adjuvant treatment: target therapies belgian breast meeting 13-14 october 2006 brussels, belgium...
TRANSCRIPT

ADJUVANT TREATMENT: TARGET THERAPIES ADJUVANT TREATMENT: TARGET THERAPIES
BELGIAN BREAST MEETING13-14 October 2006Brussels, Belgium
Fatima Cardoso, MDFatima Cardoso, MD
Jules Bordet Institute & TRANSBIGJules Bordet Institute & TRANSBIG

ENDOCRINE THERAPYFirst example of TARGETED THERAPY
ER
The target
The ligand
Aromataseinhibitors
Aromataseinhibitors
SERMS & ER DOWN REGULATORS
SERMS & ER DOWN REGULATORS

Trastuzumab upfront in combination with
platinum/taxane (BCIRG 006)
Trastuzumab after 3 months of AC, in
combination with taxane (NSABP-B31)
Trastuzumab monotherapy after 6 months of AC → T
or in combination with taxane (NCCTG-N9831)
Trastuzumab monotherapy after 6 months of standard chemotherapy (HERA Trial)
Trastuzumabfor 1 year
Trastuzumabfor 1 or 2 years
Total 12,000 women
Selection of the subgroup most likely to benefit: IHC 3+ or FISH positive in all
trials
TRASTUZUMAB IN THE ADJUVANT SETTINGTRASTUZUMAB IN THE ADJUVANT SETTINGSUMMARY OF THE FOUR MAJOR TRIALSSUMMARY OF THE FOUR MAJOR TRIALS
3-weekly
weekly&3-weekly
Only trial with a non-A arm
FinHER Trial
+

00 0.50.5 11 1.251.25
HERAHERA 1y1y
B31/N9831 B31/N9831 ACAC PHPH
BCIRG006BCIRG006 ACAC DHDH
BCIRG006BCIRG006 DCarboHDCarboH
FINHERFINHER
0.640.64
0.480.48
0.490.49
0.610.61
0.420.42
DISEASEDISEASE--FREE SURVIVALFREE SURVIVAL
HRHR
00 0.50.5 11 1.251.25
HERAHERA 1y1y
B31/N9831 B31/N9831 ACAC PHPH
BCIRG006BCIRG006 ACAC DHDH
BCIRG006BCIRG006 DCarboHDCarboH
FINHERFINHER
0.640.64
0.480.48
0.490.49
0.610.61
0.420.42
DISEASEDISEASE--FREE SURVIVALFREE SURVIVAL
HRHR
ADJUVANT TRASTUZUMAB TRIALS ADJUVANT TRASTUZUMAB TRIALS EFFICACY RESULTS AT EFFICACY RESULTS AT 2 YEARS MEDIAN FU 2 YEARS MEDIAN FU
Favors trastuzumabFavors trastuzumab
Reduction in relapses (DFS) of 52% to 68% Similar results in DDFS

00 0.50.5 11 1.251.25
HERAHERA 1y1y
B31/N9831 B31/N9831 ACAC PHPH
FINHERFINHER
0.660.66
0.670.67
0.410.41
OVERALL SURVIVALOVERALL SURVIVAL
HRHR
00 0.50.5 11 1.251.25
HERAHERA 1y1y
B31/N9831 B31/N9831 ACAC PHPH
FINHERFINHER
0.660.66
0.670.67
0.410.41
OVERALL SURVIVALOVERALL SURVIVAL
HRHR
44% reduction in mortality risk
ADJUVANT TRASTUZUMAB TRIALS ADJUVANT TRASTUZUMAB TRIALS EFFICACY RESULTS AT EFFICACY RESULTS AT 2 YEARS MEDIAN FU 2 YEARS MEDIAN FU
Favors trastuzumabFavors trastuzumab

ADJUVANT TRASTUZUMAB TRIALSADJUVANT TRASTUZUMAB TRIALSCARDIOTOXICITY RISKSCARDIOTOXICITY RISKS
No No TT
9 wks T 9 wks T withwithAnti-Anti-
micro-micro-tubules tubules
then then FEC x 3FEC x 3
Doce Doce taxel, taxel,
CarboplCarboplatin atin
and Tand T
Sequential A-Sequential A-based CTX then based CTX then
TT
AC x 4AC x 4then then T combined with T combined with
taxanetaxane
000.80.8
0.40.4 0.60.6
2.52.5
1.61.6
3.53.5
Control Control armsarms
BCIRG BCIRG 006006
HERAHERA N-9831N-9831 BCIRGBCIRG006006
Risk ofRisk ofCHFCHF
NYHANYHAClass 3-4Class 3-4
00
FinHERFinHER
Median f-upMedian f-up 121239m39m 2 y2 y 39m39m 1 y1 y 2 y2 y 2 y2 y 2 y2 y
N at riskN at risk >4000>4000 10561056 116116 16771677 718718 10681068 579579
Treatment Treatment strategystrategy
N-9831N-9831 B31B31
4.14.1
3 y3 y
846846
0
1
2
3
4
M. Piccart used with permission

ADJUVANT TRASTUZUMAB TRIALSADJUVANT TRASTUZUMAB TRIALSCARDIOTOXICITY RESULTSCARDIOTOXICITY RESULTS
REASONS FOR DIFFERENT CARDIOTOXICITY RESULTS REASONS FOR DIFFERENT CARDIOTOXICITY RESULTS AMONG ADJUVANT TRIALSAMONG ADJUVANT TRIALS
• Different follow-upDifferent follow-up
• Different sample size (FinHER)Different sample size (FinHER)
• No use of anthracyclines (BCIRG 006 TCH arm)No use of anthracyclines (BCIRG 006 TCH arm)
• Sequential administration of chemotherapy Sequential administration of chemotherapy trastuzumab (HERA) trastuzumab (HERA)
• Sequential administration of radiotherapy Sequential administration of radiotherapy trastuzumab (HERA) trastuzumab (HERA)

IMPAIRMENT IN TRASTUZUMAB ADMINISTRATION BECAUSE IMPAIRMENT IN TRASTUZUMAB ADMINISTRATION BECAUSE OF CARDIAC PROBLEMSOF CARDIAC PROBLEMS
KEY MESSAGES FOR CLINICAL PRACTICEKEY MESSAGES FOR CLINICAL PRACTICE
• Depending on age, between 1.3% and 4% of women younger Depending on age, between 1.3% and 4% of women younger than 65 cannot be started on than 65 cannot be started on upfrontupfront trastuzumab, in view of trastuzumab, in view of cardiac risk factors or cardiac diseasescardiac risk factors or cardiac diseases
• If anthracycline is given, an additional 6% to 7 % will not access If anthracycline is given, an additional 6% to 7 % will not access trastuzumab and an additional 5% to 20% will not be able to complete 1 trastuzumab and an additional 5% to 20% will not be able to complete 1 year of treatment, depending on the schedule of administration with year of treatment, depending on the schedule of administration with taxanetaxane
• An LVEF An LVEF entry criterionentry criterion of 55% after CT and RT of 55% after CT and RT (HERA trial) precludes (HERA trial) precludes access to trastuzumab to another 5-6% of womenaccess to trastuzumab to another 5-6% of women
M. Piccart –ESMO 2006-used with permission
UNANSWEREDUNANSWERED / OPEN QUESTIONS / OPEN QUESTIONS
• The benefit versus harm ratio remains unknown for women with The benefit versus harm ratio remains unknown for women with
cardiac risk factors, age above 70 and / or small (cardiac risk factors, age above 70 and / or small (1cm) node 1cm) node
negative tumors (negative tumors (ATTENTION WHEN DESIGNING CLINICAL TRIALSATTENTION WHEN DESIGNING CLINICAL TRIALS))
• Optimal Optimal durationduration of trastuzumab treatment (9 ws vs. 1 vs. 2 years) of trastuzumab treatment (9 ws vs. 1 vs. 2 years)
• Optimal Optimal timingtiming to initiate trastuzumab to initiate trastuzumab
• Optimal Optimal scheduleschedule (sequential vs. concomitant with CT) (sequential vs. concomitant with CT)
• Is CT always necessary? Role of HT + TrastuzumabIs CT always necessary? Role of HT + Trastuzumab
• Mechanisms of resistance to trastuzumabMechanisms of resistance to trastuzumab (MBC: only at the most (MBC: only at the most
50% of HER-2-positive BC respond & median duration response 9 ms)50% of HER-2-positive BC respond & median duration response 9 ms)

CO-AMPLIFICATION OF cMYC AND HER-2 PREDICTS FOR CO-AMPLIFICATION OF cMYC AND HER-2 PREDICTS FOR TRASTUZUMAB’S BENEFIT TRASTUZUMAB’S BENEFIT (S. PAIK, SABCC 2005)(S. PAIK, SABCC 2005)
BackgroundBackground • HER-2 and cMYC: only independent prognostic factors HER-2 and cMYC: only independent prognostic factors in NSABP-B28in NSABP-B28
• 25% of HER-2+ patients have coamplification of cMYC25% of HER-2+ patients have coamplification of cMYC
NSABP-B31NSABP-B31 Coamplification of cMYCCoamplification of cMYC
NoNo YesYesTrastuzumab’s benefitTrastuzumab’s benefit
HR DFS HR DFS 0.630.632p = 0.0072p = 0.007
0.240.242p < 0.00012p < 0.0001
HR O.S.HR O.S. NO GAINNO GAIN 0.360.362p = 0.0122p = 0.012
HypothesisHypothesis Trastuzumab turns on the pro-apoptotic function of Trastuzumab turns on the pro-apoptotic function of deregulated cMYCderegulated cMYC
M. Piccart –ESMO 2006-used with permission

m-TOR, m-TOR, PTENPTEN AND SENSITIVITY TO TRASTUZUMAB IN AND SENSITIVITY TO TRASTUZUMAB IN HER-2 (+) CANCER CELLSHER-2 (+) CANCER CELLS
Pandolfi, 2004

HER-2 P95 POSITIVE TUMORS RESPOND LESS TO TRASTUZUMAB
N= 36 patients treated with trastuzumab
Courtesy J. Baselga

CONFIDENTIAL – NOT FOR
DISTRIBUTION
LAPATINIB IN (NEO) ADJUVANT THERAPY OF HER-2 + LAPATINIB IN (NEO) ADJUVANT THERAPY OF HER-2 + BREAST CANCER: RATIONALEBREAST CANCER: RATIONALE
• Trastuzumab only partially activeTrastuzumab only partially active• Lapatinib:Lapatinib:
– Has a Has a different mechanismdifferent mechanism of action of action– Active in trastuzumab resistantActive in trastuzumab resistant patients patients – May be May be active in HER2 p95 positiveactive in HER2 p95 positive tumors tumors– High level of High level of activity in singleactivity in single agent first line setting agent first line setting– Preclinical synergyPreclinical synergy with the combination of lapatinib and with the combination of lapatinib and
trastuzumab. Encouraging activity of the combination in trastuzumab. Encouraging activity of the combination in patients with prior therapy with trastuzumabpatients with prior therapy with trastuzumab
– May be May be active against brain (micrometastatic) active against brain (micrometastatic) diseasedisease

In combination with In combination with capecitabine (X) capecitabine (X)
improves TTPimproves TTP in women in women pretreated with pretreated with
anthracycline/taxanes anthracycline/taxanes and trastuzumab and trastuzumab
(late breaking)(late breaking)
As single agent shows As single agent shows modest but real modest but real
activity against brain activity against brain metastasesmetastases in in
trastuzumab "failures"trastuzumab "failures"(abstr # 503)(abstr # 503)
In a review of 3127 In a review of 3127 lapatinib-treated lapatinib-treated
patients, patients, shows very shows very little cardiotoxicitylittle cardiotoxicity
(abstr # 585)(abstr # 585)
ASCO 2006 METASTATIC BREAST CANCERASCO 2006 METASTATIC BREAST CANCERHER-2 + BREAST CANCERHER-2 + BREAST CANCER
New drugs: New drugs: LAPATINIBLAPATINIB
Single agent Lapatinib active in relapsed/refractory IBC
(abstr # 502)

CONFIDENTIAL – NOT FOR
DISTRIBUTION
NEOADJUVANTNEOADJUVANT ADJUVANTADJUVANT
20072007 20082008 20092009 20102010 20112011
Neo-AdjuvantNeo-Adjuvant
AdjuvantAdjuvant
Build confidence Build confidence in lapatinib in lapatinib
(interim look)(interim look)
Build translational Build translational research hypothesis and research hypothesis and
validate themvalidate them

CONFIDENTIAL – NOT FOR
DISTRIBUTION
NEO-ADJUVANT: RANDOMIZED PHASE II TRIALNEO-ADJUVANT: RANDOMIZED PHASE II TRIAL
RRAANNDDOOMMIIZZAATTIIOONN
HER2 3+HER2 3+TumorsTumors> 2 cm> 2 cm(N=450)(N=450)
Trastuzumab x 6 weeks
Trastuzumab + paclitaxel x 12 weeks
Lapatinib x 6 weeks
Lapatinib + paclitaxel x 12 weeks
+ Lapatinib x 6 weeks
Trastuzumab
+ paclitaxel x 12 weeks
Trastuzumab + lapatinib
SSUURRGGEERRYY
Trastuzumabx 34 weeks
Lapatinibx 34 weeks
Trastuzumab+ lapatinibx 34 weeks
BiopsyBiopsy(Pet Scan)(Pet Scan)
Week 2: BiopsyWeek 2: Biopsy(Pet Scan)(Pet Scan)
pCR ratepCR rate
TranslationalTranslationalresearchresearch
Disease-free Disease-free survivalsurvival
FECFEC
FECFEC
FECFEC
450 PTS (150 x arm)

CONFIDENTIAL – NOT FOR
DISTRIBUTION
•Women considered candidates for adjuvant taxanes receive weekly paclitaxel concomitantly with the biologic therapy.Women considered candidates for adjuvant taxanes receive weekly paclitaxel concomitantly with the biologic therapy.•Patients with ER or PgR-positive tumors receive endocrine therapy selected accordingly to menopausal status; administered concurrent Patients with ER or PgR-positive tumors receive endocrine therapy selected accordingly to menopausal status; administered concurrent with biologics and continuing for at least 5 years.with biologics and continuing for at least 5 years.•N=8000 women HR 0.78 between experimental-arm and trastuzumab; (3 pair wise comparisons; 80% power; 691 events for each N=8000 women HR 0.78 between experimental-arm and trastuzumab; (3 pair wise comparisons; 80% power; 691 events for each comparison)comparison)
ADJUVANT DESIGN – HERA MODELADJUVANT DESIGN – HERA MODEL
Trastuzumabfor 1 year
Lapatinibfor 1 year
Lapatinibfor 6 months
Trastuzumab 3-weekly + lapatinib for 1 year
Centrally-determined HER2 +
Surgery, complete (neo)adjuvant anthracycline-based chemotherapy (selected from an approved list); complete adjuvant radiation therapy (if given)
LVEF 50
RANDOMIZATION
Locally-determined HER2-positive invasive breast cancer
(For patients with neoadjuvant treatment, the Her2 determination should be done on a tissue sample taken before the treatment is started)
Trastuzumab 3-weekly for 6 months
8000 PTS

CONFIDENTIAL – NOT FOR
DISTRIBUTION
DESIGN – high risk patients: taxanesDESIGN – high risk patients: taxanes
Locally-determined HER2-positive invasive breast cancer
(For patients with neoadjuvant treatment, the Her2 determination should be done on a tissue sample taken before the treatment is started)
Centrally-determined HER-2 +
Surgery, complete (neo)adjuvant anthracycline-based chemotherapy
LVEF 50
1
YEAR
Lapatinib +
3-weekly trastuzumab
Lapatinib +Weekly
trastuzumab12 weeks
Weekly trastuzumab
12 weeks
Lapatinib
3-weekly trastuzumab
6 months
Weekly paclitaxel12 weeks
3-weekly trastuzumab
Lapatinib6 months
Radiotherapy (if indicated)
Weekly paclitaxel12 weeks
Radiotherapy (if indicated)
Weekly paclitaxel12 weeks
Radiotherapy (if indicated)
Weekly paclitaxel12 weeks
Radiotherapy (if indicated)
RANDOMIZATION

View of a Medical Oncologist and a Clinical/Translational Researcher
1) … 2) … 3) Lapatinib and Bevacizumab will
be the next targeted therapies to be tested in the breast adjuvant setting, with the possibility of Lapatinib taking the place of Trastuzumab.
The Breast Cancer Observatory:Innovation and care in the next
12 months
TUMOR VASCULATUREN Engl J Med 351 (3): 216, 2004

BEVACIZUMAB IN METASTATIC BREAST CANCER
Author N of pts Treatment RR (%) PFS (mo) OS (mo)
Miller (2005)
462 (pretreated)
Capecitabine ± Bevacizumab
20 vs. 9(p=0.001)
5 vs 4(p=0.98)
15 vs.15 15 vs.15 (p=nr)(p=nr)
Miller (2005)
715(1st line)
Weekly paclitaxel ± Bevacizumab
29 vs. 14(p<0.0001)
11 vs 6(p<0.001)
HR 0.67 HR 0.67 (p=0.01)(p=0.01)
IMP since always
RARE in MBC
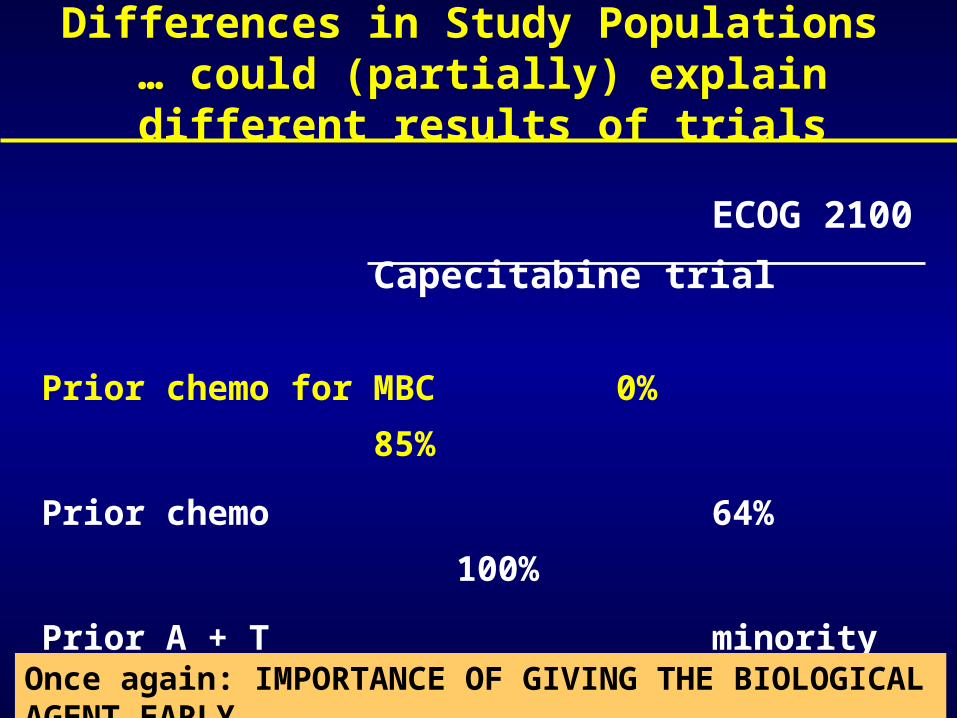
ECOG 2100
Capecitabine trial
Prior chemo for MBC 0% 85%
Prior chemo 64% 100%
Prior A + T minority 100%
HER-2+ hardly any 25%
Prior trastuzumab hardly any 23%
Differences in Study Populations … could (partially) explain different results of trials
Once again: IMPORTANCE OF GIVING THE BIOLOGICAL AGENT EARLY

Bevacizumab: A “Targeted Therapy” Without A Target ??!!
…and an expensive one…
Unlike trastuzumab, to date, no predictive factors of response to bevacizumab, including VEGF
expression, have been identified

HER-2 TESTING IN N9831
• Modest level of concordance between local and central laboratories for both IHC and FISH (n=1815 pts)
– 802 with HercepTest™: 81% (78-83%)
– 550 with FISH: 87% (84-90%)
– 463 with non-HercepTest: 74% (70-80%)
• High level of agreement between central and reference laboratory results for HER-2
Updated from Perez EA, et al. ASCO 2004 (abstract 567)

“THE HERCEPTIN HYPE”
Cancerworld, Anna Wagstaff, March-April2006
Balanced enthusiasm is also OUR responsibility