bowel elimination professor hill, rn, mn, msg an bernardino valley college nursing 102
TRANSCRIPT
Bowel Bowel EliminationElimination
Professor Hill, RN, MN, MSG
an Bernardino Valley College
Nursing 102

At The End of This Lecture, The Learner Will..
Explain the role of the GI system in digestion & elimination
Describe factors that influence elimination
Assess bowel elimination through subjective & objective assessments
Discuss 3 elimination problems and the nursing interventions for each
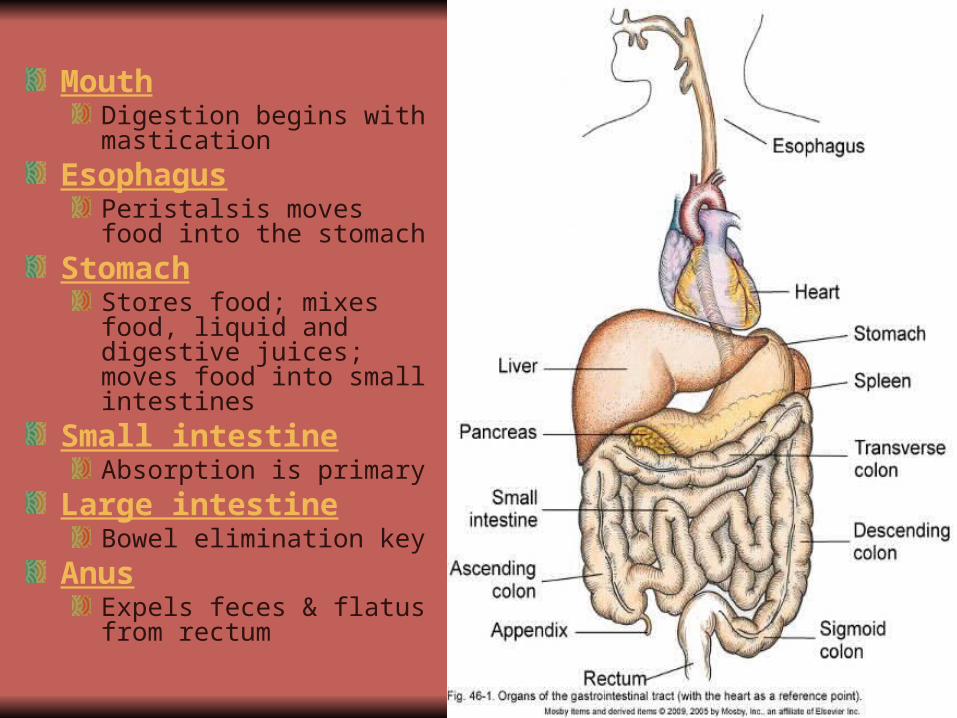
Mouth Digestion begins with mastication
EsophagusPeristalsis moves food into the stomach
Stomach Stores food; mixes food, liquid and digestive juices; moves food into small intestines
Small intestineAbsorption is primary
Large intestineBowel elimination key
Anus Expels feces & flatus from rectum

http://www.youtube.com/watch?v=HA8iL7hs5YY

Factors Affecting Bowel Elimination
Food & fluid Physical activityPsychological factorsBowel habitsMedicationsDiagnostic testsPathological conditionsSurgery & pain

Effects of Aging on GI Tract
Periodontal disease
Decrease in saliva
Decrease in gastric secretions
Smooth muscle changes, decreased esophageal peristalsis
Decreased GI motility


Subjective Assessment Questions
Usual pattern of bowel elimination?
Aids to elimination?
Recent changes in
bowel elimination?
Problems with bowel
elimination?
Physical Assessment
Inspect mouth
AbdomenInspection
Auscultation
Palpation

Stool Characteristics
Color
Odor
Consistency
Shape
Volume
Constituents

Laboratory Tests
Fecal specimens for labMedical asepsis- wear gloves
Obtain specimen, label & seal container
Place container in biohazard bag
Send immediately to lab
Fecal occult blood testing @ bedside (POCT)Medical asepsis
Small amount of stool
Follow instructions per tester
Void firstNO toilet paper!Menstruating?


Diagnostic Studies
Esophagogastroduodenoscopy
(EGD)
Endoscopy
Upper GI series
Barium enema
Sigmoidoscopy
Before:Consent signedNPOLower GI studies: Bowel cleansing
Aftercare:Vital signsThroat sorenessAssess stoolsCathartics to cleanse barium from GI tract
Nursing Care

Upper GI series Barium Enema Flexible Sigmoidoscopy


Constipation (Symptom!)
Slowed gastric motility
Slowed passage of feces in large intestine
Fecal water content absorbed through walls
Result is dry, hard stool
Constipation
Signs: infrequent bowel movements
difficulty passing stools
Excessive straining
Hypoactive bowel sounds

Constipation
Causes:Decreased fiber
Reduced fluid intake
Immobility
Anxiety, depression
Medications
Abuse of laxatives
Delaying defecation

Valsalva Maneuver
Individual bears down
Thoracic/abdominal pressure
Blood flow to atria/ventricles = low CO
Bearing down stops
Large amount of blood returns to heart = BP
Nursing Interventions- Constipation
Provide privacy
Positioning
High fiber intake
Ambulation
Increase fluid intake to 2,000-3,000ml/day

Cathartics & Laxatives
Bulk forming Metamucil Stool swells
Emollient/stool softeners
Docusate sodium (colace)
Water & fat penetrates BM
Saline MOM, Fleet enema
Draws water into intestine
Stimulant Bisacodyl (dulcolax)
Irritate mucosa
Increase motility
Lubricants Mineral oil Coats & softens
feces
Enemas
Instillation of solution into rectum/colon
Promotes peristalsis
Fluid breaks up fecal mass
Stretches the rectal wall
Initiates defecation reflex
Indicated for relief of constipation, Impacted feces, diagnostic test/surgery

Types of Cleansing Enemas
Hypotonic- Tap water- give once onlyNormal Saline -safestHypertonic Solutions- Fleets enemaSoapsuds-castile soapOil retention -lubricate/hold for hours
**Enemas till clear- do not repeat more than 3 times

Enemas
Patient positioning
Preparation of equipment
High enema- cleanses higher up colon12-18 inches above anus
Low enema- cleanses rectum & sigmoid12 inches or lower
Return flow enemas (Harris flush)

Impaction
Collection of hardened feces wedged in rectumCan be palpated by digital examSigns: oozing of diarrhea stool, frequency, rectal painTreatment: oil retention enema, cleansing enemas, suppositories, last resort…Manual removal of impacted feces

Diarrhea
Signs:
Passage of excessively liquid, unformed stools
Contents pass through GI system too quickly = too much fluid & mucous
Causes:Altered GI flora
Enteral nutrition
Food allergies
Food intolerances
Clostridium difficile
Food borne pathogens
Abdominal cramps
HyperactiveBowel sounds
Nausea & vomiting
Fluid & Electrolyte Imbalances

Diarrhea Treatment
Acute diarrhea: oral rehydration therapy,
Chronic diarrhea > 3-4 wks:
Replacement of fluids with electrolytes
Oral if tolerated
If severe, may need IV fluid replacement
Act on GI smooth muscle to slow motility
Paregoric (opiate deriv)
Lomotil
Imodium
Act as an absorbent Kaopectate

In Closing….
http://www.youtube.com/watch?v=Ve_XxOpj-MY

QUESTIONS