5 y 0 learning objectives 0 slide 7 of 37 overall mortality … risk prediction and hiv slide 20 of...
TRANSCRIPT
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 3 of 37
Learning Objectives
After attending this presentation, participants will
be able to:
Recognize important cardiovascular risk factors in HIV infection.
Access cardiovascular risk score programs for clinical use.
Describe the appropriate use of statin therapy in the setting of HIV disease.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 7 of 37
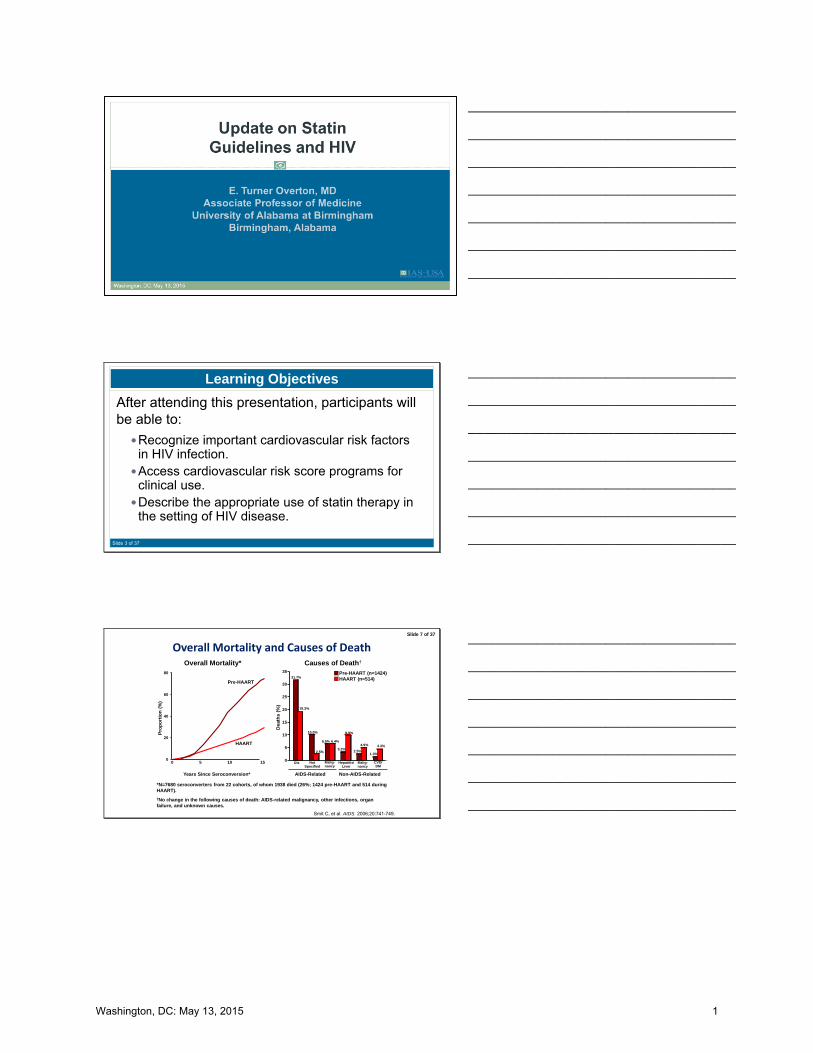
Overall Mortality and Causes of Death
Smit C, et al. AIDS. 2006;20:741-749.
Overall Mortality*
0
20
40
60
80
Pro
po
rtio
n (
%)
Years Since Seroconversion*
0 5 10 15
Pre-HAART
HAART
Causes of Death†
De
ath
s (
%)
Pre-HAART (n=1424)
HAART (n=514)
*N=7680 seroconverters from 22 cohorts, of whom 1938 died (26%; 1424 pre-HAART and 514 during
HAART).
†No change in the following causes of death: AIDS-related malignancy, other infections, organ
failure, and unknown causes.
0
5
10
15
20
25
30
35
OIs NotSpecified
Hepatitis/Liver
Malig-nancy
CVD/DM
AIDS-Related Non-AIDS-Related
31.7%
19.3%
10.0%
2.5%3.2%
9.9%
2.5%
4.9%
1.3%
4.3%
6.5% 6.4%
Malig-nancy
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 1

Slide 8 of 37
AgingChronic HIV
Infection
Impact on Non-AIDS Comorbidities
Decreased Physical Functioning
Insulin Resistance
DyslipidemiaInflammation &Fibrosis
END-ORGAN DISEASE
ART ToxicityGenetics
Obesity, Exercise, Diet, Smoking
HCV and other Co-infections
Warriner AH et al.ID Clin N Am. 2014
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 10 of 37
Incident rate ratio for acute MI by age
30-39 40-49 50-59 60-69 70-79
2.2 1.3 1.8 1.5 1.5
Impact of HIV on risk comparable to traditional risk factors including HTN, DM and hyperlipidemia.
Models adjusted for recognized risk factors
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 2
Slide 11 of 37Houston, we have a CVD problem.• CVD Mortality (729)
– 145,009 HIV+ subjects reported 2001-2012• 71% male, median age 49 yrs
– CVD mortality 54% ↑increase (HR 1.54) (713%)• Decreasing in gen population
– Rate if VL suppressed: 3.9/1000pt yr
– Rate if VL > 400cp/mL: 7.7/1000pt yr
• Smoking in the MACS Cohort (743)– 1005 MSM (621 HIV+); Median age 53-55; 82% VL < 50 – Smoking associated with numerous parameters by CAC and coronary CT angiography
• Kidney disease in D:A:D (742) – 34,793 subjects; median 6.3 yrs F/U– 1033 persons 1251 CVD events
Hannah DB et al. CROI 2015. February 23-26, 2015. Seattle, Washington. Abstract 729. Kelly SG et al. CROI 2015. February 23-26, 2015. Seattle, Washington. Abstract 743. Ryom L et al. CROI 2015. February 23-26, 2015. Seattle, Washington. Abstract 742.
eGFR % of Cohort
% of CVD Events
>90 70% 47%
>30 - <90 29.8% 52%
<30 0.2% 1%
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 12 of 37
Two Approaches to Assessing CVD Risk
ACC/AHA Guidelines NLA Recommendations
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 13 of 37Many Similarities • Lipid screening for primary prevention at 5-year
intervals
• Lifestyle therapy is the recommended first step
• CVD risk reduction is the goal of lipid-lowering therapy
• Moderate- or high-intensity statin therapy is recommended
• Patient-provider discussion is central to decisions on drug treatment
• Repeat lipid assessment is suggested to monitor adherence
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 3

Slide 14 of 37
Differences
• ACC/AHA
– Used data from RCT with CVD outcomes and meta-analyses of RCT.
• Only highest level of evidence on statin was used.
• NLA (NCEP Guidelines)
– Included RCT, meta-analyses of RCT, selected post-hoc analyses from RCT, genetic, metabolic, and mechanistic studies.
• Broader approach consistent with previous NCEP recommendations and international guidelines.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 15 of 37ACC/AHA Statin Benefit Groups• Known ASCVD (Atherosclerotic Cardiovascular Disease)
• Primary elevation in LDL cholesterol > 190 mg/dL
• Age 40-75 with either– Diabetes and LDL cholesterol > 70mg/dL
– 10-year ASCVD Risk Score > 7.5%
• Perspective on statins– Do not recommend dose titration to achieve a pre-specified lipid
level
– Do not recommend non-statin therapies
• Limited ASCVD risk reduction
• Potential for adverse events > benefits
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 16 of 37
ACC/AHA ASCVD Risk Calculator
Please use “Launch Web Version” to calculate ASCVD Risk Score
The calculator to calculate the 10-year ASCVD is located at the following website:http://my.americanheart.org/professional/StatementsGuidelines/PreventionGuidelines/PreventionGuidelines_UCM_457698_SubHomePage.jsp
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 4

Slide 17 of 37NLA Recommendations
• Start with risk assessment and patient-provider discussion
• Lifestyle modification is first step
• Judicious use of moderate- to high-dose statins is associated with optimal CVD risk reduction
– Statin therapy is the most potent and evidence-based approach to reducing ASCVD events
– “Lower is better” for atherogenic lipoproteins
• Consider addition of non-statin therapy when statin therapy inadequate
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 18 of 37
NLA Stepwise Approach
• Identify ASCVD risk category
• If very high risk begin with moderate- or high-intensity statin.–Goal LDL <70mg/dL or non-HDL <100mg/dL
• If not high risk, consider statin therapy based on risk factors–Goal LDL <100mg/dL or non-HDL <130mg/dL
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 19 of 37
NLA Criteria for Statin Therapy
Jacobson TA e al. J Clin Lipidol. 2014;8(5):473-88.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 5

Slide 20 of 37CVD Risk Prediction and HIV• NA-ACCORD
– 25,094 ppts, 271 primary MIs, 219 secondary MIs– CVD RF: age, male, HTN, DM, low HDL, CKD, statin use– HIV RF: lower CD4, detectable viremia, H/O AIDS
• From the HOPS – 2392 participants, 204 CV events – 4 risk equations tested that included age, sex, SBP, smoking, T Chol, with some
including other factors such as type of ART– All 4 underestimate CVD Risk: E/O ratio: 0.75-0.85
• Framingham and ACC/AHA CVD Risk Equations – 2270 subjects: 38% female; 35% HTN; 20% DM; 38% smokers– Median CD4 508; VL<50: 68%– Both equations underestimate risk; particularly bad if risk > 5% for 5-yr prediction
Drozd DR et al. CROI 2015. February 23-26, 2015. Seattle, Washington. Abstract 748.Lichtenstein K et al. CROI 2015. February 23-26, 2015. Seattle, Washington. Abstract 747.Triant V et al. CROI 2015. February 23-26, 2015. Seattle, Washington. Abstract 751.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 21 of 37Residual CVD Risk Even With Suppressed HIV Viremia
• Atherosclerosis is an inflammatory process
– Endothelial smooth muscle disruption
– Macrophage activation and infiltration
– Oxidized lipid accumulation
– Plaque formation
• Vascular inflammation is greater with HIV infection
– Increased metabolically active macrophages
– Greater non-calcified, metabolically active, rupture-prone plaques
Yarasheski et al. J Inflammation. 2012. Zanni et al. AIDS. 2013.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 22 of 37
Despite ARTInflammatory Biomarkers Remain Elevated
Neuhaus JID 2010; Nixon and Landay, Curr Opin HIV/AIDS 2010
-While ART partially reduces some biomarker levels, they may still remain elevated compared with healthy non–HIV-infected individuals.
-Furthermore, inflammatory markers are more strongly associated with end-organ disease and mortality than in HIV-negative populations.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 6

Slide 23 of 37
STATINS as “Wonder Drugs”?
Blocking HMG-CoA
Reductase ↓ Mevalonate
Decreased precursor for
Cholesterol
&
Geranyl/farensyl
pyrophosphate
THUS
SUBSEQUENTLY
Signaling proteins
-do not undergo requisite
post-translational
modification
-cannot embed in lipid
rafts in membranes
(prerequisite for their biologic
function)
AND VOILA
Greenwood. Nature Rev Immun. 2006; 6:358-70.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 24 of 37
Statins have emerged as potential modulators of the process of inflammation, particularly in
diseases that are immune-related or diseases where aberrant activation of T cells plays an important role.
Greenwood and Mason. Trends in Immunology. 2007; 28:87-98. Mach F. Circulation. 2004; 109:II-15-17.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 25 of 37
Endpoints
Co-Primary CVD: FMD
Bone: % change in hip & lumbar spine BMD
Secondary IMT and CAC
Systemic & vascular inflammation
Lymphocyte & monocyte activation
Insulin resistance
Body composition
SATURN-HIV Design
Week 0 Week 48 Week 96
RosuvastatinN=72
PlaceboN=75
Inclusion
•HIV-1 & ≥18 years
•On ART >6mo & HIV-1 RNA ≤1000 cps/mL
•Fasting LDL-C≤130mg/dL
•Heightened immune activation (CD8+CD38+DR+ ≥19% or hsCRP ≥2μg/mL)
•No CVD or diabetes
•No fragility fractures
•No immunomodulatory, bone tx, or hypolipemics
Stratified by:• PI vs not• Osteopenia vs not• CAC vs not
McComsey GA et al. CROI 2014
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 7

Slide 26 of 37
sC
D1
4 R
ela
tive
Ch
an
ge
fro
m W
ee
k 0
(%
)
480
p=0.0056
24
p=0.002
480 24
p=0.0049p=0.0366
CD
14
dim
CD
16
+ T
F+
Re
lati
ve
Ch
an
ge
fro
m W
ee
k 0
(%
)
Visit Week from Randomization Visit Week from Randomization
-Rosuvastatin durably reduced sCD14.
-Rosuvastatin significantly reduced inflammatory monocyte population.
Rosuvastatin and Monocytes
McComsey GA et al. CROI 2014
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 27 of 37
Visit Week from Randomization
480 24
p=0.0009
p=0.9293
CD
4+
CD
38
+D
R+
Re
lati
ve
Ch
an
ge
fro
m W
ee
k 0
(%
)
Visit Week from Randomization
480 24
p=0.0035
p=0.5091
CD
8+
CD
38
+D
R+
Re
lati
ve
Ch
an
ge
fro
m W
ee
k 0
(%
)
-Rosuvastatin durably reduced T cell activation.
Longer exposure required to detect the effect on circulating T cells.
Rosuvastatin and T cell Activation
McComsey GA et al. CROI 2014
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 28 of 37
0
25
50
75
100
125
150
175
+
-
+
+
+
+
+
+
+
-
+
-
****
CD4 T-cells
% o
f S
EB
pro
life
rati
on
Statin
MA
0
25
50
75
100
125
150
175
+
-
+
+
+
+
+
+
+
-
+
-
**
**
CD8 T-cells
Pravastatin
Atorvastatin
Rosuvastatin
Not All Statins are Equal
Overton et al. AIDS 2014.
-Rosuvastatin and Atorvastatin, but not Pravastatin reduce T cell proliferation.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 8

Slide 29 of 37
Lo J et al. Lancet HIV. 2015;2:e52-e63. Lo J et al. CROI 2015. February 23-26, 2015. Seattle, Washington. Abstract 136.Longenecker CT et al. CROI 2015. February 23-26, 2015. Seattle, Washington. Abstract 137.
Statins Reverse Atherosclerosis!• Atorvastatin: Reduction in Coronary Artery Plaque Volume by
coronary CT angiography (CCTA) – Coronary plaque in
• 53% of the HIV group (also ↑rupture-prone noncalcified plaque)• 35% of the HIV-negative group
– Regression with Atorvastatin beyond expected with LDL lowering alone
• Rosuvastatin: Stabilization of CIMT– Daily rosuvastatin stopped progression of CIMT– Also decreased monocyte and lymphocyte activation,
decreased NT-proBNP and Lp-PLA2– Factors predicted a bigger drop in CIMT:
• higher baseline CIMT, IL-6 (an inflammation marker), and percentage of patrolling monocytes (CD14dimCD16 cells)
Baseline
Month 12
Images courtesy of Dr. Janet Lo.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 30 of 37
Statins: Ideal Strategy to Reduce Non-AIDS and Vascular Events in HIV
• Traditional effects to lower LDL, effective to lower LDL (-26%), with few AE’s (myositis 1.9%) in HIV Silverberg Annals 2009
• Pleiotropic effects to reduce monocyte activation, chemo-attraction and vascular inflammation FunderburgCID 2013, Eckard JID 2014
• Reduce events even among non-HIV patients with low LDL but increased inflammation Jupiter NEJM 2008
• Use is low among HIV patients (19.6% in ACTG), clinicians awaiting results from RCTs ACTG survey
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 31 of 37Need for a Large RCT to Inform Clinical Practice• HIV patients with low traditional risk scores are at
increased risk for CVD with subclinical plaque and inflammation
• It is unknown if statins will prevent CVD and should be recommended for the HIV population
• Though largely well tolerated to date in small studies, there are no data from large RCTs in HIV investigating tolerability, AEs and efficacy
• How will statins uniquely work in HIV
– LDL lowering
– Effects on inflammatory pathways
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 9

Slide 32 of 37Randomized Trial to Prevent Vascular Events
in HIV REPRIEVE (A5332)
Intervention
Clinical
Primary Endpoint
TimeScreening
And
Consent
Asymptomatic HIV+ patients with no history of CVD
Pitavastatin 4mg/dayPlacebo
MICV Death Unstable Angina Arterial Revasc
Secondary
Endpoints
Individual components of primary endpoint
All Cause Death
RandomizationR
Incidence/Progression of noncalcified plaque; High-risk plaque
Mechanistic
Study
Inflammatory, immunological, metabolic biomarkers
Mechanistic
Primary Endpoint
Coronary plaque, vascular inflammation, immune activation
Stroke
Predictors of statin effects
Statin safety and non AIDS comorbidities: DM, Infections, Cancer
All cause death
Figure 4. Schematic overview of REPRIEVE trial design.
Intervention
Clinical
Primary Endpoint
TimeScreening
And
Consent
Asymptomatic HIV+ patients with no history of CVD
Pitavastatin 4mg/dayPlacebo
MICV Death Unstable Angina Arterial Revasc
Secondary
Endpoints
Individual components of primary endpoint
All Cause Death
RandomizationR
Incidence/Progression of noncalcified plaque; High-risk plaque
Mechanistic
Study
Inflammatory, immunological, metabolic biomarkers
Mechanistic
Primary Endpoint
Coronary plaque, vascular inflammation, immune activation
Stroke
Predictors of statin effects
Statin safety and non AIDS comorbidities: DM, Infections, Cancer
All cause death
Figure 4. Schematic overview of REPRIEVE trial design.
6 year
F/u
(n=6500)
(n=800)
Funded by NHLBI and NIAID. Supported by KOWA Pharmaceuticals.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 33 of 37
Summary• Despite ART, low-grade inflammation persists.
–Soluble inflammatory biomarkers
–T cell activation and senescence
– Inflammatory monocytes
• Interventions to reduce inflammation are needed to reduce morbidity and mortality.
• Statins have robust anti-inflammatory properties that may serve this role effectively.
–Need to assess in an RCT.
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Slide 37 of 37
Acknowledgements
• UAB CFAR– Anju Bansal– Greer Burkholder– Paul Goepfert– Sarah Sterrett– Alan Zajac– Andy Westfall– Shannon Kahan– Mike Saag
• Shared ideas/data– Grace McComsey– Nick Funderburg– Janet Lo
• REPRIEVE Study Team– Steve Grinspoon– Pam Douglas– Udo Hoffmann– Heather Ribaudo– Carl Fichtenbaum– Judy Aberg– Markella Zanni– Katie Fitch– Barbara Bastow
• Mentors– Kevin Yarasheski– Pablo Tebas
Funding: NIH funded CNICS (R24 AI067039); UAB CFAR (P30 AI027767); REPRIEVE (R01 HL123336-01).
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Washington, DC: May 13, 2015 10