cabg in 2012: implications of the new esc/eacts guidelines
TRANSCRIPT
David P Taggart MD PhD FRCS Professor of Cardiovascular Surgery, University of Oxford
Conflicts of Interest: (i) Clinical: Cardiac Surgeon (ii) Political: President SCTS GB and Ireland; Chair ESC Working Group Cardiovascular Surgery (iii) Commercial: Consultant to Medtronic, Abbott, AstraZeneca, Novadaq, VGS, (iv) One of 25 ESC/EACTS Guidelines Writers on Myocardial Revascularization
CABG in 2012: Implications of the New ESC/EACTS Guidelines
Southern Thoracic Surgical Association 2011
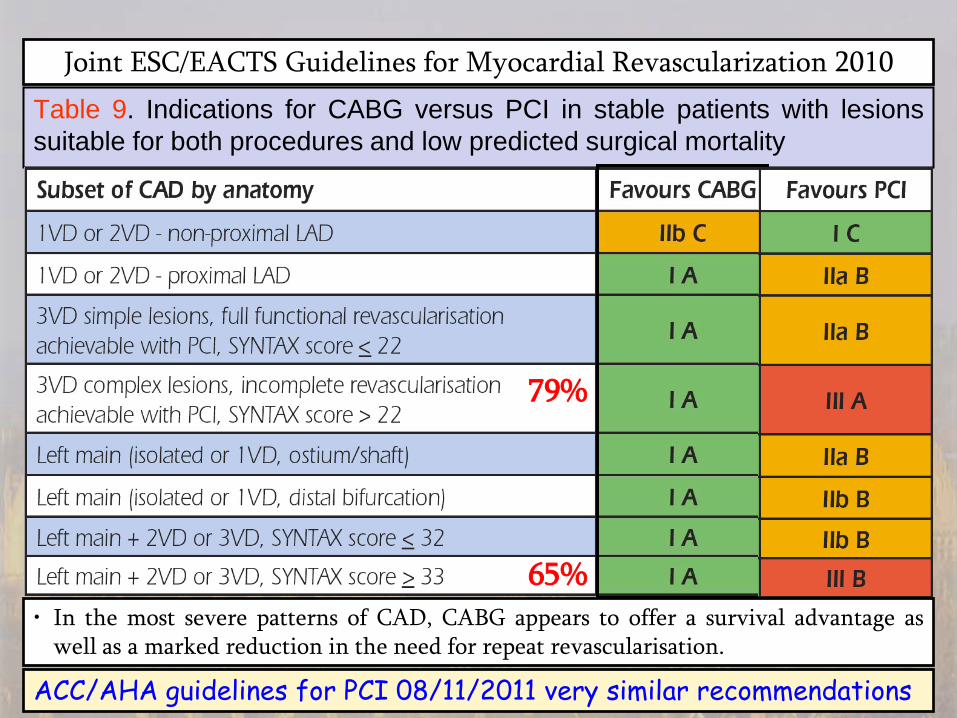
Joint ESC/EACTS Guidelines for Myocardial Revascularization 2010 Table 9. Indications for CABG versus PCI in stable patients with lesions suitable for both procedures and low predicted surgical mortality
• In the most severe patterns of CAD, CABG appears to offer a survival advantage as well as a marked reduction in the need for repeat revascularisation.
79%
65%
ACC/AHA guidelines for PCI 08/11/2011 very similar recommendations
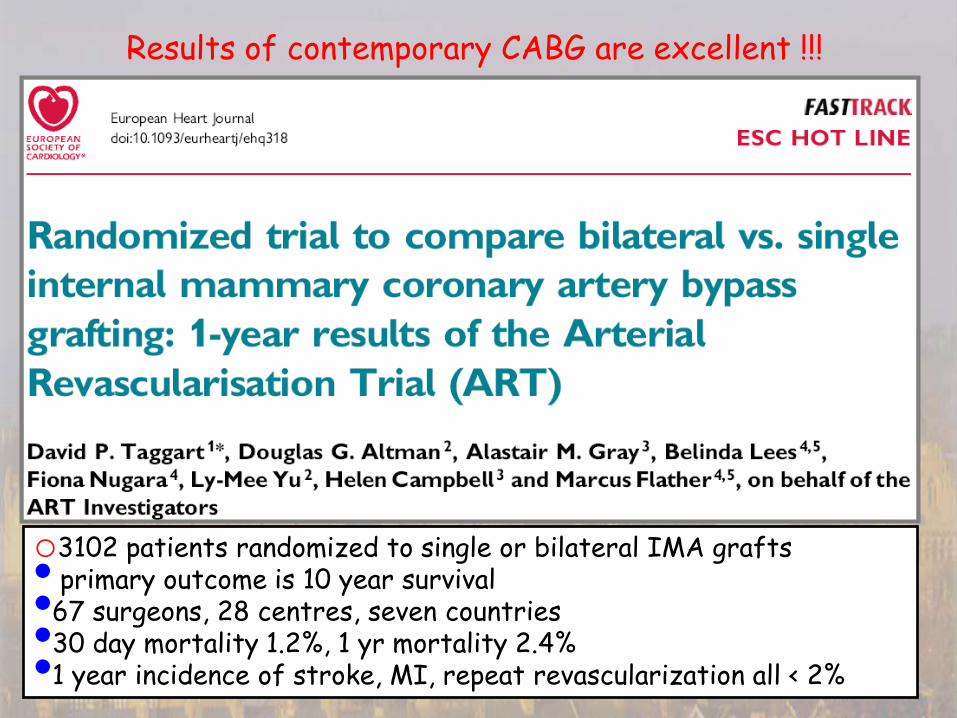
o3102 patients randomized to single or bilateral IMA grafts • primary outcome is 10 year survival •67 surgeons, 28 centres, seven countries •30 day mortality 1.2%, 1 yr mortality 2.4% •1 year incidence of stroke, MI, repeat revascularization all < 2%
Results of contemporary CABG are excellent !!!
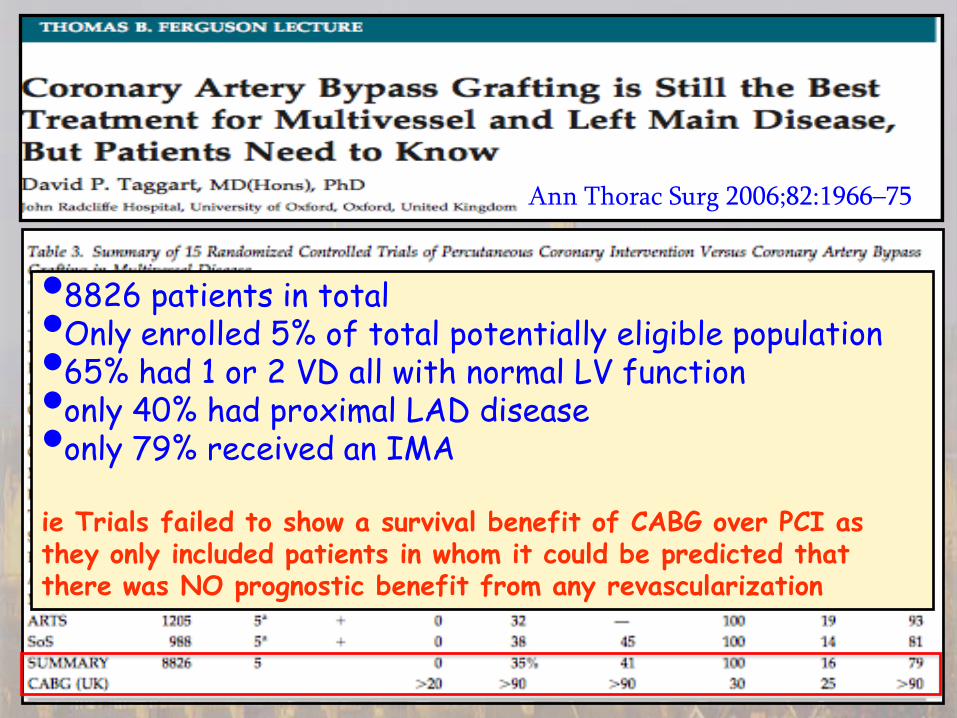
Ann Thorac Surg 2006;82:1966–75
•8826 patients in total •Only enrolled 5% of total potentially eligible population •65% had 1 or 2 VD all with normal LV function •only 40% had proximal LAD disease •only 79% received an IMA
ie Trials failed to show a survival benefit of CABG over PCI as they only included patients in whom it could be predicted that there was NO prognostic benefit from any revascularization
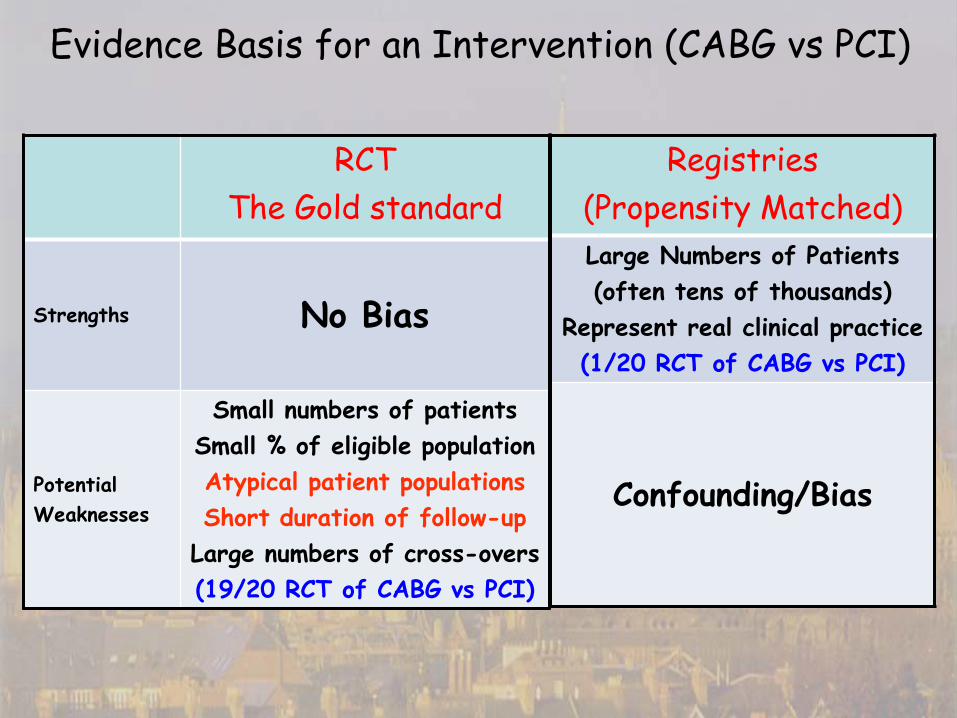
Evidence Basis for an Intervention (CABG vs PCI)
RCT The Gold standard
Strengths No Bias
Potential Weaknesses
Small numbers of patients Small % of eligible population Atypical patient populations Short duration of follow-up
Large numbers of cross-overs (19/20 RCT of CABG vs PCI)
Registries (Propensity Matched) Large Numbers of Patients (often tens of thousands)
Represent real clinical practice (1/20 RCT of CABG vs PCI)
Confounding/Bias

3VD (No Left Main)
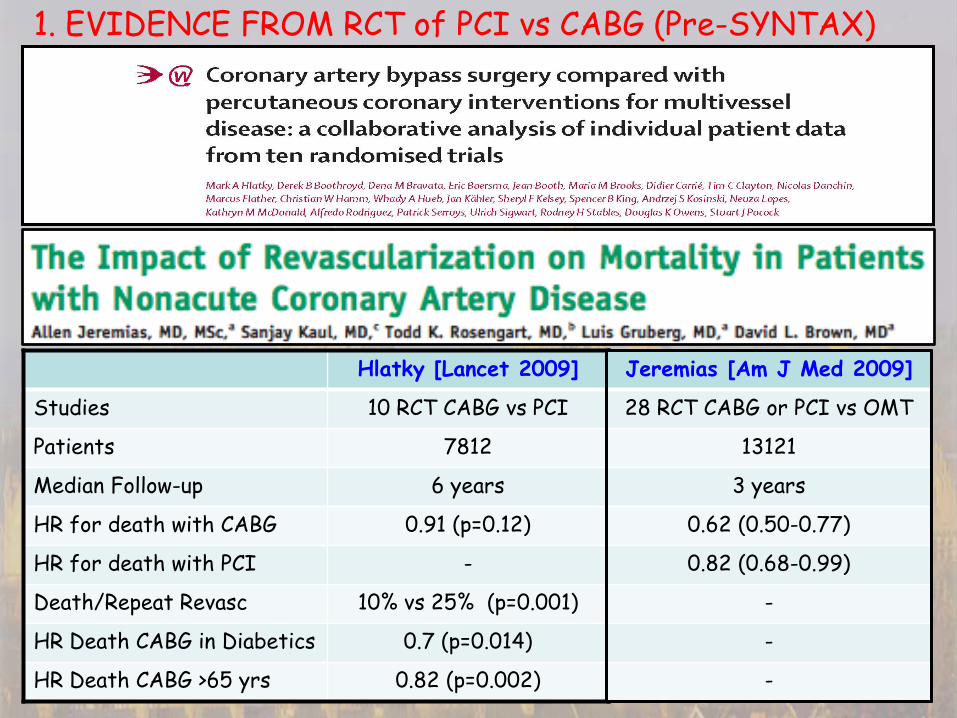
Hlatky [Lancet 2009]
Studies 10 RCT CABG vs PCI
Patients 7812
Median Follow-up 6 years
HR for death with CABG 0.91 (p=0.12)
HR for death with PCI -
Death/Repeat Revasc 10% vs 25% (p=0.001)
HR Death CABG in Diabetics 0.7 (p=0.014)
HR Death CABG >65 yrs 0.82 (p=0.002)
Jeremias [Am J Med 2009]
28 RCT CABG or PCI vs OMT
13121
3 years
0.62 (0.50-0.77)
0.82 (0.68-0.99)
-
-
-
1. EVIDENCE FROM RCT of PCI vs CABG (Pre-SYNTAX)
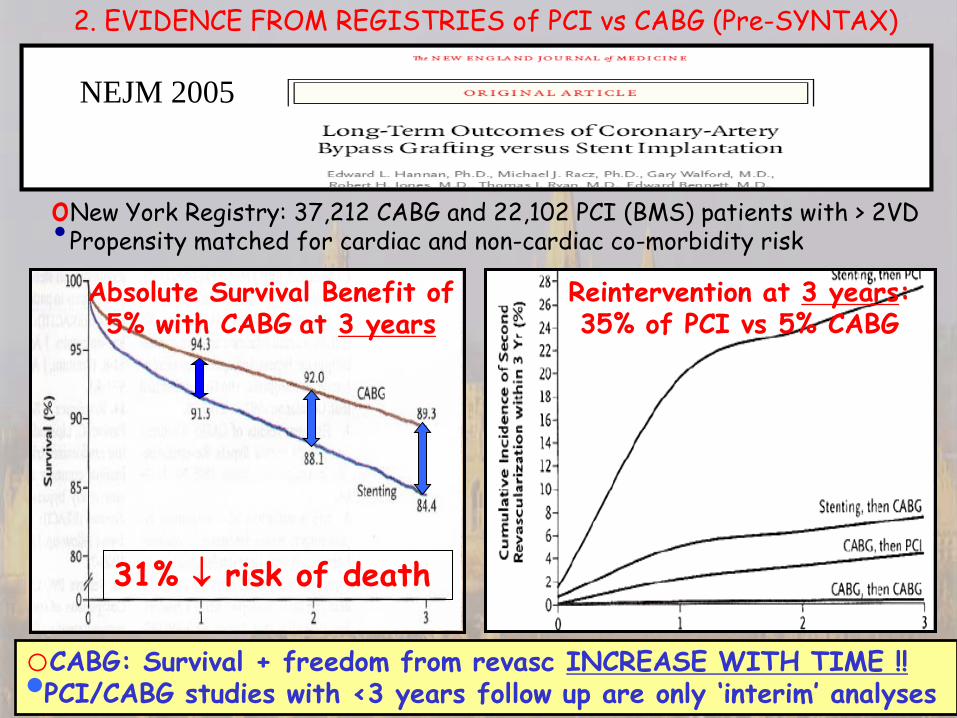
oNew York Registry: 37,212 CABG and 22,102 PCI (BMS) patients with > 2VD •Propensity matched for cardiac and non-cardiac co-morbidity risk
Absolute Survival Benefit of 5% with CABG at 3 years
Reintervention at 3 years: 35% of PCI vs 5% CABG
NEJM 2005
31% ↓ risk of death
oCABG: Survival + freedom from revasc INCREASE WITH TIME !! •PCI/CABG studies with <3 years follow up are only ‘interim’ analyses
2. EVIDENCE FROM REGISTRIES of PCI vs CABG (Pre-SYNTAX)
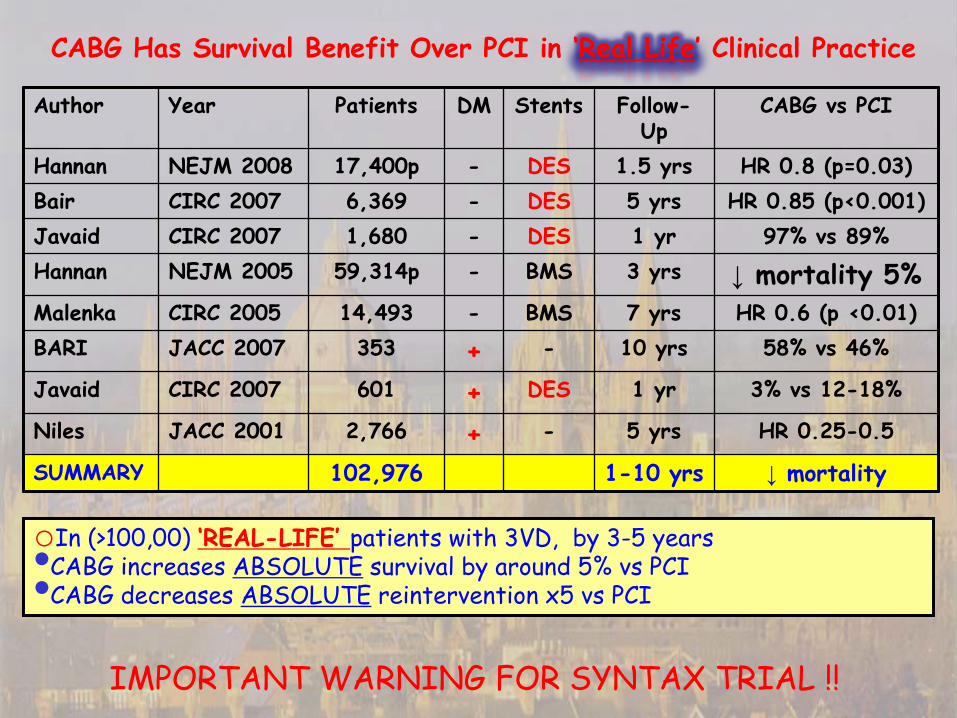
Author Year Patients DM Stents Follow-Up
CABG vs PCI
Hannan NEJM 2008 17,400p - DES 1.5 yrs HR 0.8 (p=0.03) Bair CIRC 2007 6,369 - DES 5 yrs HR 0.85 (p<0.001) Javaid CIRC 2007 1,680 - DES 1 yr 97% vs 89% Hannan NEJM 2005 59,314p - BMS 3 yrs ↓ mortality 5% Malenka CIRC 2005 14,493 - BMS 7 yrs HR 0.6 (p <0.01) BARI JACC 2007 353 + - 10 yrs 58% vs 46%
Javaid CIRC 2007 601 + DES 1 yr 3% vs 12-18%
Niles JACC 2001 2,766 + - 5 yrs HR 0.25-0.5
SUMMARY 102,976 1-10 yrs ↓ mortality
oIn (>100,00) ‘REAL-LIFE’ patients with 3VD, by 3-5 years •CABG increases ABSOLUTE survival by around 5% vs PCI •CABG decreases ABSOLUTE reintervention x5 vs PCI
CABG Has Survival Benefit Over PCI in ‘Real Life’ Clinical Practice
IMPORTANT WARNING FOR SYNTAX TRIAL !!
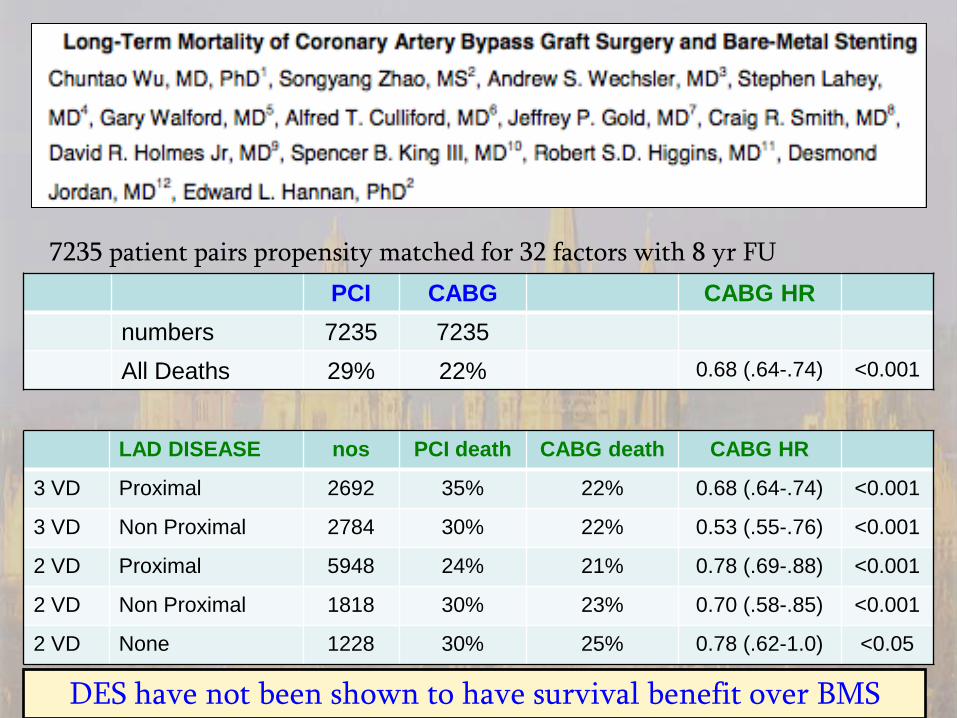
7235 patient pairs propensity matched for 32 factors with 8 yr FU PCI CABG CABG HR
numbers 7235 7235 All Deaths 29% 22% 0.68 (.64-.74) <0.001
LAD DISEASE nos PCI death CABG death CABG HR
3 VD Proximal 2692 35% 22% 0.68 (.64-.74) <0.001
3 VD Non Proximal 2784 30% 22% 0.53 (.55-.76) <0.001
2 VD Proximal 5948 24% 21% 0.78 (.69-.88) <0.001
2 VD Non Proximal 1818 30% 23% 0.70 (.58-.85) <0.001
2 VD None 1228 30% 25% 0.78 (.62-1.0) <0.05
DES have not been shown to have survival benefit over BMS
‘Most significantly, the randomized trials only enrolled around 5%-10% of the eligible population, the majority of whom had single or double vessel disease and normal left ventricular function [2], a group in whom it was already well established that there was no prognostic benefit of CABG [3]. By largely excluding patients with a known survival benefit from CABG (left main+/- triple vessel coronary artery disease and especially with impaired ventricular function [3]), the trials ignored the prognostic benefit of surgery in more complex coronary artery disease. Nevertheless, the inappropriate generalization of the trial results from their highly select populations to most patients with multivessel disease has been ubiquitous in the literature and has, at least in part, justified the explosive growth in PCI in developed countries.’
Taggart DP. Lancet 2009; 373:1150-2
[2] Taggart DP. Thomas B. Ferguson Lecture. Coronary artery bypass grafting is still the best treatment for multivessel and left main disease, but patients need to know. Ann Thorac Surg 2006;82:1966-75. [3] Yusuf S, et al. Effect of coronary artery bypass graft surgery on survival: overview of 10-year results from randomised trials by the Coronary Artery Bypass Graft Surgery Trialists Collaboration. Lancet 1994 ;344:563-70.
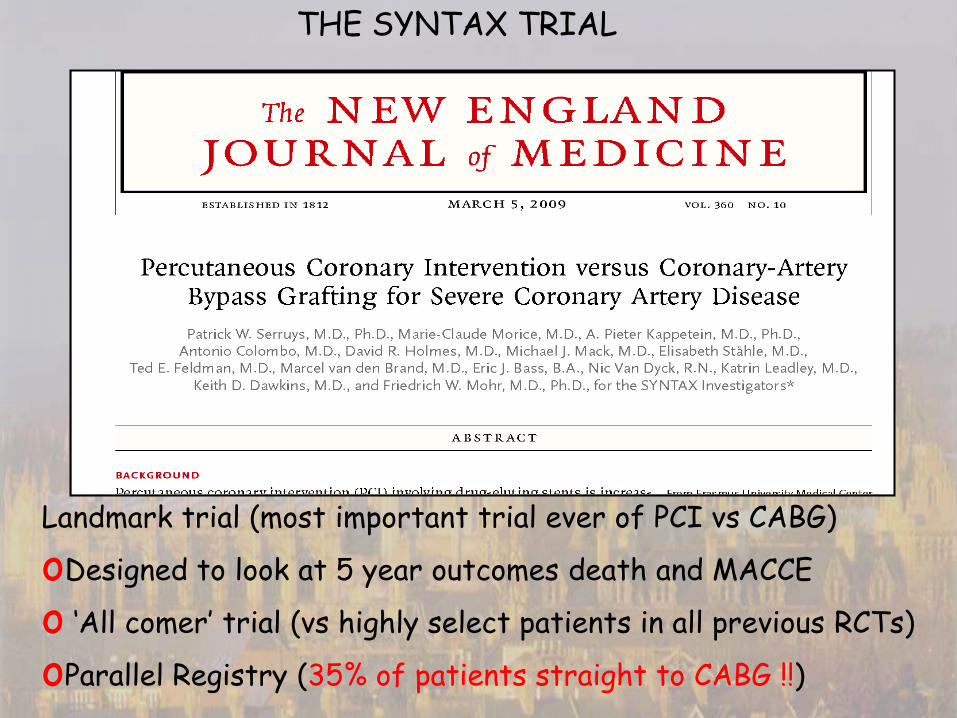
THE SYNTAX TRIAL
Landmark trial (most important trial ever of PCI vs CABG)
oDesigned to look at 5 year outcomes death and MACCE
o ‘All comer’ trial (vs highly select patients in all previous RCTs)
oParallel Registry (35% of patients straight to CABG !!)
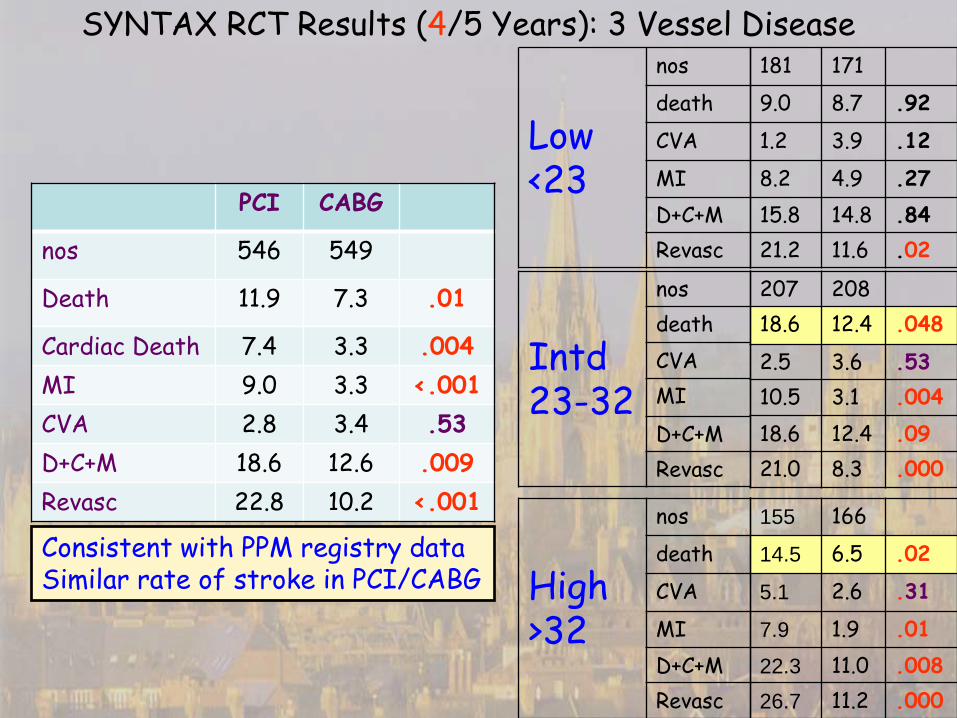
SYNTAX RCT Results (4/5 Years): 3 Vessel Disease 181 171
9.0 8.7 .92
1.2 3.9 .12
8.2 4.9 .27 15.8 14.8 .84 21.2 11.6 .02
207 208 18.6 12.4 .048
2.5 3.6 .53 10.5 3.1 .004 18.6 12.4 .09 21.0 8.3 .000
155 166
14.5 6.5 .02
5.1 2.6 .31
7.9 1.9 .01 22.3 11.0 .008 26.7 11.2 .000
Low <23
nos
death
CVA
MI D+C+M Revasc
Intd 23-32
nos death CVA MI
D+C+M Revasc
High >32
nos
death
CVA
MI D+C+M Revasc
PCI CABG
nos 546 549
Death 11.9 7.3 .01
Cardiac Death 7.4 3.3 .004 MI 9.0 3.3 <.001 CVA 2.8 3.4 .53 D+C+M 18.6 12.6 .009 Revasc 22.8 10.2 <.001
Consistent with PPM registry data Similar rate of stroke in PCI/CABG
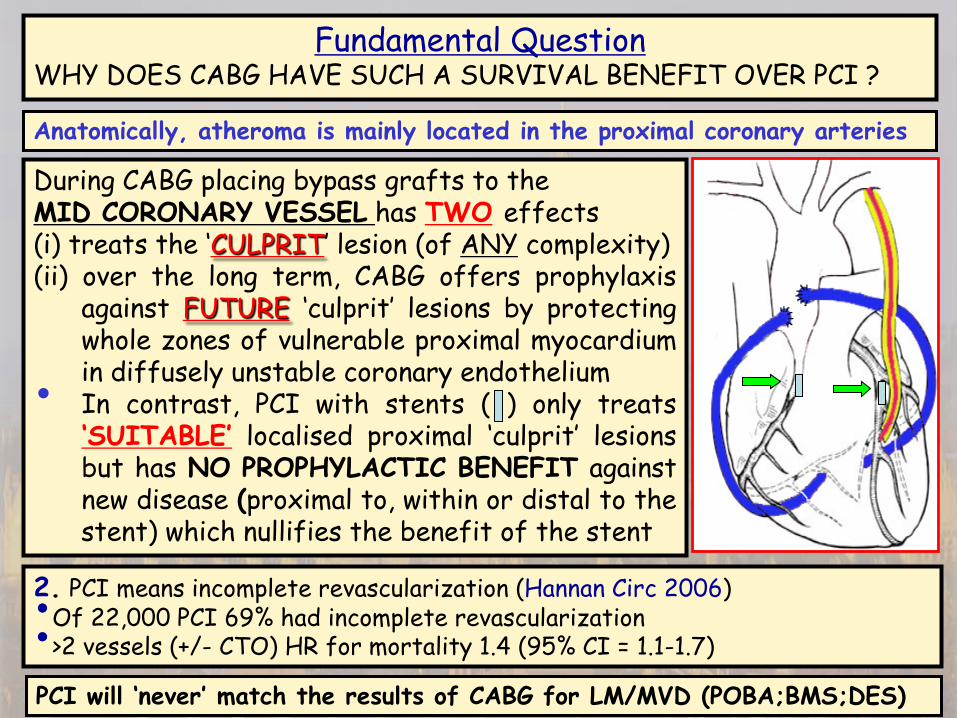
Fundamental Question WHY DOES CABG HAVE SUCH A SURVIVAL BENEFIT OVER PCI ?
During CABG placing bypass grafts to the MID CORONARY VESSEL has TWO effects (i) treats the ‘CULPRIT’ lesion (of ANY complexity) (ii) over the long term, CABG offers prophylaxis
against FUTURE ‘culprit’ lesions by protecting whole zones of vulnerable proximal myocardium in diffusely unstable coronary endothelium • In contrast, PCI with stents ( ) only treats ‘SUITABLE’ localised proximal ‘culprit’ lesions but has NO PROPHYLACTIC BENEFIT against new disease (proximal to, within or distal to the stent) which nullifies the benefit of the stent
2. PCI means incomplete revascularization (Hannan Circ 2006) •Of 22,000 PCI 69% had incomplete revascularization •>2 vessels (+/- CTO) HR for mortality 1.4 (95% CI = 1.1-1.7)
PCI will ‘never’ match the results of CABG for LM/MVD (POBA;BMS;DES)
Anatomically, atheroma is mainly located in the proximal coronary arteries

Left main (+/- 1,2,3 vCAD)
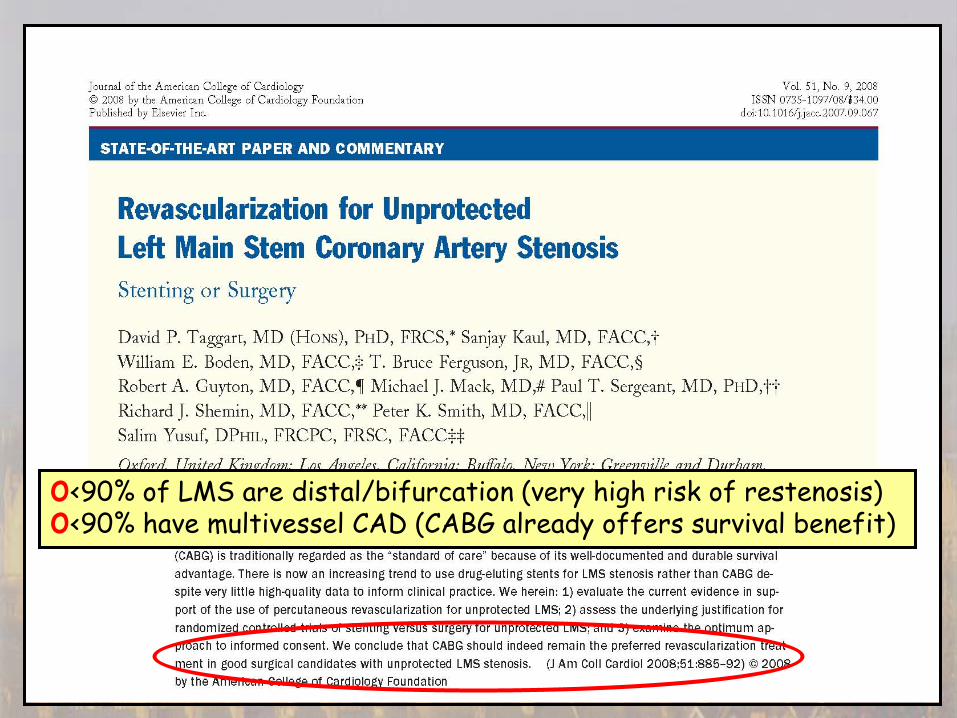
o<90% of LMS are distal/bifurcation (very high risk of restenosis) o<90% have multivessel CAD (CABG already offers survival benefit)
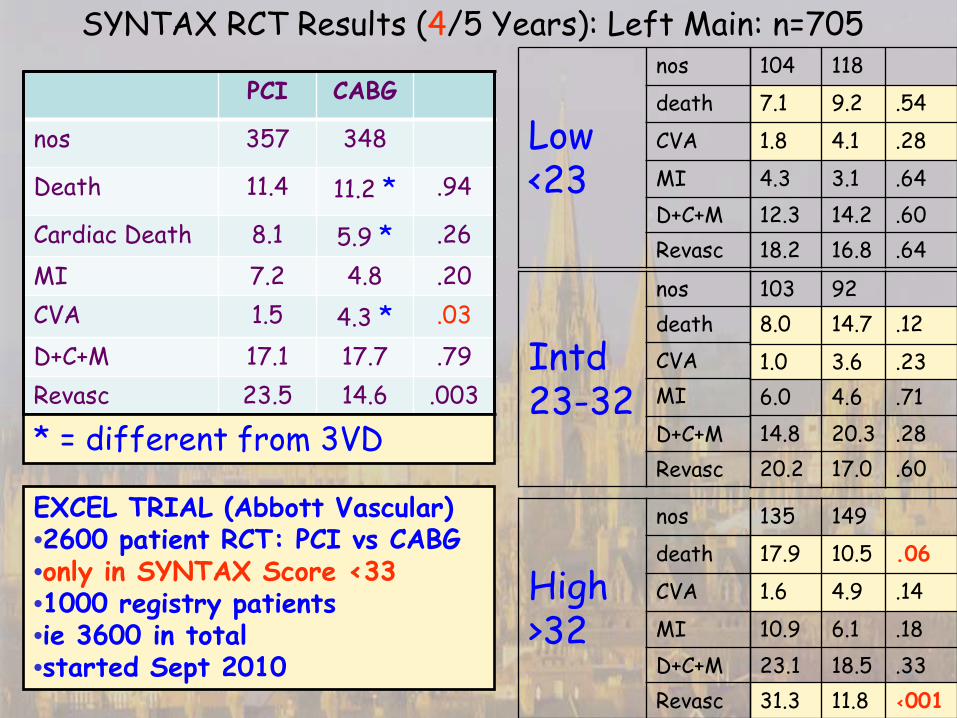
SYNTAX RCT Results (4/5 Years): Left Main: n=705 104 118
7.1 9.2 .54
1.8 4.1 .28
4.3 3.1 .64 12.3 14.2 .60 18.2 16.8 .64
103 92 8.0 14.7 .12
1.0 3.6 .23 6.0 4.6 .71 14.8 20.3 .28 20.2 17.0 .60
135 149
17.9 10.5 .06
1.6 4.9 .14
10.9 6.1 .18 23.1 18.5 .33 31.3 11.8 <001
Low <23
nos
death
CVA
MI D+C+M Revasc
Intd 23-32
nos death CVA MI
D+C+M Revasc
High >32
nos
death
CVA
MI D+C+M Revasc
PCI CABG
nos 357 348
Death 11.4 11.2 * .94
Cardiac Death 8.1 5.9 * .26 MI 7.2 4.8 .20 CVA 1.5 4.3 * .03 D+C+M 17.1 17.7 .79 Revasc 23.5 14.6 .003
EXCEL TRIAL (Abbott Vascular) •2600 patient RCT: PCI vs CABG •only in SYNTAX Score <33 •1000 registry patients •ie 3600 in total •started Sept 2010
* = different from 3VD
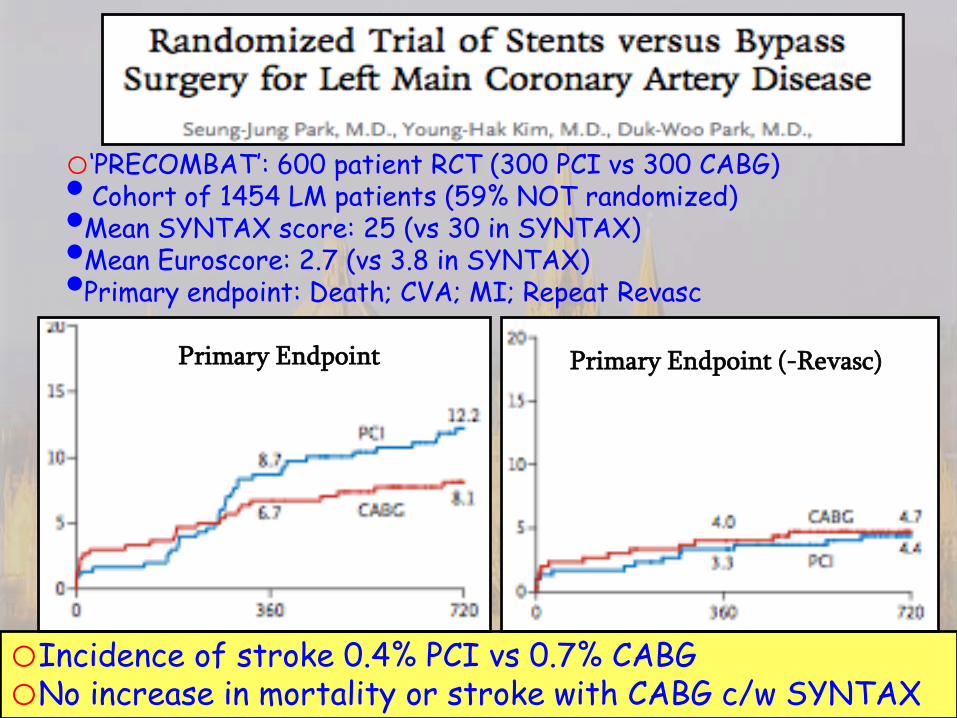
o‘PRECOMBAT’: 600 patient RCT (300 PCI vs 300 CABG) • Cohort of 1454 LM patients (59% NOT randomized) •Mean SYNTAX score: 25 (vs 30 in SYNTAX) •Mean Euroscore: 2.7 (vs 3.8 in SYNTAX) •Primary endpoint: Death; CVA; MI; Repeat Revasc
oIncidence of stroke 0.4% PCI vs 0.7% CABG oNo increase in mortality or stroke with CABG c/w SYNTAX
Primary Endpoint Primary Endpoint (-Revasc)
o25 members from 13 European countries •9 non interventional cardiologists, •8 interventional cardiologists, •8 cardiac surgeons
Reflects the ‘Heart Team’ !!!
oExtensively reviewed by external referees before publication
oJoint Cardiology (ESC) and Cardiac Surgery (EACTS)
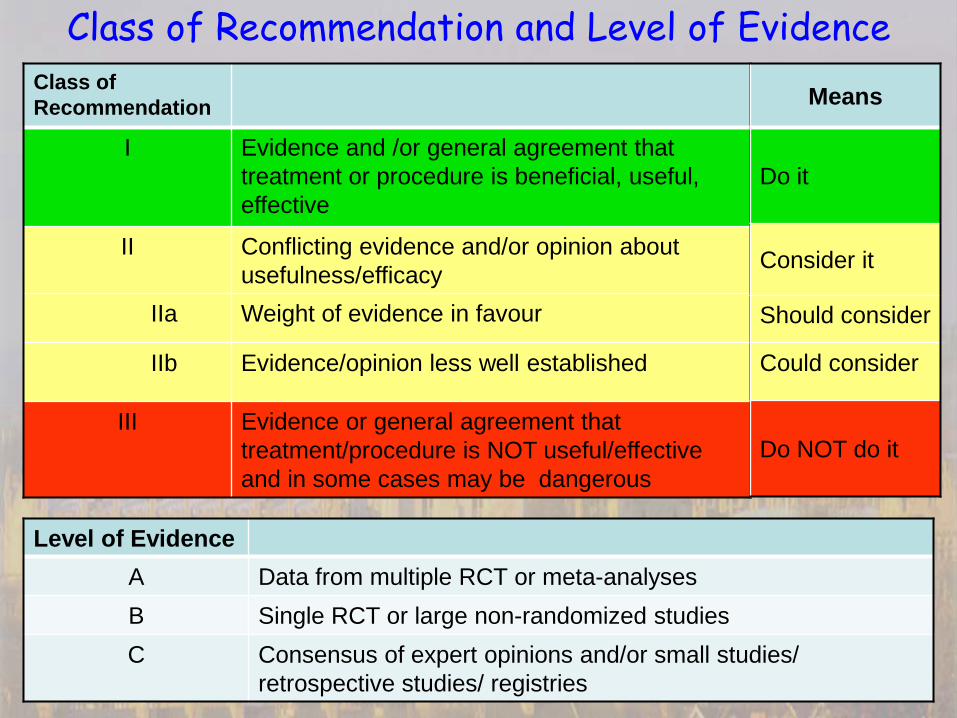
Class of Recommendation
I Evidence and /or general agreement that treatment or procedure is beneficial, useful, effective
II Conflicting evidence and/or opinion about usefulness/efficacy
IIa Weight of evidence in favour
IIb Evidence/opinion less well established
III Evidence or general agreement that treatment/procedure is NOT useful/effective and in some cases may be dangerous
Level of Evidence A Data from multiple RCT or meta-analyses B Single RCT or large non-randomized studies C Consensus of expert opinions and/or small studies/
retrospective studies/ registries
Class of Recommendation and Level of Evidence Means
Do it
Consider it
Should consider
Could consider
Do NOT do it
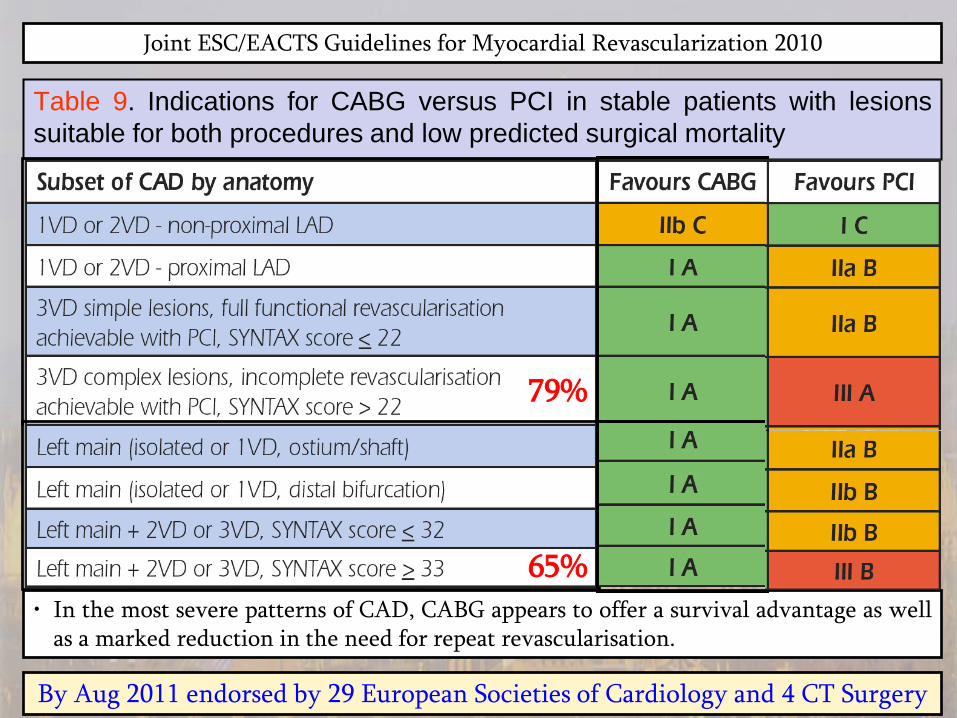
Joint ESC/EACTS Guidelines for Myocardial Revascularization 2010
Table 9. Indications for CABG versus PCI in stable patients with lesions suitable for both procedures and low predicted surgical mortality
• In the most severe patterns of CAD, CABG appears to offer a survival advantage as well as a marked reduction in the need for repeat revascularisation.
By Aug 2011 endorsed by 29 European Societies of Cardiology and 4 CT Surgery
79%
65%
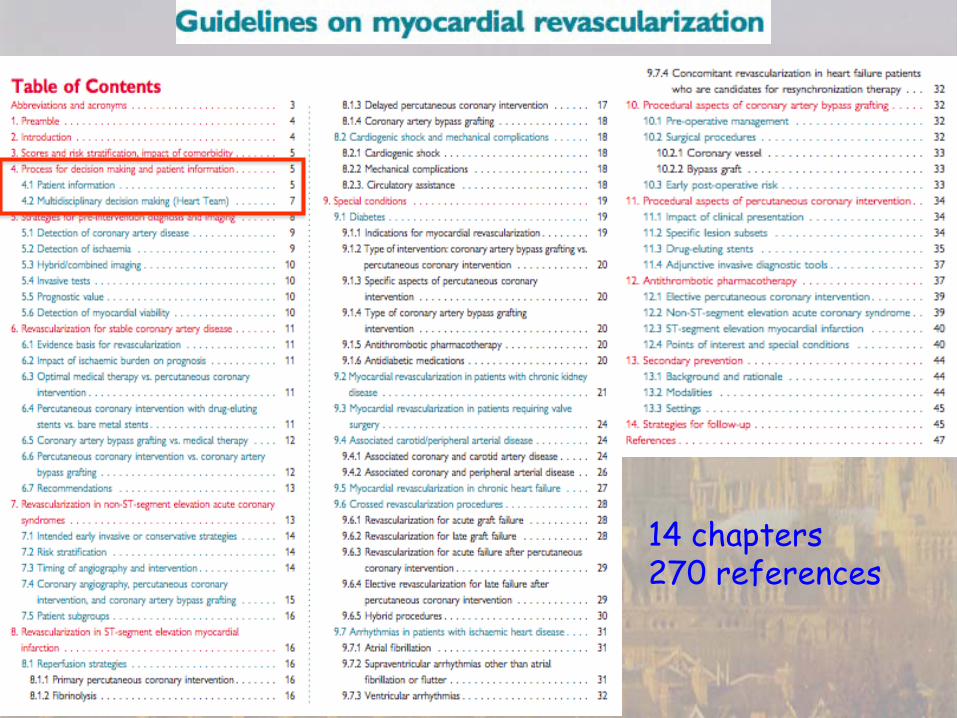
14 chapters 270 references
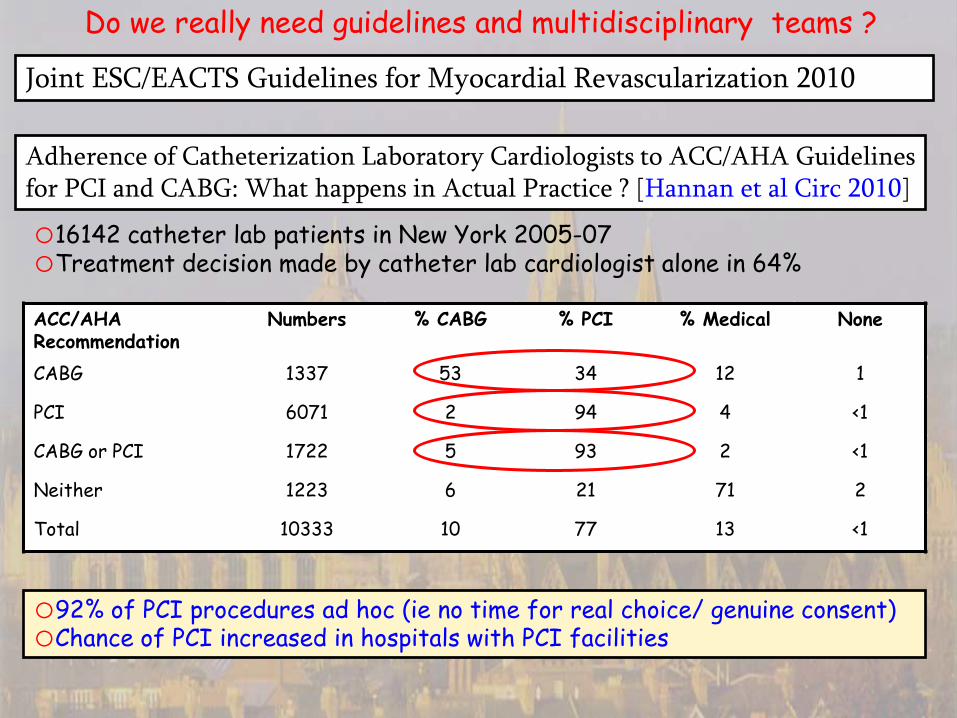
ACC/AHA Recommendation
Numbers % CABG % PCI % Medical None
CABG 1337 53 34 12 1
PCI 6071 2 94 4 <1
CABG or PCI 1722 5 93 2 <1
Neither 1223 6 21 71 2
Total 10333 10 77 13 <1
o16142 catheter lab patients in New York 2005-07 oTreatment decision made by catheter lab cardiologist alone in 64%
o92% of PCI procedures ad hoc (ie no time for real choice/ genuine consent) oChance of PCI increased in hospitals with PCI facilities
Do we really need guidelines and multidisciplinary teams ?
Adherence of Catheterization Laboratory Cardiologists to ACC/AHA Guidelines for PCI and CABG: What happens in Actual Practice ? [Hannan et al Circ 2010]
Joint ESC/EACTS Guidelines for Myocardial Revascularization 2010
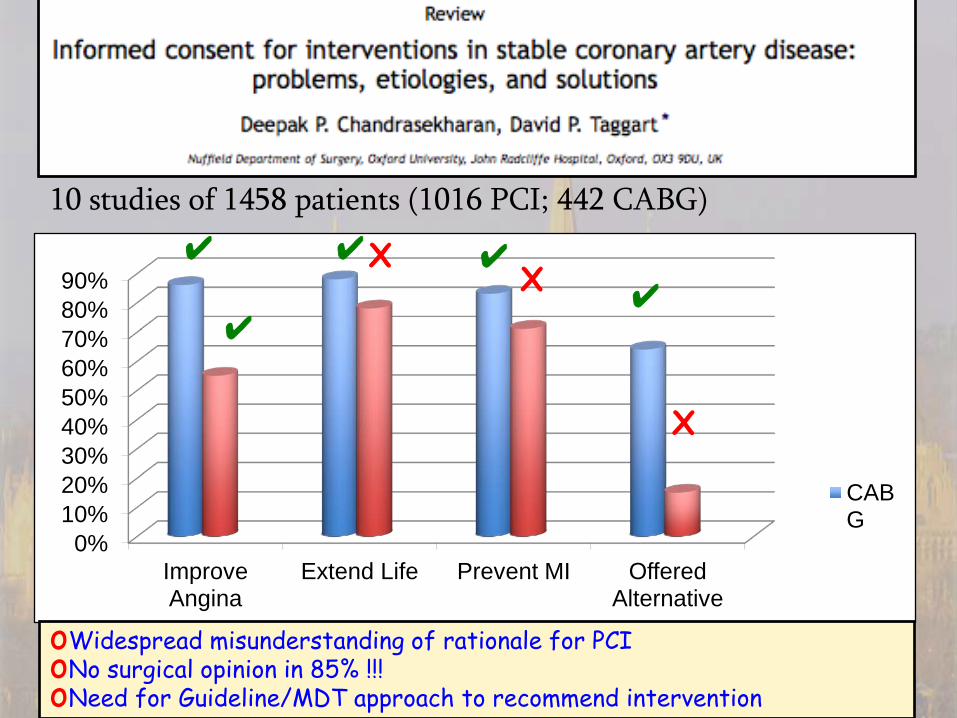
0% 10% 20% 30% 40% 50% 60% 70% 80% 90%
Improve Angina
Extend Life Prevent MI Offered Alternative
CABG
✔ ✔
✔ ✔
X X
X
✔
oWidespread misunderstanding of rationale for PCI oNo surgical opinion in 85% !!! oNeed for Guideline/MDT approach to recommend intervention
10 studies of 1458 patients (1016 PCI; 442 CABG)
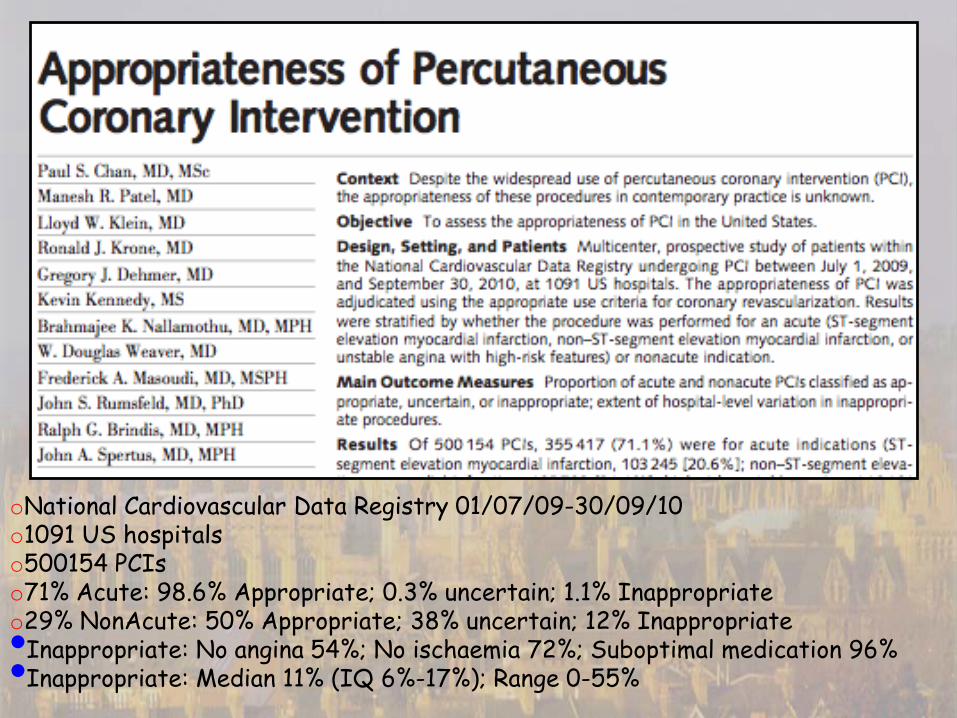
oNational Cardiovascular Data Registry 01/07/09-30/09/10 o1091 US hospitals o500154 PCIs o71% Acute: 98.6% Appropriate; 0.3% uncertain; 1.1% Inappropriate o29% NonAcute: 50% Appropriate; 38% uncertain; 12% Inappropriate •Inappropriate: No angina 54%; No ischaemia 72%; Suboptimal medication 96% •Inappropriate: Median 11% (IQ 6%-17%); Range 0-55%
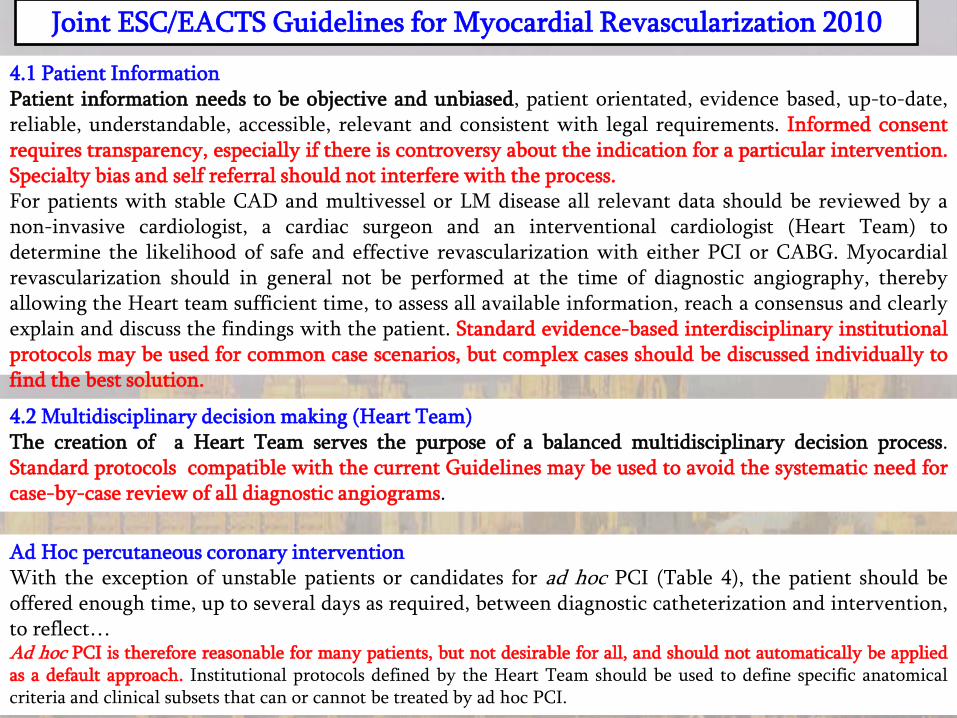
4.1 Patient Information Patient information needs to be objective and unbiased, patient orientated, evidence based, up-to-date, reliable, understandable, accessible, relevant and consistent with legal requirements. Informed consent requires transparency, especially if there is controversy about the indication for a particular intervention. Specialty bias and self referral should not interfere with the process. For patients with stable CAD and multivessel or LM disease all relevant data should be reviewed by a non-invasive cardiologist, a cardiac surgeon and an interventional cardiologist (Heart Team) to determine the likelihood of safe and effective revascularization with either PCI or CABG. Myocardial revascularization should in general not be performed at the time of diagnostic angiography, thereby allowing the Heart team sufficient time, to assess all available information, reach a consensus and clearly explain and discuss the findings with the patient. Standard evidence-based interdisciplinary institutional protocols may be used for common case scenarios, but complex cases should be discussed individually to find the best solution.
4.2 Multidisciplinary decision making (Heart Team) The creation of a Heart Team serves the purpose of a balanced multidisciplinary decision process. Standard protocols compatible with the current Guidelines may be used to avoid the systematic need for case-by-case review of all diagnostic angiograms.
Ad Hoc percutaneous coronary intervention With the exception of unstable patients or candidates for ad hoc PCI (Table 4), the patient should be offered enough time, up to several days as required, between diagnostic catheterization and intervention, to reflect… Ad hoc PCI is therefore reasonable for many patients, but not desirable for all, and should not automatically be applied as a default approach. Institutional protocols defined by the Heart Team should be used to define specific anatomical criteria and clinical subsets that can or cannot be treated by ad hoc PCI.
Joint ESC/EACTS Guidelines for Myocardial Revascularization 2010
o79% of ALL 3VD (SYNTAX>22) and 65% ALL LM (SYNTAX >32)
•CABG has superior survival, freedom from MI and repeat revasc at 3yrs
•Consistent with registry evidence in the literature
•CABG has same risk of CVA as PCI for 3VD but 4.0% vs 1.2% for LM
•PCI may be best treatment for ostial/mid shaft LM (EXCEL trial)
•PCI has an important role in patients unfit for or who refuse CABG
Summary and Conclusions: CABG vs PCI in 2012
o Strong evidence that most PCI patients misunderstand its rationale
•MDTs/Heart Team must ensure patients receive appropriate information
•If intervention follows guideline recommendations no need for MDT
•‘Ad hoc’ PCI denies real patient choice and genuine informed consent o Results of contemporary CABG are excellent but could be even better
•More use of arterial grafts (especially 2nd IMA)
•More off pump CABG in higher risk patients
•Confirmation of graft patency in operating room