ajcc-june
DESCRIPTION
AJCC-June journelTRANSCRIPT

In This Issue
— Cardiac Rehabilitation
— Study of Association between Metabolic Syndrome and Acute Coronary Syndrome
— Study of Cardiac Manifestations of HIV/AIDS and their Correlation with CD4+ T-cell Count
— Left Atrial Myxoma Presenting as Severe Pulmonary Hypertension
— Atrioventricular Re-entrant Tachycardia: Clues to Underlying Accessory Pathway and its Location
— Initial Assessment of Evaluation of the Patient with Acute Chest Pain
— Right-Sided Cardiophrenic Mass in an Older Woman
— AAN Releases Guideline on Magnetic Resonance Imaging for Diagnosing Acute Ischemic Stroke
— Insight on Medicolegal Issues
Volume 15, Number 2, June 2012 Pages 41-80

Volume 15, Number 2, June 2012
IJCP Group of PublicationsDr Sanjiv Chopra
Prof. of Medicine & Faculty Dean Harvard Medical SchoolGroup Consultant Editor
Dr Deepak ChopraChief Editorial Advisor
Dr KK AggarwalCMD, Publisher, Group Editor-in-Chief
Dr Veena AggarwalMD, Group Executive Editor
Advisory BodiesHeart Care Foundation of India
Non-Resident Indians Chamber of Commerce & IndustryWorld Fellowship of Religions
IJCP Editorial BoardObstetrics and Gynaecology Dr Alka Kriplani, Dr Thankam Verma, Dr Kamala SelvarajCardiology Dr Praveen Chandra, Dr M Paul Anand, Dr SK ParasharPaediatrics Dr Swati Y Bhave, Dr Balraj Singh Yadav, Dr Vishesh KumarDiabetology Dr Vijay Viswanathan, Dr CR Anand Moses, Dr Sidhartha Das, Dr A Ramachandran, Dr Samith A ShettyDentistry Dr KMK Masthan, Dr Rajesh ChandnaGastroenterology Dr Ajay KumarDermatology Dr Hasmukh J ShroffNephrology Dr Georgi AbrahamNeurology Dr V NagarajanJournal of Applied Medicine & Surgery Dr SM Rajendran
Dr Praveen ChandraGuest Editor, AJCC
[email protected] Editor: Dr Nagendra Chouhan, Dr Dharmendar Jain
InternationalDr Fayoz ShanlDr Alain CribierDr Kohtian HaiDr Tanhuay CheemDr Ayman MegdeDr Alan YoungDr Gaddy GrimesDr Jung bo GegDr Rosli Mohd. AliDr S SaitoNationalDr Mansoor HassanDr RK Saran
Dr SS SinghalDr Mohd. AhmedDr PK JainDr PK GuptaDr Naresh TrehanFACultyDr GK Aneja Dr Ramesh ThakurDr Balram BhargavaDr HK BaliDr HM MardikarDr Sanjay MehrotraDr Vivek MenonDr Keyur Parikh
Dr Ajit MullasariDr Kirti PunamiyaDr MS HiramathDr VS NarainDr SK DwivediDr Raja Baru PanwarDr Vijay TrehanDr Rakesh VermaDr Suman BhandariDr Ravi KasliwalDr Atul AbhyankarDr Tejas PatelDr Samir Dani
AJCC SPECIAlIty PANElADVISOry BOArD
Anand Gopal BhatnagarEditorial Anchor
Journal ofCLINICALCARDIOLOGYA
sian
FrOM tHE DESK OF GrOuP EDItOr-IN-CHIEF
45 New 2012 Heart Failure Guidelines KK Aggarwal
rEVIEw ArtIClE
47 Cardiac rehabilitation Mark B. Stephens
OrIGINAl ArtIClE
53 Study of Association between Metabolic Syndrome and Acute Coronary Syndrome
Virendra Dhakhada, Madhu Panjwani, Ajay Dabhi
ClINICAl StuDy
57 Study of Cardiac Manifestations of HIV/AIDS and their Correlation with CD4+ t-cell Count
Anjum Parvez, Mohammad Asif, Lubna Zafar, Asif Hasan, HS Khan
CASE rEPOrt
61 left Atrial Myxoma Presenting as Severe Pulmonary Hypertension
Deep Chandra Pant, Hema Pant
63 Atrioventricular re-entrant tachycardia: Clues to underlying Accessory Pathway and its location
Avinash Talele, S Kabde, N Kumar, MK Jain
ClINICAl AlGOrItHM
66 Initial Assessment of Evaluation of the Patient with Acute Chest Pain
Courses Available:
Course Fee : 50,000/*
45Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
Editorial Policies
The purpose of IJCP Academy of CME is to serve the medical profession and provide print continuing medical education as a part of their social commitment. The information and opinions presented in IJCP group publications reflect the views of the authors, not those of the journal, unless so stated. Advertising is accepted only if judged to be in harmony with the purpose of the journal; however, IJCP group reserves the right to reject any advertising at its sole discretion. Neither acceptance nor rejection constitutes an endorsement by IJCP group of a particular policy, product or procedure. We believe that readers need to be aware of any affiliation or financial relationship (employment, consultancies, stock ownership, honoraria, etc.) between an author and any organization or entity that has a direct financial interest in the subject matter or materials the author is writing about. We inform the reader of any pertinent relationships disclosed. A disclosure statement, where appropriate, is published at the end of the relevant article.
Note: Asian Journal of Clinical Cardiology does not guarantee, directly or indirectly, the qual-ity or efficacy of any product or service described in the advertisements or other material which is commercial in nature in this issue.
Published, Printed and Edited byDr KK Aggarwal, on behalf of
IJCP Publications Ltd. and Published at
E - 219, Greater Kailash, Part - 1 New Delhi - 110 048
E-mail: [email protected]
Printed at IG Printers Pvt. Ltd., New DelhiE-mail: [email protected]
© Copyright 2012 IJCP Publications ltd. All rights reserved.
The copyright for all the editorial material contained in this journal, in the form of layout, content including images
and design, is held by IJCP Publications Ltd. No part of this publication may be published in any form whatsoever
without the prior written permission of the publisher.
IJCP’s EDItOrIAl & BuSINESS OFFICESDelhi Mumbai Kolkata Bangalore Chennai Hyderabad
Dr Veena Aggarwal9811036687
E - 219, Greater Kailash, Part - I,
New Delhi - 110 048 Cont.: 011-40587513
[email protected]@gmail.com
SubscriptionDinesh: [email protected]: 09831363901
Mr. Nilesh Aggarwal 9818421222
Building No - D 10 Flat No - 43, 4th Floor Asmita Co-operative
Housing Society Near Charkop Naka
Marvey Road Malad (W)
Mumbai 400 [email protected]
Sr. BMRitu Saigal
9831363901Flat 5E,
Merlin Estate Geetanjali
25/8 Diamond Harbour Road
Kolkata - 700 008 Cont.: 24452066
Sr. BMH Chandrashekar
9845232974Arora Business
Centre, 111/1 & 111/2, Dickenson Road
(Near Manipal Centre)Bangalore - 560 042
Cont.: 25586337 [email protected]
Sr. BMChitra Mohan9841213823
40A, Ganapathy-puram
Main Road Radhanagar Chromepet
Chennai - 600 044Cont.: 22650144 [email protected]
Sr. BM Venugopal
9849083558H. No.
16-2-751/A/70 First Floor
Karan Bagh Gaddiannaram Dil Sukh Nagar
Hyderabad - 500 059
Cont.: [email protected]
Sr.: Senior; BM: Business Manager
New 2012 Heart Failure Guidelines  Compared with the ESC’s 2008 guidelines, the new guidelines call for a more liberal use of mineralocorticoid-
receptor antagonists (MRAs) i.e. aldosterone antagonists in heart failure. They are recommended for most patients who remain symptomatic despite treatment with both angiotensin-converting enzyme (ACE) inhibitors and b-blockers. It can now be given to New York Heart Association (NYHA) Class 2 patients with a left ventricular ejection fraction (LVEF) <35%.
 The new guidelines also give new weight to reduction of heart rate (HR) as a specific treatment target by adding ivabradine if the rate remains 70 bpm or higher despite triple-drug therapy: Optimized b-blockers, ACE inhibitors and MRAs (SHIFT trial).
 Drugs that should not be given specifically for heart failure include statins and oral anticoagulants, except in patients with atrial fibrillation.
 Drugs that may actually be harmful in heart failure include thiazolidinediones and calcium-channel blockers that are negatively inotropic i.e. most of them.
 In atrial fibrillation, it is possible of course to use the new anticoagulants (oral direct thrombin inhibitors and oral factor Xa inhibitors). But these drugs are contraindicated in severe renal impairment - and a lot of patients with heart failure, as we know, have this condition.
 Patients expected to survive with good functional status for more than one year should receive cardiac resynchronization therapy (CRT) if they are in sinus rhythm, their LVEF is low (<30%), and QRS duration is markedly prolonged irrespective of symptom severity.
 Application to NYHA Class 2 heart failure is what’s new based on the MADIT-CRT and RAFT trials, in addition to reduced certainty that CRT will benefit patients with a right-bundle-branch-block (RBBB) QRS morphology or atrial fibrillation.
 CRT should be done in patients with NYHA Class 2 with a QRS duration >130 ms with a left-bundle-branch block (LBBB) morphology and LVEF <30%.
 For non-LBBB morphology, look for a QRS width of >150 ms, and that gets a Class IIa (‘should be considered’) recommendation.
 In considering CRT in NYHA Class 2 patients within the QRS-duration window of 120-150 ms take a clinical decision. “Do you see strong convincing evidence of mechanical dyssynchrony with an imaging technique? Is there left ventricular dilatation? Is there LBBB? Has the patient recently been more symptomatic?”
 Recommendations for use of coronary artery bypass graft (CABG) in heart failure have broadened as a result of the STICH trial, which saw benefits from the surgery in patients with systolic heart failure but only mild angina.
 As a result of the PARTNER trials, transcatheter aortic valve implantation (TAVI) enters the guidelines. It should be considered in patients with aortic stenosis who are not appropriate candidates for conventional surgery.
Dr KK AggarwalPadma Shri and Dr BC Roy National AwardeeSr. Physician and Cardiologist, Moolchand Medcity, New DelhiPresident, Heart Care Foundation of IndiaGroup Editor-in-Chief, IJCP Group and eMedinewSChairman Ethical Committee, Delhi Medical CouncilDirector, IMA AKN Sinha Institute (08-09)Hony. Finance Secretary, IMA (07-08)Chairman, IMA AMS (06-07)President, Delhi Medical Association (05-06)[email protected]://twitter.com/DrKKAggarwalKrishan Kumar Aggarwal (Facebook)
from the desk of group editor-in-chiefPHOtO quIz
67 right-Sided Cardiophrenic Mass in an Older woman
rESEArCH rEVIEw
69 Journal Scan
PrACtICE GuIDElINES
71 AAN releases Guideline on Magnetic resonance Imaging for Diagnosing Acute Ischemic Stroke
ArOuND tHE GlOBE
72 News and Views
MEDIlAw
73 Insight on Medicolegal Issues
Sudhir Gupta
lIGHtEr rEADING
74 lighter Side of Medicine

47Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 201246 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
 Left ventricular assist devices (LVADs) are now ‘recommended’ in patients who are also candidates for transplantation and have ‘should-be-considered’ status for destination therapy.
 LVADs may be increasingly used in selected patients with less severe disease than end stage, ‘before right-ventricular or multiorgan failure develops.
 The ventricular assist devices may ultimately become a more general alternative therapy to transplantation, because the current 2-3 year survival rates with continuous-flow devices seem superior not only to medical therapy but also to pulsatile flow devices.
 In the new guidelines there is a smaller presence of recommendations relating to lifestyle changes. With only two exceptions, you will not see in the new guidelines any recommendation in relation to lifestyle. The exceptions, both Class IA recommendations: “Regular aerobic exercise is encouraged in patients with heart failure to improve functional capacity and symptoms,” and patients are advised to enrol in a ‘multidisciplinary-care management program’ to lower the risk of heart-failure hospitalization. (www.escardio.org/guidelines).
from the desk of group editor-in-chief
Cardiovascular disease remains the leading cause of death in the United States. More than 850,000 annual deaths in the United States are attributed
to cardiovascular disease.1 On a worldwide basis, 30 percent of deaths (an estimated 17 million deaths per year) are attributable to cardiovascular disease.2 An estimated 80 million (nearly one in three) Americans have cardiovascular disease, and nearly 8 million have a heart attack each year.1 Nearly 7 million cardiovascular procedures are performed annually in U.S. hospitals.1 In 2006, the total estimated direct and indirect costs associated with treatment of cardiovascular disease exceeded $400 billion.3 Primary prevention remains a national health priority. Cardiac rehabilitation is an important element of a comprehensive plan for secondary prevention of cardiovascular disease, which can reduce the age-adjusted cardiovascular mortality rate by nearly 50 percent.4
Definition
Cardiac rehabilitation was initially defined by the U.S. Public Health Service as a comprehensive long-term program “involving medical evaluation, prescribed
Cardiac Rehabilitationmark B. stephens
exercise, cardiac risk factor modification, education, and counseling.”5 These programs were specifically designed to “limit the physiologic and psychological effects of cardiac illness, reduce the risk for sudden death or reinfarction, control cardiac symptoms, stabilize or reverse the atherosclerotic process, and enhance the psychosocial and vocational status of selected patients.”5 The American Association of Cardiovascular and Pulmonary Rehabilitation and the American Heart Association (AHA) have refined the definition slightly, stating that, “cardiac rehabilitation refers to coordinated, multifaceted interventions designed to optimize a cardiac patient’s physical, psychological, and social functioning, in addition to stabilizing, slowing, or even reversing the progression of the underlying atherosclerotic processes, thereby reducing morbidity and mortality.”6
The overall principles of proper patient identification, enrolment in a cardiac rehabilitation program, comprehensive risk factor reduction, and longitudinal care are consistent with the principles of family medicine and with the modern concept of the medical home. The biopsychosocial model of health embedded within the core programmatic elements of structured cardiac rehabilitation lends itself well to holistic care. Family physicians are well suited to participate in and facilitate all of these domains of care, and many routinely include elements of risk factor reduction and nutrition
AbstrAct
An estimated 80 million (nearly one in three) Americans have cardiovascular disease, which is the leading cause of morbidity and mortality worldwide. In the United States alone, more than 850,000 deaths are attributed annually to cardiovascular disease, and more than 8 million Americans have had a heart attack. Nearly 7 million cardiovascular procedures are performed annually in U.S. hospitals. Cardiac rehabilitation is a comprehensive program of patient evaluation, risk factor reduction (e.g., lipid control, weight management), physical activity, and longitudinal care designed to reduce the effects of cardiovascular disease, and is an effective means of mitigating disease and disability. Family physicians incorporate many of the fundamental principles of comprehensive cardiac rehabilitation into their daily practices. However, the use of dedicated cardiac rehabilitation programs serves to further reinforce the principles of nutrition, physical activity, risk factor reduction, and wellness. Cardiac rehabilitation services are underused in the United States, even though there is evidence that structured programs improve quality of life and reduce mortality for patients with coronary artery disease and other select forms of cardiovascular disease.
keywords: Cardiovascular disease, dedicated cardiac rehabilitation programs
review article
Mark B. Stephens, CAPT, MC, USN, FAAFP, CAQAM, is an associate professor of family medicine at the Uniformed Services University of the Health Sciences in Bethesda, Md.Source: Adapted from Am Fam Physician 2009;80(9):955-9, 960.

review articlereview article
48 49Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
increase in cardiorespiratory endurance as measured by maximum oxygen consumption (VO2max).22-25 Patients with CHF who participated in cardiac rehabilitation also showed a significant reduction in mortality compared with control groups.23
There are limited trial data examining the impact of cardiac rehabilitation in patients who have had transplant or valvular surgery. One review indicated that cardiac rehabilitation improves VO2max by 50 percent in patients with a transplant.26 Patients undergoing cardiac rehabilitation following valve replacement surgery demonstrated a 25 percent increase in VO2max
27 and a 25 percent increase in functional capacity.28 Whether cardiac rehabilitation confers a survival benefit is not clear in this population.
components of A comprehensive cArDiAc rehAbilitAtion progrAm
Cardiac rehabilitation aims to restore patients with cardiovascular disease to a state of good health through the use of programs that incorporate regular exercise, with or without patient education or psychosocial support.10 Therefore, it is important to know how individual programs are structured when referring patients for cardiac rehabilitation. Most formal cardiac rehabilitation programs have several core components that work interchangeably to improve a patient’s
exercise performance, promote lifestyle changes, and increase psychosocial well-being.
A formal patient assessment should occur on enrolment to any cardiac rehabilitation program. This initial evaluation includes the patient history and physical examination, review of pertinent testing or intervention data, and risk stratification. Patients should then have an individualized program of secondary prevention designed to target their specific risk factor profile. These elements include nutrition counseling, weight management, tobacco cessation, physical activity counseling, and a targeted prescription for physical activity. Initially, most programs use supervised exercise to ensure that patients are properly performing the recommended activities and to screen for symptoms during exercise. Established program standards29 and performance measures30 are available to guide the implementation of cardiac rehabilitation services.
Traditionally, cardiac rehabilitation programs have been assigned phases of progression, depending on the patient’s diagnosis and referral source. Phase 1 occurs in association with hospitalization for an acute MI or other similar coronary event. During this time, the patient is exposed to supervised and structured early physical activity. Patient education, risk factor modification, and risk stratification using low-level graded exercise tolerance testing often take
table 2. Performance Measures for Cardiac Rehabilitation ProgramsPerformance measure target/goal Intervention Blood pressure control Normotension (< 140/90 mm Hg, or < 130/80 mm Hg
in patients with diabetes)Lifestyle modification; medication
Depression Assess for presence of depression Use of acceptable depression screening tool, with intervention as indicated
Diabetes control A1C < 7 percent Diabetes self-education, nutrition and weight management, and physical activity programming
Exercise capacity Assess symptom-limited exercise tolerance Exercise prescription tailored to each patientLipid control For patients with cardiovascular disease, low-density
lipoprotein level < 100 mg per dL (2.59 mmol per L)Lifestyle modification; medication
Physical activity 30 minutes per day, five days per week Physical activity programming tailored to individual needs and abilities
Preventive medications Adherence to preventive medications Age- and gender-appropriate preventive counseling and intervention
Tobacco use Abstinence or cessation Tobacco cessation program Weight management Body mass index of 18.5 to 24.9 kg per m2 and waist
circumference < 40 inches for men and < 35 inches for women
Multidisciplinary program of diet modification, physical activity programming, and psychosocial support
Information from references 29 and 31.
and physical activity counseling in their practices. The advantage of a formal cardiac rehabilitation program is that it specifically incorporates key elements of secondary prevention in a structured, graded, and codified manner.
cAnDiDAtes for cArDiAc rehAbilitAtion
Cardiac rehabilitation traditionally has been used following acute myocardial infarction (MI),7 but many other patients benefit from structured cardiac rehabilitation programs as well (Table 1).6 The Centers for Medicare and Medicaid Services also recognizes coronary artery bypass grafting (CABG) surgery, stable angina pectoris, percutaneous coronary intervention (PCI), heart valve repair or replacement, and heart transplantation as additional indications for formal cardiac rehabilitation.8 Evidence also supports cardiac rehabilitation for patients with heart failure.9 Currently, Medicare covers cardiac rehabilitation programs for up to three sessions per week for three months. Medicare reimbursement applies to patients with acute MI, CABG, stable angina pectoris, PCI, valvular surgery, and heart transplantation.8
eviDence for effectiveness
A comprehensive program of cardiac rehabilitation results in multiple positive outcomes for appropriately selected patients. Symptoms such as angina, dyspnea, and fatigue are reduced.10 Depressive symptoms following a major cardiac event also are reduced.11 Exercise performance and the ability to participate
in activities of daily living are increased.10 Quality of life and the ability to individually manage one’s own disease are improved.12 Rates of hospitalization and absence from work are also decreased.12
Multiple meta-analyses have been conducted to examine the effectiveness of cardiac rehabilitation in the setting of atherosclerotic coronary artery disease and MI.13-15 Pooled data from these meta-analyses indicate that patients who undergo comprehensive cardiac rehabilitation following MI have a 15 to 28 percent reduction in all-cause mortality (number needed to treat [NNT] = 4 to 6) and a 26 to 31 percent reduction in cardiac mortality (NNT = 3 to 4) when compared with patients who do not participate in a structured program. It is estimated that roughly 50 percent of the reduction in cardiac mortality is attributable to lifestyle changes and improvements in cardiovascular risk profiles.16 The American Heart Association and American College of Cardiology clinical practice guidelines recommend cardiac rehabilitation for patients following ST-elevation MI (STEMI) and non-STEMI.17,18
A Cochrane review of the evidence for a benefit of cardiac rehabilitation following MI was performed in 2001.10 Investigators examined data from 32 separate trials that met eligibility requirements. Overall, there was a 27 percent reduction in all-cause mortality for exercise-only cardiac rehabilitation programs compared with control programs. Exercise-only programs were found to be similar to comprehensive programs (i.e., programs that included tobacco cessation, psychosocial counseling, and other risk factor modifications) in terms of overall reduction in adverse clinical outcomes. Cardiac rehabilitation was shown to confer a morbidity and mortality benefit following MI, and is recommended for patients with chronic stable angina.19
The data supporting cardiac rehabilitation following CABG are less voluminous, but equally supportive. Patients who participated in a comprehensive cardiac rehabilitation program 10 years after having CABG had an 18 percent rate of cardiovascular events, compared with a 35 percent rate of cardiovascular events for patients who did not enter cardiac rehabilitation (NNT = 5.5).20 The American College of Cardiology and AHA guideline on CABG recommends cardiac rehabilitation for patients following CABG.21
Congestive heart failure (CHF) is another indication for cardiac rehabilitation. Patients with CHF enrolled in cardiac rehabilitation exhibited a 15 to 30 percent
table 1. Indications for Cardiac Rehabilitation Patients with a history of: Atherosclerotic coronary artery disease Acute coronary syndrome Myocardial infarction Coronary artery bypass grafting Percutaneous coronary intervention Stable angina pectorisAtherosclerotic peripheral vascular disease Peripheral arterial diseaseHeart transplantationStable congestive heart failureValvular surgeryVentricular assist devices
Information from reference 6.
review articlereview article
50 51Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
9. Rees K, Taylor RS, Singh S, Coats AJ, Ebrahim S. Exercise based rehabilitation for heart failure. Cochrane Database Syst Rev. 2004;(3):CD003331.
10. Jolliffe JA, Rees K, Taylor RS, Thompson D, Oldridge N, Ebrahim S. Exercise-based rehabilitation for coronary heart disease. Cochrane Database Syst Rev. 2001;(1):CD001800.
11. Milani RV, Lavie CJ. Impact of cardiac rehabilitation on depression and its associated mortality. Am J Med. 2007;120(9):799-806.
12. Clark AM, Hartling L, Vandermeer B, McAlister FA. Meta-analysis: secondary prevention programs for patients with coronary artery disease. Ann Intern Med. 2005;143(9): 659-672.
13. Oldridge NB, Guyatt GH, Fischer ME, Rimm AA. Cardiac rehabilitation after myocardial infarction. Combined experience of randomized clinical trials. JAMA. 1988;260(7):945-950.
14. O’Connor GT, Buring JE, Yusuf S, et al. An overview of randomized trials of rehabilitation with exercise after myocardial infarction. Circulation. 1989;80(2):234-244.
15. Taylor RS, Brown A, Ebrahim S, et al. Exercise-based rehabilitation for patients with coronary heart disease: systematic review and meta-analysis of randomized controlled trials. Am J Med. 2004;116(10):682-692.
16. Taylor RS, Unal B, Critchley JA, Capewell S. Mortality reductions in patients receiving exercise-based cardiac rehabilitation: how much can be attributed to cardiovascular risk factor improvements? Eur J Cardiovasc Prev Rehabil. 2006;13(3):369-374.
17. Antman EM, Anbe DT, Armstrong PW, et al. ACC/AHA guidelines for the management of patients with ST-elevation myocardial infarction—executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 1999 Guidelines for the Management of Patients with Acute Myocardial Infarction) [published correction appears in Circulation. 2005;111(15):2013]. Circulation. 2004; 110 (5):588-636.
18. Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non-ST-Elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction) developed in collaboration with the American College of Emergency Physicians, the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine [published correction appears in J Am Coll Card. 2008;51(9):974]. J Am Coll Card. 2007;50(7):e1-e157.
19. Gibbons RJ, Abrams J, Chatterjee K, et al. ACC/AHA 2002 guideline update for the management of patients with chronic stable angina—summary article: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on the Management of Patients With Chronic Stable Angina). Circulation. 2003;107(1):149-158.
20. Hedbäck B, Perk J, Hörnblad M, Ohlsson U. Cardiac rehabilitation after coronary artery bypass surgery: 10-year results on mortality, morbidity and readmissions to hospital. J Cardiovasc Risk. 2001;8(3):153-158.
21. Eagle KA, Guyton RA, Davidoff R, et al. ACC/AHA 2004 guideline update for coronary artery bypass graft surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee to Update the 1999 Guidelines for Coronary Artery Bypass Graft Surgery) [published correction appears in Circulation. 2005;111(15):2014]. Circulation. 2004;110(14):e340-e437. http://www.acc.org/qualityandscience/clinical/guidelines/cabg/index_rev.pdf. Accessed August 13, 2009.
22. Hambrecht R, Gielen S, Linke A, et al. Effects of exercise training on left ventricular function and peripheral resistance in patients with chronic heart failure: A randomized trial. JAMA. 2000;283(23):3095-3101.
23. Piepoli MF, Davos C, Francis DP, Coats AJ, for the ExTraMATCH Collaborative. Exercise training meta-analysis of trials in patients with chronic heart failure (ExTraMATCH). BMJ. 2004;328(7433):189-198.
24. McKelvie RS, Teo KK, Roberts R, et al. Effects of exercise training in patients with heart failure: the Exercise Rehabilitation Trial (EXERT). Am Heart J. 2002;144(1): 23-30.
25. Smart N, Marwick TH. Exercise training for patients with heart failure: a systematic review of factors that improve mortality and morbidity. Am J Med. 2004;116(10): 693-706.
26. Kobashigawa JA, Leaf DA, Lee N, et al. A controlled trial of exercise rehabilitation after heart transplantation [published correction appears in N Engl J Med. 1999;340(12):976]. N Engl J Med. 1999;340(4): 272-277.
27. Jairath N, Salerno T, Chapman J, Dornan J, Weisel R. The effect of moderate exercise training on oxygen uptake post-aortic/mitral valve surgery. J Cardiopulm Rehabil. 1995;15(6):424-430.
28. Habel-Verge C, Landry F, Desaulniers D, et al. Physical fitness improves after mitral valve replacement. CMAJ. 1987;136(2):142-147.
29. King ML, Williams MA, Fletcher GF, et al. Medical director responsibilities for outpatient cardiac rehabilitation/secondary prevention programs: a scientific statement from the American Heart Association/American Association for Cardiovascular and Pulmonary Rehabilitation. Circulation. 2005;112(21):3354-3360.
place during the hospitalization. Phase 2 is the early outpatient phase of cardiac rehabilitation. During this period, which occurs after discharge from the hospital, patients participate in a supervised program of physical activity, nutrition counseling, risk factor modification, and psychosocial support. Programs based in the patient’s home, an outpatient clinic, or a wing of the hospital or community center can be designed to enhance patient adherence. Performance measures for cardiac rehabilitation programs are available (Table 2).29,31 The third phase (late outpatient) aims to maintain lifestyle changes established in phases 1 and 2. During phase 3, there are periodic reassessments of patient symptoms, risk factors, medication use, and psychosocial support. Phases 2 and 3 represent elements of secondary prevention and are the major focus of cardiac rehabilitation.
finAl comments
Despite the apparent benefits of cardiac rehabilitation in multiple populations of patients with cardiovascular disease, these programs remain largely underused. In the United States, Medicare data indicate that cardiac rehabilitation services are used by 14 percent of eligible patients following hospitalization for acute MI and 31 percent of eligible patients following CABG surgery.32 Data from the United Kingdom are similar.33
Many factors contribute to the underuse of cardiac rehabilitation programs. The most commonly cited barriers include distance from the program facility; transportation; low patient self-esteem; and lack of physician referral, perceived benefit, and social support.34 Additionally, once enrolled in a cardiac program, many patients drop out. Factors associated with nonadherence include older age, female sex, and lower premorbid levels of physical activity.34 Recognizing that cardiac rehabilitation programs are underused, that many patients fail to complete the programs, and that other patients fail to sustain lifestyle changes after program completion, the Cochrane Database of Systematic Reviews recently reviewed the available medical literature to provide evidence-based recommendations regarding use of and adherence to such programs.35
Family physicians have an important role as the central coordinating figures in the medical home. This role includes promoting cardiovascular wellness through routine provision of primary and secondary preventive services; identifying patients who would benefit from a structured cardiac rehabilitation program and helping them to enrol; encouraging current participants to
complete the program; and providing longitudinal follow-up for patients after program completion. Family physicians also play a key role in managing all three phases of cardiac rehabilitation by representing a critical aspect of patient continuity. By knowing which cardiac rehabilitation resources are available within the local community (http://www.aacvpr.org/Resources/SearchableCertifiedProgramDirectory/tabid/113/Default.aspx) and providing continuity of care, preventive counseling services, and a medical home for patients with cardiovascular disease, family physicians can help improve these patients’ quality of life while reducing morbidity and mortality.36
references
1. Lloyd-Jones D, Adams R, Carnethon M, et al. Heart disease and stroke statistics—2009 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee [published correction appears in Circulation. 2009;119(3):e182]. Circulation. 2009;119(3):e21-e181.
2. McKay J, Mensah GA. The Atlas of Heart Disease and Stroke. Geneva, Switzerland: World Health Organization; 2004.
3. Thom T, Haase N, Rosamond W, et al. Heart disease and stroke statistics—2006 update: a report from the American Heart Association Statistics Committee and Stroke Statistics Subcommittee [published corrections appear in Circulation. 2006;113(14):e696, and Circulation. 2006;114(23):e630]. Circulation. 2006;113(6):e85-e151.
4. Ford ES, Ajani UA, Croft JB, et al. Explaining the decrease in U.S. deaths from coronary disease, 1980-2000. N Engl J Med. 2007;356(23):2388-2398.
5. Wenger NK. Cardiac rehabilitation. Clinical practice guideline, no. 17. Rockville, Md.: U.S. Department of Health and Human Services, Public Health Service, Agency for Health Care Policy and Research; 1995.
6. Leon AS, Franklin BA, Costa F, et al. Cardiac rehabilitation and secondary prevention of coronary heart disease: an American Heart Association scientific statement from the Council on Clinical Cardiology (Subcommittee on Exercise, Cardiac Rehabilitation, and Prevention) and the Council on Nutrition, Physical Activity, and Metabolism (Subcommittee on Physical Activity), in collaboration with the American Association of Cardiovascular and Pulmonary Rehabilitation [published correction appears in Circulation. 2005;111(13):1717]. Circulation. 2005;111(3):369-376.
7. Wenger NK. Current status of cardiac rehabilitation. J Am Coll Cardiol. 2008;51(17):1619-1631.
8. Centers for Medicare and Medicaid Services. Decision memo for cardiac rehabilitation programs (CAG-00089R). http://www.cms.hhs.gov/mcd/viewdecisionmemo.asp?id=164. Accessed August 13, 2009.

53Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
review ArtiCle
52 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
Since, the introduction of the concept of metabolic syndrome (MetS), a relatively enormous amount of new information has evolved relevant to the role
of insulin resistance in human disease. Abnormalities related to insulin resistance have broadened considerably and the adverse clinical outcomes extend beyond type 2 diabetes and cardiovascular disease (CVD). The MetS is a cluster of metabolic abnormalities that includes insulin resistance, dyslipidemia, hypertension, a proinflammatory state and excess weight, particularly abdominal adiposity. Individuals with MetS are at increased risk for diabetes and CVD and at increased risk of mortality from CVD.1 Because inflammatory and thrombotic tendencies are part of this syndrome, the clinical outcome of foremost significance is atherosclerotic CVD.2 Adult Treatment Panel III (ATP III) of National Cholesterol Education Program (NCEP) recognized the importance of CVD risk factors of what they referred to as a “constellation of lipid and nonlipid
Study of Association between Metabolic Syndrome and Acute Coronary Syndromevirendra dhakhada*, madhu panjwani**, ajay daBhi**
AbstrAct
Aims: To ascertain the prevalence of metabolic syndrome (MetS) in patients with acute coronary syndrome (ACS) to study the impact of MetS on hospital outcomes and to find out association of each components of MetS with ACS. Study design: Hospital-based prospective cross-sectional study. Method: The study was conducted in 100 patients of ACS (ST-elevation MI [STEMI], non-STEMI, unstable angina) admitted in Sir Takhtsinhji Hospital, Bhavnagar. Patients having MetS were identified according to International Diabetes Federation (IDF) criteria. After detailed clinical evaluation and relevant investigations, correlation between MetS and ACS was explored. Results: Prevalence of MetS was 59% in ACS patients. Prevalence was higher in males (59.7%) compared to females (57.14%). Maximum numbers of patients with MetS were in age of 51-60 years. Among all parameters of MetS, positive predictive value was highest for high blood pressure (BP) followed by triglyceride (TG) level, fasting blood sugar (FBS), respectively. Conclusion: Prevalence of MetS was found more often after the age of 40 years more often commonly in males. High BP was found as a most prevalent parameter in the criteria for MetS.
keywords: Metabolic syndrome, acute coronary syndrome
risk factors of metabolic origin”, designated this cluster as the MetS and stated, “This syndrome is closely related to insulin resistance.”3 The primary goal of the ATP III in establishing criteria for making the diagnosis of the MetS is to identify individuals at increased CVD risk and initiate lifestyle changes to decrease this risk. Though both ATP III and International Diabetes Federation (IDF) have almost similar criteria for diagnosis of MetS, IDF criteria differ from ATP III in waist circumference, which is an essential criteria in IDF and also cut-off limit for waist circumference is different in different races.
mAteriAl AnD methoDs
A cross-sectional study was carried out in 100 patients of ACS (ST-elevation myocardial infarction [STEMI], non ST segment elevation MI [NSTEMI], unstable angina) admitted in Sir Takhtsinhji Hospital, Bhavnagar during the year 2010-2011. IDF criteria were used for diagnosis of MetS among these all patients. The IDF criteria for diagnosing MetS are described in Table 1.4
A detailed medical history of the patients including symptomatology, details of past illnesses, occupation, illnesses in the family, any particular habits and other morbid illness obtained. Complete physical examination
*Senior Resident**Associate Professor, Dept. of MedicineMedical College and Sir Takhtsinhji Hospital, Bhavnagar, Gujarataddress for correspondenceDr Virendra DhakhadaPlot No.: 385/244, Shyam Vandana Sagwadi, Kaliyabid, Bhavnagar - 364 001, GujaratE-mail: [email protected]
original article
30. Thomas RJ, King M, Lui K, Oldridge N, Piňa IL, Spertus J, for the ACC/AHA Task Force Members. AACVPR/ACC/AHA 2007 performance measures on cardiac rehabilitation for referral to and delivery of cardiac rehabilitation/secondary prevention services. J Cardiopulm Rehabil Prev. 2007;27(5):260-290.
31. Balady GJ, Williams MA, Ades PA, et al. Core components of cardiac rehabilitation/secondary prevention programs: 2007 update: a scientific statement from the American Heart Association Exercise, Cardiac Rehabilitation, and Prevention Committee, the Council on Clinical Cardiology; the Councils on Cardiovascular Nursing, Epidemiology and Prevention, and Nutrition, Physical Activity, and Metabolism; and the American Association of Cardiovascular and Pulmonary Rehabilitation. Circulation. 2007;115(20):2675-2682.
32. Suaya JA, Shepard DS, Normand SL, Ades PA, Prottas J, Stason WB. Use of cardiac rehabilitation by Medicare
beneficiaries after myocardial infarction or coronary bypass surgery. Circulation. 2007;116(15):1653-1662.
33. Beswick AD, Rees K, Griebsch I, et al. Provision, uptake and cost of cardiac rehabilitation programmes: improving services to under-represented groups. Health Technol Assess. 2004;8(41):iii-iv,ix-x, 1-152.
34. Daly J, Sindone AP, Thompson DR, Hancock K, Chang E, Davidson P. Barriers to participation in and adherence to cardiac rehabilitation programs: a critical literature review. Prog Cardiovasc Nurs. 2002;17(1):8-17.
35. Davies P, Taylor F, Beswick A, Harris-Wise F, Moxham T, Taylor RS. Promoting patient uptake and adherence in cardiac rehabilitation. Cochrane Database Syst Rev. 2008;(2):CD007131.
36. Williams MA, Ades PA, Hamm LF, et al. Clinical evidence for a health benefit from cardiac rehabilitation: an update. Am Heart J. 2006;152(5):835-841.

Original articleOriginal article
54 55Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
ACS patients. Prevalence was higher in males (59.7%) compared to females (57.14%) (Table 2). The maximum numbers of patients were in 51-60 years of age (Fig. 1). The prevalence of each component of MetS is shown in Figure 2. Clinical characteristics in both groups are described in Table 3.
Among all parameters, positive predictive value was highest for high blood pressure (BP) followed by triglycerides (TG) and fasting blood sugar (FBS). As waist circumference is an essential IDF criteria for MetS, positive predictive value could not be obtained.
Discussion
Although NCEP-ATP III criteria is widely used in studies related with MetS, we have used IDF criteria mainly because looking at Asian phenotype of obesity, we could underestimate many patients with MetS by applying ATP III criteria. Analysis of data from the Framingham Heart Study and Bogalusa Heart Study also suggested that increase in central fat antedates the development of coronary heart disease, atherosclerosis and related disorders.5 Ramachandran et al6 have also modified ATP III guideline in urban Asian adults with use of modified waist circumference appropriate for Indian population (male >90 cm, female >80 cm). Three meta-analyses found that the MetS increases the risk for incident coronary artery disease (CAD).7-9 In our study, most patients of ACS who had MetS were >40 years and maximum were in age group of 51-60 years. The Jaipur Heart Watch study10 and third NHANES study11 show similar results. Prevalence of MetS was higher in males (59.7%) as compared to females (57.14%), which is similar with study done by Gandhi et al.12 Study done by Gupta et al13 and
Figure 2. Prevalence of each component of MetS.
Ramachandran et al6 showed higher prevalence of MetS in females. The higher prevalence in our study may be due to other coronary risk factors in males as we have selected all patients of ACS for this study. In both the study groups, regarding the components of MetS, difference in waist circumference, high BP, TG and FBS was statistically significant with p < 0.05. In our study, we found highest positive predictive value for high BP followed by serum TG and FBS. The common presentation of ACS in both these groups was STEMI (59.32% in MS group and 65.85% in NMS group). The observed difference in mortality in both groups was statistically found to be insignificant though this could have been due to small sample size, which is similar to finding in study done by Pandey et al.14 Primary prevention of MetS through weight management and lifestyle modification will help us in preventing global burden of CVDs.
references
1. Braunwald’s Heart Disease: A Textbook of Cardiovascular Medicine. 8th edition, Libby, Bonow, Mann, Zipes (Eds.), Saunders, 2007.
2. Contemporary Diagnosis and Management of the Metabolic Syndrome. Grundy SM (Ed.), 1st edition, Handbooks in Health Care Company, 2005:p.13.
3. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA 2001;285(19):2486-97.
4. Harrison’s Principles of Internal Medicine. Fauci, Braunwald, Kasper, Hauser, Longo, Jameson, Loscalzo (Eds.), 17th edition, McGraw-Hill, 2008.
MS
NMS
70
60
50
40
30
20
10
0
Num
ber o
f pat
ient
s
59
3339
7
39
10
58
33 31
17
Waist circumference
High blood pressure
Triglyceride Fasting blood sugar
High-density lipoprotein
and systemic examination were performed.
Each patient’s anthropometrical measurements were obtained with emphasis on measurement of height, weight, waist circumference, hip circumference, body mass index (BMI). Waist circumference was measured as per National Health and Nutrition Examination Survey (NHANES) protocol: In upright position, the right iliac crest of the patient was palpated and a horizontal mark was drawn just above the lateral border of it. It was crossed with a vertical mark in the midaxillary line. The measuring tape was placed around the abdomen at this level parallel to the floor and waist circumference was measured at normal minimal inspiration without compressing skin.
Patients were diagnosed as having acute coronary syndrome (ACS)-based on ECG and cardiac biomarkers. Routine investigations including complete blood count, urine examination, renal function test, random blood sugar level were done along with fasting blood sugar, lipid profile and chest X-ray. Echocardiography, ultrasonography, CT head were done as and when required. After history and complete examination and investigations, correlation between MetS and ACS were studied. Data was entered and analyzed in SPSS software.
results
Patients were divided in two groups: MS group: MetS with ACS; NMS group: ACS only without MetS. In our study, we found 59% prevalence of MetS in
table 1. IDF Criteria for Central Adiposity4
waist circumference Men women Ethnicity ≥94 cm ≥80 cm Europid, Sub-Saharan
African, Eastern and Middle Eastern
≥90 cm ≥80 cm South Asian, Chinese and ethnic South and
Central American≥85 cm ≥90 cm JapaneseTwo or more of the following:
z Fasting TGs >150 mg/dl or specific medication z HDL cholesterol <40 mg/dl and <50 mg/dl for men and
women, respectively or specific medication z BP >130 systolic or >85 mm diastolic or previous diagnosis
or specific medication z Fasting plasma glucose ≥100 mg/dl or previously
diagnosed type 2 diabetes
table 2. Prevalence of MetS according to GenderPresentation Male Female total
No % No % No/%ACS only (NMS) 29 40.27 12 42.85 41ACS + MetS (MS) 43 59.7 16 57.14 59total 72 100 28 100 100
Age group (years)
Figure 1. Age distribution.
table 3. Clinical Characteristics in Study GroupsCharacteristics MS group
ACS + MetS (n = 59)
NMS groupACS without MetS, (n = 41)
p value
Age (years) 56.76 (mean) 57.61 (mean) NSSex Male 43 29
NS Female 16 12Tobacco 19 17 NSSmoking 30 18 NSAlcohol 05 01 NSSedentary lifestyle
41 21 NS
PresentationSTEMI 35 27 NSNon-STEMI 15 06 NSUnstable angina
09 08 NS
Components of MetSWaist circumference
59 33 p < 0.05
High BP 39 07 p < 0.05High TG 39 10 p < 0.05Elevated FBS 58 33 p < 0.05Low HDL 31 17 NSMortality 02 01 NS
MS
NMS
<40 41-50 51-60 61-70 >71
20
15
10
5
0
Num
ber o
f pat
ient
s

57Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
OriginAl ArtiCle
56 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
Study of Cardiac Manifestations of HIV/AIDS and their Correlation with CD4+ T-cell Countanjum parvez*, mohammad asif**, luBna zafar†, asif hasan,* hs khan‡
AbstrAct
Human immunodeficiency virus (HIV), which belongs to the family of retroviridae and subfamily lentivirinae, is the causative agent of acquired immunodeficiency syndrome (AIDS). Initially, the prognosis of the patients was deemed to be dismal but with the introduction of highly-active antiretroviral therapy (HAART), the morbidity and mortality of the patients has decreased drastically. The patients survive to 40-50 years and may suffer from cardiac ailments either de novo or as a consequence of infection, malignancy or treatment itself. We conducted an observational study on 60 patients with HIV/AIDS, with the aim to detect the prevalence of cardiac diseases in this population and correlate them with CD4+ T-cell count. None of the patients had pre-existing cardiac ailment. Eight patients had echocardiographic evidence of cardiac involvement. Four had pericardial effusion, two had dilated cardiomyopathy, one pulmonary hypertension and one had mild left ventricular dysfunction. Five out of eight patients with cardiac involvement had CD4+ T-cell count <100/µl.
keywords: CD4+ T-cell, HAART, pericardial effusion, dilated cardiomyopathy
clinical study
*Associate Professor**Junior Resident†Assistant Professor‡ Professor Dept. of Medicine, Jawaharlal Nehru Medical College, AMU, Aligarhaddress for correspondenceDr Anjum ParvezD-7, Abdullah Apartment, Near Abdullah Girl’s CollegeCivil Lines, Aligarh - 202 002E-mail: [email protected]
Human immunodeficiency virus (HIV) belongs to the family retroviridae and subfamily lenti-virinae. HIV causes acquired immunodeficiency
syndrome (AIDS). By definition, any HIV-infected individual with a CD4+ T-cell count of <200/µl has AIDS, regardless of the presence of symptoms or opportunistic diseases. In the mid 1990s, the advent of combination highly-active antiretroviral therapy (HAART) made a major impact on the morbidity and mortality of HIV patients. Survival to 40-50 years is no longer unusual and coronary artery disease (CAD), either de novo or as an iatrogenic consequence of newer treatment regimens, is emerging as an important problem. Recent studies report increased rates of coronary events in HIV patients or in HIV patients receiving HAART.1 Studies have suggested that HIV may exhibit a cardiac tropism, but the heart may also be affected by other opportunistic viruses, fungi and protozoa. Cardiac diseases associated with HIV may
therefore be multifactorial, and can be caused by infection or neoplastic complications or their treatment, any of the established causes of cardiac disease in other patient population, or by the HIV infection of the myocardium itself.2 Hence, the knowledge of the relative frequency of each form of heart disease in patients of HIV is constantly evolving.
Aims of stuDY
 To evaluate the prevalence of cardiac diseases in patients of HIV/AIDS.
 To find out correlation of various cardiac diseases with CD4+ T-cell count.
mAteriAl AnD methoDs
This observational study included 60 patients of diagnosed HIV/AIDS attending ART center, Medicine OPD and inpatients admitted in Medicine wards, Jawaharlal Nehru Medical College Hospital, AMU, Aligarh. The HIV serology of the study population was done by double enzyme-linked immunosorbent assay (ELISA) using microwell ELISA test at the Dept. of Microbiology, Jawaharlal Nehru Medical College, AMU, Aligarh. If ELISA was positive initially, it was repeated twice to confirm HIV seropositive state.
All patients were subjected to detailed history along with physical examination, especially cardiovascular
5. Burke GL, Webber LS, Srinivasan SR, Radhakrishna-murthy B, Freedman DS, Berenson GS. Fasting plasma glucose and insulin levels and their relationship to cardiovascular risk factors in children: Bogalusa Heart Study. Metabolism 1986;35(5):441-6.
6. Ramachandran A, Snehalatha C, Satyavani K, Sivasankari S, Vijay V. Metabolic syndrome in urban Asian Indian adults - a population study using modified ATP III criteria. Diabetes Res Clin Pract 2003;60(3):199-204.
7. Ford ES. Risks for all-cause mortality, cardiovascular disease, and diabetes associated with the metabolic syndrome: a summary of the evidence. Diabetes Care 2005;28(7):1769-78.
8. Galassi A, Reynolds K, He J. Metabolic syndrome and risk of cardiovascular disease: a meta-analysis. Am J Med 2006;119(10):812-9.
9. Gami AS, Witt BJ, Howard DE, Erwin PJ, Gami LA, Somers VK, et al. Metabolic syndrome and risk of incident cardiovascular events and death: a systematic review and meta-analysis of longitudinal studies. J Am Coll Cardiol 2007;49(4):403-14.
10. Gupta R, Sarna M, Thanvi J, Rastogi P, Kaul V, Gupta VP. High prevalence of multiple coronary risk factors in Punjabi Bhatia community: Jaipur Heart Watch-3. Indian Heart J 2004;56(6):646-52.
11. Park YW, Zhu S, Palaniappan L, Heshka S, Carnethon MR, Heymsfield SB. The metabolic syndrome: prevalence and associated risk factor findings in the US population from the Third National Health and Nutrition Examination Survey, 1988-1994. Arch Intern Med 2003;163(4):427-36.
12. Gandhi AU, et al. Study of patients with metabolic syndrome and its association with end-organ damage. Ind J Clin Prac 2011;22(6).
13. Gupta A, Gupta R, Sarna M, Rastogi S, Gupta VP, Kothari K. Prevalence of diabetes, impaired fasting glucose and insulin resistance syndrome in an urban Indian population. Diabetes Res Clin Pract 2003;61(1):69-76.
14. Pandey S, Baral N, Majhi S, Acharya P, Karki P, Shrestha S, et al. Prevalence of the metabolic syndrome in acute myocardial infarction and its impact on hospital outcomes. Int J Diabetes Dev Ctries 2009;29(2):52-5.

CliniCal StudyCliniCal Study
58 59Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
the 60 patients enrolled in our study, pericardial disease was observed in four (6.7%) patients; of these, three patients had moderate pericardial effusion. Studies done by Cordoso et al3 showed that 41% of their patients had minimal asymptomatic pericardial effusion, 13% had moderate-to-severe pericardial effusion and 0.5% had acute pericarditis. In our study, one patient with severe pericardial effusion had evidence of cardiac tamponade on echocardiogram. The analysis of pericardial fluid showed lymphocytic exudative effusion probably of tuberculous etiology.
The patient’s CD4+ T-cell count was 79/µl. Studies by Steigman et al4 and Karve et al5 reported that cardiac tamponade in HIV/AIDS patients is usually associated with Kaposi’s sarcoma and tuberculous pericarditis. The studies conducted by Rerkpattanapipat et al6 showed that small asymptomatic pericardial effusion do not require diagnostic evaluation and spontaneously resolve in upto 42% of the patients. Rerkpattanapipat et al6 and Heideneich et al7 showed that pericardial disease in HIV infection is often associated with shortened survival, independent of CD4+ T-cell count.
In our study, three (5%) patients had involvement of myocardium of which two had dilated cardiomyopathy and one patient had mild LV dysfunction. Rerkpattanapipat et al6 showed that HIV was the underlying cause in 4% of their patients with dilated cardiomyopathy. Milei et al8 reported that dilated cardiomyopathy affected 10-20% of HIV-infected patients and accounted for approximately a third of HIV-related deaths. Herskowitz et al,9 in another study, showed that global left ventricular dysfunction was detected in 15% of randomly selected HIV patients. In our study, two (3.3%) patients had global hypokinesia with ejection fraction 25-35%. Both had symptoms of congestive heart failure and opportunistic infections like oropharyngeal candidiasis.
The CD4+ T-cell count of dilated cardiomyopathy patients was between 50-150/µl in our study. Chariot et al10 showed higher frequency of dilated cardio-myopathy in patients with CD4+ T-cell count <100/µl indicating an association between the degree of immunosuppression and the development of cardiomyopathy. Apart from immunosuppression, selenium deficiency has been identified as a cause of heart muscle disease by Rerkpattanapipat et al.6 Lipshultz et al11 showed that heart failure and left ventricular dysfunction were markers of dismal prognosis.
None of the patients in our study had evidence of infective endocarditis. Barbaro et al12 showed that bacterial endocarditis in HIV is infrequent and is seen almost exclusively in intravenous drug users with prevalence of 6.3-34%. The low prevalence of endocardial involvement observed may be attributed to the low prevalence of intravenous drug users in our study. Pulmonary hypertension was noted in only in one patient in our study. The CD4+ T-cell count was 89/µl.
The study by Sitbon et al13 showed that endothelin receptor antagonist, bosentan, improved exercise tolerance and hemodynamic measurements in HIV patients. The effects of HAART on pulmonary hypertension are unknown and further studies are needed to prove its effectiveness. Recent reports from the Swiss Cohort Study by Zuber et al14 showed a decrease in pulmonary artery pressure with HAART.
conclusion
The presentation of HIV-infected individual is dominated by opportunistic infections and neoplastic complications. Our study specifically focused on the cardiac involvement in HIV/AIDS patients. The prevalence of cardiac disease as evidenced by echocardiography was 13.3% in the present study; of these, pericardial involvement constituted the majority. All of these patients had CD4+ T-cell count <300/µl. Since, the patients may be asymptomatic in the early stages of cardiac involvement and conversely the symptoms of respiratory disease and anemia may mimic heart disease, periodic echocardiographic evaluation is called for in HIV/AIDS patients. Early diagnosis and treatment of cardiac lesions may improve the quality-of-life as well as longevity of HIV infected individuals.
references
1. Holmberg SD, Moorman AC, Williamson JM, Tong TC, Ward DJ, Wood KC, et al; HIV Outpatient Study (HOPS) investigators. Protease inhibitors and cardiovascular outcomes in patients with HIV-1. Lancet 2002;360(9347):1747-8.
2. Yunis NA, Stone VE. Cardiac manifestations of HIV/AIDS: a review of disease spectrum and clinical management. J Acquir Immune Defic Syndr Hum Retrovirol 1998;18(2):145-54.
3. Silva-Cardoso J, Moura B, Martins L, Mota-Miranda A, Rocha-Gonçalves F, Lecour H. Pericardial involvement in human immunodeficiency virus infection. Chest 1999;115(2):418-22.
system examination. Apart from routine investigations like complete blood count (CBC), blood sugar, renal function tests (RFT), liver function tests (LFT), lipid profile, chest X-ray and ECG, all patients were subjected to 2D, M mode and color Doppler echo. CD4+ T-cell count was done by CD4 easy count kit-based on Flow Cytometry method, at ART center, Jawaharlal Nehru Medical College, AMU, Aligarh.
exclusion criteria
Patients with pre-existing cardiac illnesses like CAD, cardiomyopathy, rheumatic heart disease, congenital heart disease, chronic obstructive pulmonary disease (COPD) - cor pulmonale and diabetes mellitus were excluded from the study.
observAtions
Out of the total 60 patients, 14 (23.3%) were females and 46 (76.7%) were males (Table 1). The mean age of the patients at presentation was 37.05 ± 9.70 years. Of the 60 patients 42 (70%) were married, seven (11.6%) were widowed, four (6.6%) were single and seven (11.6%) were divorced or separated. Heterosexual contact was the probable mode of transmission of HIV in 53 (88.3%) patients in the study group. Injection drug use accounted for transmission in five (8.3%) of the patients. Blood transfusion, homosexual and iatrogenic route accounted for transmission in four (6.6%), two (3.3%) and one (1.6%) patients, respectively. The mode of transmission was not known in three (5%) cases (Table 2). All the 60 patients underwent 2D echo out of which eight (13.3%) demonstrated significant cardiac pathology. Pericardial effusion was present in four (6.7%) patients, followed by dilated cardiomyopathy in two (3.3%), pulmonary hypertension in one (1.6%) and left ventricular dysfunction in one (1.6%) cases (Table 3). Out of 60 patients, five showed abnormal echocardiographic findings with CD4+ T-cell count <100/µl, of which three (5%) had pericardial effusion, one (1.6%) had dilated cardiomyopathy and one (1.6%) had pulmonary hypertension. Two (3.3%) cases showed abnormal echocardiographic findings with CD4+ T-cell count 100-200/µl, of which one (1.6%) had pericardial effusion and one (1.6%) had dilated cardiomyopathy. In group with CD4+ T-cell count 200-500/µl only one (1.6%) patient had mild LV dysfunction (Table 4).
Discussion
Cardiac manifestations of HIV/AIDS have not gained much attention because the clinical picture is dominated by opportunistic infections and malignancies. Out of
table 1. Age at Presentation and Gender DistributionAge group (years)
Number of patients Percentage (%)Males Females total
15-25 3 0 3 5
26-35 19 5 24 40
36-45 10 9 19 31.6
46-55 9 0 9 15
≤56 5 0 5 8.3
total 46 14 60 100
table 2. Modes of Transmission of HIVMode of transmission
Male Female total Percentage (%)
Heterosexual 42 11 53 88.3
Homosexual 2 0 2 3.3
Blood transfusion
1 3 4 6.6
IV drug abuse 5 0 5 8.3
Iatrogenic 1 0 1 1.6
Unknown 3 0 3 5
table 3. Echocardiographic Findings in HIV/AIDS PatientsEchocardiographic findings
No. of patients Percentage (%)
Pericardial effusion 4 6.7
Dilated cardiomyopathy
2 3.3
Pulmonary hypertension
1 1.6
Mild LV dysfunction 1 1.6
total 8 13.3
table 4. Correlation of Echocardiographic Findings with CD4+ T-cell CountEchocardiographic findings
CD4+ t-cell count<100 100-200 201-500
Pericardial effusion 3 1 0
Dilated cardiomyopathy 1 1 0
Mild LV dysfunction 0 0 1
Pulmonary hypertension 1 0 0
total 5 2 1

61Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
CliniCAl Study
60 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
Myxomas are usually benign tumors of the heart and their most common site of presentation is left atrial septal region. These can be solitary or
multiple (usually familial) and present more commonly in females. Patients can present with episodes of embolic infarcts, Raynaud’s phenomenon and symptomatology can mimic those of severe mitral stenosis. These tumors respond very well to curative excision and do not usually recur unless they are part of familial syndromes.
cAse report
A 48-year-nondiabetic, nonhypertensive, nonsmoker gentleman presented with 2-year history of shortness of breath, exertional chest pain and exertional dizziness. Breathlessness had increased to NYHA Class III/IV at the time of presentation with history of pedal edema, congested neck veins and history of paroxsysmal nocturnal dyspnea since one month. There was no history of postural aggravation of his symptoms or of syncope.
AbstrAct
Myxomas are usually benign tumors of the heart and their most common site of presentation is left atrial septal region. 2D transthoracic or transesophageal echocardiography is useful in the diagnosis of cardiac myxoma and allows determination of site of tumor attachment and tumor size, which are important considerations in planning of surgical excision.
keywords: Atrial myxoma, embolic infarcts, tumor plop
On examination, patient was of normal built, afebrile, pulse rate was 100/min (normal volume, regular), blood pressure was 110/76 mmHg, jugular venous pressure (JVP) was not raised, 6 cm congestive hepatomegaly was seen with pitting pedal edema. On examination of cardiovascular system, S1 was normal, P2 component of S2 was loud, S3, S4 was not heard and there was a short mid-diastolic murmur which did not radiate and there was no positional variation of the murmur. No additional sounds were heard. Examination of chest revealed fine basilar crepitations.
On investigation, his hemogram showed normochromic, normocytic anemia, normal erythrocyte sedimentation rate (ESR) with normal reticulocyte count and hemoglobin of 9 g/dl. Blood biochemistry was within normal limits. ECG revealed a normal sinus rhythm with evidence of left atrial enlargement. Chest X-ray PA view revealed normal cardiac silhouette with mild pulmonary plethora. Two-dimensional (2D) echocardiography revealed 55 × 26 mm mass attached to left atrial septum and protruding into mitral valve orifice resulting in severe left inflow obstruction with mean diastolic gradient across the valve of 20 mmHg. Mild tricuspid regurgitation (TR) was seen with TR gradient of 76 mmHg. There was no mitral regurgitation or evidence of rheumatic activity on any of the valves. His left ventricle systolic function was within normal limits. Rest of the echocardiographic findings were within normal limits.
A diagnosis of left atrial myxoma with severe pulmonary venous hypertension with severe pulmonary arterial hypertension with congestive heart failure was
case report
Left Atrial Myxoma Presenting as Severe Pulmonary Hypertensiondeep chandra pant*, hema pant**
*Associate ProfessorDept. of Cardiology*Assistant ProfessorDept. of PathologyUFHT Medical College, Haldwani, Uttarakhandaddress for correspondence Dr Deep Chandra PantAssociate Professor Dept. of CardiologyUFHT Medical College, Haldwani, UttarakhandE-mail: [email protected]
4. Steigman CK, Anderson DW, Macher AM, Sennesh JD, Virmani R. Fatal cardiac tamponade in acquired immunodeficiency syndrome with epicardial Kaposi’s sarcoma. Am Heart J 1988;116(4):1105-7.
5. Karve MM, Murali MR, Shah HM, Phelps KR. Rapid evolution of cardiac tamponade due to bacterial pericarditis in two patients with HIV-1 infection. Chest1992;101(5):1461-3.
6. Rerkpattanapipat P, Wongpraparut N, Jacobs LE, Kotler MN. Cardiac manifestations of acquired immunodeficiency syndrome. Arch Intern Med 2000;160(5):602-8.
7. Heidenreich PA, Eisenberg MJ, Kee LL, Somelofski CA, Hollander H, Schiller NB, et al. Pericardial effusion in AIDS. Incidence and survival. Circulation 1995;92(11): 3229-34.
8. Milei J, Grana D, Fernández Alonso G, Matturri L. Cardiac involvement in acquired immunodeficiency syndrome - a review to push action. The Committee for the Study of Cardiac Involvement in AIDS. Clin Cardiol 1998;21(7): 465-72.
9. Herskowitz A, Willoughby SB, Baughman KL, Schulman SP, Bartlett JD. Cardiomyopathy associated with antiretroviral therapy in patients with HIV infection: a report of six cases. Ann Intern Med 1992;116(4):311-3.
10. Chariot P, Perchet H, Monnet I. Dilated cardiomyopathy in HIV-infected patients. N Engl J Med 1999;340(9):732; author reply 733-5.
11. Lipshultz SE. Dilated cardiomyopathy in HIV-infected patients. N Engl J Med 1998;339(16):1153-5.
12. Barbaro G, Fisher SD, Pellicelli AM, Lipshultz SE. The expanding role of the cardiologist in the care of HIV infected patients. Heart 2001;86(4):365-7.
13. Sitbon O, Gressin V, Speich R, Macdonald PS, Opravil M, Cooper DA, et al. Bosentan for the treatment of human immunodeficiency virus-associated pulmonary arterial hypertension. Am J Respir Crit Care Med 2004;170(11):1212-7.
14. Degano B, Guillaume M, Savale L, Montani D, Jaïs X, Yaici A, et al. HIV-associated pulmonary arterial hypertension: survival and prognostic factors in the modern therapeutic era. AIDS 2010;24(1):67-75.
gender-specific formula for Women’s peak heart rate ‘more Accurate’
We should start using a new gender-specific formula for a woman’s peak heart rate as it better predicts the risk of heart–related death. A simple formula, 220 minus age, has long been used to calculate peak heart rates for women and men during exercise. But this formula was based on studies of men. The new formula developed for women is 206 minus 88% of age.
At age 50, the peak heart rate for a man will be 170 beats/minute and for woman will be 162 beats/minute. Most use the peak heart rate multiplied by 65-85% to calculate maximum heart rate when exercising.
The new formula is based on an analysis of 5,437 healthy women aged 35 and older (average age 52) from the greater Chicago metropolitan area, who volunteered to take part in the St. James Women Take Heart Project, launched in 1992.
Using the old formula, one is more ‘likely’ to tell women they have a worse prognosis than they do men. The new formula predicts risk more accurately said Dr Martha Gulati, an assistant professor of medicine and preventive medicine at Northwestern University’s Feinberg School of Medicine in Chicago. There is a physiologic response in women that is different from men. The study appears in the June 28 online issue of Circulation.

63Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
CAse report
62 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
made. Patient was referred to Dept. of Cardiothoracic Surgery for evaluation for excision of the tumor.
Discussion
Atrial myxomas are the most common primary heart tumors. Myxomas account for 40-50% of the primary cardiac tumors. Most cases are sporadic and 10% tumors can be familial. Most common site of attachment is at the border of the fossa ovalis in the left atrium, although myxomas can originate from the posterior atrial wall, the anterior atrial wall or the atrial left atrial appendage. Early diagnosis is a challenge because of nonspecific symptoms. 2D echocardiography is the diagnostic procedure of choice.
Left atrial myxoma may present with general malaise, fever, embolic phenomenon like embolic cerebral infarcts or symptoms mimicking mitral stenosis.1,2 The common clinical presentation mimics that of mitral valve disease either stenosis due to tumor prolapse into mitral orifice, or regurgitation due to tumor- induced valvular trauma.4 Ventricular myxomas may cause outflow obstruction similar to that caused by subaortic or subpulmonic stenosis. The symptoms and signs of myxomas may be of sudden onset or positional in nature, reflecting changes in tumor position due to gravity and auscultatory findings, termed as ‘tumor plop’, is a characteristic low- pitched sound that may be audible during early or mid diastole and is thought to result from the tumor abruptly stopping as it strikes the ventricular wall. Presentation of cardiac myxoma with severe pulmonary hypertension as a result of left inflow obstruction is theoretically possible but has not been reported in medical literature till now. This is the first case report
of left atrial myxoma presenting with secondary severe pulmonary hypertension.
2D transthoracic or transesophageal echocardiography is useful in the diagnosis of cardiac myxoma and allows determination of site of tumor attachment and tumor size, which are important considerations in planning of surgical excision. Computed tomography (CT) and particularly magnetic resonance imaging (MRI) may provide important information regarding size, shape, composition and surface characteristics of the tumor.3 Although cardiac catheterization and angiography have previously been performed routinely before surgery, catheterization of the chamber from which the tumor arises carries the risk of tumor emboli. Catheterization is no longer considered mandatory when adequate noninvasive information is available and other cardiac diseases (e.g. coronary artery disease) are not considered likely.
suggesteD reADing
1. Pinede L, Duhaut P, Loire R. Clinical presentation of left atrial cardiac myxoma. A series of 112 consecutive cases. Medicine 2001;80(3):159-72.
2. Aggarwal SK, Barik R, Sarma TC, Iyer VR, Sai V, Mishra J, et al. Clinical presentation and investigation findings in cardiac myxoma, new insights from the developing world. Am Heart J 2007;154(6):1102-7.
3. Sharpiro LM. Cardiac tumors: diagnosis and management. Heart 2001;85(2):218-22.
4. Whitlock R, Evans R, Lonn E, Teoh K. Giant left atrial myxoma and associated mitral valve pathology. J Cardiothoracic Vasc Anesth 2007;21(1):103-5.
5. Reynen K. Cardiac myxomas. N Engl J Med 1995;333 (24):1610-7.
case report
Atrioventricular Re-entrant Tachycardia: Clues to Underlying Accessory Pathway and its Locationavinash talele*, s kaBde*, n kumar*, mk jain**
The term Wolff-Parkinson-White syndrome (WPW) designates a condition comprising both pre-excitation and tachyarrhythmias.
The term paroxysmal supraventricular tachycardia (PSVT) refers to a clinical syndrome characterized by a rapid, regular tachycardia with abrupt onset and termination. Supraventricular tachycardias (SVTs) include all tachyarrhythmias that either originate from or incorporate supraventricular tissue in a re-entrant circuit. Pre-excitation occurs in the general population at a frequency of around 0.15-0.25%.1 Of these, 50-60% of patients become symptomatic. Approximately one-third of all patients with PSVT are diagnosed as having an accessory pathway (AP)-mediated tachycardia. Patients with AP-mediated tachycardias most commonly present with the syndrome of PSVT.2 Localization of the site of AP is possible with 90% sensitivity and 99% specificity by observing d-wave and QRS morphology in sinus rhythm.3 Detection of associated AP and its location is also possible, albeit difficult, during SVT, if attention is given to certain findings like QRS alternans, ST segment depression and T-wave changes.4,5
AbstrAct
Patients with accessory pathway (AP)-mediated tachycardias most commonly present with the syndrome of PSVT. Localization of the site of AP is possible with 90% sensitivity and 99% specificity by observing d-wave and QRS morphology in sinus rhythm. Presence of QRS alternation during sustained narrow QRS tachycardia is indicative of an AP.
keywords: Wolff-Parkinson-White syndrome, paroxysmal supraventricular tachycardia, AP-mediated tachycardia
cAse report
A 28-year-old male patient presented to ICU with complaint of palpitation for two hours. The episode had started suddenly during rest. He remembered having similar palpitations on and off for few years which used to subside on its own.
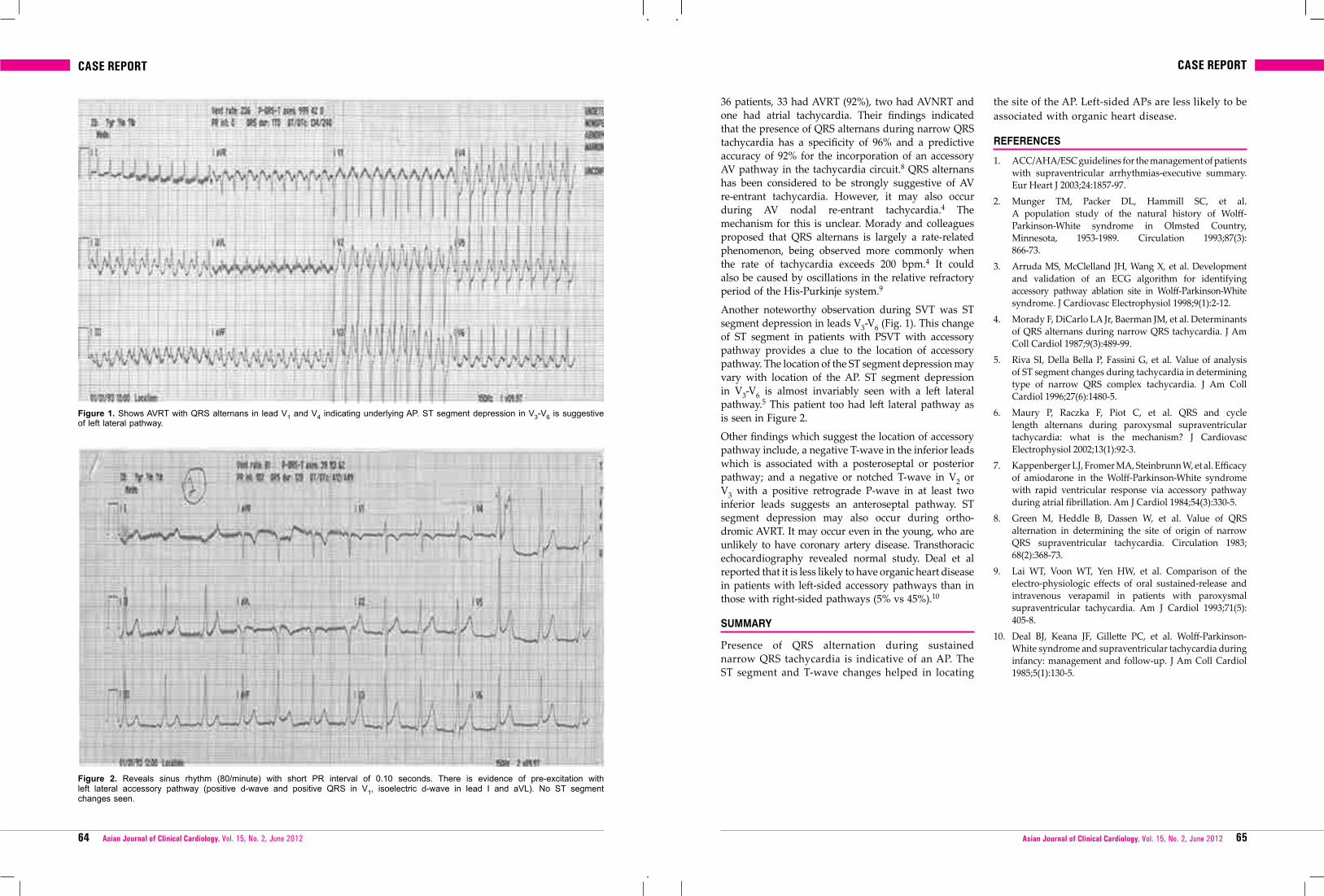
At presentation, he was uncomfortable, anxious but hemodynamically stable. His pulse rate was 232/ minute, blood pressure was 110/86 mmHg. His 12-lead ECG (Fig. 1) was recorded, which revealed SVT (AVRT) at the rate of 236/minute. RP interval was 0.08 seconds. QRS morphology shows QRS alternans (beat-to-beat oscillations in QRS) best seen in V1 and V4. ST segment depression in V3-V6 and T-wave inversion in lead I and aVL was also observed. This finding indicates presence of left lateral pathway.5 Vagal maneuvers (carotid sinus massage and valsalva maneuver) were carried out. The patient did not respond to it. Intravenous adenosine terminated the SVT. Transthoracic echocardiography was normal.
Discussion
The beat-to-beat oscillation of the QRS complex (QRS alternans) in lead V1 and V4 (Fig. 2) is the clue for tachycardia mediated with AP. QRS voltage and cycle length alternation can be seen during supraventri- cular re-entrant tachycardias, especially in atrioventricular re-entrant tachycardia (AVRT).6 QRS alternans may be present in nearly 38% of patients with circus-movement tachycardia involving AP.7 Green and co-workers reported a series of 161 patients with SVT out of which 36 had QRS alternans. Of these
*Postgraduate Student**Professor and HeadDept. of Medicine, Shyam Shah Medical College and Associated Sanjay Gandhi Memorial Hospital, Rewa, MPaddress for correspondenceDr Avinash TaleleDept. of Medicine, Shyam Shah Medical Collegeand Associated Sanjay Gandhi, Memorial Hospital, Rewa, MP
case reportcase report
64 65Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
36 patients, 33 had AVRT (92%), two had AVNRT and one had atrial tachycardia. Their findings indicated that the presence of QRS alternans during narrow QRS tachycardia has a specificity of 96% and a predictive accuracy of 92% for the incorporation of an accessory AV pathway in the tachycardia circuit.8 QRS alternans has been considered to be strongly suggestive of AV re-entrant tachycardia. However, it may also occur during AV nodal re-entrant tachycardia.4 The mechanism for this is unclear. Morady and colleagues proposed that QRS alternans is largely a rate-related phenomenon, being observed more commonly when the rate of tachycardia exceeds 200 bpm.4 It could also be caused by oscillations in the relative refractory period of the His-Purkinje system.9
Another noteworthy observation during SVT was ST segment depression in leads V3-V6 (Fig. 1). This change of ST segment in patients with PSVT with accessory pathway provides a clue to the location of accessory pathway. The location of the ST segment depression may vary with location of the AP. ST segment depression in V3-V6 is almost invariably seen with a left lateral pathway.5 This patient too had left lateral pathway as is seen in Figure 2.
Other findings which suggest the location of accessory pathway include, a negative T-wave in the inferior leads which is associated with a posteroseptal or posterior pathway; and a negative or notched T-wave in V2 or V3 with a positive retrograde P-wave in at least two inferior leads suggests an anteroseptal pathway. ST segment depression may also occur during ortho-dromic AVRT. It may occur even in the young, who are unlikely to have coronary artery disease. Transthoracic echocardiography revealed normal study. Deal et al reported that it is less likely to have organic heart disease in patients with left-sided accessory pathways than in those with right-sided pathways (5% vs 45%).10
summArY
Presence of QRS alternation during sustained narrow QRS tachycardia is indicative of an AP. The ST segment and T-wave changes helped in locating
the site of the AP. Left-sided APs are less likely to be associated with organic heart disease.
references
1. ACC/AHA/ESC guidelines for the management of patients with supraventricular arrhythmias-executive summary. Eur Heart J 2003;24:1857-97.
2. Munger TM, Packer DL, Hammill SC, et al. A population study of the natural history of Wolff-Parkinson-White syndrome in Olmsted Country, Minnesota, 1953-1989. Circulation 1993;87(3): 866-73.
3. Arruda MS, McClelland JH, Wang X, et al. Development and validation of an ECG algorithm for identifying accessory pathway ablation site in Wolff-Parkinson-White syndrome. J Cardiovasc Electrophysiol 1998;9(1):2-12.
4. Morady F, DiCarlo LA Jr, Baerman JM, et al. Determinants of QRS alternans during narrow QRS tachycardia. J Am Coll Cardiol 1987;9(3):489-99.
5. Riva SI, Della Bella P, Fassini G, et al. Value of analysis of ST segment changes during tachycardia in determining type of narrow QRS complex tachycardia. J Am Coll Cardiol 1996;27(6):1480-5.
6. Maury P, Raczka F, Piot C, et al. QRS and cycle length alternans during paroxysmal supraventricular tachycardia: what is the mechanism? J Cardiovasc Electrophysiol 2002;13(1):92-3.
7. Kappenberger LJ, Fromer MA, Steinbrunn W, et al. Efficacy of amiodarone in the Wolff-Parkinson-White syndrome with rapid ventricular response via accessory pathway during atrial fibrillation. Am J Cardiol 1984;54(3):330-5.
8. Green M, Heddle B, Dassen W, et al. Value of QRS alternation in determining the site of origin of narrow QRS supraventricular tachycardia. Circulation 1983; 68(2):368-73.
9. Lai WT, Voon WT, Yen HW, et al. Comparison of the electro-physiologic effects of oral sustained-release and intravenous verapamil in patients with paroxysmal supraventricular tachycardia. Am J Cardiol 1993;71(5): 405-8.
10. Deal BJ, Keana JF, Gillette PC, et al. Wolff-Parkinson-White syndrome and supraventricular tachycardia during infancy: management and follow-up. J Am Coll Cardiol 1985;5(1):130-5.
Figure 1. Shows AVRT with QRS alternans in lead V1 and V4 indicating underlying AP. ST segment depression in V3-V6 is suggestive of left lateral pathway.
Figure 2. Reveals sinus rhythm (80/minute) with short PR interval of 0.10 seconds. There is evidence of pre-excitation with left lateral accessory pathway (positive d-wave and positive QRS in V1, isoelectric d-wave in lead I and aVL). No ST segment changes seen.

66 67Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
Chest pain consistent with coronary ischemia
Within 10 minutesz Initial evaluation z 12 lead ECGz Establish IV access z Establish continuous ECG monitoringz Blood for baseline serum z Aspirin 160-325 mg chewed cardiac markers
Therapeutic/diagnostic tracking according to 12-lead ECG results
Nondiagnostic/normal ECG
ECG suggestive of ischemia - T wave inversion or ST depression
ST segment elevation or new bundle branch block
z Continue evaluation/monitoring in emergency department
z Serial serum cardiac marker levels - CK-MB subforms
z Serial ECGsz Consider noninvasive evaluation
of ischemiaz Consider alternative diagnoses
z Anti-ischemia therapyz Analgesia
Assess suitability for reperfusionz ? Contraindications for fibrinolysisz Availability and appropriateness
of primary angioplastyInitiate anti-ischemia therapyz Beta-blockerz NitroglycerineAnalgesia
No evidence of MI or ischemia
MI or demonstrable ischemia
Admit to unit of appropriate intensity
Admission blood work
Discharge with follow-up as appropriate (Goal:
8-12 hours)
Admission blood workz CBC z Electrolytes, BUN,
creatininez Lipid profile
Initiate fibrinolysis if
indicated. (Goal: 30 minutes from
entry to ED)
Primary PTCA, if available and suitable. (Goal:
PTCA within 90 ± 30 minutes)
Admit-CCU
Initial Assessment of Evaluation of the Patient with Acute Chest Pain
clinical algorithm
ECG: Electrocardiogram; CK-MB: Creatine kinase-MB; MI: Myocardial infarction; CBC: Complete blood count; BUN: Blood urea nitrogen; PTCA: Percutaneous transluminal coronary angioplasty; ED: Emergency department; CCU: Coronary care unit.
Source: IJCP
photo quiz
Right-Sided Cardiophrenic Mass in an Older Woman
A 76-year-old, physically active woman presented for an annual physical examination. Chest radiography revealed a large right
cardiophrenic mass (Figure 1 and 2). The patient had no remarkable medical history or physical examination findings. She had no history of tobacco use, fever, night sweats, anorexia, weight loss, shortness of breath, or dyspnea with exertion.
Question
Based on the patient’s history, physical examination, and radiographs, which one of the following is the most likely diagnosis?
A. Carcinoma.
B. Diaphragmatic eventration.
C. Morgagni hernia.
Source: Adapted from American Family Physician. 2010;82(8):971-972.
Figure 1. Figure 2.
SEE THE FOLLOWING PAGE FOR DISCUSSION.
D. Pericardial cyst.
E. Pericardial fat pad.

69Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 201268 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
Discussion
The answer is C: Morgagni hernia.
A Morgagni hernia is a congenital diaphragmatic hernia and is not usually associated with other congenital anomalies.1 Morgagni hernias result from the failure of the sternal and costal components of the diaphragm to fuse during embryogenesis. The condition represents 3 percent of all diaphragmatic hernias and is more common in women.2 Most patients are asymptomatic, but the condition may be identified incidentally on chest radiographs. Occasionally, Morgagni hernias cause nonspecific cardiovascular, gastrointestinal, or respiratory symptoms.3
The hernias are always right-sided and located in the anterior cardiophrenic sulcus.2 More than 90 percent of cases have hernia sacs, which may involve the omentum, colon, stomach, and small intestine. Classic radiographic findings include a homogeneous, rounded soft tissue opacity in the right cardiophrenic angle. A lateral chest radiograph is needed to show the anterior location of the opacity. Although rare, an air-fluid level within the opacity is considered pathognomonic of a Morgagni hernia. Computed tomography can be diagnostic in more than 80 percent of patients by showing fat and omental vessels or abdominal viscera within the soft tissue mass.4 Once the condition is diagnosed, patients should be referred for reduction of the herniated organs and surgical repair of the anatomic defect.5
Carcinoma of the lung usually obscures bronchovascular markings and appears on radiography as an irregular or spiculated mass. Atelectasis, lymphadenopathy, or pleural effusion may be an associated finding.
Diaphragmatic eventration is nonparalytic weakening of the hemidiaphragm. It is usually partial and involves the anteromedial portion of the right hemidiaphragm. Radiography shows elevation of the affected area of the diaphragm, and the common pattern is a smooth hump along the contour of the diaphragm.6
Pericardial cysts are anomalous outpouchings of parietal pericardium. On radiography, the cysts are smoothly marginated masses touching the heart, particularly at the right anterior cardiophrenic angle. Pericardial cysts are sometimes difficult to distinguish from Morgagni hernias. Computed tomography or ultrasonography can demonstrate the cystic nature of the lesions.7
Enlarged pericardial fat pads are associated with Cushing syndrome, corticosteroid therapy, and obesity. They often occupy the right cardiophrenic angle. Although the fat pads may obliterate the angle, the cardiac and diaphragmatic borders are usually visible.The density of fat pads is not as great as that of Morgagni hernias, and their margins are not as sharply delineated.
references
1. Naunheim KS. Adult presentation of unusual diaphragmatic hernias. Chest Surg Clin N Am. 1998;8(2):359-369.
2. Comer TP, Clagett OT. Surgical treatment of hernia of the foramen of Morgagni. J Thorac Cardiovasc Surg. 1966;52(4):461-468.
3. Bhasin DK, Nagi B, Gupta NM, Singh K. Chronic intermittent gastric volvulus within the foramen of Morgagni. Am J Gastroenterol. 1989;84(9):1106-1108.
4. Minneci PC, Deans KJ, Kim P, Mathisen DJ. Foramen of Morgagni hernia: changes in diagnosis and treatment. Ann Thorac Surg. 2004;77(6):1956-1959.
5. Huston JM, King H, Maresh A, et al. Hernia of Morgagni:case report. J Thorac Cardiovasc Surg. 2008;135(1): 212-213.
6. Deslauriers J. Eventration of the diaphragm. Chest Surg Clin N Am. 1998;8(2):315-330.
7. Breen JF. Imaging of the pericardium. J Thorac Imaging. 2001;16(1):47-54.
Summary tableCondition CharacteristicsCarcinoma Irregular or spiculated mass with obscured
lung markings; possibly associated atelectasis, lymphadenopathy, or pleural effusion
Diaphragmatic eventration
Elevation of the affected area of the diaphragm; smooth hump along the contour of the diaphragm
Morgagni hernia
Homogeneous, rounded mass in the right anterior cardiophrenic angle; air-fluid level within the mass is considered pathognomonic
Pericardial cyst
Anomalous outpouching of parietal pericardium; smoothly marginated mass touching the heart
Pericardial fat pad
Associated with Cushing syndrome, corticosteroid therapy, and obesity; density not as great and margins not as sharply defined as those of Morgagni hernia or pericardial cysts
photo quiz
Journal Scan
is bnp-guiDeD treAtment for heArt fAilure effective?
Background: B-type natriuretic peptide (BNP) and N-terminal pro-BNP levels are useful in diagnosing acute decompensated heart failure, and can also predict clinical outcomes in patients with chronic heart failure. It has been proposed that adjusting heart failure therapy to reduce BNP plasma levels may improve clinical outcomes. However, the benefit of this approach remains uncertain because many trials have been underpowered to detect the effect on major cardiovascular events. Porapakkham and colleagues performed a meta-analysis of prospective randomized controlled trials that examined BNP-guided therapy versus clinically guided treatment in the outpatient management of heart failure.
The Study: Trials had to have more than 20 patients and have clinically relevant end points (e.g., all-cause mortality, hospitalization) to be included in the meta-analysis. The likelihood of these end points was assessed when standard heart failure treatments (e.g., angiotensin-converting enzyme inhibitors, angiotensin receptor blockers, aldosterone antagonists, beta blockers) were titrated to improve clinical status (e.g., New York Heart Association [NYHA] functional class) versus adjusting treatment to achieve specified BNP or pro-BNP levels, with or without clinical status improvement (e.g., the Systolic Heart Failure Treatment Supported by BNP study had a target BNP level of less than 100 pg per mL [100 ng per L], whereas the Trial of Intensified versus Standard Medical Therapy in Elderly Patients with Congestive Heart Failure used a target N-terminal pro-BNP level of less than 400 pg per mL [400 ng per L] in addition to NYHA functional class II or lower in adults younger than 75 years).
Results: Eight trials with 1,726 patients were analyzed. All participants were 18 to 85 years of age and had NYHA functional class II or greater heart failure with left ventricular ejection fraction less than 50 percent. The mean follow-up duration was 17 months (range: three to 24 months). All-cause mortality was significantly lower among patients in the BNP-guided therapy group compared with those in the standard therapy group (relative risk = 0.76). Subgroup analysis
found this effect was even more significant in patients younger than 75 years (relative risk = 0.52), but BNP-guided therapy did not reduce mortality in patients 75 years and older. No significant differences were noted between groups with regard to all-cause hospitalization or hospitalization-free survival.
Conclusion: The authors conclude that BNP-guided therapy can significantly lower all-cause mortality in patients younger than 75 years with chronic heart failure compared with standard therapy. However, all-cause hospitalization and hospitalization-free survival rates remain unaffected.
Am Fam Physician. 2011;83(1):82.
no ADDeD benefit of fenofibrAte for cArDiovAsculAr risk in DiAbetes mellitus
Background: Statins reduce the increased cardiovascular risk seen in patients with type 2 diabetes mellitus, but do not eliminate it. Studies have shown conflicting results as to whether fibrates may also help reduce cardiovascular disease in this population. Ginsberg and colleagues used the ACCORD (Action to Control Cardiovascular Risk in Diabetes) trial to determine if combination lipid therapy could reduce cardiovascular risk in patients with type 2 diabetes.
The Study: A total of 5,518 patients with type 2 diabetes were randomized to receive simvastatin at 40 mg per day or less, in addition to fenofibrate (initial dosage of 160 mg per day) or placebo. All patients had an A1C level of 7.5 percent or more, a low-density lipoprotein cholesterol level of 60 to 180 mg per dL (1.55 to 4.66 mmol per L), a high-density lipoprotein (HDL) cholesterol level of less than 55 mg per dL (1.42 mmol per L), and a triglyceride level of less than 750 mg per dL (8.47 mmol per L). The mean follow-up period was 4.7 years. The primary outcome was a composite of the first occurrence of a major fatal or nonfatal cardiovascular event (i.e., myocardial infarction or stroke). Baseline characteristics were similar between groups: 37 percent had experienced a previous cardiovascular event and 60 percent were taking a statin before enrolment.
Results: No difference was noted between groups with regard to the composite cardiovascular outcome (2.2 versus 2.4 percent annual incidence for the fibrate and
research review

70 71Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
placebo groups, respectively). However, analysis based on sex showed that fibrates might have a benefit in men (11.2 versus 13.3 percent incidence of the primary outcome in the fibrate versus placebo group during the entire study; P = .01), whereas the reverse occurred in women (9.1 versus 6.6 percent, respectively; P = .01). A nonsignificant trend toward benefit occurred overall in patients with a triglyceride level of 204 mg per dL (2.31 mmol per L) or more and an HDL level of 34 mg per dL (0.88 mmol per L) or less. No differences were noted in most secondary outcomes (i.e., congestive heart failure, all-cause mortality, or separate analyses of myocardial infarction or stroke).
Conclusion: The authors conclude that, compared with simvastatin monotherapy, adding fenofibrate does not reduce the risk of cardiovascular events in patients with type 2 diabetes. This combination is not supported to prevent cardiovascular risk in most patients with type 2 diabetes; however, a small potential benefit occurred in men using both agents.
Am Fam Physician. 2011;83(5):612.
effects of intensive blooD pressure control in pAtients With DiAbetes mellitus
Background: The risk of cardiovascular disease rises as systolic blood pressure increases in patients with type 2 diabetes mellitus. Current guidelines from the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure advise lowering systolic blood pressure to less than 130 mm Hg in patients with diabetes; however, there is little evidence to indicate that this improves clinical outcomes. The Action to Control Cardiovascular Risk in Diabetes (ACCORD) Study Group evaluated the effects of intensive blood pressure control on cardiovascular events in patients with diabetes.
The Study: A total of 4,733 patients with type 2 diabetes were randomized to one of two blood pressure
control groups: intensive therapy (target systolic blood pressure of less than 120 mm Hg) or a control group (target systolic blood pressure of less than 140 mm Hg). Patients were followed for an average of 4.7 years. Blood pressure was managed using standard antihypertensive agents, but no specific strategy was enforced. The primary outcome was a composite of the first occurrence of a major fatal or nonfatal cardiovascular event (i.e., myocardial infarction or stroke). Various secondary outcomes (i.e., separate assessments for myocardial infarction, stroke, congestive heart failure, and all-cause mortality) also were evaluated.
Results: Baseline traits between groups were similar, including initial blood pressure and incidence of previous cardiovascular events. No significant difference in the primary outcome was noted between groups, despite the intensive treatment group maintaining significantly lower blood pressure than the control group (mean blood pressures: 119.3/64.4 mm Hg versus 133.5/70.5 mm Hg, respectively). Most secondary outcomes showed no differences between groups, including all-cause or cardiovascular-related mortality, congestive heart failure, or myocardial infarction. However, the intensive therapy group had a lower incidence of total strokes than did the control group (0.32 versus 0.53 percent per year, respectively; hazard ratio = 0.59; P = .01) and nonfatal strokes (0.30 versus 0.47 percent per year, respectively; hazard ratio = 0.63; P = .03).
Conclusion: The authors conclude that a more stringent blood pressure goal for patients with type 2 diabetes does not significantly reduce the primary cardiovascular outcome or most secondary outcomes compared with standard blood pressure goals. In this study, the number of total and nonfatal strokes was lower in the intensive therapy group, although the clinical benefit was limited (number needed to treat = 89 for five years to prevent one stroke).
Am Fam Physician. 2011;83(5):612-613.
research review
Computed tomography (CT) is the diagnostic standard for acute stroke even though its accuracy has not been formally established. The sensitivity of CT, which is estimated to be 12 to 92 percent, depends on the imaging features of infarction, time from onset to examination, and study populations, among other factors. Its sensitivity for diagnosing ischemic stroke in the initial hours is limited; therefore, improved accuracy is needed to develop and provide optimal stroke treatment.
Diffusion- and perfusion-weighted imaging, which are newer magnetic resonance imaging techniques, may improve diagnostic yield. Diffusion-weighted imaging measures the net movement of water in tissue due to random molecular motion, also known as Brownian motion. It shows hyperintense ischemic tissue changes within minutes to hours after arterial occlusion caused by a reduced diffusion capacity within the affected tissues. Perfusion-weighted imaging allows the measurement of capillary perfusion. The American Academy of Neurology (AAN) evaluated the evidence for the use of magnetic resonance imaging in the diagnosis of acute ischemic stroke.
clinicAl Questions AnD recommenDAtions
Diffusion- and perfusion-weighted imaging were assessed to determine their sensitivity specificity compared with other imaging modalities, and volume of diffusion- and perfusion-weighted imaging abnormality was evaluated to determine if it predicts initial clinical severity, final infarct size, and late clinical outcomes.
The AAN determined that diffusion-weighted imaging is superior to noncontrast CT for the diagnosis of acute ischemic stroke within 12 hours of symptom onset; however, there is insufficient evidence regarding the accuracy of perfusion-weighted imaging. Baseline diffusion-weighted imaging volume is probably useful in predicting baseline clinical stroke severity and final lesion volume in patients with anterior circulation stroke syndromes. It may also be useful in predicting clinical
outcomes as measured by the National Institutes of Health Stroke Scale and Barthel Index. However, it may not be useful in predicting baseline National Institutes of Health Stroke Scale score in patients with posterior circulation stroke syndromes. Baseline perfusion-weighted imaging volume may be useful in predicting baseline clinical stroke severity.
clinicAl context
Noncontrast CT can be used to assess for infarct and to exclude hemorrhage and other structural lesions that can mimic stroke in patients with acute neurologic impairment. Diffusion-weighted imaging is superior to CT in the diagnosis of acute ischemic stroke within 12 hours of symptom onset relative to clinical and imaging outcomes. In clinical practice, however, cost, availability, and medical management requirements must be considered when making decisions about which imaging modality to use.
The sensitivity of diffusion-weighted imaging is estimated to be 80 to 90 percent in the emergency evaluation of patients with possible stroke. Case series and small comparative studies have reported that diffusion-weighted imaging had almost 100 percent sensitivity for diagnosing stroke in the hyperacute stage; however, cases of diffusion-weighted imaging–negative stroke were increasingly reported. False-negative diffusion-weighted imaging may be attributable to mild strokes, brainstem location, and earlier time from onset. False-negative results may become less common as imaging improves.
Positive diffusion-weighted imaging in patients with transient ischemic attacks is common. Acute ischemic lesions on diffusion-weighted imaging are found in approximately 40 percent of patients with transient ischemic attack; this finding correlates with symptom duration. A recent study determined that diagnoses based on diffusion-weighted imaging could result in increased annual incidence of stroke and reduced annual incidence of transient ischemic attack.
practice guidelines
AAN Releases Guideline on Magnetic Resonance Imaging for Diagnosing Acute Ischemic Stroke
Source: Adapted from Am Fam Physician. 2011;83(4):483-484.

72 73Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
News and Views
ADDing mArkers ADDs little to cv preDiction
Only slight improvements in cardiovascular (CV) risk prediction were gained by adding more blood lipid-related markers to conventional factors, researchers said. Fewer than 5% of individuals would have their risk classifications changed by including such markers as apolipoprotein A-I, apolipoprotein B, lipoprotein(a), or lipoprotein-associated phospholipase A2 (LpA-PLA2) in gauging the likelihood of major cardiovascular events, reported John Danesh, FRCP, of the University of Cambridge in England, and colleagues belonging to the Emerging Risk Factors Collaboration. At best, adding more lipid markers to the risk prediction equation brought ‘slight improvement,’ the researchers wrote in the June 20 issue of the Journal of the American Medical Association. (Source: Medpage Today)
bonus info: chADs2 helps preDict post-cAbg Af risk
The CHADS2 score is routinely used to identify candidates for coronary artery bypass graft (CABG) surgery at high-risk for stroke. Since the score includes factors that also portend a greater risk of atrial fibrillation (AF), researchers tested whether it could find CABG patients at high-risk for post-operative AF, too.
citicoline proviDes no benefit in Acute ischemic stroke
Adding to a long line of negative study results for potential neuroprotective agents, the International Citicoline Trial on acUte Stroke (ICTUS) could not confirm any efficacy of this agent in the treatment of acute ischemic stroke. Antoni Dávalos, MD, PhD, from the Hospital Universitari Germans Trias i Pujol in Badalona, Spain, presented the results of this randomized, placebo-controlled, double-blind, sequential clinical trial at the XXI European Stroke Conference (ESC). Oral citicoline (cytidine-5′-diphosphocholine) had previously shown some positive results in single trials and in a meta-analysis for functional and neurologic recovery. It is an intermediate in the generation of phosphatidylcholine from choline in the body and is sold over the counter in many countries. (Source: Medscape)
grAft pAtencY Worse After off–pump cAbg in rAnDomizeD triAl
Coronary artery bypass graft (CABG) patency was significantly worse after off-pump surgeries in the Veterans Affairs Randomized On/Off Bypass (ROOBY) trial. “For most patients, on-pump should be the preferred approach,” lead investigator Dr Brack Hattler from Denver VAMC, Colorado told Reuters Health. “There certainly are a few very experienced surgeons who are able to obtain equivalent and excellent outcomes with off-pump CABG, but overall there is really no evidence to argue that off-pump results in improved long-term outcomes or graft patency.” (Source: Medscape)
DArk chocolAte: sWeet prevention for cv events
Dark chocolate may be an inexpensive way to help prevent cardiovascular events in patients at risk for heart disease, researchers found. A modeling study predicts that patients with metabolic syndrome who eat dark chocolate every day could have 85 fewer events per 10,000 population over 10 years, Chris Reid, PhD, of Monash University in Melbourne, and colleagues reported online in BMJ. “Chocolate benefits from being by and large a pleasant, and hence sustainable, treatment option,” Several recent studies have suggested that eating dark chocolate has blood-pressure and lipid-lowering effects. To assess whether it could be an effective and cost-effective treatment option in patients potentially at risk for cardiovascular events, the researchers looked at data from patients in the Australian Diabetes, Obesity, and Lifestyle study. The study was also limited by the assumption that the benefits of dark chocolate, which have only been observed in short-term trials, extend to 10 years. Still, they concluded that the findings suggest dark chocolate may be an effective and cost-effective strategy for preventing heart disease in patients with metabolic syndrome. (Source: Medpage Today)
Aspirin response in pAD preDicts long-term risk
Patients with peripheral artery disease (PAD) who are resistant to aspirin therapy have a higher long-term risk of cardiovascular events than those who respond to aspirin, researchers reported at the Society for Cardiovascular Angiography and Interventions (SCAI) meeting. (Source: Medpage Today)
around the gloBe
Insight on Medicolegal Issuessudhir gupta
inevitAble meDicAl AcciDent in heAlthcAre DeliverY
An inevitable medical accident or “unavoidable medical occurrence” in healthcare delivery is that which could not be possibly prevented by the exercise of ordinary medical/surgical/paramedics and nursing care, caution and skill. In medical profession, it means any medical/surgical accident that results in damage/injury/disability or death that was not avoidable by any such precautions as a reasonable qualified medical professional or hospital doing such an act then, “could be expected to take.” A general/reasonable medical professional is not credited by the law with exact perfection of judgment. As observed by Greene M.R., an accident is “one out of the ordinary course of things, something so unusual as not to be looked for by a person of ordinary prudence.During the course of treatment, an accident occurs which could not be avoided by any ordinary skill or care on the part of the doctor administering the treatment, the accident is said to be inevitable accident. The term ‘inevitable accident‘ has been defined as an accident not avoidable by any such precautions as a reasonable man can be expected to take’. In the case of (Gerber V. Pines 21) the plaintiff claimed damages against the defendant alleging that during the administration of a hypodermic injection the defendant left part of a broken needle in her buttock. The defendant denied liability and said that the breakage of the needle was due to a sudden muscular spasm and that no skill or care on his part could have prevented the fracture of the needle or the retention of the broken part in the plaintiff‘s body. The judge found that there had been no negligence on the part of the defendant in so far as the fracture of the needle was concerned, he found however, that had been a breach of duty on the part of defendant in not informing the plaintiff or her husband that the needle had fractured and that a piece of it was still in her body. For this the judge awarded the plaintiff a small sum by way of damages. In cases of inevitable medical accident, a very positive/sympathetic/grief sharing approach should be taken by the doctor towards his/her patient and all logistic medical/surgical services must be extended/provided to the patient without cost
medilaw
by the doctor/hospital to restore/enhance faith and trust of this profession since the service which medical professionals render to the people/society and nation is the noblest one. The patient must also be told that inevitable medical accident was due to the elementary forces of nature unconnected with the hospital/doctor and they are there to share with the patient’s suffering.
WhAt is concussion of the brAin?
Concussion of the brain is a rotational injury caused by sudden acceleration.
 As seen in autopsy it occurs when the head is free to move with sufficient velocity, but not when it is fixed. It is more commonly known as ‘stunning‘, and may be produced by direct violence on the vertex, by indirect violence as a result of a violent fall upon the feet from height, or by an unexpected fall on the ground, when pushed forcibly in any traffic accident or an injury received in industry.
 The impact on hollow structures of skull is propagated by radiating waves of motion along with the site of impact and coverage as they approach the opposite pole giving rise at the point of collision to a contralateral or countercoup injury.
 The contusion and laceration of brain occurs due to the traction as the brain is torn away from its covering by the force of its own momentum. Application of a blow to the movable head is followed by a positive pressure in the area of brain underlying the zone of impact and by a negative pressure over the contralateral brain surface where the brain pulls away from the skull.
 The injuries of the brain heal by forming adhesions and may later cause secondary epilepsy.
WhAt is the commonest cAuse of cArDiologY mAl prActice suits?
 Diagnostic errors are the leading cause of loss in cardiology liability suits. Physicians could reduce loss by ruling out conditions carrying the greatest risk if misdiagnosed and by consulting with a radiologist concerning abnormal X-rays. Lack of documentation, poor physician communication, and adverse patient perception also lead to problems.
Kuehm SL, Abraham E. Medical malpractice claims in cardiology. N J Med 1990;87(5):393-8.
Additional ProfessorForensic Medicine and Toxicology, AIIMS, New Delhi

74 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
Lighter Side of Medicine
fAce Difficulties positivelY
This parable is told of a farmer who owned an old mule. The mule fell into the farmer’s well. The farmer heard the mule praying or whatever mules do when they fall into wells.
After carefully assessing the situation, the farmer sympathized with the mule, but decided that neither the mule nor the well was worth the trouble of saving. Instead, he called his neighbors
together, told them what had happened, and enlisted them to help haul dirt to bury the old mule in the well and put him out of his misery.
Initially the old mule was hysterical! But as the farmer and his neighbors continued shoveling and the dirt hit his back, a thought struck him. It suddenly dawned on him that every time a shovel load of dirt landed on his back, HE WOULD SHAKE IT OFF AND STEP UP!
This he did, blow after blow. “Shake it off and step up…shake it off and step up…shake it off and step up!” He repeated to encourage himself. No matter how painful the blows, or how distressing the situation seemed, the old mule fought panic and just kept right on SHAKING IT OFF AND STEPPING UP!
It wasn’t long before the old mule, battered and exhausted, stepped triumphantly over the wall of that well! What seemed like it would bury him actually helped him . . . all because of the manner in which he handled his adversity.
That’s life! If we face our problems and respond to them positively, and refuse to give in to panic, bitterness, or self-pity.
—Ms Ritu Sinha
an in
spir
atio
nal
stor
y
Dr. Good & Dr. Bad
Dr KK Aggarwal
SItuAtION:
lESSON:
©IJ
CP
Aca
de
my
lighter reading
You are suffering from an inflammatory
disease
A diabetic patient was found to have high ESR and elevated CRP.
In diabetes, both ESR and CRP can be high at the same time and this can be due to IL-6 secretion by adipose tissue.
laug
h a
whi
le the cArDiologist AnD the motorcYcle
repAirmAn
A motorcycle mechanic was removing cylinder-head from the motor of a Harley-Davidson when he spotted a well-known cardiologist in his shop. The cardiologist was there waiting for the service manager to come and take a look at his bike
when the mechanic shouted across the garage, ‘Hey Doc, want to take a look at this?’ The cardiologist, a bit surprised, walked over to where the mechanic was working on the motorcycle.
The mechanic straightened up, wiped his hands on a rag and asked, ‘So Doc, look at this engine. I opened its heart, take the valves out, repair any damage, and then put them back in, and when I finish, it works just like new. So how come I make $39,675 a year and you make $1,695,000 when you and I are doing basically the same work?’
The cardiologist paused, leaned over and then whispered to the mechanic. ‘Try doing it with the engine running’.
−Dr GM Singh
quot
es
“Facts are many, but the truth is one.”
—Rabindranath Tagore
“Tis the set of the sail that decides the goal, and not the storm of life.”
—Ella Wheeler Wilcox
This may be a part of diabetes
April 2012, Pages 545-596Volume 22, Number 11
Drug Review
Review Article
Original Article
Case Report
Photo Quiz
Lighter Reading
�
�
�
�
�
�
Peer Reviewed Journal

77Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
Information for AuthorsManuscripts should be prepared in accordance with the ‘Uniform requirements for manuscripts submitted to biomedical journals’ compiled by the International Committee of Medical Journal Editors (Ann. Intern. Med. 1992;96: 766-767).Asian Journal of Clinical Cardiology strongly disapproves of the submission of the same articles simultaneously to different journals for consideration as well as duplicate publication and will decline to accept fresh manuscripts submitted by authors who have done so.The boxed checklist will help authors in preparing their manuscript according to our requirements. Improperly prepared manuscripts may be returned to the author without review. The checklist should accompany each manuscript.Authors may provide on the checklist, the names and addresses of experts from Asia and from other parts of the World who, in the authors’ opinion, are best qualified to review the paper.
Covering letter
- The covering letter should explain if there is any deviation from the standard IMRAD format (Introduction, Methods, Results and Discussion) and should outline the importance of the paper.
- Principal/Senior author must sign the covering letter indicating full responsibility for the paper submitted, preferably with signatures of all the authors.
- Articles must be accompanied by a declaration by all authors stating that the article has not been published in any other Journal/Book. Authors should mentioned complete designation and departments, etc. on the manuscript.
Manuscript- Three complete sets of the manuscript should be
submitted and preferably with a CD; typed double spaced throughout (including references, tables and legends to figures).
- The manuscript should be arranged as follow: Covering letter, Checklist, Title page, Abstract, Keywords (for indexing, if required), Introduction, Methods, Results, Discussion, References, Tables, Legends to Figures and Figures.
- All pages should be numbered consecutively beginning with the title page.
Note: Please keep a copy of your manuscript as we are not responsible for its loss in the mail. Manuscripts will not be returned to authors.
title pageShould contain the title, short title, names of all the authors (without degrees or diplomas), names and full location of the
departments and institutions where the work was performed, name of the corresponding authors, acknowledgment of financial support and abbreviations used.- The title should be of no more than 80 characters and
should represent the major theme of the manuscript. A subtitle can be added if necessary.
- A short title of not more than 50 characters (including inter-word spaces) for use as a running head should be included.
- The name, telephone and fax numbers, e-mail and postal addresses of the author to whom communications are to be sent should be typed in the lower right corner of the title page.
- A list of abbreviations used in the paper should be included. In general, the use of abbreviations is discouraged unless they are essential for improving the readability of the text.
Summary- The summary of not more than 200 words. It must
convey the essential features of the paper.- It should not contain abbreviations, footnotes or
references.
Introduction- The introduction should state why the study was carried
out and what were its specific aims/objectives.
Methods- These should be described in sufficient detail to permit
evaluation and duplication of the work by others.- Ethical guidelines followed by the investigations should
be described.
StatisticsThe following information should be given:- The statistical universe i.e., the population from which
the sample for the study is selected.- Method of selecting the sample (cases, subjects, etc.
from the statistical universe).- Method of allocating the subjects into different
groups.- Statistical methods used for presentation and analysis of
data i.e., in terms of mean and standard deviation values or percentages and statistical tests such as Student’s ‘t’ test, Chi-square test and analysis of variance or non-parametric tests and multivariate techniques.
- Confidence intervals for the measurements should be provided wherever appropriate.
results- These should be concise and include only the tables
and figures necessary to enhance the understanding of the text.
Journal ofCLINICALCARDIOLOGYA
sian

78 Asian Journal of Clinical Cardiology, Vol. 15, No. 2, June 2012
Discussion
- This should consist of a review of the literature and relate the major findings of the article to other publications on the subject. The particular relevance of the results to healthcare in India should be stressed, e.g. practicality and cost.
referencesThese should conform to the Vancouver style. References should be numbered in the order in which they appear in the texts and these numbers should be inserted above the lines on each occasion the author is cited (Sinha12 confirmed other reports13,14...). References cited only in tables or in legends to figures should be numbered in the text of the particular table or illustration. Include among the references papers accepted but not yet published; designate the journal and add ‘in press’ (in parentheses). Information from manuscripts submitted but not yet accepted should be cited in the text as ‘unpublished observations’ (in parentheses). At the end of the article the full list of references should include the names of all authors if there are fewer than seven or if there are more, the first six followed by et al., the full title of the journal article or book chapters; the title of journals abbreviated according to the style of the Index Medicus and the first and final page numbers of the article or chapter. The authors should check that the references are accurate. If they are not this may result in the rejection of an otherwise adequate contribution.Examples of common forms of references are:
ArticlesPaintal AS. Impulses in vagal afferent fibres from specific pulmonary deflation receptors. The response of those receptors to phenylguanide, potato S-hydroxytryptamine and their role in respiratory and cardiovascular reflexes. Q. J. Expt. Physiol. 1955;40:89-111.
BooksStansfield AG. Lymph Node Biopsy Interpretation Churchill Livingstone, New York 1985.
Articles in BooksStrong MS. Recurrent respiratory papillomatosis. In: Scott Brown’s Otolaryngology. Paediatric Otolaryngology Evans JNG (Ed.), Butterworths, London 1987;6:466-470.
tables- These should be typed double spaced on separate
sheets with the table number (in Roman Arabic numerals) and title above the table and explanatory notes below the table.
legends- These should be typed double spaces on a separate
sheet and figure numbers (in Arabic numerals) corresponding with the order in which the figures are presented in the text.
- The legend must include enough information to permit interpretation of the figure without reference to the text.
Please complete the following checklist and attach to the manuscript:1. Classification (e.g. original article, review, selected
summary, etc.)_______________________________2. Total number of pages ________________________3. Number of tables ____________________________4. Number of figures ___________________________5. Special requests _____________________________6. Suggestions for reviewers (name and postal address) Indian 1. ___________Foreign 1. _______________ 2. ___________ 2. _______________ 3. ___________ 3. _______________ 4. ___________ 4. _______________7. All authors’ signatures________________________8. Corresponding author’s name, current postal and
e-mail address and telephone and fax numbers __________________________________________
For Editorial Correspondence Dr KK AggarwalGroup Editor-in-Chief
Asian Journal of Clinical CardiologyE - 219, Greater Kailash, Part - 1,
New Delhi - 110 048. Phone: 011-40587513E-mail: [email protected], [email protected]
Website: www.ijcpgroup.com
Figures- Two complete sets of glossy prints of high quality
should be submitted. The labelling must be clear and neat.
- All photomicrographs should indicate the magnification of the print.
- Special features should be indicated by arrows or letters which contrast with the background.
- The back of each illustration should bear the first author’s last name, figure number and an arrow indicating the top. This should be written lightly in pencil only. Please do not use a hard pencil, ball point or felt pen.
- Color illustrations will be accepted if they make a contribution to the understanding of the article.
- Do not use clips/staples on photographs and artwork.
- Illustrations must be drawn neatly by an artist and photographs must be sent on glossy paper. No captions should be written directly on the photographs or illustration. Legends to all photographs and illustrations should be typed on a separate sheet of paper. All illustrations and figures must be referred to in the text and abbreviated as ‘Fig.’.
Online Submission Also e-issue @ www.ijcpgroup.com

REGISTRATION NO. DL (S)-01/3288/2010-2012POSTED IN NDPSO NEW DELHI
R.N.I. No. 71217/98Date of Publishing 25 of Same MonthDate of Posting 25-26 Same Month