cdh for students corrected
DESCRIPTION
CDH for Students CorrectedTRANSCRIPT


CDHCongenital Dislocation of the
Hip
By
Musa khan final year mbbsPeshawar medical college

CDH
Definition• A progressive deformation of previously
normally formed structures during the embryonic period
NOT A malformation arising during the period of organogenesis

CDHNomenclature
• CDH Congenital Dislocation of the Hip• DDH Developmental Dysplasia of the Hip• CDH Congenital Dysplasia of the Hip
• CHD Congenital Heart Disease !

CDH Spectrum
• Teratologic Hip : Fixed dislocation Occurrs prenatally Often with other anomalies
• Dislocated Hip : Completely out May or may not be reducible
• Subluxated Hip : Only partially
• Unstable Hip : Femoral head can be dislocated
• Acetabular Dysplasia : Shallow Acetabulu
Head Subluxated or in place

CDHIncidence
• Hip Instability at Birth : 0.5 – 1 % of infants
• Classic CDH : 0.1 % of infants
• Mild Dysplasia : Substantial
Contributing to adult Osteoarthritis
Up to 50 % of Hip Arthritis in Ladies
Have underlying hip dysplasia

CDH
Incidence Area Incidence per 1000
Canadian Indians 188.5
Hungary 28.7
Uppsala, Sweden 20
USA Caucaseans
Blacks
15.5
4.9
Malmo, Sweden 2.18
Chinese, Hong Kong 0.1
Bantus, Africa 0.0 among (16678)

CDH
Etiology
Multi-factorial

CDH
Etiology
Physiologic Factors
Ligament Laxity :
Hormonal :
( Estrogen, Relaxin) Females
Familial hyper laxity :
mild - moderate - Ehler Danlos
ADD Picture of knee hyperextension

CDH
Etiology
Genetic Factors• Gender : Female
Most studies:
shows that females are more commonly affected.
• Twin studies:
Monozygotic 38 %
Dizygotic 3 % (similar to siblings)

CDH
Etiology Mechanical Factors Prenatal : - Breech position - Oligohydramnious - Primigravida - Cong. Knee recurvatum/dislocation - Metatarsus adductus - Torticollis
Postnatal : - Swaddling / Strapping – Knees extended

CDH
EtiologyMechanical Factors
• Breech Presentation :
Normally 2 –4 %
CDH 16 %
The Breech position In Utero Extended knees and flexed hips

CDH
EtiologyEnvironmental & Mechanical Factors
• Swaddling / strapping ( Mihad ): Knees extended & Hips adducted
– Proven experimentally– Proven statistically
• American Indians.• Eskimos, and • Saudi Arabia
– Mechanics• Hip adduction and extension

CDHPatients At Risk
• Positive Family History : increases risk 10X• A baby girl : increases risk 4-6 times• Breech Presentation : increases risk 5-10 X• Torticollis : CDH in 10-20 % cases• Foot Deformities : ( calcaneovalgus & metatarsus adductus) signs of intrauterine crowding• Knee Deformities : ( hyperextension & dislocation )
associated with Teratologic type

CDH
Risk Factors
When Risk Factors Are Present• The infant should be examined repeatedly
• The hip should be imaged
( by U/S or X-ray )

CDHNeonatal Examination
The infant should be quiet and comfortable

CDHNeonatal Examination
LOOK :
•Wide perineum
( in bilateral )
•Lateralized contour
•External rotation attitude

CDHNeonatal Examination
LOOK :• Asymmetric thigh
folds
anterior
posterior

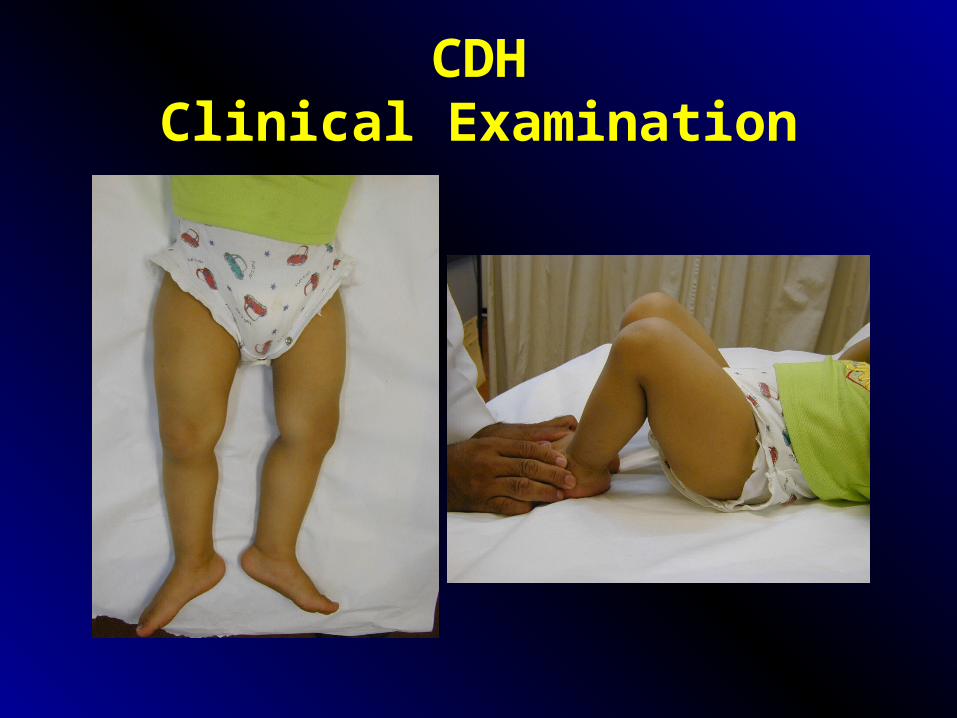
CDHClinical Examination
• Look :
Shortening ( not in neonates )
- Galeazzy sign
- in supine

CDHNeonatal Examination
FEEL :
• Empty groin
• Weak Femoral pulse

CDHNeonatal Examination
MOVE :• Hip instability
in early infancy• Limited hip abduction
in flexion - later
(careful in bilateral)
if <600 on both sides:
request imaging

Cerebral palsy
Clinical AssessmentHip Flexion Deformity
SPECIAL :• Loss of fixed flexion
deformity of hips
( early infancy )• Normally FFD
newborn 28o
at 6 weeks 19o
at 6 months 7o
FFDNormal
No FFD?CDH
Thomas Test

CDH
Neonatal ExaminationOrtolani
Feel a ClunkNot hear a click !

CDH
Neonatal ExaminationBarlow

CDHNeonatal Examination
Ortolani / Barlow
clunk
Ortolani Barlow

CDHNeonatal Examination
Ortolani / Barlow
Ortolani Barlow

CDHNeonatal Examination
Hamstring Stretch Sign• Flex hip and knee 900 each.• Keep hip flexed and gradually extend the knee• Normally a resistance is felt towards the end of
knee extension (caused by the hamstrings which are pulled from both
ends)
• In cases of CDH, no resistance is felt (when the hip is dislocated, the origin of the hamstrings are
not pulled by hip flexion)

CDHNeonatal Examination
Hamstring Stretch Sign

CDHClinical Examination
• Neonate (up to 2-3 months) : - Instability/ Ortolani-Barlow - Thomas test
• Infant ( > 2-3 months) : - Limited abduction - Shortening ( Galeazzi ) - Hamstring stretch sign
• Toddler : - Limited abduction - Shortening ( Galeazzi ) - Hamstring stretch sign
• Walking : - Trendelenburgh - Hamstring stretch sign
CDHClinical Examination

CDHClinical Examination

CDH
Clinical ExaminationThe Walking Child
• Trendelenburgh: unilateral / bilateral (waddling)

CDHScreening Program
• Clinical screening proven to be effective
• Performed by Trained personnel
• Must be DYNAMIC
with periodic examination till walking
• Adjunctive use of U/S controversial

CDHUltrasound Screening
• Incidence of hip instability declines rapidly to 50 % within the first week of neonatal life
• Better to delay U/S screening

CDHUltrasound Screening
• Early U/S screening not recommended
• Delayed U/S screening :
- Older than 6 weeks
- Those at risk only - by
History
Clinical exam

CDH
Ultrasound Referral
• If hip normal : no need
• If hip clearly unstable : no need
• If suspicious : U/S appropriate
• If at risk factors : U/S appropriate

CDHUltrasound
• Too sensitive
detects a lot of hip anomalies most of which would develop normally
• Operator dependant
Static Vs Dynamic

CDH
Radiography
• Early infancy : not reliable• By 2-3 months of age : reliable
AP view - neutral position
- draw reference lines
- acetabular index - in early infancy
< 30o : normal
30o – 40o : questionable
> 40o : abnormal
Von Rosen view : 45o abduction

CDHRadiography

CDHRadiography

CDHRadiography

CDHRadiography
Von Rosen view
in out
in out

CDHRadiography
27o 39o

CDHRadiography
in out

CDH
Treatment
Aims
• Obtain and Maintain concentric reduction
• In an Atruamatic fashion
• Without disrupting the blood supply

CDH
Treatment• Method depends on Age
• The earlier started, the easier the treatment
• The earlier started, the better the results
• Should be detected EARLY

CDH
Treatment• Birth to 6 months : Pavlik harness or hip spica cast• 6 months – 12 months : closed reduction UGA and hip spica casts• 12 months – 18 months : possible closed / possible open reduction• Above 18 months : open reduction and ? Acetabuloplasty• Above 2 years : open reduction,acetabulplasty, and femoral osteotomy• Above 8 years : open reduction,acetabulplasty cutting three bones, and femoral
osteotomy

CDHTreatment
Hip instability in the neonatal period
Most resolve spontaneously• Observation
• Pavlik harness
• Double /triple diapers ??

CDH
Treatment
Hip instability in the neonatal period
Double / Triple Diapers• Often inadequate : therefore inappropriate• Gives illusion patient is in “treatment” while
wasting valuable time• Most hip instability improves spontaneously in
early infancy , giving this ineffective management credit

CDH
Treatment
Birth – 6 months
Hip instability (dislocatable)
Established dislocation (reducible)
• Should be actively treated until hip is normal clinically and radiographically
• Pavlik harness
• Hip Spica Cast

CDH
Treatment
Birth – 6 monthsPavlik harness

CDH
Treatment
Birth – 6 months
Other Devices - Frejka pillow - Craig
- Von Rosen splint Soft abduction splints: Not good enough
Rigid abduction splints: Risk AVN

• Initially non operative – closed reduction• Reduction under anesthesia and immobilization in hip
spica cast• Position: Human
Avoid severe abduction
Avoid Frog position
• Must be stable and concentrically reduced otherwise needs open reduction
CDHTreatment
6 – 12 months
Better Picture

CDH
Treatment
12 – 18 months
• Possibly closed reduction !!
when hip stable and concentrically reduced• Probably open reduction
when hip unstable or not concentrically reduced• Arthrography guided:

CDHTreatment
ArthrographyClosed Reduction
Too lateralized Acceptable

CDHTreatment
Above 18 months
• Open reduction
? and acetabulplasty
? And femoral shortening – if high

CDHTreatment
Above 3 years
• Open reduction
• And acetabulplasty
• And femoral shortening

Redirectional Acetabuloplasty
Salter’s
Add Picture with K wires

Pemberton’s
Need for a lot of improvement in coverNeed for a lot of improvement in cover

Triple Steel
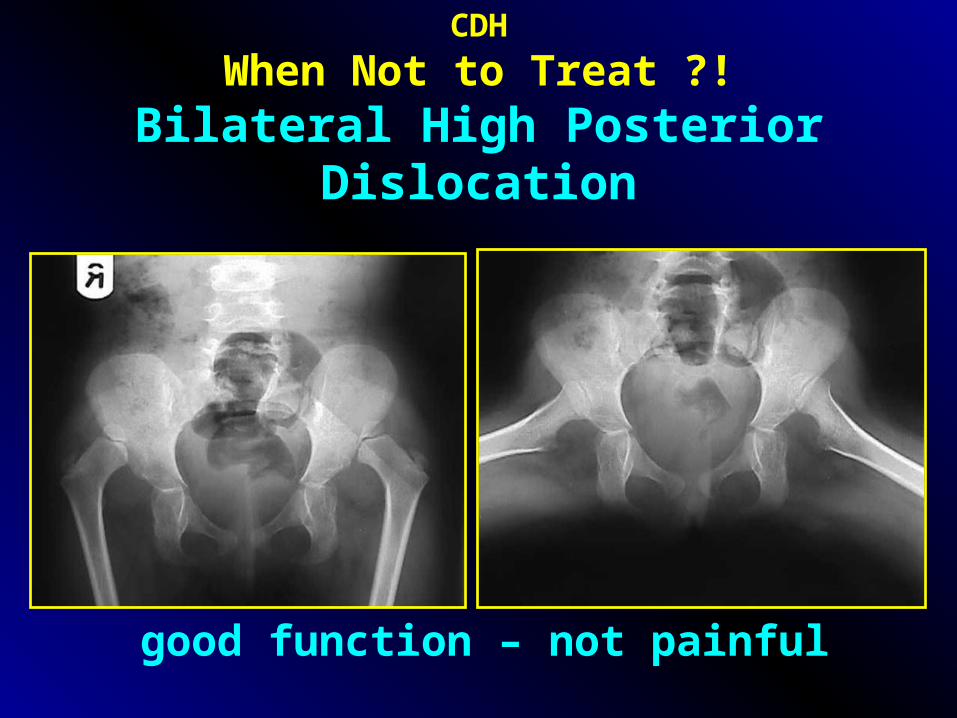
CDH
When Not to Treat ?!Bilateral High Posterior Dislocation
good function – not painful

CDH
When Not to Treat !
الدواِء� بعضِ من وخيٌرالداِء�
Painful stiff left hip Painful stiff right hip in adduction

CDH
When Not to Treat !
الدواِء� بعضِ من وخيٌرالداِء�
Painful right hip & ankylosed left hip

CDH
Summary
• Complex multi-factorial, endemic– treatable.• Dr’s awareness and health education.• Screening programs are needed.• Learning proper examination methods.• Identify at-risk groups.
– repeat examination & imaging.
• Efficient referral system.• Proper management in referral centers.

