cardiac diseases - trnotebook.yolasite.comtrnotebook.yolasite.com/resources/convulsive... · web...
TRANSCRIPT

1
Convulsive Disorders,Cardiac Diseases, and Stroke

2
CONVULSIVE DISORDER OVERVIEW
DEFINITIONS
What is a convulsive disorder?
The term convulsion, or seizure, refers to an involuntary spasm or contraction of muscles resulting from chemical imbalances in the body. The causes of these chemical imbalances may come from a variety of sources, such as insufficient amounts of sugar or calcium in the blood, toxic poisoning, and disease or injury to the brain or central nervous system. The diagnostic category of Epilepsy represents the largest subgroup of convulsive disorders, however it should be noted that not all clients who have convulsions are epileptic.
What is epilepsy?
Epilepsy is a neurological condition that from time to time produces brief disturbances in the normal electrical functions of the brain. Normal brain function is made possible by millions of tiny electrical charges passing between nerve cells in the brain and to all parts of the body. When someone has epilepsy, this normal pattern may be interrupted by intermittent bursts of electrical energy that are much more intense than usual. They may affect a person’s consciousness, bodily movements or sensations for a short time. These physical changes are called epileptic seizures. This is why sometimes epilepsy is called a seizure disorder. The unusual bursts of energy may occur in just one area of the brain (partial seizures), or may affect nerve cells throughout the brain (generalized seizures). Normal brain function cannot return until the electrical bursts subside. Conditions in the brain that produce these episodes may have been present since birth, or they may develop later in life due to injury, infections, structural abnormalities in the brain, exposure to toxic agents, or for unknown reasons or because of an underlying problem that cannot be corrected, the condition is known as epilepsy. Epilepsy affects people of all ages, all nations, and all races. Epilepsy can also occur in animals, including dogs, cats, rabbits, and mice.
What is seizure?
A seizure is a sudden, uncontrollable event that occurs when the brain’s electrical system malfunctions. Instead of discharging energy in a controlled manner, the brain’s cells keep firing, often randomly. Some seizures cause a person to fall unconscious and shake. When it is over, the person may feel sleepy and will not remember what happened. However, many seizures involve only portions of the brain and result in a loss of attention, distorted communication, staring spells that look like daydreaming, or random, jerking movements in one part of the body. Most seizures last only a minute or two. A person with epilepsy may have seizures only once in a while or every day. Older terms for seizures exist: fits, spells, or falling out, may still be used by the general public in some communities. In the medical community, the Latin word "ictus" may be used to

3
describe a seizure. Related terms are used to define events associated with a seizure. Using this lexicon, "ictus" refers to the seizure itself; "ictal" defines the period in which the seizure occurs; "pre-ictal" and "post-ictal" describe periods before and after the seizure; while inter-ictal refers to the period between seizures. Thus, when an EEG reading, for example, is described as "inter-ictal," it means that it was recorded between seizures.
Differences between epilepsy and seizures
Seizures are a symptom of epilepsy. A person has epilepsy when he or she has seizures more than once because of a brain disorder. Sometimes people use the term seizure to indicate epilepsy.
ONE SEIZURE --------------------- JUST ONE SEIZUREMULTIPLE SEIZURES------------------------ EPILEPSY
CAUSATION
About on half of all seizures have no known cause. The other half is linked to disease or injury of the brain. During development, and the first few years childhood, the brain undergoes a lot of growth. During this growth, the brain is at danger of certain diseases due to infections, poor nutrition, and insufficient oxygen. Some of these diseases are associated with epilepsy. The neurons of the brains develop into complex webs of wires.
o Defects of wires during brain development, can lead to epilepsy.
o After a head injury after an accident or a stroke, the brain repairs itself by making new wires. If the wiring is abnormal, then it can cause seizures.
o Disease of the brain such as hydrocephalus and meningitis can cause epilepsy.
o Poisoning of the brain, such as lead and carbon monoxide poisoning, can lead to seizures.
o Exposure to street drugs and overdoses to anti-depressants can also lead to seizures.
o Some types of epilepsy tend to run in families, suggesting hereditary causes.
o Older people sometimes develop diseases of the brain. These types of diseases can lead to epilepsy:
o Brain tumors of any kind may cause seizures. If an operation is done to remove the tumor, the seizures may stop.

4
o Stroke is the most frequent cause of seizures that begin in later life. As people age, arteries may become narrowed or clogged, depriving parts of the brain of blood and oxygen. The resulting damage may produce seizures. Bleeding in the brain, which is another form of stroke, may also leave a person with seizures afterwards.
o Disease. Alzheimer's disease, or other brain diseases that change the internal structure of the brain, may cause seizures. Complications of kidney disease, liver disease, alcoholism and even diabetes may make people more likely to have seizures in later life.
o Heart attacks may temporarily cut off oxygen to the brain, with a similar result.o infections, and bleeding.
SEIZURE MECHANISMS AND THRESHOLD
Seizure is a massive disruption of electrical communication between neurons in the brain, leading to the temporary release of excessive energy in a synchronized form. Neurons communicate with each other by firing electrical impulses. These impulses travel from the neuron along the axon, and then stimulate the release of neurotransmitters which flow across the synaptic cleft (the gap between the cells) to the dendrites of the receiving cell.
If more excitatory than inhibitory transmitters are released, the cell will fire; if more inhibitory neurotransmitters are released, the cell will not fire. Since large numbers of cells are involved in even simple actions, the on/off action serves to control physical and mental functioning.
However, if there is a consistently higher level of the excitory neurotransmitters, or too few inhibitory ones, the likelihood of a seizure—an uncontrolled, continuing firing of neurons in the brain—is increased. Some of the newer medications relate directly to this process and are designed to increase the level of inhibitory neurotransmitters, especially gamma-aminobutyric acid (GABA), or to decrease the amount of the excitatory ones, such as glutamate.
A sudden burst of neuronal firing may not be sufficient to cause an obvious seizure (although it might show up as a sudden spike on the EEG); however, if the discharge of electrical energy has sufficient power and affects enough neurons, it will produce
5
symptoms characteristic of the area in which the discharge took place. The result could be a sudden muscle jerk, an abrupt fall, a distorted vision. If the disturbance flashes across the whole brain at once, it could produce a convulsive seizure, temporarily disrupting many of the functions of the brain.
SEIZURE THRESHOLD
This concept holds that everyone has a certain balance (probably genetically determined) between excitatory and inhibitory forces in the brain. The relative proportions of each determine whether a person has a low threshold for seizures (because of the higher excitatory balance) or a high threshold (because of greater inhibition). According to this view, a low seizure threshold makes it easier for epilepsy to develop, and easier for someone to experience a single seizure.
DIAGNOSIS
The diagnosis of epilepsy requires the presence of recurrent, unprovoked seizures; accordingly, it is usually made based on the medical history. EEG, brain MRI, SPECT, PET, and magnetoencephalography may be useful to discover an etiology for the epilepsy, discover the affected brain region, or classify the epileptic syndrome, but these studies are not useful in making the initial diagnosis.
Long-term video-EEG monitoring for epilepsy is the gold standard for diagnosis, but it is not routinely employed owing to its high cost and inconvenience. It is, however, sometimes used to distinguish psychogenic non-epileptic seizures from epilepsy.
The epileptic syndromes are classified according to seizure types, symptoms, clinical findings and the causes of epilepsy. The seizures are classified according to symptoms and findings during the attack and this depends on which brain region is involved.
Brain region affected SymptomFrontal lobe Motor phenomena, eg tonic-clonic
seizures or jerksParietal lobe Sensory phenomenaTemporal lobe Changes in mood and smell,
gastrointestinal symptomsLimbic system Changes in consciousness
CLASSIFICATIONS FOR SEIZURES
There are many different types of seizures. People may experience just one type or more than one. The kind of seizure a person has depends on

6
which part and how much of the brain is affected by the electrical disturbance that produces seizures. Experts divide seizures into generalized seizures (absence, atonic, tonic-clonic, myoclonic) and partial (simple and complex) seizures.
GENERALIZED SEIZURES
Generalized seizures are caused by abnormal electrical activity that occurs over the entire brain simultaneously. This group of seizures affect the level of awareness and muscle movement of all extremities. Following are the main types of generalized seizures.
Absence Seizures: This type of seizure is also known as “petit mal”. They are described as staring spells. At times they are difficult to distinguish from normal daydreaming spells. These seizures typically start in childhood and are often outgrown by adolescence, although adults can occasionally also have absence seizures. They can happen dozens of times a day but are very brief, usually lasting just a few seconds, so they are not always noticed. The child may get a dazed look on their face, have some eye blinking or head bobbing and not respond to any type of stimulus. After the seizure is over, the child usually continues his previous activity as if nothing happened. An EEG is very helpful with diagnosing this type of seizure. Patients usually respond very well to medication.
Myoclonic Seizures: These are characterized by sudden brief jerks of a single muscle or muscle group. You may see a sudden jerk of the hand or arm that will cause them to drop or knock things over. It may appear as if they have been startled. You may see the head or body suddenly bend forward or backward. At times the jerk can be so strong that the child can be thrown to the ground. These seizures are not the same thing as the periodic muscle spasms one often experiences when falling asleep.
Atonic Seizures: These are also very sudden brief seizures, but they involve loss of all muscle tone. The child will suddenly go limp and fall to the ground. There is significant risk of head injury during the fall. So, many children with this seizure type wear helmets for protection.
Tonic Seizures: These seizures involve stiffening of parts of the body or the entire body, sometimes causing the child to fall down. Unlike tonic-clonic seizures, there is no progression to a clonic phase (see below).
Tonic-Clonic Seizures: Also known as “grand mal”, these are very intense and can often be very frightening to witness. They generally start with a tonic phase with stiffening of the entire body. The eyes may roll back in the head, the back arches, and arms and legs stiffen. The muscles in the chest can also stiffen so it may appear that the person is not breathing and you may see blue around the lips. There may be an increase in saliva or “foaming at the mouth”. The clonic part is described as rhythmic jerking of the entire body. Once the seizure is over, they may feel worn out and may even sleep for a period of time. They may also experience some confusion.

7
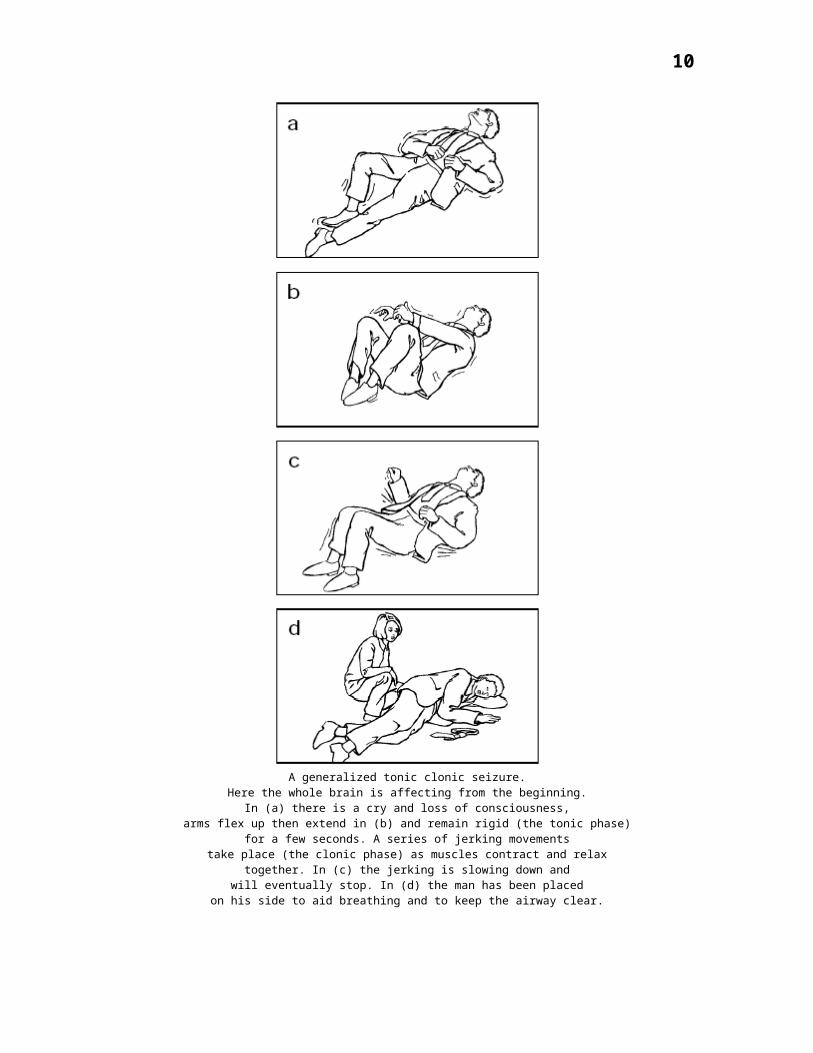
A generalized tonic clonic seizure.Here the whole brain is affecting from the beginning.
In (a) there is a cry and loss of consciousness,arms flex up then extend in (b) and remain rigid (the tonic phase)
for a few seconds. A series of jerking movementstake place (the clonic phase) as muscles contract and relax
together. In (c) the jerking is slowing down andwill eventually stop. In (d) the man has been placed
on his side to aid breathing and to keep the airway clear.

8
Partial Seizures
Partial seizures, also called focal, are those seizures that begin in one part of the brain instead of all over. Depending on which lobe of the brain the seizure comes from will determine the way the seizure looks. Partial seizures can be classified based on either the symptoms of the seizure or the part of the brain where they start.
Based on the symptoms of the seizures, partial seizures can be divided into simple partial seizures and complex partial seizures.
Simple partial seizures: Simple partial seizures are noted for staying in just one area of the brain and not interfering with the level of consciousness. Depending on the area of the brain affected, these seizures could be expressed as shaking of a small part of the body, an unusual tingling or numbness of a localized body part, or even an unusual smell, visual hallucination, or ill-defined feeling. Simple partial seizures are often also called “auras”. Regardless of the specific symptom, in all simple partial seizures, the person remains completely aware and alert during the seizure.
A simple partial seizure with motor symptoms.Here the neuronal discharge begins in the motor stripin the right hemisphere of the brain, affecting first onemuscle then another on the left side of the body as it spreads.In (a) first the fingers then the hand and arm are jerking.In (b) it has spread to the upper shoulder.In (c) the woman's head is drawn towards her shoulder.In (d) the leg is drawn up. The woman remains conscious butunable to prevent her muscles' response to the excessive stimulationthey are receiving from her brain.
Complex partial seizures: A complex partial seizure happens when the abnormal electrical activity involves parts of the brain that affect level of consciousness. Thus, the critical feature of the complex partial seizure is that the person has altered consciousness,

9
so that he may be confused or staring unresponsively. There may also be subtle, repetitive and stereotypical movements of the face or extremities (automatisms). Although complex partial seizures can look similar to absence seizures, they usually last longer, typically 1-2 minutes. In addition, unlike absence seizures, complex partial seizures often are preceded by an aura and are followed by a state of sleepiness. Sometimes a complex partial seizure can start in just one area and spread throughout the entire brain, resulting in a generalized tonic-clonic seizure. This type is known as complex partial with secondary generalization.
Following are descriptions of the different types of seizures and how they typically appear depending on where in the brain they take place. However, sometimes only detailed testing by a neurologist can determine with certainty where seizures are originating.
Frontal lobe: These seizures are usually very short and often occur during sleep. They may be described as twitching or a funny feeling in the face, a finger or leg. The person may be aware all of this is happening (simple partial seizure). Sometimes the head will turn to one side, and the arm on that same side will stiffen. In other cases, very bizarre or complicated movements of the entire body can occur. The seizure may spread causing awareness to be affected and jerking of extremities may happen.
Temporal Lobe: This type usually involves complex partial seizures with staring and repetitive movements that seem to happen without purpose. These movements are called automatisms. There may also be a complaint of a funny feeling around the mouth, be unable to speak, and have increased saliva and twitching of the mouth. You may also see twitching, jerking, or stiffening on one side of the body. At the beginning of the seizure, they may experience a funny smell, a sensation of fear or a funny feeling in the stomach or chest.
Parietal Lobe: There may be a feeling of electricity or tingling sensation that may start in a certain area, or may spread. They may complain that one part of the body feels like it is moving. Sometimes there is a feeling of sinking, choking or nausea, or pain.
Occipital Lobe: These classically begin with visual problems, such as seeing flashes of light or hallucinations. Often the child will complain that they can’t see and have rapid eye blinking. The loss of vision is temporary and will return after the seizure is over.
ASSOCIATED SYMPTOMS
Generalized seizures: All areas of the brain (the cortex) are involved in a generalized seizure. Sometimes these are referred to as grand mal seizures.
o To the observer, the person experiencing such a seizure may cry out or make some sound, stiffen for some seconds, then have rhythmic movements of the arms and legs. Often the rhythmic movements slow before stopping.
10
o Eyes are generally open.
o The person may not appear to be breathing. The person is often breathing deeply after an episode.
o The return to consciousness is gradual and should occur within a few moments.
o Loss of urine is common.
o Often people will be confused briefly after a generalized seizure.
Partial or focal seizures: Only part of the brain is involved, so only part of the body is affected. Depending on the part of the brain having abnormal electrical activity, symptoms may vary.
o If the part of the brain controlling movement of the hand is involved, for example, then perhaps only the hand may show rhythmic movements or jerking.
o If other areas of the brain are involved, symptoms might include strange sensations or small repetitive movements such as picking at clothes or lip smacking.
o Sometimes the person with a partial seizure appears dazed or confused. This may represent a partial complex seizure. The term complex is used by doctors to describe a person who is between being fully alert and unconscious.
o Déjà vu (unfamiliar things seem familiar)
Absence or petit mal seizures: These are most common in childhood.
o Impairment of consciousness is present with the person often staring blankly.
o Repetitive blinking or other small movements may be present.
o Typically, these seizures are brief, lasting only seconds. Some people may have many of these in a day.
o Other seizure types exist particularly in very small children.

11
SYNDROMES
Benign Rolandic Epilepsy
Benign Rolandic epilepsy (also known as benign partial epilepsy of childhood) accounts for more than one-third of all cases of epilepsy that begin in middle childhood, accounting for 16 percent of those beginning before age 15. There is a family history in 18 percent of cases and the condition is probably genetically determined.
Rolandic epilepsy is the most common type of benign partial epilepsy. Seizures start as simple partial, usually beginning in the face. There may be drooling and temporary inability to speak, although consciousness is preserved. The seizures then generalize to tonic-clonic convulsions.
Most of the seizures are nocturnal and occur during sleep. Neurological and other functioning is usually normal, while the EEG shows a dramatic focal spike most often in the centrotemporal regions of the brain. Most children are seizure free five years after onset; by age 14, 95 percent will have undergone permanent remission.
Childhood Absence Epilepsy
Childhood absence epilepsy (also called petit mal epilepsy, pyknolepsy) accounts for 2 to 4 percent of all cases of epilepsy in children. Seizures are non-convulsive staring spells associated with a distinct 3 per second spike and wave EEG pattern. The seizures tend to occur in clusters (hence pyknolepsy -- derived from the Greek word for "cluster").
Children with this syndrome are otherwise normal; 40 percent outgrow the seizures, and as a group their I.Q. scores are 10 points above average. The syndrome is inherited (probably autosomal dominant trait with age-dependent expression).
Despite its overall benign nature, approximately half of the children with absence epilepsy can expect to have a generalized tonic clonic seizure. The risk is higher if the EEG background readings are abnormal, or if the child has neurological deficits. The risk is reduced if seizures are quickly controlled with medication.
Remission of childhood absence epilepsy is most likely when the child is young at onset, the seizures are easily controlled with medication and there are no other neurological problems.

12
Febrile Seizures
Febrile seizures have the characteristics of an epileptic syndrome in that they involve generalized seizures, begin at a specific time, and are time limited in their effect. However, not all authorities consider them to be epilepsy.
During their lifetimes, 10 percent of people will have at least one convulsion, and febrile (fever-generated) seizures represent by far the most common type of convulsive episode. Three to 4 percent of all children have at least one febrile seizure. Although febrile convulsions are generally benign, they are extremely frightening for the child’s family. The vast majority of children who have one or more febrile convulsions are otherwise completely normal.
Febrile convulsions occur in children aged 3 months to 6 years whose temperatures are elevated from any cause other than a central nervous system (CNS) infection. The peak age is 18 months, with the majority of episodes occurring between 6 months and 3 years. Thirty to 40 percent of children with a single febrile convulsion experience a recurrence; 3 percent will develop epilepsy by age 7.
Elevated temperature is the hallmark of febrile convulsions; 75 percent of the affected children had rectal temperatures above 39 degrees Celsius (102.2 Fahrenheit), although seizures may occur at lower levels. Brain damage is seldom a consequence of febrile seizures, and occurs only when the convulsion is prolonged.
In most cases physicians do not prescribe long-term use of anticonvulsants to prevent febrile seizures because of the potential side effects and questionable effectiveness for febrile seizures. However, a doctor sometimes may decide that medicine given only while the child has a fever may be the best alternative. Physicians may recommend that children especially prone to febrile seizures be treated with the drug diazepam, given orally or rectally, when they have a fever.
Frontal Lobe Epilepsy
Partial seizures beginning in the frontal lobe may produce weakness or the inability to use certain muscles, including the muscles that make it possible to talk. Sudden thrashing movements during sleep are also characteristic of frontal lobe epilepsy; as is posturing with the head jerking to one side, and the arm rising with it into a brief, frozen state. Sometimes a generalized convulsion follows the slow march of these movements.
Complex partial seizures in the frontal lobe have some distinct features in contrast to those in the temporal lobes. They usually last less than a minute, are less likely to be followed by confusion or fatigue, and often occur in a series or cluster.
Frontal lobe epilepsy has significant social effects because the seizures it generates are more likely to involve brief episodes of screaming, bicycling movements, or even
13
movements suggestive of sexual activity. Treatment includes medication and, in some cases, surgery.
Infantile Spasms
West syndrome and infantile spasms are two conditions which occur together so frequently that the two terms are used interchangeably. West syndrome involves developmental arrest and possible loss of developmental milestones and has a distinctive EEG pattern called hypsarrhythmia.
Infantile spasms are clusters of brief seizures involving various combinations of flexion and extension of the trunk and limbs, most common in the early morning or upon wakening from naps. In the most common form, the body bends as the outstretched arms jerk forward -- so called "salaam seizures. The condition is often mistaken for colic, at least initially, because the babies double up during the spasm and cry afterwards.
Eighty-five percent of children who develop infantile spasms do so before the age of 12 months; most stop having spasms by age 5. During this period, 40 percent will have other types of seizures.
The most common causes are tuberous sclerosis and perinatal asphyxia (lack of oxygen). In 40 percent of cases, there is no known cause and these children have the best prognosis; causes that are symptomatic have the worst. As many as 20 percent die before age 5; 75 percent are mentally retarded; and more than 50 percent have persistent epilepsy, half of whom develop Lennox-Gastaut syndrome.
Juvenile Myoclonic Epilepsy
Juvenile myoclonic epilepsy (also called Janz's syndrome, impulsive petit mal, myoclonic epilepsy of adolescence and jerk epilepsy) was first described in 1956 by Dr. Dieter Janz, who called it impulsive petit mal because of the sudden jerking (myoclonic) seizures that are a prominent part of the syndrome. The syndrome is characterized by myoclonic seizures (sudden jerks of arms and legs), especially on awakening.
Juvenile myoclonic epilepsy generally appears at puberty, but may have existed prior to that time and it is usually not outgrown; it is also associated with generalized tonic-clonic seizures. Seizures may be precipitated by sleep deprivation; early awakening; alcohol and drug use; stress; strong emotion, photic stimulation, and menstruation.
Landau-Kleffner Syndrome
Landau-Kleffner syndrome, a rare disorder, causes children to develop the inability to speak. They have trouble understanding speech and may seem not to hear or

14
understand what is said to them. Many children will also have seizures; these seizures vary in type. Speech in children with the syndrome slowly declines over time. There are epilepsy-related abnormalities on the EEG, even though some of the children do not have seizures.
The syndrome typically begins in children between 3 to 7 years old. Understanding spoken language is usually affected, but the children may also lose the ability to speak as well. Seizures often occur while the child is asleep and may be quite infrequent. Simple partial and tonic-clonic seizures may occur. Treatment with standard anti-epileptic drugs is not very effective; treatment with steroids has been tried with some success. Multiple subpial transection, a form of surgery designed to spare the speech areas, has also been tried.
Language for many of these children will improve slowly over time, but may not return to a normal level for age. EEGs may continue to be abnormal, even when the speech has improved.
Lennox-Gastaut Syndrome
Lennox-Gastaut syndrome (also known as myoclonic-astatic epilepsy) is a combination of seizures usually including atypical absense seizures (starting with automatic behavior without conscious control); tonic seizures (stiffening) atonic or astatic seizures (drop attacks); mental retardation; a distinct slow spike-and-wave EEG; and onset between 1 and 5 years of age.
Some children are developmentally normal when the syndrome begins, but then lose skills, sometimes dramatically, in association with uncontrolled seizures. By age 6 most children with Lennox-Gastaut have some degree of mental retardation.
Children with Lennox-Gastaut syndrome typically have more than one type of seizure. The atonic-astatic (drop attack) seizures are most troubling because of the injuries caused by repeated falls. Many children wear protective helmets. The tonic (stiffening) seizures are most common during sleep, including naptime, whereas generalized tonic-clonic seizures (convulsions) occur most often on awakening.
Some of these children are prone to develop non-convulsive status epilepticus (a continuous seizure state that is associated with a change in the child's level of awareness. This requires medical intervention to bring it to an end).
As children with Lennox-Gastaut syndrome grow older, the types of seizures change. In most cases, the drop seizures abate. They are replaced by partial, complex partial, and secondarily generalized convulsions. Among teenagers with Lennox-Gastaut, complex partial seizures are the most common form.
15
This seizure syndrome is difficult to treat and often does not respond to the usual seizure medications. Other treatment choices may include the ketogenic diet, vagus nerve stimulation therapy or occasionally corpus callosotomy surgery.
Progressive Myoclonic Epilepsy
A rare form of epilepsy with myoclonic (jerking) and tonic-clonic (grand mal) seizures. Children with this condition may have trouble with maintaining balance and experience rigid muscles. There is also a loss of mental ability. A gene for this disorder has recently been discovered.
Rasmussen's Syndrome
Rasmussen's syndrome, also known as Rasmussen's encephalitis, begins in childhood and produces a slow deterioration of one whole side (hemisphere) of the brain with loss of function on the opposite side of the body. An autoimmune response to a viral infection has been suggested as a possible cause. Various types of treatment have been tried, including surgical removal of the affected side of the brain. In children, the remaining hemisphere may compensate for functions lost, but weakness on the affected side will remain.
The condition typically starts with seizures, with weakness appearing later in the course of the disorder. Simple partial seizures affecting movement are the most common form.
Reflex Epilepsy
Reflex epilepsy is the name given to seizures which are triggered by individual sensitivity to sensory stimulation in the environment.
The most common form is photosensitive epilepsy -- that is, seizures caused by exposure to intense or fluctuating levels of light. Some people have seizures triggered by flashing lights or rapidly alternating light and dark patterns. The condition usually begins in childhood and may be outgrown by adulthood.
A flickering fluorescent light, the flicker of sunlight while driving past standing trees, certain video games, or flashing strobe lights can trigger seizures in photosensitive people. The reflex response may be absence (staring) seizures, myoclonic (jerking) seizures, or generalized convulsions. Wearing polarized sunglasses with blue lenses has been cited as good protection against photosensitive reflex seizures.
While flashing or flickering light is the most common trigger for reflex epilepsy, rare triggers include certain sounds, music, tone of voice, reading, immersion in hot water, and even eating.

16
Temporal Lobe Epilepsy
The temporal lobes, one on each side of the head, just above the ears, are the sites of one of the most common forms of epilepsy. Complex partial seizures with automatisms (unconscious actions), such as lip smacking or rubbing the hands together, are the most common seizures in temporal lobe epilepsy.
Seventy-five percent of patients also experience simple partial seizures which may include such features as: a mixture of thoughts, emotions, and feelings that are hard to describe; sudden emergence of old memories or feelings of strangeness in familiar surroundings; hallucinations of voices, music, smells, or tastes, and feelings of unusual fear or joy. While partial seizures dominate, approximately half the people with temporal lobe epilepsy have generalized tonic-clonic seizures as well.
The seizures characteristic of temporal lobe epilepsy often begin in the deeper parts of the temporal lobe (part of the limbic system), which control emotions and memory. Memory problems may develop over time in people with this syndrome. Treatment is with medication or surgery, or in some cases, VNS therapy.
TREATMENT
Epilepsy is a condition in which a person has a tendency to have recurring seizures. Medication can provide seizure control for approximately 70 per cent of people with epilepsy. For some people, surgery is successful if medication fails. Avoiding known triggers and attention to lifestyle can sometimes improve seizure control.
Many people experience a single seizure, while approximately 50 per cent go on to have further seizures. It is not possible to know for certain who will have more than one seizure. The circumstances of the seizure, the family history or the test results might suggest that the risk of another seizure is higher in some people. Treatment aims to prevent seizures and maximize quality of life.
Antiepileptic medications Medication can be given to prevent seizures. When deciding whether or not to start medication, or which type of medication is to be prescribed, various issues will be taken into account. These will include the:
o Type of seizure o Likely risk of having other seizures o Age of the person o Gender of the person o Person's general health

17
o Opinion of the person.
Medication is not a cureMedication does not 'cure' epilepsy; its role is to stop the seizures. To prevent seizures, the prescribed doses must be taken regularly to maintain an effective level of the drug in the body.
Medication may not be necessary foreverRegular medical reviews are important. Many people only need medication for a limited time, usually a few years. However, medication should never be stopped suddenly – your doctor should guide any changes.
Side effects and interactionsSide effects may be experienced from your medication. These can vary, depending on which medication that is prescribed. Possible side effects can include tiredness, weight changes or a skin rash. Sometimes side effects will settle over time but, if they are particularly troublesome, a doctor may suggest a change of medication.
Seizure medication can interact with other medications. It can reduce the effectiveness of other drugs, like the contraceptive pill. Taking some common over-the-counter treatments can lessen the anti-seizure effect. A doctor should be notified about any other medications you take, including vitamin supplements or herbal treatments.
Important issues about medication Some general points about antiepileptic medications include:
o Medication may be started slowly and the dose gradually increased. o A doctor should guide changes to the type or dose of medication – the medication
should not be altered without professional consulting.o A new medication is often introduced before or while the old medication is
reduced. o Sometimes a combination of medications is used. o Dosage should be constant, if missed, a doctor should be consulted. o A dosette box can help people to remember their medication. o Notify a doctor if side effects occur. Sometimes, changes can be made. o If seizures still occur while taking medication, a doctor should be notified. o Plan ahead so as not to run out of your medication. o Illness, diarrhoea and vomiting may affect the absorption of medication. o Women planning pregnancy should discuss with their doctor or specialist whether
to modify their medication and also ensure that they are taking folate supplements to reduce the risk of neural tube defects in their baby.
o Seizure medication should not be stopped suddenly.
Surgery Epilepsy is sometimes caused by an area of abnormal brain tissue, frequently located in the temporal lobe of the brain. If surgery can remove this tissue, seizures can often be

18
prevented. The chance of successful surgery and the risks of complications differ for each person.
Surgery is usually only used where medication fails. It is not intended to be a substitute for medication. If surgery is considered to be a possible treatment for your epilepsy, extensive tests will first be carried out. Your doctors will then discuss with you the possible outcomes of surgery in your case, so that you can make an informed choice.
Vagal nerve stimulator (VNS)The vagal nerve stimulator is a device that is implanted just beneath the pectoral or chest muscle. About the size of a stopwatch, it has a lead that attaches to the vagus nerve in the neck and carries a regular electric pulse. By stimulating the vagus nerve, the brain's potential to generate or spread abnormal seizure activity can be reduced. This procedure is not a substitution for medication and is only performed when medication is not effective.
Ketogenic dietThe ketogenic diet has been reported to reduce seizures in a very small number of children. Low in carbohydrate, the diet forces the body to break down muscle to make glucose. This state, known as ketosis, causes changes in body chemistry that may help to control seizures. The diet is extremely severe and must be carried out under medical supervision. It is not usually considered for adults and usually only suggested when other treatments fail.
Avoiding triggersIn some cases, a very specific trigger, such as reading, causes seizures. In these rare cases, avoiding the trigger may prevent seizures. There are a number of other factors that may trigger seizures in some people. These can vary from person to person. Avoiding or reducing these triggers may help to reduce seizures in some people, but not all triggers can be avoided and seizures can still occur without the suspected triggers. Some possible triggers include:
o Lack of sleep o Missed medication o Alcohol o Certain drugs (prescription and recreational) o Flickering lights or patterns o Stress o Menstruation o Illness (especially with diarrhea or vomiting) o Overheating o Low blood sugar o Certain smells, colors or sounds.
Complementary therapiesComplementary therapies may help a person with epilepsy by improving overall health

19
and wellbeing. However, research does not suggest that complementary therapies are likely to improve seizure control in most cases. In some situations, they have been shown to trigger seizures.
If you are interested in using a complementary therapy, discuss this with your doctor. If you use a complementary therapy, it is usually strongly recommended that you do not stop your antiepileptic medication unless advised to do so by your doctor.
Where to get help
The doctor Neurologist Epilepsy Foundation of Victoria Tel. (03) 9805 9111 Epilepsy Helpline Tel. 1300 852 853
Things to remember
Medication can provide seizure control for approximately 70 per cent of people with epilepsy.
Do not stop taking antiepileptic drugs suddenly without medical advice. Epilepsy surgery may prevent seizures for some patients where medication fails. Attention to lifestyle issues may improve seizure control.
What can I do to help myself?
Keep a diaryThere is often no apparent reason why a seizure occurs at one time and not another. However, some people with epilepsy find that certain 'triggers' make a seizure more likely. These are not the cause of epilepsy, but may trigger a seizure on some occasions. Possible triggers include:
o Stress or anxiety. o Alcoholic drinks or street drugs. o Some medicines such as anti-depressants, anti-psychotic medication, and other
less commonly used medicines. o Lack of sleep or tiredness. o Irregular meals which cause a low blood sugar. o Flickering lights such as from strobe lighting. o Menstruation (periods). o Illnesses which cause fever such as 'flu or other infections.
If you suspect a 'trigger' it may be worth keeping a diary to see if there is any pattern to the seizures. Some are unavoidable, but treatment may be able to be tailored to some triggers. For example:
o Keeping to regular meal times and bedtimes may be helpful for some people.

20
o Learning to relax may help. Your doctor may be able to advisc about relaxation techniques.
o A small number of people with epilepsy have 'photosensitive' seizures. This means that seizures may be triggered by flickering lights from the TV, video games, disco lights, etc. Avoiding these may be an important part of treatment for some people. (Photosensitive epilepsy can be confirmed by hospital tests. Most people with epilepsy do not have photosensitive seizures and do not have to avoid TVs, videos, discos, etc.)
TR IMPLICATIONS
TR specialists often work with clients who also have a secondary diagnosis such as mental illness, retardation, physical handicaps, etc. Recognizing potential limitations concerning medications, activity restrictions, etc, The therapist should then take an active role in some of the psychosocial roles of this population. Three central topics are:
Stress Reduction
Most individuals with epilepsy and other convulsive disorders suffer from frightening fears of future seizures, with the majority believing that they may die during the next seizure. Realistic or perceived, TR specialists can be fundamental in teaching effective stress reduction methods and relaxation skills to help manage these fears.
Leisure Lifestyle
Society carries a heavy stigmatism concerning epilepsy, and clients commonly reflect affective disorders such as anxiety and depression. TR specialists can promote strong experiential work in social settings. By strengthening a client’s leisure skill repertoire and developing a rewarding leisure lifestype with others, TR services can assist individuals to remain active participants in social activities, dispelling some of the disorder’s stigmatization.
Locus of Control
In addition, clients often feel that they have no control over their lives, (tend to have a low internal locus of control.) Although a natural and real consequence of having a chronic illness, it may be very debilitating by making the individual feel they have no control in all aspects of their lives. Therefore, TR specialists can assist clients by helping them develop master experiences. Only through feelings of personal competence and higher levels of skill can individuals be convinced to change their perceptions of locus of control.
GLOSSARY
Adjunctive

21
Additional, add on. As in adjunct or adjunctive therapy, concerning a drug which is added to an existing medication.
Affect Mood, level of emotional responsiveness.
Affective Concerning or influencing mood and level of responsiveness.
Amygdala Part of the limbic system of the brain. Seizures arising in this area include a rising sensation in the stomach, nausea, movements of the mouth, chewing, fear, panic, and flushing of the face and other autonomic symptoms.
Anoxia Lack of oxygen.
Aphasia Defect in or loss of the ability to express oneself using speech, writing, or signs, or to comprehend spoken or written language as a result of injury to or disease of the brain's speech centers.
Apnea Cessation of breathing.
Apraxia Loss of ability to carry out familiar, purposeful movements, especially inability to make proper use of an object.
Arteriovenous malformation (AVM) A tangle of blood vessels in the brain, may produce seizures when they bleed.
Aspartate An excitatory neurotransmitter.
Autoinduction A process whereby the body learns to metabolize (process) an antiepileptic drug, such as carbamazepine (Tegretol) more effectively over time, requiring a higher dose to control seizures than was initially needed.
Automatism Involuntary, undirected movements during complex partial seizures and atypical absence seizures.
Autonomic nervous system System of the brain that controls key bodily functions not under conscious control, such as heartbeat, breathing, sweating. System may be affected by seizures.
Blood level The concentration or amount of antiepileptic or other drug present in the bloodstream, usually expressed as micrograms or nanograms per milliliter.
Catamenial epilepsy Epilepsy in which there is a tendency for a woman's seizures to occur primarily at the time of menstruation.
Clinical trials Multi-phased, organized systems of testing new drugs in human populations, and subsequent analysis of the results.
Compliance

22
Refers to patient adherence to physician directions for taking antiepileptic drugs. Computerized tomography (CT)
A scanning method that uses X-rays and computers to create images of the internal structure of the brain, produced at different levels, in a series of 'slices.'
Convulsive syncope A seizure caused by fainting in which the supply of oxygen to the brain is limited.
Corticography Direct recordings of brain activity from the surface of the cortex, usually during brain surgery.
Cryptogenic Of unknown origin.
Cyanosis A blueish discoloration, particularly of the skin and mucous membranes, due to lack of oxygen.
Dose-related effect A negative side effect produced by high dosage of an antiepileptic or other type of drug.
Dysmemnesia Impaired memory.
Dysphasia Difficulty in swallowing.
Encephalopathy Any degenerative disease of the brain.
Epidural electrode placement Placement of electrodes on or outside the dura mater, a membrane covering the surface of the brain.
Epilepsia partialis continua A prolonged simple partial seizure affecting movement.
Epileptiform Appearing to be like epilepsy, as in an epileptiform discharge on an EEG.
Epileptogenic Causing epilepsy or an epileptic response.
Focal seizure Older term for partial seizure.
Focus Identified area of the brain from which partial seizures arise.
Gamma aminobutyric acid (GABA) A neurotransmitter which inhibits neuronal firing.
Generic The name of the drug as opposed to a brand name developed by the manufacturer.
Glutamate An excitatory neurotransmitter.
Gustatory Related to the sense of taste.
Half-life

23
Length of time needed for half of a substance to decay or be metabolized. In epilepsy, refers to the half-life of an antiepileptic drug in the body.
Hemiplegia Paralysis of one side of the body.
Hyperventilation Rapid, deep breathing. Use in EEG testing may produce abnormalities or even a seizure.
Hypsarrhythmia A distinctive EEG pattern associated with infantile spasms in babies.
Ictal Pertaining to, characterized by, or caused by an epileptic seizure.
Idiopathic Of unknown origin or cause.
Idiosyncratic reaction With reference to medication side effects, describes unusual sensitivity or an allergic-like reaction to a drug which others take without problems.
Intractable Not responding to treatment.
Kindling A procedure used in animals in which unprovoked seizures (epilepsy) can be produced by a series of provoked seizures.
Landau-Kleffner syndrome A rare, childhood condition producing seizures and progressive loss of the ability to speak.
Magnetic resonance imaging An imaging method using magnets instead of X-rays. Produces detailed pictures of the internal structure of the brain.
Mechanism of action How a drug or physical process works in the body.
Minor motor seizure An older term for a partial seizure affecting movement.
Monotherapy Treatment with a single drug.
Neoplasia Formation of new and abnormal cell growth.
Olfactory Related to the sense of smell.
Onset Beginning. As in age of onset, referring to the age at which the condition began.
Paroxysmal A sudden outburst or eruption.
Pharmacokinetics The behavior of drugs in the body, specifically rates of absorption, achievement of peak levels, and metabolism.
Photic stimulation

24
Stimulation of the brain through intense or flashing light or alternating patterns of light and dark.
Positron emission tomography (PET) An imaging technique that shows metabolic activity in the brain.
Prodromal Indicating the onset of a disease. In epilepsy, indicating the onset of a seizure.
Prognosis The expected course or outlook for a given medical illness.
Psychic (as in psychic symptoms) Referring to emotional, intellectual or mood effects.
Rasmussen's encephalitis A rare form of epilepsy affecting one whole hemisphere of the brain; progressive in nature.
Refractory Difficult to treat, unresponsive or of limited response to medication.
Single-photon emission computerized tomography (SPECT) An imaging technique to measure blood flow in the brain.
Slowing A type of EEG wave associated with lower levels of arousal, sleepiness, drugs, and the after effects of seizures.
Somatosensory Related to bodily sensation.
Steady state A state of balance or equilibrium. Refers to drug levels which stay steady so long as the rate of metabolism is balanced by continued intake of enough medication to replace what has been used up.
Sturge-Weber syndrome A blood vessel disorder affecting the face, eyes and brain, also associated with seizures.
Subdural electrode placement Placement of electrodes deep in the brain.
Symptomatic A condition arising out of a specific cause.
Therapeutic range Blood levels at which a drug can be expected to produce a beneficial effect without toxicity.
Transient hemiplegia Temporary paralysis of one side of the body.
Trough level In blood level monitoring of antiepileptic drugs, the minimum level of drug in the blood prior to absorption of the next dose.
Tuberous sclerosis A genetic condition in which tumors arise in the brain, eyes, skin, and internal organs, producing seizures. Mental retardation may be associated with the condition.
Versive
25
Turning as in involuntary turning during a seizure. Vertigo
Dizziness.
REFERENCES
Internet
o [email protected] www.cdc/gov/nccdphp o www.aesnet.orgo www.naecepilepsy.org o www.chronicdisease.org o www.epilepsy.com o www.epilepsyfoudation.com o www.medlineplus.gov
Books
o Austin, David R. Therapetuic Recreation. Allyn & Bacon; Needham Heights, MA., 2001.

26
Cardiac Diseases
Cardiac diseases are conditions affecting the heart’s ability to work effectively.http://www.apshealthcare.com/mellon/cardiac.htm
From the moment it begins beating until the moment it stops, the human heart works tirelessly. In an average lifetime, the heart beats more than two and a half billion times, without ever pausing to rest. Like a pumping machine, the heart provides the power needed for life. http://sln.fi.edu/biosci/heart.html
This website is a good one for viewing the anatomy of the heart.http://www.cardioconsult.com/anatomy/
1. Right Coronary 2. Left Anterior Descending 3. Left Circumflex 4. Superior Vena Cava 5. Inferior Vena Cava 6. Aorta 7. Pulmonary Artery 8. Pulmonary Vein
9. Right Atrium 10. Right Ventricle 11. Left Atrium 12. Left Ventricle 13. Papillary Muscles 14. Chordae Tendineae 15. Tricuspid Valve 16. Mitral Valve 17. Pulmonary Valve
Aortic Valve (Not pictured)

27
Cardiac Disease: Affects Men and Women differently, but despite common beliefs, does not necessarily affect men more than it affects women
Think of a heart attack victim and you'll probably picture a middle-aged man, perhaps a little paunchy, most likely a workaholic executive type. It's a stereotype that has been reinforced by the media and by the medical profession itself, which in the past has focused much of its research into heart disease on this type of patient.
Not Just a Man's DiseaseThe facts, however, tell quite a different story. Heart disease is more than just a man's disease—much more. One in 9 women between the ages of 45 and 64 has some form of cardiovascular disease, ranging from coronary artery disease to stroke or renal vascular disease. By the time a woman reaches 65, she has a 1 in 3 chance of developing cardiovascular disease. And a number of studies show that African-American women are at even greater risk than these averages.
Heart disease, in its various forms, is the leading killer of American women. The following statistics paint a graphic picture:
One-third of all deaths of American women each year are attributable to heart disease. Heart disease kills more women each year than cancer, accidents, and diabetes combined.
All forms of cardiovascular disease kill nearly 500,000 American women a year. Stroke alone kills 88,000.
Myocardial infarction, commonly known as a heart attack, kills 244,000 women a year.
Forty percent of women with heart disease will eventually die of it.
The reason that so much more attention has been focused on men is that they are much more likely to be stricken with heart disease in their prime middle years, whereas women tend to get it 10 to 20 years later. For most women, it is only after menopause that heart disease becomes a problem. But a woman of 60 is about as likely to get heart disease as a man of 50, and by time they are in their 70s, men and women get heart disease at equal rates.
http://www.healthsquare.com/heartdisease.htmIncidence of cardiovascular disease in selected age groups, by gender;

28
Source: American Heart Association
Cardiovascular Disease Mortality Trends for Males and Females United States: 1979-2002Source: CDC/NCHS.
Leading Causes of Death for All Males and Females United States: 2002
A Total CVD (Preliminary)B CancerC AccidentsD Chronic Lower Respiratory DiseasesE Diabetes MellitusF Alzheimer’s Disease
380400420440460480500520
Years
Deat
hs in
Tho
usan
ds
Males Females

29
Heart Disease in Children
Diseases, Conditions and Treatments
The two types of heart disease in children are "congenital" and "acquired." Congenital heart disease (also known as a congenital heart defect) is present at birth. Some defects in this category are patent ductus arteriosis, atrial septal defects and ventricular septal defects. Acquired heart disease, which develops sometime during childhood, includes diseases such as Kawasaki disease, rheumatic fever and infective endocarditis. Common diagnostic tests for these diseases are explained here.
About 40,000 children are born with a heart defect each year. Most of these children can benefit from surgery even if the defect is severe. When surgery is necessary, many medical treatments are available to help the heart work properly. There is nothing that parents could have done to prevent these defects. Learn about conditions that can interfere with the work of the heart and treatment options in this section.
Kawasaki disease is an example of acquired heart disease that occurs primarily in children who are 5 years old or younger. Although medical knowledge of the disease is still developing, there are steps you can take to recognize the symptoms and deal with the disease's effects.
At least 8 of every 1,000 infants born each year have a heart defect. About 1 million Americans with cardiovascular defects are alive today. Though research is ongoing, at least 35 defects have now been identified.
30
Specific Diseases of the Heart: A Brief summary and Explanationhttp://www.cardiac-disease.net/ and http://www.americanheart.org
Congestive Heart Failure
Congestive heart failure (CHF), or heart failure, is a condition in which the heart can't pump enough blood to the body's other organs. This can result from
narrowed arteries that supply blood to the heart muscle — coronary artery disease.
past heart attack, or myocardial infarction, with scar tissue that interferes with the heart muscle's normal work.
high blood pressure. heart valve disease due to past rheumatic fever or other causes. primary disease of the heart muscle itself, called cardiomyopathy. heart defects present at birth — congenital heart defects. infection of the heart valves and/or heart muscle itself — endocarditis and/or
myocarditis.
The "failing" heart keeps working but not as efficiently as it should. People with heart failure can't exert themselves because they become short of breath and tired.
As blood flow out of the heart slows, blood returning to the heart through the veins backs up, causing congestion in the tissues. Often swelling (edema) results. Most often there's swelling in the legs and ankles, but it can happen in other parts of the body, too. Sometimes fluid collects in the lungs and interferes with breathing, causing shortness of breath, especially when a person is lying down.
Heart failure also affects the kidneys' ability to dispose of sodium and water. The retained water increases the edema.
How do you diagnose and treat congestive heart failure?
Your doctor is the best person to make the diagnosis. The most common signs of congestive heart failure are swollen legs or ankles or difficulty breathing. Another symptom is weight gain when fluid builds up.
CHF usually requires a treatment program of
rest proper diet modified daily activities drugs such as
o ACE (angiotensin-converting enzyme) inhibitorso beta blockerso digitalis

31
o diureticso vasodilators
Various drugs are used to treat congestive heart failure. They perform different functions. ACE inhibitors and vasodilators expand blood vessels and decrease resistance. This allows blood to flow more easily and makes the heart's work easier or more efficient. Beta blockers can improve how well the heart's left lower chamber (left ventricle) pumps. Digitalis increases the pumping action of the heart, while diuretics help the body eliminate excess salt and water.
When a specific cause of congestive heart failure is discovered, it should be treated or, if possible, corrected. For example, some cases congestive heart failure can be treated by treating high blood pressure. If the heart failure is caused by an abnormal heart valve, the valve can be surgically replaced.
If the heart becomes so damaged that it can't be repaired, a more drastic approach should be considered. A heart transplant could be an option.
Most people with mild and moderate congestive heart failure can be treated. Proper medical supervision can prevent them from becoming invalids.
See the Related Items box above for links to the Cardiology Patient Page in Circulation, Journal of the American Heart Association:
What affects one side of the heart eventually will affect both sides as the heart and lungs are interconnected systems. Left side failure occurs when left ventricular output is less than the volume of blood received from the right side of the heart via the pulmonary circulation. Congestion in the pulmonary circuit ensues and the systemic blood pressure falls. Myocardial infarction is the most common cause of left heart failure but it can also be caused by hypertension, aortic insufficiency or cardiomyopathy.
Right heart failure, similarly, occurs when the right ventricle cannot pump the volume of blood returned to it. The resulting congestion of the systemic venous system and decreased output to the lungs causes venous distention, swelling of distensible organs to produce hepatomegaly, splenomegaly and peripheral edema. In addition, many of the effects of left heart failure are seen because of the inadequate return from the lungs and output of the left ventricle. The causes of right heart failure are left heart failure, obstructive lung disease, and congenital heart defects.
Treatments are generally aimed at increasing the pumping ability of the heart, reducing the volume of blood that must be pumped, reducing fluid retention and management of vascular tone.
Cardiogenic shock

32
An often-fatal complication called cardiogenic shock — the heart’s failure to pump due to sustained interruption of its blood supply
Any factor that depresses myocardial function can precipitate cardiogenic shock. The most common cause is myocardial infarction. The prognosis once shock ensues is not good and the mortality rate following myocardial infarction is 60-80%. When the pumping ability of the heart is diminished, systolic blood pressure drops, and the sympathetic nervous system is activated causing peripheral vasoconstriction and increased heart rate (tachycardia). The net effect increases the load on the heart in an effort to maintain coronary and cerebral blood flow. These mechanisms may compensate and maintain arterial pressure or they might be inadequate and irreversible shock is the end. Peripheral tissues are functioning under anaerobic conditions and it is the lactic acid produced that eventually cause cellular death.
CardiomyopathyConditions that affect the ventricular muscle and decrease the pumping ability of the heart are classified as cardiomyopathies. Inflammation of the myocardium due to infection or damage caused by radiation or chemicals is called myocarditis. Many types of myocarditis will resolve with bed rest, drug therapy, and fluid restriction.
Congestive cardiomyopathy is a feature of beriberi, alcoholism, diabetes, drug toxicity and some neuromuscular disorders. Enlargement of the heart that is seen is a result of dialation and enlargement of the heart that can no longer pump efficiently. The symptoms are then characteristic of double sided congestive heart failure.
Hypertrophic cardiomyopathy is an asymmetric increase in ventricular muscle mass. The ventricular septum is especially enlarged causing the left ventricle to be misshapen and obstructing the blood flow from the ventricle. Symptoms are basically those of left congestive heart failure.
Coronary artery disease
A condition caused by thickening of the walls of the arteries that supply blood to the heart muscle. When these arteries become blocked, the heart is deprived of oxygen and can become damaged. Severe cases can result in heart attack.
Coronary artery disease occurs when the interior of the vessels supplying the heart become blocked and restrict blood flow to the heart. It occurs when fatty plaques are formed inside the lumen of the arteries. The levels of low density lipoproteins (LDL), specifically oxidized LDL, in the blood correlate with the severity of atherosclerosis. Blood clots can form at the plaque and cut off the flow of blood.
Treatments for coronary artery disease include bypass surgery, balloon angioplasty, and laser angioplasty. Bypass surgery consists of taking a vessel from somewhere else in the body (usually the leg) and grafting it into the coronary circulation to reroute blood flow

33
around the blockage. Coronary bypass surgery is very effective in treating angina. Balloon angioplasty has become a very common procedure where a catheter is introduced into an artery in the leg or arm and is guided to the blockage. A small balloon is inflated that flattens the plaque against the artery so that the vessel is opened and blood flow is restored. Laser angioplasty operates in a similar fashion except the catheter delivers an optical fiber to the blocked area. The plaque is destroyed by irradiation with laser light and blood flow is restored.
Defective Heart ValvesThe heart valves keep the flow of blood moving through the heart in one direction by opening and closing in sequence with the contraction of the heart muscle. When valve disease is present, one or more of the heart valves do not work properly. The valve may be "narrowed," which limits the ability of the chamber of the heart to fill completely, or the valve may "leak," which allows some blood to back up against the normal direction of flow.
Most valve defects are mild and have little effect on the pumping function of the heart. However, some defects become progressively worse and may cause weakening of the heart.
Heart catheterization allows the cardiologist to see the operation of the heart vales and monitor the flow of blood through the heart. This allows the doctor to confirm the diagnosis of heart valve disease and measure the severity of a valve’s narrowing or leakage.
Congenital Heart DefectsA congenital heart defect is a deformity of the heart that is present at birth. Common examples of congenital heart defects include an abnormal hole between heart chambers, or a narrowed valve.
When congenital heart defects are severe, the pumping action of the heart may be compromised, limiting its efficiency in delivering oxygen-rich blood to the body. Some congenital heart defects make the heart work harder to compensate for the deformity, which, with the passage of time, causes the heart to weaken and decrease in efficiency.
Cardiac catheterization is often used to confirm the diagnosis of congenital heart defects and to assess the extent of the problem.
Ischemic heart disease The most prevalent form of heart disease, in which narrowed or blocked coronary arteries result in decreased blood supply.
Angina pectoris, or chest pain, is caused by decreased oxygen delivery to the myocardium usually due to blockage of the coronary arteries. The severe pain usually radiates to the left shoulder and down the left arm but may also radiate to the abdomen, back or jaw. The steady severe pain and feeling of pressure in the chest may last from a
34
few seconds to several minutes. Inhalation of amyl nitrate or sublingual nitroglycerin can help to dilate the coronary vessels temporarily.
Angina may be treated surgically by bypassing problem areas, opening the blood vessels (angioplasty) or by transmyocardial revascularization. This latter procedure involves the use of a laser to drill small holes in the myocardium that allow blood to enter and muscular access to oxygen. Laser transmyocardial revascularization is used in patients that have angina that isn't eliminated by opening up the coronary arteries. An alternative procedure, percutaneous transluminal myocardial revascularization, uses a catheter inserted into an artery in the thigh or arm that is then placed into the left ventricle where 15-30 holes are laser drilled into the myocardium before the catheter is withdrawn. This procedure is less invasive than direct transmyocardial revascularization as it does not require opening the chest. Sometimes transmyocardial revascularization is used in addition to bypass for patients with severe angina.
ArrhythmiaAn abnormal rhythm or rate of the heartbeat caused by disturbances in the movement of electrical impulses through the heart.
The normal heat beat is initiated at the pacemaking sinoatrial node. An irregular heart beat is known as an arrhythmia including alterations in rate and atrioventricular conduction. Physiological, pathological and pharmacological causes can effect the conduction or discharge of impulses within the heart. An arrhythmia can be a tachycardia or increased heart rate, usually over 100 beats/minute, or a slower heart rate called bradycardia which is usually under 60 beats/minute. Physiological causes of tachycardia include emotion, exercise, fever, or stress. Bradycardia is normally seen during sleep. Arrhythmias are common in patients with acute myocardial infarction (80%), during anesthesia (50%), and in about 25% of patients on digitalis.
The arrhythmia may represent a lack of normal communication between the atrial conduction system and the ventricles. Because the atria are electrically isolated from the ventricles except for the conductive fibers, the atria can enter tachycardia without the ventricles being effected. An ectopic focus is usually involved in this case. An ectopic focus is an area of myocardial tissue that takes over pacemaker functions because it spontaneously discharges more rapidly than the sinoatrial node, usually because of injury. Ectopic foci can occur in the ventricles too and frequently do following a myocardial infarct. Some drugs, such as digitalis, sympatholytics, or cholinergics can alter heart rate due to direct effects on cardiac muscle or the nervous regulation of the heart.
Therapy for arrhythmias is aimed at decreasing pacemaker activity and modifying impaired conduction. The mechanisms involve the use of sodium channel blockers, calcium channel blockers and/or beta blockers in an effort to decrease the automaticity, conduction, and excitability of the heart or increase the refractory period of cardiac muscle. the effect is more pronounced in depolarized or injured tissue than in normal cardiac muscle. Drug-induced arrhythmias can result from toxic effects on cardiac conduction systems with increased dosages.
35
Atrial fibrillation is where the atria beat rapidly and incompletely in a disorderly and irregular manner. This is due multiple waves of excitation passing over the atria. Ventricular fibrillation, similarly, is when the ventricular muscle contracts in an uncoordinated fashion due to the rapid discharge of multiple ventricular ectopic foci. Fibrillating atria or ventricles cannot efficiently pump blood and in the case of ventricular fibrillation that lasts more than a few minutes it is fatal if the patient is not treated. Electronic defibrillators can stop ventricular fibrillation by initiating an electric shock that resets and restores normal rhythm to the heart.
Myocardial infarction (AKA Heart Attack)Ischemic necrosis of the myocardium results from inadequate blood flow and therefore oxygen delivery to the myocardium that causes irreversible cell damage and cellular death. Symptoms are pain similar to angina pectoralis, shock, arrhythmias, cardiac failure, and possibly sudden death. Some 10-25% of myocardial infarcts occur without chest pain so angina is not a perfect indicator.
The electrocardiogram (ECG) is the most useful direct test available for diagnosis of a heart attack. Laboratory tests are often inconclusive but several parameters give abnormal results in most patients and can therefore be used as indicative of an infarct. Cellular death releases myocardial enzymes that can be used to diagnose the severity of the infarct. Enzymes such as lactate dehydrogenase, creatine phosphokinase, and serum aspartate aminotransferase levels are elevated at certain times after an infarct has occurred and may also give some indication of the severity of the damage.
The time between the onset of ischemia and muscle cell death is about 15 to 20 minutes in most cases. Almost always the infarction occurs in the left ventricle and left ventricular function may be significantly diminished. The larger the affected area of the myocardium the greater the loss of contractility. All myocardial infarctions have a central area of necrosis that is surrounded by an area of injury. Myocardial tissue does not regenerate after injury so the necrotic tissue is replaced by scar tissue that may inhibit contractility. If a large area of tissue is involved the heart as a pump may be compromised and the symptoms of congestive heart failure or cardiogenic shock will be seen.
Complications of myocardial infarction include various disturbances in the normal heart rhythm, congestive heart failure, cardiogenic shock, thromboembolisms, pericarditis, and myocardial rupture. Ninety percent of patients will have some disturbance of rhythm following myocardial infarction. This is a result of local changes that effect automaticity and conduction of the heart muscle.
Ten percent of those that die from a myocardial infarction have emboli to the brain, kidney, spleen or mesentery. Emboli almost always originate in the peripheral venous system due to bed rest and heart failure. With modern day management including anticoagulation therapy and early mobilization, pulmonary embolisms have become rare complications of heart attacks. Rupture of the myocardial wall can occur in cases of severe myocardial damage and results in almost immediate death.
36
InfectionsInfections of the pericardium or endocardium of the heart may be caused by a variety of organisms including bacteria, fungi, rickettsiae, and sometimes viruses or parasites. The infective organism is usually of low virulence and therefore slow growing causing the infection to develop gradually over weeks and months. Sometimes however, a more virulent organisms can cause rapid development of an infection.
In endocarditis, the infection invades the cardiac valves and leaflets thus preventing normal alignment of the cusps. This can lead to incomplete closure of the valves or regurgitation leading to cardiac murmurs. Symptoms include fever, blood in the urine, enlarged spleen, nodules on the pads of the fingers, petechiae (small pinpoint hemorrhages in the skin), and anemia. Treatment involves determining the causative agent and directing antibiotic therapy at the microorganism. Without treatment recovery is rare and death usually results.
When the pericardial sac is inflamed due to open heart surgery, myocardial infarction, viral or bacterial infections, tumors, or trauma it may become thickened and fibrotic. The change in compliance of the pericardial membrane restricts ventricular filling. In acute pericarditis, chest pain and electrocardiographic changes are seen but the most important sign is that of an audible pericardial friction rub that sounds like sandpaper rubbing the pressure rises. When it equals or exceeds that of the heart during diastole, structures such as the right atrium and ventricle become compressed and blood is not returned to the heart. This is life-threatening and death may occur from circulatory collapse.together. When fluid accumulates between the layers of the pericardium cardiac compression and tamponade can result. As fluid accumulates in the pericardium,
Heart Attack Warning SignsSome heart attacks are sudden and intense — the "movie heart attack," where no one doubts what's happening. But most heart attacks start slowly, with mild pain or discomfort. Often people affected aren't sure what's wrong and wait too long before getting help. Here are signs that can mean a heart attack is happening:
Chest discomfort. Most heart attacks involve discomfort in the center of the chest that lasts more than a few minutes, or that goes away and comes back. It can feel like uncomfortable pressure, squeezing, fullness or pain.
Discomfort in other areas of the upper body. Symptoms can include pain or discomfort in one or both arms, the back, neck, jaw or stomach.
Shortness of breath. May occur with or without chest discomfort. Other signs: These may include breaking out in a cold sweat, nausea or
lightheadedness
As with men, women's most common heart attack symptom is chest pain or discomfort. But women are somewhat more likely than men to experience some of the other common symptoms, particularly shortness of breath, nausea/vomiting, and back or jaw pain.

37
If you or someone you're with has chest discomfort, especially with one or more of the other signs, don't wait longer than a few minutes (no more than 5) before calling for help. Call 9-1-1... Get to a hospital right away.
Calling 9-1-1 is almost always the fastest way to get lifesaving treatment. Emergency medical services staff can begin treatment when they arrive -- up to an hour sooner than if someone gets to the hospital by car. The staff are also trained to revive someone whose heart has stopped. Patients with chest pain who arrive by ambulance usually receive faster treatment at the hospital, too.
If you can't access the emergency medical services (EMS), have someone drive you to the hospital right away. If you're the one having symptoms, don't drive yourself, unless you have absolutely no other option.
Risk Factors and Coronary Heart Diseasehttp://www.americanheart.org/presenter.jhtml?identifier=500
Extensive clinical and statistical studies have identified several factors that increase the risk of coronary heart disease and heart attack. Major risk factors are those that research has shown significantly increase the risk of heart and blood vessel (cardiovascular) disease. Other factors are associated with increased risk of cardiovascular disease, but their significance and prevalence haven't yet been precisely determined. They're called contributing risk factors.
The American Heart Association has identified several risk factors. Some of them can be modified, treated or controlled, and some can't. The more risk factors you have, the greater your chance of developing coronary heart disease. Also, the greater the level of each risk factor, the greater the risk. For example, a person with a total cholesterol of 300 mg/dL has a greater risk than someone with a total cholesterol of 245 mg/dL, even though everyone with a total cholesterol greater than 240 is considered high-risk.
What are the major risk factors that can't be changed?
Increasing age — Over 83 percent of people who die of coronary heart disease are 65 or older. At older ages, women who have heart attacks are more likely than men are to die from them within a few weeks.
Male sex (gender) — Men have a greater risk of heart attack than women do, and they have attacks earlier in life. Even after menopause, when women's death rate from heart disease increases, it's not as great as men's.
Heredity (including Race) — Children of parents with heart disease are more likely to develop it themselves. African Americans have more severe high blood pressure than Caucasians and a higher risk of heart disease. Heart disease risk is also higher

38
among Mexican Americans, American Indians, native Hawaiians and some Asian Americans. This is partly due to higher rates of obesity and diabetes. Most people with a strong family history of heart disease have one or more other risk factors. Just as you can't control your age, sex and race, you can't control your family history. Therefore, it's even more important to treat and control any other risk factors you have.
What are the major risk factors you can modify, treat or control by changing your lifestyle or taking medicine?
Tobacco smoke — Smokers' risk of developing coronary heart disease is 2–4 times that of nonsmokers. Cigarette smoking is a powerful independent risk factor for sudden cardiac death in patients with coronary heart disease; smokers have about twice the risk of nonsmokers. Cigarette smoking also acts with other risk factors to greatly increase the risk for coronary heart disease. People who smoke cigars or pipes seem to have a higher risk of death from coronary heart disease (and possibly stroke) but their risk isn't as great as cigarette smokers'. Exposure to other people's smoke increases the risk of heart disease even for nonsmokers.
High blood cholesterol — As blood cholesterol rises, so does risk of coronary heart disease. When other risk factors (such as high blood pressure and tobacco smoke) are present, this risk increases even more. A person's cholesterol level is also affected by age, sex, heredity and diet.
High blood pressure — High blood pressure increases the heart's workload, causing the heart to thicken and become stiffer. It also increases your risk of stroke, heart attack, kidney failure and congestive heart failure. When high blood pressure exists with obesity, smoking, high blood cholesterol levels or diabetes, the risk of heart attack or stroke increases several times.
Physical inactivity — An inactive lifestyle is a risk factor for coronary heart disease. Regular, moderate-to-vigorous physical activity helps prevent heart and blood vessel disease. The more vigorous the activity, the greater your benefits. However, even moderate-intensity activities help if done regularly and long term. Exercise can help control blood cholesterol, diabetes and obesity, as well as help lower blood pressure in some people.
Obesity and overweight — People who have excess body fat — especially if a lot of it is at the waist — are more likely to develop heart disease and stroke even if they have no other risk factors. Excess weight increases the heart's work. It also raises blood pressure and blood cholesterol and triglyceride levels, and lowers HDL ("good") cholesterol levels. It can also make diabetes more likely to develop. Many obese and overweight people may have difficulty losing weight. But by losing even as few as 10 pounds, you can lower your heart disease risk.
39
Diabetes mellitus — Diabetes seriously increases your risk of developing cardiovascular disease. Even when glucose levels are under control, diabetes increases the risk of heart disease and stroke, but the risks are even greater if blood sugar is not well controlled. About three-quarters of people with diabetes die of some form of heart or blood vessel disease. If you have diabetes, it's extremely important to work with your healthcare provider to manage it and control any other risk factors you can.
What other factors contribute to heart disease risk?
Stress — Individual response to stress may be a contributing factor. Some scientists have noted a relationship between coronary heart disease risk and stress in a person's life, their health behaviors and socioeconomic status. These factors may affect established risk factors. For example, people under stress may overeat, start smoking or smoke more than they otherwise would.
Alcohol — Drinking too much alcohol can raise blood pressure, cause heart failure and lead to stroke. It can contribute to high triglycerides, cancer and other diseases, and produce irregular heartbeats. It contributes to obesity, alcoholism, suicide and accidents. The risk of heart disease in people who drink moderate amounts of alcohol (an average of one drink for women or two drinks for men per day) is lower than in nondrinkers. One drink is defined as 1-1/2 fluid ounces (fl oz) of 80-proof spirits (such as bourbon, Scotch, vodka, gin, etc.), 1 fl oz of 100-proof spirits, 4 fl oz of wine or 12 fl oz of beer. It's not recommended that nondrinkers start using alcohol or that drinkers increase the amount they drink.
Diagnostic Tests
Echocardiogram
What is an Echocardiogram?
An echocardiogram is a test that uses ultrasound waves to examine the heart. Because it is a non-invasive test, it is a safe and painless way to help doctors diagnose a number of abnormalities of the heart.
Is the Echocardiogram Safe?
The echocardiogram is very safe. It is a non-invasive procedure using ultrasound waves. There are no known risks from the ultrasound waves.
The echocardiogram is also painless, although you may feel slight discomfort when the transducer is held firmly against the chest.
What Does It Show?

40
Doctors can see how well your heart functions during exertion by studying what happens during the exercise test.
Size and shape of the heart. The images may be used to measure the size of the heart chambers and thickness of the heart muscle.
Pumping efficiency of the heart. The images show the efficiency with which the heart pumps blood, as well as whether the heart is pumping at full strength or is weakened. The scans may also show whether the various parts of the heart pump equally.
Valve abnormalities. An echocardiogram shows the shape and motion of the heart valves. It can reveal if a heart valve is narrowed or leaking and show how severe the problem is.
Other uses. The test may also detect the presence of fluid around the heart; blood clots, or masses inside the heart; and abnormal holes between heart chambers.
Preparing For A Test
Do not eat or drink 3 hours prior to the test. This will prevent the possibility of nausea, which may accompany vigorous exercise after eating. If you are diabetic and take medications for diabetes, get special instructions from your doctor.
If you are currently taking any heart medications, check with your doctor. You may be asked to stop certain medications a day or two before the test. This can help get more accurate test results.
Wear loose, comfortable clothing that is suitable for exercise. Men usually don't wear a shirt during the test, and women generally wear a bra and a lightweight blouse or a hospital gown. You should also wear comfortable walking shoes or sneakers.
Before the test, you will be given an explanation of the test and asked to sign a consent form. Feel free to ask any questions about the procedure.
Several areas on your chest and shoulders will be cleansed with alcohol and an abrasive lotion, to prepare the skin for the electrodes. Men may need to have areas of their chest shaved, to ensure that the electrodes stay in place.
What Happens During the Test?
The echocardiogram can be performed in the doctor's office or at the hospital. No special preparation is necessary for this test. If you are scheduled for an exercise echocardiogram, however, you will be given special instructions.
You will be asked to remove clothing above the waist, and put on a hospital gown or a sheet to help keep you warm and comfortable. You will then lie on an examination table.
Electrodes (small sticky patches) and wires will be attached to your chest and shoulders to record your electrocardiogram (ECG or EKG). The ECG shows your heart's electrical activity during the test.
41
Next, you will lie on your back or on your left side. To improve the quality of the pictures, a colorless gel is applied to the area of the chest where the transducer will be placed.
A technician moves the transducer over the chest, to obtain different views of the heart. He or she may ask you to change positions. You may also be asked to breathe slowly or hold your breath, in order to get a better picture. A thorough examination usually takes from 20 minutes to an hour, depending on the number of views and whether the Doppler echo is used.
How Does An Echocardiogram Work?
An echocardiogram works very much like sonar. Ultrasound waves are transmitted into the chest and the reflection of these waves off the various parts of the heart is analyzed by sophisticated equipment.
A transducer, which is a small microphone-like device, is held against the chest. The transducer sends and receives the ultrasound waves. By moving the transducer to various positions on the chest, different structures of the heart may be analyzed.
A computer assembles the reflected ultrasound waves to create an image of the heart. These images appear on a television screen. The images may be recorded on videotape or printed on paper for review by the cardiologist.
An echocardiogram study typically involves three different techniques. The most basic technique, called M-mode echo, produces an image that appears as a tracing than an actual heart. The exact size of the heart chambers may be measured using the M-mode echo technique.
Two-dimensional (2-D) echo shows the actual shape and motion of the different heart structures. This advanced technique provides images that represent "slices" of the heart in motion.
Doppler echo is a third technique that portrays the flow of blood through the heart. The images representing the flow of blood through the heart may be displayed as a series of black-and-white tracings or as color images on the television screen.
During a Doppler echo procedure, you will hear some unusual sounds. These whooshing or pulsating sounds are computer-generated to provide the technologist with audio feedback. They are not the sounds of your heart.
The Benefits
A Major benefit of the echocardiogram is that it gives information about the heart's structures and blood flow without anything other than sound waves entering the body. The information gained from the echocardiogram allows your doctor make an accurate

42
diagnosis and develop a treatment plan that is best for you. The major limitation is that it is often difficult to obtain good quality images from persons who have broad chests, are obese, or are suffering from chronic lung disease.
The Results
Typically, the doctor will review the images at a later time and prepare a report detailing his findings. This may take several days before the completed report is ready.
http://www.cardioconsult.com/DiagnosticTechniques/Echocardiogram.asp
Resting Echocardiogram
You will be asked to lie on a hospital bed or examination table. To improve the quality of the pictures, a colorless gel is applied to the area of the chest where the transducer will be placed.
A technician moves the transducer to various places over the left side of your chest. Pictures of your heart at rest are recorded on videotape.
Exercise ECG (Stress Text)
What is an Exercise ECG?
An ECG, or electrocardiogram, is a graphic representation of the electrical activity of the heart muscle as it contracts and relaxes. When the ECG is obtained on a heart that is working harder due to exercise or medication-induced stress, the test is called an exercise ECG, or "stress test." This test is useful in detecting problems that may not be apparent while the heart is at rest.
Is the Exercise ECG Safe?
The exercise test is generally safe. A small amount of risk does exist since exercise stresses the heart. Extremely rare complications include abnormal heart rhythms and a heart attack. Experienced personnel are available to handle any emergency.
What Does It Show?
Doctors can see how well your heart functions during exertion by studying what happens during the exercise test.
How long were you able to exercise? Generally, people with a healthy heart and in good physical condition are able to exercise longer?
43
Did you have significant symptoms? It is normal to feel tired and short of breath during strenuous exercise. However, if you develop chest pain or become extremely short of breath, this may indicate a heart problem.
What happened to your heart rate and blood pressure? The heart rate and blood pressure normally rise during exercise. An abnormal heart rate (too fast, too slow) or a fall in blood pressure may indicate heart disease.
What did the ECG show? Certain changes in the ECG tracing may indicate that the heart muscle is not getting enough oxygen-rich blood. Sometimes, the ECG during exercise shows arrhythmias (abnormal heart rhythms).
The exercise test is especially useful in diagnosing blockages in the coronary arteries. When the coronary arteries are blocked or narrowed, the heart muscle may not be getting enough oxygen during exercise. This often results in symptoms of angina (chest pain) and abnormal changes on the ECG.
Preparing For A Test
Do not eat or drink 3 hours prior to the test. This will prevent the possibility of nausea, which may accompany vigorous exercise after eating. If you are diabetic and take medications for diabetes, get special instructions from your doctor.
If you are currently taking any heart medications, check with your doctor. You may be asked to stop certain medications a day or two before the test. This can help get more accurate test results.
Wear loose, comfortable clothing that is suitable for exercise. Men usually don't wear a shirt during the test, and women generally wear a bra and a lightweight blouse or a hospital gown. You should also wear comfortable walking shoes or sneakers.
Before the test, you will be given an explanation of the test and asked to sign a consent form. Feel free to ask any questions about the procedure.
Several areas on your chest and shoulders will be cleansed with alcohol and an abrasive lotion, to prepare the skin for the electrodes. Men may need to have areas of their chest shaved, to ensure that the electrodes stay in place.
What Happens During the Test?
The exercise ECG test can be performed in the doctor's office or at the hospital. A trained technician will place several electrodes (small sticky patches) on your chest and shoulders to allow recording of the ECG during exercise. Wires link the electrodes to an ECG machine. A cuff will be applied to your arm to monitor your blood pressure during the test.
You will be shown how to step onto the treadmill and how to use the support railings to maintain your balance. The treadmill starts slowly, and then the speed and incline are increased gradually.

44
Your blood pressure will be checked every few minutes, and the ECG will be carefully watched for abnormal changes. You will be instructed to report any symptoms, such as chest pain, shortness of breath, leg fatigue, or dizziness.
The test may end when you become too tired to continue or when you experience significant symptoms. Other times, the test may be stopped when you reach your peak heart rate or when your ECG shows abnormal changes.
After the exercise portion of the test is over, you'll be helped to a chair or a bed. Your blood pressure and ECG will be monitored while you recover. The technician will remove the electrodes and cleanse the electrode sites. The test typically takes between 45 minutes to one hour, which includes preparation for the test, the exercise portion, and the recovery period.
The Results
Typically, the doctor will review the images at a later time and prepare a report detailing his findings. We will forward a report to the patient's doctor as well as notify the patient of the results. It may take three to four days for the doctor to receive the report.
http://www.cardioconsult.com/DiagnosticTechniques/ExerciseECG.asp
Cardiolyte/Thallium Scan
What Is an Exercise Cardiolyte/Thallium Scan?
A thallium scan is a test that uses a radioactive substance (known as a tracer) to produce images of the heart muscle. When combined with an exercise test, the thallium scan helps determine if areas of the heart do not receive enough blood.
The exercise thallium scan is especially useful in diagnosing coronary artery disease, the presence of blockages in the coronary arteries (the vessels that supply oxygen-rich blood to the heart muscle).
Is The Exercise Cardiolyte/Thallium Scan Safe?
The radiation exposure during a cardiolyte/thallium scan is extremely small, and the doses used are safe. Cardiolyte/thallium is excreted rapidly by the kidneys. However, if you are pregnant, suspect you may be, or are a nursing mother, discuss the matter with your doctor.
The exercise test is also safe. A small amount of risk does exist, however, because it stresses the heart. Possible rare complications include abnormal heart rhythms and a heart attack. Experienced personnel are available to handle any emergency.
45
What Do Cardiolyte/Thallium Scans Show?
During the test, a tiny amount of thallium tracer is injected into a vein in your arm while you walk on a treadmill. For patients who cannot exercise, the test may be done after the injection of a drug that produces a stress on the heart similar to exercise.
The tracer travels in the bloodstream, is carried through the coronary arteries, and is picked up by the heart muscle cells. Areas of the heart muscle that have an adequate blood supply pick up the tracer almost immediately. Areas that do not have an adequate blood supply pick up the tracer very slowly or not at all. This will show up as a lighter area, called a "defect".
A second set of images is taken several hours later, while you are at rest. These images help differentiate between areas that temporarily do not receive enough blood (the defect returns to normal) and areas that are permanently damaged from a previous heart attack (the defect persists).
What Happens During Tests?
The exercise cardiolyte/thallium test is usually performed at a clinic or hospital, in the nuclear medicine or radiology department.
The test has two parts: the exercise portion and the imaging portion.
Exercise Portion
The exercise portion of the test can be performed in the doctor’s office or at the hospital. A trained technician will place several electrodes (small sticky patches) on your chest and shoulders to allow recording of the ECG during exercise. Wires link the electrodes to an ECG machine. A cuff will be applied to your arm to monitor your blood pressure during the test.
You will be shown how to step onto the treadmill and how to use the support railings to maintain your balance. The treadmill starts slowly, and then the speed and incline are increased gradually.
Your blood pressure will be checked every few minutes, and the ECG will be carefully watched for abnormal changes. You will be instructed to report any symptoms, such as chest pain, shortness of breath, leg fatigue, or dizziness.
The test may end when you become too tired to continue or when you experience significant symptoms. Other times, the test may be stopped when you reach your peak heart rate or when your ECG shows abnormal changes.
After the exercise portion of the test is over, you will be helped to a chair or a bed. Your blood pressure and ECG will be monitored while you recover. The technician will

46
remove the electrodes and cleanse the electrode sites. The test typically takes between 45 minutes to one hour, which includes preparation for the test, the exercise portion, and the recovery period.
Imaging Portion
You will lie flat on a special table under a scanning camera. During imaging, the camera takes pictures at various angles. You should remain still while the pictures are being taken. This part of the test usually takes 10-20 minutes.
After the initial set of pictures, you will be asked to remain relatively quiet for the next 2-4 hours. You may leave the area, and may be allowed limited beverages, but no solid food.
When you return, you will have additional pictures taken, without repeating the exercise. These pictures represent the heart in its resting state. In some cases, more pictures are taken the next day.
The Benefits
The exercise thallium scan is generally more accurate and provides more information than an exercise ECG test. This information helps your doctor make an accurate diagnosis and develop a treatment plan that’s best for you.
The Results
The doctor conducting the test may be able to give you preliminary results before you leave. A complete interpretation, however, usually takes several days.
http://www.cardioconsult.com/DiagnosticTechniques/CardiolyteThallium.asp
Cardiac Catheterization
What Is Cardiac Catheterization?
Cardiac catheterization is a diagnostic procedure that involves the insertion of a catheter (a long, thin, flexible tube) into the heart. The catheter is introduced into the body through a vein or artery, usually in the leg, and guided by the doctor toward the heart. The doctor uses special x-ray equipment to monitor the progress of the catheter as he maneuvers it through the vein or artery toward the heart.

47
Once the catheter is inside the heart, the doctor is able to position it and inject dye into the chambers and vessels of the heart. When viewed with the special x-ray equipment, this dye allows the doctor to see the pumping action of the heart, the function of the heart valves, and the blood flow in the coronary arteries, which supply oxygen-rich blood to the heart muscle.
Other terms may be used to describe cardiac catheterization. These terms include coronary angiography, angiogram, and cardiac (or heart) cath.
Why Is Catheterization Important?
Cardiac catheterization allows the doctor to see the heart as it pumps blood. He is able to view the expansion and contraction of the chambers of the heart; the opening and closing of the heart valves; and the flow of blood through the coronary arteries.
As compared to other diagnostic tests, cardiac catheterization provides more accurate and detailed information. This is especially important when visualization of the coronary arteries is required. This test provides the doctor with a picture of the arteries of the heart and allows him the assess the presence, location, and degree of severity of blockages in the coronary arteries. This information will allow the cardiologist to chose the best treatment for you.
The Uses Of Catheterization
Cardiac catheterization enables doctors to diagnose a number of common heart conditions.
Coronary Artery Disease
The inside walls of arteries are normally smooth and flexible, allowing blood to flow through them easily. With time, fatty deposits may accumulate on the inside of an artery’s wall, causing it to become plugged.
As the build up of fatty deposits on the interior of the arteries continues, the opening of the arteries narrows with the result being a reduction in the flow of blood. When blockages occur in the coronary arteries, symptoms of angina (chest pain or discomfort) may result. Severe blockages may even cause a heart attack.
If your doctor suspects you have coronary artery disease, a cardiac catheterization is often recommended. During the heart catheterization, the x-ray dye is injected into the coronary arteries. Pictures taken show the flow of blood through the coronary arteries. Actual blockages will appear as areas where the vessel is pinched, resulting in a dramatic reduction of blood flow. The x-ray pictures allow the doctor to identify the
48
points where blockage of the coronary vessels is present and evaluate the severity of the blockage.
Defective Heart Valves
The heart valves keep the flow of blood moving through the heart in one direction by opening and closing in sequence with the contraction of the heart muscle. When valve disease is present, one or more of the heart valves do not work properly. The valve may be "narrowed," which limits the ability of the chamber of the heart to fill completely, or the valve may "leak," which allows some blood to back up against the normal direction of flow.
Most valve defects are mild and have little effect on the pumping function of the heart. However, some defects become progressively worse and may cause weakening of the heart.
Heart catheterization allows the cardiologist to see the operation of the heart vales and monitor the flow of blood through the heart. This allows the doctor to confirm the diagnosis of heart valve disease and measure the severity of a valve’s narrowing or leakage.
Congenital Heart Defects
A congenital heart defect is a deformity of the heart that is present at birth. Common examples of congenital heart defects include an abnormal hole between heart chambers, or a narrowed valve.
When congenital heart defects are severe, the pumping action of the heart may be compromised, limiting its efficiency in delivering oxygen-rich blood to the body. Some congenital heart defects make the heart work harder to compensate for the deformity, which, with the passage of time, causes the heart to weaken and decrease in efficiency.
Cardiac catheterization is often used to confirm the diagnosis of congenital heart defects and to assess the extent of the problem.
Preparing For A Catheterization
In some instances, the decision to perform a heart catheterization may be made while you are hospitalized. In other cases, you may go to the hospital specifically for the heart catheterization procedure, generally arriving at the hospital in the morning on the day of the procedure. In those instances where you know in advance that you are going to undergo a heart catheterization, there are a number of things you can do to prepare for the procedure:

49
Generally, you should not eat or drink anything for 6-8 hours before the procedure. This will minimize the chance of an upset stomach during the test. Small sips of water to swallow your medications are fine.
Make arrangements to have a family member or friend drive you home after the procedure.
Bring an "overnight bag" in case the doctor keeps you overnight in the hospital. A robe, slippers, pajamas or nightgown, and toiletries are recommended.
Bring a list of all medications you are currently taking. Be sure to include the exact names and dosages.
Mention to the doctor if you are allergic to x-ray dyes (contrast media).
Several routine tests will be performed before the procedure, including an ECG and blood tests. For your convenience, these tests may be done one or two days prior to the heart catheterization.
In preparation for the procedure, the area where the catheter will be inserted is cleaned and shaved. This makes it easier for the cardiologist to insert the catheter and minimizes the risk of infection. Usually, the preferred site for placing the catheter is the groin; however, in some cases, the crease of the arm is used.
Empty your bladder as completely as possible before the test starts. (A bedpan or urinal will be available during the procedure). Generally, you’ll be allowed to wear your dentures, hearing aids, and eyeglasses during the procedure. A small intravenous needle ("IV line") is inserted into a vein in your arm so that medications may be injected directly into the vein, if needed. A sedative will be given to help you relax.
What Is A Cardiac Catheterization Lab Like?
Cardiac catheterization is performed in a specially equipped x-ray room, called a cardiac catheterization laboratory, or simply "cath lab". Since you will be mildly sedated, you will be taken to the cath lab on a movable bed. Once in the cath lab, you will be transferred to a special x-ray table and draped with sterile sheets. The cath lab has a large x-ray camera above the table, several television screens showing views from the x-ray camera, heart monitors, and other special equipment.
The cath lab team generally includes a cardiologist, an assistant, a nurse, and one or two technicians. It is important to the cath lab team that you be comfortable throughout the procedure, so be sure to let them know of any concerns you may have. You will need to keep your legs and arms as still as possible during the procedure.
During The Heart Cath Procedure
The area where the catheter will be inserted is cleansed thoroughly. A tiny needle is used to inject a local anesthetic into the skin at the site where the catheter will be inserted. This numbs area to minimize discomfort during the procedure. The injection may cause a mild stinging sensation.

50
Once the area is numb, a small incision is made in the skin. A needle is inserted in the blood vessel into which a sheath (a small tube) will be inserted. The cardiologist will place the various catheters through this small tube during the procedure.
After insertion into the blood vessel, the catheter is carefully guided toward the heart. The television screen connected to the x-ray camera allows the doctor and staff to follow the progress of the catheter.
What Does It Show?
Once the catheter is in place inside the heart, the cardiologist is able to assess the function of the heart in several ways. The pressures inside the heart can be measured and x-ray dye injected into the heart chambers and coronary arteries.
Pressure readings taken inside the heart allows the doctor to assess the heart’s pumping function and estimate the severity of valve defects. Monitor screens in the cath lab display the pressure readings. These readings may also be recorded on special tracing paper.
Pictures taken of the blood flow through the coronary arteries are called coronary angiograms. Specially shaped catheters are placed into the heart, one after the other. The special shape of these catheters allows the x-ray dye to be directed toward the openings of the coronary arteries. Once in position, the x-ray dye is injected through the catheter into each coronary artery. The x-ray camera takes pictures. These pictures reveal blockages in the coronary arteries and show their impact upon blood flow.
When the doctor takes pictures of the heart’s main pumping chamber (the left ventricle), the procedure is called a left ventriculogram. A special catheter is maneuvered into the left ventricle. Then, x-ray dye is injected under pressure into the left ventricle. A series of pictures are taken to view the left ventricle during its pumping action.
When a leaky valve or a hole in the heart is present, the x-ray dye inside the heart shows abnormal flow of dye going in the "wrong" direction.
During the heart catheterization, the x-ray camera is tilted at various angles to obtain the best views of the coronary arteries and heart chambers.
What Is It Like To Have A Heart Catheterization?
Although you will be mildly sedated, you will be awake during the procedure. Cardiac catheterization usually is not painful; however, you will experience some unusual sensations.
You will feel a stinging or burning sensation when the groin area is anesthetized. Some pressure may also be felt in the area when the sheath is placed. You will not feel the catheters moving through the blood vessels and into your heart. When x-ray dye is

51
injected into the coronary arteries, you may feel some tingling or discomfort; however, this sensation subsides in seconds. The injection of dye into the left ventricle causes a warm sensation ("hot flash") over your body, lasting for 10-20 seconds.
A complete cardiac catheterization study generally lasts about one hour. Lying still on the x-ray table for this period of time may be uncomfortable. The staff will do their best to help you stay comfortable throughout the procedure.
After Cardiac Catheterization
Once the procedure is completed and the catheters are removed, firm pressure is applied over the insertion site for 10-20 minutes. This is to stop the bleeding from the arterial site.
You will be taken back to your room or the recovery area. A pressure device will be applied to the insertion site. For a period of time, usually four to six hours, you will lie flat in bed, to allow the puncture in the artery to form a seal. During that time, do not bend or lift the extremity where the catheters were inserted. To relieve stiffness, you may move your foot or wiggle your toes. You may bend the other leg at the knee to relieve stress on your back.
The nurse will check your pulse and blood pressure frequently, and will also keep checking the site where the catheters were inserted. If you feel sudden pain at the site, or if you notice a warm, sticky sensation of fluid, notify the nurse immediately.
You will be able to eat shortly after returning to your room. You will be given fluid through an I.V. or asked to drink plenty of liquids to "flush" the x-ray dye out of the body.
The doctor who performed the study may be able to discuss with you some of the results soon after the test. A complete, detailed analysis of all the findings will take more time.
As You Recover From Heart Catherization
Limit your activity during the first 24 hours after the procedure. Once you return home, you can move about, but do not strain or lift heavy objects for a few days.
If you notice new blood on the dressing, place your fingers over the site and press firmly for about 20 minutes. If bleeding continues, call your doctor or go to the nearest emergency room while continuing to apply pressure.
Leave the dressing over the insertion site in place until the day after the procedure. You will be instructed on how to take it off and when it’s OK to take a shower.
A bruise or swelling under the skin at the insertion site is common. These generally disappear within three to four weeks.

52
Call the doctor if the insertion site becomes painful or warm to the touch, or if it shows signs of infection.
The doctor will tell you when you can return to your normal activities, and whether there are any specific restrictions.
The doctor may prescribe medications after the procedure or adjust the medications you were taking before the heart cath. Be sure to follow his instructions.
Is Catheterization Safe?
Cardiac catheterization is an "invasive" procedure that requires the insertion of a catheter into the body. Therefore, the procedure has a small level of risk. Thanks to modern equipment and techniques, heart catheterization is considered a relatively safe procedure.
Most complications associated with cardiac catheterization are minor and of no long-term consequence. These include nausea and vomiting, allergic skin rash (hives), and heartbeat irregularity. Some patients may bleed at the insertion site. If blood collects under the skin, swelling and/or a "bruise" may develop.
Less frequently, catheterization may be associated with more serious complications. These include damage to blood vessels, formation of blood clots, infection, abnormal heart rhythms, a heart attack, or a stroke. Fatalities are extremely rare.
Most patients who undergo catheterization do not experience complications. Nonetheless, you should be aware of the risks of the procedure. Be sure to ask you doctor about any special risks that apply to you.
Benefits
In most cases, the benefits of cardiac catheterization far outweigh the risks. Catheterization provides important information about the heart’s pumping function and the condition of the coronary arteries and heart valves. This information often cannot be obtained by any other means. It allows the doctor to make an accurate diagnosis and begin treatment before irreversible damage to the heart occurs.
http://www.cardioconsult.com/DiagnosticTechniques/CardiacCatheterization.asp

53
Many individuals with cardiac disease carry internal devices which help their hearts to work properly. The Recreational Therapist should be aware of any such devices and take appropriate precautions to see that the client is not overworked and no action istaken that could impair or compromise the function of any implanted device.
Implantable cardioverter defibrillators (ICDs) An implantable cardioverter defibrillator (ICD) is a device that is implanted in people’s chests that can be programmed to monitor for and, if necessary, correct episodes of an abnormal heart rhythm (arrhythmia). If the heartbeat gets too fast (ventricular tachycardia), the ICD will stimulate the heart to restore a normal rhythm (anti-tachycardia pacing). In potentially fatal cases where the heart no longer beats but merely “quivers” or fibrillates (ventricular fibrillation) the ICD can deliver an electric shock (defibrillation) to “reset” the heartbeat.

54
The ICD has an electronic memory that a physician can retrieve during follow up visits or even by telephone (transtelephonic monitoring). The memory stores information such as the following:
Number and types of treatments given Success of each treatment Status of the heart during the most recent episodes State of the ICD’s batteries and programmed settings
An ICD is similar in many respects to pacemaker, which is another type of device that corrects an abnormal heart rhythm. However, pacemakers are usually chosen to correct a heart rhythm that is too slow (bradycardia), whereas ICDs are commonly used to detect and correct a heart rhythm that is too fast (ventricular tachycardia). Pacemakers cannot deliver the high energy electrical shock required for defibrillation. However, ICDs can be programmed to function as a pacemaker and combination devices are being developed to detect and treat multiple heart rhythm problems in the same patient.
For more information on ICDs, see: Implantable Defibrillator (ICD).
PacemakersAlthough the heart has its own natural pacemaker that sets its rhythm, the term “pacemaker” most commonly refers to an artificial electronic device that is implanted in the chest to regulate the heart’s rhythm. Generally, pacemakers correct an abnormally slow heartbeat by sending electrical impulses to one or more chambers of the heart. These signals make the heart contract in a more regular rhythm than the chamber would otherwise.
Pacemakers are implanted into the patient’s chest during a minor surgical procedure. A short stay in the hospital may be required, and some patients may need to take medications afterward that help the heart maintain a normal rhythm (antiarrhythmics).
55
Once the pacemaker is in place, it runs on batteries that last for about 5 to 10 years. Pacemaker batteries will not run out unexpectedly. Physicians can detect when the battery is running low during a routine office visit.
Nearly 200,000 pacemakers are implanted annually in the United States. People with pacemakers enjoy significant improvement in their quality of life. However, caution is advised in certain situations. While the risk of a life-threatening problem is small, people with pacemakers are encouraged to:
Avoid walking through a metal detector, or spending any length of time near store security gates or entrances.
Avoid magnetic resonance imaging (MRI) machines and tests.
Hold cell phones at least 6 inches from the pacemaker at all times, even if the phone is turned off. Use and store the cell phone on the side of the body opposite the location of the pacemaker.
Avoid any areas or equipment that generate strong electrical or magnetic fields, such as slot machines, remote-control toys, amusement park rides and attractions, power plants, junk yards that use large magnets, stereo speakers (when held close to the pacemaker), or poorly shielded car engines.
Avoid working on car engines while they are running.
Lifestyle considerations with pacemakers Following the insertion procedure, patients will be given a card providing basic information on the implanted pacemaker as well as emergency instructions. This card should be kept with them at all times. In addition, patients should memorize their pacemaker make and model number. Although mechanical problems are rare, this information will prepare patients in the event of a pacemaker recall by a manufacturer. Patients may want to wear a medical alert ID bracelet or necklace that provides information about their heart rhythms and pacemaker, as well as an access number for their medical files.
According to a report published in The Journal of the American Medical Association (August 15, 2001), recalls and safety alerts for implanted heart devices were on the rise between January 1990 and December 2000. In that 10-year period, 52 Food and Drug Administration (FDA) advisories were issued, affecting more than 400,000 pacemakers and 114,000 implantable cardioverter defibrillators (ICDs). While more pacemakers were affected, investigators found that ICDs had a higher recall rates. In that same time period, the number of people in the United States with implanted heart devices increased 49 percent. Researchers speculated that increased vigilance on the part of the FDA and manufacturers might account for the increase. Changing technologies within this field may also have played a role. An advisory is not the same as a recall. However, advisories may lead to device checks and/or future recalls. The increasing frequency of advisories underscores the need to patients to memorize their pacemaker make and model number

56
and to carry their device information card. That way, patients will be able to determine quickly if an advisory concerns their implanted device.
Patients should know the rate at which their pacemakers are set and then take their resting pulse rate for one full minute each day, contacting their physician if their pulse is five beats or more below the programmed rate. A faster rate is not a concern unless it is more than 100 beats per minute at rest. A program of daily moderate exercise is also recommended. Patients who want to exercise more strenuously will need to speak with their physician about designing a healthy exercise program. All patients should consult their physicians before starting to exercise.
Starting about two to three months after implantation, patients will have regularly scheduled pacemaker checks with their physicians every six to 12 months, depending on the model that was implanted. These visits may include a medical history update, blood pressure check, x-ray, electrocardiogram (EKG) and/or a stress test. Both the programming and the battery strength of the device will be checked by a radio transmitter that is used to communicate with the device.
Lifestyle considerations for Mechanical ValvesPeople with mechanical heart valves will need to see their physician periodically for follow-up visits. Part of these follow-up visits will usually include a painless echocardiogram, which can reveal any malfunction or leaking of the valve.
People with mechanical heart valves face an increased risk of developing a potentially dangerous inflammation called bacterial endocarditis. This risk is increased when bacteria enter the bloodstream, such as during a dental, medical or surgical procedure. Once in the blood stream, the bacterial can infect the tissue surrounding the valve, or the valve itself. Therefore, people with mechanical heart valves are generally advised by their physicians to take antibiotics before any of these procedures to minimize their risk of bacterial endocarditis.
All people with mechanical heart valves will also need to take medications called anticoagulants for the rest of their lives. These medications help prevent the body’s

57
natural response of forming blood clots around a foreign object, such as a mechanical heart valve. Anticoagulants reduce the risk of blood clot formation, thus reducing the patient’s risk of valve malfunction, stroke and other potentially dangerous complications.
Patients taking anticoagulants may need to undergo regular blood tests to monitor their medication dosage. These tests usually require the patient to visit a hospital, physician’s office or laboratory on a monthly, bimonthly or weekly basis. Since some prescription and over-the-counter medications can affect coagulation, patients should inform their physicians about any such products they are taking.
It is also wise for patients carry a form of identification (e.g., card, necklace, bracelet) stating that they have a mechanical heart valve, in case of emergency. www.heartcenteronline.com
Precautions: Drugs and MedicationsTR: Ensure that TR intervention is consistent with the lifestyle considerations involved with any medication a patient might be
taking
Lifestyle considerations with ACE inhibitors When first taking ACE inhibitors, patients should avoid operating heavy machinery (e.g., driving) until they know how the medication will affect them. Many patients taking ACE inhibitors for high blood pressure (hypertension) will be on the medication for the rest of their lives, provided no serious side effects occur. Patients should remember that ACE inhibitors control high blood pressure but do not cure it. Even though they may not have any symptoms (which is very common among those with high blood pressure), patients should continue to take their medication exactly as directed and to keep all scheduled follow-up appointments with their physician. Patients should take and record their blood pressure readings regularly if ordered to do so, reporting anything unusual to their physician.
Patients on ACE inhibitors should inform their physician if they become ill, especially with severe vomiting or diarrhea. These conditions can cause the body to lose too much water and potassium, leading to low blood pressure (hypotension).
Patients are more likely to have side effects from ACE inhibitors if they spend too much time in the heat. Therefore, patients should be certain to drink enough liquids during exercise or in hot weather and to follow their physician’s orders about exercise, activity levels and diet.
Lifestyle considerations with antiarrhythmics When first taking antiarrhythmics, patients should avoid operating heavy machinery (e.g., driving) until they know how the medication will affect them. Most patients on medication to treat arrhythmias will be taking it for the rest of their lives, provided no serious side effects occur. Patients should remember that antiarrhythmics control

58
abnormal heart rates, but do not cure them. Even if all their symptoms are relieved, patients should continue to take their medication exactly as directed and to keep all scheduled follow-up appointments with their physicians. In addition to taking medication, patients may be advised to make lifestyle modifications, especially concerning diet, exercise and stress management.
Lifestyle considerations with ARBs A-II receptor blockers (ARBs) are only one part of a treatment plan for high blood pressure, heart failure or other conditions. That plan usually includes a number of lifestyle changes including weight loss, eating a heart healthy diet, regular exercise and more. ARBs reduce the symptoms, but do not cure the underlying condition. Therefore, many patients taking ARBs will be on the medication for the rest of their lives, provided no serious side effects occur.
When first taking ARBs, patients may be advised to avoid driving or operating heavy machinery until they know how the medication will affect them. Often, the symptoms that led the patients to seek medical attention will stop once ARBs are introduced. Patients should still continue to take their medication exactly as directed and to keep all scheduled follow-up appointments with their physician.
Patients are more likely to have side effects from ARBs or other antihypertensives if they spend too much time in the heat. Therefore, patients should be certain to drink enough liquids during exercise or in hot weather. Patients may also be directed to take their own blood pressure readings regularly, reporting anything unusual to their physicians.
Patients taking ARBs should inform their physician if they become ill from any cause, especially if severe diarrhea or vomiting occurs. These conditions can cause the body to lose too much water and potassium, leading to low blood pressure (hypotension).
Patients should not stop taking ARBs abruptly unless advised by their physician. Doing so might lead to medical complications.
Lifestyle considerations with anticoagulants When first taking anticoagulants, patients should avoid operating heavy machinery (e.g., driving) until they know how the medication may affect them. Patients should remember that anticoagulants can control many conditions, but do not cure them. Patients should continue to take their medication exactly as directed and to keep all scheduled follow-up appointments with their physician.
Patients taking anticoagulants need to undergo regular blood tests to monitor their medication dosage. These tests usually require the patient to visit a hospital, physician’s office or laboratory on a monthly, bimonthly, weekly or biweekly basis. Studies are underway to test the feasibility of at-home coagulation testing.
Patients on anticoagulants need to avoid cutting themselves, including when shaving, brushing their teeth (a soft toothbrush is recommended) or flossing, because their blood will not clot as effectively. Similarly, patients are advised against playing contact sports
59
(e.g., football) or any other activity where there is risk of injury (e.g., skiing or motorcycle riding).
Vitamin K plays an integral role in blood clot formation and inhibits the action of anticoagulant medications. Dosages of these medications will therefore depend on the levels of vitamin K in the patient’s diet. Patients should not make any changes to their diet that would greatly increase or decrease their levels of vitamin K intake without consulting with their physician, who may need to alter the dosage of the anticoagulants. Vitamin K is most prevalent in green leafy vegetables (including spinach, broccoli, cabbage, kale and lettuce) and some vegetable oils.
Care should also be exercised in patients with Factor V (five) Leiden. This is a variation in a gene that affects the clotting process, increasing coagulation. Factor V Leiden is the most common inherited blood disorder in the United States. It is present in four to six percent of Caucasians; two percent of Hispanic Americans; a little over one percent of African-Americans and Native Americans; and about one-half of one percent of Asian Americans. Treatment is typically unwarranted unless there is evidence of a blood clot, in which case warfarin or other anticoagulants are prescribed. Depending on the situation, anticoagulants may be recommended to help afford advance protection against the development of blood clots. For example, women with a Factor V Leiden mutation may be advised to take anticoagulants during pregnancy and in the postpartum period.
Lifestyle considerations with antibiotics Vaginal yeast infections are a common side effect of some antibiotics because they can cause an overgrowth of normal body organisms such as yeast. This can be avoided by daily consumption of “live culture” yogurt (available at any grocery store) while undergoing antibiotic therapy.
Symptoms usually lessen after two to three days after starting oral antibiotic treatment. However, patients need to continue taking the remainder of their medication. Unless all of the bacteria are completely killed, the bacteria can change into another form and produce symptoms again. Furthermore, the change (mutation) of the bacteria increases the risk of being infected by bacteria that are more difficult to kill with antibiotics. This is known as antibiotic resistance, and it is a worldwide healthcare concern. Antibiotic-resistant strains of bacteria already exist and new ones are created daily. Patients can help to slow the creation of resistant strains by:
Finishing all antibiotic medications prescribed, even if symptoms stop. This includes not missing or skipping doses. Blood levels of the antibiotic must stay within a high enough range to kill bacteria.
Avoiding some "antibacterial" soaps and cleansers. Choose products with bleach, alcohol, ammonia or hydrogen peroxide, which kill bacteria without promoting resistance.
Immunization. Many bacterial infections can be prevented through immunization. Patients should discuss the options with their physicians. Specifically, patients with

60
chronic conditions and those over the age of 60 should receive the pneumococcal vaccine.
TR Implications
Activities that assist patients in reducing stress and other factors (such as obesity, smoking, lack of exercise, and poor nutrition) are necessary components of the rehabilitation process. Efforts designed to assist patients in developing lifestyle changes that reduce the likelihood of further cardiac problems are often included in patient education programs.
The American Heart Association identifies three outcomes from a cardiovascular rehabilitation program, including improved functional capacity, reduced symptoms of heart disease, and a sense of well-being and optimism about the future. These outcomes are brought about through a program of counseling, exercise, lifestyle changes, vocational guidance, and emotional support. The TR specialist can be instrumental in meeting these goals. Programs such as stress reduction, use of leisure activities to incorporate more physical activity gradually into the patient’s life, and lifestyle education all aim at identifying and removing risk factors such as poor nutrition, smoking, and lack of physical activity.
The Benefits Of Recreation
Although I have tried to classify the benefits of recreation into its health, social, economical and environmental aspects, they are interdependent and integration is necessary in many cases for the full value to be realized!
For individual health and well-being:Exercise reduces stress and relieves tension. Stress is a contributing
factor in a wide variety of emotional and behavioral difficulties including anxiety and depression (Greenberg & Valletutti, 1980). Stress is also a contributing factor in most physical illnesses including heart attacks, diabetes, angina, bronchitis, arthritis, etc. (Pelletier, 1977). Exercise reduces blood pressure and heart rate, and reduces other bronchitis, arthritis, etc. (Pelletier, 1977). Exercise reduces blood pressure and heart rate, and reduces other physiological changes set off during the alarm stage of the general adaptation syndrome. Exercising helps to give more physical strength to handle stressful crises. The therapeutic value of stress managementhttp://scholar.google.com/scholar?hl=en&lr=&q=cache:_6Ou6bow9ZwJ:www.lin.ca/lin/resource/html/sp0107(2).pdf+therapeutic+Recreation+for+heart+diseases

61
Glossary
ACE (angiotensin converting enzyme) inhibitors — A type of heart failure medication that works by preventing the body from creating angiotensin, a substance in the blood that causes vessels to tighten and raises blood pressure. In large-scale studies, ACE inhibitors have been proven to slow the progression of heart failure.
Advance Directive — A written document that states a person's healthcare choices and names someone to make those choices, should the person become unable to make their own decisions about medical care. The most common types of Advance Directives are a living will and a durable power of attorney for healthcare.
Anemia — A reduction in the amount of oxygen-carrying red blood cells. Anemia can have many causes, but the most common is a lack of iron in the body. Also known as iron-poor blood.
Angiography — An X-ray test used to detect diseases of the blood vessels, such as weakening of the vessel walls and the narrowing or blocking of vessels. The X-ray is taken after the vessels have been injected with a substance that allows them to be seen on film.
Angioplasty — A procedure that reopens blocked blood vessels to the heart. A physician inserts a hollow needle (catheter) into the diseased artery and pushes a small deflated balloon into the blocked section. Then the physician inflates the balloon to widen the artery.
Angiotensin II receptor blocker — A medication that blocks the action of a special chemical called angiotensin, which normally raises the heart rate and blood pressure.
Arrhythmia — An abnormal rhythm or rate of the heartbeat caused by disturbances in the movement of electrical impulses through the heart.
Atrial fibrillation — Rapid, uneven contractions in the upper heart chambers (atria), which cause the lower chambers (ventricles) to beat irregularly.
Atrium — One of the two upper chambers of the heart.
Beta blockers — Medications that reduce the heart's tendency to beat faster by blocking specific receptors ("beta receptors") on the cells that make up the heart.
Blood thinners — Medications, such as warfarin and heparin, used to prevent blood clotting. Some people with heart failure are prescribed blood thinners to reduce the risk of stroke.

62
Calcium channel blocker — A drug that prevents calcium from entering the heart's muscle cells. This causes the muscles to relax, lowering the heart rate.
Cardiac rehabilitation — A supervised program of increasing exercise, mental support and training to allow a person with a heart condition to resume normal activities.
Cardiologist — A doctor who diagnoses and treats heart problems.
Cardiomyopathy — Any weakening or deformity of the heart muscle that causes decreased pumping force. This leads to less-efficient circulation of blood through the lungs and the rest of the body.
Cardiomyoplasty — An investigational surgical treatment for heart failure that involves taking muscles from the person's back or abdomen and wrapping them around the heart. Its goal is to increase the heart's pumping power.
Caregiver — Anyone who helps a chronically ill patient cope with an illness. Caregivers can be home healthcare workers, family members or friends. They assist in many ways, from making sure patients take their medications properly to helping out with day-to-day activities.
Chronic illness — An illness or condition that develops slowly and persists for a long time. Heart failure is almost always a chronic illness.
Congenital heart disease — Any heart condition or abnormality that a person was born with.
Congestive heart failure — A common form of heart failure that results in a patient retaining excessive fluid, often leading to swelling of the legs and ankles and congestion in the lungs.
Coronary artery bypass — A procedure used to reroute the blood supply around a blocked section of a coronary artery. Surgeons remove healthy blood vessels from another part of the body, such as a leg or the chest wall. Then they surgically attach the vessels to the diseased artery to let the blood flow around the blocked section.
Coronary artery disease — A condition caused by thickening of the walls of the arteries that supply blood to the heart muscle. When these arteries become blocked, the heart is deprived of oxygen and can become damaged. Severe cases can result in heart attack.
Defibrillator — A device that delivers pacing or an electric countershock to the heart when an abnormal rhythm is detected. A surgically implantable version is called a pacemaker.
Diabetes — A condition in which the body doesn't produce the right amount of insulin, the hormone that allows cells to absorb glucose (sugar) from the bloodstream. Some
63
people with diabetes must inject themselves with insulin every day to maintain a healthy glucose level. Others are able to control the condition with pills or a special diet.
Diastolic pressure — The pressure of blood inside arteries when the heart is at rest. This is the bottom number in a blood pressure reading.
Digoxin (or digitalis) — A medication that increases the force of the heart's contractions and slows certain types of irregular heartbeats (arrhythmia).
Diuretic — A medication that promotes the formation and release of urine. It helps to reduce fluid overload in people with heart failure. Also called a water pill.
Drug interaction — A change in the effect of a drug when taken with a certain other drug or food. Its effect may increase or decrease, or a side effect may occur.
Dyspnea — Difficult or labored breathing, often caused by heart conditions.
Dysrhythmia — A disturbance in heart rhythm, sometimes used as an alternative to the term "arrhythmia."
Echocardiography — A test that obtains an image of the structure and motion of the heart using ultrasound (inaudible, high-frequency sound waves). Used to detect cardiomyopathy and other abnormalities of the heart wall, valves and large blood vessels.
Edema — An abnormal accumulation of fluid in body tissues. Edema is common in the legs, ankles and lungs of people with heart failure.
Ejection fraction — The amount of blood released during each contraction of the lower ventricle of the heart. It's usually expressed as a percentage: an ejection fraction of 60 percent means that 60 percent of the total amount of blood in the left ventricle is expelled with each heartbeat.
Electrocardiogram (EKG or ECG) — A record of the electrical activity of the heart, allowing diagnosis of abnormal heart conditions.
Endocarditis — Inflammation of the lining of the heart and the heart valves, usually due to bacterial infection.
Heart attack — Sudden death of a portion of the heart muscle caused by a sudden decrease in blood supply to that area. Also known as myocardial infarction or MI.
Heart disease, ischemic — The most prevalent form of heart disease, in which narrowed or blocked coronary arteries result in decreased blood supply.
Heart failure — The inability of the heart to keep up with its workload. When someone has this condition, their heart can't pump enough blood to the lungs and the rest of the

64
body. Heart failure is often a chronic condition that can be treated with medications, diet and other lifestyle changes, and in some cases, surgery.
Heart transplant — Surgery that replaces a damaged heart with a healthy heart taken from a donor who has been declared brain dead.
Heart valve — One of the four structures in the heart that control the flow of blood by opening and closing with each heartbeat. The valves permit the flow of blood in only one direction.
Hypertension — The medical term for abnormally high blood pressure.
Hyperthyroidism — Overactivity of the thyroid gland, leading to overproduction of thyroid hormones. It can make the body's metabolism overactive, leading to symptoms such as weight loss and rapid heart rate.
Hypotension — Abnormally low blood pressure.
Left-ventricular assist device — A mechanical pump used to aid the natural pumping action of the heart's left ventricle.
Left-ventricular heart failure — Heart failure in which the left side of the heart must work harder to pump the same amount of blood. This type of heart failure usually causes breathing difficulties.
MUGA (Multigated Acquisition) — A test in which a radioactive tracer is injected into the bloodstream and scanned as it passes through the heart. A computer then calculates the size and shape of a patient's ventricles based on the amount and distribution of radiation emitted from them.
Myocardial infarction — Sudden death of a portion of the heart muscle caused by a sudden decrease in blood supply to that area. See Heart Attack.
Myocarditis — Inflammation of the heart muscle.
Potassium — A mineral that, together with sodium and calcium, regulates the body's water balance, maintains normal heart rhythm, and is responsible for nerve impulse conduction and muscle contraction.
Primary care doctor — A general internist or family physician who provides patients with routine preventive healthcare and is their first contact when medical problems arise.
Pulmonary edema — Fluid in lung tissues, often caused by congestive heart failure.
Right-ventricular heart failure — Heart failure caused by damage to the right-side chambers of the heart, leading to decreased blood flow, and swelling in the hands, legs

65
and abdomen.
Side effect — Any reaction that results from a medication or therapy. Heart failure medications can cause side effects such as headaches, nausea, dizziness, kidney complications and low blood pressure.
Sodium — A mineral that, together with potassium and calcium, regulates the body's water balance, maintains normal heart rhythm, and is responsible for nerve impulse conduction and muscle contraction. Excessive intake of sodium from food contributes to high blood pressure in some people. In people who already have high blood pressure, too much sodium may increase the risk of stroke, heart disease and kidney damage.
Stress test — An exercise test that examines how well the heart works. Patients are asked to walk on a treadmill to increase their heart rate. During the test, a doctor monitors electrocardiogram (ECG or EKG) readings from the heart to check for any heart rhythm irregularities .
Systolic pressure — The pressure of blood inside arteries when the heart contracts. This is the top number in a blood pressure reading.
Vaccine — Weakened or dead germs, given by injection, that protect against infectious disease. People with heart failure should receive a yearly influenza vaccine and a one-time pneumococcal vaccine (to guard against pneumonia).
Valve replacement — Surgery to replace a defective or diseased heart valve.
Vasoconstriction — A narrowing of a blood vessel, causing decreased blood flow to a part of the body.
Vasodilator — A medication that causes widening or relaxation of blood vessel walls. Examples include ACE inhibitors, angiotensin II receptor blockers, beta blockers, calcium channel blockers, natriuretic peptides and nitrates.
Ventricle — One of the two lower chambers of the heart that receive blood from the atria (upper chambers). The right ventricle pumps blood to the lungs and the left ventricle pumps blood to the rest of the body.
Some Great ResourcesGeneral Cardiac InformationAmerican Heart Associationhttp://www.americanheart.org/presenter.jhtml?identifier=1477Women’s Health Association: Cardiologyhttp://www.healthsquare.com/heartdisease.htm

66
Cardiac Disease Onlinehttp://www.cardiac-disease.net/Medical College of Wisconsinhttp://healthlink.mcw.edu/heart-diseaseMedline Plus Medical Encyclopediahttp://www.nlm.nih.gov/medlineplus/ency/article/000147.htmHeart Pointhttp://www.heartpoint.com/TR ImplicationsPhysical Medicine and Rehabilitationhttp://www.theuniversityhospital.com/physservdirectory/html/rehab.htmWQED Multimedia City Guidehttp://www.wqed.org/mag/cityguide/healthguide.shtmlRehabilitation Service Programshttp://www.nsmc.partners.org/healthsv/skrhpro.html
What is Stroke?http://www.strokeassociation.orgStroke is a type of cardiovascular disease. It affects the arteries leading to and within the brain. A stroke occurs when a blood vessel that carries oxygen and nutrients to the brain is either blocked by a clot or bursts. When that happens, part of the brain cannot get the blood (and oxygen) it needs, so it starts to die.
What Are the Types of Stroke?If we consider an isolated blood vessel, blood flow to the brain tissue can be hampered in two ways:1. the vessel clogs within (ischemic stroke)2. the vessel ruptures, causing blood to leak into the brain (hemorrhagic stroke)
IschemicIschemic stroke accounts for about 83 percent of all cases.
Ischemic strokes occur as a result of an obstruction within a blood vessel supplying blood to the brain. The underlying condition for this type of obstruction is the development of fatty deposits lining the vessel walls. This condition is called atherosclerosis. These fatty deposits can cause two types of obstruction:

67
Cerebral thrombosis refers to a thrombus (blood clot) that develops at the clogged part of the vessel.
Cerebral embolism refers generally to a blood clot that forms at another location in the circulatory system, usually the heart and large arteries of the upper chest and neck. A portion of the blood clot breaks loose, enters the bloodstream and travels through the brain's blood vessels until it reaches vessels too small to let it pass. A second important cause of embolism is an irregular heartbeat, known as atrial fibrillation. It creates conditions where clots can form in the heart, dislodge and travel to the brain.
HemorrhagicHemorrhagic stroke accounts for about 17 percent of stroke cases.It results from a weakened vessel that ruptures and bleeds into the surrounding brain. The blood accumulates and compresses the surrounding brain tissue. The two types of hemorrhagic strokes are intracerebral hemorrhage or subarachnoid hemorrhage.
Hemorrhagic stroke occurs when a weakened blood vessel ruptures. Two types of weakened blood vessels usually cause hemorrhagic stroke: aneurysms and arteriovenous malformations (AVMs).
An aneurysm is a ballooning of a weakened region of a blood vessel. If left untreated, the aneurysm continues to weaken until it ruptures and bleeds into the brain. Download more information on aneurysm.
An arteriovenous malformation (AVM) is a cluster of abnormally formed blood vessels. Any one of these vessels can rupture, also causing bleeding into the brain. Download more information on AVM.
Transient ischemic attacksAlso called TIAs, transient ischemic attacks are minor or warning strokes. In a TIA, conditions indicative of an ischemic stroke are present and the typical stroke warning signs develop. However, the obstruction (blood clot) occurs for a short time and tends to resolve itself through normal mechanisms.
Even though the symptoms disappear after a short time, TIAs are strong indicators of a possible major stroke. Steps should be taken immediately to prevent a stroke.
Statistics!According to the National Institute of Neurological Disorders and Stroke (NINDS), about 700,000 people have a stroke each year--500,000 first strokes and 200,000 recurrent strokes. Stroke is the leading cause of long-term disability and the third-leading cause of death for Americans after heart disease and cancer.

68
Learn To Recognize A Stroke
Stroke is a medical emergency. Know these warning signs of stroke and teach them to others. Every second counts:
Sudden numbness or weakness of the face, arm or leg, especially on one side of the body
Sudden confusion, trouble speaking or understanding Sudden trouble seeing in one or both eyes Sudden trouble walking, dizziness, loss of balance or coordination Sudden, severe headache with no known cause
Call 9-1-1 immediately if you experience symptoms!Time lost is brain lost!
Diagnosis
TestsWhen someone has shown symptoms of a stroke or a TIA (transient ischemic attack), a doctor will gather information and make a diagnosis. He or she will review the events that have occurred and will:
get a medical history do a physical and neurological examination have certain laboratory (blood) tests done get a CT scan of the patient study the results of other diagnostic tests that might be needed

69
What are the types of diagnostic tests?Diagnostic tests examine how the brain looks, works and gets its blood supply. They can outline the injured brain area. Most of them are safe and painless.
Diagnostic tests fall into three categories.
Imaging tests give a picture of the brain similar to X-rays. Electrical tests record the electrical impulses of the brain. Blood flow tests show any problem that may cause changes in blood flow to the
brain.
What are some common imaging tests?
CT scan (Computed Tomography) or CAT scan is a key imaging test. It uses radiation to create a picture of the brain. It's usually one of the first tests given to patients suspected of stroke. CT test results give valuable information about the cause of stroke and the location and extent of brain injury.
MRI (Magnetic Resonance Imaging) uses a large magnetic field to produce an image of the brain. Like the CT scan, it shows the location and extent of brain injury. The image produced by MRI is sharper and more detailed than a CT scan so it's often used to diagnose small, deep injuries.
What is an electrical activity test?Two basic tests, EEG and Evoked Response, show the brain's electrical activity.
In an EEG (electroencephalogram), small metal discs (electrodes) are placed on a person's scalp to pick up electrical impulses. These electrical signals are printed out as brain waves.
An Evoked Response test measures how the brain handles different sensory information. Electrodes record electrical impulses related to hearing, body sensation or vision.
What is a blood flow test?
Several blood flow tests exist; most use ultrasound technology. A probe is placed over the suspect artery -- especially arteries in the neck or at the base of the skull -- and the amount of blood flow is determined.
Examples of blood flow tests are: B-mode imaging, Doppler testing and duplex scanning. These tests give detailed information about the condition of arteries.
70
Another blood flow test is a medical procedure called angiography (arteriography or arteriogram). In this, special dyes are injected into the blood vessels and an X-ray is taken.
Angiography gives a picture of the blood flow through the vessels. This allows the size and location of blockages to be evaluated. This test can be especially valuable in diagnosing aneurysms and malformed blood vessels and providing information before surgery.
How can I learn more?
Talk to your doctor, nurse or healthcare professional or call the American Stroke Association.Just dial 1-888-4-STROKE (478-7653).
If you've had a stroke or have heart disease, members of your family also may be at higher risk. It's very important for them to make changes now to lower their risk.
Reducing Risk
Stroke Risk Factors
Risk factors are traits and lifestyle habits that increase the risk of disease. Extensive clinical and statistical studies have identified several factors that increase the risk of stroke. Most of them can be modified, treated or controlled. Some can’t.
The more risk factors you have, the higher your chances of having a stroke. The best way to prevent a stroke is to reduce your stroke risk factors. A healthcare provider can help you change factors that result from lifestyle or environment.
What risk factors for stroke can be controlled or treated?
High blood pressure — High blood pressure (140/90 mm Hg or higher) is the most important risk factor for stroke. It usually has no specific symptoms and no early warning signs. That’s why everybody should have their blood pressure checked regularly.
Tobacco use — Cigarette smoking is a major, preventable risk factor for stroke. The nicotine and carbon monoxide in tobacco smoke reduce the amount of oxygen in your blood. They also damage the walls of blood vessels, making clots more likely to form. Using some kinds of birth control pills combined with smoking cigarettes greatly increases stroke risk. If you smoke, get help to quit NOW!
Diabetes mellitus — Diabetes is defined as a fasting plasma glucose (blood sugar) of 126 mg/dL or more measured on two occasions. While diabetes is treatable, having it still increases a person's risk of stroke. Many people with diabetes also have high blood pressure, high blood cholesterol and are
71
overweight. This increases their risk even more. If you have diabetes, work closely with your doctor to manage it.
Carotid or other artery disease — The carotid arteries in your neck supply blood to your brain. A carotid artery narrowed by fatty deposits from atherosclerosis (plaque buildups in artery walls) may become blocked by a blood clot. Carotid artery disease is also called carotid artery stenosis.
People with peripheral artery disease have a higher risk of carotid artery disease, which raises their risk of stroke. Peripheral artery disease is the narrowing of blood vessels carrying blood to leg and arm muscles. It's caused by fatty buildups of plaque in artery walls.
Atrial fibrillation — This heart rhythm disorder raises the risk for stroke. The heart's upper chambers quiver instead of beating effectively, which can let the blood pool and clot. If a clot breaks off, enters the bloodstream and lodges in an artery leading to the brain, a stroke results.
Other heart disease — People with coronary heart disease or heart failure have a higher risk of stroke than those with hearts that work normally. Dilated cardiomyopathy (an enlarged heart), heart valve disease and some types of congenital heart defects also raise the risk of stroke.
Transient ischemic attacks (TIAs) — TIAs are "warning strokes" that produce stroke-like symptoms but no lasting damage. Recognizing and treating TIAs can reduce your risk of a major stroke. It's very important to recognize the warning signs of a TIA or stroke. Call 9-1-1 to get medical help immediately if they occur.
Certain blood disorders — A high red blood cell count thickens the blood and makes clots more likely. This raises the risk of stroke. Doctors may treat this problem by removing blood cells or prescribing "blood thinners."
Sickle cell disease (also called sickle cell anemia) is a genetic disorder that mainly affects African Americans. "Sickled" red blood cells are less able to carry oxygen to the body's tissues and organs. They also tend to stick to blood vessel walls, which can block arteries to the brain and cause a stroke.
High blood cholesterol — A high level of total cholesterol in the blood (240 mg/dL or higher) is a major risk factor for heart disease, which raises your risk of stroke. Recent studies show that high levels of LDL ("bad") cholesterol (greater than 100 mg/dL) and triglycerides (blood fats, 150 mg/dL or higher) increase the risk of stroke in people with previous coronary heart disease, ischemic stroke or transient ischemic attack (TIA). Low levels (less than 40 mg/dL for men; less than 50 mg/dL for women) of HDL ("good") cholesterol also may raise stroke risk.
Physical inactivity and obesity — Being inactive, obese or both can increase your risk of high blood pressure, high blood cholesterol, diabetes, heart disease and stroke. So go on a brisk walk, take the stairs, and do whatever you can to make your life more active. Try to get a total of at least 30 minutes of activity on most or all days.
Excessive alcohol — Drinking an average of more than one alcoholic drink a day for women or more than two drinks a day for men can raise blood pressure and may increase risk for stroke.
72
Some illegal drugs — Intravenous drug abuse carries a high risk of stroke. Cocaine use has been linked to strokes and heart attacks. Some have been fatal even in first-time users.
What are the risk factors for stroke you can't change?
Increasing age — People of all ages, including children, have strokes. But the older you are, the greater your isk for stroke.
Sex (gender) — Stroke is more common in men than in women. In most age groups, more men than women will have a stroke in a given year. However, women account for more than half of all stroke deaths. Women who are pregnant have a higher stroke risk. So do women taking birth control pills who also smoke or have high blood pressure or other risk factors.
Heredity (family history) and race — Your stroke risk is greater if a parent, grandparent, sister or brother has had a stroke. African Americans have a much higher risk of death from a stroke than Caucasians do. This is partly because blacks have higher risks of high blood pressure, diabetes and obesity.
Prior stroke or heart attack — Someone who has had a stroke is at much higher risk of having another one. If you've had a heart attack, you're at higher risk of having a stroke, too.
For stroke information, call the American Stroke Association at 1-888-4-STROKE.
How Cardiovascular & Stroke Risks Relate
Excerpted from "When Risk Factors Unite," appearing in Stroke Connection Magazine January/February 2005.
Several types of heart disease are risk factors for stroke. Likewise, stroke is a risk factor for coronary heart disease. Both coronary heart disease and stroke share many of the same risk factors such as high LDL (“bad”) cholesterol levels, low HDL (“good”) cholesterol levels, high blood pressure, smoking, diabetes, physical inactivity, and being overweight or obese.
Individuals with coronary heart disease, angina, or who have had a heart attack due to atherosclerosis, have more than twice the risk of stroke than those who haven’t. If you have
atherosclerosis in the coronary arteries you are very likely to have atherosclerosis in other parts of your body.
Hard ArteriesAtherosclerosis is often referred to as "hardening of the arteries." The word comes from the Greek words athero (meaning gruel or paste) and sclerosis (hardness). more

73
Quivering HeartIn atrial fibrillation, the upper chambers of the heart (the atria) quiver instead of beating effectively to move blood into the ventricle. more
Problems at the PumpCongestive heart failure (CHF) can also increase stroke risk. CHF is a condition in which the heart cannot pump out all the blood that returns to it. more
Converging Risk FactorsCommon risk factors for coronary heart disease and stroke that can be controlled or treated include high LDL cholesterol levels, low HDL cholesterol levels, high blood pressure, smoking, diabetes, physical inactivity, and being overweight or obese. more
What You Can Do
Excerpted from the Stroke Connection Magazine January/February 2005 article "When Risk Factors Unite"
Although heart disease and stroke account for the vast majority of deaths each year in America, you can do things to lessen your risk:
Eat a healthy diet.
Healthy food habits can help you reduce three risk factors for heart attack and stroke — high blood cholesterol, high blood pressure and excess body weight. The American Heart Association Eating Plan for Healthy Americans outlines a healthy diet. It’s based on these dietary guidelines, which are easier to follow than you may think:
Eat five or more servings per day of fruits and vegetables. Eat six or more servings per day of grain products, including whole grains. Eat fish at least twice a week, particularly fatty fish, such as mackerel, lake trout,
herring, sardines, albacoretuna and salmon.
Include fat-free and low-fat milk products, legumes (beans), skinless poultry and lean meats.
Choose fats and oils with 2 grams or less of saturated fat per serving (1 tablespoon). Examples are liquid and tub margarines, and canola, olive, corn, saffl ower and soybean oils.
Limit your intake of foods high in calories or low in nutrition, including high-sugar foods like soft drinks and candy.
Limit foods high in saturated fat, trans fat and/or cholesterol. Examples include full-fat milk products, fatty meats, tropical oils, and partially hydrogenated vegetable oils. Egg yolks are high in cholesterol.
Eat less than 6 grams of salt per day. That’s equal to about 1 teaspoon of salt.

74
Following this eating plan will help you enjoy a healthy, nutritious diet. This may help you gain such benefits as a healthy body weight, a desirable blood cholesterol level and a normal blood pressure. Every meal doesn’t have to meet all the guidelines. Apply the guidelines to your overall eating pattern over at least several days.
These guidelines may do more than improve your heart health. They could also reduce your risk for type 2 diabetes, some forms of cancer and other health problems.
Exercise every day. Balance the number of calories you eat with those you use up each day, to maintain your best weight. Walk or do other physical activities for at least 30 minutes on most or all days. To lose weight, use up more calories than you eat every day. But before you start, check with your doctor. more
Know your blood pressure. High blood pressure may not have any symptoms. The only way you will know if your pressure is high is to have it checked. If it is high, you may be able to reduce it with diet and exercise, but if that doesn’t work, medication will likely be necessary. If you take medication, take it exactly as prescribed, not just when you feel like it. more
Stop smoking. There are many benefits to giving up tobacco. If you or a loved one need an incentive to quit, check out some of the toxic substances in cigarette smoke. more
Know the Facts
Heart disease and stroke are major health risks for all people. But African Americans are at particularly high risk. Consider this:
Blacks have almost twice the risk of first-ever strokes compared to whites. Blacks have higher death rates for stroke compared to whites.

75
The prevalence of high blood pressure in African Americans in the United States is the highest in the world.
Among non-Hispanic blacks age 20 and older, 62.9 percent of men and 77.2 percent of women are overweight or obese.
In 2001, 27.7 percent of black or African-Americans only, used any tobacco product. Heavy cigarette smoking approximately doubles a person’s risk for stroke when compared to light smokers..
Black women have higher prevalence rates of high blood pressure, obesity, physical inactivity, and diabetes than white
TR Implications
• Complementary therapies: stress management, relaxation therapy, acupressure, yoga, Ti chihttp://www.burke.org/medservices/inpatient/stroke.cfm
The rehabilitation team can also recommend support groups and leisure activities in the community.
Recreation Therapy:
The recreation therapist provides specialized and individualized adaptive techniques and equipment for the patient surviving stroke.
Treatment Programs include a community reentry program and pet visitation.
http://www.forumhealth.org/forumhealth/hillside/strokecenter_hillside.php

76