2016 opps rule changes - mainehfma€¦ · 2016 opps rule changes maggie fortin, cpc, cpc -h, chc...
TRANSCRIPT

2016 OPPSRule Changes
Maggie Fortin, CPC, CPC-H, CHCSenior Manager
Janet Hodgdon, CPA, CPCDirector
December 2015

OPPS - Talking points
2
• CMS Objectives- Incentivize efficient care- Reduce administrative burden for more accuracy of
payment• Achieve long-term goal to create a single prospective payment for
the entire outpatient encounter by packaging payment for all C–APC services

ALSO:Statutory reduction for failure to meet quality reporting of 2%Wage index to be used will be final IPPSOVERALL DECREASE IN PAYMENTS ESTIMATED AT $133 MILLION
Market Basket 2.4%Multifactor Productivity (.5)%ACA (.2)%Packaged lab issue (2.0)%
Overall update (.3)%
Final Payment Updates

SCH rural adjustment for
outpatient continues at
7.1%
Drugs, biologicals and radio-
pharmaceuticals are set at the ASP plus 6%
Other Updates and Adjustments

OPPS Operational
Updates
5

OPPS
In the 2016 OPPS rule change we continue to see CMS implementing changes to this ever-evolving complex
payment system
CMS continues to revise the “packaging "of items and services to make the system more
prospective
Rework: Composite APC logic
Addition to the new C-APC list
Movement of certain APC weights
Reclassification of current APC groups
Changes and additions to APC status indicators
6

2016 Comprehensive APC
Comprehensive APC definition: a primary service payment inclusive of integral, supportive, dependent and adjunctive services and items
provided to support the delivery of the primary service
This newest APC category recognizes an
additional 10 clinical groups in 2016
Comprehensive APC will be paid a single payment when a primary procedure is performed and all
other services related and reported on the claim will be packaged with
few exceptionsSTATUS INDICATOR J1
7

Comprehensive APC Packaging
8
• Comprehensive APC logic uses the expanded definition of “packaging”
- Payment is packaged for adjunctive and secondary items, services and procedures
• Including diagnostics and treatments*, evaluation and assessments, uncoded ancillary, drugs, supplies and equipment
- Identification of the most costly procedure at the claim level resulting in:
• A single prospective payment
∗ Repetitive, recurring account billing will continue to be allowed; UB-04 Occurrence Span code 74 (IOM 100-04, Section 60)
C-APC Packaging Exclusion • Certain services are excluded from C-APC logic and will remain
separately payable- Ambulance- Diagnostic and screening mammography- Brachytherapy- PT, OT and ST services provided under a plan of care
• Allowed to be billed separately as a recurring account- Preventive services
- Self-administered drugs• Drugs that are usually self-administered and do not function as supplies in the
provision of the comprehensive service- Services assigned to OPPS status indicator ‘‘F’’ (Hepatitis B vaccines and
corneal tissue acquisition)- Certain Part B inpatient services
• Ancillary Part B inpatient services payable under Part B when the primary ‘‘J1’’ service for the claim is not a payable Part B inpatient service (for example, exhausted Medicare Part A benefits, beneficiaries with Part B only)
9

C-APC Complexity Adjustments
• Expanded logic for complexity adjustments• When a code combination represents a complex costly form
or version of the primary service- CMS developed a list of “family” related HCPC codes
• Two or more status indicator J1 procedures reported on the same claim
• System will default to the highest APC in the family group
10
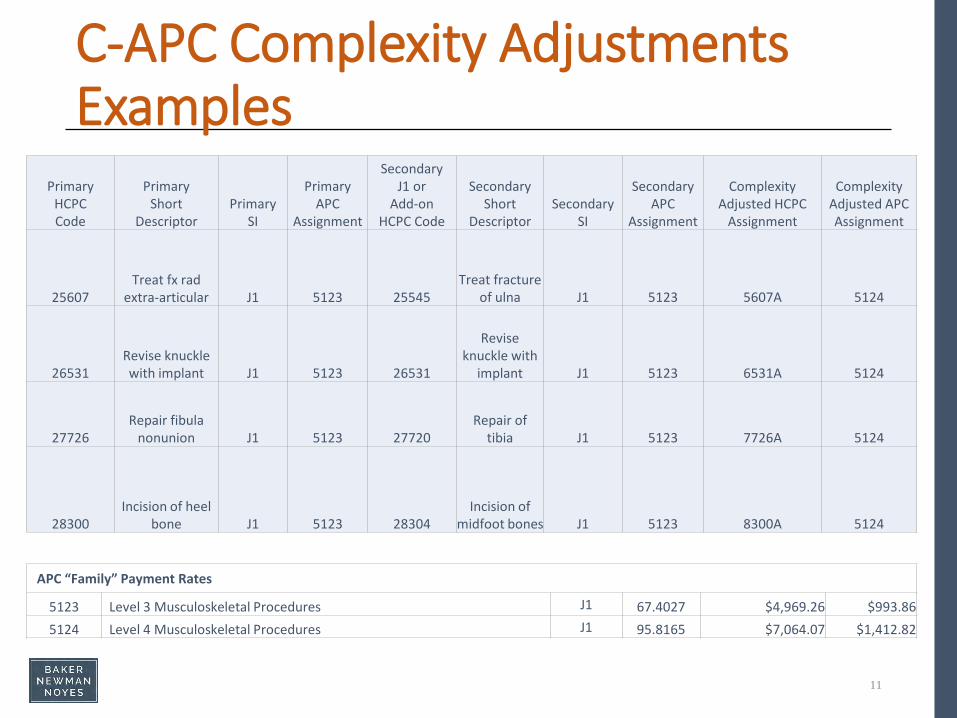
C-APC Complexity Adjustments Examples
Primary HCPCCode
Primary Short
DescriptorPrimary
SI
Primary APC
Assignment
Secondary J1 or
Add-on HCPC Code
Secondary Short
DescriptorSecondary
SI
Secondary APC
Assignment
Complexity Adjusted HCPC
Assignment
Complexity Adjusted APC Assignment
25607Treat fx rad
extra-articular J1 5123 25545Treat fracture
of ulna J1 5123 5607A 5124
26531Revise knuckle with implant J1 5123 26531
Revise knuckle with
implant J1 5123 6531A 5124
27726Repair fibula
nonunion J1 5123 27720Repair of
tibia J1 5123 7726A 5124
28300Incision of heel
bone J1 5123 28304Incision of
midfoot bones J1 5123 8300A 5124
11
APC “Family” Payment Rates
5123 Level 3 Musculoskeletal Procedures J1 67.4027 $4,969.26 $993.865124 Level 4 Musculoskeletal Procedures J1 95.8165 $7,064.07 $1,412.82

Observation Stays
• 2015 Observation service logic: services deemed payable (criteria met) and not “packaged”, currently pay an APC 8009
- Observation G0378 or direct admit to observation G0379/G0378
- No major procedure (SI = T)- 8 or more units of service (Rev code 762)- Emergency room E&M 99284 or 99285 or Critical Care
99292 or Clinic G0463- Unadjusted $1,235
12

New C-APC for Observation Stays2016 Observation services; APC 8011• Criteria
- Observation G0378 or direct admit to observation G0379/G0378
- No major procedure (SI=T)- No status indicator J1 procedure- 8 or more units of service (Rev code 762)- Any level Emergency Room (99281-99285)
• CMS will deem all other OPPS services and items to be adjunctive; creating a single payment C-APC- Exception SI = F, G, H, L and U
• Unadjusted $2,275- Status indicator J2
13
Lab Packaging - Expanded
• CMS will only provide lab testing payments when:- Only service on the claim- Lab ordered by a different practitioner for a different purpose
from the primary service on the claim- Continued use of the L1 Modifier
• Expands FISS editing for lab packaging to the entire claim; not just primary service dates
• New status indicator definition added to Q4• Excludes lab packaging for CPT codes in the ranges of 81200
through 81383, 81400 through 81408 and 81479 (molecular lab)
14

Status Indicators Affected by2016 Updates
ADDENDUM D1. - FINAL OPPS PAYMENT STATUS INDICATORS FOR CY 2016
Status Indicator Item/Code/Service OPPS Payment Status
A Services furnished to a hospital outpatient that are paid under a fee schedule or payment system other than OPPS, for example:
Not paid under OPPS. Paid by MACs under a fee schedule or payment system other than OPPS. Services are subject to deductible or coinsurance unless indicated otherwise.
● Ambulance Services
Not subject to deductible or coinsurance.
● Separately Payable Clinical Diagnostic Laboratory Services
● Separately Payable Non-Implantable Prosthetics and Orthotics
● Physical, Occupational, and Speech Therapy
● Diagnostic Mammography
● Screening Mammography
C Inpatient Procedures Not paid under OPPS. Admit patient. Bill as inpatient.
15

Status Indicators Affected by 2016 Updates
Status Indicator Item/Code/Service OPPS Payment Status
Q1 STV-Packaged Codes Paid under OPPS; Addendum B displays APC assignments when services are separately payable.1. Packaged APC payment if billed on the same date of service as a HCPCs code assigned
status indicator “S,” “T,” or “V.”2. In other circumstances, payment is made through a separate APC payment.
Q2 T-Packaged Codes Paid under OPPS; Addendum B displays APC assignments when services are separately payable.1. Packaged APC payment if billed on the same date of service as a HCPCs code assigned
status indicator “T.”2. In other circumstances, payment is made through a separate APC payment.
Q3 Codes that may be paid through a composite APC
Paid under OPPS; Addendum B displays APC assignments when services are separately payable.Addendum M displays composite APC assignments when codes are paid through a composite APC. 1. Composite APC payment based on OPPS composite-specific payment criteria.
Payment is packaged into a single payment for specific combinations of services.2. In other circumstances, payment is made through a separate APC payment or
packaged into payment for other services.Q4 Conditionally
packaged laboratory tests
Paid under OPPS or CLFS.1. Packaged APC payment if billed on the same claim as a HCPCs code assigned published
status indicator “J1,” “J2,” “S,” “T,” “V,” “Q1,” “Q2,” or “Q3.”2. In other circumstances, laboratory tests should have a SI = A and payment is made
under the CLFS.
16

Status Indicator Item/Code/Service OPPS Payment Status
J1 Hospital Part B services paid through a comprehensive APC
Paid under OPPS; all covered Part B services on the claim are packaged with the primary "J1" service for the claim, except services with OPPS SI=F,G, H, L and U; ambulance services; diagnostic and screening mammography; all preventive services; and certain Part B inpatient services.
J2 Hospital Part B services that may be paid through a comprehensive APC
Paid under OPPS; Addendum B displays APC assignments when services are separately payable.
1. Comprehensive APC payment based on OPPS comprehensive-specific payment criteria. Payment for all covered Part B services on the claim is packaged into a single payment for specific combinations of services, except services with OPPS SI=F,G, H, L and U; ambulance services; diagnostic and screening mammography; all preventive services; and certain Part B inpatient services.
2. Packaged APC payment if billed on the same claim as a HCPCS code assigned status indicator “J1.”
3. In other circumstances, payment is made through a separate APC payment or packaged into payment for other services.
17
Status Indicators Affected by 2016 Updates

Miscellaneous OPPS Updates
Inpatient Only List (Status Indicator C) criteria for exclusion:1. Most outpatient departments are equipped to provide the
services to the Medicare population.2. The simplest procedure described by the code may be performed
in most outpatient departments.3. The procedure is related to codes that have already been removed
from the inpatient-only list.4. A determination is made that the procedure is being performed in
numerous hospitals on an outpatient basis.5. A determination is made that the procedure can be appropriately
and safely performed in an ASC, and is on the list of approved ASC procedures or has been proposed by us for addition to the ASC list.
18
Miscellaneous OPPS UpdatesInpatient only procedures deleted in 2016:• CPT code 0312T; Vagus nerve blocking therapy• CPT code 20936; Autograft for spine surgery only (includes harvesting
the graft• CPT code 20937; Autograft for spine surgery only (includes harvesting
the graft); morselized• CPT code 20938; Autograft for spine surgery only (includes harvesting
the graft); structural, bicortical or tricortical• CPT code 22552; Arthrodesis, anterior interbody, including disc space
preparation; cervical below C2, each additional interspace• CPT code 54411; Removal and replacement of all components of a
multi-component inflatable penile prosthesis through an infected field at the same operative session, including irrigation and debridement of infected tissue
19

766 APCin 2015
663 APC for 2016
With 200+ APC reassigned tonew APC number
20
Major Restructuring of APC Groupings
Other Changes
21

Changes/Updates to Reimbursement
• Payment Update for Partial Hospitalization Programs (PHPs)
- Hospital-based PHPs Per Diem payments adjusted
• Level I (three services)• Level II (four or more services)
• Mental Health services rendered on a single day will not exceed the Level II PHP per diem
- Changes from APC 0034 to APC 8010
22
$183.41$212.67
$212.67

OPPS Outliers
Outlier payments are triggered when:
Costs exceed 1.75 times the APC payment amount and exceeds the APC payment
rate plus a $3,250 fixed dollar threshold
Outlier payments are equal to 50% of the excess as noted above
23
• Stays less than 2 days may be paid as inpatient admissions under MS-DRGs
- Based on clinical judgment of admitting physician and- Must be reasonable and necessary; supported by
documentation in the medical record• Exception on a case by case basis• Expectation that consideration of the policy be rare• RAC review has been transferred to QIO effective
10/01/2015• QIO will make referrals to the Recovery Auditor for additional
review of high denial rates or failures to improve after QIO assistance
24
2 Midnight Rule

CMS clarifies the requirements for OPPS payment associated with CCM- CPT 99490: Chronic care management services (CCM), at least 20 minutes of
clinical staff time directed by a physician or other qualified health care professional, per calendar month
• Multiple (two or more) chronic conditions expected to last at least 12 months, or until the death of the patient;
• Chronic conditions place the patient at significant risk of death, acute exacerbation/decompensation, or functional decline; and
• Comprehensive care plan established, implemented, revised or monitored
- Hospital billing under OPPS:• Service must meet the definition of a hospital outpatient and meet the
supervision requirements for therapeutic care (general supervision)- Established relationship
• Patient is admitted as an inpatient or registered as an outpatient in the last 12 months
25
Chronic Care Management (CCM)
(cont.)- Required to have documented in the hospital’s medical record the patient’s
agreement to have the services provided or, alternatively, to have the patient’s agreement to have the CCM services provided documented in the beneficiary’s medical record that a hospital can access
• Notation of the beneficiary’s decision to accept or decline the services.- CMS expects the physician or practitioner under whose direction the services
are furnished to have discussed with the beneficiary that hospital clinical staff will furnish the services and that the beneficiary could be liable for two separate copayments from both the hospital and the physician.
- Only one hospital can render care- Use of a certified EHR is required
26
Chronic Care Management (CCM)

Questions or Comments
27

Healthcare Consulting DivisionToll Free: 1-800-244-7444
Fax: 207-774-1793
Maggie Fortin, Senior ManagerDirect Line: 207-791-7547
Janet Hodgdon, DirectorDirect Line: 207-791-7508
28
Contact the Presenters