behind doors closed
TRANSCRIPT
TERAPROOF:User:michaelcrowley Date: 20/11/2007 Time: 09:36:01Edition: 20/11/2007 ExSupplement XS2011DRUGSPage:12 Zone:XS1
EXPERT VIEW
VIEW FROM THE GROUND
EXPERT VIEW
After 22 years’e x pe rience, DrCiaran Donovanshares his insight
I’VE been a GP in this city for 22years and so I’ve seen lots ofchanges in drug usage.Alcohol was always there and with
the Celtic Tiger, it’s got worse as there’smore money for it, off-licences are nowon every corner, pubs open later and su-permarkets offering cut-price deals.
In the first 15 years, cannabis was theonly real illegal drug in use to anygreat degree and up to four or fiveyears ago, cocaine was an extreme rari-ty. Ecstasy has been there for the past10 years but I have to say that this didnot seem to do the huge immediatedamage that cocaine is doing.
Cocaine is incredibly expensive andincredibly addictive and I have peoplein here who admit to spending€1,200-€1,400 a week on it. Young menworking in the building industry, forexample, now have huge amounts ofmoney available to them. I suppose itwasn’t sold here before as there justwasn’t the market as people didn’t havethe money. I think that nowadays, ec-stasy has been superceded by cocaineas the drug being used by 17-25 yearolds at the weekends.
The classic situation where we meetaddicts is on a Monday morning.They’ll arrive in front of me at the endof their tether and wanting an instantcure. They may have run into troublewith the law or ran up huge debts butthe main problem is that there aren’timmediate services. If you have a frac-tured femur or a brain tumour, I knowexactly what point of contact to sendyou to. I will tell you the hospital andthe consultant but for acute drug abuse,I can only send you to A&E.
There is no coherent HSE treatmentpathway for drug abusers in the South.Mainstream psychiatry services such asSt Michael’s at the Mercy or GF at CorkUniversity Hospital don’t want drugusers. They don’t see it as part of theirremit. They will, if they have to, takedrug abusers but it’s a revolving doorwith a huge reliance on voluntarygroups like the youth services on Shan-don Street. In Cork, we don’t even havea psychiatrist with an interest in addic-tion.
I have no doubt that it’s a class issueas the abusers who suffer most aregenerally working class. The middleclasses can afford to go to a costly pri-vate clinic. There’s a waiting list ofover a month for Arbour House in Corkcity. What are you supposed to do in be-tween? Alcohol is still the main drugabused in Ireland and there is still hugedenial around it but at least you have awell-developed Alcoholics Anonymousnetwork in this country.”
■ Dr Ciaran Donovan is a GP onCommons Road in Cork city.
A&Es are usedas drop-incentres and it’swrong, writesChris Luke
HOSPITAL emergency de-partments are normallyone of the first places tosee big changes in a so-
ciety.From Avian flu and tuberculo-
sis to increased violence anddrug misuse, we are faced withthese changes far earlier thanthe academics and the bureau-crats that collate statistics fromour reports.
Extreme violence caused bycocaine usage is my big concern.You commonly see it on a Sun-day morning — young peoplecoming in, off their heads oncoke, causing mayhem. Just theother day we had a very violentyoung man causing havoc forother patients. His girlfriend waswith him — off her head too. It’sro u t ine.
The normal scenario is thatsomebody comes in after a bigfight or because they are actingdelirious or displaying psychoticbehaviour. Others are self-harm-ing.
DRUG INDUCED HEARTATTACKS
Common cocaine users areaged 18-35 and they’re havinghear tattacks, seizures and strokes.We’ve also had collapsed lungs.A great number of people are dy-ing. Sudden cardiac arrest iscommon.
Cocaine is absolutely every-where. It’s particularlywidespread in the northside ofthe city (Cork) but also in thecounty and on the southside.The middle classes are also us-ing it in towns and villagesacross the county. We are seeinga steady trickle of heroin casesin Cork. This a new develop-ment.
HEROINE USE IS RISING
Heroin was mainly in Dublin,Limerick and Waterford. We arenot being afflicted by intra-venous drug usage yet. It’s still,for the most part, ‘chasing thedragon’ or smoking heroin.There are, however, reports ofneedles being found in the vicin-ity of the hospital. Just the othernight, we saved the life of ayoung man who had overdosedon heroin.In the past 18 months, I’ve eas-ily seen about half a dozen seri-ous cases, where people are over-dosing on a cocktail of drugs in-cluding heroin. The typical hero-in user lives in the north innercity, is unemployed and a poly-substance abuser. Generally,they drink heavily and regularlytake valium and codeine.
A growing number are fromthe homeless community andthey’ll take any drug going andthat’s how heroin starts. We’llregularly see them at the Mercy,which is more like the Mater orSt James’s in Dublin in thatthere is a large inner cityspread, while at Cork UniversityHospital (CUH) it’s more subur-ban, bourgeois and rural.
PRESCRIPTION DRUGS
Large numbers are also abus-ing prescription drugs — uppersand downers. They’re oftenrobbed from family members.These have been abused fordecades — the likes of benzodi-azepines temaze- pam and distal-gesic, prozac andviagra. Most are taken withdrink.
People don’t realise that theyounger you are taking these,the more vulnerable you are togetting sick and delirious.
I can’t remember a single mi-grant drug issue. I don’t remem-ber one African or Eastern Euro-pean. A lot of the Africans in in-ner city areas like ShandonStreet smoke khat — an indige-nous drug derived from the Cocaleaf. It’s a mild psychedelic andstimulant.
As for the lack of treatmenthere, it’s the same everywhere.For instance in Liverpool whereI worked before, there was achronic heroin problem andthere was just one four-bed treat-ment centre.
People are more sympatheticto harm reduction than treat-ment. Yes, A&E is being used asa drop in centre and it’s notright.
■ Chris Luke is a consultant inemergency medicine at Cork Uni-versity Hospital
BEHINDCLOSED
DOORS
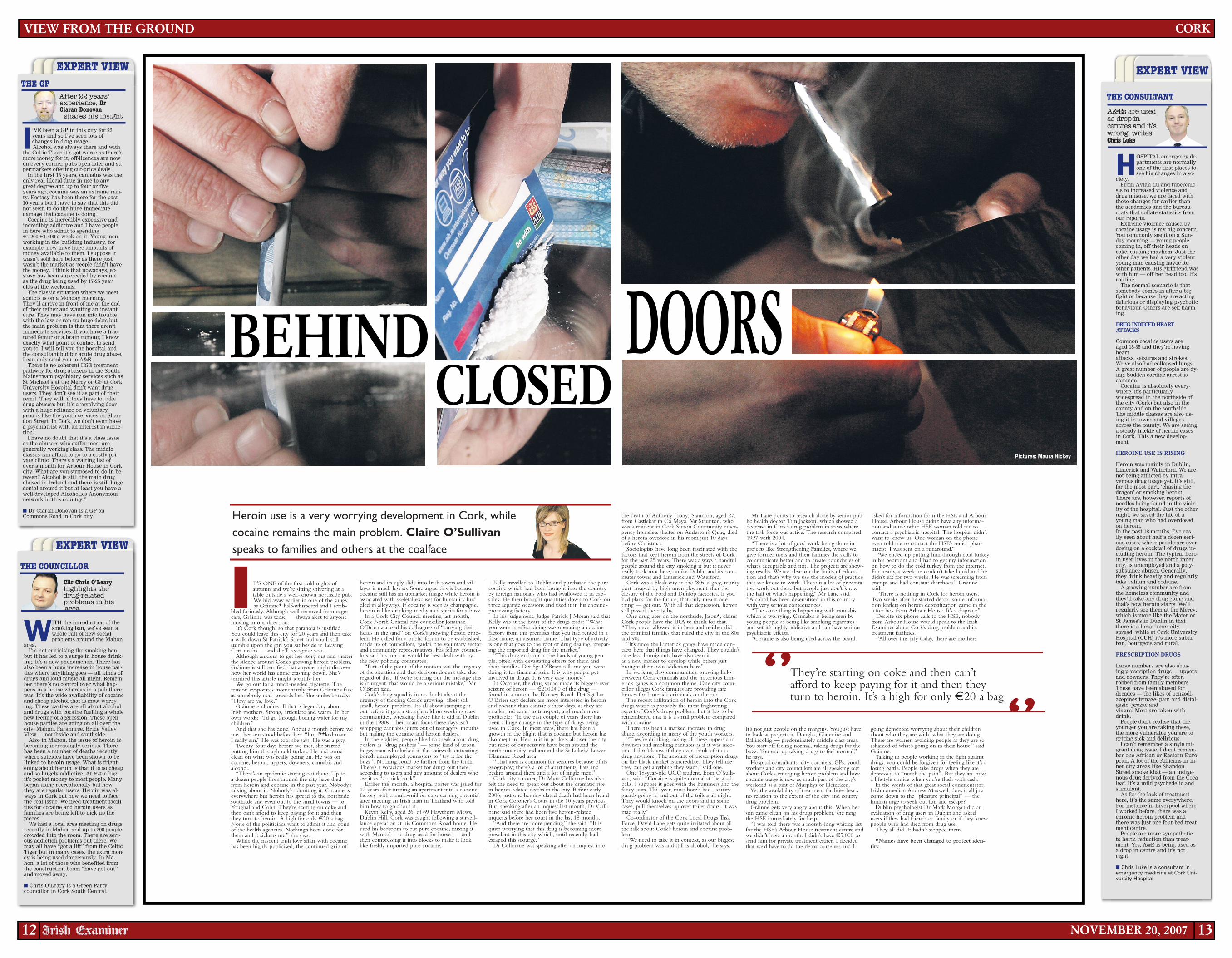
They’re starting on coke and then can’tafford to keep paying for it and then theyturn to heroin. It’s a high for only €20 a bag
‘’‘’
Cllr Chris O’Learyhighlights thed r u g- r elat edproblems in hisarea
NOVEMBER 20, 200712 13
WITH the introduction of thesmoking ban, we’ve seen awhole raft of new socialproblems around the Mahon
a rea.I’m not criticising the smoking ban
but it has led to a surge in house drink-ing. It’s a new phenomenon. There hasalso been a huge increase in house par-ties where anything goes — all kinds ofdrugs and loud music all night. Remem-ber, there’s no control over what hap-pens in a house whereas in a pub therewas. It’s the wide availability of cocaineand cheap alcohol that is most worry-ing. These parties are all about alcoholand drugs with cocaine fuelling a wholenew feeling of aggression. These openhouse parties are going on all over thecity- Mahon, Farannree, Bride ValleyView — northside and southside.
Also in Mahon, the issue of heroin isbecoming increasingly serious. Therehas been a number of deaths recentlywhere suicides have been shown to belinked to heroin usage. What is fright-ening about heroin is that it is so cheapand so hugely addictive. At €20 a bag,it’s pocket money to most people. Manybegan using recreationally but nowthey are regular users. Heroin was al-ways in Cork but now we need to facethe real issue. We need treatment facili-ties for cocaine and heroin users asfamilies are being left to pick up thepiece s.
We had a local area meeting on drugsrecently in Mahon and up to 200 peoplecrowded into the room. There are seri-ous addiction problems out there. Wemay all have “got a lift” from the CelticTiger but in many cases, the extra mon-ey is being used dangerously. In Ma-hon, a lot of those who benefited fromthe construction boom “have got out”and moved away.
■ Chris O’Leary is a Green Partycouncillor in Cork South Central.
CORK
THE GP
THE COUNCILLOR
EXPERT VIEW
THE CONSULTANT
Heroin use is a very worrying development in Cork, whilecocaine remains the main problem. Claire O’Sullivanspeaks to families and others at the coalface
I T’S ONE of the first cold nights ofautumn and we’re sitting shivering at atable outside a well-known northside pub.We hid away earlier in one of the snugsas Gráinne* half-whispered and I scrib-
bled furiously. Although well removed from eagerears, Gráinne was tense — always alert to anyonemoving in our direction.
It’s Cork though, so that paranoia is justified.You could leave this city for 20 years and then takea walk down St Patrick’s Street and you’ll stillstumble upon the girl you sat beside in LeavingCert maths — and she’ll recognise you.
Although anxious to get her story out and shatterthe silence around Cork’s growing heroin problem,Gráinne is still terrified that anyone might discoverhow her world has come crashing down. She’sterrified this article might identify her.
We go out for a much-needed cigarette. Thetension evaporates momentarily from Gráinne’s faceas somebody nods towards her. She smiles broadly:“How are ya, love.”
Gráinne embodies all that is legendary aboutIrish mothers. Strong, articulate and warm. In herown words: “I’d go through boiling water for mychild ren.”
And that she has done. About a month before wemet, her son stood before her: “I’m f**ked mam.I really am.” He was too, she says. He was a pity.
Twenty-four days before we met, she startedputting him through cold turkey. He had comeclean on what was really going on. He was oncocaine, heroin, uppers, downers, cannabis andalcohol.
“There’s an epidemic starting out there. Up toa dozen people from around the city have diedfrom heroin and cocaine in the past year. Nobody’stalking about it. Nobody’s admitting it. Cocaine iseverywhere but heroin has spread to the northside,southside and even out to the small towns — toYoughal and Cobh. They’re starting on coke andthen can’t afford to keep paying for it and thenthey turn to heroin. A high for only €20 a bag.None of the politicians want to admit it and noneof the health agencies. Nothing’s been done forthem and it sickens me,” she says.
While the nascent Irish love affair with cocainehas been highly publicised, the continued grip of
heroin and its ugly slide into Irish towns and vil-lages is much less so. Some argue this is becausecocaine still has an upmarket image while heroin isassociated with skeletal excuses for humanity hud-dled in alleyways. If cocaine is seen as champagne,heroin is like drinking methylated spirits for a buzz.
In a Cork City Council meeting last month,Cork North Central city councillor JonathanO’Brien accused his colleagues of “burying theirheads in the sand” on Cork’s growing heroin prob-lem. He called for a public forum to be established,made up of councillors, gardaí, the voluntary sectorand community representatives. His fellow council-lors said his motion would be best dealt with bythe new policing committee.
“Part of the point of the motion was the urgencyof the situation and that decision doesn’t take dueregard of that. If we’re sending out the message thisisn’t urgent, that would be a serious mistake,” MrO’Brien said.
Cork’s drug squad is in no doubt about theurgency of tackling Cork’s growing, albeit stillsmall, heroin problem. It’s all about stamping itout before it gets a stranglehold on working classcommunities, wreaking havoc like it did in Dublinin the 1980s. Their main focus these days isn’twhipping cannabis joints out of teenagers’ mouthsbut nailing the cocaine and heroin dealers.
In the eighties, people liked to speak about drugdealers as “drug pushers” — some kind of urbanbogey man who lurked in flat stairwells entreatingbored, unemployed youngsters to “try it for thebuzz”. Nothing could be further from the truth.There’s a voracious market for drugs out there,according to users and any amount of dealers whosee it as “a quick buck”.
Earlier this month, a hospital porter was jailed for12 years after turning an apartment into a cocainefactory with a multi-million euro earning potentialafter meeting an Irish man in Thailand who toldhim how to go about it.
Kevin Kelly, aged 26, of 69 Hawthorn Mews,Dublin Hill, Cork was caught following a surveil-lance operation at his Commons Road home. Heused his bedroom to cut pure cocaine, mixing itwith Manitol — a drug used for horses — andthen compressing it into blocks to make it looklike freshly imported pure cocaine.
Kelly travelled to Dublin and purchased the purecocaine which had been brought into the countryby foreign nationals who had swallowed it in cap-sules. He then brought quantities down to Cork onthree separate occasions and used it in his cocaine-processing factory.
In his judgement, Judge Patrick J Moran said thatKelly was at the heart of the drugs trade: “Whatyou were in effect doing was operating a cocainefactory from this premises that you had rented in afalse name, an assumed name. That type of activityis one that goes to the root of drug dealing, prepar-ing the imported drug for the market.”
“This drug ends up in the hands of young peo-ple, often with devastating effects for them andtheir families. Det Sgt O’Brien tells me you weredoing it for financial gain. It is why people getinvolved in drugs. It is very easy money.”
In October, the drug squad made its biggest-everseizure of heroin — €200,000 of the drug —found in a car on the Blarney Road. Det Sgt LarO’Brien says dealers are more interested in heroinand cocaine than cannabis these days, as they aresmaller and easier to transport, and much moreprofitable: “In the past couple of years there hasbeen a huge change in the type of drugs beingused in Cork. In most areas, there has been agrowth in the blight that is cocaine but heroin hasalso crept in. Heroin is in pockets all over the citybut most of our seizures have been around thenorth inner city and around the St Luke’s/ LowerGlanmire Road area.
“That area is common for seizures because of itsgeography; there’s a lot of apartments, flats andbedsits around there and a lot of single men.”
Cork city coroner, Dr Myra Cullinane has alsofelt the need to speak out about the dramatic risein heroin-related deaths in the city. Before early2006, just one heroin-related death had been heardin Cork Coroner’s Court in the 10 years previous.But, speaking after an inquest last month, Dr Culli-nane said there had been five heroin-relatedinquests before her court in the last 18 months.
“And there are more pending,” she said. “It isquite worrying that this drug is becoming moreprevalent in this city which, until recently, hadescaped this scourge.”
Dr Cullinane was speaking after an inquest into
the death of Anthony (Tony) Staunton, aged 27,from Castlebar in Co Mayo. Mr Staunton, whowas a resident in Cork Simon Community emer-gency homeless shelter on Anderson’s Quay, diedof a heroin overdose in his room just 10 daysbefore Christmas.
Sociologists have long been fascinated with thefactors that kept heroin from the streets of Corkfor the past 25 years. There was always a handfulpeople around the city smoking it but it neverreally took root here, unlike Dublin and its com-muter towns and Limerick and Waterford.
Cork was a bleak city in the ‘80s, a grey, murkyport ravaged by high unemployment after theclosure of the Ford and Dunlop factories. If youhad plans for the future, that only meant onething — get out. With all that depression, heroinstill passed the city by.
One drug user on the northside, Jason*, claimsCork people have the IRA to thank for that.“They never allowed it in here and neither didthe criminal families that ruled the city in the 80sand 90s.
“It’s since the Limerick gangs have made con-tacts here that things have changed. They couldn’tcare less. Immigrants have also seen itas a new market to develop while others justbrought their own addiction here.”
In working class communities, growing linksbetween Cork criminals and the notorious Lim-erick gangs is a common theme. One city coun-cillor alleges Cork families are providing safehouses for Limerick criminals on the run.
The recent infiltration of heroin into the Corkdrugs world is probably the most frighteningaspect of Cork’s drugs problem, but it has to beremembered that it is a small problem comparedwith cocaine.
There has been a marked increase in drugabuse, according to many of the youth workers.
“They’re drinking, taking all these uppers anddowners and smoking cannabis as if it was nico-tine. I don’t know if they even think of it as adrug anymore. The amount of prescription drugson the black market is incredible. They tell methey can get anything they want,” said one.
One 18-year-old UCC student, Eoin O’Sulli-van, said: “Cocaine is quite normal at the gradballs. I suppose it goes with the hummers and thefancy suits. This year, most hotels had securityguards going in and out of the toilets all night.They would knock on the doors and in somecases, pull themselves up over toilet doors. It wasmad really.”
Co-ordinator of the Cork Local Drugs TaskForce, David Lane gets quite irritated about allthe talk about Cork’s heroin and cocaine prob-lem.
“We need to take it in context, as our biggestdrug problem was and still is alcohol,” he says.
Mr Lane points to research done by senior pub-lic health doctor Tim Jackson, which showed adecrease in Cork’s drug problem in areas wherethe task force was active. The research compared1997 with 2004.
“There is a lot of good work being done inprojects like Strengthening Families, where wegive former users and their families the skills tocommunicate better and to create boundaries ofwhat’s acceptable and not. The projects are show-ing results. We are clear on the limits of educa-tion and that’s why we use the models of practicethat we know to work. There is a lot of preventa-tive work out there but people just don’t knowthe half of what’s happening,” Mr Lane said.“Alcohol has been desensitised in this countrywith very serious consequences.
“The same thing is happening with cannabiswhich is worrying. Cannabis is being seen byyoung people as being like smoking cigarettesand yet it’s highly addictive and can have seriouspsychiatric effects.
“Cocaine is also being used across the board.
It’s not just people on the margins. You just haveto look at projects in Douglas, Glanmire andBallincollig — predominately middle class areas.You start off feeling normal, taking drugs for thebuzz. You end up taking drugs to feel normal,”he says.
Hospital consultants, city coroners, GPs, youthworkers and city councillors are all speaking outabout Cork’s emerging heroin problem and howcocaine usage is now as much part of the city’sweekend as a pint of Murphys or Heineken.
Yet the availability of treatment facilities bearsno relation to the extent of the city and countydrug problem.
Gráinne gets very angry about this. When herson came clean on his drugs problem, she rangthe HSE immediately for help.
“I was told there was a month-long waiting listfor the HSE’s Arbour House treatment centre andwe didn’t have a month. I didn’t have €5,000 tosend him for private treatment either. I decidedthat we’d have to do the detox ourselves and I
asked for information from the HSE and ArbourHouse. Arbour House didn’t have any informa-tion and some other HSE woman told me tocontact a psychiatric hospital. The hospital didn’twant to know us. One woman on the phoneeven told me to contact the HSE’s senior phar-macist. I was sent on a runaround.”
“We ended up putting him through cold turkeyin his bedroom and I had to get my informationon how to do the cold turkey from the internet.For nearly, a week he couldn’t take liquid and hedidn’t eat for two weeks. He was screaming fromcramps and had constant diarrhoea,” Gráinnesaid.
“There is nothing in Cork for heroin users.Two weeks after he started detox, some informa-tion leaflets on heroin detoxification came in theletter box from Arbour House. It’s a disgrace.”
Despite six phone calls to the HSE, nobodyfrom Arbour House would speak to the IrishExaminer about Cork’s drug problem and itstreatment facilities.
“All over this city today, there are mothers
going demented worrying about their childrenabout who they are with, what they are doing.There are women avoiding people as they are soashamed of what’s going on in their house,” saidG r áinne.
Talking to people working in the fight againstdrugs, you could be forgiven for feeling like it’s alosing battle. People take drugs when they aredepressed to “numb the pain”. But they are nowa lifestyle choice when you’re flush with cash.
In the words of that great social commentator,Irish comedian Andrew Maxwell, does it all justcome down to the “pleasure principal” — thehuman urge to seek out fun and escape?
Dublin psychologist Dr Mark Morgan did anevaluation of drug users in Dublin and askedusers if they had friends or family or if they knewpeople who had died from drug use.
They all did. It hadn’t stopped them.
*Names have been changed to protect iden-t i t y.
Pictures: Maura Hickey

TERAPROOF:User:jackiebolandDate:16/11/2007 Time:18:14:55Edition: 20/11/2007 ExSupplement XS2011DRUGSPage:14Zone:XS1
EXPERT VIEW
Crisis asserious now as10 years ago,says Anna Quigley
MANY people will remember thescenes in the mid-1990s of angrycrowds marching in the streets toprotect their communities from
d r u g s.Dublin’s disadvantaged communities were
in the grip of a devastating heroin crisis as aresult of the State’s failure to respond to aproblem that was first highlighted by com-munity leaders in the late 1970s and early198 0 s.
In 1996, a combination of the streetcampaign in local communities, politicalcampaigning by community leaders, and theshocking murder of Veronica Guerin finallyled to a co-ordinated government response.
The Local Drugs Task Forces (LDTFs)were set up so that local communities andState agencies could work together in part-nership to deliver a response to the drugscrisis in the communities most affected.
Communities were given a link tonational policy-making with a representa-tive on the National Drugs Strategy Team(NDST).
Between 1996 and 2002 funding of IR£25million was allocated between the 14 LDTFSand a whole range of drug projects were de-veloped in local communities.
In 2002, the Government launched the Na-tional Drugs Strategy, which outlined 100 ac-tions to be carried out by 2008. Itincluded the setting up of Regional DrugsTask Forces to cover all areas outside ofDublin and Cork.
This progress was welcomed by communi-ty leaders. Despite this community concernswere growing during 2002 that the politicalwill was waning.
There was a slowdown in funding tolocal projects and LDTFs were not beingasked by government to draw up futureplans. Comments made during the 2002 elec-tion gave the impression that the drug prob-lem was more or less sorted out.
After the election, the junior ministrydealing with the drugs issue was effectivelydowngraded to a half-time position.
A further indication of how drugs slippeddown the political agenda was the slow re-sponse to the emerging cocaine problem.
Citywide first highlighted this problem inSeptember 2002 and we called on the Gov-ernment to give the Local Drugs Task Forcesa mandate to respond to cocaine.
The Government said there wasn’t a seri-ous problem. The delay meant crucial yearswere lost, with a huge cost to individuals,families and communities.
Research by Citywide in October 2006found an increase in dealing, public nui-sance and anti-social behaviour, and 90% ofprojects saw an increase in violent crime intheir communities since 2004.
Families were living in fear of dealers andmoney lenders, with threats of violence overmoney owed.
There were also serious delays in settingup the Regional Drugs Task Forces.
In 1999, we said it would be “absolutely in-excusable” for any other city or town to ex-perience a heroin epidemic similar toDublin, but that this would happen unlesspreventative strategies were put in place.
Figures for heroin use outside of Dublinhave grown steadily. NACD research in 2004indicated approximately 2,000 heroin usersoutside of the Dublin region, and all of theRDTFs indicate a growing problem withheroin use.
Heroin and cocaine are of major concern,but a whole mix of drugs are being used, in-cluding illegal drugs, legal drugs such as al-cohol and prescription drugs such as benzo-diazepines.
The NACD cocaine report shows a300-400% increase in those seeking treatmentfor cocaine use, while Garda data showsnearly a 400% increase in cocaine seizuresbetween 2000 and 2005.
There is evidence of crack cocaine use insome communities, and there are concernsof crystal meth in parts of Dublin. Commu-nity projects are concerned heroin use is onthe increase again in Dublin. This is backedup by Garda seizures and reports of hugeopium harvests in Afghanistan.
There is no doubt there has been a majorexpansion in drug services during the last 10years and that structures have been put inplace to enable local communities and statu-tory agencies to work together. But there isno doubt that the initial momentum of thelate 1990s has not been maintained and weare facing a drug problem every bit as seri-ous as 10 years ago and a lot more complex.
Following this year’s election, Citywidewelcomed the return of a full-time ministeri-al position with responsibility for drugs. Ifthe Government is serious we must see:■ An immediate mandate to be given to Lo-cal Drugs Task Forces to draw up new plansto respond to the changing drug problems.■ A commitment to Regional Drugs TaskForces that work on new plans will begin in2008 so that they can respond to the rapidlychanging situation in the regions.■ Allocation of an adequate budget for theimplementation of the Report on Drugs Re-habilitation in 2008.■ Full implementation of the actions in theNational Drugs Strategy by the target date ofend 2008.
■ Anna Quigley is co-ordinator of the City-wide Drugs Crisis Campaign
The number of drug seizures have risen, from 5,603 in 2002 to 7,550 last year.
A NEW GLOBAL TRENDDespite greater numbers of seizures, the price ofdrugs has actually fallen, writes Cormac O’KeeffeI T APPEARS a bit baffling. Every
second day comes news of anoth-er major drugs haul.
But the seizures never seem tohave any effect on availability. If
anything, availability has grown in recentyear s.
Prices, often considered a good indica-tion of availability, have not risen. Thisshould happen if supply is being squeezedby seizures. If anything, prices have fallen.
This picture is not peculiar to Ireland —it is replicated across Europe and globally.
All the official figures here point togreater and greater successes by gardaí andCustoms. The number of drug seizureshave risen, from 5,603 in 2002 to 7,550 lastyea r.
The volume of drugs seized has alsojumped in most cases over the same period.
Seizures of cannabis resin rose from threetonnes to seven tonnes. Hauls of heroinjumped from 17kg to 128kg. The volumeof cocaine intercepted rose from 32kg to190kg.
“Seizures don’t stop supply,” said Detec-tive Chief Superintendent Cormac Gordonof the Garda National Drugs Unit(GNDU).
He said the GNDU carried out researchin the Clondalkin area of west Dublin inOctober 2006 following the seizure of54kg of heroin by a city centre drug unit inthe area — the single-biggest seizure ofheroin in the history of the State.
“We checked the implications and wefound it had no effect on street dealing oron prices. There was no apparent differencein supply or availability.”
This trend is reflected across Europe. Re-search published by the European Monitor-ing Centre for Drugs and Drug Addiction(EMCDDA) found despite greater seizures,the prices of drugs had actually fallen acrossthe continent.
Commenting, the head of the EuropeanCommission drug policy unit, Carel Ed-wards, said: “What this seems to suggest isthat a lot more drugs are in the system thanwe estimated. If increased seizures are nothaving an effect on prices, indeed priceshave come down, whatever we are seizingis not hitting the market.”
The United Nations estimated that 42%of all cocaine traffic was intercepted in2006, almost twice the amount seized in2002. But despite this, the UN said theconsumption of the drug had increased sig-nificantly in Europe, doubling or tripling inseveral countries. Ireland was among the
world’s top five countries with “large in-creases” in cocaine use.
A British Home Office study estimatedthat to have a significant effect, law en-forcement authorities would need to inter-cept about 80% of all drugs in the system.
UN figures show more than 220,000acres were under coca cultivation in 2000,which had a potential to manufacture 880metric tonnes of cocaine.
By 2006, the area under cultivation fellby 30% to 157,000, but the potential man-ufacture increased to over 980 metrictonnes.
The bulk of cocaine from South Americaenters Europe through Spain, Portugal andthe Netherlands. In a new trend, manyshipments are stopping along the relativelyun-policed West African coast for onwarddelivery to Europe.
West African gangs have become majorplayers in global trafficking and have re-cruited Eastern Europeans to carry thedrug through European airports, includingthose in Ireland.
“Cocaine is the drug of choice at themoment,” said Chief Gordon. “Europe issecond after the US for cocaine use. Therehas been a rise of 10% each year in recentyears in Europe.”
The mushrooming of flights to Spain andacross Europe has increased the opportunityfor criminals to make contact with suppli-er s.
The expansion of the EU has meant thatmore and more people can fly around theEU without impediment. Under EU law,customs officers can’t stop people flyingwithin the EU without having prior suspi-cion. Official figures show that 28 millionpeople flew into Irish airports in 2006.
In addition to the threat to Irish airportsand ports, there is an unknown level oftrafficking along the isolated Irish coastline.
Last July, more than €110m worth of co-caine was accidentally found off the westCork coast, while last September €1.4mworth of cannabis resin was found off theAran Islands.
Customs and Garda drug units operate
on the basis of intelligence and surveillanceas well as tip-offs from sources, includingpeople in the drug trade.
They also receive information throughgreater co-operation with law enforcementauthorities in other EU states. The GNDUhas liaison officers in several key countries,including Spain and the Netherlands. TheGNDU and Customs also have officers inE u ropol.
Last September, a new EU agency wasset up to combat drug trafficking, particu-larly cocaine, through European waters, ofwhich 16% are in the Irish zone.
The UN has repeatedly warned aboutgreater production of heroin fromAfghanistan, which is resulting in greateravailability of the drug and higher puritylevels, posing a risk to users.
“Last year, the volume of heroin seizedwas more than four times that of the previ-ous year,” said Chief Gordon. “There is in-creased demand for it nationally. We hadestablished heroin problems in areas likeAthlone, but in the last 18 months increas-
ing amounts of heroin have been seized inGalway, Cork and elsewhere.”
Chief Gordon said there was “an increas-ing number of people” involved in drugtrafficking, facilitated by vastly expandedtravel opportunities and attracted by possi-ble substantial profits.
He said criminal organisations involved intrafficking were more loosely structuredthan depicted in the media. He said a num-ber of Irish players act as facilitators forgangs. “They put people in contact withother people. They know ways and meansof bringing drugs in.”
He said there were a large number ofIrish people based in Spain — who haveeither fled on warrants or to escape theCriminal Assets Bureau — who have madeconnections with local suppliers. He saidthere are people between the suppliersabroad and the gangs in Ireland who are“generally not known” to the authorities.
“They could be individuals employed bylegitimate companies or individuals in theirown right who transport goods.”
He said drug trafficking gangs here oper-ate a fairly sophisticated business.
“They bring in large quantities withoutdetection, they store them, manage the dis-tribution of them at different levels. Theremight be half a dozen people below themain guy, each of them might have four tofive people below them.
“Drugs is run like a business, but it isbased on fear and threat. If someone owesmoney they might distribute the next loadto work off the debt.”
The GNDU and the Customs DrugsLaw Enforcement Team, conduct constantoperations against traffickers, often jointly.Other garda units, including the NationalBureau of Criminal Investigation also targetdrug gangs.
As well as national operations, theGNDU, along with local gardaí, conductundercover operations in local areas.
Last June, Operation Scarf resulted in thearrest of 11 suspected heroin and cocainedealers in Galway. The previous month,Operation Fossil saw the arrest of 18 sus-
pected heroin and cocaine dealers in Tal-laght, Dublin.
Operation Anvil, which runs nationwide,targets serious gangs and gun crime, muchof it linked to the drugs trade.
The CAB targets the assets and incomeof drug traffickers and other criminals andis increasingly examining lower level dealersin Dublin and in the regions.
Both the CAB and the GNDU reportgangs are becoming more sophisticated inlaundering their money.
Chief Gordon said they are seizing a lotof cash where they expect to find drugsand that there are over 20 forfeiture ordersin the courts. He said many gangs aresmuggling the cash out of the country andspend it elsewhere in the euro-zone.
He said while seizures don’t stop the sup-ply of drugs, they do have an impact.
“You are taking an illegal commodity outof the market. There are effects on thepeople involved. They are out of pocket fora while. It may lead to a prosecution andconv ic t ion.”
Members of the Baltimorelifeboat going dangerously close
to shore to recover the large€110m haul of cocaine that was
found in the sea near MizenHead, in Dunlough Bay, Co Cork.
Picture: Richard Mills
THE CAMPAIGNER
SUPPLY AND CONTROLTHE INDUSTRY
14 NOVEMBER 20, 2007
TERAPROOF:User:jackiebolandDate:16/11/2007 Time:18:17:17 Edition: 20/11/2007 ExSupplement XS2011DRUGSPage:15Zone:XS1
Minister of StatePat Carey on what isneeded to beat drugab u s e
Far from the cosy world of recreational drugs is a grim,savage reality, writes Cormac O’Keeffe
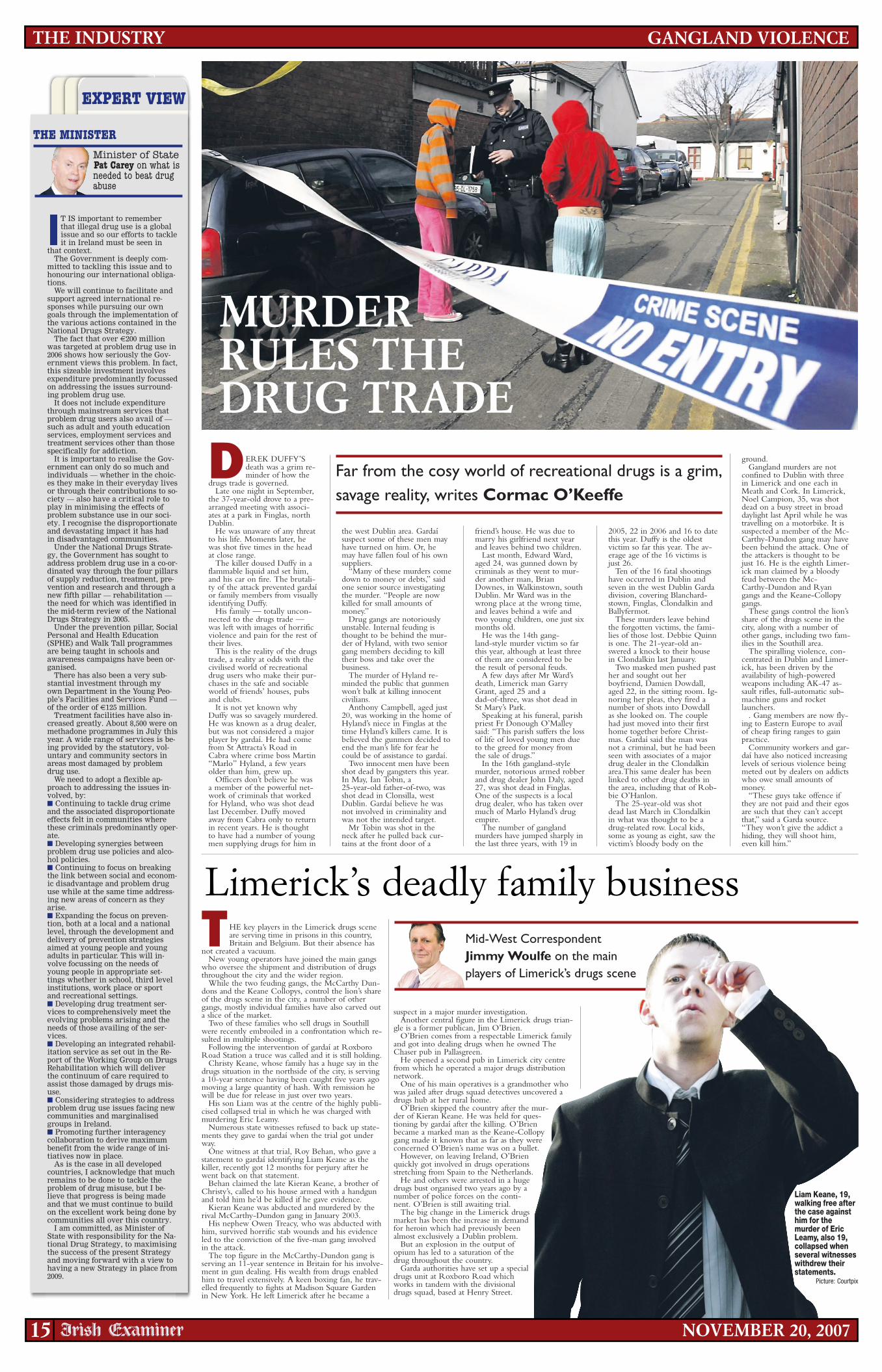
D EREK DUFFY’Sdeath was a grim re-minder of how the
drugs trade is governed.Late one night in September,
the 37-year-old drove to a pre-arranged meeting with associ-ates at a park in Finglas, northD u blin.
He was unaware of any threatto his life. Moments later, hewas shot five times in the headat close range.
The killer doused Duffy in aflammable liquid and set him,and his car on fire. The brutali-ty of the attack prevented gardaíor family members from visuallyidentifying Duffy.
His family — totally uncon-nected to the drugs trade —was left with images of horrificviolence and pain for the rest oftheir lives.
This is the reality of the drugstrade, a reality at odds with thecivilised world of recreationaldrug users who make their pur-chases in the safe and sociableworld of friends’ houses, pubsand clubs.
It is not yet known whyDuffy was so savagely murdered.He was known as a drug dealer,but was not considered a majorplayer by gardaí. He had comefrom St Attracta’s Road inCabra where crime boss Martin“Marlo” Hyland, a few yearsolder than him, grew up.
Officers don’t believe he wasa member of the powerful net-work of criminals that workedfor Hyland, who was shot deadlast December. Duffy movedaway from Cabra only to returnin recent years. He is thoughtto have had a number of youngmen supplying drugs for him in
the west Dublin area. Gardaísuspect some of these men mayhave turned on him. Or, hemay have fallen foul of his ownsupplier s.
“Many of these murders comedown to money or debts,” saidone senior source investigatingthe murder. “People are nowkilled for small amounts ofmoney.”
Drug gangs are notoriouslyunstable. Internal feuding isthought to be behind the mur-der of Hyland, with two seniorgang members deciding to killtheir boss and take over thebu s ine s s .
The murder of Hyland re-minded the public that gunmenwon’t balk at killing innocentciv ilian s .
Anthony Campbell, aged just20, was working in the home ofHyland’s niece in Finglas at thetime Hyland’s killers came. It isbelieved the gunmen decided toend the man’s life for fear hecould be of assistance to gardaí.
Two innocent men have beenshot dead by gangsters this year.In May, Ian Tobin, a25-year-old father-of-two, wasshot dead in Clonsilla, westDublin. Gardaí believe he wasnot involved in criminality andwas not the intended target.
Mr Tobin was shot in theneck after he pulled back cur-tains at the front door of a
friend’s house. He was due tomarry his girlfriend next yearand leaves behind two children.
Last month, Edward Ward,aged 24, was gunned down bycriminals as they went to mur-der another man, BrianDownes, in Walkinstown, southDublin. Mr Ward was in thewrong place at the wrong time,and leaves behind a wife andtwo young children, one just sixmonths old.
He was the 14th gang-land-style murder victim so farthis year, although at least threeof them are considered to bethe result of personal feuds.
A few days after Mr Ward’sdeath, Limerick man GarryGrant, aged 25 and adad-of-three, was shot dead inSt Mary’s Park.
Speaking at his funeral, parishpriest Fr Donough O’Malleysaid: “This parish suffers the lossof life of loved young men dueto the greed for money fromthe sale of drugs.”
In the 16th gangland-stylemurder, notorious armed robberand drug dealer John Daly, aged27, was shot dead in Finglas.One of the suspects is a localdrug dealer, who has taken overmuch of Marlo Hyland’s drugempi re.
The number of ganglandmurders have jumped sharply inthe last three years, with 19 in
2005, 22 in 2006 and 16 to datethis year. Duffy is the oldestvictim so far this year. The av-erage age of the 16 victims isjust 26.
Ten of the 16 fatal shootingshave occurred in Dublin andseven in the west Dublin Gardadivision, covering Blanchard-stown, Finglas, Clondalkin andBallyfer mot.
These murders leave behindthe forgotten victims, the fami-lies of those lost. Debbie Quinnis one. The 21-year-old an-swered a knock to their housein Clondalkin last January.
Two masked men pushed pasther and sought out herboyfriend, Damien Dowdall,aged 22, in the sitting room. Ig-noring her pleas, they fired anumber of shots into Dowdallas she looked on. The couplehad just moved into their firsthome together before Christ-mas. Gardaí said the man wasnot a criminal, but he had beenseen with associates of a majordrug dealer in the Clondalkinarea.This same dealer has beenlinked to other drug deaths inthe area, including that of Rob-bie O’Hanlon.
The 25-year-old was shotdead last March in Clondalkinin what was thought to be adrug-related row. Local kids,some as young as eight, saw thevictim’s bloody body on the
g round.Gangland murders are not
confined to Dublin with threein Limerick and one each inMeath and Cork. In Limerick,Noel Campion, 35, was shotdead on a busy street in broaddaylight last April while he wastravelling on a motorbike. It issuspected a member of the Mc-Carthy-Dundon gang may havebeen behind the attack. One ofthe attackers is thought to bejust 16. He is the eighth Limer-ick man claimed by a bloodyfeud between the Mc-Carthy-Dundon and Ryangangs and the Keane-Collopygangs.
These gangs control the lion’sshare of the drugs scene in thecity, along with a number ofother gangs, including two fam-ilies in the Southill area.
The spiralling violence, con-centrated in Dublin and Limer-ick, has been driven by theavailability of high-poweredweapons including AK-47 as-sault rifles, full-automatic sub-machine guns and rocketlauncher s.
. Gang members are now fly-ing to Eastern Europe to availof cheap firing ranges to gainp r ac t ice.
Community workers and gar-daí have also noticed increasinglevels of serious violence beingmeted out by dealers on addictswho owe small amounts ofmoney.
“These guys take offence ifthey are not paid and their egosare such that they can’t acceptthat,” said a Garda source.“They won’t give the addict ahiding, they will shoot him,even kill him.”
MURDERRULES THEDRUG TRADE
Mid-West CorrespondentJimmy Woulfe on the mainplayers of Limerick’s drugs scene
THE key players in the Limerick drugs sceneare serving time in prisons in this country,Britain and Belgium. But their absence has
not created a vacuum.New young operators have joined the main gangs
who oversee the shipment and distribution of drugsthroughout the city and the wider region.
While the two feuding gangs, the McCarthy Dun-dons and the Keane Collopys, control the lion’s shareof the drugs scene in the city, a number of othergangs, mostly individual families have also carved outa slice of the market.
Two of these families who sell drugs in Southillwere recently embroiled in a confrontation which re-sulted in multiple shootings.
Following the intervention of gardaí at RoxboroRoad Station a truce was called and it is still holding.
Christy Keane, whose family has a huge say in thedrugs situation in the northside of the city, is servinga 10-year sentence having been caught five years agomoving a large quantity of hash. With remission hewill be due for release in just over two years.
His son Liam was at the centre of the highly publi-cised collapsed trial in which he was charged withmurdering Eric Leamy.
Numerous state witnesses refused to back up state-ments they gave to gardaí when the trial got underw a y.
One witness at that trial, Roy Behan, who gave astatement to gardaí identifying Liam Keane as thekiller, recently got 12 months for perjury after hewent back on that statement.
Behan claimed the late Kieran Keane, a brother ofChristy’s, called to his house armed with a handgunand told him he’d be killed if he gave evidence.
Kieran Keane was abducted and murdered by therival McCarthy-Dundon gang in January 2003.
His nephew Owen Treacy, who was abducted withhim, survived horrific stab wounds and his evidenceled to the conviction of the five-man gang involvedin the attack.
The top figure in the McCarthy-Dundon gang isserving an 11-year sentence in Britain for his involve-ment in gun dealing. His wealth from drugs enabledhim to travel extensively. A keen boxing fan, he trav-elled frequently to fights at Madison Square Gardenin New York. He left Limerick after he became a
suspect in a major murder investigation.Another central figure in the Limerick drugs trian-
gle is a former publican, Jim O’Brien.O’Brien comes from a respectable Limerick family
and got into dealing drugs when he owned TheChaser pub in Pallasgreen.
He opened a second pub in Limerick city centrefrom which he operated a major drugs distributionne t wo r k.
One of his main operatives is a grandmother whowas jailed after drugs squad detectives uncovered adrugs hub at her rural home.
O’Brien skipped the country after the mur-der of Kieran Keane. He was held for ques-tioning by gardaí after the killing. O’Brienbecame a marked man as the Keane-Collopygang made it known that as far as they wereconcerned O’Brien’s name was on a bullet.
However, on leaving Ireland, O’Brienquickly got involved in drugs operationsstretching from Spain to the Netherlands.
He and others were arrested in a hugedrugs bust organised two years ago by anumber of police forces on the conti-nent. O’Brien is still awaiting trial.
The big change in the Limerick drugsmarket has been the increase in demandfor heroin which had previously beenalmost exclusively a Dublin problem.
But an explosion in the output ofopium has led to a saturation of thedrug throughout the country.
Garda authorities have set up a specialdrugs unit at Roxboro Road whichworks in tandem with the divisionaldrugs squad, based at Henry Street.
Limerick’s deadly family business
GANGLAND VIOLENCETHE INDUSTRY
15 NOVEMBER 20, 2007
EXPERT VIEW
THE MINISTER
IT IS important to rememberthat illegal drug use is a globalissue and so our efforts to tackleit in Ireland must be seen in
that context.The Government is deeply com-
mitted to tackling this issue and tohonouring our international obliga-t ion s.
We will continue to facilitate andsupport agreed international re-sponses while pursuing our owngoals through the implementation ofthe various actions contained in theNational Drugs Strategy.
The fact that over €200 millionwas targeted at problem drug use in2006 shows how seriously the Gov-ernment views this problem. In fact,this sizeable investment involvesexpenditure predominantly focussedon addressing the issues surround-ing problem drug use.
It does not include expenditurethrough mainstream services thatproblem drug users also avail of —such as adult and youth educationservices, employment services andtreatment services other than thosespecifically for addiction.
It is important to realise the Gov-ernment can only do so much andindividuals — whether in the choic-es they make in their everyday livesor through their contributions to so-ciety — also have a critical role toplay in minimising the effects ofproblem substance use in our soci-ety. I recognise the disproportionateand devastating impact it has hadin disadvantaged communities.
Under the National Drugs Strate-gy, the Government has sought toaddress problem drug use in a co-or-dinated way through the four pillarsof supply reduction, treatment, pre-vention and research and through anew fifth pillar — rehabilitation —the need for which was identified inthe mid-term review of the NationalDrugs Strategy in 2005.
Under the prevention pillar, SocialPersonal and Health Education(SPHE) and Walk Tall programmesare being taught in schools andawareness campaigns have been or-ganised.
There has also been a very sub-stantial investment through myown Department in the Young Peo-ple’s Facilities and Services Fund —of the order of €125 million.
Treatment facilities have also in-creased greatly. About 8,500 were onmethadone programmes in July thisyear. A wide range of services is be-ing provided by the statutory, vol-untary and community sectors inareas most damaged by problemdrug use.
We need to adopt a flexible ap-proach to addressing the issues in-volved, by:■ Continuing to tackle drug crimeand the associated disproportionateeffects felt in communities wherethese criminals predominantly oper-at e.■ Developing synergies betweenproblem drug use policies and alco-hol policies.■ Continuing to focus on breakingthe link between social and econom-ic disadvantage and problem druguse while at the same time address-ing new areas of concern as theya r i s e.■ Expanding the focus on preven-tion, both at a local and a nationallevel, through the development anddelivery of prevention strategiesaimed at young people and youngadults in particular. This will in-volve focussing on the needs ofyoung people in appropriate set-tings whether in school, third levelinstitutions, work place or sportand recreational settings.■ Developing drug treatment ser-vices to comprehensively meet theevolving problems arising and theneeds of those availing of the ser-v ice s.■ Developing an integrated rehabil-itation service as set out in the Re-port of the Working Group on DrugsRehabilitation which will deliverthe continuum of care required toassist those damaged by drugs mis-u s e.■ Considering strategies to addressproblem drug use issues facing newcommunities and marginalisedgroups in Ireland.■ Promoting further interagencycollaboration to derive maximumbenefit from the wide range of ini-tiatives now in place.
As is the case in all developedcountries, I acknowledge that muchremains to be done to tackle theproblem of drug misuse, but I be-lieve that progress is being madeand that we must continue to buildon the excellent work being done bycommunities all over this country.
I am committed, as Minister ofState with responsibility for the Na-tional Drug Strategy, to maximisingthe success of the present Strategyand moving forward with a view tohaving a new Strategy in place from2009.
Liam Keane, 19,walking free afterthe case againsthim for themurder of EricLeamy, also 19,collapsed whenseveral witnesseswithdrew theirstatements.
Picture: Courtpix

User:jackiebolandDate:16/11/2007 Time:18:16:40 Edition:20/11/2007 ExSupplement XS2011DRUGSPage:16 Color:
USER’S STORY: What begins as child’s play ends in a lifetime struggle to get clean
NO WAY OUTConor Kane looks at drugs misuse in Clonmel wherea heroin epidemic is considered a possibility by some
L IKE most other largetowns, Clonmel has had itsshare of problems with
drugs over the years, but it’s only inthe last two years that the inexorabletide of heroin has started to washover the big estates, the hang-outs,the dark alleyways and the riversidenooks and crannies where surveil-lance can easily be evaded.
The prospect of large-scale heroinaddiction in the town is one thatwill be resisted by the professionals,who can see the roots of the prob-lem bedding down and can onlyhope that they will be weeded outbefore it’s too late.
However, some think it already istoo late. One recovering drug user,who experimented with smokingheroin in the past, but put a stop toher need before it progressed to in-jecting, predicts that, within a shortfew months, the heroin problemwill “blow up” around Clonmel.
“The amount of heroin that’saround the town is just unnatural.It’s going around like hash used tobe a few years ago,” she says. “It’sjust everywhere. The wrong peopleare taking it. That would be theworrying thing, I’d say, in Clonmel.”
While those who work withdrug-users and are in a position toobserve the trends as they changeover the years would be more mea-sured in their attitude, it’s generallyagreed that heroin has become morereadily available in the area, as hascocaine.
“I have to say, as a treatmentprovider, that there seems to be anincrease in cocaine and certainly anincrease in heroin,” says south Tip-perary substance misuse co-ordina-tor Johnny Casey. “We’re not seeingit in clients here, but that may bebecause they’re out there having toomuch of a good time and it’s not aserious issue for them yet. Anecdo-tally, I know from clients who tell usabout the availability, and we knowto some degree from the generalhospital services and the GPs.”
The substance misuse centre inClonmel, where counselling andmany other support services areavailable, has gone from a positionof having no heroin users on itsbooks a couple of years ago, to hav-ing a small but measurable amountnow. And, it’s reckoned, for everyuser that comes into a clinic orcounselling service looking for help,there could be three more out onthe streets.
One professional who works inthe field, who didn’t want to benamed, told the Irish Examiner thatcertain sections of local authorityhousing estates in the town are“flooded with heroin” and that
young people are using each other’shouses to shoot up.
There’s a growing belief that thetown’s proximity to Limerick isleading to certain elements of theLimerick crime scene setting upshop in Clonmel and using it as an“outsourced” market, as well as aconvenient trading post — 50 milesfrom Limerick, 30 miles from Wa-terford, 60 from Cork and 100 fromD u blin.
“There is a Limerick connection,we’d certainly see that,” said asource. “There’s a lot of weaponsaround and that’s where they’recoming from, and then you havetwo big factions against each other.”Some criminals who originated in
Limerick have already made theirway to the local courts. However,gardaí claim there is no evidence toback this up and play down any talkof a heroin epidemic.
Accepting that heroin has begunto make its presence felt in the last18 months, the garda spokesmansaid Clonmel was no worse than anyother town in this regard and gardaíhave made a number of heroinseizures recently which should helpto stem the flow.
Cocaine has become much morepopular, he pointed out, whilecannabis remains “the drug ofchoice” for the majority of users.
Gardaí say there are sufficient re-sources to fight the supply of thedrugs, but a multi-agency approach
is needed to deal with demand, witheducation top of the list.
Hilery Condron of the ClonmelCommunity-Based Drugs Projectagrees that heroin is “creeping intothe town”, particularly in the last 12months. “Smoking heroin is thebiggest concern we have at the mo-ment. That’s coming from the factthat it was inevitable it was going tohappen at some point. What I’mseeing on the ground is smokingheroin and it’s about eight monthsto a year before it gets quite bad andyou end up injecting. This summerit really started to dominate.”
If the problem isn’t dealt with, shesaid, it could be at epidemic propor-tions five or six years down the line.
But how can it be dealt with?“Methadone and needle exchange,that’s the way Dublin is dealing withit. If they’re coming in, they’relooking for methadone. They’re notcoming in for a cup of tea and acha t .”
Official figures for 2006 show15.6% of drug users seen at centresacross south Tipperary were onheroin, with three-quarters of thosefrom Clonmel. The main drug ofchoice remains cannabis (51.9%),but the worrying thing for those atthe coalface is that heroin use, whilestill relatively low in the area, wasnon-existent not too long ago.
Cocaine use was present in 7.8%of drug-users who presented them-selves at service-providers last year,
also up from a low base but not yetswamping the toilet-cisterns andkitchen marble-tops of middle-classsociety, presented as the reality insome parts of Ireland.
Meanwhile, the ecstasy situationmoves in cycles, but is thought tohave peaked some years ago in thearea, with cocaine becoming moreaffordable and heroin more available.
Meanwhile, Johnny Casey likensthe drugs trade to a pyramid-sellingscheme, where each small-time sup-plier in a community buys from alarger-scale supplier somewhere upthe line, who in turn is receivingfrom an even bigger player, and soon. Often, removing one small linkin the chain makes little difference.
“It’s pyramid-selling at its best, andif you have that system, how do youbreak it down? There’s not an awfullot to be gained by sending some-one away for one or two years fors u ppl y.”
As with many towns and cities,drug use tends to be focused on de-prived areas and, in Clonmel, this isas much the case as in any other ur-ban centre. Two areas in particularcome up in conversation when peo-ple talk about drug problems: ElmPark and The Wilderness, two largelocal authority estates which havesuffered their share of woe in thepast. Both communities have activeresidents’ associations, supported byofficial agencies, but can do littlewhen groups of young people set
upon getting involved in the use,and then supply, of illegal sub-stances. Indeed, in the past, differentgangs have set themselves up as ri-vals between the two estates — evenusing the pages of the Bebo websiteto trumpet their “feud” — but thishas been overblown and suchself-publicising is often more aboutbravado than real territory-marking.Those really involved in the tradetend to keep a lower profile.
However, much remains to bedone. The Clonmel Communi-ty-based Drugs Project at TheWilderness is an oasis of sorts, aclean, respected base for many ser-vices which are available to anyonewho wants to drop in, run by com-
mitted staff and volunteers.Yet it’s difficult to escape the set-
ting. Outside, over the fence whichseparates the project HQ’s groundsfrom the rest of The Wilderness, re-mains the typical urban decay oftelevision cliché. Rubbish strewnacross a green area, old vehiclesabandoned, boarded-up houses andyoungsters wandering aimlessly. De-spite the best will in the world frommany residents, Ireland’s recent pros-perity hasn’t had the desired effectsin these pockets of our towns.
As one person involved in thedrugs project puts it, staring acrossthe bleak wasteland on this edge ofClonmel: “You look out and see thereality of it. What the fuck is goingon in this country?”
Hillary Condron, Jenny Ryan, Audrey Cotter and Catherine Guerin,community drugs workers at the Wilderness Centre, Clonmel.
Hillary Condron, community drugs worker, Wilderness Youth andCommunity Centre, Wilderness Grove, Clonmel.
Clonmel, where arecovering user says the
amount of heroin in use issimilar to the levels of
cannabis a few years ago.Pictures: Patrick Browne jnr
Drug usersare startingyoungerConor Kane talks tomembers of supportservices in Clonmel
ALL those involved with treating drugusers and trying to break the viciouscircle of substance abuse agree that theage profile of drug users in the Clon-mel area is getting younger.
USERS AS YOUNG AS 16
With ecstasy available for as little as€2.50 per tablet, cannabis cheaperthan ever and more money floatingaround, that’s probably no surprise.“An average young lad going outwould get plenty for €15 [euro],” saysHilery Condron of the Clonmel Com-munity Based Drugs Project.
Voluntary drugs youth workerAudrey Cotter, based at the Wildernesslocal authority estate, says drug usersare coming in as young as 16, most ofthem having started off onalcohol and progressed to cannabis —possibly via glue or aerosol-sniffing.
“Cannabis would be very prevalent,”she says, “and cocaine is getting hereand it’s getting here hard and fast.”
SOMEWHERE TO TURN
Seeing the damage caused by drugabuse, Hilery says that it’s important tohave a presence in the communitywhich can be a first contact point forthose seeking help, or for those tryingto stay away from drugs: “We’re herefor the benefit of the young adults thatuse the service. We’re not going toquestion where they get it from orwhere it comes from. The priority isthem, helping them.”
FAMILY TIES ARE KEY
Hilery Condron, who has worked inthe field for 13 years, says relationshipsand trust within families is key tokeeping young people away fromdrugs: “Once the relationship is bro-ken, then the child is at sea. Sometimeschildren just need an excuse to getaway from doing drugs, so that theydon’t look like a geek. If a child comeshome and says, ‘all my friends aresmoking hash’, and they’re looking fora reason not to, if you say to them totell their friends you’re not allowed be-cause your mam is a lunatic and she in-sists on a weekly urine test, sometimesthey could be delighted with that.They’re just looking for a way out.”
ALCOHOL THE GATEWAY
Alcohol is widely seen as the biggestgateway drug, with up to 90% of thosewho come into the state and voluntaryservices with drug problems havingstarted off by drinking.
Clonmel-based substance misuseco-ordinator Johnny Casey said: “I’dargue with anyone that our biggestproblem in this country and in southTipperary is alcohol, still. If you wantto talk about your main gateway sub-stance, then alcohol is your main gate-w a y.”
But, for young children, it can alsostart with substances as apparently in-nocent as a can of ‘squirty cream’.
What it has in common with house-hold items such as spray polish and de-odorant is butane gas.
“Unfortunately it stops the oxygengoing to the brain and literally onedose of it could kill you. Within amatter of seconds, they could becomevery drunk, they could black out. It’squite instant. A side effect can bedeath,” explains Ms Condron.
CAUSE AND TREATMENT
The point about easy drug availabili-ty in this day and age is echoed by MrCa s ey.
“It’s available pretty much anywhere.There’s a normalisationof drug use among the youth culturetoday, in that many young people areaware of what’s available and where it’savailable and whose selling it.”
The substance misuse centre in PeterStreet, Clonmel, has been widelypraised for its work in helping drugusers, while the HSE-run CoolgreaneyHouse at Queen Street in the townconcentrates on mental health issuessurrounding alcohol and addiction,with inevitable overlaps.
■ Clonmel Community-BasedDrugs Project, The Wilderness,Clonmel■ South Tipperary Outreach DrugsProject, 052-76871.■ South Tipperary Substance Mis-use Centre, Peter Street, Clonmel,052-77900.■ Coolgreaney House Alcohol andAddiction Service, Queen Street,Clonmel, 052-26533.■ HSE (south-east), Western Road,Clonmel, 052-77000.
USEFUL NUMBERS
16 NOVEMBER 20, 2007
CLONMELVIEW FROM THE GROUND
“I WAS using for about 13 years, fromabout the age of 13. It just started off, likewith most other children, with experiment-ing.
“There was a lot of us together and we allstarted at the same time. We started offsmoking and then we used to sniff glue oraerosols, and then we all started smokingdope together. That would have been be-fore first year in secondary school. The old-er lads would have been selling it.
“It was just something to do. Therewasn’t much else. It’s very different today— there was no services in place back then.You came from a shit area and stayed in ashit area and that was it. My parents weredealing with their own stuff at that time aswell and it was just a very different life.
“I grew up in a corporation estate in Clon-mel and neither of my parents was workingfull-time. There was addiction in the familyanyway, not that we knew it as addiction atthe time. But it wasn’t a healthy, normalchildhood.
“It wasn’t just hash. There was magicmushrooms if you couldn’t get your handson dope or you hadn’t any money. Then wemoved on slowly to acid, LSD, Es, whatev-er. You just move on to what’s in fashion.Hash was always available, that neverstopped. Anything else is usually availablein Clonmel.
“I never started robbing or anything likethat. I was a single mother when I was 16and that was late for my group because oneof the girls had her first child in second
year, so I had my [social welfare] book ev-ery week and the children’s allowance. Iwas never in full-time employment. Therewas always little jobs you’d pick up nowand then.
“The baby was fine, health-wise, but withme there was just one bad relationshipafter another. I was never in full-timeemployment, just being able to get by.
“I smoked heroin, never injected it. Iwould know the scene well in Clonmel andI’d see the gaps in the services.
“There’s nowhere for the lads who are us-ing downtown to drop in when they’restrung out. They’re sitting down on thequay and drinking and trying to come off it.I grew up with most of these people. You’rejust depending on other people or volun-
teers in the service. It’s not enough.“I’m in recovery myself. I’ve been
going to the community-based drugproject for about two years. I just had tostop. I would have been injecting otherwiseand then I’d have lost everything and every-one would have known.
“ If you’re really serious about it, you’llgive it a try. I’m at a different stage of mylife as well. You never say you’rerecovered, but getting there. I hope I amanyway.
“In Clonmel, I think in a few months’ timeit’s going to completely blow up. Theamount of heroin that’s around the town isjust unnatural. It’s going around like hashused to a few years ago. It’s just every-where.”
TERAPROOF:User:jackiebolandDate:16/11/2007 Time:18:23:42 Edition: 20/11/2007 ExSupplement XS2011DRUGSPage:17 Zone:XS1
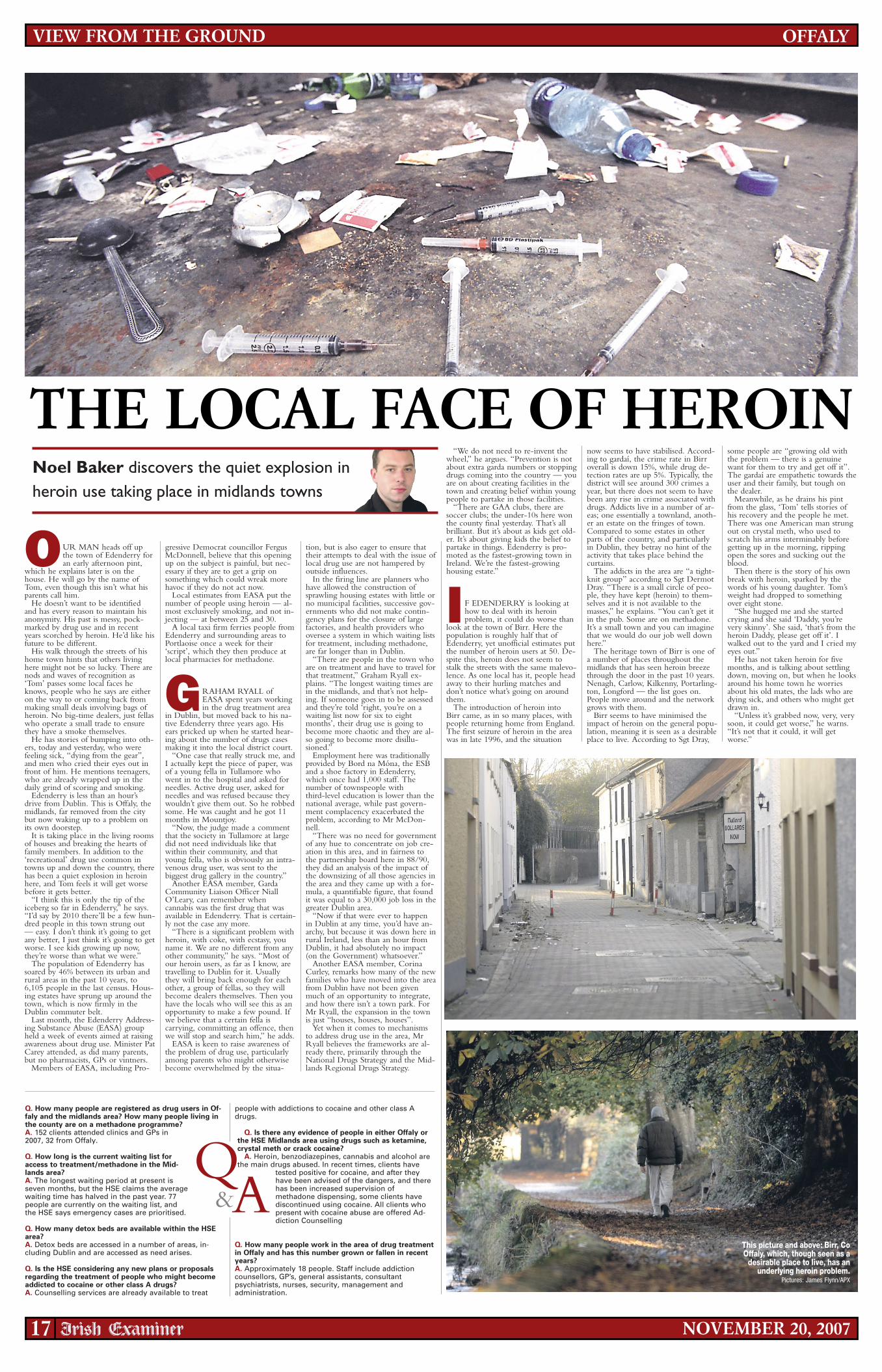
THE LOCAL FACE OF HEROINNoel Baker discovers the quiet explosion inheroin use taking place in midlands towns
17 NOVEMBER 20, 2007
OFFALYVIEW FROM THE GROUND
This picture and above: Birr, CoOffaly, which, though seen as a
desirable place to live, has anunderlying heroin problem.
Pictures: James Flynn/APX
OUR MAN heads off upthe town of Edenderry foran early afternoon pint,
which he explains later is on thehouse. He will go by the name ofTom, even though this isn’t what hisparents call him.
He doesn’t want to be identifiedand has every reason to maintain hisanonymity. His past is messy, pock-marked by drug use and in recentyears scorched by heroin. He’d like hisfuture to be different.
His walk through the streets of hishome town hints that others livinghere might not be so lucky. There arenods and waves of recognition as‘Tom’ passes some local faces heknows, people who he says are eitheron the way to or coming back frommaking small deals involving bags ofheroin. No big-time dealers, just fellaswho operate a small trade to ensurethey have a smoke themselves.
He has stories of bumping into oth-ers, today and yesterday, who werefeeling sick, “dying from the gear”,and men who cried their eyes out infront of him. He mentions teenagers,who are already wrapped up in thedaily grind of scoring and smoking.
Edenderry is less than an hour’sdrive from Dublin. This is Offaly, themidlands, far removed from the citybut now waking up to a problem onits own doorstep.
It is taking place in the living roomsof houses and breaking the hearts offamily members. In addition to the‘recreational’ drug use common intowns up and down the country, therehas been a quiet explosion in heroinhere, and Tom feels it will get worsebefore it gets better.
“I think this is only the tip of theiceberg so far in Edenderry,” he says.“I’d say by 2010 there’ll be a few hun-dred people in this town strung out— easy. I don’t think it’s going to getany better, I just think it’s going to getworse. I see kids growing up now,they’re worse than what we were.”
The population of Edenderry hassoared by 46% between its urban andrural areas in the past 10 years, to6,105 people in the last census. Hous-ing estates have sprung up around thetown, which is now firmly in theDublin commuter belt.
Last month, the Edenderry Address-ing Substance Abuse (EASA) groupheld a week of events aimed at raisingawareness about drug use. Minister PatCarey attended, as did many parents,but no pharmacists, GPs or vintners.
Members of EASA, including Pro-
gressive Democrat councillor FergusMcDonnell, believe that this openingup on the subject is painful, but nec-essary if they are to get a grip onsomething which could wreak morehavoc if they do not act now.
Local estimates from EASA put thenumber of people using heroin — al-most exclusively smoking, and not in-jecting — at between 25 and 30.
A local taxi firm ferries people fromEdenderry and surrounding areas toPortlaoise once a week for their‘script’, which they then produce atlocal pharmacies for methadone.
GRAHAM RYALL ofEASA spent years workingin the drug treatment area
in Dublin, but moved back to his na-tive Edenderry three years ago. Hisears pricked up when he started hear-ing about the number of drugs casesmaking it into the local district court.
“One case that really struck me, andI actually kept the piece of paper, wasof a young fella in Tullamore whowent in to the hospital and asked forneedles. Active drug user, asked forneedles and was refused because theywouldn’t give them out. So he robbedsome. He was caught and he got 11months in Mountjoy.
“Now, the judge made a commentthat the society in Tullamore at largedid not need individuals like thatwithin their community, and thatyoung fella, who is obviously an intra-venous drug user, was sent to thebiggest drug gallery in the country.”
Another EASA member, GardaCommunity Liaison Officer NiallO’Leary, can remember whencannabis was the first drug that wasavailable in Edenderry. That is certain-ly not the case any more.
“There is a significant problem withheroin, with coke, with ecstasy, youname it. We are no different from anyother community,” he says. “Most ofour heroin users, as far as I know, aretravelling to Dublin for it. Usuallythey will bring back enough for eachother, a group of fellas, so they willbecome dealers themselves. Then youhave the locals who will see this as anopportunity to make a few pound. Ifwe believe that a certain fella iscarrying, committing an offence, thenwe will stop and search him,” he adds.
EASA is keen to raise awareness ofthe problem of drug use, particularlyamong parents who might otherwisebecome overwhelmed by the situa-
tion, but is also eager to ensure thattheir attempts to deal with the issue oflocal drug use are not hampered byoutside influences.
In the firing line are planners whohave allowed the construction ofsprawling housing estates with little orno municipal facilities, successive gov-ernments who did not make contin-gency plans for the closure of largefactories, and health providers whooversee a system in which waiting listsfor treatment, including methadone,are far longer than in Dublin.
“There are people in the town whoare on treatment and have to travel forthat treatment,” Graham Ryall ex-plains. “The longest waiting times arein the midlands, and that’s not help-ing. If someone goes in to be assessedand they’re told ‘right, you’re on awaiting list now for six to eightmonths’, their drug use is going tobecome more chaotic and they are al-so going to become more disillu-s ioned.”
Employment here was traditionallyprovided by Bord na Móna, the ESBand a shoe factory in Edenderry,which once had 1,000 staff. Thenumber of townspeople withthird-level education is lower than thenational average, while past govern-ment complacency exacerbated theproblem, according to Mr McDon-nell.
“There was no need for governmentof any hue to concentrate on job cre-ation in this area, and in fairness tothe partnership board here in 88/90,they did an analysis of the impact ofthe downsizing of all those agencies inthe area and they came up with a for-mula, a quantifiable figure, that foundit was equal to a 30,000 job loss in thegreater Dublin area.
“Now if that were ever to happenin Dublin at any time, you’d have an-archy, but because it was down here inrural Ireland, less than an hour fromDublin, it had absolutely no impact(on the Government) whatsoever.”
Another EASA member, CorinaCurley, remarks how many of the newfamilies who have moved into the areafrom Dublin have not been givenmuch of an opportunity to integrate,and how there isn’t a town park. ForMr Ryall, the expansion in the townis just “houses, houses, houses”.
Yet when it comes to mechanismsto address drug use in the area, MrRyall believes the frameworks are al-ready there, primarily through theNational Drugs Strategy and the Mid-lands Regional Drugs Strategy.
“We do not need to re-invent thewheel,” he argues. “Prevention is notabout extra garda numbers or stoppingdrugs coming into the country — youare on about creating facilities in thetown and creating belief within youngpeople to partake in those facilities.
“There are GAA clubs, there aresoccer clubs; the under-10s here wonthe county final yesterday. That’s allbrilliant. But it’s about as kids get old-er. It’s about giving kids the belief topartake in things. Edenderry is pro-moted as the fastest-growing town inIreland. We’re the fastest-growinghousing estate.”
I F EDENDERRY is looking athow to deal with its heroinproblem, it could do worse than
look at the town of Birr. Here thepopulation is roughly half that ofEdenderry, yet unofficial estimates putthe number of heroin users at 50. De-spite this, heroin does not seem tostalk the streets with the same malevo-lence. As one local has it, people headaway to their hurling matches anddon’t notice what’s going on aroundthem.
The introduction of heroin intoBirr came, as in so many places, withpeople returning home from England.The first seizure of heroin in the areawas in late 1996, and the situation
now seems to have stabilised. Accord-ing to gardaí, the crime rate in Birroverall is down 15%, while drug de-tection rates are up 5%. Typically, thedistrict will see around 300 crimes ayear, but there does not seem to havebeen any rise in crime associated withdrugs. Addicts live in a number of ar-eas; one essentially a townland, anoth-er an estate on the fringes of town.Compared to some estates in otherparts of the country, and particularlyin Dublin, they betray no hint of theactivity that takes place behind thecur tains.
The addicts in the area are “a tight-knit group” according to Sgt DermotDray. “There is a small circle of peo-ple, they have kept (heroin) to them-selves and it is not available to themasses,” he explains. “You can’t get itin the pub. Some are on methadone.It’s a small town and you can imaginethat we would do our job well downhe re.”
The heritage town of Birr is one ofa number of places throughout themidlands that has seen heroin breezethrough the door in the past 10 years.Nenagh, Carlow, Kilkenny, Portarling-ton, Longford — the list goes on.People move around and the networkgrows with them.
Birr seems to have minimised theimpact of heroin on the general popu-lation, meaning it is seen as a desirableplace to live. According to Sgt Dray,
some people are “growing old withthe problem — there is a genuinewant for them to try and get off it”.The gardaí are empathetic towards theuser and their family, but tough onthe dealer.
Meanwhile, as he drains his pintfrom the glass, ‘Tom’ tells stories ofhis recovery and the people he met.There was one American man strungout on crystal meth, who used toscratch his arms interminably beforegetting up in the morning, rippingopen the sores and sucking out theblood.
Then there is the story of his ownbreak with heroin, sparked by thewords of his young daughter. Tom’sweight had dropped to somethingover eight stone.
“She hugged me and she startedcrying and she said ‘Daddy, you’revery skinny’. She said, ‘that’s from theheroin Daddy, please get off it’. Iwalked out to the yard and I cried myeyes out.”
He has not taken heroin for fivemonths, and is talking about settlingdown, moving on, but when he looksaround his home town he worriesabout his old mates, the lads who aredying sick, and others who might getdrawn in.
“Unless it’s grabbed now, very, verysoon, it could get worse,” he warns.“It’s not that it could, it will getwor se.”
Q. How many people are registered as drug users in Of-faly and the midlands area? How many people living inthe county are on a methadone programme?A. 152 clients attended clinics and GPs in2007, 32 from Offaly.
Q. How long is the current waiting list foraccess to treatment/methadone in the Mid-lands area?A. The longest waiting period at present isseven months, but the HSE claims the averagewaiting time has halved in the past year. 77people are currently on the waiting list, andthe HSE says emergency cases are prioritised.
Q. How many detox beds are available within the HSEarea?A. Detox beds are accessed in a number of areas, in-cluding Dublin and are accessed as need arises.
Q. Is the HSE considering any new plans or proposalsregarding the treatment of people who might becomeaddicted to cocaine or other class A drugs?A. Counselling services are already available to treat
people with addictions to cocaine and other class Adrugs.
Q. Is there any evidence of people in either Offaly orthe HSE Midlands area using drugs such as ketamine,crystal meth or crack cocaine?
A. Heroin, benzodiazepines, cannabis and alcohol arethe main drugs abused. In recent times, clients have
tested positive for cocaine, and after theyhave been advised of the dangers, and therehas been increased supervision ofmethadone dispensing, some clients havediscontinued using cocaine. All clients whopresent with cocaine abuse are offered Ad-diction Counselling
Q. How many people work in the area of drug treatmentin Offaly and has this number grown or fallen in recentyears?A. Approximately 18 people. Staff include addictioncounsellors, GP’s, general assistants, consultantpsychiatrists, nurses, security, management andadministration.
Q&A

TERAPROOF:User:jackiebolandDate:16/11/2007 Time:18:58:41Edition: 20/11/2007 ExSupplement XS2011DRUGSPage:18Zone:XS1
edged more by the communi-ties outside of Dublin that thisis not going to go away as anissue,” he says. “They couldlearn a lot from the local DrugsTask Forces in Dublin.
He says that waiting lists fortreatment are also a problem,particularly in some parts of thecountry, although a report intotreatment for under 18s, draftedsome years ago by the Depart-ment of Health and Children,and which outlined plans foradolescent specific services,would improve the current sit-uation, even if it is being“slowly funded and implement-ed”.
The APA organisers are re-ported to be considering an-other festival next year, andwill doubtless be hoping to at-tract more people in thegates. They are probablynot the only ones.
tradictory relationship with alco-hol, children and teenagers willbe provided with a readymaderoute into possible problems withother substances.
“Alcohol abuse is at the core,or a major drive, for substanceabuse,” he says, adding that par-ents are “increasingly tolerant” oftheir children’s drunkenness,which could actually be providingcamouflage for other problems, inaddition to weakening a person’sresolve and reasoning regardingthe taking of other substances.
Also significant is the gendershift which has seen a greaternumber of girls admitting to be-ing drunk, while there has been asimilar shift regarding the use ofcannabis.
At the sharper end, however, itseems the situation is not as grimas it once was. Dr Smyth admitsthat there are 14 and 15 year oldsusing heroin, but the numberspresenting with problems inDublin have fallen sharply. While200 people under the age of 18were known to have a heroinproblem in 1997, that figure hasdropped to between 10 and 15 —a level similar to that in the early‘90s.
“Heroin has a bad name andpeople have moved from it,” hesays, adding that the implementa-tion of aspects of the NationalDrugs Strategy were important inreducing the problem.
The number of under-18s whohave come forward with cocaineproblems has slowly risen since2000, however, although DrSmyth is wary of “overplaying”the situation. The most recentfigures for Dublin, dating from2004/2005, show no more thaneight under-18s presenting withcocaine problems, although thismay have risen since then.
“With cocaine they do not seethe drug as a huge problem forthemselves, they view it as a bitof fun,” he says.
“What can happen is they canend up in debt pretty quickly,getting into debts of thousands ofeuro in a few weeks. dealers canput them or their parents un-der pressure [to pay up].”
A number of these caseshave occurred and, ac-cording to Dr Smyth,from across the so-cio-economic spec-trum. To many par-ents the prospectof demands andthreats from un-savoury charac-ters is an “ut-terly alienwo r ld”.
More wor-rying again isthe growthof heroinuse amongteenager soutside ofD u blin.
“It has tobe acknowl-
Johnny Connolly t race sthe Irish drug marketto its global roots
IT HAS been claimed that theillicit drug market is now thethird most profitable in theworld, surpassed only by oil
and arms.The United Nations Office on
Drugs and Crime estimates that thewholesale value of the illicit drugmarket worldwide is US $94 billion(€64bn), compared with $24bn forwine and beer and $21.6bn fort obacco.
In Ireland, the number of heroinand cocaine seizures has increasedsignificantly so far this decade.
Heroin seizures rose from 598 in2000 to 1,115 in 2006. In the sameperiod, the number of cocainehauls jumped from 206 to 1,324.
The number of people treated forproblem drug use rose from 8,931 in2001 to 12,397 in 2005.
Europol believes Colombianorganised crime groups dominatecocaine supply, with cells in Spain,Britain and the Netherlands.
Turkish organised crime groupsdominate the heroin market.
The Netherlands and Belgium arethe primary locations for theproduction of synthetic drugs, likeecstasy.
Most cannabis resin used inIreland originates in Morocco.
The Garda Síochána believe thedistribution of drugs within Ire-land is organised by networks ofcriminal gangs.
The impact of drug markets,drug-related crime and antisocialbehaviour harms individuals andcomm u ni t ie s.
The forms of crime that causemost harm are the violence andintimidation associated with drugmarkets and the property crimecommitted by problematic drugusers to fund their habit.
Systemic types of crime sur-rounding drug distribution includegangland murders and fights overorganisational and territorial is-sues and disputes over transactionsor debt collection.
The available evidence, whenconsidered along with newspaperand court reports, suggests there isa significant and increasingamount of violence associated withthe drugs trade in Ireland.
This can have a profound effecton feelings of public safety and in-stil a sense that the problem is outof hand.
Policing initiatives strive todisrupt markets and thus reduce orcontrol supply.
On the other hand, demand-re-duction strategies attempt to targetusers and divert them into drugtreatment, by means of arrestreferral schemes, for example.
Ultimately, it is assumed that byreducing supply and demand themarket will shrink and drug-relat-ed crime will decrease accordingly.
A number of writers in this areahave shown, however, that lawenforcement initiatives can haveunintended consequences.
Applying basic market logic, itcan be assumed that successfulattempts to stifle supply shouldlead to higher prices and this inturn should reduce consumption.
In reality, however, most esti-mates of prices through Europe areeither stable or falling.
There are a number of possiblecauses of this. First, although thehidden nature of drug marketsrender them impossible to measureaccurately, it is estimated that lawenforcement activity leads to theseizure of 10%-20% of the drugs inci rc u lat ion.
Consequently, the amount thatremains undetected is such that thelong-term impact of successfulenforcement will be minimal.
Second, drug distribution sys-tems adapt quickly, so that wheredrug suppliers have been arrested,they will quickly be replaced.
Third, demand is often inelasticfor problematic drug users, relativeto moderate or recreational users,and increased prices may simplylead them to engage in greaterlevels of crime in order to pay thehigher prices.
Effective intervention strategiesmay be those which combineattempts to disrupt local marketswith attempts to divert drugoffenders into treatment services.
There is a growing consensusthat a partnership approach, com-bining law enforcement, social andhealth services and local communi-ties, offers the most sustainablemethod of responding to manydrug problems.
■ Johnny Connolly is researchofficer with the Alcohol and DrugResearch Unit, Health ResearchBoard.
ALCOHOL ROUTE TOTEEN DRUG ABUSE
Drink and cannabis are the drugs ofchoice for children, writes Noel BakerT HE VERDICT on
a uniquedr ink-and-drugs-freeconcert forteenagers in Offaly
this summer seemed to be quiteunanimous: deadly.
Organised by teenagers fromthe Alternative Persons Associa-tion (APA) in Laois, the one-daybash at Charleville Castle attract-ed a number of bands fromaround the Midlands, in additionto a lot of goodwill, and 300 mu-sic fans. The only downside wasthat it had originally been hopedthat more than 1,000 puntersmight show.
Therein lies the rub as far asIreland’s relationship with drinkand drugs is concerned. The lastESPAD (European School SurveyProject on Alcohol and OtherDrugs) contains data for countriesacross the European Union, dat-ing from 2003, and by any reck-oning we compare unfavourablyto many of our EU neighbours.
For example, the only area inwhich Irish students did notmatch or exceed the ESPAD av-erage was in the taking of tran-quillisers and sedatives. Accordingto the figures, the proportion ofIrish students who had drank al-cohol in the last 12 months (88%)is higher than the average of 83%,while the percentage of Irish stu-dents who had been drunk in thesame period was much higherthan the average: 72% versus53%.
The smoking of cannabis byIrish students is much higher thanthe ESPAD average — 39% ver-sus 21%, while the use of in-halants is also higher, at 18% forIrish students versus 10%.
Figures contained in the IrishHealth Behaviour in School-AgedChildren (HBSC) study, based oninformation gathered over a num-ber of years, showed that a highpercentage of children are familiarwith drugs such as tobacco, alco-hol and harder substances.
Overall, 36% reported that theyhad smoked tobacco, althoughthe number seems to have fallenfrom 21% in 1998 to 15% lastyear. More than half of childrensurveyed had taken alcohol, al-though again, this figure seems tohave decreased compared withthat in previous years.
Some 16% of children reportedusing cannabis during their life-time — an increase of 4% com-pared with 2002, while 12% saidthey had used cannabis in the pastyear. Rates were highest for thosein the 15 to 17 year age group.Almost one-in-three boys (27.5%)in this age group said they hadused cannabis in the preceding 12months, with the percentage ris-ing among those in lower so-cio-economic brackets. This fig-ure is a cause for concern, andwhile the corresponding statisticfor girls showed cannabis use tobe less of a problem, girls in the15 to 17 years age group werejust as likely to have been drunkin the preceding 30 days as theirmale classmates.
Dr Bobby Smyth, consultantchild and adolescent psychiatristat the Drug Treatment CentreBoard, argues that until Irish soci-ety comes to terms with its con-
Youth workers play pivotal role in fight against drugs
15 NOVEMBER 20, 2007
YOUNG USERS
EXPERT VIEW
Youth work is different from other services — young peopleparticipate because they want to, writes Clodagh O’BrienR ECENT years have seen
the issue of drug misusebecoming one of the
most important social and politicalissues affecting young people.
In this current climate of politicalchange and development in relationto how the drugs issue is addressed,it seems that more young people arecoming into contact with drugsthan ever before.
While a lot of work has beendone in regards to education, pre-vention and treatment — particular-ly in the Dublin and Cork areasthrough the establishment of 14 Lo-cal Drugs Task Forces and the de-velopment of the Young People’sFacilities and Services Fund — theNational Youth Council of Ireland(NYCI) believes that there is still aserious “supply” issue which needsto be addressed.
The NYCI believes that youngpeople’s health and wellbeing mustbe safeguarded and it is the right ofeach young person to live a healthyand safe life without drugs. Ourwork in the area of drugs is basedon some simple but essential under-standings.
Firstly, we believe that drug mis-use must be understood as an aspect
of modern society and a problemwhich does not have an easy singlesolution. It needs to be tackled in amulti-faceted way.
Drug misuse is a health issue, butwe must not confine ourselves tojust looking at it from a health pointof view. The misuse of drugs is of-ten linked to justice and crime, butoveremphasis on this element hasproven not to work.
Secondly, we believe that allresponses to the problem of drugmisuse must be based on respect forthe person. Too often the drug useris identified only as a problem, anda nuisance to society. But they alsohave needs that should be met andthe right to be treated with respectjust like the rest of society. Also, theuse of ‘scare tactics’ to turn peopleoff drugs has been found not towork. Often the shared experienceis at odds with young people’s ownknowledge and experience of drugs,making such approaches ineffective.
Thirdly, drug misuse should not
be treated as an isolated issue. Socialfactors, including the influence ofpeers, family, social class, work,education and geography all play apart in whether particular youngpeople participate in drug misuse aswell as influencing the type of drugsthey use.
Fourthly, the NYCI believesstrongly in the necessity of usingprevention as the key approach intackling drug misuse. This does notin any way detract from the need touse other approaches and strategies,such as risk reduction, treatment orsupply reduction. In order to workeffectively in the current climate,the various approaches should com-plement each other. We believe,however, that strategies based onprevention have been ignored in thepast. They have huge potential foreffecting change and need to besignificantly developed.
Many youth organisations havebeen to the forefront in developingdrug prevention and education
interventions in the context of aholistic, health promoting approach.
While drugs education is essentialin a school setting as well, it is oftenservices, such as those provided byyouth organisation outside this typeof environment, in a more informalyet structured setting prove moresuccessful.
Youth workers can play a pivotalposition in relation to young peopleand drug use. Due to the nature oftheir roles they engage with youngpeople on a regular basis, particular-ly those in vulnerable positions.
“Youth work is different fromother services as it is outside ofschool, young people participate inyouth organisations because theywant to. There they have the op-portunity to take part in a range ofenjoyable, creative activities. Thistype of activity can encourage thedevelopment of skills and knowl-edge among young people andmake them feel like genuine part-ners with adults. This helps the
young person to make informeddecisions about their personal healthand development and feel empow-ered to say ‘no’ or refuse to bow topeer pressure in relation to drugs,”said Mary Cunningham, directorof the National Youth Council ofI reland.
A number of groups which theNYCI represents are involved indealing with the issue of drugs andyoung people.■ Foróige has a number of projectsand services funded to target youngpeople at risk in North Dublin.■ Youth Work Ireland Galwayfacilitates the CAPE Projectmworking with young people onissues around drug abuse.■ Catholic Youth Care (CYC) hasthree dedicated drug educationteams in Bray, Finglas andSwords/Baldoyle and supports thedevelopment of The Parachute Pro-gramme in Dun Laoghaire.■ Pavee Point work under theTraveller Specific Drugs Initiativewhich was established in 2000 aspart of the National Drugs StrategyTeam.■ Clodagh O’Brien is communica-tions officer with the NationalYouth Council

TERAPROOF:User:jackiebolandDate:16/11/2007 Time:18:57:14Edition: 20/11/2007 ExSupplement XS2011DRUGSPage:19Zone:XS1
THE LEGAL DEBATEKeeping cannabis illegal causes moreharm to users, writes Fr Sean Cassin
Reducing demand by prevention, is theway forward, says Gráinne Kenny
IRELAND’S drug epidemic hasled to calls for drug legalisation. Ithas been suggested that drugs
should be given free of charge.What is meant by ‘regulate’ and
‘control’? These are terms used for de-criminalisation/legalisation. They meanone thing: to take illegal, addictive,toxic substances and make them freelyavailable to addicts. How are drugs‘controlled’, if they are freely available?How will we stop them seeping downto young teenagers? Who would be re-sponsible for their strength and qualityand who would supply them?
Somehow, it would be hard to imag-ine the local pharmacy becoming a dis-tributor. If heroin is given freely on de-mand how do we keep up with de-mand?
Methadone was introduced becauseof it’s long-term action. The effects ofheroin wears off within a couple ofhours. The heroin addict would need aconstant supply of heroin and cleanneedles throughout the day to keephim or her away from the black mar-ket. Who will pay for the additionalfamily and addiction counsellors? Wecan’t cope, as it is.
Why would there be a black market?Presumably, addictive, toxic substanceswould not be available to under-18’s inline with alcohol and tobacco restric-tions. So a black market would be es-tablished to supply them. Ireland hasthe youngest cannabis/binge drinkingpopulation in Europe. How would wepropose to stop these substances seep-ing down to Irish kids.
Recent UN figures claimed mostpeople are introduced to illicit drugs inthe school or its vicinities. Not at thetertiary stage. Cigarettes, alcohol andcannabis are proven gateway drugs.
A recent example is our near neigh-bour England. Acting on the advice ofa committee of drug liberals and with-out the advice of psychiatrists workingin the field of addiction psychosis,Home Secretary David Blunkett down-graded cannabis. There was uproarfrom mental health charities, for exam-ple SANE. As predicted, there has beena 85% rise in mental hospital admis-sions.
Since 1997, use among 13- to14-year-olds has increased by 1% and isstill rising among 11- to 12-year-oldboys. Older teens are moving to co-caine and the police are reporting ahuge rise in street dealing.
Mr Brown’s government is activelyconsidering reversing downgrading ofcannabis. Scientists and researchers inIreland and internationally agree that aliberal drugs policy creates a particularrisk among young people. Those alsoat risk are the poor and those who arementally vulnerable. Even the Dutchare becoming alarmed.
It should be remembered that crime,violence and drug use gohand-in-hand. Alcohol is already caus-ing significant problems. Adding anoth-er cocktail of mood-altering substanceswould only add to the violence. Crim-inal gangs are known to use cocaine topsyche themselves up before going on acrime spree.
There are many questions that shouldbe asked for instance, how would theGarda deal with the rise in druggeddriving? They will now have to testroad accident victims for alcohol. Whatabout drugs? If illegal drugs are chargedfor and taxed, the revenues raised couldbe used to pay for treatment, they ar-gue. But if too much is charged thenthe blackmarket will thrive with cheap-er and stronger drugs. If too little ischarged the demand will grow.
How will the Government handlethe international treaty signed with theUnited Nations together with 200 oth-er countries? Can we expect the tax-payer to pay for this when their rela-tives lie on hospital trollies. What aboutfamily violence closely associated withsubstance abuse? Will those who pro-mote drug legalisation take responsibili-ty for the new wave of mentally ill oraddicted youngsters in Ireland? Nocountry, not even the Netherlands, haslegalised drugs. Sweden is the mostsuccessful country in Europe in tack-ling drugs. They employ a restrictivedrugs policy. Swedes have the lowestfigures of drug use and it is illegal toconsume a drug there.
In simple terms, the proposal is thatthe so-called ‘War on Drugs’ is not anappropriate way to deal with the drugsepidemic. I would argue that there hasnever been a War on Drugs. All wehave to defend the health and safety ofour vulnerable citizens are our police,customs and, further afield, crop eradi-cation. Drug substitution throughmethadone is another ‘weapon’. Theseapproaches will never work to solve aproblem unravelling the fabric of ours ocie t y.
That is why, in 1989, a group ofconcerned European citizens brought anew dimension to the so-called wardemand reduction.
We in EURAD believe reducing thedemand for illegal drugs by prevention,together with strong legal measures, is,and must remain, an intricate part ofthe solution. Legal sanctions are the lastline of protection the citizen has a rightto expect. Drugs are illegal becausethey are dangerous. Changing the lawwill not alter this fact. It is a policy ofde s pai r.
■ Gráinne Kenny is InternationalPresident of Europe Against Drugs(EURAD). For further information logon to www.eurad.net
WHILE watching myhome county, Kilkenny,take the plaudits from
Henry Shefflin on their win of theAll-Ireland against Limerick I wentfrom euphoric to shudder in a millisec-ond.
He included in the thanks the suppli-ers of the most available and problem-atic drug used in the country, Dia-geo/Guinness.
Most of our young people that endup in casualty units and in treatmentcentres do so from use of this drugrather than from cannabis, ecstasy, co-caine or heroin put together.
This is neither a ban drink rant nor ademonise illegal drugs tirade. It’s a pleato people to stop adding to the harmcaused by illegal drugs by the fact ofthe drugs they use are illegal.
It’s mostly our young people whochoose cannabis drug over alcohol be-cause it doesn’t give you the hangoveralcohol does, isn’t as expensive and theeffects of a single spliff (joint orcigarette) last longer than a drink.
Taken orally in a tea or biscuitremoves the high cancer risk that goeswith smoking. Most of these 300,000users do so with little or no harm asthey use the drug occasionally and notto excess.
Most know that becoming ‘zonked’on the drug is an unpleasant sensationthat needs to be avoided, just as be-coming drunk is mostly avoided bypeople. The periods between their usesare adequate to allow their bodies andminds to recover from it.
Yet the use of this drug is illegal. Forpossession of the drug you can be finedor sent to prison.
It’s hypocritical, harmful and senselessto treat cannabis users in this way. A re-cent Lancet Paper on cannabis suggest-ed a link between psychosis (mentalproblems) and cannabis use.
This fuelled the prohibition of drugslobby to ban the drug, makesevere penalties and lock up for longerperiods those found supplying and orusing it.
All drugs carry a potential for harm,especially alcohol, and this is why wetry to control how much, how oftenand when people take alcohol.
Putting in place such controls forcannabis as the Dutch coffee shopsmakes sense, where licensedpremises control the supply andcontrol who buys it, and makes somerevenue in taxes for Government.
The notion that keeping cannabis il-legal will somehow lessen its use is evi-dently mistaken as the numbers using itare increasing every year as indeed isthe supply of it.
Children as young as 14 are trying itout and it’s the drug of choice of hun-dreds of thousands. Our young peoplehave the third highest rate of illegal
drug use in the EU. (All consistentdrug use legal or illegal can adverselyaffect adolescents’ development).
Keeping drugs illegal does not workin reducing use. Reducing demandmay be more effective.
Where the state seeks to block, seizeand remove illegal drugs results in themarket being entirely in the hands ofunscrupulous criminals.
It results in millions of euros goinginto the criminal underworld.
The State has been operating a veryeffective heroin short circuit for the lastten years and is supplyingalmost 9,000 opiate users with asynthetic opiate that normalises theirlives and improves their health andemployment prospects.
It keeps them out of the crime need-ed to finance illegal drugs.
Keeping the cannabis issue in thecriminal zone causes more harm tousers of the drug than the drug itself.
In July 2001, Portugal’s governmentimplemented such a decriminalisationdrug policy.
Users of any illegal drugapprehended by police were broughtnot before the courts, but before spe-cial commissions of health, legal, andsocial work professionals. Their aimwas to give users access to treatment foraddiction and other problems related todrug use.
The State began viewing drug usersnot as criminals, but as victims ofdrugs. Experience of this initiative sofar allows some conclusions:■ The Portuguese authoritiesimplemented a national programme ofchange in the way they deal with drugoffenders without major delays or ad-ministrative problems■ It has been possible for the police,health and social services to worktogether to prioritise the help to drugusers rather than punishment■ The system has led to animprovement in the ability of theauthorities to intervene early in ayoung person’s drug problem, and todeal with cases more quickly andcheaply than the courts■ The new approach has not ledto a significant increase in drug uset he re
If anything is to come from thisdebate, there must, at least, be agree-ment, that users of cannabis shouldn’tend up more harmed by our laws thanby any drugs they use.
■ Sean Cassin is a Franciscanpsychotherapist who has worked withdrug users and their families for 20years. He founded the MerchantsQuay Drugs Project and is the chair ofthe National Voluntary Drug Sector, amember of the National Drug Strategyteam and chair of the Drug Policy Ac-tion Group.
VIEWS
19 NOVEMBER 20, 2007

User:jackiebolandDate:16/11/2007 Time:18:22:06 Edition:20/11/2007 ExSupplement XS2011DRUGSPage:20 Color:
What heroin had done to me in the previous 10 years wasnothing compared to what cocaine done to me in the last four
years. Cocaine has absolutely wiped the floor with me
‘’‘’
THIS IS JULIE
Cormac O’Keeffe talks to an addictabout her 14-year battle with drugsJ ULIE’S hands and legs
look like they have beenrepeatedly stabbed andclobbe red.
They are badly disfiguredwith lumps, sores, abscesses and scars.There are large black sores, which looklike little craters.
The tissue around some of them haseaten into the skin.
Some of the sores are abscesses, withyellow puss. Many of the scars andlumps are red and raw looking. Bloodoozes out if Julie even lightly scratchesthem.
The palms of her hands are riddledwith prick marks. So are her fingertips. Julie reckons she has around 45marks in her upper body and about 50in her legs and feet.
“This is all from injecting cocaine.You will stick the needle in anywherewith cocaine,” said Julie, from Darndalein north Dublin.
“You keep sticking it in anywhere toget a vein, into your neck, your breasts,stomach, legs, you name it. You will doanything to get the cocaine into you.”
She said as bad as the scars are now,they were 10 times worse a few monthsago.
“My hands looked like there werebig blackberries on them,” she said.
Now 27, and a mother of a 12-year-old daughter, Julie is at her wits end.
“I’m sick of this life, the depressionI’m going through. I think I’ll be deadnext year if I don’t get help.”
Julie’s story is the story of cocaine,particularly intravenous cocaine use,and how it is ravaging the same parts ofthe country, mostly in Dublin, thatwere devastated by heroin epidemics inthe 1980s and 1990s.
The fear is that, like the heroinepidemic, the State is responding toos low l y.
And with cocaine use, far morewidespread across the country andsocial classes than heroin ever was, thefear is that the impact will be farg reater.
As a sign of an unusually openrelationship between her and hermother, Julie is willing to show herwounds, and tell her story in hermother’s company.
Rachel has stood by her daughteragainst all the odds. She lives a life ofsuch stress and anxiety that only parentsof addicts can truly comprehend.
“I am very, very worried. I worrythat one day I’ll walk into the roomand find her gone. It worries me sick.It’s like a devil eating my child away.”
Julie was only 12 when she gotinvolved with an older crowd, througha neighbour three years older than her.
That was back in 1994-95, at theheight of the last heroin epidemic.
She started on cannabis and ecstasy,but graduated to heroin at just 13,smoking at first and then injecting.
She started going out with a guyand at 15 became pregnant.
“It was the only time in my life thatI was completely drug free. I stuck bymy mam’s side.”
Rachel said when her daughter was14 she thought she was anorexic. “Iremember we went in for Christmasclothes and she was fitting and Ipulled across the curtain and I got anawful shock. Her bones were juststicking out. She wouldn’t admit it,but I discovered she was on heroin.”
She said she had to conduct a“24-hour watch” during Julie’s preg-nancy and couldn’t let her daughterout of her sight.
Julie said that six weeks after givingbirth, she went out to buy SudoCream for her baby.
“I met one of me old friends andshe said she had a bag and did I wantto go for a smoke and I got strungout again.”
Julie went on a methadone mainte-nance course for her heroin addictionat 17 and has been on it ever since.She tried a detox at Beaumont Hospi-tal but it didn’t work.
She said as bad as her life was onheroin, everything changed for theworse at 23 when she started injectingcocaine.
A guy she was going out with atthe time (who soon after died from acocaine-induced heart attack) askedher if she wanted to have a “turn on”(inject). “I said f**k it, come on we’lldo it. I said a prayer beforehand,saying I really don’t want to do it. Igot the vein, got the hit and it wasf***ing brilliant.”
But she added: “What heroinhad done to me in the previous10 years was nothing compared towhat cocaine done to me in the lastfour years. Cocaine has absolutelywiped the floor with me. I haven’ttouched heroin in the last four years.This cocaine has destroyed mylife.”
She said she immediately had acraving for cocaine and started“banging” or injecting every day.
“With heroin you give yourself ahit, you’re out of your head for four,five hours. But with coke it’smadness, you have a turn on and itlasts for two minutes — that’s even along time — and it’s gone.”
The short duration of the effects,and the psychological addiction, saysJulie, makes the drug so much worsethan heroin.
“I could take cocaine and go downto me ma and waffle the ears off her.Then all of a sudden it’s gone and Ineed another turn on. She might tryand talk to me and I’d go ‘I’m not inthe humour, I’m not in the humour’— total Jekyll and Hyde stuff.”
She said dealers often give a “layon” or drugs on credit, to be paid forthe following week. This makes surethe addict comes back for more andmay even mount up more debt inbe t ween.
“As soon as you use it, you’re para-noid, knowing you owe money. Oneday I was walking in the area and aguy I know came up to me and saidhe has seen me looking behind me20 times as if I was being followed.”
She said her mother had bailed herout a number of times to pay offdebts after she was threatened.
“I have paid money for her afterthreats she’d be beaten up if I didn’tpay,” said Rachel.
“She came crying to me, she wasterrified. I’ve done it about threetimes, around €400-€500 each time.One time they had her social welfarecard. I couldn’t tell anyone for fearshe’d be beaten or have her faces la s hed.”
Such was her addiction that Juliehad to find some way of earningmoney.
Her mother offered to leave duringthe interview. She knows what herdaughter did for money, saying it“really, really hurts” her, but under-standably does not want to hear itdirectly from her own daughter.
Julie said she started prostituting andworked in the well-known districts inthe city centre. She’d take cocainebefore and during her work and gotcocaine off a dealer who suppliedwomen in the area.
“I was prostituting for a long time.You could make a lot of money,” shesaid.
But all the time her addiction wasgetting worse and worse. “It was get-ting to the stage that I was forgettingwhere I was putting needles in thehouse. I used to be careful about that,because of my daughter.”
She tried detox in Beaumont Hos-pital again, over a year ago. She lastedfour weeks, but was dying to have a“turn on” when she got out, just onehit.
“When I got out, I had one andgot a vein. But it wasn’t just one. Iwas back to prostituting. My familyhad enough of me.”
A couple of nights later, she nearlydied.
“I put a bit into the needle, itlooked like muck. I had a quarter of agramme left. Don’t ask me how Ilived, but I am still here to tell thetale. I said ‘will I put it all in?’ It was
hard for me to get veins, so I put thewhole lot in.
“I started feeling out of it. I said ‘thisis nice coke’. Then me knees startedwobbling, it’s called the wobblers. It’slike an epileptic fit while you areawake, you can’t control what yourbody is doing.”
She said her legs gave in and shesmacked her head off a load of DVDsand couldn’t remember after that.
Luckily, her mother heard the smashand rang for an ambulance.
“My ma said she really thought Iwas going to die. She said my bodywas hopping off the floor,” said Julie.
“When the ambulance came, I said‘I’m OK’. The ambulance men weresearching me. I’d said ‘I’m OK, I’mOK’. I still had a little bit of coke leftin my bra. Even though what wasafter happening to me, all I couldthink was ‘get these ambulance menout of here because I want the rest ofthis coke’.”
The doctor in the emergency wardtold her she was lucky to be alive. “Hesaid ‘I don’t know how your heart isstill going. You’ll be dead next year, ifyou don’t stop’.” The doctor found aclot, but was able to disintegrate it. Itake aspirin every day to thin theblood.”
But she didn’t stop.“My ma thought I’d get a fright, but
I didn’t. The next day I was usingagain. I was still selling myself, stillbanging up. I didn’t care. I said tomyself ‘it’s inevitable, I’m going to diefrom this, why not have a good one’.”
Her local doctor referred her toTrinity Court treatment centre onPearse Street to be assessed after shestarted injecting into her neck, breastsand shoulders. Julie wanted to go backto St Michael’s Ward in BeaumontHospital for detoxification.
Rachel went in with her. “Fromdealing with her for 13-14 years, sheseemed fully determined to go toBeaumont and a residential centre for ayear or two. But the person who inter-viewed her got the impression that shejust wanted to avoid being evicted byher parents.”
She was very low after being turneddown. She continues to drink a bottleof vodka every night, a habit shedeveloped in place of taking heroin.
Julie said it’s three weeks since shewent on a binge with cocaine and onlyhad one slip last week, when she got a€50, or half gramme, bag of cocaine.
“I had a little slip last week, but Icould have another and then go on abinge. I still owe the €50. When I goback, they’ll say ‘I’ve lovely coke here’.Cocaine is in my head every day. I justwant a chance to get out of here.”
... sheis 27.She isscar redf romt h ree
years ofinjectingcocaine.She wasassessedfor detox
at BeaumontHospital.She wastur neddow n. Picture: Maura Hickey