boards part 1 review - stritch school of medicine · as radial glia act as scaffolds along ......
TRANSCRIPT

Brain Midline1

Midline MRI

Brain Diagram
TemporalLobe
LobeFrontal
Cerebral Cortex
ParietalLobe
LobeThalamus
Hypothal.
Corticospinal Tract
Cervical armmuscles
Thoracic
Lumbosacral
Spinal Cord
Medulla
BasalGanglia
SC
ICMidbrain
PinealOcciptal
CerebellumPons
Pituitary
Neuron Numbers:
100 Billion in cerebellum
25 Billion in cerebral cortex
1 Billion in rest of brain
126 Billion in brain

BBB1
nuc
Redrawn after figure on page 76 of "The Blood Brain Barrier" by GW Goldstein and AL Betz (Sci. Amer. 255:74−83, 1986)
Astrocyte Foot Processes
EndothelialCell Basement
Membrane
Tight Junctions here
CapillaryLumen

CSF Circulation
arachnoidtrabeculae
SuperiorSagittalSinus
CSF leaving subarachnoid space and entering the venous circulation in the superior sagittal sinus via arachnoid villi.
Cerebrum
Corpus Callosum
Plexus secretesCSF intoventricles
Cerebellum
CSF leaving ventriclesand entering subarachnoidspace
Third Ventricle
Cerebral Aqueduct
Fourth Ventricle
Brain Stem
sulcus
gyrus
endosteal dura
blood vesselon top of pia
Dura (solid line)
Arachnoid (dashed line)
Pia (dash−dot−dot line)
Spinal Cord
meningeal dura
SpaceSubarachnoid
Choroid

Vertebrobasilar Circulation
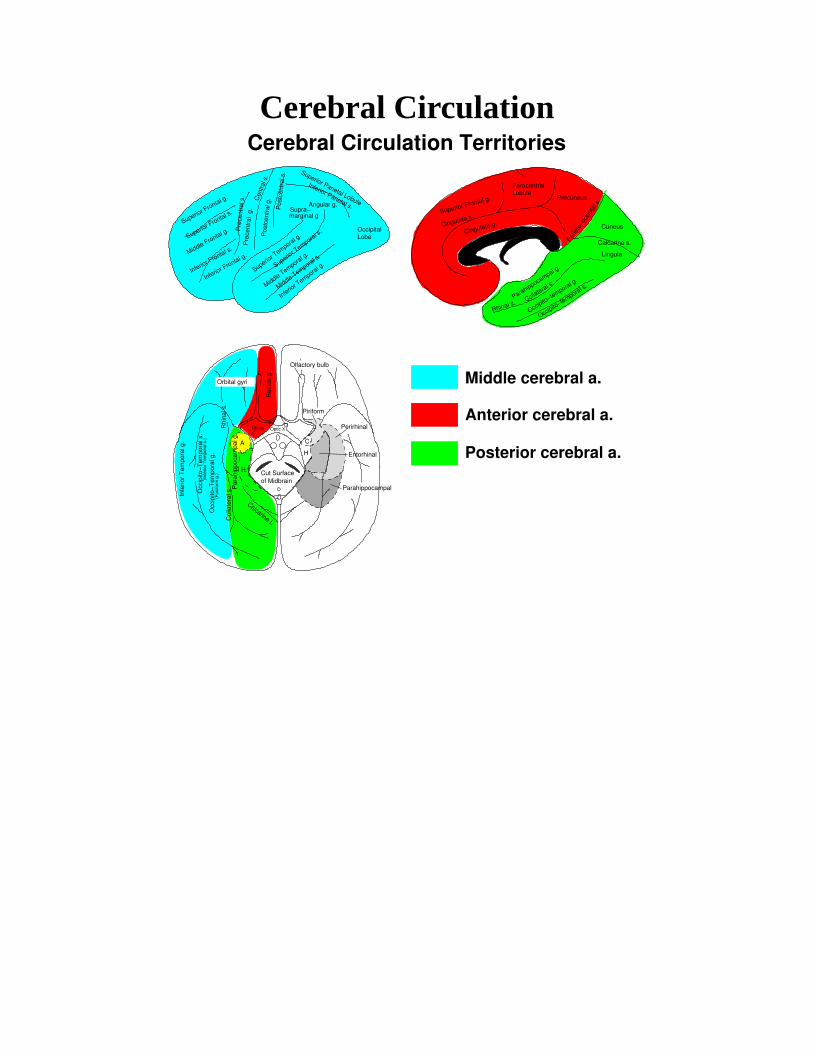
Cerebral Circulation
Middle cerebral a.
Posterior cerebral a.
Anterior cerebral a.
Cerebral Circulation Territories
OccipitalLobe
ParacentralLobule
Cut Surfaceof Midbrain
Optic X
(Fus
iform
g.)
Piriform
Perirhinal
Entorhinal
Parahippocampal
A
H
H
C
Rec
tus
g.
Infe
rior
Tem
pora
l g.
Occ
ipito
−Tem
pora
l s.
Occ
ipito
−Tem
pora
l g.
Col
late
ral s
.R
hina
l s.
Calcarine f.
(Inf
erio
r T
empo
ral s
.)
Orbital gyri
Olfactory bulb
Par
ahip
poca
mpa
l g.
Uncus
Inferior Parietal s.
Pre
cent
ral s
.
Superior T
emporal g.
Middle Temporal g.
Inferior T
emporal g.
marginal g
Angular g.Supra−
Precuneus
Cuneus
Lingula
Parahippocampal g.
Pre
cent
ral
g.
Pos
tcen
tral
g.
Superior Parietal Lobule
Superior T
emporal s. Cingulate g.
Superior Frontal g.
Cingulate s.
Calcarine s.
Superior Frontal g.
Middle Frontal g.
Middle Temporal s.
Cen
tral s
.
Superior Frontal s.
Inferior Frontal s.
Inferior Frontal g.
Pos
tcen
tral
s.
Parie
to−o
ccip
tal s
.
Occipito−temporal s.
Occipito−temporal g.
Collateral s.
Rhinal s.
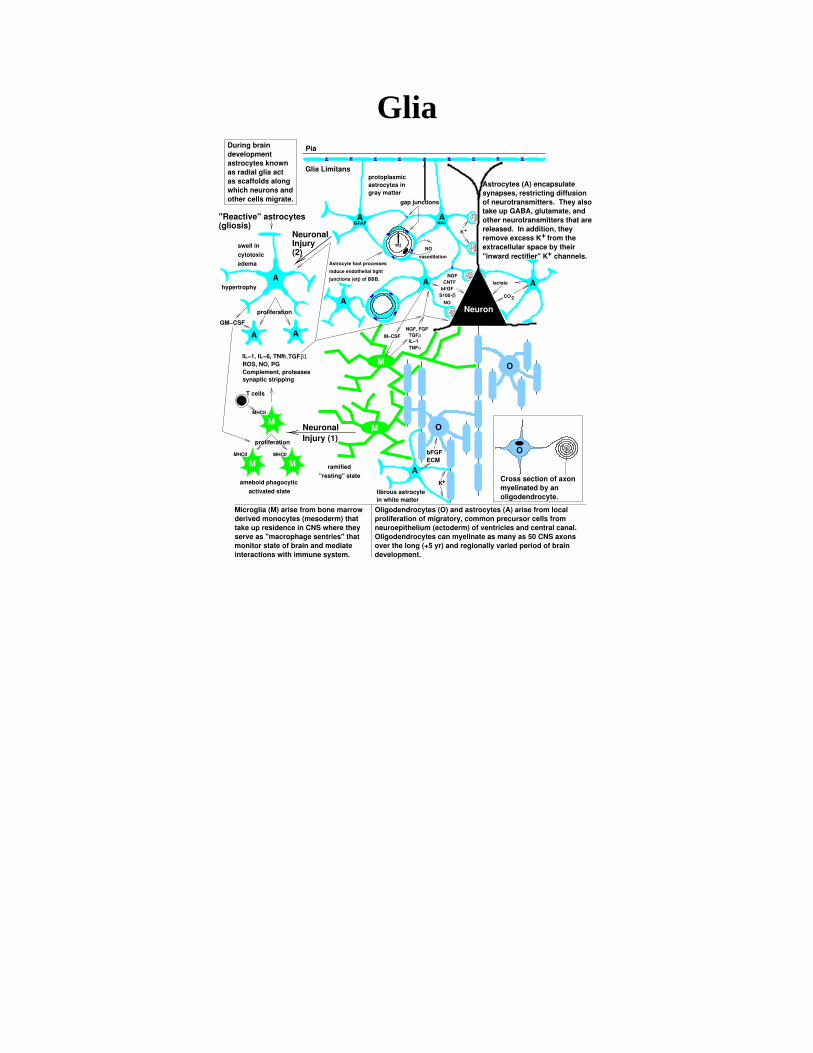
GliaDuring braindevelopmentastrocytes known as radial glia act as scaffolds along which neurons and other cells migrate.
swell in
cytotoxic
edema Astrocyte foot processes
induce endothelial tight
junctions (etj) of BBB.
"Reactive" astrocytes(gliosis) GFAP
+
Astrocytes (A) encapsulatesynapses, restricting diffusionof neurotransmitters. They alsotake up GABA, glutamate, andother neurotransmitters that arereleased. In addition, theyremove excess K from the extracellular space by their
Microglia (M) arise from bone marrowderived monocytes (mesoderm) thattake up residence in CNS where they serve as "macrophage sentries" thatmonitor state of brain and mediate interactions with immune system.
Oligodendrocytes (O) and astrocytes (A) arise from localproliferation of migratory, common precursor cells fromneuroepithelium (ectoderm) of ventricles and central canal.Oligodendrocytes can myelinate as many as 50 CNS axonsover the long (+5 yr) and regionally varied period of braindevelopment.
Cross section of axonmyelinated by anoligodendrocyte.
NeuronalInjury (1)
NeuronalInjury(2)
fibrous astrocytein white matter
"resting" stateameboid phagocytic
activated state
proliferation
hypertrophy
proliferation
GM−CSF
Pia
Glia Limitansprotoplasmicastrocytes ingray matter
NGFCNTF
bFGFS100−
NO
Neuron
NO
vasodilation
K+
A
A
A
A
A
MAOA
A
O
O
O
ECM
K+
ramified
M
M
M
M
M−CSF
NGF, FGF
IL−1βTGF
TNFα
T cells
etj
gap junctions
β
lactate
CO2
bFGF
A
A
+"inward rectifier" K channels.
MMHCIIMHCII
MHCII
ROS, NO, PGComplement, proteasessynaptic stripping
α,TGFIL−1, IL−6, TNF β1

Neuron
myelin sheath
cell body
axon from another neuron
dendrites
synapse
axon
axon continues
nuc.
axon
spines
axon
synaptic cleft(10 nm)
postsynaptic receptorscan open or close ion channels
dendriteshaft
synaptic vesiclesaxon terminal
neurotransmitter
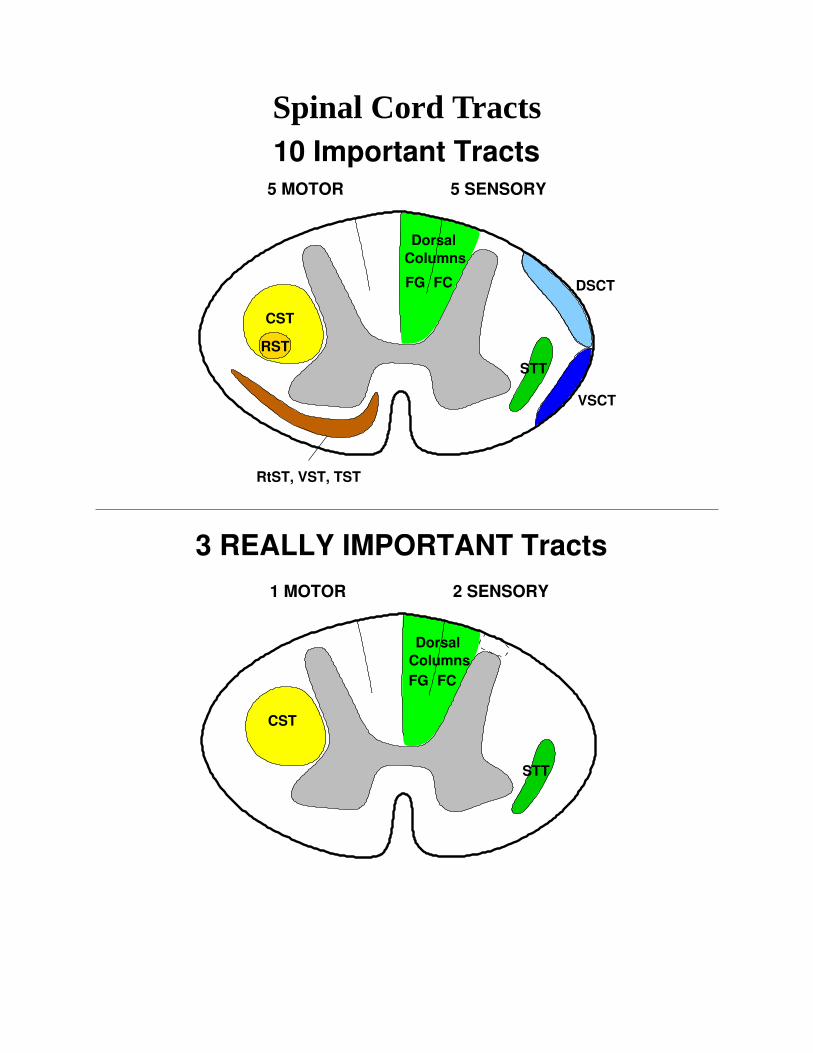
Spinal Cord Tracts
ColumnsDorsal
CST
DSCT
VSCT
STT
RtST, VST, TST
RST
5 MOTOR 5 SENSORY
FG FC
10 Important Tracts
ColumnsDorsal
CST
STT
1 MOTOR 2 SENSORY
FG FC
3 REALLY IMPORTANT Tracts
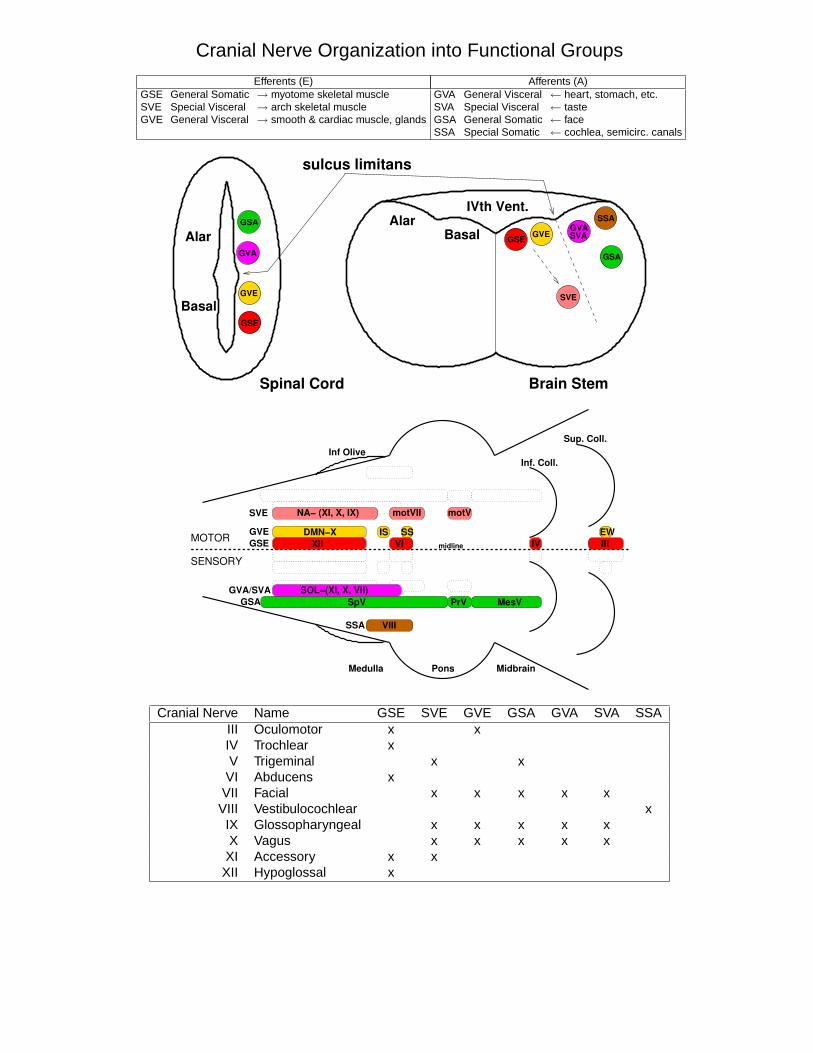
Cranial Nerve Organization into Functional Groups
Efferents (E) Afferents (A)GSE General Somatic → myotome skeletal muscle GVA General Visceral ← heart, stomach, etc.SVE Special Visceral → arch skeletal muscle SVA Special Visceral ← tasteGVE General Visceral → smooth & cardiac muscle, glands GSA General Somatic ← face
SSA Special Somatic ← cochlea, semicirc. canals
sulcus limitans
Brain StemSpinal Cord
GSEGVE
GVA
SVE
SSA
GSA
SVA
GVA
GVE
GSA
Basal
Alar BasalAlar
IVth Vent.
GSE
midline
GVEGSE
GVA/SVAGSA
SSA
MOTOR
SENSORY
Medulla Pons Midbrain
Inf OliveSup. Coll.
Inf. Coll.
SVE
SpV
NA− (XI, X, IX)
DMN−XXII VI
motVII
IS
motV
SS EWIII
SOL−(XI, X, VII)
VIII
PrV MesV
IV
Cranial Nerve Name GSE SVE GVE GSA GVA SVA SSAIII Oculomotor x xIV Trochlear xV Trigeminal x x
VI Abducens xVII Facial x x x x x
VIII Vestibulocochlear xIX Glossopharyngeal x x x x xX Vagus x x x x x
XI Accessory x xXII Hypoglossal x

Lateral Medullary Syndrome (Wallenberg)

Pathways in the Brain Stem
Corticospinal Tract, Dorsal Column/Medial Lemniscus, Spinothalamic Tract
ColumnsDorsal
Medulla
PonsMidbrain
CST
Spinothalamic Tract
Pyramid
Medial Lemniscus
Crus Cerebri
NG,NC
MLF and Lateral Vestibulospinal Tract
Semicircular canals
46
Vestibular nuclei
3
lateral vestibulospinal tr.
PPRF
AP
H
descending MLF ascending MLF
PPRF and Ascending MLF
46 3ascending MLF
PPRF
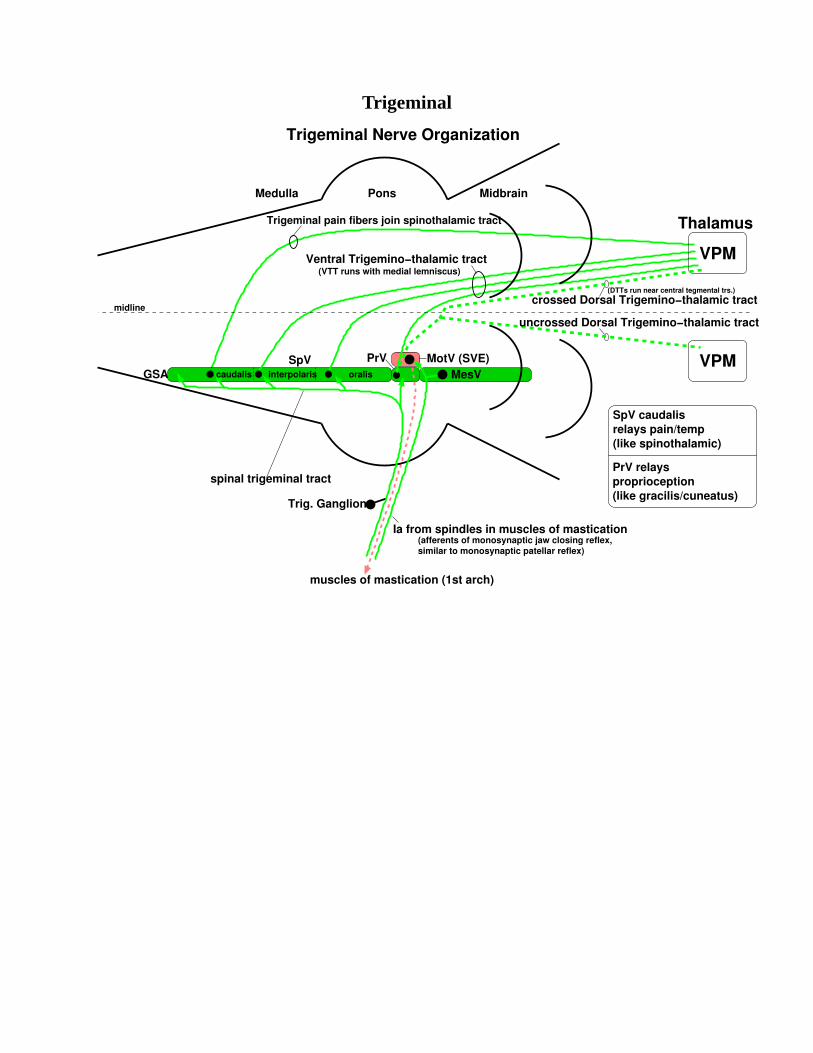
Trigeminal
Trigeminal pain fibers join spinothalamic tract
(VTT runs with medial lemniscus)Ventral Trigemino−thalamic tract
muscles of mastication (1st arch)
Trigeminal Nerve Organization
midline
GSASpV PrV MotV (SVE)
MesVoralisinterpolariscaudalis
spinal trigeminal tract
Trig. Ganglion
Ia from spindles in muscles of mastication(afferents of monosynaptic jaw closing reflex,similar to monosynaptic patellar reflex)
SpV caudalisrelays pain/temp(like spinothalamic)
PrV relaysproprioception(like gracilis/cuneatus)
VPM
VPM
crossed Dorsal Trigemino−thalamic tract
uncrossed Dorsal Trigemino−thalamic tract
(DTTs run near central tegmental trs.)
Medulla MidbrainPons
Thalamus
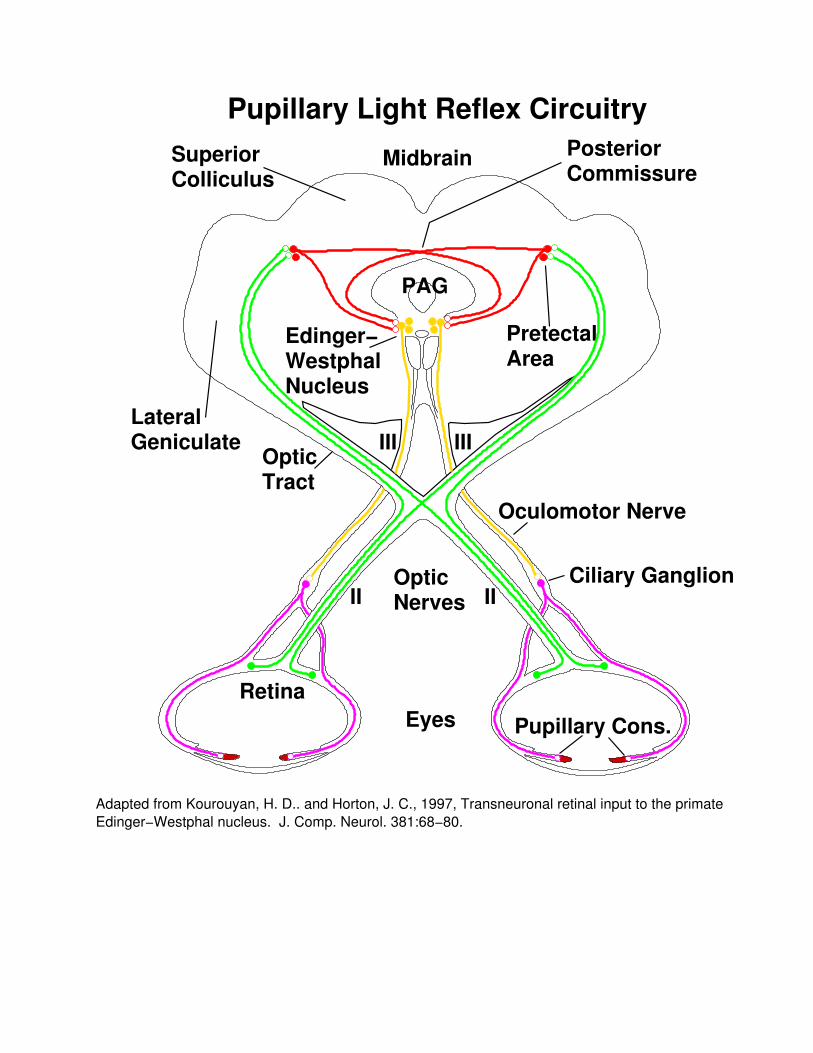
OpticNerves
OpticTract
SuperiorColliculus
PosteriorCommissure
PretectalArea
LateralGeniculate
Edinger−WestphalNucleus
Oculomotor Nerve
Ciliary Ganglion
EyesRetina
Adapted from Kourouyan, H. D.. and Horton, J. C., 1997, Transneuronal retinal input to the primateEdinger−Westphal nucleus. J. Comp. Neurol. 381:68−80.
Pupillary Light Reflex Circuitry
II II
III III
Midbrain
Pupillary Cons.
PAG

Locus Ceruleus/Raphe

Cortex
Cut Surfaceof Midbrain
H
Parahippocampal g.
Occipito−Temporal g.
Pre
cent
ral g
.
Middle Temporal g.
Marginal br.
Cuneus
Piriform
Parahippocampal
Rec
tus
g.
Calc. f.
Orbital gyri
Olfactory bulb
Optic X
C
H
Precuneus
Lingula
Paracentral
Inferior T
emporal g.
Superior T
emporal g.
Middle Frontal g.
Pos
tcen
tral
g.
Subcallosal g.
Anterior C
ingulate g. Posterior Cingulate g.
Uncus
A
Infe
rior
Tem
pora
l g.
Occ
ipito
−T
empo
ral (
fusi
form
) g.
Par
ahip
poca
mpa
l g.
Pre
cent
ral s
.
Cen
tral
s.
Supramarginal
Superior Parietal Lobule
Inferior T
emporal s.
Superior T
emporal s.Superior F
rontal g.
Inferior F
rontal g.
Superior Frontal s.
Inferior F
rontal s.
Intraparietal s.Angular g.
Pos
tcen
tral
s.
Occipital g.
Superior Frontal g.
Collateral s.
Parie
to−O
ccip
ital s
.
Calcarine f.
Cingulate s.
Rhi
nal s
.
Occ
ipito
−T
empo
ral s
.
Col
late
ral s
.
Par.−Occ. s.
Perirhinal
Entorhinal
Central s.

Cerebellum
MCP
ICP
SCP
Cortex
TemporalLobe
LobeFrontal
Cerebral Cortex
ParietalLobe
LobeThalamus
Hypothal.
Corticospinal Tract
Cervical armmuscles
Thoracic
Lumbosacral
Spinal Cord
Medulla
BasalGanglia
SC
ICMidbrain
PinealOcciptal
Pons
Pituitary
Neuron Numbers:
100 Billion in cerebellum
25 Billion in cerebral cortex
1 Billion in rest of brain
126 Billion in brain
Cerebellum
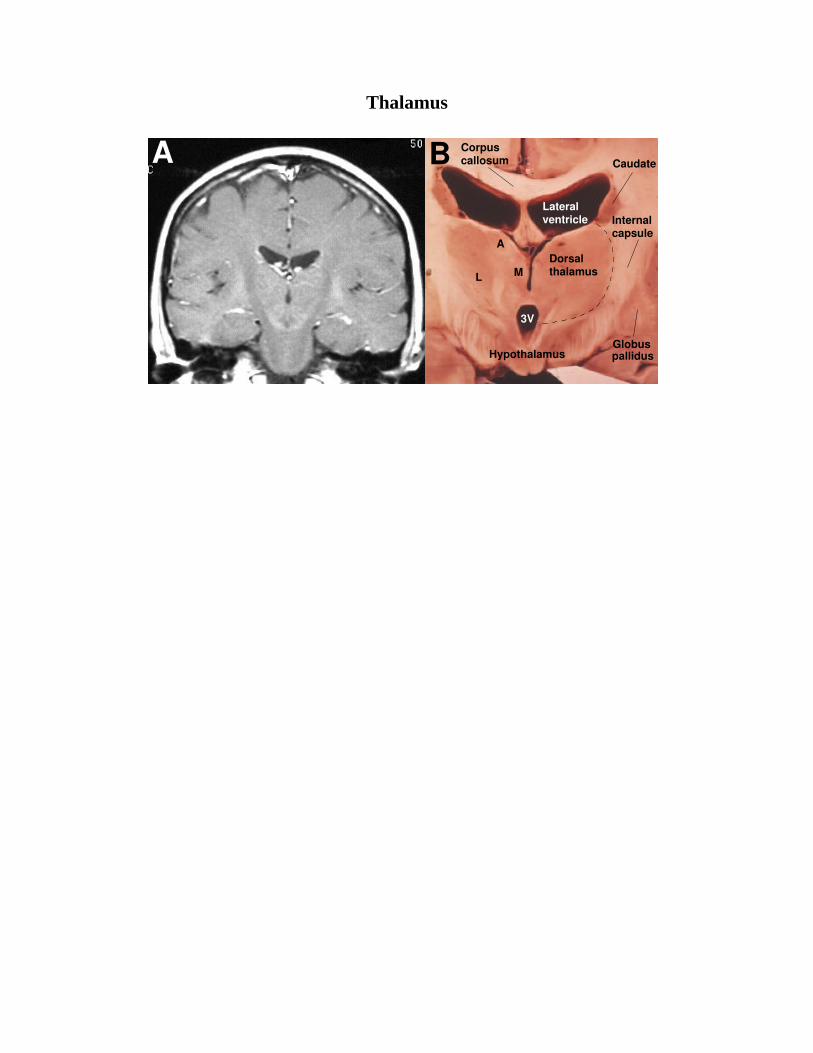
Thalamus
Internalcapsule
CorpuscallosumA B Caudate
Lateral
Hypothalamus
3V
M
A
L
Dorsal
ventricle
thalamus
Globuspallidus
MGLG
Pul
VL
VAAV
MD
ILN
VPL/VPM
Visual
SomatosensoryMotorPremotor
Prefrontal
Calcarinesulcus
Cingulataesulcus
Central sulcus
A
B
C
Auditory
AssociationCortex
LP/PUL
LP/PUL
VAVLVPL/VPM
ZI
PULLP
LDMDl
MDm
ANT
ET
MGLG
IML
MEDIAL
LATERAL
ANT.
METATHALAMUS
3V
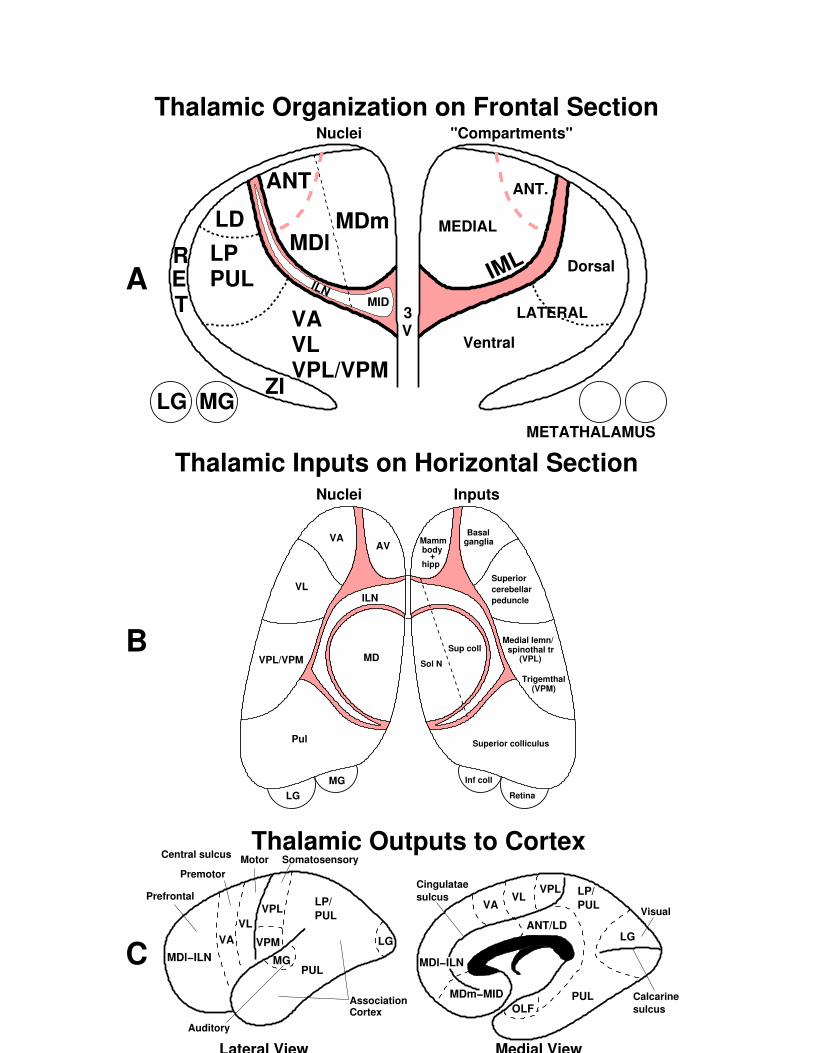
"Compartments"Nuclei
Thalamic Inputs on Horizontal Section
Thalamic Organization on Frontal Section
MIDILN
R Dorsal
Ventral
Nuclei Inputs
Retina
(VPL)
BasalMamm
+
(VPM)
Sol N
body
hipp
ganglia
spinothal trMedial lemn/
Sup coll
Superiorcerebellarpeduncle
Trigemthal
Superior colliculus
Inf coll
PUL
VPL
VPM
MG
VLVA
MDl−ILN MDl−ILN
MDm−MIDOLF
PUL
ANT/LD
VPLVL
VA
Lateral View Medial View
LG LG
Thalamic Outputs to Cortex

Thal-BG
Splenium ofCorpusCallosum
Thalamus
Genu ofCorpusCallosum
CL
GPPost
Caudate
Putamen
LV
LV
Ant
Genu
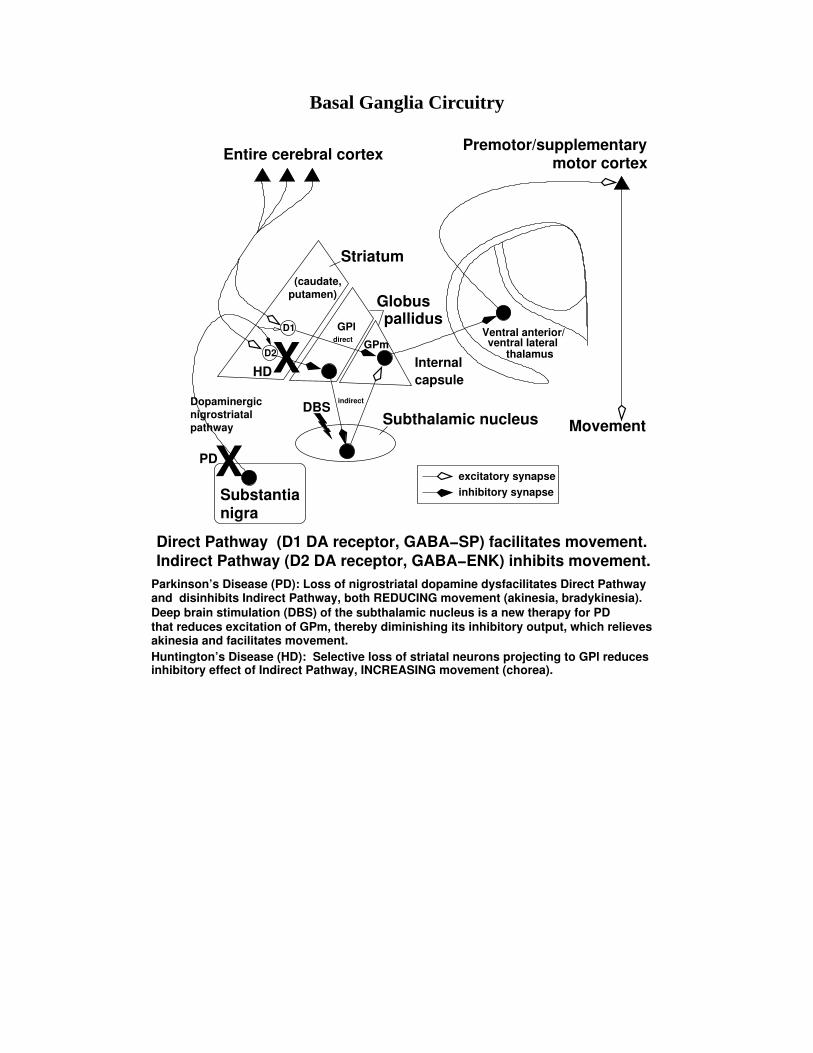
Basal Ganglia Circuitry
Indirect Pathway (D2 DA receptor, GABA−ENK) inhibits movement.Direct Pathway (D1 DA receptor, GABA−SP) facilitates movement.
D1
excitatory synapseinhibitory synapse
Internalcapsule
Dopaminergicnigrostriatal pathway
Substantianigra
Movement
GPl
XPD
XHD
motor cortexPremotor/supplementary
Ventral anterior/
Entire cerebral cortex
Striatum
Globuspallidus
(caudate,putamen)
Subthalamic nucleus
GPm ventral lateralthalamus
DBS
Parkinson’s Disease (PD): Loss of nigrostriatal dopamine dysfacilitates Direct Pathwayand disinhibits Indirect Pathway, both REDUCING movement (akinesia, bradykinesia).
D2
direct
indirect
Deep brain stimulation (DBS) of the subthalamic nucleus is a new therapy for PD
akinesia and facilitates movement.Huntington’s Disease (HD): Selective loss of striatal neurons projecting to GPl reducesinhibitory effect of Indirect Pathway, INCREASING movement (chorea).
that reduces excitation of GPm, thereby diminishing its inhibitory output, which relieves

(Houk, JC and Rymer, WZ 1981. Neural control of muscle length and tension. Handbook of Physiology.Section 1. The Nervous System, Vol. II, Motor Control, Part 1. Am Physiol Soc, Bethesda, pp 257−323)
Load
Gammamotor neurons
Alpha
Descending control signals
Length Force
ServoMotor
motor neurons
Muscle
spindlesMuscle Tendon
organs
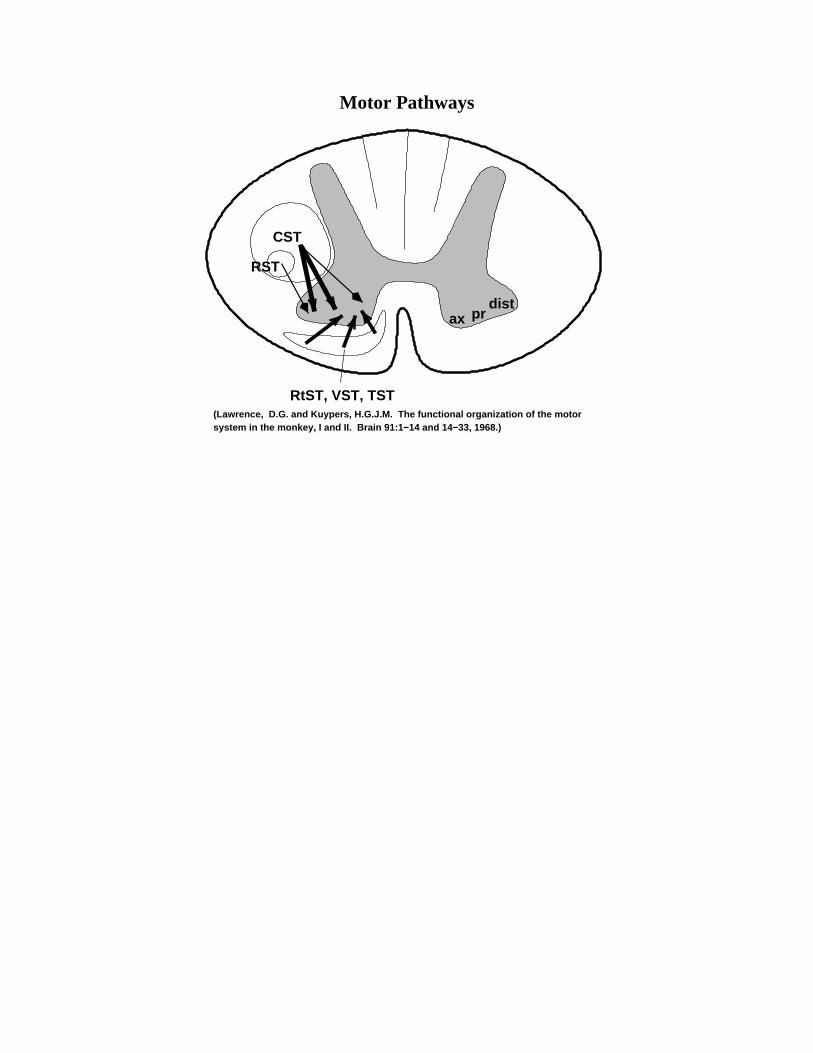
Motor Pathways
system in the monkey, I and II. Brain 91:1−14 and 14−33, 1968.)(Lawrence, D.G. and Kuypers, H.G.J.M. The functional organization of the motor
CST
RtST, VST, TST
distax pr
RST
synapse
effectsBrain Stem
Ret. Form.Upper
Motor
Neuron
α
+
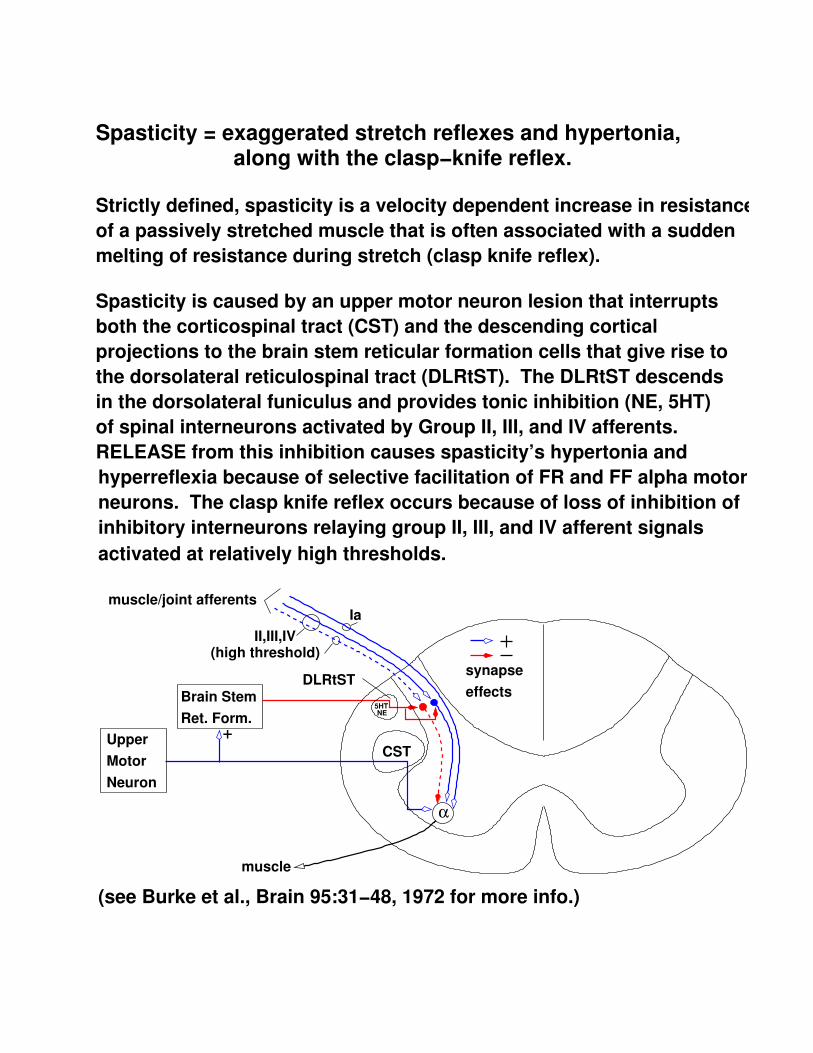
Strictly defined, spasticity is a velocity dependent increase in resistanceof a passively stretched muscle that is often associated with a suddenmelting of resistance during stretch (clasp knife reflex).
Spasticity is caused by an upper motor neuron lesion that interruptsboth the corticospinal tract (CST) and the descending cortical projections to the brain stem reticular formation cells that give rise to the dorsolateral reticulospinal tract (DLRtST). The DLRtST descendsin the dorsolateral funiculus and provides tonic inhibition (NE, 5HT) of spinal interneurons activated by Group II, III, and IV afferents.RELEASE from this inhibition causes spasticity’s hypertonia andhyperreflexia because of selective facilitation of FR and FF alpha motorneurons. The clasp knife reflex occurs because of loss of inhibition ofinhibitory interneurons relaying group II, III, and IV afferent signals activated at relatively high thresholds.
(see Burke et al., Brain 95:31−48, 1972 for more info.)
muscle/joint afferents
(high threshold)
Ia
DLRtST
muscle
CST
II,III,IV
5HTNE
Spasticity = exaggerated stretch reflexes and hypertonia, along with the clasp−knife reflex.
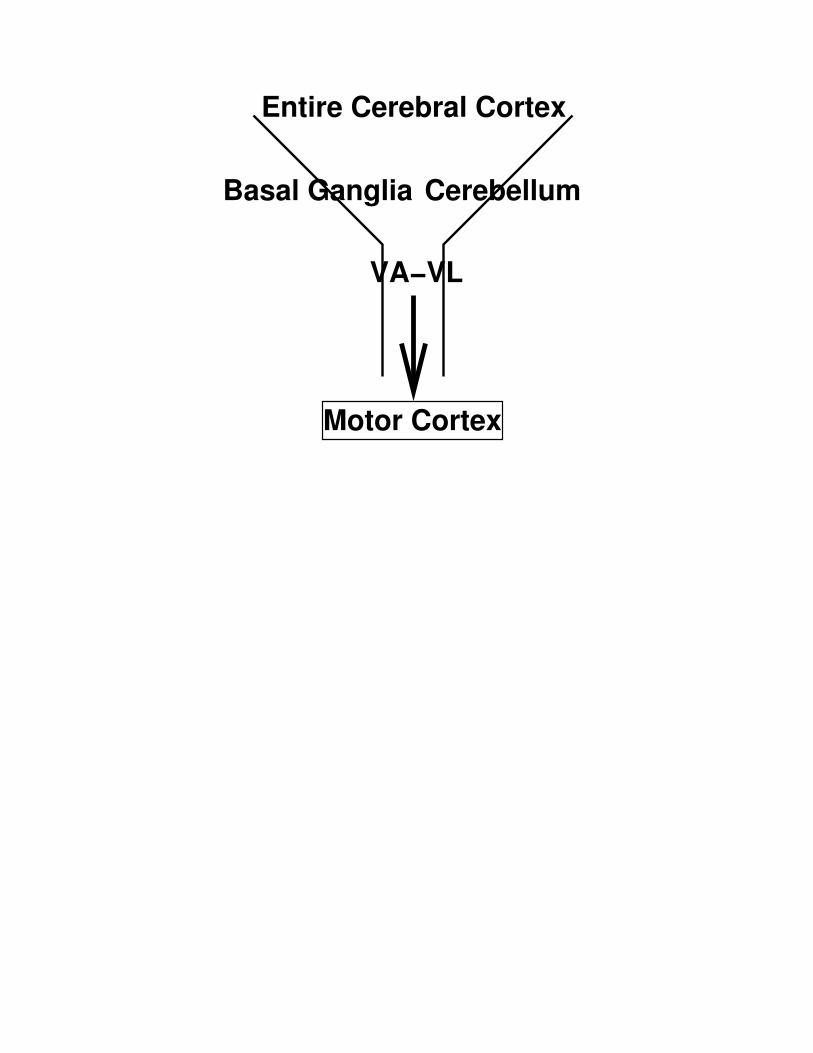
Basal Ganglia Cerebellum
Motor Cortex
Entire Cerebral Cortex
VA−VL
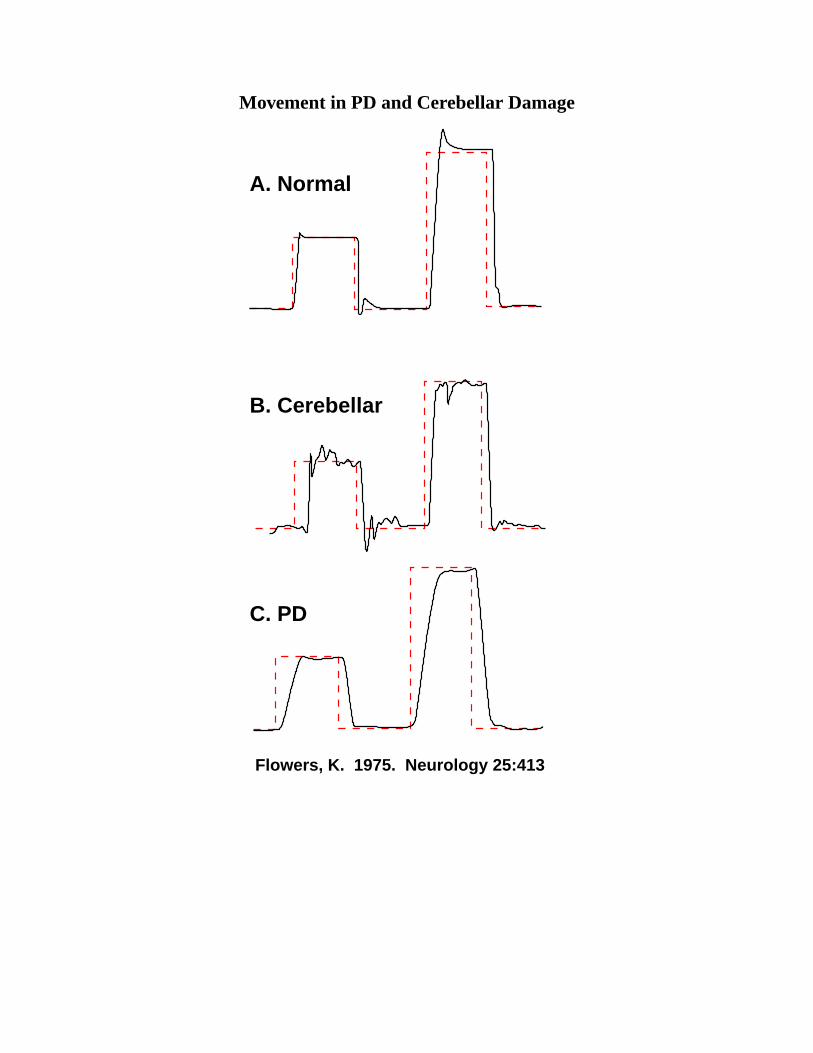
Movement in PD and Cerebellar Damage
Flowers, K. 1975. Neurology 25:413
B. Cerebellar
C. PD
A. Normal

layers
46
4
6
17
18
39
I
V
IIIII
IV
VI
Supragranular = Cortico−cortical"Association Cortex"
IIIIII
IV
VVI
Granular = Input or "Sensory Cortex"
Infragranular = Output or "Motor Cortex"
Outputs from cortical layers Inputs to cortical layers
Contralateral Cortex (callosal)
Ipsilateral Cortex
Striatum, Brainstem, Spinal Cord
Thalamus and Claustrum
Non−specific (locus ceruleus, raphe, nucleus basalis)
Cortico−cortical
Thalamus
Cerebral Cortex Layers
Cerebral Cortex Cytoarchitecture

Cortex Big Picture
Vision
Body
VisionEyes−Head
Viscera/Hormones
Eyes−Head
Where?
What?
Body
What?
Move Speech
SpeechProduction
Hearing
What?
Perception
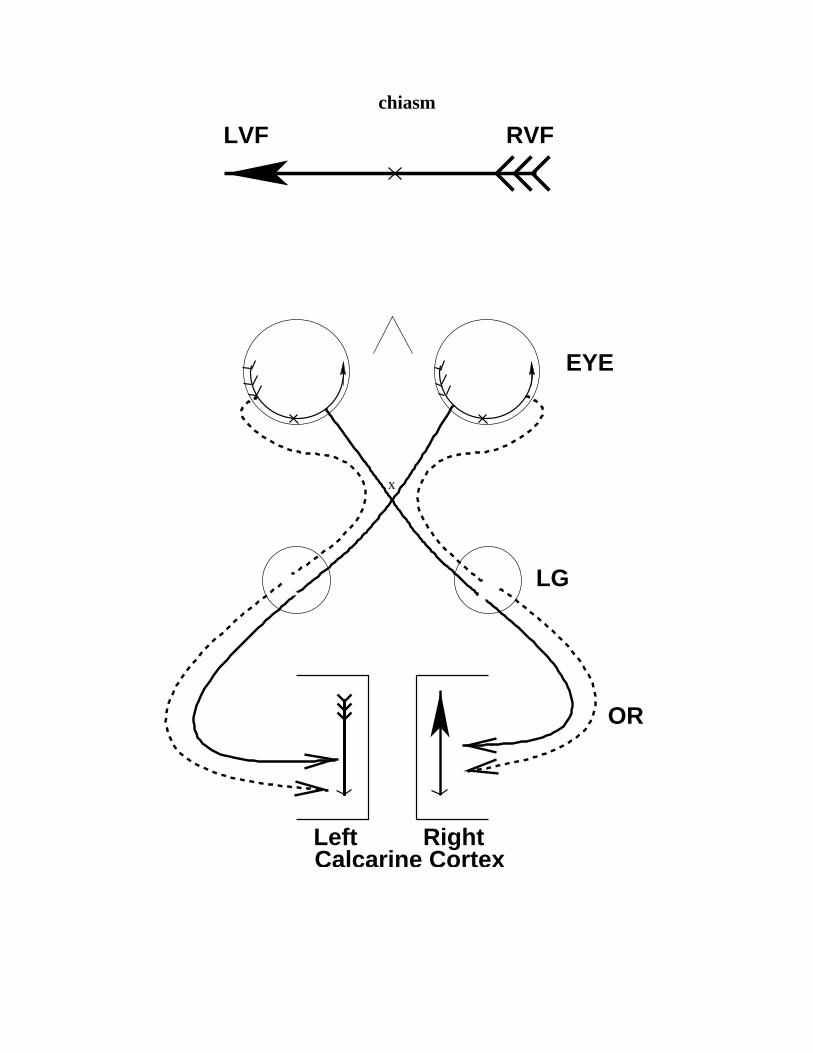
chiasm
EYE
x
LG
OR
Calcarine Cortex
LVF RVF
Left Right
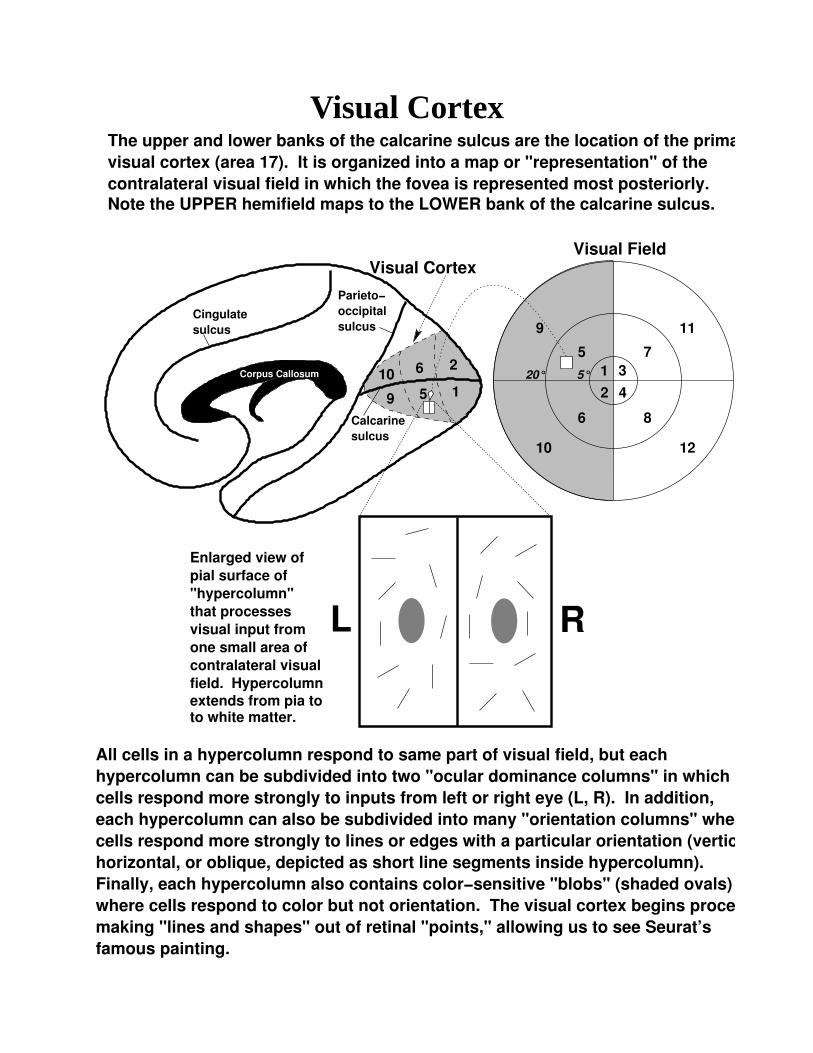
Visual Cortex
5°20°
Calcarinesulcus
Cingulatesulcus
Parieto−
sulcusoccipital
visual cortex (area 17). It is organized into a map or "representation" of thecontralateral visual field in which the fovea is represented most posteriorly.Note the UPPER hemifield maps to the LOWER bank of the calcarine sulcus.
The upper and lower banks of the calcarine sulcus are the location of the primary
Visual Field
11
12
8
73
4
1
2
5
6
10
9
1
26
59
10
pial surface of "hypercolumn" that processes visual input fromone small area ofcontralateral visual
Enlarged view of
Visual Cortex
Corpus Callosum
field. Hypercolumnextends from pia toto white matter.
All cells in a hypercolumn respond to same part of visual field, but eachhypercolumn can be subdivided into two "ocular dominance columns" in whichcells respond more strongly to inputs from left or right eye (L, R). In addition, each hypercolumn can also be subdivided into many "orientation columns" wherecells respond more strongly to lines or edges with a particular orientation (vertical,horizontal, or oblique, depicted as short line segments inside hypercolumn).
where cells respond to color but not orientation. The visual cortex begins process of making "lines and shapes" out of retinal "points," allowing us to see Seurat’s famous painting.
Finally, each hypercolumn also contains color−sensitive "blobs" (shaded ovals)
L R

odpattern
Cingulatesulcus
Parieto−
sulcusoccipital
Corpus Callosum
Calcarinesulcus
Simplified view of overall patternof ocular dominance "stripes" in primary visual cortex. Light bandrepresents LEFT eye dominance, andblack band represents RIGHT eyedominance. Small white rectanglecorresponds to hypercolumn on previous figure. Note that stripes"flow" into calcarine sulcus and then reemerge onto cortical surface.
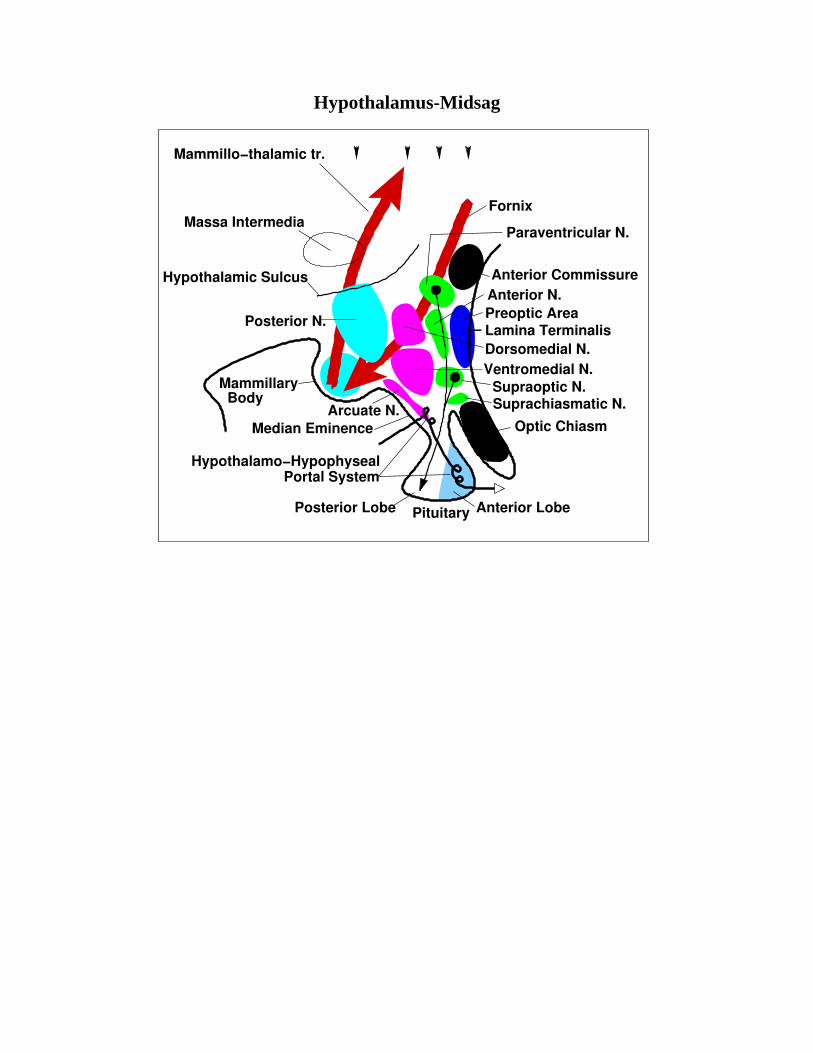
Hypothalamus-Midsag
Anterior Commissure
Paraventricular N.
Anterior N.Preoptic AreaLamina TerminalisDorsomedial N.Ventromedial N.
Supraoptic N.Suprachiasmatic N.
Optic Chiasm
Anterior LobePituitaryPosterior Lobe
Median EminenceArcuate N.
MammillaryBody
Posterior N.
Hypothalamic Sulcus
Massa Intermedia
Mammillo−thalamic tr.
Fornix
Portal SystemHypothalamo−Hypophyseal
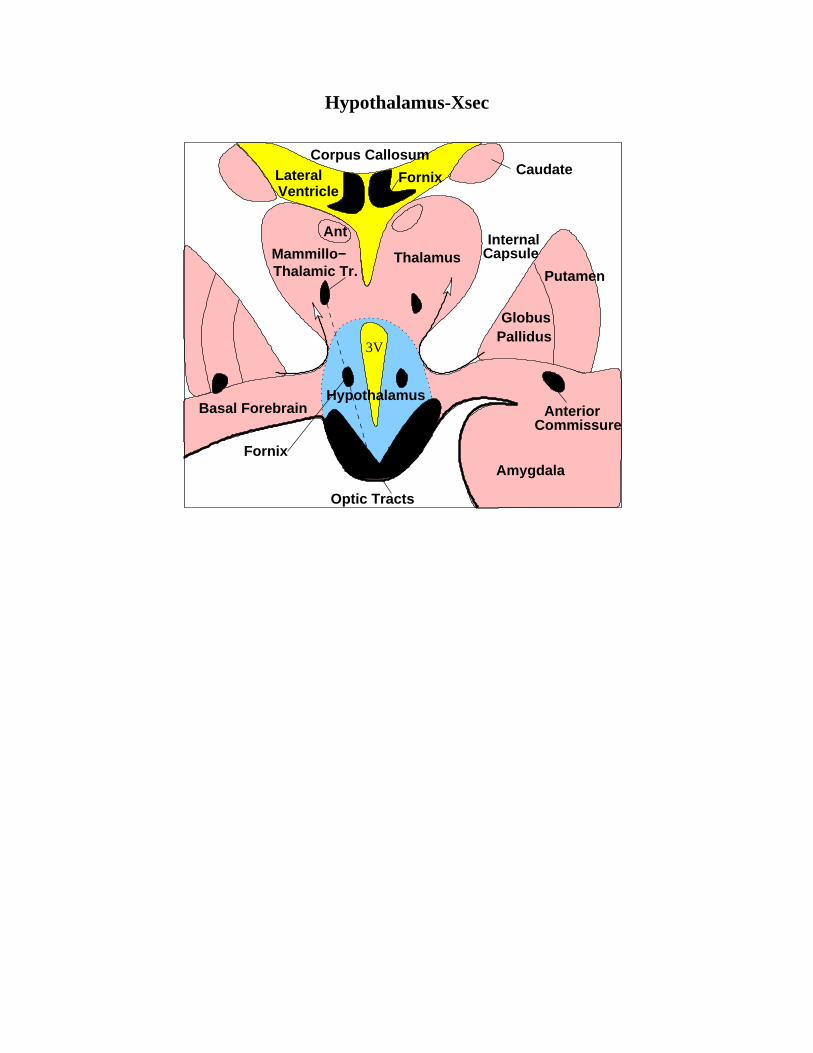
Hypothalamus-Xsec
3V
Caudate
Internal
AnteriorCommissure
Corpus Callosum
Mammillo−Thalamic Tr.
Thalamus
GlobusPallidus
Putamen
Basal Forebrain
Fornix
FornixVentricleLateral
Hypothalamus
Optic Tracts
Amygdala
Ant
Capsule
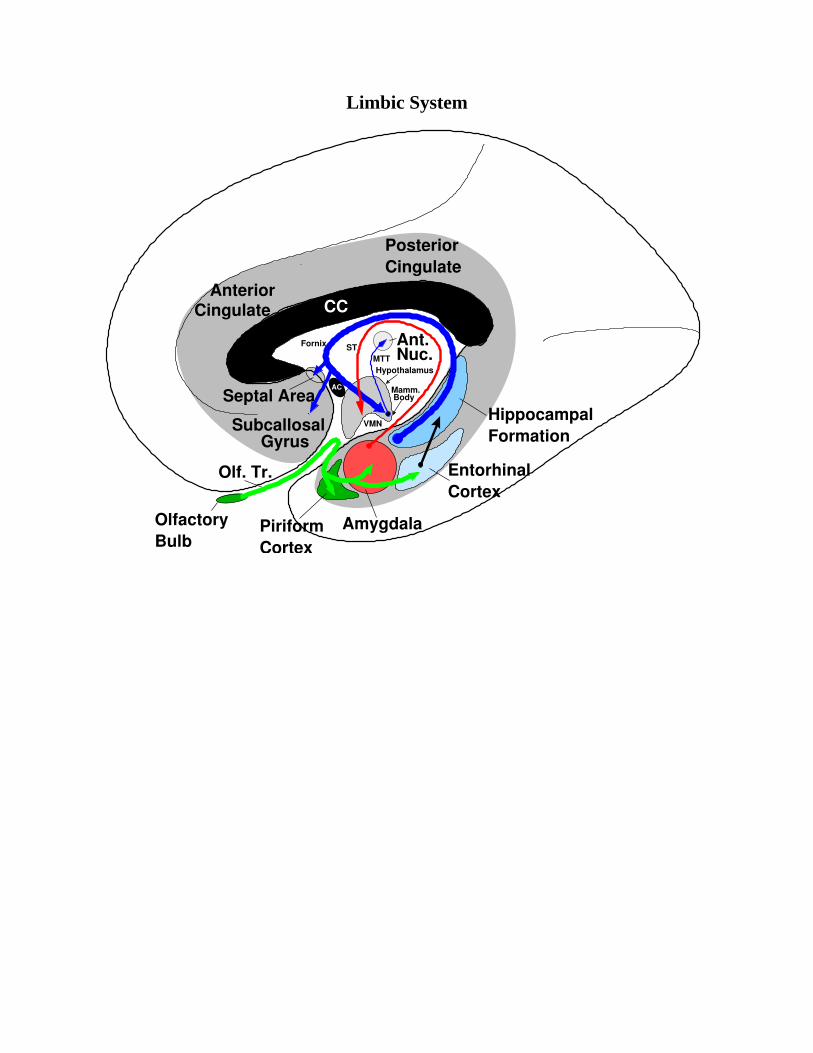
Limbic System
PiriformCortex
OlfactoryBulb
PosteriorCingulate
HippocampalFormation
CortexEntorhinal
Amygdala
Olf. Tr.
Septal Area
CingulateAnterior
CC
Ant.Nuc.ST
AC
Fornix
MTT
Body
Hypothalamus
VMNSubcallosalGyrus
Mamm.
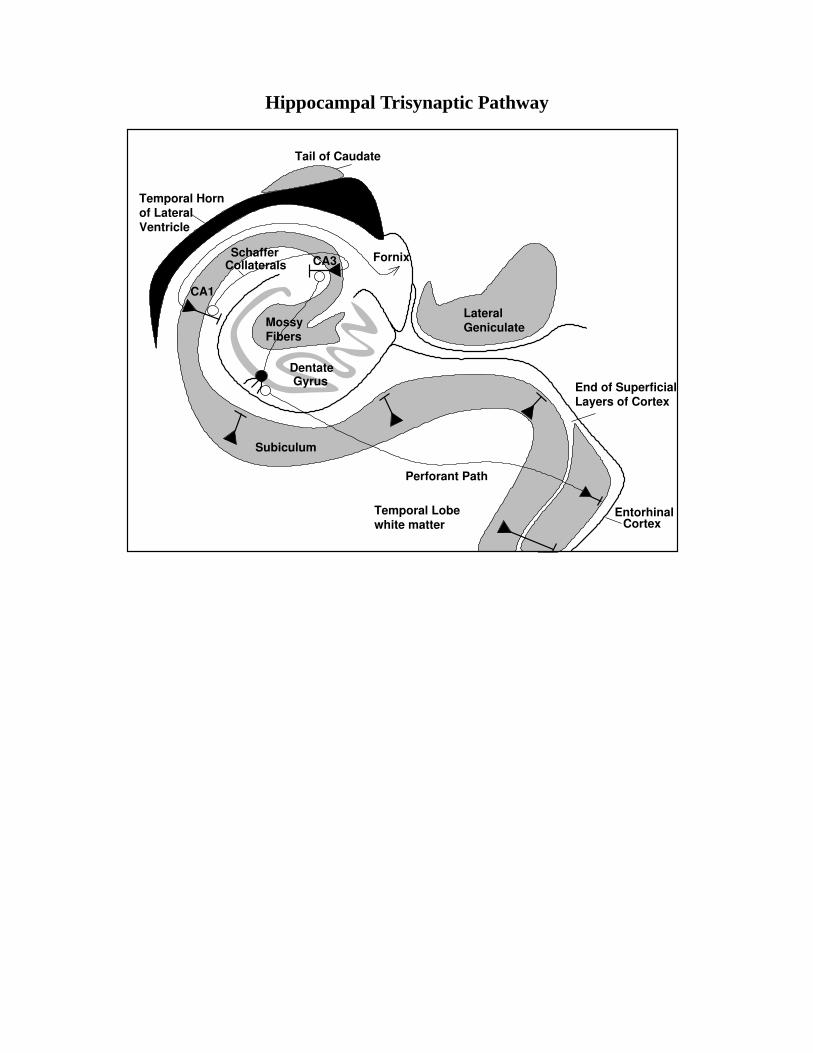
Hippocampal Trisynaptic Pathway
Temporal Horn
Ventricleof Lateral
Subiculum
white matterTemporal Lobe Entorhinal
Cortex
End of SuperficialLayers of Cortex
Fornix
Geniculate
Dentate
MossyFibers
Gyrus
CA1
SchafferCollaterals CA3
Tail of Caudate
Lateral
Perforant Path
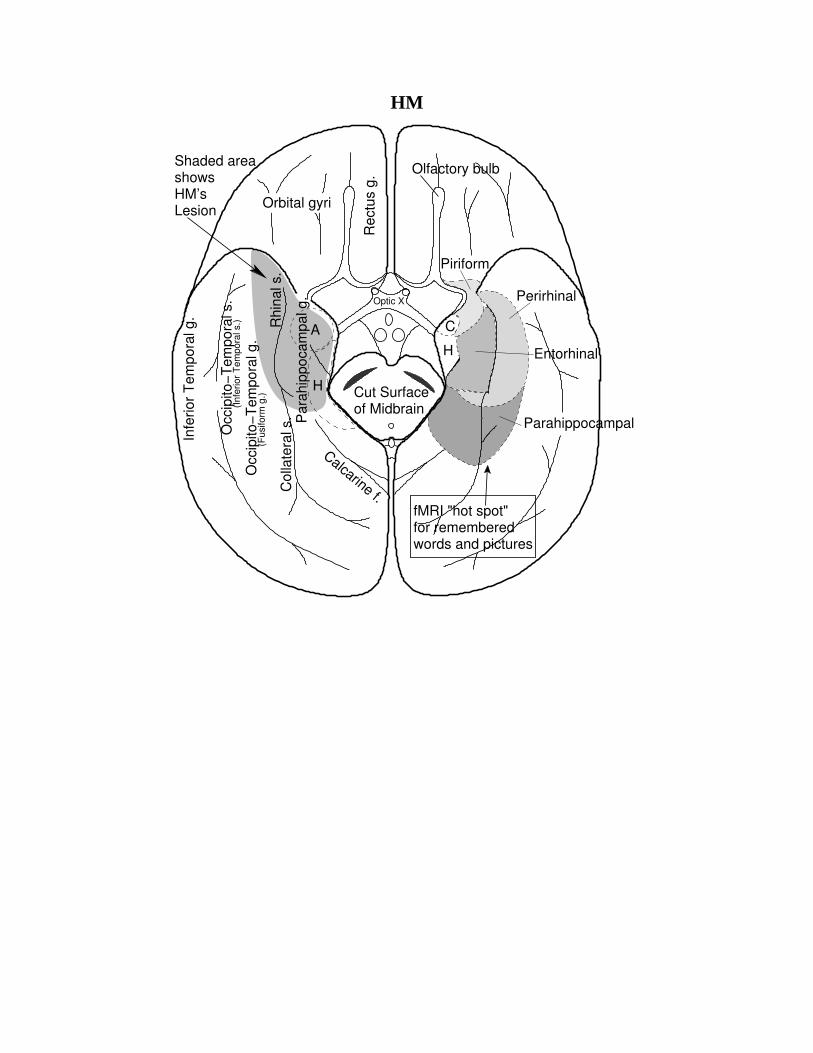
HM
Shaded areashowsHM’sLesion
A
Optic X
Calcarine f.
(Inf
erio
r T
empo
ral s
.)
Perirhinal
Parahippocampal
Piriform
Olfactory bulb
Rec
tus
g.
Infe
rior
Tem
pora
l g.
Occ
ipito
−Tem
pora
l s.
Occ
ipito
−Tem
pora
l g.
Col
late
ral s
.R
hina
l s.
Par
ahip
poca
mpa
l g.
H
(Fus
iform
g.)
fMRI "hot spot"for rememberedwords and pictures
Cut Surfaceof Midbrain
C
H
Orbital gyri
Entorhinal
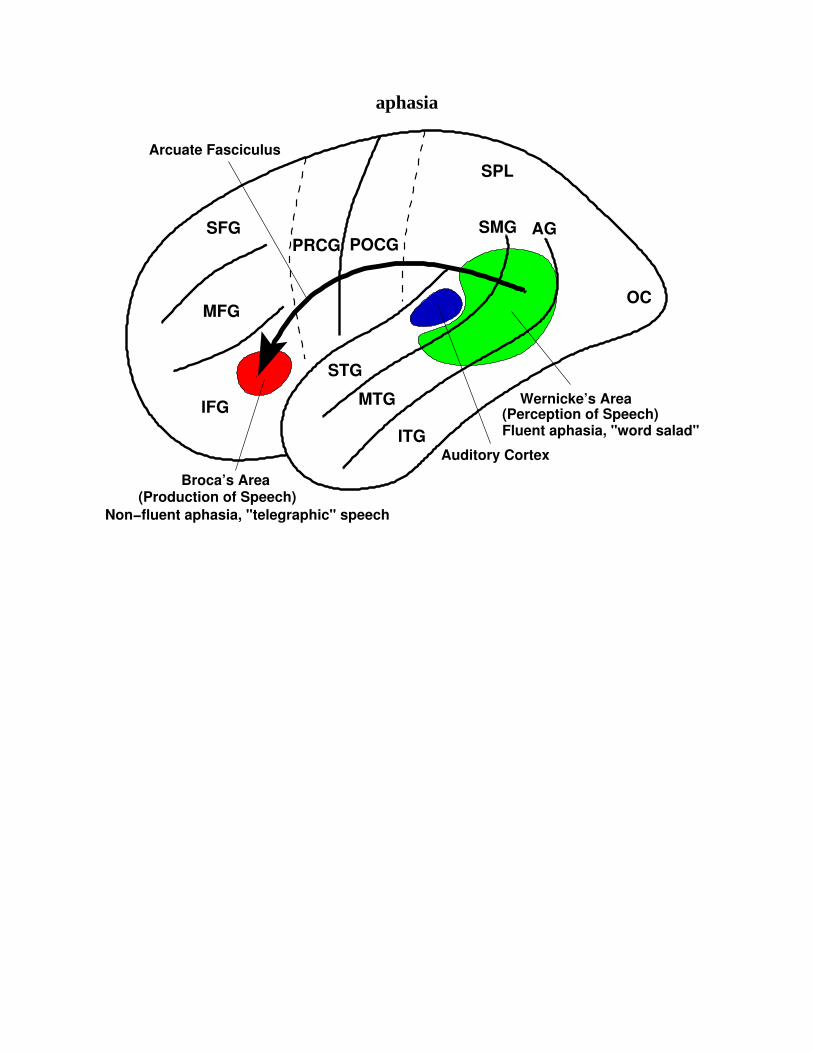
aphasia
SFG
MFG
IFG
SPL
SMG AG
OC
ITG
MTG
STG
Arcuate Fasciculus
Broca’s Area(Production of Speech)
Auditory Cortex
Wernicke’s Area(Perception of Speech)
POCGPRCG
Fluent aphasia, "word salad"
Non−fluent aphasia, "telegraphic" speech

Radersheidt: Contralateral Neglect
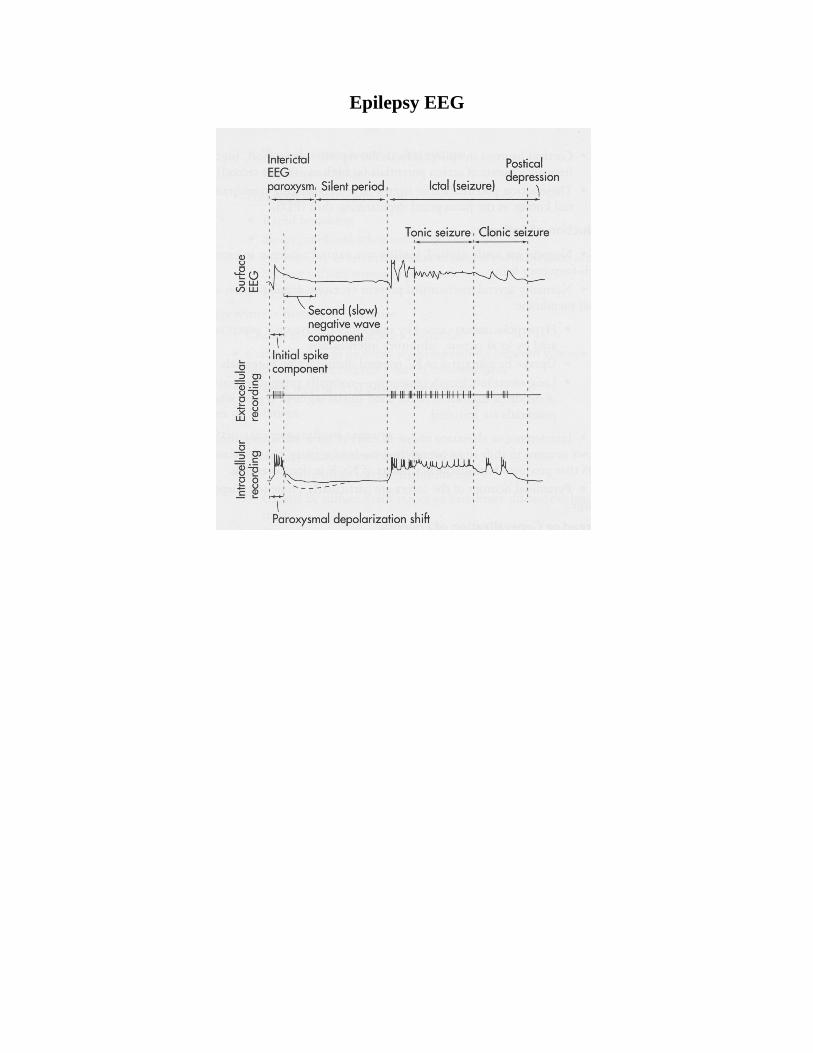
Epilepsy EEG
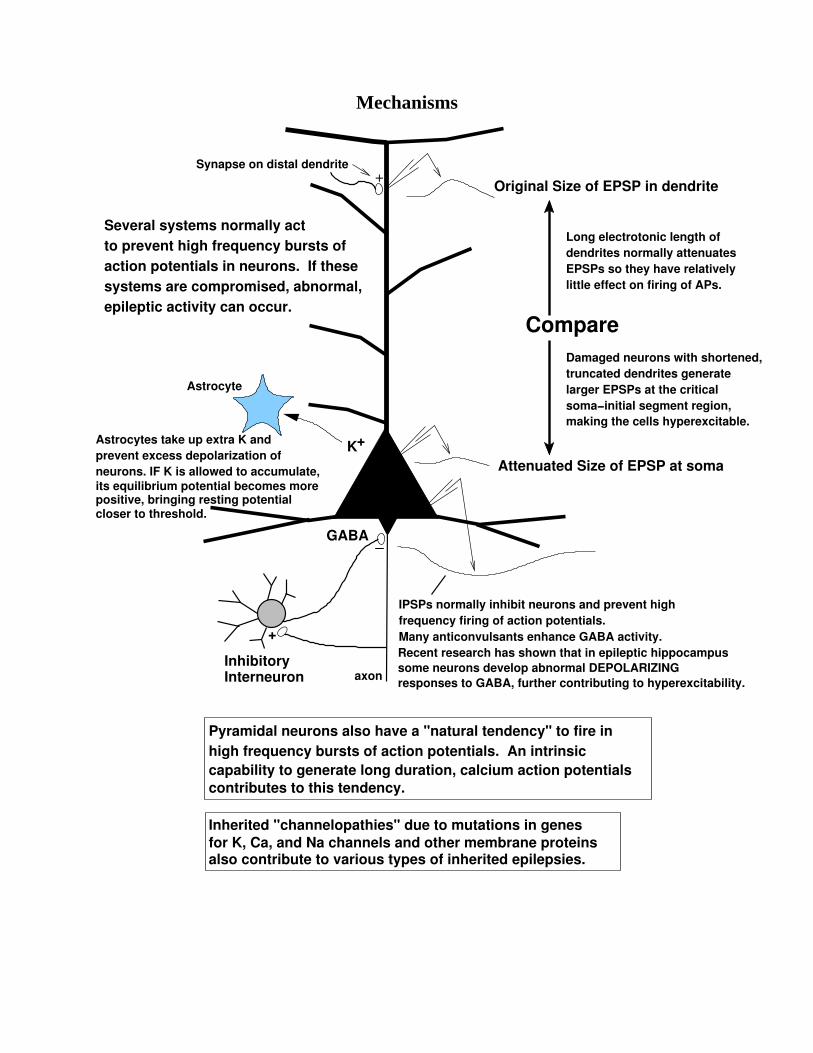
Mechanisms
K+
Pyramidal neurons also have a "natural tendency" to fire in
contributes to this tendency.
high frequency bursts of action potentials. An intrinsiccapability to generate long duration, calcium action potentials
action potentials in neurons. If these to prevent high frequency bursts ofSeveral systems normally act
epileptic activity can occur.systems are compromised, abnormal,
Original Size of EPSP in dendrite
InhibitoryInterneuron
Compare
Inherited "channelopathies" due to mutations in genes
also contribute to various types of inherited epilepsies.for K, Ca, and Na channels and other membrane proteins
GABA
Long electrotonic length of dendrites normally attenuatesEPSPs so they have relativelylittle effect on firing of APs.
Astrocytes take up extra K andprevent excess depolarization ofneurons. IF K is allowed to accumulate,its equilibrium potential becomes morepositive, bringing resting potentialcloser to threshold.
+
Attenuated Size of EPSP at soma
Astrocyte
Synapse on distal dendrite
Damaged neurons with shortened,truncated dendrites generatelarger EPSPs at the criticalsoma−initial segment region, making the cells hyperexcitable.
_
+
IPSPs normally inhibit neurons and prevent highfrequency firing of action potentials.Many anticonvulsants enhance GABA activity.
axon
Recent research has shown that in epileptic hippocampus
responses to GABA, further contributing to hyperexcitability.some neurons develop abnormal DEPOLARIZING