“antibiotics and corticosteroids: indications and approaches” raymond cross, m.d., m.s., agaf...
TRANSCRIPT
“Antibiotics and corticosteroids: Indications and approaches”
Raymond Cross, M.D., M.S., AGAFAssociate Professor of Medicine
Director of the Inflammatory Bowel Disease ProgramUniversity of Maryland School of Medicine
Co-Director, Digestive Health CenterUniversity of Maryland Medical Center
12/4/14

Goals of Therapy
• Induce remission• Maintain steroid-free remission• Enhance quality of life• Achieve mucosal healing• Prevent/treat complications of disease• Avoid short and long term toxicity of therapy
PGA of Disease Activity
• Remission: No symptoms• Mild disease activity: No limitations in activity (i.e.,
not missing work, not canceling social engagements)
• Moderate disease activity: Impaired activity (i.e., missing days of work, canceling some social engagements)
• Severe disease activity: Severely impaired activity (i.e., housebound, bathroom bound, hospitalized)

AMINOSALICYLATES

AMINOSALICYLATE DISTRIBUTION

5-ASA Content of 5-ASA Preparations Generic Trade 5-ASA Content
(%)Usual Dosage Amount of 5-
ASA DeliveredSulfasalazine Azulfidine,
Azulfidine EN, Sulfazine, Sulfazine EC
38 4 g 1.6 g
Mesalamine Apriso, Asacol HD, Canasa, Delzicol, Lialda, Pentasa, Rowasa, SfRowasa,
100 2.4-4.8 g 2.4-4.8 g
Balsalazide Colazal, Giazo 35 3.3-6.75 g 1.2 g-2.4 g
Olsalazine Dipentum 100 1 g 1 g
Adapted from: Ulcerative Colitis-The Complete Guide to Medical Management (Lichtenstein)

Oral 5-ASA Are Effective For Induction Of Remission In UC
Cochrane Database of Systematic Reviews17 OCT 2012 DOI: 10.1002/14651858.CD000543.pub3http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000543.pub3/full#CD000543-fig-00101

No Difference in Remission Rates between 5-ASA Preparations
Cochrane Database of Systematic Reviews17 OCT 2012 DOI: 10.1002/14651858.CD000543.pub3http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000543.pub3/full#CD000543-fig-00401

High Dose Oral 5-ASA is Not More Effective at Induction of Remission than Moderate Dose in UC
Cochrane Database of Systematic Reviews17 OCT 2012 DOI: 10.1002/14651858.CD000543.pub3http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000543.pub3/full#CD000543-fig-00501
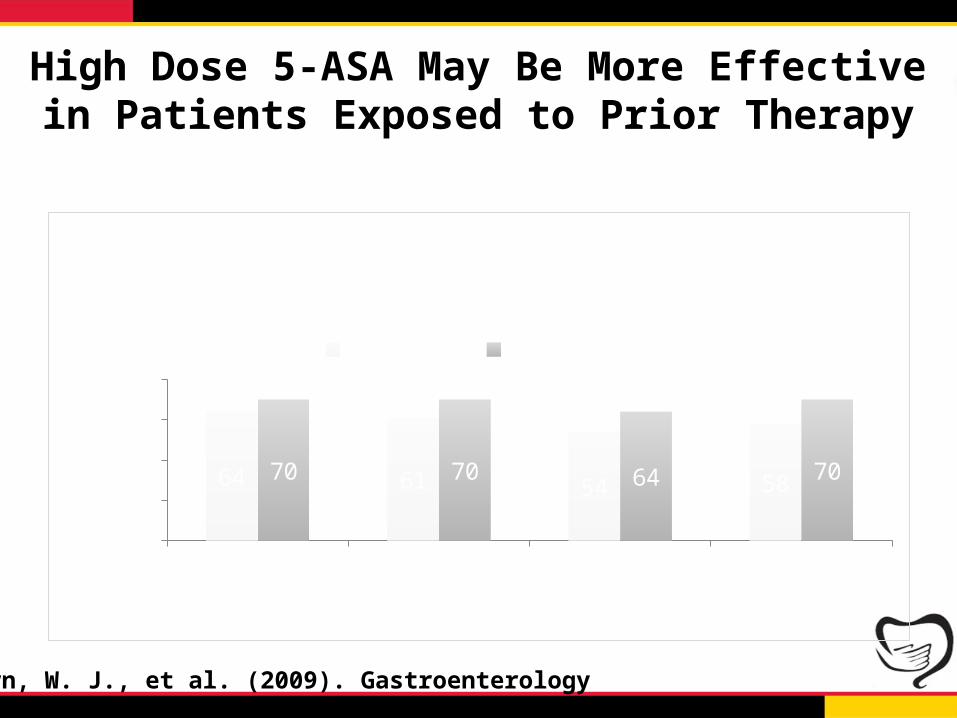
High Dose 5-ASA May Be More Effective in Patients Exposed to Prior Therapy
Oral 5-ASA Rectal therapies Steroids ≥2 meds0
1020304050607080
64 61 54 5870 70 64 70
Treatment Success at Week 6 in Patients Having Taken Previous UC Therapy
2.4 g/day 4.8 g/day
Perc
ent o
f Pati
ents
Sandborn, W. J., et al. (2009). Gastroenterology
P=0.05 P=0.01

Efficacy of Once vs. Twice Daily 5-ASA for Induction of Remission in UC
Series105
10152025303540
Clinical and Endoscopic Remission at Week 8
MMX BID MMX QD Placebo
Perc
ent o
f Pati
ents
Lichtenstein, G. R., et al. (2007). Clin Gastroenterol Hepatol

ORAL VERSUS RECTAL MESALAMINE VERSUS COMBINATION THERAPY IN ACTIVE DISTAL
ULCERATIVE COLITIS

Dose of Oral 5-ASA Not Important For Maintenance of Remission in UC
Cochrane Database of Systematic Reviews17 OCT 2012 DOI: 10.1002/14651858.CD000544.pub3http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD000544.pub3/full#CD000544-fig-00501
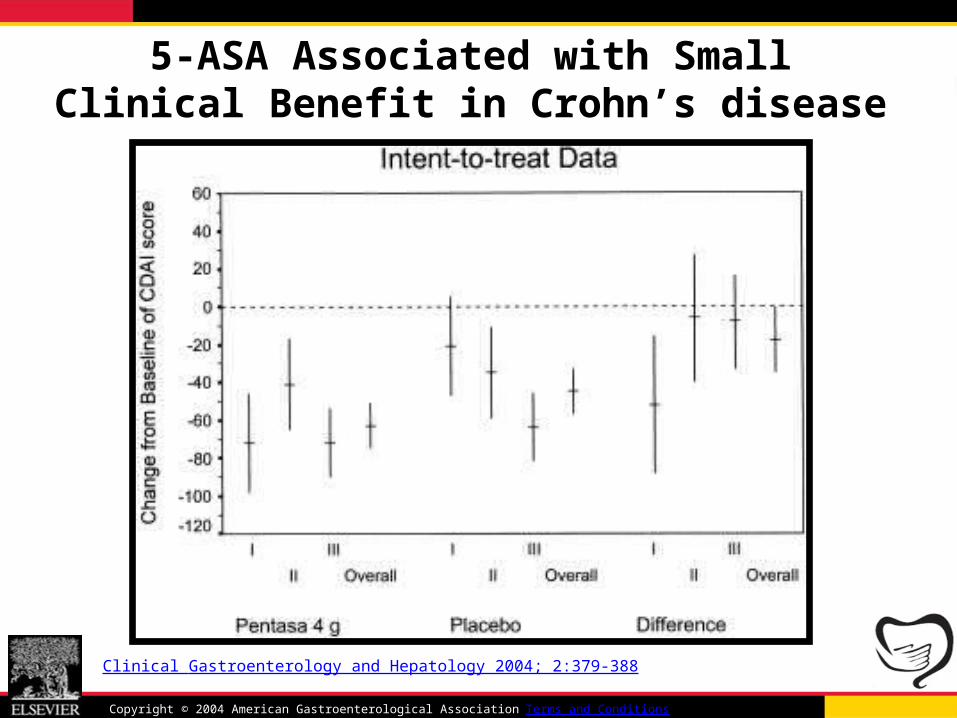
Pentasa reduces CDAI compared to placebo
Clinical Gastroenterology and Hepatology 2004; 2:379-388
Copyright © 2004 American Gastroenterological Association Terms and Conditions
5-ASA Associated with Small Clinical Benefit in Crohn’s disease

5-ASA is Not Protective Against Colon Cancer in IBD
• Meta-analysis of non-referral populations– 4 studies included
• Association between ≥ 1 year of 5-ASA use and neoplasia
• aOR 0.95 (0.7-1.4)• Significant heterogeneity among trials
Nguyen, G. C., et al. (2012). Am J Gastroenterol

Budesonide MMX 9 mg Effective at Induction of Remission in UC
Remission Response Symptom Resolution05
10152025303540
7.4
24.816.517.9
33.328.5
13.2
30.6 28.9
12.1
33.925
Combined Clinical and Endoscopic Remission at Week 8
Placebo (n=121) MMX 9 mg (n=121) MMX 6 mg (n=123)5-ASA 2.4 g (n=123)
Perc
ent o
f Pati
ents
*
*
*
16
*
Sandborn et al, Gastroenterology. 2012*p<0.05

Budesonide Foam Effective for Treatment of UP and UPS
Remission Rectal Bleeding=0 Endoscopy Score ≤1
0
10
20
30
40
50
60
42.250.3
55.8
31.8 35.746.8
BFPlacebo
Perc
ent o
f Pati
ents
5-A
SA E
xpos
ed S
ub-G
roup *
*
P<0.05Sandborn, WJ. ACG 2014
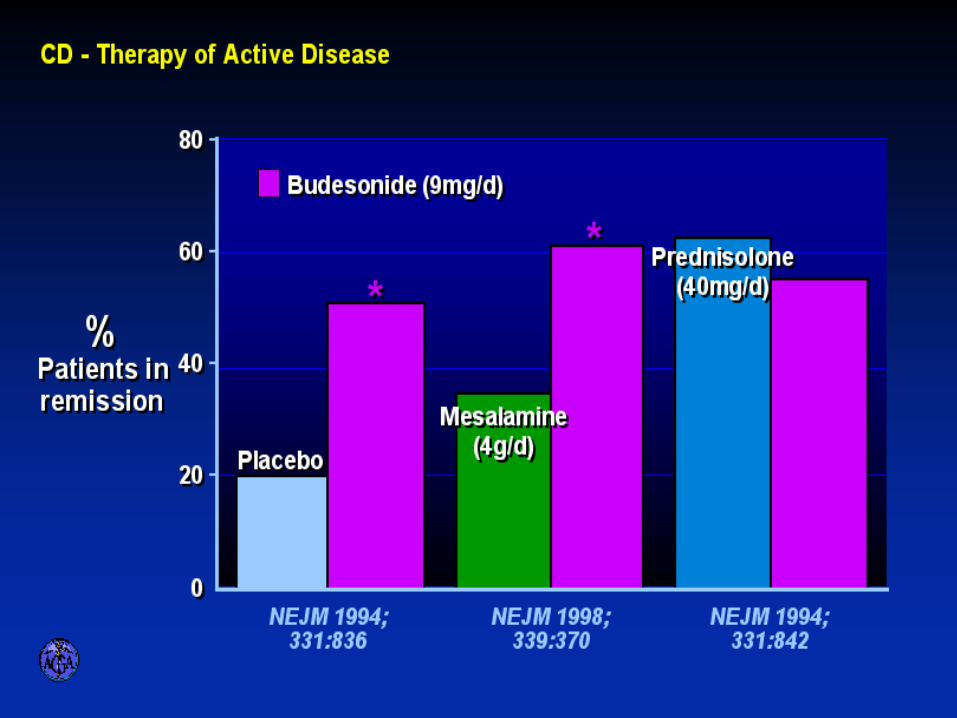
ORAL BUDESONIDE IN ACTIVE CROHN’S DISEASE
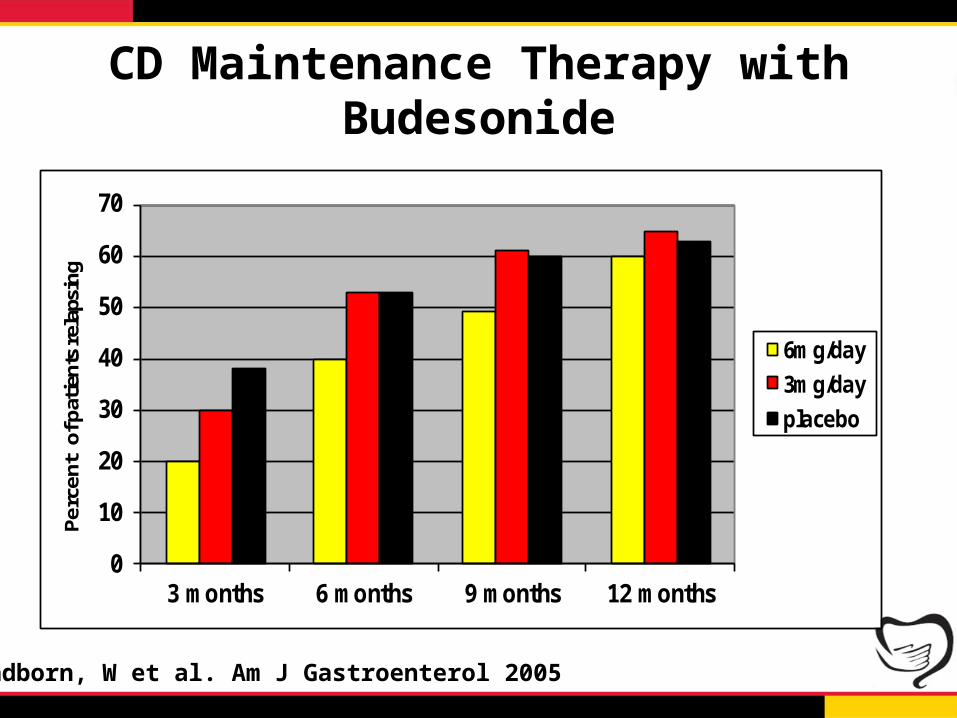
CD Maintenance Therapy with Budesonide
0
10
20
30
40
50
60
70
3 months 6 months 9 months 12 months
Perc
ent
of p
atie
nts
rela
psin
g
6mg/day
3mg/day
placebo
p<0.01
p<0.05
*
**
Sandborn, W et al. Am J Gastroenterol 2005
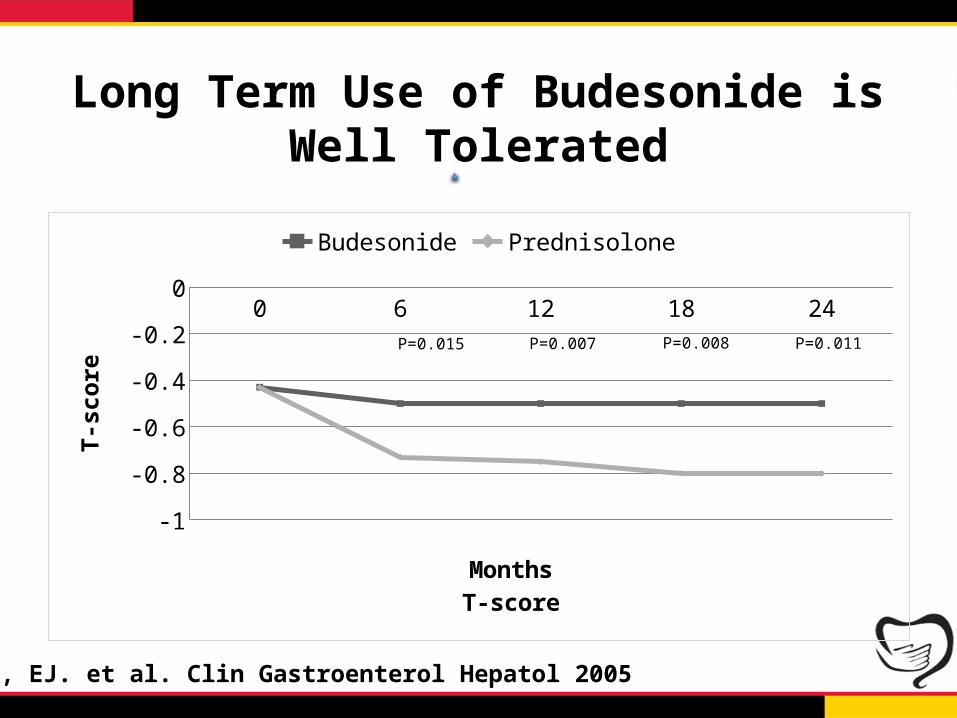
Long Term Use of Budesonide is Well Tolerated
0 6 12 18 24
Budesonide -0.43 -0.5 -0.5 -0.5 -0.5
Prednisolone -0.43 -0.73 -0.75 -0.8 -0.8
-0.85-0.75-0.65-0.55-0.45-0.35-0.25-0.15-0.05
Budesonide Prednisolone
MonthsT-score
T-sc
ore
P=0.015 P=0.007 P=0.008 P=0.011
Schoon, EJ. et al. Clin Gastroenterol Hepatol 2005

Corticosteroid Therapy for UC
*30 days after initiating corticosteroid therapy
Complete Remission
54%(n = 34)
PartialRemission
30%(n = 19)
Immediate Outcome*(n = 63)
1-YearOutcome(n = 63)
Steroid Dependent
22%(n = 14)
Prolonged Response
49%(n = 31)
Surgery 29%
(n = 18)
NoResponse
16%(n = 10)
Faubion, W., et al. Gastroenterology 2001

Corticosteroid Therapy for Crohn’s Disease
*30 days after initiating corticosteroid therapy
Complete Remission
58%(n = 43)
PartialRemission
26%(n = 19)
Immediate Outcome*(n = 74)
1-YearOutcome(n = 74)
Steroid Dependent
28%(n = 21)
Prolonged Response
32%(n = 24)
Surgery 38%
(n = 28)
NoResponse
16%(n = 12)
Faubion, W., et al. Gastroenterology 2001

IV Steroids
• No need to give more than 60 mg of Methylprednisolone sodium succinate or 300 mg of hydrocortisone
• Can give once daily• Response generally occurs within 5-7 days!• ~60% of patients completely respond to IV
steroids
Truelove, SC and Jewell, DP. Lancet 1974Truelove, SC et al. Lancet 1978Jarnerot, G et al. Gastroenterology 1985Gustavsson, A et al. Am J Gastroenterol 2007
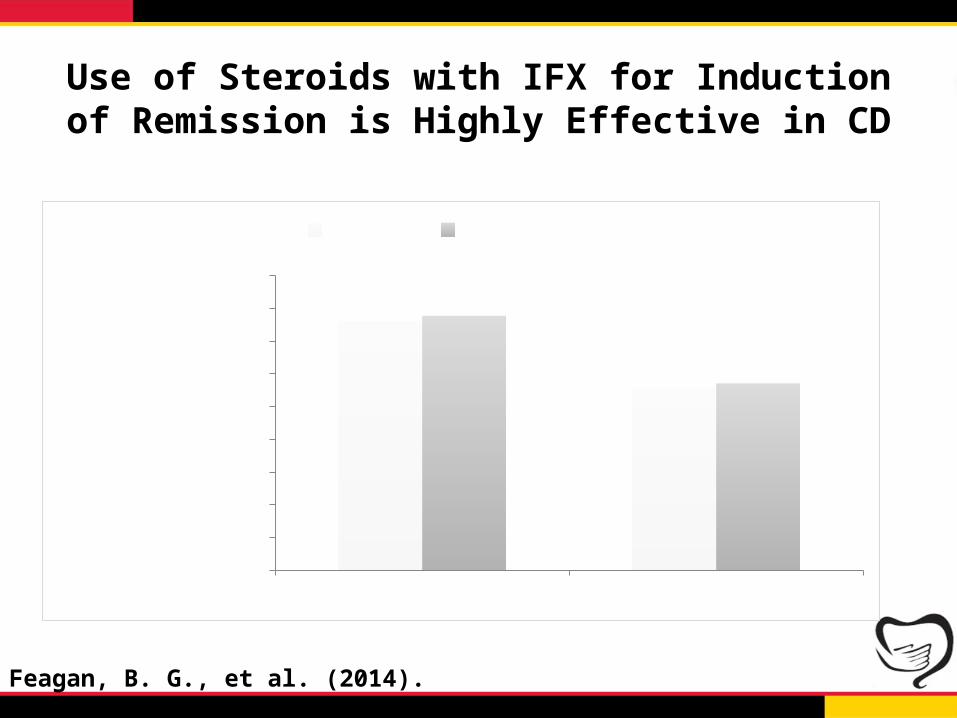
Use of Steroids with IFX for Induction of Remission is Highly Effective in CD
Week 14 Week 500%
10%20%30%40%50%60%70%80%90%
IFX+MTX IFX+Placebo
Percent of Pa-tients
Feagan, B. G., et al. (2014). Gastroenterology

IV Steroids Premedication Reduces ATI in CD
ATI Level ATI +05
1015202530354045
Placebo HC
Perc
ent o
f Pati
ents
P=0.02
P=0.06
Farrell, R. J., et al. Gastroenterology 2003
Conclusions• 5-ASA is effective for induction and maintenance of
remission in patients with UC• Combination of oral and topical 5-ASA more effective
for distal disease• 5-ASA is of marginal benefit in patients with CD• All 5-ASA are effective when given at equal dose• Moderate and high dose 5-ASA equally effective for
induction of remission in UC• Once daily dosing is equally effective to split dosing
(and likely associated with better adherence)
Conclusions (cont.)
• Budesonide is effective for induction of remission in mild to moderate ileocolonic Crohn’s disease and UC– Has a limited role in maintenance of remission
• Prednisone is effective at induction of remission– Poor side effect profile– No role for maintenance of remission– May be used in combination with an anti-TNF to induce
remission in moderate to severe Crohn’s disease• IV steroids may be used prior to IFX to decrease ATI