available in quantity, the division ;shown , here acting independently might be replaced after a few days bsr^ft.^tj^ • ' entirely fresh formation. The layout in the Combat Zone was-ndw^iîiHr^"*-'' very fluid state and no delegates could speak officially on. the'-policy of his country in the matter. In the United States.,, the thinking,,at i r ; / — present was to attendît to reduce the size of medical units, in/the^-j ,..,/// ! Combat Zone. ' ' 1 ' " . .'. .'j v
Croup Captain Baricer suggested that medical, units, be-kept clear of likely target areas, and so avoid destruction,/' or at least be more widely dispersed In smaller units, .'* ' »..' /r V-VTV^V- 7 ,
T r , • S -1, .. : » • r TJ y Y J 1. - * /y VAl * 4 If W *- • Y
Colonel CroSse pointed out that medical' aid m - -on the spot, and with the fighting man, but this medical add must' be jT cut to the minimum. Brigadier Hunter said that, we were going to; . . fight U w
Conventionalw as well as a nHuclearw war. The'fighting^., TCfli f r
troops must not go without lmnediate medical aid'.'' "' •• ; ; \ •
Group Captaïn- (Cellars showed that on the awëï the Corpaf e Medical 1Cantre was placed "in line on a straight- road« and. this; pre- .."l;/'• sented a-target for aircraft. . :. . . . / . . ^
' • . -if- *-.• : , ijts? "-/•'•-'''
: 1
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Colonel Crosse stated that he had not neglected this fac-tor in his planning, and that the sites of his CCSs as shown on the.1 r ^ ^ model were diagramatic rather than factual. " ' ; y
, Colonel Casters agreed'that, since the number of medical^.'' personnel would not be large, it became important to. accelerate l'Iti j f casualty evacuation out .of the Combat Zone. He 'thought ;it; import-ant to keep medical units well away from military targets, to er^ f^^ courage th» en « y to abide by the Geneva convention. He asked how 5^v V,'"' the echëlons of casualty evacuation behind the divisional àrèâ Were1^frt organized in the British Amy. He said that certain wounded would ''' require treatment successively in Divisional, Corps and Army Medical ITriitS . I , - •• t'j ' 3 • '•'•'•
; Genaral' Harris, replied by an explanation of the1 use ôt i e r r t ^ ambulance cars, ambulance trains and aircraft in the rearward '- y^; areas. ' : ' '
. ' . • ; - ' _ ./. WMM Ii If H Ifi, w JUUL MMW JtJLlC- JUUL JUUf- W W H , 1 !-V • 0 # -¾ if '
. H H H R H U H H M T* H H T ^ H 7 . , H H P H H H H H H H L T h
.. ^ • .v . 1 : - .lo.-dtf
THB PROBLEM OF ADMS U DIVISION (DIVISIONAL SURGEON) AT 1600'HOCBS ON D PLUS 9. i .e.. 9 OCTOBm 1957
The AIMS J+6 Div, Colonel Marks, will present to you his " L ^ plan to meet the casualties expected in the battle In which his ^ Division expecte to be Involved at any mcraent now. The time is , 1600 hours'on 9 October 1957 (i.e., D plus 9). He is assisted by a visitor. '' . , V--T ^SJ
. ' H If If 'AflfH Iflf-Yf "" j • ". * f' 'JfcW LT. COLCMELMARIte. . * * * * * * * * * * * * ^ l w • , • "-'.<• • • • ' ' ' - . . ** s ^ • <- -. .-. - ;--/-1 .-»C'-f
The aim of this serial is to examine the problems of atomic^ Jrl* warfare at' divisional level with the present British organization. • ' '
We have seen something of the problems In the Ccm Z ahd Base,; -. at Arny l*v«l and in the Corps, but in many ways the problem' !« the Division la the most complex because It is, complicated.by thet tactical,^? situation, aa I hope to show you. " - ; f-?
. . . . . - . - . .. . . .,. . - . • . - . . -,-- i . . ^
' 'S'-'1 • 'J.:' -'• S-f^i , •. . ••-. "- V ::..:- ".-.» ?•'
Is there any real justification for considering this prob- " lean in the Division? Will the enemy have enough weapons to use them,4.; tactically over the Division? The answer is, of course, yes, and in ^ two main circumstances? M
v a. As waa! stated inthe Exercise Setting, having caused „ ^ as much disruption and disorganization as possible In the rear areas, /f'/~ as a final coup de grace he will attack our defensive j>ositioA with ' r' ' • a view to breaking-.through it and making rapid and deep penetration into our rear areas.'
b. At any time, particularly in the attack, when there might J ^ be' a concentration of troops maklng a worthwhile target* * -
0* The enemy will have enough weapons of various types and, be able to use them tactically at any time when the mission of his ground forces is sufficiently important to justify their -Use -Whether " ' we at that time offer a worthwhile target or not. ' iT j :1"
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
It is in ths defence that the problem is most' complex, V ' \ and it, is that problan that I wish mainly to discuss..* Porfthe< pur~ ^ *• pose of Uiis exercise I assume a division to be directly attacked and not by-pasaed„ as might occur If there were gaps betwéen the; divisional defensive positions, • " • • -^'1 ^ "''V
THE MEDICAL PROBLEM ",
: ; • -'• KV, .... .. '..
Casualty Estimates -.-1 -—-—
sV .;
In the varioiis exercises andstudies during tHe w V ^ ^ we have considered the use of -one both' over- the divisiohï7butV^ a " '/.' -r ^ s
you have heard, careful study suggests that the enemy will "aim; at^ ! * producing 20-25 of • casualties in the division and this 'may entail^' ^ ^ in a European theatre, the use of 3 or U weapons of '20 KT energy or^"^.' relative numbers of smaller or greater weapons* - 'The mmbers of cas-ualties that we must consider are*of the order:of 3 j000-£,000. Vftsft^f us take an arbitrary, but we think, realistie^ figure of 3/500 in j/ j,*;/. addition to the conventional'casualties resulting from likely ä^T; :1'' /,' , tillery activity on the fringe areas and the associated ground 'attach?9-' ' The figure of casualties trill vary, of course, but this figure may be taken as representative of the order of magnitude of the .problem :' with which we have to deal. ,- _>•--'..•:-, '
Prcm the medical point of view, we want to:: knw'the" pro ' - '*'''' portion killed to wounded. However, there will be mäny,*4iö « e - s t i l l ' ' alive after the incident and will have received InJuries from which they will sooner or later feertainly die for these men, but it.is obvious that sorting is available, the medical effort will be wasted.
,e. We will tryH<d<^^ethinip ^-;' in many cases', until''Skilled > ; c
It has been estimated that rather more- than hal^itheZtortl^^^ f casualties will require full treatment by the medical servieSa^î»et&- * « * us say 1,500-2,000 in the division. Of these, the Mfrritjrwill^ be burns either alone or complicated by blast and/or radlatiori in^ury.-1 • *"• 1
_ ; ., . j. • 1 . ;• . i r ' T f h -A • • ** r * .--h,
These will require, according to their sevisri ty^somé oif: all' -Zjy. of the following measures: ' M'-;?.^- .v1"/ '
• a. BurnB -DreISISiInff - to minimise infection« to fort in transportation and possibly to reduce fluid;loss.tit^Tn-Jv" ' - ^ "
b. Morphine ..Deep intramuscular inj^tionPfbf ^ 'm^;^^ - ; i V ï : severe cases. Milder eases (less than 15$ of body area) may be given -.. a milder analgesia. i • ' •
c* Antibiotics - These may not-be eaeentialwlthirittie first 2 hours, but are best started as early as possible. ' :: k-
d. Intravenous Fluids — These will be réqnir^fôKall^&es'' ' of 20$ to 30$ body burns. The level at which transfusions Wili bivgiven* ' will depend rather upon the time lapse after the incident, than 'distance -so that in effect every medical installation; capable of doing; so must be prepared to initiate intravenous. transfUions. Blood is;unllicely .to-be ' available or practicable at divisional level. Most' British Surgical, authorities agree that the fluids^of choice for infusion at diviSional level is dextran. • ,T ' - ; .
e. Any or all of those procedures NOT carried'out farther* :, forward must be carried out in the Advanced Dressing Station (Clearing } Station.) • -
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
•X
•
Traumatic (Blast) Injuries - - . - ' . - . ^
The treatment of these eases .will be as;for orthodoxcas- - bX:.. ualties frcm conventional weapons except for those complicated.by: burns or radiation injury.
Radiation Sickness • . • -.-.t. -.1.-...-,1 - •'
The main requirement in these cases le a means of esti- " mating the dosage of gamma radiation.received* This Isof particular Importance for casualties incurred when ln sllt trenches where it is likely that many bums will have incurred sane ganma radiation. The srf rapidity of onset of symptoms may provide seme guide as to the-dosage received, but the symptoms in the early stages as we heardlast evening : .. from Colonel Meneeesp is non-specific. These cases will require no treatment at divisional level, but the problem will be to decide which '/.- ", are to be evacuated and which are not. (I understand that-the question ^ -of the issue of tactical dosimeters to every soldier is still under con- ' sideratlon.) . '• - - -• ' . 1 '•
" ' - • • . - ^ - • • . - • / - • ' • - • — , *'!.V •
THE TACTICAL PROBLEM .-, ' -• .. • • 1 . - . .- . - - . .'.;'..-• J ' / f y - •
Tn considering the tactical problem It must be assumed that ' t ' the enemy will follow up the use of his atomic weapons by a> major ground attack with armour and infantry in Armoured Pereonnel,Carrlera jtor. a^^.t :,-1 j-,-; ploit the füll effect of the weapons. Such an attack may,be expected-»-./ quickly, possibly within an hour or so of Uie incidents in order>tot1"« Vj'-ï ~ ' effect penetration before we can recover coordinated action and before • our major counter attack forces arrive. .. • < ., , ^ '
Peployment of He ical Unjts" ' .
The JMS in his appreciation said wWe must plan for the or^ ^ * thodox battle but at the same time be in a position to cope with ai .t-Sx« ' -number of atomic incidents.
Oollectlng ' . , !
Applying that principle to the divisional medical services in a defensive position it is obvious that the de/ployment of Casualty . Collec- :, ting Posts will not initially be affected by the atomic problem.^JThey/i should be, therefore, deployed as we normally do In support of a 'defen-sive battle—that is one Casualty Collecting Post in each-Brigade (régi-1'l^ ment) at about the IevaLof Brigade. Headquarters. Any reserve that we.i , ' can keep out of the conventional battle might be held with one of the Clearing Stations in a potentially safe place.
- 1 . \ I • .- »,- i\t :
Clearing / -• -.:v* .-
In the British Medical Services the. three .'Advanced Dressing f Stations (ADS) of the 3 Field Ambulance normally are used separately* ' .- :.: They do not normally carry out surgery and do not bold casualties. :. * Their taak is sorting casualties and giving a high quality of first ' aid treatment to enable the casualty to survive the fürther journey ' >j to the Surgeon in the Corps Area and to («rive there In good con-. j dltion. To support this battle we will deploy our,Unit's;ae follows*»'..V; . '
1 . ! -, . - . . ". -• ••• .> .-.v.'- '.-.'•..:,.' -tH'r«' *
1;;*
!
a. One AD3 between the gun area and divisional HQ area••ttf'WSïY^ ' i receive the bulk of the casualties from-the conventional battle.«: Iti^a" may be that we put this unit at ride from atomic attack on the gun * ^ ^ area, but we feel that the conventional battle must be adequately v.. covered and we normally like an ADS as far forward as that, 1V . !
' ; ;. vy^fvv' _ i - j
- ••/ f:
NATO CONFIDENTIAL ' - - V ..... . ." • • ' - ' 'V- -<• :.
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
b» One ADS closed and packed on trucks unless it is re». , < quired either because the number of casualties Justified its opening or because roads are such that one ADS cannot cover the Whole " slon. This unit we will put another two miles or so to the rear* *
c. The ADS we will hold well back in the divisional admini-strative area or even Just behind the divisional rear boundàry in; » -potentially safe place. It will also be the atomic reserve m«iie^l\(t' , unit either for use in its own division, or to be called upon by the ia^.a& Coros Surgeon for help in a neighbouring division if requir'ed;
d. The Field Dressing Station -is deployed iri/ïhej -Ir J - '+ - Mi- -DivisionalAdministrativeAreaholdingminorslck. ' ." ' ' . ' ^
e. Medical Units In neighbouring divisions are' deployed r v . on similar lines. [.sr - i ^ - ./M
Now iS the enemy' has four bombs or weapons to use over the Division, he might use them on one or other of the following areas:
• • • r , ' -," t - a. The Forward Brigades
b. The reserve Brigade v . - - • , -e. TheGunAreas * - • d* Divisional Troopa and Main Division Headquarters ' ,, .,,,. e. DivlsionAdminlstrativeArea ,.,,.:,-^1^-The Forward Brigades ;;..• . ,. <r.-
. , - . / - ---, **'• t*?'
These must obviously be attacked, but it ÎBeems llkely that^6¾. the CE of the bomb will be well to the rear of the brigade areae'for.^^ two reasons: - , . , . ;
a. The most forward troops are probably thebeet^dispersed^.' and best dug in or protected and therefore offer us poor dividends in casualties. . . .,.-: ^
b. Unless «no man's land" is wide, I would hayerto Wiibdwtw Ic, my forward troops to avoid their becoming casualties* . This"is" not a.' ..', good thing to do Just before a major attack.
. Th? Rgagf™ p r i c e s TiVA-1;'''
This offers good prospects because if suffi^ent^*ïè<^^ ,' ^ mated the lmnedlate counterattack forces cannot be brou rt," into ^ i s /
' action thus giving greater' freedom of movement when a break-througHj . ., r_ is effected.
The Gun Areas V . / '•-.'-V' •**'-•"** .•»'>*>
If the gun areas are reasonably concentrated,they offer an , v . . excellent-target because: - ^ \ , V ' r V
. . . . . . .-,.(- ., ,-..
a. At present the 25 pdr gun pit cannotbegiven,overhead,, cover without limiting the elwVStion, etc, of the gun. ; V ,. "
b. Loss of defensive fire would make the enany tasksnich V easier*
- Divisional Troops aM'.Pi^slonàl' Headqua r t e r s^ . .
The aim here would be disruption of command camninications v .
12a - .'.'••
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
and control and there will be a certain number of InatallatlonBi e. g. , Tehicle workshops, medical units and so on, that cannot, go .„ - > underground. " . "
The Divisfon Adainistrative Area
This can be pretty widely dispersed,, perhaps over 5 miles ^ square and so does not in fact offer a very good' target. Furthermore,/ ' if ground attack comes in quickly, the cutting off of suppliss and- / j ammunition is not7llkely to effect the Immediate battle. .It may, well be that in a defensive battle in atonic warfare the brigade sectors and guns may be self-contained for at least a 24 hour battle. We wil l take it then that the enemy will "use his four bombs thus: .„.. ,
a. One each to the rear of the forward brigade affecting also some of the reserve brigade, leaving; a "crust" of forward defen-sive positions.
b. One over the reserve brigade and part of. the/gim/àrea .- ;
c. One over the rear of the gun area and affecting part of ' / the Divisional Troops area. And after that, the enemy will attack. <.
THE BATTIC
Medical Units
It looks then as if all our deployed Casualty Oolleetlng Posts have become casualties. One ADS has been destroyed and this one (in Div Troops Area) is partly damaged, canvas blown,down.,<fThe Divisional SUrgson (If he survives) calls the rearmost,of,the AbSs Vjyet^-forward to open alongside the'dSmaged one. At the same time Öivis"ion^rw . al Surgeon would call,on the Corps Surgeon for help. The ADS from a" *" neighbouring Division which had,been earmarked for this role might - ^ then move forward and take up positions either with the two. already, ,. j ^na-functioning or perhaps better on one side of the incidents so -that. ? thfcy can start clearing casualties from further forward. The Field Dressing Station cannot easily be moved as it is holding minor sick but it can be used to accommodate many of the less serious cases, , ,„ t :% „
Deoloment
As I see It, whatever collecting element you have got will . go forward after a brief reconnaissance and open up.as far,*Intor-the affected area as they can get. They function merely as. collecting.. posts and,ambulance loading posts. They will require. as'many ebctra i i j/T stretdieK bearers as can be found and as many vehicles as are avail-«-Ji, -able. Cases either walk or are transported to ADS where they may wait, are sorted and treated, then held or evacuated in that.order on a -strictly priority basis. The primary task of medical officers » i l l be firstly sorting, and secondly, treatment of the more difficult oases. . . », . ...., •-, ...-
Other Ranks (enlisted men) will work on the tesm.principle ' with departments organized .on a product ion. line basis. -If.there.is,, "any hold up in evacuation frort ADS Which is most likely, cases must be held In the open air if necessary, and with, the,most serious;ones under observation.''
In the meantime, .the «lany's main attack will-have come in possibly in this manner- (fWrital'âttack vdth - hooks"<m"eteh fiank and our own counter attack or "stop gap", force will be moving.forward into the rear of the divisional area.
I i S
NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

If th« enony Is successful the atomic casualties in the forward part of the division and the casualties in the "crusWfron the ground battle will inevitably beccme the enemy's responsibility.' - - -. ' Further, if he makes rapid progress, our main medical effort here, which should be in position before the reserve force has reached the division, may well find Itself between the opposing forces or even • -V-
- overrun by the enemy in its turn. Similarly, medical units on the r flanks may-be involved in counter attack battles by the flanking divisions, . •'. ' ••-•
This is painting the worst (picture—if the "crust^can^^v '. hold the enemy off long enough to give our reserves time to get „. well up into the divisional area our problem is'simpler^and we ; v > might then have the medical units of the reserve force to help -us; • . . -Furthermore, we can and indeed, must, incorporate at, least « e ^ ' ^^f;' 1
platoon of the Ambuiance cars in the order of march- of the reserve /.w.
force so that we can get seme reasonable amount of medical transport . forward on a high priority and that is the mosrt likely way -of doing -it, when roads must be reserved for the reserve force onlyi?« Vt . 's,?-'rzti, Evacuation ^ /
As an estimate, we might say that about one third of our - V -surviving casualties will require urgent evacuation, that is-to s.-' -r arrive at the Surgical Units within 6 hours. On our figures this-is seme 500-700 cases. These will not be all ready for evacuation at J v once, owing to the difficulties of collection, sorting and prelimin-ary treatment. Further, they will be distributed throughout" the" • •> area and therefore between the two or three ADSs brought forward.*v --u It may be that the ADS on the flank can evacuate their share, -sayr ^ ' 150-200 fron their own divisional resources leaving the balance at .-the. back of the area to be evacuated by the platoon of ambuianceHcarst> fr^ coming up with the reserve formation« This may be within 2 3,*hocB» by which time most of the cases that had been collected would; be--v ^ ready for evacuation.
The less urgent cases must wait and will be evacuated Itt' . due course using the troop carrying 3-ton trucks of the reserve y force and any other transport available either from Div Coin or from unit B Echelons. _ : ^
Helicopters ..
In the more distant future it is probable, that' suppiy mndvt -some movement of reserve forces will be by helicopter, in.which case;
a proportion of these helicopters could be made available for' casualty« évacuation on the return trip. By this means many of the mbrë sèriotis' cases could be given a swift smooth journey to the Surgical Onits7Ini'1 ;
Corps or even to the Amy General Hospitals. , The ability,of. the heli-copters to function even with enemy air superiority, its speed, smooth-ness and flexibility of distribution of casualties will be the ultimate answer to the evacuation problem in atmic warfare..- .•-•»•-.<•.. ..?.>-,
COHaUSION ..-. V-Vi-':^
If the figures we have used are approximately ..correct -Jt (3,000-4,000 atomic casualties, 1,500-2,000 requiring medical treat-. • ment, 400=-600 requiring urgent evacuation) It is possible for"the' ,- : present organisation of medical services in the division to.cope*with: the task with some outside help. This:
can be done> byi a deployment1 ~ that is not far trcm that required In a normal defensive - battle. :
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
NATO CONFIDENTIAL
The following requirements seem to stand out:
a. The necessity for a number of efficient and mobile but":
economical units to collect and stage the large numbers of atonic V casualties back to the surgical units behind the division. " : v /
b. The necessity for keeping one complete Clearihg-Statlorii-^v
(or equivalent) well back out of harm's way so that it may survive • the attack on the division and be available to clear its share of the atomic casualties.
c. The absolute necessity for rapid communication between'1. ' the Divisional Surgeon and his Hedical Units so that he could move /'-'L >
them as soon as his plan was made. This means the existence of a v
medical wireless net, ^si . , • . " ' . • '> ' • * '
d. The necessityforextra stretcher bearers from other arms for collecting of the casualties so that medical manpower can be concentrated more on to sorting and treatment.
e. Medical transport is unlikely to be able to move any-thing like all the casualties, therefore we must call on Q for help with extra vehicles both in front of and behind the Clearing Stations,
f . To . stress more strongly the tremendous advantage of -the helicopter in casualty evacuation, especially in conditions of. ' !
atomic welfare. "'
It is evident that the task depicted will rsquire a medical service of a very sound state of training, of the highest morale and ; • of a devotion to duty equal to or greater than many of the fine écain-*' - ' pies of the past. . . ..
tij. OfrW HWMMM « IfJMt^ Atilf AfcJfcJt W W tf tt W WtfttWW T n T T K l r n n i r h n ft H H N H N 1H N N N H H H J I H H H N S H
# # * * *
DISCUSSION ON SERIAL A3 "
General Dale spoke of the type and scope of medical treat* -ment available In the divisional area, and recalled that Colonel, Maries had said that only first aid treatment would be carried out. If the division should be isolated by the enemy, it would obviously ^ " be necessary to provide more elaborate facilities. He also commented :1
on the fact that two out of three dressing stations were deployed ; leaving an "atomic reserve" of only one clearing station. He asked " T* whether it would not be advisable to open one dressing station only, keeping two in reserve in case of atosiic attack,
Lt. Colonel Marks replied that if there was a gross «hold- J' . up in casualty evacuation and if a'large number of serious traumatic k
cases were being held at divisional level, the Divisional Surgeon must ask the Corps Surgeon to bring forward surgical teams and form an advanced surgical centre in the divisional area. HoweverVthe ; Divisional Surgeon would hope and .plan to get as many casualties^ ' ' as possible out of the battle area. There were many circumstances. -./ " \ in which General Dale's suggestions of holding two dressing stations "'• in reserve would be right and feasible, but In the present situation^ ' ^1-' he felt that a divisional front of seven miles called for two ' ' functioning dressing stations.
h
•
T"
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Oensral Fastlng-Hansen thought it unnecessary that a wunded man be treated successively at all ths echelons of medical units, i.e., at the battalion aid post, the Casualty Collecting Post and the Ad-vanced Dressing Station.
General Harris agreed, and said it was not the British prac-tice to offer treatment at each medical echelon as routine. In many instances the casualty would not even be taken out of the Ambulance Car but wuld be checked by a doctor to make sure there was no need.to start emergency treatment for bleeding or shock and that the wound dressing and splints were adequate. This practice made tor more rapid casualty evacuation and a quicker turn-around of ambulance cars.
Air Marshal Kilpatrick showed the necessity for good communi-cations between medical units, and pointed out how difficult'If not im-possible the control of casualties would be if there was no ttedical radio net in the Divisional Area. He said that all casualty evacuation would be a matter of perhaps fleeting opportunity, and good eomnuni- . (/ cations were essential or ths opportunity would be lost. ' He Said that* evacuation by helicopter was the best method but was glad to 'see that' our attention was being paid to other means. No one was yet In a., „/ position to say whether air enemy could interdict movmnent by hsll-copter and it was wise to make use of all forms of transport ft*» ths battlefield.
Lt. Colonel Dickson wondered whether a Field Ambulance could adequately treat 2,000 wounded in 24 hours, and suggested that the capabilities of so email a unit had perhaps been over-estimated. (NOTE General Harris and General Relllnger both confirmed, subsequently, that they had personal war. experience of a field ambulance dealing with up to 2,000 wounded in 24 hours. It could not continue to work at/this //" pitch for more than about 24 hours.)
tMU M A* U hji H M IfH " ^ " " " HRM-A MUMM MHMM Tnnnr WWinr
THE EPILOGUE
INTRODUCTION b£
Lieutenant General Sir Frederick Harris Colonel T. M. B. Ahem ; ;. . /.
LT. GSiroAL HARRIS ~~ / - // - -Ve have now presented our picture and tried to show-you how
our present field medical units would cope with all-out atonic war. ' I have told you that I think these units need modification to meet atomic war, and have given you a handout. (See page 129).
But who can really forecast the future? « . /
Ih 1929 we were told that Ihissla would launch eha&cai war» fare within 24 hours of entering a war—Voroahilov said so 'publicly.
Ih 1942 we rather shamefacedly began dumping all the Gas ' Equipnent we had been dragging around for nearly 4 years of war.
Wiat is the lesson?
Vfe must be wary lest we abandon our tried methods for some-thing that may never materialise.
125
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
On the other hand, there is a difference today. Ve have to counter massive manpower with nuclear weapons. Thus we simply . -must ensure that our medical organization can cope with nuclear war- ' '*, fare as well as conventional weapons.
In this exercise so far we have seen that there have been two salient problmast c-
Firstt ,
The.present 6% bed cover in a field force as normally allotted by the British General Staff would have proved inadequate ' : ' ' without a 50$ crisis expansion.
52SSGâî-
The possibilities of interdiction by nuclear weapons is pro-; . bable at any level from front line to baseband will produce casualties "7 at any level. There are sane indications that the present British;; ; ;
Field Medical organization, which I consider to have been admirable for^ the needs of the old pre-1945 type of warfare, needs same readjustment" to meet the changed task.
The answer to the problem of bed percentage is really a matter of manpower priorities for the General Staff, but the second problem was a harder one.
Have a look at this Chart. v . Civ: . . * ;
Tou will see at the top there is a division and the medical"; . potential for the two functions of collection and treatment. Tou will ~
' see that' thècolleetion potential is high and the treatment-potential low, since it is designed only to give essential first aid during evacuation out of the division.
By contrast you will see that behind division the treatment potential is very high and the collection potential low. In fact, a reversal of the position in division.
In the old conventional warfare this was perfectly logical, most efficient and economical. Now, however, it will be necessary to be Ale both to treat and collect casualties at any level from front to base, and in the simplest terms, the Field.Medical Organization .-muat be adjusted to füll in the gaps shown here—better treatment potential within divisions, and provision of collection facilities behind division. I propose to show you one way by which it might be done. By replacement of =
Fd Ambs and CCS ' • -by Med Collecting Unit
Med Clearing Unit , Casuflty Evacuation Hospital and the addition of some Medical Collecting Units and Medical Stagint Units to rearward areas
I will now call on Colonel Ahern to give you the tactical setting of what we might expect in future war. He will describe the picture as applicable to a Corps of three Divisions.
* * * * * # # * * * * * * * *
m I
NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

COLCWEL AHgiM
Colonel Ahern then demonstrated the tactical setting an a cloth model, and spoke as follows:
"Because the NATO Nations will never be the aggressors, -we are showing our own forces in a defensive position—as they would be at the start of a war, defending a river obstacle. We show here the deployment of an Atmy Corps of three Infantry Divisions with an armoured brigade (regiment) in reserve.
Each Division covers a frontage of about 30 miles but is not necessarily or even probably spread out along this frontage.- A front of say 15 miles is IlkMy at times, and the Intervening gaps would be heavily uinèd. The whole of this area would be covered with atomic artillery.
Thirty miles to the rear would be commodity dumps/ and here-abouts would be found the Corps Headquarters, now a purely tactical; -, HQ, shorn of its logistics functions.
lying well back and at about this Ievi would be the counter-penetration force, our Armfmred Reserve, which would be divisible into. Battle Groups or Combat Teams.
There may be no Corps rear boundary, iince the headquarters is purely tactical, but about 30 miles behind Corps Headquarters is the Army Rear Boundary which may also be the rear boundary of the Com-bat Zone. Forward of this boundary are found Army Headquarters and the Amy Maintenance Area. The latter has acquired an increased -im- .. portance since Corps HQ logistics functions have passed to Arny HQ. . :
H Vt Vf W M If I f If If i t t f If -M i t i L M . J t i O t HflH H H H H H H TT H Hl^ N p N T n T T
When thqpattack, the enemy will most likely try to pene-trate between our divisions, but whatever form the attack may take, it is our aim to force the enemy to concentrate and to provide a tar-get for our atomic weapons.
Should they succeed in getting through they will be engaged by our counter-penetration Amoured Reserve and the battle may occur in the area forward of Corps HQ,
The current concept for the Lnfantry Division sea&s to be. that infantry and armour will became more integmebAAd. Each Brigade (regiment) might be formed of three infantry battalions and one armoured battalion.
The Armoured Division may have two Brigades-(Regiments), one of four armoured battalions, the other of four infantry battalions. The Armoured Division could then split into four identical armoured/ infantry battle groups.
** ** " JJ -M fc*^ " «j »*MI« M U I* M à. M 1Rn H H HR W.H R * RUR I R K HlMr
These assumptions, if correct, have three important impli-cations for the medical services:
a. Our Casualty Clearing Stations (Evacuation Hospitals) may find thanselvea in the middle of the battlefield. Without heli-copters, casualty evacuation might be impossible.
b. The forward Infantry Divisions may be isolated,
127
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

KATO CCNFIOMriAL
c. There will he mobile armoured/infantry counter-penetration battles with Brlgade/Regiàental or even Battallnn Battle groups acting independently and isolated from ortè another. '
If W If WWW MHW * * * M N K If M M
(SNEtAL HARRIS * I
ïou have now had the problem presented to you and the tactical ' setting irtiich Is still not firm. In addition I would like to quote Crom Brigadier Richardswip DEHS 1 (British) Corps as to what he thinks of the • battlefield of the futures \
'lThe task will be collection and évacuation of casualties (which may be much heavier than in the last war), and from ljtuch wider divisional • fronts (up to 30 miles) with a greater liability to fnemy penetration, • and the likelihood that battles wül be fought as Brigade battles to an % even greater extent than hitherto. Formationes especially armoured formations, may often be moved at very short notice o another sector« The use of atomic weapons would add to this picture f risk of-Very -,
< heavy casualties beyond the capacity of a formation's own medical re- V r sources, and needing special supplies in amounts whiçh these could not • , in any case carry with them. This task will call for an increase rather than a reduction in our facilities for collection an<| treatment, and in-crease in their flexibility by providing adequate mobile reserves, and an ability to decentralise control to brigades. The weakness of the single divisional unit under one Lt. Colonel would be that it would centralise control. The present tendency for lines of evacuation from brigades to converge to a single point may have to be abandoned. They -; may have to be parallel and not Inter-dependent;11 - p
Ve are therefore in a position to try to extract -from the wel-ter of views and new ideas, certain points on which to work despite the'"'i • changing tactics and equipment.
Comnander in Chief, Northern Army Group, said, in 1953J
"The side which enters the next war with the mentality of the'' last will suffer from a disadvantage /ram which it might not recover.41 ,
Our old ccmeeptian of Colleff^ng the Casualties and evacuating them for treatment may have to be scrapped.
We may have to bring treatment to them more or less where they lie at various levels. A two-way flow system.
Essential Requirements which however conflict strong* * - • *
a. To keep in line with the rest of the Army, we mustt
Deereasemedlcalmanpower -Reduce our transport Increase our mobility » *
BUT -
Ve must increase our medical potential, and our facilities for holding and treating casualties»
b. Divisional Commanders - especially Armoured Divisions - would like to be rid of -
heavy field dressing.atatlcaa-which limit mobility,.BUT, they often want, for reasons of moral*- - awrgery artd^lodcftrausfusion .
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
fürther forward than we consider ideal.
c. Many Senior Medical Officers are against using medical manpower to improve facilities for treatment within divisions. * Thsy say it is apt to be sketchy and if more,merely delays th«" casualties' progress to the Surgeon,
But,
Recent exercises have suggested, and Divisional and-other Conmanders confirm, that we cannot be sure of evacuating them for a variety of reasons such as enemy penetration or chaos in rearward echelons, Then we must have something on which to build adequate treatment—Including surgery on the spot.
d. Even if air evacuation is in full use, holding facilities would be needed in the division as a cushion against delays, where also' casualties would be sorted.
These views are paradoxal. We have potentially more casual-ties—we are being asked to do it with less men and materiel, and under more difficult conditions«
»
An easy method would be to try to insist in filling our gaps by asking for more manpower. In a type Aray of 10 divisions the bill might be to convert a Brigade of Infantry into Medical Corps personnel.
The general staff ars, however, faced with-a ruthless enemy with no regard for casualties. Their job is to put all Mphasison beating the enemy, not on building their non-combat tail.
Our Job is therefore to produce a field medical organisation • which will -
a. Meet our professional task
b. Meetpresent and future tactical requirements \ . .
c. Meet in a no-cost basis, or saving, by putting our re-sources to the best advantage.
This means thinking radically. We must be prepared to take an administrative risk.
We must for instance realize that our first-class cross-country frehicles that go anywhere can save Stretcher Bearers—we must avoid duplication.
I have given much thought to the medical organization of the future, In the same way that you probably have, and I believe that with the likely tactical setting, the impact of nuclear weapons and the pro-fessional requirements which are familiar to all of us,, that there are already certain discernible trends.
I feel that the requirement is for small interchangeable units which can be used at any level from Bde to Base. They would be capable of being built up into a medical task force at the place and time it is required. This postulated the provision of atainistrative headquarters on which bricks can be built.
We are therefore considering the replacement of the present one FDS three field ambulances in each division (two in an armoured
1¾^
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
division) by one medical collecting unit and on «medical staging unit, and by the replacement of 10 CCSs in the type Any by ten evacuation hospitals. We are also thinking of adding a certain number of medical collecting and medical staging units to the rear- • ward areas* I would, howevera stress that in Serial which follows-now, we are dealing solely with one division engaged in an atomic •• battle—that is, we do not take you further back than divisional headquarters,
### * # * * * * * * * # « * # # # « # * «##
» • I NOTES ON EPILOGUE
A study is being made of the following new British Field Medical organization consequent on the advance of thermonuclear war-fare.
Present British Field Medical Organization includes:
a. Division
i* Allotment
Three Fiel d AmbulanceA per Infantry Division, > Two Field Ambulances per Armoured Division.. One -, Field Dressing Station per Infantry or Armwxred Division,
i i . Organization
Field Ambulance - 13 offioers, 211 OB -224. HQ which forms an advanced dressing station, one-coy with a small HQ and three sections each forming casualty clearing posts.
Field Dressing station - 7 officers,, 109 OR - 116.
Small administrative HQ and two equal sections each desisted to hold 50 cases.
Iii. Role
Field Apbulances - The primary role is rapid collection of sick and wounded, rendering of first aid to casualties, their preparation,-: classification and documentation for further- -*•• disposal. A mobile unit designed to provide the simplest accomodation and essential treat-ment.
field Dressing Statiwi - The primary role is to hold minor sick and Injured and mild exhaustion cases -ex-pected to be fit for duty within 7 days. The Divisional Field Dressing Station Is identical with the Corps and Army Field-Dressing Station, and an ; additional role of those units is to act as the . nucleus for attaching field surgical and field transfusion teams when forming an advanced surgi-' -cal centre.
JiSO
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
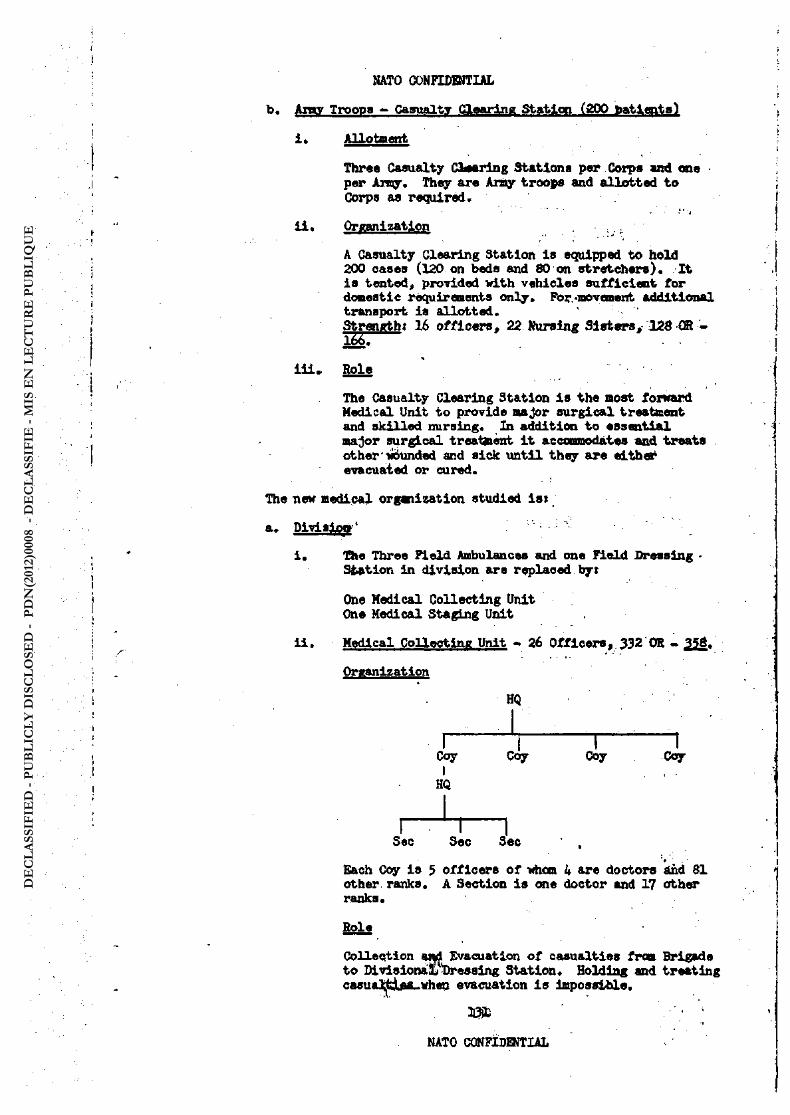
b. Aray Troopa - Casualty Claarlng Sbaticn (200 toatiqits)
i . Allotngnt
Three Casualty Ctearlng Stations per Corps and one per Amy. They are Arfty troops and allotted to Corps as required.
i i . Orfianizatipn
A Casualty Clearing Station is equipped to hold 200 cases (120 on beds and 80 on stretcher«). It is tented, provided with vehicles sufficient for domestic requirements only. Fbr..movement additional transport is allotted. Strength? 16 officers, 22 Nursing Siafcws, 128 CR -Ï55I
Iliv Hole
The Casualty Clearing Station Is the most forward Medical Unit to provide major surgical treatment and skilled nursing. In addition to essential major surgical treatment it accommodâtes and treats other wounded and sick until they are either evacuated or cured.
The new medical organization studied ist
a. Division * • :
i. !Qie Three Field Ambulances and one Field Dressing -Station in division ars replaced by:
One Medical Collecting Unit One Medical Staging Unit
i i . Medical Collecting Unit - 26 Officers, 332 OR - 356.
Organization
HQ
1 " I 1 — — 1 Coy Coy Ooy Coy I
HQ
r — — I Sec Sec Sec ,
' t '
Each Coy Is 5 officers of whan 4 are doctors and 61 other ranks. A Section is one doctor and 17 eft her ranks.
Role
Collection at d Evacuation of casualties from Brigade to Divisional) "Dressing Statical* Holding and treating casual|ui&a_vhea evacuation is impossible.
jj3it • • ;
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Deployment In An Infantry Division
One company Is affiliated to each brigade and the company commander acts as senior medical officer to the brigade. One canpany is deployed to cover divisional troops and as an immediate atomic reserve.
Ii i . Medical Staging Unit - 15 Officers, 220 OR - 235.
Qrganiaatiwi
HQ
J L ' i 1 J L Each company consista of 3 doctors and '42 OR.
M s The staging (and when necessary, holding) and treating of casualties. Eaoh company has a nominal capacity of 100 cases and when staging casualties is divisible into reception, treatment and evacuation sections.
Deployment
One or two companies form divisional dressing stations for battle casualties!
One Company holding divisional light sick. One company held in a nSafett locality as an immediate atomic reserve.
iv. Manpower Implications
Infantry Division.
Present
Three Field Ambulances ... ... One Field Dressing Station ...
Proposed
One Medical Collecting Unit .. One Medical Stating Unit
In -Uie case of an armoured division it Is for con- -sidsration whether three instead of four companies are required in the Medical Collecting Unit* If this is so the proposed organisation is 507 as against the proposed 564* "
•fogy Troops * Evacuationmoapital .(500 patients) - 32 Officers, 37 Nursing Officers, 301 OR - 222
132
... 672 . . . 116
... 35Ö
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
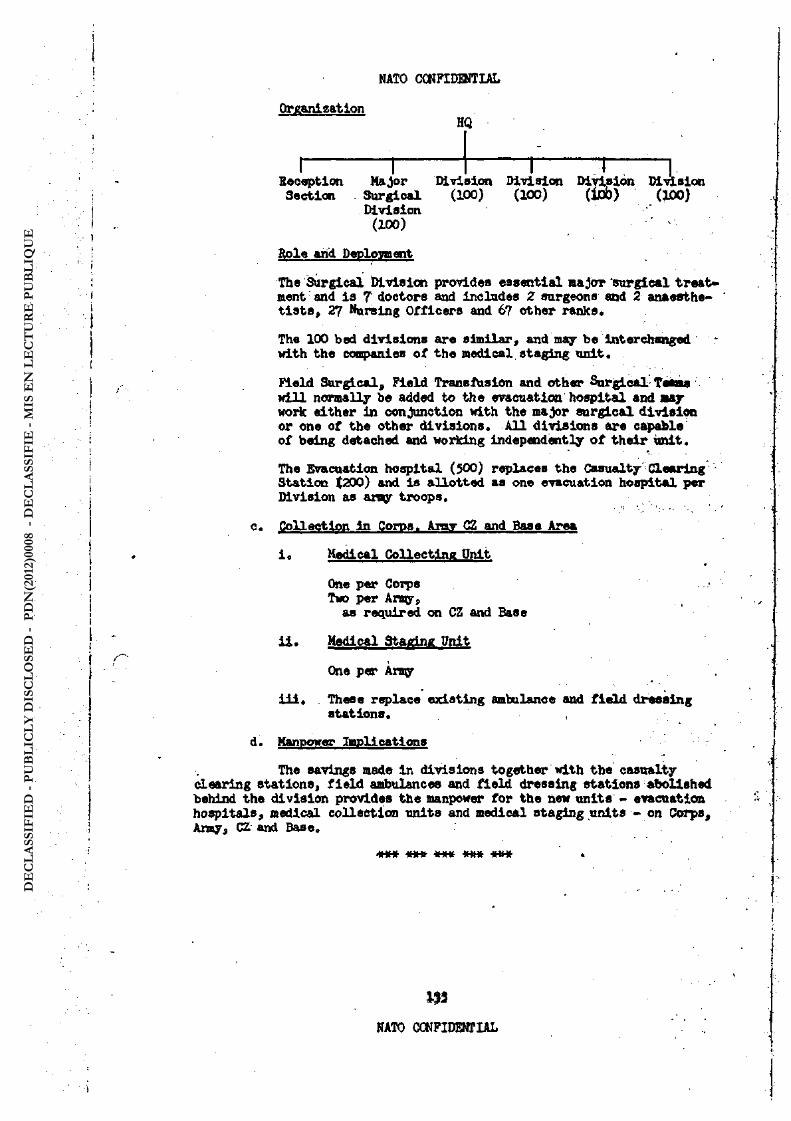
Organization HQ
1 1 1 T T Recaption Major Divisint Division Division Division Ssction . Surgical (100) (100) (lob) (JJOO)
Division (100) ' -
Hols arid Deploment The Surgical Division provides essential major surgical treat* ment: and is T doctors and includes Z surgeons and 2 anaesthe-tists, 27 Hursing Officers and 67 other ranks.
The 100 bed divisions are similar, and may be interchanged * with the companies of the medical staging unit.
Field Surgical, Field Transfusion and other Surgical Tesma will normally be added to Uie evacuation hospital and »ay work either in conjunction with the major surgical division or one of the other divisions. AU divisions are capable of being detached end working independently of their Unit.
The Svacuatian hospital (500) replaces the Casualty Clearing -Station (200) and is allotted as one evacuation hospital per Division as amy troops.
c. Collection in Corps. Aimr CZ and Base Area
i« Medical Collecting Pnlt
One per Coips Two per Army,
as required on CZ and Base
U . Medical Staging Pnit
One per Arny
i l l . These replace existing ambulance and field dressing stations.
d. Manpower applications
The savings made In divisions together with the casualty clearing stations, field ambulances and field dressing stations abolished behind the division provides the manpower for the new units - evacuation hospitals, medical collection units and medical staging units - on Corps, Amy, CZ and Base,
i U U l U t i w W W If I f H i f V t f t f . H Jl |F H Jl M H M H H SI Jl H H Jl *
in NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
EPILOGUE
Twenty Yaars On At 1755 on 6 May 1977
Twenty years have elapsed since the Great War of 1957; and it is now 6 May 1977* You will see the following three old friends, now naturally sanewhat frail, sitting together in the NATO Officers' Clab in London:
Major General Hopeful, now retired and somewhat somnolent. You will remmnber that he was D.M.S. Expeditionary Foi1Ce in 1957» »
Major General Bichard Maries, retired, who, you will recall, was Colonel Maries, A.D.M.S. 46 Divt 1957.
Lt. General Sir John Crosse, KGB, KBE, etc, retired, who was Brigadier Crosse, D.D.M.S. 2 Corps, in 1957.
JUUi W If W If 1f tt MHtt JUMfc MKM -H HW MWH ItKtT a a h n TrjrW n h 1H m mh h hm Tnnr
We will also Introduce si newcomer—Major Richardson, DSO MC, RAMC, who is none other than the son of Lt. General Sir Frank Richardson, KCB1 KBE, etc, who*is now retired and living on his estate in the Highlands, and although a little past his best, is still a player of repute of the bagpipes.. His son is a bright and "up and caaing Officer"—Just like his father was in his palmy days.
i y M j Ji fcyi J ^ Q i J U Q f i^ut JU Jk AMMt W^W ^^nT
H If M W V w HMW J U U t H I f t i i U U f c MW-M N M M NHH HHA HHH HHH i n n W*W ,
TIME i s m
SETTING a. Stage, Reading Room of the Senior NATO Club, St.' J an es's.
STAGE b. Floor, setting ground model, adjusted to show division.
STACT Curtained background j notice bung centrally reading "SILENCE PLEUSE" In 6 languages. Chairs arranged around the centre of the stage as though the conductor's rostrum was a fireplace. Two occasional tabled. . * *
SCBJE Three elderly officers (retired) in civilian clothes are seated , in the three forward chairs, feet and legs extended towards the fire. Two are reading suitable newspapers and periodicals; the third is fast asleep with a newspaper over his-face. .-They are - . Major Generals Crosse, Marks and Kfcpoflil. . ^ .
CERTAIN As the curtains part, gram, off is playing Brahm's "Lullaby". Y-This fades out as Captain Rory Richardson, of the SHAPE Medical Staff Department comes on L.. He is a smart young officer, and he carries a » a l l parcel.
Li fcJiU J J ^ J U U U t M i U ^ ^ ^ i TnHnf winn»'. f ooT ^ H W w nnr
Rory nI hoped you would be here, General John. Hullo, General Dicky."
(Uncle John hastily puts his paper down and begins to rise.)
Rory "No, please, don't get up Sir. I Just came to give you these cigars,..and to wish you a very happy 70th birthday."
134
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Ut John "Don't be Indiecreets Rory. At my age you don't acknowledge birthdays, Tou just nod to,them as they slip-quietly'around the corner. But thank you for the cigars, Rory. Very civil of you—very civil indesd ... in spite of the fact that you've • forgotten that I don't smoke - .-••},.-i.-. L-.f)
Rory "Oh, I ssy ,, . I'm frightfully sorry, sir. But perhaps you could keep then and give them to General DidQr on.his birthday, "
.-. <:' '••••• •• '.."•• ^Vtli . ùft.*»»
U. Dicky "To ny birthday, too, we'll share them,' Looking;â: bit under • ^ the weather, Isn't he, John? Are they working yoU'too hard at .
SHAPE, young man,' or are you taking toO :much- advantage of the local amenities?"
• ' . • • ï -. • .-. ,..., •„-;../< Rory "Oh, no. Sir, as a matter of fact, we're-,working very hard at
the monrent, Sir« We're working up to an Exercise .; . " 1 • U. John wWhat . . . another ... ?" ^ rs
-.: .--..1 -V Ti * -\'"tt : • ' • '
Rory Tes, Sir. Tactical use of supersonic weapons d .their effects upon the medical services. Tou know, Uncle^tMs is\going to make quite a difference to the présent deployment of our medical groups probably even means redesigning someiof the unlts
. altogether." • v , •. .... . - .,..- •• . • ;>..•• . .- - jf . « "i* '
U. Dicky nRory < M you fellows from the NATO' Staff Sollege "imaze me. It shouldn 't be any harder to fit in with the* new weapons than it was to f i t in with the atonic weapons in our days.,"- . :
• - - • XfcSS1VL'
U, John "If my mmnory serves me right, Dicky, we had' an- Sxerolse at SHAPE about that time ... there's an- awful-lot of nonsense' ; ' talked at exercises, you know, " • 1V ^ . . J-'. • • ' .
s..,-'•. , • ••; • • <:• \i i"H t ;,' . -
U. Dicky "One good thing-csme out of itanyway, John. Ve earnesto the . r same conclusion in respect of the re-organiaatlonof:our medical units."- ,, ' > ; . .
U. John "And your father didn't take at all kindly to- 0ul~-feh0pping Up (to the old ones, either. I know. He called it the rape of his Rory) .:- Princess of Medical Units , the Field Ambulance, -Tt
Rory "Would you care to t i l l us about Itj General Johni*-»-I',should think it might be of some value to us n v v*v liiX',
U. John "Impudent young puppy .. . 'sti l l , still.- I auppose it-would V help. Have yon read anything about the subject'at all?"
Rory wTes .., I've been looking In SHAPE records;and" I read ths verbatim report of the British Director General'sstat ment of the problan. I must say he put it very clearly ana was justified by events. General Harris, wasn't it?" ' •
. ; . -. „-v.-y,. - .w-.^
U. John "Dicky - you remember - we helped to write £t. Well,-there was the problem, as you have read." ,.f..^ :
Rory - "What happened*1, Sir?"
U. Dicky "We tackled the problem just before the outbreak of the Atomic War, and obviously we looked first of all at the forward units -in the Division. The old Field Ambulance was half collecting
. and half a low-grade treatment set up, the whole thing being an, . evacuation unit, whilst: the Field Dressing Station's»normal role
was that of caring for light sick. They had' to go and we sub-stituted two new medical units, each with a distinct and separ-ate role, giving equal or better services t Hhey also/saved a1
considerable amount of manpower which was «Utilized elsewhere In
135 -V.,;.. .
NATO CONFIDENTIAL r-V
tY-"'. >:
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
the Com Z and Bas«." . . < > i
U. John "And they were the units which you now know as the Medical Collecting Unit and the Medical Staging Unit." -
Rory "Welre they identical with the ones we use now?" •
U. John "Not quite. The Medical Collecting Unit, was commanded by a '.»"' Lt. Colonel and consisted of four companies* each of three,/¾¾t* sections. They had the job of collecting and transporting --casualties to the Medical Staging Unit."
Rory "How many to a Division?" •
U. Dicky "One, originally. It gained - approval around the Geneiral :, Staff because the job which was done before by three Lt'. Colonels could now bè done by ewe. The treatment facili-..:. - v
ties were better, too, if required." , . : . - . - - . . V • - ' d Rory "And the other unit?";
U. Dicky ttTheMedicalStagingUnit? .. . this was to be a unit conman- ; ded by a Lt. Colonel whose job it was to provide a high level of medical attention without the distraction of having to -look after the collection of patients from the forward areas j or their evacuation back." . 1
U. Dicky "There was again a Headquarters and four companies. Each coo-• . ^ pany was to be mobile and have a 100 casualty capacity.; It?was, ii
roughly equal to two of the old Field Dressing Stations in*, < strength, but double their normal capacity.- It could do all '.'•' the Advanced and Field Dressing Stations could do with a higher ..
-m .. ,-. level of treatment and with less, waste of effort-, It-alao ,?.--, t? . • » afforded a reasonable.Divisional Reserve*". -;r..-.
"I see, and how did you deploy them within the new Corps •'••"' organisation?". . . ,
"Well, as you know, Rory, there are thousands of musifcal 0* variations on any given thane. The first variations oh our y "New Look", went something like 'this: there wastobea Medical .; Collecting Unit.and one Medical Staging Unit with, each'Divi- " sion, and another Collecting Unit in the Corps area as'we v knew it . The consideration was that the sizeandohape of the \>. new units would permit variations such as three collecting com« panies and one staging company, Ve had helicopter évacuation-.; fron Division to Army." r ' , '
"But what about this higher grade treatment; in the Anqy area? If you were flying casualties from Division to Army you would want something special around there, wouldn't you?" -v.
wAh .. that's where the third wNew Look" unit came Into oper-ation, the Evacuation Hospital. This was to be a unit which would not only carry the first class surgical treatment ele- w-i ment, but which was to be constructed in such a way as to be * able to move easily and readily where it was wanted either in ' conventional or atonie warfare. It was to be a unit 'consis-ting of a Headquarters and three other parts,"- Its' casualty capacity was -nominally 500, The second-part of 100: beds would be a surgical unit, including resuscitation, X-Ray and having
136
Rory
U, John
Rory »
U. Kcky
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

its own blood refrigeration van. It would be fUlly mobile; able to attach itself, of course, to companies :of ^MédicalÏ; H Staging Unit. The first part would be a small reception ele-ment. We found that* there was a genuine need for.-.this1 as re* ception was very poorly catered for In the old:Casualty Clearing Station. The third part was to be more or less the
• equivalentof the Medical- Staging Unit, of.. four, sections or - -^ii : 100 patient capacity self-contained companies'.".a r\ •
Roiy • "I'm beginning to see Just a dimmer of reasoning In.all this;- , General. Even to my dim witj? the beauty of theee new«units would betheir comparative interehang^abllity* ^ljaeaiLAhat you would pile up either collecting, staging or'tréatmerrt sections in strong otmkbers just where you wanted «thent^ Ih ''•-..• fact, you could cope with any heavy casualties occurring any- , where within the theatre.", .• . ,, .-. 1:- ••;:,-, '''Vr-. , . -, .- ' '-V- . .
t^-". \
U. John "As your late and distinguished grandparent would have.said, Rory, you have a highly developed capacity , for stressing,the obvious.." ^ . .. ' 'i-U
Rory "Hadn't he?" . , -
Ij-J1
U. John ttBy a strange coincidence, I happen to have the very rehart X want to illustrate the advantage of our proposed.units.' There is the distribution of new units froa Diviaion tOfBaae> showing-'
. the comparative manpower and the distritwtion .-ofcthe.,saving from the forward area. Tou will see we made a saving<lnthe division-of a Tjrpe Army - 11 equivalent Divisions, of-nearlyil$300^<'and ' about 700-300 at Base. We used our surplus manpower-mainly at Corps and ArnQr level where we wanted it, .and we increased our -J ; overall trained manpower.11 ..- --.-,..^12-^¾
Rory "Well, sir, that seems fair enough. May-I -go,-back£tocthe .1 Division, General? I'd like to see the deploymàhLt:of;yôur :
- new forward units." :. -', . . . - h W Ji .-,- , '-Vi •• -..-:-, •'^•^•^•/^ïèt.'SKéstSÇtj-*.'-:';. '-•'- ""V
U. Dicky "Fair enough, Rory. Now take the Division here^Wlthin the; boundary you have your three brigades, with artillery behind . ' t,. _ the reserve Brigade, the whole dispersed as -well at^cl^cum-1^, ¾1
stances penult. Let.us call the companies ;•of-thöiColleöting • -.' Unit A, .B, C and D. Now, A, B and-C were.ito bé^lcwat« with the Brigades, whilst D was in reserve in the Div Tpsi'aTea, to-
/ gether with HQ. This covers the collecting of àll^casualties :... in the Div Area whether it be a conventional orv-Atanleiinci-dent» - . ' - *
- , , . • '. ; . V V •••<. z-.:Ai î V - .->
NoW we bring the Staglrfg lfnlt into the picturei. -Ve will name the companies E, F, G änd H. E and F companies were/-allotted ,>< to the Dlv Tps Area to stage casualties and evacuatei.1by.heli- -copter. G was In the Div Admin Area.and H was located further
bade; G was open and taking care of local sldciandiwoundedj-.the. other closed and ready to handle any. «mergencyvineludinga move forward' or bade. The HQ we will site with G*Coy. Thdt., then, was a possible deployment of these units in the Division."
Rory "Did the counter penetration force have its own medical units?", <
U. Dicky-,"Of course. If it was of Divisional strength, it carried1a ">i Collecting and Staging Unit.- If only Independent -Brigade • ,- ; strength, then it had a company of the Colleeting Unit, and either - -I G or H Company , of the Div Staging Unit went:. forward-.and staged , J casualties," fc.v*
. . . . . 1 3 7 - ^ : , . . : . .
NATO CONFIDENTIAL . ' : ' V-."'.. . . ' .- ' ..•' . -VVV-'.:.:: : ¾
• :
-• ••- -v" V- " v - V •
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

U. John "There is another point which mads thsss units an attrac- , ' ; ' tive proposition. Apart fraa-these. Divisional-. Units 'there ' were similar units-ail' the wayback to base,and- of course1 ' they were completely interchangeable." - ... ::.
Rory "One thing nhich you haven't mentioned yet, Sir - what»about. : . your blood supply?" v'jCI. vy ; . > •
' * » ' ' 1I ' ' • - • , , • 1
U. John "Obtained" 'a pied'as it were. ' We intended to put'à taking ' VT-^. • section of a Transfuoion Company with each of the Rein- ,, : forcement Holding Units at Corps, Army and Ccm Z. This ; • - : ^ would step up supply, particularly if it was ;not possible to * • deliver from Base by normal methods." V.-O-.VÜ* • ;
Rory "I see. General, frcm all this could you possibly give me <a,, ;Vr. sunmary of the advantages of a proposal like this ... after all, it is so radical that I imagine it shook./the;old 'fogiesöfe Cl:}'
• in the Club to their foundations." (Figure grunts). "He is :-,..-alive."
U. John "Ton asked for a sunmary of advantages. First - thatvfull v^rà facilities for collection and treatment would be providsd at .. ' all levels in a balanced and fleodble form." • '• . .u'.r*'.
U. Dicky "Second, that the composition-of the forward units;-being: ^ -self-contained canpaniea ofroughly equivalent.strength and, - .
. now used in all areas, gives you advantages in maintenance, ;. • "" 1 provision arid interchangeability." • ' <. ••'" r •" ' • -
U. John "Third, and that you have a fully mobile surgical hospital, v of first quality and capacity of 500and you can-graft on other staging companies as necessary and build up a medical task * •'•'>"• force -with great speed." ' - - -
U. Dicky "Fourth, that you have a higher potential "patient capacity,' pins a hitler professional standard, available at ths place and time that you require it," --:¾ -\£*V- Y tM
. J • . ' • ' - - . .
:--.-,:7 ••
Rory - "Tour last point in particular would strongly appeal-to my. Chief, Sir, Admiral Evan C. Stone, Jr. Veil .. tharik you so much for a most enlightening and instructive session» .
,- I t b e e n a great help to mev" - ^ i • -: - .,.-,1
U. John "Fifth, econcny in medical manpower and equipment.
>.i
Rory "There's one thing .. . Gwieral John .. . Ifttat you have been describing to me .. what you have shown now..."that was only' .'•'•'
• what you proposed as a result of seme-exercise «•< other*. • What really happened. Did it get through?" ; = *-.- ;.'-'• ' v-.
U. John "Well, as we all realize, getting propositions turned into downright facts takes many committees, many hours „;"days .. /, •months .„" ' " ' ' • • ' . > •-.•- • - - - . ..':/-,.'.,-.;
Roiy "Not at SHAPE, sir." , ' '
U. John "In fact, the whole thing was still on paper as à result of a body of opinion which felt that the. scheme should be tried : " • v out when the next minor emergency occurred .. and it' did."
U. Slcky "ïou could hardly call it a-minor emergency, 20 hydrogen and 150 atomic missiles from Brussels to Winnipeg in the -
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

j. ;
first 72 hours were very conducive to quick thinking and before you could say "radio-active isotope? FieldrAmbulance commandera found themselves canmanding Medical Collecting Units, and there was a lot of coming and going,until they grasped that the old war with Germany finished iin,1945»,t
U. John nThe interesting thing is that the new organization>• no matter how hastily it was put into operation, worked Very
, . well indeed. Of course, it was modified slightly during ; , • the six week period of the atomic war,butitbecamemore or less the organizationwhich you k^wtc-day..-.«*.".,'*
' „ "i'v-* s* - £ "iiij'i.tj.r
U. Dicky tt and which apparently you: are now considerinig*relé- V 'gating to the limbo of half-forgotten things.*1; j- -,1-- v 1 •
Î . • . • • • •<• • t' V.;. -.:
Roiy ttTell me, sir ... did any particular shags occur other'than , ..-.- those resulting'upon complete changes intypesof-units?" ' . ' ''TV--VV S -.-i -'r-tO;. •.;• . - V 1 V J U. Dicky "Well, yes. One or two lessons were forcibly.driven home. I . We had to exercise the most rigid economy in both medical i ' manpower and materiel . . . not so much Intheirv supply,;-but -I - - in their use, Weunderestimated air own casualties-inVsupp-; lies and men. This meant that we had to reducewa stage to /J
a minimum, a n d actual p e n a l t i e s . . . severe ones ,, . were j - i m p o s e d f o r offences in connection w i t h t h e misuse or.waste
...,. of m e d i c a l H a t e r i a l S o w . - » • . : • • • • - j - y . . - g u ,.- -,-^/- •
Rory "Allowing for the losses owing to enemy action, was the supply rate of materials equal to consumption?", , 1'-''
U. Dicky "No, it was- too,low. That was the second l.«seon» aWe,had to > ' step up supplies immediately, and the items most affected - •'
. were supplies of blood and transfusion fluide,antibiotics, j .and idiat our distinguished America friends, describe;as ' 'surgical-textiles'," ^
. - - ' - : - . - : : . - .: • • ..-J:"-' v<: ;!V;: Rory "And how did the new units get on in the forward. areas?"
U. John "I must say that the decision to use interchangeable .com- . -panies was justified up to the hilt. But tell-us about your
-v. Division, Dicky.*1 ,. .- 1 _;,: "v .: Kfew^Vjtv*^ ' V -U. Dicky "I was AOS /»6th UK Div at the time, and John here was.my
DCHS, and we were right flank division of-,the UK- 2nd .Corps. On my right was 3 Corps separated frcct us.fcy. aigap^ofabout . -.,<
.. 10 miles. The idea was- that this gap, Iikepthers^befcween - ' j ,: the Corps, would show an area of possible penetration^ and > Concentration, and thus ôffer a iworthwhile targetfor-rlarger . j - , atonic missiles. The action I am describing began and; eoded i
in a day and a half. " , . " : •-i.-:-VV , :,v ; . "The set up in my division was more or lees as you-, see- it on f
the ground plan. . A, B and C Collecting, Coys 'were .with- their Brigades, whilst D Coy was with the HQ near the Dlv axis. »
. That eovered the gun area and fomed Aar colleoting reserve for the Brigades, Mlthln the Brigades,the companies weTe in three sections,, the first two forming-a Casualty Collecting
.: Post .for the two forward, battalions, the third section and Coy HQ with the reserve battalions." • -
' ' ', 1 • \ ' î wThe Staging Unit's, companies formed Dressing Stations in this way, E and F Coys were at the rear of the Div Tps area, "'
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
^ ... north and south of the DIT axis, supporting the forward -Brigades on each flank. C Coy was with HQ on the axis close to the DIT HQ, holding light sick. H was in a . / -safs location, I considered it to^be ay reserve to covër any emergency." ••••' • - •• ^----trr.
"I had, of course, a call on the Corps Collecting Unit and. V -
the Arny Staging Unit, if required.' The eneay began con-ventional Celling on IOA and IO -Bdes Just before dawn; . and the attack developed all along the: Corps-front. SeveriL / attempts at a river crossing were made at the same time, without success. At 1000 hours he began ground to ground ' atomic Shelling on a wide arc ranging fror106 Bde Ares .,1-. Just short of Dlv HQj and by 1400 hours the arc was-'about . o , ^ 5 miles In width." . ' .
"The direct attacks on the other Brigade fronts were'appar-ent Iy a diversion, as enemy armour and infantry began to . - . v form up opposite the gap between us andthe U3- Division on -K..
• «is right. This was apotted;<and a 20KT atomic-bomb wis dropped on their side of the river. Unfortunately;-i*ost. i of the armour was across with the equivalent of'two'Brigades , / / of Infantry. The armour came through'very fast„ following the arc of the shelling, and got through into the rear: Div • t -and Corps area, closely followed by their-infantry,, and it < was in this area that they were met by our counter penetration force." v.v' .-.,:. -.- . •••• 1 • . - -.: i ^ i - O i I
"This was an Annoured Division consisting of 2 Brigades^or -,.-.. Regiments, one Infantry and one Armoured. The Infantxy Brlg-V ade had k battalions , and the Armoured' had ''4' ^atwwred)battais ' .-V
1ions. The force formed into two battle » groups ,¾ each' o f2Inf and Z Arad Bns and counter attacked on each flank of. the en«y line of advance. This split the eneqy columns into small groups. There was some pretty severe dogfightlng, but by midday the v ' following day the situation was falrly well under oontrol.""
V -L- .v.,- . . . ^ j ; "My Probiens were two-folds
First, divisional problems as à result'of -the'Stomle^hemng,' '-<-and second, I had to look Ovfcrmy ah ou Idert,,'as itwerfei to keep an eye on the problems arising in the Corps area Miere the main action was taking place. In thedivlsion,' I lostvby.'V-c ^ shelling, B Collecting Coy and one Section of C Coy. 'F Coy of the Staging Unit was also lost, and before I could get G Coy away, both G Coy and HQ'were overrun by the advancingenaay. As you can Imagine, «casualties in the 106 tBde and the' Gun and Div Tps Area were-heavy, so I sent a section" of D -Coy to 106 . . Bde perimeter and replaced the section at-105: Bde siting this. to help clear the Div Tps area as well." :: r,rA '••«••••'• . * • . , • . , • i - • i . ' "At the ADS formed by E; Coy of the Staging Unit, t1\ilfeS were, not going too well; Air sorties for evacuation to. AriSy were .. not enough and serious surgical cases were pilinfc lip;-.:.*-1 there- / fore asked for and 'got two field surgical teanHr-and -a1 Field ' v ;•' Traherfusion Team which were flown in, and formed-'an advanced x surgical centre there. -By this time it- was/possibré/to add H :, Coy, ertlich was also flowh ihV and this took the more lightly '•'•' wounded. Tou must remanber thatfrontal attacks continued«! 104 and 105 Bdes throughout the day, and this made the holding: *
- problem much worse, so I asked hy Deputy DirectoV for one 100-
1tfi
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
bedded division of the Evacuation hospital to be Hxnot in. This was done and that gave sufficient decent accomodation at leastfor the post-operative cases, I was satisfied that -my two field . surgical teams, together with theflyiftg out of about 3% of the most serious casess wouldcope;withthe sur-gical problem. In the battle area, further backp things were a little better. The: Jtaad Div Collecting and: Staging Units \ copes quite well, : Indeed, their reeerve Staging Conpanywas>''' not in use, .They did .require extra collecting facilities, and
. got one ccmpany of the Corps Collecting Unit, The oounter-penetration battle took place preciselywhereit was planned, so there was no aedieal problaa."
Rory "Where did you get your blood for these surgical units?"
U. Dicky "The Advanced Surgical Centre got theirs from the-Tatdiig Section with the RHU here in the Div Admin^Area - The Evac-uatian Hospital got theirs from the Army RHU..-«-V
Rory "I should Imagine that you had a considerable number of burns cases from the shelled area there. : Did they, creatv any great problan?" - • .--., . - u -;YV:
U. Dicky "Well, the atomic shelling was quite dense inthe/arc of fire so that either the man was in a lethal area, or his bums were severe and complicated by secondary blast injury,: The numbers were greater than in the conventional div battles, I-. had known but not so great as to completely overwhelm the Dlv Medical '
, units. The difficulty was that: the caaualtiesv-aHs-occurredx in-a relatively short time, and hence there was the necessity of " stepping up the aircraft sorties, .and getting in theField4'.<-' Surgical' Team l and increasing holding capacity; but, of course,
. It is obvious that under -these conGitions oneycouldtnot exj&ot Johns Hopkins or St* Bartholomew1 Btandardstof'treataient'k
....... , .'• .' •'•"•'••".a-/:;.
Rory .:-=. "Then had you any aeriouo difficulties at allî^vv: '-¾-, ;:/-.-1-
U. Dicky "Yes, Indeed, With the loss ofthe subninitsj; particularly : in the Headqiarters of the Staging unit, i-had to-Mly; cn i^t ' -1 • medical supplies could be brought forward by airJfTa^the Advanced Medical Equipment Depbt. This wasn't enough.and I told my DEMS after, that it was time the Advanced. Medical Equipment Depot really advanced and organize&^ts 'own? fcir ' 11V delivery s y s t e m . • . . •'•>»• v V- - •--"And how would you say your new units stood up to what must have been shall we say, a rather stiff lnitied test?"
"Better than the old ones would have, -I thlnk -vWe had more medical losses In the Division than I experienced^before, and * we had more ccmbat casualties occurring in a Short, space of - V time within a prescribed area. In apite of Jhis, we had no great difficulty in replacing our medical losses, and the
casualties were given a higher level of treatment than the old organization could have produced." ' ( , - , . .:.-: , • ' --. . '• . , •• '• -. .1 • ..-'. -.-"• • "Well, thank you again, General, for your trouble: t/.. both of you. It has been most Instructive a damn,sight better V than most of our out-of-date text books. ...-.. " .j , : > . . , ;
"You'd better be careful what you say, Rory .«. Your father'1
wrote than. Still, I suppose we are a littler out of date now,"
I U ' ; -• • .
Rory
U, Dicky
Rory
U. John
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

BWTBt KOSLOFF . '."•=-
U. Dicky nHuIlo ... here's saneone who tookavery poor view of our - "New Look" .. . Kosloff .. he was the Fantasian Divisional Ccmmander opposite me at the time. Here/ Kosloff, meet, scmeone under 70 for a change .. Rory Richardson." v
Kosloff - "How do you do, young man
Rory
r .
Much too healthy, obviously;". v i • • . ' - . . . . . , . ' .
"The General has been telling me of your-service int the ' ^ .'•"< Atomic War, sir." .."'^.'ï.Jïhî-'-'.:'iViiO'
Kosloff "Not to speak of my discomfiture,' young man. These con-: . founded friends of yours were a little ahead of J»e in' their^^S ' planning, I 'm afraid. I anticipated that my attack on the - > •'-. V
. Division would demoralize the men because of their lnablllty-^' to ccpe with atomic casualties. It seems that whén I dropped "*, my bigger, bri($iter and better bombs ... welly yotf.'Wstre ready' for them. ••' '-.-,> :
Eiccuseplease ... Igoand read Churchill's Memoires1-'« the Atonic. War." - / (> ' "
•tHBBBBHBBBHHHBBBt HXK-HHB M M-tfrM-B-H K 4HBHHHBHBBB8BtflHHHHKBHHHHHB)<
The Fourth and final day of the Conference was opened by MaJor General Rrank-S-. Besson, Jr., US'Army, Assistant Chief of Staff/Logistics, .. SHAPE: . ' , • -J .'V .
General Besson referred to the great increase in medical " work-load that would begenerated by nuclear war; the great bloeSof \ . casualties occurring simultaneously, and the long periods of hospitali-zation to be expected In those Injured by nuclear weapons. »There would «* be requirements for increases in supplies, In facilities, and for equipment, such as helicopters. The present chilly f inancialc llmat e/ï-' v."-would make the .realization of these requirements a long and tedious , job. ' • . . - . • - ' . .-: ' <'• - . . ^ p * ! * ' -
- - , He thanked the Conferees, on behalf of SHAPE/for the time . and trouble they had put into the Conference, and assured 'thaa-Vthat y SHAPE was anxious and willing to assist in any possible way;* V '
: -<Bt K KH BKHHH BM B HHM B B-BBHH HHHHH 1
^ •..-,'
The Chairman, General Hall, then introduced Colonel Howard B. Nelson,. USAF (MSC), who presented a paper on "Medical Materiel -..--. V V .: Report, 1955", as follows*. -- V, , v
Gentlement • ;
-- '•/• '"^v*- • -'/_.
In ay presentation last year regarding current'national production capabilities of medical supplies for the NATO countries . . of Europe in the event of war, I advised there were only three coun- W tries which possessed sufficient production capabilities to meet their Internal requirements. and to continue with'their normal* export-ing patterns in warj there were two countries which had adequate pro-duction in seme, categories of supplies and inadequate; for others,. i n : addition, there were four countries which depend primarily upon-Imports for their medical materiel.
1 ½
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

To add to our knowledge regarding potential* medical-supply for NATO in war the Medical Branch of SHAPE during the past year sub-mitted to Subordinate Ccnmands an exclusively military supply questionn-aire called "The Medioal Materiel and Supply Status Report*1, also known asLOGISTICS REPDfiT NO. 57, A number of la^rtant facts-were brought to light regarding military medical supply capabilities. The countries »v>.v. which have accumulated the greater reserve of supplies were those which have superior production capabilities..' The countries with the leasts satisfactory reserves of supplies were those, which depend primarily upon imports. This would indicate that the current statu sof thesopply situ- • ation is almost' la direct proportion to a country's manufacturing capa-bilities. . . , , ,- -
Answers to the questionnaire also furnished information that/
no country has. accumulated supplies, required for the additional "needs of. caring for ABCaCasualties. . All estimated casualty rateé and suppliés to care for them/on the basis of World War II experienceasmodified-bythe Korean War. No country has reached the minimum days of'supply,'forwar,; as reccraoended by SHAPE. - - r ^ - '-;-». ------
Some countries have indicated, that they have:90-days-bf v'^-'''1; reserve for some items, but when their supply levels are compared to their own expected casualty rates, it is' quite obviousthat their usage rates are too' low for many important items. It l s therefore essential* ' that the countries who .indicate their preparedness as satisfactory should-again review their expected casualty rates and the amount of supplies ' -. Which would be necessary to take care of these casualties adequately« ' -In the .reviews made here in SHAPE, it would seem for some'cbuntriës the ;
supply personnel did not have the latest casualty estimates available tdr' than as calculated by their own services when- the supply status^repOrt^^V was prepared. - • •• •'•-:•"*' '••. r-, ^ ^ . *
• - ••• :..-.'s .ïsiS-tx - vi>->c'
The replies to the total national producticnvqii^iötthair*>df '> last year and military medical supply questionnaire of this, year-have furnished considerable information which will be the basia-'for/iiy-dis- - -cuseion here today, together with specific requests for discussions o f -topics of special interest to sane countries. .
. . . . • - . » « » -
We are especially concerned here in SHAPE with the-Uimited :"«•«<•-"'' progress that has been made in the accumulation of reserves of^Supplié^ ^ -in some countries, especially those countries which have little -or rio 1HrJ
manufacturing capacity« These countries will have maximum difficulty in obtaining their supplies, since they must depend upen MothertCOun T" tries for thai. " " '--. --:.< " . v . - . .-.-u
SHAPE is also concerned that no country has begun to revisé" --its supply levels so as to meet the threat of ABC warfare. -The NATO forces have atomic weapons, and SACEDR has announced publicly that these weapons form an integral part of his war plan . The Medical supply support now available for any country is not' sufficient to cöpe " -with the casualties which will result from the enemy's use of atemle weapons. - - - . - , . : '•-. '•'••
: I would like to go now frcm these generalisations 1Of thé '-' status of our problems, to discussing In detail seme of the -elements • which seriously handicap the adequate development of NATO medical supply preparedness. .--. -. ' -.-.-:..'.-'••>••-•
Many countries do not have their potential kqy supply personnel identified, so Uiat a peacetime training programme for all assignments,, can be developed. I think we are all agreed that- the next war, if there ' is one, will come without warning, and our - staffs, if -they are to do 'their jobs, must operate with utmost efficiency as if they had been working td- ' gether for many months. •'*.'-
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Many countries do not have medical supply catalogues; nor do they have an adequate Inventory system which identifies their supplies r«^ and keeps them properly reoorded. If the present accounting-systems of'i*r sane, countries are not modernized, supplies could be on hand'but .would-tU not be. promptly available because present records would notYindieate1» 4 -.-*'. where they were,- or how many were on hand./ Many countries have not;
. developed pertinent regulations and operating procedures which will- A? -,» provlde guidance for requisitioning, purchasing and other operations; which are.fundamental to the operation of supply. ,.'.•; :
, One of the most basic problems In the operation of: supply' is^-M depots. I have visited depots In most countries of NATO and I have:'; .7-¾ Y found that many are not properly located for efficient operation. Sagie ; are too remote and have long distances to railways,^higiways-andair-..v -.:,,-" ports. Many of these depots are inoperative in peacetime,- except- for"- . dead storage* These depots have very, small staffs even for peacetime ' --' operation. Stocks, as they are accumulated, are being stbred-*in every^'i^ location that can be found until every bit o^ space is used. The prob^i-l«a of getting these supplies out selectively will bemost '. dlf fldnlt*-K' . Obtaining supplies is, of course, important, but ability to distribute promptly must also be kept in mind. ^ •'• .- - .
Such buildings as barracks are being used, Where there are ' V -*, many>small rooms, small doors, inadequate:lighting, and with inadequate^*.^ areas for loading and unloading. Some of these depot sstore. import snt 'r -supplies and it will take days,-if not weeks, to furnish supplies r -Jv;"; from these storage points. It is possible to modify some of these U V ',TÎW buildings without great expense and such activity should be encouraged-and engaged in during this preparation period. For example> it?is ; visfyga, possible :to erect skids or chutes from other than the ground'floor »-vK.i. to.thft ground to provide for-a prompt aaptying of these small storage«*' -'• rooms. Heavy items which would be almost impossible to move should not be placed where their rentoval would constitute a serious problm. . . .
Sane of the depots are in areas where thère are only a few 7¾¾¾ - people In the near vicinity, very few of whan would: furnish suitable t ^ ^ personnel for the operation of the depot. : Most of the personnel mast ft/fr«. come from many miles away. Before reliance is placed upon such' pery sonnel, a test.should be made as to the dependency which can be^placed v-„ ' on the i personnel who must come considerable distances to Join "the or^T^^ ganization, * » - . - . î. . .--:-,. ".;:vv.i.: *
-. •>-•., • -.•• .,. :. • -Y:' VY- 1 ' -Y ' Y-YWiiîï:'
During the past year we have engaged in a .critical revi#* 6f "the practice of utilizing large central depots for the storage ïofrmêdi*-^* cri supplies. You have been told many times during this conference of the necessity ,for having supplies on hand In order to save as; many-lives as possible.^-It is believed that the centraV depot ayataa utili*edby •>* mary countries will not serve tills purpose. It is essentlalwthat Some v ' modifications be developed which will meet the ohallenge of a future war. , It is my opinion that the central depot will not be able to fur- fi-nish supplies promptly enough in (a5-future war, but if'large enough|>wUTYA-furnish a worthwhile target for the enemy's atomic or thermonuclear'bombs This is especially true of those depots located in larger depot areas where there are other supplies such as ordnance, signal, QK, etc, stores, as well as medical. It becomes imperative that these, supplies be1 dis-persed as closely to the points where they are to be required as is« xi'^i humanly possible. Depots should retain only backup supplies, and should'-* not retain supplies which must be distributed if your medical support ~ Is to function during the early period of a war. : 4," v V'v*'- v-
I believe that hospitals Should have on hand.a much IargSr ' : w- '-supply of life-saving and life-preserving materials than they have ever had in the past. With the expected casualty rates of a future war, it is '
I U \* '
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
believed that sufficient ABC medical supplies should be on hand of f such items-as antibiotics, sulfas, blood giving and taking equipment, burn treatment, and so forth. We believe that these supplies should be safeguarded by storing in the safest possible places. Such units as airfields should choose perimeter points for supply storage which will be located in three, four and more places, to serve the expected routes for evacuation of wounded. , This will also mset the challenge of not having all our eggs in one basket, and will conserve supplies by having them dispersed over such a large area, so that even if a portion of these are destroyed,, a significant part will still remain. We are convinced that the nature of the next war will not peralt supplies to arrive at a base frcm the Central Depot in tine to prevent the needless loss of life. We believe that the supplies must be on hand, promptly available, within the first day.
, In "order to prove this point, your supply personnel should calculate- how may truces and railway cars would be needed to get sufficient supplies to the locations where they will be needed. They should' also include factors such as disruption of transportation, as well as destruction of part or all of some depots. When they have considered-all of the problems in a realistic manner, I believe they will agroe that some-modifications of present practicss must be made such as pardmeter vbase .supply on the* outer edge of military Installa-tions in safer. Iocationsf and much larger levels of supply In hospitals.
Another potential solution to this problem is requiring each man to be a mall depot. I know that it is difficult for the medical profession to decide to furnish items to individuals that the medical -profession can use-more economically and effectively. Nevertheless, the number of potential casualties are so great that some system of first-aid, is-absolutely essential. We must reach conclusions as to whether to give each military man supplies for the treatment of burns. We might have to give him atropine and other supplies which they can be trained to use. Wo.jnuat .face the prçblaii of requiring each man to be certified as having 'learned how to treat with accepted first-aid measures a burn of the trunk,; extremities, face epid hands. We will need some sort of motto, the, buddya1SyStemw, :or tTI will keep you alive and you keep me alive*n We know that Jjhis worked in the l û t war when many men, at the risk of their/owitlives, retrieved their comrades and brought them back to/whwe they. could; be treated promptly.
Saae countries have already reviewed what types of first-aid -supplies should be given to each man and the training he must have to use it-effectively. This is potentially wasteful of supplies, but there is no other equally satisfactory .answer to this problaa than to have supplies where they are needed—in the hands of those who are trained to use them as. well as possible. I am convinced that the depots which have the major part of supplies for a nation's military effort will never emptyHheir stores within a period of time that will handle the initial casualty , impact satisfactorily. We must provide alternative solutions and perimeter as well as Individual supply are two of the more obvious answers, .v ,,.,'
An automatic supply system was developed in the early stages ofyWorldïWar II by many countries. We know that it is also potentially wasteful, because some Items will be furnished which will not be required but I see no alternative to the automatic supply system being established again for the early days of the war. Automatic supply should be limited to items: which are absolutely vital for the major problems of the treat-ment of .burns, inflictions and the supply of fluids and blood .and should cease immediately when units advise they can requisition as needed.
• . . U5
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
• NATO CONFIDENTIAL ' • ' _ '
Planning.should take into consideration that many weeks . or months will elapse before replenishment of supplies can come-* ; - * from irvdustf-y. Mwiy countries will have to establish their procui^ Tt-fciii- ' ment operation for supplies, and this will take many weeks before it - * '«'-y- ::
operates satisfactorily. Tour supply staff should carefully plan: : - • ^v ^ how procurement will proceed and Industry should know beforehand how YY they will operate and what is estimated to the first • few months needsi .iftv If this is not don e y industry will be unprepared for military r equlre* WPb -Y ments, let alone civilian. VL:; i ' V
I have- reviewed the amount of time considered reasonable': t y 1 ^ ^ two countries from date of requisition to receipt of supplies.' -Thesej V countries have adequate production capabilities, a fully operating •••'<- -1V > " peacetime supply syste^,adequately trained staffs and ample transport'V\ 'v;i • tation. The average minimum time is 7 to 10 days under conditions ö fV^ * ' * peacetime. Now I can assure you that such à supply pipeline will have_. \ great difficulty to operate In less time during war. ; This again illus- ,.•/' trates the necessity for a promptl distribution of supplies fran' t h e ' v V-central depot activity. A point I want to make at this Juncture is V V \ ' • that a pipeline requires a lot of supplies before th e person who had . requisitioned on the receiving end will receive supplies.' > • • ' -;••:••• >••</ h <r- \ : Y ' . •-:,••• .--,-...-.,-, : -1 .-.:•_--,Jî -^---¾¾^^ •.-.-• ' , Y
- Those-countries which do not; have a fully acftiVfit^peaceiVV^Vv - .1 . ' time medical service are at a considerable disadvantage *NMR mob&li--*- VV:.-.-- " T zation takes place. Those countries with a peacetime supply activity^-*;? . • hive all the -.essential operations in being with supplies flowing ^ - V , ~ through the pipeline.-. This pipeline has a large quantity of supplies :/j'V in it. Those countries whichoperate only In wartime must calculate V'^iV " Y how many supplies will be needed in the pipeline and this facto* müst^*'^ ,-"* be added to your reserve levels to ensure-they do represeht--days: of^re^4^C - ' • serve that-are completely-useable. - - ! î,- > i— - '-: - -- --. ' v'i
, - • . , ' , .-..-. '4 --. : •• - Jt' -B1 : - ; : - ' " ' *3 - - • 1 - - - - 1 - - - ; - V - - 1- . r " . ' - 1Jl ^Tl • > • , ••,
. - Additional problems which should receive your-, e a r l y *att • : ' '-'.f tion are: sqae of the reported discrepancies which yoù are^ihcluding ^^ftati, -f. -1 ., • V r in yöur supply returns, I rsfer to the fact that some cotintrles^re-^^^^ ,:y . ...,- .,: port they have most of their reserve supplies retained atv their h o m e - M base. Again, I think it wise to consider the logistics of -this prO » . ' • | gramme, and to reach conclusions as to how much-of the 'reserves' c a n ; ' > be brought forward to the point where they will be needed immediately.V1 v> ; , . ! Even with such supplies as antibiotics which do not have great weight' > • y ' ) V j or bulk, it may be found that air shipment priority will not; p S n n i t ^ ^ ^ r V 4 air shipment during the first few days.* Saite countries indicate that '>-..--.'• - , ' they will procure their supplies from another country during wartime* , - j
. ; • . '< 'V-r --. . . , J
I would, suggest that Where these plans arebeing considered/ 7 [ that they determine whether the country upon which they
are dependent -y*.*• . _. , will accept such responsibility. Of course, this also-appllestcrthei^V-;
dependency upon other countries' facilities, such as hospitals and •*•' »v ^ depot stocks. ' \ • •-••' ^ • • *
Some countries have reported that they do not have varibus • a^V' ' • T types of supplies in their reserve stocks at all becausethèy will1 ^ Y' * , j be able to obtain them frcm industry as needed. This may bE -ROSsibley"^ • but it is wise to review what Industry has normally on hand and their . f capabilities to meet
emergency demands and in the quantities which . 4 . •'• ) have been planned. I spent three years reviewing the production;caï^^-H'1 - '. • bllities of the O.S., and found that industry was quite incapable o f * . meeting aiiergency demands on short notice which civil defence and the ' v military expected to place upon -them; There are many ' it ems especially - : blologicals, irtiich are produced oh a seasonal bails andJ industry stocks^ . - '> may be at the year's lowest levels, completely inadequate to meet-the ^;;71,':' requirements of the military as well as the civilian population'. * De-pendencies which are going to be placed upon another country; or in- - '"• dustry or any other elaaent should be thoroughly Investigated before . . . : the plans are considered to be finished. Furthermore, these plans - ' should be reviewed on an annual or seal-annual basis to make certain that changes have not occurred which would hazard this dependency. „ ,
146 -.'•' '' . V -
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

We have had a number or requests to discuss the problmn •*• of rotating perishable stocks within NATO. At the present timé^tf^jf^C^t* is impossible to review how NATO may cooperate in this progranme, since '-* ' there is no NATO medical stockpile of supplies. Since"all'tfedleal pr^' paredness is a national responsibility, it follows th at roiatioti^of 'i v stocks must be developed within the ctmntriesoWhaariufactti suppliers. The necessity for rotation of stocks "can be kejttötö^A-^s*^ minimum by the proper choice of supplies. An example is^the' 0röcuJ»e£®7 ment of penicillin in a dry powder form, propei%rpackaged» There is ' • • • considerable evidence'to Justly the use of properly :packaged*dry ' ' ^ penicillin no matter how long it has been stored; Other prodù'éts 'CSn » be purchased so that their storage will have a-maxlmim (Jfi sif e3dtbräfe8 "t^rf
life; There is also the problem that various côuntrlës*will Jia¥I J M^ / I * their stock items which would not be uaefulto ancrther c^tryj(fcta{<ir^i-f A fore this problan becomes one of primary responsibility of the countiy'n
concerned. It is hoped that manufacturers and suppliers''èC6 ell'%8* ** users such as civilian hospitals will cooperate with you in utilieing'•*•... your stocks while they are still within normal storage pèrlodJJiand to '.' *.-obtain replacements which are completely newandposs es S1 the aASJAmi 'j<' of storage potentialities, ' iVasJ tv.ir:; yjîv
There is one additional comment I would'like to make. When *:/' • you have an adequate stockpile of supplies to handle your expected casualties for both military and civil def ence'/ you ndst lrtSy t the^^ fact you cannot rotate your Stocks so asto ' prevent^fletertb^if^i-' The level of supplies will be much too large. HowéVerj^hé^ôst'bf'-. > replacing medical deteriorating items is a drop in'the bucket' com- -v ;-:-.-pared to the cost of replacing deteriorating anmmititm.'^rj"
- We have' discussed a' number of problems assè<&àtéi%itîHtheK;^ ? medical materiel situation and I have tried to- poixif bùtt-What^shbtoa^ w ^ be some, of your more immediate activities. I believe that'1 thei inuSt'*4* -" be a very prompt development in: each country of Yj
problm is so ithat stocks aan be obtained and where they will be required. I would also urgently reccmmend;'<that; ^ ^ those countries which do not have peacetime supply' eyfctenfs KWrt ireiyN^ v effoH to determine that their plans are* effeAiVey ,ffe^e^ ^ to ensure that key personnel continue to be dependably available,1
and that they be given frequent opportunities to become prof itffent*/-? •' •
SUMMARY ' '•''*• ' - -M ¢1¾ .'ifc
- It is believed that the following -are thé a ^ l ^ ^ ^ Ä b l i l f f i ^ receive your attention during the next year* - - , v tvu'-Jïifc ^ifyivAiaM* -.
a. Rwewed efforts to ensure usage rates take into consider-'. ' atlon latest casualty estimates, : — - V u o w •
•s • - • • • - : ; ., < I v<? lit« mu b. 'Review all logistics planning and in oMer 'to locateVV iii L.
supplies where needed. -- J- -Cw:.. arra.-si A
" c„ Modify dépoté where necessary to enhance: ability^iîô* frat^j''* nish supplies immediately. 1 .-.: ^ .:.- (: . -1... >l
d. Review dependencies such as storing réserves àth<® S1Vaife-J7-depending upon production of industry; depending upon another countries* ' facilities or supplies, to make Oertain that they do passr the test of dependability and, if not,-to make the changes necessaryî'SO- ttiat"-your medical, services will be able to provide adequàte -Medical Wippbït'.''*''-0flS7
' e . And, finally, ^ if we are to do bur' best 'ih vinjTil^ lives we can, we nnist make important basic changes in lOur'' supply's^ténÂV Supply procedures found to be so effective in the past do not meet the " challenge of a future war without many' Aindsmental revisions. W v i;
' 1 - ' , ' • V ' * '' •1 • 3" * • , yfl i" ii
1 ... -V .-,•' •• V ' , . -
NATO CONFIDENTIAL •->.
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
CffiMERAL HALL - . v . <
The Chairman, in continuing, on Oolonel Nelson's paper, said , . that the Medical Services, by keying abreast with current.plans for, V-;^'-tactical. deployment of forces in the field should be able to make sub-"!. 0 . stantial progress in fashioning the Aiture medical services to the needs , of nuclear warfare.. . -•.../•-.'i'V'îi 3¾^
Dispersal of supplies has become ivery important, ,as had.the-;,;v_ need for underground storage where'this was possible. General OrUerrther, had said that a future war might come quite suddenly thus forces actMSTLy in being on M Day—including, of course, medical materiel—would becc*ne>N all-Important. Nations would have to survive without re-supply,of men or materiel for many days or weeks., This was a matter that required,.the . most serious thought by all responsible for medical1 planning.r -V^fVKr^
• • • _ ' .. f • ' :i ,016¾
The Chairmai then said that reports from HQ ACLANT. and, from NATO Nations' Medical Services would follow. , .V "
^iv'ÏJ
4B8S- -JWBt ###
. PMSBHTATION BT SACLANT REFRES1MTATIVE AT -SHAPE l^C&vVv^;^ . -OONFBtENCE. PABISn FRANCE. 7 MAY 1955. BY CAPTAIN VAN. ,
v PEEMEN. MC USN . . . , .
General Hall;-Gsntlémenî ï / ; ^r ^
. ,:, This marks the third successive SHAPE Medical Conference to be attended by representatives of the Medical Affairs Section ofthe Staff of SACLANT. ,It is a pleasure to-be here, to convey the greetingsiV of the Supreme, Commander, and to briefly report again to you on the^ ^ ^ functions of our section. ""VrXvq''
, In my report to you I propose to teU you who we are,-what we "; are trying to do, how we are attempting to do it, and our planning ob- J. -/,. jective. V , / ' V • . ".. .
Because of his presence on this Continent and more particularly because of his presence in this impressive headquarters, and also bèoausé^ of his constantly-felt influence on his widespread forces, SACEUR i s ' tremely well known to you. It appears to 'us, howéver, that his sea-going counterpart, SACLANT, is not so familiar a figure and for that, reason. e. feel that a few words regarding SACLANT might be appropriate. ~ v
As a result of the North Atlantic Council Meeting at Brussels^ in December 1950, it was decided to appoint a Supreme Allied Conmander' ', Atlantic, to round out the military command structure of NATO. The > ' Atlantic Command, the first international ocean command in peacetime;, * j was establish in January 1952, with headquarters in Norfolk, Va. ^ f N Acbniral Iynde D. McCormick, U.S. Navy, was the first Allied Commander . - . Atlantic. He was relieved in April 1954 by Admiral Jerauld Wright, U.S. Navy, the present incumbent, who has as his deputy supreme v ' ccumander,. Vice Admiral J.F.~ Stevens (R.N.) ,, ...- . . . ^ - ;
As in the case of SACBUR, SACLANT IB directly .responsible- to . the Standing Group of the North Atlantic Treaty- Organization whose'/* headquarters, are in Washington. The staff of SACLANT is combined and j, a joint international one, and is composed of officers from the navies and air forces of «sevsn countries j namely, Canada, France,, the Nether- .. lands, Norway, Portugal, the United Kingdcm and, the United-States, y ,. ,.. ?r
: . - . •. ' ^8 • / ,v ••. • v ^ ¾ ^ .
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

The Headquarters of 3ACLANT are organized in seven divisions-which include Personnel and .Administration} Intelligence; ;•; Claris, Policy and OperatiOrtsj Logistics; CanmmicationsJ*Budget and Finance, and Public Information. Tha Medical Affairs Section is- a' * ' portion 6f the Logistics Division of SACLANT. / ; \ .
the primary task of SACLANT in wartime is to keep the IJorth Atlantic Sea Laneb open,vand to deny the use ofthanto.the en emy. ' Geographically j his area'dfoperations;extends from the.North Pole
. south of the Tropic .of Cancer, and from the shores; of the North American Continent Eastiard to the 100 fathom curve around the .British Isles and the European Continent. ; * ' ' r . , ^ 1 ¾
During times of peace, SACLANT has the responsibiii^ of V developing Defence Plans for his designated a rea ; for determining T'' force requirements to support those plans; and for the organization and. conduct of combined training; exercises both of jnajor .and minor natures; to advise the Standing CSroup and National Author it ies on^ T, J military questions within his orbit; and to provide an organization'' within the AGLANT area to serve as a nucleus for wartime expansion.
Organizationally, this has been done by appointment' of Area Commanders-in-Chief in the Western and Eastern-Atlantic,and by .the appointment of'Sub-Area Conmanders under than. In addi ton ttrere is provided a Comnander Striking Fleet Atlantic who heada .an operational offensive force rather than a geographical area and who Wensins directly subordinate to SACLANT, In general, the higher Coomand Posts are filled by officers having multiple appointments bothin NATO and in National Fbrces. This is technically known as the "Principle of Multiple Hats," , . ; ^ ^ ' ' ' /
Having'sketched very briefly the major activities ofJSACLANT I shall return to my theme for to-day; "A Report on Medical1Matters,"
The.Medical Affairs Section of SACLAKT'ls principally con-' , earned with logistic matters involving medical care of personnel, ^ . ' evacuation of casualties, preventive medicine, medical and dental supply,%and with the training of personnel in the medical aspects of ; ABC Warfare Defence. , , .- .. f ......./.- '
Medical planning procedures of any'International' staffvare similar, in most respects. SACLANT, ,however, unlike SACEDR, is ..ah , ' Ocean Comnand to which -no forcée1 aré^âesigned in peacetime,-butaréV'., only earmarked fer assignment in caseof-warand during ;'NATO Bbcervt. cistes. This fact, together with the composition'of his forces and the nature of his operations tend to create^ in the planning for logistic support, problans soniewhat dlfferent fron those of SA'CHJR. ., ,
" In,the field of Logistic Planning, we reCeive our guidance,', from SACLANT's Terms of Referencey and his Lojgistie Policy and , Planning Directive No. 1." This guidance states (1) it is SACLANT's f responsibility in peacetime to ensure that forces ! earmarked for his Coomand
are organised, equipped, trained and ready to Operate to—' gether to implement war plans. (2) SACLANT will inform.the Area Ctmnanders and the Nations of his strategic requirements .for Logis-'" tic support of his eamarked forces. .This^logistic;support includes . men, ships, aircraftP base facilities and reserve stocks—àïl to bé V available »dien and where required. (3) It is the responsibility of" each nation to develop detailed logistic requiranents for the support of its own forces and, in general, for the provision of such supports
The responsibility for coordination, however, rests with; '
149
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
SACLANT and his subordinate commanders. In the field of logistics, ."„ the ensuring of adequate' logistic support for operating forces is1; possible only if the commander has the same degree of. control and \ . ; V-authority over the Logistics Plans as he has over- operational plans. , In ACLAHT that is not the case. Apart fraa coordination of national efforts, an ACLANT commander when endeavouring to ensure logistic -readiness, can do no more than obtain information, evaluate and .v. present deficiencies to the appropriate authorities,
This means that SACLANT must have sufficient detailed y > : information from the nations' to determine that adequate logistic _ ' , ^ V ^ support is planned or ready to support his war plans. ' Likewise, ' " ' he must be aware of any Important deficiencies so that he can make . ' representations for their corrections. v-V. v/-. ;
' ' ' • « • . . ' 'H
The sources of information Include the report of the AnriuaT'' •'/'' ReviewTravel1Team, the Semi-Annual Materiel Status Report, and re- •• ports on the status of bilateral agreements. s ' ;;
An'example of the detailed information desired is seen' in 'i VV the case of Naval and Air, bases. Here we'desire to knowi . : -
- - - t ^ i f - j 1, The Location and the maximum force to be supported aV
that location at any one time. -%'..:•'' ,.v
- 2. The type of logistic support required by different . national elements at each base. V ; "
• ' • • . ' " " ' ' • ' ' • '
y. The method by which the nations have determined .that ..>.-logistics support for their own forces will be provided, and . ' " v
- • : ' . • - ' . - - . - • ' . ••
4. A statement of the current logistic support situation,
-Within this broad logistic concept the Medical Affairs Séc-; V-, tion is interested in such matters as:
• • ' v - ^ - , . , ; - ; ; ^ ' 1. The number Of hospital beds1 required, and when. _ ' •
2. The number of days of medical and dental supply required 1
for X number of personnel, and at what time phase, ' 1V '•*••• ' -V • ' - v* va ..- • -X-V-; '"'ni-J-
3. What will be provided, by the.user nation themselves.^d^g; what will be required fran host nations by means of bilateral -agree-1, X f'. ments.. . * ' .;. V"' ', '".• !.',
4. From the host nations, a description of;existing f a c i l i - ^ ties such as hospitals, infirmaries and dispensaries. Based on oper-' - a-atlonal deployment plans, a statement of requirements for themselves V-and for user nations. A report of planned additional facilttes,with the . , date of their readiness, and of plans for the development of additional' facilities. . . V ./"^V.
As was previously stated our information is secured by means, , of the Annual Review, the national Status'Reports and records of.bi- . lateral agreements, The 1954 Annual Review Travel Team was furnished'''; y • questions to be presented to the nations pertaining to. the-status of , ,-medical and dental personnel, medical materiel and the ABC training of , V overall forces earmarked for assignment to SACLANT. Since Insufficient;: information was received, the 1955 Travel Team, Whieh1Is now visiting !•.' the NATO Nations, has been furnished with revised questionnaires for use' in their discussions.
150 '
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
The present Medical Hateriel Statue Report ist'a.revised / concept of previous reports. Heretofore this report y requéstéd^tW-,^ status of material for forces earmarked for SACLANT'C" It^isjao*^ ent that the nations do not maintain.materiel forJ9AT0yfoi'ces^Tjpirttely-,/ and apart'from stocks for the rest of their for c ers'ï Tt-^pp éart' logièëlu i to assume that If all of a nations* naval f orc es ; could oe, su^Örted if or rJ a certain number of days under wartime coriditions*,'. t hen • «tHe'NÂTO fbrcédV , * of thatNation should also be supported for the same period;' ThS't bas lc 'i-v {gestion of this report is 2 how long could the NATO forces of eaCH^mtiwi.! be supported, under war conditions, with the stocks; available on; thé daté of the report, allowing for the tim^phased employment ' of|those>fôrîséS;^ ;*„,' during the first 90 days of an emergency? .The level;.reported liiitei?ms^of days support should reflect the overall situation: DeificiencièS wtiichi do1 not significantly affect the general supply status sho^d'not/refece thei;
number of days support Indicated. Previous reports have|"höt"iiidlcated-:any critical deficiencies in medical materiel. .. , *- ^ ; ; ' • u V - v
A review of our records shows that much too formation is being obtained through normal channelsiVWe^p^^söj^therei'^ fore, rto submit to the National Liaison Representatives and the;'Navai-Yv-. Hedical Representatives of the NATO Nations, copies of medical questionnaires which were glven_td:the^travÄ|tem that we can get on with our evaluations for trie Suprême OommanderV "' y J
In addition to this lack of detailed ^ 0 ^ 1 1 ¾ ¾ ¾ ¾ ¾ ^ ¾ is directed towards medical, planning problems cönnectwf with'nuorewr üaiv fare. Previous planning was, of necessity,
, based on past -experiencé. ... We think that this is a very sound procedure >dienvplaruring^OT^ôhvœHri>Y tionàl warfare, but we are now faced with a different probleal'v-Kedical 'V planners everywhere realise the.deetructivecapabilitiesröf^noelear^: weapons and visualise an enormous increase in casualtlSsi^However J^^r^^ until probable casualty rates were developed it was hôt^j^ssiÉà^jto^-^-^' begin an intelligent reappraisal of réquirrtents.^thi'é?i£^^^ taken special interest in thd work of the NATO Mb^^ l i f f i f e t tw^Mi^S nated by the NATO Council to deal,with, i n t e r n a t i o n a l * p V g resources. A starting point in the' developmentrôf à^iclpatei& ties was made by the studies of a SHAPE Committee of jAtciii^^etos** ^ last year. Their very realistic calculation of probable^cÄsualties;under varying combat conditions was presented by 'Captain. Cogginis lh Jils,splen- did paper delivered here in 1954.' It appears to us ;that tMs brkrwill'„ ? constitute important guidance for the logistic plarttër's of^tHW'ftrtweï V' Certainly it is time to begin t'o revise our medical tables.of.organi-ssation and allowance both for personnel.and m a t e r i e l ^ ^ ^ à V ^ - V
The project on which the NATO Medical Committee isiengaged is--a very large one, which we hope will eventually enable the,NATO .coun-tries to close the gaps in the field of planning fox adequate medical-resources in the event of war. We visualise that as/a. lmg^t^ :stùdy -and we believe therefore - that interim measures should-beyconiideredrto: . bring forces up to highest standards1 "of-readiness possible,with;:theV;; -V data and facilities now available. , , - ; r-. w.i, V..4--
Defence against .atonic attack requires deployment of-fo»rces over a wide area. It seems logical,, therefore, to apply/'this samesf principle of dispersal to medical facilities. In'the^fiejlditodiUt1^^:;^ advance bases within the ACLANT.theatre we feel that imerWsvSi^ill:? ? ' 7 units instead of large hospital units should be used. •• Thsseismallerk- V medical units should be established on chassis of; sufficient-false--toV permit multifold expansion if and when required.v' For^MpWbious .land-ings, the defence pattern will Undoubtedly ret^rt^idde^S^^^Msp'efrtriv of landing craft along a. beachhead and the positionlng of hospital VjV ships and hospital transports at à considerable distance tfrwavthev^ ,1,^ beaches. This will create additional transportation and cotmnunlcat ion a problems which need investigation and planning. , . W
•••••• ' - - • - •••. o.rV-VV -.: ...
. . 151 - v.. -NATO CONFIDENTIAL '• ! '
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Our concept of unconventional warfare at sea envisions extensive usé of lfobile Surgical Teams, In support of the Striking' y-Fleet quite possibly these Teams will be located among the,;vessels' ; .. £. y
' of the Underway Replenishment Group partially staffing those Vessels^ V under ordinary operating conditions but immédiat elyavailatole when"";^ ^ emergencies arise. Likewise, transports of the amphibious':force „yf-should, have, available surgical teams to support beachhead,operations^^ of that force, Othar surgical teams'should be ready among:for eeé '/;. " j fJg^ based ashore at advance base« for use anywhere, ashore or afloat,, as f \ emergencies require. These teams would, of course, be available^to augnent the medical staffs of hospital ships, patient evacuation 'ships j, transport' aircraft and ashore wherever and whenever need arises. ' Transportation of these teams' should be by means required and availabifc;^-whether by helicopter, othir aircraft, surface vessels or^toarlnéî^
In the field of medical supply, NATO directives estabiish/ the''4 1
ultimate target' for the peacetime buildup of war reserve stocks, to 90 ' vV days, based on national usage rates. The purpose of such stocks ie;to^.. ensure capacity for . sustained combat operations until wrartime proauctièrT:; and restipply can meet demands. We feel that a 90-day ' supply may be' ' ' >v adequate for those items normally in quantity production when increased"^" manufacturing capacity is readily apparent, There is, however, a group of items havliig a long production lead-time. Also the critical itmäs dé-"' manded by any kind of warfare, conventional or unconventional, including antibiotics, burn dressings, blood products and,plasma;expanders,,and^ ^y opiates which would be required in astronanical quantities. Certainly ^ '/ the 90 days reserve of such items would be entirely inadequàte regard-; :ry. less of ; wiether „they were based ori' normal or wartime usage rates., V
' ' We feel that these items should be set apart. Cognisance y should be taken of long production lead-time and stockpiling increased" accordingly, particularly for non-deteriorating Items, Forthose' items';', in which Consumption will be Influenced by the type of weapons emplôyed^ ;; revised percentage' requirenent factors should be applied.,- The SHAPK . ; Studies" of Probable Casualty Rates previously alluded to. shoülä ' be helpftil in developing these new requirement faotors, ';' '..;"'./"• Vl
V - . In closing, it is realized that we have not wen aentioriÂ^/^C Suchp important topics as standardization, transportation of câsualties^^^J
and proféssional training. "* ***
we Jiope5 however, that1 we have conveyed a broad-brush pic- V. turé of our overall situation, problems and objectives; " ' "" • ' •
'WNT'N K « K K K K * K K » K * * K K K K K K ) H I K K K K K K « .•"• ~ •" •• .- ... . . - . ; • •••.••• \ -. • •' • ^--v. v ' ••••'. - r ' ..- •
: '• • • i-?
REPORT OH PRQgtESS MADE BY THE BELGIAN MEDICAL SBEVICBS "•'••'".'••. SINÇE MAÏ, : , , . ¾ ¾
COLONEL MAGE, Belgiuma . W1
t • * l.r'« ' T „A' ''H1
We propose to review the main fields in which progress has been accomplished by the. Belgian Armed Forces Medical Services since the last 7 Medical Planning Conference held in May 1954. ..- • ' . " " "
I. LAND FORCES . ;
The most maHced progress has been made invorganizing the Medical Ser-; vices on a war footing. . , J/, ,r ^ :
- 152 " ' "'.'•'•' ''7'' :';'.
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
'Vy V'-' l '
a. Adaptation to ABC Tfarfare ' ' ' -, . V .-•« - - ;•< • ' Y ,., ' - . N_ - ,
Before all else, we began' to- adapt our organization \ ;J
to meet the requirements of ABC warfare« I have already spoken to you of those matters relating to the training of medical per^ sonnel and informed you of what has been achieved in perfecting -equipment. We shall therefore consider solely the adaptation of , , medical units and of stocks. • , - ^
i. Adaptation of Medical Units - v' V
The 750-bed Evacuation Hospitals that were con- ."" . ". \ > sidered cumbersome are to be conVerted and'split up into 2 semi-mobile 400-bed evacuatioh hospitalsi -The number of beds at reserve hospitals is. to be doubled. We are contemplating setting',à mobile ' reserve of medical personnel in1 the for® of 1Vlium "''>f;; ber of additional independent units for the support '., of troops in the Combat Zone, based on the" pattern of existing units Ï " *
Independent Sorting Companies - ".«v,.-, j .r.r.., v -: Independent Collecting Companies^ Independent Ambulance Companies '•" ' ' ' ^ - Y r v -Independent Medical Transit Caupfcnleet
- Anti-Shock Detachments V Y • V i W • ' ... ' ., > ..>-,;.. ; • A"''-••'
All the hospitals are equipped With" a* beds for burn cases; certain reserve hospitals" will - " be installing 60. " , -
. . - V 'ï:.!'.<-,
- • i i . Stocks ' •• • ~ : • --r <
Considerabls additional stocks of éq^ipmént'i^ ' V medicines are being built up for first aid tor'iïi*/ 2 main groups of casualties, i.e., burn and radiation cases; •••• •
. • . . • • - - . . --:- ' •• - 1 ' -. •' ' • .
1. Stretchers and blankets—quantities issued are.to. ' / be doubled and brought up to 10$ of total strength.
2. Burn Dressings. <
3* Isotonic salt solution, plasma and, plasma deriva-. tives (Dextran). • i
4. Antibiotics, morphine, vitamins, and. salt bicar-bonate pills. . . V ' : . .
Detection and protective equipment for atcmlc warfare has beeil developed. The same remarks apply to anti— baceteriologlcal and anti-ch«mical equipment. Part of this equipment will be issued to medical units in 1955*
• b. Medical Service Mobilisation Organisation •.
Vhereas at this time last year we had S,000 beds>" our'hos^ pital formations now have nearly 15¢000 beds, representing an increase of 7,000 in a.year, an increase of 5QJÉ higher,than-achieved l^ '^ear ; ' / Ih the near future we plan to increase the number of reserve hospitals within the national territory to 33. '
- . - 153 ••.•••• - : • ; • > - r ' I * 1
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Tbe extension of the Medical Sarrice outside the;national , territory is a necessity for th« Belgian Forces, Belgium.intends to . request the setting up outside.her own frontiers of a canpltoc of :„'„ hospitals comprising 32 reserve hospitals totalling 16,000-beds ï /ûv7 Nead Jtuie we shall begin issuing ful l -scale equipment"-.to our-nrtidi-. l f d cal reserve units. These units wil l be fu l ly fitted out^by 1956^/1¾'
. ... . •• ,•..;••.,..•. Ü-,--..--:, •• V''"'*';(»vjVSjt,.• ;
Among the equipment with which the Belgian Medical Unite; Lt icW;. are issued we report two important and new i t «ns? ambulances and-, --,:-7-^. ' tents designed by the Belgian Medical Service and produced.by Ger-- - v ^ / y •man fiims* -,.,/.:• /.>77, v-.
These ambulances can carry four patients lying, and two ;
seated, or ten seated, plus the aecompanyipfe medical orderly. They - V :7-contain a plasma cupboard, instruments and f i rst aid medical supp- / } . l ies and-there i s a device for holding a plasma container .fitted :-/7/^ ^ - ^ to the ceiling. Transfusions can thus be carried out while travel l ing. :/;/
A wide, high central aisle enables the accompanying medical orderly to give treatment to the stretcher cases* 1 . ' 'y"-:Vv
The tents have a light standard lateral metal framework without centre poles and can thus easily accommodate 20 cot casual- . t ies . They have a white linen lining and can be lined up end to ehd 7 - -v without using an-intersecting tent. Intersecting teats with standard) ,.¾^f. lateral metal framework and without centre-poles makes/it possible to , .; link up two tents lengthwise, or four tents in cross pattern, or may " / y be used as a transverse link between parallel tent-lines. These!tentsy: ;'-/ are light and can be-pitched and taken down quickly.' •• /-^.--^7- -W...:
c. Treatment of Burns Cases , , • ^ ' -,; "' 7/--
Amoftgthe outstanding points-of progress made this year/; . we should like - to draw attention to the headway made in-modernising , . ^ the treatment of burn cases, - v- Z-^vyiZn-
' , -, -.," . - . . ' . . - . . • ,, , -.. • : :'-, > :, /'v.Tv W 1, Instmctions have been issued to alls doctors .with-. .- -,- /4 -
a view to Standardizing f i r s t aid techniques - for,^tv 6 .. .s-, .., • burn cases. . , -..,- '<• -'y / - 0 ^ 7 . 1 ^ - ^
2. The organization of treatment centres for burn cases >'>••„;. in ths large military hospitals at Bruaéele and Ant- -7.,7--werp has been extended, ' •
3* A system of evacuation by air enables burn cases from .. the,most
remote units,'Including those in Germany, to7.7; be brought to these hospitals within roughly four 7 ' hours, even in the most di f f icult circumstances.
I I , AIR FORCE ; .' .r-h.".- . : 7 : ' - / r . ^ . y
Steady progress has also been made, In,the medical f ie ld in the .- 7 . Air Forceï
a, Aeroaedical trainingprogrannies for flying personnel-have-. \ been carried out in compliance with NATO Instructions (STANAG 31H) t ' : I -7.; talks on theory, practical demonstration, pressure chambers, films loaned by the USAF, evasion exercises, survival exercises in: snow and U-; A-;,. cold in. the Tyrol, trials and development 0 f new equipment > and--Specialv 1; 7to rations, - .. , . . - . -, .. • -.-^.--1:^. .--,- . : -.-1;.- ^tin-jx ÏM^-S^v
1 , • ^ . y -.. '.j ,' - -Zrio
b. Medical passive defence measures in the f ie ld of ABC war- " fare are already very far advanced in a l l Air Force units j stockpiling'
154 -.. 7 . / \ : • . . / '. • . .
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Ofreaervesf born kits, special bum-dressings, atropine ampoules - , stretchers, provision of premises for accommodating wounded Sndi s / ' burn cases within a range of 20 km around airfields and Air Forcé' ' vr<r bases, in-anticipation-of heavy1 casualties» -J -^V1;
c. A special survival:kit for the Belgian"Congo has been- ' ~' developed and tested which is well fitted to the cUmatlc conditions and geographic conditions of that region î it is an aluminum box . attached to the back- of the parachute and it contains medical supplies * • and food. Whatever the circumstance of the accident,'(baling-out,' *• ' forced landing)^ the airman always has this kit with him.' jtIn the plané- • ' he is seated on the kit, which lies on his parachute.
. d. A group of pscycho-sensitive testfl - foi~ the selection 1Of "7 ^ -pilot cadets has been tried out over- a period of four years Itcom-:*^" prises only tests that yield objectively measurable results d i r e c t l y - ^ related to flyings Reaction time, visual memory, stereoscopic vision,; -'• coordination of the four'limbs, concentration, etc. •
1 • - , - , - . • . . . . , - --.-. -h-Characters and personality teBts have beert discarded; this *
group of tests, which is ' far simpler than the USAF group, gives better results in tests on Belgians. ^ V 1 ' '
e. A biométrie study of. a l l flying personnel that hâve ----' served frcm 1945 up to 1954 has been made in order to determine the particular features that should be aimed at in designing the special '*• ' clothing of the diving suit type that will sdon be worn by^àilvflyingîfci.^ personnel. The conclusions frcst tests run on 2,400 Belgian airmen- d is-establish that the proportions of heights, weights, chest measure- 1
ments and leg lengths, are almost Identical to those of American^ British and Canadian airmen; there is a substantial disparity in the comparison with French flying personnel, despite the geographic praxi- •• oity. These conclusions have immediate practical'applications for" ; — tthe manufacture of different types o r special flying geàr ' andres— pecially with regard to the proportion of the different* S^edi geartr--In the Air Force (as in the Navy), the Hedioal Service operates only the first echelon^ the other echelons being operated by'the-Army Kedi-" cal Services . The operation of the Medical Services of operations'unit s of the Air Forces therefore^ in many circumstances, poses the-difficult. - ;
problai of cross-servicing. We take - the liberty of calling attention-to V the fact that the Belgian delegation already requested clarificatlon 'on this point, at the Conference held in June 1953. : - - : ; v • . i ; - V
f . Medical Evacuation by Air '. I • ' • r -
We should like to mention, in conclusion, the problaa of medical evacuation by air.
This problan took on ho particular urgency for the Belgian Medical Services until 1952 for two reasons? '
1. The base was on national territory aijd was very close to the Combat Zone.
2. The concept of ABC warfare was not rè&lly taken, into consideration until after 1953« y -
The constitution of a Belgian Base outside the national terri -tory and the vital necessity för-large-soale, rapid evacuation-of heavy :
casualties over long distances in the event of atomic "attack make i t essential 1Miat the concept of medical evacuation be reviewed. At present two types of units are being formed in the Belgian Medical Services with a view to providing the medical infrastructurenecessary for evacuation by airs - 1
155,
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
NATO CONFIDENTIAL ' . -. . .
a. A medical air evacuation squadron. is being set,up y i i d d n ^ f c the Air Force and i ^ already partially in being. . The medical and^nursing^ p ï s î L r ï o î S n v ^ g casualties has been-trained. The medical, squip- . * m S r S t h whlch^adrcraft are to be f i t t e r s ^ ^ ^ ^ ^ ^ ^ oSgen equipment, medical kits, etc.) Tents and hospital équipait for •. the holding unite will become available very shortly., ^ w - ^ t
b. Transit companies belonging to the.Aimy:Medical Seryice^^ m«r i f necessarybe called upon to constitute ,the initial ho ld ing -^é t f ^ , S s " t o S S t o their role of transportation of casualties f r a s ^ ^ hospitals to airfields. . - . • ^ ' ^ r ^
The infrastructure on the ground bring thus ^ ^ ¾ ¾ ¾ ^ like to know the medical air evacuation' p r ^ r ^ l w m e d ^ S H ^ fo* the use of the air transport fleet that SACEUR might i ^ e . a v U l a b l e ^ t o . ^ î £ mescal service« who have made the ^ t r i b u ^
medical infrastructure. We hope most earnestly that, SHAPE { ^ u w :. i U pSlcy on a q u e s t s that is of ertreme importance . t o ^ ^ , '
the Belgian Medical Service. . ,. , ?
: ^ ' * # * #** *** *** ****** *** ***";*****».. .'./V: Sills'"
RAMADIAM MEDTfiAT. PREPAREDNESS V-•
FORJttR' ' ,- r. \ '" .-:- f iV is-i '."'; _• ' -.-. - v ;
m. McFARLANE. Osnadai- - - - • -.'•. J
M O T M , . ' ^ •; -z/SÊMi ' It may be said that from the standpoint of the.teedio^ s e i ^ ^ w s
Vlces n Canada is making some progress towards the n e c e s s i t i e s ^ * * , ^ - .¾¾¾ future w T Trained personnel aSd equipment are W d i a t e l y availatte^ ^
- to mee^the., requirements of the overseas ^ ^ ^ ^ ^ ^ ^ to Hutmlv ln the early stages of a war..; Thls is a-great..Improvmenti- ^ ^ t^ î î Â s ë u a î Â c h . e î i s t e d ^ i n Canada in ^ ^ Ä S l preparedness is sufficiently satisfactory to meet aw&r which starts with a reasonable period of warning,,1s f ou^t w i t h , j / .
weaoons and which leaves the resources of , the homeland, urKtfö-t S Ä t S ? m S o r n o t l t is sufficient to;meet the d«ands^gavwar of the ^ture willedepend upon the nature of th^ war. - T h e j ^ ^ y ^ ^ î L t i t is not suf f i e l e t , is causing considerable ttjgga..ot , medical planners and a good deal of study is being devoted to finding . -means OflImproving the situation. ,. , /
MANPOWER 11 . /
Canada depends upon volunteers; to meet the manpower require- - . s Bients of theamed forces. Whether this situation « m l * be c h a n g e d , ^ :-. the event of a general mobilisation is a political decision the results _ ofwhi ch cannot be forecast. Meanwhile, under circumstances of volirn-t L £ enlistment and during a period of , economic p r o s p e r i t y Wgh -c ivLian employment the number of men required by the ax^ed forces have, • been>«sonably well met. (A rapid expansion o f the armed f o r e « j n . .,, peacetime would probably cause mbarrassment from the point of view of , meeting the Increased demands for manpower. Any worsening orthe , . - - , economic and «ploymmt situation in the, country.ava ^ o l ^ w o u U v ^ , doubtless be reflected in increased enlistments in.the armed
The forces are planning on meeting-their manpower>Te«p^^^^i;sft mentsion mobilisation by calling on their reserves. Many individuals., ,
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
in the reserves are involved in medical teachings the medical organization for civil defence or other key positions in civilian l i f e . : It is feared that the calling up of these individuals mi it seriously disrupt the civilian medical situation and in-the long run, reflect adversely on the war effort. A. study is noir under , way to determine to what degree the mobilisation requirements of the forces can be met from the resjrves without serious disruption of the civilian medical economy. - The results of this study may require seme degree of reorganization In the reserves.., , < .,-:.,.77-.
A plan has bam developed for an organization which wi l l control the allocation of medical and related personnel to the forces.' It is considered that this plan is capable of operation either under ., the circumstances of voluntary enlistment or ofrselective;serviöei7 . y :-.-7,-.
. It is hoped that this organization will be able to safeguard the mèdi- \ cal interests of the forces, of civil defence, and of Canadian industry. ,r.
• ' 7 ' ' " V • . > ~ .'. ' 1 V -
1 'V-ii, ' i.v' j '
r'- r'r:*
The peacetime requirements of the armed* fore és~ for mediMa^v ^ -," officers'have now been pretty well met. This MeftUr^jpftgely tliétlMainséess : of a program»-of subsidization of- selected medical 3tudènta,-in return ., for which the young doctor serves as a medical officer, for! a.stipulated . i number of years. It is anticipated that dontinuation of tMe plan .will ' meet any future daaands' of the forces in peacetime. 7 . :
The.rate'of enlistment of.nurses has not been able to keep ^ pace with wastage due to marriage and there is a considerable Aortage , 7 t of nurses in the forces. This causes seme embarrasment; in the-day.to7 ? day operation of the medical services. However, the net résuit is- the -. formation of a large reserve pool of rturses in the.country who could,, on mobilization, either re-enter the services or replace unmarried ;7:' v nurses in civilian hospitals for duty in the armed forces. -^.,.--
' CIVIL DEFBJCS - ' ' ' '..7 - 7-.: ,7../77^. * .'7 • 1 . t. • -.ri j. Civil Defence in Canada is not a primary responsibility of
the armed forces but of another department of the government. An „„-i., v organization for civil defence has been put on paper.and a. very con«-' siderable amount of useful training has been provided.' It can probably. -be said now that the/Skeleton of an effective civi l defence organization; i -exists. The problem is to place muscles on these bones. cThearned forces are committed to assist the civi l defence, organization as a temporary. ., : ; r-measure i f i t Is faced with a situation beyond.its own resources.; It- • ". is most probable that a demand for medical assistance will,be made on the • forces in the event of an attack on a major Canadian city, f The ,forces : are not organized or equipped to assume f u l l responsibility "for-medical care In major civilian disasters, and at the same time to play their jnrimary role of coning to grips with Uie en any. Some modification of. the' organization and training of the medical services of the reserves may . . make i t possible to improve the assistance which could be rendered to civil defence authorities. This question is being, studied. ...'••-
The medical services of the forces act as agents of the civi l défence authority in. the procurement and'storage of médical supplies 1
being stockpiled for civil défènee. These supplies are held in medical r equipment depots of the armed forces to be issued at the revest of civi l defence. The perishable Items of the total stockpile are(üsed by various goverrment departments and replaced as used. Thus, wastage due to out "dating is kept, to a minimum.
In view of the possibility of attack on major Canadian cities the location of many of these deports is felt to be unsatisfactory. A programne of relocation of depots has now begun and should be complete • in about fair years, - ' ^ .
157
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Medical equipment has been1 accumulated in sufficiéiht ' > quantity to meet the early stages of a conventional war. * Ejdstihggapa/ 7 in the stockpile are rapidly being f i l l ed in. I t is felt',thatrthe in- <^|tf dustrial potential of Canada, i f le f t undisturbed, is capable of 3 . / . meeting the demands of the armed forces at war before the stockpile À^'J:/-. has been exhausted. The programme of stockpiling jointly with civil,. defence authorities has been mentioned above. ' ^ j ! ;
, . '. • . ''vVV'tlJ .f'
TRAINING . ' • • • • • . " • • ' • 11^ ½
Training of the medical services along the lines of cœvéïw/^"^^. tional warfare has proceeded satisfactorily* It is realized-that the'/*-/' probIans of newer weapons have created a requirement for 'modification^ . ,; ' in training programmes. At a recent tactical exercise the.medical ser^ f Ci - . Tice of the Army considered the problems created by the UseiOf atomic . • ; v < :
weapons in the f ie ld and also the problems of assistance to'civilian ; "V * defence when a large Canadian city is attacked with an àtadc.weaponi'v^v»; As a result of this, exercise suggestions for the solution of 'a ;feW^ of-, the problems have been forthccming and scme other problemshavé'beén^^^/;*-placed-in reasonable perspective. It is obvious that a "great.' deal^of k
study remains to be done before a satisfactory solution can be found,- ? ', • --Meanwhilec ramberous courses in the medical aspects of special weapons ^y have been conducted and a l l medical officers off the forces have re-, . ceived instruction. A good deal of information of this"sort, has been"". V f-'' disseminated1 to the civilian medical profession.
RESEARCH : '
Defence research, in Canada, including many aspects, of medical -research for defence purposes, i s carried out' by the Defence Research a./ Board, Some of it i s conducted in laboratories opened by the Board,~butÄf,*;
-the greater part is carried out by a programme of support to the univer- - ' s lt les, Investigations cover a wide f ie ld , including Infection and ,„. . .-. • ionrunity, treatment of bums and wounds, aviation mediolne,and:problaasA7^t relating to blood transfusion. Because of its importance, larger'grahts^l^' have been made in connection with investigations into pröblms öf.'.rédli^*;*^ tien protection and treatment, A spécial unit for this purpose has been " established.in one Canadian University, and increased grants have;also;Vr" ,•_."•-been made to workers in this f ie ld in other Canadian universities; . Prb^/*y bably on account of its geographical position Canada is expected- by hér^^fc, friends to be particularly well informed on quaatlomsof Proteiitiorii fJi - J0I against cold and the treatment of injury by cold, Qrants for reseArcn / , in this f ield have been extended and a new unit for i t s investigation ; ' TCV; has been established in connection with one.of the Canadian universities
CONCLUSION . '
Planning for war, even by thosewho have the ultimate responsi-b i l i ty for the tactics of defence and offence must be based^firat on the experiences of the past, then the day to day development"ofnew methods and thé limited experience of teats and exercises afforded lIn" "'" . ; ;; peace time training, and finally on an attempt to foresee .the. effects. the nations Involved of such new developments in a f ü l l scale war. vThé,^ ^ V medical planners, the men who are responsible in time o i f f o r 'tM^ g ^ .-'-maintmance of the health of nations' and the treatment' of ' l l l and "ite-V^yf.*;' juredj face particular diff iculties when they try to foresae the 'ccÉçl « , . problems which may face them in a global war. The work of civilian doc-. •> tors and service doctors undoubtedly wi l l need to be closely intégrated, 7 and i t wi l l be unlikely that such sharp lines as in the past will- be .'drawn between the work and obligations, of the doctors and'nurses of the three ; services,- "''.,'.'"'.""
156 1 . • NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
The Canadian.Forces Medical Council, of whichBrigadier Hunter has told you something at the last conference, has been , established ! » Canada in an effort tc integrate as effectively as possible in peacetime the health services of her army, navy-and air force* Seme progress has been made towards that end and aV least a foundation has been laid for dealing with the highly, complex problan which will-face the nation in the event of an all-out etrugfcle. Ko nation, particularly one such as Canada, will be able to afford the ; luxury of prodigality in medical and nursing services.. 1N,There'is-no short-cut in the training of doctors and. nurses. Harsh'necessity will demand that those-available be used to the greatest advantage, : for both civilian and service needs, •• ••• r .
ADDRESS JOIHT Fi
BY THE D.D.M.SV. FORCES. KEMMABK
VV.r. j-'.
/-'..y*.: „ f c - - . - - . - , COLONEL J. HEMFEL-JitBGEMSEH
Mr. Chairman, Gentlemeni / . . V v , ^ ^ " • • •- • /.'if. •!..':. .. - ' .
, As regards Denmark we have procured in the financial-year . '. 1954-55* the following; V ^ i ; , , . , ; . . , , ' "
1. Bquipnent for a l l established unit s, (battalion -y, r egi- ( . -,¾ -ments,'etc) has been completed. "' ' '
Beyond this there have been bought sparestores 7Iarge ~ enough to r « w » the stocks for the unitsaSf reg ies , t dressings snd medicines three times. _ • . . . , . - . : , / . . V , ;
- ' . -. . : f ••• - : V • •. Vi- -••; ' V f f V ^ "/./• •:' .2. 600 cdntainers for buiw-treatoent, imitations-of ;:thevt :
Eritish with the following deviations: ^ ^
i . We have not the 50 portions of penicillin in the, - • -- container, because this-amount-of ^penicillin-is .
to be,found inthe knapsack of the orderly, -.-.. .-v .v.::.:.--v.Vv'- -
. . -\ ••-,;/- ii i l . The gloves are not compressed.
• •>• * '- :- v:»/, i l l . There are.no printed directions f o r / u s e . ^ _ , -
iv. The sulfa powder is not placed in the^gloves^but, in diminutivs sprinkling boxes.,. : - ^ ¾ ¾ . '
• tZ -. ' '-< -• ' • • / '/JjTii-L.
7 t. 3. Three field ambulances. U-U
. . • • • • - ! • • . • . -. r .i" - V • JU : •/:•• V:V A field ambulance includes! S-V ^Ï , . .
. . . . . . :•.«. -V-If1;.' 1. ; 2, treatment sections (a kind, of advanced dresslng, .
station)- ,. • ../.
i l , 1 collecting post for walking wounded. -.j> . Y -, •' • . - / / •:- • •••• ' - • .. . ,.- w e - - .:-.-.-,- •»•" -r-.-
I i i . , 3 aatoulance cars loading points (where.the.sorting-: - takes place—a kind of COP) ; . "-, . •
.'• J : - -- ' •. ,.-' ' .: ."-. •' • • '•"•>• -- ;< :,-v.;- i J MMiI--^!' I v . 2 field.transfusion teams of;which only-«ie will.be
appointed to the^field ambulance ; t h e other wil l be at the disposal of the AEM5.
159 ,
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Ut One reduced field ambulance for the Bornholm Island.
5i Two field lazarets (200 beds) (a kind of casualty ' clearing station). .
6. Two field lazarets (almost exclusively personnel) .in- - ^ tended for reinforcement of a field laiaret. j - '^P* rtaii^f
7 i One ambulance reserve, which includes Î '•'-• ' v v - i * : -. . -- - ,. -, -. -. • 'JV.-i -Vji." Tcfo-'-fiiy.itt-
i . Ctoe replacement platoon (stretchers with stret^ ö Akt«, -cher bearers) ' j ' •
' .••••• f-v^'^'-r; i i . One field infirmary (100 beds)(corps field - - ' 1. -"/ ; 1
dressing station).
• W ' i i i . Two blister gas ablution platoons.
' ' ' - , H -Il ^ t -1T iv. Tw6 field surgical teams. - --r
• ' . \ v : : - . . : ^^¾¾¾^ 8. Four independent surgical teams. . v N
ADDRESS BY DIRECTOR GENERAL« FRENCH MILITARY MEDICAL SEOTICBS
MAJOR GENERAL REILDJGMi . • ' ' ' V {* "' ' V
Mister Chaiiman, Gentlemen; ••'-.'" ' •/'''-. \
The French Medical Service is particularly concerned at the * ' - - . present time about a matter which affects the capital equipment pro- '
\grsnnes not only of our own country, but also of the other countries ^ - \ represented at this Conference. " '' ' - *•
'""Tftbaj today's meeting which'brings together represeintativesÀ' - y ; ^ of a l l the'NATO countries, seemed a propitious occasion for giving-you ' . a brief outline of this problem. It concerns the hospital infrastruc- " ' -ture plan. * -V ^ ' ' '
Upon mobilization, a l l the belligerents are to set up in the .'.. ; conmnicatiohs wne'a certain number of hospital units to-receive '. "-casualties who have been given primary « i r r e a l treatment in field V " units." As far as we are concerned, this complementary hospiial infra- ^ structurels organized on Uis basis of requisitioned establishment,^ such y ; as hotels, schools, and administrative buildings which are converted. ** V > v V into hospitals as soon as possible after the openihg^of hostilities 1 ' : . ; =.: We have had a l ist of suoh buildings for several years, and we p o s s e s s . ^ .'•'"• a comprehensive .catalogue of our real estate- resources.' These resources ' have been called upon heavily as plans have developed and now ,the question < arises as to how we can meet al l ' oUr future requirements with -thmn • 7-:.VV?-
•• •••' ' 1 •]••- / ' . - ^ 1 - , ' ' : . : '
I can te l l you immediately that it w i l l be very difficult , for us."; ; to meet our obligations, both national and NATO. -The fact is that,' where-» ' as in previous wars national hospittl infrastructure was designed s o l e l y : - . to meet military requirements, we must now plan for a very large number • of beds to be made available for civilian sich and wounded'. Tou are' a l l . ' ^ " represented on the NATO Medical Committee which is at present studying ; , '• the coordination-of civilian and military plans;'and therefore you h&ve V -an idea of the huge amount of resources that are needed In this field.;
160
NATO CONFIDENTIAL -V ' . " ' ' ' . .'V..1--
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
KAIO COflFIDEHTiAL *» • • s
•• • . r ~ '•/••
Iti our .country He have practically Toached the1Saturation ti;,;, .; point already and in some eases we have had to reaort to arbitration •• in determining the number of beds to be allocated to civiliansand? - ./ .,-, to military eases. This situation wil l become even more-critical.,.'; since, as you Jcnowi, SHAPE has recently reccsmtendsd that'ithe number of*; ..¾.-infrastructure beds be brought up to 16£ of Combat. Troop Strengthr^in • order to meet the number of anticipated atomic warfare, casualties.-^ But in addition to these national civilian and milltaryrequirements/% v, > some of the nations among us wil l be fighting near-wr -fKmtiorsv^iThe fact is that France's geographic position is such that her tSrr Itory r^ f /j -wi l l serve as the natural communications zone of a large proportion of'. - . -the Allied Amies operating in the Central European theatre'.. Moreover, some geographically small countries will have to extend .their logistic • System into our territory, due to the insufficient,depth afforded by. ; ' their own. <0 - r-:* ••'.«•. fr''
. - . , • ' . • """ '. >'••• f In view of these strategic necessities, vaçious^natlons, have.^ Vl
already asked us to set aside a certain number of^beds for them ;on »our,., i • territory« in areas selected on the basis Of respective. national>plans'/s:) f j
We may subsequently have to provide f o r similar .requirements r ' . on the part of the Gernan Armed Forces. Finally,. allow .me ,to -mention .¾ j merely in passing, that the medical problems caused- by-the»ifi^sible> »Vv mass influx of refugees into France wil l be tremendous. These doands ' . are a l l perfectly legitimate and our staffs are studying the«jLn*an > \ . earnest desire to satisfy them. It Is nonethelessa, fact. that-great ^ r difficulty is being.eotperienced owing to the great numbers^of . r e - , ^ i ^ o r quirements .and the fact that resources cannot be st re t ch ed< out j fo rever. • v -
There is thus a critical problem which can by coordination, at SHAPE level, : I thought i t neces8ary>to.i,telli jod*»;?^ of these difficulties, because they have a bearing, «a both,ouiyown ft:Ufc
plans and yours, . ... - • -.-,. t . .yj
Talking trm a strictly national viewpoint,, I can^say-.that'-^s^T^v. 1955 maries a crucial stage in our developnent. Now, in. fact.,v*«r:cari;,<,.-<.-look back and make a fttll assessment of each of our Oariier lPlansj •.-and look forward to laying the foundations of an organlsatiwi^eared to atomic., warf are, ' .-, ' -.....1. - . i r '
If we examine our past activities, based on SHAPE direCtivee^Vjr i t is clear that the plans required for the support of the Combat ' /• Forees assigned to SACEUS have been .fully implemented. >,Th« field medical-units have a l l been created and service and ccrabatunits.havebeer^iesued . with their medical equipment. This applies to a l l three Amed Services. These programmes were JLnanced by. the-national budget and,carried.out en-tirely by French industry. • - .,,.-.-.-i ,v. - , -
With regard to stocks,!'we have a.month's,supply in hand -for ths , Combat Forces, and funds granted this year wil l enable us to build ; up a further month's supply during the .coming year. . : v - :"'••••'• ~
Turning now to future prospects, 1955 i s for us ^ year of study and experiment, designed to adjust our organisation to the new strategy, which was on the agenda of the. last medical conference..^With . this goal in view, our High Comnand hass set up major;units .of new .types ,., that wil l be tested on a war footing during the caning yèèu'./^VejTiave. ',/< ' studied and broughtlnto being divisional medical support förV these.major, . units, units based on the-two requirements of atomic wa^fare^-mobility .. and .dispersion. Consequently, the two types of medical..battalion, Onef,.... : for the Infantry Division and the other for the Armoured Divisimir'llàve 'X ,
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
been lightened and the number of their component unit« increased ,/ -V':' V to achieve greater operational f lex ib i l i ty . Our effort was to bear mainly on increasing the capabilities of our' collecting units^ f ^ -. with a view to speeding up as much as possible the evacuation -of ; eas^^®^--11 -ualties from the f ir ing line to the sorting units." Furthermore,"equip- f j ^ l :
ment has been developed for sorting and treating burn1 and 'radiation * • » ' *•<,* cases. Itorevoers we are playing an active part ccBihiittees set up to define the composition aartd organisation of t h e ^ 7 ¾ ..." Vj general reserve formations in support of combat forces of this , type. But X should like to make i t clear that we have^hot-got-bejjj^ -W/f™. OMtf X BUVIMU XUV VV IDH XU ViWM IMiav ». 6*» «B/vlW ' . f , .^^.; ^ the eaperiemental stagej that no conclusions can b> drawn - until - ' '^i careful study has been made of the lessons learned> and that for; ^ ¾ ¾ ¾ ^ 1 ^ . / * time being our mobilisation plans are s t i l l based on conventional : -warfare.
Uhat is more, this inevitable development of in the. light of the use of atomic weapons is ;
of a l l the NATO countries and we are very pleas Sd that the Medical Services in the. light o f t h e use of atomic weapons is a constant côrtciiiTi ' '
Branch of SHAPEl took the initiative in putting on the agenda a p r a^^ * - ' . ^ ^ '-r tical demonstration relating tà this Important Exercise Amernus5 which was remarkably well mounted our British friends, whom we should Uke to. congratulate — —
,cepts were a keen source of interest for us, and we shall be drawing: , .^¾¾¾^ useful information from them to help' us in our own SXperlAehtSiw -
•• FihallyV I should like to draw your -stfWfelflnr^lT^ périmants carried out by the French Air Force and Naval Msdieàl ^ V - -vices on problems concerning the survival of aircrews brtWftfc do>Ä ^ ^ over the sea or unfriendly territory. Some veryinte^fcttf*\<fo&'»r-vations have been gathered in a l l fields,, both on the quSStMhof nourishment and on protection from heat and cold. Kônethéieé's'i we V ..f <. , feel-that a new idea Should be given special attenUbn/-1 TttU ' V cents the possibility of subsistence for 5 or 6 days at*«eai on J of sea water-alone. I f s as the early results lead one to béU'évè, t h l s ^ ^ v " . - ' ',1' theory is definitely confirmed, the rescue of crews In distress wi l l b e ' V , ; -,, greatly simplified. ' • ' ' •' ; ' 'k
To oondude «y presentation, Gentlemen', i t is, - a - j w ^ i i j ü ^ ^ ^ v pleasure-for"me to thank the SHAPE Medical Branch and its c h i e ^ ^ V ^ ^ C .. " "T General HaUp for the r«markable organisation of the conference»-and ^ v ' -for the very -warn' welcome that we have been given , during our stay » t ^ ' l ^ ^ i ^' ^ A^?^^^
' ,,--. - #*#*•#*** *##» ***»- **•# ***» -OJ -1
.... . . ..,.. . -..-- - ,-,- v..;', " \ Vvj
- .- HEPOHT ON THE PROGRESS AND PBOBLBfe r- ^ ^ t ^ c ^ - "' Vf OF THE MEDICAL 3IRVICES OF THE .}
ITALIAN ARMED FORCES . _ ; V - . . - - , , , - J
S E w P a l . - V
Mister President, Honorable CoUeaguest ' . _ : ^ L ^
"I 8hall.haVe the pleasure of br ie f ly d e s c ^ l n é ^ ^ ^ ^ t h i ^ V ^ ^ - *": : 'V^j ! • a-' - t,iiijjl ft ^ . ' . , r i main poihts of progress achieved by the. Itiallan'Amed Forces' Médical^ ' , . ^ • h Services since my last remarks on this subjeet i t the Medical' Conferœcè^? 'y / , held in June 1953. .. . •
; As far as. territorial organization iô concernedthe Ariy.has.' ; : • ' been proceeding with the installation and improvanent of 28 miiitary horf- ' "
vpltals and 2 thermal springs establishments. .This has been . accomplished ' • S. '
Vl ^ 1 6 2 . • •. ' •-• • '•-•• V-.,, •
' • • ' . ,' . J NATO CONFIDENTIAL ' - V
1 ' 1 ^ ' ' * ' . *i.' -I* r •' . ' ' t*
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
by means of reconstruction and Isprovsmerit workssupply of up'to date technical and scientific devices, and modernizaticm of the medical and' 1
other kinds of equipment Ini the various departments. ; •• r '
We have also arranged for the creation of 3 new garrison 1 hospitals, provided with 150 beds each, at Trieste, Treviso and Alex-andria. -,.- - >• •••;• • - • f'' j-.!? ,v
... , . . •• .• 1 • ..• •.•..•. '-..•• .-.•.• - ....-. ; î v ^ n Zf. ' V:- J u.i"'vw-w
The Navy has improved their medical establishments,^ too,-with • ° particular stress upon their specialised examination departments, and ' has created at the Taranto Naval Hospital its f i r s t Audiometrie Centre provided with a soundproof room. . , » \ '•
Important progress was achieved in the blood transfusion ser—" . vice towards instilling into a l l military personnel the sense of duty
involved in offering to supply blood, and-extendJaigthe organisation, of 1
this service to a l l Italian-military areas. •-. -Kii^ -V' ' • -u
The Araty Blood Bank, locatsd at Florence, has been actively operating since October 1953* and besides using blood given bjr volun-. teer military donors in Tuscany, has started collecting blood also ^ Vt :
from neighbouring provinces, for example TfrIIia, and solving the complex problon of transporting blood over-long distances. The collected , blood is for the greater part utilized and stored In the form of. Iypphlllsed plasma. . I can state that the use of this plasma has so far nof-resul-ted in a single case of hepatitis or any other infeotlouB?-disease.'---- •
Two transfusion centres are being created In Sicily, in'coo- . peration with the civi l medical authorities^ one in Palermo, the other: in Catania, where blood collected from military personnel on the^ aland wi l l be concentrated. , - , ' • .•••: 1 ^¾^¾^1^.^1^
The blood storage rooms installed in the military, hospitals• ' s- " are being Improved, and the personnel assigned to this service-are developing technical knowledge and experience. ^ - ^ : .--
Following the proposalwe had made the Army BeneraT Staff " ' " has lately authorized us to extend the appeal for blood donors and -';/' blood collecting operations tooths various military schools- and com-pulsory-service training centres. The student officersöfvthe.'Medical Corps Sdiool at Florwice were the f i r s t to volunteer to'^glve bloodto".- ' Increase' the already considerable supplies of lyophllized plasma stored at the Milan, Turin and Borne military hospitals, as well- as at the blood bank In Florence. 1 • - . ;
The Navy has recently created, at its Taranto hospital, a blood storage room that wi l l soon be equipped for plasma lyophilisation.
In the hygiene and disease prevention f ie ld, the additional' ' food rations allotted to the men of the Armed Forces has been revised and adapted to modern biochemical concepts.'
> . . « '
- Some progress has also been made since June 1953« in .building up the f ield medical units to be assigned to the Army in operation, but budgetary ShoHages have unfortunately limited our practical -accomplish-ment a, which have not actually met our, desires.
Ve have managed,-however, to increase by % few units the nùm- -ber of each type of mobilization medical units, .namely Field, Hospitals, Medical Seotitwis at Division level, suf-glcal centres, Mobile I-Hay and Dental Units and hospital trains. ' : ' '
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Wartime attrition and consumption rates hare beam worked.out* " for each,category of medical equipment, and supplies including th.e, vajS-a.'' loua types of f ield medical units, whose equipment has been brought-up ^ to date according to the new standards* -
In accordance with SHAPE'S "request, a plan has been drawn, up a-v.:; for, the evacuation and hospitalization of casualties and for suppliesWJ . according to estimates of battle casualties and non-battle casualties In relation to evacuation transport capabilities and bed/troop:Tâtios, and.for the necessary reserves of medical, equipment, and phamaeeutlcal^ V. . supplies. . . . . . •
' -.•!•> y v, - ' r.-j:».? fH'ajf-tftrtq/;'. ' >
The requirements for a Quartermaster Corps ("Intendenza") .,>'• y ^ ,.. medical warehouse and its various branches has beendefined*y;V'
.,.,...- • v • • . • ." •::.'.;•. I,: • • i ^ s & K UÇ i
The quantities were computed on the basis,/Of the'attrition j ^ ^ ^ / and consumption rates for the various materials,so 'as. to.:ensure^* 30:-days supply. 1 . ' I • -•••/• 'v--'- v ! ; ! ! ^ ^ ' ^ ; : ^ . ? :
Available funds did not, and do not for the time tbeing,-, -nake^p^v:;,,. i t possible 'for these oentral stroes and branches, to be -, a c t u a l l y ^ ¾ ¾ ¾ ^ ^ up, as they involve a very high cost. , • .. ^ " • v-.-t".-. -:• • • = ,;>>''
... : The Ouartermaster Corps chemical, toxicologlcal. and bacterio-^^ . , logical laboratory has been reinforced and subdivided into. mobile v
sections provided with their own means for the transportation. 'ofV - ' v
personnel and equipment. : / ; • ' ' , „ , , .The creation of a. special surgical unit for' assignment to «a-s^i^ -
Paratroop. Brigade has been studied and defined*. This new • unit i i r t ^ ^ v*' have personnel and equipment capable of being parachuted.-in'«order4to'\K^"^' > provide the wounded with aaergency surgical treatment on the spot. v. where dropped. - ---.'•• 1 ...-:.•:••.-: .»>• ..: :< •• ??,. /
/,-,1-.-. :..v '. . • • -. . •• - •••..fc-.if-:---:--, grrààî-vt
Following practical testson the transfer of . casualties: from<i!>>> : one ship to another, the Italian Navy has adopted the US Navy. type ; r ; w- -, stretcher,, whieh is now being supplied. • ••; i ' ; • '.>. • . i*' , -
, The Air Force-Medical Corps has examined new - types. - of*f irst-cgtf;; aid treatment kits for air-sea motor, ambulances, and have • suppUed ' their first-aid stations with equipment for shock .treatment', J.,:. -.--- • V ' '" ' .--- ,..-. : ,,-. fâï
. .A plan has been established- for setting up on the nat ional^ v .. territory, in the event of an emergency, 36 protected medical- areas jfowjft^ containing 75^000 beds.
This programne is provided for, as you know, in .Article: 23,.!st. r a. ' • • of the First Geneva Convention of 1949 concerning the safety of wounded and sick casualties of armies in wartime.
nrtt nwt ; ' hm ' wnt,^ . • f*, ï ^ / , t ~ • ^
, NATIONAL REPORT FBCM UlXaSOOBG; .-, : .- -••• .-.- r--
1 '«'1 .'-
iJf-
ji1-f'ifii' > •
MAJOR FELTENi -, .. -..- • » .hsu-; • .
The Luxembourg Army Medical Ser1Vice has -made some progress / v ; during 195A}, as .regards organization and preparation.^, ^v ,--1 : •
..... . , . - , .; -.., . ^ - . ,.-. î: '•. , ;. • . .- .-.:-., Î-.0 ÏSrf ' • .
-, ;. For the f i rst time, we have been able to/create a medlCaû:-111^1
company of 200 men, SNCOs nursing orderlies and-stretehSi>bearsrs«"^iT^T The CoB any has an adequate staff of reserve medical officers whose -numbers.have increased considerably during the past.year. ;
. . 164 .. ,-.,-
'< ' NATO CONFIDENTIAL ••''
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

A training centra haa been e8tabll8hed. ,,; Thi8 ,centre, iinder ... the control of the Medical Service, will; provide professional andy military training for reserve-medical officersahd senior,NOOai. -: ^
Professional technical training is given to the nursing orderlies,-who also attend courses In the varlous^infimarles^ ,-Steps' have been taken to make these courses more effective* • v.-,;, .:, ^ .v J
, A chest X-Ray examination has been introduced for: a l l regular serving personnel, officers and Senior NOOs. This ^examination ;will be . • repeated yearly, in March. . , -
An agreement has been reached between the Ministry of Public Health and the Amy Medical Servite under whichthe. bacteriological;- -'.,-,-.< .< laboratory, which has ample facilities-and is creating new departments, will keep the Anqy Medical Service informed weekly of the infectious v disease position^ and of the possible outbreak of an epidonic in the • country. Where required, this information wi l l be sent through Ahe -.- --most direct Cheumel to the Chief of the SHAPE Medical Branch.-, , :
t , * .*
In 1954 the Luxembourg Army held a field exercise withJ+,000 -. -men and a considerable number of vehicles. This .exercise lasted- ^ r . ; weeks and constituted a tough test both for the men and eqaipriNHt. ! - -.,, The medical company operated with Uie troops during the wholeof the. exercise. It provided us with an opportunity of organizing.-a fu l l --br. . evacuation chain, from the sick or wounded* casualty in-the forward .area-... to the base hospital. For this purpose, the medical company has been-. --.<.. provided with a l l its TQSeE equipment, particularly ambulance jeeps. It operated as an independent unit« Battalion f irst aid^posta .and . casualty clearing stations were staggered over, a .distance^ 10 to v.l2,--.,v;/ kms. The clearing point centre was constituted byour Mobile Surgi cal. : -
'Unit, which was of considerable service on this occasion; In less than 10 minutes, the entire Clearing Station was ready to move. «As« changes ; were frequent, i t was possible to train the medical personnel in carrying out rapid movements. Thus, the 1954 exercise.provided a wealth of ex- , perience and lessons for-the Medical Service of our 'ArmyV-• Thank you>. -
hIUMI. M tf Ir JUtH dfcttnlt MMM """ v. " W ü KIT Tl H H HKH MHn. H H fl HH^ WW^ JQ n n r- 7.:-.-, .
SUMMAHT OF THE PR0C5ŒSS HADE BY * i >••<"•
THE BOIAL NETHERLANDS AEMT and
AIR FORCE MEDICAL SERVICE . - . ' • ' ' •' V; .• --•;--• -,- .; ;
MAJOR GEMTOAL VAN PER GIESSEMi /
(Notes The f i rst part of this presentation was graded.COSMIC TOP SECRET, and cannot therefore be published.- The second part was given as follows«)
Progress made In the Field of Military Medical Preparedness in the Past Year . *
Ih the past year logistical instructions have been given for th» Royal Netherlands Army and the Royal Netherlands Air Force, organizing -
' the medical and dental care of the units in the combat zone, the LOC and the Zone of the Interior, that i s , from the f i r s t up to the f i f th echelon.
An important progress was made in the past year iAèn in AO civil hospitals beds were-placed at our disposal for the hospitalization of : military patients in wartime. By the lack of depth in our territory, in the present situation our LOC and Zone of Interior f a l l together; never-
- 165 . ' -NATO CONFIDENTIAL
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
' ' ' ••'•!•"'. t
V
theless a sharp differentiation between the medical formations 4Of the 4th and those.of the 5th Echelons inust be made, also h o w , ' . ^ 5 7 . : -account of the difference of their task. - 1 ; •• /----..1 --•• ; fit-': '
As 5th Echelon medical formations are earmarked: the*. Mili - , . ' tary Hospitals in the Hague and Utrecht, the psychiatric • Clinics a t ' & Leyden and Bergon-op-Zoom and the. Military Revalidation ^ Aardenburg at Doom. Fürther more we are planning the InstallatlMi • of Military Centres for Burns, a Centre for FlasticrSurgery and a.-:,' j;/'' Centre for Maxillo-Facial Surgery. '
---- t&ï^fyvyK I hope you wil l allow me to make seme remarks hererrtirtnrtu' ^ / '
the caoputation of fixed hospital bed requirements. It is known to ,, ' you, that in this respect A basic data are necessary. TheSe are: ;.:. J-'Z&ÏÏ^'y the troop strengths, the daily admission rate, tha accumulation factorWMx:; and the dispersion factor. As to-the daily admission ratej • you- also'knbwV-what circumstances have an effect upon this percentage/ that among ! " other things the category of patients, taken Into consideration, is of^vr^ ' -influence, so that battle casualties have another admission rate than ^ j x i 7 non-battle casualties.
There is , however, one circumstance I wish to bring under yonr / ' attention, namely the war experience of the troops . I t stands, t o v^r -;>.. reason that experienced troops have a lower casualty figure »and.icpn^& ^i7? . sequently a lower daily admission rate than those troops which'. lackÀt^i»'^1' was experience. Ih the computations given by SHAPE; this >f&'ctor>is*not^'* mentioned. '. :-•'•- -öl;*./,-
: In PM 101-10 i t is stated that during the last year »of World' War I I * in the ETO the daily acfaisaion rate for battle c a s u a l t i W ^ ^ ^ V ' f amounted to 0.6%? and 'this concerned experienced troops. iw-j»/ 'S-SSt- *;\ zkfi: '.:
-, .. • / v. v.' SHAPE has now raised this figure by 50* for the foUowlngV^W Of ; ' '
reasons Î .=:-.1 - . .' -. -':-.< s---: , ^ £ ^ ¾ . ^ ¾ ¾ ^
a. Larger effect of the .conventional weapons .".>,••»''.'*: b. A possible use of tactical atcmic weapons .'."•-'•';:'* c. A probable use of nerve gas. j • • '-.'•• '-'v^-^'/-
• ' Because of this the dally admission rate for battle casualties ? :jr is fixed now at 0*9*. . • '
Ve are of the opinion that this figure ought to be raised .it ' least for the f irst 30 days of war, on account of the inexperience of the troops, • • -,
* . .-• • . • , for the f i rst 15 days by 15*, by which the DAR would become ,
I.035*s rounded off upwards to 1.04*. V
for the second 15 days by 7®S, by whichthe DAR would be •:.-.-. j>-.J:. 0.9675*, rounded off upwards to 0,97*.
'..... " • . • .: t.^.èt.'ésÂ?'.'' The DAR for non-battle casualties in the ETO may-be Maintained
at 1*, as is stated in the FM 101-10, although i t might be considered , that also here the inexperience of the troops should.be taken into -, : account. • •• -.- ..'••"..'". •;•• --. - - - - •• .
y ; In our opinion the area of our country is so limited' that- no objection can be raised against using the same hospital admission rate forthe troops of our army corps and those in our LOC or Zorie-Of 'Interior'.' '
166
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

f'L Î • V j
. f
a i
1 ' V i
* ' ' '• •• ir
ii'i **' In computing the fixed hospital bed requirements ! i t ehould^. •
be kepb in mind that in case of mobilization there is always-a number j--of patients who are already occupying beds, who were ewiBlltted iri peacei . > time. Of course, a number of them can be sent back to their ..units ; j a certain percentage to a convalescent centre, but st i l l -wé^hal l have! * to take Into account that at least half-of these peacetime^atients will,-have to be kept in hospital. --- \
There ls another, feature, we must certainly^pay attention toj and that ±s the lapse of time between the mobilization andj the* outbreak
' of hostilities. This is especially of great importance, In case-only; à comparatively small number of beds are ^available. .4* • r- « r • i
; -(• b , I should like to iUustrate this pointsby-an^example — I f .
we consider how many fixed beds are required for a troop strength-of. 100,000 men, this wi l l be for a war period of 30 days:
. f.'
« • ï • "i :
.v> r
f 1Ii:;
1I /1 . .
} "i? » : 'iI f
! +
'' i "i ~ "' i-V 3
for battle casualties ti for non-battle casualties 's
2,064 beds L 1,626 beds
Totally, we shall need 4*490 beds.
,/• V-..V 1 '
" I f this number of beds is indeed; available^ so if-there are51 * enough beds for a war period of one month,' then it does ndt. matter much how much time wil l elapse between mobilization and D-Day, ias .the. num-j . ber of non-battle casualties accumulating in the hospitals before IW)ay will be discharged in 20 days, ,
. I f , however, the number of available beds that they do not suffics for 20 days, then i t is an
/. I should bis sa SmalXi easential point ;. J
for how many days the forces will have been mobilised before hostilities break out.
> The longer we Shall have to wait for D-Day, the j shorter wi l l be the period of the war, for which the number of beds available wi l l be> sufficient. In this diagram (See page 166), the abscis• dicat es the number of days, the ordinate the number of fixed beds ^required for a troop strength of 100,000 men. . /1,/ ,
piusthe. non-battle^ casualties,..withrtich et cöme. The other linès :ifcdloete.the 1>sd.
i . The broad line indicates how many beds are reqjuired fo r the , peacetime patients (the troop strength in peacetime is estiaated att;^ • '
..half ths number 50¢000, m « ) » . we assums that D Day has not yet requirements for battle casualties and non-battle casualties - after.-D 4*500 beds appear to be sufficient "for war.period of one month, regardless of the moment when.D Day comes. /, . f " ' . • i -.; - '. ' • .'.-.< ; ' •'.;" • • -•. . ; -, •' I
If there are only 3,000 beds available, t&is number wil l be' isufficiisnt for 16 dayss i f hostilities break out Immediately after . :1 -< 'mobilization. If D day should come 10' days later, .the number: of beds' will be sufficient for a fortnight 's warfare. I f D Day should ecrae a; \ - , month later, the number of beds wil l be sufficient for 12 days. .. Should '. we have to wait a longer time, for Instance .2 months,1 in that - case the number of beds wil l be sufficient for 9 days only. i - ,
, -M M-M B H B W M M M M B M M X * - J H H t - M ^ H H H H H H H t M K B M O l N M J t • - ä -V-
• "i
1 • 167
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
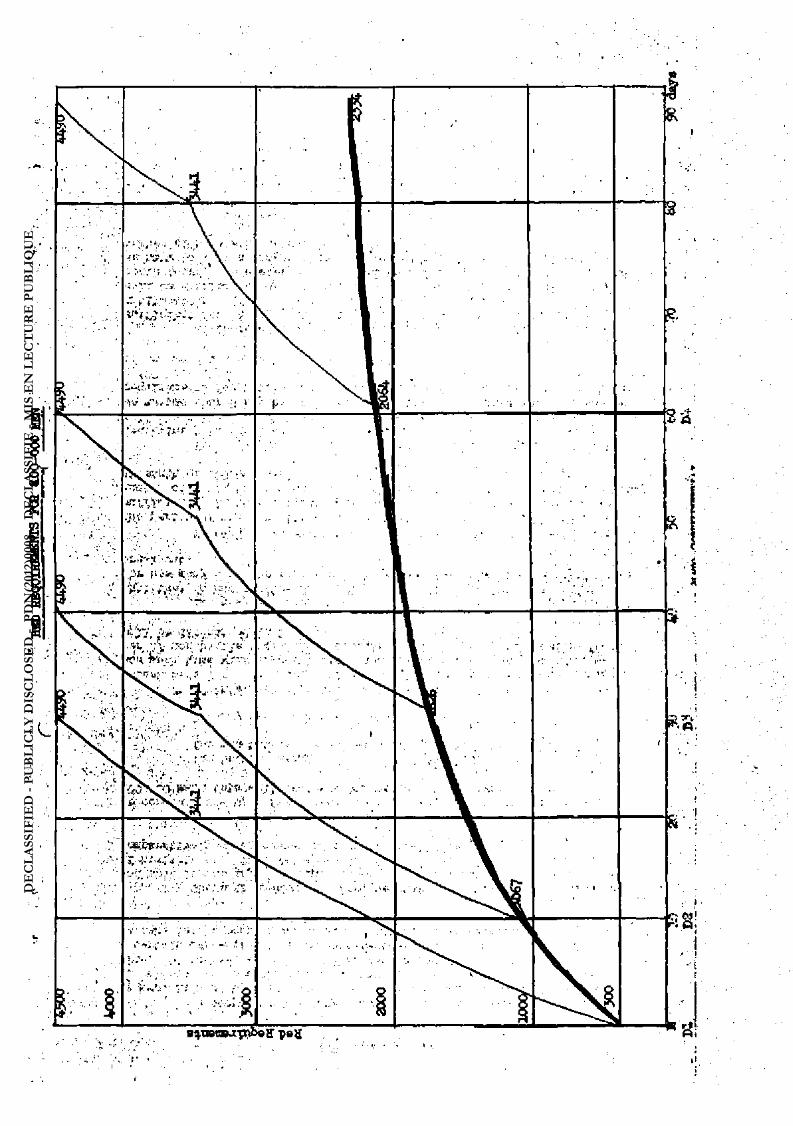
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

' QEffijfeALi ,DALEs
TMO YEARS ago I hade the privilege of talking to thisMedi-r cal Planning Conferenee about acne major medical problems with Whleh the Norwegian Medical Services are working.
I shall now te l l you briefly what progress' has been; made, in-,-, solving the problems listed In mypresenta-W/mof 1953? \^¾ ¢- »-'-v-r- I' •
1. Hospital Service, in Peacetime for Military Personnel '.-7-" • . • ' • ' • • •..-•.v.':;
Our single military hospital ls : s t i l l only, a 65' bedded £ hospital. It has, however, been modernized and made more.effective. Although this is an improvement, the hospital is st i l l ' insufficient , .; . because of its small size, and consequently we are -st i l l -unable to*,» give medical personnel in-the forces training and practice in .a. , 7--military hospital. .,--.-. . .-,. '..' /-.-.:. >. .Ï--.V.••
-. / , •:.••'• y - : :.--7,-7 -V-". 2. Ve have continued to study the orfanlaation of the ser- - ,
vice in the rear echelons. A -recent NATO staff exercise on the logis-tlc support of NATO forces in Norway has been of great benefit by f ' ' bringing out new problems and ,by throwing light upon'>ldvpreblaM^an&r^ weaknesses. In this connection, I should like to mention-the--eaceelleht--cooperation we have had with the medical representative o'fAlHed _n.| • Forces Northern Europe - Colonel J.P. Douglas. We feel very much in-debted to him for good advice and for sharing with us his\ valuable experience. Provided that the necessary Ainds are available, - I have;} • no doubt that we shall be able to solve our problem* in this particular field. ) • . * -
7.7 :". l: -:--:vJî;s?-t.Psî!! 3. Blood Transfusion Service - - y y ;• /• >.*7,
..'.-.'. .,.-. -.--. 7. ' , -T - ' .-, '•'}.. I regret to sty that progress has been slow, and*! have",
found it necessary to put more pressure upon the responsiblerindlvld-; uals and institutions both civil and military. .^Recent, develofments^y^-. sean to premise a change, however, and there is reason to.hope.(that.->7-an efficient .service will be organized, provided ag^n'thatyltods/arv;."^ made available. • -. - . --• / - *
4* In the field of ABC, two things have happened which ». , probably will prove to be very importantt .-77 j--? •
L '-.>' •
:f- T- - . - -7- S * -
rVt-
a. A Central organization has been establisheds charged with the responsibility of planning-ABC defence with-in the anted forces. This organization wil l establish a school for ABC lnstruetors, for.courses-in 'ABC.de-
-..'.. fence, etcj i t will study developments:ln the ABC field, make recommendations for'the.selectionand<use of ABC equipment, etc. -.-... • •" - • • . .••»•)*». . s^ , - . ' ' -1 i -J1 "f Vj ' " " • V
... • . b. Tactical and organizational problems connected with atomic warfare have been taken up, and are now ac-, tlvely studied by military general staffs,. Earlier on ABC was considered to be a medical probl«a. This was obviously a wrong appfoach, which caused much de-lay and confüsion. ' ' ,
. --1Ä9 - .î''- V-. .:..-,¾..
MAJOR MEDICAL PROBLEMS • ; • > ,..-.-. -. . - .- - - . . - . ,
MEDICAL SERVICE OF THE.: NORWEGIAN, FORCES - .
: . : . - . V .' i.'^J- - : .77 • .. .. .... ..,.- :--.-7 J.-, ..
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

NATO CONFIDENTIAL * ' -'• •:•- - £ ,f-* - • - * ;. \'
1 - •'. ?" ' -v - • , .-'
' . - . • • V ,-. .• ' -T V , -, V, i . , 5. We have worked very hard to persuade the .authorities'that " ' • . 'V." "
service conditions, pay, etc, for military doctors will have'to be;such > f'—v ' -.-that they Sttract f i rst class doctors. An arrangement has^^nowvbeoii - \ V. agreed whereby regular medical officers, shall be permitted"to carry on * v ' with other medical activities while th<py are serving, thus making than; . . able to earn more money or to work for a medical specialty.; Office - y /. hours have been regulated accordingly* In our country mediçalÀoffieeiÜfc:•IV recelve no other compensation for ths expense they have had and for the ':,Vv ...-. . time they have spent in studying médieine. - •" i ^ ' C y ^ V * ' V
6, Each winter a group of specialists is brought t'og«tiUr, ; for one week in the mountains to study specific pröbleras connected with ; -.. ^ * medical service in winter warfare. This last winter prbblaas' of medi-• ' : . 'v cal tactics were brennt into focus together with ' t h e ; - p r o b l t o s ^ o f > ' î : C . transportation. -
1V. , : V-.
ive:ahd continuous"-^¾Y-> 4 ^ m .> ' • • J ' I '•• y r Vv- • •-
7 . In the ATDQT there has been an extensive build-up. The Term of Compulsory service for national tServicaaen• ; v < /-Y"' has been extended by k months, Which has resulted in ^proximàtely:^^^. ;^; .... 5O5S increase in the numbers of troops under training. An e«tra.%û-^yÂ'. ; ' ,<; .- ; .?, training brigade including a msdical company and a Ii^t'field'.-hoi^ii'alC^ft j ' ' -Yf has been established. The msdical recruit training centrer / . / , panded and made more effective. Hore personnel have been appointeditaive. • ''Î/-Medical Service in mountainous country has been studied In connection : v • • V. '" « with refresher training of reserve units. • • -•' -^vVVi-; 1V V ••• v -Wv '^y : . . , ;
, Ô. In the Air Force, the Medical Service has "been COTcwned - ; V , with the organization of air evacuation, aercmedical indoctrination>of •/ '
taircrews, medical service for troops defending-air fields and revising'«-TOtEs for Air Force Medical Units. v .-, ::-.--.5^^:-.-.,. ••
- — -:-:-. ¾ 'vi'.'ii-T.'..
/ MEDICAL REPORT - PORTUGAL ,- v- - .,• S*, ci- v » y--
LT. COLONEL DE BETTgNOOüRT: ' -• ••/•"'-Î.1 V :">'.'"" '
• •-• • ' 'S-
. •* -/-----5
•. - •
This is the f irst time that I have had the honour to v att end J/ - ; v J* the SHAPE Atmual Medical Conference. It has given me the opportunity ' ' to enter into direct contact with the leading officers of the ;SHAPEais^ V-; y 'v Medical Manch and to become familiar with the main problemsrofiedn^iiH, •'.,-. eern to the various nations represented here. I have thus been .able-K":- y':-J.. \v to see for ays elf the high level of these meetings, scientifically tasH«,^.^v.: •-•', well as intellectually, and how effective and valuable they hawun -^M; : . •> '.' questionably proven to be. : / Ti --
-- - ' V : ,„-(:- - i '
Please accept, Hr. President and a l l attending'delegates ?andi colleagues j my congratulations on these meetings, and allow me to thank you for your kindness and the assistance I havereceived. I salute you a l l on behalf of the Portugese Médical Oorps.- ^ fV •
As you a l l know, Portugal faced a hard ordeal in 1954 because V --V' : of the situation in Portugese IncUA, which hiwever, did not«alter by" any V ';i>V means the military training programme set up by the Goveranent. Never- ; .v*'- -* . i theless, i t will be easily understood that our military and >conosdc . 'r
j.;': ' " efforts were to a large « tent devoted to the territories, the d e f e n c s . > ;-v-< *f
of which is for us a matter of honour and a duty, prescribed by.!our Con-vv- ' - ; stitution. , . • - -, . . -M''
• - .. " '- ---.1 :•'".,'-"• ' -,. .'"•'. :% The development of Portugal's military programme is pro-. ' ' ^ • '
ceeding at the rhythm permitted by our available funds*
under three headings; Organization, Training and Equipment. - . „• : : As for our Medical Service, its activities may be summarized
tion,
170
... V.;.-Vi- V '' -^l • :-1-.,-.
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

Organization
Ve may say that the plan for the organization of our field forces has been completed, and the corresponding regulations .. have been published.
The organizational plan was set up on the basis of our military capabilities and requirements which provide for our par-ticipation in the European and Iberian Peninsula Theatres, the de-fence of our continental territory, of our islands in the Atlantic and our overseas provinces. The general rules l a id down for war-time military regulations were adapted to our military traditions and to our own terminology,, We now have available an organization which, while having characteristics of our own, i s perfectly adaptable to the collective organization to which we belong.
Training
Training in the various branches of the Medical Service i s being continued most actively. I should like to mention, as an exampl e , the
manoeuvres carried out at the Santa Margarita Training Camp, where the Medical Corps Command had the opportunity'to work at the Division and Anoy Corps levels. Bauippent
The present plan provides for the replacement by up to date equipment of part of the divisional medical equipment which is con-sidered obsolete. Our equipment allotments include the dressing and pharmaceutical supplies required for ABC warfare.
Civil Defence
There has been considerable activity In organizing the Civil Defence of the Portugese territory. The Civil Deftance Central Training School in Lisbon has continued its series of courses with: particular stress upon basic training in the various branches of Civil Defence.
The Civil Defence Organization comprises severd. thousand volunteers to take at least the basic course. Our Civil Defence de-partments have been Inspected 1sy the NATO Civil Defence Advisor who _ noted the efficiency of our organization, and the compliments ex-pressed to our Civil Defence Department were definitely more than mere words of courtesy.
In conclusion, we can state that activities of organization and preparation are proceeding at an appropriate pace within a l l branches of our Military Medical Service,
The past years were devoted to solid preparation. The Aiture years wil l be marked by the thorough Implementation of our programme, to Milch we are willingly committed by our international obligations.
MEDICAL SBPORT — TOBKET
MAJOR GENERAL OOGBN
Gentlemen;
SHAPE'S annually held medical meetings while acting as an
171
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

enlightening guide by covering the discussions on many important subjects they also provide the opportunity for a l l the delegates of NATO Nations to acquire a brief idea on the medical status of other friendly nations.
Using my chance of ten minutes which is used to be given to every country's delegate on the last day of the meeting, I would like to cover present medical status of the Turkish Arsqr in a few words.
Shortage of medical officers in the regular army, s t i l l stands as a subject which becomes more critical day by day. Recent economic progress of our country provides to the individuals better employment fields beside the army and satisfaction of personal en-terprise have/SSSrcised by more people every day. Just because of these two facts the number of medical officers parting from the army by their own wi l l goes up and up each day* As a precaution against this, In addition to the one In Ankara, another military medical school has been opened in Istanbul with anticipation of maintaining and keeping a higher number of medical officers in the Army. IAth the supply of medical officers of such a school, i t is thought that the loss caused by the resignations can be made up.
Shortage of pharmacists officers in the army is again offering a critical shortage. Three quarters of the T/Os are s t i l l vacant. Big difficulties are met in conducting necessary services.-Since the law on restriction on pharmacies is no more in effect, or in other words permission can now be obtained by every pharmacist for opening a shop results in great numbers of pharmacist officers resigning from the army. The vacuum created by these resignations we are trying to f i l l by MS officers.
How.jw.ij Much the number of dentist officers is not com-plete, shortage in this branch is not as critical as In the other medical branches. But a critical future shortage can easily be fore-seen. Number of students which are educated at the f i rst and second grades of dental school on accoint of Ministry of National Defence, is not more than one or two. It means that the source of dental officers Is already dried up.
In spite of these shortages, in every branch of the medi-cal services of the regular army, we'have enough reserve officers to f i l l and meat wartime needs.
As far as the nurses are concerned, we have again a limited number in hand, which is far below our needs. In order to make this brandi more attractive a l l of our efforts are towards giving nurses the same rights as officers—unfortunately, these have not yet been In a positive course.
However, our amy s t i l l h as shortages of medical NCOs, but this situation premises an improvement for the future. Ibtvy and Air Force are given the duty of conducting their own NCO training by opening one school of each. In this way, those two services will be able to supply their own medical NCO requirements within their organi-zation. Both of these new NCO Schools wil l start to conduct training by September 1955* In addition to these, provisions are made on the expansion and enlargement of present NCO Schools.
MC courses and their training* At the medical faculties of Ankara and Istanbul UniversitiLes, there are students making their education on account of the Ministry of National Defence. Among these the ones from medical faculty, upon the completion of their sixth, den tistr, and pharmacists fourth year, are called to the clinic of the
172
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
Military Medical Academy for one year's course* During that period they receive training on the subjects of Field medical services, war surgery and military hygiene both in theoretical and practical ways. They are then assigned to units.
Anqy nurses are trained at Red Crescent's nurse school in Istanbul for the Ministry of National Defence. There are prepar-ations for opening another nurse school organic to the Army.
Four years ago a medical NCO school was opened in Ankara* Medical technicians are trained by this school. There is a practical work period allotted for the students of this school in the Military Medical Academy.
Until recently a l l medical enlisted men were trained through a certain period of practical work In military hospitals. Just because of this type of training never having been found to be satisfactory, a new HRTC had to be opened. This training centre is in operation since last year.
At this training centre, a 100 bed hospital has been set up for practical work purposes.
Our intention of having a MFSS opened at this centre is just about to come into realization. In this way i t will be possible to organize an AMC Uke the one at Fort Sam Houston, in Texas.
According to the NATO it is ijrt ended'XfcctnHlifc rupp a l l medical equipment, medicine and antibiotic stbcks to auch level that' it will be possible to supply a l l requirements within the f irst 90 days of war. Today war stocks are known to us, of a l l important medicines.
We have a considerable stock of Sulfonamid and i t is even more than the NATO requirements. Naturally expenditure of seme certain antibiotics would show ap a big increase during wartime. So to make a 90 day stock of such antibiotics would be rather difficult and a time-consuming business. Our penicillin stocks are enough for 18 days, cal-culating an expenditure of 40,000 bottles each day. Necessary precautions will be taken In order to bring that stock up to the desired level by 1957*
Thanking you a l l , again, gentlemen, for your precious moments given to listen to me, I would like to extend my gratitude to Brigadier General Wlford F0 Hall, USAF (MC), Medical Officer, SHAPE Logistic Division, whose great efforts made this meeting possible.
UNITED KINGDOM REPORT QN
MAJOR MEDICAL PROBLEMS
AIR MARSHAL KIIfATRICK î
General Hall, Gentlanmii
We have become accustomed to a high degree of efficiency of organization and conduct of these Medical Conferences at SHAPE, Al l will agree that the Conference this year reaches the highest standard. I should like to acknowledge gratefully the careful thought and the hard work of General Hall and of his staff in making our attendance so instructive, and so comfortable and trouble-free.
173
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

I wish to speak of some problems of aviation medicine. Hen can exploit the air only to the degree that environment is adapted to their physiology j and these problems are certainly of major import-ance to us.
The background of this conference has been predominantly on the operation of ground forces, and the importance of this aspect is obvious; it is obvious also that I t would be impossible In any reason---able time to consider a l l arms in detail. But a l l wi l l agree that there are decisive battlefields above the ground as well as on i t , so decisive perhaps that unless the air battle is won the ground battle may be lost before it is Joined.
This is not the time, nor am I the person to conduct any sort of critical review of the whole field of aviation medicine. But I select three problans Which, we think, would merit Interchange and co-ordination of views and findings. They are not new problems, but they are basic problems of added importance as the performance of aircraft increases. They ares
Fitness for Flying Fatigue
Pathology of Aircraft Accidents
Fitness for Flving j
Considering the vast experience of f l i g i t which has now been collected, i t is ranarkable how small is the area of true validation of tests or selecting procedures. There is of course a reason, as every caBe is conditioned by an indefinite factor which we may call X, this symbol representing the quality variously known as motivation, or the wi l l to f ly , or more crudely and expressively as " f ire in the belly,n
We a l l know of cases where resolution and the wil l to f ly and flight have overcome gross disability; we also know of cases where a l l the appropriate and measurable physical and mental attributes have not been enough to bring success in flying.
Ideally i t should be the task of aviation medicine to de-fine the conditions which f i t the machine, however exotic, to the aver-age alrerew, for we certainly cannot assume an lnexhaustllte supply of supermen. But we stultify our purpose i f through over-caution we cast aside the efficient man, or on the other hand i f we unwisely accept the inferior man for a task which demands the efficient man.
Where is the dividing line between fitness and unfitness? How do we assess factor X?
Fatjgue
There is no argument that prevention of fatigue among air -crew is a matter of f irst Importance. But we should be much more con-fident of our ability to prevent fatigue i f we really knew what we meant by fatigue. In this complex field we need an objectivity in definition and measurement which is not obvious at present.
Some schools of Physiologleal thought approach the assessment of fatigue in terms of decrease fron a standard performance, and there is promise in this outlook. But in the meantime we, as doctors having the imnediate care of aircrew as our charge, are In a dllana, Must we wait to act until a pilot is so tired (whatever we mean by the term) that his per-formance declines significantly? Or is each one of us to Judge by his own ill-defined standard that a fatigue state is approaching, and perhaps
174
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
needlessly Interrupt the flying of a perfectly competent pilot?- Unin— • formed answers to these questions mean waste of skil ly whichever ea^ - ' «'•.. trewe is chosen, and we cannot afford to waste flying ski l l ; p -'^ i--' h';* ' >
Pathology of Aircraft Accidents • • ...-Ï- ••'--•
The problem of pathological investigation following flying' ^ ' 'A f accidents i s , again, no new problem, and-thé importànVe»of ^full>-lâibw^ vu- -a.^», ledge is obvious. In the past the result s of- ma joraceideritshave^some^ r-'t" • ; • times appeared so overwhelming as to rule out any hopé öf detäiled ^v ; - - ? ' -pathological study. We now tend to believe that we have accepted this -J--iV situation too readily.
Investigation into the Comet accidents-has browgHbhome to us that much more can be done than we thought possible in gaining- know-ledge from• slender élues. The painstaking work of FrdfesSor-FWnSri^of >• ,••'':>-•' the University of Pisa in relation to these accidents was of the greatest assistance in the investigation, and indicates the value of intefnatIorfaI -cooperation in this, as in other fields. •'•••• - ;. > -i-V
As we see i t , we must do two things;- f i r s t we must-ensure* ' that our pathologists carrying out thia task have close knowledge of - ' aviation medicine, and second, we must develop techniquestô draw in - . formation from even the most unpromising material which the*pithoiö£-<\ k>.'-.e, ist may receive. Clearly, we cannot promote flight safety I f Zthe0Iessons ' ' of accidents are lost to us. • ' '^y
jjsasksisa • 1
:". • • ^,-^fJP^yr
I have not selected these examples in Sinyt ispirli.-of-de^* *> pair, as I am confident of the increase of knowledge in vail, of *theoi~ > * I have chosen than rather as indications for widening the effort; toràlrd'e v . their solution. The fresh approach is valuable to a woAeK^o'-has^tùrnedr, % * -over a problem for- a Ioig time. It is'possible that rth'ert' Û observations on these problems unpublished, or buried int l i terät i l t t re^ -^^^v not recognized as relevant, which may f i l l some of the -^ps :-Insi oiir ledge. Coordination of effort, i t seems to me, ie likely to-produce« answers more surely than individualism. - •' V'. Jt-". ;••
"• •'•' '• - ' - • - . • ^ r ' 1 ' ' ' ^r^fs'.r.r:^.;,^ -'.: • iiu.o k ^ ^ . M U i M t j yu i ; J^fe^ MjUt, wuL ^ -j i j »ft1 " i * ' .. ' ^flW TT^T , r- W^TT j * ,* , J1 , *
' -V1 -7-. -:.,. iV j • • . r •.: >~ - »..;-<>,'r> Ji-;'.:. v >:-,-,
NATIONAL BEPOflT FROM THE UNITED STATES. BY THE . t.w 1 ,. • . . . . . . . . . . . . . . f . -.-• • : V-
SURGEDN GEMlRALn U.S. Amv . . ^ ' J ;."> ' . - - . . . . .....j.... •-. .- ;'-J-U Vti .... < .-
General Hall, Centimen s . V U H . - V ^ . - •-: T should'first like to bring to this Conference* the greetings
bf our Assistant Secretary of Defence for-Health and Medicine, Doctor Frank Berry. As you a l l khow, he is represented here by his'Deputy, Dr. • • -, Cushing; and also by one of his advisory conmitteanen,' Dr. Rourke. Dri - - - ' Berry has just returned to Washington affairs before we 'departedhiving ? y-been on a rather extensive trip through the Middle • and Far iEast, and- felt-: that hè could not absent himself Arom Washington longer at thisparticu-Iar moment,. I also know that there are two other individuals,'fellow r ' . fct<untryaeniof"ttiéejj who "1SWiiId warit t o b e remembered'to the 'individuals on duty in :the Medical Secfclcn at SHAPE, and also to the->C<mferees-l.of this* -J planning conference, . And I refer to Dr.Casberg, whrnmanyofyGu-will kTe- . cal l , Dr. Berry's predecessor; and our dear friend, GeneralKeraiardy'for' •, whom a l l of us developed so much admiration ,and'respect during the period he was here. The Stresses and strains of planning for a- future war. have'7' been so rdugh that we've had some casualties in our-group, arid most 'of you
175
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE
know that Admiral PugJi and Gmnaral Kermard have both, had episodes, but you will be. pleased to know.that both of thma hSkVé'made a very remarkable recovery» :••-,•.;.. : - : : -•
After listening to Colonel Nelson this mornlngi-I lMtd' a moments of very sincere depression. I fe lt that that was a^very"grlS^*,. .
. sort of report; and yet, as I reflect upon a l l of the presentations of , yy *•" this conference » and as I have listened this, morning to the. reports ; - z, given by delegates of the various NATO countries rsprsisented at; t h i s i ' ^ ' ^ y ^ conference—I- go from mytemporary period of depression into one.of~r.v?r let ' s not say %exultation, exactly--but certainly, a more hopeful a n d , . more encouraged state than I fe l t at, the termination of Colonel N e l - , - I i - ; ^ . ' son's report. 'V "'
. ---.--., ^y • ., -..-v. v.T:-t I'm sure that General Dale and General,Ferri,,and, . othw;^.
who are here who haW attended a l l of the preceding conferences vinUst '. ', recognize that great strides have been taken by a l l us. And while1 w e ' r é f • a l l frank to admit those defects which we have not been able to alleviate^-.• because of finances or politics of for some other reason in our^yarlciuSj^^,^ countries,'nevertheless I insist that we have a l l made a great stridé. since our initial meeting some few years ago., ' v ',,^ V;^'J t -^ l iK
Our problems are no different from those that have been. ported here thls^morning. Several of the reports havs mentioned, d i f f i - ^ ^ cultles.iri obtaining health personnel for even our peacetime r e q u i r e - , I - 1
ment s. I'm very happy to report to the able report ed, from. Canada^hat, ^ based upon that country's experience, we are about to persuade our Con- ' gress to glvs us a similar subsidisation programs for giving lis pftyw^ slcians and dentists for our regular corps. We s t i l l , however,' Huetf'' resort to oonscription to obtain the number of personnel in the health -professions required for what we oonsider a period of semi-mobilisation.
, Ths problem of acquaintingour,colleagues-->dththe,probl«w;^£,:^ that would face us in the event of . a happening such as was/poHrayed.so graphically and so ,ably by our British colleagues yesterday ^is-somettB^^d^^.-that keeps us,worrying constantly and leads to many a slseplsss. hour^in the middle of the night. , -....,. ,. -., .,......- ; , - • ^ ¾ ^ ^ ¾ ^ ¾ ^ ¾ ^
Wein uniform particularly are at a disadvantage when we "tryyv ;; to warn our civilian colleagues relative to the magnitude^ of/thëse ïïrob- 'yî^û Iems which we may have to meet. And i f .we're not -careful,, we' 11 accused of war-mongering; and therefore we must approach the thing-Mv,^'V^'. : diplomatically as possible, and st i l l - t ry to f u l f i l l our responsibiUtiesi^ } And for your interest, we Tiave tried to approach" this particular problem in at least three ways: In the f i rst place, the Army. Medical Service • : and the Navy Medical Service have invited to their courses in 'the problems^'/ in nuclear .warfare - not only our reserves, but also, representatives^of-those medical personnel engaged in civil defence activities, as well as Vepreseh-". . tatives from our medical schools. Secondly, we have organized teams and'are . holding-programmes in our large medical centres dealing with a l l of the 'Y problems from the f irst aid that one must given oneself-or to one's nsigfr-.y' •-. bour—something that has been mentioned several times; the' f i r s t aid tbatCV; :
must bs given by -trained nedical personnel, triage, evacuation^ and f inal ly,^ plans of not only military, but civilian hospitals, .to me e t a terrif ie flux of casualties. - .-.y
• Two Other professional problems are dealt with in the Sameyj; programme) namely,, the new principles which one must apply,in the,treat-''i^J*'-ment of casualties coming from-nuclear weapons; and the problem, which General . Norstad mentioned—namely, ,howto. deal with the psychological^, "•/.^2-problems which may be of eve»' mbre-tremendous importance than the p h ^ ^ ^ ' i M -sical; and thirdly, we have established in, some of our medical y Schoolsj-,, ,-and we hope to establish ,it in a l l - what we call the firoflysaftf -of, Medicals. •
I • • • V -' • .., • . .: I, .
, 176 ' ..;.: .: .,-
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE

^NATOTdMDbfTBai » I il l
Education for Katlonal Dcfonce. The teaching in this particular course is done by the various departments already existing in the schools. And we Jiope that in the Aitxire our physicians who are graduated and who have coupleted their internship will be able inmediately to take their place either in the military or in the broad field of civil defence.
Our next greatest problem has to do with the latter subjects; how much responsibility must we take or will we have to take in the field of civil defence? As you know, in our country i t has been decided that this is a civil problem and that it will be carried out by civilian personnel. And yet, as has been pointed out here and was exploited nicely yesterday, there is no question, I'm sure, in the minds of any person present, but what the military will be compelled to assist in this problem. Actually, it may be of such importance as to influence the battle itself . And I'm -very happy to report to you that Dr, Gushing, who informed me during this conference, that our Chief Executive has Just appointed a Camnittee of our top secretaries in the appropriate branches of our Executive Department to give us the guidance in this Miole problem of civil defence. We understand that the medical will be very strongly con- ' sidered.
I want to express for a l l the delegates from the DSA our deep appreciation, General Hall, to you and your colleagues. I think, that a l l feel that this has been a most profitable conference and I'm'sure that we'll look forward in our country to another invi-tation to a similar conference next year.
Thank you so much.
L
GEMERAL HALLs
The Chairman, after thanking General Armstrong for his ~ ranarks, said that the U,S. Army Medical Services, under General Armstrong, had given the most valuable support to the SHAPE Staff over the past four years. General Armstrong was about to retire from the Service, not to rest, but to'undertake an even bigger job at' Kew Yoric University, and he would take with him the best wishes and gratitude of the SHAPE Staff, and of a l l present at the Conference.
After thanking General Reilinger, as the Senior FTendt representative present for the hospitality which France and Paris had always shown SHAPE and the NATO Nations, the Chairman declared the Conference closed.
»»»MWWBMM H * * * * * * * *
* * * * * *
177
DE
CLA
SSIF
IED
- PU
BLI
CLY
DIS
CLO
SED
- P
DN
(201
2)00
08 -
DÉ
CLA
SSIF
IÉ -
MIS
EN
LE
CT
UR
E P
UB
LIQ
UE