role of tp53 mutations in therapy related acute myeloid leukaemia(t-aml)
TRANSCRIPT
Role of TP53 mutations in the origin and evolution of therapy-related
acute myeloid leukaemia(t-AML)T N. Wong, Richard K. Wilson et alDepartment of Medicine, Division of Oncology,
Washington University, St Louis
Siteman Cancer Center, Washington University, St Louis
Nature, December 2015
1
Mohsin Graduate student AIIMS
Introduction
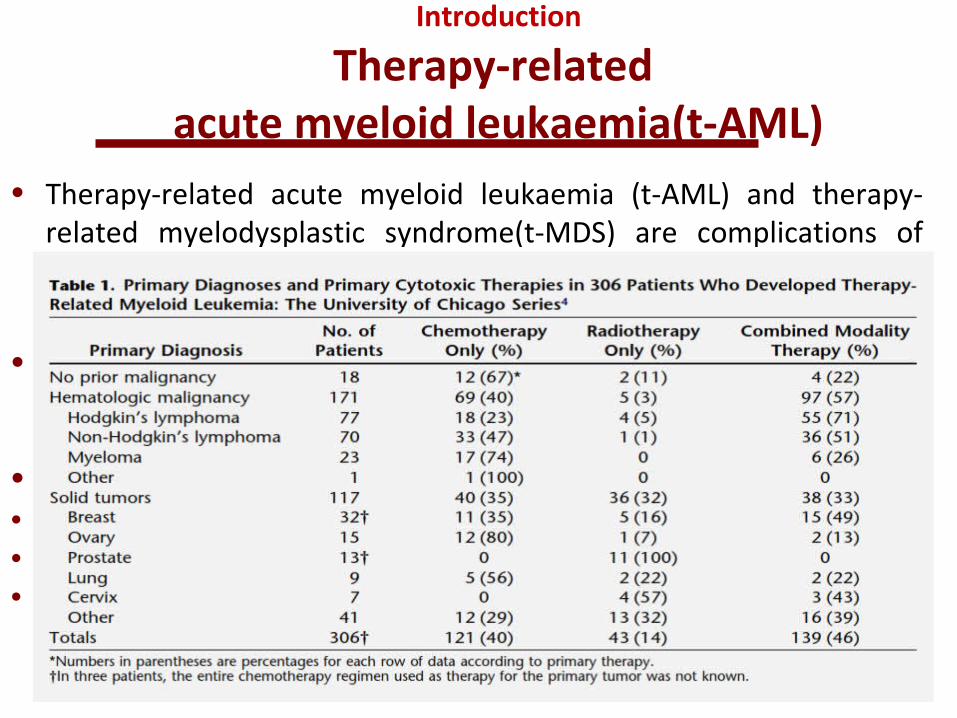
Therapy-related acute myeloid leukaemia(t-AML)
• Therapy-related acute myeloid leukaemia (t-AML) and therapy-related myelodysplastic syndrome(t-MDS) are complications of cytotoxic chemotherapy and/or radiotherapy (1-5 years)
• WHO Classification of Tumours of Haematopoietic and Lymphoid- Tissues - therapy-related myeloid neoplasms (t-MN)
• Several features that distinguish t-AML from de novo AML• abnormalities of chromosomes 5 or 7• complex cytogenetics and a reduced response to chemotherapy• Higher incidence of TP53 mutations
2
• T-MN 10 to 20 percent of all cases of AML, MDS, and MDS/MPN• Median age 61, incidence varies (cytotoxic agents(alkylating
agents/Topoisomerase II Inhibitors), specific agents, timing of exposure, and dose )
• Some patients may have a heritable predisposition to the development of t-MN
• clinical presentation of t-MN is variable but most patients have symptoms similar to patients with de novo AML or MDS
• Pancytopenia and symptoms related to this
3
Methods
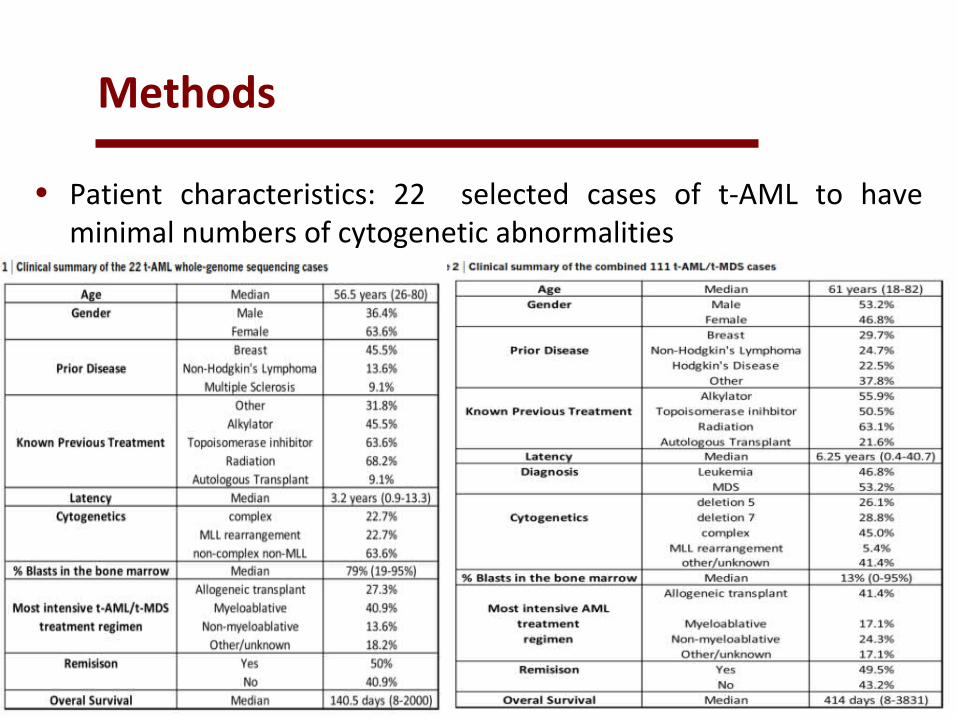
• Patient characteristics: 22 selected cases of t-AML to have minimal numbers of cytogenetic abnormalities
• additional 89 cases of t-AML/t-MDS were randomly selected fromthose samples with sufficient tumour and skin DNA
4
Whole-genome sequencing and variant detection
• Illumina DNAsequencing was used to generate sequence • Validation and extension sequencing with variant
detection,custom sequence capture arrays from Roche Nimblegen that targeted variants detected by whole-genome sequencing
• Detection of somatic TP53 mutations in cancer-free subjects. Amplicons were prepared from healthy control genomic DNA samples using primers designed to amplify exons 4–8 of TP53
• Generation and analysis ofTp53 +/- bone marrow chimaeras. Tp53 +/- ,Mice type mice were inbred on a C57BL/6 strain.
5
• Flowcytometry. Flow cytometry data were collected on a Gallios 10-colour, 3-laser flow cytometer (Beckman Coulter)
• Cells were stained by standard protocols with the following antibodies (eBiosciences)
• Ly5.1 (A20, CD45.1), Ly5.2 (104, CD45.2), Ly6C/G (RB6-• 8C5, Gr-1), CD3e (145-2C11), CD45R(RA3-6B2, B220), CD11c
(N418), TER-119, CD117 (ACK2, c-Kit) and Ly-6A/E (D7, Sca).
6
Aim
• To understand better how prior cytotoxic therapy contributes to the high incidence of TP53 mutations and karyotypic abnormalities in t-AML/t-MDS
7
RESULTS(To know the mutational spectrum of t-AML)
• Genomes of 22 cases of t-AML were sequenced• compared to whole-genome sequence data previously
reported for de novo AML And secondary AML(s-AML) arising from MDSfor which patients did not receive chemotherapy except hydroxyurea
• The Cancer Genome Atlas Research Network. Genomic and epigenomic landscapes of adult de novo acute myeloid leukemia. N. Engl. J. Med. 368,2059–2074 (2013)
• Walter, M. J. et al. Clonal architecture of secondary acute myeloid leukemia. N. Engl. J. Med. 366, 1090–1098 (2012)
• Walter, M. J. et al. Clonal diversity of recurrently mutated genes in myelodysplastic syndromes. Leukemia 27, 1275–1282 (2013)
• 23% had rearrangements of MLL (also known as KMT2A), 23% had complex cytogenetics, and 36% had normal
cytogenetics
8
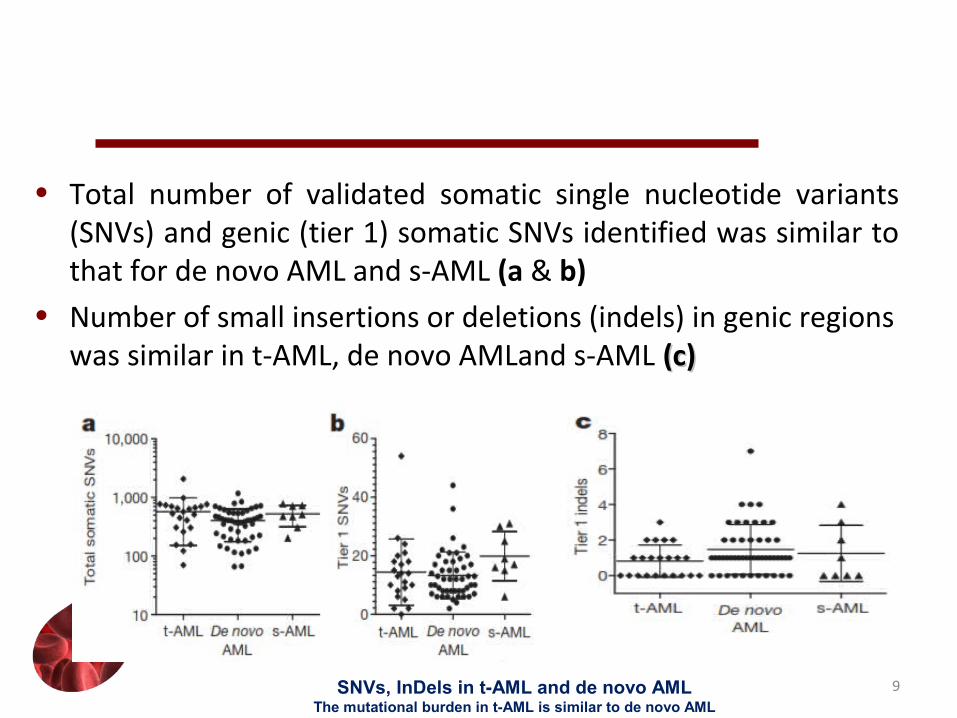
• Total number of validated somatic single nucleotide variants (SNVs) and genic (tier 1) somatic SNVs identified was similar to that for de novo AML and s-AML (a & b)
• Number of small insertions or deletions (indels) in genic regions was similar in t-AML, de novo AMLand s-AML (c)(c)
9SNVs, InDels in t-AML and de novo AMLThe mutational burden in t-AML is similar to de novo AML

• The percentage of transversions (where a purine is substituted for a
pyrimidine, A->C vice versa), and in fact of all six classes of SNVs, was similar in all three cohorts
• these data show that the mutation burden of t-AML genomes is similar to that of de novo AML genomes.
10Transversions
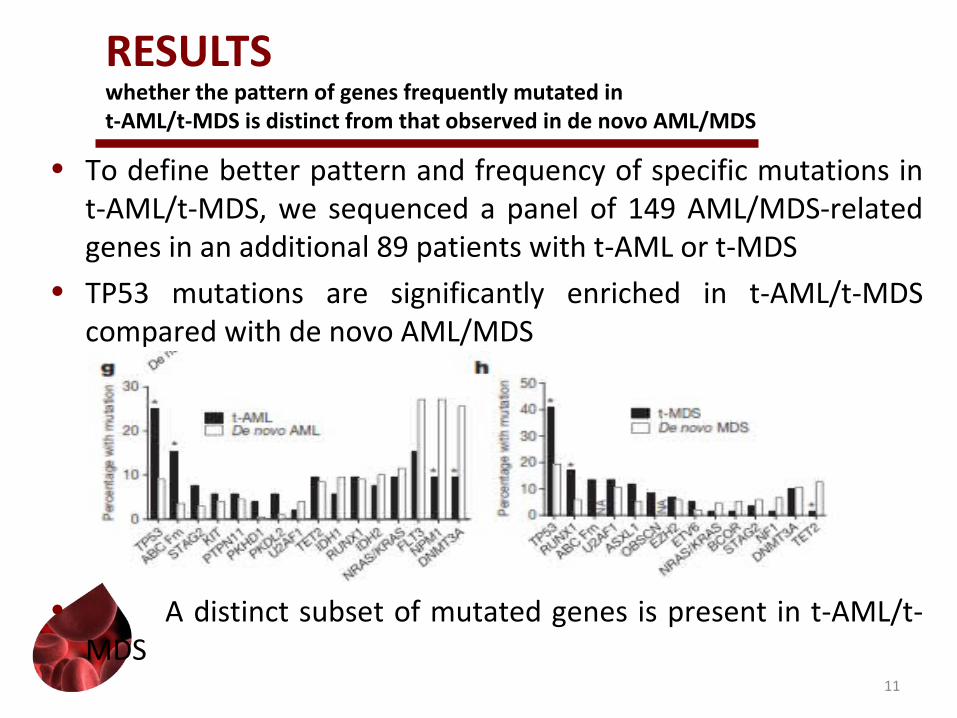
RESULTSwhether the pattern of genes frequently mutated int-AML/t-MDS is distinct from that observed in de novo AML/MDS
• To define better pattern and frequency of specific mutations in t-AML/t-MDS, we sequenced a panel of 149 AML/MDS-related genes in an additional 89 patients with t-AML or t-MDS
• TP53 mutations are significantly enriched in t-AML/t-MDS compared with de novo AML/MDS
• A distinct subset of mutated genes is present in t-AML/t-MDS
11
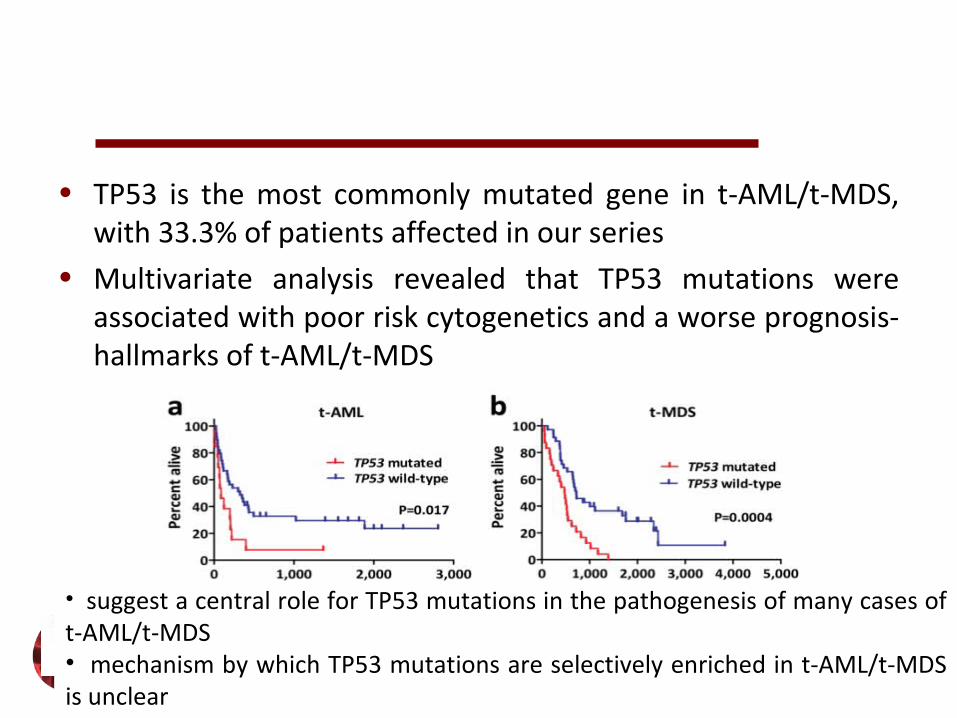
• TP53 is the most commonly mutated gene in t-AML/t-MDS, with 33.3% of patients affected in our series
• Multivariate analysis revealed that TP53 mutations were associated with poor risk cytogenetics and a worse prognosis- hallmarks of t-AML/t-MDS
12
• suggest a central role for TP53 mutations in the pathogenesis of many cases of t-AML/t-MDS• mechanism by which TP53 mutations are selectively enriched in t-AML/t-MDS is unclear
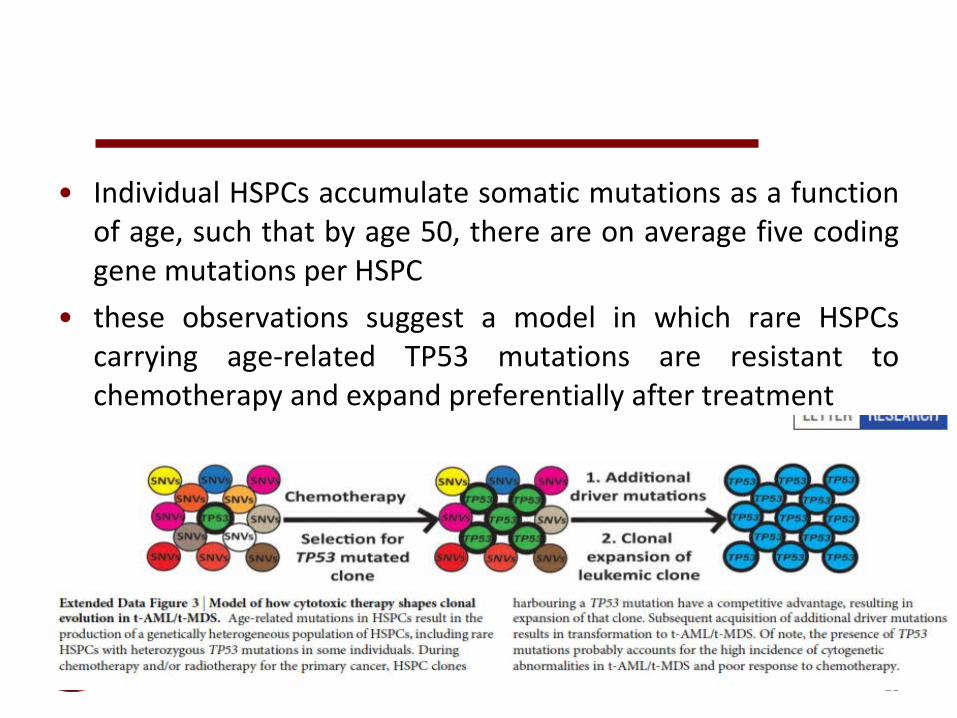
• Individual HSPCs accumulate somatic mutations as a function of age, such that by age 50, there are on average five coding gene mutations per HSPC
• these observations suggest a model in which rare HSPCs carrying age-related TP53 mutations are resistant to chemotherapy and expand preferentially after treatment
13

• t-AML containing clonal TP53 mutations, HSPCs harbouring the specific TP53 mutation will be present long before the development of overt t-AML??
• seven cases of t-AML/t-MDS with specific TP53 mutations for which we had leukapheresis or bone marrowspecimens banked
14
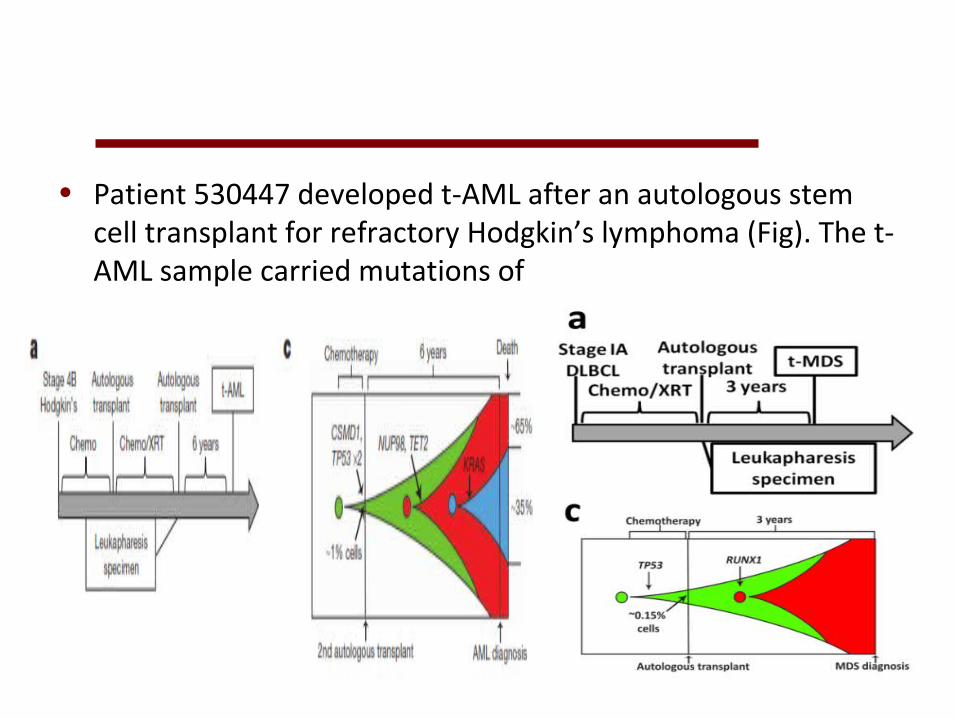
• Patient 530447 developed t-AML after an autologous stem cell transplant for refractory Hodgkin’s lymphoma (Fig). The t-AML sample carried mutations of
• TP53, missense mutations of TET2 and NUP98, a silent mutation of CSMD1, and a subclonal KRAS mutation.
• Analysis of a leukapheresis sample obtained 6 years before the development of t-AML revealed that both TP53 mutant alleles were present and CSMD1 mutation was also present (passenger mutation)However, two
• potential driver mutations (TET2 and NUP98) were not detectable,
• So, TP53 mutations preceded the development of t-AML 15
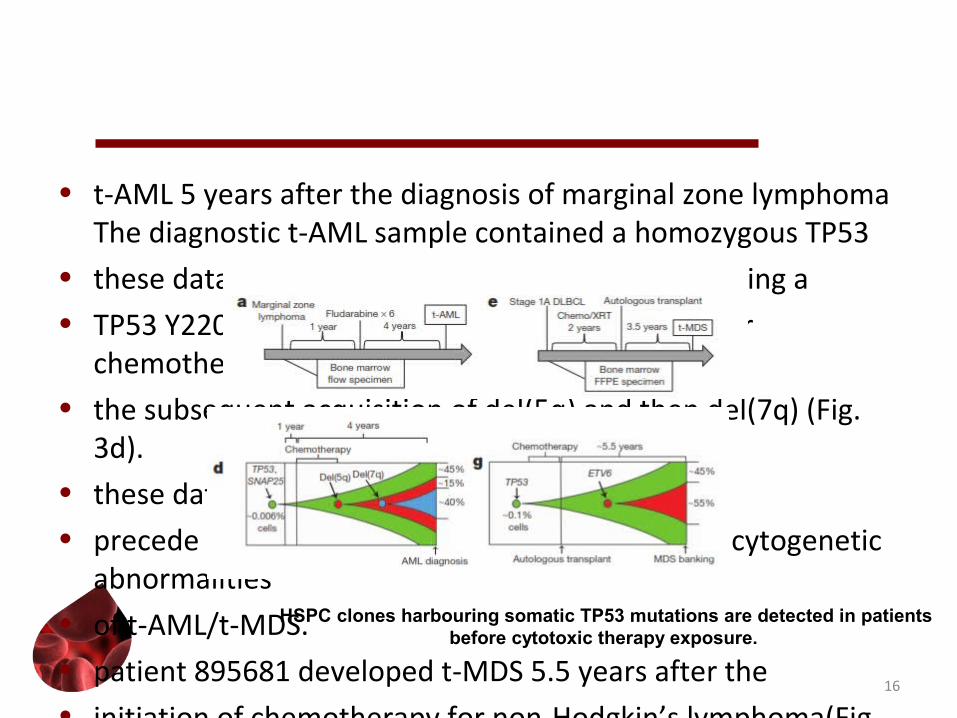
• t-AML 5 years after the diagnosis of marginal zone lymphoma The diagnostic t-AML sample contained a homozygous TP53
• these data provide evidence that an HSPC harbouring a• TP53 Y220Cmutation preferentially expanded after
chemotherapy with• the subsequent acquisition of del(5q) and then del(7q) (Fig.
3d). • these data suggest that TP53 mutations• precede the development of these characteristic cytogenetic
abnormalities• of t-AML/t-MDS.• patient 895681 developed t-MDS 5.5 years after the• initiation of chemotherapy for non-Hodgkin’s lymphoma(Fig.
3e). The• diagnostic t-MDS sample contained a clonal TP53 H179L
mutation.
16
HSPC clones harbouring somatic TP53 mutations are detected in patients before cytotoxic therapy exposure.
whether HSPCs harbouring TP53 mutations are presentin healthy individuals
• peripheral blood leukocytes from 20 elderly (68–89 years old) cancer-free donors who had not received prior cytotoxic therapy
• sequencing to exons 4–8 of TP53 since the majority of pathogenic mutations in TP53 are located in these exons
• TP53 mutations dectected in 9 of 19 evaluable cases, • These data suggest that functional• TP53 mutations may confer (even in the absence of cytotoxic• therapy) a subtle competitive advantage that results in
modest HSPC• expansion over time
17
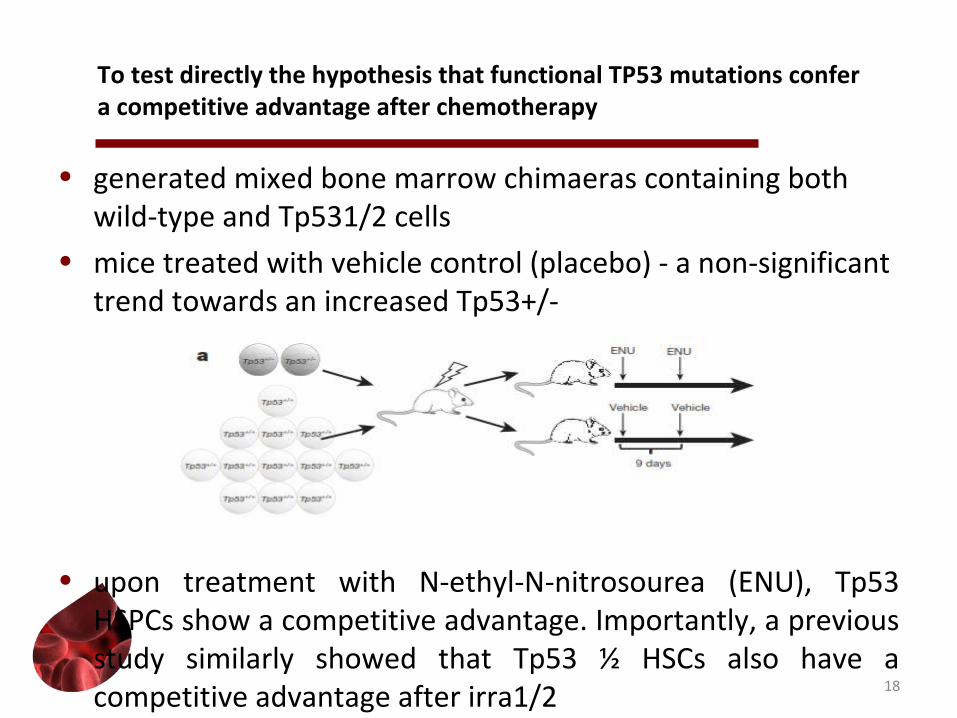
To test directly the hypothesis that functional TP53 mutations confera competitive advantage after chemotherapy
• generated mixed bone marrow chimaeras containing both wild-type and Tp531/2 cells
• mice treated with vehicle control (placebo) - a non-significant trend towards an increased Tp53+/-
• upon treatment with N-ethyl-N-nitrosourea (ENU), Tp53 HSPCs show a competitive advantage. Importantly, a previous study similarly showed that Tp53 ½ HSCs also have a competitive advantage after irra1/2 18
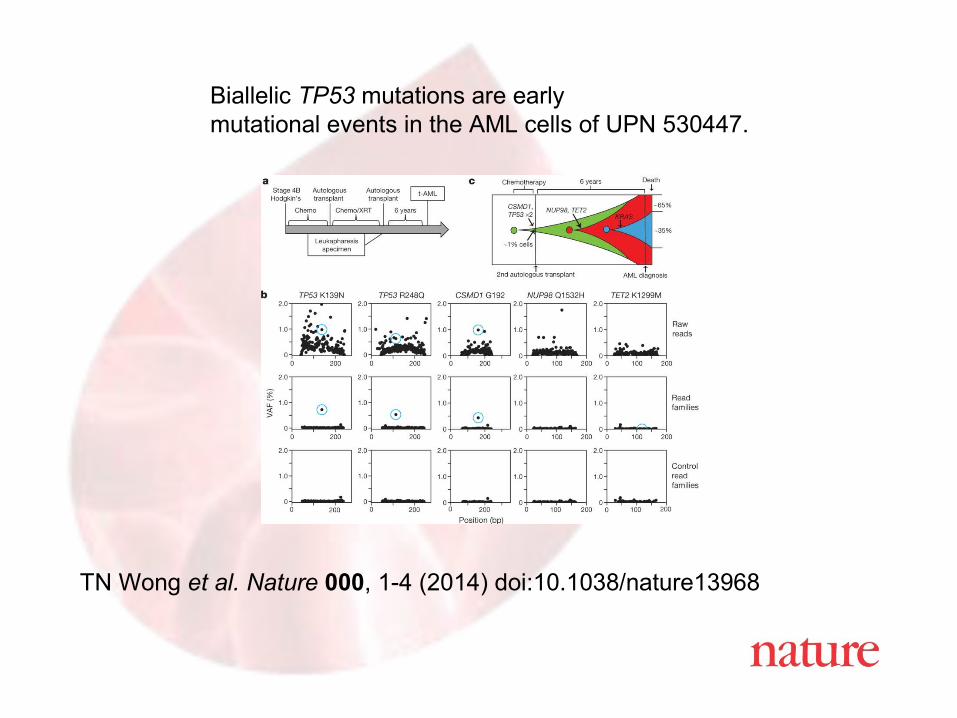
TN Wong et al. Nature 000, 1-4 (2014) doi:10.1038/nature13968
Biallelic TP53 mutations are earlymutational events in the AML cells of UPN 530447.
References & More Information• WHO Classification of Tumors of Hematopoietic and Lymphoid Tissues ,
4th edition, S. Swerdlow, E. Campo, N. Lee Harris, E. Jaffe, S. Pileri, H. Stein, J. Thiele, J. Vardiman, IAR C, Lyon, France, 2008
• 2010 Hematopoietic and Lymphoid Neoplasm Case Reportability and Coding Manual, C. Hahn Johnson, M. Adamo, S. Peace, NCI SEER, 2009
• Advances in Understanding and Management of Myeloproliferative Neoplasms, Alessandro M. Vannucchi, Paola Guglielmelli and Ayalew Tefferi, CA Cancer J Clin 2009;59;171-191; Apr 15, 2009
• Proposed Classification of Lymphoid Neoplasms for Epidemiollogic Research from the International Lymphoma Epidemiology Consortium (Inter-Lymph), L. Morton, J. Turner, J. Cernan, Blood, DOI 10.1182/2006-11-0515672; Mar 27, 2007
20

• Thank you
21
Conclusion
• The new hematopoietic and lymphoid neoplasm rules go into effect for cases diagnosed January 1, 2010, and after
• Email address for questions [email protected]
22