8 fri 430 - wapner prenatal genetics
TRANSCRIPT
10/2/2015
1
T21
T 18
T21
T 18
Copy Number Variants
T 1345, XO
47, XXY47, XXX
47, XYY
T 1345, XO
47, XXY47, XXX
47, XYY
Diagnostic Procedure
Improved Screening Diagnostic TestingMore Information
Other Chromosome Abnormalites

10/2/2015
2
Chromosomal Microarray Analysis (CMA)
Karyotype
Resolution:>7-10 Million Base Pairs
(7-10 Mb)
Resolution:< 0.5 Million Base Pairs
(< 500 kb)
Chromosomal Microarray(CMA)
10/2/2015
3
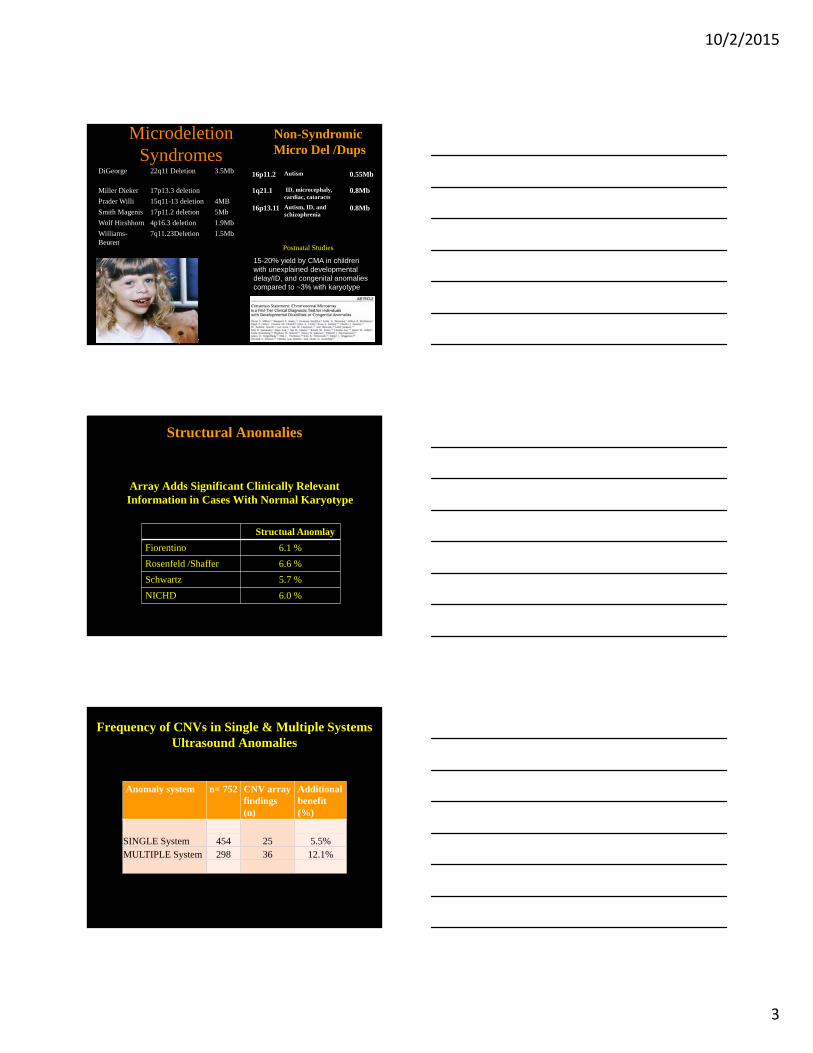
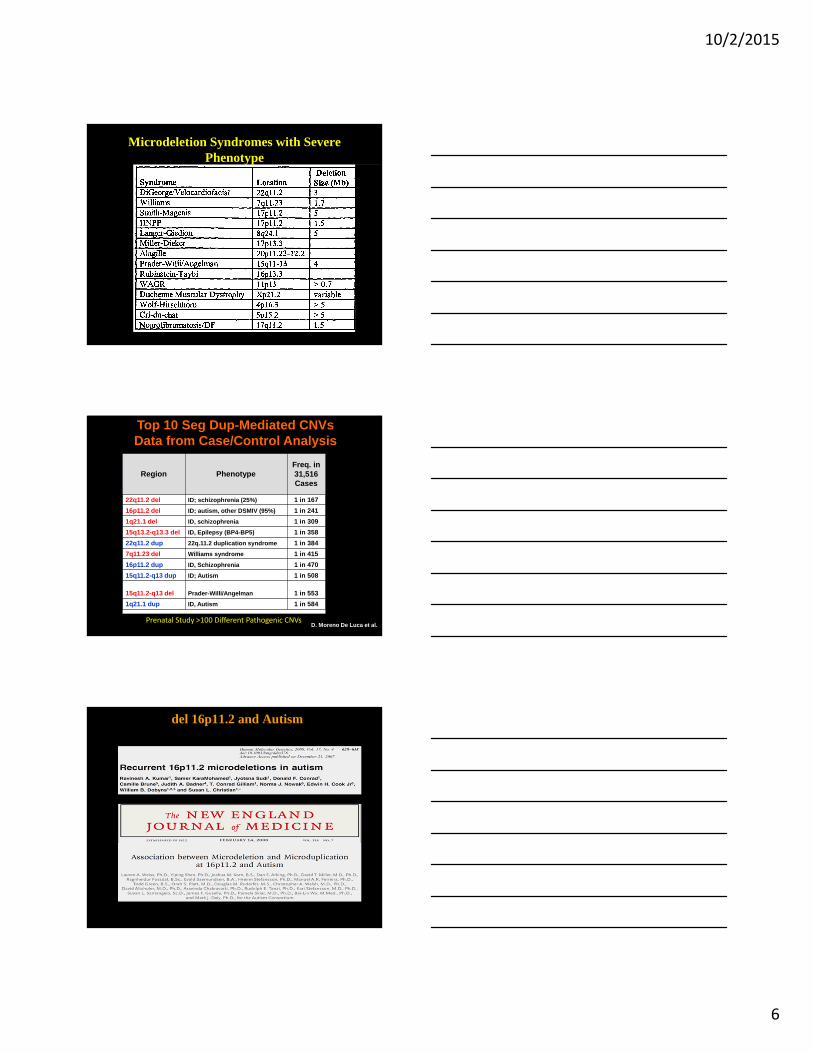
Microdeletion Syndromes
DiGeorge 22q11 Deletion 3.5Mb
Miller Dieker 17p13.3 deletion
Prader Willi 15q11-13 deletion 4MB
Smith Magenis 17p11.2 deletion 5Mb
Wolf Hirshhorn 4p16.3 deletion 1.9Mb
Williams-Beuren
7q11.23Deletion 1.5Mb
Non-SyndromicMicro Del /Dups
15-20% yield by CMA in children with unexplained developmental delay/ID, and congenital anomalies compared to ~3% with karyotype
16p11.2 Autism 0.55Mb
1q21.1 ID, microcephaly, cardiac, cataracts
0.8Mb
16p13.11 Autism, ID, and schizophrenia
0.8Mb
Velo Cardio Facial Syndroe
Postnatal Studies
Structural Anomalies
Array Adds Significant Clinically Relevant Information in Cases With Normal Karyotype
Structual Anomlay
Fiorentino 6.1 %
Rosenfeld /Shaffer 6.6 %
Schwartz 5.7 %
NICHD 6.0 %
Frequency of CNVs in Single & Multiple Systems Ultrasound Anomalies
Anomaly system n= 752 CNV array findings (n)
Additionalbenefit (%)
SINGLE System 454 25 5.5%MULTIPLE System 298 36 12.1%
10/2/2015
4
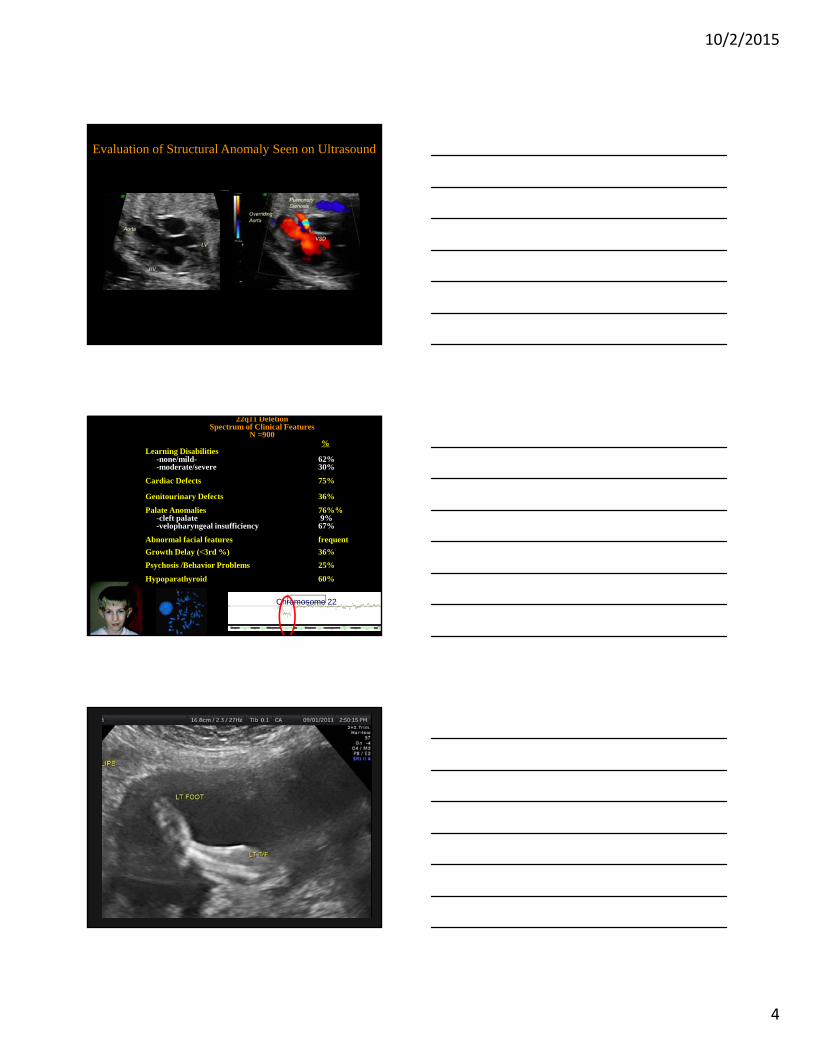
Evaluation of Structural Anomaly Seen on Ultrasound
22q11 DeletionSpectrum of Clinical Features
N =900%
Learning Disabilities-none/mild- 62%-moderate/severe 30%
Cardiac Defects 75%
Genitourinary Defects 36%
Palate Anomalies 76%%-cleft palate 9%-velopharyngeal insufficiency 67%
Abnormal facial features frequent
Growth Delay (<3rd %) 36%
Psychosis /Behavior Problems 25%
Hypoparathyroid 60%
Chromosome 22
10/2/2015
5
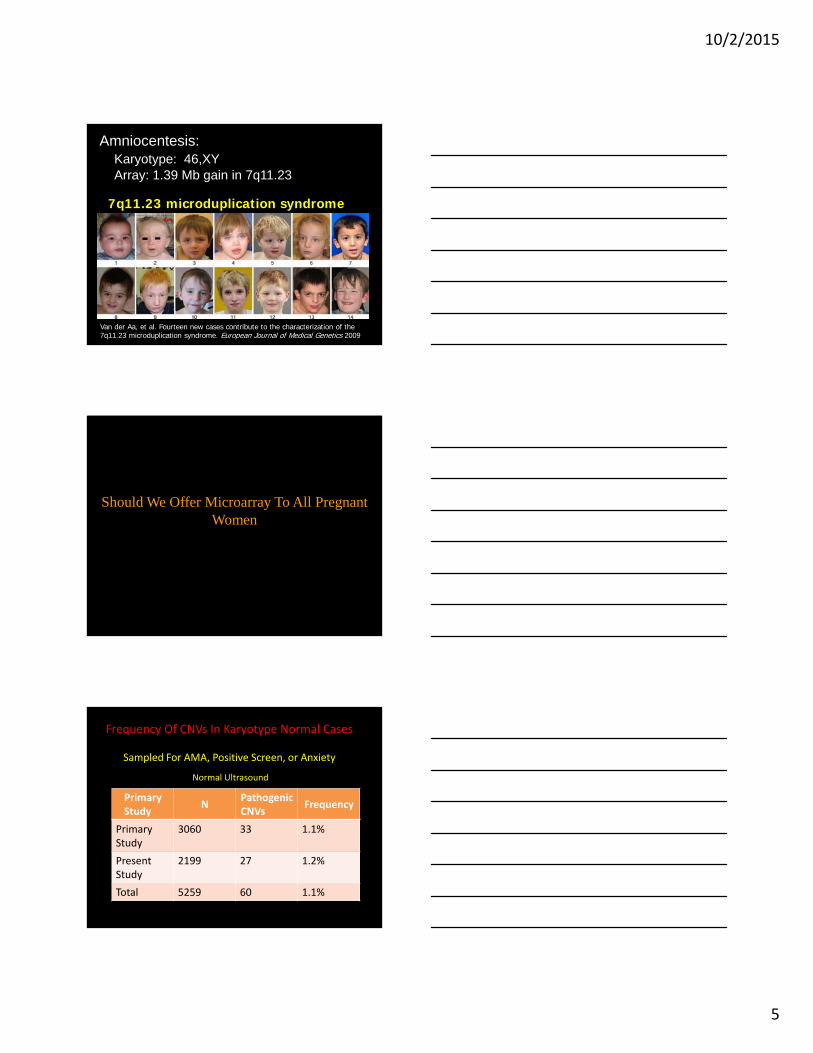
7q11.23 microduplication syndrome
Amniocentesis:Karyotype: 46,XYArray: 1.39 Mb gain in 7q11.23
Van der Aa, et al. Fourteen new cases contribute to the characterization of the 7q11.23 microduplication syndrome. European Journal of Medical Genetics 2009
Should We Offer Microarray To All Pregnant Women
PrimaryStudy
NPathogenic CNVs
Frequency
PrimaryStudy
3060 33 1.1%
Present Study
2199 27 1.2%
Total 5259 60 1.1%
Frequency Of CNVs In Karyotype Normal Cases
Sampled For AMA, Positive Screen, or Anxiety
Normal Ultrasound
10/2/2015
6
Microdeletion Syndromes with Severe Phenotype
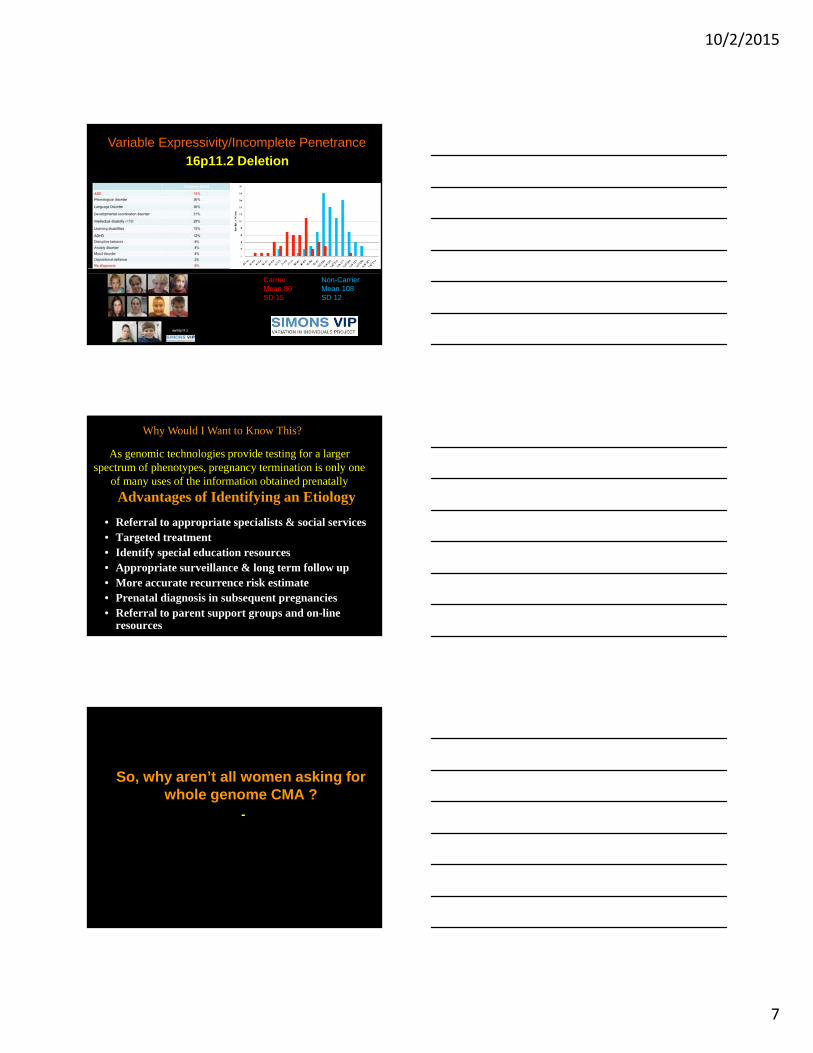
Region PhenotypeFreq. in 31,516 Cases
22q11.2 del ID; schizophrenia (25%) 1 in 167
16p11.2 del ID; autism, other DSMIV (95%) 1 in 241
1q21.1 del ID, schizophrenia 1 in 309
15q13.2-q13.3 del ID, Epilepsy (BP4-BP5) 1 in 358
22q11.2 dup 22q.11.2 duplication syndrome 1 in 384
7q11.23 del Williams syndrome 1 in 415
16p11.2 dup ID, Schizophrenia 1 in 470
15q11.2-q13 dup ID; Autism 1 in 508
15q11.2-q13 del Prader-Willi/Angelman 1 in 553
1q21.1 dup ID, Autism 1 in 584
D. Moreno De Luca et al. Mol Psych 2013
Top 10 Seg Dup-Mediated CNVs Data from Case/Control Analysis
Prenatal Study >100 Different Pathogenic CNVs
del 16p11.2 and Autism
10/2/2015
7
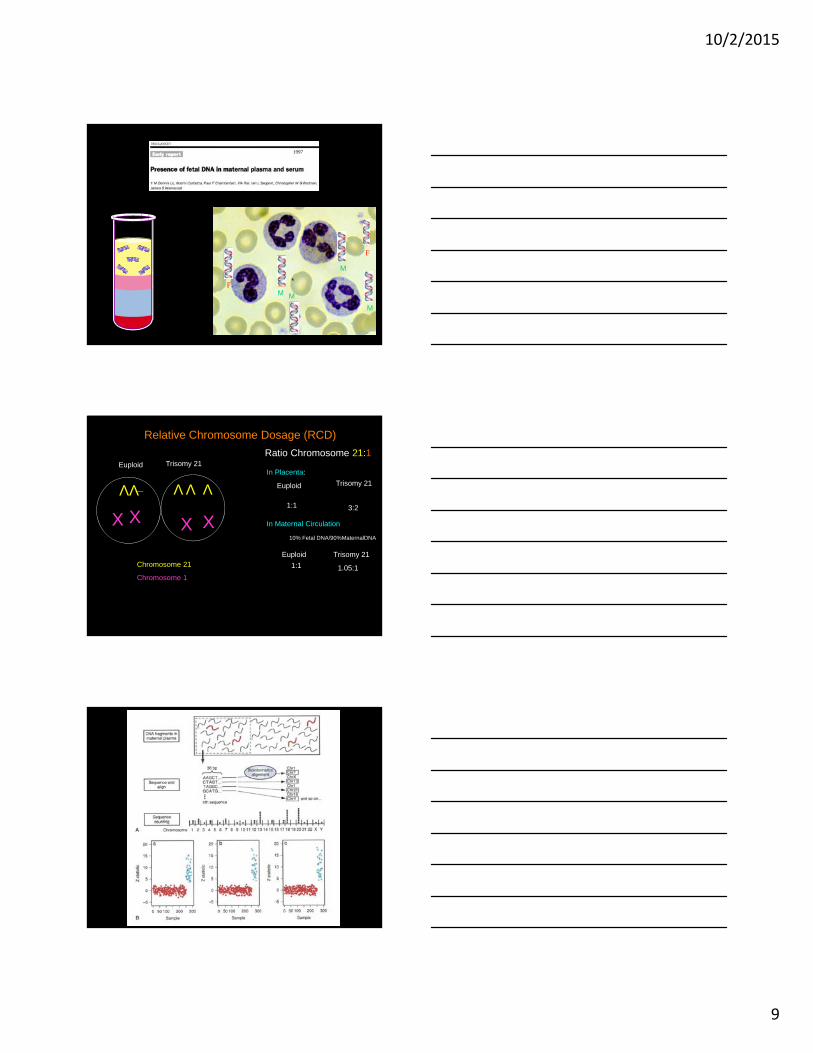
Non-CarrierMean 108SD 12
16p11.2 Deletion
CarrierMean 80SD 15
Variable Expressivity/Incomplete Penetrance
Advantages of Identifying an Etiology
• Referral to appropriate specialists & social services • Targeted treatment• Identify special education resources• Appropriate surveillance & long term follow up• More accurate recurrence risk estimate• Prenatal diagnosis in subsequent pregnancies• Referral to parent support groups and on-line
resources
As genomic technologies provide testing for a larger spectrum of phenotypes, pregnancy termination is only one
of many uses of the information obtained prenatally
Why Would I Want to Know This?
21
So, why aren’t all women asking for whole genome CMA ?
-
10/2/2015
8
NIPD for Common Trisomys
Trisomy 18 Trisomy 13 Trisomy 21
Detection rate
False positive
Detection rate
False positive
Detection rate
False positive
Sequenom ‐ Lo 84% 2% 44% 6% 100% 2.1%
Sequenom ‐ Lo(GC correct)
92% 2% 100% 1% n/a n/a
Sequenom – Palomaki 100% 0.3% 92% 1% 98.6% 0.2%
Sequenom – Palomaki(GC correct)
100% 0.7% 92% 0.5% 99.1% 0.1%
Verinata – Bianchi* 97% 0% 79% 0% 100% 0%
Verinata – Bianchi (all samples**)
97% 0.6% 81% 0% 100% 1.5%
Ariosa ‐Sparks 98% 0.1% N/A N/A 100% 0.1%
*with the “no call zone”**at z=2.5 cut‐off
Chen et al. (2011), PLoS ONE; Chiu et al. (2011), BMJ; Palomaki GE et al. (2011), Genet. Med; Palomaki GE et al. (2012), Genet. Med.; Bianchi et al. (2012) Obstet Gynecol
cffDNAAn Excellent Screening Test
• Not Diagnostic
• False Negative Results
• False Positive Results
10/2/2015
9
M
M
MM
1997
F
F
Chromosome 21
Chromosome 1
VV V V
Euploid Trisomy 21
X X
V
Ratio Chromosome 21:1
Euploid Trisomy 21
1:1
X X3:2
10% Fetal DNA/90%MaternalDNA
In Placenta:
In Maternal Circulation
Euploid
1:1
Trisomy 21
1.05:1
Relative Chromosome Dosage (RCD)
10/2/2015
10
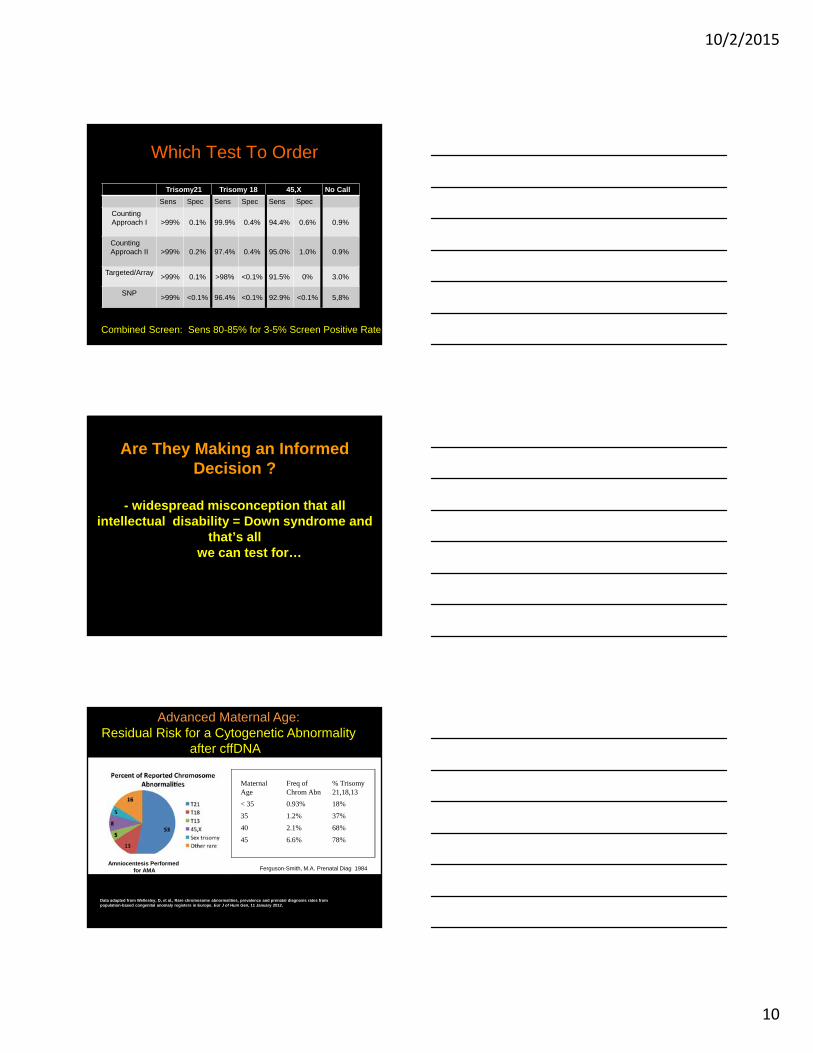
Which Test To Order
Trisomy21 Trisomy 18 45,X No Call
Sens Spec Sens Spec Sens Spec
Counting Approach I >99% 0.1% 99.9% 0.4% 94.4% 0.6% 0.9%
Counting Approach II >99% 0.2% 97.4% 0.4% 95.0% 1.0% 0.9%
Targeted/Array>99% 0.1% >98% <0.1% 91.5% 0% 3.0%
SNP>99% <0.1% 96.4% <0.1% 92.9% <0.1% 5,8%
Combined Screen: Sens 80-85% for 3-5% Screen Positive Rate
29
Are They Making an Informed Decision ?
- widespread misconception that all intellectual disability = Down syndrome and
that’s all we can test for…
Data adapted from Wellesley, D, et al., Rare chromosome abnormalities, prevalence and prenatal diagnosis rates from population-based congenital anomaly registers in Europe. Eur J of Hum Gen, 11 January 2012.
Ferguson-Smith, M.A. Prenatal Diag 1984
Maternal Age
Freq of Chrom Abn
% Trisomy 21,18,13
< 35 0.93% 18%
35 1.2% 37%
40 2.1% 68%
45 6.6% 78%
Advanced Maternal Age:Residual Risk for a Cytogenetic Abnormality
after cffDNA
Amniocentesis Performedfor AMA
10/2/2015
11
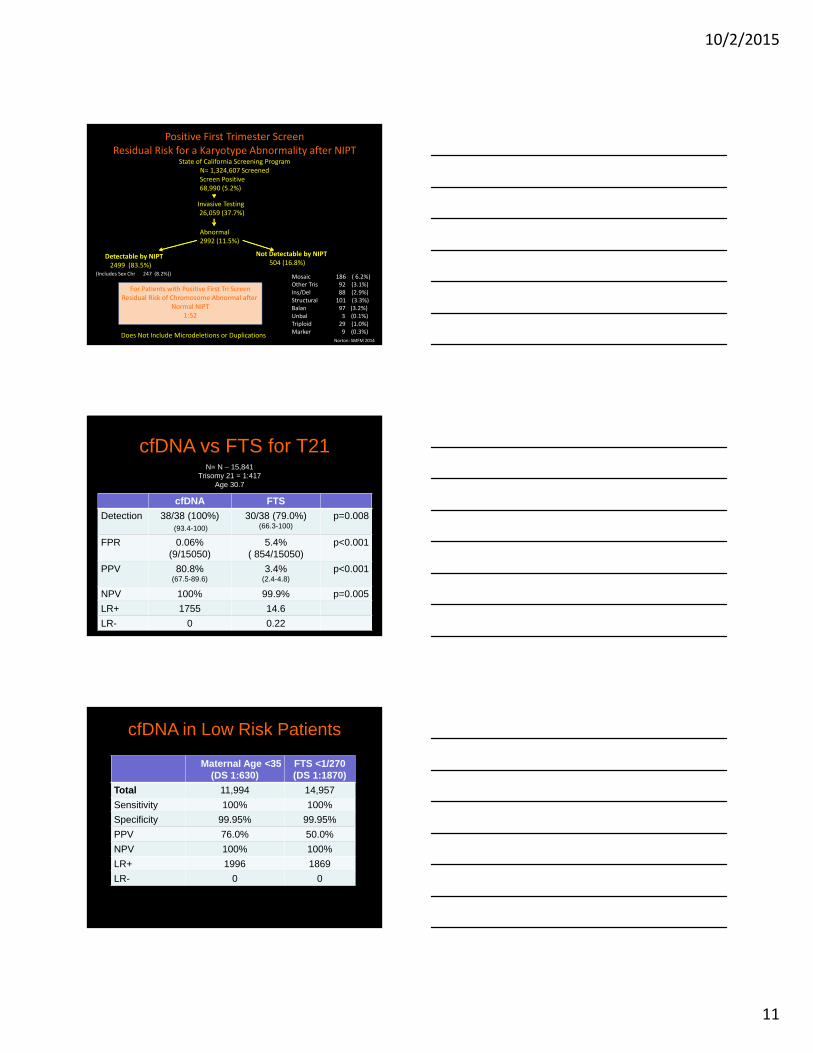
Positive First Trimester ScreenResidual Risk for a Karyotype Abnormality after NIPT
State of California Screening Program N= 1,324,607 Screened
Mosaic 186 ( 6.2%)Other Tris 92 (3.1%)Ins/Del 88 (2.9%)Structural 101 (3.3%)Balan 97 (3.2%)Unbal 3 (0.1%)Triploid 29 (1.0%)Marker 9 (0.3%)
Norton: SMFM 2014
Screen Positive68,990 (5.2%)
Invasive Testing26,059 (37.7%)
Abnormal2992 (11.5%)
Not Detectable by NIPT504 (16.8%)
Detectable by NIPT2499 (83.5%)
For Patients with Positive First Tri ScreenResidual Risk of Chromosome Abnormal after
Normal NIPT1:52
(Includes Sex Chr 247 (8.2%))
Does Not Include Microdeletions or Duplications
cfDNA FTS
Detection 38/38 (100%)(93.4-100)
30/38 (79.0%)(66.3-100)
p=0.008
FPR 0.06%(9/15050)
5.4%( 854/15050)
p<0.001
PPV 80.8%(67.5-89.6)
3.4%(2.4-4.8)
p<0.001
NPV 100% 99.9% p=0.005
LR+ 1755 14.6
LR- 0 0.22
cfDNA vs FTS for T21N= N – 15,841
Trisomy 21 = 1:417Age 30.7
Maternal Age <35(DS 1:630)
FTS <1/270(DS 1:1870)
Total 11,994 14,957
Sensitivity 100% 100%
Specificity 99.95% 99.95%
PPV 76.0% 50.0%
NPV 100% 100%
LR+ 1996 1869
LR- 0 0
Confidential
cfDNA in Low Risk Patients
10/2/2015
12
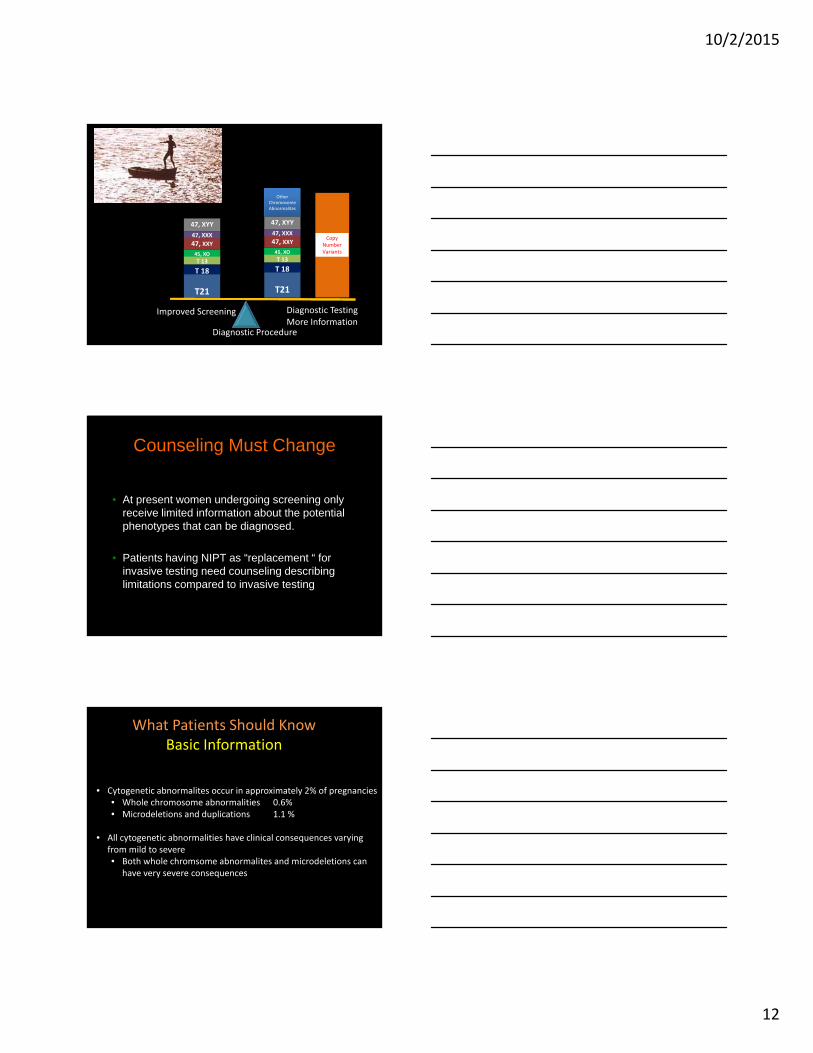
T21
T 18
T21
T 18
Copy Number Variants
T 1345, XO
47, XXY47, XXX
47, XYY
T 1345, XO
47, XXY47, XXX
47, XYY
Diagnostic Procedure
Improved Screening Diagnostic TestingMore Information
Other Chromosome Abnormalites
Counseling Must Change
• At present women undergoing screening only receive limited information about the potential phenotypes that can be diagnosed.
• Patients having NIPT as “replacement “ for invasive testing need counseling describing limitations compared to invasive testing
What Patients Should KnowBasic Information
• Cytogenetic abnormalites occur in approximately 2% of pregnancies• Whole chromosome abnormalities 0.6%• Microdeletions and duplications 1.1 %
• All cytogenetic abnormalities have clinical consequences varying from mild to severe• Both whole chromsome abnormalites and microdeletions can
have very severe consequences
10/2/2015
13
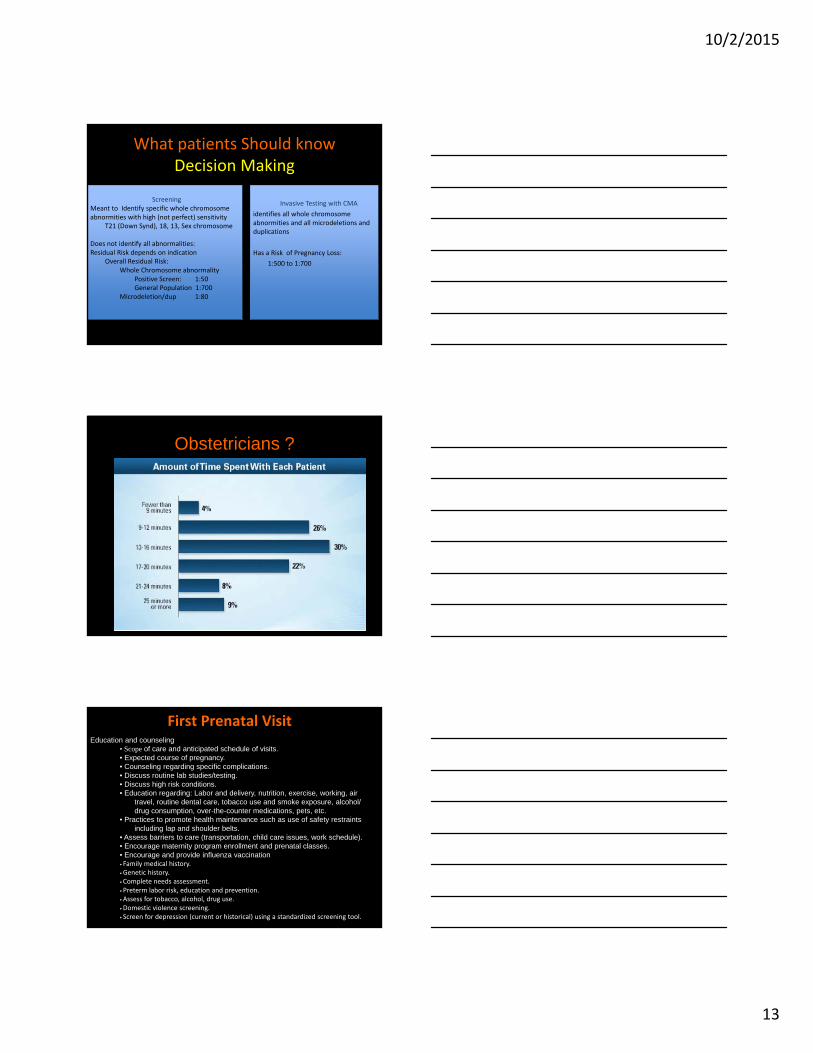
ScreeningMeant to Identify specific whole chromosome abnormities with high (not perfect) sensitivity
T21 (Down Synd), 18, 13, Sex chromosome
Does not identify all abnormalities:Residual Risk depends on indication
Overall Residual Risk:Whole Chromosome abnormality
Positive Screen: 1:50General Population 1:700
Microdeletion/dup 1:80
What patients Should knowDecision Making
Invasive Testing with CMA
identifies all whole chromosome abnormities and all microdeletions and duplications
Has a Risk of Pregnancy Loss:
1:500 to 1:700
Obstetricians ?
First Prenatal Visit Education and counseling
• Scope of care and anticipated schedule of visits. • Expected course of pregnancy. • Counseling regarding specific complications. • Discuss routine lab studies/testing. • Discuss high risk conditions. • Education regarding: Labor and delivery, nutrition, exercise, working, air
travel, routine dental care, tobacco use and smoke exposure, alcohol/drug consumption, over-the-counter medications, pets, etc.
• Practices to promote health maintenance such as use of safety restraints including lap and shoulder belts.
• Assess barriers to care (transportation, child care issues, work schedule). • Encourage maternity program enrollment and prenatal classes. • Encourage and provide influenza vaccination • Family medical history. • Genetic history. • Complete needs assessment. • Preterm labor risk, education and prevention. • Assess for tobacco, alcohol, drug use. • Domestic violence screening. • Screen for depression (current or historical) using a standardized screening tool.
10/2/2015
14
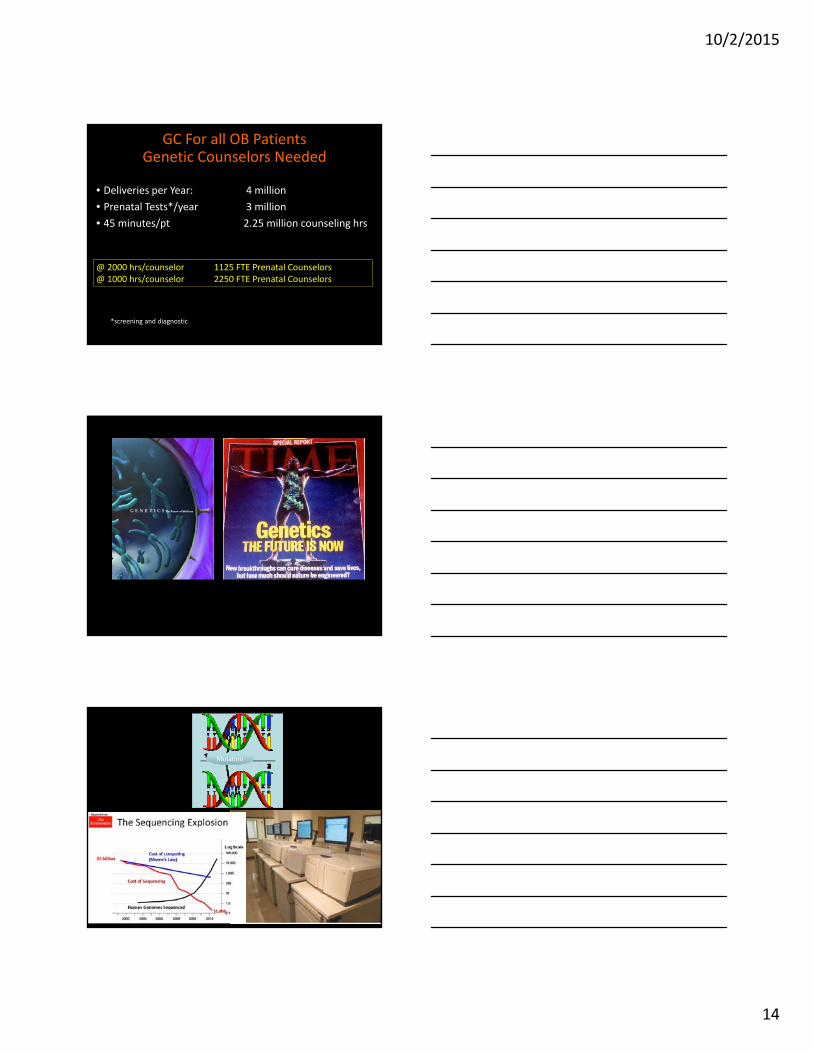
GC For all OB PatientsGenetic Counselors Needed
• Deliveries per Year: 4 million
• Prenatal Tests*/year 3 million
• 45 minutes/pt 2.25 million counseling hrs
*screening and diagnostic
@ 2000 hrs/counselor 1125 FTE Prenatal Counselors@ 1000 hrs/counselor 2250 FTE Prenatal Counselors
Mutation
10/2/2015
15
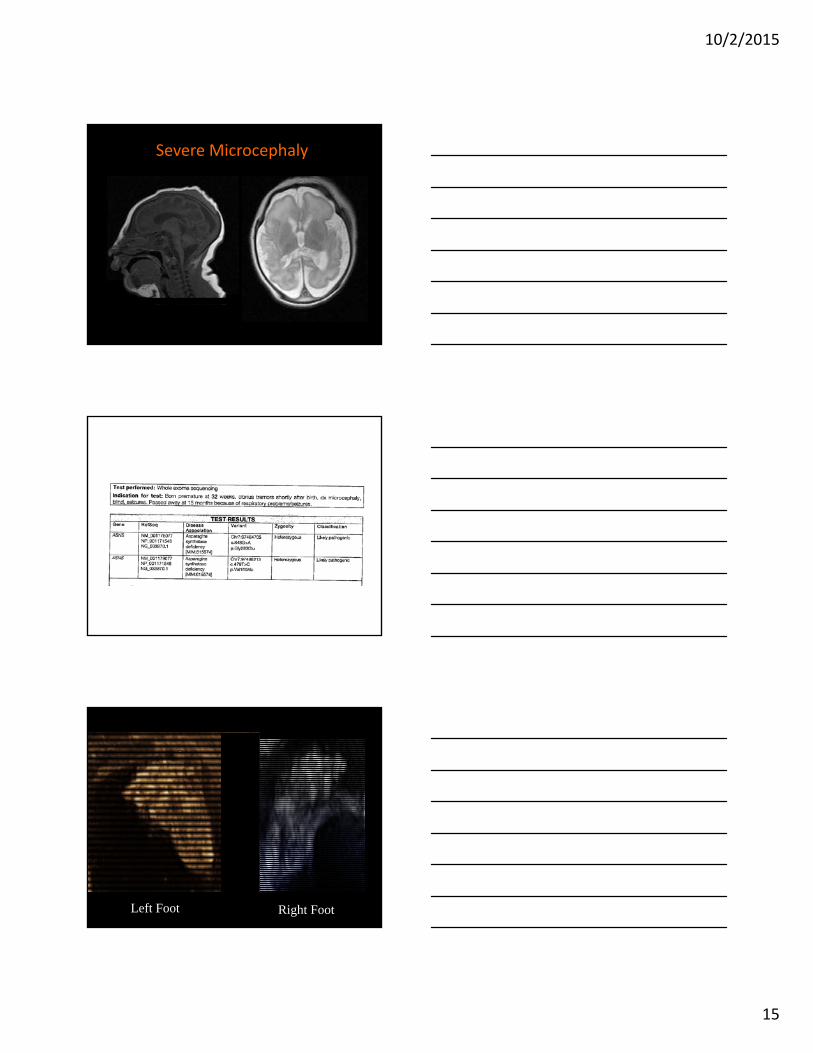
Severe MicrocephalySevere Microcephaly
Left Foot Right Foot
10/2/2015
16
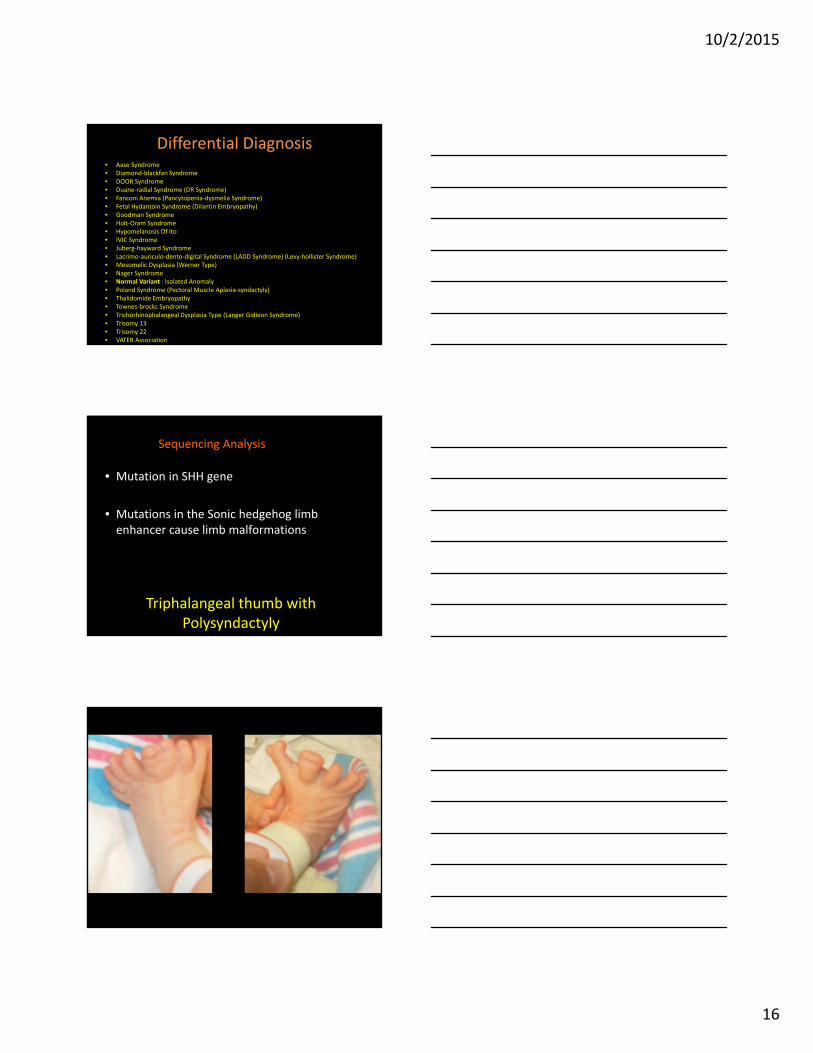
Differential Diagnosis• Aase Syndrome• Diamond‐blackfan Syndrome• DOOR Syndrome• Duane‐radial Syndrome (DR Syndrome)• Fanconi Anemia (Pancytopenia‐dysmelia Syndrome)• Fetal Hydantoin Syndrome (Dilantin Embryopathy)• Goodman Syndrome• Holt‐Oram Syndrome• Hypomelanosis Of Ito• IVIC Syndrome• Juberg‐hayward Syndrome• Lacrimo‐auriculo‐dento‐digital Syndrome (LADD Syndrome) (Levy‐hollister Syndrome)• Mesomelic Dysplasia (Werner Type)• Nager Syndrome• Normal Variant : Isolated Anomaly• Poland Syndrome (Pectoral Muscle Aplasia‐syndactyly)• Thalidomide Embryopathy• Townes‐brocks Syndrome• Trichorhinophalangeal Dysplasia Type (Langer Gidieon Syndrome)• Trisomy 13• Trisomy 22• VATER Association
Triphalangeal thumb with Polysyndactyly
• Mutation in SHH gene
• Mutations in the Sonic hedgehog limb enhancer cause limb malformations
Sequencing Analysis
10/2/2015
17
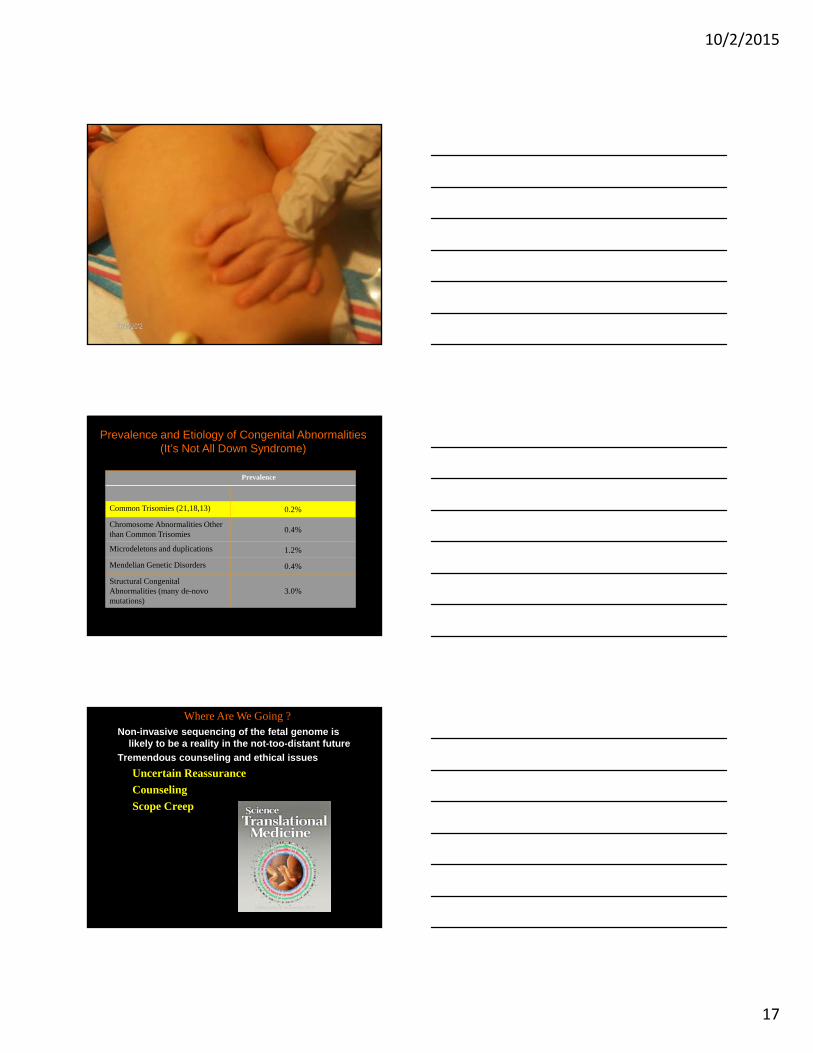
Prevalence
Common Trisomies (21,18,13) 0.2%
Chromosome Abnormalities Other than Common Trisomies 0.4%
Microdeletons and duplications 1.2%
Mendelian Genetic Disorders 0.4%
Structural Congenital Abnormalities (many de-novo mutations)
3.0%
Prevalence and Etiology of Congenital Abnormalities(It’s Not All Down Syndrome)
Non-invasive sequencing of the fetal genome is likely to be a reality in the not-too-distant future
Tremendous counseling and ethical issues
Uncertain Reassurance
Counseling
Scope Creep
Where Are We Going ?
10/2/2015
18
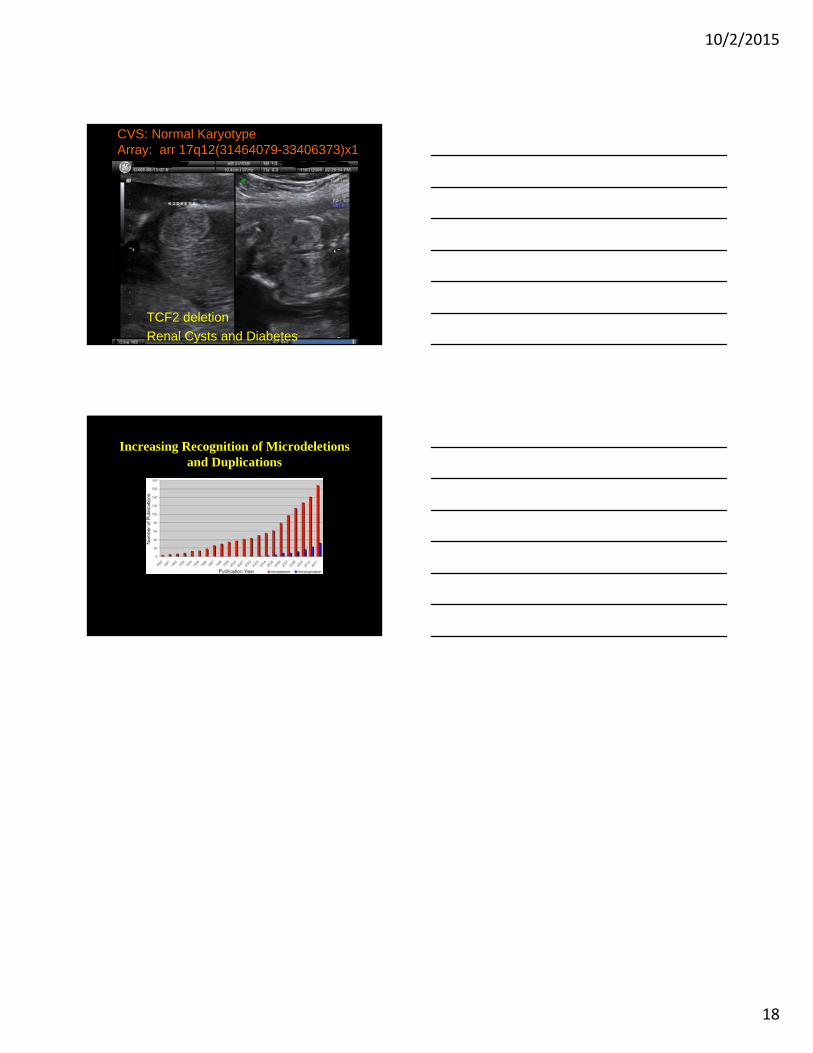
CVS: Normal KaryotypeArray: arr 17q12(31464079-33406373)x1
TCF2 deletion
Renal Cysts and Diabetes
Increasing Recognition of Microdeletionsand Duplications