cerebellum 78
TRANSCRIPT
1
Cerebellum, Cerebellum, Psychiatric Aspects Psychiatric Aspects & Routine Disorders& Routine Disorders
Dr Khalid MansourConsultant Psychiatrist
Letterkenny General Hospital 2017
Index 1. Introduction: Some Basic Facts.2. Anatomy. 3. Physiology: Models of Functioning. 4. Psychiatric Aspects of Cerebellar
Disorders.5. Cerebellar Abnormities in Psychiatric
Disorders.6. Cerebellar Mental Therapies. 7. Clinical Reflections:
a. Non-motor Dyspraxiab. Routine Disorders.c. Cerebellar Circuits and Mental Disorders. 2
Introduction1- 10% of the weight of the brain (Llinas et al, 2004) but contains 80% of brain neurones (Herculano-Houzel, 2010).
2- Traditional thinking is that cerebellum involved in posture, balance & motor activity.• Not involved in initiating motor activity, but coordinating them (Flourens, 1824).
Introduction 3- Abundant connections > non-motor brain regions > involved in coordinating all non-motor functions e.g. perceptions, emotions, cognition, speech, personality, etc.
4- Cerebellar abnormalities exist in most mental illnesses and mental illnesses exist in most cerebellar disorders.
4
Anatomy
5
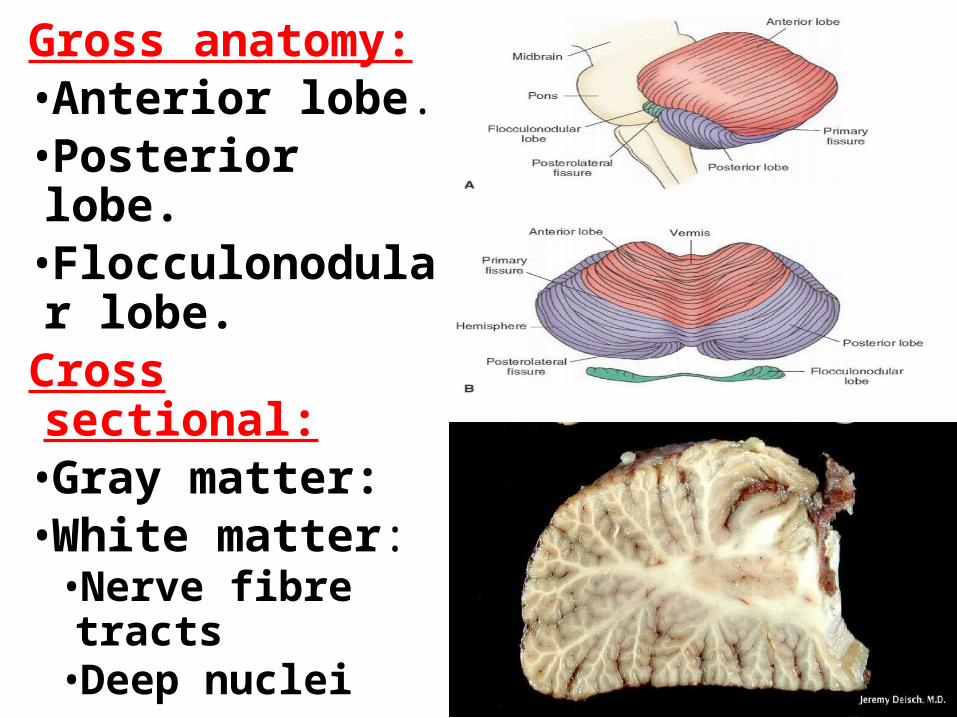
Gross anatomy: •Anterior lobe. •Posterior lobe.•Flocculonodular lobe.
Cross sectional:•Gray matter:•White matter:
•Nerve fibre tracts•Deep nuclei
6
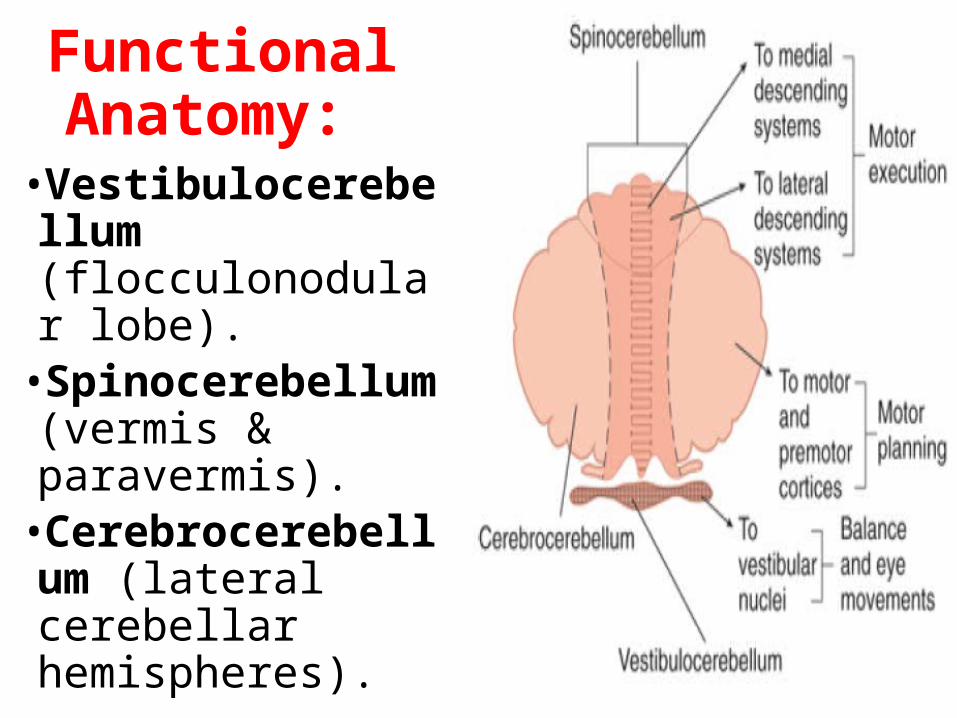
Functional Anatomy:
•Vestibulocerebellum (flocculonodular lobe).
•Spinocerebellum (vermis & paravermis).
•Cerebrocerebellum (lateral cerebellar hemispheres).
7
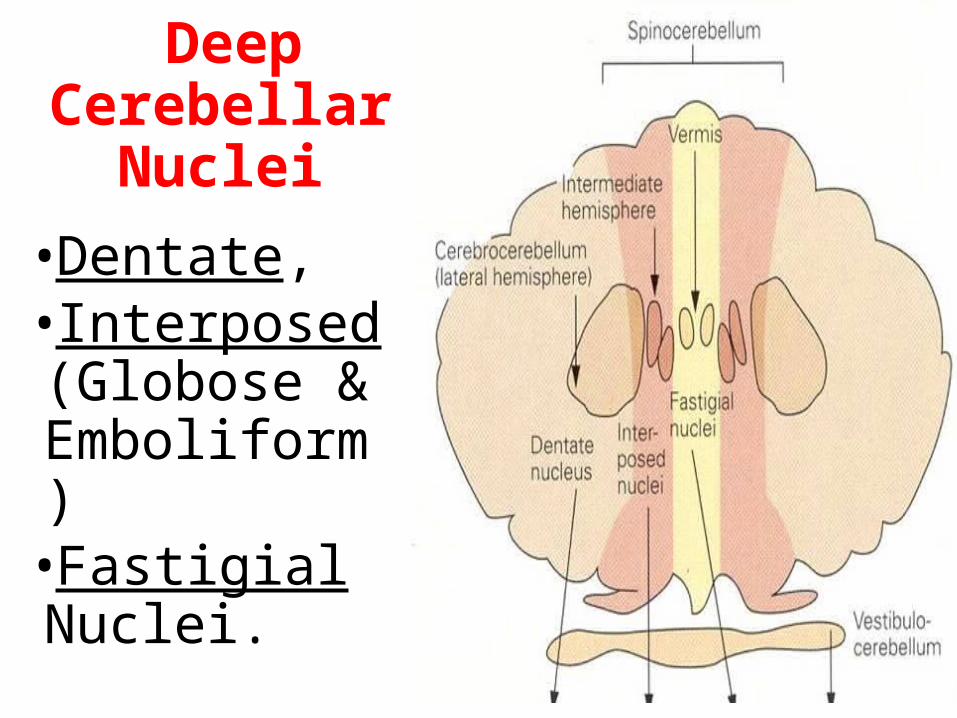
Deep Cerebellar
Nuclei•Dentate, •Interposed (Globose & Emboliform)
•Fastigial Nuclei.
8
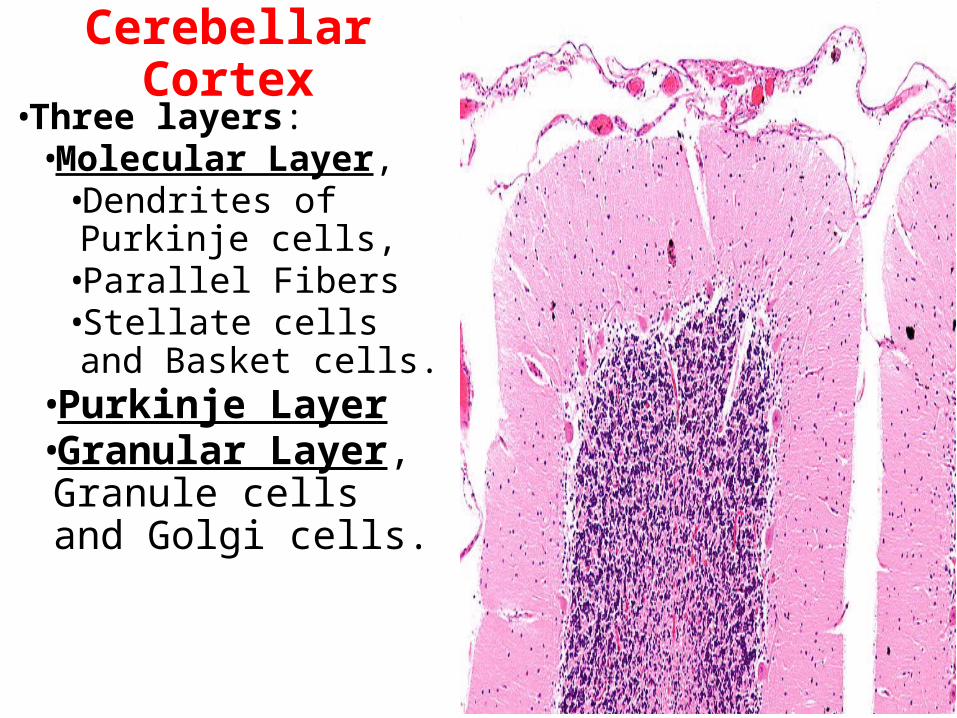
Cerebellar Cortex•Three layers:
•Molecular Layer, •Dendrites of Purkinje cells,
•Parallel Fibers •Stellate cells and Basket cells.
•Purkinje Layer•Granular Layer, Granule cells and Golgi cells. 9
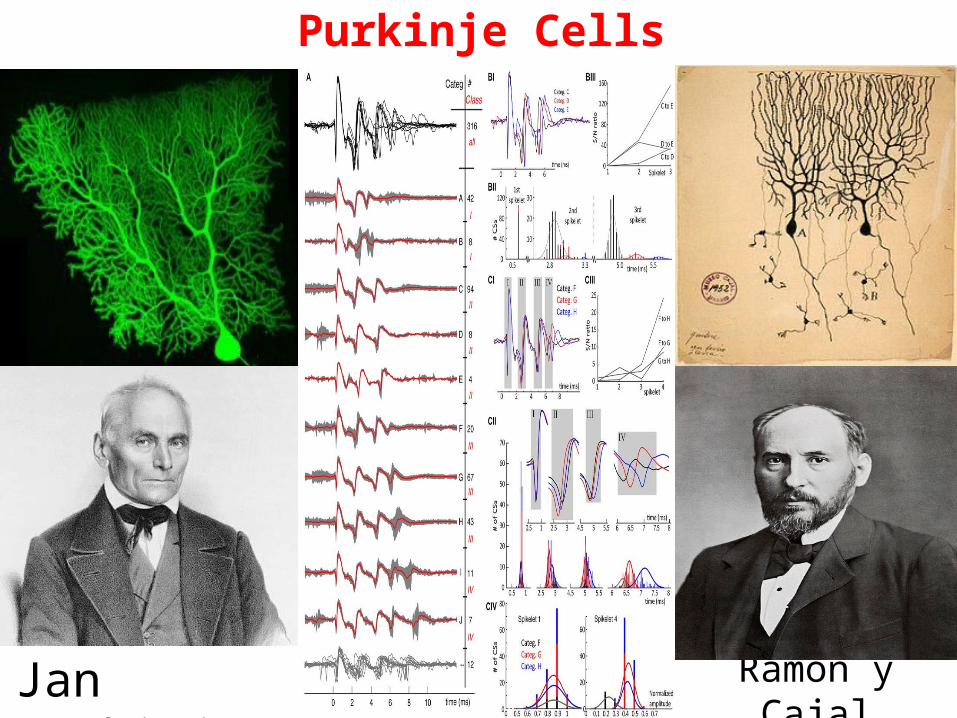
Purkinje Cells
Ramón y CajalJan Purkinje
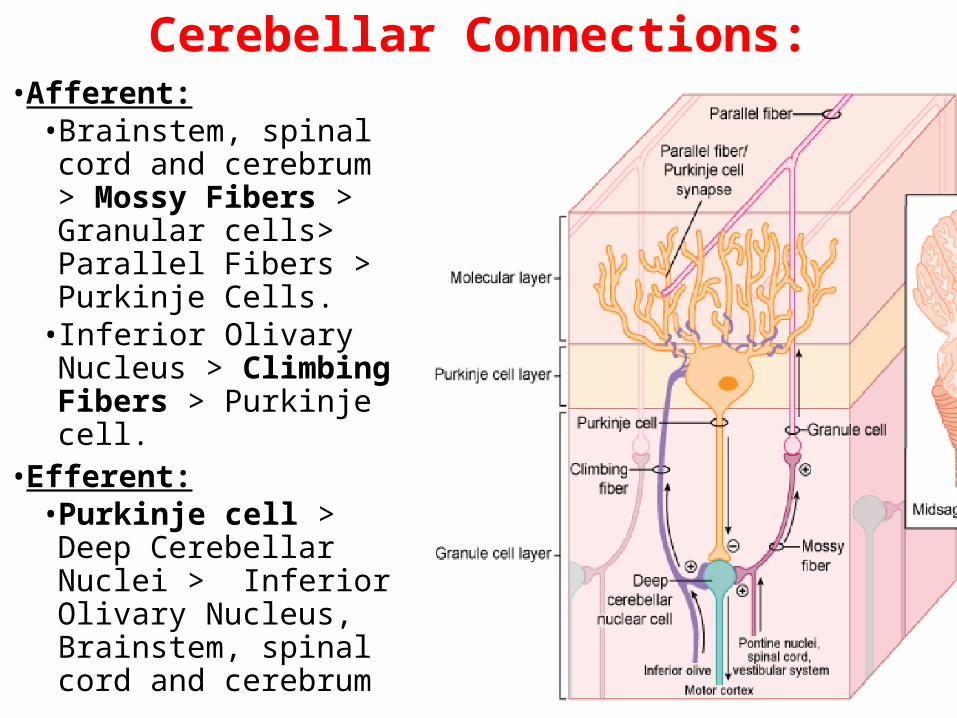
Cerebellar Connections:• Afferent:
• Brainstem, spinal cord and cerebrum > Mossy Fibers > Granular cells> Parallel Fibers > Purkinje Cells.
• Inferior Olivary Nucleus > Climbing Fibers > Purkinje cell.
• Efferent: • Purkinje cell > Deep
Cerebellar Nuclei > Inferior Olivary Nucleus, Brainstem, spinal cord and cerebrum 11
Models of Cerebellar Functioning
12
Marr & Albus Model for Cerebellar Learning (Eccles, Ito & Szentagothai,1967)
•Several theories about cerebellum and learnt behaviour.
•Most theories about Cerebellar functioning / learning are derived from early models of David Marr (1969) and James Albus (1971).
•Albus (1971) formulated his model as a software algorithm: Cerebellar Model Articulation Controller, which has been tested in a number of computer applications.
13
David Marr
James Albus
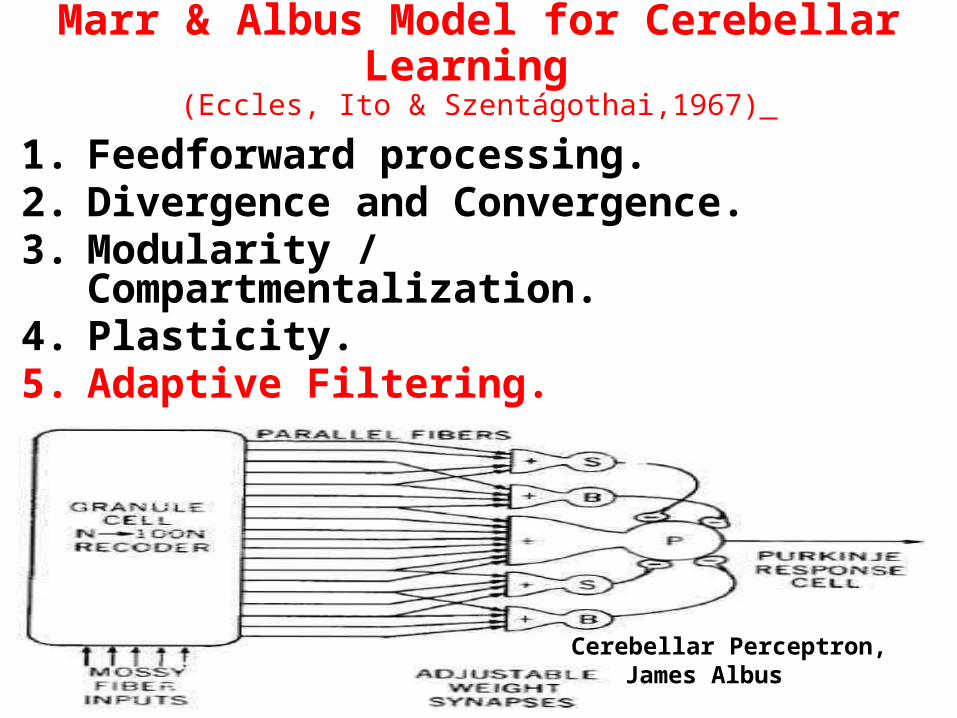
Marr & Albus Model for Cerebellar Learning (Eccles, Ito & Szentágothai,1967)
1. Feedforward processing.2. Divergence and Convergence.3. Modularity / Compartmentalization.4. Plasticity.5. Adaptive Filtering.
14
Cerebellar Perceptron, James Albus
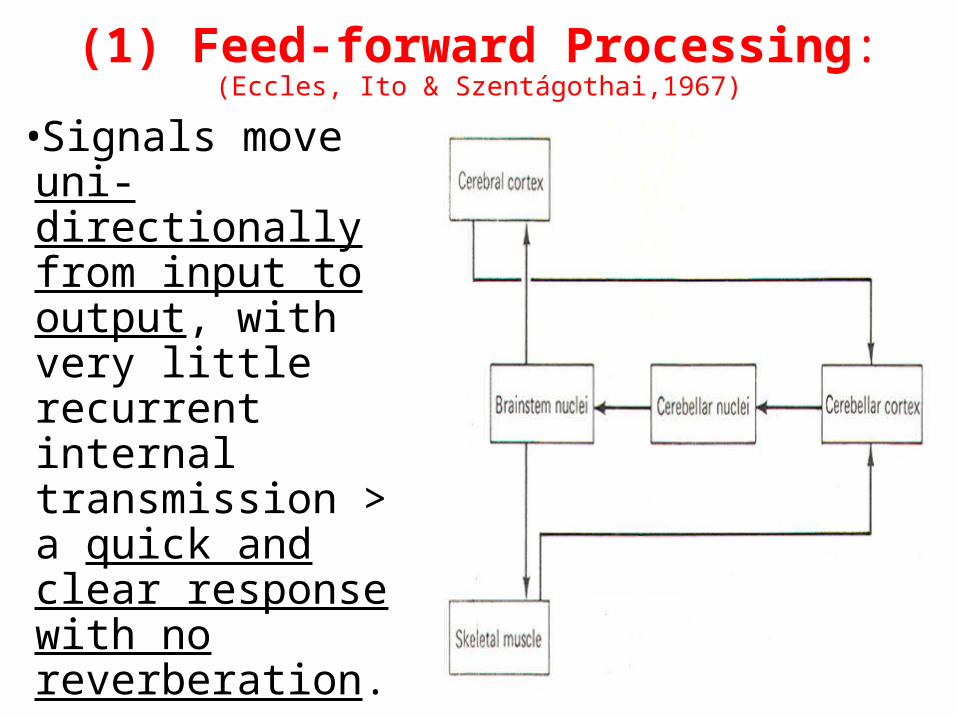
(1) Feed-forward Processing:(Eccles, Ito & Szentágothai,1967)
•Signals move uni-directionally from input to output, with very little recurrent internal transmission > a quick and clear response with no reverberation.
15
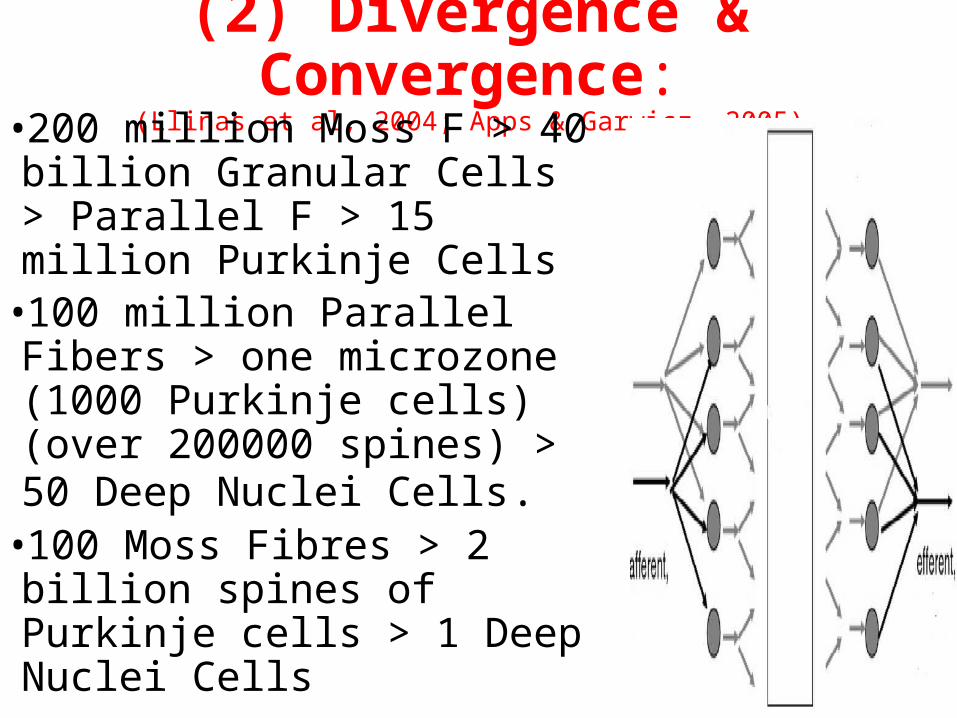
(2) Divergence & Convergence:(Llinas et al, 2004; Apps & Garwicz, 2005)
•200 million Moss F > 40 billion Granular Cells > Parallel F > 15 million Purkinje Cells
•100 million Parallel Fibers > one microzone (1000 Purkinje cells) (over 200000 spines) > 50 Deep Nuclei Cells.
•100 Moss Fibres > 2 billion spines of Purkinje cells > 1 Deep Nuclei Cells
16
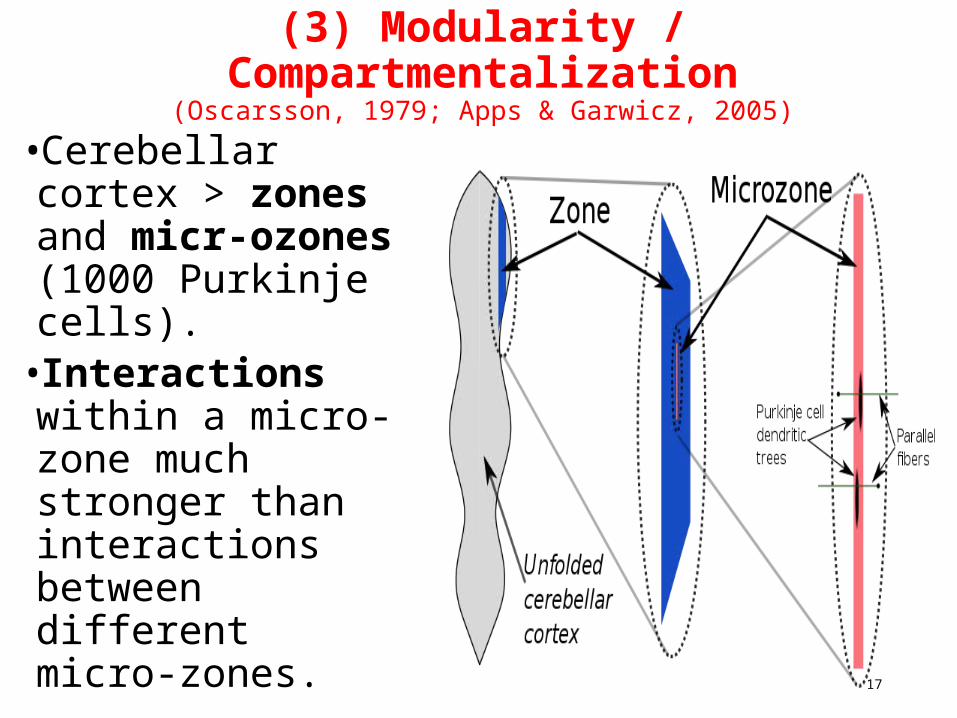
(3) Modularity / Compartmentalization(Oscarsson, 1979; Apps & Garwicz, 2005)
•Cerebellar cortex > zones and micr-ozones (1000 Purkinje cells).
•Interactions within a micro-zone much stronger than interactions between different micro-zones. 17
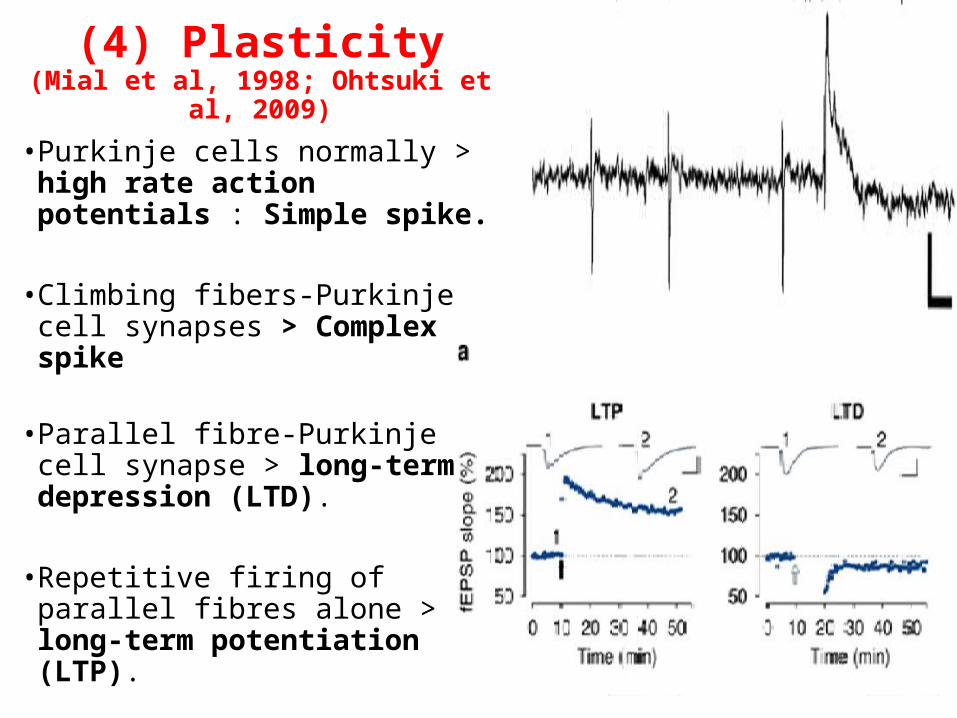
(4) Plasticity(Mial et al, 1998; Ohtsuki et al, 2009)
• Purkinje cells normally > high rate action potentials : Simple spike.
• Climbing fibers-Purkinje cell
synapses > Complex spike
• Parallel fibre-Purkinje cell synapse > long-term depression (LTD).
• Repetitive firing of parallel fibres alone > long-term potentiation (LTP).
18
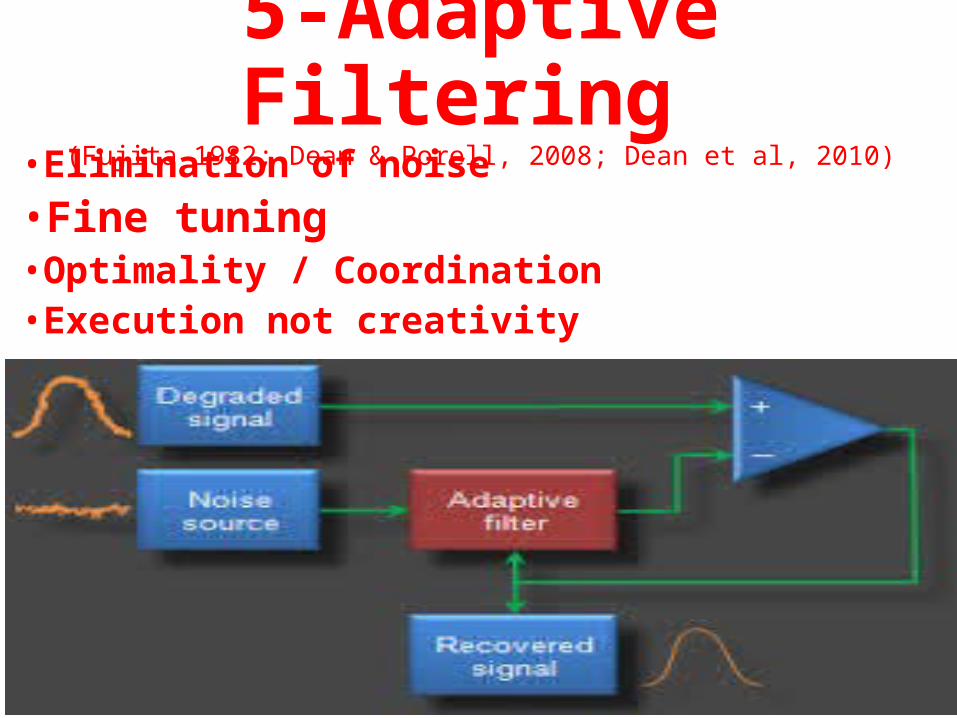
5-Adaptive Filtering (Fujita 1982; Dean & Porell, 2008; Dean et al, 2010)
•Elimination of noise•Fine tuning • Optimality / Coordination•Execution not creativity
19
•Kenji Doya (2000): “Neural computation”. •Katz & Steinmetz (2002): “Regulates brain processes”.•Boydon (2004): “Makes fine adjustments to the way an action is performed”.
•Masao Ito (2005): “Matches intentions with actual performance”.
•Reeber et al (2013):“computational task … recognizing neural patterns … predict optimal movements”. 20Masao Ito
Kenji Doya
Cerebellar Learning: “Software Programmer”
Cerebellar Learning:
(Burguiere et al, 2010, Kalmbach et al, 2011)Cerebellum > does not initiate new learning.> It develops frequently needed learnt behaviour into a Routine with:
1. Minimum Errors2. Minimum Time 3. Minimum Effort 4. Minimum Attention /
awareness5. Maximum Stability 21Chase Britton
Psychiatric Aspects of Cerebellar Disorders
22
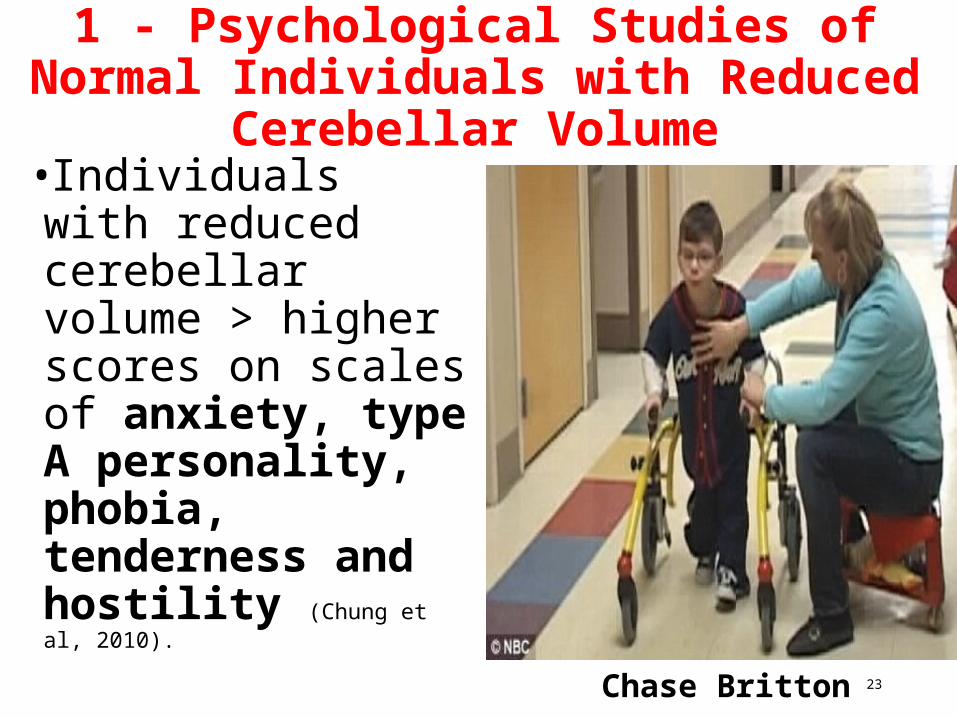
1 - Psychological Studies of Normal Individuals with Reduced Cerebellar
Volume•Individuals with reduced cerebellar volume > higher scores on scales of anxiety, type A personality, phobia, tenderness and hostility (Chung et al, 2010).
23Chase Britton
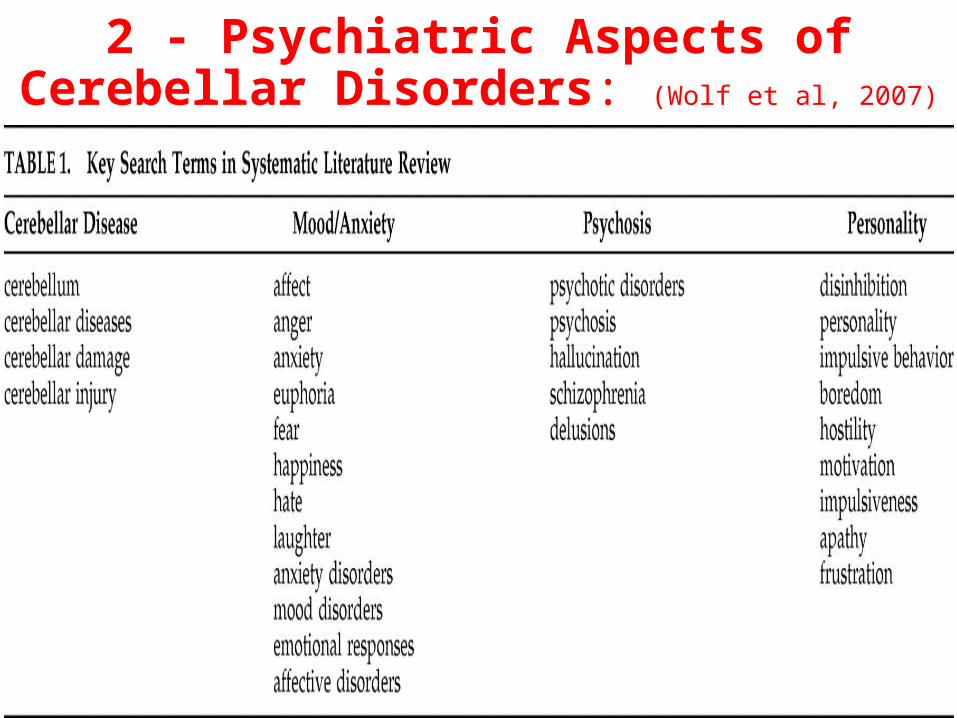
2 - Psychiatric Aspects of Cerebellar Disorders: (Wolf et al, 2007)
24
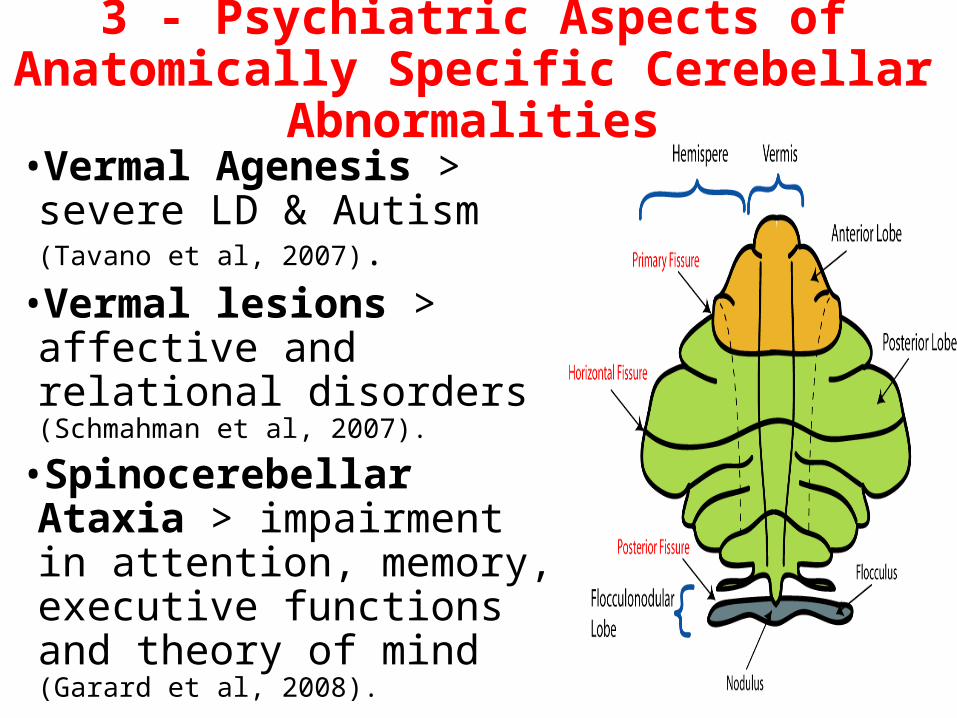
3 - Psychiatric Aspects of Anatomically Specific Cerebellar Abnormalities
•Vermal Agenesis > severe LD & Autism (Tavano et al, 2007).
•Vermal lesions > affective and relational disorders (Schmahman et al, 2007).
•Spinocerebellar Ataxia > impairment in attention, memory, executive functions and theory of mind (Garard et al, 2008).
25
4 - Cerebellar Cognitive Affective Syndrome (Schmahman et al, 2007; Tavano et al, 2007; Levisohn et al, 2000):
26
Cerebellar Syndromes > motor impairments +Cognitive impairments: Executive dysfunctions, visuo-spatial abnormalities, linguistic dysfunction.Affective impairments: Anxiety, lethargy, depression, lack of empathy, ruminativeness, perseveration, anhedonia and aggression.
Jeremy Schmahmann
Cerebellar Abnormalities in Psychiatric Disorders:
General
27
Cerebellar Abnormalities in Psychiatric Disorders
•Bipolar Affective Disorder: e.g. reduced Cerebellar / Vermis volume (Glaser et al, 2006)
•Anxiety: e.g. cerebellar-vestibular dysfunction (Levinson, 1989)
•Depression: e.g. reduced posterior cerebellar activities (Fitzgerald et al, 2009)
28
ADHD: •Smaller cerebellar volume (Berquin et al 1998; Giedd et al, 2001).
•Abnormalities in post-inferior cerebellar hemispheres and vermis (Casey et al, 2007; Steinlin, 2007).
•Reduction in the activity of cerebellum and vermis (Mackie et al, 2007).
Cerebellar Abnormalities in Psychiatric Disorders:
•Post Traumatic Stress Disorder: e.g. altered function of the vermis (Anderson et al, 2002)
•Alcohol abuse: e.g. induced reduction in Cerebellar / Vermis volume (Glaser et al, 2006) 29
•Gender differences: (Dean & McCarthy, 2008)
•Antisocial Personality Disorder: e.g. reduced Cerebellar volume (Barkataki et al, 2006).
•Alzheimer Dementia: e.g. cerebellar atrophy (Wegiel et al, 1999)
Cerebellar Abnormalities in Psychiatric Disorders:
Dyslexia, Schizophrenia & Autism
30
(1) Cerebellum & Dyslexia:•Developmental Dyslexia:
(Stoodley & Stein, 2011; Nicolson et al, 2001; Pernet et al, 2009) •Dyslexia > cerebellar structural and functional abnormalities in 80% of cases.
•Dyslexia > impairment in the ability to perform skills automatically.
•Cerebellar syndromes > impairments in reading and writing characteristic of dyslexia.
31
The Cerebellar Deficit Hypothesis of Dyslexia: (Nicolson & Fawcett, 1990; Nicolson et al,
2001): dyslexia is an impaired automatization of high-order sensory-motor procedures in reading.
(2) Cerebellum & Schizophrenia: General Studies
• ↑ Imaging studies > cerebellar abnormalities in schizophrenia (Vernas et al, 2007):
• ↑ Cerebellar-Motor Dysfunction in Schizophrenia and Psychosis-Risk (Bernard & Mittal, 2014).
• ↓ Cerebellar volume (Bottmer et al, 2005)
• ↓ Blood flow on PET scan (Andreasen et al, 1996).
32
• ↓ Level of N-acetylaspartate in Magnetic Resonance Spectroscopy Imaging (MRSI) studies (marker of neurone density and viability) in vermis and cerebellar cortex (Ende et al, 2005).
• ↓ Volume in the cerebello-thalamic-cortical network (Rusch et al, 2007).
• Neuronal disorganisation in the superior peduncle on Diffusion Tensor Imaging (DTI) studies (Okugawa et al, 2006).
(2) Cerebellum & Schizophrenia: Specific Symptoms (Picard et al, 2008)
•Hallucinations (Shergill et al, 2003; Neckelman et al, 2006)
•Formal Thought Disorder (Kircher et al, 2001; Levitt et al, 1999)
•Affect symptoms (Stip et al, 2005; Paradiso et al, 2003; Abel et al, 2003)
•Cognition (Szesko et al 2003; Toulopoulou et al 2004)
•Attention (Eyler et al, 2004; Honey et al, 2005; Aasen et al, 2005)
•Language (Shergill et al, 2003; Boksman et al 2005; Kircher et al 2005)
•Memory (all types) (Mendrek et al, 2005; Whyte et al 2006)
33
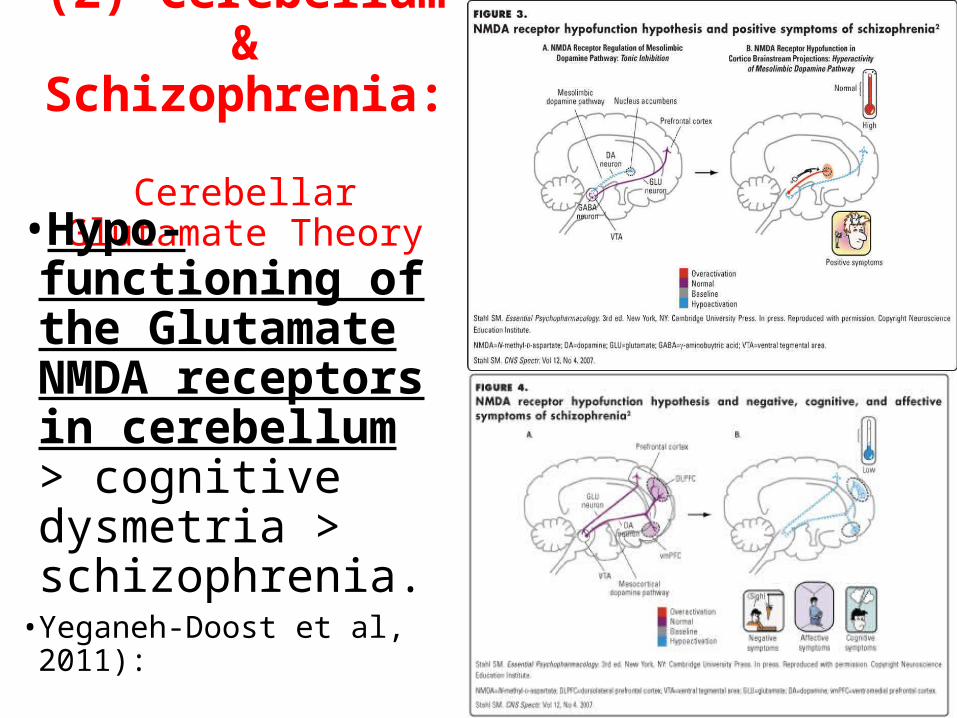
(2) Cerebellum & Schizophrenia: Cerebellar Glutamate
Theory
34
•Hypo-functioning of the Glutamate NMDA receptors in cerebellum > cognitive dysmetria > schizophrenia.
• Yeganeh-Doost et al, 2011):
(2) Cerebellum & Schizophrenia: Cognitive Dysmetria Theory
(Andreasen et al, 1998) •The Cortico-Cerebellar-Thalamo-Cortical circuit is dysfunctional > poor mental coordination > (Cognitive Dysmetria) > Schizophrenia.
•The theory has been criticised by other researchers (e.g. Kaprinis et al, 2002, Kaprinis et al, 2002; Shanagher et al, 2006) Nancy
Andreasen
(2) Cerebellum & Schizophrenia: Secondary Cerebellar Abnormalitites
•Schizophrenia > increased dopaminergic activities > cerebellar disorder > motor disorders in schizophrenia (even neuroleptics naïve) (Mittleman et al, 2008; Hoppenbrouwers et al, 2008; Varambally et al, 2006; Picard et al, 2007).
36
(3) Cerebellar & Autism:General Studies
•One of the most consistent abnormalities found in ASD (DiCicco-Bloom et al, 2006).
• 95% of post mortem examinations of autistic individuals (Delong, 2005)
•Consensus related to cerebellar involvement in autism (Fatemi et al, 2012):
• Abnormal cerebellar anatomy, • Abnormal neurotransmitter systems, • Oxidative stress, • Cerebellar motor and cognitive deficits, • Neuro-inflammation
37
S. Hossein Fatemi
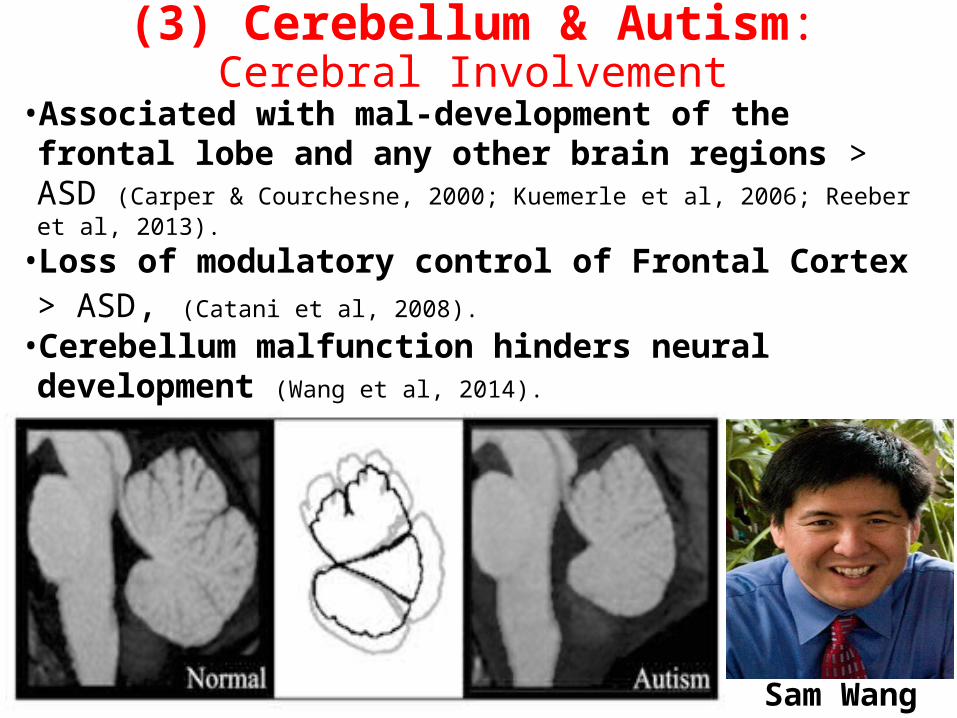
(3) Cerebellum & Autism:Cerebral Involvement
•Associated with mal-development of the frontal lobe and any other brain regions > ASD (Carper & Courchesne, 2000; Kuemerle et al, 2006; Reeber et al, 2013).
•Loss of modulatory control of Frontal Cortex > ASD, (Catani et al, 2008).
• Cerebellum malfunction hinders neural development (Wang et al, 2014).
Sam Wang

Cerebellar Mental Therapies
39
Cerebellar Exercises / Training (Schmahmann, 2010)
• Some claims (e.g. DORE) > Physical exercises (movement + balance) > speed up information processing and improve cerebellar functioning > improve dyslexia, ADHD and Asperger’s syndrome:
• ? Could improve some mental illnesses like schizophrenia . • No known scientific studies. • Controversial treatments (Reynolds & Nicolson, 2007; Bishop,
2007; Rack, 2007)
40

Dance & Movement Therapy(Levi, 1988; Jeong et al, 2005)
41
Cerebellar Transcranial Magnetic Stimulation (TMS) (Schmahmann, 2010)
•Demirtas-Tatlidede et al (2010): stimulation of the vermis in 8 schizophrenic patients > improvements in mood, alertness, memory, attention, visual-spatial skills and energy.
•Very early stages (Minks et al, 2010)
•No RCT
42
Cerebellum: Clinical Reflections
43

Non-motor Dyspraxia
44
Non-motor Dyspraxia•Clumsy expression of, well developed, emotional, social, communication interactions due to difficulties in expression.
•Possible examples: dyslexia and dyscalculia.
•Primarily an “Ideomotor or Executive Dyspraxia” rather than “Ideational or Planning Dyspraxia” (Gibbs et al 2007).
45
Routine Disorders
46
Routine Disorders vs Dyspraxia•Dyspraxia does not usually include complex behavioural patterns that, coordinated by cerebellum, e.g. “Habits” and “Routines”.
•This seems to be the case with other similar clinical conditions as they are manly describe motor performance problems e.g. • The Clumsy Child Syndrome• Minimal Brain Dysfunction (MBD)• Developmental Apraxia• Specific developmental disorder of motor function (ICD-10)
• Developmental Coordination Disorder (DCD) (DSM-5). 47
•Most of daily behaviour for adults are made of learnt routines (habits) (Betsch et al, 2001; Beach & Potter, 1992).
•biologically, Routines are the main product or expression of the brain and cerebellum functioning.
•Explain many aspects of learning, coping, health, pathology, future choices and therapy (Bernacer & Murillo, 2014). 48
Routines : Clinical Perspectives
Routines : Clinical Perspectives
“Routines” are written in a book designed by cerebrum and written by cerebellum.The book contain thousands if not millions of routine > defining the individual. •Neurological (motor) disorders > like misprints of the book.•Routine disorders > like discovering wrong chapters in the book.
49
Healthy Routines vs Routine Disorders
50
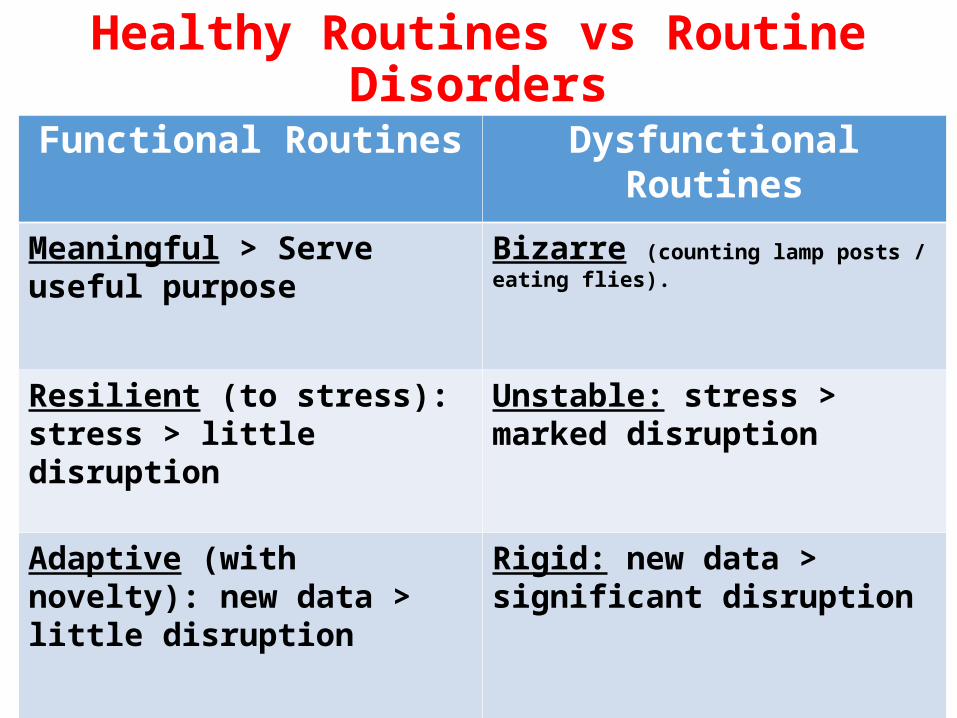
Functional Routines Dysfunctional Routines
Meaningful > Serve useful purpose
Bizarre (counting lamp posts / eating flies).
Resilient (to stress): stress > little disruption
Unstable: stress > marked disruption
Adaptive (with novelty): new data > little disruption
Rigid: new data > significant disruption
Cerebellar Circuits and Mental Disorders
51

Cerebellar Circuits of Learnt Behaviour
•Best way to understand Cerebellar Circuits of Learnt Behaviour > follow motor cerebellar learning:•Well studied•Must be linked physiologically to non-motor functioning.
52
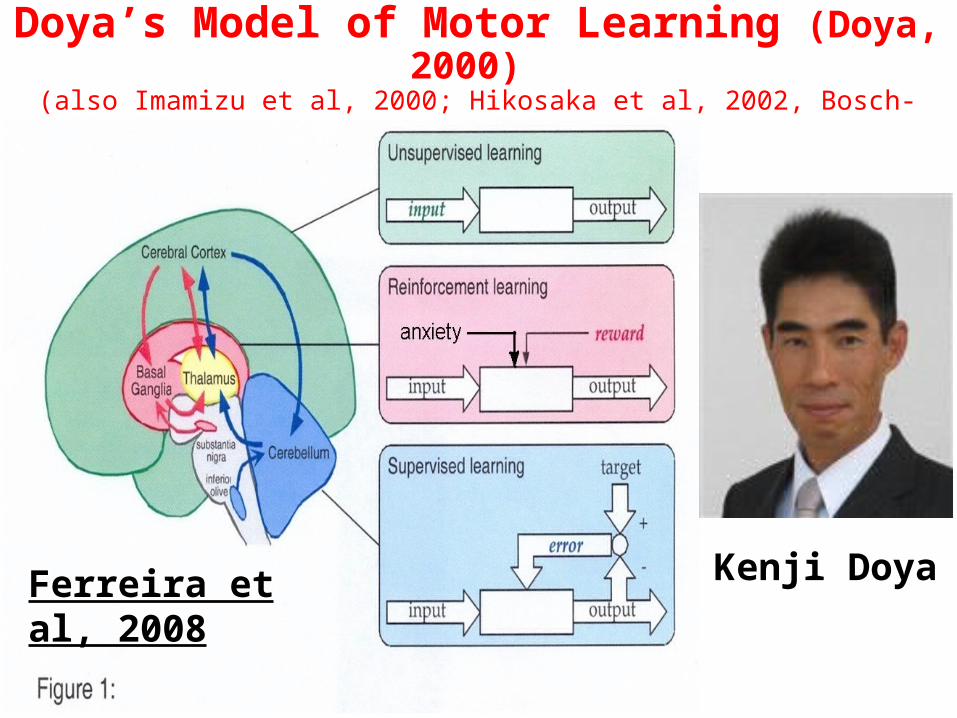
Doya’s Model of Motor Learning (Doya, 2000) (also Imamizu et al, 2000; Hikosaka et al, 2002, Bosch-Bouju et al, 2013)
Kenji DoyaFerreira et al, 2008
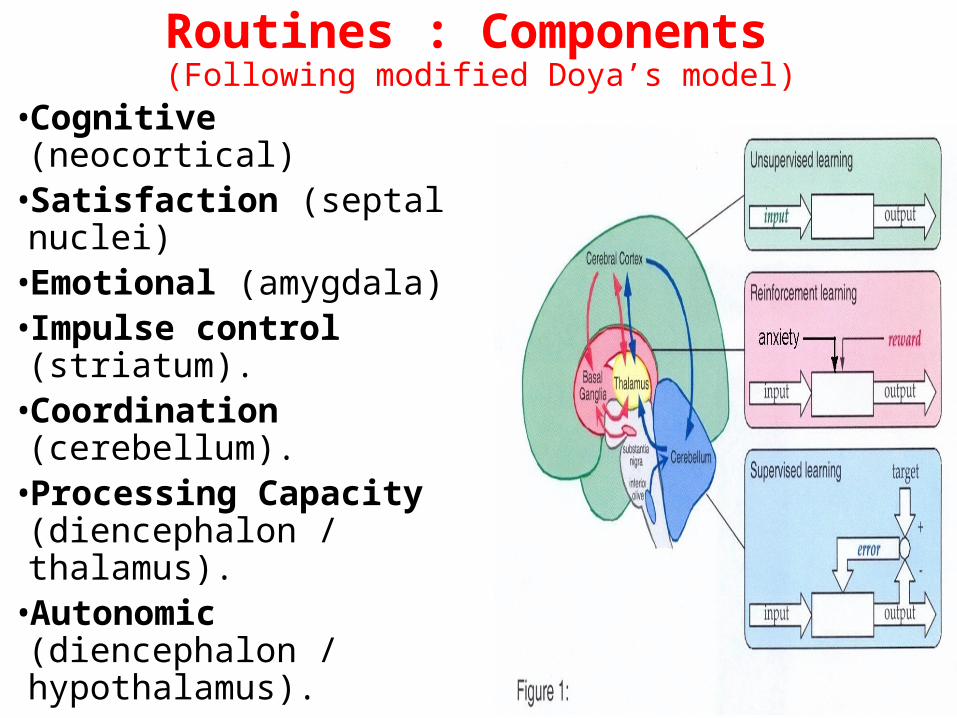
Routines : Components (Following modified Doya’s model)
•Cognitive (neocortical)•Satisfaction (septal nuclei)•Emotional (amygdala)•Impulse control (striatum).
•Coordination (cerebellum).
•Processing Capacity (diencephalon / thalamus).
•Autonomic (diencephalon / hypothalamus). 54
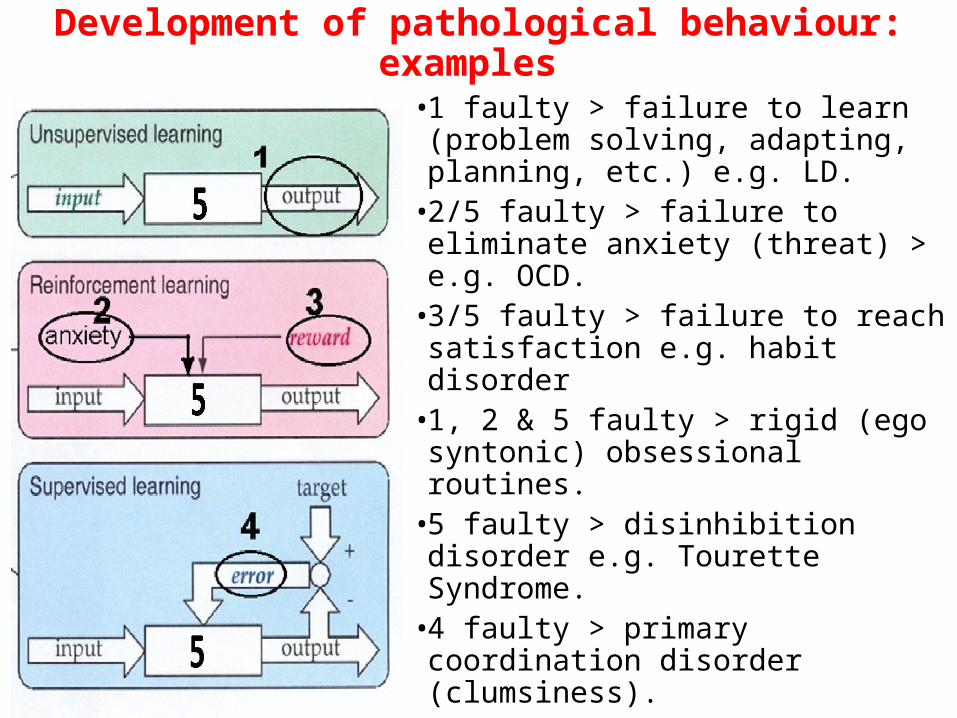
Development of pathological behaviour: examples
•1 faulty > failure to learn (problem solving, adapting, planning, etc.) e.g. LD.
•2/5 faulty > failure to eliminate anxiety (threat) > e.g. OCD.
•3/5 faulty > failure to reach satisfaction e.g. habit disorder
•1, 2 & 5 faulty > rigid (ego syntonic) obsessional routines.
•5 faulty > disinhibition disorder e.g. Tourette Syndrome.
•4 faulty > primary coordination disorder (clumsiness).
Development of Biological Disorders from Stress
- Stress effects on the brain > Cerebellum to create circuits that enhance pathological responses.- This explain how stress
reactions turn by cerebellum into biologically based pathology.
- Also explains how originally stress related behaviours can later become treatable by psychiatric medications through changing brain chemistry. 56

57
Thank you
Comments