case 3 martha bishop pitman, m.d. - britishcytology.org.uk
TRANSCRIPT
Case 3
Martha Bishop Pitman, M.D. Director, Cytopathology
Massachusetts General Hospital Professor of Pathology
Harvard Medical School Boston, MA
Patient History
• 68 year old female
• Asymptomatic until dental procedure, after which she experienced abdominal pain
• CT showed a pancreatic cyst in the head
• Referred for EUS-FNA

EUS An anechoic lesion suggestive of a cyst was identified in the pancreatic head. The lesion measured 30 mm by 25 mm There was a single compartment. The outer wall of the lesion was thick. There was no associated mass. There was internal debris within the fluid-filled cavity. One pass was made with the 22 gauge needle using a transduodenal approach. The amount of fluid collected was 12 mL. The fluid was opaque, yellow and thin.
Clinical Diagnosis: Pseudocyst




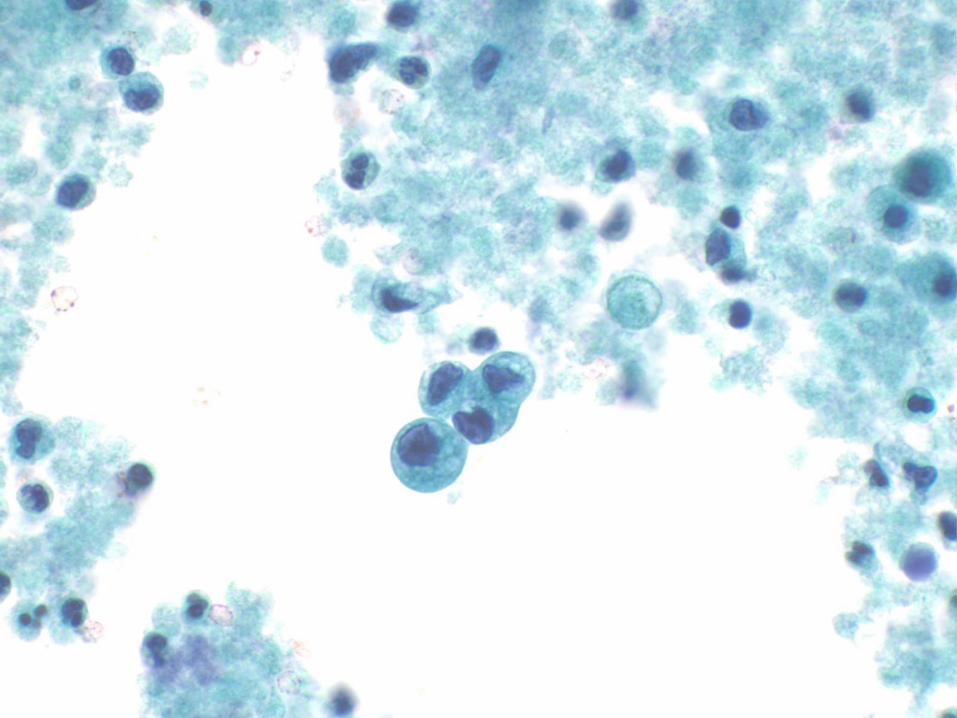
Common Diagnosis:
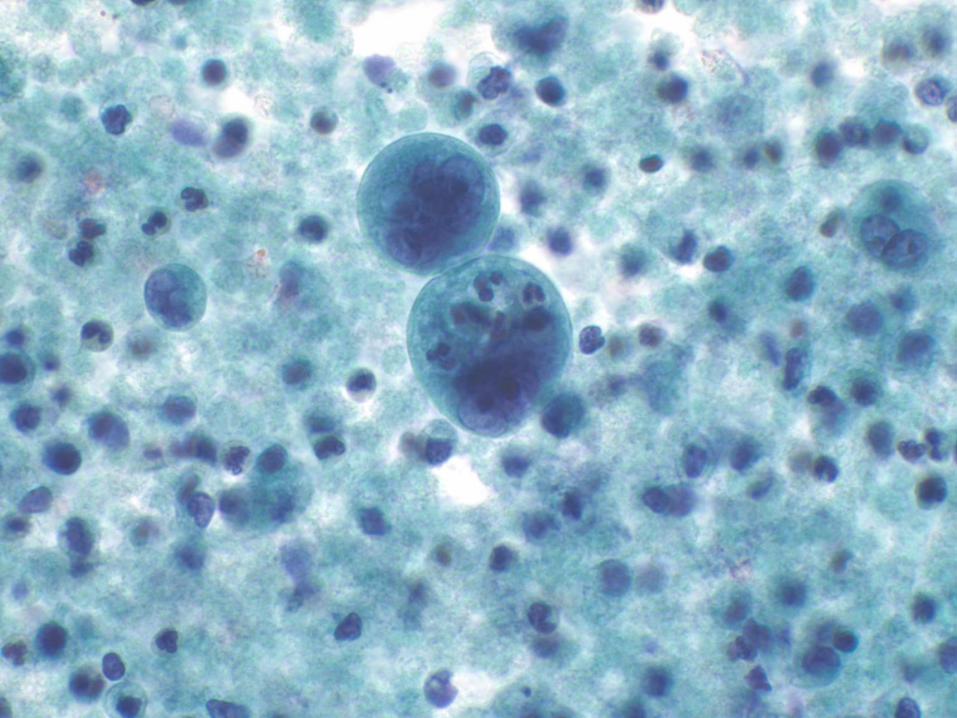
Atypical
Cyst fluid with atypical epithelial cells and acute inflammation

Consequences of “Atypical” Interpretation
• Unclear significance for the patient
• May be interpreted as “not cancer” so just follow the patient
• Cannot manage or treat the patient with an atypical diagnosis
• Results in an expensive repeat EUS-FNA with its risks
• Delays a potentially significant diagnosis and surgery

Can we do better?
• Can we at least determine if the cyst is mucinous or non-mucinous?
• Can we assess the risk of malignancy from the cells to help determine if the patient needs surgery?

Mucinous HGA
IPMN with LGD
GI duplication
cyst
Non-neoplastic
Mucinous cyst
Cystic PanNET
Cystic Acinar
Cell carcinoma
SPN
IPMN/MCN with HGD
IPMN/MCN with
Invasive carcinoma
Cystic PDAC
IPMN with IGD
PCT
LEC
SCA
Surgery
MCN
with
LGD
Cytological Preparations
• Cysts
– Direct smears
• If fluid thick enough
– Fresh undiluted cyst fluid
• CEA; Amylase
• Molecular
• Cytology
– Cytospin
– Cellblock
No-ROSE
HARVARD MEDICAL SCHOOL
MASSACHUSETTS GENERAL PHYSICIANS ORGANIZATION
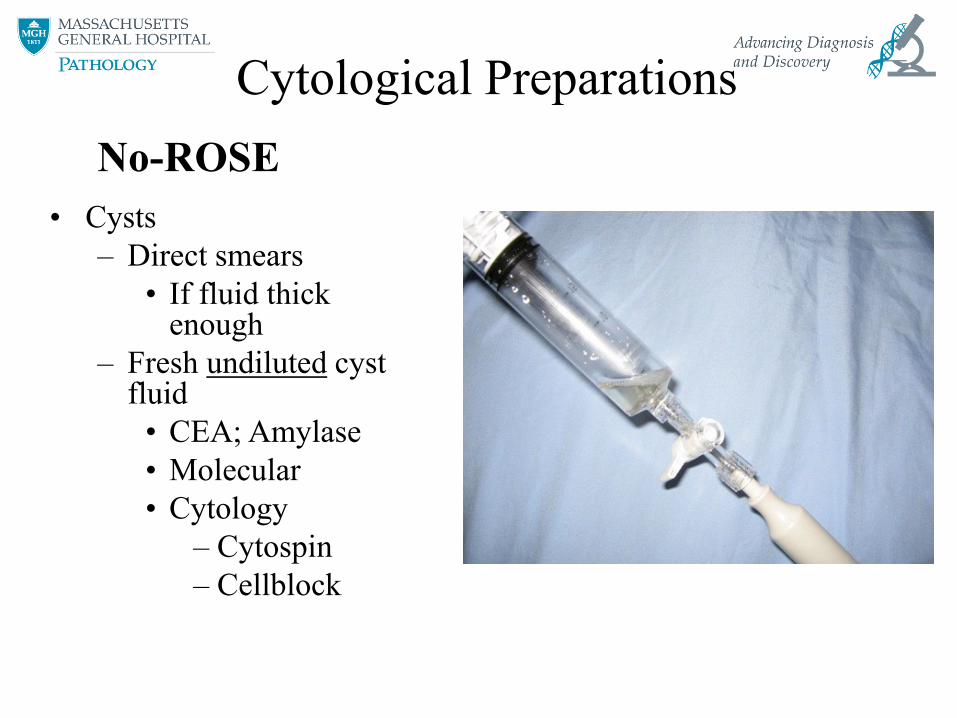
Pancreatic Cyst Fluid Triage

HARVARD MEDICAL SCHOOL
MASSACHUSETTS GENERAL PHYSICIANS ORGANIZATION
Two basic questions for Cyst analysis
1) Is the cyst mucinous or non-mucinous?
2) Is the cyst low-risk or high-risk for malignancy, e.g. does the cyst contain high-grade dysplasia or carcinoma (HGA)?
Gross Cyst Fluid
Mucinous cyst fluid
• Thick
• Viscous
• Sticky
• White
• Opaque

Acellular thick, colloid-like mucin is NOT non-diagnostic!
HARVARD MEDICAL SCHOOL
MASSACHUSETTS GENERAL PHYSICIANS ORGANIZATION
Include Secondary Pathology
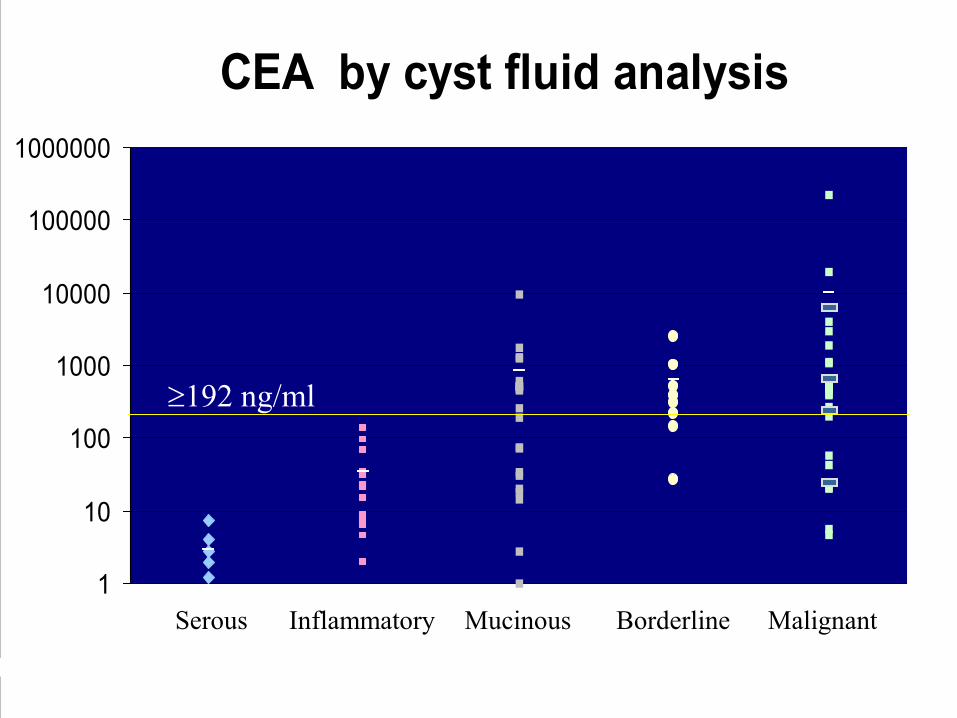
CEA by cyst fluid analysis
1
10
100
1000
10000
100000
1000000
Serous Inflammatory Mucinous Borderline Malignant
192 ng/ml
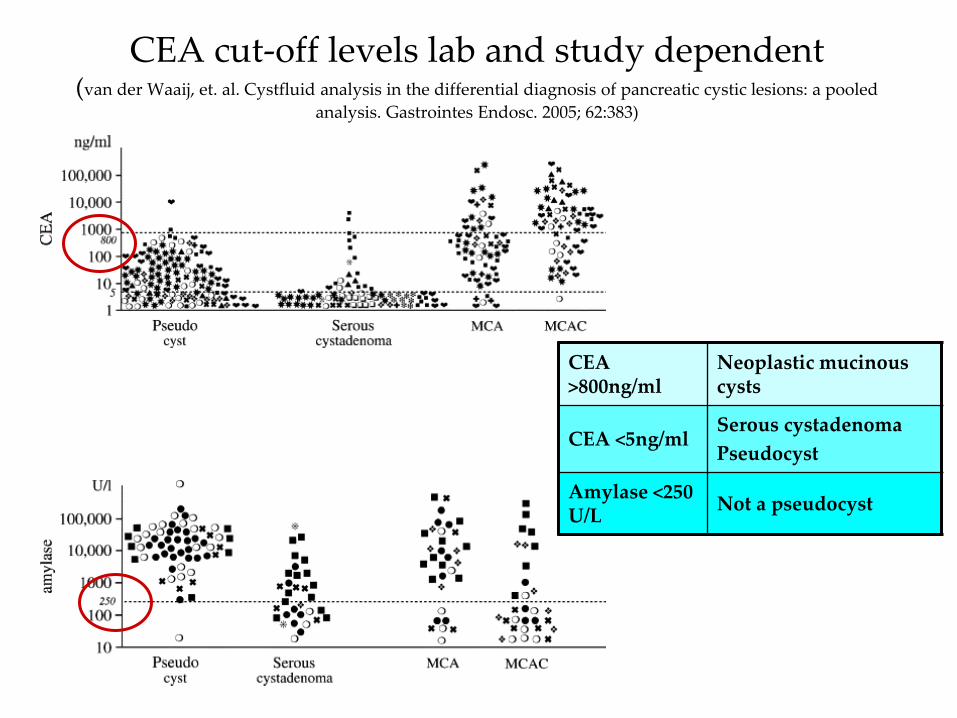
CEA cut-off levels lab and study dependent (van der Waaij, et. al. Cystfluid analysis in the differential diagnosis of pancreatic cystic lesions: a pooled
analysis. Gastrointes Endosc. 2005; 62:383)
CEA >800ng/ml
Neoplastic mucinous cysts
CEA <5ng/ml Serous cystadenoma
Pseudocyst
Amylase <250 U/L
Not a pseudocyst
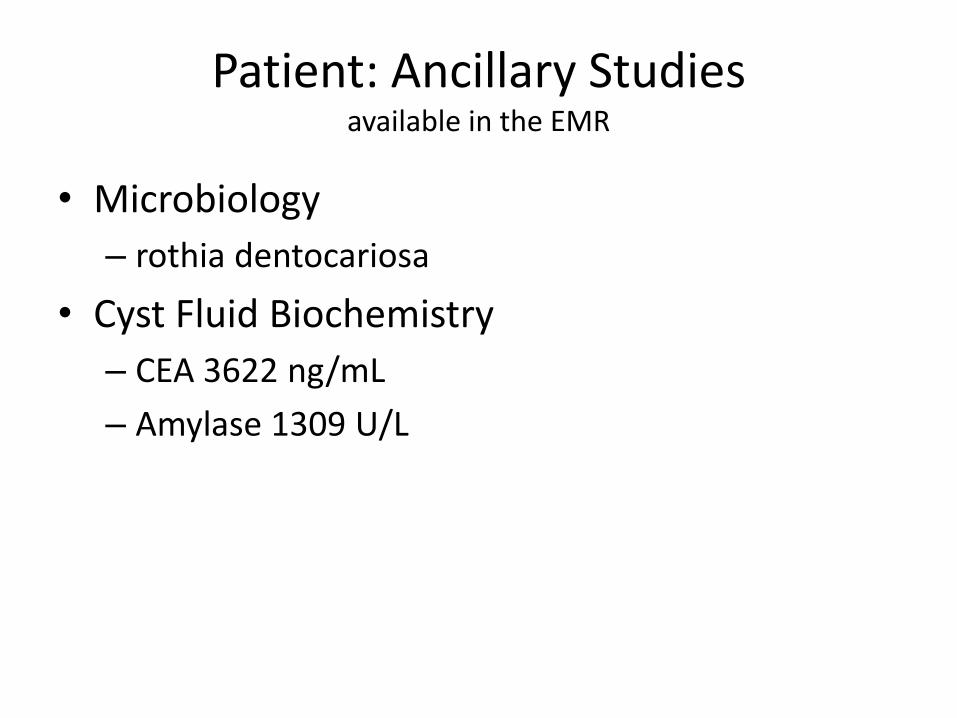
Patient: Ancillary Studies available in the EMR
• Microbiology
– rothia dentocariosa
• Cyst Fluid Biochemistry
– CEA 3622 ng/mL
– Amylase 1309 U/L

Question 1: Is the Cyst mucinous?
YES
CEA of patient’s cyst 3622 ng/mL
Cells contain mucin vacuoles

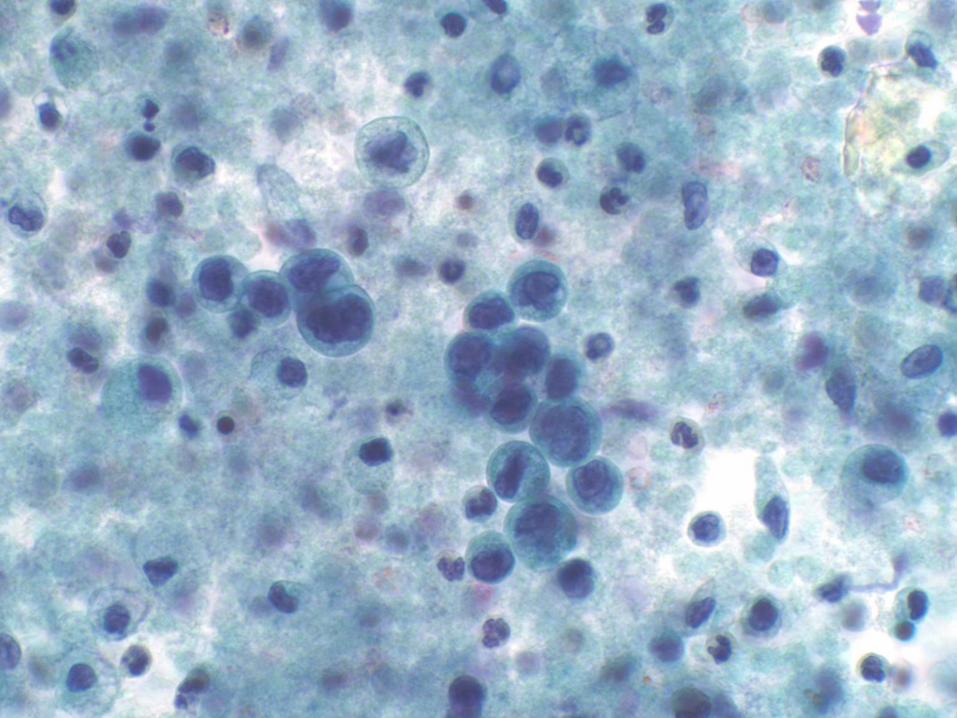
Question 2: Is the Cyst high-risk?

Are the cells high-grade or low-grade?

Cytological Criteria of High-Grade Epithelial Atypia in the Cyst Fluid of Pancreatic Intraductal Papillary
Mucinous Neoplasms Martha B. Pitman, MD, Barbara A. Centeno, MD, Ebubekir S. Daglilar, MD,
William R. Brugge, MD, and Mari Mino-Kenudson, MD Cancer Cytopathology 2014;122(1):40-47.
HGA is most accurately identified in mucinous cyst fluids by: 1. an increased N/C ratio, 2. an abnormal chromatin pattern 3. background necrosis
Reference duodenal enterocyte Low-grade High-grade
HARVARD MEDICAL SCHOOL
MASSACHUSETTS GENERAL PHYSICIANS ORGANIZATION
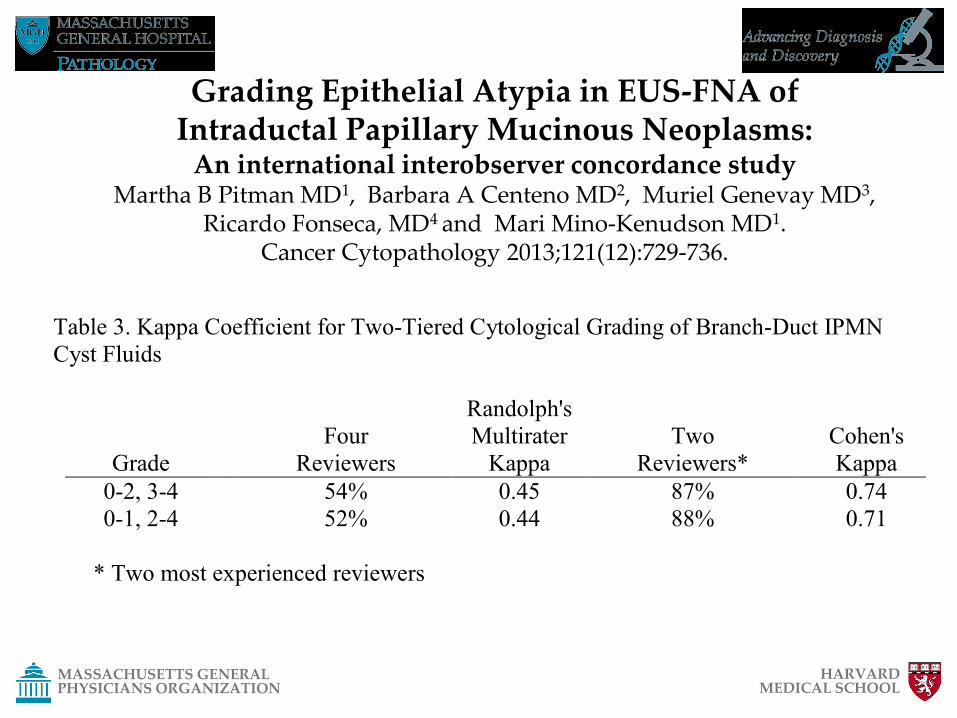
Grading Epithelial Atypia in EUS-FNA of Intraductal Papillary Mucinous Neoplasms:
An international interobserver concordance study Martha B Pitman MD1, Barbara A Centeno MD2, Muriel Genevay MD3,
Ricardo Fonseca, MD4 and Mari Mino-Kenudson MD1. Cancer Cytopathology 2013;121(12):729-736.
Table 3. Kappa Coefficient for Two-Tiered Cytological Grading of Branch-Duct IPMN
Cyst Fluids
Grade
Four
Reviewers
Randolph's
Multirater
Kappa
Two
Reviewers*
Cohen's
Kappa
0-2, 3-4 54% 0.45 87% 0.74
0-1, 2-4 52% 0.44 88% 0.71
* Two most experienced reviewers
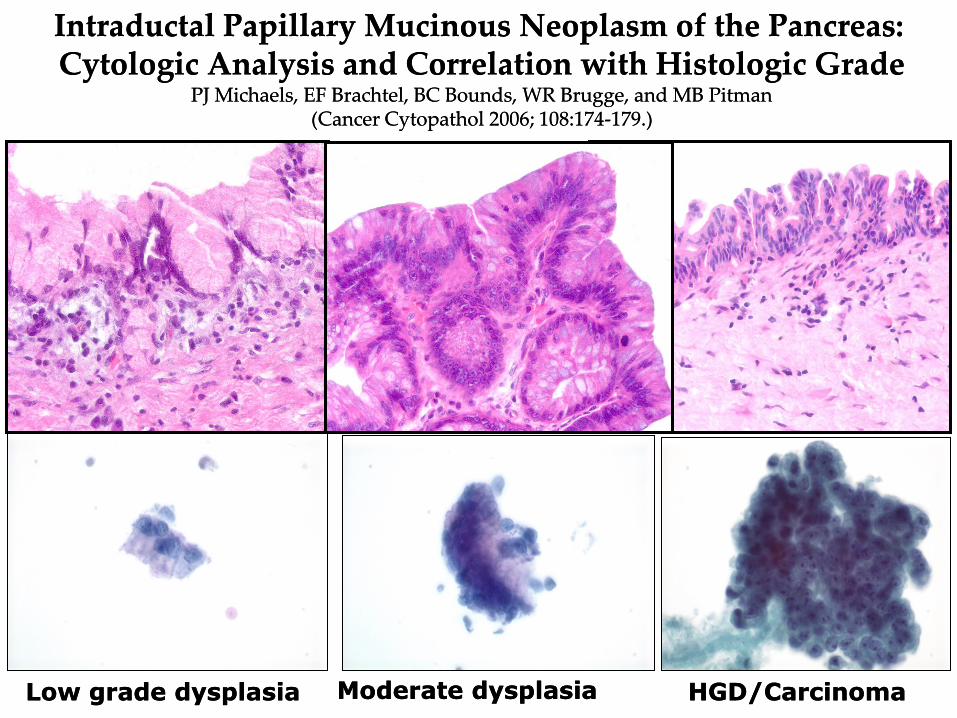
HGD/Carcinoma HGD/Carcinoma
Intraductal Papillary Mucinous Neoplasm of the Pancreas: Cytologic Analysis and Correlation with Histologic Grade
PJ Michaels, EF Brachtel, BC Bounds, WR Brugge, and MB Pitman (Cancer Cytopathol 2006; 108:174-179.)
Intraductal Papillary Mucinous Neoplasm of the Pancreas: Cytologic Analysis and Correlation with Histologic Grade
PJ Michaels, EF Brachtel, BC Bounds, WR Brugge, and MB Pitman (Cancer Cytopathol 2006; 108:174-179.)
Low grade dysplasia Low grade dysplasia Moderate dysplasia Moderate dysplasia

Atypical Epithelial Cells
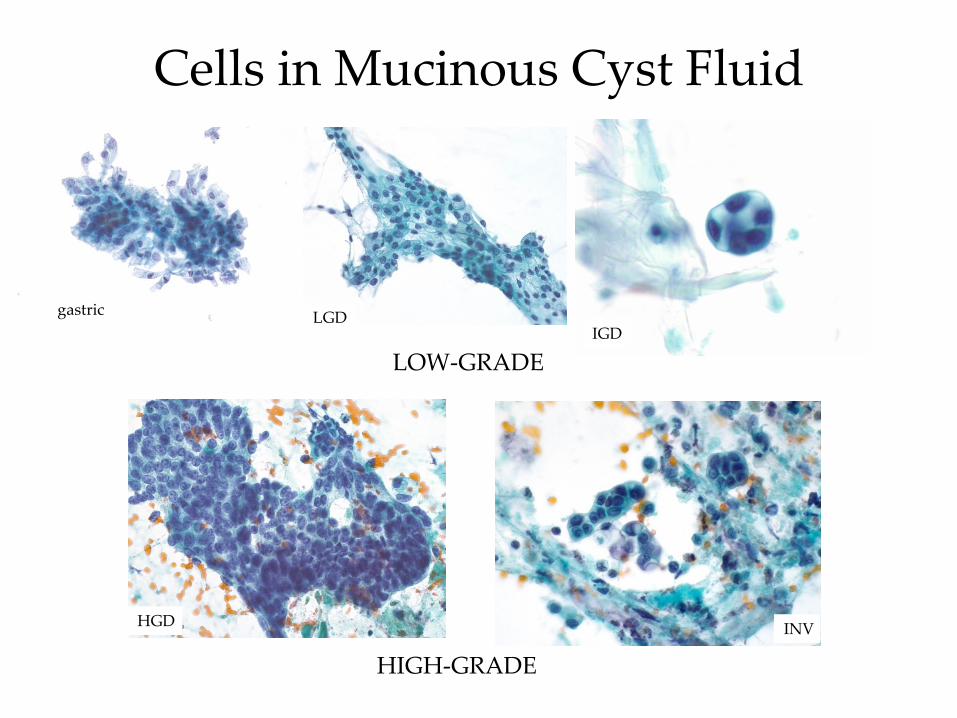
Cells in Mucinous Cyst Fluid
LOW-GRADE
HIGH-GRADE
gastric
INV
LGD
HGD
IGD
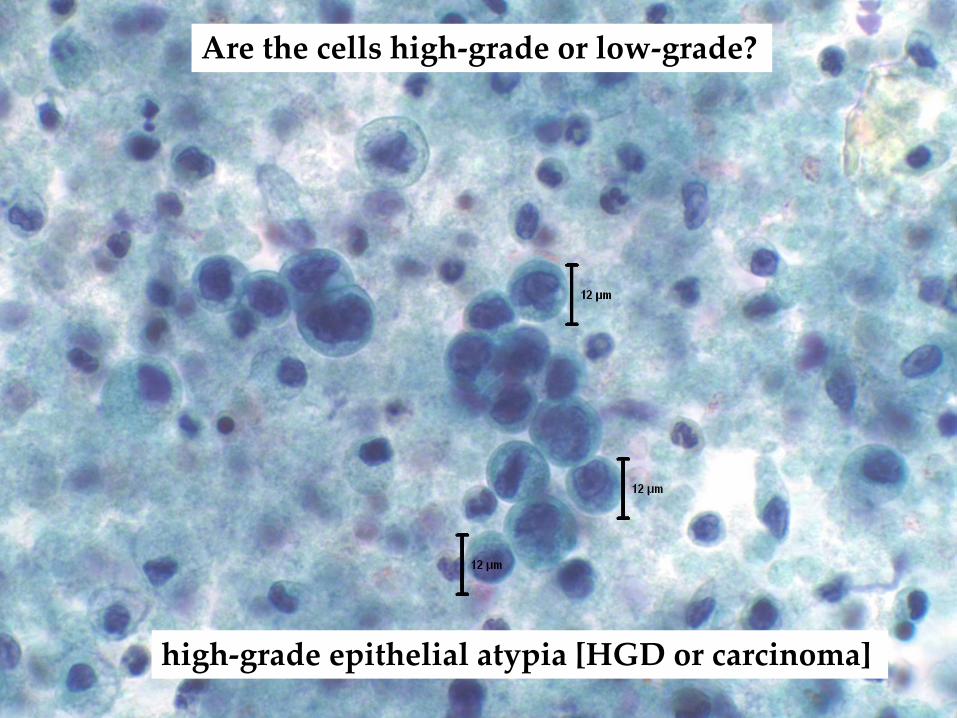
Are the cells high-grade or low-grade?
high-grade epithelial atypia [HGD or carcinoma]

HARVARD MEDICAL SCHOOL
MASSACHUSETTS GENERAL PHYSICIANS ORGANIZATION
Recommended Terminology: PSC System
• Neoplastic: Other
• MCN- low, intermediate and high-grade dysplasia [low-grade or high-grade atypia]
• IPMN-low, intermediate and high-grade dysplasia [low-grade or high-grade atypia]
• Mucinous cyst, NOS with low, intermediate and high-grade dysplasia [low-grade or high-grade atypia]

HARVARD MEDICAL SCHOOL
MASSACHUSETTS GENERAL PHYSICIANS ORGANIZATION
Template for Diagnosis Appendix A
• Neoplastic: Other
• Cyst contents consistent with a neoplastic mucinous cyst. See note.
• Note: The diagnosis is supported by: [check all that apply]
• Thick, colloid-like extracellular mucin
• Degenerative debris within the mucin
CEA > 192 ng/ml (give value)
• KRAS mutant
• GNAS mutant [this mutation supports an IPMN]
• Mucinous epithelium with low-grade atypia [low-grade dysplasia or intermediate grade dysplasia]
Epithelium with high-grade atypia [high-grade dysplasia or invasive carcinoma]
• Well-differentiated neuroendocrine tumor [with cystic degeneration].
Better Cytological Interpretation than “Atypical Cells”
Neoplastic: Other
Neoplastic mucinous cyst with high-grade epithelial atypia. See note.
Note: The CEA of 3622 ng/mL supports a mucinous etiology. The epithelium also appears mucinous and may
represent high-grade dysplasia or invasive carcinoma.
Based on cytological diagnosis
Patient underwent a Whipple procedure
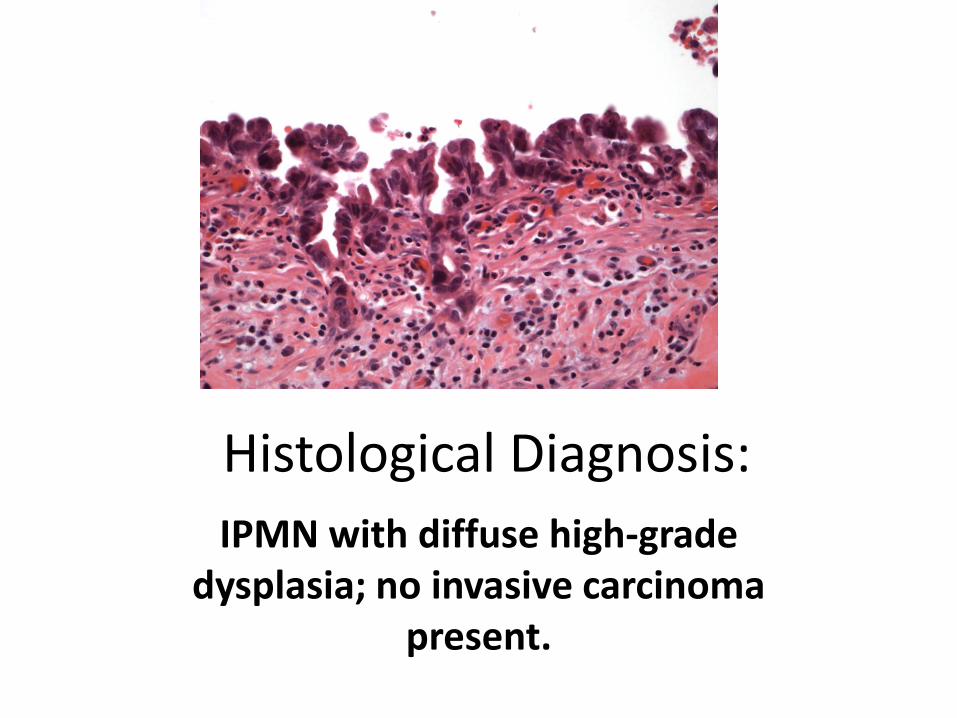
Histological Diagnosis:
IPMN with diffuse high-grade dysplasia; no invasive carcinoma
present.
Cytology Interpretation Optimized • Multimodal Approach
– Clinical Information • Patient age and gender • Symptoms • Past medical history
– Radiological Information • Location of mass in the pancreas (and thus organ traversed for
EUS) • Mass characteristics
– Solid or cystic » Size, contours, invasion » Cyst structure: uni- or multilocular; thick/thin wall, Ca++,
nodule/mass in the wall » Gross cyst contents: thick, viscous, thin, water, clear, brown
– Ancillary tests: CEA, amylase, molecular analysis

Patient Follow-Up
• Alive without disease at 7 years

Thank You!