cardiology for finals fy1s poornima mohan & ghazal saadat
TRANSCRIPT

Cardiology for Finals
FY1s Poornima Mohan & Ghazal Saadat

Overview
• Scars• Acute coronary syndromes• Valvular heart disease• Infective Endocarditis• Dextrocardia• Arrhythmias

Midline sternotomy scar
What is this scar?
Which 3 procedures would cause this scar?
What else would you look for?

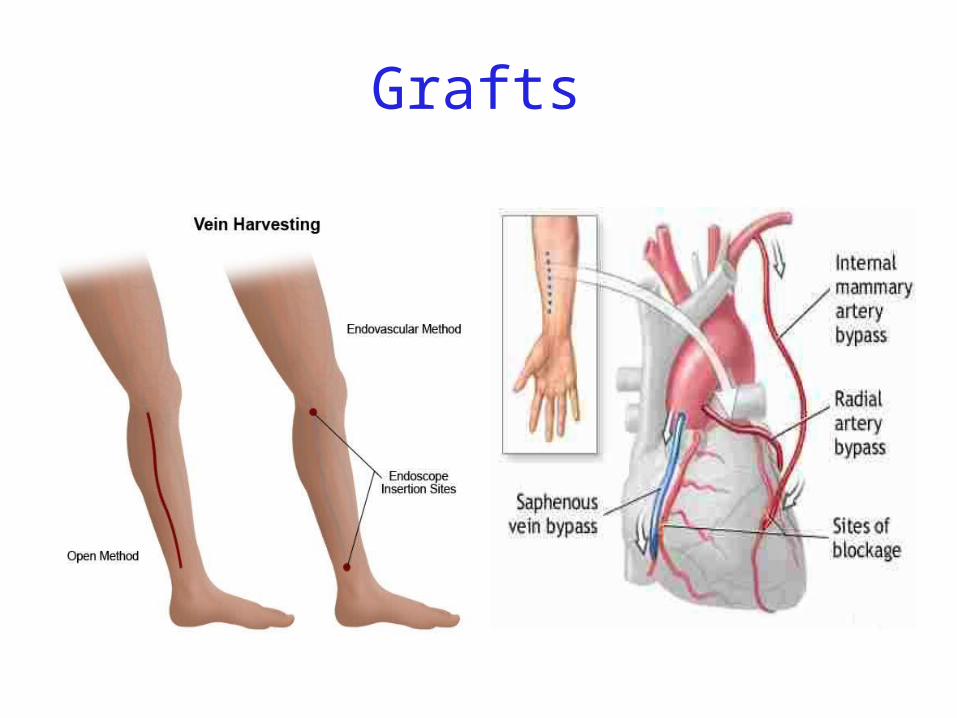
Grafts

What could this be?What are the indications?
Where else should you look?

“We have this patient with chest pain”
66 year old with a background of DM type 2, hypertension and a 40 pack yr smoking hx. Day 1 post inguinal hernia repair.
Has been having central crushing chest pain for last 15 minutes. No relief from GTN. Hot & sweaty, vomited twice.
Obs: BP- 120/60 P-75 RR- 24 Sats 98% on RA

What ECG features suggest an STEMI??
ST elevation in 2mm in 2 or more contigous limb leads ST elevation in 2 or more contigous chest leads
New onset LBBB Posterior MI
.What features suggest an to NSTEMI ???
ST depression and /or T wave inversion in 2 or more leads. Risk is assessed using the TIMI score.

What does this ECG show?
ManagementWhat would you do as an F1?1) Assess haemodynamic stability2) oxygen(?) 3) Initiate ACS protocol4) Nitrates
5) Analgesia
STEMI - Primary PCI NSTEMI – Risk assessment and PCI Unstable angina – Functional Testing +/- Angiogram
Universal Secondary Prevention and Cardiac Rehabilitation
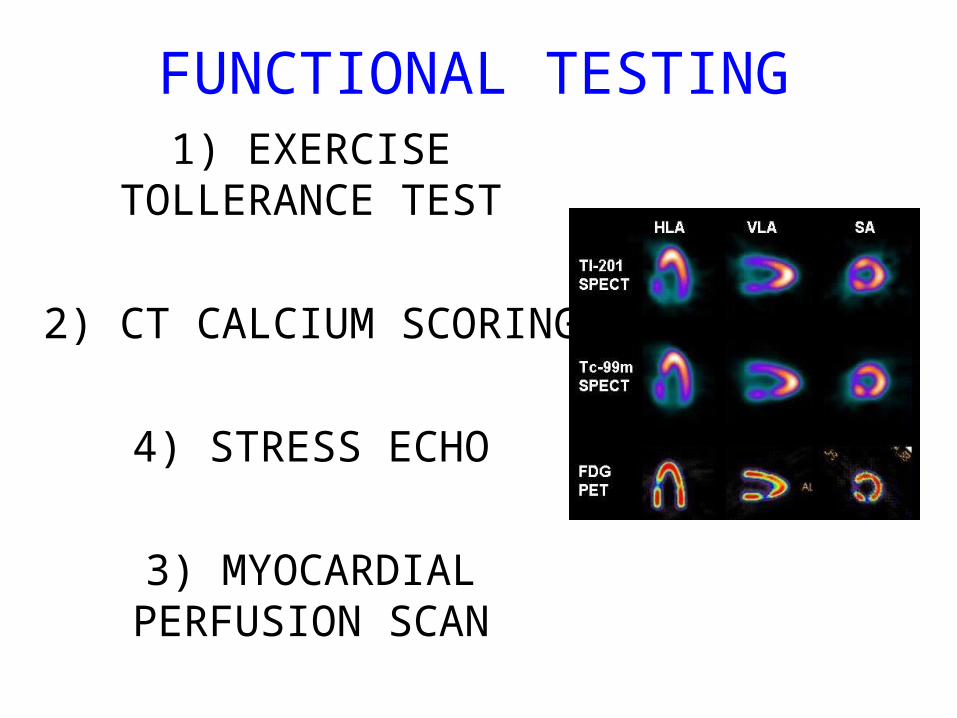
FUNCTIONAL TESTING
1) EXERCISE TOLLERANCE TEST
2) CT CALCIUM SCORING
4) STRESS ECHO
3) MYOCARDIAL PERFUSION SCAN

Valvular heart disease • Common exam question
• Can find lots of patients with valve replacement • Things to know are - Which valve - What the cause could have been - Clinical signs - Basic principles of management
• Questions about complications of surgery
“ A 72 year gentleman man presents with a history of collapse as he was rushing up a hill to catch a bus.
There was no LOC. He reports no associated weakness/numbness/tingling in the limbs, visual
disturbance, slurred speech, headache, chest pain, or palpitaions. This had never occurred before.
He has noticed that he is increasingly SOB of late whilst gardening/ doing house-work etc.
He has no previous cardiac history. He suffers from hypertension and gout.”
Scenario 1
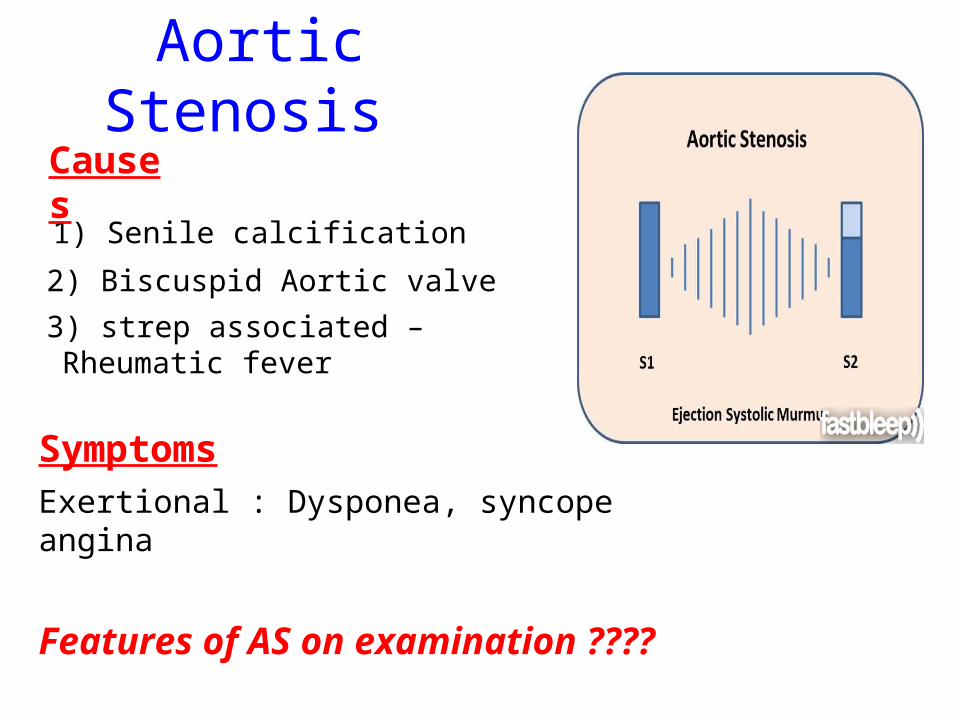
Aortic Stenosis
1) Senile calcification
2) Biscuspid Aortic valve
3) strep associated – Rheumatic fever
Symptoms Exertional : Dysponea, syncope angina
Features of AS on examination ????
Causes

Features on Examination narrow pulse pressure
slow rising pulse
LV heave
Forcefull apex beat
ESM radiating to the carotid- heard all over the precordium
Features of left ventricular dysfunction
Severe Stenosis → 1) Narrow PP 2) Quite or loss of S2
DDX for an ESM → 1) HOCM 2) VSD 3) Aortic sclerosis.
Management : TAVI vs Open AVR +/- CABG?
Exam tip : Which heart sound is metallic in an AVR??

Mitral Regurgitation
Causes
“ A 72 year old lady presents with a history of increasing SOB, orthoponea and palpitations over a few months. She has a history of Angina, Hypertension. She is found to be in Atrial fibrillation”
Valve Annulus Leaflets Papillary Muscle
ACUTE Infective Endocarditis
MyocardiaIschemia
CHRONIC Function – Chronic ischemia (post MI)
CCF (LV dilatation)
Prolapse
Connective tissue disorders
Amyloid- infiltration of the chords.

Mitral Regurgitation Clinical features
AF
small volume pulse
displace apex beat
loud PSM radiating to the axilla
bibasal crepitations
• MGX: mitral valve clip vs Open MVR +/- CABG. Discuss indication. Decision is often based on a TOE.

Mitral RegurgitationManagementConsider patients pre-morbid state Medical : Diuresis
Rate control
Anti coagulation
ACE inhibitors and B-blockers. Surgical : Assessment with an TTE / TOE and angiogram.
Mitral clip or an open Valve Replacement

Mitral Stenosis Cause: Congenital
Rheumatic Heart disease
Senile Degeneration
Clinical Signs
Malar flush
Irregular pulse
Tapping apex beat – palpable 1st HS
Left parasternal heave / Enlarged LA
Loud 1st heart sound
Opening snap
Mid-diastolic murmur.

On investigation CXR- Enlarged left atrium,
calcified valves and pulmonary
oedema.
ECG – p-mitrale and AF
Management
Medical : Rate control (digoxin)
Anti-coagulate
Valvuloplasty
Surgical : Valve replacement
Valveotomy (open / closed)

Aortic Regurgitation Causes : Acute (inf. Endocarditis)
Chronic: Connective tissue disorders (RA), Rheumatic heart disease, syphilitic heart disease . Aortitis: Marfans / Anklysing spondylitis
Clinical features: Wide PPcollapsing pulse – hyperdynmaic apex beatEponymous signsEarly diastolic murmur

Aortic Regurgitation
Other causes of a collapsing pulse? Anything that causes a high circulating volume:
Pregnancy
Anaemia
PDA
Thyrotoxicosis
Management Valve replacement vs conservative management
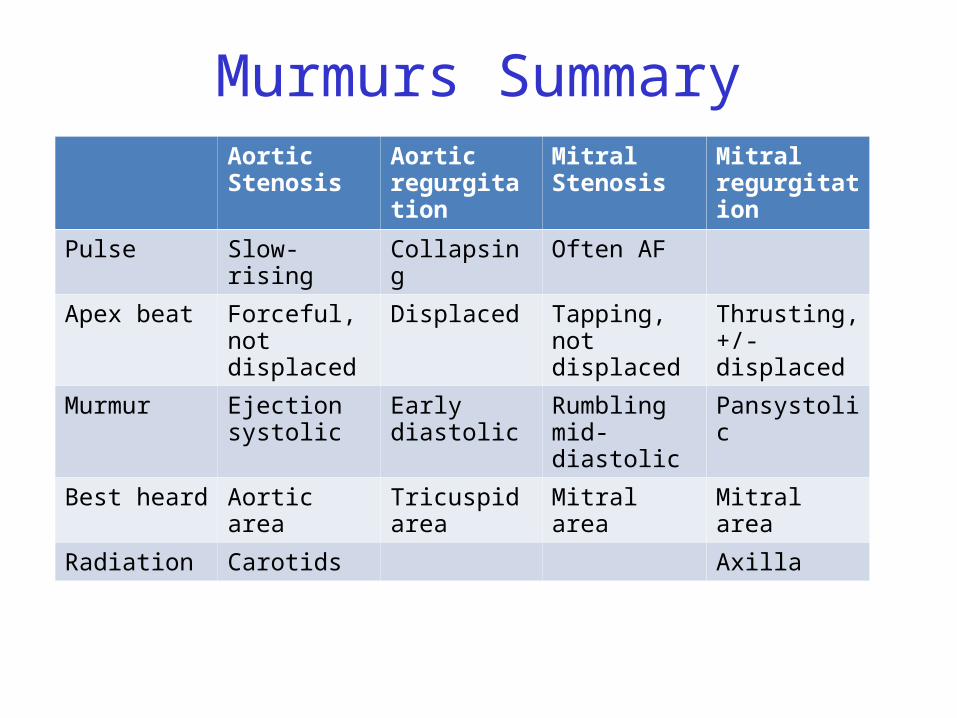
Murmurs SummaryAortic Stenosis
Aortic regurgitation
Mitral Stenosis
Mitral regurgitation
Pulse Slow-rising Collapsing Often AF
Apex beat Forceful, not displaced
Displaced Tapping, not displaced
Thrusting, +/- displaced
Murmur Ejection systolic
Early diastolic Rumbling mid-diastolic
Pansystolic
Best heard Aortic area Tricuspid area Mitral area Mitral area
Radiation Carotids Axilla
Complications of Valve replacements
• INFECTION : early vs late.
• FAILURE OF VALVE: early vs late
• DISLODGEMENT
• THROMBUS FORMATION vs HAEMMOHRAGE

Management
• What would you do as an F1?• ECG• CxR• Inform seniors• Echo• Conservative: if AF, rate control. Diuretics
improve symptoms• Surgical: Valve repair/ replacement
“ A 54 year old lady initially presents with an abscess.
She vascular infarcts on CT and is admitted to the acute stroke unit. She has no major risk factors for a CVA.
On doing base line bloods she has CRP 300Urine dip show blood +++
She’s on the stroke ward, she has some left sided weakness. Obs stable, and apyrexial so far “
What is the diagnosis???
Infective endocarditis
What would you look for ???

What would you look for?
• Signs of sepsis• New murmur or
change in existing murmur
• Microscopic haematuria, ARF, splenomegaly
• Embolic features e.g. abscesses

What would you do as an FY1?
• Bloods• Blood cultures• ABG• Urine dip & MCS• CxR• ECG• Echo (TOE)• Inform seniors

Common questions
1. Risk factors?Lifestyle factors (IVDU), cardiac lesions, aortic or mitral valve
disease, PDA, VSD, coarctation, prosthetic valve
2. Organisms?• Strep viridans (35-50%), HACEK (Haemophilus, actinobacillus,
cardiobacterium, Eikenella)• Fungi • SLE – Libman-Sachs endocarditis
3. Criteria for Diagnosis?

Duke criteria for diagnosis
2 major OR 1 major and 3 minor OR all 5 minor criteria
Major• +ve blood culture
typical organism in 2 separate cultures or persistently +ve blood cultures
• Endocardium involved• Positive echo or new valvular regurgitation
Minor • Predisposition• Fever >38C• Vascular/immunological signs• +ve blood cultures that do not meet major criteria• +ve echo that does not meet major criteria
Management
• MDT decision • Conservative management: Long-term
antibiotics and serial echos• Surgical management: Valve replacement
Dextrocardia A congenital defect where the heart is situated on the right side of the body
2 types:
Isolated dextrocardia – heart placed further to the right in thorax, associated with other cardiac abnormalitiesDextrocardia situs inversus – heart placed to the right side as a mirror image

Dextrocardia CxR

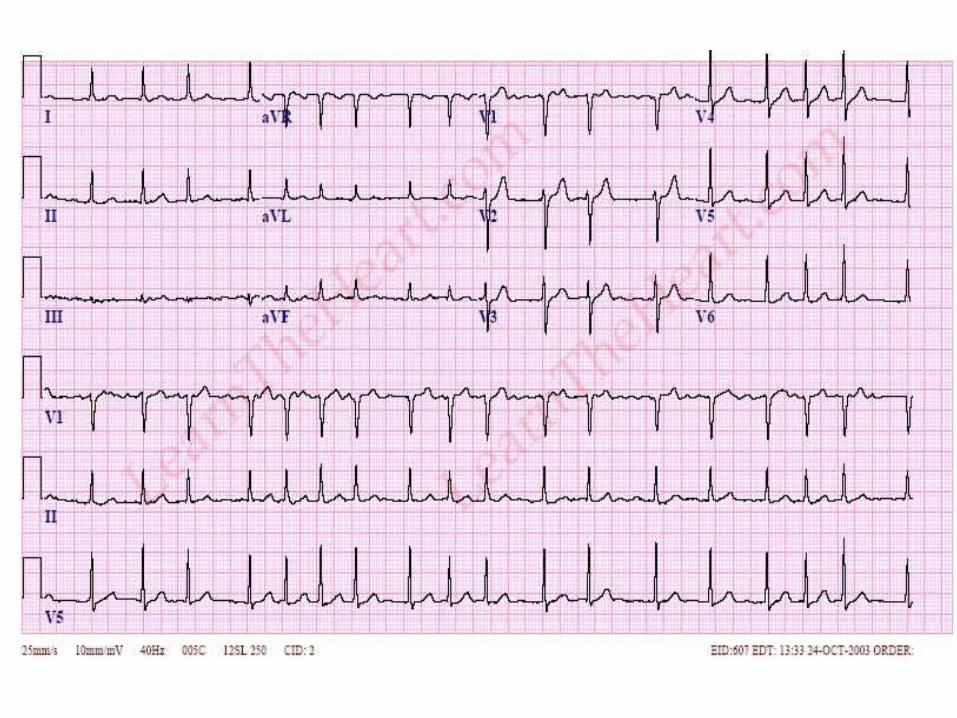
Dextrocardia ECG





THANK YOU