clinical, histological and genetic investigation of buschke–fischer–brauer's disease in...
TRANSCRIPT

Letters to the Editor / Journal of Dermatological Science 54 (2009) 43–6354
tacrolimus on GLI1 expression, and provide strength to thehypothesis that GLI1 regulates the expression of BCL-2 and ofbasal lamina molecules including laminin.
Acknowledgements
This paper is devoted to the memory of Paolo Carli, M.D., whopassed away on April 6, 2007, while the results of this research,that had been launched and strongly promoted by him, were stillgenerated.
Additional funds were provided by the University of Florenceand by Tuscany region (project TRESOR—scientific director Prof. M.Serio).
Appendix A. Supplementary data
Supplementary data associated with this article can be found, in
the online version, at doi:10.1016/j.jdermsci.2008.10.006.
Conflict of interest
The study was supported in part by Fujisawa GmbH (Munich,Germany), now Astellas Europe (Staines, UK).
References
[1] Villavicencio EH, Walterhouse DO, Iannaccone PM. The sonic hedgehog-patched-gli pathway in human development and disease. Am J Hum Genet2000;67:1047–54.
[2] Ghali L, Wong ST, Green J, Tidman N, Quinn AG. Gli1 protein is expressed inbasal cell carcinomas, outer root sheath keratinocytes and a subpopulation ofmesenchymal cells in normal human skin. J Invest Dermatol 1999;113:595–9.
[3] Green J, Leigh IM, Poulsom R, Quinn AG. Basal cell carcinoma development isassociated with induction of the expression of the transcription factor Gli-1. BrJ Dermatol 1998;139:911–5.
[4] Hatta N, Hirano T, Kimura T, Hashimoto K, Mehregan DR, Ansai S, et al.Molecular diagnosis of basal cell carcinoma and other basaloid cell neoplasmsof the skin by the quantification of Gli1 transcript levels. J Cutan Pathol2005;32:131–6.
[5] Goto T, Kino T, Hatanaka H, Nishiyama M, Okuhara M, Kohsaka M, et al.Discovery of FK-506, a novel immunosuppressant isolated from Streptomycestsukubaensis. Transplant Proc 1987;19:4–8.
[6] Kim A, DiCarlo J, Cohen C, McCall C, Johnson D, McAlpine B, et al. Are keloidsreally ‘‘gli-loids’’?: High-level expression of gli-1 oncogene in keloids. J AmAcad Dermatol 2001;45:707–11.
A R T I C L E I N F O
Keywords:
Palmoplantar keratoderma; Punctate PPK;
Haplotype; Linkage analysis
[7] Macaron NC, Cohen C, Chen SC, Arbiser JL. GLI-1 oncogene is highly expressedin granulomatous skin disorders, including sarcoidosis, granuloma annulare,and necrobiosis lipoidica diabeticorum. Arch Dermatol 2005;141:259–62.
[8] Zhan M, Zhao H, Han ZC. Signalling mechanisms of anoikis. Histol Histopathol2004;19:973–83.
[9] Evans AV. The expanding role of topical tacrolimus in dermatology. Clin ExpDermatol 2005;30:111–5.
[10] Niwa Y, Terashima T, Sumi H. Topical application of the immunosuppressanttacrolimus accelerates carcinogenesis in mouse skin. Br J Dermatol2003;149:960–7.
P. Di Gennaroa
R. Sestinib
S. Baccia
A. Pacinia
P. PinzaniL. Domenicia
A. Toscanoa
D. Massic
P. Carlid
M. Genuardib
P. Romagnolia,*
aDepartment of Anatomy, Histology, and Forensic Medicine,
University of Florence, Viale Pieraccini 6, Florence 50139, ItalybDepartment of Clinical Physiopathology, University of Florence,
Viale Pieraccini 6, Florence 50139, ItalycDepartment of Human Pathology and Oncology,
University of Florence, Viale Morgagni 85,
Florence 50134, ItalydDepartment of Dermatological Sciences, University of Florence,
Via della Pergola 58-64, Florence 50121, Italy
*Corresponding author. Tel.: +39 055 4271389;fax: +39 055 4271385
E-mail address: [email protected]
13 May 20086 October 2008
25 October 2008
doi:10.1016/j.jdermsci.2008.10.006
Letter to the Editor
Clinical, histological and genetic investigation of Buschke–Fischer–Brauer’s disease in Tunisian families
Dear Editor,
Buschke–Fischer–Brauer’s disease or the type I of punctate PPK(MIM 148600) is a rare hereditary skin disease that is usuallyinherited as an autosomal dominant trait and its incidence wasreported as 1.17/100,000 inhabitants in Croatia [1].
Punctate PPK is characterized by multiple punctate keratosesover the entire palmoplantar surfaces. The age of onset ranged
between 12 and 30 years [2]. The molecular basis of punctate PPK isstill unknown. Recently, two punctate PPK loci were found to mapto 15q22–15q24 and to 8q24.13–8q24.21 [3,4]. However, in arecent study, Gao et al. failed to confirm genetic linkage to theirprevious locus on 8q and showed significant evidence for linkage to15q22–15q24 (9.98 cM). This candidate region was reduced to5.06 cM on 15q22.2–15q22.31 [5].
In the present study, we report the clinical, histological andgenetic findings in five Tunisian families (PPK1 to PPK5) with atotal of 15 patients (6 women and 9 men). The diagnosis wasestablished based on clinical examination and confirmed byhistopathological findings. The explored patients exhibited classi-cal PPK phenotype and a positive family history was observedwhich confirmed the autosomal mode of transmission of thedisease in informative families. Patients presented with hyperker-atosis and verrucoid punctate lesions on the palmoplantar area.Lesions were yellowish, of 2–3 mm in diameter and usuallycoalesce on the soles subject to continuous high pressure. Therewas no nail involvement. The age of onset of the disease rangedfrom 10 to 35 years. However, for the patient (IV-1) in family PPK1,
Letters to the Editor / Journal of Dermatological Science 54 (2009) 43–63 55
the lesions started to appear by the fifth decade. Such occurrencewas described in one patient reported by Emmert et al. [6] whodeveloped the lesions at the sixth decade and at the fourth decadein another patient reported by Al-Mutairi et al. [7].
Although several groups have reported association of punctatePPK with malignancies, we did not observe any type of malignancyassociated with type I punctate PPK on the examined Tunisianpatients. Special clinical findings were observed in the studiedfamilies. There was occurrence of punctate PPK with moderatehearing impairment in three members within family PPK2 (III-1,IV-1 and IV-2). Mutational analysis of the coding exon of the GJB2
gene showed no mutation in this gene. Clinical association of thepunctate PPK with sensorineural hearing loss has been recentlyreported [8]. Probands III-1 in pedigree PPK2, II-1 in family PPK3and II-1 in family PPK4 presented clinical association of punctatePPK with ichthyosis vulgaris. Recently, association of punctate PPKwith other dermatological manifestations (psoriasis) was reported[7] but association with ichthyosis has not been previouslydescribed. This co-occurrence could be fortuitous because of thehigh prevalence of this type of ichthyosis worldwide.
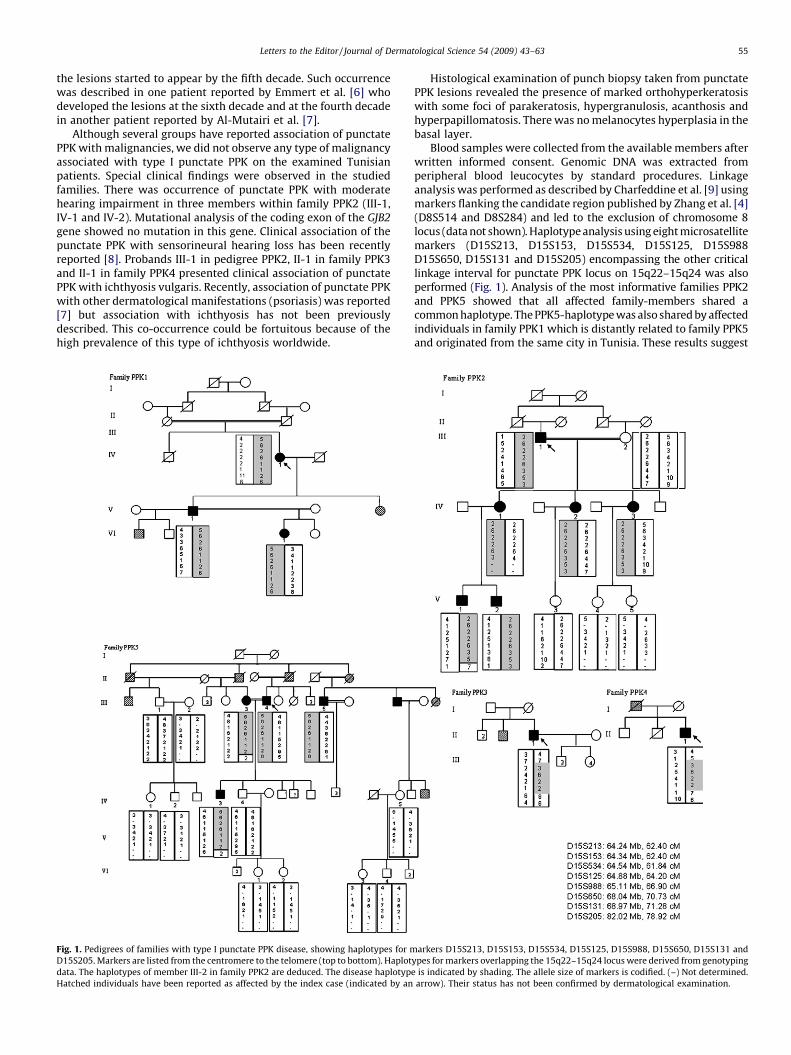
Fig. 1. Pedigrees of families with type I punctate PPK disease, showing haplotypes for m
D15S205. Markers are listed from the centromere to the telomere (top to bottom). Haplot
data. The haplotypes of member III-2 in family PPK2 are deduced. The disease haplotyp
Hatched individuals have been reported as affected by the index case (indicated by an
Histological examination of punch biopsy taken from punctatePPK lesions revealed the presence of marked orthohyperkeratosiswith some foci of parakeratosis, hypergranulosis, acanthosis andhyperpapillomatosis. There was no melanocytes hyperplasia in thebasal layer.
Blood samples were collected from the available members afterwritten informed consent. Genomic DNA was extracted fromperipheral blood leucocytes by standard procedures. Linkageanalysis was performed as described by Charfeddine et al. [9] usingmarkers flanking the candidate region published by Zhang et al. [4](D8S514 and D8S284) and led to the exclusion of chromosome 8locus (data not shown). Haplotype analysis using eight microsatellitemarkers (D15S213, D15S153, D15S534, D15S125, D15S988D15S650, D15S131 and D15S205) encompassing the other criticallinkage interval for punctate PPK locus on 15q22–15q24 was alsoperformed (Fig. 1). Analysis of the most informative families PPK2and PPK5 showed that all affected family-members shared acommon haplotype. The PPK5-haplotype was also shared by affectedindividuals in family PPK1 which is distantly related to family PPK5and originated from the same city in Tunisia. These results suggest
arkers D15S213, D15S153, D15S534, D15S125, D15S988, D15S650, D15S131 and
ypes for markers overlapping the 15q22–15q24 locus were derived from genotyping
e is indicated by shading. The allele size of markers is codified. (–) Not determined.
arrow). Their status has not been confirmed by dermatological examination.

Letters to the Editor / Journal of Dermatological Science 54 (2009) 43–6356
that the Tunisian families are likely linked to the previouslyidentified critical 15q22–15q24 interval. For families PPK3 andPPK4, no other cases could be investigated. Nevertheless, it isnoteworthy that the two patients belonging to these families shareda common haplotype between markers D15S534 and D15S650.
Parametric multipoint linkage analysis gave the maximumcumulative lod score value of 5.33 for marker D15S650. Theseresults support genetic linkage of the PPK-families to the testedcritical interval on 15q22–15q24.
It is noteworthy that in family PPK2, individuals IV-1 and IV-2born to a consanguineous marriage were homozygous for theinterval between microsatellite markers D15S213 and D15S988;this segment is likely inherited from a common ancestor. As theirmother III-2 was healthy, this suggests that the disease locusshould be distal to marker D15S988.
In the present study, we provide confirmatory evidence for thelocation of the punctate PPK in 15q22–15q24 although the precisegene interval should be reconsidered when compared to the studyof Gao et al. that suggested that the disease is proximal to D15S988,based on recombinant healthy individuals [5].
To our knowledge, this is the first report of Buschke–Fischer–Brauer’s disease in North African families.
Acknowledgements
We are especially grateful to the patients and their familymembers for their interest and cooperation in this study. This workwas supported by the Tunisian Ministry of Higher Education andScientific Research (Research Unit on ‘‘Molecular Investigation ofGenetic Orphan Disorders’’ UR 26/04 and Research Unit on‘‘Hereditary Keratinisation Disorders’’ UR 24/04) and the Ministryof Health.
References
[1] Stanimirovic A, Kansky A, Basta-Juzbasic A, Skerlev M, Beck T. Hereditarypalmoplantar keratoderma, type papulosa, in Croatia. J Am Acad Dermatol1993;29:435–7.
[2] Stevens HP, Kelsell DP, Leigh IM, Ostlere LS, MacDermot KD, Rustin MH.Punctate palmoplantar keratoderma and malignancy in a four-generationfamily. Br J Dermatol 1996;134:720–6.
[3] Martinez-Mir A, Zlotogorski A, Londono D, Gordon D, Grunn A, Uribe E, et al.Identification of a locus for type I punctate palmoplantar keratoderma onchromosome 15q22–q24. J Med Genet 2003;40:872–8.
[4] Zhang XJ, Li M, Gao TW, He PP, Wei SC, Liu JB, et al. Identification of a locus forpunctate palmoplantar keratodermas at chromosome 8q24.13–8q24.21. JInvest Dermatol 2004;122:1121–5.
A R T I C L E I N F O
Keywords:
Prototheca zopfii; Protothecosis; Nested
PCR; Nuclear small subunit ribosomal DNA
[5] Gao M, Yang S, Li M, Yan KL, Jiang YX, Cui Y, et al. Refined localization of apunctate palmoplantar keratoderma gene to a 5.06-cM region at 15q22.2–15q22.31. Br J Dermatol 2005;152:874–8.
[6] Emmert S, Kuster W, Hennies HC, Zutt M, Haenssle H, Kretschmer L, et al. 47patients in 14 families with the rare genodermatosis keratosis punctatapalmoplantaris Buschke–Fischer–Brauer. Eur J Dermatol 2003;13:16–20.
[7] Al-Mutairi N, Joshi A, Nour-Eldin O. Punctate palmoplantar keratoderma(Buschke–Fischer–Brauer disease) with psoriasis: a rare associationshowing excellent response to acitretin. J Drugs Dermatol 2005;4:627–34.
[8] Erkek E, Erdogan S, Tuncez F, Kurtipek GS, Bagci Y, Ozoguz P, et al. Type Ihereditary punctate keratoderma associated with widespread lentigo simplexand successfully treated with low-dose oral acitretin. Arch Dermatol2006;142:1076–7.
[9] Charfeddine C, Mokni M, Ben Mousli R, Elkares R, Bouchlaka C, Boubaker S, et al.A novel missense mutation in the gene encoding SLURP-1 in patients with Malde Meleda from northern Tunisia. Br J Dermatol 2003;149:1108–15.
Mbarka Bchetniaa,b
Cherine Charfeddinea
Selma Kassarb,c
Imen Hanchid
Haifa Tounsi-Guettitic
Ahmed Rebaie
Amel Dhahri-Ben Osmand
Christian Kubischf
Sonia Abdelhaka,*
Samir Boubakerc
Mourad Moknib,d
a‘‘Molecular Investigation of Genetic Orphan Diseases’’ Research Unit,
Institut Pasteur de Tunis, Tunis, Tunisiab‘‘Hereditary Keratinization Disorders’’ Research Unit,
Hopital La Rabta de Tunis, Tunis, TunisiacPathology Department, Institut Pasteur de Tunis, Tunis, Tunisia
dDermatology Department, Hopital La Rabta, Tunis, TunisiaeBioinformatic department, Centre de Biotechnologie de Sfax, Sfax,
TunisiafInstitute of Human Genetics, University Hospital Cologne, Germany
*Corresponding author at: Institut Pasteur de Tunis, BP 74, 13 Place,Pasteur, 1002 Tunis, Belvedere, Tunisia. Tel.: +216 71 849110;
fax: +216 71 791833E-mail addresses: [email protected];
[email protected] (S. Abdelhak)
doi:10.1016/j.jdermsci.2008.11.008
Letter to the editor
Rapid identification of Prototheca zopfii by nested polymerasechain reaction based on the nuclear small subunit ribosomalDNA
The genus of achlorophyllous unicellular algae, Prototheca
was first described in 1894 by Kruger [1,2], and shown to have asimilar life cycle to algae from the genus Chlorella. P. zopfii andP. wickerhamii has been reported as a pathogen involved inrefractory subcutaneous disease and systemic infection in humans
and in animals [2–4]. Especially, P. zopfii causes bovine mastitis andcanine fatal systemic infection, which have recently become majorworldwide problems [4,5]. Recently, the incidences of P. zopfii
infection have been increasing rapidly in both cattle and humans[2–5]. Therefore, a system to effectively and rapidly identify thepathogen in infected cattle or humans is necessary. P. wickerhamii
is another pathogen belonging to this genus, and P. wickerhamii
infections are relatively easily treated with antifungal agents,especially amphotericin B. However, the prognosis of subcuta-neous infection with P. zopfii is poor, even though this alga issensitive to azoles in vitro [2]. One reason for this is the difficulty inidentifying the alga and thus in selection of effective antifungalagents.
Here, the specific nested PCR system was evaluated withreference strains from Japanese culture collections and isolatesfrom bovine mastitis. To our knowledge, this is the first report of amolecular identification system for this pathogenic alga.