acute myeloid leukaemia...1 acute myeloid leukaemia mapping the policy response to an acute cancer...
TRANSCRIPT

mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
Acute Myeloid Leukaemia
Supported by:
1Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Contents2 About this report
4 Executive summary
7 Chapter 1: Introduction—what is AML? 7 An acute leukaemia7 A genetically complex malignancy 8 Understanding and quantifying the burden in Europe
13 Chapter 2: Navigating the healthcare and patient care experience 13 Diagnosis and testing for AML20 Mapping the treatment pathway 22 Stem cell transplants—only for younger, fitter patients?
26 Chapter 3: The costs of AML 26 Economic costs of AML 27 Cost of intensive therapy27 Cost of supportive care and less intensive therapy29 Indirect costs29 Impact on patients, their families and carers29 Side effects of treatment30 Fertility preservation: a key consideration for younger patients 32 Psychosocial support is crucial 33 Financial impact on patients
35 Chapter 4: AML heath policy under the spotlight 35 National policy and evidence-based treatment guidelines36 Specialist cancer nurses and the multidisciplinary care team 37 Centralised, specialist centres37 Humanising hospitals39 Vaccination of healthcare staff and reducing infections41 Measuring and monitoring AML 43 Awareness, advocacy and education: the role of patient groups and expert
patients
45 Conclusion

2Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Acute Myeloid Leukaemia: mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK is an Economist Intelligence Unit report, supported by Amgen, a pharmaceutical company. It considers the healthcare system approaches to the management of acute myeloid leukaemia (AML), as well as its costs and patient experience, to make recommendations for policy responses going forward.
The research reviews AML care across five European countries and explores a number of factors that play a part in the development of high-quality services for patients with AML.
This report is based on desk-based research and in-depth interviews with 13 experts drawn from healthcare professionals, patient groups, patients, government organisations and health economists. Our thanks are due to the following for their time and insights (listed alphabetically):
• Simone Boselli, public affairs director, EURORDIS (Rare Diseases Europe)
• Felicetto Ferrara, chief of Haematology Unit, Cardarelli Hospital, Naples, Italy
• Arnold Ganser, director of the Department of Haematology, Haemostasis, Oncology and Stem Cell Transplantation, Hannover Medical School, Germany
• Jan Geissler, steering committee member of the Acute Leukemia Advocates Network (ALAN); founder and chief executive of Patvocates; former director of the European Patients’ Academy (EUPATI); and co-founder of LeukaNET, the CML Advocates Network and the Leukemia Patient Advocates Foundation.
• Deborah Harkins, AML patient; chief officer health and wellbeing (director of public health), Dudley Council, West Midlands, UK
• Alessandro Isidori, professor of haematology, Haematology and Stem Cell Transplant Centre, Marche Nord Hospital, Pesaro, Italy
• Harpreet Kaur, consultant haematologist, Sheffield Teaching Hospitals NHS Foundation Trust, UK
• Pau Montesinos, haematologist, Haematology Department, Hospital Universitari i Politècnic La Fe, València, Spain
About this report

3Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
• Jenna Ostrowski, AML patient, corporate solicitor, Birmingham, UK
• Christian Récher, head of the haematology department, Toulouse University Hospital Centre, Toulouse University Cancer Institute Oncopole, France; and Chairman of the French Innovative Leukemia Organisation (FILO) study group working party on AML.
• Nicola Shepherd, clinical nurse specialist in leukaemia and lymphoma, Guy’s Hospital, London, UK
• Gemma Trout, leukaemia clinical nurse specialist at University College London Hospitals NHS Trust, UK
• Amer Zeidan, associate professor of internal medicine (haematology), Department of Internal Medicine, Yale Cancer Center and Smilow Cancer Hospital, Yale University School of Medicine, US
This report was written by Ingrid Torjesen and edited by Elizabeth Sukkar of The Economist Intelligence Unit. The findings and views expressed in this report are those of The Economist Intelligence Unit and do not necessarily reflect the views of the sponsor.
December 2019

4Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Executive summary
Acute myeloid leukaemia (AML) is the most common form of acute leukaemia in adults, although it is considered a rare disease. The disease often affects older people and is uncommon in people under the age of 45. However, incidence is expected to rise with an ageing population, which will place demands on healthcare systems.
The direct healthcare costs of AML increase with the complexity of the care required and most of the limited research specifically on the direct costs of AML has focused on treatment of younger patients who are fit enough to receive intense treatment.
This report looks at five countries in Europe—France, Germany, Italy, Spain and the UK—finding that the UK has the highest prevalence of the condition, at more than 5,000 cases, while Spain has the lowest, at under 2,300 cases. The condition also has the fifth worst five-year survival by cancer type, after pancreatic, lung, liver and oesophageal cancers, and is responsible for 62% of all leukaemia deaths.
AML occurs when there is a build-up of cytogenetic changes in blood stem cells (haematopoietic stem cells) that interferes with the production of normal blood cells.
Patients initially experience non-distinct symptoms such as fatigue and repeated infections, but as the number of abnormal blood cells (known as blast cells) rises, patients are likely to exhibit bruising and bleeding. Ultimately, their blood will contain so few normal cells that the condition becomes life threatening.
The goal of active treatment is remission, and current approaches are focused on high
intensity chemotherapy and haematopoietic stem cell transplants. These approaches are physically and mentally demanding for patients, requiring several bouts of hospital stays lasting several weeks, and generally only feasible in relatively fit and, therefore, younger patients. Other patients are currently provided with supportive care.
This report looks at the incidence, diagnosis, treatment and costs of AML and the experience of patients in these five European countries, with the aim of highlighting areas of particular attention to policymakers. Based on qualitative interviews and desk-based research, it is clear that there are a number of challenges that policymakers and healthcare professionals will need to address to improve outcomes for those living with AML.
Key findings:
Awareness raising of symptoms among primary care physicians and the public could speed up diagnosis
Although the initial symptoms of AML are indistinct, a simple blood test will show an imbalance of blood cells that warrants urgent investigation. However, as is the case with most rare diseases, patients report difficulties in obtaining a diagnosis. This is especially the case in the UK, where general practitioners (GPs) act as gatekeepers to hospital services (where patients with AML will ultimately receive treatment). Unexplained bleeding or bruising, alongside indistinct symptoms such as fatigue and infections, should prompt a blood test to exclude haematological malignancy. Raising awareness of this among primary care physicians and the public could help to speed up diagnosis for some patients.
5Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Guidelines with a greater focus on holistic management and maximising patients’ quality of life needed
Management of AML in Europe is based primarily on the 2017 European LeukaemiaNet (ELN) guidelines.1 This document is focused on clinical management of the disease in the acute stage. The extent to which patients receive holistic and psychosocial support from a multidisciplinary team and support services varies between and within European countries. Wider-ranging guidance is needed, taking into account treatment side effects, impact on quality of life and need for psychosocial support.
Greater centralisation of services is warranted
The care of rare and complex diseases is usually best placed within a few centres of excellence, so that patients are treated by professionals who have broad experience of managing the condition, as well as access to a wide range of dedicated support services. Experts recommend that this would be the best approach for AML.
Faster genetic testing is required for diagnosis and monitoring
Each patient with AML has a unique profile of cytogenetic abnormalities, and these affect their prognosis and which treatments are most likely to be effective. Therefore, patients with AML should receive genetic testing. The speed at which the results of cytogenetic tests are available post diagnosis to haematologists varies across Europe, from a few days to a few weeks. The results of these tests will become
ever more important as a greater number of targeted therapies, which are only effective for patients with particular mutations and need to be started soon after diagnosis, become available. As the cytogenetics of AML evolve and change, these tests also need to be repeated intermittently to ensure that the management approach taken offers patients the best potential outcome. Such testing allows more accurate detection of minimal residual disease to stratify patients according to their risk of relapse and prognosis.2 Investing in these tests has the potential to improve outcomes for patients.
Improving the care experience for patients
It is not uncommon for patients to spend at least four weeks at a time in hospital to receive intensive chemotherapy, where they will be kept isolated to protect them from infection. Extended visiting hours, and access to free WiFi and television can greatly improve patients’ hospital experience by enabling them to maintain relationships, keep up to date with work or study, and generally remain occupied. Initiatives to provide more “homely” accommodation alternatives to regular hospital wards—or allowing patients to be treated as outpatients where possible—can also have benefits for wellbeing and reduce costs. In the future, greater availability of targeted medications is likely to increase the potential for patients to be treated as outpatients; it would be prudent to design clinical pathways to support this, as well as ensuring the availability to health providers of appropriate services needed to manage more patients closer to home through shared care arrangements.
1 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-08-733196 2 Hante A, Stock W, Kosuri S, “Molecular Minimal Residual Disease Testing in Acute Myeloid Leukemia: A Review for the Practicing Clinician”, Clinical lymphoma, myeloma & leukemia, Vol. 18 No. 10, 2018, pages 636-647. https://linkinghub.elsevier.com/retrieve/pii/S2152-2650(18)30480-4

6Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
A louder patient voice
Most patient support organisations that focus on haematological cancers are small and resource poor, and focused on giving support to patients during active treatment. Patients would benefit if these groups were able to extend the support that they offer to after-care for “survivors” who need advocacy support to help them speak about their experiences to raise awareness of the condition among the public and among policy makers. Expert patients can provide useful support, information and hope for patients recently diagnosed with the disease. Policymakers should involve patient representatives more in decisions in policy and service development around rare acute leukaemia.
Improving data collection will inform service provision
Comprehensive data on the epidemiology, genetics, management and outcomes (survival and minimal residual disease) of AML is not currently collected. Initiatives to improve data collection and share it across Europe should be supported. Where registries exist, they are focused on patients who are actively managed through clinical trials. A more accurate picture of incidence and prevalence is needed so that countries can ensure that their specialist services can cope with the growing number of patients with AML, the right numbers of specialist healthcare staff are trained and recruited, and services and treatments are appropriately funded. Europe-wide collection of anonymised patient data will also support efforts to better understand the disease mechanism of AML, as well as which cytogenetic profiles are linked with the best responses to particular treatments and their long-term outcomes.
7Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
3 Löwenberg B, Rowe JM, “Introduction to the review series on advances in acute myeloid leukemia (AML)”, Blood, Vol. 127, No.1, 2016, epub. https://doi.org/10.1182/blood-2015-10-6626844 Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM. Epidemiology of acute myeloid leukemia: Recent progress and enduring challenges. Blood Rev. 2019 Jul;36:70-87. Doi: 10.1016/j.blre.2019.04.005. Epub 2019 Apr 29.5 Editorial, “Closing in on targeted therapy for acute myeloid leukaemia”, Lancet Haematology, Vol. 6, 2019, page e1. https://doi.org/10.1016/S2352-3026(18)30223-06 Löwenberg B, Rowe JM, “Introduction to the review series on advances in acute myeloid leukemia (AML)”, Blood, Vol. 127, No.1, 2016, epub. https://doi.org/10.1182/blood-2015-10-6626847 Bloodwise, “Acute Myeloid Leukaemia”. https://bloodwise.org.uk/info-support/acute-myeloid-leukaemia8 Löwenberg B, Rowe JM, “Introduction to the review series on advances in acute myeloid leukemia (AML)”, Blood, Vol. 127, No.1, 2016, epub. https://doi.org/10.1182/blood-2015-10-6626849 Ibid.10 De Kouchkovsky I, Abdul-Hay M, “Acute myeloid leukemia: a comprehensive review and 2016 update”, Blood Cancer Journal, Vol. 6, 2016, page e441. http://dx.doi.org/10.1038/bcj.2016.50
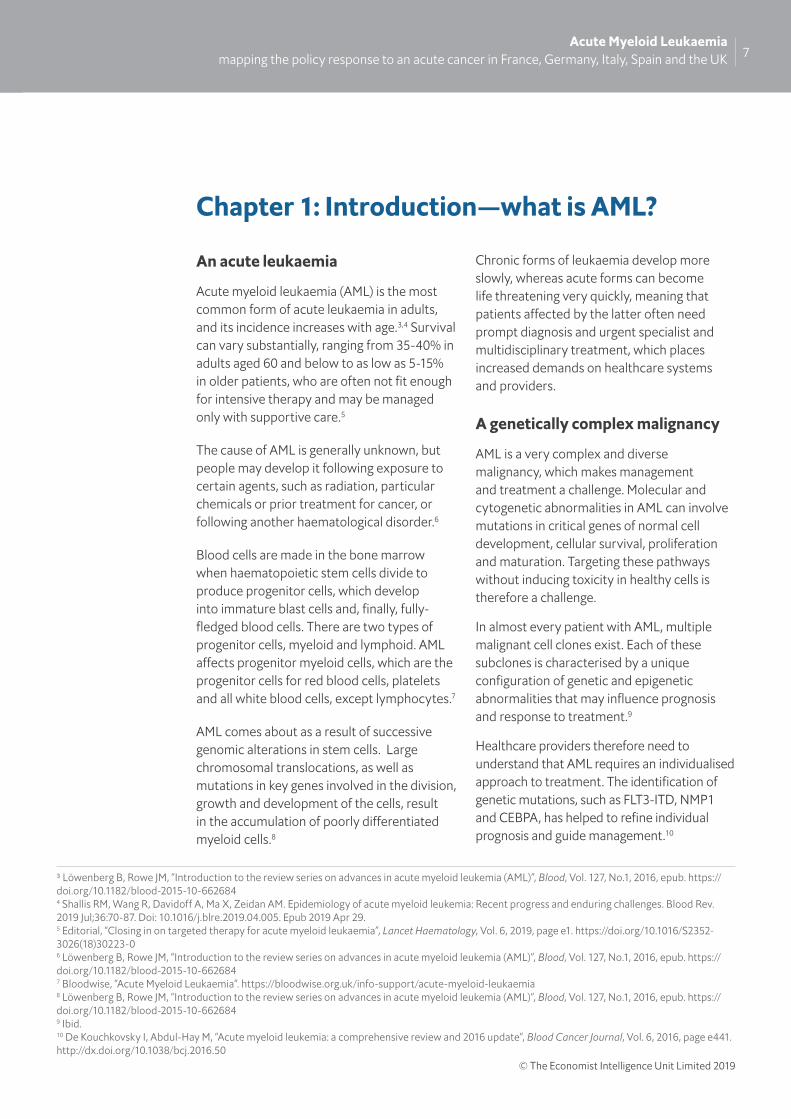
Chapter 1: Introduction—what is AML?
An acute leukaemia
Acute myeloid leukaemia (AML) is the most common form of acute leukaemia in adults, and its incidence increases with age.3,4 Survival can vary substantially, ranging from 35-40% in adults aged 60 and below to as low as 5-15% in older patients, who are often not fit enough for intensive therapy and may be managed only with supportive care.5
The cause of AML is generally unknown, but people may develop it following exposure to certain agents, such as radiation, particular chemicals or prior treatment for cancer, or following another haematological disorder.6
Blood cells are made in the bone marrow when haematopoietic stem cells divide to produce progenitor cells, which develop into immature blast cells and, finally, fully-fledged blood cells. There are two types of progenitor cells, myeloid and lymphoid. AML affects progenitor myeloid cells, which are the progenitor cells for red blood cells, platelets and all white blood cells, except lymphocytes.7
AML comes about as a result of successive genomic alterations in stem cells. Large chromosomal translocations, as well as mutations in key genes involved in the division, growth and development of the cells, result in the accumulation of poorly differentiated myeloid cells.8
Chronic forms of leukaemia develop more slowly, whereas acute forms can become life threatening very quickly, meaning that patients affected by the latter often need prompt diagnosis and urgent specialist and multidisciplinary treatment, which places increased demands on healthcare systems and providers.
A genetically complex malignancy
AML is a very complex and diverse malignancy, which makes management and treatment a challenge. Molecular and cytogenetic abnormalities in AML can involve mutations in critical genes of normal cell development, cellular survival, proliferation and maturation. Targeting these pathways without inducing toxicity in healthy cells is therefore a challenge.
In almost every patient with AML, multiple malignant cell clones exist. Each of these subclones is characterised by a unique configuration of genetic and epigenetic abnormalities that may influence prognosis and response to treatment.9
Healthcare providers therefore need to understand that AML requires an individualised approach to treatment. The identification of genetic mutations, such as FLT3-ITD, NMP1 and CEBPA, has helped to refine individual prognosis and guide management.10

8Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
However, in addition to genetic alterations in the DNA, AML is also affected by epigenetic alterations, which may profoundly disrupt a variety of key intracellular pathways. Epigenetic alterations are changes in gene expression that are inheritable by cell division but not caused by changes in the DNA itself.11
In 2016 the World Health Organisation (WHO) updated its classification of myeloid cancers and acute leukaemias, recognising the significant cytogenetic and molecular subgroups of AML. Although most cases of acute leukaemia or myelodysplastic syndrome are not inherited genetic defects, the WHO recognises that some cases are associated with germline mutations that are inherited.12,13
Other types of AML include:
• therapy-related myeloid neoplasms, where patients develop cancer following cytotoxic treatment;
• AML with myelodysplasia-related changes, which has a particularly poor prognosis and is more common in the elderly;14
• acute promyelocytic leukaemia (APL); this form of AML is considered a medical emergency and managed differently, but is curable if treated promptly.15 Almost all
patients have a specific faulty gene called PML/RARA, where there is a translocation of chromosomes 15 and 17 - t(15;17).16 Patients with suspected APL undergo a different clinical management to AML;
• AML types that do not fit into other groups.17
Understanding and quantifying the burden in Europe
AML is generally a disease of older people and is uncommon before the age of 45. The average age of people when they are first diagnosed with AML is about 68.18,19
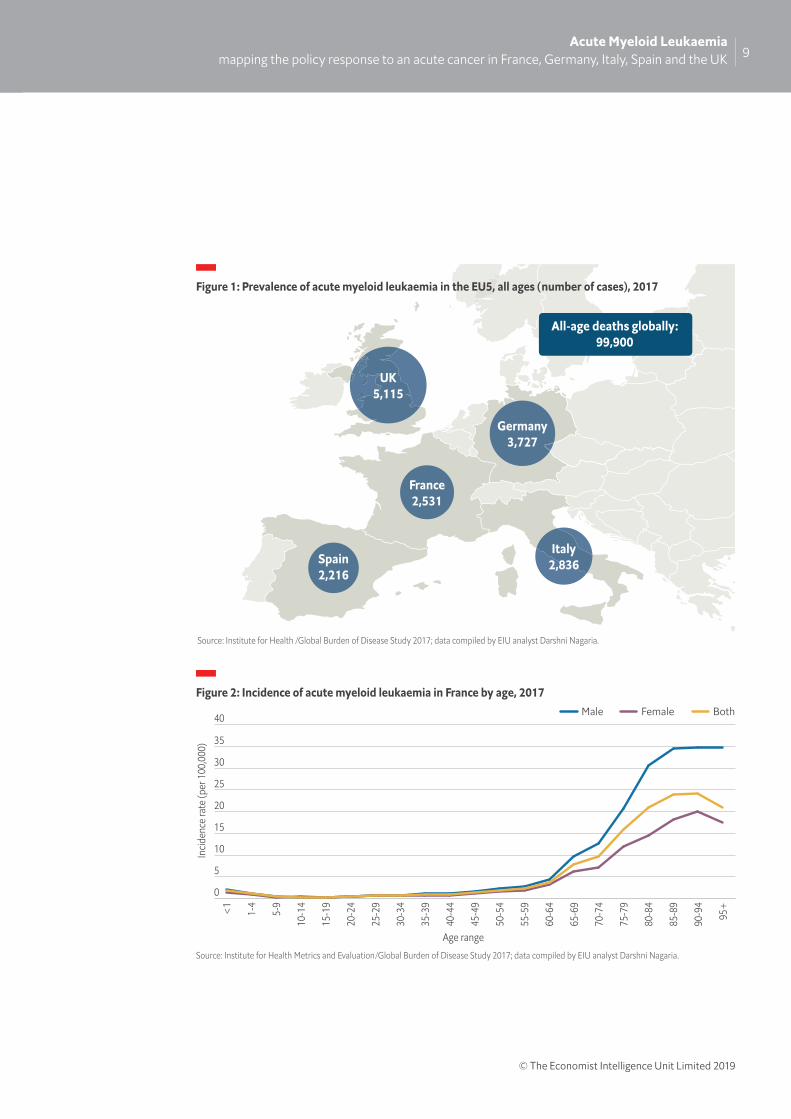
This report looks at five major economies in Europe, finding that the UK has the highest prevalence of AML, at more than 5,000 cases, while Spain has the lowest at under 2,300 cases, according to data from the Global Burden of Disease Study 2017 (see Figure 1 ).
AML is slightly more common among men than women, and the average lifetime risk of AML in both sexes is about 0.5%.20
The incidence of AML is believed to be broadly similar across European countries, at around 3.5 cases per 100,000 population per year (there were an estimated 17,746 new cases in the EU in 2013).21, 22
11 Wouters BJ, Delwel R. Epigenetics and approaches to targeted epigenetic therapy in acute myeloid leukemiaBlood Vol 127, 2016, pages42-52; doi: https://doi.org/10.1182/blood-2015-07-60451212 West AH, Godley LA, Churpek JE, “Familial myelodysplastic syndrome/acute leukemia syndromes: a review and utility for translational investigations”, Ann N Y Acad Sci, Vol. 1310, 2014, pages 111-118. https://doi.org/10.1111/nyas.1234613 Arber DA, Orazi A, Hasserjian R, et al, “The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia”, Blood, Vol. 127, No. 20, 2016, pages 2391-2405. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-03-64354414 American Cancer Society, “Acute Myeloid Leukemia (AML) Subtypes and Prognostic Factors”. https://www.cancer.org/cancer/acute-myeloid-leukemia/detection-diagnosis-staging/how-classified.html15 Sanz MA, Fenaux P, Tallman MS et al, “Management of acute promyelocytic leukemia: Updated recommendations from an expert panel of the European LeukemiaNet”, Blood, Vol. 133, No. 15, 2019, pages 1630-1643. https://doi.org/10.1182/blood-2019-01-894980.16 Bloodwise, “Acute promyoelcytic leukaemia”. https://bloodwise.org.uk/info-support/acute-promyelocytic-leukaemia17 Arber DA, Orazi A, Hasserjian R, et al, “The 2016 revision to the World Health Organization classification of myeloid neoplasms and acute leukemia”, Blood, Vol. 127, No. 20, 2016, pages 2391-2405. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-03-64354418 American Cancer Society, “Key Statistics for Acute Myeloid Leukemia (AML)”. https://www.cancer.org/cancer/acute-myeloid-leukemia/about/key-statistics.html19 Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM, “Epidemiology of acute myeloid leukemia: Recent progress and enduring challenges”, Blood Rev, Vol. 36, 2019, pages 70-87. https://linkinghub.elsevier.com/retrieve/pii/S0268-960X(18)30139-5 20 American Cancer Society, “Key Statistics for Acute Myeloid Leukemia (AML)”. https://www.cancer.org/cancer/acute-myeloid-leukemia/about/key-statistics.html21 Miranda-Filho A, Piñeros M, Ferlay J et al, “Epidemiological patterns of leukaemia in 184 countries: a population-based study”, Lancet Haematol Vol. 5, 2018. Pages e14–24. https://doi.org/10.1016/S2352-3026(17)30232-622 Gatta G, Capocaccia R, Botta L et al, “Burden and centralized treatment in Europe of rare tumours: results of RARECAREnet—a population-based study”, Lancet Oncol, Vol. 18, No. 8, 2017, pages 1022-1039. https://linkinghub.elsevier.com/retrieve/pii/S1470-2045(17)30445-X
9Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Figure 2: Incidence of acute myeloid leukaemia in France by age, 2017
Source: Institute for Health Metrics and Evaluation/Global Burden of Disease Study 2017; data compiled by EIU analyst Darshni Nagaria.
0
5
10
15
20
25
30
35
40 Male Female Both95
+
90-9
4
85-8
9
80-8
4
75-7
9
70-7
4
65-6
9
60-6
4
55-5
9
50-5
4
45-4
9
40-4
4
35-3
9
30-3
4
25-2
9
20-2
4
15-1
9
10-1
4
5-9
1-4
<1
Incid
ence
rate
(per
100
,000
)
Age range
Spain2,216
France2,531
Germany3,727
UK5,115
Italy2,836
All-age deaths globally:99,900
Figure 1: Prevalence of acute myeloid leukaemia in the EU5, all ages (number of cases), 2017
Source: Institute for Health /Global Burden of Disease Study 2017; data compiled by EIU analyst Darshni Nagaria.

10Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Figure 3: Incidence of acute myeloid leukaemia in Germany by age, 2017
Source: Institute for Health Metrics and Evaluation/Global Burden of Disease Study 2017; data compiled by EIU analyst Darshni Nagaria.
Male Female Both
0
5
10
15
20
25
30
35
40
95+
90-9
4
85-8
9
80-8
4
75-7
9
70-7
4
65-6
9
60-6
4
55-5
9
50-5
4
45-4
9
40-4
4
35-3
9
30-3
4
25-2
9
20-2
4
15-1
9
10-1
4
5-9
1-4
<1
Incid
ence
rate
(per
100
,000
)
Age range
Figure 4: Incidence of acute myeloid leukaemia in Italy by age, 2017
Source: Institute for Health Metrics and Evaluation/Global Burden of Disease Study 2017; data compiled by EIU analyst Darshni Nagaria.
Male Female Both
0
5
10
15
20
25
30
3595
+
90-9
4
85-8
9
80-8
4
75-7
9
70-7
4
65-6
9
60-6
4
55-5
9
50-5
4
45-4
9
40-4
4
35-3
9
30-3
4
25-2
9
20-2
4
15-1
9
10-1
4
5-9
1-4
<1
Incid
ence
rate
(per
100
,000
)
Age range
11Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
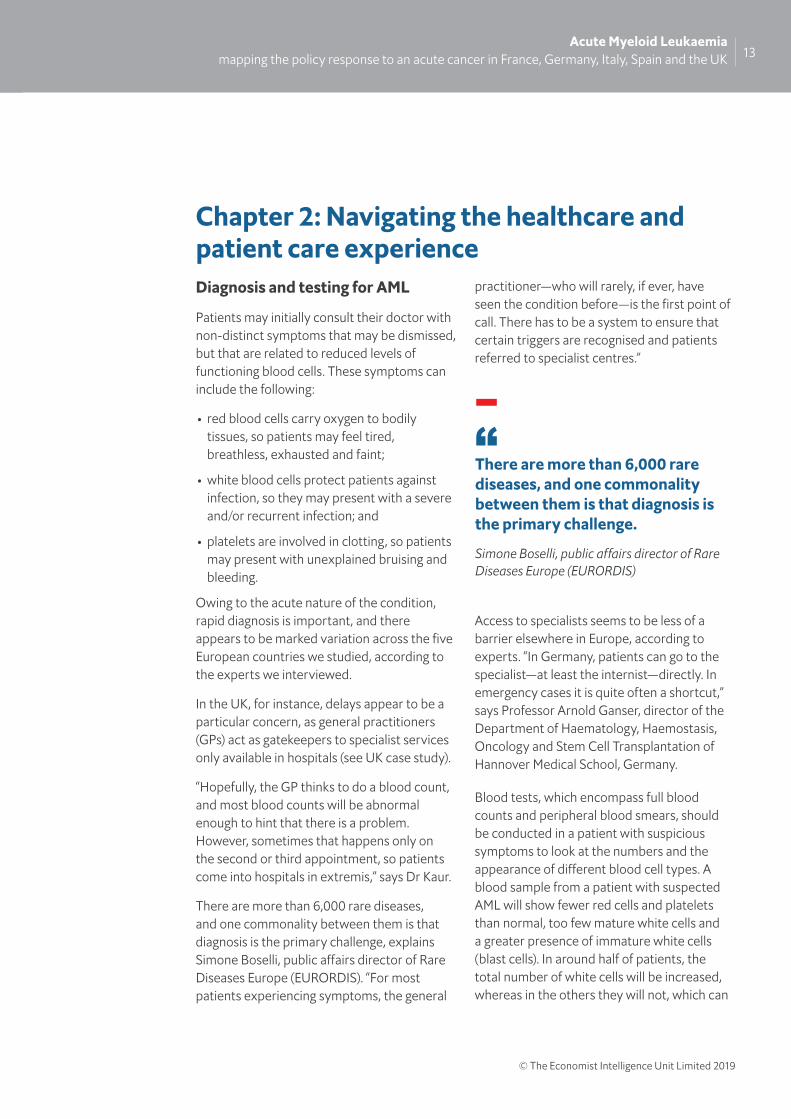
Figure 6: Incidence of acute myeloid leukaemia in UK by age, 2017
Source: Institute for Health Metrics and Evaluation/Global Burden of Disease Study 2017; data compiled by EIU analyst Darshni Nagaria.
Male Female Both
0
10
20
30
40
50
60
70
80
95+
90-9
4
85-8
9
80-8
4
75-7
9
70-7
4
65-6
9
60-6
4
55-5
9
50-5
4
45-4
9
40-4
4
35-3
9
30-3
4
25-2
9
20-2
4
15-1
9
10-1
4
5-9
1-4
<1
Incid
ence
rate
(per
100
,000
)
Age range
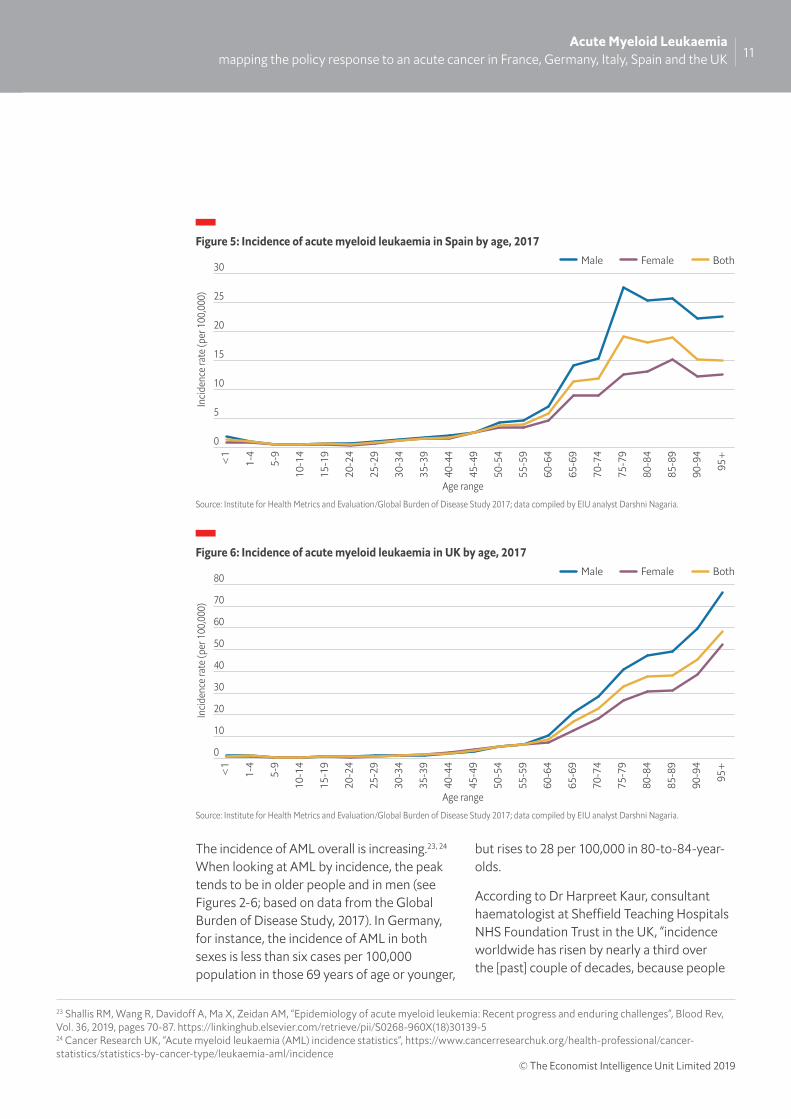
Figure 5: Incidence of acute myeloid leukaemia in Spain by age, 2017
Source: Institute for Health Metrics and Evaluation/Global Burden of Disease Study 2017; data compiled by EIU analyst Darshni Nagaria.
Male Female Both
0
5
10
15
20
25
30
95+
90-9
4
85-8
9
80-8
4
75-7
9
70-7
4
65-6
9
60-6
4
55-5
9
50-5
4
45-4
9
40-4
4
35-3
9
30-3
4
25-2
9
20-2
4
15-1
9
10-1
4
5-9
1-4
<1
Incid
ence
rate
(per
100
,000
)
Age range
23 Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM, “Epidemiology of acute myeloid leukemia: Recent progress and enduring challenges”, Blood Rev, Vol. 36, 2019, pages 70-87. https://linkinghub.elsevier.com/retrieve/pii/S0268-960X(18)30139-5 24 Cancer Research UK, “Acute myeloid leukaemia (AML) incidence statistics”, https://www.cancerresearchuk.org/health-professional/cancer-statistics/statistics-by-cancer-type/leukaemia-aml/incidence
The incidence of AML overall is increasing.23, 24 When looking at AML by incidence, the peak tends to be in older people and in men (see Figures 2-6; based on data from the Global Burden of Disease Study, 2017). In Germany, for instance, the incidence of AML in both sexes is less than six cases per 100,000 population in those 69 years of age or younger,
but rises to 28 per 100,000 in 80-to-84-year-olds.
According to Dr Harpreet Kaur, consultant haematologist at Sheffield Teaching Hospitals NHS Foundation Trust in the UK, “incidence worldwide has risen by nearly a third over the [past] couple of decades, because people

12Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
are living longer and the age of onset is fairly elderly and patients treated with biological agents for other cancers are surviving but damage has been done to other bystander organs, including the bone marrow”.25
Survival rates for rare cancers are lower than for more common cancers, and for AML they are particularly low. AML has the fifth worst five-year survival by cancer type (after pancreatic, lung, liver and oesophageal cancers), and is responsible for 62% of all leukaemia deaths.26
Based on data from 94 cancer registries in Europe from 2000 to 2007, five-year survival for AML in the EU was estimated at 17.5%.27 More recent US data from 2016 estimate five-year survival to be 24%, with median survival of 8.5 months.28 While mortality from chronic forms of leukaemia such as chronic myeloid leukaemia and chronic lymphocytic leukaemia has been falling, the mortality rate for AML remained relatively stable between 2005 and 2016.29
Survival rates for AML vary markedly between age groups owing to the treatment they receive. Approximately 35-40% of patients under 60 years of age may obtain long-term survival with current forms of aggressive treatment, while elderly patients can rarely tolerate aggressive regimens, and so their prognosis is much worse.30 Overall, median overall survival for a patient diagnosed aged 65 years or more is 2.7 months, and nearly 80% of patients in this group will die within one year, with the most elderly having the shortest survival time.31
Across patients receiving aggressive treatment there is also a wide variation in survival, due to the range of genetically distinguishable subsets of the disease, with some subtypes having particularly poor outcomes.
European LeukaemiaNet classifies patients into three prognostic risk groups according to their genetics: favourable, intermediate and adverse.32 Validation of this classification in the under 60s found five-year survival rates to be 57% in the favourable group, 37% in the intermediate group and 18% in the adverse group.33 In the over 60s, another study found three-year overall survival for patients with a favourable prognosis to be 30%; this drops to 12% for those in the intermediate group and 6% in the adverse risk group.34
25 Ibid.26 Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM, “Epidemiology of acute myeloid leukemia: Recent progress and enduring challenges”, Blood Rev, Vol. 36, 2019, pages 70-87. https://linkinghub.elsevier.com/retrieve/pii/S0268-960X(18)30139-5 27 Gatta G, Capocaccia R, Botta L et al, “Burden and centralized treatment in Europe of rare tumours: results of RARECAREnet—a population-based study”, Lancet Oncol, Vol. 18, No. 8, 2017, pages 1022-1039. https://linkinghub.elsevier.com/retrieve/pii/S1470-2045(17)30445-X 28 Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM, “Epidemiology of acute myeloid leukemia: Recent progress and enduring challenges”, Blood Rev, Vol. 36, 2019, pages 70-87. https://linkinghub.elsevier.com/retrieve/pii/S0268-960X(18)30139-5 29 Ibid.30 Editorial, “Closing in on targeted therapy for acute myeloid leukaemia”, Lancet Haematology, Vol. 6, 2019, page e1. https://doi.org/10.1016/S2352-3026(18)30223-0 31 Shallis RM, Wang R, Davidoff A, Ma X, Zeidan AM, “Epidemiology of acute myeloid leukemia: Recent progress and enduring challenges”, Blood Rev, Vol. 36, 2019, pages 70-87. https://linkinghub.elsevier.com/retrieve/pii/S0268-960X(18)30139-5 32 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-08-733196 33 Prajwal C, Boddu MD, Tapan M, Kadia MD, Garcia-Manero G et al, “Validation of the 2017 European LeukemiaNet classification for acute myeloid leukemia with NPM1 and FLT3‐internal tandem duplication genotypes”, Cancer Vol. 125, No. 7, 2019, pages 1091-1100. https://doi.org/10.1002/cncr.3188534 Eisfeld AK, Kohlschmidt J, Mrozek K, et al, “Mutation patterns identify adult patients with de novo acute myeloid leukemia aged 60 years or older who respond favorably to standard chemotherapy: an analysis of alliance studies”, Leukemia, Vol. 32, 2018, pages 1338‐1348. http://dx.doi.org/10.1038/s41375-018-0068-2
Five-year survival for AML is estimated to be around 24%
13Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Chapter 2: Navigating the healthcare and patient care experience Diagnosis and testing for AML
Patients may initially consult their doctor with non-distinct symptoms that may be dismissed, but that are related to reduced levels of functioning blood cells. These symptoms can include the following:
• red blood cells carry oxygen to bodily tissues, so patients may feel tired, breathless, exhausted and faint;
• white blood cells protect patients against infection, so they may present with a severe and/or recurrent infection; and
• platelets are involved in clotting, so patients may present with unexplained bruising and bleeding.
Owing to the acute nature of the condition, rapid diagnosis is important, and there appears to be marked variation across the five European countries we studied, according to the experts we interviewed.
In the UK, for instance, delays appear to be a particular concern, as general practitioners (GPs) act as gatekeepers to specialist services only available in hospitals (see UK case study).
“Hopefully, the GP thinks to do a blood count, and most blood counts will be abnormal enough to hint that there is a problem. However, sometimes that happens only on the second or third appointment, so patients come into hospitals in extremis,” says Dr Kaur.
There are more than 6,000 rare diseases, and one commonality between them is that diagnosis is the primary challenge, explains Simone Boselli, public affairs director of Rare Diseases Europe (EURORDIS). “For most patients experiencing symptoms, the general
practitioner—who will rarely, if ever, have seen the condition before—is the first point of call. There has to be a system to ensure that certain triggers are recognised and patients referred to specialist centres.”
Access to specialists seems to be less of a barrier elsewhere in Europe, according to experts. “In Germany, patients can go to the specialist—at least the internist—directly. In emergency cases it is quite often a shortcut,” says Professor Arnold Ganser, director of the Department of Haematology, Haemostasis, Oncology and Stem Cell Transplantation of Hannover Medical School, Germany.
Blood tests, which encompass full blood counts and peripheral blood smears, should be conducted in a patient with suspicious symptoms to look at the numbers and the appearance of different blood cell types. A blood sample from a patient with suspected AML will show fewer red cells and platelets than normal, too few mature white cells and a greater presence of immature white cells (blast cells). In around half of patients, the total number of white cells will be increased, whereas in the others they will not, which can
There are more than 6,000 rare diseases, and one commonality between them is that diagnosis is the primary challenge.
Simone Boselli, public affairs director of Rare Diseases Europe (EURORDIS)

14Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
sometimes be misleading for the GP, according to Dr Ganser.
Blood does not usually contain blast cells, and they usually only make up less than 5% of cells in the bone marrow.35 A diagnosis of AML requires at least 20% blast cells in the marrow or blood, unless genetic testing shows that the blasts have a specific chromosome change (translocation or inversion), such as t(15;17), t(8;21), inv(16), or t(16;16).36 Presence of the specific chromosomal change t(15;17) indicates a particular subtype of AML called APL.37
If blood tests suggest AML, a bone marrow aspiration or biopsy will be carried out to confirm the diagnosis. This involves removing a small sample, usually from the iliac crest (part of the largest of one of the three hip
bones), to allow the cells to be examined under microscope.
Cytogenetic and molecular analyses play a critical role in the diagnosis, classification, prognosis and management of AML, and are usually carried out on aspirate samples taken from the bone marrow, but can be carried out on blood (see box).
“Genetically, we have improved our understanding of myeloid disorders in the last six or seven years and that’s accelerated in the last two to three years,” says Dr Kaur. “So much so that the research into genetic testing has rolled out into the clinical realm, both to give information about the patient’s disease—how they’re likely to do, the prognostic information—and, moving forward, what can we do about it in terms of targeted therapy.”
35 American Cancer Society, “Tests for Acute Myeloid Leukemia (AML)”. https://www.cancer.org/cancer/acute-myeloid-leukemia/detection-diagnosis-staging/how-diagnosed.html36 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-08-733196 37 Sanz MA, Fenaux P, Tallman MS et al, “Management of acute promyelocytic leukemia: Updated recommendations from an expert panel of the European LeukemiaNet”, Blood, Vol. 133, No. 15, 2019, pages 1630-1643. https://doi.org/10.1182/blood-2019-01-894980.
For some patients living with AML, a bone marrow biopsy/aspiration can be an unpleasant experience. UK patient Jenna Ostrowski, a solicitor based in Birmingham, received a new type of therapy through a clinical trial and now has a bone marrow aspiration every three months to monitor her progress.
“They really are ridiculously painful, and then you have to wait a few weeks to get
the results and that’s quite stressful,” she says. “If they could develop it and have it as a blood test that would be amazing. I have heard that if you’re elderly or if you’re a child you get an anaesthetic. The rest of us just have the option of having gas and air, which I always opt for. They are just horrible. It’s a pain I can’t describe. It feels like somebody is taking a needle to your bone, which is exactly what they are doing.”
Patient experience of bone marrow aspiration/biopsy

15Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Microscopic analysis can detect major structural or numerical chromosome abnormalities (karyotyping), and this can be supported by more sensitive techniques such as fluorescence in-situ hybridisation (FISH) and microarray comparative genomic hybridisation to determine the presence, absence, position and copy number of DNA segments.
Specific tests can also screen for specific mutations that may be associated with a worse or better prognosis or suggest that a particular treatment may be beneficial. Currently, patients are usually screened for at least NPM1, FLT3 and CEBPA mutations, following recommendations first made in the previous European LeukaemiaNet (ELN) guidelines in 2010, and the number of tests for specific genetic markers continues to grow.38
Around 30% of AML patients carried FLT3 mutations39 which can indicate that the patient may benefit from certain treatments; NPM1 and CEBPA mutations generally indicate a better prognosis, while mutations in RUNX1, TP53 and ASXL1 are associated with poorer prognosis. However, the expected outcome will differ according to the range of mutations present. For example, while NPM1 mutations are generally associated with better prognosis, if FLT3 is also present it would indicate a poorer prognosis. Mutations in both ASXL1 and RUNX1 confer a particularly poor prognosis.40
As management of the condition may be influenced by the results of molecular tests, it is important to have these results in good time.41 Previously it was important to have the results of cytogenetic tests within a few weeks after the commencement of induction chemotherapy, as the sole purpose was to provide information on prognosis and determine whether a younger, fit patient should undergo allogeneic stem cell transplantation. However, the ability to add targeted therapy to induction chemotherapy has meant that the results are needed sooner, according to the experts that we spoke to.
The 2017 ELN guidelines recommend that results from cytogenetics should be available preferably within five to seven days, and results from NPM1 and FLT3 mutational screening within 48-72 hours, at least for patients eligible for intensive chemotherapy. Any further molecular genetic results should be available within the first treatment cycle.42 However, speed of access varies markedly across the five European countries covered in this report (see table).
38 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-08-733196 39 Daver N, Schlenk RF, Russell NH et al, “Targeting FLT3 mutations in AML: review of current knowledge and evidence”, Leukemia, Vol. 33, 2019, pages 299–312. http://dx.doi.org/10.1038/s41375-018-0357-9 40 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-08-733196 41 He J, Abdel-Wahab O, Nahas MK et al, “Integrated genomic DNA/RNA profiling of hematologic malignancies in the clinical setting”, Blood, Vol. 127, No. 24, 2016. pages 3004-3014. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2015-08-66464942 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2015-08-664649
The 2017 ELN guidelines recommend that results from cytogenetics should be available preferably within five to seven days.

16Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Jenna Ostrowski, 35, started experiencing intermittent headaches and infections that she could not shake off, for which she was prescribed antibiotics by her GP. She put these symptoms down to being busy at work and took time off for a holiday to Bali.
While there she developed what she thought was a gum infection—her gums kept bleeding and became quite ulcerated, and she had a temperature and felt very unwell.
On her return, unable to get a same day appointment with her regular GP or dentist, Ms Ostrowski called NHS 111, the UK health service helpline, and they suggested that she went to an emergency dental hospital, where, again, she was given antibiotics. After two weeks, the gum problem had not cleared up, and the headaches were becoming more persistent, so she went to see her regular dentist. He felt her glands and noticed that she had quite a few bruises on her legs. He told her that he didn’t think she had a gum infection and that something else was going on; he advised her to make an urgent appointment with her GP and to ask her GP to call him.
“I went to my GP, who said that he didn’t need to phone my dentist. I went through my symptoms and the GP said that he couldn’t talk about my headache in that appointment, because it was only a ten-minute appointment and I was giving him too many symptoms. He said that if I wanted to discuss my headaches then
I should book into the headache clinic separately,” Jenna says. “I said “I think the symptoms are linked … I think there’s something going on”. He turned around to me and said “with all due respect you’re not a medical professional”.” The GP finally agreed to give Jenna a blood test, but the GP’s receptionist told her that there wasn’t one available at the surgery for 2.5 weeks.
“I didn’t want to wait that long because I was obviously panicked,” says Ms Ostrowski, “so I phoned my private health insurance through work, and they said that I could get a blood test next morning if I went to a private hospital.”
She went to the private hospital the next morning and the results were sent to her NHS GP who phoned her at lunchtime and told her that her results were “severely abnormal”. “The GP said that he would urgently refer me to a consultant haematologist. The impression I got was that it would take a couple of weeks.
“I went into panic mode, because I had actually lost my uncle to blood cancer seven years earlier, when he was just 40 years of age. I made a few calls to try to get an appointment with a private haematologist through my private health insurance. At around 8:00pm that evening I had a phone call from a mobile number I didn’t recognise. It was a consultant haematologist, and he sounded very worried and told me to come to the private hospital as soon as possible and bring an overnight bag.
UK case study: My GP dismissed my symptoms, but my dentist recognised them

17Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Dr Alessandro Isidori of the Haematology and Stem Cell Transplant Centre at Marche Nord Hospital in Pesaro, Italy, says that it is important to have all this information within one week of diagnosis of AML, because certain therapy and care decisions must be made within seven days.
Germany is an example of what can be done elsewhere in Europe, thinks Professor Christian Récher, head of haematology at Toulouse University Hospital Centre, Toulouse University Cancer Institute Oncopole, France, and Chairman of the French Innovative Leukemia Organisation (FILO) study group working party on AML. “All of Europe should also try to respond in a few days,” he says. “I hope that in the months or years to come France will be able to offer faster testing. It is a huge objective for us to cover all patients in France.”
Stratifying older patients with cytogenetics or molecular data is becoming increasingly important. Older patients are often reluctant to have chemotherapy because of adverse effects, and the presence of certain karyotypes or mutations can indicate that they will be less likely to respond, and so can be given other agents instead, Mr Récher explains. And now, with the approval of new therapies on the cards, this information is going to be needed for patients in their 70s and 80s who can benefit much earlier, he adds. Cytogenetic tests should be performed again to assess the deepness of response, he says, but at the moment in France this is only happening at some big centres. “It is very important to understand if our patient is responding very well or not, so we know whether to continue the treatment or change it.” (See Case study: use of molecular testing to monitor patients in Germany.)
“The consultant saw my bruises when I arrived and asked how long I had them. Then he took me up into a room and told me I had leukaemia. I was given a platelet transfusion straightaway. The next day I was admitted to an NHS hospital, where I spent the most part of seven months in an isolation room, having four rounds of chemotherapy, with just short breaks at home between the rounds of chemotherapy.”
“If I had waited for the GP, there’s a chance that I would’ve been dead by then—that’s something they told me, given how far advanced my leukaemia was,” Ms Ostrowski says.
“When I got to the hospital, they said it was pretty bad, and that if they hadn’t started chemotherapy within a few days, I may have had as little as a week before things got really bad.”

18Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Table. Speed of cytogenic testing—views from the haematologists
European guidelines recommend that results from cytogenetics should be available within five to seven days, and results from NPM1 and FLT3 mutations within 48 to 72 hours (at least in patients eligible for intensive chemotherapy).43
Germany
“Genetic testing is done in almost every patient now. In our two major centralised laboratories for molecular testing we do it within 48 hours after arrival of the samples. In Germany it is very quick because we work at night and at weekends,” says Professor Arnold Ganser, director of the Department of Haematology, Haemostasis, Oncology and Stem Cell Transplantation of Hannover Medical School. Outside the main centres in Germany, it may take a little longer, he adds.
Italy
“We have a very fast [genetic] test for APL [a type of AML]. In two hours, I have the results. Regarding other molecular testing it might take a little bit longer, five to seven days at the upmost,” says Dr Alessandro Isidori of the Haematology and Stem Cell Transplant Centre at Marche Nord Hospital in Pesaro.
Spain
“We have the availability for rapid diagnostic testing for patients in the vast majority of institutions. With younger patients, we are trying to start therapy as soon as possible. Within seven days we will usually have the results of tests to decide whether to include targeted therapy,” says Dr Pau Montesinos of the Haematology Department at Hospital Universitari i Politècnic La Fe in Valencia.
France
Professor Christian Récher, head of the Haematology Department at Toulouse University Hospital Centre, Toulouse University Cancer Institute Oncopole, and Chairman of the FILO study group working party on AML, suspects that the turnaround in France is somewhere between the UK and Germany. “In France I think most patients can have [test results] in one to two weeks.”
UK
The UK 2012 cytogenetic guidelines44 recommend a two-week turnaround time, which needs updating, says Dr Harpreet Kaur, consultant haematologist at Sheffield Teaching Hospitals NHS Foundation Trust. These guidelines were produced long before the availability of licensed drugs which require the patient to “have a particular genetic make up to be eligible for them,” and need to be started early in treatment. Some specialists in the UK report turnarounds of 28-31 days, she adds.
43 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2015-08-664649 44 Association for Clinical Cytogenetics, “Professional Guidelines for Clinical Cytogenetics. Acute myeloid leukaemia and myelodysplastic syndromes, 2012”. https://www.acgs.uk.com/media/10780/acc_aml_mds_bp_mar2012_100.pdf
19Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Germany is a leader in rapid molecular diagnostics, according to Dr Ganser, and academic centres in the country are now using it to monitor response to therapy.45, 46
Traditionally, patients will undergo bone marrow aspiration every three months and the bone marrow cells that are collected are examined under microscope. A patient will be considered to be in remission if there are fewer than 5% blast cells.
Molecular testing allows more accurate detection of minimal residual disease (MRD) to stratify patients according to their risk of relapse and prognosis.47 For assessing MRD to predict risk of relapse, explains Dr Ganser, “molecular monitoring is 1,000 times more sensitive than using a microscope”.
“With molecular diagnostics, we can identify one in 10,000 [one malignant cell with the mutation among 10,000 normal nucleated white blood cells], so sometimes we can say the patient doesn’t have to go to transplant, the patient is already probably cured, with much more certainty than before.
“We also pick up relapses earlier, and we can start therapy again before the patient has a full relapse, so patients who haven’t yet had
transplantation can go to transplantation in a much better shape with better outcomes.”
Dr Ganser explains that at his centre molecular testing is conducted every three months. One advantage is that they can use blood cells, and do not always have to take a bone marrow sample, which can place a burden on patients and healthcare providers.
“The tests are more sensitive with bone marrow, but our test systems are also very good using just blood, and it is easier for the patient,” says Dr Ganser. “For a patient who has to undergo bone marrow aspiration every three months, that makes a difference.”
He says that many patients in Germany receive molecular testing, as the country has several laboratories that are “really good at it and fulfil the quality requirements”.
Ultimately, molecular testing could potentially be used to decide to stop therapy completely in patients who appear to have gone into remission. “I think we are getting closer to that, but at least we are able to take the decision on whether to prepare a patient for transplant or not—that’s already a major difference.”
Case study: use of molecular testing to monitor patients in Germany
45 Schuurhuis GJ, Heuser M, Freeman S et al, “Minimal/measurable residual disease in AML: a consensus document from the European LeukemiaNet MRD Working Party”, Blood, Vol. 131, No. 12, 2018, pages 1275-1291. doi: 10.1182/blood-2017-09-801498. 46 Zach O, Clausen J, “Molecular monitoring of minimal residual disease in acute leukemia”, Magazine of European Medical Oncology, Vol. 7, No. 3, 2014, pages 144–147. https://link.springer.com/article/10.1007/s12254-014-0169-147 Hante A, Stock W, Kosuri S, “Molecular Minimal Residual Disease Testing in Acute Myeloid Leukemia: A Review for the Practicing Clinician”, Clinical lymphoma, myeloma & leukemia, Vol. 18, No. 10, 2018, pages 636-647. https://linkinghub.elsevier.com/retrieve/pii/S2152-2650(18)30480-4

20Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Mapping the treatment pathway
The management and treatment of AML involves a complex path involving many healthcare professionals in healthcare systems (see Figure 7).48 According to the experts we spoke to, AML management in Europe is mainly based on the ELN guidelines.
Figure 7: Treatment algorithm for acute myeloid leukaemia
Source: Adapted from UCLH Cancer Collaborative- The Cancer Alliance for north and east London. "Pan-London Haemato-Oncology Clinical Guidelines: acute leukaemias and myeloid neoplasms, Part 2: acute myeloid leukaemia", September 2018.
Diagnosis
Start supportive treatment, consider emergency cytoreduction with
chemotherapy and sperm cryopreservation
Patient fit for high intensity chemotherapy
Second induction followed by 1-2 consolidation chemotherapy cycles
Patient not fit for high intensity chemotherapy
Supportive care + low intensity treatment
Induction chemotherapy, consider tyrosine kinase inhibitors if FLT3 mutation detected
Remission
Low High
Refractory
Fit for re-induction?Risk of relapse assessment
Yes No
Consider stem cell transplant
Remission Refractory
These guidelines suggest that assessment is based on a number of factors, including the performance status of the patient, the level of significant comorbidities and an adverse cytogenetic or molecular genetic profile. The ELN guidelines also highlight that there are various tools that can aid healthcare professionals in AML assessment.
48 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2015-08-664649

21Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
After diagnosis, patients with high blast counts may require emergency cytoreductive treatment.49 In addition, most patients need transfusions of red blood cells and platelets. The patient is then assessed to determine whether they are suitable for intensive induction chemotherapy, based on the risk of treatment-related mortality with the regimen.
Some countries, such as Italy, assess fitness using a formal tool, whereas others, such as the UK, do not.50 In the UK, “you get a general impression of a patient’s fitness when they walk into your clinic, and then you ask them very targeted questions about the rest of their health,” says Dr Kaur.
Few patients over 65 are suitable for intensive chemotherapy, as they are likely to have a greater number of comorbidities. However, in recent years a growing number of patients aged over 60 have been offered intensive chemotherapy, as fitness levels among older people have generally increased.51 Some such patients can tolerate intensive chemotherapy, and can potentially benefit from improved quality of life in the long term.52, 53 “The older patients get better and better,” says Mr Récher. “They are in better health generally than 20 or 30 years ago.”
Intensive treatment, which aims to induce remission, begins with a general course of high-intensity induction chemotherapy aimed at reducing the blast count dramatically, which may be supplemented with specific drugs in patients with certain mutations. Patients who do not respond will receive another course of induction therapy, and responders can expect to receive at least one to two courses of consolidation chemotherapy. Patients who are resistant to chemotherapy or at high likelihood of relapse will be considered for a stem cell transplant.54
“In the Toulouse area,” says Mr Récher, “we have improved the overall survival in patients by the means of intensive chemotherapy, by
49 Röllig C , Ehninger G, “How I treat hyperleukocytosis in acute myeloid leukemia” Blood, Vol. 125, No. 21, 2015, pages 3246-3252. https://doi.org/10.1182/blood-2014-10-55150750 Ferrara F, Barosi G, Venditti A et al, “Consensus-based definition of unfitness to intensive and non-intensive chemotherapy in acute myeloid leukemia: a project of SIE, SIES and GITMO group on a new tool for therapy decision making”, Leukemia, Vol. 27, No. 5, 2017, pages 997-999. http://dx.doi.org/10.1038/leu.2012.303 51 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2015-08-664649 52 Mohamedali H, Breunis H, Timilshina N et al, “Older age is associated with similar quality of life and physical function compared to younger age during intensive chemotherapy for acute myeloid leukemia”, Leukemia Research, Vol. 36, No. 10, 2012, pages 1241-48. https://linkinghub.elsevier.com/retrieve/pii/S0145-2126(12)00245-753 Alibhai SM; Breunis H; Timilshina N et al, “Quality of life and physical function in adults treated with intensive chemotherapy for acute myeloid leukemia improve over time independent of age”, Journal Of Geriatric Oncology, Vol. 6, No. 4, 2015, pages 262-71. https://linkinghub.elsevier.com/retrieve/pii/S1879-4068(15)00031-454 Bertoli S, Tavitian S, Huynh A, Borel C, Guenounou S, Luquet I, Delabesse E, Sarry A, Laurent G, Attal M, Huguet F, Bérard E, Récher C, “Improved outcome for AML patients over the years 2000-2014”, Blood Cancer J, Vol. 7, No. 12, 2017, page 635. https://www-ncbi-nlm-nih-gov.proxy.insermbiblio.inist.fr/pubmed/29184070
The older patients get better and better. They are in better health generally than 20 or 30 years ago.
Christian Récher, head of haematology department, Toulouse University Hospital Centre, France

22Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
a better understanding of the chemotherapy dosing, supportive care (new antifungal treatments) and [by] refining the indications for stem cell transplantation.”
Patients unsuitable for high -intensity chemotherapy receive supportive care. This includes prophylaxis to reduce the chance of (and treat) infections, blood and platelet transfusions, and, in some cases, therapy to reduce bruising and bleeding. Some may also receive low-intensity therapy to prolong survival slightly and improve quality of life.55
According to Dr Amer Zeidan, associate professor of internal medicine (haematology) in the Department of Internal Medicine at Yale Cancer Center and Smilow Cancer Hospital, “the lack of well-tolerated, effective oral therapies, until recently, is one major reason why many older AML patients are not receiving active therapy.”
The ELN guidelines point out that treatment of unfit patients and most older patients is “currently unsatisfactory” and “strongly recommends” enrolling these patients in clinical trials.56 After several decades of little advancement in the management of AML, new therapies are on the horizon. In some cases, they have already been made available to patients in Europe through clinical trials.
Stem cell transplants—only for younger, fitter patients?
AML is the most frequent indication for haematopoietic stem cell transplants from an allogeneic donor and the number of such transplants performed worldwide is rising.57
The decision to perform an allogeneic stem cell transplant is based on a risk-benefit assessment that looks at the risk of mortality, morbidity and relapse. It also considers the cytogenetic features of the cancer and the patient’s fitness levels. Several formal risk scores for assessing patients exist.58 Allogeneic stem cell transplant is generally recommended when the relapse incidence without the procedure is expected to be more than 35%.59 It is likely that roughly 30-40% of patients with AML will undergo a stem cell transplant at some stage, experts we spoke to suggest, although the proportion will decrease with the age of the patient.
Across the five European countries we studied, we found little variation in approaches. Spain, for instance, is on par with average transplant activity rates in other European countries, according to Dr Pau Montesinos, a haematologist at the Haematology Department of the Hospital Universitari i Politècnic La Fe in Valencia. “In European
55 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2015-08-66464956 Ibid.57 Ibid.58 Elsawy M, Sorror ML, “Up-to-date tools for risk assessment before allogeneic hematopoietic cell transplantation”, Bone Marrow Transplant, Vol. 51, No. 10, 2016, pages 1283-1300. http://dx.doi.org/10.1038/bmt.2016.14159 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2015-08-664649

23Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
countries, around one-third of the younger patients receive transplants during frontline therapy, and many patients receive it in the relapse setting.”
In Italy, says Dr Isidori, around 30-40% of patients living with AML would receive a transplant, while in France, according to Mr Récher, more patients have received transplants in the last ten years, as have a higher number of older patients. “Nowadays it’s not rare to propose transplantation for a patient older than 55 years, something that we didn’t practice 15 years ago. I can see that increasing further,” he says.
In Germany, Dr Ganser thinks that stem cell transplants have a real upper limit of 70 or 75 years. “Above 65 years of age, fewer than 10% of patients receive a transplant,” he says.
Crucial to any transplantation service, healthcare systems need a steady stream of donors, and Germany has been very successful in recruiting donors to its stem cell register (see Box: Germany—a world leader
in stem cell donation). Healthcare providers need to undertake a number of procedures before performing the transplant. To reduce the likelihood of complications and immune system reactions, such as graft-versus-host disease (GvHD) or rejection of the graft, the donor’s stem cells must be of a tissue type that closely matches the patient’s, so the best donor is often a close relative. Donors can include a sibling, parent, cousin or child, or a matched unrelated donor.
Before the transplant takes place, the patient is usually admitted to hospital to undergo a course of conditioning therapy, using intensive chemotherapy alone or in combination with total body irradiation.60 Myeloablative regimens to kill bone marrow and cancer cells are generally recommended for younger patients in otherwise good clinical condition, and reduced intensity conditioning regimens can allow allogeneic transplantation in older patients.61 However, few elderly patients living with AML undergo transplantation because of comorbidities, toxicity of prior therapy, inability to achieve remission and early relapse or refractory leukaemia.62
Autologous transplants are occasionally used for people with AML who are in remission after initial treatment, do not have a matched donor for an allogeneic transplant, and have relapsed and need high-dose treatment. This involves giving the patient back their own stem cells after the treatment. These stem cells would
60 Ibid.61 Ibid.62 Ibid.
In Italy, around 30-40% of patients living with AML would receive a transplant.
Alessandro Isidori, professor of haematology, Marche Nord Hospital, Italy

24Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
have been collected while the patient is in remission and stored, so may contain some cancerous cells.
It can be difficult to find a matched donor in various countries, particularly for patients who are of mixed race or from an ethnic minority.63,
64 Because of this, efforts to encourage more people to register as donors are important.
“The problem, of course, is that the potential donors are mainly Caucasians, so if you have African, Middle Eastern, Indian or Chinese origins, or if you have children of mixed
nationalities, it is much more difficult to find somebody,” says Dr Ganser.
In the next chapter we will look at the impact of AML in terms of the cost burden on health systems and the effects that the disease has on patients, their families and carers. This includes the short-and long-term effects of treatment and their impact on quality of life, the need for psychosocial support for patients and their carers, and the financial consequences of being out of the workforce for long periods during treatment and recovery.
63 Passweg JR, Baldomero H, Bader P, Basak GW, Bonini C, Duarte R, Dufour C, Kröger N, Kuball J, Lankester A, Montoto S, Nagler A, Snowden JA, Styczynski J, Mohty M; European Society for Blood and Marrow Transplantation (EBMT), “Is the use of unrelated donor transplantation leveling off in Europe? The 2016 European Society for Blood and Marrow Transplant activity survey report”, Bone Marrow Transplant, Vol. 53, No. 9, 2018, pages 1139-1148. http://dx.doi.org/10.1038/s41409-018-0153-1 64 Switzer GE, Bruce JG, Myaskovsky L et al, “Race and ethnicity in decisions about unrelated hematopoietic stem cell donation”, Blood, Vol. 121, No. 8, 2013, pages 1469–1476. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2012-06-437343
25Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
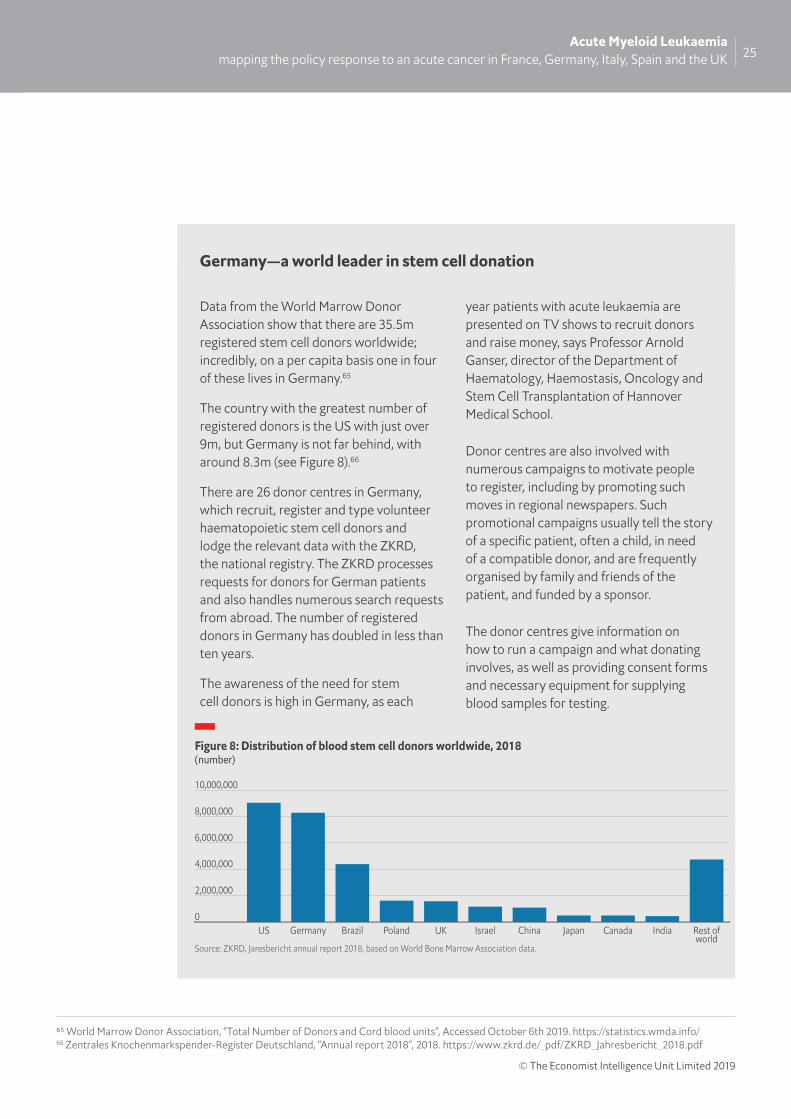
Data from the World Marrow Donor Association show that there are 35.5m registered stem cell donors worldwide; incredibly, on a per capita basis one in four of these lives in Germany.65
The country with the greatest number of registered donors is the US with just over 9m, but Germany is not far behind, with around 8.3m (see Figure 8).66
There are 26 donor centres in Germany, which recruit, register and type volunteer haematopoietic stem cell donors and lodge the relevant data with the ZKRD, the national registry. The ZKRD processes requests for donors for German patients and also handles numerous search requests from abroad. The number of registered donors in Germany has doubled in less than ten years.
The awareness of the need for stem cell donors is high in Germany, as each
year patients with acute leukaemia are presented on TV shows to recruit donors and raise money, says Professor Arnold Ganser, director of the Department of Haematology, Haemostasis, Oncology and Stem Cell Transplantation of Hannover Medical School.
Donor centres are also involved with numerous campaigns to motivate people to register, including by promoting such moves in regional newspapers. Such promotional campaigns usually tell the story of a specific patient, often a child, in need of a compatible donor, and are frequently organised by family and friends of the patient, and funded by a sponsor.
The donor centres give information on how to run a campaign and what donating involves, as well as providing consent forms and necessary equipment for supplying blood samples for testing.
Germany—a world leader in stem cell donation
Figure 8: Distribution of blood stem cell donors worldwide, 2018(number)
Source: ZKRD, Jaresbericht annual report 2018, based on World Bone Marrow Association data.
0
2,000,000
4,000,000
6,000,000
8,000,000
10,000,000
Rest ofworld
IndiaCanadaJapanChinaIsraelUKPolandBrazilGermanyUS
65 World Marrow Donor Association, “Total Number of Donors and Cord blood units”, Accessed October 6th 2019. https://statistics.wmda.info/ 66 Zentrales Knochenmarkspender-Register Deutschland, “Annual report 2018”, 2018. https://www.zkrd.de/_pdf/ZKRD_Jahresbericht_2018.pdf

26Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Chapter 3: The costs of AML
Economic costs of AML
As AML is a rare disease, there is little information available about the financial costs associated with treating, living with and surviving it. Nor is significant information available on the wider economic impact of the condition, as few studies have been conducted specifically on this disease.
It is estimated that all types of malignant blood disorders cost 31 European countries (the 28 EU countries plus Iceland, Norway and Switzerland) €12bn (US$13.3bn) in 2012, with the five most populous countries—France, Germany, Italy, Spain and the UK—shouldering two thirds (€8bn) of these costs.67
For the 31 countries as a whole, direct healthcare made up 62% of these costs (€7·3bn), productivity losses 30% (€3·6bn) and informal care 8% (€1bn). For the 28 EU countries, malignant blood disorders represented 12% (€6·8bn) of the total healthcare expenditure on cancer (€57 billion), a proportion second only to breast cancer.68
The direct healthcare costs of AML increase with the complexity of the care required, and most of the limited research specifically on the direct costs of AML has focused on treatment of younger patients who are fit enough to receive intensive treatment. These younger, fitter patients tend to receive hospital-based therapies in the form of intensive
chemotherapy and allogeneic haematopoietic stem cell transplantation. The majority of studies have been conducted in the US, where the cost of drugs and other treatments are far higher than in Europe, and many patients are burdened with co-payments or are not adequately insured.
One study found that average direct healthcare costs for the first six months of therapy ranged from US$14,014 to US$352,682 in the US and from US$5,837 to US$177,187 in the UK, according to the type of treatment given. In the US, US$14,014 was for best supportive care only, US$57,039 for low-intensity chemotherapy, US$324,502 for high-intensity chemotherapy and US$352,682 for allogeneic stem cell transplantation. In the UK the corresponding costs were lower: US$5,837 for best supportive care only, US$45,854 for low-intensity chemotherapy, US$59,426 for high-intensity chemotherapy and US$177,187 for stem cell transplantation.69
European data are limited and are mainly derived from the UK and Scandinavia, where the healthcare systems and registries make it easier to conduct this type of research. Dr Isidori also explains that regionalism can also add to the complexity of working out costs. “In Italy we have 21 different regions, which have different prices for everything. So it is difficult to collate the direct costs within the country,” he says.
67 Burns R, Leal J, Sullivan R, Luengo-Fernandez R, “Economic burden of malignant blood disorders across Europe: a population-based cost analysis”, Lancet Haematol, Vol. 3, No. 8, 2016, pages e362-70. https://linkinghub.elsevier.com/retrieve/pii/S2352-3026(16)30062-X 68 Ibid.69 Zeidan AM, Mahmoud D, Kucmin-Bemelmans IT et al, “Economic burden associated with acute myeloid leukemia treatment”, Expert Review of Hematology, Vol. 9, No. 1, 2016, pages 79-89. http://www.tandfonline.com/doi/full/10.1586/17474086.2016.1112735
27Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Cost of intensive therapy
Intensive induction chemotherapy has been the recommended first-line treatment for young (<60 years) and medically fit patients with AML since the 1970s and is generally administered on an inpatient basis, requiring lengthy hospital stays of 30-36 days.70
A French study estimated the mean direct medical cost for induction chemotherapy in a trial conducted over 15 years ago at €41,852 (US$46,341), with a mean length of hospital stay of 36.2 days. If the level of blast cells in the bone marrow had not fallen to less than 5%, an additional course of different chemotherapy was administered and, if necessary, a salvage course, increasing the cost by 38% and 15% respectively, owing primarily to the greater length of hospital stay.71
“I think it is much more expensive now,” says Mr Récher, who was involved with the French trial, “and that is only for the cost of one course of chemotherapy; then you have consolidation chemotherapy [and a] second or third round.”
Costs for consolidation chemotherapy in the US have been reported to range between US$29,842 and US$70,925 per cycle.72, 73
Consolidation chemotherapy can be administered in both an inpatient and an outpatient setting, but the cost of delivery in the outpatient is up to five times lower per cycle.74 Increasing the proportion of AML therapy administered on an outpatient setting is one way to decrease the direct healthcare costs of AML.75
Induction chemotherapy is usually followed by at least one cycle of consolidation chemotherapy for patients proceeding to haematopoietic stem cell transplantation, and at least two or three cycles are used for patients being consolidated with high-dose chemotherapy alone.
In the US, the direct cost of medical care for a patient proceeding to haematopoietic stem cell transplantation is reported to be four to 23 times higher than the cost for patients treated with supportive care only, and up to double the cost for patients treated with intensive chemotherapy alone.76
Cost of supportive care and less intensive therapy
Elderly and other patients not fit enough for intensive therapy will receive supportive care, including less intensive chemotherapy.
70 Bewersdorf JP, Shallis RM, Wang R et al, “Healthcare expenses for treatment of acute myeloid leukemia”, Expert Review of Hematology Vol. 12, No. 8, 2019, pages 641-650. http://www.tandfonline.com/doi/full/10.1080/17474086.2019.162786971 Nerich V, Lioure B, Rave M et al, “Induction-related cost of patients with acute myeloid leukaemia in France”, Int J Clin Pharm, Vol. 33, 2011, pages 191–199. https://dx.doi.org/10.1007/s11096-010-9462-1 72 Zeidan AM, Mahmoud D, Kucmin-Bemelmans IT et al, “Economic burden associated with acute myeloid leukemia treatment”, Expert Rev Hematol, Vol. 9, No. 1, 2016, pages 79–89. http://www.tandfonline.com/doi/full/10.1586/17474086.2016.111273573 Stein EM, Bonifacio G, Latremouille-Viau D et al, “Treatment patterns, healthcare resource utilization, and costs in patients with acute myeloid leukemia in commercially insured and medicare 550 populations”, J Med Econ, Vol. 21, No. 6, 2018, pages 556–563. http://www.tandfonline.com/doi/full/10.1080/13696998.2018.142520974 Ibid.75 Bell JA, Galaznik A, Farrelly E et al, “Economic burden of elderly patients with acute myeloid leukemia treated in routine clinical care in the United States”, Leuk Res, Vol. 71, 2018, pages 27–33. https://linkinghub.elsevier.com/retrieve/pii/S0145-2126(18)30131-0 76 Bewersdorf JP, Shallis RM, Wang R et al, “Healthcare expenses for treatment of acute myeloid leukemia”, Expert Review of Hematology Vol. 12, No. 8, 2019, pages 641-650. http://www.tandfonline.com/doi/full/10.1080/17474086.2019.1627869

28Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
A 2013 US study found that the mean direct medical costs for elderly patients after a diagnosis of AML was more than US$96,000. Of these, 57% received only supportive care and had a median survival of just 1.5 months; 43% received low-dose chemotherapy and had a median survival of 7 months.77 The main contributors to the cost of supportive care are hospital stays, and the cost of antibiotics and antifungals for prophylaxis and treatment.78
Approximately 26% of AML patients will require an intensive care unit (ICU) admission at some point during the disease course, a level that increases to nearly 40% in patients aged 60 years or older.79, 80 One study estimated the mean cost of each hospitalisation for patients requiring ICU admission as US$88,325 for patients admitted to US hospitals in 2004-12.81
“For a long time, the main driver of the costs was the inpatient hospitalisation,” says Dr Zeidan. “The patients being actively treated were the younger patients needing intensive chemotherapy [who] had to be admitted to the hospital for a month and subsequently required a lot of care in hospital.”82
He adds, “Over the last two years we are starting to see a shift in these costs, which I think is being driven by use of more expensive oral medications that are becoming more available and are mostly used in the older patients rather than in the younger patients.”
In the future, the cost of drugs is likely to account for a greater slice of the total medical costs for AML,83 says Dr Zeidan. “We used to do only chemotherapies, and those chemotherapies were generally generic and not that expensive. The main drivers of costs were hospitalisations for chemotherapy, transplants, transfusions and managing infections.”
In order to keep costs down it will be important to understand the best way to use new therapies, such as by using genetic testing to identify patients most likely to respond, so that their use can be targeted, says Dr Zeidan. Molecular testing has become increasingly
77 Meyers J, Yu Y, Kaye JA, “Medicare Fee-for-Service Enrollees with Primary Acute Myeloid Leukemia: An Analysis of Treatment Patterns, Survival, and Healthcare Resource Utilization and Costs”, Appl Health Econ Health Policy, Vol. 11, 2013, pages 275-286. https://dx.doi.org/10.1007/s40258-013-0032-2 78 Rieger CT, Cornely O, Hoppe-Tichy T et al, “Treatment cost of invasive fungal disease (IFD) in patients with acute myelogenous leukaemia (AML) or myelodysplastic syndrome (MDS) in German hospitals”, Mycoses, Vol. 55, No. 6, 2012, pages 514-520. https://doi.org/10.1111/j.1439-0507.2012.02193.x 79 Bell JA, Galaznik A, Farrelly E et al, “Economic burden of elderly patients with acute myeloid leukemia treated in routine clinical care in the United States”, Leuk Res, Vol. 71, 2018, pages 27–33. https://linkinghub.elsevier.com/retrieve/pii/S0145-2126(18)30131-0 80 Halpern AB, Culakova E. Walter RB Lyman GH, “Association of 610 risk factors, mortality, and care costs of adults with acute myeloid leukemia with admission to the intensive care unit”, JAMA Oncol, Vol. 3, No.3, 2017, pages 374–381. https://jamanetwork.com/journals/jamaoncology/fullarticle/10.1001/jamaoncol.2016.485881 Bewersdorf JP, Shallis RM, Wang R et al, “Healthcare expenses for treatment of acute myeloid leukemia”, Expert Review of Hematology Vol. 12, No. 8, 2019, pages 641-650.82 Bewersdorf JP, Shallis RM, Wang R et al, “Healthcare expenses for treatment of acute myeloid leukemia”, Expert Review of Hematology Vol. 12, No. 8, 2019, pages 641-650. http://www.tandfonline.com/doi/full/10.1080/17474086.2019.162786983 Ibid.
Approximately 26% of AML patients will require an intensive care unit (ICU) admission at some point during the disease course.
29Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
essential for tailoring treatment strategies and predicting prognosis.
Indirect costs
There have been very few assessments of the indirect costs of AML in terms of the wider economic impact of the disease, such as through inability to work or reduced productivity of working-age patients and their carers.84
One US study surveyed 26 patients six months post-diagnosis of AML to assess perceived economic hardship, finding that patients with AML reported higher levels of economic hardship and distress compared with those with other cancers. Around three-quarters were concerned about their finances and being able to pay their bills.85
“My sense is that, given that half of AML patients are 67 years and older and probably 40% are younger than 60, I think a lot of the indirect costs come from the younger patients,” says Dr Zeidan. “Around half of them are not going to be cured, so that is a lot of indirect loss of income.”
Dr Zeidan speculates that the indirect costs of AML are highest for younger patients who do not survive because they receive the most intensive treatment coinciding with lower productivity. In addition is the loss of income and contribution to the wider economy when such patients die. In contrast, older patients are less likely to be working and their median
survival is low, meaning that any fall in the productivity and economic contribution of their carers will be short-lived.
Impact on patients, their families and carers
Side effects of treatment
Patients will have different responses to therapy, and it is important that treatments are tailored to specific patients’ needs and they are involved in decision making. The type and severity of treatment side effects vary according to the type of therapy given and how an individual responds to it. In general, however, more intensive treatments such as high-intensity chemotherapy and stem cell transplants are associated with more severe side effects, which impact substantially on patients’ quality of life.86
For example, chemotherapy reduces the bone marrow’s ability to produce blood cells, so numbers of red blood cells, platelets and white blood cells will fall in the weeks immediately after treatment, meaning that patients are likely to feel tired, may experience anaemia, can bruise and bleed more easily, and are at greater risk of infections.
To minimise the risk of infection while receiving high-intensity rounds of chemotherapy for induction or consolidation, or as a conditioning therapy prior to transplantation, patients are usually
84 Ibid.85 Bala-Hampton JE, Dudjak L, Albrecht T et al, “Perceived Economic Hardship and Distress in Acute Myelogenous Leukemia”, Journal of Oncology Navigation & Survivorship, Vol. 8, No. 6, 2017, pages 258-264. http://www.jons-online.com/issues/2017/june-2017-vol-8-no-6/1631-perceived-economic-hardship-and-distress-in-acute-myelogenous-leukemia86 Korol EE, Wang S, Johnston K, Ravandi-Kashani F, Levis M, van Nooten F, “Health-Related Quality of Life of Patients with Acute Myeloid Leukemia: A Systematic Literature Review”, Oncology and Therapy, Vol. 5, No. 1, 2017, pages 1-16. https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/28680951/

30Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
hospitalised—usually for 4-6 weeks for induction chemotherapy—and kept in isolation, sometimes in rooms with filtered air. There they may also receive blood transfusions, platelet replacement, and both antibiotic and antifungal prophylaxis as recommended by the ELN guidance.87
For healthcare providers, therefore, infection control is a hugely important consideration. “There is a 6% risk of death during first chemotherapy, and that is not [due to] a lack of response but infection,” says Dr Kaur.
Although most countries provide antibiotic prophylaxis during chemotherapy, according to experts we interviewed, France uses only antifungal prophylaxis. “In general, in France, we do not give antibiotics in primary prophylaxis; it is different from other countries,” says Mr Récher. “We give antibiotics only when the patient is neutropenic and febrile.”
As they are immunocompromised, patients living with AML—whether treated intensively or not—will at some point develop infections, requiring them to be hospitalised and treated with antibiotics.
Cancer treatments are also often associated with nausea and vomiting, changes in taste and smell, dry mouth, mucositis (inflammation of the lining of the mouth, throat or gut), hair
loss, and damage to the gut causing cramping, wind, abdominal swelling and diarrhoea.88 Cancer treatments can also cause bystander organ damage and may cause a temporary or permanent reduction in fertility. In women the impact on fertility can sometimes lead to premature menopause.89
In addition to these side effects, patients who undergo allogeneic stem cell transplantation are at risk of graft versus host disease (GvHD), as donor stem cells contain immune cells from the donor and these cells can sometimes attack cells in the recipient.90 GvHD can be severe—even life threatening—although mild GvHD can be beneficial, as it is an immune system reaction that can help to kill off any remaining leukaemia cells.91
Fertility preservation: a key consideration for younger patients
Whereas it is possible that men diagnosed with AML who need to start chemotherapy within a day or two could preserve their possible fertility by freezing sperm, for women there is not enough time for egg harvesting.92
“There is discussion about [egg] retrieval, but you have to stimulate the ovaries for about four weeks prior to collection, so it is [only available] for the minority of patients, because we have to get therapy started so quickly,” says Gemma Trout, leukaemia clinical
87 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-08-73319688 Leukaemia Foundation, “Side effects of AML treatment”, 2019. https://www.leukaemia.org.au/disease-information/leukaemias/acute-myeloid-leukaemia/how-is-it-treated/side-effects-of-treatment/89 Ibid.90 Cancer Research UK, “Side effects of a transplant”. https://www.cancerresearchuk.org/about-cancer/acute-myeloid-leukaemia-aml/treating-aml/bone-marrow-stem-cells-transplant-aml/side-effects-transplant91 Ibid.92 RM Partners, South East London Cancer Alliance, UCLH Cancer Collaborative. “Pan-London Haemato-Oncology Clinical Guidelines Acute Leukaemias and Myeloid Neoplasms. Part 2: Acute Myeloid Leukaemia”, 2018. https://rmpartners.nhs.uk/wp-content/uploads/2018/11/PanLondon_AML_Guidelines_Sept2018_v2.pdf

31Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
nurse specialist at University College London Hospitals NHS Foundation Trust. “If they have chemotherapy only, there is a reasonable chance that women will still be fertile, but their fertility window may be shorter. If they go for a bone marrow transplant, it unfortunately means that their fertility is lost, if they receive total body irradiation as part of the transplant. Our fertility experts do counsel the female patients regarding these issues.”
If a patient has been stablised on chemotherapy ahead of a haematopoietic stem cell transplant, sometimes it can be possible to delay the latter sufficiently to allow eggs to be harvested, says Ms Trout.
Fertility preservation is generally offered by health systems to cancer patients in all five countries covered in this report, but there may be age restrictions, waiting lists and local variations in what is funded.93
In the UK, for example, access depends on local policies. According to Dr Montesinos, women in Spain with AML will receive fertility treatment funded under the public health system, but there are long waiting lists and it is difficult for those over the age of 40 to access it.
Germany seems to have the most work to do in this area. A foundation operates in the country for young cancer patients who are advocating for the reimbursement of fertility treatments. This is because patients currently must pay more than half the cost of the first three attempts for in-vitro fertilisation out of pocket, and all costs after those attempts have failed, says Jan Geissler, co-founder and steering committee member of the Acute Leukemia Advocates, an independent global network of patient organisations dedicated to improving outcomes for patients with acute leukaemia by strengthening patient advocacy.
In most European countries it is also possible for women whose eggs are no longer viable after cancer treatment to have children using donated eggs. However, in Germany the use of donated eggs is illegal.94 Some German women go to Spain, which has some of the most advanced private fertility services in the world, paying around €10,000.95, 96 However, doctors are not allowed to suggest this, explains Mr Geissler, who is also the chief executive of Patvocates, which is a patient-driven think-tank and patient-focused consultancy focused on patient advocacy.
93 ESHRE Working Group on Oocyte Cryopreservation in Europe, Shenfield F, de Mouzon J, Scaravelli G et al, “Oocyte and ovarian tissue cryopreservation in European countries: statutory background, practice, storage and use”, Hum Reprod Open, Vol. 29, No. 1, 2017, page hox003. https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/30895222/94 Jen Willows, “Move to legalise egg donation and surrogacy in Germany”, BioNews, August 19th 2019. https://www.bionews.org.uk/page_14445695 Cyan Turan, “‘IT WAS OUR LAST CHANCE’ Couple talk of their experience at one of the world’s best IVF clinics”, The Sun, November 20th 2016. https://www.thesun.co.uk/living/2203815/it-was-our-last-chance-couple-talks-of-their-experience-at-one-of-the-worlds-best-ivf-clinics/96 Jen Willows, “Move to legalise egg donation and surrogacy in Germany”, BioNews, August 19th 2019. https://www.bionews.org.uk/page_144456
If they have chemotherapy only, there is a reasonable chance that women will still be fertile, but their fertility window may be shorter.
Gemma Trout, leukaemia clinical nurse specialist, University College London Hospitals NHS Foundation Trust, UK

32Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Physicians in Germany who advise a patient to go to Spain are at high risk of criminal investigation and subsequently loss of their licence to practise as a doctor, as doing so is seen as advising patients to take illegal actions in another country, he says.
Psychosocial support is crucial
An AML diagnosis is life threatening and life changing. Treatment is long, physically gruelling and mentally draining, and its effects difficult in terms of changes to body image and self-perception are hard to come to terms with. It is recognised that patients with cancer should be offered access to psychological services as a matter of course, although this is not what happens in practice.97, 98, 99 How a patient copes with an AML diagnosis and what follows varies dramatically, and many people will benefit from some form of psychosocial support at some stage, although availability varies both within and between countries.
“Fatigue is all consuming. Acute leukaemia chemotherapy is extremely intensive and it takes about a month for your bone marrow to recover,” says Ms Trout. “Then there is the loss of identity—not being able to work, not being able to parent, not being able to see your friends, and the impact on finances and body image. People can put on weight or lose weight, which means their clothes don’t fit any more.” She believes that everyone living with AML should have access to counselling services.
Ms Ostrowski describes her experience: “For me the worst was loss of control of my life—going from working full time and fully in control of my life to being in isolation in hospital for months and having somebody come around to give me my tablets.” She felt that her hair was part of her identity, so before she lost it, she had it cut off and made into a wig.
The large hospitals of northern Europe offer very tailored psychosocial support, which is available for families, carers and friends where needed, although provision at smaller hospitals and in the community after treatment is more patchy, according to the experts we interviewed. In Germany psycho-oncologists—psychologists with special training in oncology—are involved with nearly every patient, says Dr Ganser.
Deborah Harkins, who is recovering from AML and is also director of public health at Dudley Council in the UK’s West Midlands, tells how her consultant was more concerned about her partner than her, because he was distressed while she had a relatively positive frame of mind.
“Before I received the diagnosis, I suspected it was going to be one of three things, the worst of which was acute leukaemia. So I’d sort of got my head around it and mentally prepared myself, but my partner was so devastated,” she says.
97 Jordan K, Aapro M, Kaasa S et al, “European Society for Medical Oncology position paper on supportive and palliative care”, Annals of Oncology, Vol. 29, No. 1, 2018, pages 36-43. https://academic.oup.com/annonc/article-lookup/doi/10.1093/annonc/mdx757 98 National Institute for Health and Care Excellence, “Guidance on improving supportive and palliative care for adults with cancer”, 2004. https://www.nice.org.uk/guidance/csg499 National Institute for Health and Care Excellence, “Haematological cancers: impro Haematological cancers: improving outcomes. NICE guideline”, 2016. https://nice.org.uk/guidance/ng47

33Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
100 Grassi L, Fujisawa D, Odyio P et al; IPOS Federation of Psycho-oncology Societies’ coauthors, “Disparities in psychosocial cancer care: a report from the International Federation of Psycho-oncology Societies”, Psychooncology, Vol. 25, No. 10, 2016, pages 1127-1136. https://onlinelibrary.wiley.com/doi/full/10.1002/pon.4228 101 Pivodic L, Van den Block L, Pardon K et al, on behalf of EURO IMPACT, “Burden on family carers and care-related financial strain at the end of life: a cross-national population-based study”, Eur J Public Health, Vol. 24, No. 5, 2014, pages 819–826. https://academic.oup.com/eurpub/article-lookup/doi/10.1093/eurpub/cku026 102 Macmillan Cancer Support. “Cancer’s hidden price tag: Revealing the costs behind the illness”, 2013. https://www.macmillan.org.uk/_images/Cancers-Hidden-Price-Tag-report-England_tcm9-270862.pdf 103 Pivodic L, Van den Block L, Pardon K et al, on behalf of EURO IMPACT, “Burden on family carers and care-related financial strain at the end of life: a cross-national population-based study”, Eur J Public Health, Vol. 24, No. 5, 2014, pages 819–826. https://academic.oup.com/eurpub/article-lookup/doi/10.1093/eurpub/cku026
Psychosocial support appears to be less available in southern Europe, where austerity measures in recent years have hindered the development of these services.100 In addition, the region’s tradition of strong family support networks have become more disparate as more people move away for work, according to the experts we interviewed.101
In Italy, only around 50 % of hospital centers offer psychological support, says Dr Felicetto Ferrara, chief of the haematology unit at Cardarelli Hospital in Naples, Italy. In Spain, mental health support is available in theory, but in practice it is not always offered, leaving patients’ associations to fill in the gaps. “Perhaps psychosocial support is something that is not considered as relevant by physicians, scientific groups and the health institutions,” says Dr Montesinos. “It is something that could clearly be improved.”
Patients who have “survived” the disease often need psychosocial support but tend to be forgotten by healthcare providers, says Mr Geissler. “Healthcare professionals think that clinically these people have survived, but actually everything in their lives seems to be broken into pieces,” he explains. “What is gone is the normal sex life and the normal home life. Many patients get into menopause, they lose the opportunity to have their own children, they sometimes break up with their partners—their whole life is a mess. That is the difference
between a clinical reality and reality. I don’t think we are set up in our healthcare systems to provide that psychosocial support to live with and after cancer.”
Financial impact on patients
The need for repeated long stays in hospital can have a massive financial impact on patients of working age, even when they qualify for sick pay or benefits.102, 103
Ms Ostrowski, who worked as a solicitor, says that her salary fell by 40%, which made paying the bills difficult. “One thing that I found very frustrating was that I didn’t know about the benefits at the time. I tried to make a retrospective claim but was told it had to be done at the time, and I wasn’t aware of my potential entitlement until afterwards.”
Healthcare professionals think that clinically these people have survived, but actually everything in their lives seems to be broken into pieces.
Jan Geissler, steering committee member of the Acute Leukemia Advocates Network

34Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
104 Leunis A, Redekop WK, Uyl-de Groot CA, Löwenberg B, “Impaired health-related quality of life in acute myeloid leukemia survivors: a single-center study”, European Journal Of Haematology, Vol. 93, 3, 2014, pages 198-206. https://doi.org/10.1111/ejh.12324105 Redaelli A, Stephens JM, Brandt S, Botteman MF, Pashos CL, “Short- and long-term effects of acute myeloid leukemia on patient health-related quality of life”, Cancer Treatment Reviews, Vol. 30, No. 1, 2004, pages 103-17. https://linkinghub.elsevier.com/retrieve/pii/S0305737203001427
“Everyone you speak to struggles financially,” says Ms Harkins. She had not been in her job for a year, and so was not entitled to full sick pay. “I carried on working from my isolation room,” she says, and she borrowed money from her parents.
“When you’re in this position you need to be able to scale down your hours, get extra holidays, get financial support, get tax breaks,” says Mr Geissler. “What disability laws don’t really do is protect people who are in a
very cyclical situation—for example, cancer patients who might be able to work, then be out of work for some time, because they relapse and need more treatment. Our laws are not set up for that, so we send people into early retirement.”
This leaves people with no means of real existence, low quality of life, lack of self-confidence and, according to Mr Geissler, the feeling that they are a nuisance to society because they are not able to work.104, 105
35Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Chapter 4: AML heath policy under the spotlight National policy and evidence-based treatment guidelines
Management of AML across Europe is similar, as it tends to be based on the ELN guidelines, which were last updated in 2017.106 Any national guidelines are based around the ELN or are outdated.
In Germany, the diagnostic and treatment strategy is based on ELN recommendations, and the guidelines of the German Society of Haematology and Medical Oncology.107 France also follows the ELN, but the French Society of Haematology is drafting its own guidelines, although these are yet to be published and will support ELN advice.
In Italy, there are old national guidelines, of which Dr Ferrara was a coauthor.108 However, he says that most Italian haematologists follow the ELN recommendations. “Policymakers or stakeholders in Italy have not yet carried out any research or issued policy documents on the state of care in AML, neither to assess it nor to ensure that it follows any guidelines,” he says.
The situation is similar in the UK, where the British Society for Haematology (BSH) guidelines on AML are more than 12 years old.109 The BSH is due to update its recommendations around the management of AML in pregnancy.110
In Spain, AML care is organised around two major co-operative groups of institutions, the PETHEMA and CETLAM groups. Each has their own guidelines, but these are only available on their intranet webpages. According to Dr Montesinos, they are similar to the ELN guidelines.
The ELN guidance is focused on the clinical management of the acute condition, and it does not include information about the impact of treatment side effects or how to manage the holistic needs of the patient or the importance of caring for patients through a multidisciplinary team.111
Ensuring that clinical pathways address all these factors is always a challenge with rare diseases, says Mr Boselli.112, 113 “A recognised clinical pathway is needed, and collaboration between the countries is fundamental to
106 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-08-733196 107 Röllig C, Beelen DW, Braess J et al, “Guidelines of the German Society of Hematology and Medical Oncology on acute myeloid leukaemia”, 2019. https://www.onkopedia.com/de/onkopedia/guidelines/akute-myeloische-leukaemie-aml/@@guideline/html/index.html 108 Morra E, Barosi G, Bosi A, Ferrara F, Locatelli F, Marchetti M, Martinelli G, Mecucci C, Vignetti M, Tura S, “Clinical management of primary non-acute promyelocytic leukemia acute myeloid leukemia: practice Guidelines by the Italian Society of Hematology, the Italian Society of Experimental Hematology and the Italian Group for Bone Marrow Transplantation”, Haematologica, Vol. 94, No.1 , 2009, pages 102-112. https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/19001282/109 Milligan DW, Grimwade D, Cullis JO et al on behalf of British Committee for Standards in Haematology, “Guidelines on the management of acute myeloid leukaemia in adults”, Br J Haematol, Vol. 135, No. 4, 2006, pages 450-74. https://doi.org/10.1111/j.1365-2141.2006.06314.x 110 Personal communication with Dr Harpreet Kaur; Ali S, Jones GL, Culligan DJ et al on behalf of the British Committee for Standards in Haematology, “Guidelines for the diagnosis and management of acute myeloid leukaemia in pregnancy”, British Journal Haematology, Vol. 170, No. 4, 2015, pages 487-495. https://doi.org/10.1111/bjh.13554 111 Döhner H, Estey E, Grimwade D et al, “Diagnosis and management of AML in adults: 2017 ELN recommendations from an international expert panel”, Blood, 2017 Vol. 129, No. 4, 2017, pages 424-447. https://ashpublications.org/blood/article-lookup/doi/10.1182/blood-2016-08-733196 112 Jordan K, Aapro M, Kaasa S et al, “European Society for Medical Oncology position paper on supportive and palliative care”, Annals of Oncology, Vol. 29, No. 1, 2018, pages 36-43. https://academic.oup.com/annonc/article-lookup/doi/10.1093/annonc/mdx757 113 Melnychuk M, Vindrola-Padros C, Aitchison M, et al, “Centralising specialist cancer surgery services in England: survey of factors that matter to patients and carers and health professionals”, BMC Cancer, Vol. 18, No. 1, 2018, page 226. https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/29486730/

36Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
achieving this,” he says. “That pathway then needs to be integrated within national health policies.”
But there are some positive policy moves. The European Commission and member states have set up the European Reference Networks for knowledge sharing in rare diseases that require highly specialised treatment and a concentration of knowledge and resources. One of the first 24, EuroBloodNet, is focused on haematological diseases.114
Specialist cancer nurses and the multidisciplinary care team
Large specialist centres in the five countries studied have a wide range of different specialist professionals to call upon to support patients with AML, including consultants, specialist nurses, psychologists and physiotherapists. Any staffing issues reflect wider issues within the country—for example, a general shortage of nurses, physiotherapists or psychological support.
There are a wide variety of different specialist cancer nursing roles across different European countries—for example, clinical nurse specialists, consultant nurses and advanced nurse practitioners. These have been developed for a variety of reasons, including a shortage of doctors, more complex care pathways and the need for care co-ordination.115
Several studies have shown that nurses can improve patients’ emotional wellbeing, enhance symptom management and reduce hospital re-admission.116
In northern Europe, particularly in the UK, patients are likely to have a named clinical nurse specialist as their point of contact. In large centres a nurse may only work with patients living with AML, whereas in the smaller centres nurses are likely to see a range of patients with haematological diseases.117 Nurses play a crucial role—they are the key healthcare professional responsible for supporting the patient, their family and carers through diagnosis and treatment, providing information, answering questions, and linking and signposting patients to support and holistic services as required.
“We have a phone line which is staffed by two admin assistants who then phone us or email us with any patient queries. We also have an out-of-hours line as well,” says Ms Trout. “We have smartphones so we can check emails, and the administrators phone us directly if anyone is unwell or distressed. During out-
114 EuroBloodNet, “European Reference Networks”. http://eurobloodnet.eu/erns/115 Schneider F, Faithfull S, “What does a specialist nurse mean across Europe?” European Oncology Nursing Society Newsletter Spring 2011, 2011, pages 23-31. https://www.cancernurse.eu/documents/newsletter/2011spring/EONSNewsletter2011springPage28.pdf116 Farrell C et al, “Exploring the scope of oncology specialist nurses’ practice in the UK”, Eur J Oncol Nursing, Vol. 15, No. 2, 2011, pages 160-6. https://linkinghub.elsevier.com/retrieve/pii/S1462-3889(10)00123-7117 Aerts E, Fliedner M, Redmond K et al, “Defining the scope of haematology nursing practice in Europe”, European Journal of Oncology Nursing, Vol. 14, No. 1, 2010, pages 55-60. https://linkinghub.elsevier.com/retrieve/pii/S1462-3889(09)00081-7
In northern Europe, particularly in the UK, patients are likely to have a named clinical nurse specialist as their point of contact.

37Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
of-hours they can call a mobile which is held by one of the inpatient wards, so patients and families should feel very confident that they have someone to talk to 24 hours a day, seven days a week.”
In Spain it is not usual for patients to be given mobile numbers for a nurse or a hotline, says Dr Montesinos. “If there’s an emergency they contact the emergency room or the regular [hospital] telephone number.”
“If you’re in one of the larger centres of excellence,” says Mr Geissler, “they have all the facilities—not only the acute treatment, but the psycho-oncology unit, home nursing, etc.” Many mid-range hospitals are trying to manage AML patients in a better way, but they can’t allocate a specific nurse specialised in the disease to a patient, he notes. “That’s where the problem starts, because the clinicians are obviously handling the clinical effects of AML, but the nurses have such an important role in managing everything that comes afterwards.”
Centralised, specialist centres
Within all countries we studied there are several specialist centres for AML that focus on the care of patients who receive high-intensity treatment, but the proportions of patients treated in these hospitals versus smaller centres varies from country to country. It is accepted that centralisation of care is better for patients in terms of outcomes and access to a multidisciplinary team of professionals and support services.118, 119
The need for rapid diagnosis, the growing complexity of therapy and the complications of the disease are arguments for centralising therapy in a few specialised sites, says Dr Montesinos. In Spain he would like to see the current number of hospitals treating AML—which number around 120—reduced by half.
The German Cancer Society has recently started accrediting leukaemia and lymphoma centres, and one of the requirements for accreditation is that centres treat at least ten AML patients per year. “This will reduce the number of sites treating AML,” says Dr Ganser.
In Italy, says Dr Isidori, only a few sites have support for patients from an emergency doctor that specialises in haematological disorders.
Humanising hospitals
Patients treated intensively spend long periods, sometimes a month or more at a time, in the institutional setting of a hospital, and are often isolated. Visits from family and friends may be severely restricted, and television and internet access may not be available or must be paid for.
This is the case in Italy, where patients are isolated, visiting hours are limited to one or two hours a day and some hospitals do not have free WiFi or television. “I think the humanisation of the hospital would be very useful for the patient,” says Dr Isidori.
118 Melnychuk M, Vindrola-Padros C, Aitchison M, et al, “Centralising specialist cancer surgery services in England: survey of factors that matter to patients and carers and health professionals”, BMC Cancer, Vol. 18, No. 1, 2018, page 226. https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/29486730/ 119 Morris S, Hunter RM, Ramsay AI, “Impact of centralising acute stroke services in English metropolitan areas on mortality and length of hospital stay: difference-in-differences analysis”, BMJ, Vol. 349, page g4757. http://www.bmj.com/cgi/pmidlookup?view=long&pmid=25098169

38Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Television and WiFi had to be paid for in one of the hospitals Ms Harkins spent time in. She describes herself as an outdoor person, and says that the hardest part of the care was having to spend a total of six months in hospital in isolation. “The main objective for me was to be at home, and I said “I’ll do anything if you let me go home”.”
One idea receiving some attention is alternative types of outpatient care. University College Hospital in the UK, for example, has set up an ambulatory care unit, which enables some patients to stay in a specially adapted hotel while they receive their treatment (see case study below).
The hospital also tries to help patients who live out of London to receive some of their care closer to home through phone clinics and shared care arrangements. However, Ms Trout says that more investment is needed for local hospitals, physiotherapy and, in particular, psychological services to provide quicker access to counselling services via a GP.
Most older patients living with AML are managed at home with supportive care either alone or with low intensity therapy, and it is important to be able to pick up any deterioration or infections quickly.
Mr Récher says that at the institution where he works, Toulouse University Cancer Institute Oncopole, in France, much work is being undertaken to better follow-up with such patients at home through a programme
called Ambulatory Medical Assistance (AMA). “We have one or two nurses dedicated to monitoring those patients by phone,” he says.
Patients are called twice a week, and the nurse monitors blood counts from tests conducted twice a week.
The nurse can also arrange a platelet or blood transfusion at the hospital when required. The nurse also decides whether the patient should take antibiotics or not, so that complications and re-hospitalisations can be minimised.
“Generally, these kinds of patients need a specific organisation, a better follow-up at home by doctors and nurses, and also to have intravenous products and antibiotics at home rather than in hospital. We could develop that if we could have the funding and resources,” Mr Récher says.
Generally, these kinds of patients need a specific organisation, a better follow-up at home by doctors and nurses, and also to have intravenous products and antibiotics at home rather than in hospital.
Christian Récher, head of the haematology department, Toulouse University Hospital Centre, France.

39Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
120 Compaci G, Rueter M, Lamy S, Oberic L, Recher C, Lapeyre-Mestre M, Laurent G, Despas F, “Ambulatory Medical Assistance - After Cancer (AMA-AC): A model for an early trajectory survivorship survey of lymphoma patients treated with anthracycline-based chemotherapy”, BMC Cancer, Vol. 15, 2015, page 781. https://bmccancer.biomedcentral.com/articles/10.1186/s12885-015-1815-7 121 Walburg V, Rueter M, Lamy S, Compaci G, Lapeyre-Mestre M, Laurent G, Despas F, “Fear of cancer recurrence in Non- and Hodgkin lymphoma survivors during their first three years of survivorship among French patients”, Psychol Health Med, Vol. 24, No. 7, 2019, pages 781-787. https://www.tandfonline.com/doi/abs/10.1080/13548506.2019.1574354 122 Guys and St Thomas’ NHS Foundation Trust, “Geriatric oncology referrals”. https://www.guysandstthomas.nhs.uk/our-services/cancer/treatment-care/geriatric-oncology/referrals.aspx123 Kapiris M, Karapanagiotou L, Mansi JL, “Development of GOLD (Geriatric Oncology Liaison Development) service to improve outcomes in older people with cancer”, Annals of Oncology, Vol. 30, No.5, 2019, page mdz265.004. https://doi.org/10.1093/annonc/mdz265.004124 World Health Organisation (WHO) Regional Office for Europe, “Influenza vaccination coverage and effectiveness”. http://www.euro.who.int/en/health-topics/communicable-diseases/influenza/vaccination/influenza-vaccination-coverage-and-effectiveness125 Kassianos G, “Willingness of European healthcare workers to undergo vaccination against seasonal influenza: current situation and suggestions for improvement”, Drugs Context, Vol. 4, 2015, page 212268. http://dx.doi.org/10.7573/dic.212268
The institute also has a programme called Ambulatory Medical Assistance—After Cancer (AMA-AC).120 In this programme, nurses follow-up with patients with quality of life questionnaires, link in with the patient’s GP to assess and analyse how patients are reintegrated into active and social life, detect late adverse events, and help to manage fear of relapse and post-traumatic stress disorders.121
In order to achieve the best outcomes and experience for the patient, it is important to also consider their holistic health and wellbeing needs, says Nicola Shepherd, clinical nurse specialist in leukaemia and lymphoma at Guy’s Hospital in London.
Guy’s and St Thomas’ NHS Foundation Trust has set up a dedicated programme to do this, the Geriatric Oncology Liaison Development (GOLD) service, which patients can be referred to.122, 123
“The service sees patients, often with family members, and gives them a bit of a [health check-up], looks at what medication they are on, other illnesses (comorbidities) and any social care needs. They will be referred on to any services that may be beneficial, and their medication will be optimised so that they are able to tolerate their cancer treatment better,” explains Ms Shepherd. “It also gives them the
opportunity to raise anything the hospital team or the GP has not talked to them about.”
Patients also need to be empowered to be involved and active in their own care. When Ms Harkins was diagnosed with AML she asked her consultant a question: “What can I do to get the best possible outcome from this?” Her consultant advised her to drink lots of water while in therapy, fully engage with her treatment (that is, to know everything that is happening to her and check everything that should be happening is happening), and think of something positive every day. “In periods at home between hospital stays I went for a walk every day to help me keep positive and keep my fitness up,” she says.
The hospital she was in also gave her electronic access to her notes. “I found that really helpful,” Ms Harkins says. “I could log on every morning and see my results. I can still do that now if I have a clinic appointment. Things like that empower people to take control.”
Vaccination of healthcare staff and reducing infections
Uptake of influenza vaccination by healthcare workers in Europe is low, at below 40% in most countries, with even countries such as the UK, where uptake is highest, achieving little more than 50% coverage.124, 125

40Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
This has led to debate about whether it should be mandatory for healthcare workers, particularly those dealing with immunocompromised patients, to have the vaccine to protect their patients.
A survey of 5,424 healthcare workers from 14 European countries found that 43.8% reported that they had not received a seasonal influenza vaccine in the past ten years, and 65.6% reported not receiving the pandemic influenza vaccine in 2009.126
Ms Harkins says that she developed influenza twice while hospitalised and believes that on both occasions the source was a healthcare worker. “The second time I was told that a staff member had swabbed positive for the flu and they weren’t immunised, so we’re going have to give you prophylaxis for the flu, and I ended up getting it,” she says. “I cannot think why somebody working as a care worker on a haematology ward would think that not having the flu vaccine was a sensible thing to do. If they choose not to have it, they should work on a different ward.”
126 Karnaki P, Baka A, Petralias A et al, “Immunization related behaviour among healthcare workers in Europe: Results of the HProImmune survey”, Cent Eur J Public Health, Vol. 27, No. 3, 0219, pages 204-211. https://doi.org/10.21101/cejph.a5514
Currently, at the University College Hospital in London only high dependency, very ill and new patients receive chemotherapy as inpatients. Instead, all other patients receive chemotherapy in an out-patient setting, staying at a specially adapted hotel nearby.
“With new patients we have to see how they experience chemotherapy and how they recover and that judgement then allows us to see whether they are appropriate for ambulatory care in the future,” explains Gemma Trout, leukaemia clinical nurse specialist at University College London Hospitals NHS Foundation Trust.
The patient must be fit enough, and have good mobility, good spoken English, a mobile phone and someone to stay with them in their twin room when they are not receiving treatment.
“Being in the ambulatory care facility also helps patients’ fitness levels, and it is a better experience for them, as they meet other patients to gain peer support,” says Ms Trout. “Being in a single room on the ward when you can’t really see what is going on can be disheartening and lonely.”
For the hospital, use of the hotel service reduces the use of inpatient beds, making bed management easier, and it is more cost-effective, as it cuts the length of each patient’s hospital stay, she says.
Sometimes, inpatient beds are kept available in case patients need to be re-admitted. “Nursing staff do daily assessments and will admit people sooner rather than later to avoid overnight admissions,” says Ms Trout.
Innovative hospital hotel allows patients to receive chemotherapy as outpatients

41Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Mandatory influenza vaccination for healthcare workers was introduced in the US a decade ago.127 In 2018 the state of New South Wales in Australia made vaccination mandatory for doctors and nurses working with patients on high-risk wards, including cancer and transplant wards. Staff who are not vaccinated are either moved to other wards or have to wear masks.128
Germany has recently made another vaccine compulsory: in July 2019 it was announced that from March 2020 it would be mandatory for all healthcare workers born after 1970 to have the measles, mumps and rubella (MMR) vaccine if they are to work in health facilities.129
Measuring and monitoring AML
Some European countries collect data on the epidemiology and outcomes of AML treatment through registries, but these registries rarely cover all patients and are focused on younger, fitter patients receiving active treatment, particularly through clinical trials, according to the experts that we interviewed. National and European data on incidence, prevalence and survival are therefore based on extrapolated figures.
In Italy, data can be collected by the National Co-operative GIMEMA Group, but only for patients registered into clinical trials. “We have no official data on epidemiology, morbidity, mortality [or] treatments provided [in Italy],” says Dr Ferrara.
Matters appear to be more positive in France. “There are few regional registries in France. We also have an AML database covering a region [Toulouse and Bordeaux] of six million inhabitants. All cases of AML, whatever the age or initial treatment, are registered and followed. To date, more than 3,500 patients are included,” says Mr Récher.
Spain, on the other hand, does not appear to have reliable data about the incidence and prevalence of AML. “We don’t have an epidemiological registry like the Swedish registry. As far as I know, that is the only one in Europe,” Dr Montesinos says.
Accurate data on prevalence and incidence is important for planning health services and ensuring that they are appropriately resourced. The incidence and prevalence of AML is growing, owing to an aging population and more patients surviving treatment for other cancers, but the actual size of the growing burden is unknown, owing to the lack of robust data. A more accurate picture of incidence and prevalence is needed, so that countries can ensure that specialist services can cope with the growing number of patients with AML, the right numbers of specialist healthcare staff are trained and recruited, and services and treatments are appropriately funded.
Germany is trying to improve data collection. All of its 16 states now must have a clinical cancer registry, the data from which are collated in a federal registry.
127 Maltezou HC, Theodoridou K, Ledda C, et al, “Vaccination of healthcare workers: is mandatory vaccination needed?”, Expert Rev Vaccines, Vol. 18, No. 1, 2019, pages 5-13. http://www.tandfonline.com/doi/full/10.1080/14760584.2019.1552141 128 AAP, “Mandatory flu vaccination for medical staff in NSW”, Health Times, June 1st 2018. https://healthtimes.com.au/hub/immunology/31/news/aap/mandatory-flu-vaccination-for-medical-staff-in-nsw/3391/129 Bundesministerium für Gesundheit, “Bundesgesundheitsminister Jens Spahn: ‘Wir wollen möglichst alle Kinder vor einer Masernansteckung bewahren’”, July 17th 2019. https://www.bundesgesundheitsministerium.de/en/presse/pressemitteilungen/2019/3-quartal/masernschutzgesetz.html

42Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
“In the future the treatment and outcomes of every cancer patient in Germany should be recorded,” says Dr Ganser. However, he adds, “the need for co-operation does not end at the national border.”
Most patients living with AML in Germany who are fit for clinical therapy are treated within a clinical trial, but as the understanding of the cytogenetic mechanisms involved in AML increases, it no longer becomes feasible to conduct small prospective clinical trials within one institution of the country. “We have to analyse and select so many patient subgroups that we need international collaboration,” Dr Ganser says.
Mr Geissler, who works extensively with patients, says that it is difficult to learn from a single study of say, only 200 people, because there will be so many different subtypes of AML, and for each subtype there may only be a couple of patients. “But if you put all the data into a single pot and analyse the genomics, the biomarkers, clinical outcomes and whatever else, then suddenly you see a pattern
emerging, the breakthrough where we start to understand more about the disease,” he says.
The Harmony Alliance, funded by the European Commission and the private sector through the Innovative Medicines Initiative, will use big data to deliver information that will help to improve the care of patients with these diseases.130 Specifically, the project will gather, integrate and analyse anonymous data of 45,000 patients with seven haematological cancers from a number of high-quality sources to define prognostic factors, clinical endpoints and outcomes for these diseases. It will also enable the success of treatment pathways to be analysed across different genomic subgroups.
“The pilot disease is AML, and so far we have collected data on about 3,500 AML patients,” says Mr Geissler, co-founder of LeukaNET, one of the Harmony Alliance’s partner organisations. “Harmony is one of the most exciting things happening at the moment in terms of better understanding of a patient’s disease.”
“Perhaps in the future we will be able to predict which patients may come through AML without being exposed so hard with treatment,” says Mr Geissler. “We are probably overtreating a population that we don’t understand enough about as yet. If you could prevent 10-20% of the survivors from having to be exposed to the devastating side effects of the most intensive treatment with all the repercussions that has for their future, such as the loss of the ability to have their own children, that would also be a great achievement.”
130 Harmony Alliance, “The HARMONY Big Data Platform: Algorithms To Transform Knowledge Into Better Medicine Outcomes”. https://www.harmony-alliance.eu/
In the future the treatment and outcomes of every cancer patient in Germany should be recorded.
Arnold Ganser, director of the Department of Haematology, Haemostasis, Oncology and Stem Cell Transplantation, Hannover Medical School, Germany

43Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
131 Harmony Alliance, “HARMONY Launches a Delphi Survey to Develop a Core Outcome Set for Acute Myeloid Leukemia”, April 30th 2019. https://www.harmony-alliance.eu/en/news/wp2/harmony-launches-a-delphi-survey-to-develop-a-core-outcome-set-for-acute-myeloid-leukemia132 Buckley SA, Jimenez-Sahagun D, Othus M, Walter RB, Lee SJ, “Quality of life from the perspective of the patient with acute myeloid leukemia”, Cancer, Vol. 124, No. 1, 2018, pages 145-152. https://www.ncbi.nlm.nih.gov/pmc/articles/pmid/28881384/133 Leukaemia Care. https://www.leukaemiacare.org.uk/134 Macmillan Cancer Support. https://www.macmillan.org.uk/135 Deutsche Leukämie- und Lymphom-Hilfe. https://www.leukaemie-hilfe.de/startseite.html
There is also no consensus on what clinicians, patients and the regulatory agencies believe should be the core outcomes for AML beyond survival, he says. Harmony is surveying representative groups of stakeholders over several rounds to try to reach a consensus.131
This is important because quality of life issues are not captured effectively in clinical studies,132 says Mr Geissler. “We need to generate meaningful data about quality of life during studies.”
Awareness, advocacy and education: the role of patient groups and expert patients
The UK stands out across Europe in terms of the support that it provides patients and their families through patient groups and other charities. “The UK has a charity culture, and that is quite unique in Europe,” says Mr Geissler, pointing to strong disease-specific
organisations such as LeukaemiaCare, which run public awareness campaigns and advocacy for patients, and provide support services, alongside more widely focused charities such as Macmillan Cancer Support.133, 134 Elsewhere in Europe, there are few patient groups and less support for them, says Mr Geissler, and those that exist struggle to provide advocacy.
As well as supporting patients directly, patient advocacy groups can have a role in engaging with policymakers and other stakeholders to improve care and outcomes for patients. For example, stronger patient advocacy could help to push for faster return of results of genetic testing and its wider use—ensuring that it is available to all patients and performed regularly to monitor disease and treatment response.
Germany has the Deutsche Leukämie- und Lymphom-Hilfe (DLH), an umbrella organisation for specialist support groups, which receives funds from German Cancer Aid (Deutsche Krebshilfe) and supports the many regional patient groups.135 However, Mr Geissler points out that AML is just one of around 50 diseases that the DLH covers. LeukaNET has been trying to build more dedicated support for patients with AML for many years in Germany but it has been very difficult, says Mr Geissler. “AML is a disease where people are usually hospitalised within 24 hours after diagnosis, so there is no way that patients can really inform themselves much before treatment starts. Then mortality
There is also no consensus on what clinicians, patients and the regulatory agencies believe should be the core outcomes for AML beyond survival.
Jan Geissler, steering committee member of the Acute Leukemia Advocates Network

44Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
is so high that the community is really divided into those that unfortunately don’t make it and those that want to move on afterwards. So there’s not much readiness really in the patient community to support patient advocacy work.”
In Italy, Dr Isidori helps to organise meetings twice a year in which patients living with AML and doctors that treat the condition get together and share their experiences. These
meetings are organised by the Associazione Italiana contro le leucemie, linfomi e mielomi, which also fully covers expenses incurred by patients in attending the meetings.
“It is something that is really emotional,” he says. “At one of these meetings I met a patient I had cured in Bologna and we cried together.” The treatment experience is intense for long periods of time for both the patients and those who treat them, he says. “I spend more time with my patients than with my family, so I think the benefits of these kinds of patient advocacy, awareness and engagement days are hugely important.”
In the UK, patient advocacy is more developed, and patients benefit from it. When Ms Harkins was being treated in hospital for AML, she remembered being visited by a woman from a charity who had been diagnosed and treated for AML 15 years ago and was giving foot massages. “She was the embodiment of hope,” she recalls.
AML is a disease where people are usually hospitalised within 24 hours after diagnosis, so there is no way that patients can really inform themselves much before treatment starts.
Jan Geissler, steering committee member of the Acute Leukemia Advocates Network
45Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
Conclusion: Looking ahead—key issues for policymakers AML is an acute life-threatening condition, which means that patients often undergo intense therapy that can have a huge impact on their physical and psychological wellbeing.
Patients are taken out of their daily lives immediately for months at a time, which affects their family, social and work life, as well as their finances, both at the time and into the future. Although wider support services exist to provide help during the therapy phase, there is little support provided afterwards through patient-specific advocacy groups.
“There is so much focus on symptom management and the acute handling of the disease, people forget about the human being afterwards when it comes to non-clinical effects of cancer,” says Mr Geissler.
As more people age, the incidence of AML is expected to rise, meaning that healthcare service providers in Europe will need to be prepared to deal with the specific demands of the condition on health systems. In particular, policymakers must focus more closely on recognising the impact of the disease on patients’ quality of life, not only relating to decisions about care, but aftercare too.
The following measures could help to improve patient care:
Ensure awareness of AML among both the public and primary care physicians
A delayed diagnosis can mean death for those with AML. Initially, patients may present with indistinct symptoms such as tiredness and recurrent infections, before more characteristic signs such as bruising
and bleeding appear. If the patient is sent for a blood test, the result will be extremely abnormal, and treatment needs to be initiated immediately. More efforts need to be made so that primary care healthcare professionals can recognise these patterns as red flags for AML. Awareness campaigns for healthcare professionals and the public, focusing on the warning symptoms of acute forms of leukaemia such as AML, would be of benefit.
Ensure greater centralisation of highly specialised services
As AML is a rare and complex cancer, active management is best undertaken within a few centres of excellence, rather than through numerous smaller hospitals. Shared care arrangements and a multidisciplinary approach should be used where possible to enable patients to have blood testing done locally and gain access closer to home to services such as psychotherapy and physiotherapy.
Increase delivery of care outside of hospital
As most AML-related healthcare costs are currently incurred in the inpatient setting, increasing the proportion of treatment given on an outpatient basis or through ambulatory care could reduce the economic burden of AML. At the same time, it could improve the patient experience. Early studies suggest that outpatient management is safe if precautions are maintained, although patients treated on such basis do require close outpatient follow-up and frequent blood transfusions, and are at risk of rehospitalisation. The development

46Acute Myeloid Leukaemiamapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
of oral medications delivered in the outpatient setting also means that the proportion of patients actively treated in this setting is likely to grow in years to come, and services will need to be designed around this.
Establish faster genetic testing for diagnosis and monitoring
Several targeted therapies are available for treating AML and the number will increase as we learn more about the genetic basis of the condition. This will increase the need to have the results of cytogenic tests quickly after diagnosis so that patients can be given the most appropriate treatment. Repeat testing is necessary to monitor the response to treatment and any subsequent genetic changes that could influence the treatment approach taken.
Improve data collection
Collection of data on patients living with AML is currently patchy, and registries are focused on those who are actively managed through clinical trials. Initiatives to improve data collection and share it across Europe should be supported, as such data can be used in research and for designing services to improve patients’ care and outcomes. A more accurate picture of incidence and prevalence is needed, so that countries can ensure that specialist services can cope with the growing number of patients with AML and services are appropriately funded. Studies are also needed on the economic burden of AML in Europe, as information is currently limited.
“Humanise” the hospital experience
Patients often spend months hospitalised for treatment. Extended visiting hours, alongside
access to free WiFi and television, can greatly improve patients’ experience while in hospital by enabling them to maintain relationships, keep up to date with work or study, and be generally occupied. Initiatives to provide more “homely” accommodation alternatives to hospital can also have benefits for patient wellbeing and reduce costs.
Increase uptake of influenza vaccination among healthcare workers
Viral infections such as influenza can pose a real risk to immunocompromised AML patients, especially those treated with high-intensity chemotherapy and/or stem cell transplants. Uptake of flu vaccination is low among the healthcare workers who will be managing the care of such patients. Greater uptake of flu vaccination needs to be encouraged among healthcare workers, either on a voluntary basis or via mandatory vaccination of staff working with immunocompromised patients on cancer and transplant wards.
Improve patient advocacy to give patients a stronger voice
Patient advocacy around AML is absent or extremely limited in many European countries. Most patient support organisations that focus on haematological cancers are small and resource-poor, and are focused on giving support to patients who are being actively treated. There would be benefits for the patient population if patient groups were able to widen the support they provide to aftercare for “survivors”, who will need advocacy support to help them speak up on their experience of the disease. European policymakers could also do more to involve

47Acute Myeloid Leukaemia
mapping the policy response to an acute cancer in France, Germany, Italy, Spain and the UK
© The Economist Intelligence Unit Limited 2019
patient groups in decision making to assist policy and service development around rare acute forms of leukaemia. Stronger patient advocacy could help to usher in improved care, such as improved use of genetic testing.
Develop more comprehensive clinical guidance
Management of AML in the five European countries we studied is based primarily
on the 2017 ELN guidance. This guidance is focused on clinical management of the disease in the acute stage. Wider guidance is needed that takes into account treatment side effects, the impact on quality of life, and the patient’s holistic needs and how these are best met. This should be oriented around a multidisciplinary team approach and access to a network of services.

While every effort has been taken to verify the accuracy of this information, The Economist Intelligence Unit Ltd. cannot accept any responsibility or liability for reliance by any person on this report or any of the information, opinions or conclusions set out in this report. The findings and views expressed in the report do not necessarily reflect the views of the sponsor.
4The future of healthcare in Africa
Progress on five healthcare scenarios
© The Economist Intelligence Unit Limited 2019
LONDON20 Cabot SquareLondon, E14 4QWUnited KingdomTel: (44.20) 7576 8000Fax: (44.20) 7576 8500Email: [email protected]
NEW YORK750 Third Avenue5th FloorNew York, NY 10017United StatesTel: (1.212) 554 0600Fax: (1.212) 586 1181/2 Email: [email protected]
HONG KONG130112 Taikoo Wan RoadTaikoo ShingHong KongTel: (852) 2585 3888Fax: (852) 2802 7638 Email: [email protected]
GENEVARue de l’Athénée 321206 GenevaSwitzerlandTel: (41) 22 566 2470Fax: (41) 22 346 93 47Email: [email protected]
DUBAIOffice 1301aAurora TowerDubai Media CityDubaiTel: (971) 4 433 4202Fax: (971) 4 438 0224Email: [email protected]
SINGAPORE8 Cross Street#23-01 Manulife TowerSingapore 048424Tel: (65) 6534 5177Fax: (65) 6534 5077 Email: [email protected]