colour flow duplex imaging in veno-lymphatic ulcer a. cavezzi s.benedetto del tronto, bologna
TRANSCRIPT

COLOUR FLOW DUPLEX COLOUR FLOW DUPLEX IMAGINGIMAGING
IN VENO-LYMPHATIC ULCER IN VENO-LYMPHATIC ULCER
A. Cavezzi A. Cavezzi
S.Benedetto del Tronto, BolognaS.Benedetto del Tronto, Bolognawww.cavezzi.itwww.cavezzi.it

PHLEBO-LYMPHOPATHIC ULCER PHLEBO-LYMPHOPATHIC ULCER Causes: Causes:
- Secondary Deep Venous Insufficiency- Secondary Deep Venous Insufficiency (Post-thrombotic syndrome) or Primary Deep (Post-thrombotic syndrome) or Primary Deep Venous InsufficiencyVenous Insufficiency
- Superficial Venous Insufficiency Superficial Venous Insufficiency
- Functional Venous Insufficiency: Muscle-Functional Venous Insufficiency: Muscle-Vascular Pump dysfunction, obesity, etc.Vascular Pump dysfunction, obesity, etc.
- Lymphatic DysfunctionLymphatic Dysfunction
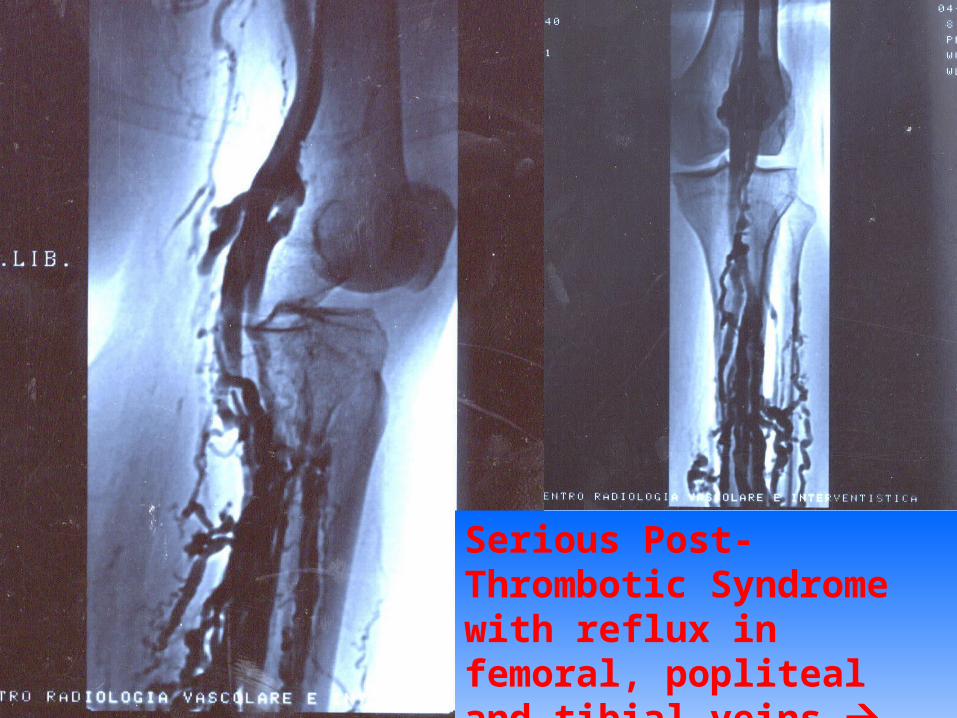
Serious Post-Thrombotic Syndrome with reflux in femoral, popliteal and tibial veins supra-malleolar ulcer
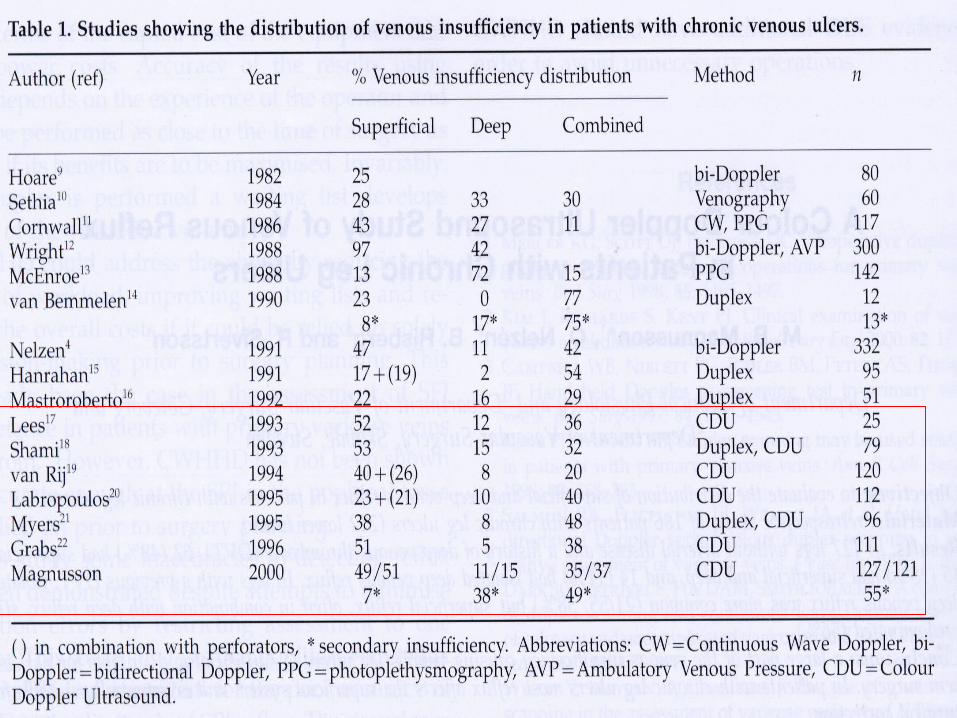
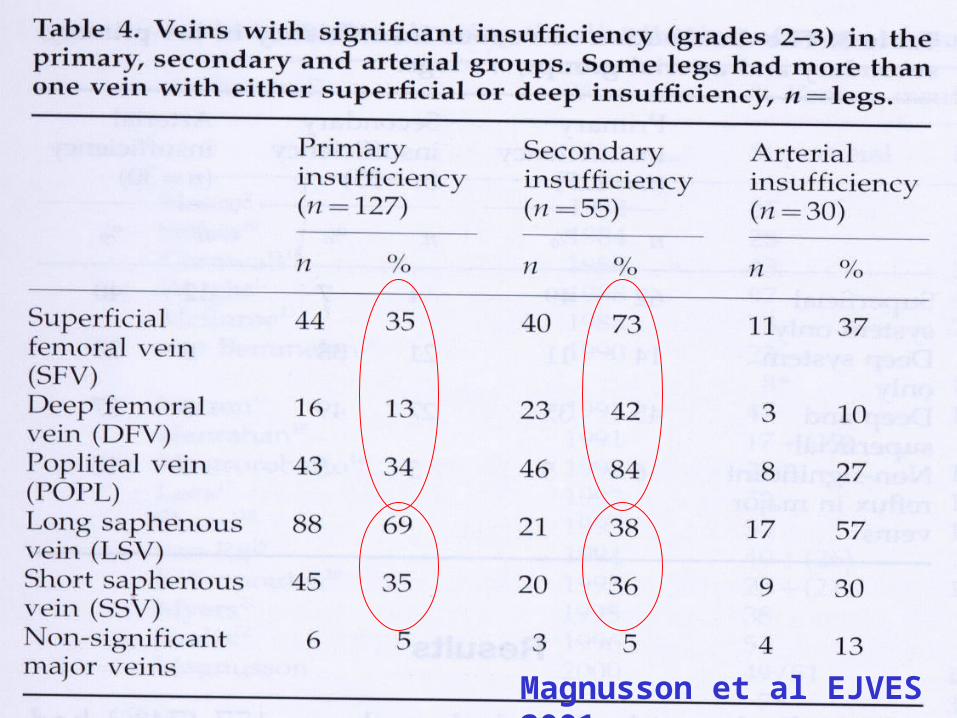
Magnusson et al EJVES 2001
LITERATURE DATALITERATURE DATA
A)A) MetanalysisMetanalysis 1980-1998 (1249 limbs with venous ulcers) 1980-1998 (1249 limbs with venous ulcers) * 92% with reflux, 8% without reflux * 92% with reflux, 8% without reflux * 45% reflux only in SVS, 12% reflux only in DVS, 43% * 45% reflux only in SVS, 12% reflux only in DVS, 43% reflux in SVS and DVS reflux in SVS and DVS (Tassiopoulos AK, Golts E, Oh DS, Labropoulos N., (Tassiopoulos AK, Golts E, Oh DS, Labropoulos N., EJVES )EJVES )
B)B) L’incompetence of popliteal vein is a negative prognostic factor L’incompetence of popliteal vein is a negative prognostic factor for ulcer healing (42 vs 10% ) for ulcer healing (42 vs 10% ) ( Brittenden J, Bradbury AW, Allan PL, Prescott RJ, Harper ( Brittenden J, Bradbury AW, Allan PL, Prescott RJ, Harper DR, Ruckley CV, Br J Surg)DR, Ruckley CV, Br J Surg)
C) Limbs with venos ulcer, in confrontation with healthy limbs, C) Limbs with venos ulcer, in confrontation with healthy limbs, have a decreased ejection fraction and an increased post-exercise have a decreased ejection fraction and an increased post-exercise residual (pump dysfunction..) residual (pump dysfunction..) (Araki CT, Back TL, Padberg FT, Thompson PN, Jamil Z, Lee (Araki CT, Back TL, Padberg FT, Thompson PN, Jamil Z, Lee BC, Duran WN, Hobson RW; J Vasc Surg)BC, Duran WN, Hobson RW; J Vasc Surg)

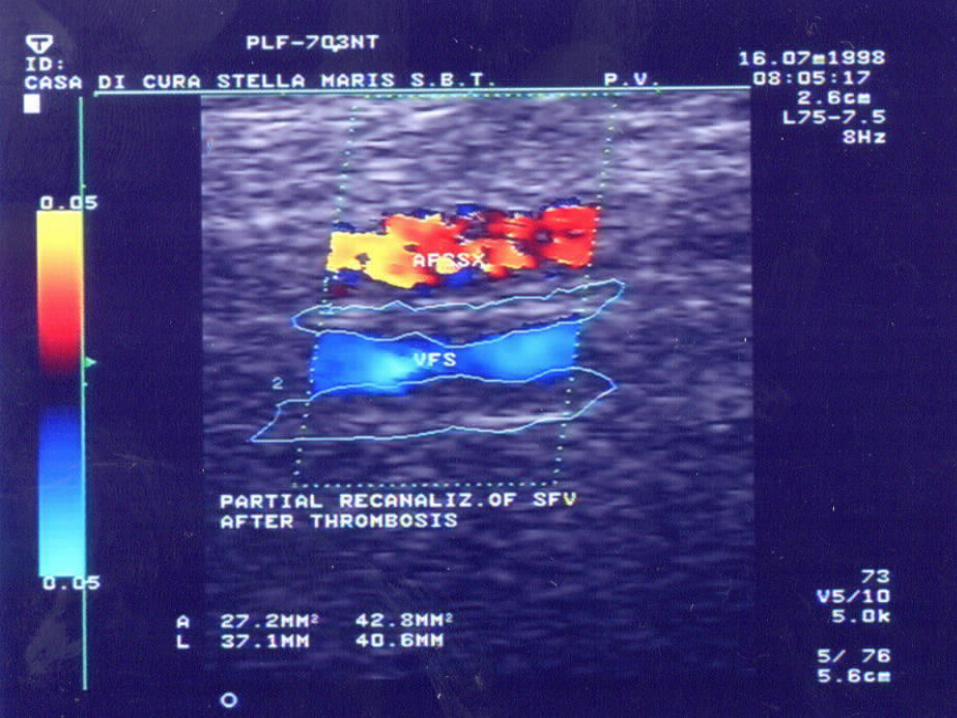
CFDI AND SECONDARY DEEP CFDI AND SECONDARY DEEP VENOUS INSUFFICIENCY VENOUS INSUFFICIENCY - POST-THROMBOTIC SYNDROME -- POST-THROMBOTIC SYNDROME -
- possible persistent occlusions (8%) - possible persistent occlusions (8%) - reflux due to post-thrombotic - reflux due to post-thrombotic valvular incompetence (33% isolated, valvular incompetence (33% isolated, 50% with thrombotic sub-occlusive 50% with thrombotic sub-occlusive changes) - changes) - morphologic and functional state of morphologic and functional state of saphenous stems and of perforators saphenous stems and of perforators - dilatation of collateral branches - dilatation of collateral branches

POST-THROMBOTIC SYNDROMEPOST-THROMBOTIC SYNDROME

S.P.T.: DIFFERENZA ECOGRAFICA TESSUTI IN SEDE SOPRA (SX) ED ENTRO (DX) DISTROFIE CUTANEE
S.P.T. - Stenosi V. Iliaca Esterna S.P.T. - Stenosi V. Iliaca Esterna
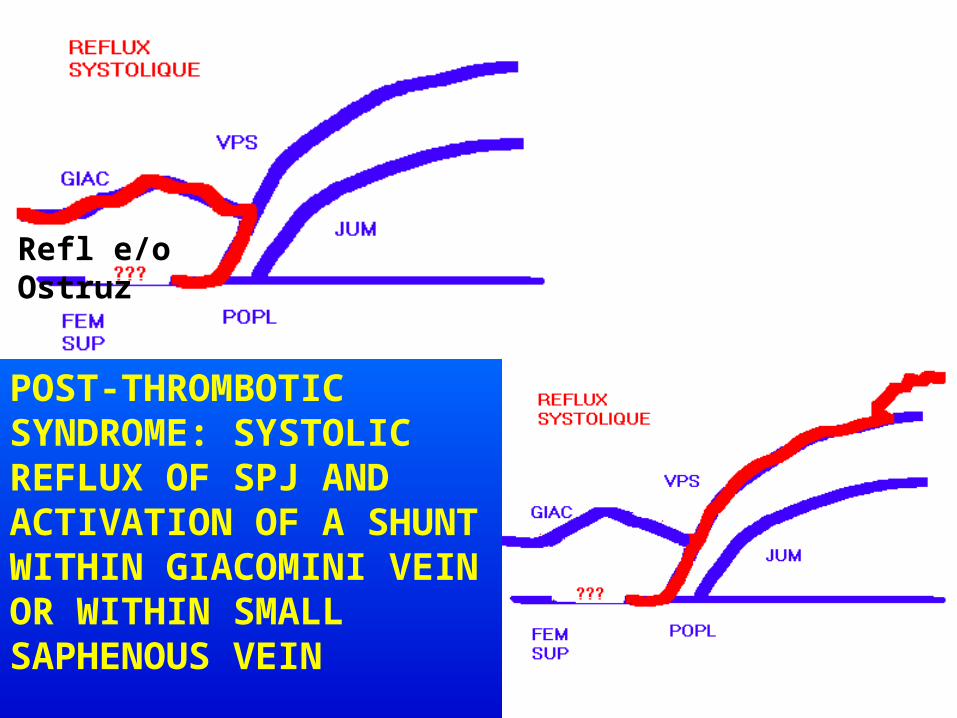
POST-THROMBOTIC SYNDROME: SYSTOLIC REFLUX OF SPJ AND ACTIVATION OF A SHUNT WITHIN GIACOMINI VEIN OR WITHIN SMALL SAPHENOUS VEIN
Refl e/o Ostruz
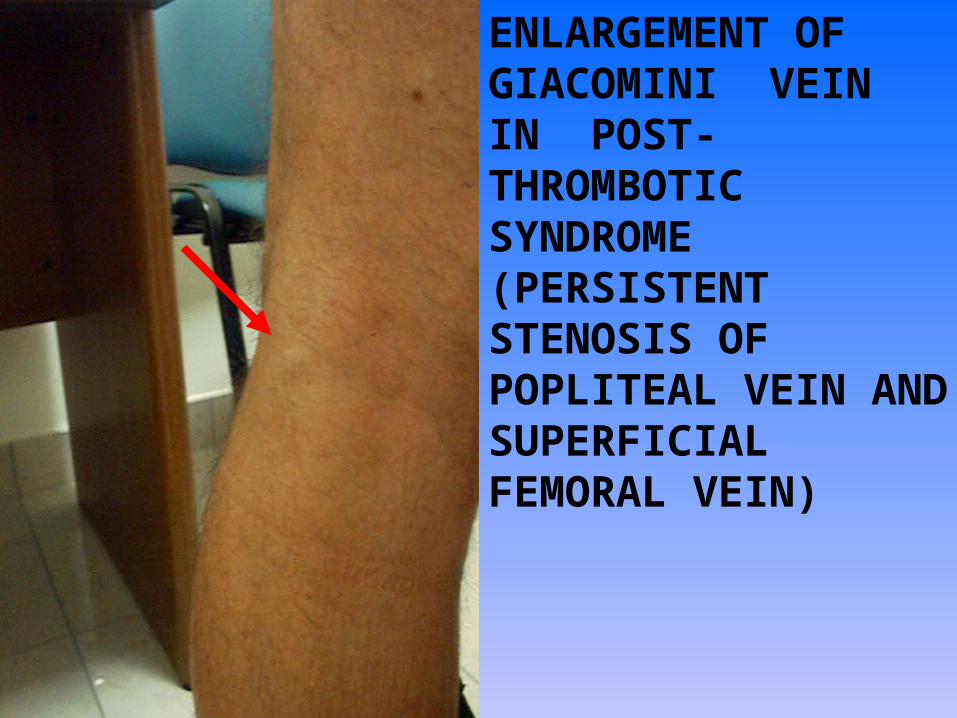
ENLARGEMENT OF GIACOMINI VEIN IN POST-THROMBOTIC SYNDROME (PERSISTENT STENOSIS OF POPLITEAL VEIN AND SUPERFICIAL FEMORAL VEIN)
CFDI AND SUPERFICIAL VENOUS CFDI AND SUPERFICIAL VENOUS INSUFFICIENCYINSUFFICIENCY
- Reflux/Retrograde flow in saphenous stemsReflux/Retrograde flow in saphenous stems
- Incompetence of saphenous junctions or Incompetence of saphenous junctions or extra-junction refluxesextra-junction refluxes
- Morphologic and haemodynamic state of Morphologic and haemodynamic state of perforatorsperforators
-Patency and competence of deep veinsPatency and competence of deep veins

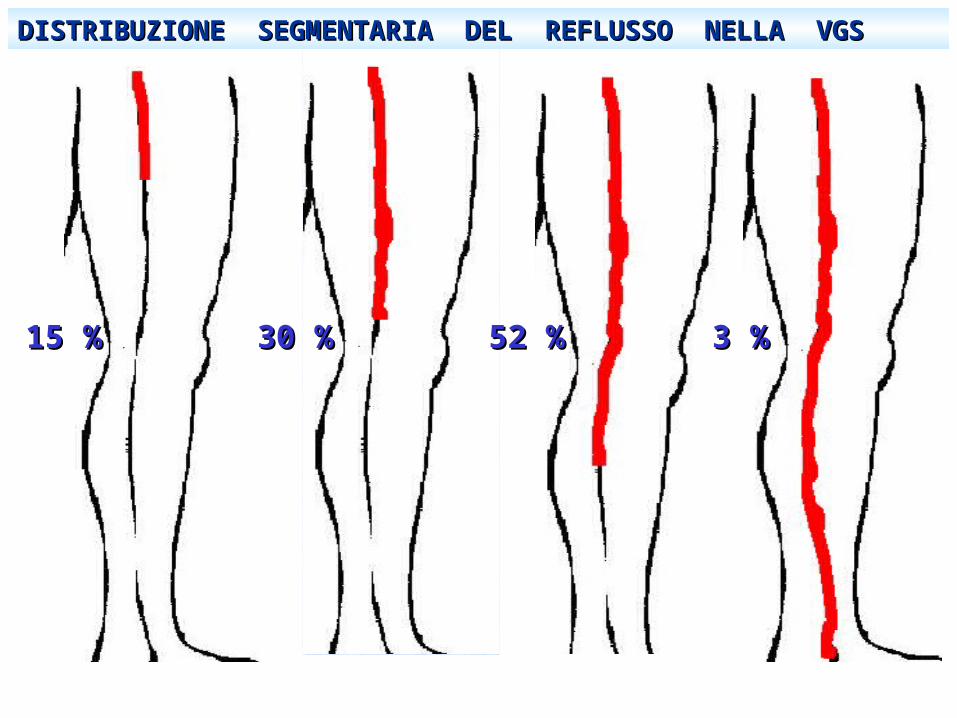
DISTRIBUZIONE SEGMENTARIA DEL REFLUSSO NELLA VGSDISTRIBUZIONE SEGMENTARIA DEL REFLUSSO NELLA VGS
15 %15 % 30 %30 % 52 %52 % 3 %3 %

FROM BJORDAL ….1971…..FROM BJORDAL ….1971…..
PERFORATING VEINS : THEIR ROLE PERFORATING VEINS : THEIR ROLE
IN PRIMARY VARICOSE VEINSIN PRIMARY VARICOSE VEINS • In primary varicose veins the majority of PV in the leg In primary varicose veins the majority of PV in the leg
has a main or single role of re-entry in the deep venous has a main or single role of re-entry in the deep venous systemsystem
• Bi-directional flow in PV means incompetence, but not Bi-directional flow in PV means incompetence, but not always pathogenicity: in the “terminal” PVs of the leg always pathogenicity: in the “terminal” PVs of the leg the balance (the net flow) of the bi-directional flow in the balance (the net flow) of the bi-directional flow in the systolic phase (calf contraction) and in the diastolic the systolic phase (calf contraction) and in the diastolic phase (calf relaxation) is largely in favour of the re-entry phase (calf relaxation) is largely in favour of the re-entry in the DVS: the PV may be incompetent, but it is not in the DVS: the PV may be incompetent, but it is not pathologic …pathologic …
(Perthes, Bjordal, Bassi, Tibbs, Franceschi (Perthes, Bjordal, Bassi, Tibbs, Franceschi etc.)etc.)

BASIC KNOWLEDGE ABOUT BASIC KNOWLEDGE ABOUT PERFORATORS PERFORATORS
a) healthy subjects may have bi-directional flow a) healthy subjects may have bi-directional flow (which were traditionally considered as pathologic (which were traditionally considered as pathologic
in the past literature ) in 20-30% of the limbs in the past literature ) in 20-30% of the limbs
(Coleridge- Smith et al.)(Coleridge- Smith et al.)
b) up to 50% of the perforators in the calf have NO b) up to 50% of the perforators in the calf have NO valves…. , thus favoring an inflow or an outflow valves…. , thus favoring an inflow or an outflow
according to the pressure gradients in the according to the pressure gradients in the superficial and deep venous compartmentssuperficial and deep venous compartments
(Several old and new anatomic studies)(Several old and new anatomic studies)
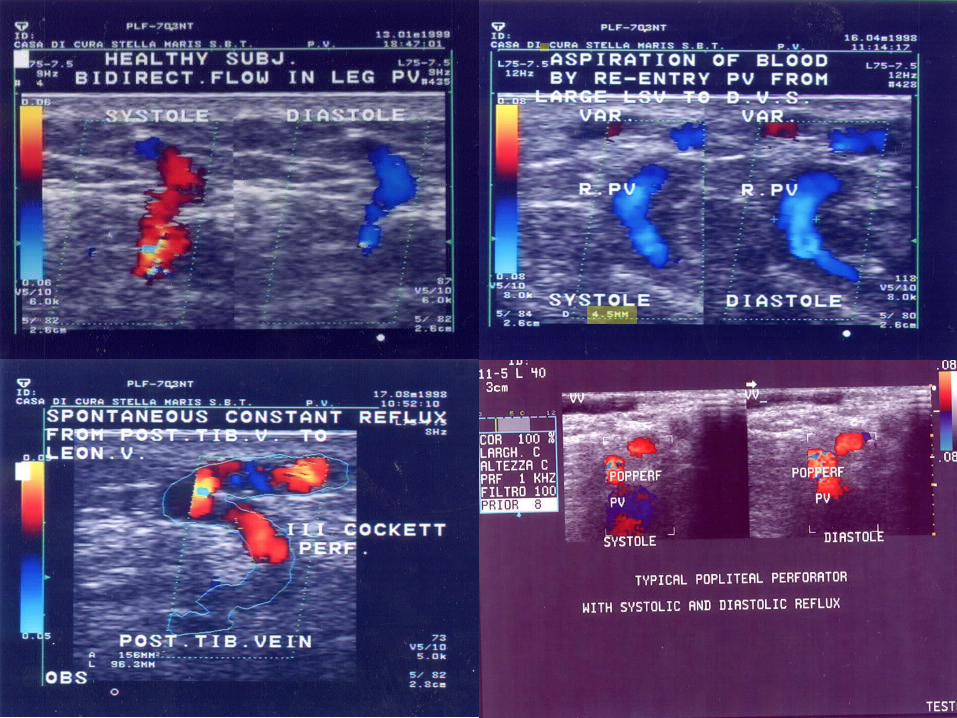
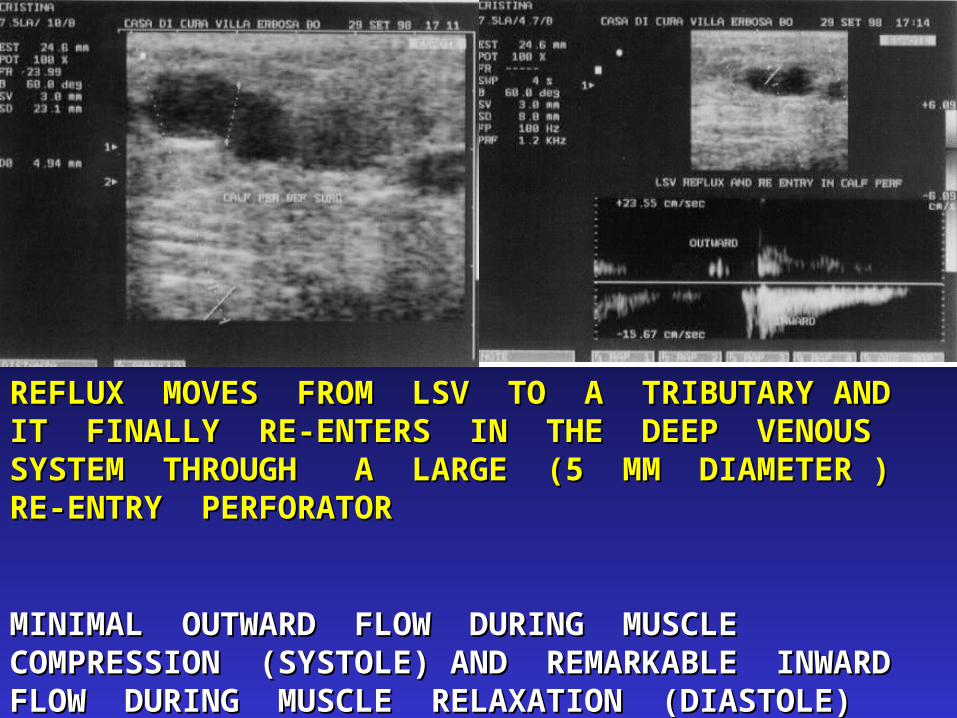
REFLUX MOVES FROM LSV TO A TRIBUTARY AND IT REFLUX MOVES FROM LSV TO A TRIBUTARY AND IT FINALLY RE-ENTERS IN THE DEEP VENOUS SYSTEM FINALLY RE-ENTERS IN THE DEEP VENOUS SYSTEM THROUGH A LARGE (5 MM DIAMETER ) RE-ENTRY THROUGH A LARGE (5 MM DIAMETER ) RE-ENTRY PERFORATORPERFORATOR
MINIMAL OUTWARD FLOW DURING MUSCLE MINIMAL OUTWARD FLOW DURING MUSCLE COMPRESSION (SYSTOLE) AND REMARKABLE INWARD COMPRESSION (SYSTOLE) AND REMARKABLE INWARD FLOW DURING MUSCLE RELAXATION (DIASTOLE)FLOW DURING MUSCLE RELAXATION (DIASTOLE)

COLOUR-DUPLEX INVESTIGATION IN ULCER AREACOLOUR-DUPLEX INVESTIGATION IN ULCER AREA

CFDI EVALUATION OVER ULCER AREA
Rare incompetent perforators….
PRIMARY DEEP VENOUS PRIMARY DEEP VENOUS INSUFFICIENCY INSUFFICIENCY
- Reflux in deep veinsReflux in deep veins
- Reflux of saphenous veinsReflux of saphenous veins
- No findings compatible with previous No findings compatible with previous DVT (thrombotic changes etc.)DVT (thrombotic changes etc.)
- Generalised Dilatation of deep veinsGeneralised Dilatation of deep veins
-Incidence ???????Incidence ???????
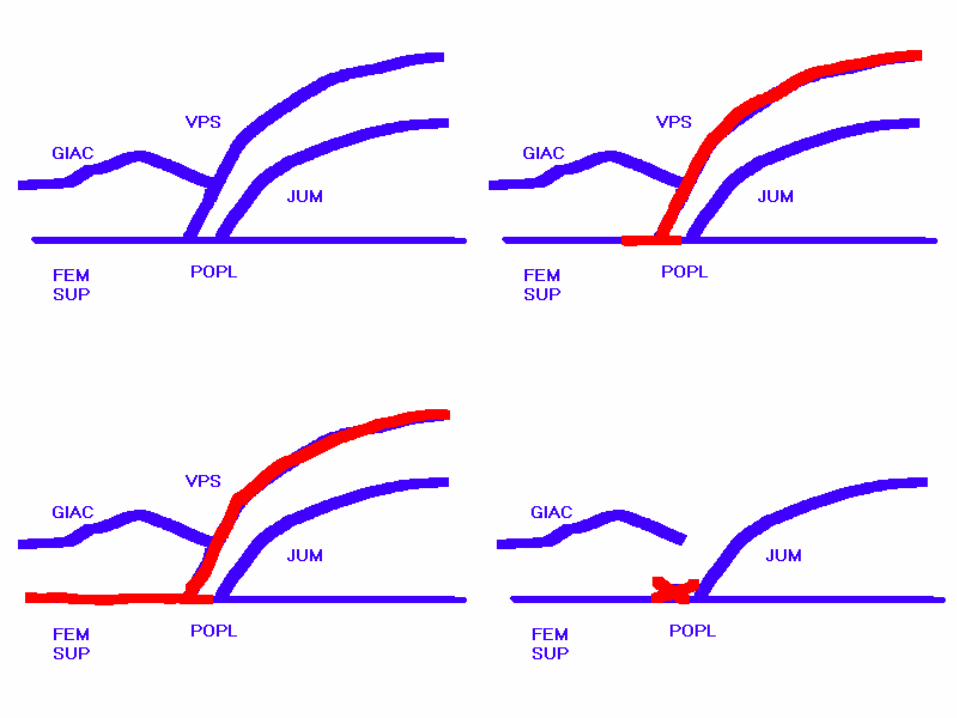

ABOLITION OF DEEP ABOLITION OF DEEP VEIN REFLUX AFTER VEIN REFLUX AFTER SURGERY / SURGERY / SCLEROTHERAPY OF SCLEROTHERAPY OF SMALL SAPHENOUS SMALL SAPHENOUS VEINVEIN
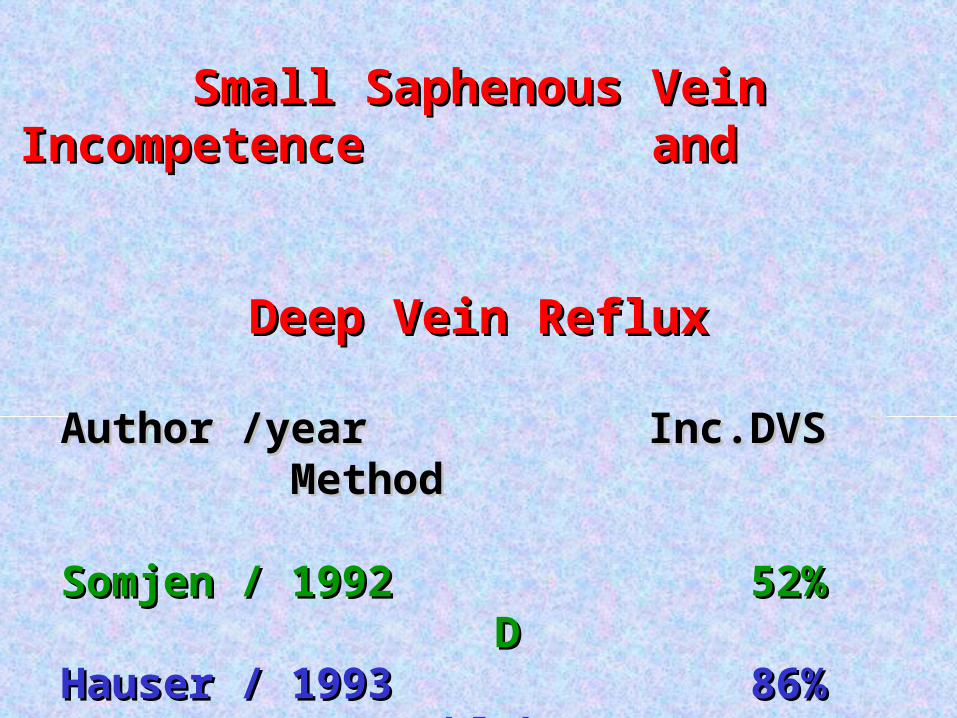
Small Saphenous Vein Incompetence Small Saphenous Vein Incompetence and and
Deep Vein RefluxDeep Vein Reflux
Author /year Inc.DVS MethodAuthor /year Inc.DVS Method Somjen / 1992 52% DSomjen / 1992 52% D Hauser / 1993 86% D+Phleb.Hauser / 1993 86% D+Phleb. Sakurai / 1997 44,9% (SFJ incl.) CDSakurai / 1997 44,9% (SFJ incl.) CD Brunner / 1997 68,7% D+PhlebBrunner / 1997 68,7% D+Phleb Daher / 2001Daher / 2001 39,7% 39,7% DD Recek / 2002 100%Recek / 2002 100% DD
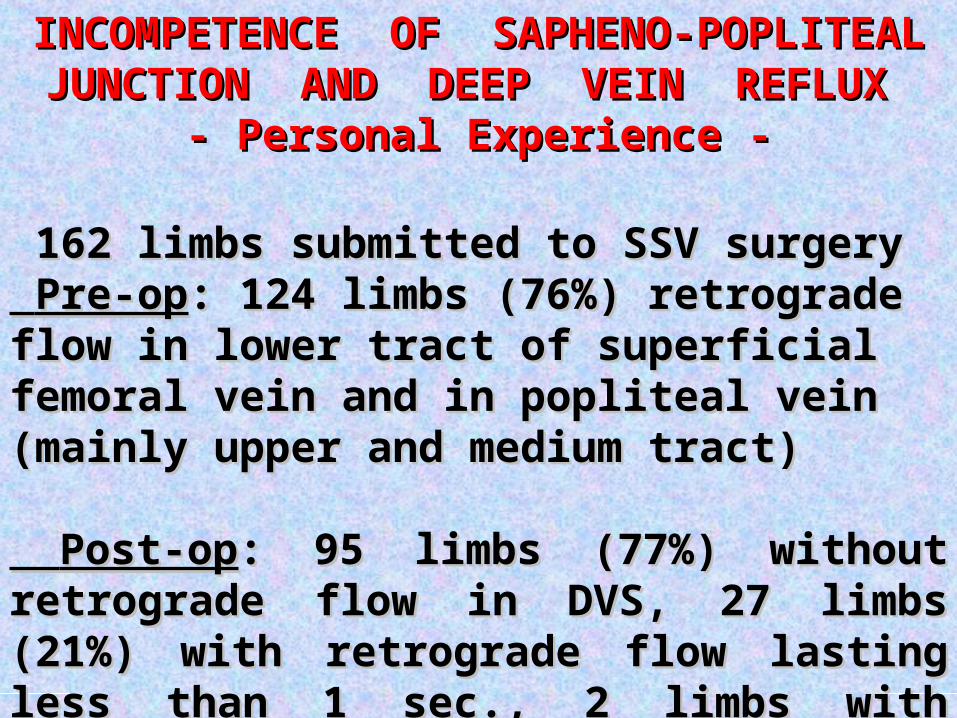
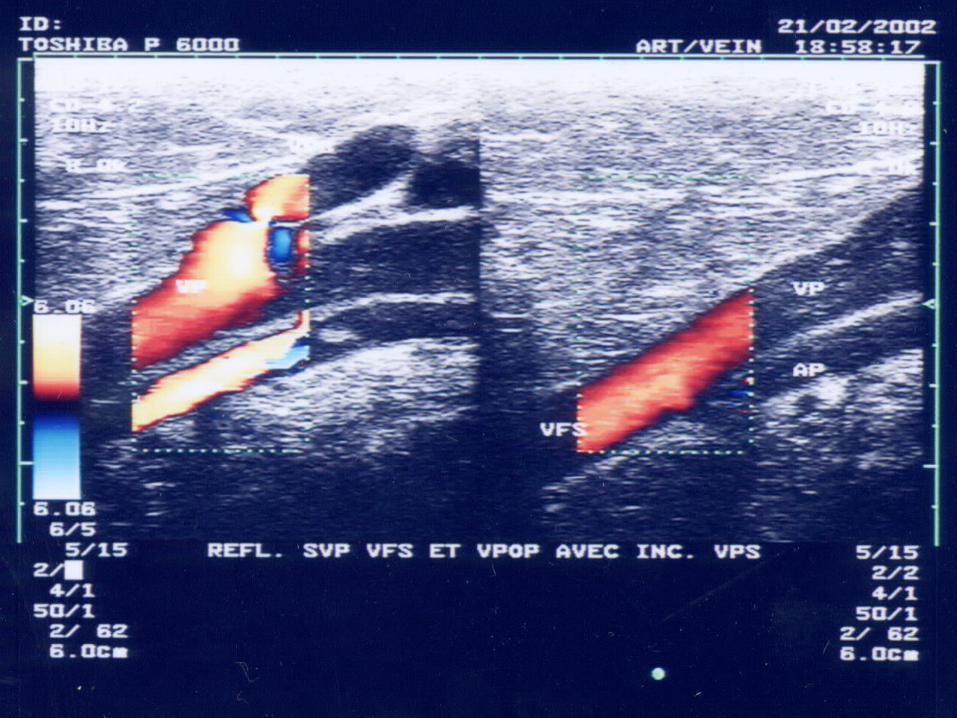
INCOMPETENCE OF SAPHENO-POPLITEAL INCOMPETENCE OF SAPHENO-POPLITEAL JUNCTION AND DEEP VEIN REFLUX JUNCTION AND DEEP VEIN REFLUX
- Personal Experience -- Personal Experience -
162 limbs submitted to SSV surgery162 limbs submitted to SSV surgery Pre-opPre-op: : 124 limbs (76%) retrograde flow in lower 124 limbs (76%) retrograde flow in lower tract of superficial femoral vein and in popliteal tract of superficial femoral vein and in popliteal vein (mainly upper and medium tract) vein (mainly upper and medium tract)
Post-opPost-op: 95 limbs (77%) without retrograde flow : 95 limbs (77%) without retrograde flow in DVS, 27 limbs (21%) with retrograde flow in DVS, 27 limbs (21%) with retrograde flow lasting less than 1 sec., 2 limbs with persistent lasting less than 1 sec., 2 limbs with persistent retrograde flow in DVSretrograde flow in DVS
(Cavezzi, Ta(Cavezzi, Tarabini, Collura, Sigismondi, Barboni, Carigi; rabini, Collura, Sigismondi, Barboni, Carigi; Phlébologie 2002 )Phlébologie 2002 )
THE UNBEARABLE THE UNBEARABLE HEAVINESS OF BEING HEAVINESS OF BEING (M.Kundera revisited) …(M.Kundera revisited) …
Functional Venous Functional Venous Insufficiency with Veno-Insufficiency with Veno-Lymphatic UlcerLymphatic Ulcer
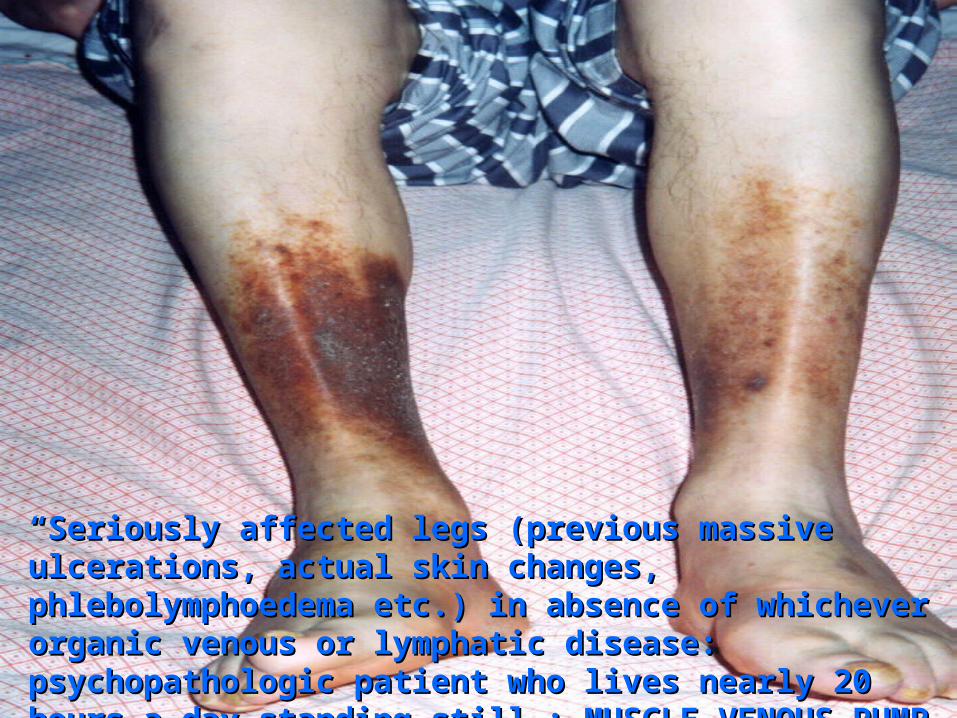
““Seriously affected legs (previous massive ulcerations, actual skin Seriously affected legs (previous massive ulcerations, actual skin changes, phlebolymphoedema etc.) in absence of whichever organic changes, phlebolymphoedema etc.) in absence of whichever organic venous or lymphatic disease: psychopathologic patient who lives venous or lymphatic disease: psychopathologic patient who lives nearly 20 hours a day standing still…: MUSCLE-VENOUS PUMP nearly 20 hours a day standing still…: MUSCLE-VENOUS PUMP DYSFUNCTON…. DYSFUNCTON….