a case of crohn’s disease rich rames, m3 may/june 2013 dr. joy sclamberg, dr. james cameron, dr....
TRANSCRIPT

A Case of Crohn’s Disease
Rich Rames, M3
May/June 2013
Dr. Joy Sclamberg, Dr. James Cameron, Dr. Aditi Gulabani

• CC: RLQ abdominal pain, constipation, nausea
• HPI: 24 y/o male presents to the ED with 4-6 week h/o progressive vague abd pain with 2 weeks of constipation and watery stool with regular laxative use.
• PMH: Pyloric stenosis (2-3 months old)
• PSH: Pyloroplasty
• Pertinent negatives: vomiting, dysuria, blood in stool, no recent travel, weight loss
• Pertinent positives: fever, chills, fatigue
Clinical History
2
• Focused PE:– Abd: • Horizontal scar noted over RUQ
• Soft, non-tender, not distended
• Bowel Sounds-positive
• Pain to deep palpation of RLQ
• No rebound or guarding
• Notable Labs:– C-Reactive Protein: 181.6
–WBC: 11.68
Clinical History
• Inflammatory Bowel Disease
• Bowel obstruction
• Chronic appendicitis
• Plan– UA- negative
– Abdominal X-ray (obstruction?)
– CT Pelvis/Abd with contrast (IBD, Chronic appendicitis?)
– Colonoscopy
DDx

• Bowel wall thickening
• Mesenteric inflammation (“fat stranding”)
• Lymph node size and number
• Extra-luminal collections– Fistulae, abscesses, sinuses
What are we looking for on CT?

Pelvic Region
Post-contrast Pelvic/Abdominal CT Axial
MRN: 6561716
Accession: 5273942
Diffuse Wall Thickening of Segment of Terminal Ileum
Pelvic Region
Post-contrast Pelvic/Abdominal CT Axial
MRN: 6561716
Accession: 5273942
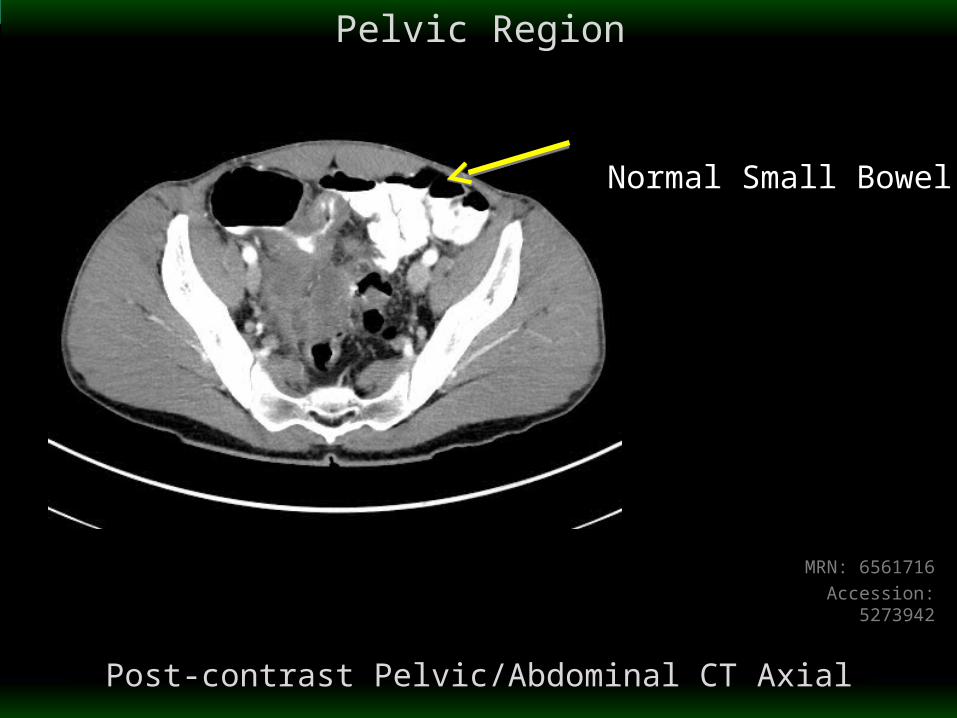
Normal Small Bowel

Pelvic Region
Post-contrast Pelvic/Abdominal CT Axial
MRN: 6561716
Accession: 5273942
Enterocolic Fistula

Pelvic Region
Post-contrast Pelvic/Abdominal CT Axial
MRN: 6561716
Accession: 5273942
Adjacent InflammatoryFat Stranding

Abdomen-Pelvis
Post-contrast Pelvic/Abdominal CT Coronal
MRN: 6561716
Accession: 5273942

Appropriateness Criteria
11
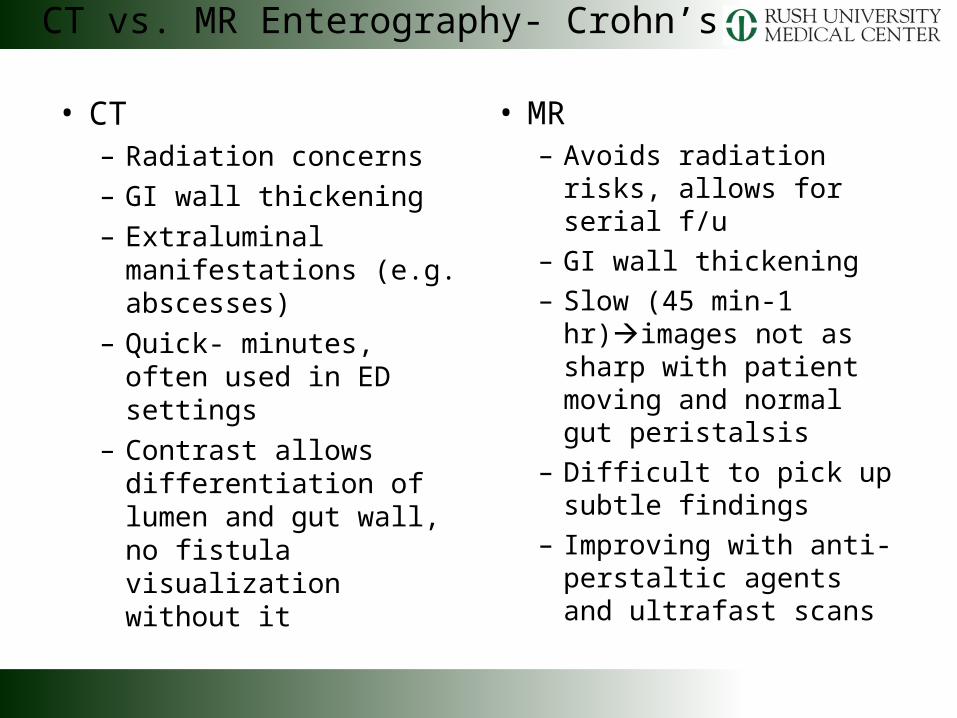
• CT– Radiation concerns
– GI wall thickening
– Extraluminal manifestations (e.g. abscesses)
– Quick- minutes, often used in ED settings
– Contrast allows differentiation of lumen and gut wall, no fistula visualization without it
• MR– Avoids radiation risks,
allows for serial f/u
– GI wall thickening
– Slow (45 min-1 hr)images not as sharp with patient moving and normal gut peristalsis
– Difficult to pick up subtle findings
– Improving with anti-perstaltic agents and ultrafast scans
CT vs. MR Enterography- Crohn’s

CT vs. MR Enterography- Crohn’s
CT
MR- T2 Weighted
http://www.mghradrounds.org/index.php?src=gendocs&link=2009_september

MR Enterography
http://www.radiology.ucsf.edu/patient-care/sections/pediatric/advanced-techniques/imaging2
T2 Weighted, Coronal MR Abdomen
• Inflammatory Bowel Disease
• Transmural inflammation of lining of digestive tract
• Common Signs and Symptoms– Diarrhea
– Abdominal Pain and Cramping
– Blood in stool
– Ulcers
– Decreased appetite and weight loss
Crohn’s Disease
• Complications– Bowel Obstruction
– Ulcers
– Fistulas– Anal Fissure
–Malnutrition
– Colon Cancer
Crohn’s Disease
• Following CT- patient admitted
• Colonscopy– Ileocecal valve: severe ulceration, granularity and
erythema with deformation of the valve
– Single ulcer in sigmoid colon, polyp
• Discharged after with appropriate medication- repeat labs in 2 weeks
Follow Up

• learningradiology.com/notes/ginotes/crohnsdiseasepage.htm
• www.mayoclinic.com/health/crohns-disease/DS00104
• http://emedicine.medscape.com/article/367666-overview
• http://www.mghradrounds.org/index.php?src=gendocs&link=2009_september
References

• Questions?