b lunt a bdominal t rauma dr. sean wilde, pgy-3 (ccfp-em) aug 18 2011 preceptor: dr. trevor langhan
TRANSCRIPT
Blunt
Abdominal
TraumaDr. Sean Wilde,PGY-3 (CCFP-EM)Aug 18 2011Preceptor:Dr. Trevor Langhan
Game Plan• Stepwise approach to
BAT– The baseball diamond
approach– Adults only
• Intra-abdominal & GU trauma
• Classification by stability and patient evaluability
• Role of FAST• When can you avoid a CT
13% of all injuries areAbdominal Trauma
Case mortality is8%
Most deaths are in bluntabdominal trauma
Meet the Players…

Motor Vehicle Collisions
50-75% of BAT

Direct blows tothe abdomen
15%
(assaults and recreational activities)
Falls froma height
6-9%

Mechanisms
• Abrupt Intra-abdominal pressure changes
• Compression of abdominal contents
• Acceleration-deceleration forces

At Risk
• Spleen• Liver• Small bowel• Retroperitoneum• Kidneys• Bladder• Colorectal• Diaphragm• Pancreas

CHALLANGES
•Altered LOC
•Unreliable Physical Exam
•Multiple diagnostictests
•Significant miss ofintestinal andpancreatic injuries
Often multi-trauma

Develop the BAT reflex
Have a simple, step-wise approach to the management of the blunt abdominal trauma victim…
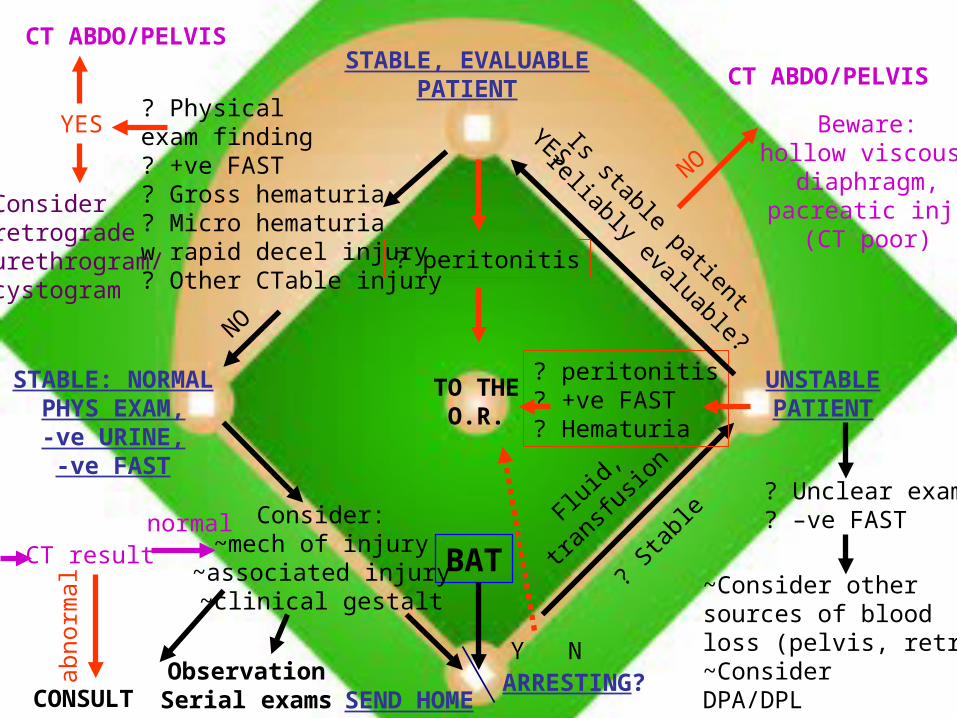
STABLE, EVALUABLEPATIENT
ARRESTING?
UNSTABLEPATIENT
STABLE: NORMALPHYS EXAM,-ve URINE,-ve FAST
BAT
SEND HOME
TO THEO.R.
Y N
? peritonitis? +ve FAST? Hematuria
? Unclear exam? –ve FAST
Fluid,
trans
fusio
n
~Consider othersources of bloodloss (pelvis, retroP)~ConsiderDPA/DPL
? Sta
ble
Is stable patient
reliably evaluable?
NO
CT ABDO/PELVIS
YES
? peritonitis
CT ABDO/PELVIS
? Physicalexam finding? +ve FAST? Gross hematuria? Micro hematuriaw rapid decel injury? Other CTable injury
Considerretrogradeurethrogram/cystogram
NO
YES
CONSULT
CT result
abno
rmal
Consider:~mech of injury
~associated injury~clinical gestalt
normal
ObservationSerial exams
Beware:hollow viscous,
diaphragm,pacreatic inj.
(CT poor)

ABC’s in BAT
• ABC / OIL
• Prioritize the injuries– Airway > Chest > Abdomen > Head > GU
• Don’t forget the Abdomen in multi-trauma!
• Feel the Belly!– More than once
• FAST scan is part of primary survey– Do it BEFORE the log roll.

The Baseball Diamond Approach to BAT
1. Stability• Arresting, unstable or stable?
2. OR Red flags• In the unstable vs stable patient• Initial resuscitation
3. To CT or not to CT• Is the patient evaluable?• What findings mandate/avoid a CT?• When is DPL useful?
4. Reassuring findings• going for home
Case 1
• 40yo male, MVC• Restrained driver• Passenger fatality• Unconscious at scene• Cardiac arrest pulling into
ambulance bay after 2 litres NS
• Diffuse chest and abdominal bruising with distended abdomen
• No major open injuries• CPR in progress,
asystole on monitor
I would:
A) Crack the chest for open cardiac massage
B) ATLS/ACLS and 2 fridges of blood
C) ED Laparotomy
D) Do nothing (“He’s dead Jim”)
E)

Plan:
Mortality after BAT arrest is dismal; worse than penetrating or chest trauma
Doing nothing is a valid option*
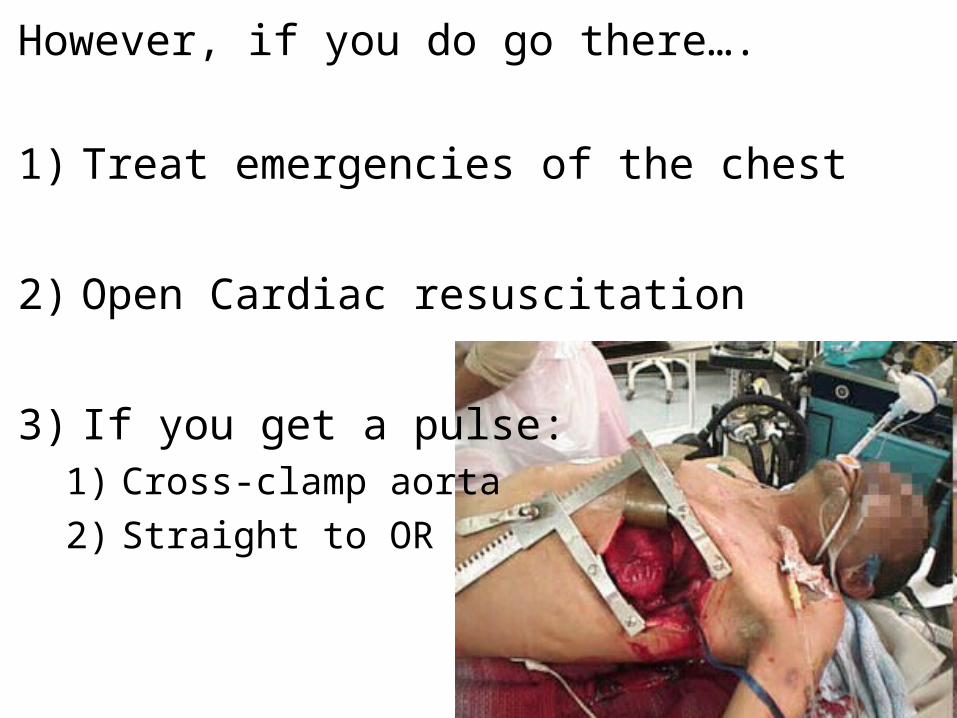
However, if you do go there….
1) Treat emergencies of the chest
2) Open Cardiac resuscitation
3) If you get a pulse:1) Cross-clamp aorta
2) Straight to OR

Fluid Resuscitation
• Colloids
– NS, Ringer’s
• Blood Early
• Massive Transfusion Protocols
6:6:1
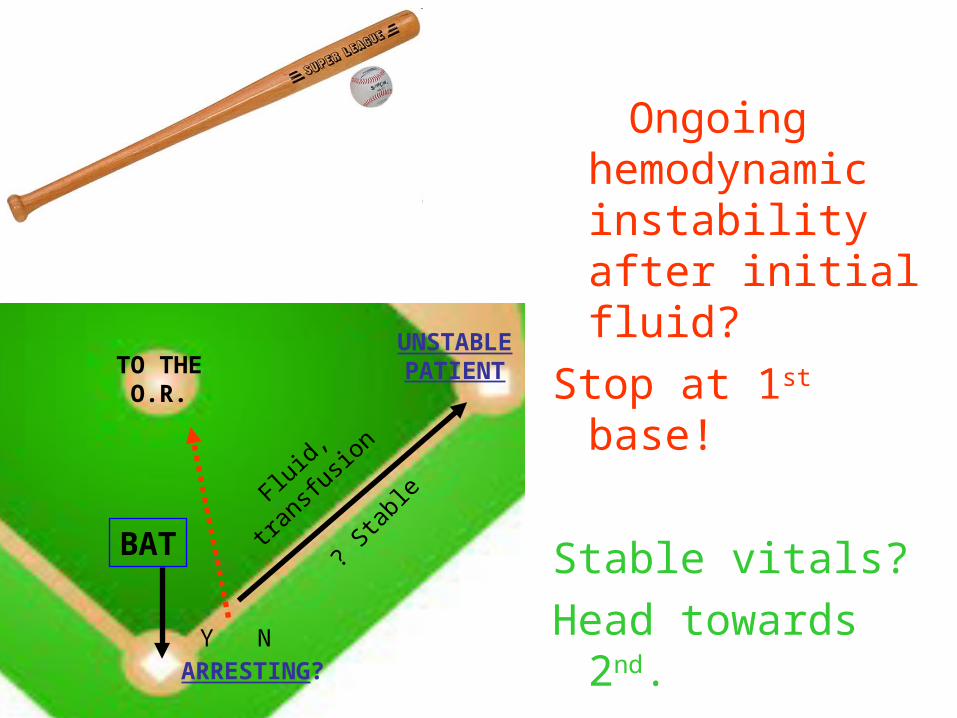
ARRESTING?
BAT
TO THEO.R.
Y N
Fluid,
tran
sfusio
n
? Sta
ble
UNSTABLEPATIENT
Ongoing hemodynamic instability after initial fluid?
Stop at 1st base!
Stable vitals?
Head towards 2nd.

Case 2• 29y F, thrown from bike in
motocross accident• GCS 11-14, fluctuating• Non-ambulatory at scene• Full spinal precautions• HR 135, BP 70/55, O2
95% on 2L NP• Cries in pain when
transferred to bed• Hurts “everywhere!”
• Now what?
Trauma Survey– Chest unremarkable– Diffuse mild tenderness to abdomen– Pelvis stable but painful– FAST –ve– Long bones look OK– Lots of pain to RLQ/right hip on log roll
• Resuscitation– Brief improvement in vitals/GCS with fluid, then rapid
decline• Getting more drowsy• Hg 105 on ABG
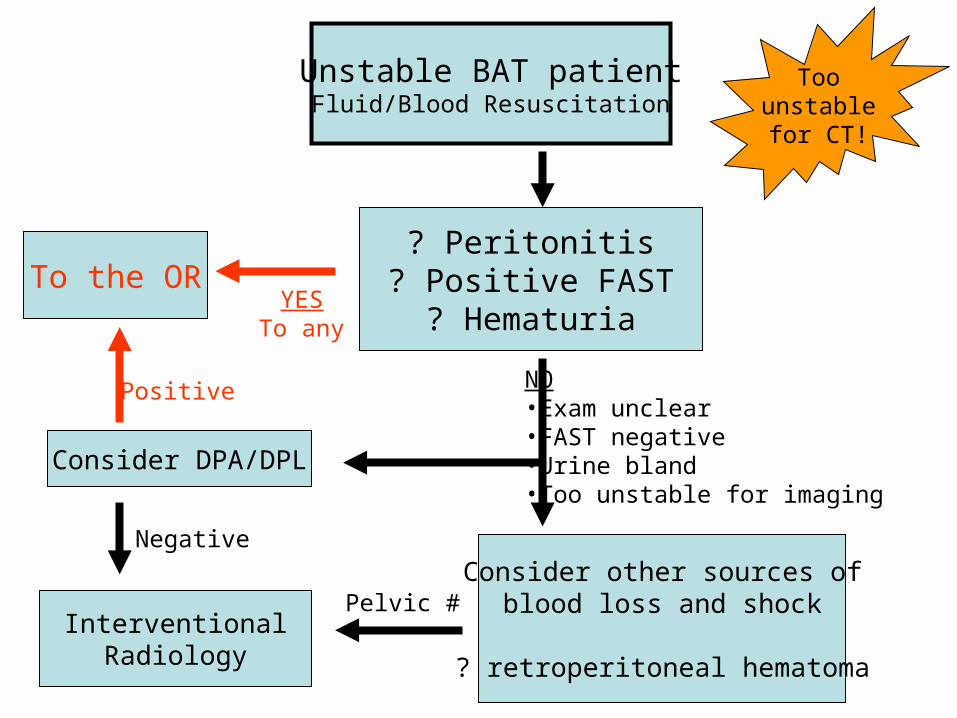
Unstable BAT patientFluid/Blood Resuscitation
? Peritonitis? Positive FAST
? HematuriaTo the OR
Consider other sources ofblood loss and shock
? retroperitoneal hematoma
Consider DPA/DPL
YESTo any
NO•Exam unclear•FAST negative•Urine bland•Too unstable for imaging
Positive
InterventionalRadiology
Pelvic #
Negative
Toounstablefor CT!
Case cont…
• FAST is negative
• No peritonitis
• Microscopic hematuria after catheter
• Non displaced pelvic fracture on x-ray
• But the belly seems more tender than earlier…
FAST Facts
• Poor sensitivity– 200cc fluid for positive scan– Cannot use a negative scan alone to rule out
need for surgery
• Good specificity– For free abdominal fluid– Blood vs Urine
DPL?
1. Unstable, multi-injured patient with questionable abdominal source
2. Replace serial abdominal exam in head injured patient
3. Post normal CT with ongoing high suspicion of the abdomen
4. Remote area where CT unavailable- i.e. O.R. before transport?
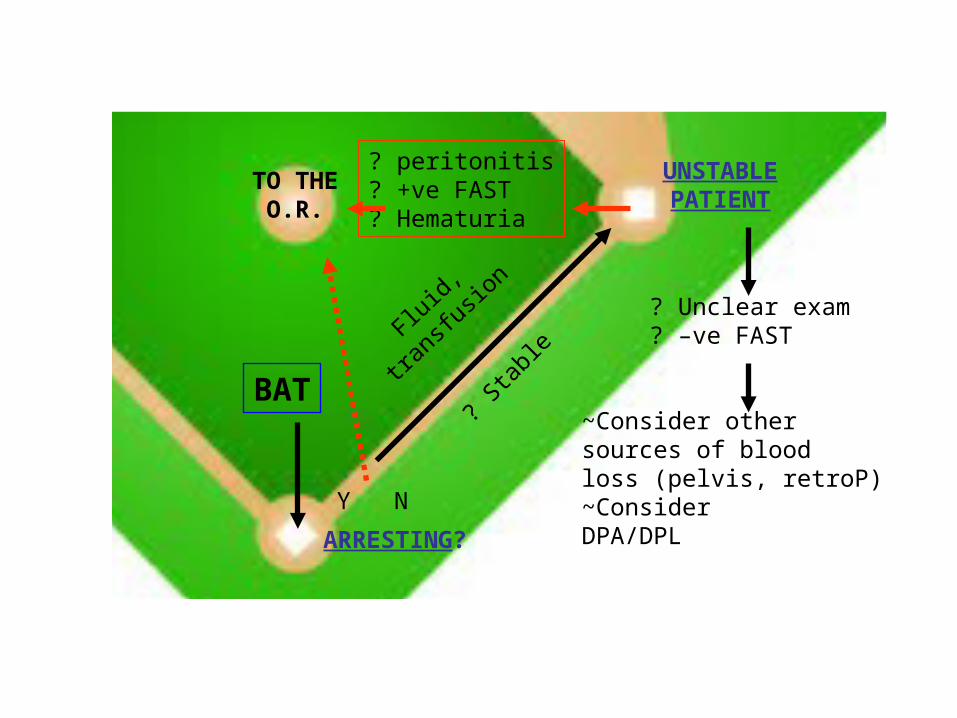
ARRESTING?
UNSTABLEPATIENT
BAT
TO THEO.R.
Y N
? peritonitis? +ve FAST? Hematuria
? Unclear exam? –ve FAST
Fluid,
tran
sfusio
n
~Consider othersources of bloodloss (pelvis, retroP)~ConsiderDPA/DPL
? Sta
ble
STABLE, EVALUABLEPATIENT
BAT
Fluid,
trans
fusio
n
? Sta
ble
Is stable patient
reliably evaluable?
YESNO
CT ABDO/PELVIS
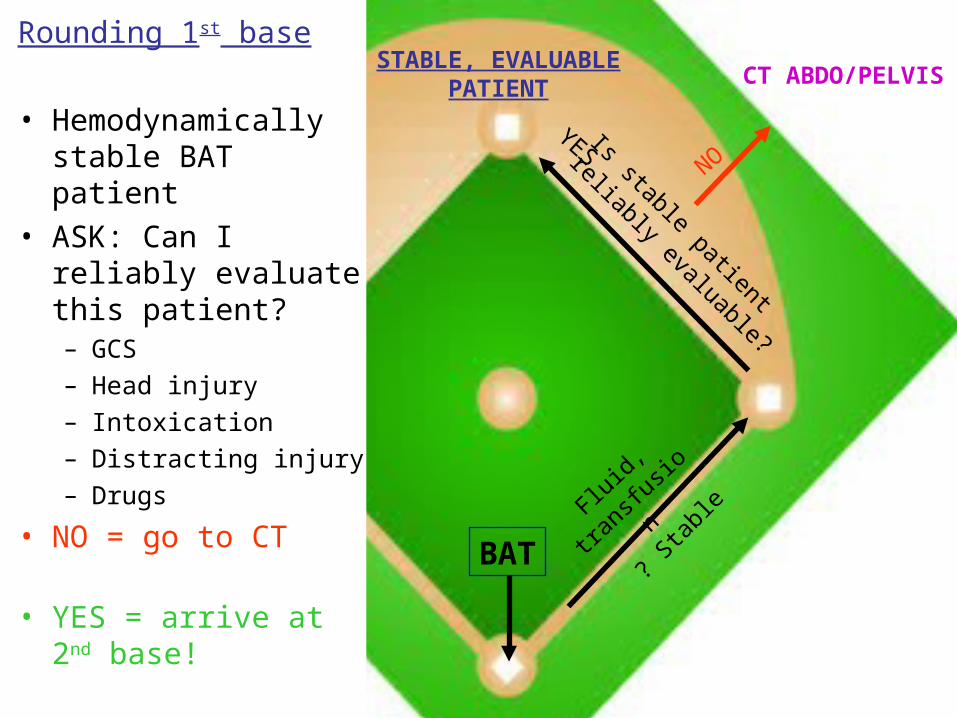
Rounding 1st base
• Hemodynamically stable BAT patient
• ASK: Can I reliably evaluate this patient?– GCS– Head injury– Intoxication– Distracting injury– Drugs
• NO = go to CT
• YES = arrive at 2nd base!

Case 3
• 45y M kicked in the stomach 7 hours ago
• Ongoing discomfort• Vitals normal and stable• Generalized abdo pain on
palpation– No peritonitis– No guarding– No visible bruising
• Urine clean• Next?
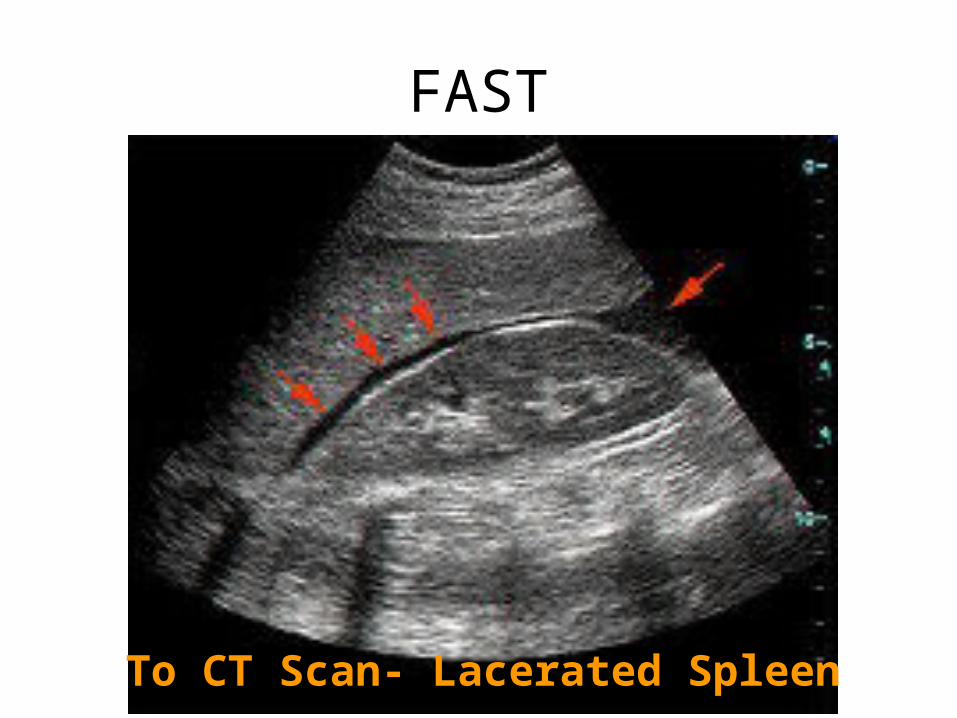
FAST
To CT Scan- Lacerated Spleen
CAT Scan in BAT
Very good sensitivity and specificity
Normal CT scan can be considered very reassuring
Critical management decisions
Oral Contrast?• Does not increase detection of HVI• Impractical/Risky (NG feeds on spine board)• Local trauma surgeons rarely use it
• Negative CT- Consider missed:– GI (hollow viscous) injuries– Diaphragmatic injuries– Pancreatic injuries
• Serial exams and CT Scans as indicated will catch most.
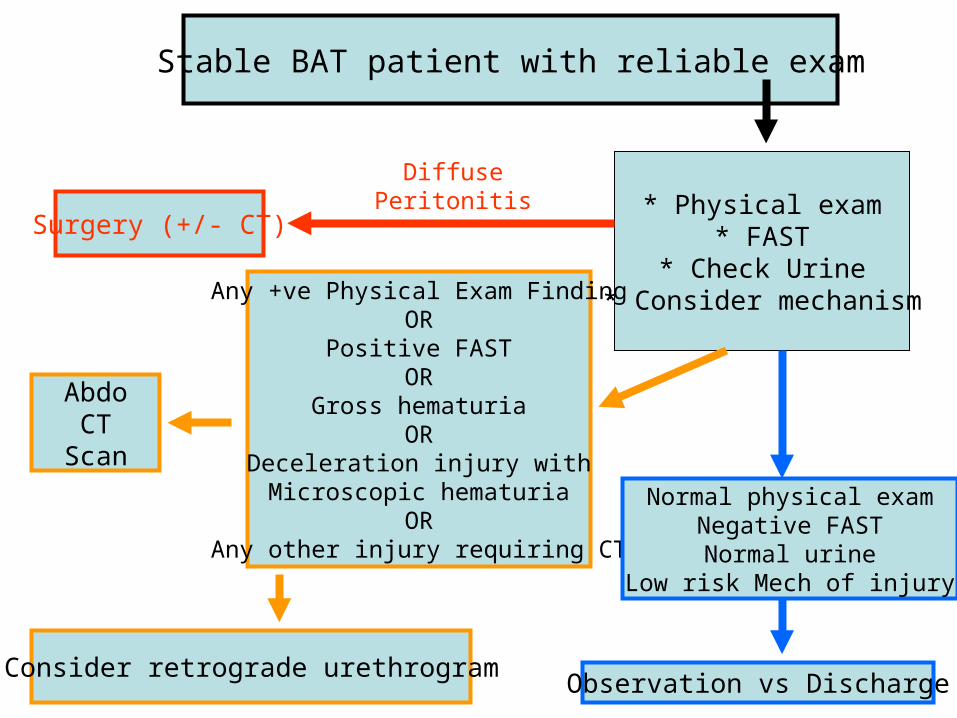
* Physical exam* FAST
* Check Urine* Consider mechanism
Surgery (+/- CT)
Any +ve Physical Exam FindingOR
Positive FASTOR
Gross hematuriaOR
Deceleration injury withMicroscopic hematuria
ORAny other injury requiring CT
Normal physical examNegative FASTNormal urine
Low risk Mech of injury
Observation vs DischargeConsider retrograde urethrogram
Stable BAT patient with reliable exam
DiffusePeritonitis
AbdoCT
Scan

Abdominal seatbelt sign:
IA injury rate 23% with, 3% without
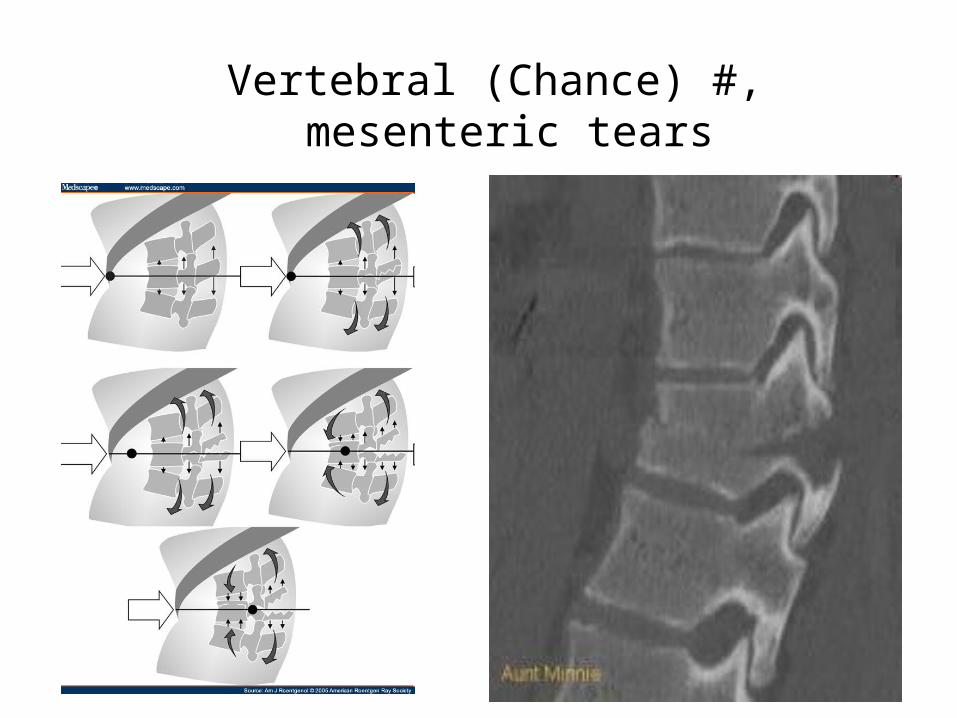
Vertebral (Chance) #, mesenteric tears
BAT Physical Exam +ves
• Abdominal Seatbelt sign
• Pain with guarding
• Any peritoneal findings
• Remember value of repeat exams!!!

STABLE, EVALUABLEPATIENT
STABLE: NORMALPHYS EXAM,-ve URINE,-ve FAST
CT ABDO/PELVIS
? Physicalexam finding? +ve FAST? Gross hematuria? Micro hematuriaw rapid decel injury? Other CTable injury
Considerretrogradeurethrogram/cystogram
NO
YES • Rounding 2nd base to 3rd
• Avoiding a CT so far…
• What’s between you and home plate?
Case 3 the remix…
• As before, kicked in stomach, ongoing pain.
• Vitals stable• This time all
investigations negative, including FAST
• What now?
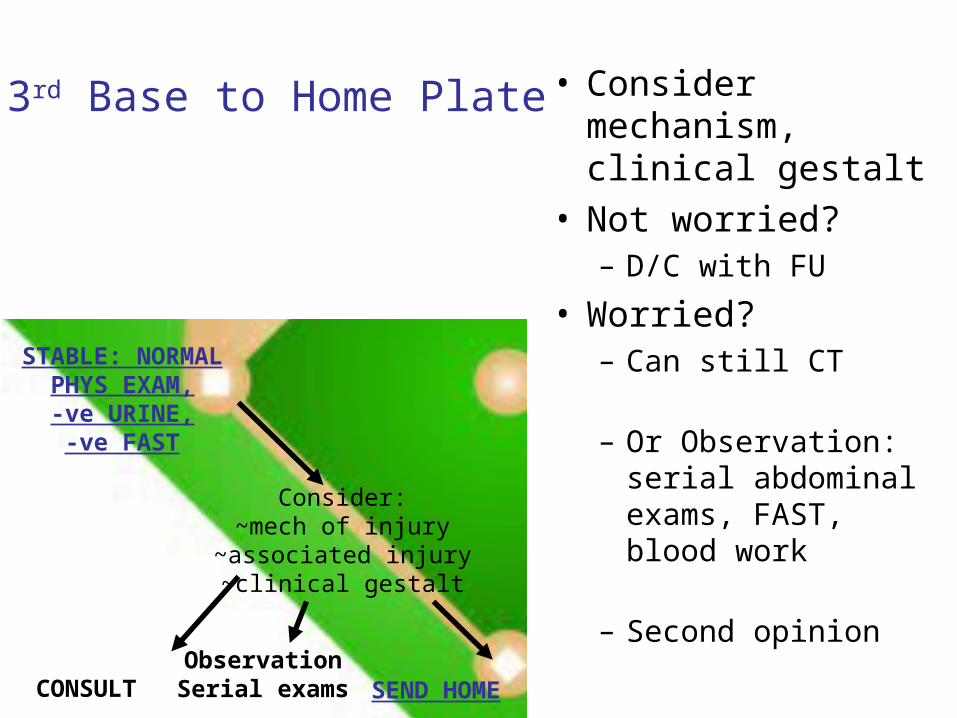
STABLE: NORMALPHYS EXAM,-ve URINE,-ve FAST
SEND HOMECONSULT
Consider:~mech of injury
~associated injury~clinical gestalt
ObservationSerial exams
• Consider mechanism, clinical gestalt
• Not worried?– D/C with FU
• Worried?– Can still CT
– Or Observation: serial abdominal exams, FAST, blood work
– Second opinion
3rd Base to Home Plate

Holmes, 2009. Low risk Clin Pred Rules in BAT
If none of:• GCS <14• Abdominal/costal margin tenderness• Hematuria• Hematocrit < 30%• Femur fracture• CHXR trauma findings
Negative predictive value of 99% for intra-abdominal injury

Serial abdominal exams (at least 2)
Negative FAST
Clean Urine
The Bare Minimum…
Case 4
• 29y M fell 12ft off “scissor lift.”
• Landed on his bottom• Stable, alert, c/o sore
buttocks• Head/spines cleared• Abdomen non-tender• FAST negative• Urine dips 3+ blood

GU Trauma• Blood at meatus• High riding/boggy
prostate• Unable to void• Hematuria (esp
gross)
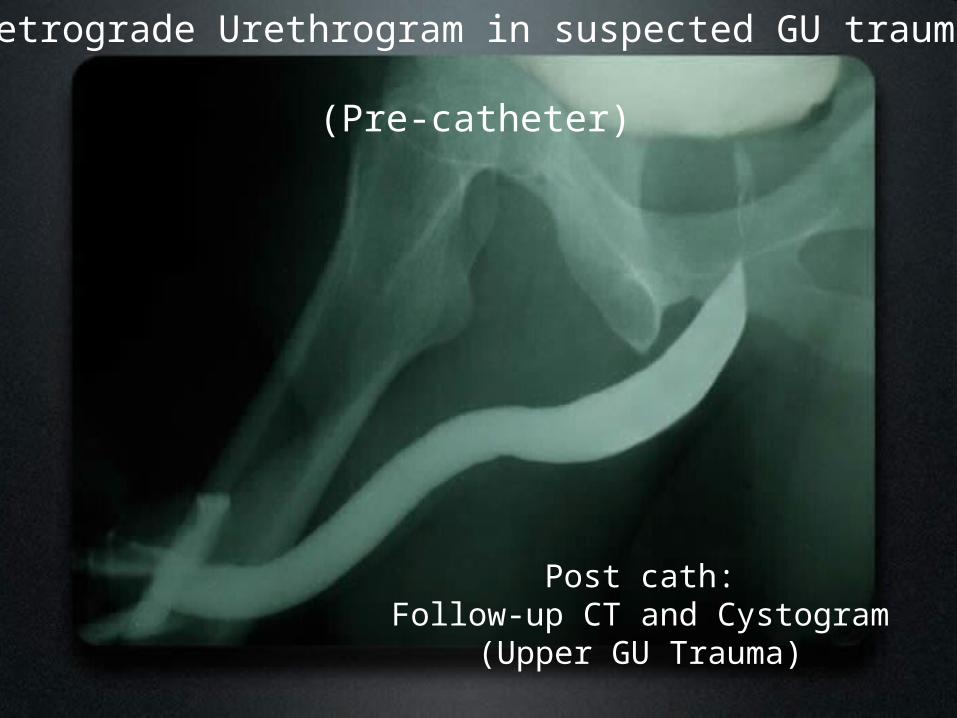
Retrograde Urethrogram in suspected GU trauma
(Pre-catheter)
Post cath:Follow-up CT and Cystogram
(Upper GU Trauma)

STABLE, EVALUABLEPATIENT
ARRESTING?
UNSTABLEPATIENT
STABLE: NORMALPHYS EXAM,-ve URINE,-ve FAST
BAT
SEND HOME
TO THEO.R.
Y N
? peritonitis? +ve FAST? Hematuria
? Unclear exam? –ve FAST
Fluid,
trans
fusio
n
~Consider othersources of bloodloss (pelvis, retroP)~ConsiderDPA/DPL
? Sta
ble
Is stable patient
reliably evaluable?
NO
CT ABDO/PELVIS
YES
? peritonitis
CT ABDO/PELVIS
? Physicalexam finding? +ve FAST? Gross hematuria? Micro hematuriaw rapid decel injury? Other CTable injury
Considerretrogradeurethrogram/cystogram
NO
YES
CONSULT
CT result
abno
rmal
Consider:~mech of injury
~associated injury~clinical gestalt
normal
ObservationSerial exams
Beware:hollow viscous,
diaphragm,pacreatic inj.
(CT poor)