2007 perugia, università di medicina. quale terapia nelle channelopatie
TRANSCRIPT

Quale terapia Quale terapia nelle Channelopatie ? nelle Channelopatie ?
Stefano Nardi MD, PhD
AZIENDA OSPEDALIERA SANTA MARIA TERNIAZIENDA OSPEDALIERA SANTA MARIA TERNIDIPARTIMENTO CARDIOTORACOVASCOLAREDIPARTIMENTO CARDIOTORACOVASCOLARE STRUTTURA COMPLESSA DI CARDIOLOGIA STRUTTURA COMPLESSA DI CARDIOLOGIA
UNITA’ OPERATIVA DI ARITMOLOGIA CARDIACA UNITA’ OPERATIVA DI ARITMOLOGIA CARDIACA

THE PROBLEM
Arrhythmogenic Hereditary Syndromes Arrhythmogenic Hereditary Syndromes (ARVD, CPVT, LQTcS, SQTcS, Brugada)(ARVD, CPVT, LQTcS, SQTcS, Brugada)are inherited arrhythmogenic diseasesare inherited arrhythmogenic diseases
Some concepts applied for risk stratificationSome concepts applied for risk stratificationare common to the different inherited syndromesare common to the different inherited syndromes
Share genetically determined Susceptibility Share genetically determined Susceptibility to VTs and Sudden Cardiac Deathto VTs and Sudden Cardiac Death
in the absence of recognizable structural HDin the absence of recognizable structural HD
RisK Stratification
• Wide Spectrum of underlined substrate
• Different combination between ARRHYTHMIA and SUBSTRATE with different Clinical Presentation and Risk
THE PROBLEM
SUBSTRATESUBSTRATE
• ARVD
• Cathecolaminergic Polimorfic VTs
• Brugada Syndrome• QT long Syndrome• QT short Syndrome
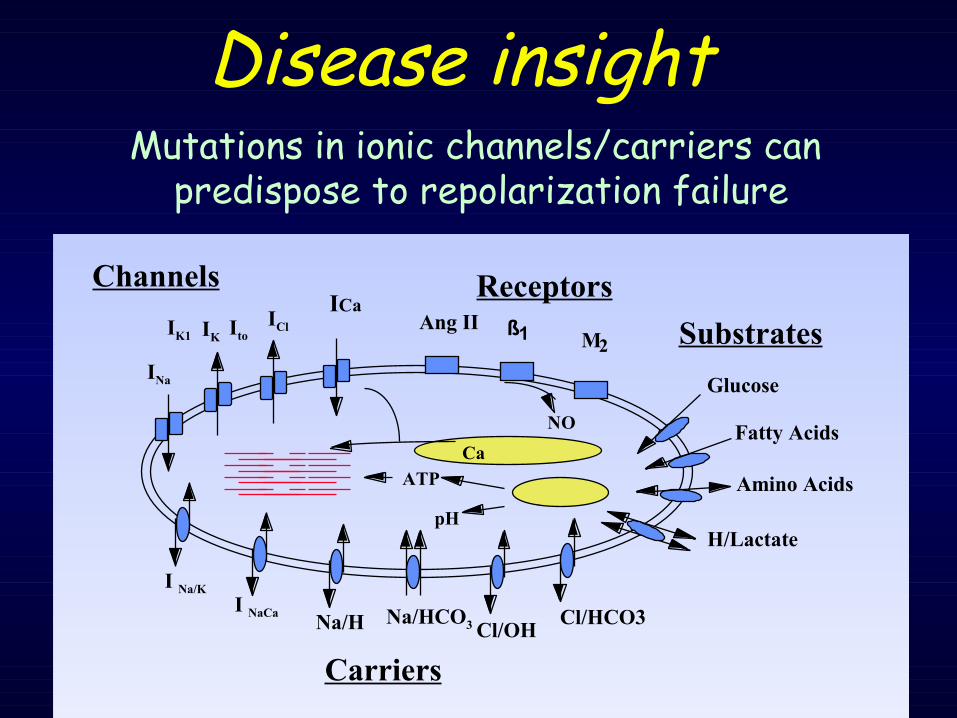
INa
IClIK1 IK Ito
ICaChannels
I Na/K
I NaCaNa/H Na/HCO3 Cl/OH
Cl/HCO3
Carriers
Ca
pH
ATP
Glucose
Fatty Acids
Amino Acids
H/Lactate
SubstratesAng II1
2
NO
ßM
Receptors
Disease insightMutations in ionic channels/carriers can
predispose to repolarization failure

The problem

The problemThere are around 35,000 genes in the Human Genome
Coding > 100,000 proteins
We know the function of only a very small proportion – genes or proteins
Yet most biological functions depend on many genes & proteins interacting
organism organtissue
cellular sub-cellularpathwaysprotein
gene

T waves flattened, inverted (esp in V1-V3)
Precordial QRS prolongation
ε waves (small amplitude pot. at start of ST – “intrav. myocardial defect”)
Perception of Problem

• QTC 470 ms.
Perception of Problem
Magnitude
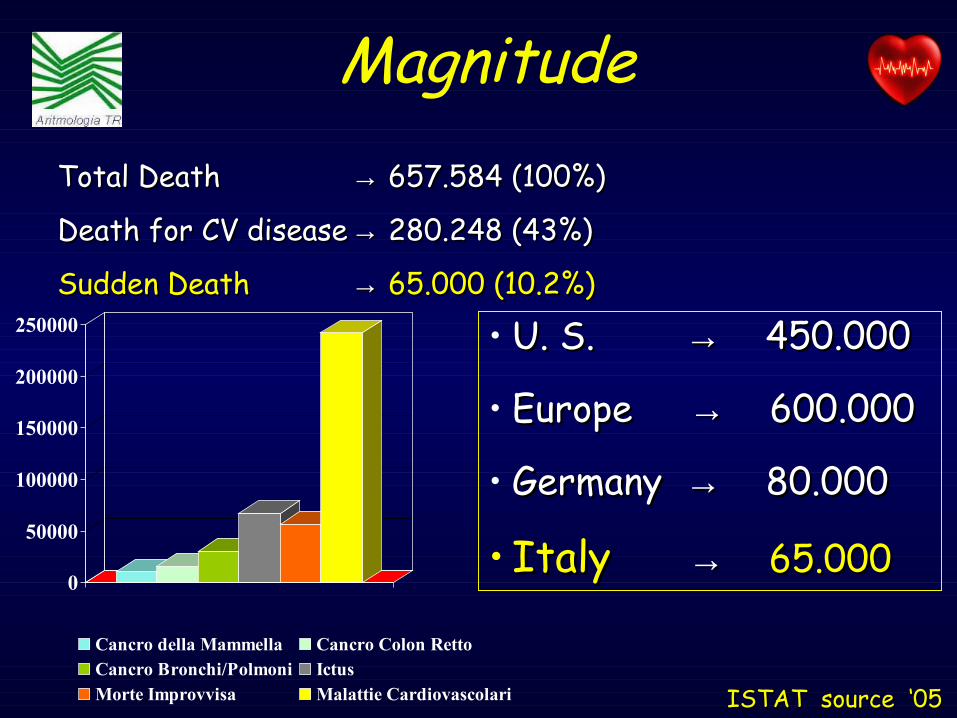
• U. S. U. S. →→ 450.000 450.000
• Europe Europe →→ 600.000 600.000
• Germany Germany →→ 80.000 80.000
• ItalyItaly →→ 65.00065.000
ISTAT source ‘05ISTAT source ‘05
0
50000
100000
150000
200000
250000
Cancro della Mammella Cancro Colon RettoCancro Bronchi/Polmoni IctusMorte Improvvisa Malattie Cardiovascolari
Total Death Total Death →→ 657.584 (100%) 657.584 (100%)
Death for CV diseaseDeath for CV disease →→ 280.248 (43%) 280.248 (43%)
Sudden DeathSudden Death →→ 65.000 (10.2%)65.000 (10.2%)
Magnitude

Magnitude and Etiology of SCD
° ion-channel abnormalities
15% CM
5% °
4 Zheng Z. Circulation. ‘01
Data on the natural history are potentially biased by the fact that it is more likely that a highly symptomatic case is referred to a registry
80% CAD
Esiste un modo per stratificare i pazienti?
La maggior parete dei soggetti che SPERIMENTA un Arresto Cardiaco non sopravvive
per poterlo raccontare

BradiaritmiaBradiaritmia15-20%15-20%
VT/VF 75-80%VT/VF 75-80%
EMD 5%EMD 5%
Ritmo registrato nei pz Ritmo registrato nei pz risuscitati ad arresto risuscitati ad arresto cardiaco extraospedaliero cardiaco extraospedaliero o nei pazienti deceduti o nei pazienti deceduti improvvisamente durante improvvisamente durante registrazione Holter registrazione Holter
Cummins RO, Annals Emerg Med. ‘89Albert CM. Circulation ‘03
Bayés de Luna A. Am Heart J. ‘89
DIMENSION of PROBLEM

Esiste oggi una strategia diagnostica e terapeutica che può essere considerata il GOLD STANDARD nelle CARDIOPATIE
ARITMOGENE ?
Quali sono le INDICAZIONI univocamente ACCETTATE ?

• Non esistono Non esistono TRIALS RANDOMIZZATI TRIALS RANDOMIZZATI a a supporto delle attuali indicazionisupporto delle attuali indicazioni
• Le indicazioni proposte son prevalentemente Le indicazioni proposte son prevalentemente
basate su basate su STUDI RETROSPETTIVI STUDI RETROSPETTIVI o piccoli o piccoli STUDI PROSPETTICI STUDI PROSPETTICI (level B) o sull’opinione (level B) o sull’opinione degli degli ESPERTIESPERTI (level C) (level C)
• I criteri di stratificazione non sono ben definitiI criteri di stratificazione non sono ben definiti
… … il PRESENTE …il PRESENTE …
Priori S - Eur Heart J ‘01
• La revisione sintetica dei dati raccolti dalla Task Force della ESC ci ha fornito delle raccomandazioni (NON LINEE GUIDA !!!) in base alla EBM che coinvolgono la fase diagnostica e terapeutica dell’approccio alla morte improvvisa
… … il PRESENTE …il PRESENTE …
orienta l’investigatore circa la strategia da utilizzare nei singoli casi!
Priori S - Eur Heart J ‘01

• “ARVC” proposed in 1977 by Fontaine• Occurs in teenagers and young adults (>80% diagnosed by age 40)
– Rarely in early childhood
• INCIDENCE: unknown (6/10000 ???)
• PREVALENCE: unknown
• Italian study - 20% of postmortem SD in pts < 35 ys old and 25% in young athletes (one of the major causes of SCD in pre CAD age) • Incidence 1:~5,000
1:5000
ARVD

• Degeneration • Inflammatory• Infectious• Myocarditis • Apoptosis • Trans-differentiation
Etiology
I Ca 2+
43
66
47
22
81
45 48
69
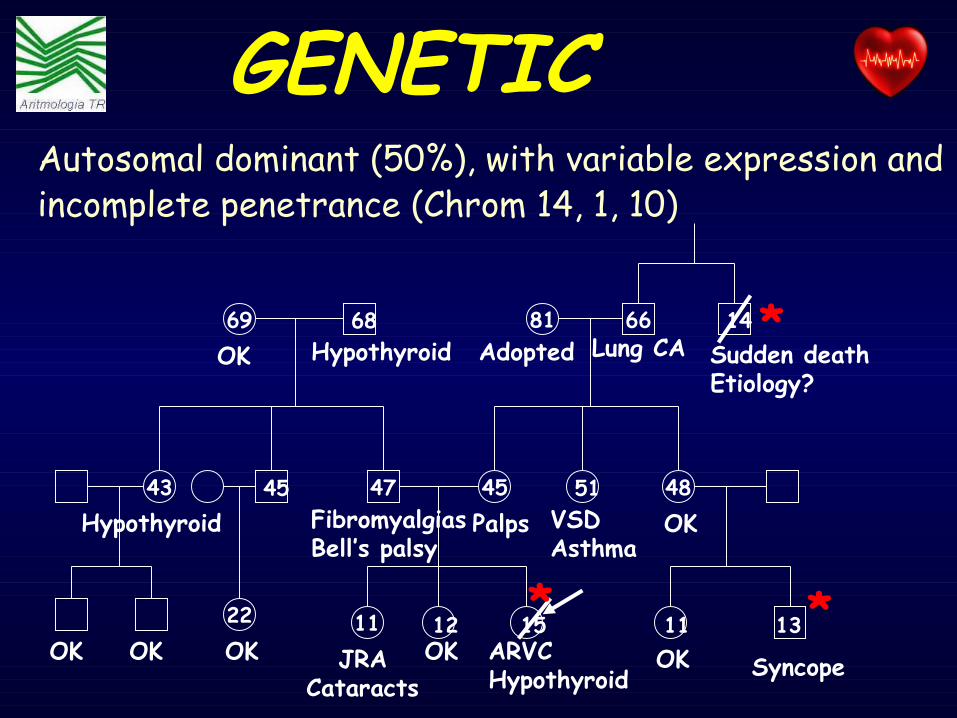
11 12 15JRA
CataractsSyncope
1311
Adopted Lung CA Sudden deathEtiology?
VSDAsthma
Hypothyroid FibromyalgiasBell’s palsy
Hypothyroid
45 51
1468
ARVCHypothyroid
OK OK OK OK
OK
Palps OK
OK
* *
*
Autosomal dominant (50%), with variable expression and incomplete penetrance (Chrom 14, 1, 10)
GENETIC

CLINICALPRESENTATION
• PALPITATIONS (67%)• Sincope (29%)• Cardiac Arrest (7-23%)• Chest Pain (27%)• Dispnea (11%) • ASIMPTOMATICS (?)
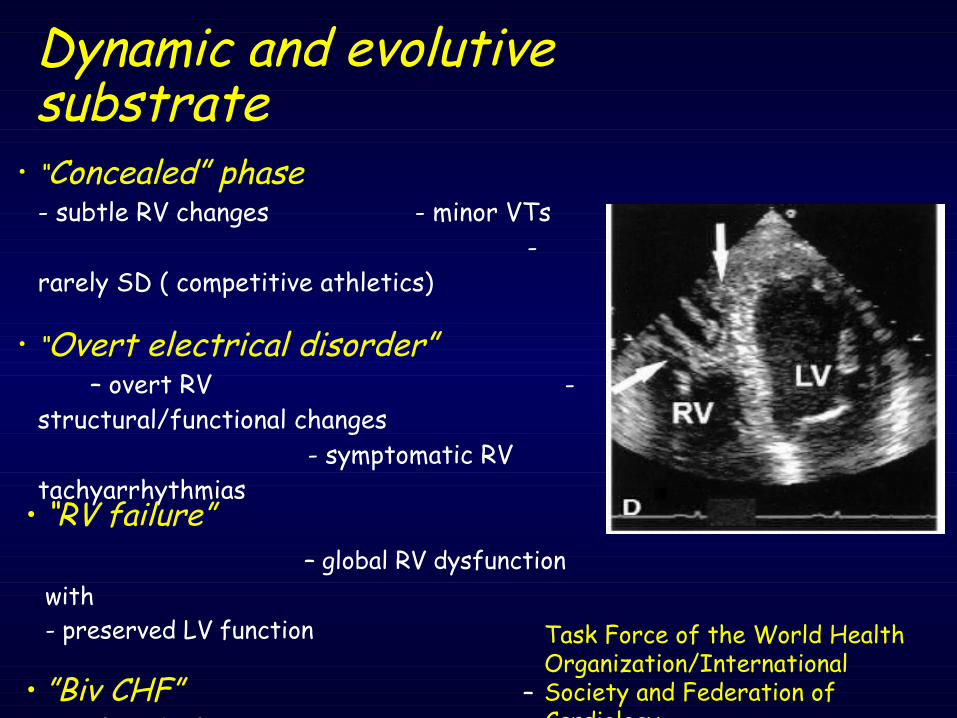
• “Concealed” phase - subtle RV changes - minor VTs
- rarely SD ( competitive athletics)
• “Overt electrical disorder” – overt RV - structural/functional changes - symptomatic RV tachyarrhythmias
• “RV failure” – global RV dysfunction with - preserved LV function
• ”Biv CHF” – signif LV dysfunction
Task Force of the World Health Organization/International Society and Federation of Cardiology
Dynamic and evolutive substrate
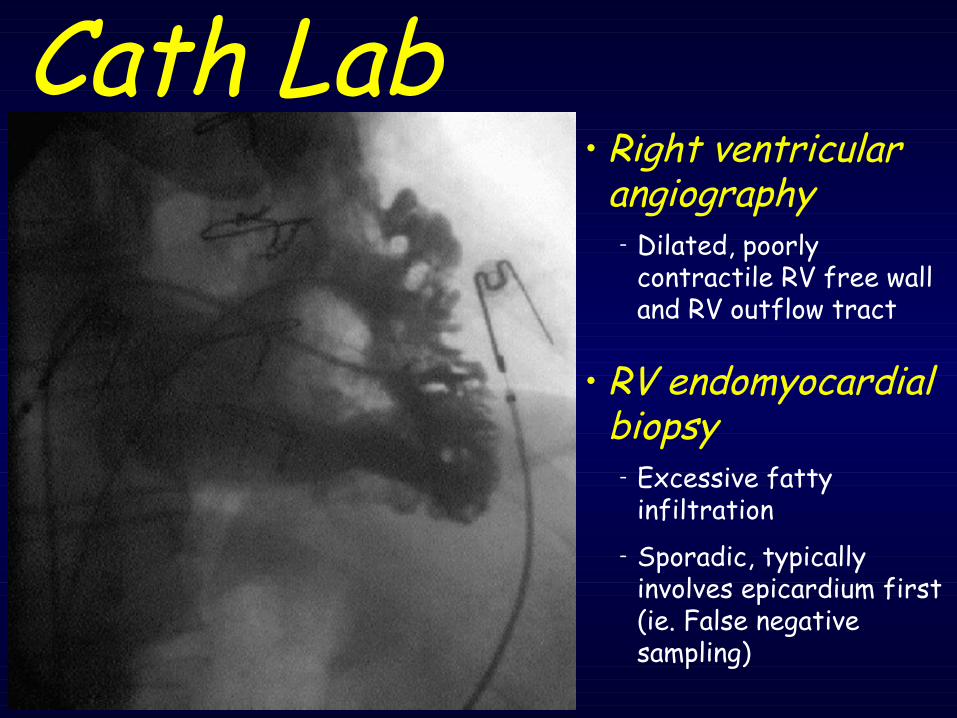
Cath Lab• Right ventricular
angiography– Dilated, poorly
contractile RV free wall and RV outflow tract
• RV endomyocardial biopsy
– Excessive fatty infiltration
– Sporadic, typically involves epicardium first (ie. False negative sampling)

a) enlargement of the RV
b) regional RV wall motion abnormalities or aneurysms.
c) Presence of fat and fibrosis
the definitive TEST ?
MRI

METHODOLOGICAL ASPECTS
Typical ECG, VTs and Structural/Functional RV Typical ECG, VTs and Structural/Functional RV abnormalities represent only one EXTREME abnormalities represent only one EXTREME
of the disease spectrum of the disease spectrum
Clinically silent cases are not recognized because ASYMPTOMATIC
Data on the natural history are potentially biased Data on the natural history are potentially biased because it’s more likely that because it’s more likely that a
HIGHLY SYMPTOMATIC case is referred to a registry
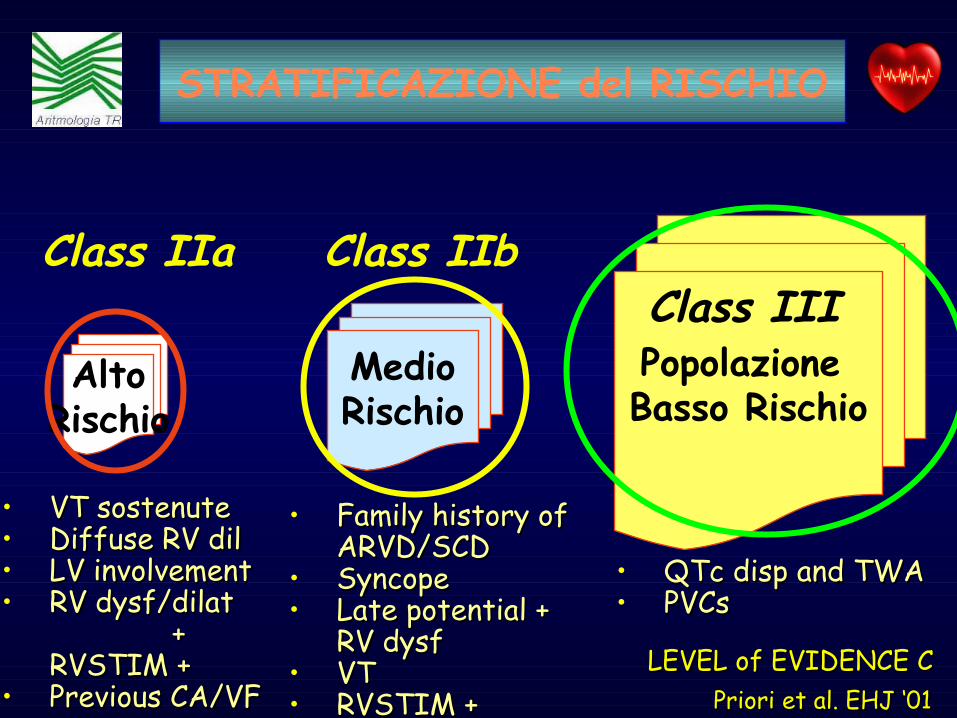
AltoRischio
MedioRischio
Popolazione Basso Rischio
• Family history of Family history of ARVD/SCDARVD/SCD
• SyncopeSyncope• Late potential + Late potential +
RV dysfRV dysf• VTVT• RVSTIM + RVSTIM +
• QTc disp and TWAQTc disp and TWA• PVCs PVCs
Class IIa Class IIbClass III
Priori et al. EHJ ‘01Priori et al. EHJ ‘01
• VT sostenuteVT sostenute• Diffuse RV dilDiffuse RV dil• LV involvementLV involvement• RV dysf/dilat RV dysf/dilat
+ + RVSTIM +RVSTIM +
• Previous CA/VF Previous CA/VF LEVEL of EVIDENCE CLEVEL of EVIDENCE C
STRATIFICAZIONE del RISCHIO

• Il valore PREDITTIVO dei MARKERS non è stato definito in studi prospettici su larga scala
• I dati riportati sono basati su PICCOLI STUDI (prevalentemente derivanti da centri terziari nei
quali il paziente era giunto per l’aritmia
• Il PROFILO di RISCHIO dei pts asimptomatici (albero genialogico) NON E’ STATO sistematicamente
VALUTATO
CONSIDERAZIONI

•AADs•Ablation•ICD
Therapeutic Approach

• Limited information are available on Limited information are available on AADs AADs efficacy efficacy (retrospective or “non (retrospective or “non randomized” randomized” prospective studies) prospective studies)
• AADs is often used as primary Rx (level of evidence 2B) (1st Sotalol, 2nd
Amiodaron and β blocker) however this approach is often INEFFECTIVE
AADs
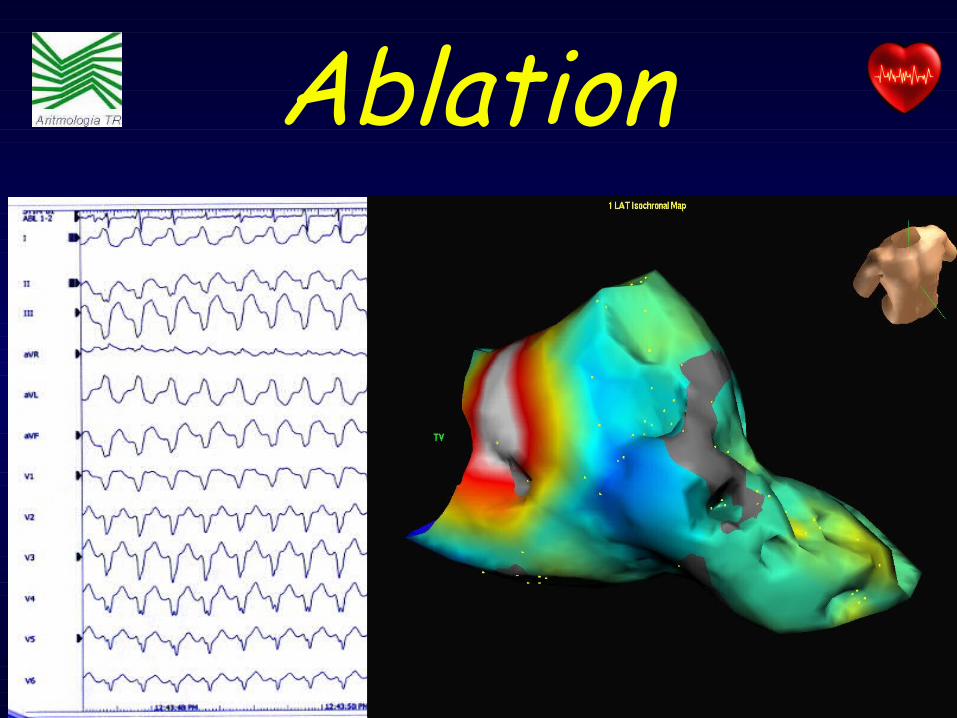
Ablation

Indications•Previous Cardiac Arrest
•Spontaneous and Sustained VT
•Sincope + Inducible VT at EPS
Cost
Efficacy
ICD

• Manifests with VTs, however the initial presenting symptom may be SINCOPE or Sudden Death
• One prevalent Familiar Autosomal Dominant syndrome (Chromosomal locus 1q42-q43 in two families) and one inheritent Autosomal Recessive
• Described in ‘99 by Swan (Coumel ’83 Lenhardt ’95)
• NO ECG abnormalities at rest (QTc normal, no ST segment elevation)
• Stress/Emotion/Exercise induced polymorphic VTs (typical ECG pattern of bi-directional VTs), in absence of detectable structural HD.
CPVT

ARVD2 maps at the same locus of hRyR2 (may represent allelic variants)
hRyR2 located in a region that involve Ca2+ release from the SR in response to the activation of the ICa2+ current through the dihydro/R during the plateau. β-mediated VTs due to “Trigger Activity” during ICa2+ overload (delayed dep)
I Ca 2+CPVT

• Occurs in young, healthy children and young adults • Familiary history of Syncope or SCD 1/3 cases
• INCIDENCE: unknown
• PREVALENCE: unknown
Background
I IIa IIb
•Familiarità SCD•NSVT•Sincope (età pediatrica)
• VF • Sincope
Cathecolaminergic Polimorfic VT
• ECG Holter• Ergometric Stress Test• Isoproterenol Test • EPS• Reveal
DIAGNOSTIC APPROACH

•β bocker•ICD
Cathecolaminergic Polimorfic VT
Therapeutic Approach

• AUTOSOMAL DOMINANT trait, incomplete penetrance and variable expression.
• Genetic defects in the α-subunit of cardiac Na+ channel, (SCN5A)
• Abnormal EP activity in the RV epicardium
BRUGADA syndrome
BRUGADA syndrome
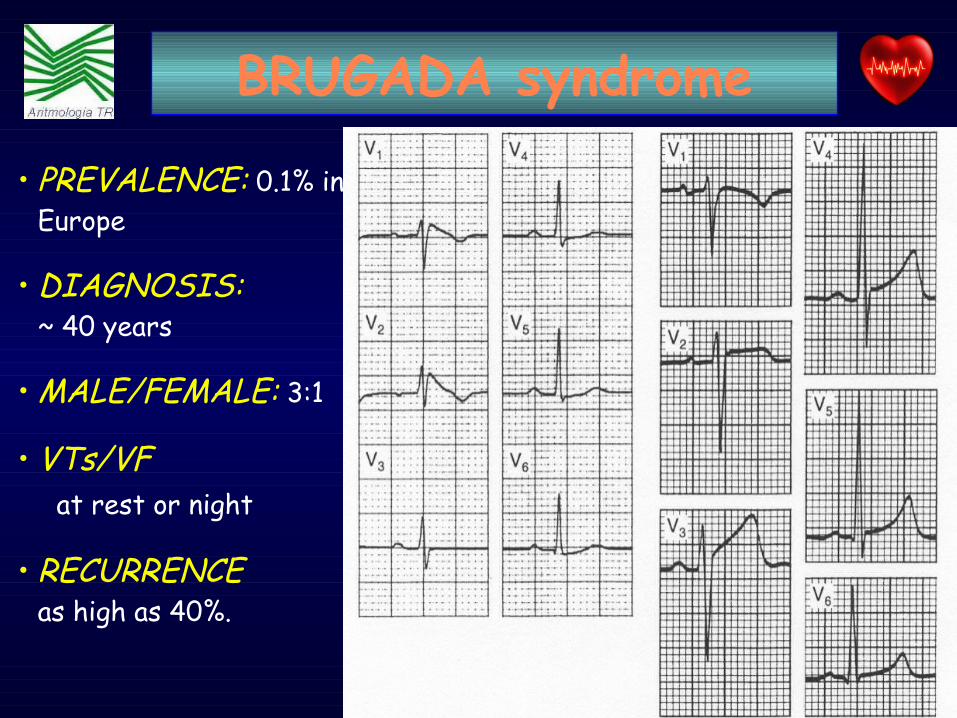
• PREVALENCE: 0.1% in Europe
• DIAGNOSIS: ~ 40 years
• MALE/FEMALE: 3:1
• VTs/VF at rest or night
• RECURRENCE as high as 40%.
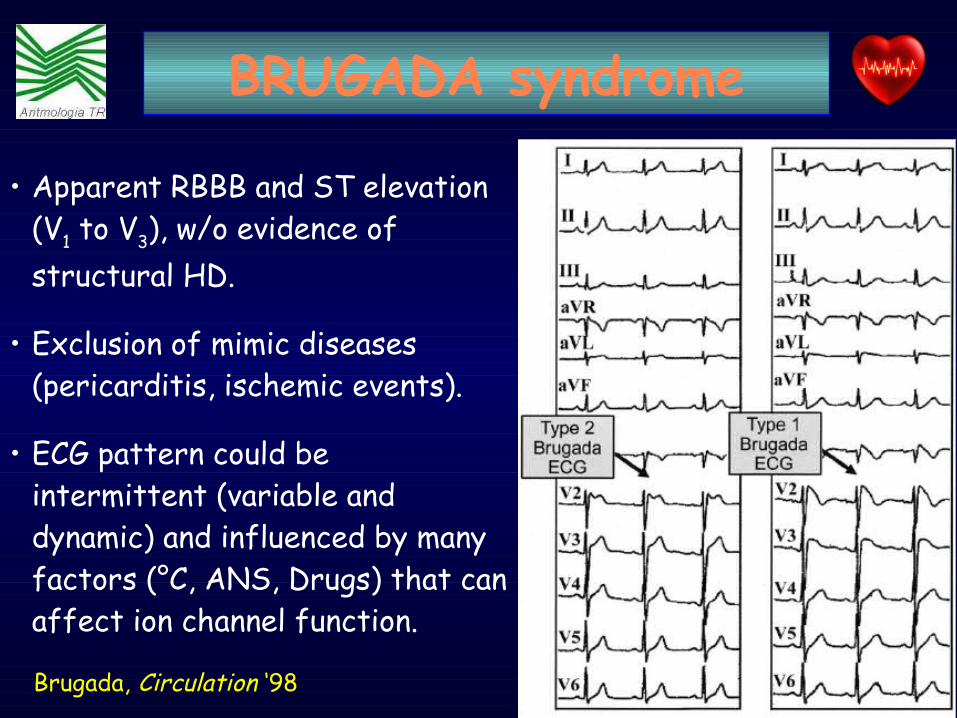
• Apparent RBBB and ST elevation (V1 to V3), w/o evidence of structural HD.
• Exclusion of mimic diseases (pericarditis, ischemic events).
• ECG pattern could be intermittent (variable and dynamic) and influenced by many factors (°C, ANS, Drugs) that can affect ion channel function.
BRUGADA syndrome
Brugada, Circulation ‘98

• Provocative test with Na+ channel blockers proposed to unmask the diagnostic ECG pattern.
– Ajmaline (1mg/kg IV) or– Flecainide (2mg/kg IV) or– Procainamide (10mg/kg IV) as a bolus over 10 m’.
– ST-segment further elevation > 2 mm
SCN5A

Brugada - Circulation ‘05
547 “coved type”
124 Sincope 170
Routine
253 Familiarità
391 Spointanei
156 dopo ajmalina
28±42 mesi Follow Up45 (8%) eventi
Età media 40 aa
BRUGADA syndrome
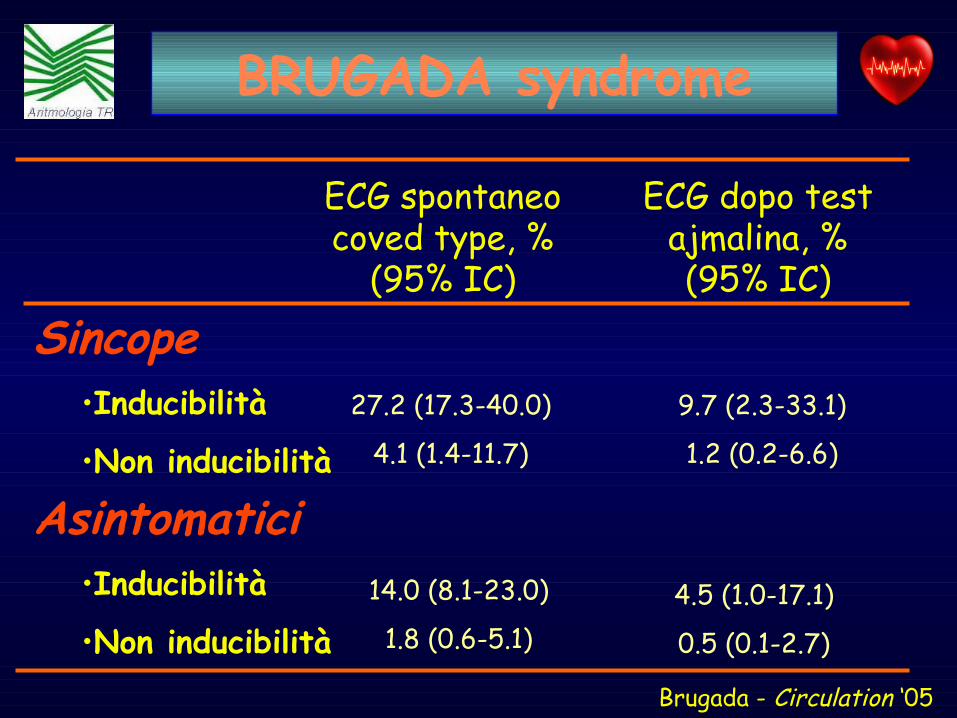
Brugada - Circulation ‘05
ECG spontaneo coved type, %
(95% IC)
ECG dopo test ajmalina, % (95% IC)
Sincope•Inducibilità
•Non inducibilità
Asintomatici•Inducibilità
•Non inducibilità
27.2 (17.3-40.0)
4.1 (1.4-11.7)
4.5 (1.0-17.1)
0.5 (0.1-2.7)
14.0 (8.1-23.0)
1.8 (0.6-5.1)
9.7 (2.3-33.1)
1.2 (0.2-6.6)
BRUGADA syndrome

• Storia di sincope
• Un episodio di arresto cardiacoICD
• Ma qual è il RISCHIO degli altri pazienti?
BRUGADA syndrome
Analisi di REGRESSIONE LOGISTICA: Sincope sufficiente rischio da giustificare un ICD (1.2 % -27.2 %)

Possibile strategia “insertable LR + ICD esterno”
Alto rischioRapporto di rischio: 6.4
Rischio intermedio Rapporto di rischio: 2.1
Basso rischio
Priori et al - Circulation ‘02
Rischio
Sincope e pattern
ECG positivo
Pattern ECG positivo
Pattern ECG negativo con o senza sincope
Percentuale popolazione
10 %
41 %
49 %ICD
Terapie
Ulteriori controlli in caso di sintomi
BRUGADA syndrome

•NON ESISTE una terapia medica di sicura e documentata efficacia.
• ICD funziona in pazienti che SVILUPPANO o SVILUPPERANNO una VF
• Altrimenti ……….. tutti i rischi dell’impianto e nessun beneficio
BRUGADA syndrome
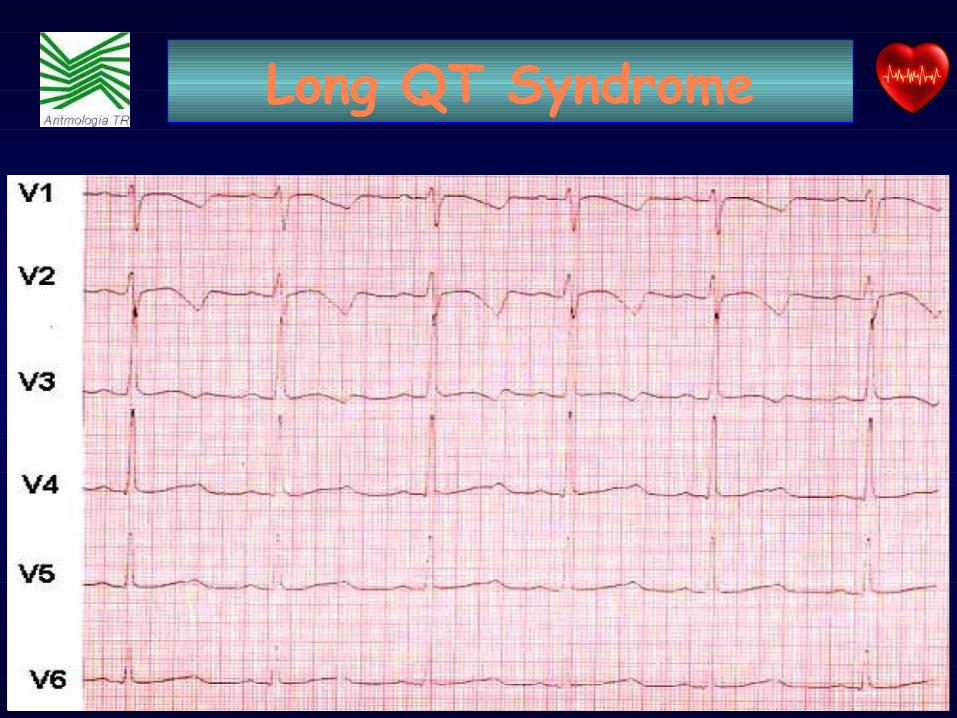
• Primary electrical disorder with BROAD SPECTRUM• NO macroscopic EVIDENCE of structural HD• PROLONGED QTc interval• DEFORMATION of T wave/presence of U wave• STRESS MEDIATED life-threatening VTs• One variant AUTOSOMAL RECESSIVE (J-LN)• One prevalent AUTOSOMAL DOMINANT (RW)
• Estimated PREVALENCE 5/10.000 (0,5/1000)
Long QT Syndrome

LQTS Type
Chromosomal Locus
Mutated Gene Ion Current
AffectedLQT1 11p 15.5 KVLQT1 IKs
LQT2 7q 35-36 HERG IKr
LQT3 3p 21-24 SCN5A INa
LQT4 4q 25-27 ? ?LQT5 21q 22.1-22.2 KCNE1
(heterozygotes)IKs
LQT6 21q 22.1-22.2 MiRP1 IKr
Long QT Syndrome
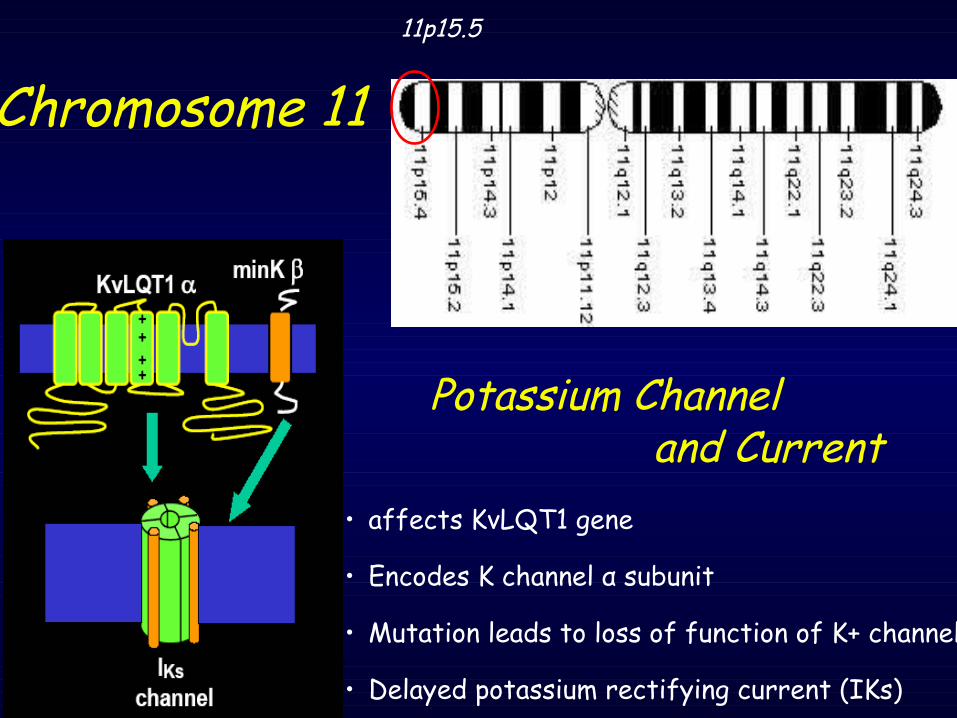
Chromosome 1111p15.5
Potassium Channel and Current
• affects KvLQT1 gene
• Encodes K channel α subunit
• Mutation leads to loss of function of K+ channel
• Delayed potassium rectifying current (IKs)
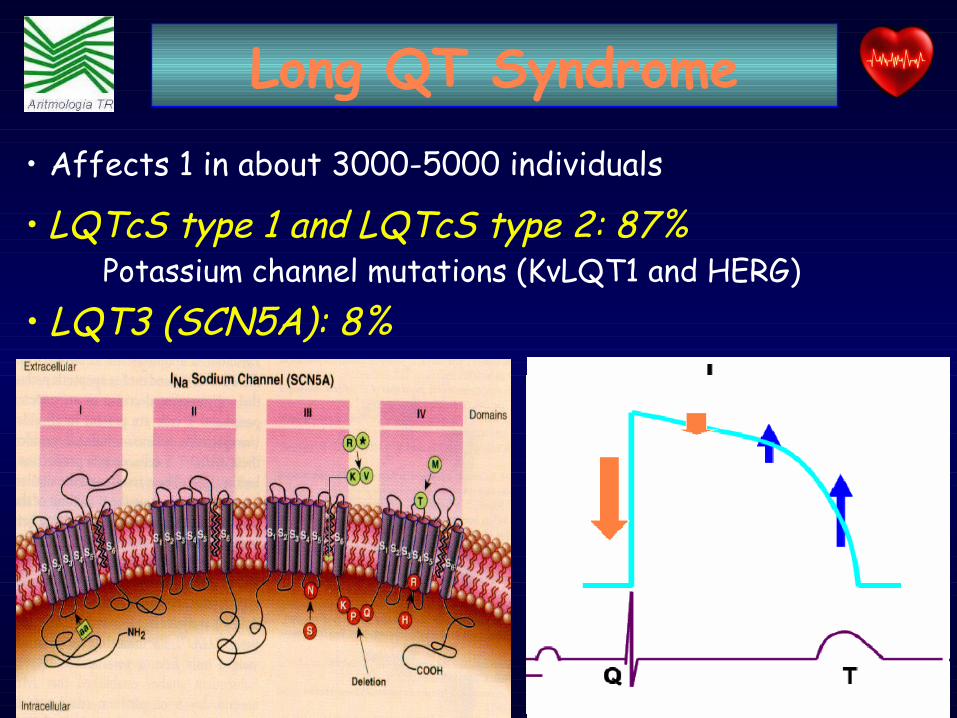
• Affects 1 in about 3000-5000 individuals
• LQTcS type 1 and LQTcS type 2: 87% Potassium channel mutations (KvLQT1 and HERG)
• LQT3 (SCN5A): 8%
Long QT Syndrome

• LQT1 (IKs) is more susceptible to cardiac events occurring during exercise (particularly swimming)
• LQT2 (IKr) is more susceptible to cardiac events occurring during rest or emotion (characteristically
acoustic stimuli)
• LQT3 carrying mutations in the SCN5A (cardiac Na channel) is susceptible to cardiac events occurring at rest and during sleep
Long QT Syndrome

• Any QTc > 440 msec is considered prolonged
What is borderline QT ?What is borderline QT ?
• A QT between 450 to 470 msec is considered borderline
• The average QTc for who has L-QTS is 490 msec
• A QTc ≥ 480 msec in females or 470 msec in males, is probably a sign for L-QT S, in the absence of drugs, electrolyte disturbance, or other conditions that might independently lengthen the QT-interval.
Long QT Syndrome

≥ 50 %
30-49%
< 29%S. Priori, NEJM ‘03
Probabilità di evento cardiaco prima dei 40 anni e prima della tx (sincope, CA, SCD)
QTc≥500 msLQT1LQT2
M, LQT3
QTc<500 msF, LQT2F, LQT3M, LQT3
QTc≥500 msF, LQT3
QTc < 500 msM, LQT2
LQT1
Risk Stratification
Long QT Syndrome
LEVEL of EVIDENCE B

I IIa IIbClasse•QTc > 600ms•Evento Cardiaco nei neonati•Post-partum•Sind + BAV •Alternanza onda T•Sesso Femminile
• TdP / VF / AC• Sincope• JLN• LQT3
• Familiarità di SCD∀↑ Dispersione del QT
Priori et al. Eur Heart J ‘01Priori et al. Eur Heart J ‘01
STRATIF RISCHIO
Long QT Syndrome

Indicazioni Indicazioni CONSOLIDATECONSOLIDATE
• Sopravvissuti a MI
• TV sostenute spontanee
• Sincope + TV inducibile
ICD
Costo
Beneficio

Indicazioni Indicazioni CONSOLIDATECONSOLIDATE
• Sopravvissuti a MI
• TV sostenute spontanee
• Sincope + TV inducibile
• I-DCM - Riduzione LVEF - NSVT - Sincope
EMERGENTIEMERGENTI
• ARVD
• Cathecolaminergic Polimorfic VTs
• Brugada Syndrome• QT long Syndrome• QT short Syndrome
ICD
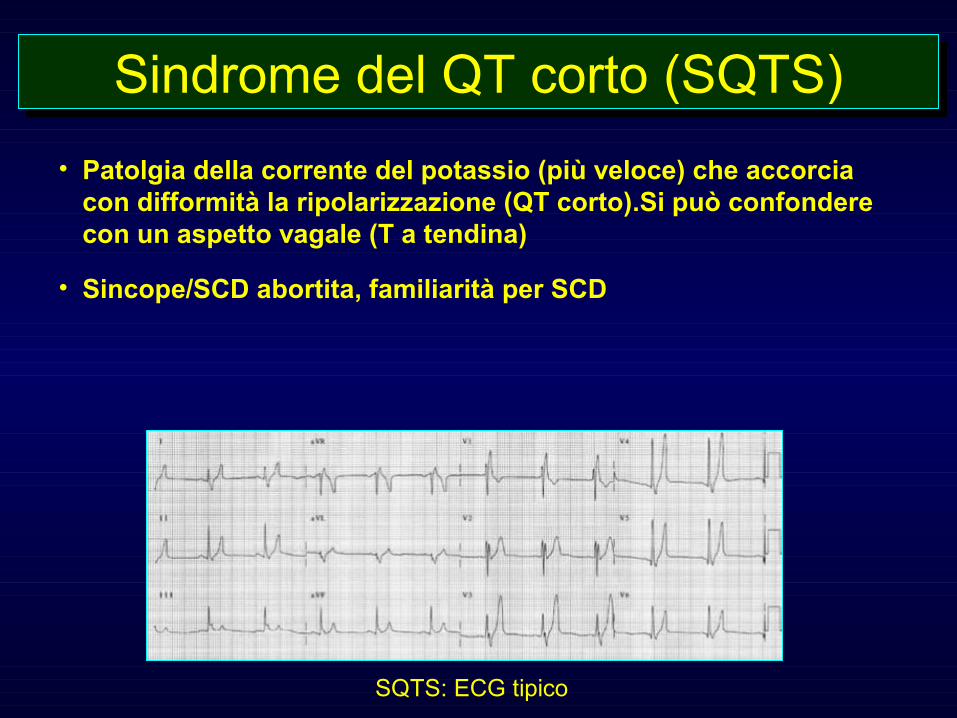
• Patolgia della corrente del potassio (più veloce) che accorcia con difformità la ripolarizzazione (QT corto).Si può confondere con un aspetto vagale (T a tendina)
• Sincope/SCD abortita, familiarità per SCD
Sindrome del QT corto (SQTS)Sindrome del QT corto (SQTS)
SQTS: ECG tipico
•Diagnosi: •Clinica, ECG, laboratorio (escludere acidosi,iperkaliemia, ipercalcemia), genetica
•Terapia: •ICD (+ chinidina)•Chinidina (pediatrici)
Sindrome del QT corto (SQTS)Sindrome del QT corto (SQTS)

– Vincoli metodologici legati ai filtri a maglie strette della EBM, determinano il fatto che strategie terapeutiche che prevedono l’impiego dell’ICD sono confinate a popolazioni limitate (costo) e selezionate (rischio elevato MI), con conseguente generazione di ipotesi di lavoro forzate
… … il PRESENTE …il PRESENTE …
CONSEGUENZA: possibile mancanza di verifica legata ai vincoli!

… … il PRESENTE …il PRESENTE …• Tale condizione rende di DIFFICILE realizzazione
una indagine SISTEMATICA circa gli effetti delle strategie profilattiche e terapeutiche nelle specifiche condizioni.
• La maggioranza delle considerazioni estrapolate dai dati a nostra disposizione NON sono SEMPRE TRASFERIBILI direttamente a pazienti che malgrado segni e sintomi di uguale espressione, presentano condizioni di base profondamente DIVERSE.

STRATIFICAZIONE del RISCHIO
AltoRischio
MedioRischio
Popolazione Basso Rischio
In quale popolazione esiste un REALE BENEFICIO ????

Age and Sex
Prolonged QTc (sec)
Reference Range (sec)
Children (< 15 y)
> .46 < .44
Adult Males
> .45 < .43
Adult Females
> .46 < .45
Long QT Syndrome
Ma qual è il GRADO di RISCHIO ?????


Heart sodium channel mutationsgreen : IVF mutations red : long QT mutations
(Chen et al, Nature, 19 March 1998)

PROBLEMA 1:la funzione di ogni singolo gene non e`specificata nel linguaggio del DNA
PROBLEMA 2: ogni singolo GENE puo` giocare un ruoloimportante in funzioni MULTIPLE
PROBLEMA 3: ogni singola funzione presuppone la cooperazione di molti geni
PROBLEMA 4 :una determinata funzione dipende anche da importanti proprieta`, NON specifiche dei geni
Noble D ’02 Phys News ‘02

RISK stratification
AltoRischio
MedioRischio
Popolazione Basso Rischio
In quale popolazione esiste un REALE BENEFICIO ?
Patologie EMERGENTIPatologie EMERGENTI
• Brugada syndrome• ARVD• CPVT• QTLS
QUAL’ E’ IL RISCHIO QUAL’ E’ IL RISCHIO DI MORTE NELLEDI MORTE NELLECHANNELOPATIECHANNELOPATIE
??

Total DeathTotal Death →→ 557.584 (100%) 557.584 (100%)
Death for CV diseaseDeath for CV disease →→ 242.248 (43%) 242.248 (43%)
Sudden DeathSudden Death →→ 57.000 (10.2%)57.000 (10.2%)
ISTAT source ‘00ISTAT source ‘00
0
50000
100000
150000
200000
250000 Cancro dellaMammellaCancro ColonRettoCancroBronchi/PolmoniIctus
Morte Improvvisa
MalattieCardiovascolari
Mor
ti p
er a
nno
DIMENSION of PROBLEM


PERCEZIONE del PROBLEMA

PRESENTAZIONE CLINICA
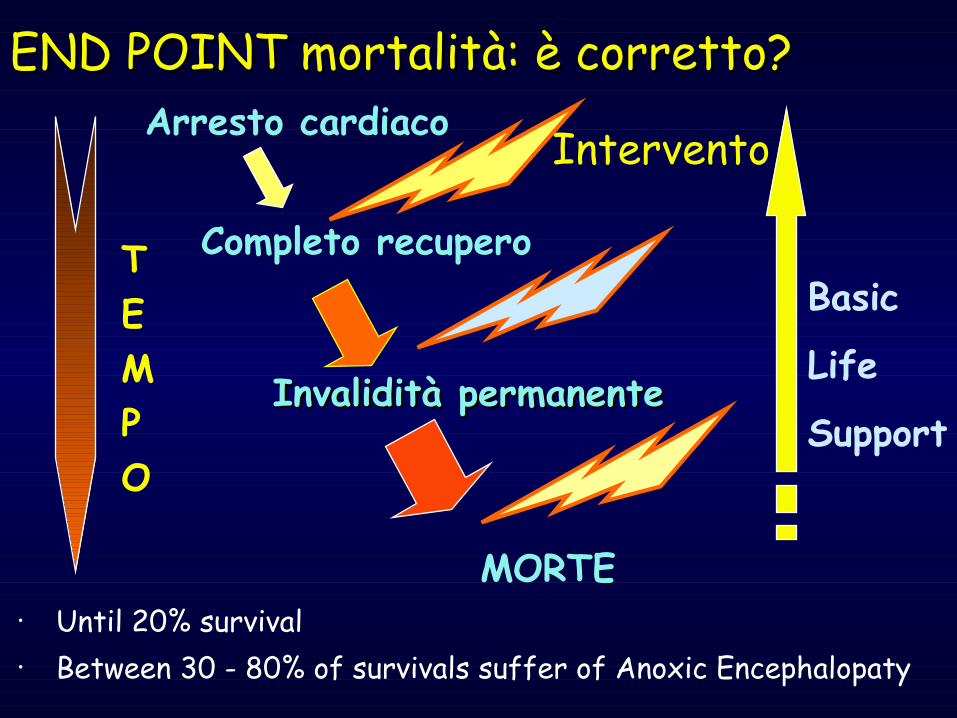
END POINT mortalità: è corretto?END POINT mortalità: è corretto?Arresto cardiaco
Completo recupero
Intervento
Invalidità permanenteInvalidità permanente
MORTE
Basic
Life
Support
TEMPO
• Until 20% survival • Between 30 - 80% of survivals suffer of Anoxic Encephalopaty
Disease that involve Plakoglobin, an intracellular adhesion molecule involved in the apoptosis process (fibro-fatty replacement)
Manifests with VTs, however the initial presenting symptom may be SINCOPE (29%) or CA (7-23%)
Familiar disease with autosomal dominant (50%), with variable expression and incomplete penetrance(Chrom 14, 1, 10)
ARVD
Task Force of the World Health Organization International Society and Federation of Cardiology

SCN5A
• ECGs can normalize over time. A completely normal ECG in one moment doesn’t mean it will always be normal.
• If the ECG ever becomes abnormal, you then FU with AADs, then EP testing (EPS).
Clinical decision making
BRUGADA syndrome
• In all pts where we had genetic confirmation of the disease, we did not have a single false negative or false positive with Flecainide
• The Flecainide test was consistently reproducible

Indication for ICD– symptomatic Brugada syndrome patients including syncope, cardiac arrest or documented VT
– Asymptomatic individuals with a positive ECG and a family history of sudden death and/or inducible during electrophisiological study
Clinical decision making
BRUGADA syndrome

Asymptomatics • In every single patients, if the base ECG is abnormal, then we follow with EP testing.
• In these pts, 2/3 are non-inducible.
• If non-inducible, we do a Genetic test
• If Genetic test is negative, we do nothing, because the event rate is extremely low.
• Events in asymptomatic pts with abnormal basal ECG occurred in pts who were inducible by EP testing.
BRUGADA syndrome

Stratificazione del rischio
Letalità patologia
Vantaggio dell’ICD
Costo
Beneficio
Per la serie: le ultime parole famose... Maggiore è il rischio di MORTE ARITMICA
Maggiore il beneficio dell’ICD

Se è difficile la corretta stratificazione di patologie ad alta prevalenza nella
popolazione generale
... che richiede TEMPO e COLLABORAZIONE
Stratificare il rischio in patologie (relativamente ) rare diventa un obiettivo ...
… … il PRESENTE …il PRESENTE …
• Non esistono Non esistono TRIALS RANDOMIZZATI TRIALS RANDOMIZZATI a a supporto delle attuali indicazionisupporto delle attuali indicazioni
• Le indicazioni proposte son prevalentemente Le indicazioni proposte son prevalentemente
basate su basate su STUDI RETROSPETTIVI STUDI RETROSPETTIVI o piccoli o piccoli STUDI PROSPETTICI STUDI PROSPETTICI (level B) o sull’opinione (level B) o sull’opinione degli degli ESPERTIESPERTI (level C) (level C)
• I criteri di stratificazione non sono ben definitiI criteri di stratificazione non sono ben definiti
• La diagnosi e` spesso La diagnosi e` spesso CASUALE CASUALE
… … il PRESENTE …il PRESENTE …
• Non esistono evidenze circa l’efficacia, nella prevenzione della mortalità (totale ed improvvisa)
per nessuno degli AADs
• Storicamente, impiego clinico diffuso non validato per alcune categorie in alcune forme
(ß-bloccanti in LQTS)
… … il PRESENTE …il PRESENTE …

The severity of the EKG phenotipe The severity of the EKG phenotipe is generally a marker of increased risk of SCD is generally a marker of increased risk of SCD
In the BRUGADA syndrome by the spontaneousIn the BRUGADA syndrome by the spontaneouspresence of ST segment elevation in the presence of ST segment elevation in the
Right precordial leads Right precordial leads
In Long QTC Syndromes the “severe” phenotype In Long QTC Syndromes the “severe” phenotype is represented by the presence of ais represented by the presence of a
QTc exceeding 500 ms QTc exceeding 500 ms
In CPVT by VTs induced byIn CPVT by VTs induced byExercise stress test Exercise stress test
… … il PRESENTE …il PRESENTE …

• La revisione sintetica dei dati raccolti dalla Task Force della ESC ci ha fornito delle raccomandazioni (NON LINEE GUIDA !!!) in base alla EBM che coinvolgono la fase diagnostica e terapeutica dell’approccio alla morte improvvisa
orienta l’investigatore circa la strategia da utilizzare nei singoli casi!
… … il PRESENTE …il PRESENTE …

E` Necessario trovare il giusto “link” tra RICERCA e PRATICA CLINICA
… … ed il FUTURO …ed il FUTURO …
Perfezionare le conoscenze sui meccanismi fisiopatologici delle aritmie
Migliorare ulteriormente la fase DIAGNOSTICA

Grazie per la Grazie per la CORTESECORTESE
ATTENZIONEATTENZIONE