c-arm fluoroscopy draping: a comparison of three … · background / objectives methods discussion...
TRANSCRIPT
Background / Objectives
Methods
Discussion
C-Arm Fluoroscopy Draping: A Comparison of Three Techniques Grigory Gershkovich MD, David Hampton MD, Nathan Tiedeken MD, Ross Budacki MD, Minn Saing, MD, Solomon Samuel D. Eng.
Department of Orthopedic Surgery, Einstein Medical Center, Philadelphia PA
Results Background: Sterility is of paramount importance in the operative theatre. Maintaining a sterile field while using large intraoperative equipment becomes difficult. Objective: To directly compare three draping techniques of the c-arm x-ray machine in their ability to maintain a sterile field and surgeon.
Set-up: Glo GermTM powder is spread beneath the OR table to simulate contamination. Glo GermTM fluoresces blue with UV light. It is checked after each trial for proximity to the sterile field or presence on the surgeon’s gown or gloves. To be considered true contaminant, it had to measure at least 5 mm thick. The five closest contaminants were recorded. Trials: After sterile draping, the c-arm was maneuvered 10 times from the AP to lateral positions. During the trials, the surgeon moved above and below the c-arm 6 times to simulate intra-op movement. Five trials were performed for the traditional method, 3 for the clip-drape, and 4 for the C-Armor®. Draping techniques: • Traditional - A three-quarter sterile sheet was attached
to the side of the OR table. The free end fell towards the ground with the c-arm in the AP position, but hung freely over the c-arm when in the lateral position.
• Clip drape – similar to the traditional technique, but the sterile sheet free end was clipped to the side of the table with towel clips during the AP position.
• C-Armor® – a commercially available product created a sterile pouch for the c-arm during the lateral position. In AP position, the pouch was secured to the bed with pre-designed Velcro strips.
Distance of contaminant from
top of drape
Gown or gloves dirty?
Traditional #1 0 0 0 0 0 yes
#2 0 6 7 8 10 yes
#3 0 0 0 2 2.5 yes
#4 0 0 0 0 0 yes
#5 10 10 10 17 33 yes
Clip-drape #1 43 46 48 55 63 No
#2 49 52 55 57 61 No
#3 90 91 87 90 91 No
C-Armor® #1 57 > 100 > 100 > 100 > 100 No
#2 85 86 >110 >110 No
#3 100 102 105 >110 >110 No
#4 105 110 >110 >110 >110
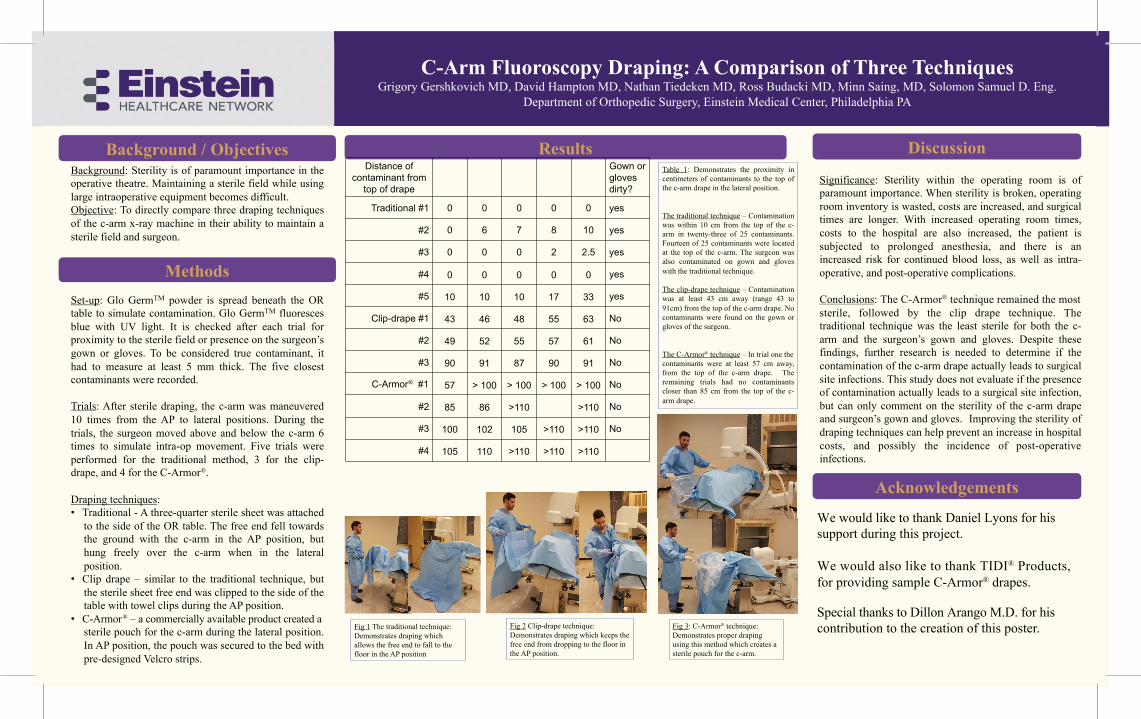
Table 1: Demonstrates the proximity in centimeters of contaminants to the top of the c-arm drape in the lateral position. The traditional technique – Contamination was within 10 cm from the top of the c-arm in twenty-three of 25 contaminants. Fourteen of 25 contaminants were located at the top of the c-arm. The surgeon was also contaminated on gown and gloves with the traditional technique. The clip-drape technique – Contamination was at least 43 cm away (range 43 to 91cm) from the top of the c-arm drape. No contaminants were found on the gown or gloves of the surgeon. The C-Armor® technique – In trial one the contaminants were at least 57 cm away, from the top of the c-arm drape. The remaining trials had no contaminants closer than 85 cm from the top of the c-arm drape.
Significance: Sterility within the operating room is of paramount importance. When sterility is broken, operating room inventory is wasted, costs are increased, and surgical times are longer. With increased operating room times, costs to the hospital are also increased, the patient is subjected to prolonged anesthesia, and there is an increased risk for continued blood loss, as well as intra-operative, and post-operative complications. Conclusions: The C-Armor® technique remained the most sterile, followed by the clip drape technique. The traditional technique was the least sterile for both the c-arm and the surgeon’s gown and gloves. Despite these findings, further research is needed to determine if the contamination of the c-arm drape actually leads to surgical site infections. This study does not evaluate if the presence of contamination actually leads to a surgical site infection, but can only comment on the sterility of the c-arm drape and surgeon’s gown and gloves. Improving the sterility of draping techniques can help prevent an increase in hospital costs, and possibly the incidence of post-operative infections.
Acknowledgements
We would like to thank Daniel Lyons for his support during this project. We would also like to thank TIDI® Products, for providing sample C-Armor® drapes.
Special thanks to Dillon Arango M.D. for his contribution to the creation of this poster.
Fig 1 The traditional technique: Demonstrates draping which allows the free end to fall to the floor in the AP position
Fig 2 Clip-drape technique: Demonstrates draping which keeps the free end from dropping to the floor in the AP position.
Fig 3: C-Armor® technique: Demonstrates proper draping using this method which creates a sterile pouch for the c-arm.