annual report 2008/09
DESCRIPTION
Clatterbridge Centre for Oncology Annual Report and Accounts 2008/09TRANSCRIPT
The Centre for cancer care
2008/09
AnnuAl RepoRT AND ACCounTS

2008/09
AnnuAl RepoRT AND ACCOUNTS
Presented to Parliament pursuant
to Schedule 7, paragraph 25(4)
of the National Health Act 2006.
Contents
Annual Report
Chairman’s Statement 5
Directors’ Report 7
Operating & Financial Review (OFR) 8
Patient Care 12
Developing our services 15
Governance 19
Quality Report
Quality Strategy priorities 36
Priorities and initiatives for 2009/10 38
Quality Overview 40
Annual Accounts
Foreward to the Accounts 45
Statement of accounting officer’s responsibilities 46
Statement of Directors’ responsibilities 47
Independent Auditors Report 48
Statement of Internal Control 50
Notes to the Accounts 64
Remuneration Report 70
5
Introduction
Chairman’s Statement
Reaching the end of the financial year 2008/09 is an opportune time to reflect on the work of the Trust during the course of the year.
I am pleased to report that Clatterbridge Centre for Oncology (CCO) continues to provide the highest quality clinical care possible and in recognition of this the Healthcare Commission has awarded the Trust its ‘excellent’ rating for both the quality of services and for the use of resources; the two areas it inspects for the year 2007/08 and we are confident that we will receive a similarly high rating for 2008/09. In addition, the Foundation Trust Regulator has awarded the organisation the highest ratings possible for the two key issues he monitors ie governance and finance.
CCO is achieving all the required NHS targets including 62 day waiting time target (urgent referral to treatment for all cancers) and the 18 week waiting time target (point of initial referral up to the start of any treatment). Infection control continues to present particular difficulties for this Centre because virtually all our patients are referred from other hospitals but I am pleased to report that MRSA bacteraemia infections have remained at zero throughout the year.
Furthermore, the Trust has achieved a strong balance sheet with a surplus of £4.45m, which has enabled us to develop a £3m investment programme to upgrade facilities and services at the centre.
In December 2008 Cherie Blair, who has agreed to champion our fundraising appeal, officially opened the new Out-Patient Department. The first completed phase of the investment plan. The new department includes state-of-the-art clinic rooms and patient waiting areas. A conservatory has also been built out into a landscaped water garden as an extension to the patient waiting area. The conservatory was funded by the Melanie Beattie Appeal, for which we are most grateful.
Construction work has now started on the second phase to completely remodel Sulby Ward to include more single room and en-suite facilities and the development of a dedicated Teenage and Young Adult Unit. This four-bedded facility, which is on schedule to be completed by the end of July 2009, will accommodate patients aged 16-24 years, offering privacy and independence - as well as additional space for overnight stays by family members. The Centre is working in partnership with the Teenage Cancer Trust on the project.
We pride ourselves on leading the way when it comes to technological advances in modern radiotherapy treatments and it is a core value of the Trust to ‘put patients first’. In December we became the first cancer facility in the UK to offer patients a revolutionary radiotherapy treatment known as Rapidarc. The treatment significantly reduces patient treatment times.
We are also the only Trust in the UK to provide low energy proton treatments for eye cancers.New forms of proton treatment are now available to deal with other types of tumours and we are currently in discussion with the Department of Health seeking to negotiate a financial
5
Introduction
Chairman’s Statement
Reaching the end of the financial year 2008/09 is an opportune time to reflect on the work of the Trust during the course of the year.
I am pleased to report that Clatterbridge Centre for Oncology (CCO) continues to provide the highest quality clinical care possible and in recognition of this the Healthcare Commission has awarded the Trust its ‘excellent’ rating for both the quality of services and for the use of resources; the two areas it inspects for the year 2007/08 and we are confident that we will receive a similarly high rating for 2008/09. In addition, the Foundation Trust Regulator has awarded the organisation the highest ratings possible for the two key issues he monitors ie governance and finance.
CCO is achieving all the required NHS targets including 62 day waiting time target (urgent referral to treatment for all cancers) and the 18 week waiting time target (point of initial referral up to the start of any treatment). Infection control continues to present particular difficulties for this Centre because virtually all our patients are referred from other hospitals but I am pleased to report that MRSA bacteraemia infections have remained at zero throughout the year.
Furthermore, the Trust has achieved a strong balance sheet with a surplus of £4.45m, which has enabled us to develop a £3m investment programme to upgrade facilities and services at the centre.
In December 2008 Cherie Blair, who has agreed to champion our fundraising appeal, officially opened the new Out-Patient Department. The first completed phase of the investment plan. The new department includes state-of-the-art clinic rooms and patient waiting areas. A conservatory has also been built out into a landscaped water garden as an extension to the patient waiting area. The conservatory was funded by the Melanie Beattie Appeal, for which we are most grateful.
Construction work has now started on the second phase to completely remodel Sulby Ward to include more single room and en-suite facilities and the development of a dedicated Teenage and Young Adult Unit. This four-bedded facility, which is on schedule to be completed by the end of July 2009, will accommodate patients aged 16-24 years, offering privacy and independence - as well as additional space for overnight stays by family members. The Centre is working in partnership with the Teenage Cancer Trust on the project.
We pride ourselves on leading the way when it comes to technological advances in modern radiotherapy treatments and it is a core value of the Trust to ‘put patients first’. In December we became the first cancer facility in the UK to offer patients a revolutionary radiotherapy treatment known as Rapidarc. The treatment significantly reduces patient treatment times.
We are also the only Trust in the UK to provide low energy proton treatments for eye cancers.New forms of proton treatment are now available to deal with other types of tumours and we are currently in discussion with the Department of Health seeking to negotiate a financial
6
arrangement to provide and operate a very expensive proton treatment machine which will enable CCO to be the first Centre in the UK to provide these types of treatment. Proton therapy has significant benefits particularly for children and young people.
One of the key drivers for the Trust Board has been to try and deliver our services as near as possible to the patient. We already have seven chemotherapy clinics located in acute hospitals throughout Cheshire and Merseyside but all our radiotherapy is undertaken at the Clatterbridge site. With this in mind we will in the near future commence building a Satellite Radiotherapy Centre ‘Clatterbridge Cancer Centre – Liverpool’ on the Walton/Aintree Hospital site in North Liverpool. The cost of the project will be met by the Trust with the help of charitable funds. Our colleagues from the Marina Dalglish Appeal are working hard to raise a significant proportion of the money required to ensure that this facility opens at the end of 2010. Needless to say we are most grateful for all their hard work.
Clearly 2008/09 has been a productive year for the Trust. I am confident that with the support of our Governors and Members and the commitment and hard work of our Staff 2009/10 will prove to be equally demanding and successful.
Alan White - Chairman, Clatterbridge Centre for Oncology NHS Foundation Trust
7
Directors’ Report
Background Information
Clatterbridge Centre for Oncology was licensed as a Foundation Trust from 1st August 2006.Our vision as an NHS Foundation Trust is to provide ‘world class cancer care.’
Fundamental to our success in achieving our vision has been our focus on delivering our strategic objectives. These are:
To be the provider of choice for non-surgical (solid tumour) cancer services to the population of Cheshire and Merseyside. This is our core service.
To develop key partnerships that will further strengthen core business To remain the employer of choice for staff both within the local, general employment
market, and nationally for staff with specific expertise in cancer services To become an organisation that is fully responsive and accountable to its membership
Trust profile
Clatterbridge Centre for Oncology is one of the largest cancer centres in the UK – registering over 8,300 new patients each year and providing more than 131,000 attendances for treatment. In addition to the facilities provided on the main Clatterbridge site, many of our out-patient and treatment clinics are run in the surrounding general hospitals of Merseyside, Cheshire and the Isle of Man where we serve a population of 2.3 million.
We employ over 650 staff and volunteers and spend approximately £56m per year on all aspects of cancer treatment, diagnosis and care.
The cancer centre is located on the Clatterbridge Hospital site in Bebington, Wirral. Within the centre we provide a range of radiotherapy and chemotherapy treatments in out-patient and in-patient settings. We also provide out-patient consultations and support services.
The treatment centre has undergone significant financial investment over the past five years and now hosts one of the best equipped radiotherapy centres in the UK. Research and development, including participation in national and international clinical trials, is an important feature of the cancer centre.
6
arrangement to provide and operate a very expensive proton treatment machine which will enable CCO to be the first Centre in the UK to provide these types of treatment. Proton therapy has significant benefits particularly for children and young people.
One of the key drivers for the Trust Board has been to try and deliver our services as near as possible to the patient. We already have seven chemotherapy clinics located in acute hospitals throughout Cheshire and Merseyside but all our radiotherapy is undertaken at the Clatterbridge site. With this in mind we will in the near future commence building a Satellite Radiotherapy Centre ‘Clatterbridge Cancer Centre – Liverpool’ on the Walton/Aintree Hospital site in North Liverpool. The cost of the project will be met by the Trust with the help of charitable funds. Our colleagues from the Marina Dalglish Appeal are working hard to raise a significant proportion of the money required to ensure that this facility opens at the end of 2010. Needless to say we are most grateful for all their hard work.
Clearly 2008/09 has been a productive year for the Trust. I am confident that with the support of our Governors and Members and the commitment and hard work of our Staff 2009/10 will prove to be equally demanding and successful.
Alan White - Chairman, Clatterbridge Centre for Oncology NHS Foundation Trust
7
Directors’ Report
Background Information
Clatterbridge Centre for Oncology was licensed as a Foundation Trust from 1st August 2006.Our vision as an NHS Foundation Trust is to provide ‘world class cancer care.’
Fundamental to our success in achieving our vision has been our focus on delivering our strategic objectives. These are:
To be the provider of choice for non-surgical (solid tumour) cancer services to the population of Cheshire and Merseyside. This is our core service.
To develop key partnerships that will further strengthen core business To remain the employer of choice for staff both within the local, general employment
market, and nationally for staff with specific expertise in cancer services To become an organisation that is fully responsive and accountable to its membership
Trust profile
Clatterbridge Centre for Oncology is one of the largest cancer centres in the UK – registering over 8,300 new patients each year and providing more than 131,000 attendances for treatment. In addition to the facilities provided on the main Clatterbridge site, many of our out-patient and treatment clinics are run in the surrounding general hospitals of Merseyside, Cheshire and the Isle of Man where we serve a population of 2.3 million.
We employ over 650 staff and volunteers and spend approximately £56m per year on all aspects of cancer treatment, diagnosis and care.
The cancer centre is located on the Clatterbridge Hospital site in Bebington, Wirral. Within the centre we provide a range of radiotherapy and chemotherapy treatments in out-patient and in-patient settings. We also provide out-patient consultations and support services.
The treatment centre has undergone significant financial investment over the past five years and now hosts one of the best equipped radiotherapy centres in the UK. Research and development, including participation in national and international clinical trials, is an important feature of the cancer centre.
8
Operating & Financial Review (OFR)
Financial Summary
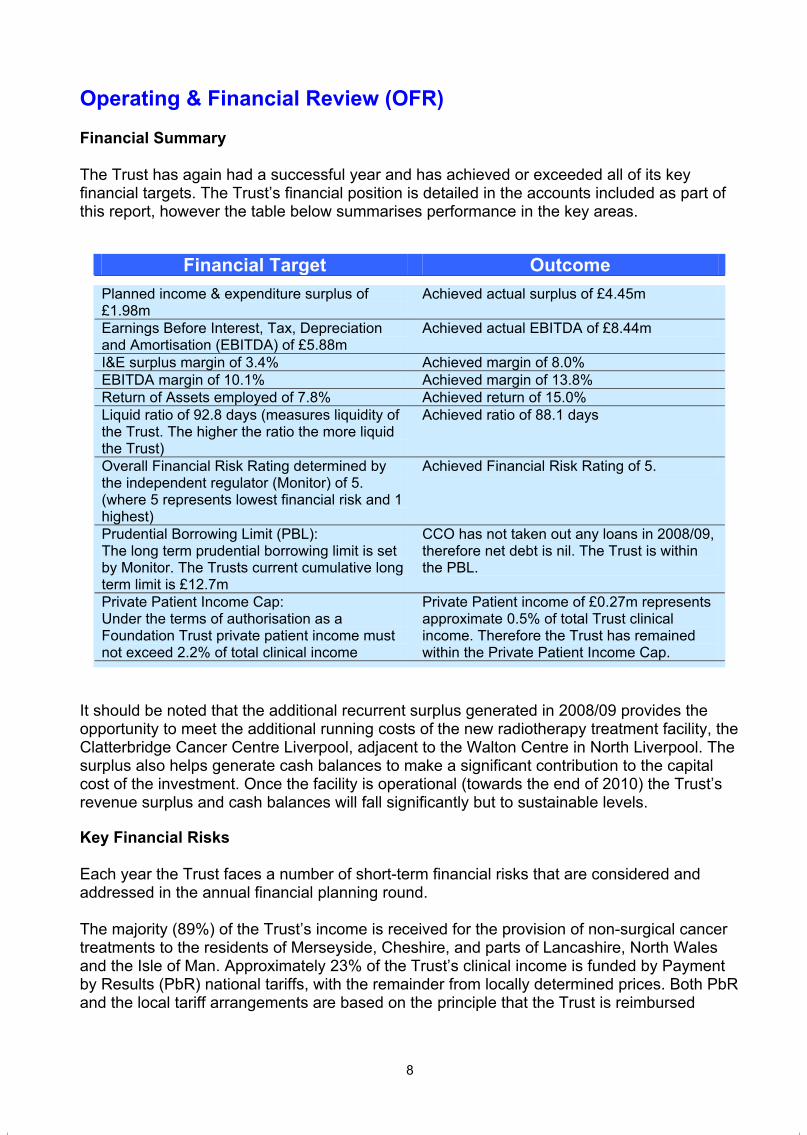
The Trust has again had a successful year and has achieved or exceeded all of its key financial targets. The Trust’s financial position is detailed in the accounts included as part of this report, however the table below summarises performance in the key areas.
Financial Target OutcomePlanned income & expenditure surplus of £1.98m
Achieved actual surplus of £4.45m
Earnings Before Interest, Tax, Depreciation and Amortisation (EBITDA) of £5.88m
Achieved actual EBITDA of £8.44m
I&E surplus margin of 3.4% Achieved margin of 8.0% EBITDA margin of 10.1% Achieved margin of 13.8% Return of Assets employed of 7.8% Achieved return of 15.0% Liquid ratio of 92.8 days (measures liquidity of the Trust. The higher the ratio the more liquid the Trust)
Achieved ratio of 88.1 days
Overall Financial Risk Rating determined by the independent regulator (Monitor) of 5. (where 5 represents lowest financial risk and 1 highest)
Achieved Financial Risk Rating of 5.
Prudential Borrowing Limit (PBL): The long term prudential borrowing limit is set by Monitor. The Trusts current cumulative long term limit is £12.7m
CCO has not taken out any loans in 2008/09, therefore net debt is nil. The Trust is within the PBL.
Private Patient Income Cap: Under the terms of authorisation as a Foundation Trust private patient income must not exceed 2.2% of total clinical income
Private Patient income of £0.27m represents approximate 0.5% of total Trust clinical income. Therefore the Trust has remained within the Private Patient Income Cap.
It should be noted that the additional recurrent surplus generated in 2008/09 provides the opportunity to meet the additional running costs of the new radiotherapy treatment facility, the Clatterbridge Cancer Centre Liverpool, adjacent to the Walton Centre in North Liverpool. The surplus also helps generate cash balances to make a significant contribution to the capital cost of the investment. Once the facility is operational (towards the end of 2010) the Trust’s revenue surplus and cash balances will fall significantly but to sustainable levels.
Key Financial Risks
Each year the Trust faces a number of short-term financial risks that are considered and addressed in the annual financial planning round.
The majority (89%) of the Trust’s income is received for the provision of non-surgical cancer treatments to the residents of Merseyside, Cheshire, and parts of Lancashire, North Wales and the Isle of Man. Approximately 23% of the Trust’s clinical income is funded by Payment by Results (PbR) national tariffs, with the remainder from locally determined prices. Both PbR and the local tariff arrangements are based on the principle that the Trust is reimbursed
9
based on activity performed. Therefore a reduction in activity levels represents a financial risk to the Trust, largely because most of the costs it incurs are fixed or semi-fixed for its foreseeable activity levels. However the Trust is able to mitigate in part against this risk by:
Employing contract tolerances to reduce in-year income volatility Agreeing local tariffs with commissioners for 77% of clinical income that are not,
therefore, subject to the same degree of price volatility as the nationally determined tariffs within Payment by Results.
Agreeing cancer drug developments to ensure drug funding based on actual drug usage.
Setting a prudent level of financial reserves and maintaining strong levels of liquidity
Another key financial risk is the delivery of the Trust’s cost improvement programme (CIP) and improvements in unit efficiency. However the target was achieved in 2008/09 and 75% of the 2009/10 programme has been identified.
In addition to the above, there are also a number of medium term risks that need to be kept under review, with appropriate action plans being developed and executed to manage any adverse consequences. It is becoming increasingly clear that the difficult economic outlook and the consequences for NHS funding, in particular beyond 2010/11, will pose a significant challenge to the Trust and its Commissioners as it seeks to deliver more and higher quality treatments in the future. The Trust will increase its efforts to deliver continuous improvements in its efficiency. The risk is increased to the extent that a significant part of the financial headroom will be removed due to the trust’s commitment in respect of the development of the Clatterbridge Cancer Centre Liverpool described above. Finally the policy direction of the Department of Health is to widen the scope of activity subject to national rather than local tariffs. Although it is unlikely that tariffs will be set for radiotherapy and the majority of chemotherapy before 2011/12 this may be a source of future income volatility.
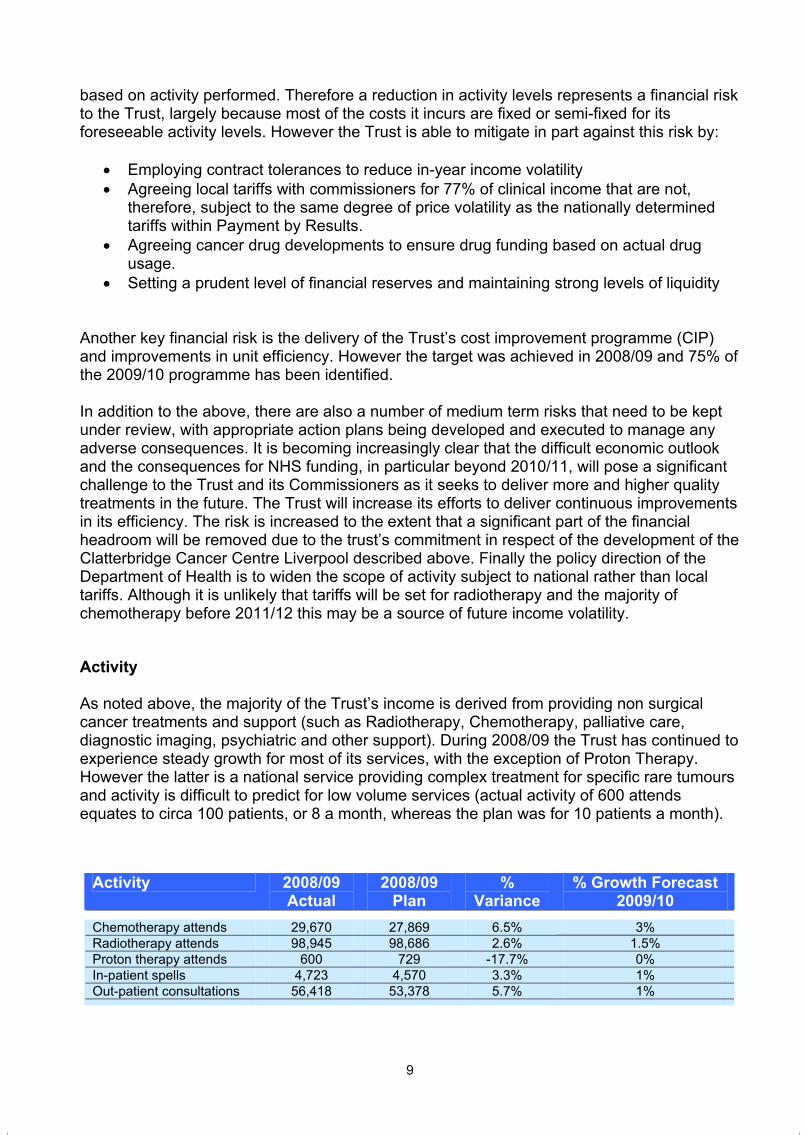
Activity
As noted above, the majority of the Trust’s income is derived from providing non surgical cancer treatments and support (such as Radiotherapy, Chemotherapy, palliative care, diagnostic imaging, psychiatric and other support). During 2008/09 the Trust has continued to experience steady growth for most of its services, with the exception of Proton Therapy. However the latter is a national service providing complex treatment for specific rare tumours and activity is difficult to predict for low volume services (actual activity of 600 attends equates to circa 100 patients, or 8 a month, whereas the plan was for 10 patients a month).
Activity 2008/09Actual
2008/09Plan
%Variance
% Growth Forecast 2009/10
Chemotherapy attends 29,670 27,869 6.5% 3%Radiotherapy attends 98,945 98,686 2.6% 1.5%Proton therapy attends 600 729 -17.7% 0%In-patient spells 4,723 4,570 3.3% 1%Out-patient consultations 56,418 53,378 5.7% 1%
8
Operating & Financial Review (OFR)
Financial Summary
The Trust has again had a successful year and has achieved or exceeded all of its key financial targets. The Trust’s financial position is detailed in the accounts included as part of this report, however the table below summarises performance in the key areas.
Financial Target OutcomePlanned income & expenditure surplus of £1.98m
Achieved actual surplus of £4.45m
Earnings Before Interest, Tax, Depreciation and Amortisation (EBITDA) of £5.88m
Achieved actual EBITDA of £8.44m
I&E surplus margin of 3.4% Achieved margin of 8.0% EBITDA margin of 10.1% Achieved margin of 13.8% Return of Assets employed of 7.8% Achieved return of 15.0% Liquid ratio of 92.8 days (measures liquidity of the Trust. The higher the ratio the more liquid the Trust)
Achieved ratio of 88.1 days
Overall Financial Risk Rating determined by the independent regulator (Monitor) of 5. (where 5 represents lowest financial risk and 1 highest)
Achieved Financial Risk Rating of 5.
Prudential Borrowing Limit (PBL): The long term prudential borrowing limit is set by Monitor. The Trusts current cumulative long term limit is £12.7m
CCO has not taken out any loans in 2008/09, therefore net debt is nil. The Trust is within the PBL.
Private Patient Income Cap: Under the terms of authorisation as a Foundation Trust private patient income must not exceed 2.2% of total clinical income
Private Patient income of £0.27m represents approximate 0.5% of total Trust clinical income. Therefore the Trust has remained within the Private Patient Income Cap.
It should be noted that the additional recurrent surplus generated in 2008/09 provides the opportunity to meet the additional running costs of the new radiotherapy treatment facility, the Clatterbridge Cancer Centre Liverpool, adjacent to the Walton Centre in North Liverpool. The surplus also helps generate cash balances to make a significant contribution to the capital cost of the investment. Once the facility is operational (towards the end of 2010) the Trust’s revenue surplus and cash balances will fall significantly but to sustainable levels.
Key Financial Risks
Each year the Trust faces a number of short-term financial risks that are considered and addressed in the annual financial planning round.
The majority (89%) of the Trust’s income is received for the provision of non-surgical cancer treatments to the residents of Merseyside, Cheshire, and parts of Lancashire, North Wales and the Isle of Man. Approximately 23% of the Trust’s clinical income is funded by Payment by Results (PbR) national tariffs, with the remainder from locally determined prices. Both PbR and the local tariff arrangements are based on the principle that the Trust is reimbursed
9
based on activity performed. Therefore a reduction in activity levels represents a financial risk to the Trust, largely because most of the costs it incurs are fixed or semi-fixed for its foreseeable activity levels. However the Trust is able to mitigate in part against this risk by:
Employing contract tolerances to reduce in-year income volatility Agreeing local tariffs with commissioners for 77% of clinical income that are not,
therefore, subject to the same degree of price volatility as the nationally determined tariffs within Payment by Results.
Agreeing cancer drug developments to ensure drug funding based on actual drug usage.
Setting a prudent level of financial reserves and maintaining strong levels of liquidity
Another key financial risk is the delivery of the Trust’s cost improvement programme (CIP) and improvements in unit efficiency. However the target was achieved in 2008/09 and 75% of the 2009/10 programme has been identified.
In addition to the above, there are also a number of medium term risks that need to be kept under review, with appropriate action plans being developed and executed to manage any adverse consequences. It is becoming increasingly clear that the difficult economic outlook and the consequences for NHS funding, in particular beyond 2010/11, will pose a significant challenge to the Trust and its Commissioners as it seeks to deliver more and higher quality treatments in the future. The Trust will increase its efforts to deliver continuous improvements in its efficiency. The risk is increased to the extent that a significant part of the financial headroom will be removed due to the trust’s commitment in respect of the development of the Clatterbridge Cancer Centre Liverpool described above. Finally the policy direction of the Department of Health is to widen the scope of activity subject to national rather than local tariffs. Although it is unlikely that tariffs will be set for radiotherapy and the majority of chemotherapy before 2011/12 this may be a source of future income volatility.
Activity
As noted above, the majority of the Trust’s income is derived from providing non surgical cancer treatments and support (such as Radiotherapy, Chemotherapy, palliative care, diagnostic imaging, psychiatric and other support). During 2008/09 the Trust has continued to experience steady growth for most of its services, with the exception of Proton Therapy. However the latter is a national service providing complex treatment for specific rare tumours and activity is difficult to predict for low volume services (actual activity of 600 attends equates to circa 100 patients, or 8 a month, whereas the plan was for 10 patients a month).
Activity 2008/09Actual
2008/09Plan
%Variance
% Growth Forecast 2009/10
Chemotherapy attends 29,670 27,869 6.5% 3%Radiotherapy attends 98,945 98,686 2.6% 1.5%Proton therapy attends 600 729 -17.7% 0%In-patient spells 4,723 4,570 3.3% 1%Out-patient consultations 56,418 53,378 5.7% 1%

10
Forecast growth is related to the increase in estimated numbers of our catchment population that are over 50 years of age, and is based on the same assumptions that underpin the Trust’s 5 year Service Development Strategy and 3 year Forward Plan.
Other Income and Non-healthcare Activities
As noted above, the majority of the Trust’s income is derived from providing clinical cancer services. In addition, the remaining 11% of income is derived from:
Undertaking research & development Education and training External drug sales to the private sector Hosting non-clinical services, such as the National Cancer Services Analysis Team. In
CCO’s accounts income for these services matches expenditure and therefore there is no impact on the Trust’s EBITDA and overall I&E surplus.
Support from charities and recharges to other NHS and non-NHS bodies.
Investment Activity
The Trust invested just under £2 million in new and replacement capital equipment and building refurbishment in 2008/09. The main schemes were:
£0.9m for Clatterbridge Cancer Centre – Liverpool. As noted under Post Balance Sheet Events above the total cost of this scheme is forecast to be £17.5m, and the new Centre is expected to open in December 2010. It will increase the Trust’s capacity to deliver radiotherapy treatments to meet increasing forecast demand as well as providing access to services closer to a significant proportion of the Trust’s population.
£0.5m to improve outpatient facilities, increase accommodation and maintain the good physical condition of the Trust’s estate.
£0.2m commencing works for Sulby ward refurbishment. The Trust is committed to spend a further £1.25m in 2009/10 to complete the project, which includes the construction of a dedicated Teenage and Young Adult unit (see note 20 in the Trust’s Annual Accounts).
£0.2m to replace a Cobalt source for Cobalt treatment machine.
All of the above represented investments in assets that are protected to deliver cancer services to our patients as part of the core business of the Trust, with the expectation that the improvements will build on the existing high standard of care provided.
In addition to completing the Sulby / Teenage & Young Adult Unit and continuing with the Clatterbridge Cancer Centre – Liverpool, the Trust is planning further capital expenditure in 2009/10 to commence the next phase of the ward refurbishment programme, and continue with its on-going equipment replacement programme. Capital investment will be made to enable the expansion of the stereotactic radio-surgery service in partnership with the Walton
11
Centre for Neurology & Neurosurgery NHS Trust. A number of projects are also planned to improve Information Management and Technology services and systems at the Trust.
In the longer term the Trust’s plans for capital investments include:
Refurbish the remaining wards on the Clatterbridge site Rationalise the estate to reduce the number of modular buildings , improve storage &
office capacity To evaluate the case for a second radiotherapy treatment centre in Liverpool, in
conjunction with the Cancer Network, commissioners and the Royal Liverpool University & Broadgreen Hospitals NHS Trust. This may take the form of a Trust response to a tender for radiotherapy services led by Liverpool PCT
Working in partnership with the Royal Liverpool University Hospital and the University of Liverpool to develop an Academic Oncology Centre
Develop an evaluation of the Trust’s options in respect of providing a high-energy proton therapy service if the Department of Health seek to establish such a facility in England.
Accounting Policies
There have been no significant changes to the Trust’s accounting policies from those in 2007/08. A comprehensive list of the accounting policies are included as part of the Annual Accounts.
Charitable Funding
The Board of CCO are also the Corporate Trustee of Clatterbridge Centre for Oncology Charitable Funds. During 2008/09, £142,949 has been spent by the charity in support of the Foundation Trust. The main areas of expenditure were:
Contribution to capital - refurbishment of outpatients department £35,000 Research & development - £104,876 Improving patients welfare - £1,110 Improving staff welfare - £1,963
Going Concern
The following financial accounts statements have been prepared on a going concern basis. After making enquiries the directors have a reasonable expectation that the NHS Foundation Trust has adequate resources to continue in operational existence for the foreseeable future. For this reason they continue to adopt the going concern basis in preparing the accounts.
10
Forecast growth is related to the increase in estimated numbers of our catchment population that are over 50 years of age, and is based on the same assumptions that underpin the Trust’s 5 year Service Development Strategy and 3 year Forward Plan.
Other Income and Non-healthcare Activities
As noted above, the majority of the Trust’s income is derived from providing clinical cancer services. In addition, the remaining 11% of income is derived from:
Undertaking research & development Education and training External drug sales to the private sector Hosting non-clinical services, such as the National Cancer Services Analysis Team. In
CCO’s accounts income for these services matches expenditure and therefore there is no impact on the Trust’s EBITDA and overall I&E surplus.
Support from charities and recharges to other NHS and non-NHS bodies.
Investment Activity
The Trust invested just under £2 million in new and replacement capital equipment and building refurbishment in 2008/09. The main schemes were:
£0.9m for Clatterbridge Cancer Centre – Liverpool. As noted under Post Balance Sheet Events above the total cost of this scheme is forecast to be £17.5m, and the new Centre is expected to open in December 2010. It will increase the Trust’s capacity to deliver radiotherapy treatments to meet increasing forecast demand as well as providing access to services closer to a significant proportion of the Trust’s population.
£0.5m to improve outpatient facilities, increase accommodation and maintain the good physical condition of the Trust’s estate.
£0.2m commencing works for Sulby ward refurbishment. The Trust is committed to spend a further £1.25m in 2009/10 to complete the project, which includes the construction of a dedicated Teenage and Young Adult unit (see note 20 in the Trust’s Annual Accounts).
£0.2m to replace a Cobalt source for Cobalt treatment machine.
All of the above represented investments in assets that are protected to deliver cancer services to our patients as part of the core business of the Trust, with the expectation that the improvements will build on the existing high standard of care provided.
In addition to completing the Sulby / Teenage & Young Adult Unit and continuing with the Clatterbridge Cancer Centre – Liverpool, the Trust is planning further capital expenditure in 2009/10 to commence the next phase of the ward refurbishment programme, and continue with its on-going equipment replacement programme. Capital investment will be made to enable the expansion of the stereotactic radio-surgery service in partnership with the Walton
11
Centre for Neurology & Neurosurgery NHS Trust. A number of projects are also planned to improve Information Management and Technology services and systems at the Trust.
In the longer term the Trust’s plans for capital investments include:
Refurbish the remaining wards on the Clatterbridge site Rationalise the estate to reduce the number of modular buildings , improve storage &
office capacity To evaluate the case for a second radiotherapy treatment centre in Liverpool, in
conjunction with the Cancer Network, commissioners and the Royal Liverpool University & Broadgreen Hospitals NHS Trust. This may take the form of a Trust response to a tender for radiotherapy services led by Liverpool PCT
Working in partnership with the Royal Liverpool University Hospital and the University of Liverpool to develop an Academic Oncology Centre
Develop an evaluation of the Trust’s options in respect of providing a high-energy proton therapy service if the Department of Health seek to establish such a facility in England.
Accounting Policies
There have been no significant changes to the Trust’s accounting policies from those in 2007/08. A comprehensive list of the accounting policies are included as part of the Annual Accounts.
Charitable Funding
The Board of CCO are also the Corporate Trustee of Clatterbridge Centre for Oncology Charitable Funds. During 2008/09, £142,949 has been spent by the charity in support of the Foundation Trust. The main areas of expenditure were:
Contribution to capital - refurbishment of outpatients department £35,000 Research & development - £104,876 Improving patients welfare - £1,110 Improving staff welfare - £1,963
Going Concern
The following financial accounts statements have been prepared on a going concern basis. After making enquiries the directors have a reasonable expectation that the NHS Foundation Trust has adequate resources to continue in operational existence for the foreseeable future. For this reason they continue to adopt the going concern basis in preparing the accounts.
12
Patient Care Using our freedoms as an NHS Foundation Trust
The principle way that the Trust has sought to exploit the opportunities afforded to it as a Foundation Trust is through the development of its plans to build a satellite radiotherapy unit adjacent to the Walton Centre for Neurology & Neurosurgery NHS Trust on the Aintree Hospital campus in North Liverpool. The proposed investment is for the establishment of an ambulatory radiotherapy treatment facility at an estimated capital cost of some £17.5m. A decision by the Board to proceed is anticipated in early May 2009.
The facility is expected to be operational by the end of 2010. It will provide accessible services to a significant proportion of the Trust's catchment population North of the River Mersey, who currently have to travel to the Wirral. The service will continue to provide high quality treatment services and a patient experience (e.g. adjacent free car parking, pleasant environment) equivalent to that in place at CCO.
Foundation Trust freedoms have been critical to the proposal in a number of ways. These include; the ability to generate significant revenue surpluses to finance a significant proportion of the investment and retain the cash generated until it is required and access to the Foundation Trust Financing Facility to obtain a loan. However the most significant issue is the autonomy that the Trust is able to exercise in deciding that this is a high priority investment. Due to the size of the proposed investment relative to the organisation's turnover the Regulator will need to assess the impact on the Trust's Financial Risk Rating. However Monitor will not pass judgement on the service need for the investment. This is a matter for the Board. This degree of oversight/approval processes is in contrast that the Trust would have been subject to before achieving FT status.
Performance against key targets 2008/09
As of January 1st 2009, the Cancer Reform targets were introduced which changed the reported performance levels for both the 31 day and 62 day cancer waiting times targets, in order to align them with the 18 week pause model. That is, the majority of usable adjustments, such as patient thinking time, time out for patient holidays, medical suspensions, were removed. The impact of this was that reported performance was seen to drop significantly, even though in reality patients were being seen and treated just as quickly as before.
Since the target rationales were changed in the last quarter, with as yet no criteria set for the new targets, the following is the performance related to the first three quarters of the year, upon which it is expected that performance achievement will be considered:
All patients who had suspected cancer and were referred urgently by their G.P.’s were seen within 14 days.
99.8% of patients were treated within 31 days from the time of decision to treat (target threshold 98%).
93.3% of patients were treated within 62 days from the date of urgent GP referral (target threshold 93%).
13
No patient has waited longer than 6 weeks (target 13 weeks) for Imaging (CT and MRI at CCO).
We have had no incidence of a MRSA bacteraemia (our target is no more than 2).
The following is the performance for the full year:
As at March 2009 97.3% of new admitted patients were seen within 18 weeks from there initial GP referral to being admitted for their treatment, this compares very favourably against the national requirement against this target of 90% . (This measure includes the entire pathway that the patient goes through e.g. outpatients, diagnostic tests and inpatient treatment).
For non admitted patients 98.5% of newly referred patients were seen within 18 weeks, again this compares very favourably with the national standard for this target which stands at 95%.
The 62-day cancer waiting time standard
The Trust has worked particularly hard to deliver the 62-days Cancer Waiting time standard. This standard is a particular challenge for CCO as a tertiary provider of services. The improvement in performance is evidence of the effective management of the patient pathway and co-operation with secondary care Trusts that make referrals to CCO.
The achievement of the 62 day waiting time standard has remained a high priority for the Trust, this target monitors the maximum waiting time for suspicion of cancer patients from the point of urgent GP referral to the start of treatment.
Considerable effort has been put in across the Trust in achieving this target, similarly we have worked hard to build effective working relations with partner NHS Trusts who refer patients into the Trust, to help ensure that patients are referred to us as quickly as possible.
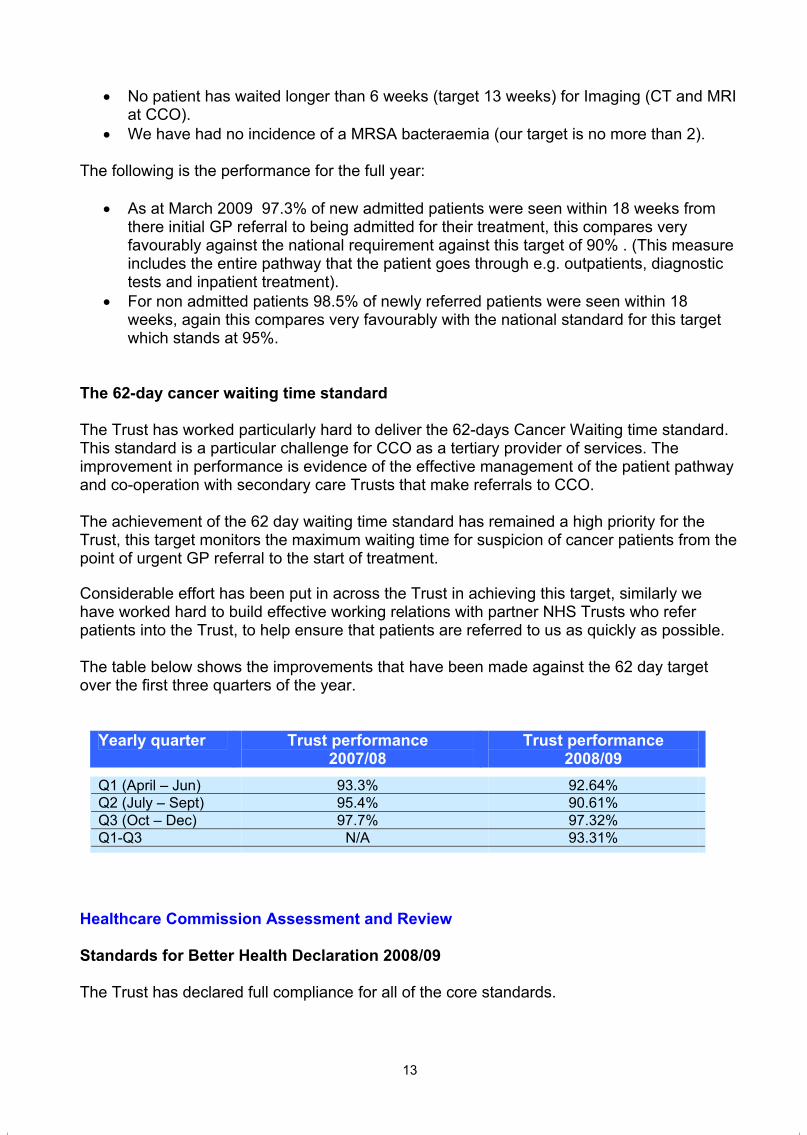
The table below shows the improvements that have been made against the 62 day target over the first three quarters of the year.
Yearly quarter Trust performance2007/08
Trust performance 2008/09
Q1 (April – Jun) 93.3% 92.64%Q2 (July – Sept) 95.4% 90.61%Q3 (Oct – Dec) 97.7% 97.32%Q1-Q3 N/A 93.31%
Healthcare Commission Assessment and Review
Standards for Better Health Declaration 2008/09
The Trust has declared full compliance for all of the core standards.
12
Patient Care Using our freedoms as an NHS Foundation Trust
The principle way that the Trust has sought to exploit the opportunities afforded to it as a Foundation Trust is through the development of its plans to build a satellite radiotherapy unit adjacent to the Walton Centre for Neurology & Neurosurgery NHS Trust on the Aintree Hospital campus in North Liverpool. The proposed investment is for the establishment of an ambulatory radiotherapy treatment facility at an estimated capital cost of some £17.5m. A decision by the Board to proceed is anticipated in early May 2009.
The facility is expected to be operational by the end of 2010. It will provide accessible services to a significant proportion of the Trust's catchment population North of the River Mersey, who currently have to travel to the Wirral. The service will continue to provide high quality treatment services and a patient experience (e.g. adjacent free car parking, pleasant environment) equivalent to that in place at CCO.
Foundation Trust freedoms have been critical to the proposal in a number of ways. These include; the ability to generate significant revenue surpluses to finance a significant proportion of the investment and retain the cash generated until it is required and access to the Foundation Trust Financing Facility to obtain a loan. However the most significant issue is the autonomy that the Trust is able to exercise in deciding that this is a high priority investment. Due to the size of the proposed investment relative to the organisation's turnover the Regulator will need to assess the impact on the Trust's Financial Risk Rating. However Monitor will not pass judgement on the service need for the investment. This is a matter for the Board. This degree of oversight/approval processes is in contrast that the Trust would have been subject to before achieving FT status.
Performance against key targets 2008/09
As of January 1st 2009, the Cancer Reform targets were introduced which changed the reported performance levels for both the 31 day and 62 day cancer waiting times targets, in order to align them with the 18 week pause model. That is, the majority of usable adjustments, such as patient thinking time, time out for patient holidays, medical suspensions, were removed. The impact of this was that reported performance was seen to drop significantly, even though in reality patients were being seen and treated just as quickly as before.
Since the target rationales were changed in the last quarter, with as yet no criteria set for the new targets, the following is the performance related to the first three quarters of the year, upon which it is expected that performance achievement will be considered:
All patients who had suspected cancer and were referred urgently by their G.P.’s were seen within 14 days.
99.8% of patients were treated within 31 days from the time of decision to treat (target threshold 98%).
93.3% of patients were treated within 62 days from the date of urgent GP referral (target threshold 93%).
13
No patient has waited longer than 6 weeks (target 13 weeks) for Imaging (CT and MRI at CCO).
We have had no incidence of a MRSA bacteraemia (our target is no more than 2).
The following is the performance for the full year:
As at March 2009 97.3% of new admitted patients were seen within 18 weeks from there initial GP referral to being admitted for their treatment, this compares very favourably against the national requirement against this target of 90% . (This measure includes the entire pathway that the patient goes through e.g. outpatients, diagnostic tests and inpatient treatment).
For non admitted patients 98.5% of newly referred patients were seen within 18 weeks, again this compares very favourably with the national standard for this target which stands at 95%.
The 62-day cancer waiting time standard
The Trust has worked particularly hard to deliver the 62-days Cancer Waiting time standard. This standard is a particular challenge for CCO as a tertiary provider of services. The improvement in performance is evidence of the effective management of the patient pathway and co-operation with secondary care Trusts that make referrals to CCO.
The achievement of the 62 day waiting time standard has remained a high priority for the Trust, this target monitors the maximum waiting time for suspicion of cancer patients from the point of urgent GP referral to the start of treatment.
Considerable effort has been put in across the Trust in achieving this target, similarly we have worked hard to build effective working relations with partner NHS Trusts who refer patients into the Trust, to help ensure that patients are referred to us as quickly as possible.
The table below shows the improvements that have been made against the 62 day target over the first three quarters of the year.
Yearly quarter Trust performance2007/08
Trust performance 2008/09
Q1 (April – Jun) 93.3% 92.64%Q2 (July – Sept) 95.4% 90.61%Q3 (Oct – Dec) 97.7% 97.32%Q1-Q3 N/A 93.31%
Healthcare Commission Assessment and Review
Standards for Better Health Declaration 2008/09
The Trust has declared full compliance for all of the core standards.

14
Healthcare Commission Performance Ratings 2007/08
The Healthcare Commission performance ratings for 2007/08 were published in the autumn of 2008. The ratings are derived from a wide range of indicators and are summarised to a rating on two categories; quality of services and use of resources.
Quality of Services: Excellent
This rating ranks the Trust higher than the average in England. The overall rating is a consolidation of the following areas:
Component Rating
Meeting core standards Fully Met Existing national targets Fully met New national targets Excellent
The rating for existing national targets reflects the particularly difficult challenge the Trust faced in respect of achieving a maximum waiting time of two months from urgent GP referral to treatment for all cancers.
Use of Resources: Excellent
The Trust achieved the best available ranking which is based on Monitor’s assessment of the Trust’s financial performance for the year.
Healthcare Commission inspection: Hygiene Code
In September 2008 Trust received a planned inspection from the Healthcare Commission in relation to compliance with the Hygiene Code. Overall the report was positive however a breach was identified against Duty 4: “The trust must provide and maintain a clean and appropriate environment for healthcare”. Immediate steps were taken and all areas were rectified. The Trust was then able to declare full compliance with the Hygiene Code in its application for registration with the care Quality Commission.
Independent Risk Management Assessments
Achievement of NHSLA level 3
In November 2007 the Trust was successfully assessed against NHSLA level 3 (the highest available) and became the second Trust in the country (not including the pilot Trusts) to gain this level of attainment. The assessment reflects the Trust’s robust risk management systems and processes and the extent to which a risk aware culture is embedded in the organisation.
15
Maintenance of ISO 9001:2000 Standard
The ISO 9001:2000 Standard is a national (externally assessed) standard based around the principles of customer satisfaction, a systematic approach to management, and encouraging a culture of continual improvement across all departments within the Trust.
CCO is thought to have been the first NHS Trust to achieve this accreditation for the organisation as a whole. The accreditation is reviewed periodically and it is pleasing to report that it has been retained throughout 2008/09.
Developing our services
Radiotherapy
Radiotherapy continues to be busy with 9 Linear Accelerators and a cobalt unit all operational. During 2008 CCO was the first UK centre to treat patients using RapidArc which has been installed on one of the Varian Linacs and enables some patients to be treated with a very fast Intensity Modulated Radiotherapy technique significantly reducing the time they have to spend on the treatment couch. The use of this technology is currently being expanded into other anatomical sites.
The radiotherapy development on the Walton / Aintree site is progressing with detailed building plans having been developed with multi-disciplinary engagement. The business case having been accepted by the Trust Board in April 2009 is with Monitor for approval and it is anticipated that building works will begin very soon. It is anticipated that a radiotherapy service will commence at the end of 2010.
The Therapy Radiography workforce at CCO is currently being re-structured with an emphasis on improving services for patients, the introduction of the 4 tier model and improving career progression for staff.
Chemotherapy
The Trust is committed to delivering chemotherapy treatments as close as possible to the patient. A significant proportion of the Trust’s chemotherapy service is already delivered by CCO from District General Hospitals in the cancer network. However the Trust is committed to building up capacity at these treatment clinics across Cheshire and Merseyside, addressing the tension inherent within the requirement to deliver a uniformly high quality of service whilst at the same time delivering this service as close to patients as possible.
In support of enhancing our chemotherapy services, CCO has:
Nurse led clinics have been implemented across all clinics and across all major treatment pathways.
The new role for Nurse Clinicians has been discussed, and training analysis for such post is underway, this will improve the patient pathway, and reduce pressures on Clinicians

14
Healthcare Commission Performance Ratings 2007/08
The Healthcare Commission performance ratings for 2007/08 were published in the autumn of 2008. The ratings are derived from a wide range of indicators and are summarised to a rating on two categories; quality of services and use of resources.
Quality of Services: Excellent
This rating ranks the Trust higher than the average in England. The overall rating is a consolidation of the following areas:
Component Rating
Meeting core standards Fully Met Existing national targets Fully met New national targets Excellent
The rating for existing national targets reflects the particularly difficult challenge the Trust faced in respect of achieving a maximum waiting time of two months from urgent GP referral to treatment for all cancers.
Use of Resources: Excellent
The Trust achieved the best available ranking which is based on Monitor’s assessment of the Trust’s financial performance for the year.
Healthcare Commission inspection: Hygiene Code
In September 2008 Trust received a planned inspection from the Healthcare Commission in relation to compliance with the Hygiene Code. Overall the report was positive however a breach was identified against Duty 4: “The trust must provide and maintain a clean and appropriate environment for healthcare”. Immediate steps were taken and all areas were rectified. The Trust was then able to declare full compliance with the Hygiene Code in its application for registration with the care Quality Commission.
Independent Risk Management Assessments
Achievement of NHSLA level 3
In November 2007 the Trust was successfully assessed against NHSLA level 3 (the highest available) and became the second Trust in the country (not including the pilot Trusts) to gain this level of attainment. The assessment reflects the Trust’s robust risk management systems and processes and the extent to which a risk aware culture is embedded in the organisation.
15
Maintenance of ISO 9001:2000 Standard
The ISO 9001:2000 Standard is a national (externally assessed) standard based around the principles of customer satisfaction, a systematic approach to management, and encouraging a culture of continual improvement across all departments within the Trust.
CCO is thought to have been the first NHS Trust to achieve this accreditation for the organisation as a whole. The accreditation is reviewed periodically and it is pleasing to report that it has been retained throughout 2008/09.
Developing our services
Radiotherapy
Radiotherapy continues to be busy with 9 Linear Accelerators and a cobalt unit all operational. During 2008 CCO was the first UK centre to treat patients using RapidArc which has been installed on one of the Varian Linacs and enables some patients to be treated with a very fast Intensity Modulated Radiotherapy technique significantly reducing the time they have to spend on the treatment couch. The use of this technology is currently being expanded into other anatomical sites.
The radiotherapy development on the Walton / Aintree site is progressing with detailed building plans having been developed with multi-disciplinary engagement. The business case having been accepted by the Trust Board in April 2009 is with Monitor for approval and it is anticipated that building works will begin very soon. It is anticipated that a radiotherapy service will commence at the end of 2010.
The Therapy Radiography workforce at CCO is currently being re-structured with an emphasis on improving services for patients, the introduction of the 4 tier model and improving career progression for staff.
Chemotherapy
The Trust is committed to delivering chemotherapy treatments as close as possible to the patient. A significant proportion of the Trust’s chemotherapy service is already delivered by CCO from District General Hospitals in the cancer network. However the Trust is committed to building up capacity at these treatment clinics across Cheshire and Merseyside, addressing the tension inherent within the requirement to deliver a uniformly high quality of service whilst at the same time delivering this service as close to patients as possible.
In support of enhancing our chemotherapy services, CCO has:
Nurse led clinics have been implemented across all clinics and across all major treatment pathways.
The new role for Nurse Clinicians has been discussed, and training analysis for such post is underway, this will improve the patient pathway, and reduce pressures on Clinicians
16
Continued to work with Commissioners to ensure access to evidence based treatment regimes.
Appointed to the new post of Chemotherapy Service Manager to lead on the development of the service
Begun to implement new Service Level Agreements (SLAs) with our partner organisations to deliver increased treatment capacity, improved patient environment, appropriate staff facilities and support for our doctors and nurses working out-with the CCO centre.
New chemotherapy satellite established at Halton, all North Cheshire patients are now treated in this purpose built/modeled unit, enhancing the patient experience.
Repatriation of patients to local DGH satellite clinics has taken place, with additional provision planned at the Liverpool Women’s Hospital and at the Liverpool Heart and Chest Hospital.
Development of a stand alone Triage Service has commenced Telephone follow up service commenced for all new patients who receive a phone call
within 24 hours of receiving first chemotherapy intervention Pre-assessment clinics commenced to reduce waiting times, and to improve
communication and information giving to patients prior to chemotherapy. Links have been developed with Christie Hospital, and partnership working and
collaboration is progressing well. Posters and presentations have been delivered at a number of events across the
region and nationally, and more are planned to continue to raise the profile of CCO.
Diagnostic Imaging
Diagnostic Imaging has continued to play a key role in providing a range of services to support the core services of radiotherapy and chemotherapy. Activity levels have generally remained consistent, although a worldwide shortage of radioisotopes between September 2008 and February 2009 resulted in a slight reduction in activity in Nuclear Medicine. Waiting times have consistently reached the national target of less than 6 weeks. A large number of patients taking part in clinical trials have undergone imaging investigations.
A PET/ CT scanning service for patients across Cheshire and Merseyside commenced at CCO in April 2008, as part of the national agreement for provision of diagnostic services. Currently, a mobile facility provided by Alliance Medical Ltd (AML) visits once a week, although there are plans to increase the frequency of visits to meet the increasing demand for this service and consideration is being given to improving this service by provision of a static facility in the future. Clinicians across Cheshire and Merseyside have been able to refer their patients for PET/CT scans, which were not available in the North West beforehand.
Trust staff have been working closely with AML staff to ensure that the service is well integrated, sharing some Trust patient facilities. It has been well received by patients, as demonstrated by the results of satisfaction surveys carried out by AML.
Dr Christopher Romaniuk, one of our Consultant Radiologists plays a key role in the local team providing reporting services. He is also the Administration of Radioactive Substances Advisory Committee (ARSAC) certificate holder for CCO, offering advice and ensuring that safe practices are followed.
17
The third Consultant radiologist took up post in July 2008. Unfortunately, the full effect of this additional appointment has not been fully felt, as it coincided with additional commitments arising for the existing Consultant radiologists, such as PET/CT reporting. Requirements for the future are currently being considered.
An agreement with Wirral Primary Care Trust has for provision of diagnostic imaging services has greatly improved access for patients referred by local General Practitioners and Intermediate Services. This agreement has resulted in some additional income being generated for the Trust. Early availability of diagnostic results has resulted in many more patients being cared for in the primary care setting and others being referred to secondary care, already having had a diagnosis made.
Developing our Workforce
The Trust has developed an organisational development strategy that set out our approach to issues such as leadership, workforce engagement and other aspects of how we manage and develop our people. Clear goals were outlined within the strategy and progress has been made in a number of areas.
Work has continued, and significant progress made, on embedding the core values that have been developed through engagement with our workforce. The values now play a core part in Trust processes and inform decisions made around recruitment, induction, staff awards and internal communication channels. The Trust was selected by the Department of Health as one of five organisations to feature in a promotional DVD on ‘Values led organisations’.
The Trust has become a member of the NHS Northwest Leadership Academy and has ensured participation in each development programme launched. We have reviewed and further developed our internally created and managed Key Skills for Managers programme and have now had a total of 68 first and second line management participants.
The Trust has also begun a programme of initiatives around employee health & wellbeing, which has seen free health checks, nutritional advice, complementary therapies and a stress awareness campaign.
Supporting a strategy to provide managers with the right tools to enable effective management of their people, the Trust successfully implemented the Electronic Staff Record and rapidly completed a subsequent assessment that demonstrated appropriate use of the system.
HSJ Awards
The Chief Executive and Director of HR travelled to London with 8 other members of the Clatterbridge team on 2nd March to accept the Trust’s place in the HSJ’s Top 100 Healthcare employers list.
The list has been compiled to identify the top healthcare providers to work for in the UK and was open to both NHS and independent healthcare providers. Out of the 100 companies short listed for the awards Clatterbridge Centre for Oncology ranked 40th in the overall list.
16
Continued to work with Commissioners to ensure access to evidence based treatment regimes.
Appointed to the new post of Chemotherapy Service Manager to lead on the development of the service
Begun to implement new Service Level Agreements (SLAs) with our partner organisations to deliver increased treatment capacity, improved patient environment, appropriate staff facilities and support for our doctors and nurses working out-with the CCO centre.
New chemotherapy satellite established at Halton, all North Cheshire patients are now treated in this purpose built/modeled unit, enhancing the patient experience.
Repatriation of patients to local DGH satellite clinics has taken place, with additional provision planned at the Liverpool Women’s Hospital and at the Liverpool Heart and Chest Hospital.
Development of a stand alone Triage Service has commenced Telephone follow up service commenced for all new patients who receive a phone call
within 24 hours of receiving first chemotherapy intervention Pre-assessment clinics commenced to reduce waiting times, and to improve
communication and information giving to patients prior to chemotherapy. Links have been developed with Christie Hospital, and partnership working and
collaboration is progressing well. Posters and presentations have been delivered at a number of events across the
region and nationally, and more are planned to continue to raise the profile of CCO.
Diagnostic Imaging
Diagnostic Imaging has continued to play a key role in providing a range of services to support the core services of radiotherapy and chemotherapy. Activity levels have generally remained consistent, although a worldwide shortage of radioisotopes between September 2008 and February 2009 resulted in a slight reduction in activity in Nuclear Medicine. Waiting times have consistently reached the national target of less than 6 weeks. A large number of patients taking part in clinical trials have undergone imaging investigations.
A PET/ CT scanning service for patients across Cheshire and Merseyside commenced at CCO in April 2008, as part of the national agreement for provision of diagnostic services. Currently, a mobile facility provided by Alliance Medical Ltd (AML) visits once a week, although there are plans to increase the frequency of visits to meet the increasing demand for this service and consideration is being given to improving this service by provision of a static facility in the future. Clinicians across Cheshire and Merseyside have been able to refer their patients for PET/CT scans, which were not available in the North West beforehand.
Trust staff have been working closely with AML staff to ensure that the service is well integrated, sharing some Trust patient facilities. It has been well received by patients, as demonstrated by the results of satisfaction surveys carried out by AML.
Dr Christopher Romaniuk, one of our Consultant Radiologists plays a key role in the local team providing reporting services. He is also the Administration of Radioactive Substances Advisory Committee (ARSAC) certificate holder for CCO, offering advice and ensuring that safe practices are followed.
17
The third Consultant radiologist took up post in July 2008. Unfortunately, the full effect of this additional appointment has not been fully felt, as it coincided with additional commitments arising for the existing Consultant radiologists, such as PET/CT reporting. Requirements for the future are currently being considered.
An agreement with Wirral Primary Care Trust has for provision of diagnostic imaging services has greatly improved access for patients referred by local General Practitioners and Intermediate Services. This agreement has resulted in some additional income being generated for the Trust. Early availability of diagnostic results has resulted in many more patients being cared for in the primary care setting and others being referred to secondary care, already having had a diagnosis made.
Developing our Workforce
The Trust has developed an organisational development strategy that set out our approach to issues such as leadership, workforce engagement and other aspects of how we manage and develop our people. Clear goals were outlined within the strategy and progress has been made in a number of areas.
Work has continued, and significant progress made, on embedding the core values that have been developed through engagement with our workforce. The values now play a core part in Trust processes and inform decisions made around recruitment, induction, staff awards and internal communication channels. The Trust was selected by the Department of Health as one of five organisations to feature in a promotional DVD on ‘Values led organisations’.
The Trust has become a member of the NHS Northwest Leadership Academy and has ensured participation in each development programme launched. We have reviewed and further developed our internally created and managed Key Skills for Managers programme and have now had a total of 68 first and second line management participants.
The Trust has also begun a programme of initiatives around employee health & wellbeing, which has seen free health checks, nutritional advice, complementary therapies and a stress awareness campaign.
Supporting a strategy to provide managers with the right tools to enable effective management of their people, the Trust successfully implemented the Electronic Staff Record and rapidly completed a subsequent assessment that demonstrated appropriate use of the system.
HSJ Awards
The Chief Executive and Director of HR travelled to London with 8 other members of the Clatterbridge team on 2nd March to accept the Trust’s place in the HSJ’s Top 100 Healthcare employers list.
The list has been compiled to identify the top healthcare providers to work for in the UK and was open to both NHS and independent healthcare providers. Out of the 100 companies short listed for the awards Clatterbridge Centre for Oncology ranked 40th in the overall list.
18
Service improvements following staff or patient surveys or comments and Healthcare Commission reports
55% of CCO staff responded to the 2008 staff survey, which noted that the Trust scored in the top 20% of all acute specialist trusts nationally in 22 of the 36 key areas. The Trust continually reviews the survey results and implements service improvements accordingly. Such developments have included a review of the Performance & Development Review process (leading to a significantly increased completion rate), the development of a Stress working group and the introduction of trained ‘mentors’ to support anyone who has concerns about unacceptable behavior in the workplace.
In the 2008 Healthcare / Care Quality Commission in-patient survey the Trust scored in the top 20% of all acute Trusts nationally in 53 out of the 62 key areas. For 10 areas we scored the top score achieved by any Trust. The Trust will continue to monitor patients experience throughout the year and aim to continually improve on current performance. CCO has also put into place an internal survey where we offer all patients who complete a course of treatment or in-patient stay the opportunity to provide feedback in ‘real time’. Further information on the survey results are contained within the Quality Report.
As a result of the information obtained in these surveys we have greatly improved our processes for ensuring that patients and their GPs receive appropriate discharge information, whilst we are aiming to minimise patient waiting times within the departments we have put in place free tea and coffee through our volunteer service to improve the patients experience whilst waiting. We have also increased the availability of our hand and foot massage service to patients in the radiotherapy department and have revised what refreshments are on offer in our coffee bar facilities and have improved the environment in relation to privacy and dignity for radiotherapy patients.
Improvements in patient/carer information
Throughout 2008/09 we have continued the programme of review of our patient information in order to improve the design and accessibility of information to patients, carers and their families. The Trust has also joined a pilot project facilitated by the Merseyside and Cheshire Cancer Network to implement the national Cancer Patient Information Pathways: a project led by the National Cancer Action Team in conjunction with Macmillan and CRUK.
Complaints handling
The Trust continues to have a low number of complaints (11 in 2008/09). Complaints are managed by our Patient Experience Manager who provides an integrated complaints, PALs and patient and public involvement service and who forms part of our Clinical Governance Support Team. All complaints are reviewed and responded to by the Chief Executive. Information on complaints and lessons learned are shared with all staff via our Team Brief and information provided to the public via annual clinical governance roadshows held in public areas of the Trust.
A new complaints policy was approved in March 2009 ready for implementation from 1st April 2009.
19
Partnerships and alliances
As a Foundation Trust we recognise the need to continue to develop a broad range of partnerships to support the delivery of our plans. Over the last year we have achieved our plans for evolving partnership arrangements with:
Continued working with the independent sector to deliver PET:CT services Continued partnership with the University of Liverpool to develop an Academic Unit of
Oncology and associated research developments. Close working relationships with Aintree University Hospitals NHS FT and The Walton
Centre for Neurology and neurosurgery NHS Trust in the development of our plans for a satellite radiotherapy centre.
We have also developed key partnerships to support:
The further implementation of our distributed chemotherapy service model with host provider Trusts
Improvement to performance against Cancer Waiting Times targets where we are dependent upon the actions of others.
Working in partnership with the teenage Cancer Trust to develop our new Teenage and Young Adults unit.
Governance
NHS Foundation Trust Code of Governance
The Monitor Foundation Trust Code of Governance includes a code provision (C.2.1 “….All [other] Executive Directors should be appointed by a committee of the Chief Executive, the Chairman and Non-Executive Directors and subject to re-appointment at intervals of no more than five years). The Board considered this code provision at its meeting in March 2007 and was informed that with an employment contract of any type, there is only one way to terminate without incurring a financial penalty and that is by following due process, i.e. clear and documented performance management. The financial penalty associated with ending a rolling contract could be significantly higher than a standard contract. The Board therefore agreed that it would not comply with this code provision.
All other requirements of the Code of Governance have been met in full.
Council of Governors
Working together with the Board
During the last year our Board of Directors and Governors have worked together in a number of ways to ensure that the Governors’ views are understood and that they receive appropriate support.
18
Service improvements following staff or patient surveys or comments and Healthcare Commission reports
55% of CCO staff responded to the 2008 staff survey, which noted that the Trust scored in the top 20% of all acute specialist trusts nationally in 22 of the 36 key areas. The Trust continually reviews the survey results and implements service improvements accordingly. Such developments have included a review of the Performance & Development Review process (leading to a significantly increased completion rate), the development of a Stress working group and the introduction of trained ‘mentors’ to support anyone who has concerns about unacceptable behavior in the workplace.
In the 2008 Healthcare / Care Quality Commission in-patient survey the Trust scored in the top 20% of all acute Trusts nationally in 53 out of the 62 key areas. For 10 areas we scored the top score achieved by any Trust. The Trust will continue to monitor patients experience throughout the year and aim to continually improve on current performance. CCO has also put into place an internal survey where we offer all patients who complete a course of treatment or in-patient stay the opportunity to provide feedback in ‘real time’. Further information on the survey results are contained within the Quality Report.
As a result of the information obtained in these surveys we have greatly improved our processes for ensuring that patients and their GPs receive appropriate discharge information, whilst we are aiming to minimise patient waiting times within the departments we have put in place free tea and coffee through our volunteer service to improve the patients experience whilst waiting. We have also increased the availability of our hand and foot massage service to patients in the radiotherapy department and have revised what refreshments are on offer in our coffee bar facilities and have improved the environment in relation to privacy and dignity for radiotherapy patients.
Improvements in patient/carer information
Throughout 2008/09 we have continued the programme of review of our patient information in order to improve the design and accessibility of information to patients, carers and their families. The Trust has also joined a pilot project facilitated by the Merseyside and Cheshire Cancer Network to implement the national Cancer Patient Information Pathways: a project led by the National Cancer Action Team in conjunction with Macmillan and CRUK.
Complaints handling
The Trust continues to have a low number of complaints (11 in 2008/09). Complaints are managed by our Patient Experience Manager who provides an integrated complaints, PALs and patient and public involvement service and who forms part of our Clinical Governance Support Team. All complaints are reviewed and responded to by the Chief Executive. Information on complaints and lessons learned are shared with all staff via our Team Brief and information provided to the public via annual clinical governance roadshows held in public areas of the Trust.
A new complaints policy was approved in March 2009 ready for implementation from 1st April 2009.
19
Partnerships and alliances
As a Foundation Trust we recognise the need to continue to develop a broad range of partnerships to support the delivery of our plans. Over the last year we have achieved our plans for evolving partnership arrangements with:
Continued working with the independent sector to deliver PET:CT services Continued partnership with the University of Liverpool to develop an Academic Unit of
Oncology and associated research developments. Close working relationships with Aintree University Hospitals NHS FT and The Walton
Centre for Neurology and neurosurgery NHS Trust in the development of our plans for a satellite radiotherapy centre.
We have also developed key partnerships to support:
The further implementation of our distributed chemotherapy service model with host provider Trusts
Improvement to performance against Cancer Waiting Times targets where we are dependent upon the actions of others.
Working in partnership with the teenage Cancer Trust to develop our new Teenage and Young Adults unit.
Governance
NHS Foundation Trust Code of Governance
The Monitor Foundation Trust Code of Governance includes a code provision (C.2.1 “….All [other] Executive Directors should be appointed by a committee of the Chief Executive, the Chairman and Non-Executive Directors and subject to re-appointment at intervals of no more than five years). The Board considered this code provision at its meeting in March 2007 and was informed that with an employment contract of any type, there is only one way to terminate without incurring a financial penalty and that is by following due process, i.e. clear and documented performance management. The financial penalty associated with ending a rolling contract could be significantly higher than a standard contract. The Board therefore agreed that it would not comply with this code provision.
All other requirements of the Code of Governance have been met in full.
Council of Governors
Working together with the Board
During the last year our Board of Directors and Governors have worked together in a number of ways to ensure that the Governors’ views are understood and that they receive appropriate support.
20
The Chief Executive prepares a report with updates on performance, strategic and operational issues for each of the Council of Governors meetings. Both Executive Directors and Non-Executive Directors attend the Council of Governors’ meetings and its committees.In addition to attendance at these meetings, the Board uses opportunities to work with the Governors, as it did at the event held on 27th March which focused on the strategic development of the organisation.
The Senior Governor and Chair’s of the Council of Governors meetings have with the Chairman throughout the year to ensure Governors are kept up to date on any developments within the Trust.
Council of Governor’s roles and responsibilities and working arrangements
The Governors are elected as part of an independent process managed by Electoral Reform Services, in line with the Trust constitution.
The Council of Governors meets quarterly in public and fulfils its legal obligations as outlined in the constitution. In addition to Council meetings, there are three Committees – Membership, Communications and Fundraising, Patient Experience and Strategy
The Council of Governors has approved its standing orders which includes the development of its sub committees. Each of these committees has identified an Executive and a Non-Executive Director for advise purposes. In addition the Director of Nursing & Quality has a specific role in supporting and working with the Council of Governors playing a key role in developing links between the Board committees and the Council of Governors ensuring that key strategic themes are being addressed.
Composition of the Council of Governors
The Council is made up of 28 Governors, public, staff and nominated organisations, serving a fixed three year term of office.
Liverpool 3 Sefton 2 St Helens & Knowsley 2 Warrington & Halton 2 Chester, Ellesmere Port & Vale Royal 2 Wirral, Wales and the rest of England 4 Staff governors 6 Nominated organisations 7
Total: 28
21
Governors
Name Elected public Elected staff Nominated
Representing Meetingsheld
Meetingsattended
Member of CommitteeSee key
Year Terms ends
Michael Ashley Elected public Warrington & Halton 3 2 ST 2010Trevor Benn (from September 2008)
Elected public Wirral, Wales and the rest of England
2 2 PE 2011
Peter Benson Elected staff Non Staff 3 3 PE 2011Andrea Chambers Manx Cancer Help Association 3 3 ST 2010Michèle Christopherson Elected public Sefton 3 3 PE 2009Stuart Clutton(from September 2008)
Elected public Warrington & Halton 2 2 MCF 2011
John Cocker(until May 2008)
Nominated Metropolitan Borough of Wirral 1 0 ST 2008
Alan Comyns (from September 2008)
Elected public Chester, Ellesmere Port & Vale Royal
2 2 MCF 2011
Kerry Connon Elected public Sefton 3 3 ST 2010Nicola Cook Nominated Macmillan Cancer Support 3 1 ST 2009Reg Cox Elected public Liverpool 3 2 MCF 2009Mary Doddridge Elected public Liverpool 3 3 ST, MCF
(Chair), Nom 2010
John Earis Nominated Aintree University Hospitals NHS Foundation Trust
3 0 2009
Doug Errington Elected staff Doctor 3 2 PE, ST, Nom 2010Peter Fearnhead (until August 2008)
Elected staff Non Clinical 1 0 2008
Deborah Ferns Elected staff Non Clinical 0 0 MCF 2011Tom Fisher Elected public Wirral, Wales and the rest of
England3 3 PE, Nom 2011
Denys Floyd Elected public St Helens & Knowsley 3 2 MCF 2011June Holland(until August 2008)
Elected public Wirral, Wales and the rest of England
1 1 PE 2008
Joanne Martin(until August 2008)
Elected public Wirral, Wales and the rest of England
1 0 2008
Philip Mayles Elected staff Other Clinical 3 3 ST, MCF 2010Ray Murphy Nominated Cheshire & Merseyside Cancer
Network Task Force 3 2 ST 2009
Ruth Murray (until August 2008)
Elected public Chester, Ellesmere Port and Vale Royal
1 1 PE 2008
Ernie Natrass Elected public Liverpool 3 2 MCF 2010Gill Oliver* Elected public Chester, Ellesmere Port and
Vale Royal 3 3 MCF 2009
Kate Perkins Elected staff Radiographer 3 2 ST 2009Cherry Povall (from May 2008)
Nominated Metropolitan Borough of Wirral 2 1 2011
Susan Ramsay Elected public Wirral, Wales and the rest of England
3 1 ST 2010
Kate Smith Elected staff Nurse 3 3 PE (Chair) 2009Margaret Warriner Elected public St Helens & Knowsley 3 3 PE, MCF 2010Alistair Watson Nominated University of Liverpool 3 1 2009Hilda Whitfield(until August 2008)
Elected public Warrington & Halton 1 1 PE 2008
Ewan Wilkinson Nominated Liverpool PCT 3 2 ST (Chair) 2009Eleanor Williams (from September 2008)
Elected public Wirral, Wales and the rest of England
2 2 PE 2011
*Senior Governor PE Patient Experience MCF Membership, Communication & Fundraising ST Strategy Nom Nomination
We would like to express our thanks to former public Governors Joanne Martin, June Holland, Ruth Murray, Hilda Whitfield, staff Governor Peter Fearnhead and former nominated Governor John Cocker. Each served as a Governor during 2008/09 for a period of time, but they have since resigned from their roles or not been re-elected.
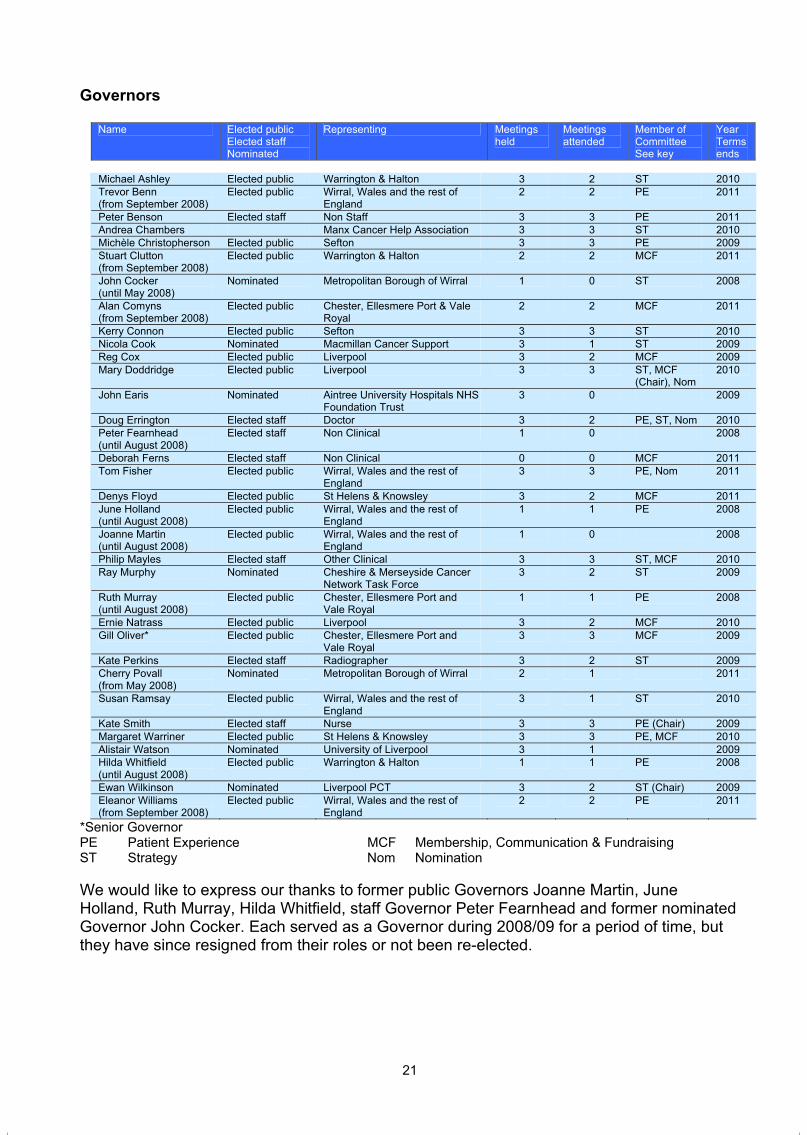
20
The Chief Executive prepares a report with updates on performance, strategic and operational issues for each of the Council of Governors meetings. Both Executive Directors and Non-Executive Directors attend the Council of Governors’ meetings and its committees.In addition to attendance at these meetings, the Board uses opportunities to work with the Governors, as it did at the event held on 27th March which focused on the strategic development of the organisation.
The Senior Governor and Chair’s of the Council of Governors meetings have with the Chairman throughout the year to ensure Governors are kept up to date on any developments within the Trust.
Council of Governor’s roles and responsibilities and working arrangements
The Governors are elected as part of an independent process managed by Electoral Reform Services, in line with the Trust constitution.
The Council of Governors meets quarterly in public and fulfils its legal obligations as outlined in the constitution. In addition to Council meetings, there are three Committees – Membership, Communications and Fundraising, Patient Experience and Strategy
The Council of Governors has approved its standing orders which includes the development of its sub committees. Each of these committees has identified an Executive and a Non-Executive Director for advise purposes. In addition the Director of Nursing & Quality has a specific role in supporting and working with the Council of Governors playing a key role in developing links between the Board committees and the Council of Governors ensuring that key strategic themes are being addressed.
Composition of the Council of Governors
The Council is made up of 28 Governors, public, staff and nominated organisations, serving a fixed three year term of office.
Liverpool 3 Sefton 2 St Helens & Knowsley 2 Warrington & Halton 2 Chester, Ellesmere Port & Vale Royal 2 Wirral, Wales and the rest of England 4 Staff governors 6 Nominated organisations 7
Total: 28
21
Governors
Name Elected public Elected staff Nominated
Representing Meetingsheld
Meetingsattended
Member of CommitteeSee key
Year Terms ends
Michael Ashley Elected public Warrington & Halton 3 2 ST 2010Trevor Benn (from September 2008)
Elected public Wirral, Wales and the rest of England
2 2 PE 2011
Peter Benson Elected staff Non Staff 3 3 PE 2011Andrea Chambers Manx Cancer Help Association 3 3 ST 2010Michèle Christopherson Elected public Sefton 3 3 PE 2009Stuart Clutton(from September 2008)
Elected public Warrington & Halton 2 2 MCF 2011
John Cocker(until May 2008)
Nominated Metropolitan Borough of Wirral 1 0 ST 2008
Alan Comyns (from September 2008)
Elected public Chester, Ellesmere Port & Vale Royal
2 2 MCF 2011
Kerry Connon Elected public Sefton 3 3 ST 2010Nicola Cook Nominated Macmillan Cancer Support 3 1 ST 2009Reg Cox Elected public Liverpool 3 2 MCF 2009Mary Doddridge Elected public Liverpool 3 3 ST, MCF
(Chair), Nom 2010
John Earis Nominated Aintree University Hospitals NHS Foundation Trust
3 0 2009
Doug Errington Elected staff Doctor 3 2 PE, ST, Nom 2010Peter Fearnhead (until August 2008)
Elected staff Non Clinical 1 0 2008
Deborah Ferns Elected staff Non Clinical 0 0 MCF 2011Tom Fisher Elected public Wirral, Wales and the rest of
England3 3 PE, Nom 2011
Denys Floyd Elected public St Helens & Knowsley 3 2 MCF 2011June Holland(until August 2008)
Elected public Wirral, Wales and the rest of England
1 1 PE 2008
Joanne Martin(until August 2008)
Elected public Wirral, Wales and the rest of England
1 0 2008
Philip Mayles Elected staff Other Clinical 3 3 ST, MCF 2010Ray Murphy Nominated Cheshire & Merseyside Cancer
Network Task Force 3 2 ST 2009
Ruth Murray (until August 2008)
Elected public Chester, Ellesmere Port and Vale Royal
1 1 PE 2008
Ernie Natrass Elected public Liverpool 3 2 MCF 2010Gill Oliver* Elected public Chester, Ellesmere Port and
Vale Royal 3 3 MCF 2009
Kate Perkins Elected staff Radiographer 3 2 ST 2009Cherry Povall (from May 2008)
Nominated Metropolitan Borough of Wirral 2 1 2011
Susan Ramsay Elected public Wirral, Wales and the rest of England
3 1 ST 2010
Kate Smith Elected staff Nurse 3 3 PE (Chair) 2009Margaret Warriner Elected public St Helens & Knowsley 3 3 PE, MCF 2010Alistair Watson Nominated University of Liverpool 3 1 2009Hilda Whitfield(until August 2008)
Elected public Warrington & Halton 1 1 PE 2008
Ewan Wilkinson Nominated Liverpool PCT 3 2 ST (Chair) 2009Eleanor Williams (from September 2008)
Elected public Wirral, Wales and the rest of England
2 2 PE 2011
*Senior Governor PE Patient Experience MCF Membership, Communication & Fundraising ST Strategy Nom Nomination
We would like to express our thanks to former public Governors Joanne Martin, June Holland, Ruth Murray, Hilda Whitfield, staff Governor Peter Fearnhead and former nominated Governor John Cocker. Each served as a Governor during 2008/09 for a period of time, but they have since resigned from their roles or not been re-elected.
22
Elections
An election process was completed in August 2008 and the outcomes were announced at the Annual Members Meeting on 14th September 2008. In addition to this a further election process was completed in March 2009 for the vacant staff Governor seat – Non Clinical
Declaration of Interests
A copy of the Register of Interests is available via the Trust website www.ccotrust.nhs.uk,alternatively you can contact Andrea Leather on 0151 482 7799 to request a copy.
Board of Directors
Board of Directors’ roles and responsibilities and working arrangements
The Board of Directors has responsibility for setting the strategic direction of the Trust and for understanding and managing significant risks. The Board also receives assurance that the Trust is fulfilling its responsibilities including compliance with standards and targets. The Board delegates specific functions to its committees identified within their terms of reference. The Trust considers that it operates a balanced and unified Board with particular emphasis on achieving an appropriate balance of skills and experience. This is reviewed as part of the Board development programme, as well as whenever a vacancy arises.
The Trust recognises that the Board of Directors should provide a portfolio of skills and expertise to reflect the business, patient care and clinical requirements of a high performing and effective organisation. The board members provide a breadth of public and private sector expertise at executive level and provide a mix of gender and age profiles. These requirements are periodically reviewed.
Board of Directors – Composition, backgrounds and interests
Non Executive members of the Board including the Chairman are appointed (and removed) by the Council of Governors at a General Meeting, as outlined in the constitution.
The Nomination / Appointment Committee for the Non Executive Directors is made up of the Chairman and three elected Governors (A White, T Fisher, D Errington, M Doddridge). This Nomination Panel is responsible for appointing Non Executive Directors by identifying appropriate candidates through a process of open competition, which takes account of the policy maintained by the Council of Governors and the skills and experience required.
The Nominations Committee followed the re-appointment process described in the Trust’s constitution for the re-appointment of Graham Morris in October 2008. These re-appointments were approved by the Council of Governors at its meeting in November 2008.
The Senior Independent Director – Douglas Buchanan was appointed as such on 5th April 2006.
23
The Board has reviewed all Non Executive Directors and considers them all to be Independent Directors.
Board Members
Alan White – ChairmanRe-appointed by the Council of Governors (2nd term of office, 3 years) until November 2010.
Alan was appointed as Chairman in 1999. Alan retired from Local Government following 10 years as Chief Executive of Wirral Metropolitan Council, the eighth largest organisation of its type in England, employing over 17,000 staff and with an operational budget of £360m, the chief executive role was both challenging and high profile. He led a successful bid for ‘City Challenge’ status as an inner city re-generation initiative developed by the then Secretary of State, Michael Heseltine. The initiative depended on the development of new partnerships between Wirral MBC and major business corporations, which included Lever Bros, General Motors and Mobil Oil. As Chair of the ‘City Lands Board’, the organisation established to lead the implementation, Alan led a 5-year programme of investment, which generated £37m of public sector and some £285m of private sector investment.
Darren Hurrell – Chief Executive
Darren was appointed as Chief Executive in July 2007. He started his career in the NHS in 1990, prior to this he worked for Newcastle University as well as spending some time living in Canada. He has undertaken a number of managerial posts in the NHS including gaining experience in managing mental health services, community services, acute care and specialist cancer care. He took up the post of Chief Executive in July 2007.
Executive Directors
Andrew Cannell – Deputy Chief Executive / Director of Finance
Andrew was appointed as Director of Finance in July 2003 and the Deputy Chief Executive role from February 2008. He is a IPFA qualified accountant who has worked almost exclusively in the NHS since 1983. Before joining the Trust he worked in a senior role as a “Link Accountant” at the North West Regional Office and Greater Manchester SHA. Prior to that he worked for a number of years as Deputy Director of Finance and then Acting Director of Finance at the Manchester Children’s Hospital NHS Trust. Andrew fulfilled the role of Acting Chief Executive until the commencement of the new substantive Chief Executive, Darren Hurrell, on 30th July 2007. In January 2008 the Board re-established the post of Deputy Chief Executive – Andrew was appointed with affect from 1st February 2008.
Dr David Husband – Medical Director
David has been Medical Director since 2000. Following a degree in Biochemistry, he trained in medicine at the University of Leeds. Post-graduate training in general internal medicine and endocrinology and diabetes followed in Leeds and Newcastle. David came to

22
Elections
An election process was completed in August 2008 and the outcomes were announced at the Annual Members Meeting on 14th September 2008. In addition to this a further election process was completed in March 2009 for the vacant staff Governor seat – Non Clinical
Declaration of Interests
A copy of the Register of Interests is available via the Trust website www.ccotrust.nhs.uk,alternatively you can contact Andrea Leather on 0151 482 7799 to request a copy.
Board of Directors
Board of Directors’ roles and responsibilities and working arrangements
The Board of Directors has responsibility for setting the strategic direction of the Trust and for understanding and managing significant risks. The Board also receives assurance that the Trust is fulfilling its responsibilities including compliance with standards and targets. The Board delegates specific functions to its committees identified within their terms of reference. The Trust considers that it operates a balanced and unified Board with particular emphasis on achieving an appropriate balance of skills and experience. This is reviewed as part of the Board development programme, as well as whenever a vacancy arises.
The Trust recognises that the Board of Directors should provide a portfolio of skills and expertise to reflect the business, patient care and clinical requirements of a high performing and effective organisation. The board members provide a breadth of public and private sector expertise at executive level and provide a mix of gender and age profiles. These requirements are periodically reviewed.
Board of Directors – Composition, backgrounds and interests
Non Executive members of the Board including the Chairman are appointed (and removed) by the Council of Governors at a General Meeting, as outlined in the constitution.
The Nomination / Appointment Committee for the Non Executive Directors is made up of the Chairman and three elected Governors (A White, T Fisher, D Errington, M Doddridge). This Nomination Panel is responsible for appointing Non Executive Directors by identifying appropriate candidates through a process of open competition, which takes account of the policy maintained by the Council of Governors and the skills and experience required.
The Nominations Committee followed the re-appointment process described in the Trust’s constitution for the re-appointment of Graham Morris in October 2008. These re-appointments were approved by the Council of Governors at its meeting in November 2008.
The Senior Independent Director – Douglas Buchanan was appointed as such on 5th April 2006.
23
The Board has reviewed all Non Executive Directors and considers them all to be Independent Directors.
Board Members
Alan White – ChairmanRe-appointed by the Council of Governors (2nd term of office, 3 years) until November 2010.
Alan was appointed as Chairman in 1999. Alan retired from Local Government following 10 years as Chief Executive of Wirral Metropolitan Council, the eighth largest organisation of its type in England, employing over 17,000 staff and with an operational budget of £360m, the chief executive role was both challenging and high profile. He led a successful bid for ‘City Challenge’ status as an inner city re-generation initiative developed by the then Secretary of State, Michael Heseltine. The initiative depended on the development of new partnerships between Wirral MBC and major business corporations, which included Lever Bros, General Motors and Mobil Oil. As Chair of the ‘City Lands Board’, the organisation established to lead the implementation, Alan led a 5-year programme of investment, which generated £37m of public sector and some £285m of private sector investment.
Darren Hurrell – Chief Executive
Darren was appointed as Chief Executive in July 2007. He started his career in the NHS in 1990, prior to this he worked for Newcastle University as well as spending some time living in Canada. He has undertaken a number of managerial posts in the NHS including gaining experience in managing mental health services, community services, acute care and specialist cancer care. He took up the post of Chief Executive in July 2007.
Executive Directors
Andrew Cannell – Deputy Chief Executive / Director of Finance
Andrew was appointed as Director of Finance in July 2003 and the Deputy Chief Executive role from February 2008. He is a IPFA qualified accountant who has worked almost exclusively in the NHS since 1983. Before joining the Trust he worked in a senior role as a “Link Accountant” at the North West Regional Office and Greater Manchester SHA. Prior to that he worked for a number of years as Deputy Director of Finance and then Acting Director of Finance at the Manchester Children’s Hospital NHS Trust. Andrew fulfilled the role of Acting Chief Executive until the commencement of the new substantive Chief Executive, Darren Hurrell, on 30th July 2007. In January 2008 the Board re-established the post of Deputy Chief Executive – Andrew was appointed with affect from 1st February 2008.
Dr David Husband – Medical Director
David has been Medical Director since 2000. Following a degree in Biochemistry, he trained in medicine at the University of Leeds. Post-graduate training in general internal medicine and endocrinology and diabetes followed in Leeds and Newcastle. David came to
24
Clatterbridge to train in Clinical Oncology in 1985 and was appointed Consultant in Clinical Oncology in 1992. He is an Honorary Lecturer in the Department of Medicine, University of Liverpool. During a varied career David has worked in some 20 Hospitals.
Dawn Jennings – Director of Human Resources (non voting)
Dawn joined the Trust in December 2005. She is a graduate of the Chartered Institute of Personnel & Development and has held a variety of Human Resources (HR) posts in both the public and private sector. Immediately prior to taking up this post, Dawn was Associate Director of HR at the Christie Hospital in Manchester. Prior to her NHS experience, Dawn worked within various business areas of the Automobile Association, including Insurance and Retail. Dawn has also held a variety of voluntary posts, including Trustee and Treasurer of a local Pre-school, Secretary of the Mid-Cheshire branch of the National Childbirth Trust and Governor of the Primary school. She is now a Parent Governor at her local high school.
Silas Nicholls – Director of Operations & Performance
Silas is an experienced general manager with fifteen years of experience in a range of health care management posts both in the NHS and in the private sector. Silas joined the Trust in February 2008 from Bolton Hospitals NHS Trust where he was the Divisional General Manager for Surgery & Anaesthesia.
Helen Porter – Director of Nursing & Quality
Helen has been a cancer nurse for over 20 years. She has worked within 4 cancer centres holding a variety of clinical and non-clinical posts. She has played a role in the national and international cancer nursing agenda through being on the committees of the RCN Cancer Nursing society; RCN Haematology Society and the International Society of Nurses in Cancer Care. She has been at the Trust since August 2000 joining as Director of Nursing. Four of these years were also spent as the Lead Cancer Nurse for the Merseyside and Cheshire Cancer Network.
Non Executive Directors
Douglas Buchanan – Vice Chairman, Senior Independent Director Re-appointed by the Council of Governors (3rd term of office, 3 years) until January 2011.
Douglas has been a Non-Executive Director since 1995 and was appointed as Vice Chairman in April 2004. He is a retired surgeon whose medical career started in Edinburgh in 1966. He enjoyed a successful 11 years working as a surgeon for the mining industry in Zambia and latterly as their Chief Medical Officer. On return to the UK in 1986, Douglas joined the British Council where in 1990 he was appointed to the post of Director of the Health Work of the Council. During his work at the British Council, Douglas visited 35 countries working with health professionals up to ministerial level. In 1996 he organised a seminar on the UK NHS reforms held at the World Bank in Washington. The UK team included Sir Alan Langlands, the CEO of the NHS and Sir Nigel Crisp, then CEO of the Oxford Radcliffe Hospital.
25
Carol Eastwood Appointed by the Council of Governors (1st term of office, 3 years) until January 2010.
In September 2007 Carol retired as a Vice President in Corporate Information Services in AstraZeneca, one of the worlds leading pharmaceutical companies. She joined ICI from university as a research scientist and was appointed as Chief Analyst for Zeneca Specialities in 1995. Carol has been a member of many different external committees, including European Research programmes, Information Governance in the Pharmaceutical industry and Regulatory Compliance. She was appointed Non-Executive Director February 2007.
Louise Martin Re-appointed by the Council of Governors (2nd term of office, 3 years) until November 2010.
Louise was appointed as a Non-Executive Director at the Trust in April 2001. She has worked within the UK National Health Service for 15 years in a number of clinical and managerial posts. In 1998 Louise left the NHS to head the project company managing the delivery of a major first-wave PFI scheme at South Manchester University Hospitals NHS Trust. Louise now works for Health Care Projects Ltd, a subsidiary of ‘Innisfree’ the Infrastructure Investment Company, where she acts as Project Director.
Graham MorrisRe-appointed by the Council of Governors (2nd term of office, 3 years) until November 2012.
Graham became a Non-Executive Director in December 2005. He is a qualified accountant (FCCA) and worked for 33 years in the electricity industry. During that time Graham gained extensive experience of finance, regulation and corporate strategy, heading up the finance function of SP Manweb plc following Scottish Power’s take-over. During this period he also worked in America, working on the merger of PacifiCorp, an American subsidiary acquired by Scottish Power in 1999.
Following his return from America, Graham helped set up a joint venture company Selectusonline Ltd – a procurement consultancy that can harmonise specifications and aggregate volumes within the utilities sector. As an elder and treasurer of Upton by Chester United Reformed Church he also has extensive involvement in charity and community activities, including being on the executive of the local pre-school association. In July 2006 he was elected on to the Finance Committee of the United Reformed Church at a national level.
Vicky Tagart Re-appointed by the Council of Governors (2nd term of office, 3 years) until November 2010.
After a degree in Biochemistry from Somerville College, Oxford, Vicky gained a Ph.D. in immunology from the University of Bristol. This was followed by two postdoctoral research positions, the first at the Clinical Research Centre, Harrow, Middlesex, and the second at Johns Hopkins University, Baltimore. On return to the UK Vicky joined the UK affiliate of the American pharmaceutical company Eli Lilly. Vicky then moved to the Head Office Personnel Department. In 1991 Vicky took the position of Head of Human Resources with Degussa Ltd., the UK affiliate of a large German chemical company. Since December 2000 she has been a Non-Executive Director.
24
Clatterbridge to train in Clinical Oncology in 1985 and was appointed Consultant in Clinical Oncology in 1992. He is an Honorary Lecturer in the Department of Medicine, University of Liverpool. During a varied career David has worked in some 20 Hospitals.
Dawn Jennings – Director of Human Resources (non voting)
Dawn joined the Trust in December 2005. She is a graduate of the Chartered Institute of Personnel & Development and has held a variety of Human Resources (HR) posts in both the public and private sector. Immediately prior to taking up this post, Dawn was Associate Director of HR at the Christie Hospital in Manchester. Prior to her NHS experience, Dawn worked within various business areas of the Automobile Association, including Insurance and Retail. Dawn has also held a variety of voluntary posts, including Trustee and Treasurer of a local Pre-school, Secretary of the Mid-Cheshire branch of the National Childbirth Trust and Governor of the Primary school. She is now a Parent Governor at her local high school.
Silas Nicholls – Director of Operations & Performance
Silas is an experienced general manager with fifteen years of experience in a range of health care management posts both in the NHS and in the private sector. Silas joined the Trust in February 2008 from Bolton Hospitals NHS Trust where he was the Divisional General Manager for Surgery & Anaesthesia.
Helen Porter – Director of Nursing & Quality
Helen has been a cancer nurse for over 20 years. She has worked within 4 cancer centres holding a variety of clinical and non-clinical posts. She has played a role in the national and international cancer nursing agenda through being on the committees of the RCN Cancer Nursing society; RCN Haematology Society and the International Society of Nurses in Cancer Care. She has been at the Trust since August 2000 joining as Director of Nursing. Four of these years were also spent as the Lead Cancer Nurse for the Merseyside and Cheshire Cancer Network.
Non Executive Directors
Douglas Buchanan – Vice Chairman, Senior Independent Director Re-appointed by the Council of Governors (3rd term of office, 3 years) until January 2011.
Douglas has been a Non-Executive Director since 1995 and was appointed as Vice Chairman in April 2004. He is a retired surgeon whose medical career started in Edinburgh in 1966. He enjoyed a successful 11 years working as a surgeon for the mining industry in Zambia and latterly as their Chief Medical Officer. On return to the UK in 1986, Douglas joined the British Council where in 1990 he was appointed to the post of Director of the Health Work of the Council. During his work at the British Council, Douglas visited 35 countries working with health professionals up to ministerial level. In 1996 he organised a seminar on the UK NHS reforms held at the World Bank in Washington. The UK team included Sir Alan Langlands, the CEO of the NHS and Sir Nigel Crisp, then CEO of the Oxford Radcliffe Hospital.
25
Carol Eastwood Appointed by the Council of Governors (1st term of office, 3 years) until January 2010.
In September 2007 Carol retired as a Vice President in Corporate Information Services in AstraZeneca, one of the worlds leading pharmaceutical companies. She joined ICI from university as a research scientist and was appointed as Chief Analyst for Zeneca Specialities in 1995. Carol has been a member of many different external committees, including European Research programmes, Information Governance in the Pharmaceutical industry and Regulatory Compliance. She was appointed Non-Executive Director February 2007.
Louise Martin Re-appointed by the Council of Governors (2nd term of office, 3 years) until November 2010.
Louise was appointed as a Non-Executive Director at the Trust in April 2001. She has worked within the UK National Health Service for 15 years in a number of clinical and managerial posts. In 1998 Louise left the NHS to head the project company managing the delivery of a major first-wave PFI scheme at South Manchester University Hospitals NHS Trust. Louise now works for Health Care Projects Ltd, a subsidiary of ‘Innisfree’ the Infrastructure Investment Company, where she acts as Project Director.
Graham MorrisRe-appointed by the Council of Governors (2nd term of office, 3 years) until November 2012.
Graham became a Non-Executive Director in December 2005. He is a qualified accountant (FCCA) and worked for 33 years in the electricity industry. During that time Graham gained extensive experience of finance, regulation and corporate strategy, heading up the finance function of SP Manweb plc following Scottish Power’s take-over. During this period he also worked in America, working on the merger of PacifiCorp, an American subsidiary acquired by Scottish Power in 1999.
Following his return from America, Graham helped set up a joint venture company Selectusonline Ltd – a procurement consultancy that can harmonise specifications and aggregate volumes within the utilities sector. As an elder and treasurer of Upton by Chester United Reformed Church he also has extensive involvement in charity and community activities, including being on the executive of the local pre-school association. In July 2006 he was elected on to the Finance Committee of the United Reformed Church at a national level.
Vicky Tagart Re-appointed by the Council of Governors (2nd term of office, 3 years) until November 2010.
After a degree in Biochemistry from Somerville College, Oxford, Vicky gained a Ph.D. in immunology from the University of Bristol. This was followed by two postdoctoral research positions, the first at the Clinical Research Centre, Harrow, Middlesex, and the second at Johns Hopkins University, Baltimore. On return to the UK Vicky joined the UK affiliate of the American pharmaceutical company Eli Lilly. Vicky then moved to the Head Office Personnel Department. In 1991 Vicky took the position of Head of Human Resources with Degussa Ltd., the UK affiliate of a large German chemical company. Since December 2000 she has been a Non-Executive Director.

26
Declaration of Interests
The Chairman has no other significant commitments.
A copy of the Register of Interests is available via the Trust website www.ccotrust.nhs.uk,alternatively you can contact Andrea Leather on 0151 482 7799 to request a copy.
Board meetings & Committees
Appropriate Board Roles and Structure
The Board has reviewed the Integrated Governance Handbook and has developed an Integrated Governance Development Plan to ensure that the Trust continues to develop and comply with best practice in its governance arrangements. The Board has approved a revised committee structure which reflects this model. The revised structure is:
Monthly Board meetings (all meetings are closed to the public) Quarterly Integrated Governance Committee Audit Committee (5 times per year) Nominations Committee (Ad hoc) Remuneration Committee (Ad hoc) Four ‘task and finish’ Board committees (IM&T, Research & Development, Vision 2020
and Investment).
The Board delegates specific functions to its committees identified within their terms of reference. The terms of reference of all Board committees are reviewed regularly as part of the annual review of the Constitution and Corporate Governance Manual (standing orders and standing financial instructions) and updated to reflect changes in the operating environment and best practice.
The Trust considers that it operates a balanced and unified Board with particular emphasis on achieving an appropriate balance of skills and experience. This is reviewed as part of the Board development programme, as well as whenever a vacancy arises.
In 2006, in preparation for Foundation Trust status, the Board commissioned Whitehead Mann consultants to provide an independent assessment of the effectiveness of the Board and of how it functions. It also reported on the roles and experience of individual Board members. The output of this review has been used to inform the Board development programme.
Learning Review
A learning review has been carried out with the Board. A number of the learning review outcomes that were subsequently agreed at the Board had a direct link to Board development, specifically that we would:
take the opportunity to work as a board to develop CCO’s long term strategy use the whole board to develop and nurture key external relationships
27
proactively stimulate and challenge our thinking, using external speakers to assist with this where appropriate.
These recommendations also support principles contained within the Department of Health’s Integrated Governance Handbook, specifically that healthcare boards should work together as whole teams in their development to ensure greater integration and corporacy.
The recommendations also support requirements contained within the Monitor Code of Governance to ensure the continuing development of Board Directors.
Audit Committee
The Audit Committee – chaired by Graham Morris - provides the central means by which the Trust Board ensures effective internal control arrangements are in place. In addition, the Audit Committee provides a form of independent check upon the executive arm of the Board.
During this year the Audit Committee undertook the following pieces of work to ensure the effective discharge of its responsibilities:
Committee review of the financial statements of exchequer and charitable funds. Review of the findings of the Healthcare Commission in the acute hospitals portfolio. Setting and reviewing progress of the annual internal audit plan using a risk-focused
approach, linked to the controls assurance framework. Receiving regular reports from both Internal Audit and External Auditors. Agreeing and reviewing the work of the Trust’s counter fraud officer. Undertaking a self assessment of its work and effectiveness, and identifying any
training needs. Reviewing and updating its terms of reference. Approving bad debt write offs and contract extensions.
Integrated Governance Committee
The role of the Integrated Governance Committee is: To provide strategic oversight to all areas of governance within the Trust, by giving
carefully consideration to the Clinical, Organisational and Performance arrangements in place.
To ensure organisation-wide co-ordination and prioritisation of risk management issues, encouraging and fostering a greater awareness and ownership of Objectives, Risks and Controls.
To oversee on behalf of the Boards, the management of healthcare and organisational risk.
During this year the Integrated Governance Committee delivered against its terms of reference in particular focusing on:

26
Declaration of Interests
The Chairman has no other significant commitments.
A copy of the Register of Interests is available via the Trust website www.ccotrust.nhs.uk,alternatively you can contact Andrea Leather on 0151 482 7799 to request a copy.
Board meetings & Committees
Appropriate Board Roles and Structure
The Board has reviewed the Integrated Governance Handbook and has developed an Integrated Governance Development Plan to ensure that the Trust continues to develop and comply with best practice in its governance arrangements. The Board has approved a revised committee structure which reflects this model. The revised structure is:
Monthly Board meetings (all meetings are closed to the public) Quarterly Integrated Governance Committee Audit Committee (5 times per year) Nominations Committee (Ad hoc) Remuneration Committee (Ad hoc) Four ‘task and finish’ Board committees (IM&T, Research & Development, Vision 2020
and Investment).
The Board delegates specific functions to its committees identified within their terms of reference. The terms of reference of all Board committees are reviewed regularly as part of the annual review of the Constitution and Corporate Governance Manual (standing orders and standing financial instructions) and updated to reflect changes in the operating environment and best practice.
The Trust considers that it operates a balanced and unified Board with particular emphasis on achieving an appropriate balance of skills and experience. This is reviewed as part of the Board development programme, as well as whenever a vacancy arises.
In 2006, in preparation for Foundation Trust status, the Board commissioned Whitehead Mann consultants to provide an independent assessment of the effectiveness of the Board and of how it functions. It also reported on the roles and experience of individual Board members. The output of this review has been used to inform the Board development programme.
Learning Review
A learning review has been carried out with the Board. A number of the learning review outcomes that were subsequently agreed at the Board had a direct link to Board development, specifically that we would:
take the opportunity to work as a board to develop CCO’s long term strategy use the whole board to develop and nurture key external relationships
27
proactively stimulate and challenge our thinking, using external speakers to assist with this where appropriate.
These recommendations also support principles contained within the Department of Health’s Integrated Governance Handbook, specifically that healthcare boards should work together as whole teams in their development to ensure greater integration and corporacy.
The recommendations also support requirements contained within the Monitor Code of Governance to ensure the continuing development of Board Directors.
Audit Committee
The Audit Committee – chaired by Graham Morris - provides the central means by which the Trust Board ensures effective internal control arrangements are in place. In addition, the Audit Committee provides a form of independent check upon the executive arm of the Board.
During this year the Audit Committee undertook the following pieces of work to ensure the effective discharge of its responsibilities:
Committee review of the financial statements of exchequer and charitable funds. Review of the findings of the Healthcare Commission in the acute hospitals portfolio. Setting and reviewing progress of the annual internal audit plan using a risk-focused
approach, linked to the controls assurance framework. Receiving regular reports from both Internal Audit and External Auditors. Agreeing and reviewing the work of the Trust’s counter fraud officer. Undertaking a self assessment of its work and effectiveness, and identifying any
training needs. Reviewing and updating its terms of reference. Approving bad debt write offs and contract extensions.
Integrated Governance Committee
The role of the Integrated Governance Committee is: To provide strategic oversight to all areas of governance within the Trust, by giving
carefully consideration to the Clinical, Organisational and Performance arrangements in place.
To ensure organisation-wide co-ordination and prioritisation of risk management issues, encouraging and fostering a greater awareness and ownership of Objectives, Risks and Controls.
To oversee on behalf of the Boards, the management of healthcare and organisational risk.
During this year the Integrated Governance Committee delivered against its terms of reference in particular focusing on:

28
Maintaining an overview of the strategies within its remit (e.g. Clinical Governance, Risk Management, Patient and Public Involvement, Infection Control) ensuring structures and systems are in place to ensure effective governance and to receive performance reports related to these strategies.
Implementing and monitoring the Trusts integrated Governance development plan. Ensuring compliance with Standards for Better Health Receiving assurance that the Trust meets all relevant statutory and regulatory
obligations Receiving assurance of the adequacy of systems for quality assurance, managing
risk and control of the environment. Ensuring that the Trust has an effective corporate risk register Keeping the Board fully informed of all significant risks which may impact on the
Trusts strategic direction and business planning process and to report to the Board on the management of significant risks.
Ensuring that the Trust has structures, processes and controls in place to assure and demonstrate the continued quality of its services and to monitor their performance
Remuneration Committee
The Remuneration Committee of the Chairman and other Non-Executive Directors, decides the terms and conditions of office including the remuneration and allowances of all the Directors, including pension rights and any compensation payments. The Committee met on 1 occasion, all members were in attendance.
Nomination Committee
The Nomination / Appointment Committee for a Chief Executive is made up of the Non Executive Directors, chaired by the Chairman. The appointment is subject to the approval of a majority of the members of the Council of Governors present and voting at a general meeting.
The Nomination / Appointment Committee for the Directors is made up of a committee consisting of the Chairman, the Chief Executive and the other Non Executive Directors.
During 2008-09 there were no new Executive Director appointments.
29
Attendance at Board of Directors and Board Committee meetings
For the period 1st April 2008 to 31st March 2009 the Board of Directors held 12 Trust Board meetings which are non public.
Board of Directors
Audit IntegratedGovernance
Remuneration InformationManagement & Technology
Research & Development
Vision2020
No. of meetings held for 2008/09
12 6 4* 1 4* 3 3*
EXECUTIVE DIRECTORS Darren Hurrell 11 - 2 - - 2 3Andrew Cannell 11 - 3 - 4 3 3Helen Porter 10 - 3 - 4 2 2Silas Nicholls 12 - 4 - 4 3 3David Husband 10 - 2 - - 2 3Dawn Jennings (non voting)
11 - 4 - 2 - 3
NON EXECUTIVE DIRECTORS Alan White 12 - - 1 - - -Louise Martin 9 5 3/4 1 1/1 - 1/2Vicky Tagart 11 6 3/3 1 1/1 3 -Douglas Buchanan 11 4 3/4 1 3/3 3 -Carol Eastwood 11 6 - 1 4/4 3 3/3Graham Morris 10 5 0/1 1 2/3 - -
NB. The Investment Committee was not required to meet during 2008/09. All meetings were quorate. *The Non Executive Director membership of these Committees changed in January 2009. Attendance has been
shown with the number of meetings held whilst the individual was a member of the relevant Committee.
Membership
Membership is open to any individual who is over the age of 16, is entitled under the constitution to be a member of one of the public constituencies or the staff constituencies, and has completed the relevant application form.
Our staff membership operates on an ‘opt out’ basis. As with staff all volunteers (with service longer than 12 months) are automatically opted in. The term ‘staff’ includes third party service providers to the hospital eg domestics and porters.
If members wish to contact their individual Governor or a Director they can do so by contacting Andrea Leather, Corporate Governance Manager on 0151 482 7799 or by email [email protected]
There is a ‘members only’ section available on the CCO website.
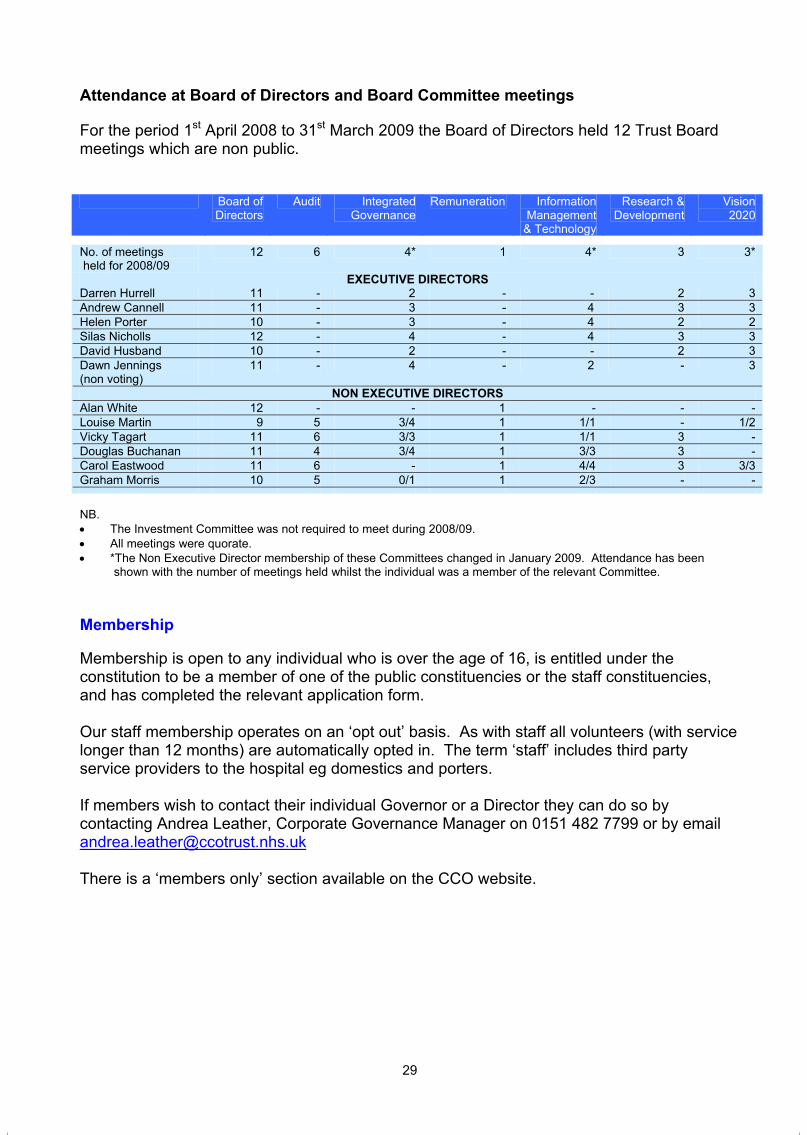
28
Maintaining an overview of the strategies within its remit (e.g. Clinical Governance, Risk Management, Patient and Public Involvement, Infection Control) ensuring structures and systems are in place to ensure effective governance and to receive performance reports related to these strategies.
Implementing and monitoring the Trusts integrated Governance development plan. Ensuring compliance with Standards for Better Health Receiving assurance that the Trust meets all relevant statutory and regulatory
obligations Receiving assurance of the adequacy of systems for quality assurance, managing
risk and control of the environment. Ensuring that the Trust has an effective corporate risk register Keeping the Board fully informed of all significant risks which may impact on the
Trusts strategic direction and business planning process and to report to the Board on the management of significant risks.
Ensuring that the Trust has structures, processes and controls in place to assure and demonstrate the continued quality of its services and to monitor their performance
Remuneration Committee
The Remuneration Committee of the Chairman and other Non-Executive Directors, decides the terms and conditions of office including the remuneration and allowances of all the Directors, including pension rights and any compensation payments. The Committee met on 1 occasion, all members were in attendance.
Nomination Committee
The Nomination / Appointment Committee for a Chief Executive is made up of the Non Executive Directors, chaired by the Chairman. The appointment is subject to the approval of a majority of the members of the Council of Governors present and voting at a general meeting.
The Nomination / Appointment Committee for the Directors is made up of a committee consisting of the Chairman, the Chief Executive and the other Non Executive Directors.
During 2008-09 there were no new Executive Director appointments.
29
Attendance at Board of Directors and Board Committee meetings
For the period 1st April 2008 to 31st March 2009 the Board of Directors held 12 Trust Board meetings which are non public.
Board of Directors
Audit IntegratedGovernance
Remuneration InformationManagement & Technology
Research & Development
Vision2020
No. of meetings held for 2008/09
12 6 4* 1 4* 3 3*
EXECUTIVE DIRECTORS Darren Hurrell 11 - 2 - - 2 3Andrew Cannell 11 - 3 - 4 3 3Helen Porter 10 - 3 - 4 2 2Silas Nicholls 12 - 4 - 4 3 3David Husband 10 - 2 - - 2 3Dawn Jennings (non voting)
11 - 4 - 2 - 3
NON EXECUTIVE DIRECTORS Alan White 12 - - 1 - - -Louise Martin 9 5 3/4 1 1/1 - 1/2Vicky Tagart 11 6 3/3 1 1/1 3 -Douglas Buchanan 11 4 3/4 1 3/3 3 -Carol Eastwood 11 6 - 1 4/4 3 3/3Graham Morris 10 5 0/1 1 2/3 - -
NB. The Investment Committee was not required to meet during 2008/09. All meetings were quorate. *The Non Executive Director membership of these Committees changed in January 2009. Attendance has been
shown with the number of meetings held whilst the individual was a member of the relevant Committee.
Membership
Membership is open to any individual who is over the age of 16, is entitled under the constitution to be a member of one of the public constituencies or the staff constituencies, and has completed the relevant application form.
Our staff membership operates on an ‘opt out’ basis. As with staff all volunteers (with service longer than 12 months) are automatically opted in. The term ‘staff’ includes third party service providers to the hospital eg domestics and porters.
If members wish to contact their individual Governor or a Director they can do so by contacting Andrea Leather, Corporate Governance Manager on 0151 482 7799 or by email [email protected]
There is a ‘members only’ section available on the CCO website.

30
Public Constituency 2008/09(plan)*
2008/09(actual)
2009/10(estimated)
Staff Constituency Doctor 42 42 48Nurse 136 136 156Non clinical 208 208 225Other clinical professional
118 118 120
Radiographer 134 134 137Non staff 121 121 172Public Constituencies Wirral, Wales and rest of England
1614 1679 1717
Liverpool 700 830Sefton 681 1105Warrington and Halton 522 563St Helens and Knowsley 619 668Chester, Ellesmere Portand Vale Royal
599 632
225 across all constituencies
Staff constituency members as of March 31, 2009 totalling 759 Public constituency members as of March 31, 2008 totalling 5477
* The Trust set a target within its Annual Plan to increase its membership by 10% in the Liverpool and Sefton constituencies and under 50’s across all areas. In addition to this, to increase its ethnic minority membership, representative of the Liverpool constituency. As outlined in the table above, the number of public members has continued to grow with 742 new members joining the Trust. A large proportion of our members come from our patient population. The number of public members identified as ‘leaving’ are predominantly due to members dying (131 out of 300) rather than opting to stop being a member. The remaining 169 have been picked up as being members who have moved home without notifying the Trust.
Membership strategy
The Membership and Communications committee is responsible for reviewing and implementing the Membership Strategy.
Public Interest Disclosures
The Trust has in place a full range of HR policies to support staff and advise managers. The Trust engages in formal and informal consultation with staff to ensure a partnership approach is in place. Formal consultation primarily occurs via the Trust’s JCNF (Joint Consultative and Negotiating Forum) and the LNC (Local Negotiating Forum). Staff open forums are held with the Chief Executive to address staff directly when any service changes are proposed (e.g. our plans for a satellite radiotherapy development). In addition the Trust Board engages staff through a visible leadership programme where executive and non executive directors visit all departments on a rotational basis. Staff are informed about policy changes via the monthly Team brief which is cascaded throughout the organisation.
31
The Trust is committed to delivering on its single equality scheme and to the development of anti-discriminatory practices and the provision of equal opportunities. Training on equality and diversity is included in the Trust’s mandatory training programme. The Trust Board hasparticipated in equality and diversity training. All new policies are impact assessed for any potential discrimination.
The Trust retained it’s ‘Two Ticks’ accreditation, annually reviewing the five commitments and what has been achieved including planning ways to improve our service and letting employees know about our progress on future plans.
Clatterbridge Centre for Oncology is committed to Diversity in Employment. We utilise the involvement of an external employment service to assess, evaluate and implement practical support to employees with a declared disability who have requested assistance in the workplace eg. the supply of ergonomic keyboards and assistance with transport to work.
The Trust has in place counter fraud policies and a local counter fraud service.
The Trust has a joint staff side and management health and safety committee. During 2007/08 this committee has developed a range of health and safety policies and monitors health and safety issues such as slips, trips and falls, advising the Trust on any actions required. Health and safety training is mandatory for all staff and specific additional training has been provided to the Board and to senior managers to ensure that they are aware of their specific responsibilities.
The Trust provides a comprehensive occupational health service via a service level agreement with Wirral University Hospital NHS Foundation Trust.
Patient and Public Involvement Activity
The Trust has contacted all its OSCs in relation to the declaration against Standards for Better Health.
The Trust continues to engage widely with its patients, governors, staff, PPI forum with regards to the Satellite Radiotherapy Centre.
The Trust has in place a PPI strategy and actively engages with its patients and public through a number of mechanisms. These have included for 2008/09:
Working closely with the Council of Governors and its Committees e.g.
The Patient Experience Committee has raised funds to furnish the ‘quiet room’ for patients.
The Membership and Communications Committee is leading the development of plans to proactively engage with existing members and attract more members. They have also introduced a scheme to link elected governors with a member of staff in a service area of interest – to improve understanding about each other’s roles
The Fundraising Committee is supporting the work of the newly established fundraising team at the Centre
30
Public Constituency 2008/09(plan)*
2008/09(actual)
2009/10(estimated)
Staff Constituency Doctor 42 42 48Nurse 136 136 156Non clinical 208 208 225Other clinical professional
118 118 120
Radiographer 134 134 137Non staff 121 121 172Public Constituencies Wirral, Wales and rest of England
1614 1679 1717
Liverpool 700 830Sefton 681 1105Warrington and Halton 522 563St Helens and Knowsley 619 668Chester, Ellesmere Portand Vale Royal
599 632
225 across all constituencies
Staff constituency members as of March 31, 2009 totalling 759 Public constituency members as of March 31, 2008 totalling 5477
* The Trust set a target within its Annual Plan to increase its membership by 10% in the Liverpool and Sefton constituencies and under 50’s across all areas. In addition to this, to increase its ethnic minority membership, representative of the Liverpool constituency. As outlined in the table above, the number of public members has continued to grow with 742 new members joining the Trust. A large proportion of our members come from our patient population. The number of public members identified as ‘leaving’ are predominantly due to members dying (131 out of 300) rather than opting to stop being a member. The remaining 169 have been picked up as being members who have moved home without notifying the Trust.
Membership strategy
The Membership and Communications committee is responsible for reviewing and implementing the Membership Strategy.
Public Interest Disclosures
The Trust has in place a full range of HR policies to support staff and advise managers. The Trust engages in formal and informal consultation with staff to ensure a partnership approach is in place. Formal consultation primarily occurs via the Trust’s JCNF (Joint Consultative and Negotiating Forum) and the LNC (Local Negotiating Forum). Staff open forums are held with the Chief Executive to address staff directly when any service changes are proposed (e.g. our plans for a satellite radiotherapy development). In addition the Trust Board engages staff through a visible leadership programme where executive and non executive directors visit all departments on a rotational basis. Staff are informed about policy changes via the monthly Team brief which is cascaded throughout the organisation.
31
The Trust is committed to delivering on its single equality scheme and to the development of anti-discriminatory practices and the provision of equal opportunities. Training on equality and diversity is included in the Trust’s mandatory training programme. The Trust Board hasparticipated in equality and diversity training. All new policies are impact assessed for any potential discrimination.
The Trust retained it’s ‘Two Ticks’ accreditation, annually reviewing the five commitments and what has been achieved including planning ways to improve our service and letting employees know about our progress on future plans.
Clatterbridge Centre for Oncology is committed to Diversity in Employment. We utilise the involvement of an external employment service to assess, evaluate and implement practical support to employees with a declared disability who have requested assistance in the workplace eg. the supply of ergonomic keyboards and assistance with transport to work.
The Trust has in place counter fraud policies and a local counter fraud service.
The Trust has a joint staff side and management health and safety committee. During 2007/08 this committee has developed a range of health and safety policies and monitors health and safety issues such as slips, trips and falls, advising the Trust on any actions required. Health and safety training is mandatory for all staff and specific additional training has been provided to the Board and to senior managers to ensure that they are aware of their specific responsibilities.
The Trust provides a comprehensive occupational health service via a service level agreement with Wirral University Hospital NHS Foundation Trust.
Patient and Public Involvement Activity
The Trust has contacted all its OSCs in relation to the declaration against Standards for Better Health.
The Trust continues to engage widely with its patients, governors, staff, PPI forum with regards to the Satellite Radiotherapy Centre.
The Trust has in place a PPI strategy and actively engages with its patients and public through a number of mechanisms. These have included for 2008/09:
Working closely with the Council of Governors and its Committees e.g.
The Patient Experience Committee has raised funds to furnish the ‘quiet room’ for patients.
The Membership and Communications Committee is leading the development of plans to proactively engage with existing members and attract more members. They have also introduced a scheme to link elected governors with a member of staff in a service area of interest – to improve understanding about each other’s roles
The Fundraising Committee is supporting the work of the newly established fundraising team at the Centre
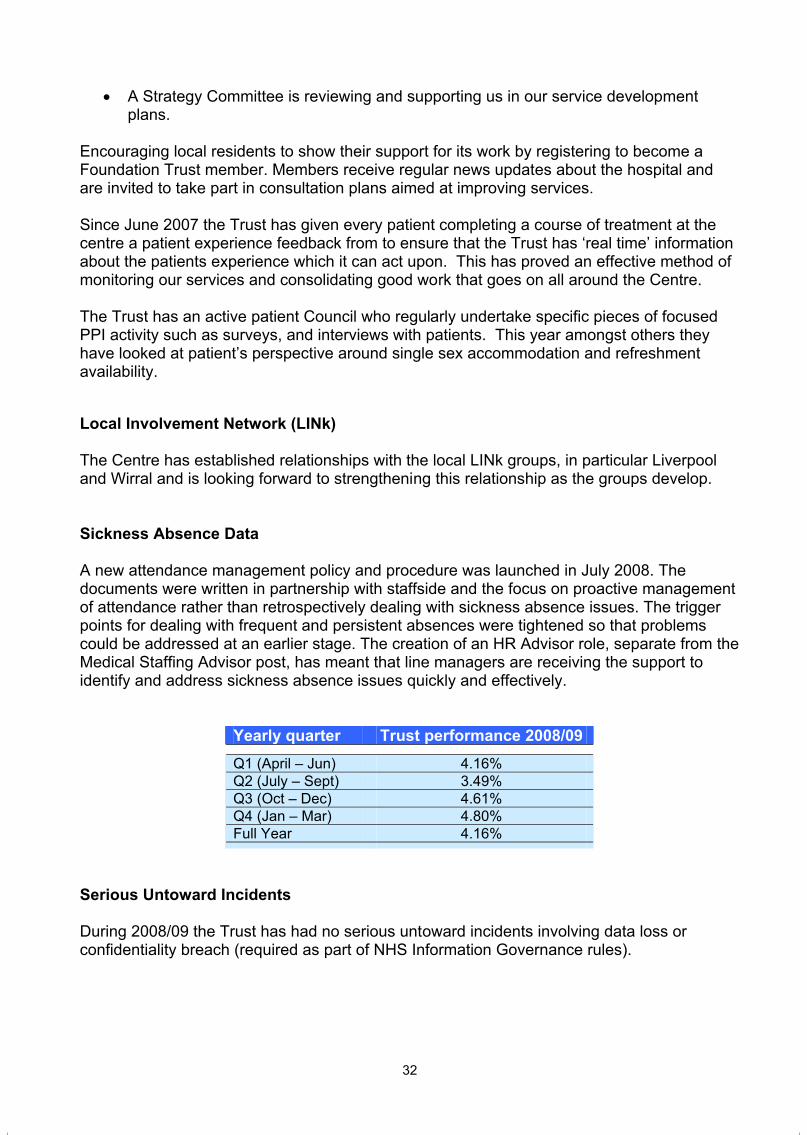
32
A Strategy Committee is reviewing and supporting us in our service development plans.
Encouraging local residents to show their support for its work by registering to become a Foundation Trust member. Members receive regular news updates about the hospital and are invited to take part in consultation plans aimed at improving services.
Since June 2007 the Trust has given every patient completing a course of treatment at the centre a patient experience feedback from to ensure that the Trust has ‘real time’ information about the patients experience which it can act upon. This has proved an effective method of monitoring our services and consolidating good work that goes on all around the Centre.
The Trust has an active patient Council who regularly undertake specific pieces of focused PPI activity such as surveys, and interviews with patients. This year amongst others they have looked at patient’s perspective around single sex accommodation and refreshment availability.
Local Involvement Network (LINk)
The Centre has established relationships with the local LINk groups, in particular Liverpool and Wirral and is looking forward to strengthening this relationship as the groups develop.
Sickness Absence Data
A new attendance management policy and procedure was launched in July 2008. The documents were written in partnership with staffside and the focus on proactive management of attendance rather than retrospectively dealing with sickness absence issues. The trigger points for dealing with frequent and persistent absences were tightened so that problems could be addressed at an earlier stage. The creation of an HR Advisor role, separate from the Medical Staffing Advisor post, has meant that line managers are receiving the support to identify and address sickness absence issues quickly and effectively.
Yearly quarter Trust performance 2008/09 Q1 (April – Jun) 4.16%Q2 (July – Sept) 3.49%Q3 (Oct – Dec) 4.61%Q4 (Jan – Mar) 4.80%Full Year 4.16%
Serious Untoward Incidents
During 2008/09 the Trust has had no serious untoward incidents involving data loss or confidentiality breach (required as part of NHS Information Governance rules).
33
Cost allocation and charging requirements
In 2008/09 the Trust has complied with the cost allocation and charging requirements set out in HM Treasury and Office of Public Sector Information Guidance.
Remuneration Report
The Remuneration Report can be found at note 5.3/1 in the enclosed Trust Accounts for the period 1st April 2008 to 31st March 2009.
Remuneration of senior managers See note 5.3/1 in the Annual Accounts
Salary See note 5.3/1 in the Annual Accounts
Other remuneration See note 5.3/1 in the Annual Accounts
Golden hellos See note 5.3/1 in the Annual Accounts
Compensation for loss of office See note 5.3/1 in the Annual Accounts
Benefits in kind See note 5.3/1 in the Annual Accounts
Pension disclosures See note 5.3/2 in the Annual Accounts
Statement of accounting officer’s responsibilities See page 46 of the Annual Accounts
Statement on internal control See page 50 of the Annual Accounts

32
A Strategy Committee is reviewing and supporting us in our service development plans.
Encouraging local residents to show their support for its work by registering to become a Foundation Trust member. Members receive regular news updates about the hospital and are invited to take part in consultation plans aimed at improving services.
Since June 2007 the Trust has given every patient completing a course of treatment at the centre a patient experience feedback from to ensure that the Trust has ‘real time’ information about the patients experience which it can act upon. This has proved an effective method of monitoring our services and consolidating good work that goes on all around the Centre.
The Trust has an active patient Council who regularly undertake specific pieces of focused PPI activity such as surveys, and interviews with patients. This year amongst others they have looked at patient’s perspective around single sex accommodation and refreshment availability.
Local Involvement Network (LINk)
The Centre has established relationships with the local LINk groups, in particular Liverpool and Wirral and is looking forward to strengthening this relationship as the groups develop.
Sickness Absence Data
A new attendance management policy and procedure was launched in July 2008. The documents were written in partnership with staffside and the focus on proactive management of attendance rather than retrospectively dealing with sickness absence issues. The trigger points for dealing with frequent and persistent absences were tightened so that problems could be addressed at an earlier stage. The creation of an HR Advisor role, separate from the Medical Staffing Advisor post, has meant that line managers are receiving the support to identify and address sickness absence issues quickly and effectively.
Yearly quarter Trust performance 2008/09 Q1 (April – Jun) 4.16%Q2 (July – Sept) 3.49%Q3 (Oct – Dec) 4.61%Q4 (Jan – Mar) 4.80%Full Year 4.16%
Serious Untoward Incidents
During 2008/09 the Trust has had no serious untoward incidents involving data loss or confidentiality breach (required as part of NHS Information Governance rules).
33
Cost allocation and charging requirements
In 2008/09 the Trust has complied with the cost allocation and charging requirements set out in HM Treasury and Office of Public Sector Information Guidance.
Remuneration Report
The Remuneration Report can be found at note 5.3/1 in the enclosed Trust Accounts for the period 1st April 2008 to 31st March 2009.
Remuneration of senior managers See note 5.3/1 in the Annual Accounts
Salary See note 5.3/1 in the Annual Accounts
Other remuneration See note 5.3/1 in the Annual Accounts
Golden hellos See note 5.3/1 in the Annual Accounts
Compensation for loss of office See note 5.3/1 in the Annual Accounts
Benefits in kind See note 5.3/1 in the Annual Accounts
Pension disclosures See note 5.3/2 in the Annual Accounts
Statement of accounting officer’s responsibilities See page 46 of the Annual Accounts
Statement on internal control See page 50 of the Annual Accounts


2008/09
QuAliTy RePORT
35
An Introduction from the Chief Executive
“This last year the Trust set a new clear direction for the continued improvement of Quality in the management of patient care at CCO. The framework for this has been the development of our first Quality Strategy which the Trust Board approved in July 2008. This Quality Strategy has provided a clear focus in setting out steps to improve Patient Safety, Patient Experience and Patient Outcomes (Clinical effectiveness). Having set out this framework we will be working with all of our staff to embed the range of challenging quality initiatives that we have set ourselves. Quality is at the heart of what all of our staff aim to achieve for patients and I would like to thank our staff for the achievements that we have made this year and for their continuing commitment to deliver quality patient care for the future”
Andrew Cannell Acting Chief Executive Clatterbridge Centre for Oncology NHS Foundation Trust.
36
Quality Strategy priorities
The Trust’s Quality Strategy, approved by the Board in July 2008, defines three key strategy aims:
A. Improving Patient Safety This is divided into two steps:
Identification of avoidable harm Reduction of avoidable harm
B. Improving Patient Experience This is divided into three steps:
Understanding what impacts on the patient experience Understanding the patient experience Improving patient reported experience
C. Improving patient outcomes (clinical effectiveness) This is divided into three sections:
Understanding our outcomes Understanding how we compare Improving our outcomes
Priorities and initiatives for 2008/09
The main priorities for 2008/09 agreed within our Quality Strategy were: Patient safety: Going further to reduce Healthcare Associated Infections Patient experience: Embedding a ‘real time’ patient survey programme with clear
performance metrics Patient outcomes (clinical effectiveness): Investment in a programme to improve the
care of the acutely ill patient
Progress against each of these areas is outlined below.
Improving Patient Safety
A key target for this year was to reduce Healthcare Associated Infections such as MRSA bacteraemia and Clostridium Difficule. Our MRSA bacteraemia rate is the lowest in the country with no attributable cases being reported for 2008/09. We have also achieved the C Diff target with only 7 attributable cases this year against a maximum threshold of 19 cases.Initiatives that we have introduced this year included:
i. Investment in our infection control team with an additional infection control nurse and an increased investment with the provision of an antimicrobial pharmacist.
35
An Introduction from the Chief Executive
“This last year the Trust set a new clear direction for the continued improvement of Quality in the management of patient care at CCO. The framework for this has been the development of our first Quality Strategy which the Trust Board approved in July 2008. This Quality Strategy has provided a clear focus in setting out steps to improve Patient Safety, Patient Experience and Patient Outcomes (Clinical effectiveness). Having set out this framework we will be working with all of our staff to embed the range of challenging quality initiatives that we have set ourselves. Quality is at the heart of what all of our staff aim to achieve for patients and I would like to thank our staff for the achievements that we have made this year and for their continuing commitment to deliver quality patient care for the future”
Andrew Cannell Acting Chief Executive Clatterbridge Centre for Oncology NHS Foundation Trust.
36
Quality Strategy priorities
The Trust’s Quality Strategy, approved by the Board in July 2008, defines three key strategy aims:
A. Improving Patient Safety This is divided into two steps:
Identification of avoidable harm Reduction of avoidable harm
B. Improving Patient Experience This is divided into three steps:
Understanding what impacts on the patient experience Understanding the patient experience Improving patient reported experience
C. Improving patient outcomes (clinical effectiveness) This is divided into three sections:
Understanding our outcomes Understanding how we compare Improving our outcomes
Priorities and initiatives for 2008/09
The main priorities for 2008/09 agreed within our Quality Strategy were: Patient safety: Going further to reduce Healthcare Associated Infections Patient experience: Embedding a ‘real time’ patient survey programme with clear
performance metrics Patient outcomes (clinical effectiveness): Investment in a programme to improve the
care of the acutely ill patient
Progress against each of these areas is outlined below.
Improving Patient Safety
A key target for this year was to reduce Healthcare Associated Infections such as MRSA bacteraemia and Clostridium Difficule. Our MRSA bacteraemia rate is the lowest in the country with no attributable cases being reported for 2008/09. We have also achieved the C Diff target with only 7 attributable cases this year against a maximum threshold of 19 cases.Initiatives that we have introduced this year included:
i. Investment in our infection control team with an additional infection control nurse and an increased investment with the provision of an antimicrobial pharmacist.
37
ii. A proactive hand hygiene campaign - the success of which has been demonstrated in our national patient survey results which for two consecutive years have shown the highest scores for doctors washing their hands.
iii. The introduction of MRSA screening for all admissions ahead of the national guidance
iv. The introduction of the Productive Ward v. Review and change of our cleaning products.
Improving Patient Experience
At CCO we have set an objective to build on our current high reported levels of patient satisfaction with the aim to provide the best patient experience at what can be a very traumatic time for our patients. Having an understating of what our patients think is key to this. We participate in the national patient survey programme, however, this only provides a picture of a small percentage of our patients. It does however provide a useful benchmark to compare with other organisations including other cancer centres. Initiatives we have introduced this year include the implementation of a Patient Survey Programme. In order to obtain ‘real time’ reporting we introduced a bespoke patient survey which was rolled out to cover all patient departments. The survey programme enables all patients who finish a course of treatment or intervention to complete a simple patient survey form based on the questions contained within the national survey. Results are monitored by the Trust Board monthly and are fed back to departmental heads for information and action. Overall the survey has yielded positive results, however we have set our selves some challenging targets. These include:
Improving the patient experience to ensure a first-class personalised service in which at least 80% of patients rate as excellent through the national Healthcare Commission Survey when asked ‘Overall, how would you rate the care you received? (the results for 2008/09 show 63.4% report as excellent)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked ‘I was treated with courtesy and respect’ (the overall results for 2008/09 are 98%)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked ‘Was the ward / department clean’ (the overall results for 2008/09 are 95%)
At least 70% of patients rate as ‘never’ in the local patient survey programme when asked ‘If they had to wait’ (the overall results for 2008/09 are 17%)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked if ‘I was included in discussions about my care’ (the overall results for 2008/09 are 90%)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked if ‘the staff washed their hands’ (the overall results for 2008/09 are 92%)
Improving patient outcomes
The profile of patients receiving inpatient care at CCO has changed over the last few years with an increasing number of patients becoming acutely ill and requiring level 2 (HDU) type interventions. This may be attributed to treatment toxicity or to the co-morbidities that patients
38
present with. A review of compliance against recent NICE guidance and expert clinical advice from within the Trust supported by an external review enabled us to identify this as a priority area for us. The areas of work that we have been able to deliver in 2008/09 include:
Investment in a Critical Care Nurse Specialist to provide expert advise and support to ward staff
Agreement to access Wirral Hospital NHS Foundation Trust Critical Care Outreach service.
Investment in capital equipment including replacing all IV pumps and syringe drivers, replacing all cardiac arrest trolleys
Improved staff training in CPR, and ILS and ALERT courses. Further work will continue in this area over 2009/10 to provide level 2 care to
patients at CCO and reduce the numbers of patients being transferred out of the hospital to A+E services.
Obtained support from the Cancer Network to support these developments
Priorities and initiatives for 2009/10
Improving Patient Safety
Our Quality strategy outlines a number of priorities and initiatives for 2009/10. These include:
The establishment of Patient Safety Leadership Rounds involving all Trust Board members in line with the guidance from the National Patient Safety Initiative. Improvements in quality and safety will be monitored through our Trust Board as part of our regular quality reporting
The implementation of the Global Trigger Tool for case note / mortality reviews. Results of GTT reviews will be reviewed by the Trust Board through our Trust Board as part of our regular quality reporting
The implementation of the North West Advancing Quality nursing metrics. These will enable us to monitor improvements within the Trust and to be able to benchmark with other North West NHS Trusts.
Patient experience
From the introduction of our ‘real time’ patient survey in 2008/09 our performance in the areas relating to waiting times within departments is well below our target. We will be developing a focused action plan to ensure that we reduce waiting times to further improve the patients experience. Performance against the patient reported metrics will be closely monitored by our Trust Board as part of our Quality report. Targeted improvement in key indicators in patient survey programme focusing in particular on the waiting times in the departments.
Patient outcomes
Our patient survey provides valuable information form patients on their experience of using our service. It does not however provide validated information on patient reported outcomes (PROMS) in relation to the delivery of our core treatments (chemotherapy and radiotherapy).

37
ii. A proactive hand hygiene campaign - the success of which has been demonstrated in our national patient survey results which for two consecutive years have shown the highest scores for doctors washing their hands.
iii. The introduction of MRSA screening for all admissions ahead of the national guidance
iv. The introduction of the Productive Ward v. Review and change of our cleaning products.
Improving Patient Experience
At CCO we have set an objective to build on our current high reported levels of patient satisfaction with the aim to provide the best patient experience at what can be a very traumatic time for our patients. Having an understating of what our patients think is key to this. We participate in the national patient survey programme, however, this only provides a picture of a small percentage of our patients. It does however provide a useful benchmark to compare with other organisations including other cancer centres. Initiatives we have introduced this year include the implementation of a Patient Survey Programme. In order to obtain ‘real time’ reporting we introduced a bespoke patient survey which was rolled out to cover all patient departments. The survey programme enables all patients who finish a course of treatment or intervention to complete a simple patient survey form based on the questions contained within the national survey. Results are monitored by the Trust Board monthly and are fed back to departmental heads for information and action. Overall the survey has yielded positive results, however we have set our selves some challenging targets. These include:
Improving the patient experience to ensure a first-class personalised service in which at least 80% of patients rate as excellent through the national Healthcare Commission Survey when asked ‘Overall, how would you rate the care you received? (the results for 2008/09 show 63.4% report as excellent)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked ‘I was treated with courtesy and respect’ (the overall results for 2008/09 are 98%)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked ‘Was the ward / department clean’ (the overall results for 2008/09 are 95%)
At least 70% of patients rate as ‘never’ in the local patient survey programme when asked ‘If they had to wait’ (the overall results for 2008/09 are 17%)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked if ‘I was included in discussions about my care’ (the overall results for 2008/09 are 90%)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked if ‘the staff washed their hands’ (the overall results for 2008/09 are 92%)
Improving patient outcomes
The profile of patients receiving inpatient care at CCO has changed over the last few years with an increasing number of patients becoming acutely ill and requiring level 2 (HDU) type interventions. This may be attributed to treatment toxicity or to the co-morbidities that patients
38
present with. A review of compliance against recent NICE guidance and expert clinical advice from within the Trust supported by an external review enabled us to identify this as a priority area for us. The areas of work that we have been able to deliver in 2008/09 include:
Investment in a Critical Care Nurse Specialist to provide expert advise and support to ward staff
Agreement to access Wirral Hospital NHS Foundation Trust Critical Care Outreach service.
Investment in capital equipment including replacing all IV pumps and syringe drivers, replacing all cardiac arrest trolleys
Improved staff training in CPR, and ILS and ALERT courses. Further work will continue in this area over 2009/10 to provide level 2 care to
patients at CCO and reduce the numbers of patients being transferred out of the hospital to A+E services.
Obtained support from the Cancer Network to support these developments
Priorities and initiatives for 2009/10
Improving Patient Safety
Our Quality strategy outlines a number of priorities and initiatives for 2009/10. These include:
The establishment of Patient Safety Leadership Rounds involving all Trust Board members in line with the guidance from the National Patient Safety Initiative. Improvements in quality and safety will be monitored through our Trust Board as part of our regular quality reporting
The implementation of the Global Trigger Tool for case note / mortality reviews. Results of GTT reviews will be reviewed by the Trust Board through our Trust Board as part of our regular quality reporting
The implementation of the North West Advancing Quality nursing metrics. These will enable us to monitor improvements within the Trust and to be able to benchmark with other North West NHS Trusts.
Patient experience
From the introduction of our ‘real time’ patient survey in 2008/09 our performance in the areas relating to waiting times within departments is well below our target. We will be developing a focused action plan to ensure that we reduce waiting times to further improve the patients experience. Performance against the patient reported metrics will be closely monitored by our Trust Board as part of our Quality report. Targeted improvement in key indicators in patient survey programme focusing in particular on the waiting times in the departments.
Patient outcomes
Our patient survey provides valuable information form patients on their experience of using our service. It does not however provide validated information on patient reported outcomes (PROMS) in relation to the delivery of our core treatments (chemotherapy and radiotherapy).
39
Unfortunately we are unable to use the national PROMS tools as they are not relevant to our patient population. During 2009/10 we aim to develop validated cancer specific PROMS tools and to proactively monitor patient reported outcomes using these tools and to develop action plans to further improve patient reported outcomes.
Reports from our regulators and other external bodies
Healthcare Commission inspection: Hygiene Code
In September 2008 Trust received a planned inspection from the Healthcare Commission in relation to compliance with the Hygiene Code. Overall the report was positive however a breach was identified against Duty 4: “The trust must provide and maintain a clean and appropriate environment for healthcare”. Immediate steps were taken and all areas were rectified. The Trust was then able to declare full compliance with the Hygiene Code in its application for registration with the care Quality Commission.
Independent Risk Management Assessments
Achievement of NHSLA level 3
In November 2007 the Trust was successfully assessed against NHSLA level 3 (the highest available) and became the second Trust in the country (not including the pilot Trusts) to gain this level of attainment. The assessment reflects the Trust’s robust risk management systems and processes and the extent to which a risk aware culture is embedded in the organisation.
Maintenance of ISO 9001:2000 Standard
The ISO 9001:2000 Standard is a national (externally assessed) standard based around the principles of customer satisfaction, a systematic approach to management, and encouraging a culture of continual improvement across all departments within the Trust.
CCO is thought to have been the first NHS Trust to have achieved this accreditation for the organisation as a whole. The accreditation is reviewed periodically and it is pleasing to report that it has been retained throughout 2008/09.
Monitor
Throughout the year all of our ratings from Monitor have been the highest rating possible as follows:
Governance: green Mandatory services and assets: green Finance: 5
40
Quality Overview
The Trust has determined a number of metrics against which it can measure performance in relation to the quality of care it provides. The Trust has chosen metrics which are relevant to its speciality i.e. non-surgical oncology. However, this does mean that data is predominantly internally generated and may not be subject to benchmarking at this stage.
Trust performance against selected metrics:
Patient safety
2008/09 2007/08
MRSA bacteraemia cases / 10,000 bed days 0 0C Diff cases / 1,000 bed days 0.2 0.6‘Never Events’ that occur within the Trust 0 0Chemotherapy medication errors* (number of errors per 1,000 doses)
0.1 0.05
Radiotherapy treatment errors (number of errors per 1,000 fractions of radiotherapy)
0.76 1.17
Falls / injuries / 1,000 inpatient admissions 32 27
All indicators: Data source: CCO
Clinical Outcome (clinical effectiveness)
2008/09 2007/08
HSMR 39.3 4230 day mortality rate (radical chemotherapy) 0.4% 1.4%30 day mortality rate (palliative chemotherapy) 8.9% 7.4%30 day mortality rate (radical radiotherapy) 0.9% 1.2%30 day mortality rate (palliative radiotherapy) 17.1% 19.5%
HSMR: Data source Dr Foster
Mortality rate: Data definition: unadjusted mortality rate as a percentage of all cases treated in
that category. Data source: CCO
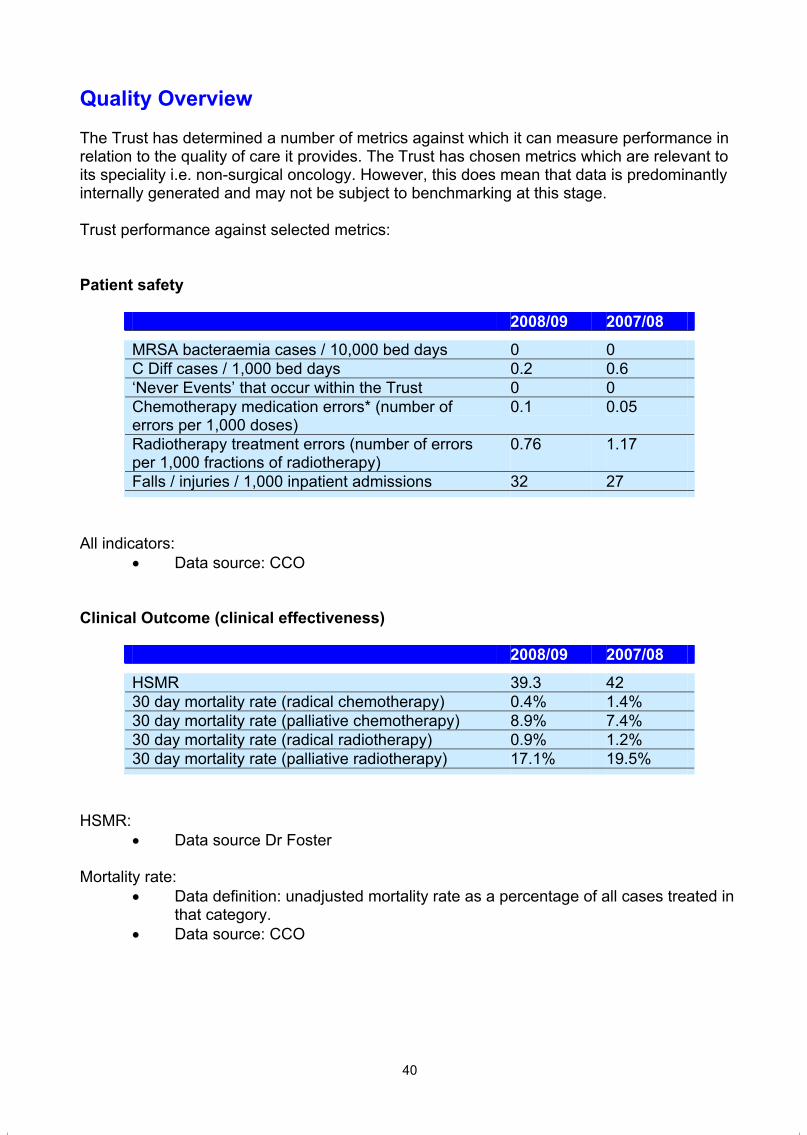
39
Unfortunately we are unable to use the national PROMS tools as they are not relevant to our patient population. During 2009/10 we aim to develop validated cancer specific PROMS tools and to proactively monitor patient reported outcomes using these tools and to develop action plans to further improve patient reported outcomes.
Reports from our regulators and other external bodies
Healthcare Commission inspection: Hygiene Code
In September 2008 Trust received a planned inspection from the Healthcare Commission in relation to compliance with the Hygiene Code. Overall the report was positive however a breach was identified against Duty 4: “The trust must provide and maintain a clean and appropriate environment for healthcare”. Immediate steps were taken and all areas were rectified. The Trust was then able to declare full compliance with the Hygiene Code in its application for registration with the care Quality Commission.
Independent Risk Management Assessments
Achievement of NHSLA level 3
In November 2007 the Trust was successfully assessed against NHSLA level 3 (the highest available) and became the second Trust in the country (not including the pilot Trusts) to gain this level of attainment. The assessment reflects the Trust’s robust risk management systems and processes and the extent to which a risk aware culture is embedded in the organisation.
Maintenance of ISO 9001:2000 Standard
The ISO 9001:2000 Standard is a national (externally assessed) standard based around the principles of customer satisfaction, a systematic approach to management, and encouraging a culture of continual improvement across all departments within the Trust.
CCO is thought to have been the first NHS Trust to have achieved this accreditation for the organisation as a whole. The accreditation is reviewed periodically and it is pleasing to report that it has been retained throughout 2008/09.
Monitor
Throughout the year all of our ratings from Monitor have been the highest rating possible as follows:
Governance: green Mandatory services and assets: green Finance: 5
40
Quality Overview
The Trust has determined a number of metrics against which it can measure performance in relation to the quality of care it provides. The Trust has chosen metrics which are relevant to its speciality i.e. non-surgical oncology. However, this does mean that data is predominantly internally generated and may not be subject to benchmarking at this stage.
Trust performance against selected metrics:
Patient safety
2008/09 2007/08
MRSA bacteraemia cases / 10,000 bed days 0 0C Diff cases / 1,000 bed days 0.2 0.6‘Never Events’ that occur within the Trust 0 0Chemotherapy medication errors* (number of errors per 1,000 doses)
0.1 0.05
Radiotherapy treatment errors (number of errors per 1,000 fractions of radiotherapy)
0.76 1.17
Falls / injuries / 1,000 inpatient admissions 32 27
All indicators: Data source: CCO
Clinical Outcome (clinical effectiveness)
2008/09 2007/08
HSMR 39.3 4230 day mortality rate (radical chemotherapy) 0.4% 1.4%30 day mortality rate (palliative chemotherapy) 8.9% 7.4%30 day mortality rate (radical radiotherapy) 0.9% 1.2%30 day mortality rate (palliative radiotherapy) 17.1% 19.5%
HSMR: Data source Dr Foster
Mortality rate: Data definition: unadjusted mortality rate as a percentage of all cases treated in
that category. Data source: CCO
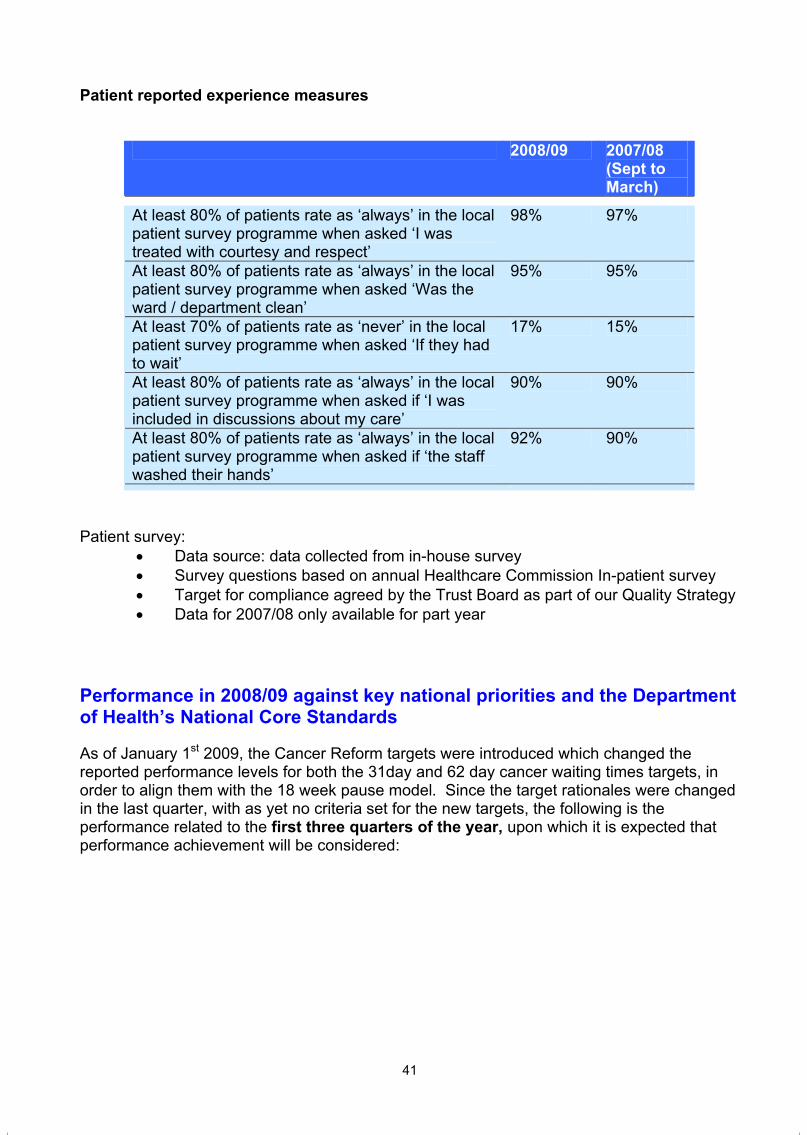
41
Patient reported experience measures
2008/09 2007/08(Sept to March)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked ‘I was treated with courtesy and respect’
98% 97%
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked ‘Was the ward / department clean’
95% 95%
At least 70% of patients rate as ‘never’ in the local patient survey programme when asked ‘If they had to wait’
17% 15%
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked if ‘I was included in discussions about my care’
90% 90%
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked if ‘the staff washed their hands’
92% 90%
Patient survey: Data source: data collected from in-house survey Survey questions based on annual Healthcare Commission In-patient survey Target for compliance agreed by the Trust Board as part of our Quality Strategy Data for 2007/08 only available for part year
Performance in 2008/09 against key national priorities and the Department of Health’s National Core Standards
As of January 1st 2009, the Cancer Reform targets were introduced which changed the reported performance levels for both the 31day and 62 day cancer waiting times targets, in order to align them with the 18 week pause model. Since the target rationales were changed in the last quarter, with as yet no criteria set for the new targets, the following is the performance related to the first three quarters of the year, upon which it is expected that performance achievement will be considered:
42
2008/09 2007/08
Standards for Better Health declaration
Declared full compliance with all standards throughout year and at year end
Declared full compliance with all standards except one throughout year and full compliance at year end
C Diff target 7 ( target no more than 19)
26 (target no more than 11 cases)
MRSA target 0 (target no more than 2)
0 (target no more than 2)
2 week wait 100% 100%
31 day 99.8% (target threshold 98%).
99.8% (target 98%)
62 day 93.3% (target threshold 93%).
94.7% (target 93%)
18 week (admitted) As at March 2009, 97.3% (target of 90%)
95.9% (target 85%)
18 week (non admitted) 98.5% (target95%).
96% (target 90%)

41
Patient reported experience measures
2008/09 2007/08(Sept to March)
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked ‘I was treated with courtesy and respect’
98% 97%
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked ‘Was the ward / department clean’
95% 95%
At least 70% of patients rate as ‘never’ in the local patient survey programme when asked ‘If they had to wait’
17% 15%
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked if ‘I was included in discussions about my care’
90% 90%
At least 80% of patients rate as ‘always’ in the local patient survey programme when asked if ‘the staff washed their hands’
92% 90%
Patient survey: Data source: data collected from in-house survey Survey questions based on annual Healthcare Commission In-patient survey Target for compliance agreed by the Trust Board as part of our Quality Strategy Data for 2007/08 only available for part year
Performance in 2008/09 against key national priorities and the Department of Health’s National Core Standards
As of January 1st 2009, the Cancer Reform targets were introduced which changed the reported performance levels for both the 31day and 62 day cancer waiting times targets, in order to align them with the 18 week pause model. Since the target rationales were changed in the last quarter, with as yet no criteria set for the new targets, the following is the performance related to the first three quarters of the year, upon which it is expected that performance achievement will be considered:
42
2008/09 2007/08
Standards for Better Health declaration
Declared full compliance with all standards throughout year and at year end
Declared full compliance with all standards except one throughout year and full compliance at year end
C Diff target 7 ( target no more than 19)
26 (target no more than 11 cases)
MRSA target 0 (target no more than 2)
0 (target no more than 2)
2 week wait 100% 100%
31 day 99.8% (target threshold 98%).
99.8% (target 98%)
62 day 93.3% (target threshold 93%).
94.7% (target 93%)
18 week (admitted) As at March 2009, 97.3% (target of 90%)
95.9% (target 85%)
18 week (non admitted) 98.5% (target95%).
96% (target 90%)


2008/09
AnnuAl ACCounTS FOR THe 12 MONTHS eNDeD 31ST MARCH 2009
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
44
Contents
Foreword to the Accounts 45
Statement of the Chief Executive's responsibilities as the accounting officer of 46 Clatterbridge Centre for Oncology NHS Foundation Trust.
Statement of Directors' responsibilities in respect of the Accounts 47
Independent Auditor's Report to the Council 48-49
Statement of Internal Control 50-54
Accounting Policies 55-63
Income and Expenditure Account 64
Balance Sheet 65
Statement of Total Recognised Gains and Losses 66
Cash Flow Statement 67
Notes to the Accounts 64-92
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
45
Foreword to the Accounts
Clatterbridge Centre for Oncology NHS Foundation Trust
The accounts for the 12 months ended 31 March 2009, have been prepared by the Clatterbridge Centre for Oncology NHS Foundation Trust in accordance with paragraph 24 and 25 of Schedule 7 of the National Health Services Act 2006 in the form which Monitor has, with the approval of the Treasury directed.
Andrew Cannell Date 8th June 2009 Acting Chief Executive
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
44
Contents
Foreword to the Accounts 45
Statement of the Chief Executive's responsibilities as the accounting officer of 46 Clatterbridge Centre for Oncology NHS Foundation Trust.
Statement of Directors' responsibilities in respect of the Accounts 47
Independent Auditor's Report to the Council 48-49
Statement of Internal Control 50-54
Accounting Policies 55-63
Income and Expenditure Account 64
Balance Sheet 65
Statement of Total Recognised Gains and Losses 66
Cash Flow Statement 67
Notes to the Accounts 64-92
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
45
Foreword to the Accounts
Clatterbridge Centre for Oncology NHS Foundation Trust
The accounts for the 12 months ended 31 March 2009, have been prepared by the Clatterbridge Centre for Oncology NHS Foundation Trust in accordance with paragraph 24 and 25 of Schedule 7 of the National Health Services Act 2006 in the form which Monitor has, with the approval of the Treasury directed.
Andrew Cannell Date 8th June 2009 Acting Chief Executive
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
46
Statement of Chief Executive's Responsibilities as the Accounting Officer of Clatterbridge Centre for Oncology NHS Foundation Trust
The National Health Services Act 2006 states that the Chief Executive is the accounting officer of the NHS Foundation Trust. The relevant responsibilities of accounting officer, including their responsibility for the propriety and regularity of public finances for which they are answerable, and for the keeping of proper accounts, are set out in the accounting officers' Memorandum issued by the Independent Regulator of NHS Foundation Trusts (“Monitor”).
Under the National Health Services Act 2006, Monitor has directed the Clatterbridge Centre for Oncology NHS Foundation Trust to prepare for each financial year a statement of accounts in the form and on the basis set out in the Accounts Direction. The accounts are prepared on an accruals basis and must give a true and fair view of the state of affairs of Clatterbridge Centre for Oncology NHS Foundation Trust and of its income and expenditure, total recognised gains and losses and cash flows for the financial year.
In preparing the accounts, the Accounting Officer is required to comply with the requirements of the NHS foundation trust Financial Reporting Manual and in particular to:
- observe the Accounts Direction issued by Monitor, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis;
- make judgements and estimates on a reasonable basis;
- state whether applicable accounting standards as set out in the NHS foundation trust Financial Reporting Manual have been followed, and disclose and explain any material departures in the financial statements; and
- prepare the financial statements on a going concern basis
The Accounting Officer is responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the NHS Foundation Trust and to enable him to ensure that the accounts comply with requirements outlined in the above mentioned Act. The Accounting Officer is also responsible for safeguarding the assets of the NHS Foundation Trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in Monitor's NHS Foundation Trust Accounting Officer Memorandum.
Andrew Cannell 8th June 2009 Acting Chief Executive
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
47
Statement of Directors' Responsibilities in Respect of the Accounts
The Directors are required under the National Health Services Act 2006 to prepare accounts for each financial year. Monitor, with the approval of the Treasury, directs that these accounts give a true and fair view of the state of affairs of the Trust and of the income & expenditure of the Trust for that period. In preparing those accounts, the Directors are required to;
select suitable accounting policies, as described on pages 55-63, and them apply them consistently
make judgements and estimates on a reasonable basis;
state whether applicable accounting standards have been followed, subject to any material departures disclosed and explained in the accounts;
prepare accounts on the going concern basis unless it is inappropriate to presume that the Trust will continue in business.
The Directors are responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the Trust and to enable them to ensure that the accounts comply with requirements outlined in the above mentioned direction of Monitor. The Directors are also responsible for safeguarding the assets of the Trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
The Directors confirm to the best of their knowledge and belief that they have complied with the above requirements in preparing the accounts.
By Order of the Board
Andrew Cannell 8th June 2009 Acting Chief Executive
John Andrews 8th June 2009 Acting Director of Finance
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
46
Statement of Chief Executive's Responsibilities as the Accounting Officer of Clatterbridge Centre for Oncology NHS Foundation Trust
The National Health Services Act 2006 states that the Chief Executive is the accounting officer of the NHS Foundation Trust. The relevant responsibilities of accounting officer, including their responsibility for the propriety and regularity of public finances for which they are answerable, and for the keeping of proper accounts, are set out in the accounting officers' Memorandum issued by the Independent Regulator of NHS Foundation Trusts (“Monitor”).
Under the National Health Services Act 2006, Monitor has directed the Clatterbridge Centre for Oncology NHS Foundation Trust to prepare for each financial year a statement of accounts in the form and on the basis set out in the Accounts Direction. The accounts are prepared on an accruals basis and must give a true and fair view of the state of affairs of Clatterbridge Centre for Oncology NHS Foundation Trust and of its income and expenditure, total recognised gains and losses and cash flows for the financial year.
In preparing the accounts, the Accounting Officer is required to comply with the requirements of the NHS foundation trust Financial Reporting Manual and in particular to:
- observe the Accounts Direction issued by Monitor, including the relevant accounting and disclosure requirements, and apply suitable accounting policies on a consistent basis;
- make judgements and estimates on a reasonable basis;
- state whether applicable accounting standards as set out in the NHS foundation trust Financial Reporting Manual have been followed, and disclose and explain any material departures in the financial statements; and
- prepare the financial statements on a going concern basis
The Accounting Officer is responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the NHS Foundation Trust and to enable him to ensure that the accounts comply with requirements outlined in the above mentioned Act. The Accounting Officer is also responsible for safeguarding the assets of the NHS Foundation Trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
To the best of my knowledge and belief, I have properly discharged the responsibilities set out in Monitor's NHS Foundation Trust Accounting Officer Memorandum.
Andrew Cannell 8th June 2009 Acting Chief Executive
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
47
Statement of Directors' Responsibilities in Respect of the Accounts
The Directors are required under the National Health Services Act 2006 to prepare accounts for each financial year. Monitor, with the approval of the Treasury, directs that these accounts give a true and fair view of the state of affairs of the Trust and of the income & expenditure of the Trust for that period. In preparing those accounts, the Directors are required to;
select suitable accounting policies, as described on pages 55-63, and them apply them consistently
make judgements and estimates on a reasonable basis;
state whether applicable accounting standards have been followed, subject to any material departures disclosed and explained in the accounts;
prepare accounts on the going concern basis unless it is inappropriate to presume that the Trust will continue in business.
The Directors are responsible for keeping proper accounting records which disclose with reasonable accuracy at any time the financial position of the Trust and to enable them to ensure that the accounts comply with requirements outlined in the above mentioned direction of Monitor. The Directors are also responsible for safeguarding the assets of the Trust and hence for taking reasonable steps for the prevention and detection of fraud and other irregularities.
The Directors confirm to the best of their knowledge and belief that they have complied with the above requirements in preparing the accounts.
By Order of the Board
Andrew Cannell 8th June 2009 Acting Chief Executive
John Andrews 8th June 2009 Acting Director of Finance
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
48
Auditors’ Report to the Council of Governors of Clatterbridge Centre for Oncology NHS Foundation Trust
We have audited the financial statements of Clatterbridge Centre for Oncology NHS Foundation Trust for the year ended 31 March 2009 under the National Health Service Act 2006. These comprise the Income and Expenditure Account, the Balance Sheet, the Cash flow Statement, the Statement of Total Recognised Gains and Losses and the related notes. These financial statements have been prepared under the accounting policies relevant to NHS Foundation Trusts set out therein.
This report is made solely to the Council of Governors of Clatterbridge Centre for Oncology NHS Foundation Trust (‘the Trust’), as a body, in accordance with the National Health Service Act 2006. Our audit work has been undertaken so that we might state to the Council of Governors of the Trust, as a body, those matters we are required to state to it in an auditor’s report and for no other purpose. To the fullest extent permitted by law, we do not accept or assume responsibility to anyone other than the Trust and the Trust's Governors as a body, for our audit work, for this report, or for the opinions we have formed.
Respective responsibilities of directors and auditors As described on page 46, the Accounting Officer is responsible for the preparation of the financial statements in accordance with directions issued by Monitor. Our responsibilities, as independent auditors, are established by statute, the Code of Audit Practice issued by Monitor and our profession’s ethical guidance.
We report to you our opinion as to whether the financial statements give a true and fair view of the state of affairs of the Trust and its income and expenditure for the year ended 31 March 2009. We review whether the statement on internal control on pages 50 to 54 reflects compliance with Monitor’s guidance issued in the NHS Foundation Trust Financial Reporting Manual. We report if it does not meet the requirements specified by Monitor or if the statement is misleading or inconsistent with other information we are aware of from our audit of the financial statements. We are not required to consider, nor have we considered, whether the directors’ statement on internal control covers all risks and controls. We are also not required to form an opinion on the effectiveness of the Trust’s corporate governance procedures or its risk and control procedures. Our review was not performed for any purpose connected with any specific transaction and should not be relied upon for any such purpose.
We read the information contained in the Annual Report and consider the implications for our report if we become aware of any apparent misstatements or material inconsistencies with the statement of accounts.
Basis of audit opinionWe conducted our audit in accordance with the National Health Service Act 2006 and the Code of Audit Practice issued by Monitor, which requires compliance with relevant auditing standards issued by the Auditing Practices Board.
An audit includes examination, on a test basis, of evidence relevant to the amounts and disclosures in the financial statements. It also includes an assessment of the significant estimates and judgements made by the Directors in the preparation of the financial statements, and of whether the accounting policies are appropriate to the Trust's circumstances, consistently applied and adequately disclosed.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
49
We planned and performed our audit so as to obtain all the information and explanations which we considered necessary in order to provide us with sufficient evidence to give reasonable assurance that the financial statements are free from material misstatement, whether caused by fraud or other irregularity or error. In forming our opinion we also evaluated the overall adequacy of the presentation of information in the financial statements.
Opinion In our opinion:
the financial statements give a true and fair view, in accordance with the accounting policies directed by Monitor as being relevant to NHS Foundation Trusts in England, of the state of the Trust’s affairs as at 31 March 2009 and of its income and expenditure for the year then ended; and
the part of the Remuneration Report to be audited has been properly prepared in accordance with the requirements of the NHS Foundation Trust Financial Reporting Manual.
Certificate We certify that we have completed the audit of the accounts in accordance with the requirements of the National Health Service Act 2006 and the NHS Foundation Trust Audit Code of Practice issued by Monitor.
Trevor Rees (Senior Statutory Auditor) for and on behalf of KPMG LLP, Statutory Auditor
Chartered Accountants KPMG LLP St James’ Square ManchesterM2 6DS
3 June 2009
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
48
Auditors’ Report to the Council of Governors of Clatterbridge Centre for Oncology NHS Foundation Trust
We have audited the financial statements of Clatterbridge Centre for Oncology NHS Foundation Trust for the year ended 31 March 2009 under the National Health Service Act 2006. These comprise the Income and Expenditure Account, the Balance Sheet, the Cash flow Statement, the Statement of Total Recognised Gains and Losses and the related notes. These financial statements have been prepared under the accounting policies relevant to NHS Foundation Trusts set out therein.
This report is made solely to the Council of Governors of Clatterbridge Centre for Oncology NHS Foundation Trust (‘the Trust’), as a body, in accordance with the National Health Service Act 2006. Our audit work has been undertaken so that we might state to the Council of Governors of the Trust, as a body, those matters we are required to state to it in an auditor’s report and for no other purpose. To the fullest extent permitted by law, we do not accept or assume responsibility to anyone other than the Trust and the Trust's Governors as a body, for our audit work, for this report, or for the opinions we have formed.
Respective responsibilities of directors and auditors As described on page 46, the Accounting Officer is responsible for the preparation of the financial statements in accordance with directions issued by Monitor. Our responsibilities, as independent auditors, are established by statute, the Code of Audit Practice issued by Monitor and our profession’s ethical guidance.
We report to you our opinion as to whether the financial statements give a true and fair view of the state of affairs of the Trust and its income and expenditure for the year ended 31 March 2009. We review whether the statement on internal control on pages 50 to 54 reflects compliance with Monitor’s guidance issued in the NHS Foundation Trust Financial Reporting Manual. We report if it does not meet the requirements specified by Monitor or if the statement is misleading or inconsistent with other information we are aware of from our audit of the financial statements. We are not required to consider, nor have we considered, whether the directors’ statement on internal control covers all risks and controls. We are also not required to form an opinion on the effectiveness of the Trust’s corporate governance procedures or its risk and control procedures. Our review was not performed for any purpose connected with any specific transaction and should not be relied upon for any such purpose.
We read the information contained in the Annual Report and consider the implications for our report if we become aware of any apparent misstatements or material inconsistencies with the statement of accounts.
Basis of audit opinionWe conducted our audit in accordance with the National Health Service Act 2006 and the Code of Audit Practice issued by Monitor, which requires compliance with relevant auditing standards issued by the Auditing Practices Board.
An audit includes examination, on a test basis, of evidence relevant to the amounts and disclosures in the financial statements. It also includes an assessment of the significant estimates and judgements made by the Directors in the preparation of the financial statements, and of whether the accounting policies are appropriate to the Trust's circumstances, consistently applied and adequately disclosed.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
49
We planned and performed our audit so as to obtain all the information and explanations which we considered necessary in order to provide us with sufficient evidence to give reasonable assurance that the financial statements are free from material misstatement, whether caused by fraud or other irregularity or error. In forming our opinion we also evaluated the overall adequacy of the presentation of information in the financial statements.
Opinion In our opinion:
the financial statements give a true and fair view, in accordance with the accounting policies directed by Monitor as being relevant to NHS Foundation Trusts in England, of the state of the Trust’s affairs as at 31 March 2009 and of its income and expenditure for the year then ended; and
the part of the Remuneration Report to be audited has been properly prepared in accordance with the requirements of the NHS Foundation Trust Financial Reporting Manual.
Certificate We certify that we have completed the audit of the accounts in accordance with the requirements of the National Health Service Act 2006 and the NHS Foundation Trust Audit Code of Practice issued by Monitor.
Trevor Rees (Senior Statutory Auditor) for and on behalf of KPMG LLP, Statutory Auditor
Chartered Accountants KPMG LLP St James’ Square ManchesterM2 6DS
3 June 2009
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
50
Statement of Internal Control
1. Scope of responsibility
As Accounting Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the NHS Foundation Trust’s policies, aims and objectives, whilst safeguarding the public funds and departmental assets for which I am personally responsible, in accordance with the responsibilities assigned to me. I am also responsible for ensuring that the NHS foundation trust is administered prudently and economically and that resources are applied efficiently and effectively. I also acknowledge my responsibilities as set out in the NHS Foundation Trust Accounting Officer Memorandum.
In my role of Chief Executive I account to the Chairman and Board of Clatterbridge Centre for Oncology NHS Foundation Trust for all matters pertaining to the delivery of strategic and operational objectives of the Trust. I hold key responsibilities for ensuring financial duties are met, clinical governance systems are robust and the development of effective partnerships with external organisations and bodies and internally with staff. To support this role there are clear systems of accountability with each Executive Director having delegated areas of operational responsibility.
In order to achieve my responsibilities a governance and management framework has been established.
Central to the organisation’s strategic management of risk identification and control is the Service Development Strategy and Annual Plans. In addition, the Trust Board regularly reviews performance monitoring and management of the Trust’s strategic objectives.
Personal objectives are agreed for all directly managed staff ensuring direct linkage to the Trust’s Service Development Strategy.
The Trust has in place a Corporate Governance Manual supported by a detailed Scheme of Reservation and Delegation, outlining statutory and operational responsibilities.
A review of the workings and membership of the Board, including the role and function of the sub-committees is undertaken, in line with guidance on integrated governance. This supports the strategic direction of the Trust and the management of risk through the Assurance Framework.
Ensuring managers’ awareness and compliance with policies and procedures takes place, including NHS codes of conduct.
The Foundation Trust operates under a formal Foundation Trust constitution.
The Trust’s principal commissioning partners are Wirral PCT who acts as co-ordinating commissioner for the other PCTs in our catchment area, supported by the Cheshire and Merseyside Specialised Commissioning Team.
2. The Purpose of the system of Internal Control
The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an ongoing process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of Clatterbridge Centre for Oncology NHS Foundation Trust, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control has been in place in Clatterbridge Centre for Oncology NHS Foundation Trust for the year ended 31 March 2009 and up to the date of approval of the annual report and accounts.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
51
As an employer with staff entitled to membership of the NHS Pension Scheme control measures are in place to ensure all employer obligations contained within the Scheme regulations are complied with.
3. Capacity to handle risk
The Trust is committed to providing high quality services in a safe and secure environment. As Chief Executive I have overall responsibility and accountability for all aspects of risk management within the Trust, making sure that the organisational structure and resources are in place to ensure this occurs. Senior leadership is delegated through the directors and operationally through departments and committee structures. This covers all aspects of governance relating to our service delivery, including: infection control, clinical care, radiation protection, Standards for Better Health, finance, contracts, information technology, health and safety, cancer standards peer review, research, and employment practices.
The Audit Committee has overarching responsibility for ensuring that risk is managed effectively within the organisation. This role is supported by Board committees that oversee specific aspects of the risk portfolio.
The system provides a central steer whilst supporting local ownership in managing and controlling risks to which the Trust may be exposed.
These systems are further supported by the evaluation of the effectiveness of risk management and control systems and implementation of recommendations from external assessments to promote both organisational and individual learning and the dissemination of good practice within the Trust.
4. The Risk and Control Framework
The key elements of the Trust’s Risk Management Strategy are to, manage and control identified risks, whether clinical, non-clinical or financial, appropriately. This is achieved through a sound organisational framework, which promotes early identification of risk, the co-ordination of risk management activity, the provision of a safe environment for staff and patients, and the effective use of financial resources. It ensures that staff is aware of their roles and responsibilities and outlines the structures and processes through which risk is assessed, controlled and managed.
Risks are identified through feedback from many sources, such as, formal risk assessment, incident reporting, audit data, complaints, legal claims, patient and public feedback, stakeholder/partnership feedback and internal/external assessment.
The Trust Board endorsed the Quality Strategy, the Operational Budget Plan and the Risk Management Strategy. In addition, a range of Trust-wide policies and procedures further supports the risk management processes.
The Trust has embedded an assurance framework at a corporate level and across all areas of the organisation. The corporate assurance framework identifies those risks deemed as strategically significant to the Trust’s objectives, the controls in place to manage / mitigate those risks and the assurances received by the Trust. All Board members have been involved in the development, identification, quantification and prioritisation of the risks and the subsequent action planning to address areas for improvement. Significant risks are escalated to the Trust Board as they arise and subsequent updates are made to the Assurance Framework. The cascading of these processes to directorates has commenced the embedding of these principles across the organisation. This assists with the development of an organisation wide risk aware culture.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
50
Statement of Internal Control
1. Scope of responsibility
As Accounting Officer, I have responsibility for maintaining a sound system of internal control that supports the achievement of the NHS Foundation Trust’s policies, aims and objectives, whilst safeguarding the public funds and departmental assets for which I am personally responsible, in accordance with the responsibilities assigned to me. I am also responsible for ensuring that the NHS foundation trust is administered prudently and economically and that resources are applied efficiently and effectively. I also acknowledge my responsibilities as set out in the NHS Foundation Trust Accounting Officer Memorandum.
In my role of Chief Executive I account to the Chairman and Board of Clatterbridge Centre for Oncology NHS Foundation Trust for all matters pertaining to the delivery of strategic and operational objectives of the Trust. I hold key responsibilities for ensuring financial duties are met, clinical governance systems are robust and the development of effective partnerships with external organisations and bodies and internally with staff. To support this role there are clear systems of accountability with each Executive Director having delegated areas of operational responsibility.
In order to achieve my responsibilities a governance and management framework has been established.
Central to the organisation’s strategic management of risk identification and control is the Service Development Strategy and Annual Plans. In addition, the Trust Board regularly reviews performance monitoring and management of the Trust’s strategic objectives.
Personal objectives are agreed for all directly managed staff ensuring direct linkage to the Trust’s Service Development Strategy.
The Trust has in place a Corporate Governance Manual supported by a detailed Scheme of Reservation and Delegation, outlining statutory and operational responsibilities.
A review of the workings and membership of the Board, including the role and function of the sub-committees is undertaken, in line with guidance on integrated governance. This supports the strategic direction of the Trust and the management of risk through the Assurance Framework.
Ensuring managers’ awareness and compliance with policies and procedures takes place, including NHS codes of conduct.
The Foundation Trust operates under a formal Foundation Trust constitution.
The Trust’s principal commissioning partners are Wirral PCT who acts as co-ordinating commissioner for the other PCTs in our catchment area, supported by the Cheshire and Merseyside Specialised Commissioning Team.
2. The Purpose of the system of Internal Control
The system of internal control is designed to manage risk to a reasonable level rather than to eliminate all risk of failure to achieve policies, aims and objectives; it can therefore only provide reasonable and not absolute assurance of effectiveness. The system of internal control is based on an ongoing process designed to identify and prioritise the risks to the achievement of the policies, aims and objectives of Clatterbridge Centre for Oncology NHS Foundation Trust, to evaluate the likelihood of those risks being realised and the impact should they be realised, and to manage them efficiently, effectively and economically. The system of internal control has been in place in Clatterbridge Centre for Oncology NHS Foundation Trust for the year ended 31 March 2009 and up to the date of approval of the annual report and accounts.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
51
As an employer with staff entitled to membership of the NHS Pension Scheme control measures are in place to ensure all employer obligations contained within the Scheme regulations are complied with.
3. Capacity to handle risk
The Trust is committed to providing high quality services in a safe and secure environment. As Chief Executive I have overall responsibility and accountability for all aspects of risk management within the Trust, making sure that the organisational structure and resources are in place to ensure this occurs. Senior leadership is delegated through the directors and operationally through departments and committee structures. This covers all aspects of governance relating to our service delivery, including: infection control, clinical care, radiation protection, Standards for Better Health, finance, contracts, information technology, health and safety, cancer standards peer review, research, and employment practices.
The Audit Committee has overarching responsibility for ensuring that risk is managed effectively within the organisation. This role is supported by Board committees that oversee specific aspects of the risk portfolio.
The system provides a central steer whilst supporting local ownership in managing and controlling risks to which the Trust may be exposed.
These systems are further supported by the evaluation of the effectiveness of risk management and control systems and implementation of recommendations from external assessments to promote both organisational and individual learning and the dissemination of good practice within the Trust.
4. The Risk and Control Framework
The key elements of the Trust’s Risk Management Strategy are to, manage and control identified risks, whether clinical, non-clinical or financial, appropriately. This is achieved through a sound organisational framework, which promotes early identification of risk, the co-ordination of risk management activity, the provision of a safe environment for staff and patients, and the effective use of financial resources. It ensures that staff is aware of their roles and responsibilities and outlines the structures and processes through which risk is assessed, controlled and managed.
Risks are identified through feedback from many sources, such as, formal risk assessment, incident reporting, audit data, complaints, legal claims, patient and public feedback, stakeholder/partnership feedback and internal/external assessment.
The Trust Board endorsed the Quality Strategy, the Operational Budget Plan and the Risk Management Strategy. In addition, a range of Trust-wide policies and procedures further supports the risk management processes.
The Trust has embedded an assurance framework at a corporate level and across all areas of the organisation. The corporate assurance framework identifies those risks deemed as strategically significant to the Trust’s objectives, the controls in place to manage / mitigate those risks and the assurances received by the Trust. All Board members have been involved in the development, identification, quantification and prioritisation of the risks and the subsequent action planning to address areas for improvement. Significant risks are escalated to the Trust Board as they arise and subsequent updates are made to the Assurance Framework. The cascading of these processes to directorates has commenced the embedding of these principles across the organisation. This assists with the development of an organisation wide risk aware culture.

Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
52
The Trust has appointed an Executive Director as the Senior Information Risk Officer. Risks relating to data are assessed through the completion of the Department of Health’s Information Governance Toolkit. The Trust has assessed itself as securing a score of 89% (a “Green” rating) against the Department of Health’s Information Governance Toolkit in 2008/09; The Trust achieved Level 2 against the requirements of the Information Governance statement of Compliance as required by Monitor’s Compliance Framework. Where relevant information risks identified in the course of the Trust’s incident reporting processes are investigated and lessons learned. The implementation of the Trust’s IM&T Strategy, including the application of data security principles continues to be subject to scrutiny at the Information Management & Technology (IM&T) Committee of the Trust Board.
In respect of public involvement the Trust has both a Patient & Public Involvement Strategy and a Membership Strategy. The latter has been implemented and in excess of 5,400 public members have been recruited to date. Elections for places within the Council of Governors are undertaken each year in conjunction with the Electoral Reform Services and the governance infrastructure was in place to enable the trust to operate effectively as an NHS Foundation Trust from 1st
August 2006. This work strengthens the input of patients, the public and staff into the strategic decision making of the Trust.
The risk and control framework continues to be reviewed and developed. In 2009/10 this will include:
Continued departmental embedding of the Assurance Framework, to ensure systematic mapping of risks to objectives throughout the organisation. Review the approved Trust Board committee structure in line with the principles of Integrated Governance to ensure its continued effectiveness. Continue to develop the operation of the Trust’s Risk Register Continue to maintain full compliance with the Standards for Better Health Core Standards The Trust continues to work with and develop arrangements with third party organisations within the Local Health Economy and on a wider scale to ensure delivery of quality healthcare services and secure appropriate funding. Continuous improvements will be made in 2009/10 in order to meet the new “going further on cancer waits” cancer waiting time standards. Work towards compliance with the new regulations for health and social care required by The Health and Social Care Act (2008) There are a number of new or emerging risks which have been considered in 2008/09 that will be kept under review. These include; risks in respect of Vision 20:20, the Trust’s response to the emerging shared services agenda (including the potential risks associated with a change to payroll provider and general ledger), maintaining income flows and key relationships with commissioners and implications of Payment by Results for specific cancer related services and the development of the proposed Satellite Radiotherapy Centre at Walton/Aintree.
5 Review of economy, efficiency and effectiveness and the use of resources
As the Accounting Officer, I am responsible for ensuring that the organisation has arrangements in place to secure value for money in the use of resources. The Trust achieves this through the following systems:
o Setting and monitor the delivery of strategic and operational objectives Monitoring and review of organisational performance Delivery of efficiency savings
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
53
Annually the Trust produces a service strategy which incorporates a supporting financial plan for approval by the Board of Directors. The strategy approved by the Board of Directors informs the detailed annual financial and performance plans. The Board monitors performance monthly through the corporate Finance & Performance Report, which provides information on current and forecast financial performance, achievement of savings targets, capital investment, contract activity and performance against key targets.
Reports on specific issues relating to economy, efficiency and effectiveness are commissioned by the Audit Committee from the Trust’s Internal Auditors and it also receives reports from the External Auditors as required. The Audit committee monitors closely the implementation of Audit recommendations.
Effective performance has been demonstrated through:
The achievement of the majority of key NHS targets A financial risk rating of 5 as determined by the independent regulator Monitor.
6 Review of Effectiveness
As the Accounting Officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review of the effectiveness of the system of internal control is informed by the work of the internal auditors and the executive managers within the NHS Foundation Trust who have responsibility for the development and maintenance of the internal control framework, and comments made by the external auditors in their management letter and other reports. I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the Board, the audit committee and a plan to address weaknesses and ensure continuous improvement of the system is in place.
The Board of Directors reviews performance across a range of indicators, which include both corporate and national objectives:
Waiting times are a critical indicator of success in terms of improving access for patients. The targets have been revised for Quarter 4. The achievement under the original methodology for the first three quarters has been 99.8% (operational target 98%) for the 31 day from decision to treat to first treatment and 93.3% (operational target 93%) against the 62-day urgent referral to first treatment target. The key issue to the Trust in continuing to achieve the 62-day target in the future is the timely referrals of patients from other hospitals.
The Trust is monitoring performance against the new cancer waiting time targets methodology introduced in quarter 4. The Trust achieved 98.7% against the 31 day subsequent treatment measure and 78.0% against the 62 day measure. Operational targets are still awaited from the Department of Health for these new measures of waiting time performance.
A “green” rating by Monitor for each quarter in 2008/09 for governance A “green” rating by Monitor for each quarter in 2008/09 for the provision of mandatory
services. Achievement of all key financial duties and a Monitor financial risk rating of 5 for each quarter
in 2008/09. Internal Audit concluded that the systems and processes in place regarding the Assurance
Framework are designed and operated to meet the requirements of the Statement of Internal Control. High Assurance has been received for this. They have also provided significant assurance regarding the systems and processes underpinning the Standards for Better Health
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
52
The Trust has appointed an Executive Director as the Senior Information Risk Officer. Risks relating to data are assessed through the completion of the Department of Health’s Information Governance Toolkit. The Trust has assessed itself as securing a score of 89% (a “Green” rating) against the Department of Health’s Information Governance Toolkit in 2008/09; The Trust achieved Level 2 against the requirements of the Information Governance statement of Compliance as required by Monitor’s Compliance Framework. Where relevant information risks identified in the course of the Trust’s incident reporting processes are investigated and lessons learned. The implementation of the Trust’s IM&T Strategy, including the application of data security principles continues to be subject to scrutiny at the Information Management & Technology (IM&T) Committee of the Trust Board.
In respect of public involvement the Trust has both a Patient & Public Involvement Strategy and a Membership Strategy. The latter has been implemented and in excess of 5,400 public members have been recruited to date. Elections for places within the Council of Governors are undertaken each year in conjunction with the Electoral Reform Services and the governance infrastructure was in place to enable the trust to operate effectively as an NHS Foundation Trust from 1st
August 2006. This work strengthens the input of patients, the public and staff into the strategic decision making of the Trust.
The risk and control framework continues to be reviewed and developed. In 2009/10 this will include:
Continued departmental embedding of the Assurance Framework, to ensure systematic mapping of risks to objectives throughout the organisation. Review the approved Trust Board committee structure in line with the principles of Integrated Governance to ensure its continued effectiveness. Continue to develop the operation of the Trust’s Risk Register Continue to maintain full compliance with the Standards for Better Health Core Standards The Trust continues to work with and develop arrangements with third party organisations within the Local Health Economy and on a wider scale to ensure delivery of quality healthcare services and secure appropriate funding. Continuous improvements will be made in 2009/10 in order to meet the new “going further on cancer waits” cancer waiting time standards. Work towards compliance with the new regulations for health and social care required by The Health and Social Care Act (2008) There are a number of new or emerging risks which have been considered in 2008/09 that will be kept under review. These include; risks in respect of Vision 20:20, the Trust’s response to the emerging shared services agenda (including the potential risks associated with a change to payroll provider and general ledger), maintaining income flows and key relationships with commissioners and implications of Payment by Results for specific cancer related services and the development of the proposed Satellite Radiotherapy Centre at Walton/Aintree.
5 Review of economy, efficiency and effectiveness and the use of resources
As the Accounting Officer, I am responsible for ensuring that the organisation has arrangements in place to secure value for money in the use of resources. The Trust achieves this through the following systems:
o Setting and monitor the delivery of strategic and operational objectives Monitoring and review of organisational performance Delivery of efficiency savings
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
53
Annually the Trust produces a service strategy which incorporates a supporting financial plan for approval by the Board of Directors. The strategy approved by the Board of Directors informs the detailed annual financial and performance plans. The Board monitors performance monthly through the corporate Finance & Performance Report, which provides information on current and forecast financial performance, achievement of savings targets, capital investment, contract activity and performance against key targets.
Reports on specific issues relating to economy, efficiency and effectiveness are commissioned by the Audit Committee from the Trust’s Internal Auditors and it also receives reports from the External Auditors as required. The Audit committee monitors closely the implementation of Audit recommendations.
Effective performance has been demonstrated through:
The achievement of the majority of key NHS targets A financial risk rating of 5 as determined by the independent regulator Monitor.
6 Review of Effectiveness
As the Accounting Officer, I have responsibility for reviewing the effectiveness of the system of internal control. My review of the effectiveness of the system of internal control is informed by the work of the internal auditors and the executive managers within the NHS Foundation Trust who have responsibility for the development and maintenance of the internal control framework, and comments made by the external auditors in their management letter and other reports. I have been advised on the implications of the result of my review of the effectiveness of the system of internal control by the Board, the audit committee and a plan to address weaknesses and ensure continuous improvement of the system is in place.
The Board of Directors reviews performance across a range of indicators, which include both corporate and national objectives:
Waiting times are a critical indicator of success in terms of improving access for patients. The targets have been revised for Quarter 4. The achievement under the original methodology for the first three quarters has been 99.8% (operational target 98%) for the 31 day from decision to treat to first treatment and 93.3% (operational target 93%) against the 62-day urgent referral to first treatment target. The key issue to the Trust in continuing to achieve the 62-day target in the future is the timely referrals of patients from other hospitals.
The Trust is monitoring performance against the new cancer waiting time targets methodology introduced in quarter 4. The Trust achieved 98.7% against the 31 day subsequent treatment measure and 78.0% against the 62 day measure. Operational targets are still awaited from the Department of Health for these new measures of waiting time performance.
A “green” rating by Monitor for each quarter in 2008/09 for governance A “green” rating by Monitor for each quarter in 2008/09 for the provision of mandatory
services. Achievement of all key financial duties and a Monitor financial risk rating of 5 for each quarter
in 2008/09. Internal Audit concluded that the systems and processes in place regarding the Assurance
Framework are designed and operated to meet the requirements of the Statement of Internal Control. High Assurance has been received for this. They have also provided significant assurance regarding the systems and processes underpinning the Standards for Better Health

Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
54
declaration, and significant assurance overall across a range of individual opinions arising from risk based audit assignments reported throughout the year.
Accreditation for National Health Service Litigation Authority for Trusts (NHSLA) level 3. Maintaining a special quality management accreditation (ISO9001:2000) across the whole
Trust from the British Standards Institute (BSI) Incorporation of feedback from Cancer Peer Review into action plans and corporate
objectives. Regular audit committee review to ensure up to date and relevant financial policies and
procedures are maintained. Compliance with Standards for Better Health core standards throughout 2008/09. The Trust has been granted full registration without conditions as a service provider from the
Care Quality Commission in March 2009.
In conclusion, the Trust has a sound system of Internal Control in place, which is designed to manage the key organisational objectives and minimise the Trust exposure to risk. No significant internal control issues have been identified.
Name: ANDREW CANNELL Signature:Acting Chief Executive Date: 8th June 2009
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
55
1. Accounting policies and other information Monitor has directed that the financial statements of NHS foundation trusts shall meet the accounting requirements of the NHS Foundation Trust Financial Reporting Manual which shall be agreed with HM Treasury. Consequently, the following financial statements have been prepared in accordance with the 2008/09 NHS Foundation Trust Financial Reporting Manual issued by Monitor. The accounting policies contained in that manual follow UK generally accepted accounting practice for companies (UK GAAP) and HM Treasury’s Financial Reporting Manual to the extent that they are meaningful and appropriate to NHS foundation trusts. The accounting policies have been applied consistently in dealing with items considered material in relation to the accounts.
1.1 Accounting convention These accounts have been prepared under the historical cost convention modified to account for the revaluation of tangible fixed assets at their value to the business by reference to their current costs. NHS foundation trusts, in compliance with HM Treasury’s Financial Reporting Manual, are not required to comply with the FRS 3 requirements to report “earnings per share” or historical profits and losses.
1.2 Acquisitions and discontinued operationsActivities are considered to be ‘discontinued’ where they meet all of the following conditions:
a. the sale (this may be at nil consideration for activities transferred to another public sector body) or termination is completed either in the period or before the earlier of three months after the commencement of the subsequent period and the date on which the financial statements are approved;
b. if a termination, the former activities have ceased permanently;
c. the sale or termination has a material effect on the nature and focus of the reporting NHS foundation trust’s operations and represents a material reduction in its operating facilities resulting either from its withdrawal from a particular activity or from a material reduction in income in the NHS foundation trust’s continuing operations; and
d. the assets, liabilities, results of operations and activities are clearly distinguishable, physically, operationally and for financial reporting purposes.
Operations not satisfying all these conditions are classified as continuing.
Activities are considered to be ‘acquired’ whether or not they are acquired from outside the public sector.
1.3 Income recognition Income is accounted for applying the accruals convention. The main source of income for the trust is under contracts from commissioners in respect of healthcare services. Income is recognised in the period in which services are provided. Where income is received for a specific activity which is to be delivered in the following financial year, that income is deferred.
The NHS foundation trust changed the form of its contracts with NHS commissioners to follow the Department of Health’s Payment by Results methodology in 2008/09.To phase in the impact of PBR. Such income is shown net of transitional relief adjustments, which are calculated by the Department of Health. NHS Foundation Trust contracts may either receive or pay back transitional relief.
1.4 Expenditure Expenditure is accounted for applying the accruals convention.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
54
declaration, and significant assurance overall across a range of individual opinions arising from risk based audit assignments reported throughout the year.
Accreditation for National Health Service Litigation Authority for Trusts (NHSLA) level 3. Maintaining a special quality management accreditation (ISO9001:2000) across the whole
Trust from the British Standards Institute (BSI) Incorporation of feedback from Cancer Peer Review into action plans and corporate
objectives. Regular audit committee review to ensure up to date and relevant financial policies and
procedures are maintained. Compliance with Standards for Better Health core standards throughout 2008/09. The Trust has been granted full registration without conditions as a service provider from the
Care Quality Commission in March 2009.
In conclusion, the Trust has a sound system of Internal Control in place, which is designed to manage the key organisational objectives and minimise the Trust exposure to risk. No significant internal control issues have been identified.
Name: ANDREW CANNELL Signature:Acting Chief Executive Date: 8th June 2009
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
55
1. Accounting policies and other information Monitor has directed that the financial statements of NHS foundation trusts shall meet the accounting requirements of the NHS Foundation Trust Financial Reporting Manual which shall be agreed with HM Treasury. Consequently, the following financial statements have been prepared in accordance with the 2008/09 NHS Foundation Trust Financial Reporting Manual issued by Monitor. The accounting policies contained in that manual follow UK generally accepted accounting practice for companies (UK GAAP) and HM Treasury’s Financial Reporting Manual to the extent that they are meaningful and appropriate to NHS foundation trusts. The accounting policies have been applied consistently in dealing with items considered material in relation to the accounts.
1.1 Accounting convention These accounts have been prepared under the historical cost convention modified to account for the revaluation of tangible fixed assets at their value to the business by reference to their current costs. NHS foundation trusts, in compliance with HM Treasury’s Financial Reporting Manual, are not required to comply with the FRS 3 requirements to report “earnings per share” or historical profits and losses.
1.2 Acquisitions and discontinued operationsActivities are considered to be ‘discontinued’ where they meet all of the following conditions:
a. the sale (this may be at nil consideration for activities transferred to another public sector body) or termination is completed either in the period or before the earlier of three months after the commencement of the subsequent period and the date on which the financial statements are approved;
b. if a termination, the former activities have ceased permanently;
c. the sale or termination has a material effect on the nature and focus of the reporting NHS foundation trust’s operations and represents a material reduction in its operating facilities resulting either from its withdrawal from a particular activity or from a material reduction in income in the NHS foundation trust’s continuing operations; and
d. the assets, liabilities, results of operations and activities are clearly distinguishable, physically, operationally and for financial reporting purposes.
Operations not satisfying all these conditions are classified as continuing.
Activities are considered to be ‘acquired’ whether or not they are acquired from outside the public sector.
1.3 Income recognition Income is accounted for applying the accruals convention. The main source of income for the trust is under contracts from commissioners in respect of healthcare services. Income is recognised in the period in which services are provided. Where income is received for a specific activity which is to be delivered in the following financial year, that income is deferred.
The NHS foundation trust changed the form of its contracts with NHS commissioners to follow the Department of Health’s Payment by Results methodology in 2008/09.To phase in the impact of PBR. Such income is shown net of transitional relief adjustments, which are calculated by the Department of Health. NHS Foundation Trust contracts may either receive or pay back transitional relief.
1.4 Expenditure Expenditure is accounted for applying the accruals convention.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
56
1.5 Tangible fixed assets
Capitalisation
Tangible assets are capitalised if they are capable of being used for a period which exceeds one year and they:
individually have a cost of at least £5,000; or
form a group of assets which individually have a cost of more than £250, collectively have a cost of at least £5,000, where the assets are functionally interdependent, they had broadly simultaneous purchase dates, are anticipated to have simultaneous disposal dates and are under single managerial control; or
form part of the initial setting-up cost of a new building or refurbishment of a ward or unit, irrespective of their individual or collective cost.
Valuation
Tangible fixed assets are stated at the lower of replacement cost and recoverable amount. On initial recognition they are measured at cost (for leased assets, fair value) including any costs, such as installation, directly attributable to bringing them into working condition. The carrying values of tangible fixed assets are reviewed for impairment in periods if events or changes in circumstances indicate the carrying value may not be recoverable. The costs arising from financing the construction of the fixed asset are not capitalised but are charged to the income and expenditure account in the year to which they relate.
All land and buildings are revalued using professional valuations in accordance with FRS 15 every five years. A three yearly interim valuation is also carried out.
Valuations are carried out by professionally qualified valuers in accordance with the Royal Institute of Chartered Surveyors (RICS) Appraisal and Valuation Manual.
The valuations are carried out primarily on the basis of depreciated replacement cost for specialised operational property and existing use value for non-specialised operational property. The value of land for existing use purposes is assessed at existing use value. For non-operational properties including surplus land, the valuations are carried out at open market value.
Additional alternative open market value figures have only been supplied for operational assets scheduled for imminent closure and subsequent disposal.
Assets in the course of construction are valued at cost and are valued by professional valuers as part of the five or three-yearly valuation or when they are brought into use.
Residual interests in off-balance sheet private finance initiative (PFI) properties are included in assets under construction within tangible fixed assets at the amount of unitary charge allocated for the acquisition of the residual with an adjustment. The adjustment is the net present value of the change in the fair value of the residual as estimated at the start of the contract and at the balance sheet date.
Operational equipment (including IT equipment), is carried at depreciated replacement cost. Equipment surplus to requirements is valued at net recoverable amount.
Depreciation, amortisation and impairments
Tangible fixed assets are depreciated at rates calculated to write them down to estimated residual value on a straight-line basis over their estimated useful lives. No depreciation is provided on freehold land, and assets surplus to requirements.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
57
Assets in the course of construction and residual interests in off-balance sheet PFI contract assets are not depreciated until the asset is brought into use or reverts to the trust, respectively.
Buildings, installations and fittings are depreciated on their current value over the estimated remaining life of the asset as assessed by the NHS foundation trust’s professional valuers. Leaseholds are depreciated over the primary lease term.
Equipment is depreciated on current cost evenly over the estimated life, which are as follows:
Engineering plant and equipment 5-15 years
Medical and other equipment 5-15 years
Office equipment, furniture and soft furnishings 5-10 years
IT Equipment 5-8 years
Vehicles 7 years
Fixed asset impairments resulting from losses of economic benefits are charged to the income and expenditure account. All other impairments are taken to the revaluation reserve and reported in the statement of total recognised gains and losses to the extent that there is a balance on the revaluation reserve in respect of the particular asset.
1.6 Intangible fixed assets
Intangible assets are capitalised when they are capable of being used in a trust's activities for more than one year; they can be valued; and they have a cost of at least £5,000.
Intangible fixed assets held for operational use are valued at historical cost and are amortised over the estimated life of the asset on a straight line basis. The carrying value of intangible assets is reviewed for impairment at the end of the first full year following acquisition and in other periods if events or changes in circumstances indicate the carrying value may not be recoverable.
Purchased computer software licences are capitalised as intangible fixed assets where expenditure of at least £5,000 is incurred and amortised over the shorter of the term of the licence and their useful economic lives.
1.7 Donated fixed assets
Donated fixed assets are capitalised at their current value on receipt and this value is credited to the donated asset reserve. Donated fixed assets are valued and depreciated as described above for purchased assets. Gains and losses on revaluations are also taken to the donated asset reserve and, each year, an amount equal to the depreciation charge on the asset is released from the donated asset reserve to the income and expenditure account. Similarly, any impairment on donated assets charged to the income and expenditure account is matched by a transfer from the donated asset reserve. On sale of donated assets, the net book value of the donated asset is transferred from the donated asset reserve to the Income and Expenditure Reserve.
1.8 Liquid Resources
Deposits and other investments that are readily convertible into known amounts of cash at or close to their carrying amounts are treated as liquid resources in the cashflow statement.
1.9 Government grants
Government grants are grants from Government bodies other than income from primary care trusts or NHS trusts for the provision of services. Grants from the Department of Health, including those for achieving three star status, are accounted for as Government grants as are grants from the Big
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
56
1.5 Tangible fixed assets
Capitalisation
Tangible assets are capitalised if they are capable of being used for a period which exceeds one year and they:
individually have a cost of at least £5,000; or
form a group of assets which individually have a cost of more than £250, collectively have a cost of at least £5,000, where the assets are functionally interdependent, they had broadly simultaneous purchase dates, are anticipated to have simultaneous disposal dates and are under single managerial control; or
form part of the initial setting-up cost of a new building or refurbishment of a ward or unit, irrespective of their individual or collective cost.
Valuation
Tangible fixed assets are stated at the lower of replacement cost and recoverable amount. On initial recognition they are measured at cost (for leased assets, fair value) including any costs, such as installation, directly attributable to bringing them into working condition. The carrying values of tangible fixed assets are reviewed for impairment in periods if events or changes in circumstances indicate the carrying value may not be recoverable. The costs arising from financing the construction of the fixed asset are not capitalised but are charged to the income and expenditure account in the year to which they relate.
All land and buildings are revalued using professional valuations in accordance with FRS 15 every five years. A three yearly interim valuation is also carried out.
Valuations are carried out by professionally qualified valuers in accordance with the Royal Institute of Chartered Surveyors (RICS) Appraisal and Valuation Manual.
The valuations are carried out primarily on the basis of depreciated replacement cost for specialised operational property and existing use value for non-specialised operational property. The value of land for existing use purposes is assessed at existing use value. For non-operational properties including surplus land, the valuations are carried out at open market value.
Additional alternative open market value figures have only been supplied for operational assets scheduled for imminent closure and subsequent disposal.
Assets in the course of construction are valued at cost and are valued by professional valuers as part of the five or three-yearly valuation or when they are brought into use.
Residual interests in off-balance sheet private finance initiative (PFI) properties are included in assets under construction within tangible fixed assets at the amount of unitary charge allocated for the acquisition of the residual with an adjustment. The adjustment is the net present value of the change in the fair value of the residual as estimated at the start of the contract and at the balance sheet date.
Operational equipment (including IT equipment), is carried at depreciated replacement cost. Equipment surplus to requirements is valued at net recoverable amount.
Depreciation, amortisation and impairments
Tangible fixed assets are depreciated at rates calculated to write them down to estimated residual value on a straight-line basis over their estimated useful lives. No depreciation is provided on freehold land, and assets surplus to requirements.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
57
Assets in the course of construction and residual interests in off-balance sheet PFI contract assets are not depreciated until the asset is brought into use or reverts to the trust, respectively.
Buildings, installations and fittings are depreciated on their current value over the estimated remaining life of the asset as assessed by the NHS foundation trust’s professional valuers. Leaseholds are depreciated over the primary lease term.
Equipment is depreciated on current cost evenly over the estimated life, which are as follows:
Engineering plant and equipment 5-15 years
Medical and other equipment 5-15 years
Office equipment, furniture and soft furnishings 5-10 years
IT Equipment 5-8 years
Vehicles 7 years
Fixed asset impairments resulting from losses of economic benefits are charged to the income and expenditure account. All other impairments are taken to the revaluation reserve and reported in the statement of total recognised gains and losses to the extent that there is a balance on the revaluation reserve in respect of the particular asset.
1.6 Intangible fixed assets
Intangible assets are capitalised when they are capable of being used in a trust's activities for more than one year; they can be valued; and they have a cost of at least £5,000.
Intangible fixed assets held for operational use are valued at historical cost and are amortised over the estimated life of the asset on a straight line basis. The carrying value of intangible assets is reviewed for impairment at the end of the first full year following acquisition and in other periods if events or changes in circumstances indicate the carrying value may not be recoverable.
Purchased computer software licences are capitalised as intangible fixed assets where expenditure of at least £5,000 is incurred and amortised over the shorter of the term of the licence and their useful economic lives.
1.7 Donated fixed assets
Donated fixed assets are capitalised at their current value on receipt and this value is credited to the donated asset reserve. Donated fixed assets are valued and depreciated as described above for purchased assets. Gains and losses on revaluations are also taken to the donated asset reserve and, each year, an amount equal to the depreciation charge on the asset is released from the donated asset reserve to the income and expenditure account. Similarly, any impairment on donated assets charged to the income and expenditure account is matched by a transfer from the donated asset reserve. On sale of donated assets, the net book value of the donated asset is transferred from the donated asset reserve to the Income and Expenditure Reserve.
1.8 Liquid Resources
Deposits and other investments that are readily convertible into known amounts of cash at or close to their carrying amounts are treated as liquid resources in the cashflow statement.
1.9 Government grants
Government grants are grants from Government bodies other than income from primary care trusts or NHS trusts for the provision of services. Grants from the Department of Health, including those for achieving three star status, are accounted for as Government grants as are grants from the Big

Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
58
Lottery Fund. Where the Government grant is used to fund revenue expenditure it is taken to the Income and Expenditure account to match that expenditure. Where the grant is used to fund capital expenditure the grant is held as deferred income and released to the income and expenditure account over the life of the asset on a basis consistent with the depreciation charge for that asset.
1.10 Private Finance Initiative (PFI) transactions
The NHS follows HM Treasury’s Technical Note 1 (Revised) “How to Account for PFI transactions” which provides definitive guidance for the application of application note F to FRS 5. Where the balance of the risks and rewards of ownership of the PFI property are borne by the PFI operator, the PFI payments are recorded as an operating expense. Where the trust has contributed land and buildings, a prepayment for their fair value is recognised and amortised over the life of the PFI contract by charge to the income and expenditure account. Where, at the end of the PFI contract, a property reverts to the trust, the difference between the expected fair value of the residual on reversion and any agreed payment on reversion is built up over the life of the contract by capitalising part of the unitary charge each year, as a tangible fixed asset.
Where the balance of risks and rewards of ownership of the PFI property are borne by the trust, it is recognised as a fixed asset along with the liability to pay for it which is accounted for as a finance lease. Contract payments are apportioned between an imputed finance lease charge and a service charge.
1.11 Stocks and work-in-progress
Stocks and work-in-progress are valued at the lower of cost and net realisable value. Work-in-progress comprises goods and services in intermediate stages of production.
1.12 Cash, bank and overdrafts
Cash, bank and overdraft balances are recorded at the current values of these balances in the NHS foundation trust’s cash book. These balances exclude monies held in the NHS foundation trust’s bank account belonging to patients (see “third party assets” below). Account balances are only set off where a formal agreement has been made with the bank to do so. In all other cases overdrafts are disclosed within creditors. Interest earned on bank accounts and interest charged on overdrafts is recorded as, respectively, “interest receivable” and “interest payable” in the periods to which they relate. Bank charges are recorded as operating expenditure in the periods to which they relate.
1.13 Research and development
Expenditure on research is not capitalised. Expenditure on development is capitalised if it meets the following criteria:
there is a clearly defined project; the related expenditure is separately identifiable; the outcome of the project has been assessed with reasonable certainty as to its technical
feasibility and its resulting in a product or services that will eventually be brought into use; and adequate resources exist, or are reasonably expected to be available, to enable the project to
be completed and to provide any consequential increases in working capital.
Expenditure so deferred is limited to the value of future benefits expected and is amortised through the income and expenditure account on a systematic basis over the period expected to benefit from the project. It is revalued on the basis of current cost. Expenditure which does not meet the criteria for capitalisation is treated as an operating cost in the year in which it is incurred. Where possible, NHS foundation trusts disclose the total amount of research and development expenditure charged in the
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
59
Income and Expenditure account separately. However, where research and development activity cannot be separated from patient care activity it cannot be identified and is therefore not separately disclosed.
Fixed assets acquired for use in research and development are amortised over the life of the associated project.
1.14 Provisions
The NHS foundation trust provides for legal or constructive obligations that are of uncertain timing or amount at the balance sheet date on the basis of the best estimate of the expenditure required to settle the obligation. Where the effect of the time value of money is significant, the estimated risk-adjusted cash flows are discounted using HM Treasury’s discount rate of 2.2% in real terms.
1.15 Contingencies
Contingent assets (that is, assets arising from past events whose existence will only be confirmed by one or more future events not wholly within the entity’s control) are not recognised as assets, but are disclosed in note 22 where an inflow of economic benefits is probable. Contingent liabilities are provided for where a transfer of economic benefits is probable. Otherwise, they are not recognised, but are disclosed in note 22 unless the probability of a transfer of economic benefits is remote. Contingent liabilities are defined as:
Possible obligations arising from past events whose existence will be confirmed only by the occurrence of one or more uncertain future events not wholly within the entity’s control; or
Present obligations arising from past events but for which it is not probable that a transfer of economic benefits will arise or for which the amount of the obligation cannot be measured with sufficient reliability.
1.16 Clinical negligence costs
The NHS Litigation Authority (NHSLA) operates a risk pooling scheme under which the NHS foundation trust pays an annual contribution to the NHSLA, which, in return, settles all clinical negligence claims. Although the NHSLA is administratively responsible for all clinical negligence cases, the legal liability remains with the NHS foundation trust. The total value of clinical negligence provisions carried by the NHSLA on behalf of the NHS foundation trust is disclosed at note 17.
1.17 Non-clinical risk pooling
The NHS foundation trust participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling schemes under which the trust pays an annual contribution to the NHS Litigation Authority and in return receives assistance with the costs of claims arising. The annual membership contributions, and any ‘excesses’ payable in respect of particular claims are charged to operating expenses when the liability arises.
1.18 Pension costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme. The Scheme is an unfunded, defined benefit scheme that covers NHS employers, General Practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying Scheme assets and liabilities. Therefore, the Scheme is accounted for as if it were a
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
58
Lottery Fund. Where the Government grant is used to fund revenue expenditure it is taken to the Income and Expenditure account to match that expenditure. Where the grant is used to fund capital expenditure the grant is held as deferred income and released to the income and expenditure account over the life of the asset on a basis consistent with the depreciation charge for that asset.
1.10 Private Finance Initiative (PFI) transactions
The NHS follows HM Treasury’s Technical Note 1 (Revised) “How to Account for PFI transactions” which provides definitive guidance for the application of application note F to FRS 5. Where the balance of the risks and rewards of ownership of the PFI property are borne by the PFI operator, the PFI payments are recorded as an operating expense. Where the trust has contributed land and buildings, a prepayment for their fair value is recognised and amortised over the life of the PFI contract by charge to the income and expenditure account. Where, at the end of the PFI contract, a property reverts to the trust, the difference between the expected fair value of the residual on reversion and any agreed payment on reversion is built up over the life of the contract by capitalising part of the unitary charge each year, as a tangible fixed asset.
Where the balance of risks and rewards of ownership of the PFI property are borne by the trust, it is recognised as a fixed asset along with the liability to pay for it which is accounted for as a finance lease. Contract payments are apportioned between an imputed finance lease charge and a service charge.
1.11 Stocks and work-in-progress
Stocks and work-in-progress are valued at the lower of cost and net realisable value. Work-in-progress comprises goods and services in intermediate stages of production.
1.12 Cash, bank and overdrafts
Cash, bank and overdraft balances are recorded at the current values of these balances in the NHS foundation trust’s cash book. These balances exclude monies held in the NHS foundation trust’s bank account belonging to patients (see “third party assets” below). Account balances are only set off where a formal agreement has been made with the bank to do so. In all other cases overdrafts are disclosed within creditors. Interest earned on bank accounts and interest charged on overdrafts is recorded as, respectively, “interest receivable” and “interest payable” in the periods to which they relate. Bank charges are recorded as operating expenditure in the periods to which they relate.
1.13 Research and development
Expenditure on research is not capitalised. Expenditure on development is capitalised if it meets the following criteria:
there is a clearly defined project; the related expenditure is separately identifiable; the outcome of the project has been assessed with reasonable certainty as to its technical
feasibility and its resulting in a product or services that will eventually be brought into use; and adequate resources exist, or are reasonably expected to be available, to enable the project to
be completed and to provide any consequential increases in working capital.
Expenditure so deferred is limited to the value of future benefits expected and is amortised through the income and expenditure account on a systematic basis over the period expected to benefit from the project. It is revalued on the basis of current cost. Expenditure which does not meet the criteria for capitalisation is treated as an operating cost in the year in which it is incurred. Where possible, NHS foundation trusts disclose the total amount of research and development expenditure charged in the
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
59
Income and Expenditure account separately. However, where research and development activity cannot be separated from patient care activity it cannot be identified and is therefore not separately disclosed.
Fixed assets acquired for use in research and development are amortised over the life of the associated project.
1.14 Provisions
The NHS foundation trust provides for legal or constructive obligations that are of uncertain timing or amount at the balance sheet date on the basis of the best estimate of the expenditure required to settle the obligation. Where the effect of the time value of money is significant, the estimated risk-adjusted cash flows are discounted using HM Treasury’s discount rate of 2.2% in real terms.
1.15 Contingencies
Contingent assets (that is, assets arising from past events whose existence will only be confirmed by one or more future events not wholly within the entity’s control) are not recognised as assets, but are disclosed in note 22 where an inflow of economic benefits is probable. Contingent liabilities are provided for where a transfer of economic benefits is probable. Otherwise, they are not recognised, but are disclosed in note 22 unless the probability of a transfer of economic benefits is remote. Contingent liabilities are defined as:
Possible obligations arising from past events whose existence will be confirmed only by the occurrence of one or more uncertain future events not wholly within the entity’s control; or
Present obligations arising from past events but for which it is not probable that a transfer of economic benefits will arise or for which the amount of the obligation cannot be measured with sufficient reliability.
1.16 Clinical negligence costs
The NHS Litigation Authority (NHSLA) operates a risk pooling scheme under which the NHS foundation trust pays an annual contribution to the NHSLA, which, in return, settles all clinical negligence claims. Although the NHSLA is administratively responsible for all clinical negligence cases, the legal liability remains with the NHS foundation trust. The total value of clinical negligence provisions carried by the NHSLA on behalf of the NHS foundation trust is disclosed at note 17.
1.17 Non-clinical risk pooling
The NHS foundation trust participates in the Property Expenses Scheme and the Liabilities to Third Parties Scheme. Both are risk pooling schemes under which the trust pays an annual contribution to the NHS Litigation Authority and in return receives assistance with the costs of claims arising. The annual membership contributions, and any ‘excesses’ payable in respect of particular claims are charged to operating expenses when the liability arises.
1.18 Pension costs
Past and present employees are covered by the provisions of the NHS Pensions Scheme. The Scheme is an unfunded, defined benefit scheme that covers NHS employers, General Practices and other bodies, allowed under the direction of the Secretary of State, in England and Wales. The scheme is not designed to be run in a way that would enable NHS bodies to identify their share of the underlying Scheme assets and liabilities. Therefore, the Scheme is accounted for as if it were a

Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
60
defined contribution scheme: the cost to the NHS Body of participating in the Scheme is taken as equal to the contributions payable to the Scheme for the accounting period.
The Scheme is subject to a full actuarial investigation every four years. The main purpose of which is to assess the level of liability in respect of the benefits due under the scheme (taking into account its recent demographic experience), and to recommend the contribution rates to be paid by employers and scheme members. The last such investigation, on the conclusions of which scheme contribution rates are currently based, had an effective date of 31 March 2004 and covered the period from 1 April 1999 to that date. Between the full actuarial valuations, the Government Actuary provides an annual update of the scheme liabilities for FRS17 purposes. The latest assessment of the liabilities of the Scheme is contained in the Scheme Actuary report, which forms part of the NHS Pension Scheme (England and Wales) Resource Account, published annually. These accounts can be viewed on the Business Service Authority - Pensions Division website at www.nhspa.gov.uk. Copies can also be obtained from The Stationery Office.
The conclusion of the 2004 investigation was that the scheme had accumulated a notional deficit of £3.3 billion against the notional assets as at 31 March 2004. This is after making some allowance for the one-off effects of pay modernisation, but before taking into account any of the scheme changes which come into effect on 1 April 2008. Taking into account the changes in the benefit and contribution structure effective from 1 April 2008, employer contributions could continue at the existing rate of 14% of pensionable pay. On advice from the actuary, scheme contributions may be varied from time to time to reflect changes in the scheme’s liabilities. Up to 31 March 2008 employees paid contributions at the rate of 6% (manual staff 5%) of their pensionable pay. From 1 April 2008, employees will pay contributions according to a tiered scale from 5% up to 8.5% of their pensionable pay.
1.19 Value Added Tax
Most of the activities of the NHS foundation trust are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
1.20 Corporation Tax
The Trust is a Health Service Body within the meaning of s519A ICTA 1988 and accordingly is exempt from taxation in respect of income and capital gains within categories covered by this. There is a power for the treasury to disapply the exemption in relation to specified activities of a Foundation Trust (s519A (3) to (8) ICTA 1988). Accordingly, the Trust is potentially within the scope of corporation tax in respect of activities, which are not related to, or ancillary to, the provision of healthcare, and where the profits there from exceed £50,000 per annum.
1.21 Foreign exchange
Transactions that are denominated in a foreign currency are translated into sterling at the exchange rate ruling on the dates of the transactions. Resulting exchange gains and losses are taken to the income and expenditure account.
1.22 Third party assets
Assets belonging to third parties (such as money held on behalf of patients) are not recognised in the accounts since the NHS foundation trust has no beneficial interest in them. However, they are
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
61
disclosed in a separate note to the accounts in accordance with the requirements of the HM Treasury Financial Reporting Manual.
1.23 Leases
Where substantially all risks and rewards of ownership of a leased asset are borne by the NHS foundation trust, the asset is recorded as a tangible fixed asset and a debt is recorded to the lessor of the minimum lease payments discounted by the interest rate implicit in the lease.
The asset and liability are recognised at the inception of the lease, and are de-recognised when the liability is discharged, cancelled or expires.
The interest element of the finance lease payment is charged to the income and expenditure account over the period of the lease at a constant rate in relation to the balance outstanding. Other leases are regarded as operating leases and the rentals are charged to the income and expenditure account on a straight-line basis over the term of the lease.
1.24 Public dividend capital
Public dividend capital (PDC) is a type of public sector equity finance based on the excess of assets over liabilities at the time of establishment of the original NHS trust.
A charge, reflecting the forecast cost of capital utilised by the NHS foundation trust, is paid over as public dividend capital dividend. The charge is calculated at the real rate set by HM Treasury (currently 3.5%) on the average relevant net assets of the NHS foundation trust. Relevant net assets are calculated as the value of all assets less the value of all liabilities, except for donated assets and cash held with the Office of the Paymaster General. Average relevant net assets are calculated as a simple mean of opening and closing relevant net assets.
1.25 Financial instruments and financial liabilities
Recognition
Financial assets and financial liabilities which arise from contracts for the purchase or sale of non-financial items (such as goods or services), which are entered into in accordance with the Trust’s normal purchase, sale or usage requirements, are recognised when, and to the extent which, performance occurs i.e. when receipt or delivery of the goods or services is made.
Financial assets or financial liabilities in respect of assets acquired or disposed of through finance leases are recognised and measured in accordance with the accounting policy for leases described above.
All other financial assets and financial liabilities are recognised when the Trust becomes a party to the contractual provisions of the instrument.
De-recognition
All financial assets are de-recognised when the rights to receive cashflows from the assets have expired or the Trust has transferred substantially all of the risks and rewards of ownership.
Financial liabilities are de-recognised when the obligation is discharged, cancelled or expires.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
60
defined contribution scheme: the cost to the NHS Body of participating in the Scheme is taken as equal to the contributions payable to the Scheme for the accounting period.
The Scheme is subject to a full actuarial investigation every four years. The main purpose of which is to assess the level of liability in respect of the benefits due under the scheme (taking into account its recent demographic experience), and to recommend the contribution rates to be paid by employers and scheme members. The last such investigation, on the conclusions of which scheme contribution rates are currently based, had an effective date of 31 March 2004 and covered the period from 1 April 1999 to that date. Between the full actuarial valuations, the Government Actuary provides an annual update of the scheme liabilities for FRS17 purposes. The latest assessment of the liabilities of the Scheme is contained in the Scheme Actuary report, which forms part of the NHS Pension Scheme (England and Wales) Resource Account, published annually. These accounts can be viewed on the Business Service Authority - Pensions Division website at www.nhspa.gov.uk. Copies can also be obtained from The Stationery Office.
The conclusion of the 2004 investigation was that the scheme had accumulated a notional deficit of £3.3 billion against the notional assets as at 31 March 2004. This is after making some allowance for the one-off effects of pay modernisation, but before taking into account any of the scheme changes which come into effect on 1 April 2008. Taking into account the changes in the benefit and contribution structure effective from 1 April 2008, employer contributions could continue at the existing rate of 14% of pensionable pay. On advice from the actuary, scheme contributions may be varied from time to time to reflect changes in the scheme’s liabilities. Up to 31 March 2008 employees paid contributions at the rate of 6% (manual staff 5%) of their pensionable pay. From 1 April 2008, employees will pay contributions according to a tiered scale from 5% up to 8.5% of their pensionable pay.
1.19 Value Added Tax
Most of the activities of the NHS foundation trust are outside the scope of VAT and, in general, output tax does not apply and input tax on purchases is not recoverable. Irrecoverable VAT is charged to the relevant expenditure category or included in the capitalised purchase cost of fixed assets. Where output tax is charged or input VAT is recoverable, the amounts are stated net of VAT.
1.20 Corporation Tax
The Trust is a Health Service Body within the meaning of s519A ICTA 1988 and accordingly is exempt from taxation in respect of income and capital gains within categories covered by this. There is a power for the treasury to disapply the exemption in relation to specified activities of a Foundation Trust (s519A (3) to (8) ICTA 1988). Accordingly, the Trust is potentially within the scope of corporation tax in respect of activities, which are not related to, or ancillary to, the provision of healthcare, and where the profits there from exceed £50,000 per annum.
1.21 Foreign exchange
Transactions that are denominated in a foreign currency are translated into sterling at the exchange rate ruling on the dates of the transactions. Resulting exchange gains and losses are taken to the income and expenditure account.
1.22 Third party assets
Assets belonging to third parties (such as money held on behalf of patients) are not recognised in the accounts since the NHS foundation trust has no beneficial interest in them. However, they are
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
61
disclosed in a separate note to the accounts in accordance with the requirements of the HM Treasury Financial Reporting Manual.
1.23 Leases
Where substantially all risks and rewards of ownership of a leased asset are borne by the NHS foundation trust, the asset is recorded as a tangible fixed asset and a debt is recorded to the lessor of the minimum lease payments discounted by the interest rate implicit in the lease.
The asset and liability are recognised at the inception of the lease, and are de-recognised when the liability is discharged, cancelled or expires.
The interest element of the finance lease payment is charged to the income and expenditure account over the period of the lease at a constant rate in relation to the balance outstanding. Other leases are regarded as operating leases and the rentals are charged to the income and expenditure account on a straight-line basis over the term of the lease.
1.24 Public dividend capital
Public dividend capital (PDC) is a type of public sector equity finance based on the excess of assets over liabilities at the time of establishment of the original NHS trust.
A charge, reflecting the forecast cost of capital utilised by the NHS foundation trust, is paid over as public dividend capital dividend. The charge is calculated at the real rate set by HM Treasury (currently 3.5%) on the average relevant net assets of the NHS foundation trust. Relevant net assets are calculated as the value of all assets less the value of all liabilities, except for donated assets and cash held with the Office of the Paymaster General. Average relevant net assets are calculated as a simple mean of opening and closing relevant net assets.
1.25 Financial instruments and financial liabilities
Recognition
Financial assets and financial liabilities which arise from contracts for the purchase or sale of non-financial items (such as goods or services), which are entered into in accordance with the Trust’s normal purchase, sale or usage requirements, are recognised when, and to the extent which, performance occurs i.e. when receipt or delivery of the goods or services is made.
Financial assets or financial liabilities in respect of assets acquired or disposed of through finance leases are recognised and measured in accordance with the accounting policy for leases described above.
All other financial assets and financial liabilities are recognised when the Trust becomes a party to the contractual provisions of the instrument.
De-recognition
All financial assets are de-recognised when the rights to receive cashflows from the assets have expired or the Trust has transferred substantially all of the risks and rewards of ownership.
Financial liabilities are de-recognised when the obligation is discharged, cancelled or expires.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
62
Classification and Measurement
Financial assets are categorised as, ‘Fair Value through Income and Expenditure’, Loans and receivables or ‘Available-for-sale financial assets’.
Financial liabilities are classified as ‘Fair value through Income and Expenditure’ or as ‘Other Financial liabilities’.
Financial assets and financial liabilities at ‘Fair Value through Income and Expenditure’
Financial assets and financial liabilities at ‘fair value through income and expenditure’ are financial assets or financial liabilities held for trading. A financial asset or financial liability is classified in this category if acquired principally for the purpose of selling in the short-term. Derivatives are also categorised as held for trading unless they are designated as hedges. Derivatives which are embedded in other contracts but which are not ‘closely-related’ to those contracts are separated-out from those contracts and measured in this category. Assets and liabilities in this category are classified as current assets and current liabilities.
These financial assets and financial liabilities are recognised initially at fair value, with transaction costs expensed in the income and expenditure account. Subsequent movements in the fair value are recognised as gains or losses in the income and expenditure account.
Loans and receivables
Loans and receivables are non-derivative financial assets with fixed or determinable payments with are not quoted in an active market. They are included in current assets.
The Trust’s loans and receivables comprise: current investments, cash at bank and in hand, NHS debtors, accrued income and ‘other debtors’.
Loans and receivables are recognised initially at fair value, net of transactions costs, and are measured subsequently at amortised cost, using the effective interest method. The effective interest rate is the rate that discounts exactly estimated future cash receipts through the expected life of the financial asset or, when appropriate, a shorter period, to the net carrying amount of the financial asset.
Interest on loans and receivables is calculated using the effective interest method and credited to the income and expenditure account.
Available-for-sale financial assets
Available-for-sale financial assets are non-derivative financial assets which are either designated in this category or not classified in any of the other categories. They are included in long-term assets unless the Trust intends to dispose of them within 12 months of the balance sheet date.
Available-for-sale financial assets are recognised initially at fair value, including transaction costs, and measured subsequently at fair value, with gains or losses recognised in reserves. When items classified as ‘available-for-sale’ are sold or impaired, the accumulated fair value adjustments recognised in reserves are included in the income and expenditure account.
Other financial liabilities
All financial liabilities are recognised initially at fair value, net of transaction costs incurred, and measured subsequently at amortised cost using the effective interest method. The effective interest
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
63
rate is the rate that discounts exactly estimated future cash payments through the expected life of the financial liability or, when appropriate, a shorter period, to the net carrying amount of the financial liability.
They are included in current liabilities except for amounts payable more than 12 months after the balance sheet date, which are classified as long-term liabilities.
Interest on financial liabilities carried at amortised cost is calculated using the effective interest method and charged to the income and expenditure account.
Determination of fair value
For financial assets and financial liabilities carried at fair value, the carrying amounts are the full value of cash in the balance sheet.
1.26 Impairment of financial assets
At the balance sheet date, the Trust assesses whether any financial assets, other than those held at ‘fair value through income and expenditure’ is impaired. Financial assets are impaired and impairment losses are recognised if, and only if, there is objective evidence of impairment as a result of one or more events which occurred after the initial recognition of the asset and which has an impact on the estimated future cashflows of the asset.
For financial assets carried at amortised cost, the amount of the impairment loss is measured as the difference between the asset’s carrying amount and the present value of the revised future cash flows discounted at the asset’s original effective interest rate. The loss is recognised in the income and expenditure account and the carrying amount of the asset is reduced.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
62
Classification and Measurement
Financial assets are categorised as, ‘Fair Value through Income and Expenditure’, Loans and receivables or ‘Available-for-sale financial assets’.
Financial liabilities are classified as ‘Fair value through Income and Expenditure’ or as ‘Other Financial liabilities’.
Financial assets and financial liabilities at ‘Fair Value through Income and Expenditure’
Financial assets and financial liabilities at ‘fair value through income and expenditure’ are financial assets or financial liabilities held for trading. A financial asset or financial liability is classified in this category if acquired principally for the purpose of selling in the short-term. Derivatives are also categorised as held for trading unless they are designated as hedges. Derivatives which are embedded in other contracts but which are not ‘closely-related’ to those contracts are separated-out from those contracts and measured in this category. Assets and liabilities in this category are classified as current assets and current liabilities.
These financial assets and financial liabilities are recognised initially at fair value, with transaction costs expensed in the income and expenditure account. Subsequent movements in the fair value are recognised as gains or losses in the income and expenditure account.
Loans and receivables
Loans and receivables are non-derivative financial assets with fixed or determinable payments with are not quoted in an active market. They are included in current assets.
The Trust’s loans and receivables comprise: current investments, cash at bank and in hand, NHS debtors, accrued income and ‘other debtors’.
Loans and receivables are recognised initially at fair value, net of transactions costs, and are measured subsequently at amortised cost, using the effective interest method. The effective interest rate is the rate that discounts exactly estimated future cash receipts through the expected life of the financial asset or, when appropriate, a shorter period, to the net carrying amount of the financial asset.
Interest on loans and receivables is calculated using the effective interest method and credited to the income and expenditure account.
Available-for-sale financial assets
Available-for-sale financial assets are non-derivative financial assets which are either designated in this category or not classified in any of the other categories. They are included in long-term assets unless the Trust intends to dispose of them within 12 months of the balance sheet date.
Available-for-sale financial assets are recognised initially at fair value, including transaction costs, and measured subsequently at fair value, with gains or losses recognised in reserves. When items classified as ‘available-for-sale’ are sold or impaired, the accumulated fair value adjustments recognised in reserves are included in the income and expenditure account.
Other financial liabilities
All financial liabilities are recognised initially at fair value, net of transaction costs incurred, and measured subsequently at amortised cost using the effective interest method. The effective interest
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
63
rate is the rate that discounts exactly estimated future cash payments through the expected life of the financial liability or, when appropriate, a shorter period, to the net carrying amount of the financial liability.
They are included in current liabilities except for amounts payable more than 12 months after the balance sheet date, which are classified as long-term liabilities.
Interest on financial liabilities carried at amortised cost is calculated using the effective interest method and charged to the income and expenditure account.
Determination of fair value
For financial assets and financial liabilities carried at fair value, the carrying amounts are the full value of cash in the balance sheet.
1.26 Impairment of financial assets
At the balance sheet date, the Trust assesses whether any financial assets, other than those held at ‘fair value through income and expenditure’ is impaired. Financial assets are impaired and impairment losses are recognised if, and only if, there is objective evidence of impairment as a result of one or more events which occurred after the initial recognition of the asset and which has an impact on the estimated future cashflows of the asset.
For financial assets carried at amortised cost, the amount of the impairment loss is measured as the difference between the asset’s carrying amount and the present value of the revised future cash flows discounted at the asset’s original effective interest rate. The loss is recognised in the income and expenditure account and the carrying amount of the asset is reduced.
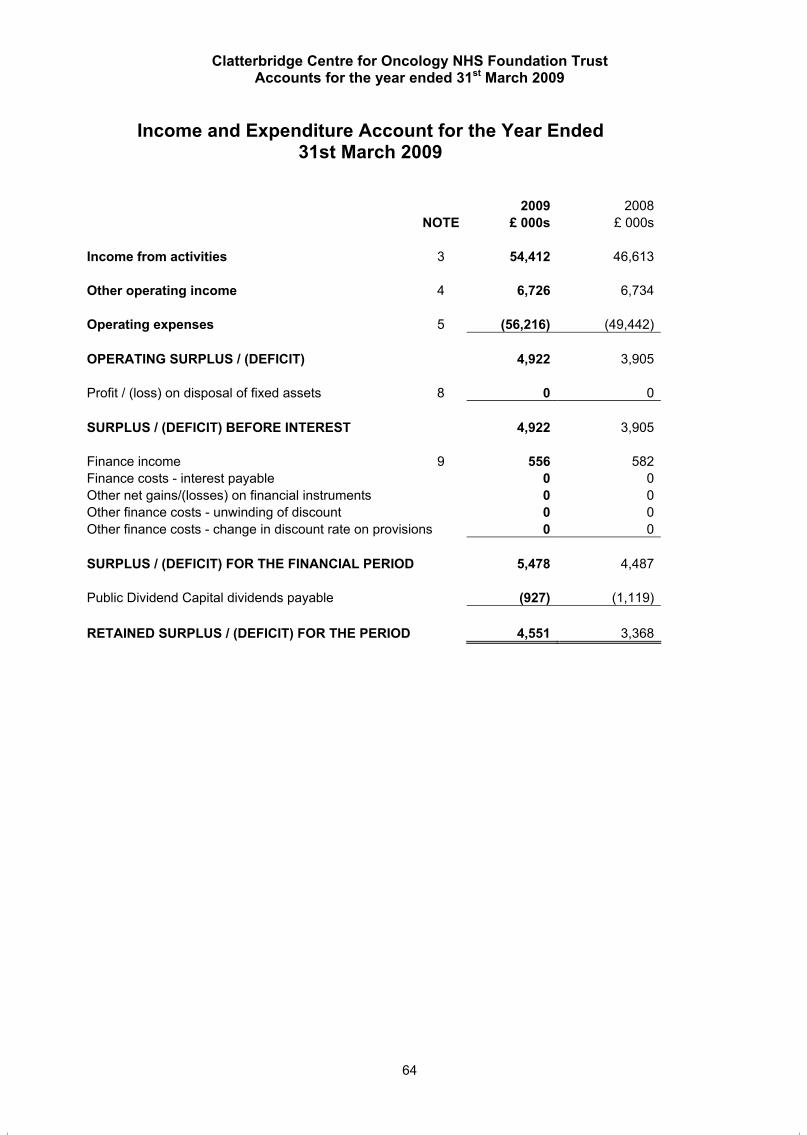
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
64
Income and Expenditure Account for the Year Ended 31st March 2009
2009 2008NOTE £ 000s £ 000s
Income from activities 3 54,412 46,613
Other operating income 4 6,726 6,734
Operating expenses 5 (56,216) (49,442)
OPERATING SURPLUS / (DEFICIT) 4,922 3,905
Profit / (loss) on disposal of fixed assets 8 0 0
SURPLUS / (DEFICIT) BEFORE INTEREST 4,922 3,905
Finance income 9 556 582Finance costs - interest payable 0 0Other net gains/(losses) on financial instruments 0 0Other finance costs - unwinding of discount 0 0Other finance costs - change in discount rate on provisions 0 0
SURPLUS / (DEFICIT) FOR THE FINANCIAL PERIOD 5,478 4,487
Public Dividend Capital dividends payable (927) (1,119)
RETAINED SURPLUS / (DEFICIT) FOR THE PERIOD 4,551 3,368
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
65
Balance Sheet as at 31st March 2009
31stMarch
31stMarch
2009 2008NOTE £ 000s £ 000s
FIXED ASSETS Intangible assets 10 9 14Tangible assets 11 31,217 33,076Investments 12 0 0
31,226 33,090CURRENT ASSETS Stocks and work in progress 13 404 332Debtors 14 2,343 3,376Investments 0 0Cash at bank and in hand 19 18,171 11,998
20,918 15,706
CREDITORS: Amounts falling due within one year 16 (9,867) (11,180)
NET CURRENT ASSETS / (LIABILITIES) 11,051 4,526
TOTAL ASSETS LESS CURRENT LIABILITIES 42,277 37,616
CREDITORS: Amounts falling due after more than one year 16 (561) (958)
PROVISIONS FOR LIABILITIES AND CHARGES 17 (818) (11)
TOTAL ASSETS EMPLOYED 40,898 36,647
FINANCED BY: Public dividend capital 18 21,245 21,245Revaluation reserve 18 5,503 5,804Donated asset reserve 18 1,721 2,021Other reserves 18 0 0Income and expenditure reserve 18 12,429 7,577TOTAL FUNDS 40,898 36,647
The Financial Statements on pages 64 to 92 were approved by the Board on 27th May 2009 and signed on its behalf.
Signed: …………………………………………………………….Acting Chief Executive Date: 8th June 2009
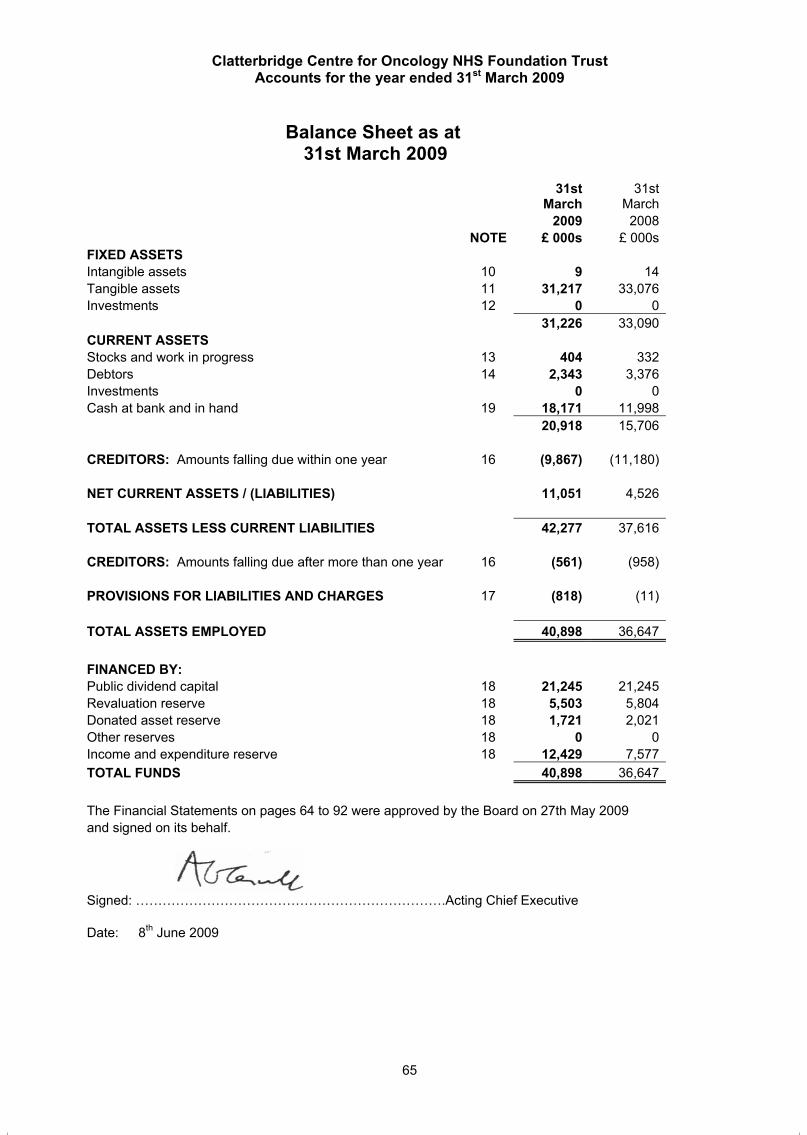
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
64
Income and Expenditure Account for the Year Ended 31st March 2009
2009 2008NOTE £ 000s £ 000s
Income from activities 3 54,412 46,613
Other operating income 4 6,726 6,734
Operating expenses 5 (56,216) (49,442)
OPERATING SURPLUS / (DEFICIT) 4,922 3,905
Profit / (loss) on disposal of fixed assets 8 0 0
SURPLUS / (DEFICIT) BEFORE INTEREST 4,922 3,905
Finance income 9 556 582Finance costs - interest payable 0 0Other net gains/(losses) on financial instruments 0 0Other finance costs - unwinding of discount 0 0Other finance costs - change in discount rate on provisions 0 0
SURPLUS / (DEFICIT) FOR THE FINANCIAL PERIOD 5,478 4,487
Public Dividend Capital dividends payable (927) (1,119)
RETAINED SURPLUS / (DEFICIT) FOR THE PERIOD 4,551 3,368
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
65
Balance Sheet as at 31st March 2009
31stMarch
31stMarch
2009 2008NOTE £ 000s £ 000s
FIXED ASSETS Intangible assets 10 9 14Tangible assets 11 31,217 33,076Investments 12 0 0
31,226 33,090CURRENT ASSETS Stocks and work in progress 13 404 332Debtors 14 2,343 3,376Investments 0 0Cash at bank and in hand 19 18,171 11,998
20,918 15,706
CREDITORS: Amounts falling due within one year 16 (9,867) (11,180)
NET CURRENT ASSETS / (LIABILITIES) 11,051 4,526
TOTAL ASSETS LESS CURRENT LIABILITIES 42,277 37,616
CREDITORS: Amounts falling due after more than one year 16 (561) (958)
PROVISIONS FOR LIABILITIES AND CHARGES 17 (818) (11)
TOTAL ASSETS EMPLOYED 40,898 36,647
FINANCED BY: Public dividend capital 18 21,245 21,245Revaluation reserve 18 5,503 5,804Donated asset reserve 18 1,721 2,021Other reserves 18 0 0Income and expenditure reserve 18 12,429 7,577TOTAL FUNDS 40,898 36,647
The Financial Statements on pages 64 to 92 were approved by the Board on 27th May 2009 and signed on its behalf.
Signed: …………………………………………………………….Acting Chief Executive Date: 8th June 2009
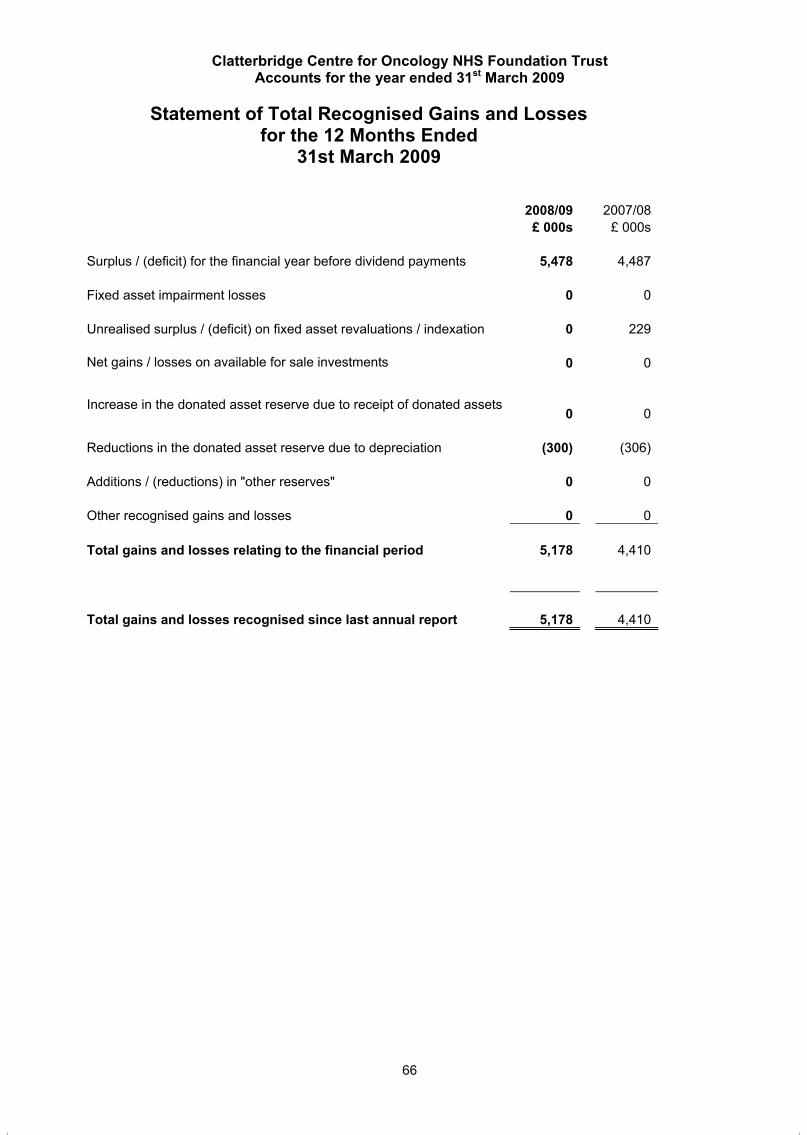
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
66
Statement of Total Recognised Gains and Losses for the 12 Months Ended
31st March 2009
2008/09 2007/08 £ 000s £ 000s
Surplus / (deficit) for the financial year before dividend payments 5,478 4,487
Fixed asset impairment losses 0 0
Unrealised surplus / (deficit) on fixed asset revaluations / indexation 0 229
Net gains / losses on available for sale investments 0 0
Increase in the donated asset reserve due to receipt of donated assets 0 0
Reductions in the donated asset reserve due to depreciation (300) (306)
Additions / (reductions) in "other reserves" 0 0
Other recognised gains and losses 0 0
Total gains and losses relating to the financial period 5,178 4,410
Total gains and losses recognised since last annual report 5,178 4,410
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
67
Cash Flow Statement for the Year Ended 31st March 2009
2008/09 2007/08NOTE £ 000s £ 000s
OPERATING ACTIVITIES Net cash inflow / (outflow) from operating activities 19.1 10,116 6,874
RETURNS ON INVESTMENTS AND SERVICING OF FINANCE: Interest received 556 582Interest paid 0 0Interest element of finance leases 0 0Net cash inflow / (outflow) from returns on investments and servicing of finance 556 582
Taxation paid / received 0 0
CAPITAL EXPENDITURE Payments to acquire tangible fixed assets (3,572) (3,383)Receipts from sale of tangible fixed assets 0 0Payments to acquire intangible fixed assets 0 (14)Receipts from sale of intangible fixed assets 0 0(Payments)/receipts for fixed asset investments 0 0Net cash inflow / (outflow) from capital expenditure (3,572) (3,397)
DIVIDENDS PAID (927) (1,119)
Net cash inflow / (outflow) before management of liquid resources and financing 6,173 2,940
MANAGEMENT OF LIQUID RESOURCES (Purchase) of current asset investments 0 0Sale of current asset investments 0 0Net cash inflow / (outflow) before financing 6,173 2,940
FINANCING Public Dividend Capital received 0 692Public dividend capital repaid 0 0Loans received from Foundation Trust Financing Facility 0 0Other loans received 0 0Loans repaid to Foundation Trust Financing Facility 0 0Other loans repaid 0 0Other capital receipts 0 0Capital element of finance lease rental payments 0 0Net cash inflow / (outflow) from financing 0 692
Increase / (decrease) in cash 6,173 3,632

Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
66
Statement of Total Recognised Gains and Losses for the 12 Months Ended
31st March 2009
2008/09 2007/08 £ 000s £ 000s
Surplus / (deficit) for the financial year before dividend payments 5,478 4,487
Fixed asset impairment losses 0 0
Unrealised surplus / (deficit) on fixed asset revaluations / indexation 0 229
Net gains / losses on available for sale investments 0 0
Increase in the donated asset reserve due to receipt of donated assets 0 0
Reductions in the donated asset reserve due to depreciation (300) (306)
Additions / (reductions) in "other reserves" 0 0
Other recognised gains and losses 0 0
Total gains and losses relating to the financial period 5,178 4,410
Total gains and losses recognised since last annual report 5,178 4,410
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
67
Cash Flow Statement for the Year Ended 31st March 2009
2008/09 2007/08NOTE £ 000s £ 000s
OPERATING ACTIVITIES Net cash inflow / (outflow) from operating activities 19.1 10,116 6,874
RETURNS ON INVESTMENTS AND SERVICING OF FINANCE: Interest received 556 582Interest paid 0 0Interest element of finance leases 0 0Net cash inflow / (outflow) from returns on investments and servicing of finance 556 582
Taxation paid / received 0 0
CAPITAL EXPENDITURE Payments to acquire tangible fixed assets (3,572) (3,383)Receipts from sale of tangible fixed assets 0 0Payments to acquire intangible fixed assets 0 (14)Receipts from sale of intangible fixed assets 0 0(Payments)/receipts for fixed asset investments 0 0Net cash inflow / (outflow) from capital expenditure (3,572) (3,397)
DIVIDENDS PAID (927) (1,119)
Net cash inflow / (outflow) before management of liquid resources and financing 6,173 2,940
MANAGEMENT OF LIQUID RESOURCES (Purchase) of current asset investments 0 0Sale of current asset investments 0 0Net cash inflow / (outflow) before financing 6,173 2,940
FINANCING Public Dividend Capital received 0 692Public dividend capital repaid 0 0Loans received from Foundation Trust Financing Facility 0 0Other loans received 0 0Loans repaid to Foundation Trust Financing Facility 0 0Other loans repaid 0 0Other capital receipts 0 0Capital element of finance lease rental payments 0 0Net cash inflow / (outflow) from financing 0 692
Increase / (decrease) in cash 6,173 3,632
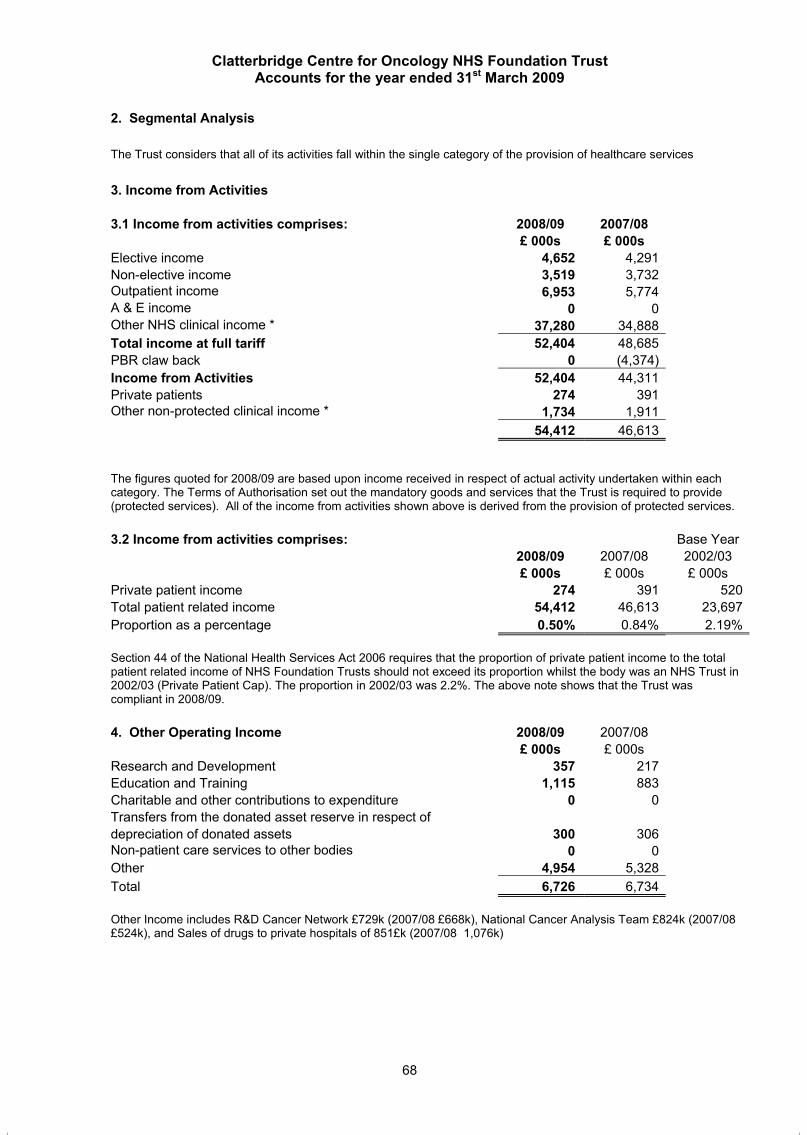
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
68
2. Segmental Analysis
The Trust considers that all of its activities fall within the single category of the provision of healthcare services
3. Income from Activities
3.1 Income from activities comprises: 2008/09 2007/08 £ 000s £ 000s
Elective income 4,652 4,291Non-elective income 3,519 3,732Outpatient income 6,953 5,774A & E income 0 0Other NHS clinical income * 37,280 34,888Total income at full tariff 52,404 48,685PBR claw back 0 (4,374) Income from Activities 52,404 44,311Private patients 274 391Other non-protected clinical income * 1,734 1,911
54,412 46,613
The figures quoted for 2008/09 are based upon income received in respect of actual activity undertaken within each category. The Terms of Authorisation set out the mandatory goods and services that the Trust is required to provide (protected services). All of the income from activities shown above is derived from the provision of protected services.
3.2 Income from activities comprises: Base Year 2008/09 2007/08 2002/03
£ 000s £ 000s £ 000s Private patient income 274 391 520Total patient related income 54,412 46,613 23,697Proportion as a percentage 0.50% 0.84% 2.19%
Section 44 of the National Health Services Act 2006 requires that the proportion of private patient income to the total patient related income of NHS Foundation Trusts should not exceed its proportion whilst the body was an NHS Trust in 2002/03 (Private Patient Cap). The proportion in 2002/03 was 2.2%. The above note shows that the Trust was compliant in 2008/09.
4. Other Operating Income 2008/09 2007/08 £ 000s £ 000s
Research and Development 357 217Education and Training 1,115 883Charitable and other contributions to expenditure 0 0Transfers from the donated asset reserve in respect of depreciation of donated assets 300 306Non-patient care services to other bodies 0 0Other 4,954 5,328Total 6,726 6,734
Other Income includes R&D Cancer Network £729k (2007/08 £668k), National Cancer Analysis Team £824k (2007/08 £524k), and Sales of drugs to private hospitals of 851£k (2007/08 1,076k)
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
69
5. Operating Expenses
5.1 Operating expenses comprise: 2008/09 2007/08
£ 000s £ 000s Services from NHS Foundation Trusts 4,408 2,488 Services from other NHS Trusts 1,822 2,416 Services from other NHS bodies 66 0 Purchase of healthcare from non NHS bodies 0 0 Executive Directors' costs 578 501 Non Executive Directors' costs 118 117 Staff costs 24,848 21,527 Drugs costs 14,452 13,115 Supplies and services - clinical (Excluding drug costs) 2,291 2,222 Supplies and services - general 203 193 Establishment 1,158 1,165 Transport 6 5 Premises 2,067 2,043 Bad debts (23) 128 Other impairment of financial assets 0 0 Depreciation and amortisation 3,184 3,082 Fixed asset impairments 483 85 Fixed asset reversal of impairments 0 0 Audit services - statutory audit 40 51 Other auditor's remuneration 21 60 Clinical negligence 54 70 Exceptional items 0 0 Other 440 174
56,216 49,442 5.2 Operating leases
5.2/1 Operating expenses include:
2008/09 2007/08 £ 000s £ 000s
Hire of plant and machinery 2 155 Other operating lease rentals 650 438
652 593
5.2/2 Annual commitments under non-cancellable operating leases are: Land and buildings Other leases 2008/09 2007/08 2008/09 2007/08 £ 000s £ 000s £ 000s £ 000s
Operating leases which expire: Within 1 year 52 54 136 155Between 1 and 5 years 0 0 457 468After 5 years 0 0 0 0
52 54 593 623
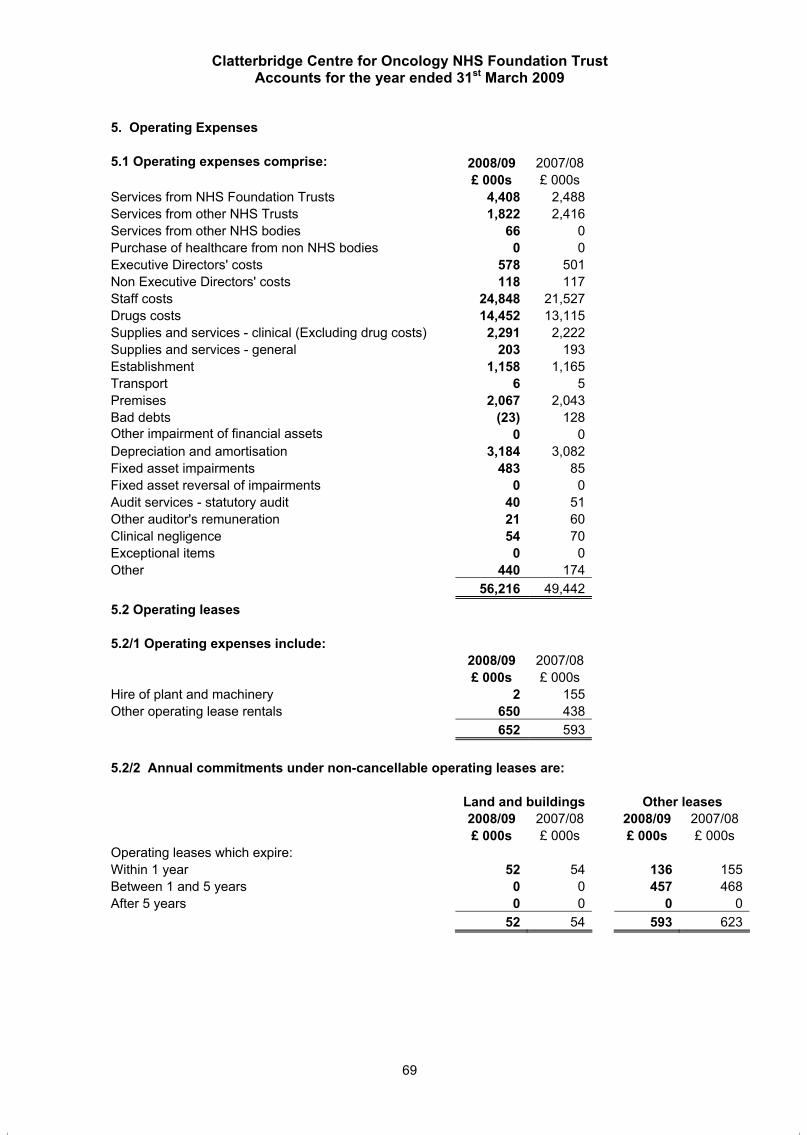
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
68
2. Segmental Analysis
The Trust considers that all of its activities fall within the single category of the provision of healthcare services
3. Income from Activities
3.1 Income from activities comprises: 2008/09 2007/08 £ 000s £ 000s
Elective income 4,652 4,291Non-elective income 3,519 3,732Outpatient income 6,953 5,774A & E income 0 0Other NHS clinical income * 37,280 34,888Total income at full tariff 52,404 48,685PBR claw back 0 (4,374) Income from Activities 52,404 44,311Private patients 274 391Other non-protected clinical income * 1,734 1,911
54,412 46,613
The figures quoted for 2008/09 are based upon income received in respect of actual activity undertaken within each category. The Terms of Authorisation set out the mandatory goods and services that the Trust is required to provide (protected services). All of the income from activities shown above is derived from the provision of protected services.
3.2 Income from activities comprises: Base Year 2008/09 2007/08 2002/03
£ 000s £ 000s £ 000s Private patient income 274 391 520Total patient related income 54,412 46,613 23,697Proportion as a percentage 0.50% 0.84% 2.19%
Section 44 of the National Health Services Act 2006 requires that the proportion of private patient income to the total patient related income of NHS Foundation Trusts should not exceed its proportion whilst the body was an NHS Trust in 2002/03 (Private Patient Cap). The proportion in 2002/03 was 2.2%. The above note shows that the Trust was compliant in 2008/09.
4. Other Operating Income 2008/09 2007/08 £ 000s £ 000s
Research and Development 357 217Education and Training 1,115 883Charitable and other contributions to expenditure 0 0Transfers from the donated asset reserve in respect of depreciation of donated assets 300 306Non-patient care services to other bodies 0 0Other 4,954 5,328Total 6,726 6,734
Other Income includes R&D Cancer Network £729k (2007/08 £668k), National Cancer Analysis Team £824k (2007/08 £524k), and Sales of drugs to private hospitals of 851£k (2007/08 1,076k)
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
69
5. Operating Expenses
5.1 Operating expenses comprise: 2008/09 2007/08
£ 000s £ 000s Services from NHS Foundation Trusts 4,408 2,488 Services from other NHS Trusts 1,822 2,416 Services from other NHS bodies 66 0 Purchase of healthcare from non NHS bodies 0 0 Executive Directors' costs 578 501 Non Executive Directors' costs 118 117 Staff costs 24,848 21,527 Drugs costs 14,452 13,115 Supplies and services - clinical (Excluding drug costs) 2,291 2,222 Supplies and services - general 203 193 Establishment 1,158 1,165 Transport 6 5 Premises 2,067 2,043 Bad debts (23) 128 Other impairment of financial assets 0 0 Depreciation and amortisation 3,184 3,082 Fixed asset impairments 483 85 Fixed asset reversal of impairments 0 0 Audit services - statutory audit 40 51 Other auditor's remuneration 21 60 Clinical negligence 54 70 Exceptional items 0 0 Other 440 174
56,216 49,442 5.2 Operating leases
5.2/1 Operating expenses include:
2008/09 2007/08 £ 000s £ 000s
Hire of plant and machinery 2 155 Other operating lease rentals 650 438
652 593
5.2/2 Annual commitments under non-cancellable operating leases are: Land and buildings Other leases 2008/09 2007/08 2008/09 2007/08 £ 000s £ 000s £ 000s £ 000s
Operating leases which expire: Within 1 year 52 54 136 155Between 1 and 5 years 0 0 457 468After 5 years 0 0 0 0
52 54 593 623
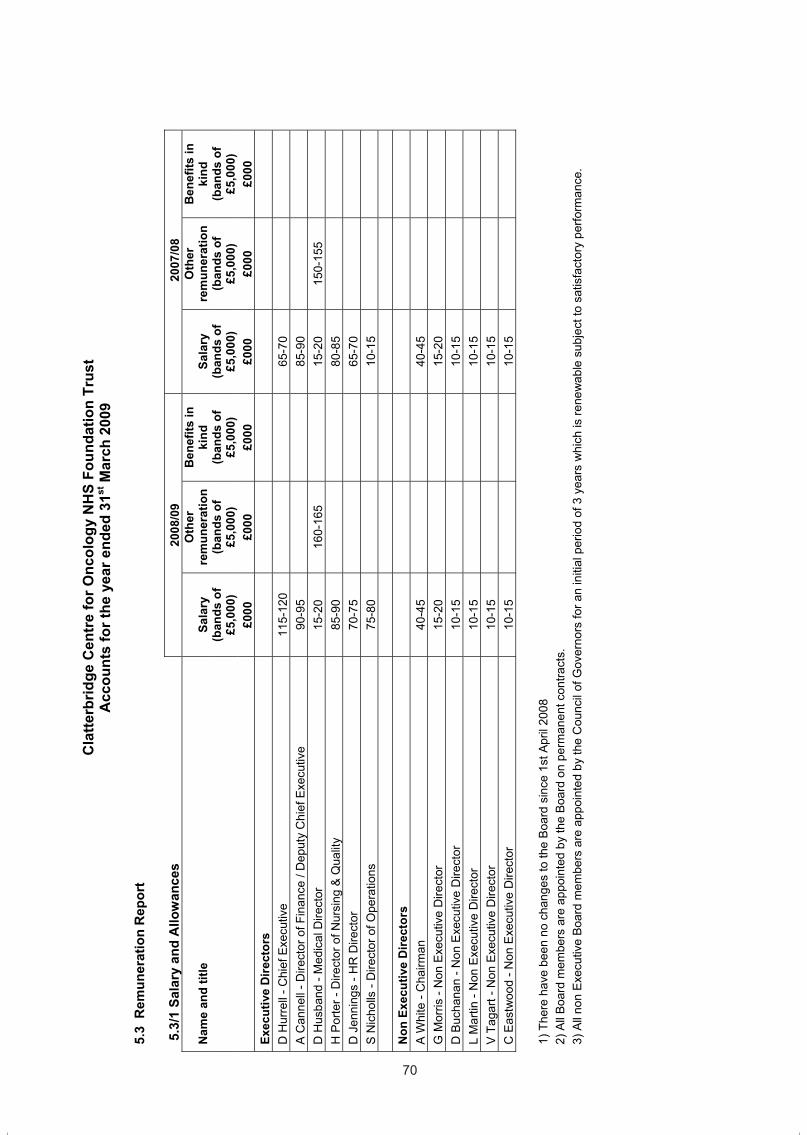
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
70
5.3
Rem
uner
atio
n R
epor
t
5.3
/1 S
alar
y an
d A
llow
ance
s 20
08/0
9 2
007/
08
Nam
e an
d tit
le
Sala
ry
Oth
erre
mun
erat
ion
Ben
efits
in
kind
Sa
lary
O
ther
rem
uner
atio
n B
enef
its in
ki
nd
(ban
ds o
f £5
,000
) (b
ands
of
£5,0
00)
(ban
ds o
f £5
,000
)(b
ands
of
£5,0
00)
(ban
ds o
f £5
,000
)(b
ands
of
£5,0
00)
£000
£0
00
£000
£0
00
£000
£0
00
Exec
utiv
e D
irect
ors
D H
urre
ll - C
hief
Exe
cutiv
e 11
5-12
0 65
-70
A C
anne
ll - D
irect
or o
f Fin
ance
/ D
eput
y C
hief
Exe
cutiv
e 90
-95
85-9
0 D
Hus
band
- M
edic
al D
irect
or
15-2
0 16
0-16
5 15
-20
150-
155
H P
orte
r - D
irect
or o
f Nur
sing
& Q
ualit
y 85
-90
80-8
5 D
Jen
ning
s - H
R D
irect
or
70-7
5 65
-70
S N
icho
lls -
Dire
ctor
of O
pera
tions
75
-80
10-1
5
Non
Exe
cutiv
e D
irect
ors
A W
hite
- C
hairm
an
40-4
5 40
-45
G M
orris
- N
on E
xecu
tive
Dire
ctor
15
-20
15-2
0 D
Buc
hana
n - N
on E
xecu
tive
Dire
ctor
10
-15
10-1
5 L
Mar
tin -
Non
Exe
cutiv
e D
irect
or
10-1
5 10
-15
V T
agar
t - N
on E
xecu
tive
Dire
ctor
10
-15
10-1
5 C
Eas
twoo
d - N
on E
xecu
tive
Dire
ctor
10
-15
10-1
5
1) T
here
hav
e be
en n
o ch
ange
s to
the
Boar
d si
nce
1st A
pril
2008
2)
All
Boar
d m
embe
rs a
re a
ppoi
nted
by
the
Boa
rd o
n pe
rman
ent c
ontra
cts.
3)
All
non
Exec
utiv
e Bo
ard
mem
bers
are
app
oint
ed b
y th
e C
ounc
il of
Gov
erno
rs fo
r an
initi
al p
erio
d of
3 y
ears
whi
ch is
rene
wab
le s
ubje
ct to
sat
isfa
ctor
y pe
rform
ance
.
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
71
5.3/
2 P
ensi
on e
ntitl
emen
ts
Rea
lin
crea
se in
pe
nsio
n at
ag
e 60
Lum
p su
m
at a
ge 6
0 re
late
d to
re
alin
crea
se in
pe
nsio
n
Tota
l ac
crue
d pe
nsio
n at
ag
e 60
at
31 M
arch
20
09
Lum
p su
m
at a
ge 6
0 re
late
d to
ac
crue
d pe
nsio
n at
31
Mar
ch
2009
Cas
h Eq
uiva
lent
Tr
ansf
er to
Va
lue
at 3
1 M
arch
200
9
Cas
h Eq
uiva
lent
Tr
ansf
er to
Va
lue
at 3
1 M
arch
200
8
Rea
lin
crea
se in
C
ash
Equi
vale
nt
Tran
sfer
Va
lue
Empl
oyer
'sco
ntrib
utio
n to
st
akeh
old
erpe
nsio
n
(ban
ds o
f £2
,500
) (b
ands
of
£2,5
00)
(ban
ds o
f £5
,000
) (b
ands
of
£5,0
00)
Rou
nd
tone
ares
t £0
0)N
ame
and
title
£0
00
£000
£0
00
£000
£0
00
£000
£0
00
£00
D H
urre
ll- C
hief
Exe
cutiv
e
7.5-
10
25-2
7.5
25-3
0 75
-80
422
217
140
0 A
Can
nell
- Dire
ctor
of F
inan
ce /
Dep
uty
Chi
ef E
xecu
tive
0-2.
5 2.
5-5
25-3
0 80
-85
469
345
81
0 D
Hus
band
- M
edic
al D
irect
or
(0-2
.5)
(0-2
.5)
50-5
5 16
0-16
5 1,
288
939
228
0 H
Por
ter -
Dire
ctor
of N
ursi
ng &
Qua
lity
0-2.
5 5-
7.5
25-3
0 75
-80
462
328
88
0 D
Jen
ning
s - H
R D
irect
or
0-2.
5 2.
5-5
0-5
5-10
53
30
15
0
S N
icho
lls -
Dire
ctor
of O
pera
tions
0-
2.5
2-5.
5 0-
5 10
-15
65
37
18
0
A
s N
on-E
xecu
tive
mem
bers
do
not r
ecei
ve p
ensi
onab
le re
mun
erat
ion,
ther
e ar
e no
ent
ries
in re
spec
t of p
ensi
ons
for N
on-E
xecu
tive
mem
bers
.
Cas
h Eq
uiva
lent
Tra
nsfe
r Val
ues
A C
ash
Equ
ival
ent T
rans
fer V
alue
(CE
TV) i
s th
e ac
tuar
ially
ass
esse
d ca
pita
l val
ue o
f the
pen
sion
sch
eme
bene
fits
accr
ued
by a
mem
ber a
t a p
artic
ular
poi
nt in
tim
e. T
he b
enef
its
valu
ed a
re th
e m
embe
r's a
ccru
ed b
enef
its a
nd a
ny c
ontin
gent
spo
use'
s pe
nsio
n pa
yabl
e fro
m th
e sc
hem
e. A
CE
TV fi
gure
is a
pay
men
t mad
e by
a p
ensi
on s
chem
e or
ar
rang
emen
t to
secu
re p
ensi
on b
enef
its in
ano
ther
pen
sion
sch
eme
or a
rran
gem
ent w
hen
the
mem
ber l
eave
s a
sche
me
and
choo
ses
to tr
ansf
er th
e be
nefit
s ac
crue
d in
thei
r fo
rmer
sch
eme.
The
pen
sion
figu
res
show
n re
late
to th
e be
nefit
s th
at th
e in
divi
dual
has
acc
rued
as
a co
nseq
uenc
e of
thei
r tot
al m
embe
rshi
p of
the
pens
ion
sche
me,
not
just
thei
r se
rvic
e in
a s
enio
r cap
acity
to w
hich
dis
clos
ure
appl
ies.
The
CE
TV fi
gure
s an
d th
e ot
her p
ensi
on d
etai
ls in
clud
e th
e va
lue
of a
ny p
ensi
on b
enef
its in
ano
ther
sch
eme
or
arra
ngem
ent w
hich
the
indi
vidu
al h
as tr
ansf
erre
d to
the
NH
S p
ensi
on s
chem
e. T
hey
also
incl
ude
any
addi
tiona
l pen
sion
ben
efit
accr
ued
to th
e m
embe
r as
a re
sult
of th
eir
purc
hasi
ng a
dditi
onal
yea
rs o
f pen
sion
ser
vice
in th
e sc
hem
e at
thei
r ow
n co
st. C
ETV
s ar
e ca
lcul
ated
with
in th
e gu
idel
ines
and
fram
ewor
k pr
escr
ibed
by
the
Inst
itute
and
Fac
ulty
of
Act
uarie
s.
Rea
l Inc
reas
e in
CET
VTh
is re
flect
s th
e in
crea
se in
CE
TV e
ffect
ivel
y fu
nded
by
the
empl
oyer
. It t
akes
acc
ount
of t
he in
crea
se in
acc
rued
pen
sion
due
to in
flatio
n, c
ontri
butio
ns p
aid
by th
e em
ploy
ee
(incl
udin
g th
e va
lue
of a
ny b
enef
its tr
ansf
erre
d fro
m a
noth
er s
chem
e or
arr
ange
men
t) an
d us
es c
omm
on m
arke
t val
uatio
n fa
ctor
s fo
r the
sta
rt an
d en
d of
the
perio
d.
70
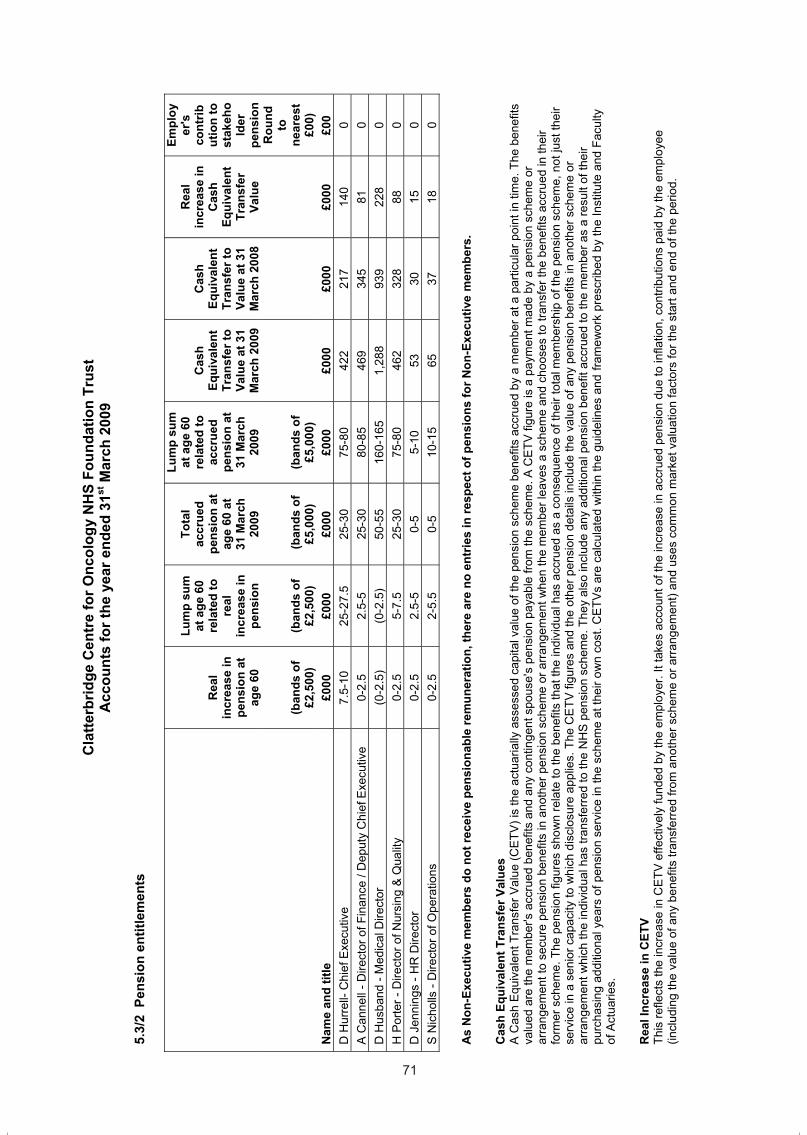
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
70
5.3
Rem
uner
atio
n R
epor
t
5.3
/1 S
alar
y an
d A
llow
ance
s 20
08/0
9 2
007/
08
Nam
e an
d tit
le
Sala
ry
Oth
erre
mun
erat
ion
Ben
efits
in
kind
Sa
lary
O
ther
rem
uner
atio
n B
enef
its in
ki
nd
(ban
ds o
f £5
,000
) (b
ands
of
£5,0
00)
(ban
ds o
f £5
,000
)(b
ands
of
£5,0
00)
(ban
ds o
f £5
,000
)(b
ands
of
£5,0
00)
£000
£0
00
£000
£0
00
£000
£0
00
Exec
utiv
e D
irect
ors
D H
urre
ll - C
hief
Exe
cutiv
e 11
5-12
0 65
-70
A C
anne
ll - D
irect
or o
f Fin
ance
/ D
eput
y C
hief
Exe
cutiv
e 90
-95
85-9
0 D
Hus
band
- M
edic
al D
irect
or
15-2
0 16
0-16
5 15
-20
150-
155
H P
orte
r - D
irect
or o
f Nur
sing
& Q
ualit
y 85
-90
80-8
5 D
Jen
ning
s - H
R D
irect
or
70-7
5 65
-70
S N
icho
lls -
Dire
ctor
of O
pera
tions
75
-80
10-1
5
Non
Exe
cutiv
e D
irect
ors
A W
hite
- C
hairm
an
40-4
5 40
-45
G M
orris
- N
on E
xecu
tive
Dire
ctor
15
-20
15-2
0 D
Buc
hana
n - N
on E
xecu
tive
Dire
ctor
10
-15
10-1
5 L
Mar
tin -
Non
Exe
cutiv
e D
irect
or
10-1
5 10
-15
V T
agar
t - N
on E
xecu
tive
Dire
ctor
10
-15
10-1
5 C
Eas
twoo
d - N
on E
xecu
tive
Dire
ctor
10
-15
10-1
5
1) T
here
hav
e be
en n
o ch
ange
s to
the
Boar
d si
nce
1st A
pril
2008
2)
All
Boar
d m
embe
rs a
re a
ppoi
nted
by
the
Boa
rd o
n pe
rman
ent c
ontra
cts.
3)
All
non
Exec
utiv
e Bo
ard
mem
bers
are
app
oint
ed b
y th
e C
ounc
il of
Gov
erno
rs fo
r an
initi
al p
erio
d of
3 y
ears
whi
ch is
rene
wab
le s
ubje
ct to
sat
isfa
ctor
y pe
rform
ance
.
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
71
5.3/
2 P
ensi
on e
ntitl
emen
ts
Rea
lin
crea
se in
pe
nsio
n at
ag
e 60
Lum
p su
m
at a
ge 6
0 re
late
d to
re
alin
crea
se in
pe
nsio
n
Tota
l ac
crue
d pe
nsio
n at
ag
e 60
at
31 M
arch
20
09
Lum
p su
m
at a
ge 6
0 re
late
d to
ac
crue
d pe
nsio
n at
31
Mar
ch
2009
Cas
h Eq
uiva
lent
Tr
ansf
er to
Va
lue
at 3
1 M
arch
200
9
Cas
h Eq
uiva
lent
Tr
ansf
er to
Va
lue
at 3
1 M
arch
200
8
Rea
lin
crea
se in
C
ash
Equi
vale
nt
Tran
sfer
Va
lue
Empl
oyer
'sco
ntrib
utio
n to
st
akeh
old
erpe
nsio
n
(ban
ds o
f £2
,500
) (b
ands
of
£2,5
00)
(ban
ds o
f £5
,000
) (b
ands
of
£5,0
00)
Rou
nd
tone
ares
t £0
0)N
ame
and
title
£0
00
£000
£0
00
£000
£0
00
£000
£0
00
£00
D H
urre
ll- C
hief
Exe
cutiv
e
7.5-
10
25-2
7.5
25-3
0 75
-80
422
217
140
0 A
Can
nell
- Dire
ctor
of F
inan
ce /
Dep
uty
Chi
ef E
xecu
tive
0-2.
5 2.
5-5
25-3
0 80
-85
469
345
81
0 D
Hus
band
- M
edic
al D
irect
or
(0-2
.5)
(0-2
.5)
50-5
5 16
0-16
5 1,
288
939
228
0 H
Por
ter -
Dire
ctor
of N
ursi
ng &
Qua
lity
0-2.
5 5-
7.5
25-3
0 75
-80
462
328
88
0 D
Jen
ning
s - H
R D
irect
or
0-2.
5 2.
5-5
0-5
5-10
53
30
15
0
S N
icho
lls -
Dire
ctor
of O
pera
tions
0-
2.5
2-5.
5 0-
5 10
-15
65
37
18
0
A
s N
on-E
xecu
tive
mem
bers
do
not r
ecei
ve p
ensi
onab
le re
mun
erat
ion,
ther
e ar
e no
ent
ries
in re
spec
t of p
ensi
ons
for N
on-E
xecu
tive
mem
bers
.
Cas
h Eq
uiva
lent
Tra
nsfe
r Val
ues
A C
ash
Equ
ival
ent T
rans
fer V
alue
(CE
TV) i
s th
e ac
tuar
ially
ass
esse
d ca
pita
l val
ue o
f the
pen
sion
sch
eme
bene
fits
accr
ued
by a
mem
ber a
t a p
artic
ular
poi
nt in
tim
e. T
he b
enef
its
valu
ed a
re th
e m
embe
r's a
ccru
ed b
enef
its a
nd a
ny c
ontin
gent
spo
use'
s pe
nsio
n pa
yabl
e fro
m th
e sc
hem
e. A
CE
TV fi
gure
is a
pay
men
t mad
e by
a p
ensi
on s
chem
e or
ar
rang
emen
t to
secu
re p
ensi
on b
enef
its in
ano
ther
pen
sion
sch
eme
or a
rran
gem
ent w
hen
the
mem
ber l
eave
s a
sche
me
and
choo
ses
to tr
ansf
er th
e be
nefit
s ac
crue
d in
thei
r fo
rmer
sch
eme.
The
pen
sion
figu
res
show
n re
late
to th
e be
nefit
s th
at th
e in
divi
dual
has
acc
rued
as
a co
nseq
uenc
e of
thei
r tot
al m
embe
rshi
p of
the
pens
ion
sche
me,
not
just
thei
r se
rvic
e in
a s
enio
r cap
acity
to w
hich
dis
clos
ure
appl
ies.
The
CE
TV fi
gure
s an
d th
e ot
her p
ensi
on d
etai
ls in
clud
e th
e va
lue
of a
ny p
ensi
on b
enef
its in
ano
ther
sch
eme
or
arra
ngem
ent w
hich
the
indi
vidu
al h
as tr
ansf
erre
d to
the
NH
S p
ensi
on s
chem
e. T
hey
also
incl
ude
any
addi
tiona
l pen
sion
ben
efit
accr
ued
to th
e m
embe
r as
a re
sult
of th
eir
purc
hasi
ng a
dditi
onal
yea
rs o
f pen
sion
ser
vice
in th
e sc
hem
e at
thei
r ow
n co
st. C
ETV
s ar
e ca
lcul
ated
with
in th
e gu
idel
ines
and
fram
ewor
k pr
escr
ibed
by
the
Inst
itute
and
Fac
ulty
of
Act
uarie
s.
Rea
l Inc
reas
e in
CET
VTh
is re
flect
s th
e in
crea
se in
CE
TV e
ffect
ivel
y fu
nded
by
the
empl
oyer
. It t
akes
acc
ount
of t
he in
crea
se in
acc
rued
pen
sion
due
to in
flatio
n, c
ontri
butio
ns p
aid
by th
e em
ploy
ee
(incl
udin
g th
e va
lue
of a
ny b
enef
its tr
ansf
erre
d fro
m a
noth
er s
chem
e or
arr
ange
men
t) an
d us
es c
omm
on m
arke
t val
uatio
n fa
ctor
s fo
r the
sta
rt an
d en
d of
the
perio
d.
71
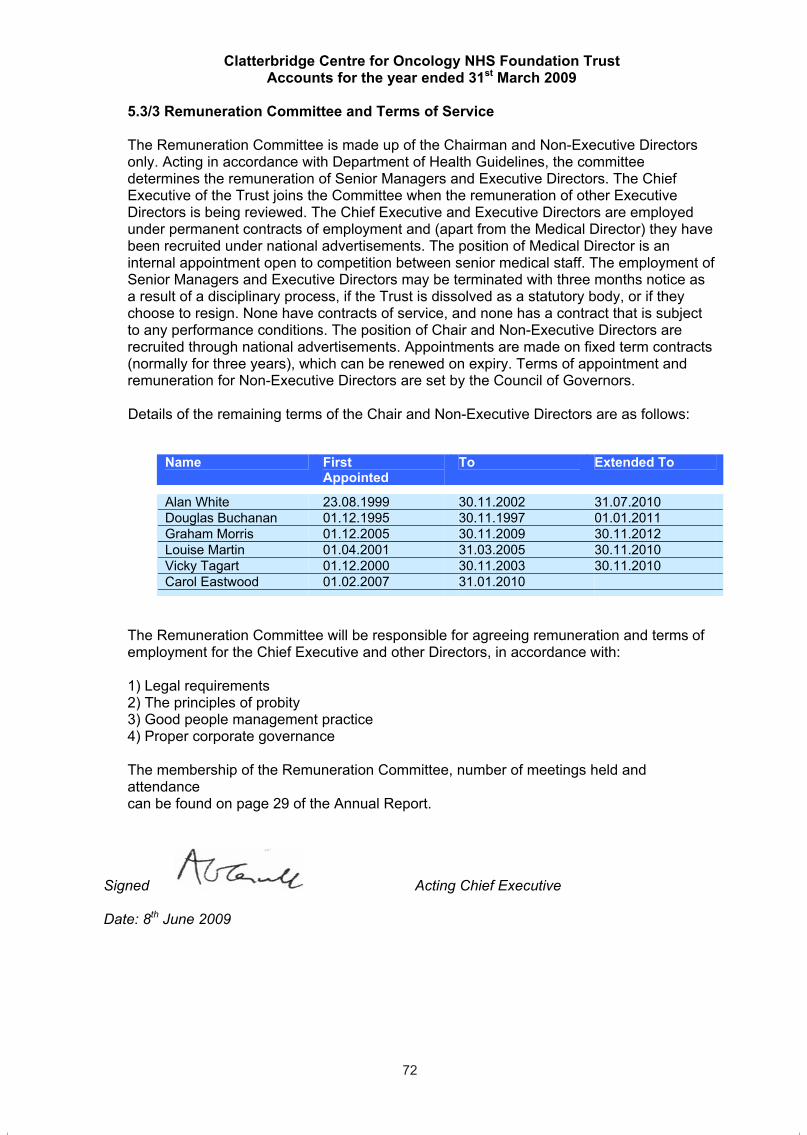
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
72
5.3/3 Remuneration Committee and Terms of Service
The Remuneration Committee is made up of the Chairman and Non-Executive Directors only. Acting in accordance with Department of Health Guidelines, the committee determines the remuneration of Senior Managers and Executive Directors. The Chief Executive of the Trust joins the Committee when the remuneration of other Executive Directors is being reviewed. The Chief Executive and Executive Directors are employed under permanent contracts of employment and (apart from the Medical Director) they have been recruited under national advertisements. The position of Medical Director is an internal appointment open to competition between senior medical staff. The employment of Senior Managers and Executive Directors may be terminated with three months notice as a result of a disciplinary process, if the Trust is dissolved as a statutory body, or if they choose to resign. None have contracts of service, and none has a contract that is subject to any performance conditions. The position of Chair and Non-Executive Directors are recruited through national advertisements. Appointments are made on fixed term contracts (normally for three years), which can be renewed on expiry. Terms of appointment and remuneration for Non-Executive Directors are set by the Council of Governors.
Details of the remaining terms of the Chair and Non-Executive Directors are as follows:
Name FirstAppointed
To Extended To
Alan White 23.08.1999 30.11.2002 31.07.2010 Douglas Buchanan 01.12.1995 30.11.1997 01.01.2011 Graham Morris 01.12.2005 30.11.2009 30.11.2012 Louise Martin 01.04.2001 31.03.2005 30.11.2010 Vicky Tagart 01.12.2000 30.11.2003 30.11.2010 Carol Eastwood 01.02.2007 31.01.2010
The Remuneration Committee will be responsible for agreeing remuneration and terms ofemployment for the Chief Executive and other Directors, in accordance with:
1) Legal requirements 2) The principles of probity 3) Good people management practice4) Proper corporate governance
The membership of the Remuneration Committee, number of meetings held and attendancecan be found on page 29 of the Annual Report.
Signed Acting Chief Executive
Date: 8th June 2009
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
73
6. Staff Costs and Numbers 6.1 Staff costs 2008/09 2007/08
£ 000s £ 000s Salaries and wages 21,169 18,330Social Security costs 1,462 1,262Employer contributions to NHSPA 2,354 2,080Other Pension Costs 0 0Agency and contract staff 441 356
25,426 22,028
All employer pension contributions in 2008/09 were paid to the NHS Pensions Agency. Accounting policies for pensions and other retirement benefits are set out in Note 1.18 on page 59 Details of senior employees’ remuneration can be found on page 70 of the Remuneration report
6.2 Average number of persons employed (Wte basis) 2008/09 2007/08
Total TotalNumber Number
Medical and dental 56 52Ambulance staff 0 0Administration and estates 163 153Healthcare assistants & other support staff 49 48Nursing, midwifery & health visiting staff 119 116Nursing, midwifery & health visiting learners 0 0Scientific, therapeutic and technical staff 186 184Social care staff 0 0Bank and agency staff 0 0Other 20 16Total 593 569
6.3 Employee Benefits None
6.4 Retirements due to ill-health This note discloses the number and additional pension costs for individuals who retired early on ill health grounds during the year. There were no such retirements, and therefore no additional cost (2007/08 – none). This information has been supplied by the NHS Pensions Agency.
6.5 Management costs
2008/09 2007/08£000 £000
Management costs 2,312 1,849Income 61,138 53,347Management costs as % of Income 3.8% 3.5%
Management costs are defined as those on the management costs website at www.dh.gov.uk/PolicyAndGuidance/OrganisationPolicy/FinanceAndPlanning/NHSManagementCosts/fs/en..www.dh.gov.uk/policyandguidance/organisation policy/financeandplanning/nhsmanagementcosts/fs/en.
72
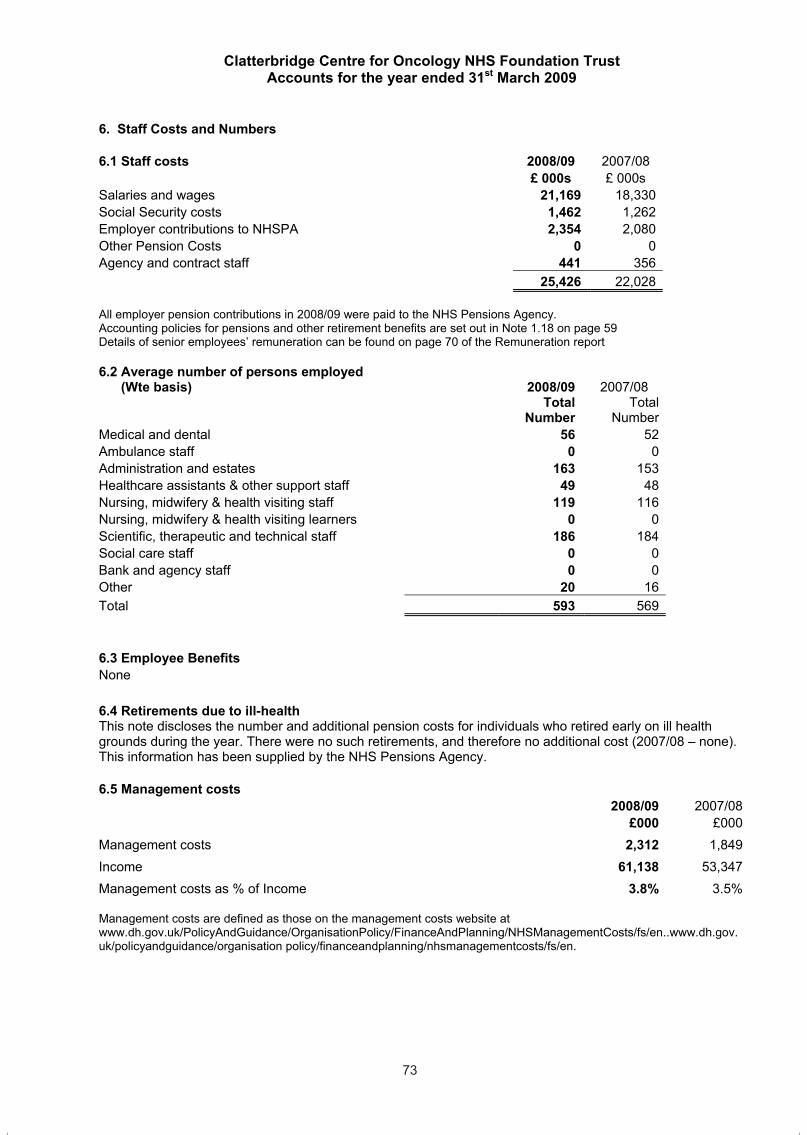
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
72
5.3/3 Remuneration Committee and Terms of Service
The Remuneration Committee is made up of the Chairman and Non-Executive Directors only. Acting in accordance with Department of Health Guidelines, the committee determines the remuneration of Senior Managers and Executive Directors. The Chief Executive of the Trust joins the Committee when the remuneration of other Executive Directors is being reviewed. The Chief Executive and Executive Directors are employed under permanent contracts of employment and (apart from the Medical Director) they have been recruited under national advertisements. The position of Medical Director is an internal appointment open to competition between senior medical staff. The employment of Senior Managers and Executive Directors may be terminated with three months notice as a result of a disciplinary process, if the Trust is dissolved as a statutory body, or if they choose to resign. None have contracts of service, and none has a contract that is subject to any performance conditions. The position of Chair and Non-Executive Directors are recruited through national advertisements. Appointments are made on fixed term contracts (normally for three years), which can be renewed on expiry. Terms of appointment and remuneration for Non-Executive Directors are set by the Council of Governors.
Details of the remaining terms of the Chair and Non-Executive Directors are as follows:
Name FirstAppointed
To Extended To
Alan White 23.08.1999 30.11.2002 31.07.2010 Douglas Buchanan 01.12.1995 30.11.1997 01.01.2011 Graham Morris 01.12.2005 30.11.2009 30.11.2012 Louise Martin 01.04.2001 31.03.2005 30.11.2010 Vicky Tagart 01.12.2000 30.11.2003 30.11.2010 Carol Eastwood 01.02.2007 31.01.2010
The Remuneration Committee will be responsible for agreeing remuneration and terms ofemployment for the Chief Executive and other Directors, in accordance with:
1) Legal requirements 2) The principles of probity 3) Good people management practice4) Proper corporate governance
The membership of the Remuneration Committee, number of meetings held and attendancecan be found on page 29 of the Annual Report.
Signed Acting Chief Executive
Date: 8th June 2009
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
73
6. Staff Costs and Numbers 6.1 Staff costs 2008/09 2007/08
£ 000s £ 000s Salaries and wages 21,169 18,330Social Security costs 1,462 1,262Employer contributions to NHSPA 2,354 2,080Other Pension Costs 0 0Agency and contract staff 441 356
25,426 22,028
All employer pension contributions in 2008/09 were paid to the NHS Pensions Agency. Accounting policies for pensions and other retirement benefits are set out in Note 1.18 on page 59 Details of senior employees’ remuneration can be found on page 70 of the Remuneration report
6.2 Average number of persons employed (Wte basis) 2008/09 2007/08
Total TotalNumber Number
Medical and dental 56 52Ambulance staff 0 0Administration and estates 163 153Healthcare assistants & other support staff 49 48Nursing, midwifery & health visiting staff 119 116Nursing, midwifery & health visiting learners 0 0Scientific, therapeutic and technical staff 186 184Social care staff 0 0Bank and agency staff 0 0Other 20 16Total 593 569
6.3 Employee Benefits None
6.4 Retirements due to ill-health This note discloses the number and additional pension costs for individuals who retired early on ill health grounds during the year. There were no such retirements, and therefore no additional cost (2007/08 – none). This information has been supplied by the NHS Pensions Agency.
6.5 Management costs
2008/09 2007/08£000 £000
Management costs 2,312 1,849Income 61,138 53,347Management costs as % of Income 3.8% 3.5%
Management costs are defined as those on the management costs website at www.dh.gov.uk/PolicyAndGuidance/OrganisationPolicy/FinanceAndPlanning/NHSManagementCosts/fs/en..www.dh.gov.uk/policyandguidance/organisation policy/financeandplanning/nhsmanagementcosts/fs/en.
73
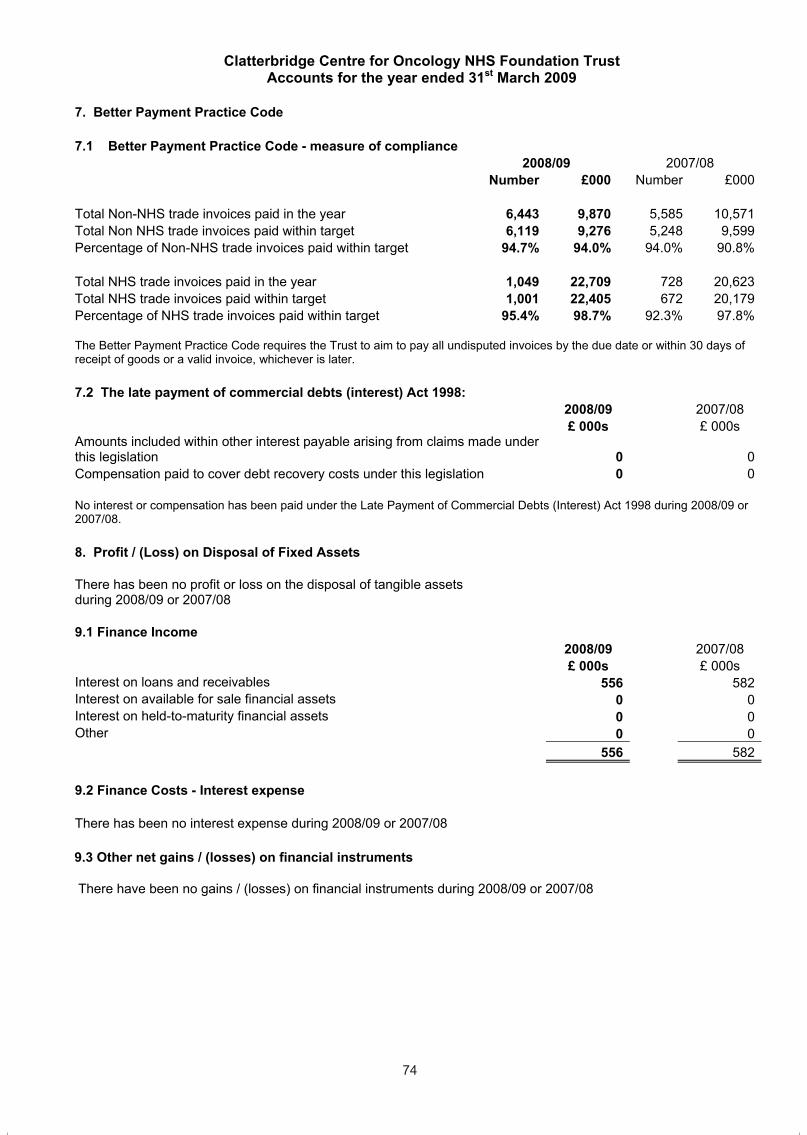
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
74
7. Better Payment Practice Code
7.1 Better Payment Practice Code - measure of compliance 2008/09 2007/08
Number £000 Number £000
Total Non-NHS trade invoices paid in the year 6,443 9,870 5,585 10,571Total Non NHS trade invoices paid within target 6,119 9,276 5,248 9,599Percentage of Non-NHS trade invoices paid within target 94.7% 94.0% 94.0% 90.8%
Total NHS trade invoices paid in the year 1,049 22,709 728 20,623Total NHS trade invoices paid within target 1,001 22,405 672 20,179Percentage of NHS trade invoices paid within target 95.4% 98.7% 92.3% 97.8%
The Better Payment Practice Code requires the Trust to aim to pay all undisputed invoices by the due date or within 30 days of receipt of goods or a valid invoice, whichever is later.
7.2 The late payment of commercial debts (interest) Act 1998: 2008/09 2007/08 £ 000s £ 000s
Amounts included within other interest payable arising from claims made under this legislation 0 0Compensation paid to cover debt recovery costs under this legislation 0 0
No interest or compensation has been paid under the Late Payment of Commercial Debts (Interest) Act 1998 during 2008/09 or 2007/08.
8. Profit / (Loss) on Disposal of Fixed Assets
There has been no profit or loss on the disposal of tangible assets during 2008/09 or 2007/08
9.1 Finance Income 2008/09 2007/08 £ 000s £ 000s
Interest on loans and receivables 556 582Interest on available for sale financial assets 0 0Interest on held-to-maturity financial assets 0 0Other 0 0
556 582
9.2 Finance Costs - Interest expense
There has been no interest expense during 2008/09 or 2007/08
9.3 Other net gains / (losses) on financial instruments
There have been no gains / (losses) on financial instruments during 2008/09 or 2007/08
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
75
10. I
ntan
gibl
e Fi
xed
Ass
ets
10.1
Inta
ngib
le fi
xed
asse
ts a
t the
bal
ance
she
et d
ate
com
pris
e th
e fo
llow
ing
elem
ents
:
Softw
are
Lice
nses
Li
cens
es
and
Trad
emar
ks
Pate
nts
Dev
elop
men
t Ex
pend
iture
G
oodw
ill
Oth
er
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
Gro
ss C
ost a
t 1 A
pril
2008
27
0
0 0
0 0
27
Impa
irmen
ts
0 0
0 0
0 0
0 R
ecla
ssifi
catio
ns
0 0
0 0
0 0
0 O
ther
in y
ear r
eval
uatio
n
0 0
0 0
0 0
0 A
dditi
ons
– pu
rcha
sed
0
0 0
0 0
0 0
Add
ition
s –
dona
ted
0 0
0 0
0 0
0 D
ispo
sals
0
0 0
0 0
0 0
At 3
1st M
arch
200
9 27
0
0 0
0 0
27
A
mor
tisat
ion
at 1
st A
pril
2008
13
00
00
013
Prov
ided
dur
ing
the
year
5
00
00
05
Impa
irmen
ts
00
00
00
0R
ever
sal o
f Im
pairm
ents
0
00
00
00
Rec
lass
ifica
tions
0
00
00
00
Oth
er in
yea
r rev
alua
tion
0
00
00
00
Dis
posa
ls
00
00
00
0A
ccum
ulat
ed d
epre
ciat
ion
at 3
1st M
arch
200
9 18
0
0 0
0 0
18
N
et b
ook
valu
e
- P
urch
ased
at 1
st A
pril
2008
14
00
00
014
- Don
ated
at 1
st A
pril
2008
0
00
00
00
Tota
l at 1
st A
pril
2008
14
0
0 0
0 0
14
- Pur
chas
ed a
t 31s
t Mar
ch 2
009
90
00
00
9- D
onat
ed a
t 31s
t Mar
ch 2
009
00
00
00
0To
tal a
t 31s
t Mar
ch 2
009
9 0
0 0
0 0
9
74

Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
74
7. Better Payment Practice Code
7.1 Better Payment Practice Code - measure of compliance 2008/09 2007/08
Number £000 Number £000
Total Non-NHS trade invoices paid in the year 6,443 9,870 5,585 10,571Total Non NHS trade invoices paid within target 6,119 9,276 5,248 9,599Percentage of Non-NHS trade invoices paid within target 94.7% 94.0% 94.0% 90.8%
Total NHS trade invoices paid in the year 1,049 22,709 728 20,623Total NHS trade invoices paid within target 1,001 22,405 672 20,179Percentage of NHS trade invoices paid within target 95.4% 98.7% 92.3% 97.8%
The Better Payment Practice Code requires the Trust to aim to pay all undisputed invoices by the due date or within 30 days of receipt of goods or a valid invoice, whichever is later.
7.2 The late payment of commercial debts (interest) Act 1998: 2008/09 2007/08 £ 000s £ 000s
Amounts included within other interest payable arising from claims made under this legislation 0 0Compensation paid to cover debt recovery costs under this legislation 0 0
No interest or compensation has been paid under the Late Payment of Commercial Debts (Interest) Act 1998 during 2008/09 or 2007/08.
8. Profit / (Loss) on Disposal of Fixed Assets
There has been no profit or loss on the disposal of tangible assets during 2008/09 or 2007/08
9.1 Finance Income 2008/09 2007/08 £ 000s £ 000s
Interest on loans and receivables 556 582Interest on available for sale financial assets 0 0Interest on held-to-maturity financial assets 0 0Other 0 0
556 582
9.2 Finance Costs - Interest expense
There has been no interest expense during 2008/09 or 2007/08
9.3 Other net gains / (losses) on financial instruments
There have been no gains / (losses) on financial instruments during 2008/09 or 2007/08
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
75
10. I
ntan
gibl
e Fi
xed
Ass
ets
10.1
Inta
ngib
le fi
xed
asse
ts a
t the
bal
ance
she
et d
ate
com
pris
e th
e fo
llow
ing
elem
ents
:
Softw
are
Lice
nses
Li
cens
es
and
Trad
emar
ks
Pate
nts
Dev
elop
men
t Ex
pend
iture
G
oodw
ill
Oth
er
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
Gro
ss C
ost a
t 1 A
pril
2008
27
0
0 0
0 0
27
Impa
irmen
ts
0 0
0 0
0 0
0 R
ecla
ssifi
catio
ns
0 0
0 0
0 0
0 O
ther
in y
ear r
eval
uatio
n
0 0
0 0
0 0
0 A
dditi
ons
– pu
rcha
sed
0
0 0
0 0
0 0
Add
ition
s –
dona
ted
0 0
0 0
0 0
0 D
ispo
sals
0
0 0
0 0
0 0
At 3
1st M
arch
200
9 27
0
0 0
0 0
27
A
mor
tisat
ion
at 1
st A
pril
2008
13
00
00
013
Prov
ided
dur
ing
the
year
5
00
00
05
Impa
irmen
ts
00
00
00
0R
ever
sal o
f Im
pairm
ents
0
00
00
00
Rec
lass
ifica
tions
0
00
00
00
Oth
er in
yea
r rev
alua
tion
0
00
00
00
Dis
posa
ls
00
00
00
0A
ccum
ulat
ed d
epre
ciat
ion
at 3
1st M
arch
200
9 18
0
0 0
0 0
18
N
et b
ook
valu
e
- P
urch
ased
at 1
st A
pril
2008
14
00
00
014
- Don
ated
at 1
st A
pril
2008
0
00
00
00
Tota
l at 1
st A
pril
2008
14
0
0 0
0 0
14
- Pur
chas
ed a
t 31s
t Mar
ch 2
009
90
00
00
9- D
onat
ed a
t 31s
t Mar
ch 2
009
00
00
00
0To
tal a
t 31s
t Mar
ch 2
009
9 0
0 0
0 0
9
75
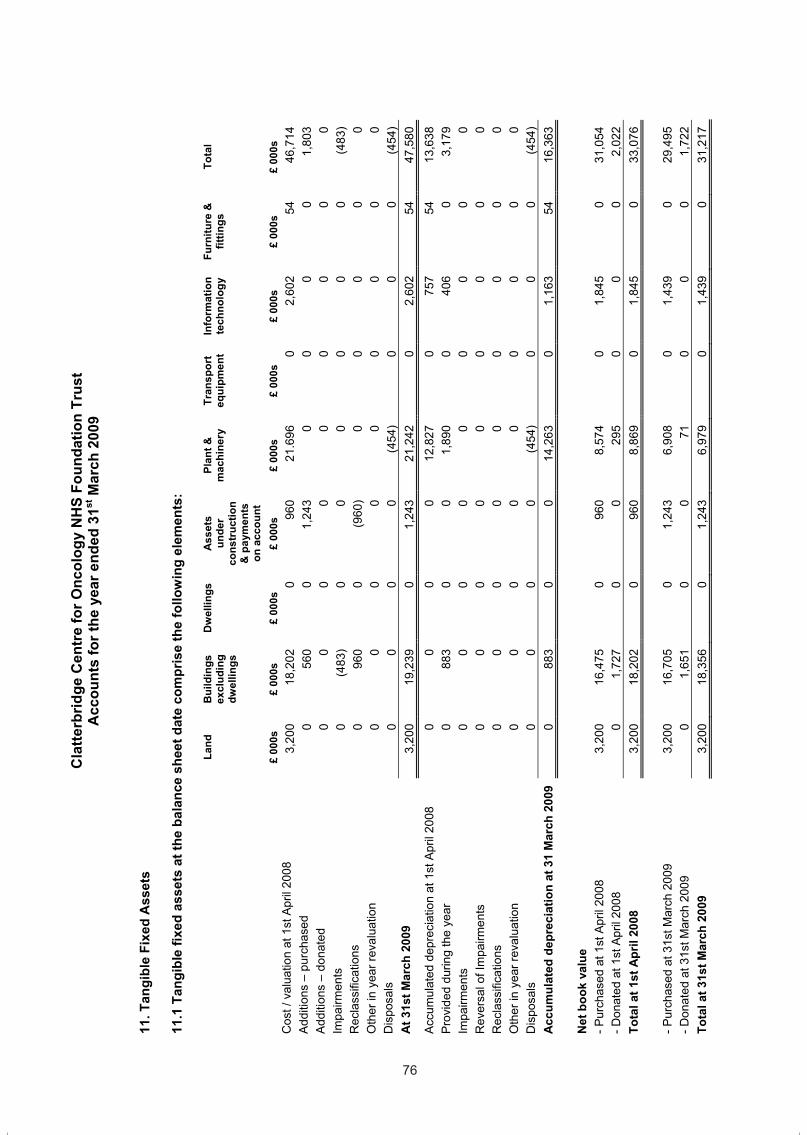
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
76
11. T
angi
ble
Fixe
d A
sset
s
11.1
Tan
gibl
e fix
ed a
sset
s at
the
bala
nce
shee
t dat
e co
mpr
ise
the
follo
win
g el
emen
ts:
Land
B
uild
ings
ex
clud
ing
dwel
lings
Dw
ellin
gs
Ass
ets
unde
rco
nstr
uctio
n &
pay
men
ts
on a
ccou
nt
Plan
t &
mac
hine
ry
Tran
spor
t eq
uipm
ent
Info
rmat
ion
tech
nolo
gy
Furn
iture
&
fittin
gs
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
Cos
t / v
alua
tion
at 1
st A
pril
2008
3,
200
18,2
02
0 96
0 21
.696
0
2,60
2 54
46
,714
A
dditi
ons
– pu
rcha
sed
0
560
0 1,
243
0 0
0 0
1,80
3 A
dditi
ons
– do
nate
d 0
0 0
0 0
0 0
0 0
Impa
irmen
ts
0 (4
83)
0 0
0 0
0 0
(483
) R
ecla
ssifi
catio
ns
0 96
0 0
(960
) 0
0 0
0 0
Oth
er in
yea
r rev
alua
tion
0
0 0
0 0
0 0
0 0
Dis
posa
ls
0 0
0 0
(454
) 0
0 0
(454
) A
t 31s
t Mar
ch 2
009
3,20
0 19
,239
0
1,24
3 21
,242
0
2,60
2 54
47
,580
Acc
umul
ated
dep
reci
atio
n at
1st
Apr
il 20
08
0 0
0 0
12,8
27
0 75
7 54
13
,638
Pr
ovid
ed d
urin
g th
e ye
ar
0 88
3 0
0 1,
890
0 40
6 0
3,17
9 Im
pairm
ents
0
0 0
0 0
0 0
0 0
Rev
ersa
l ofI
mpa
irmen
ts
0 0
0 0
0 0
0 0
0 R
ecla
ssifi
catio
ns
0 0
0 0
0 0
0 0
0 O
ther
inye
arre
valu
atio
n 0
0 0
0 0
0 0
0 0
Dis
posa
ls
0 0
0 0
(454
) 0
0 0
(454
) A
ccum
ulat
ed d
epre
ciat
ion
at 3
1 M
arch
200
9 0
883
0 0
14,2
63
0 1,
163
54
16,3
63
N
et b
ook
valu
e
- P
urch
ased
at 1
st A
pril
2008
3,
200
16,4
75
0 96
0 8,
574
0 1,
845
0 31
,054
- D
onat
ed a
t 1st
Apr
il 20
08
0 1,
727
0 0
295
0 0
0 2,
022
Tota
l at 1
st A
pril
2008
3,
200
18,2
02
0 96
0 8,
869
0 1,
845
0 33
,076
- Pur
chas
ed a
t 31s
t Mar
ch 2
009
3,20
0 16
,705
0
1,24
3 6,
908
0 1,
439
0 29
,495
- D
onat
ed a
t 31s
t Mar
ch 2
009
0 1,
651
0 0
71
0 0
0 1,
722
Tota
l at 3
1st M
arch
200
9 3,
200
18,3
56
0 1,
243
6,97
9 0
1,43
9 0
31,2
17
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
77
All l
and
and
build
ings
are
reva
lued
usi
ng p
rofe
ssio
nal v
alua
tions
in a
ccor
danc
e w
ith F
RS
15
ever
y fiv
e ye
ars.
A
thre
e ye
arly
inte
rim v
alua
tion
was
car
ried
out o
n 30
Sep
tem
ber 2
007,
by th
e V
alua
tion
Offi
ce A
genc
y us
ing
the
Exa
ct R
epla
cem
ent (
NH
S B
eaco
n) B
asis
met
hod
for r
eval
uatio
n.
A va
luat
ion
was
car
ried
out o
n tw
o bu
ildin
g pr
ojec
ts th
at w
ere
com
plet
ed in
yea
r:-
1) R
efur
bish
men
t of
Out
patie
nts
and
2) C
onst
ruct
ion
of R
esea
rch
and
Dev
elop
men
t offi
ces.
Th
is e
valu
atio
n ex
erci
se re
sulte
d in
a b
uild
ing
impa
irmen
t of £
483k
, whi
ch h
as b
een
char
ged
to th
e in
com
e &
expe
nditu
re a
ccou
nt in
200
8/09
.
11.2
Ana
lysi
s of
Tan
gibl
e fix
ed a
sset
s
Land
B
uild
ings
ex
clud
ing
dwel
lings
Dw
ellin
gs
Ass
ets
unde
r co
nstr
uctio
n &
pay
men
ts
on a
ccou
nt
Plan
t &
mac
hine
ry
Tran
spor
t eq
uipm
ent
Info
rmat
ion
tech
nolo
gy
Furn
iture
&
fittin
gs
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
Net
boo
k va
lue
- P
rote
cted
ass
ets
at 3
1st M
arch
200
9 3,
200
18,3
56
0 21
,556
- U
npro
tect
ed a
sset
s at
31s
t Mar
ch 2
009
00
0 1,
243
6,97
9 0
1,43
9 0
9,66
1 To
tal a
t 31s
t Mar
ch 2
009
3,20
0 18
,356
0
1,24
3 6,
979
0 1,
439
0 31
,217
11.3
Of t
he to
tals
at 3
1st M
arch
200
9, £
nil r
elat
ed to
land
val
ued
at o
pen
mar
ket v
alue
and
£ni
l rel
ated
to b
uild
ings
val
ued
at o
pen
mar
ket v
alue
, £ni
l rel
ated
to d
wel
lings
va
lued
at o
pen
mar
ket v
alue
.
11.4
No
asse
ts w
ere
held
und
er fi
nanc
e le
ases
and
hire
pur
chas
e co
ntra
cts
at th
e ba
lanc
e sh
eet d
ate
11.4
/1 N
o de
prec
iatio
n w
as c
harg
ed to
the
inco
me
and
expe
nditu
re in
resp
ect o
f ass
ets
held
und
er fi
nanc
e le
ases
and
hire
pur
chas
e co
ntra
cts
11.5
The
net
boo
k va
lue
of la
nd, b
uild
ings
and
dw
ellin
gs a
t 31s
t Mar
ch 2
009
com
pris
es:
31st
Mar
ch
2009
31
st M
arch
2009
31
st M
arch
20
09
£
000s
£ 00
0s
£ 00
0s
P
rote
cted
U
npro
tect
ed
Fr
eeho
ld
21,4
02
21
,402
0
11
.6 Im
pairm
ent o
f Ass
ets
31st
Mar
ch
2009
31
st M
arch
2008
£
000s
£
000s
C
hang
es in
mar
ket p
rice
483
85
2008
/09
Impa
irmen
t aris
es fr
om th
e D
istri
ct V
alue
r rev
alua
tion
of n
ew b
uild
ing
proj
ects
as
they
bec
ome
oper
atio
nal.
76
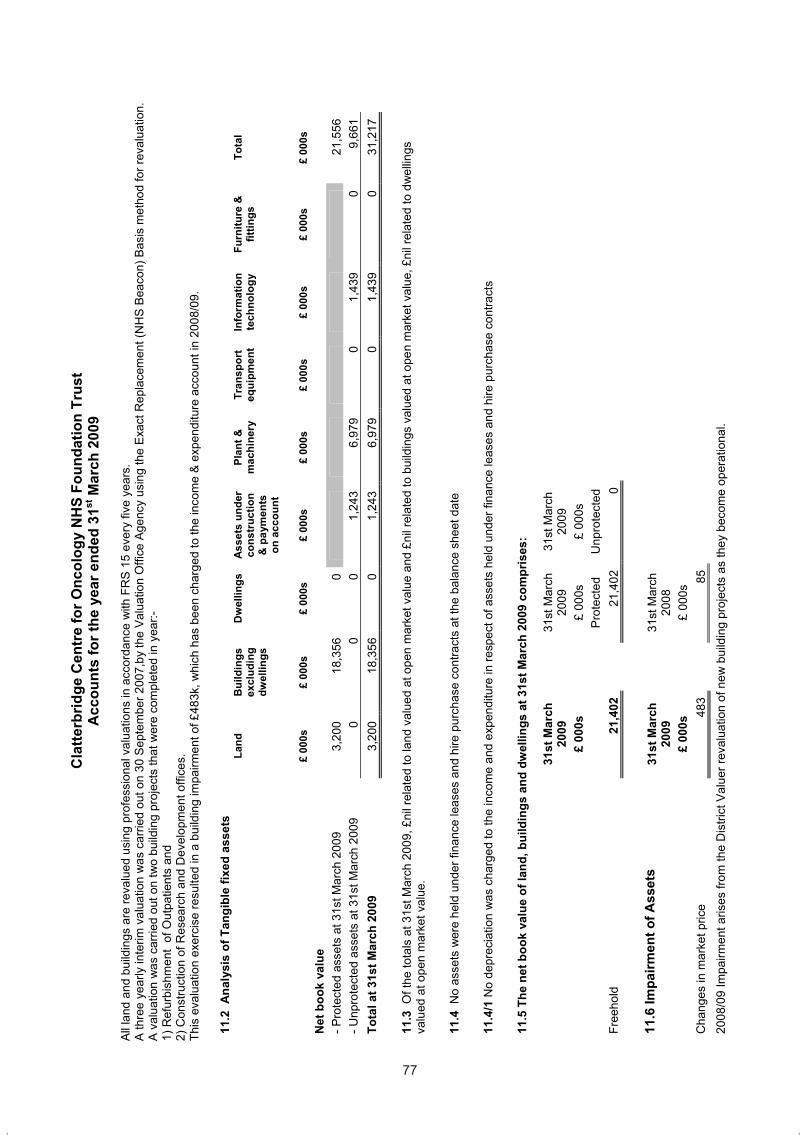
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
76
11. T
angi
ble
Fixe
d A
sset
s
11.1
Tan
gibl
e fix
ed a
sset
s at
the
bala
nce
shee
t dat
e co
mpr
ise
the
follo
win
g el
emen
ts:
Land
B
uild
ings
ex
clud
ing
dwel
lings
Dw
ellin
gs
Ass
ets
unde
rco
nstr
uctio
n &
pay
men
ts
on a
ccou
nt
Plan
t &
mac
hine
ry
Tran
spor
t eq
uipm
ent
Info
rmat
ion
tech
nolo
gy
Furn
iture
&
fittin
gs
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
Cos
t / v
alua
tion
at 1
st A
pril
2008
3,
200
18,2
02
0 96
0 21
.696
0
2,60
2 54
46
,714
A
dditi
ons
– pu
rcha
sed
0
560
0 1,
243
0 0
0 0
1,80
3 A
dditi
ons
– do
nate
d 0
0 0
0 0
0 0
0 0
Impa
irmen
ts
0 (4
83)
0 0
0 0
0 0
(483
) R
ecla
ssifi
catio
ns
0 96
0 0
(960
) 0
0 0
0 0
Oth
er in
yea
r rev
alua
tion
0
0 0
0 0
0 0
0 0
Dis
posa
ls
0 0
0 0
(454
) 0
0 0
(454
) A
t 31s
t Mar
ch 2
009
3,20
0 19
,239
0
1,24
3 21
,242
0
2,60
2 54
47
,580
Acc
umul
ated
dep
reci
atio
n at
1st
Apr
il 20
08
0 0
0 0
12,8
27
0 75
7 54
13
,638
Pr
ovid
ed d
urin
g th
e ye
ar
0 88
3 0
0 1,
890
0 40
6 0
3,17
9 Im
pairm
ents
0
0 0
0 0
0 0
0 0
Rev
ersa
l ofI
mpa
irmen
ts
0 0
0 0
0 0
0 0
0 R
ecla
ssifi
catio
ns
0 0
0 0
0 0
0 0
0 O
ther
inye
arre
valu
atio
n 0
0 0
0 0
0 0
0 0
Dis
posa
ls
0 0
0 0
(454
) 0
0 0
(454
) A
ccum
ulat
ed d
epre
ciat
ion
at 3
1 M
arch
200
9 0
883
0 0
14,2
63
0 1,
163
54
16,3
63
N
et b
ook
valu
e
- P
urch
ased
at 1
st A
pril
2008
3,
200
16,4
75
0 96
0 8,
574
0 1,
845
0 31
,054
- D
onat
ed a
t 1st
Apr
il 20
08
0 1,
727
0 0
295
0 0
0 2,
022
Tota
l at 1
st A
pril
2008
3,
200
18,2
02
0 96
0 8,
869
0 1,
845
0 33
,076
- Pur
chas
ed a
t 31s
t Mar
ch 2
009
3,20
0 16
,705
0
1,24
3 6,
908
0 1,
439
0 29
,495
- D
onat
ed a
t 31s
t Mar
ch 2
009
0 1,
651
0 0
71
0 0
0 1,
722
Tota
l at 3
1st M
arch
200
9 3,
200
18,3
56
0 1,
243
6,97
9 0
1,43
9 0
31,2
17
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
77
All l
and
and
build
ings
are
reva
lued
usi
ng p
rofe
ssio
nal v
alua
tions
in a
ccor
danc
e w
ith F
RS
15
ever
y fiv
e ye
ars.
A
thre
e ye
arly
inte
rim v
alua
tion
was
car
ried
out o
n 30
Sep
tem
ber 2
007,
by th
e V
alua
tion
Offi
ce A
genc
y us
ing
the
Exa
ct R
epla
cem
ent (
NH
S B
eaco
n) B
asis
met
hod
for r
eval
uatio
n.
A va
luat
ion
was
car
ried
out o
n tw
o bu
ildin
g pr
ojec
ts th
at w
ere
com
plet
ed in
yea
r:-
1) R
efur
bish
men
t of
Out
patie
nts
and
2) C
onst
ruct
ion
of R
esea
rch
and
Dev
elop
men
t offi
ces.
Th
is e
valu
atio
n ex
erci
se re
sulte
d in
a b
uild
ing
impa
irmen
t of £
483k
, whi
ch h
as b
een
char
ged
to th
e in
com
e &
expe
nditu
re a
ccou
nt in
200
8/09
.
11.2
Ana
lysi
s of
Tan
gibl
e fix
ed a
sset
s
Land
B
uild
ings
ex
clud
ing
dwel
lings
Dw
ellin
gs
Ass
ets
unde
r co
nstr
uctio
n &
pay
men
ts
on a
ccou
nt
Plan
t &
mac
hine
ry
Tran
spor
t eq
uipm
ent
Info
rmat
ion
tech
nolo
gy
Furn
iture
&
fittin
gs
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
Net
boo
k va
lue
- P
rote
cted
ass
ets
at 3
1st M
arch
200
9 3,
200
18,3
56
0 21
,556
- U
npro
tect
ed a
sset
s at
31s
t Mar
ch 2
009
00
0 1,
243
6,97
9 0
1,43
9 0
9,66
1 To
tal a
t 31s
t Mar
ch 2
009
3,20
0 18
,356
0
1,24
3 6,
979
0 1,
439
0 31
,217
11.3
Of t
he to
tals
at 3
1st M
arch
200
9, £
nil r
elat
ed to
land
val
ued
at o
pen
mar
ket v
alue
and
£ni
l rel
ated
to b
uild
ings
val
ued
at o
pen
mar
ket v
alue
, £ni
l rel
ated
to d
wel
lings
va
lued
at o
pen
mar
ket v
alue
.
11.4
No
asse
ts w
ere
held
und
er fi
nanc
e le
ases
and
hire
pur
chas
e co
ntra
cts
at th
e ba
lanc
e sh
eet d
ate
11.4
/1 N
o de
prec
iatio
n w
as c
harg
ed to
the
inco
me
and
expe
nditu
re in
resp
ect o
f ass
ets
held
und
er fi
nanc
e le
ases
and
hire
pur
chas
e co
ntra
cts
11.5
The
net
boo
k va
lue
of la
nd, b
uild
ings
and
dw
ellin
gs a
t 31s
t Mar
ch 2
009
com
pris
es:
31st
Mar
ch
2009
31
st M
arch
2009
31
st M
arch
20
09
£
000s
£ 00
0s
£ 00
0s
P
rote
cted
U
npro
tect
ed
Fr
eeho
ld
21,4
02
21
,402
0
11
.6 Im
pairm
ent o
f Ass
ets
31st
Mar
ch
2009
31
st M
arch
2008
£
000s
£
000s
C
hang
es in
mar
ket p
rice
483
85
2008
/09
Impa
irmen
t aris
es fr
om th
e D
istri
ct V
alue
r rev
alua
tion
of n
ew b
uild
ing
proj
ects
as
they
bec
ome
oper
atio
nal.
77
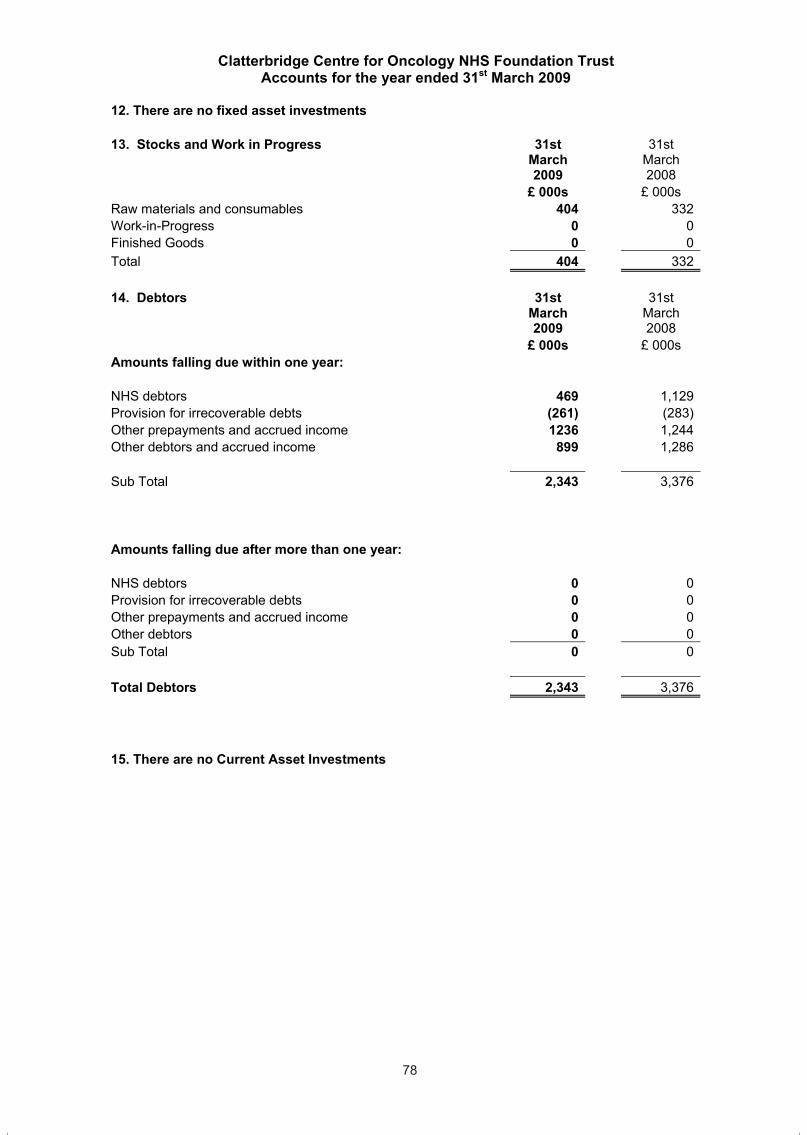
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
78
12. There are no fixed asset investments
13. Stocks and Work in Progress 31stMarch2009
31stMarch2008
£ 000s £ 000s Raw materials and consumables 404 332Work-in-Progress 0 0Finished Goods 0 0Total 404 332
14. Debtors 31stMarch2009
31stMarch2008
£ 000s £ 000s Amounts falling due within one year:
NHS debtors 469 1,129Provision for irrecoverable debts (261) (283)Other prepayments and accrued income 1236 1,244Other debtors and accrued income 899 1,286
Sub Total 2,343 3,376
Amounts falling due after more than one year:
NHS debtors 0 0Provision for irrecoverable debts 0 0Other prepayments and accrued income 0 0Other debtors 0 0Sub Total 0 0
Total Debtors 2,343 3,376
15. There are no Current Asset Investments
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
79
16.1 Creditors 31stMarch2009
31stMarch2008
£ 000s £ 000s
Amounts falling due within one year:
Bank overdrafts 0 0 Payments received on account 463 345 NHS creditors 2,886 2,470 Taxation and Social Security 517 452 Obligations under finance leases and HP contracts 0 0 Capital Creditors 625 2,394 Other creditors and accruals 2,771 1,769 Deferred government grants 397 397 Deferred income 2,208 3,353
Sub Total 9,867 11,180
Amounts falling due after more than one year:
Obligations under finance leases and HP contracts 0 0 NHS creditors 0 0 Other 561 958 Sub Total 561 958
Total Creditors 10,428 12,138
Other Creditors include : -305K outstanding pension contributions at 31st March 2009 (2007/08 £261k)
Accruals and deferred income include: Funding has been received from the Big Lottery Fund to purchase 3 Linear Accelerators and an MRI Scanner. These are deferred assets and funding will be released to the income and expenditure account over the life of the assets on a basis consistent with the depreciation charge for that assets. £397k will be released in less than 12 months and £561k will be released after more than one year.
Loans At 31st March 2009, there are no outstanding loans (2007/08 –nil)
78
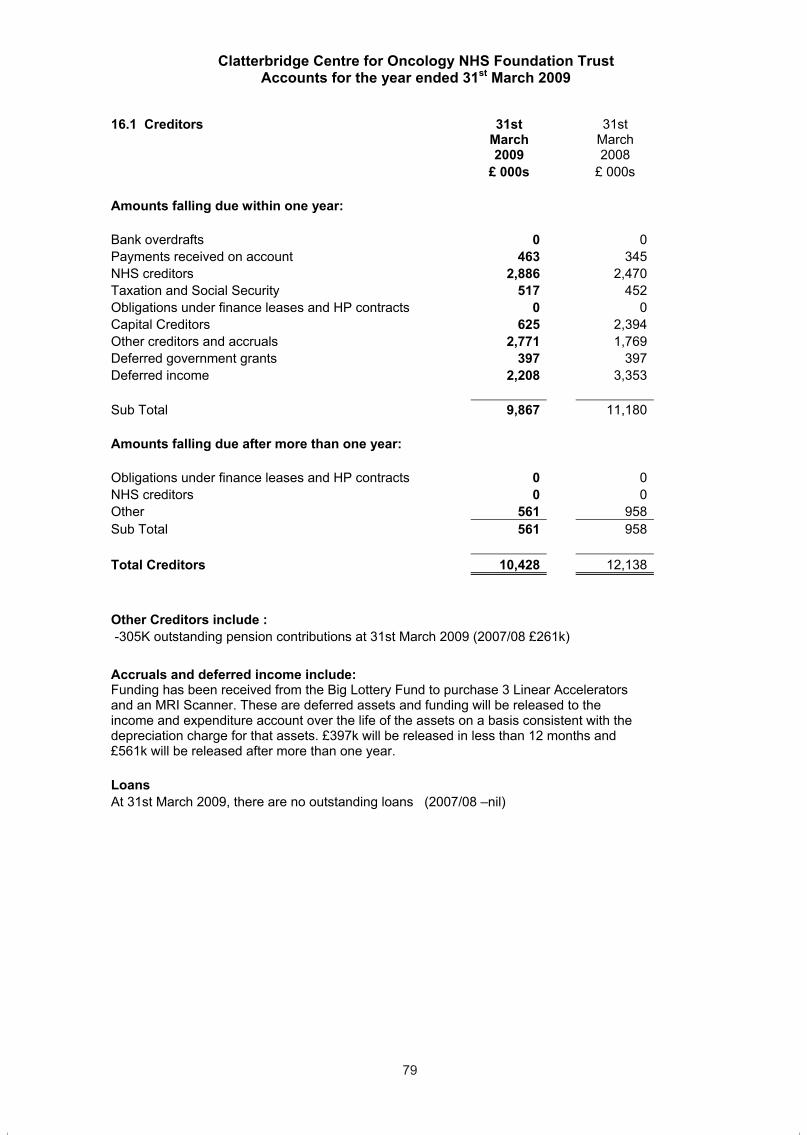
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
78
12. There are no fixed asset investments
13. Stocks and Work in Progress 31stMarch2009
31stMarch2008
£ 000s £ 000s Raw materials and consumables 404 332Work-in-Progress 0 0Finished Goods 0 0Total 404 332
14. Debtors 31stMarch2009
31stMarch2008
£ 000s £ 000s Amounts falling due within one year:
NHS debtors 469 1,129Provision for irrecoverable debts (261) (283)Other prepayments and accrued income 1236 1,244Other debtors and accrued income 899 1,286
Sub Total 2,343 3,376
Amounts falling due after more than one year:
NHS debtors 0 0Provision for irrecoverable debts 0 0Other prepayments and accrued income 0 0Other debtors 0 0Sub Total 0 0
Total Debtors 2,343 3,376
15. There are no Current Asset Investments
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
79
16.1 Creditors 31stMarch2009
31stMarch2008
£ 000s £ 000s
Amounts falling due within one year:
Bank overdrafts 0 0 Payments received on account 463 345 NHS creditors 2,886 2,470 Taxation and Social Security 517 452 Obligations under finance leases and HP contracts 0 0 Capital Creditors 625 2,394 Other creditors and accruals 2,771 1,769 Deferred government grants 397 397 Deferred income 2,208 3,353
Sub Total 9,867 11,180
Amounts falling due after more than one year:
Obligations under finance leases and HP contracts 0 0 NHS creditors 0 0 Other 561 958 Sub Total 561 958
Total Creditors 10,428 12,138
Other Creditors include : -305K outstanding pension contributions at 31st March 2009 (2007/08 £261k)
Accruals and deferred income include: Funding has been received from the Big Lottery Fund to purchase 3 Linear Accelerators and an MRI Scanner. These are deferred assets and funding will be released to the income and expenditure account over the life of the assets on a basis consistent with the depreciation charge for that assets. £397k will be released in less than 12 months and £561k will be released after more than one year.
Loans At 31st March 2009, there are no outstanding loans (2007/08 –nil)
79
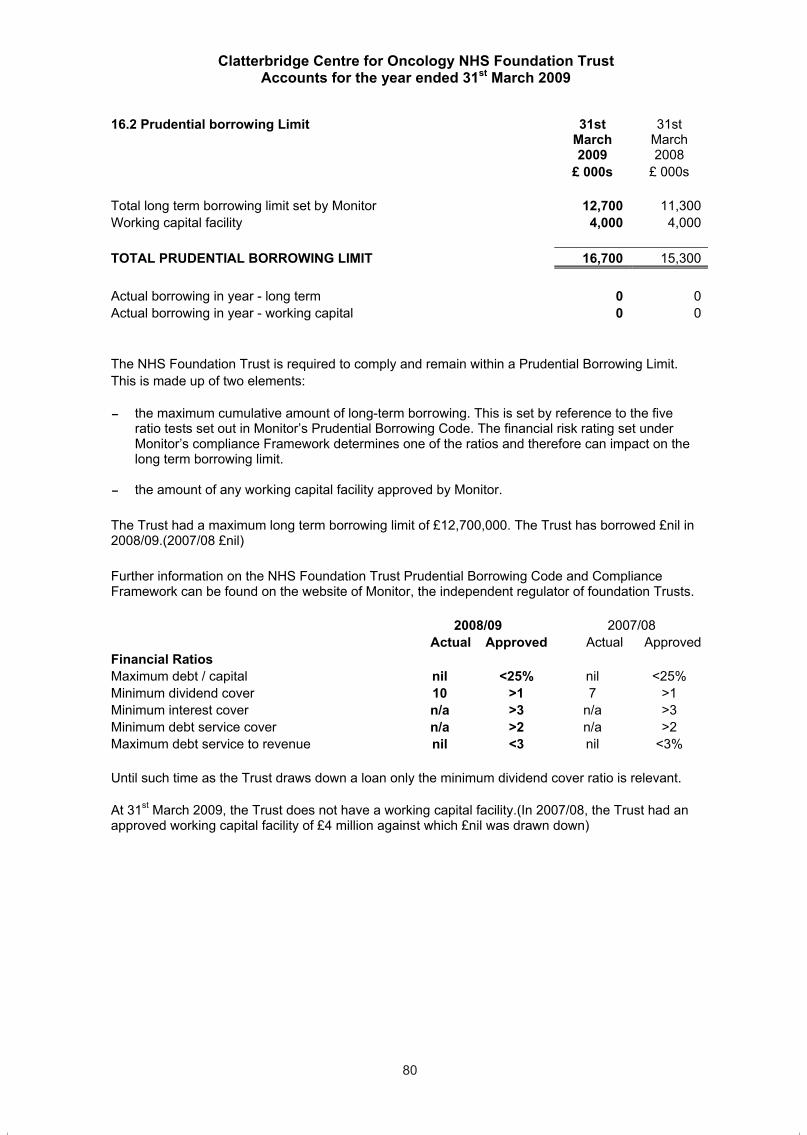
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
80
16.2 Prudential borrowing Limit 31stMarch2009
31stMarch2008
£ 000s £ 000s
Total long term borrowing limit set by Monitor 12,700 11,300Working capital facility 4,000 4,000
TOTAL PRUDENTIAL BORROWING LIMIT 16,700 15,300
Actual borrowing in year - long term 0 0Actual borrowing in year - working capital 0 0
The NHS Foundation Trust is required to comply and remain within a Prudential Borrowing Limit. This is made up of two elements:
- the maximum cumulative amount of long-term borrowing. This is set by reference to the five ratio tests set out in Monitor’s Prudential Borrowing Code. The financial risk rating set under Monitor’s compliance Framework determines one of the ratios and therefore can impact on the long term borrowing limit.
- the amount of any working capital facility approved by Monitor.
The Trust had a maximum long term borrowing limit of £12,700,000. The Trust has borrowed £nil in 2008/09.(2007/08 £nil)
Further information on the NHS Foundation Trust Prudential Borrowing Code and Compliance Framework can be found on the website of Monitor, the independent regulator of foundation Trusts.
2008/09 2007/08 Actual Approved Actual Approved
Financial Ratios Maximum debt / capital nil <25% nil <25% Minimum dividend cover 10 >1 7 >1 Minimum interest cover n/a >3 n/a >3 Minimum debt service cover n/a >2 n/a >2 Maximum debt service to revenue nil <3 nil <3%
Until such time as the Trust draws down a loan only the minimum dividend cover ratio is relevant.
At 31st March 2009, the Trust does not have a working capital facility.(In 2007/08, the Trust had an approved working capital facility of £4 million against which £nil was drawn down)
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
81
17.
Pro
visi
ons
for L
iabi
litie
s an
d C
harg
es
Pen
sion
s re
latin
g to
fo
rmer
dire
ctor
s
Pen
sion
s re
latin
g to
ot
her s
taff
Lega
lcl
aim
s O
ther
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£
000s
At 1
st A
pril
2007
0
011
0
11C
hang
e in
the
disc
ount
rate
0
00
0
0A
risin
g du
ring
the
year
0
02
816
81
8U
tilis
ed d
urin
g th
e ye
ar
00
(11)
0
(11)
Rev
erse
d un
used
0
00
0
0U
nwin
ding
of d
isco
unt
00
00
0
At 3
1st M
arch
200
9 0
02
816
2
Expe
cted
tim
ing
of c
ashf
low
s:
With
in 1
yea
r 0
00
316
31
61
- 5 y
ears
0
02
500
50
2O
ver 5
yea
rs
00
00
0
Tota
l0
02
816
81
8
Oth
er p
rovi
sion
s ar
isin
g du
ring
the
year
repr
esen
ts a
recl
assi
ficat
ion
of in
com
e re
ceiv
ed fo
r jun
ior m
edic
al s
taff
(MA
DE
L).T
his
amou
nt h
as
Acc
rued
ove
r the
pas
t fiv
e ye
ars
and
the
bala
nce
has
prev
ious
ly b
een
carr
ied
in D
efer
red
inco
me
with
in th
e cr
edito
rs s
ectio
n of
the
Bal
ance
She
et
Lega
l cla
ims
cons
ist o
f am
ount
s du
e as
a re
sult
of th
ird p
arty
and
em
ploy
ee li
abilit
y cl
aim
s. T
he v
alue
s ar
e ba
sed
on in
form
atio
n pr
ovid
ed b
y th
e
NH
S L
itiga
tion
Aut
horit
y.
Cla
tterb
ridge
Cen
tre fo
r Onc
olog
y N
HS
Fou
ndat
ion
Trus
t is
a m
embe
r of t
he N
HS
Liti
gatio
n A
utho
rity
(NH
SLA
) clin
ical
neg
ligen
ce s
chem
e. A
ll cl
inic
al
negl
igen
ce c
laim
s ar
e th
eref
ore
reco
gnis
ed in
the
acco
unts
of t
he N
HS
LA, c
onse
quen
tly th
e Tr
ust w
ill h
ave
no p
rovi
sion
for c
linic
al n
eglig
ence
cla
ims.
The
NH
S lit
igat
ion
Aut
horit
y is
car
ryin
g pr
ovis
ions
as
at 3
1st M
arch
200
9 in
rela
tion
to E
LS o
f £ni
l (20
07/0
8 £n
il) a
nd in
rela
tion
to C
NS
T of
£27
0,24
4 (2
007/
08 £
80,3
08)
mak
ing
a to
tal o
f £27
0,24
4
80

Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
80
16.2 Prudential borrowing Limit 31stMarch2009
31stMarch2008
£ 000s £ 000s
Total long term borrowing limit set by Monitor 12,700 11,300Working capital facility 4,000 4,000
TOTAL PRUDENTIAL BORROWING LIMIT 16,700 15,300
Actual borrowing in year - long term 0 0Actual borrowing in year - working capital 0 0
The NHS Foundation Trust is required to comply and remain within a Prudential Borrowing Limit. This is made up of two elements:
- the maximum cumulative amount of long-term borrowing. This is set by reference to the five ratio tests set out in Monitor’s Prudential Borrowing Code. The financial risk rating set under Monitor’s compliance Framework determines one of the ratios and therefore can impact on the long term borrowing limit.
- the amount of any working capital facility approved by Monitor.
The Trust had a maximum long term borrowing limit of £12,700,000. The Trust has borrowed £nil in 2008/09.(2007/08 £nil)
Further information on the NHS Foundation Trust Prudential Borrowing Code and Compliance Framework can be found on the website of Monitor, the independent regulator of foundation Trusts.
2008/09 2007/08 Actual Approved Actual Approved
Financial Ratios Maximum debt / capital nil <25% nil <25% Minimum dividend cover 10 >1 7 >1 Minimum interest cover n/a >3 n/a >3 Minimum debt service cover n/a >2 n/a >2 Maximum debt service to revenue nil <3 nil <3%
Until such time as the Trust draws down a loan only the minimum dividend cover ratio is relevant.
At 31st March 2009, the Trust does not have a working capital facility.(In 2007/08, the Trust had an approved working capital facility of £4 million against which £nil was drawn down)
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
81
17.
Pro
visi
ons
for L
iabi
litie
s an
d C
harg
es
Pen
sion
s re
latin
g to
fo
rmer
dire
ctor
s
Pen
sion
s re
latin
g to
ot
her s
taff
Lega
lcl
aim
s O
ther
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£
000s
At 1
st A
pril
2007
0
011
0
11C
hang
e in
the
disc
ount
rate
0
00
0
0A
risin
g du
ring
the
year
0
02
816
81
8U
tilis
ed d
urin
g th
e ye
ar
00
(11)
0
(11)
Rev
erse
d un
used
0
00
0
0U
nwin
ding
of d
isco
unt
00
00
0
At 3
1st M
arch
200
9 0
02
816
2
Expe
cted
tim
ing
of c
ashf
low
s:
With
in 1
yea
r 0
00
316
31
61
- 5 y
ears
0
02
500
50
2O
ver 5
yea
rs
00
00
0
Tota
l0
02
816
81
8
Oth
er p
rovi
sion
s ar
isin
g du
ring
the
year
repr
esen
ts a
recl
assi
ficat
ion
of in
com
e re
ceiv
ed fo
r jun
ior m
edic
al s
taff
(MA
DE
L).T
his
amou
nt h
as
Acc
rued
ove
r the
pas
t fiv
e ye
ars
and
the
bala
nce
has
prev
ious
ly b
een
carr
ied
in D
efer
red
inco
me
with
in th
e cr
edito
rs s
ectio
n of
the
Bal
ance
She
et
Lega
l cla
ims
cons
ist o
f am
ount
s du
e as
a re
sult
of th
ird p
arty
and
em
ploy
ee li
abilit
y cl
aim
s. T
he v
alue
s ar
e ba
sed
on in
form
atio
n pr
ovid
ed b
y th
e
NH
S L
itiga
tion
Aut
horit
y.
Cla
tterb
ridge
Cen
tre fo
r Onc
olog
y N
HS
Fou
ndat
ion
Trus
t is
a m
embe
r of t
he N
HS
Liti
gatio
n A
utho
rity
(NH
SLA
) clin
ical
neg
ligen
ce s
chem
e. A
ll cl
inic
al
negl
igen
ce c
laim
s ar
e th
eref
ore
reco
gnis
ed in
the
acco
unts
of t
he N
HS
LA, c
onse
quen
tly th
e Tr
ust w
ill h
ave
no p
rovi
sion
for c
linic
al n
eglig
ence
cla
ims.
The
NH
S lit
igat
ion
Aut
horit
y is
car
ryin
g pr
ovis
ions
as
at 3
1st M
arch
200
9 in
rela
tion
to E
LS o
f £ni
l (20
07/0
8 £n
il) a
nd in
rela
tion
to C
NS
T of
£27
0,24
4 (2
007/
08 £
80,3
08)
mak
ing
a to
tal o
f £27
0,24
4
81
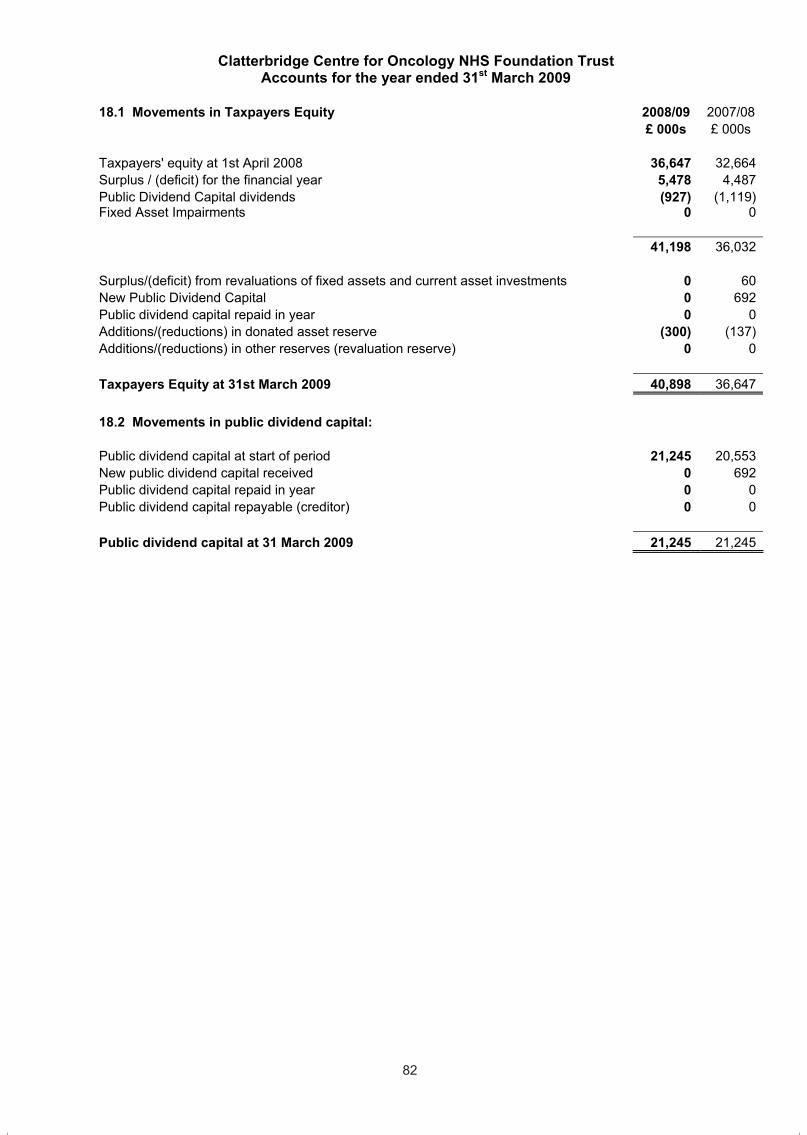
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
82
18.1 Movements in Taxpayers Equity 2008/09 2007/08 £ 000s £ 000s
Taxpayers' equity at 1st April 2008 36,647 32,664Surplus / (deficit) for the financial year 5,478 4,487Public Dividend Capital dividends (927) (1,119)Fixed Asset Impairments 0 0
41,198 36,032
Surplus/(deficit) from revaluations of fixed assets and current asset investments 0 60New Public Dividend Capital 0 692Public dividend capital repaid in year 0 0Additions/(reductions) in donated asset reserve (300) (137)Additions/(reductions) in other reserves (revaluation reserve) 0 0
Taxpayers Equity at 31st March 2009 40,898 36,647
18.2 Movements in public dividend capital:
Public dividend capital at start of period 21,245 20,553New public dividend capital received 0 692Public dividend capital repaid in year 0 0Public dividend capital repayable (creditor) 0 0
Public dividend capital at 31 March 2009 21,245 21,245
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
83
18.3
Mov
emen
ts o
n R
eser
ves
Rev
alua
tion
rese
rve
Don
ated
as
set
rese
rve
Ava
ilabl
efo
r sal
e in
vest
men
ts
Oth
erre
serv
esIn
com
e an
d ex
pend
iture
re
serv
e
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£
000s
At 1
st A
pril
2008
5,
804
2,02
10
07,
577
15
,402
Tran
sfer
from
the
inco
me
and
expe
nditu
re a
ccou
nt
00
00
4,55
1
4,55
1
Fixe
d A
sset
Impa
irmen
ts
00
00
0
0
Sur
plus
on
othe
r rev
alua
tions
/ in
dexa
tion
of fi
xed
asse
ts0
00
00
0
Tran
sfer
of r
ealis
ed p
rofit
s / (
loss
es) t
o th
e in
com
e an
dex
pend
iture
rese
rve
00
00
0
0
Rec
eipt
of d
onat
ed a
sset
s 0
00
00
0
Tran
sfer
s to
the
inco
me
and
expe
nditu
re a
ccou
nt fo
r de
prec
iatio
n, im
pairm
ent a
nd d
ispo
sal o
f don
ated
as
sets
0
(300
)0
00
(3
00)
Oth
er tr
ansf
ers
betw
een
rese
rves
(3
01)
00
030
1
0
Mov
emen
ts o
n ot
her r
eser
ves
00
00
0
0
At 3
1st M
arch
200
9 5,
503
1,72
10
012
,429
19
,653
82
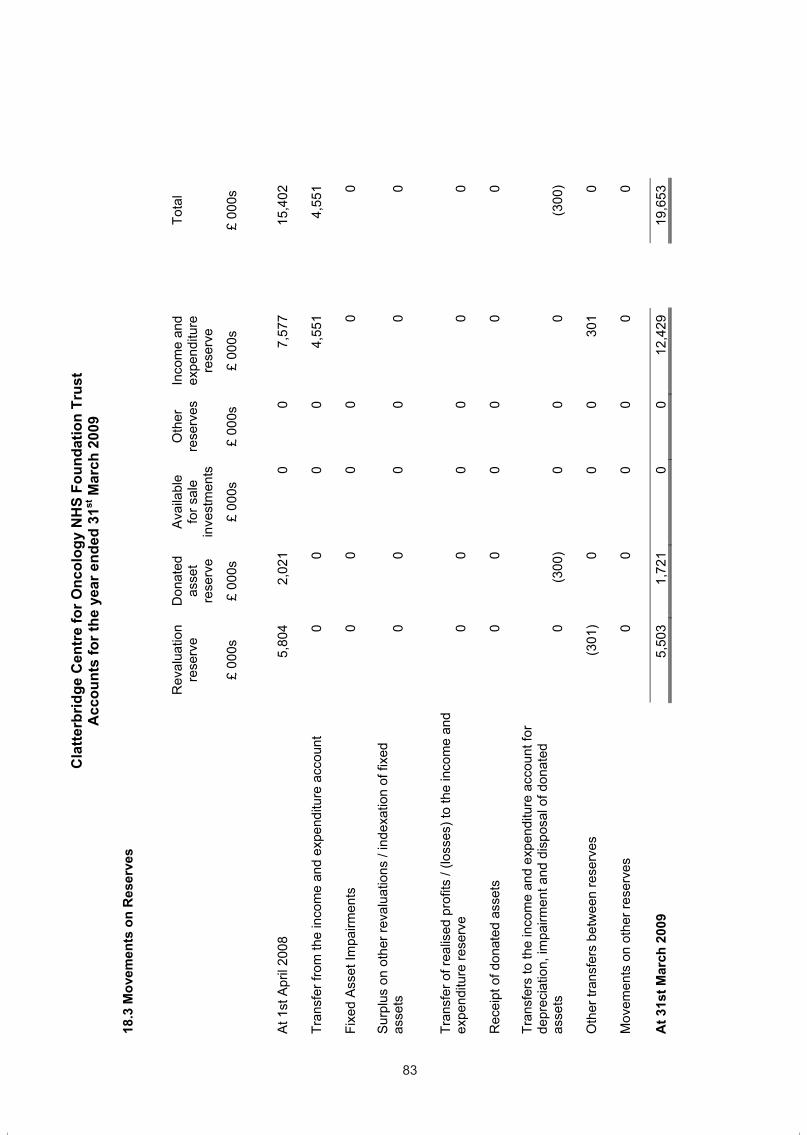
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
82
18.1 Movements in Taxpayers Equity 2008/09 2007/08 £ 000s £ 000s
Taxpayers' equity at 1st April 2008 36,647 32,664Surplus / (deficit) for the financial year 5,478 4,487Public Dividend Capital dividends (927) (1,119)Fixed Asset Impairments 0 0
41,198 36,032
Surplus/(deficit) from revaluations of fixed assets and current asset investments 0 60New Public Dividend Capital 0 692Public dividend capital repaid in year 0 0Additions/(reductions) in donated asset reserve (300) (137)Additions/(reductions) in other reserves (revaluation reserve) 0 0
Taxpayers Equity at 31st March 2009 40,898 36,647
18.2 Movements in public dividend capital:
Public dividend capital at start of period 21,245 20,553New public dividend capital received 0 692Public dividend capital repaid in year 0 0Public dividend capital repayable (creditor) 0 0
Public dividend capital at 31 March 2009 21,245 21,245
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
83
18.3
Mov
emen
ts o
n R
eser
ves
Rev
alua
tion
rese
rve
Don
ated
as
set
rese
rve
Ava
ilabl
efo
r sal
e in
vest
men
ts
Oth
erre
serv
esIn
com
e an
d ex
pend
iture
re
serv
e
Tota
l
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£ 00
0s
£
000s
At 1
st A
pril
2008
5,
804
2,02
10
07,
577
15
,402
Tran
sfer
from
the
inco
me
and
expe
nditu
re a
ccou
nt
00
00
4,55
1
4,55
1
Fixe
d A
sset
Impa
irmen
ts
00
00
0
0
Sur
plus
on
othe
r rev
alua
tions
/ in
dexa
tion
of fi
xed
asse
ts0
00
00
0
Tran
sfer
of r
ealis
ed p
rofit
s / (
loss
es) t
o th
e in
com
e an
dex
pend
iture
rese
rve
00
00
0
0
Rec
eipt
of d
onat
ed a
sset
s 0
00
00
0
Tran
sfer
s to
the
inco
me
and
expe
nditu
re a
ccou
nt fo
r de
prec
iatio
n, im
pairm
ent a
nd d
ispo
sal o
f don
ated
as
sets
0
(300
)0
00
(3
00)
Oth
er tr
ansf
ers
betw
een
rese
rves
(3
01)
00
030
1
0
Mov
emen
ts o
n ot
her r
eser
ves
00
00
0
0
At 3
1st M
arch
200
9 5,
503
1,72
10
012
,429
19
,653
83
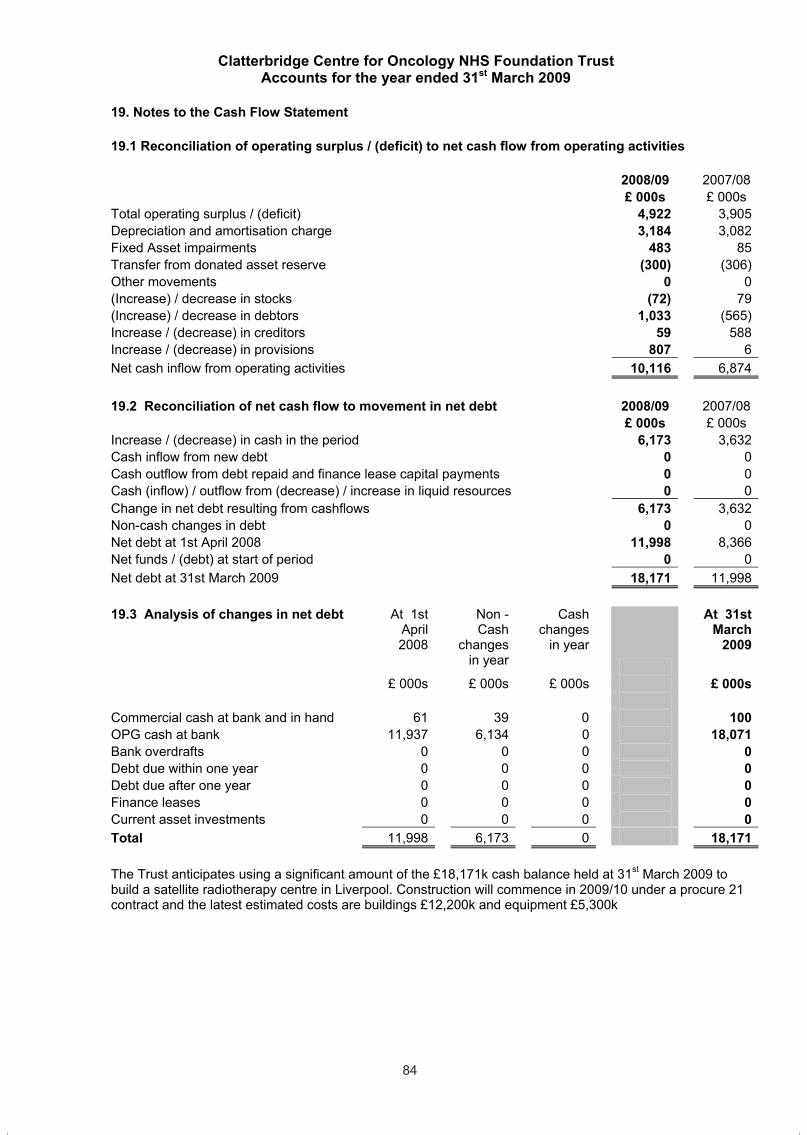
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
84
19. Notes to the Cash Flow Statement 19.1 Reconciliation of operating surplus / (deficit) to net cash flow from operating activities
2008/09 2007/08 £ 000s £ 000s
Total operating surplus / (deficit) 4,922 3,905Depreciation and amortisation charge 3,184 3,082Fixed Asset impairments 483 85Transfer from donated asset reserve (300) (306)Other movements 0 0(Increase) / decrease in stocks (72) 79(Increase) / decrease in debtors 1,033 (565)Increase / (decrease) in creditors 59 588Increase / (decrease) in provisions 807 6Net cash inflow from operating activities 10,116 6,874
19.2 Reconciliation of net cash flow to movement in net debt 2008/09 2007/08
£ 000s £ 000s Increase / (decrease) in cash in the period 6,173 3,632Cash inflow from new debt 0 0Cash outflow from debt repaid and finance lease capital payments 0 0Cash (inflow) / outflow from (decrease) / increase in liquid resources 0 0Change in net debt resulting from cashflows 6,173 3,632Non-cash changes in debt 0 0Net debt at 1st April 2008 11,998 8,366Net funds / (debt) at start of period 0 0Net debt at 31st March 2009 18,171 11,998
19.3 Analysis of changes in net debt At 1st
April2008
Non -Cash
changes in year
Cash changes
in year
At 31st March
2009
£ 000s £ 000s £ 000s £ 000s
Commercial cash at bank and in hand 61 39 0 100OPG cash at bank 11,937 6,134 0 18,071Bank overdrafts 0 0 0 0Debt due within one year 0 0 0 0Debt due after one year 0 0 0 0Finance leases 0 0 0 0Current asset investments 0 0 0 0Total 11,998 6,173 0 18,171
The Trust anticipates using a significant amount of the £18,171k cash balance held at 31st March 2009 to build a satellite radiotherapy centre in Liverpool. Construction will commence in 2009/10 under a procure 21 contract and the latest estimated costs are buildings £12,200k and equipment £5,300k
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
85
20. Contractual Capital Commitments
Commitments under capital expenditure contracts at the balance sheet date were £1,098k, (2007/08 £263k) which relate to building contracts entered into during 2008/09 which are due to be completed in 2009/10.
21. Post Balance Sheet Events
There are no post balance sheet events.
22. Contingent Assets and Liabilities
There are no contingent assets or liabilities at 31st March 2009 (2007/08 £Nil).
23.1 Related Party Transactions
Clatterbridge Centre for Oncology NHS Foundation Trust is a public interest body authorised by Monitor, the Independent Regulator for NHS Foundation Trusts.
During the year none of the Board Members or members of the key management staff, or parties related to them, has undertaken any material transactions with Clatterbridge Centre for Oncology NHS Foundation Trust.
The Register of Interests for the Council of Governors for 2008/09 has been compiled in accordance with the requirements of the Constitution of Clatterbridge Centre for Oncology NHS Foundation Trust.
The Department of Health is regarded as a related party. During the year Clatterbridge Centre for Oncology NHS Foundation Trust has had a number of material transactions with the Department, and with other entities for which the Department is regarded as the parent Department.
In addition, the Trust has had a number of material transactions with other Government Departments and other central and local Government bodies. Most of these transactions have been with HM Revenue & Customs, Health Commission Wales (on behalf of the Welsh Assembly) and National Service Division (on behalf of the Scottish Assembly).
The Trust has also received revenue payments from the Trusts charitable funds, all of the Trustees for which are also members of the NHS Trust Board.
The Trust has also had a number of material transactions with the Clatterbridge Cancer Research (CCR), which is a recognised charity supporting Cancer research.
The following related party transactions are in excess of 1% of turnover.
84
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
84
19. Notes to the Cash Flow Statement 19.1 Reconciliation of operating surplus / (deficit) to net cash flow from operating activities
2008/09 2007/08 £ 000s £ 000s
Total operating surplus / (deficit) 4,922 3,905Depreciation and amortisation charge 3,184 3,082Fixed Asset impairments 483 85Transfer from donated asset reserve (300) (306)Other movements 0 0(Increase) / decrease in stocks (72) 79(Increase) / decrease in debtors 1,033 (565)Increase / (decrease) in creditors 59 588Increase / (decrease) in provisions 807 6Net cash inflow from operating activities 10,116 6,874
19.2 Reconciliation of net cash flow to movement in net debt 2008/09 2007/08
£ 000s £ 000s Increase / (decrease) in cash in the period 6,173 3,632Cash inflow from new debt 0 0Cash outflow from debt repaid and finance lease capital payments 0 0Cash (inflow) / outflow from (decrease) / increase in liquid resources 0 0Change in net debt resulting from cashflows 6,173 3,632Non-cash changes in debt 0 0Net debt at 1st April 2008 11,998 8,366Net funds / (debt) at start of period 0 0Net debt at 31st March 2009 18,171 11,998
19.3 Analysis of changes in net debt At 1st
April2008
Non -Cash
changes in year
Cash changes
in year
At 31st March
2009
£ 000s £ 000s £ 000s £ 000s
Commercial cash at bank and in hand 61 39 0 100OPG cash at bank 11,937 6,134 0 18,071Bank overdrafts 0 0 0 0Debt due within one year 0 0 0 0Debt due after one year 0 0 0 0Finance leases 0 0 0 0Current asset investments 0 0 0 0Total 11,998 6,173 0 18,171
The Trust anticipates using a significant amount of the £18,171k cash balance held at 31st March 2009 to build a satellite radiotherapy centre in Liverpool. Construction will commence in 2009/10 under a procure 21 contract and the latest estimated costs are buildings £12,200k and equipment £5,300k
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
85
20. Contractual Capital Commitments
Commitments under capital expenditure contracts at the balance sheet date were £1,098k, (2007/08 £263k) which relate to building contracts entered into during 2008/09 which are due to be completed in 2009/10.
21. Post Balance Sheet Events
There are no post balance sheet events.
22. Contingent Assets and Liabilities
There are no contingent assets or liabilities at 31st March 2009 (2007/08 £Nil).
23.1 Related Party Transactions
Clatterbridge Centre for Oncology NHS Foundation Trust is a public interest body authorised by Monitor, the Independent Regulator for NHS Foundation Trusts.
During the year none of the Board Members or members of the key management staff, or parties related to them, has undertaken any material transactions with Clatterbridge Centre for Oncology NHS Foundation Trust.
The Register of Interests for the Council of Governors for 2008/09 has been compiled in accordance with the requirements of the Constitution of Clatterbridge Centre for Oncology NHS Foundation Trust.
The Department of Health is regarded as a related party. During the year Clatterbridge Centre for Oncology NHS Foundation Trust has had a number of material transactions with the Department, and with other entities for which the Department is regarded as the parent Department.
In addition, the Trust has had a number of material transactions with other Government Departments and other central and local Government bodies. Most of these transactions have been with HM Revenue & Customs, Health Commission Wales (on behalf of the Welsh Assembly) and National Service Division (on behalf of the Scottish Assembly).
The Trust has also received revenue payments from the Trusts charitable funds, all of the Trustees for which are also members of the NHS Trust Board.
The Trust has also had a number of material transactions with the Clatterbridge Cancer Research (CCR), which is a recognised charity supporting Cancer research.
The following related party transactions are in excess of 1% of turnover.
85
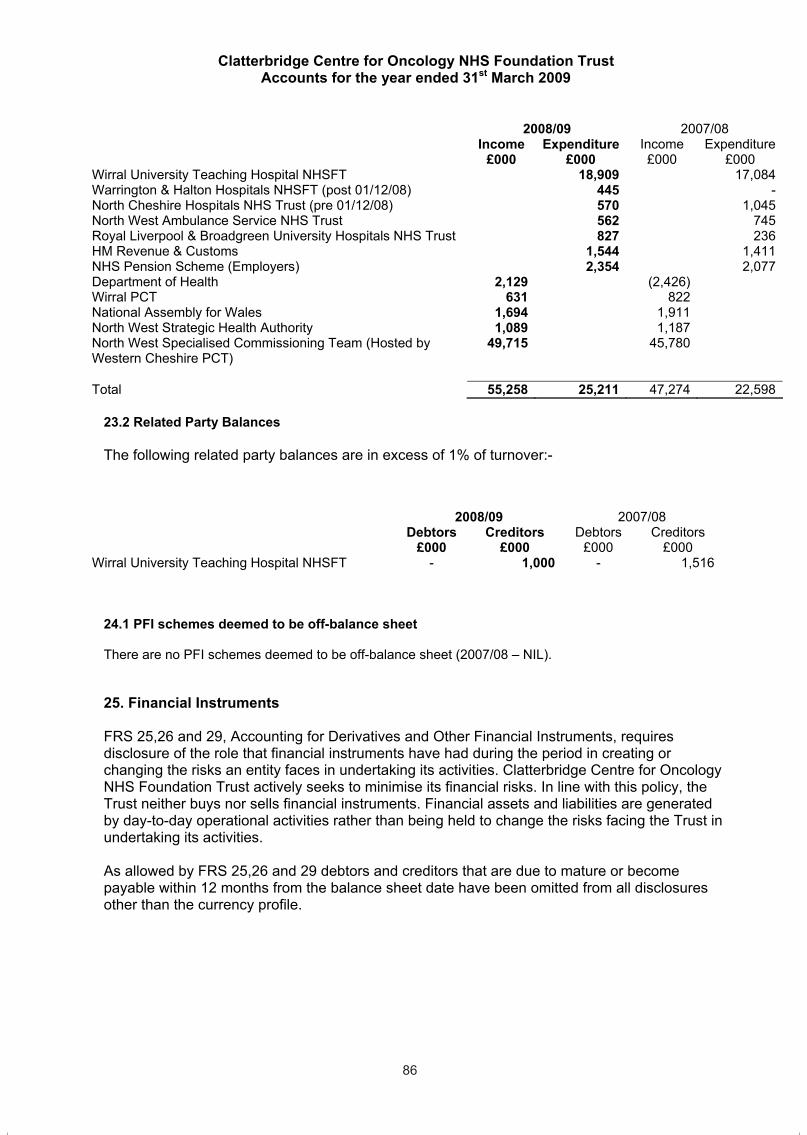
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
86
2008/09 2007/08 Income Expenditure Income Expenditure
£000 £000 £000 £000 Wirral University Teaching Hospital NHSFT 18,909 17,084Warrington & Halton Hospitals NHSFT (post 01/12/08) 445 -North Cheshire Hospitals NHS Trust (pre 01/12/08) 570 1,045North West Ambulance Service NHS Trust 562 745Royal Liverpool & Broadgreen University Hospitals NHS Trust 827 236HM Revenue & Customs 1,544 1,411NHS Pension Scheme (Employers) 2,354 2,077Department of Health 2,129 (2,426)Wirral PCT 631 822National Assembly for Wales 1,694 1,911North West Strategic Health Authority 1,089 1,187North West Specialised Commissioning Team (Hosted by Western Cheshire PCT)
49,715 45,780
Total 55,258 25,211 47,274 22,598
23.2 Related Party Balances
The following related party balances are in excess of 1% of turnover:-
2008/09 2007/08 Debtors Creditors Debtors Creditors
£000 £000 £000 £000 Wirral University Teaching Hospital NHSFT - 1,000 - 1,516
24.1 PFI schemes deemed to be off-balance sheet
There are no PFI schemes deemed to be off-balance sheet (2007/08 – NIL).
25. Financial Instruments
FRS 25,26 and 29, Accounting for Derivatives and Other Financial Instruments, requires disclosure of the role that financial instruments have had during the period in creating or changing the risks an entity faces in undertaking its activities. Clatterbridge Centre for Oncology NHS Foundation Trust actively seeks to minimise its financial risks. In line with this policy, the Trust neither buys nor sells financial instruments. Financial assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks facing the Trust in undertaking its activities.
As allowed by FRS 25,26 and 29 debtors and creditors that are due to mature or become payable within 12 months from the balance sheet date have been omitted from all disclosures other than the currency profile.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
87
Liquidity risk
The Trust's income is negotiated under three year agency purchase contracts with local Primary Care Trusts, which are financed from resources voted annually by Parliament. The Trust receives such contract income in accordance with Payment by Results (PBR), which is intended to match the income received in year to the activity delivered in that year by reference to a National / Local Tariff unit cost. The Trust receives cash each month based on an annually agreed level of contract activity and there are periodic corrections made to adjust for the actual income due under the contract. The Trust’s activity hasremained ahead of plan during 2008/09 which has contributed to an increase in cash holdings such that the working capital facility which expired on 31st July 2008 has not needed to be renewed.
The Trust presently finances its capital expenditure from internally generated funds. In addition, the Trust can borrow, both from the Department of Health Financing Facility and commercially to finance capital schemes. Financing is drawn down to match the spend profile of the scheme concerned and the Trust is not, therefore, exposed to significant liquidity risks in this area.
Interest rate risk
The only asset or liability subject to fluctuation of interest rates are cash holdings at the OPG and a UK high street bank. Clatterbridge Centre for Oncology NHS Trust is not, therefore, exposed to significant interest-rate risk. Note 25.1 and note 25.2 show the interest rate profiles of the Trust's financial assets and liabilities.
Foreign currency risk
The Trust has negligible foreign currency income, expenditure, assets or liabilities.
Credit Risk
The Trust has considered credit risk under FRS29, and concluded that this note is not applicable to the Trust.
86
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
86
2008/09 2007/08 Income Expenditure Income Expenditure
£000 £000 £000 £000 Wirral University Teaching Hospital NHSFT 18,909 17,084Warrington & Halton Hospitals NHSFT (post 01/12/08) 445 -North Cheshire Hospitals NHS Trust (pre 01/12/08) 570 1,045North West Ambulance Service NHS Trust 562 745Royal Liverpool & Broadgreen University Hospitals NHS Trust 827 236HM Revenue & Customs 1,544 1,411NHS Pension Scheme (Employers) 2,354 2,077Department of Health 2,129 (2,426)Wirral PCT 631 822National Assembly for Wales 1,694 1,911North West Strategic Health Authority 1,089 1,187North West Specialised Commissioning Team (Hosted by Western Cheshire PCT)
49,715 45,780
Total 55,258 25,211 47,274 22,598
23.2 Related Party Balances
The following related party balances are in excess of 1% of turnover:-
2008/09 2007/08 Debtors Creditors Debtors Creditors
£000 £000 £000 £000 Wirral University Teaching Hospital NHSFT - 1,000 - 1,516
24.1 PFI schemes deemed to be off-balance sheet
There are no PFI schemes deemed to be off-balance sheet (2007/08 – NIL).
25. Financial Instruments
FRS 25,26 and 29, Accounting for Derivatives and Other Financial Instruments, requires disclosure of the role that financial instruments have had during the period in creating or changing the risks an entity faces in undertaking its activities. Clatterbridge Centre for Oncology NHS Foundation Trust actively seeks to minimise its financial risks. In line with this policy, the Trust neither buys nor sells financial instruments. Financial assets and liabilities are generated by day-to-day operational activities rather than being held to change the risks facing the Trust in undertaking its activities.
As allowed by FRS 25,26 and 29 debtors and creditors that are due to mature or become payable within 12 months from the balance sheet date have been omitted from all disclosures other than the currency profile.
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
87
Liquidity risk
The Trust's income is negotiated under three year agency purchase contracts with local Primary Care Trusts, which are financed from resources voted annually by Parliament. The Trust receives such contract income in accordance with Payment by Results (PBR), which is intended to match the income received in year to the activity delivered in that year by reference to a National / Local Tariff unit cost. The Trust receives cash each month based on an annually agreed level of contract activity and there are periodic corrections made to adjust for the actual income due under the contract. The Trust’s activity hasremained ahead of plan during 2008/09 which has contributed to an increase in cash holdings such that the working capital facility which expired on 31st July 2008 has not needed to be renewed.
The Trust presently finances its capital expenditure from internally generated funds. In addition, the Trust can borrow, both from the Department of Health Financing Facility and commercially to finance capital schemes. Financing is drawn down to match the spend profile of the scheme concerned and the Trust is not, therefore, exposed to significant liquidity risks in this area.
Interest rate risk
The only asset or liability subject to fluctuation of interest rates are cash holdings at the OPG and a UK high street bank. Clatterbridge Centre for Oncology NHS Trust is not, therefore, exposed to significant interest-rate risk. Note 25.1 and note 25.2 show the interest rate profiles of the Trust's financial assets and liabilities.
Foreign currency risk
The Trust has negligible foreign currency income, expenditure, assets or liabilities.
Credit Risk
The Trust has considered credit risk under FRS29, and concluded that this note is not applicable to the Trust.
87
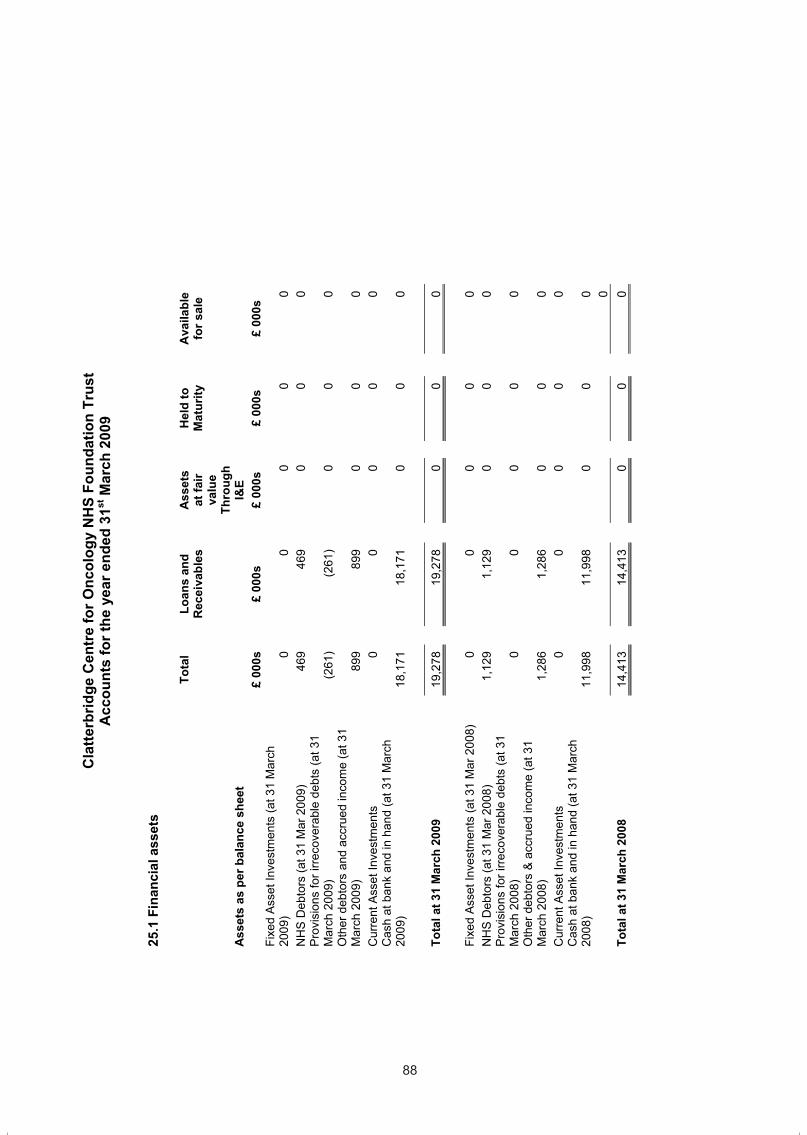
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
88
25.1
Fin
anci
al a
sset
s
Ass
ets
as p
er b
alan
ce s
heet
Tota
l
Loan
s an
d R
ecei
vabl
es
A
sset
s at
fair
valu
e Th
roug
h I&
E
H
eld
to
Mat
urity
Ava
ilabl
e fo
r sal
e
£ 00
0s
£
000s
£
000s
£
000s
£
000s
Fi
xed
Ass
et In
vest
men
ts (a
t 31
Mar
ch
2009
)
0
0
0
0
0
NH
S D
ebto
rs (a
t 31
Mar
200
9)
46
9
469
0
0
0
Pro
visi
ons
for i
rreco
vera
ble
debt
s (a
t 31
Mar
ch 2
009)
(261
)
(261
)
0
0
0 O
ther
deb
tors
and
acc
rued
inco
me
(at 3
1 M
arch
200
9)
89
9
899
0
0
0
Cur
rent
Ass
et In
vest
men
ts
0
0
0
0
0
Cas
h at
ban
k an
d in
han
d (a
t 31
Mar
ch
2009
)
18,1
71
18
,171
0
0
0
Tota
l at 3
1 M
arch
200
9
19,2
78
19
,278
0
0
0
Fixe
d A
sset
Inve
stm
ents
(at 3
1 M
ar 2
008)
0
0
0
0
0N
HS
Deb
tors
(at 3
1 M
ar 2
008)
1,12
9
1,12
9
0
0
0P
rovi
sion
s fo
r irre
cove
rabl
e de
bts
(at 3
1 M
arch
200
8)
0
0
0
0
0
Oth
er d
ebto
rs &
acc
rued
inco
me
(at 3
1 M
arch
200
8)
1,
286
1,
286
0
0
0
Cur
rent
Ass
et In
vest
men
ts
0
0
0
0
0
Cas
h at
ban
k an
d in
han
d (a
t 31
Mar
ch
2008
)
11,9
98
11
,998
0
0
0
0 To
tal a
t 31
Mar
ch 2
008
14,4
13
14
,413
0
0
0
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
89
25.2
Fin
anci
al L
iabi
litie
s
Liab
ilitie
s as
per
bal
ance
she
et
Tota
l
Loan
s an
d R
ecei
vabl
es
A
sset
s at
fair
valu
e Th
roug
h I&
E
H
eld
to
Mat
urity
Ava
ilabl
e fo
r sal
e
£ 00
0s
£
000s
£
000s
£
000s
£
000s
B
ank
Ove
rdra
fts (a
t 31
Mar
200
9)
0
0
0
0
0Lo
ans
(at 3
1 M
ar 2
009)
0
0
0
0
0N
HS
cre
dito
rs (a
t 31
Mar
ch 2
009)
1,80
1
1,80
1
0
0
0O
ther
cre
dito
rs (a
t 31
Mar
ch 2
009)
2,77
1
2,77
1
0
0
0C
apita
l cre
dito
rs (a
t 31
Mar
ch 2
009)
625
62
5
0
0
0Fi
nanc
e le
ase
oblig
atio
ns (a
t 31
Mar
ch
2009
)
0
0
0
0
0 P
rovi
sion
s un
der c
ontra
ct (a
t 31
Mar
ch
2009
)
818
81
8
0
0
0
Tota
l at 3
1 M
arch
200
9
6,01
5
6,01
5
0
0
0
Ban
k O
verd
rafts
(at 3
1 M
ar 2
008)
0
0
0
0
0Lo
ans
(at 3
1 M
ar 2
008)
0
0
0
0
0N
HS
cre
dito
rs (a
t 31
Mar
ch 2
008)
2,47
0
2,47
0
0
0
0O
ther
cre
dito
rs (a
t 31
Mar
ch 2
008)
0
0
0
0
0C
apita
l cre
dito
rs (a
t 31
Mar
ch 2
008)
0
0
0
0
0Fi
nanc
e le
ase
oblig
atio
ns (a
t 31
Mar
ch
2008
)
0
0
0
0
0 P
rovi
sion
s un
der c
ontra
ct (a
t 31
Mar
ch
2008
)
11
11
0
Tota
l at 3
1 M
arch
200
8
2,
481
2,
481
0
0
0
88
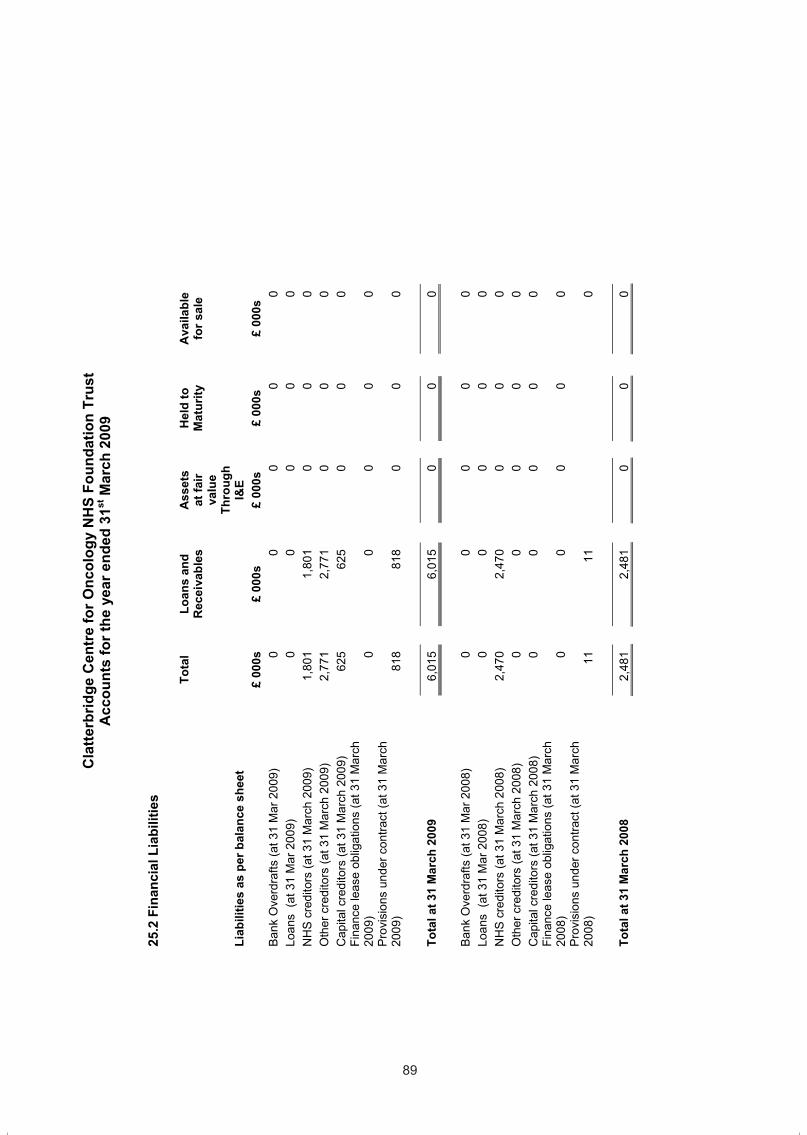
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
88
25.1
Fin
anci
al a
sset
s
Ass
ets
as p
er b
alan
ce s
heet
Tota
l
Loan
s an
d R
ecei
vabl
es
A
sset
s at
fair
valu
e Th
roug
h I&
E
H
eld
to
Mat
urity
Ava
ilabl
e fo
r sal
e
£ 00
0s
£
000s
£
000s
£
000s
£
000s
Fi
xed
Ass
et In
vest
men
ts (a
t 31
Mar
ch
2009
)
0
0
0
0
0
NH
S D
ebto
rs (a
t 31
Mar
200
9)
46
9
469
0
0
0
Pro
visi
ons
for i
rreco
vera
ble
debt
s (a
t 31
Mar
ch 2
009)
(261
)
(261
)
0
0
0 O
ther
deb
tors
and
acc
rued
inco
me
(at 3
1 M
arch
200
9)
89
9
899
0
0
0
Cur
rent
Ass
et In
vest
men
ts
0
0
0
0
0
Cas
h at
ban
k an
d in
han
d (a
t 31
Mar
ch
2009
)
18,1
71
18
,171
0
0
0
Tota
l at 3
1 M
arch
200
9
19,2
78
19
,278
0
0
0
Fixe
d A
sset
Inve
stm
ents
(at 3
1 M
ar 2
008)
0
0
0
0
0N
HS
Deb
tors
(at 3
1 M
ar 2
008)
1,12
9
1,12
9
0
0
0P
rovi
sion
s fo
r irre
cove
rabl
e de
bts
(at 3
1 M
arch
200
8)
0
0
0
0
0
Oth
er d
ebto
rs &
acc
rued
inco
me
(at 3
1 M
arch
200
8)
1,
286
1,
286
0
0
0
Cur
rent
Ass
et In
vest
men
ts
0
0
0
0
0
Cas
h at
ban
k an
d in
han
d (a
t 31
Mar
ch
2008
)
11,9
98
11
,998
0
0
0
0 To
tal a
t 31
Mar
ch 2
008
14,4
13
14
,413
0
0
0
Cla
tterb
ridge
Cen
tre
for O
ncol
ogy
NH
S Fo
unda
tion
Trus
t A
ccou
nts
for t
he y
ear e
nded
31st
Mar
ch 2
009
89
25.2
Fin
anci
al L
iabi
litie
s
Liab
ilitie
s as
per
bal
ance
she
et
Tota
l
Loan
s an
d R
ecei
vabl
es
A
sset
s at
fair
valu
e Th
roug
h I&
E
H
eld
to
Mat
urity
Ava
ilabl
e fo
r sal
e
£ 00
0s
£
000s
£
000s
£
000s
£
000s
B
ank
Ove
rdra
fts (a
t 31
Mar
200
9)
0
0
0
0
0Lo
ans
(at 3
1 M
ar 2
009)
0
0
0
0
0N
HS
cre
dito
rs (a
t 31
Mar
ch 2
009)
1,80
1
1,80
1
0
0
0O
ther
cre
dito
rs (a
t 31
Mar
ch 2
009)
2,77
1
2,77
1
0
0
0C
apita
l cre
dito
rs (a
t 31
Mar
ch 2
009)
625
62
5
0
0
0Fi
nanc
e le
ase
oblig
atio
ns (a
t 31
Mar
ch
2009
)
0
0
0
0
0 P
rovi
sion
s un
der c
ontra
ct (a
t 31
Mar
ch
2009
)
818
81
8
0
0
0
Tota
l at 3
1 M
arch
200
9
6,01
5
6,01
5
0
0
0
Ban
k O
verd
rafts
(at 3
1 M
ar 2
008)
0
0
0
0
0Lo
ans
(at 3
1 M
ar 2
008)
0
0
0
0
0N
HS
cre
dito
rs (a
t 31
Mar
ch 2
008)
2,47
0
2,47
0
0
0
0O
ther
cre
dito
rs (a
t 31
Mar
ch 2
008)
0
0
0
0
0C
apita
l cre
dito
rs (a
t 31
Mar
ch 2
008)
0
0
0
0
0Fi
nanc
e le
ase
oblig
atio
ns (a
t 31
Mar
ch
2008
)
0
0
0
0
0 P
rovi
sion
s un
der c
ontra
ct (a
t 31
Mar
ch
2008
)
11
11
0
Tota
l at 3
1 M
arch
200
8
2,
481
2,
481
0
0
0
89
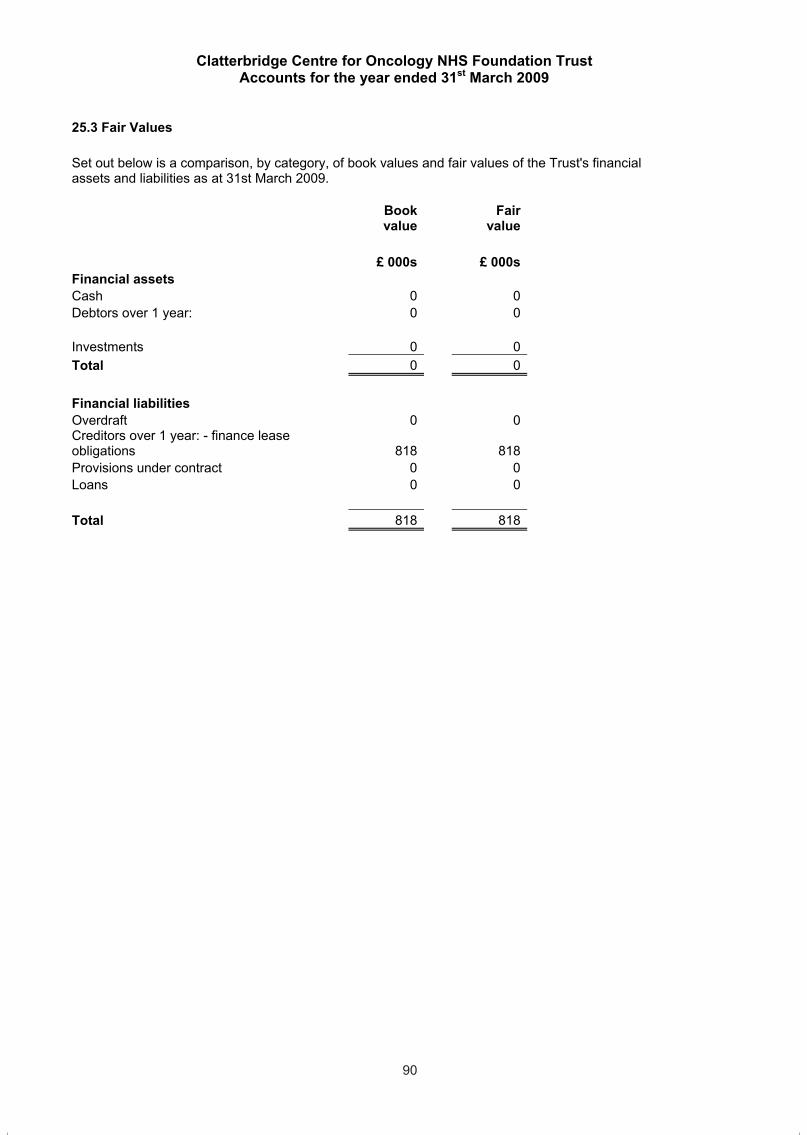
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
90
25.3 Fair Values
Set out below is a comparison, by category, of book values and fair values of the Trust's financial assets and liabilities as at 31st March 2009.
Bookvalue
Fairvalue
£ 000s £ 000s Financial assets Cash 0 0 Debtors over 1 year: 0 0
Investments 0 0 Total 0 0
Financial liabilities Overdraft 0 0 Creditors over 1 year: - finance lease obligations 818 818 Provisions under contract 0 0 Loans 0 0
Total 818 818
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
91
26. Third Party Assets
The Trust held £NIL cash at bank and in hand at 31st March 2009 (2007/08 £Nil) which relates to monies held by Trust on behalf of patients
27. Intra-Government and Other Balances (FTC 20)
Debtors: amounts
fallingdue
within one year
Debtors: amounts
falling due after more than one
year
Creditors: amounts
fallingdue
within one year
Creditors: amounts
fallingdue after
morethan one
year NHS and other WGA Debtors and Creditors £000 £000 £000 £000 Due within one year
English NHS Foundation Trusts 53 0 1,202 0English NHS Trusts 6 0 567 0Department of Health 0 0 0 0English Strategic Health Authorities 40 0 5 0English Primary Care Trusts 353 0 9 0RAB Special Health Authorities 1 0 18 0NHS CGA bodies 0 0 0 0NHS WGA bodies 16 0 0 0
Total NHS debtors / creditors 469 0 1,801 0Other WGA bodies 41 0 721 0TOTAL DUE WITHIN ONE YEAR 510 0 2,522 0
Analysis of NHS and Other WGA Debtors and Creditors due within one year Total NHS debtors / creditors 469 0 1,801 0Less amounts included in other categories: Loans 0 0 0 0Total NHS debtors / creditors 469 0 1,801 0Add back: amounts included in other categories 0 0 0 0Analysis of other WGA bodies Loans 0 0 0 0Corporation tax receivable / payable 0 0 0 0Other tax and social security costs 0 0 517 0Other debtors / creditors 0 0 0 0Other: NHS Pension Scheme (Employers) 0 0 204 0 HM Customs & Excise (VAT) 41 0 0 0TOTAL DUE WITHIN ONE YEAR 510 0 2,522 0
90
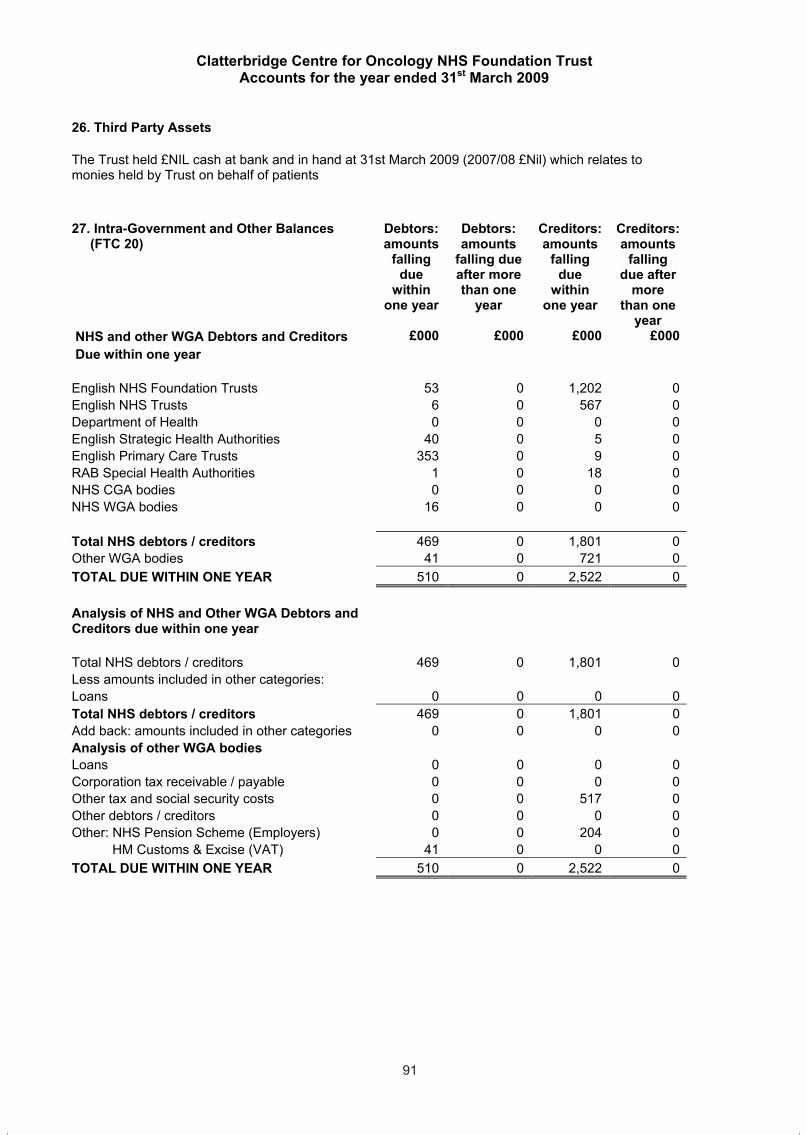
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
90
25.3 Fair Values
Set out below is a comparison, by category, of book values and fair values of the Trust's financial assets and liabilities as at 31st March 2009.
Bookvalue
Fairvalue
£ 000s £ 000s Financial assets Cash 0 0 Debtors over 1 year: 0 0
Investments 0 0 Total 0 0
Financial liabilities Overdraft 0 0 Creditors over 1 year: - finance lease obligations 818 818 Provisions under contract 0 0 Loans 0 0
Total 818 818
Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
91
26. Third Party Assets
The Trust held £NIL cash at bank and in hand at 31st March 2009 (2007/08 £Nil) which relates to monies held by Trust on behalf of patients
27. Intra-Government and Other Balances (FTC 20)
Debtors: amounts
fallingdue
within one year
Debtors: amounts
falling due after more than one
year
Creditors: amounts
fallingdue
within one year
Creditors: amounts
fallingdue after
morethan one
year NHS and other WGA Debtors and Creditors £000 £000 £000 £000 Due within one year
English NHS Foundation Trusts 53 0 1,202 0English NHS Trusts 6 0 567 0Department of Health 0 0 0 0English Strategic Health Authorities 40 0 5 0English Primary Care Trusts 353 0 9 0RAB Special Health Authorities 1 0 18 0NHS CGA bodies 0 0 0 0NHS WGA bodies 16 0 0 0
Total NHS debtors / creditors 469 0 1,801 0Other WGA bodies 41 0 721 0TOTAL DUE WITHIN ONE YEAR 510 0 2,522 0
Analysis of NHS and Other WGA Debtors and Creditors due within one year Total NHS debtors / creditors 469 0 1,801 0Less amounts included in other categories: Loans 0 0 0 0Total NHS debtors / creditors 469 0 1,801 0Add back: amounts included in other categories 0 0 0 0Analysis of other WGA bodies Loans 0 0 0 0Corporation tax receivable / payable 0 0 0 0Other tax and social security costs 0 0 517 0Other debtors / creditors 0 0 0 0Other: NHS Pension Scheme (Employers) 0 0 204 0 HM Customs & Excise (VAT) 41 0 0 0TOTAL DUE WITHIN ONE YEAR 510 0 2,522 0
91

Clatterbridge Centre for Oncology NHS Foundation Trust Accounts for the year ended 31st March 2009
92
28. Losses and Special Payments
There were 31 cases of losses and special payments totaling £33k paid during 2008/09. (2007/08 13 cases totaling £4k). There were no cases exceeding £250k in year.
Note: The total costs included in this note are on a cash basis and will not reconcile to the amountsin the notes to accounts which are prepared on an accruals basis.
29. Auditors Liability
The auditors liability for losses in connection with the external audit is not limited.
92

Clatterbridge Centre for OncologyClatterbridge RoadBebington, Wirral
CH63 4JY
Telephone. 0151 334 1155www.ccotrust.nhs.uk
Large Print and Braille versions or translations available on request.