comparisons among botulinum toxins: an evidence-based review · strain of clostridium botulinum...
TRANSCRIPT

COSMETIC
Comparisons among Botulinum Toxins:An Evidence-Based Review
Arnold W. Klein, M.D.Alastair Carruthers,
F.R.C.P.C.Steven Fagien, M.D.
Nicholas J. Lowe, M.D.
Los Angeles, Calif.; Boca Raton, Fla.;and Vancouver, British Columbia,
Canada
Background: Botulinum neurotoxin treatment is the most common aestheticprocedure in the United States. A number of serotypes and formulations areavailable worldwide. Similarities and differences among these toxins were eval-uated by reviewing the existing literature.Methods: Reports of botulinum neurotoxin for aesthetic use, published inpeer-reviewed literature or presented at recent professional congresses, werereviewed to summarize key features of different toxins. Data from therapeuticuses in comparable anatomical areas were included in the review when aestheticliterature was limited.Results: Serotypes of neurotoxins share molecular structures and mechanismsof action but exhibit important differences between serotypes and betweendifferent formulations within the same serotype, including differences in dis-tribution/diffusion patterns and risk/benefit profiles. The differences attrib-utable to dissimilarities in bacterial strains, manufacturing techniques, andassays are likely to influence clinical performance.Conclusions: Injection patterns, techniques, dilutions diffusion, and injectionvolumes established for a specific formulation of botulinum neurotoxin are notlikely to be applicable to other formulations, and formulations are not inter-changeable by any single conversion ratio. A large proportion of the clinicalliterature documents the aesthetic uses of the Allergan formulation of botuli-num toxin type A. Additional studies are needed to establish optimal proceduresfor the Ipsen formulation and botulinum neurotoxin, and for diverse aestheticuses. (Plast. Reconstr. Surg. 121: 413e, 2008.)
The cosmetic use of botulinum neurotoxintype A altered aesthetic medicine, providingan effective, safe, and noninvasive method of
improving facial appearance. Over time, botuli-num neurotoxin type A uses have evolved, bothreflecting and spurring changes in aesthetic treat-ment goals that embrace a broader concept offacial enhancement and creation of a more nat-ural, relaxed look tailored to individual goals.1–3
Several commercial preparations of botuli-num neurotoxin are available which, unlike ge-neric, nonbiological agents, are unique and there-fore not interchangeable in clinical use. This
review explores the issues that must be consideredwhen evaluating a botulinum neurotoxin. It pro-vides an in-depth, evidence-based comparison ofthe two most frequently used formulations of bot-ulinum neurotoxin type A: the 900-kDa formula-tion (Botox; Allergan, Inc., Irvine, Calif.)4 and the
From the David Geffen School of Medicine, University ofCalifornia, Los Angeles, and the Department of Dermatology,University of British Columbia.Received for publication December 19, 2006; accepted July19, 2007.Reprinted and reformatted from the original article publishedwith the June 2008 issue (Plast Reconstr Surg. 2008;121:413e–422e).Copyright ©2012 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e318269cb48
Disclosure: Alastair Carruthers, F.R.C.P.C., is aconsultant to Allergan, Inc., Medicis, Inc., SolsticeNeurosciences, Inc., and Merz GmbH; StevenFagien, M.D., is a consultant to Allergan, Inc., andMedicis Inc.; Nicholas J. Lowe, M.D., is a consul-tant to and has received research and educationalgrants from Allergan, Inc., Medicis, Inc., and Men-tor FzioMed, and is a stockholder in Allergan, Inc.,and Medicis, Inc.; Dr. Arnold W. Klein, M.D., is aconsultant to Ortho-Neutrogena. He serves as aninvestigator to Anika, and Medicis Inc., and is aninvestigator and shareholder for Skin Medica. Hehas received an educational grant from Allerganand Medicis Inc.
www.PRSJournal.com 91S
500- to 900-kDa formulation (Dysport, expected tobe marketed as Reloxin in the United States; IpsenLtd., Berkshire, United Kingdom),5 and discussesknown and potential clinical consequences oftheir differences. Another botulinum neurotoxintype A, without complexing proteins (Xeomin;Merz Pharmaceuticals GmbH, Frankfurt, Ger-many), is currently approved for therapeutic ap-plications in Germany.6
PROPERTIES AND PREPARATIONS OFBOTULINUM NEUROTOXINS
Botulinum neurotoxins occur in seven knownserotypes, two of which are in clinical use, types A
and B (Tables 1 and 2).4,5,7–14 All serotypes sharemolecular structures and mechanisms of actionbut differ in specific characteristics that may ininfluence clinical performance.8,15 Differencesalso may occur within serotypes because of dis-similarities in manufacturing, bacterial strainsused in fermentation, purification methods, andinactive ingredients in the formulation. Dispar-ities in assays also influence the potency andantigenicity of each product.11,16
Botulinum neurotoxins are macromolecularprotein complexes with molecular weights of 300to 900 kDa comprising a 150-kDa neurotoxin pro-tein, plus varying amounts of nontoxin proteins.17
These variations, and pH and physiologic condi-tions at the injection site, may affect the stabilityof the toxins, which could influence distributionwithin target muscles or diffusion to nontargetedmuscles.14,18,19 The development of new toxinswithout complexing proteins should allow addi-tional examination of this hypothesis.20,21
PRECLINICAL STUDIES ONBOTULINUM NEUROTOXINS
Botulinum neurotoxins should act only in thetargeted muscle to reduce adverse events fromdiffusion to nontargeted muscles.22,23 Relative po-tency based on muscle weakening, efficacy, safety,and distribution/diffusion properties of botuli-num neurotoxins have been examined in preclin-ical studies.8,24,25 For example, in the mouse digitabduction scoring assay, groups of mice are givenincreasing doses of botulinum neurotoxin in-jected into the targeted gastrocnemius muscle.24
Muscle weakening is rated by eliciting a startle
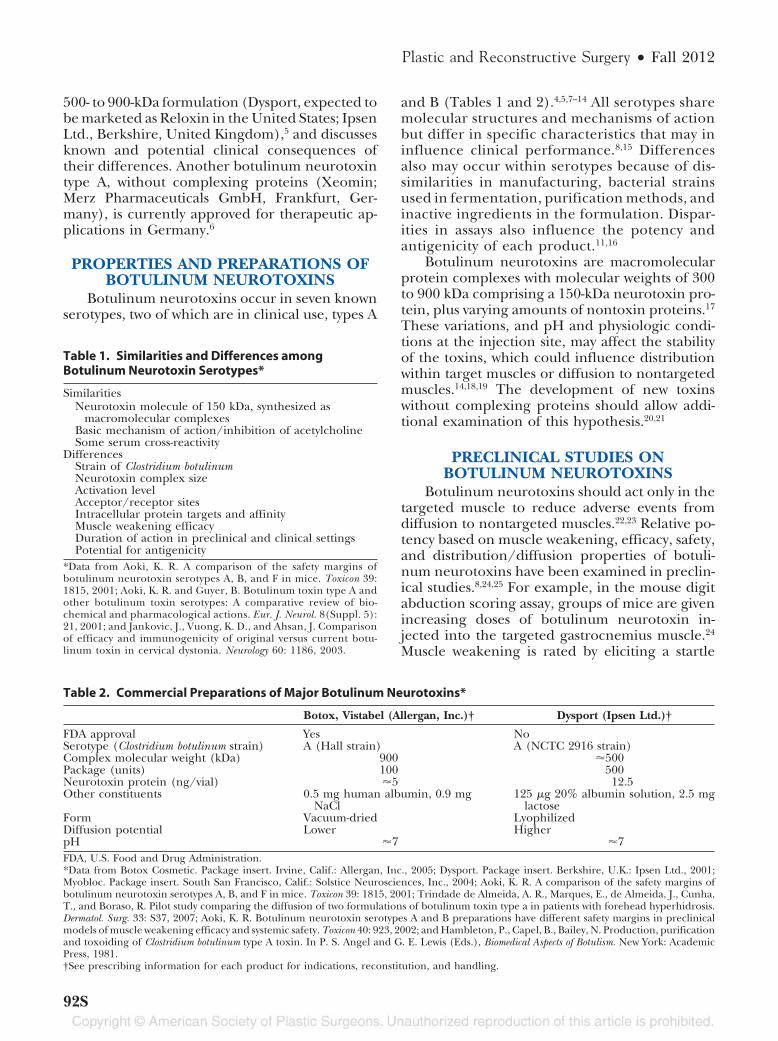
Table 1. Similarities and Differences amongBotulinum Neurotoxin Serotypes*
SimilaritiesNeurotoxin molecule of 150 kDa, synthesized as
macromolecular complexesBasic mechanism of action/inhibition of acetylcholineSome serum cross-reactivity
DifferencesStrain of Clostridium botulinumNeurotoxin complex sizeActivation levelAcceptor/receptor sitesIntracellular protein targets and affinityMuscle weakening efficacyDuration of action in preclinical and clinical settingsPotential for antigenicity
*Data from Aoki, K. R. A comparison of the safety margins ofbotulinum neurotoxin serotypes A, B, and F in mice. Toxicon 39:1815, 2001; Aoki, K. R. and Guyer, B. Botulinum toxin type A andother botulinum toxin serotypes: A comparative review of bio-chemical and pharmacological actions. Eur. J. Neurol. 8(Suppl. 5):21, 2001; and Jankovic, J., Vuong, K. D., and Ahsan, J. Comparisonof efficacy and immunogenicity of original versus current botu-linum toxin in cervical dystonia. Neurology 60: 1186, 2003.
Table 2. Commercial Preparations of Major Botulinum Neurotoxins*
Botox, Vistabel (Allergan, Inc.)† Dysport (Ipsen Ltd.)†
FDA approval Yes NoSerotype (Clostridium botulinum strain) A (Hall strain) A (NCTC 2916 strain)Complex molecular weight (kDa) 900 �500Package (units) 100 500Neurotoxin protein (ng/vial) �5 12.5Other constituents 0.5 mg human albumin, 0.9 mg
NaCl125 �g 20% albumin solution, 2.5 mg
lactoseForm Vacuum-dried LyophilizedDiffusion potential Lower HigherpH �7 �7FDA, U.S. Food and Drug Administration.*Data from Botox Cosmetic. Package insert. Irvine, Calif.: Allergan, Inc., 2005; Dysport. Package insert. Berkshire, U.K.: Ipsen Ltd., 2001;Myobloc. Package insert. South San Francisco, Calif.: Solstice Neurosciences, Inc., 2004; Aoki, K. R. A comparison of the safety margins ofbotulinum neurotoxin serotypes A, B, and F in mice. Toxicon 39: 1815, 2001; Trindade de Almeida, A. R., Marques, E., de Almeida, J., Cunha,T., and Boraso, R. Pilot study comparing the diffusion of two formulations of botulinum toxin type a in patients with forehead hyperhidrosis.Dermatol. Surg. 33: S37, 2007; Aoki, K. R. Botulinum neurotoxin serotypes A and B preparations have different safety margins in preclinicalmodels of muscle weakening efficacy and systemic safety. Toxicon 40: 923, 2002; and Hambleton, P., Capel, B., Bailey, N. Production, purificationand toxoiding of Clostridium botulinum type A toxin. In P. S. Angel and G. E. Lewis (Eds.), Biomedical Aspects of Botulism. New York: AcademicPress, 1981.†See prescribing information for each product for indications, reconstitution, and handling.
Plastic and Reconstructive Surgery • Fall 2012
92S

response, measured by the degree of digit abduc-tion. The resulting data provide the median ef-fective dose, therapeutic margin (an estimate ofunwanted diffusion), and safety margin (an esti-mate of side effects caused by distant actions). Thismodel has consistently demonstrated the 900 kDabotulinum toxin type A (Botox) to be 4- to 5-foldmore potent than the 500- to 900-kDa botulinumtoxin type A (Dysport), consistent with the clinicalliterature.8,24,25 Estimates of the therapeutic mar-gin and safety margin for Botox were larger thanfor Dysport, suggesting a reduced tendency forBotox to cause undesired local or distant effectsthrough diffusion (Table 3).8,15,25 These findingsclarify clinical results suggesting that similar effi-cacy at a specific ratio of Dysport to Botox units isattained with a higher incidence of Dysport-asso-ciated adverse events.26 These results also suggestthat equivalence in both safety and efficacy cannotbe achieved with a single dose-conversion ratio;that formulations of botulinum neurotoxins arenot interchangeable; and that adjustment in in-jection volumes, techniques, and patterns wouldbe required to achieve similar clinical results.
CLINICAL STUDIESBotox has been used to treat hyperfunctional
facial lines since the early 1990s.27,28 Documenta-tion of its safety, predictability, and efficacy for allareas of the face and neck is extensive and unsur-passed by any other formulation or serotype.2,29,30
Detailed guidelines for aesthetic uses of Botox,based on expert experience and clinical trials, havebeen published only for the Botox formulation ofbotulinum toxin type A.2 Only Botox Cosmetic isapproved by the U.S. Food and Drug Administrationfor glabellar lines at the present time. All other cos-metic uses constitute off-label use.
Controlled Noncomparative Trials
Glabellar LinesTwo large, identical, 1-year, multicenter, ran-
domized, controlled trials were conducted withBotox and pooled results reported.31 A double-blind, placebo-controlled, 4-month phase was fol-lowed by an 8-month open-label phase. Subjectsfirst received either placebo injections (n � 132)or 20 U of Botox (n � 405), divided among fivesites (0.1 ml each) in the glabellar area. Subse-quently, 373 subjects received injections of Botoxat day 120 and 4 months later. Investigator andsubject assessments showed Botox to be signifi-cantly more effective than placebo at maximumattempted contraction and at rest. Successivetreatments progressively improved appearance atrest.31 Adverse events differing significantly be-tween Botox treatment and placebo were blepha-roptosis (Botox, 3.2 percent; placebo, 0 percent)and acne (Botox, 0.5 percent; placebo, 3.1 per-cent). Blepharoptosis decreased with successivetreatments, from 3.0 percent to 2.2 percent to 0.8percent, suggesting that injection technique con-tributed to this adverse event.
Dysport was investigated in a randomizedcontrolled trial for the treatment of glabellarlines.32 Subjects received placebo (n � 17) oractive treatment (25, 50, or 75 U of Dysport [n� 34 per group]) injected into five sites. Theinjection volume was 0.05 ml to minimize dif-fusion to nontargeted muscles.32 At maximumattempted contraction and at rest, each dose ofDysport was significantly more effective thanplacebo.32 All groups treated with Dysport re-ported satisfaction, with the highest percentageof complete satisfaction attained 1 month afterinjection, by 65.5 percent in the 50-U group.Nine adverse events were considered possibly orprobably treatment-related, including one in aplacebo-treated subject. No subject experiencedblepharoptosis. Headache, migraine, foreheadrigidity, vertigo, and rosacea (one each) oc-curred in the 25-U group. Three adverse eventsin the 50-U group included forehead musclespasm, headache, and forehead ecchymosis. Noadverse events were reported in the 75-U group.The authors concluded that the 50-U dose wasoptimal, representing a ratio of 2.5:1 Dysport toBotox. A recent phase II trial, similar in designto the one described above, confirmed that adose of 50 U was optimal for treating glabellarlines.33
The results of these trials cannot be com-pared directly because of substantial differences
Table 3. Comparative Effects of BotulinumNeurotoxins in Animal Models of Efficacy and Safetyafter Intramuscular Administration*
Measure Rank Order
DAS (highest to lowest) Botox � BTX-A � Dysport �Myobloc
Safety margin(LD50/DAS ED50)(greatest to least)
Botox � BTX-A � Dysport �Myobloc
Intermuscular diffusion(most to least)
Myobloc � Dysport � BTX-A �Botox
DAS, digit abduction scoring assay; LD, lethal dose; ED, effectivedose; BTX-A, botulinum toxin type A.*From Aoki, K. R., Satorius, A., Ardila, C., et al. Pharmacology ofBotox, Dysport, Myobloc and BTX-A in animal models of efficacy andsafety. Abstract presented at the International Conference on Basicand Therapeutic Aspects of Botulinum and Tetanus Toxins, Denver,Colorado, June 23–25, 2005.
Volume 130, Number 5S-3 • Comparisons among Botulinum Toxins
93S
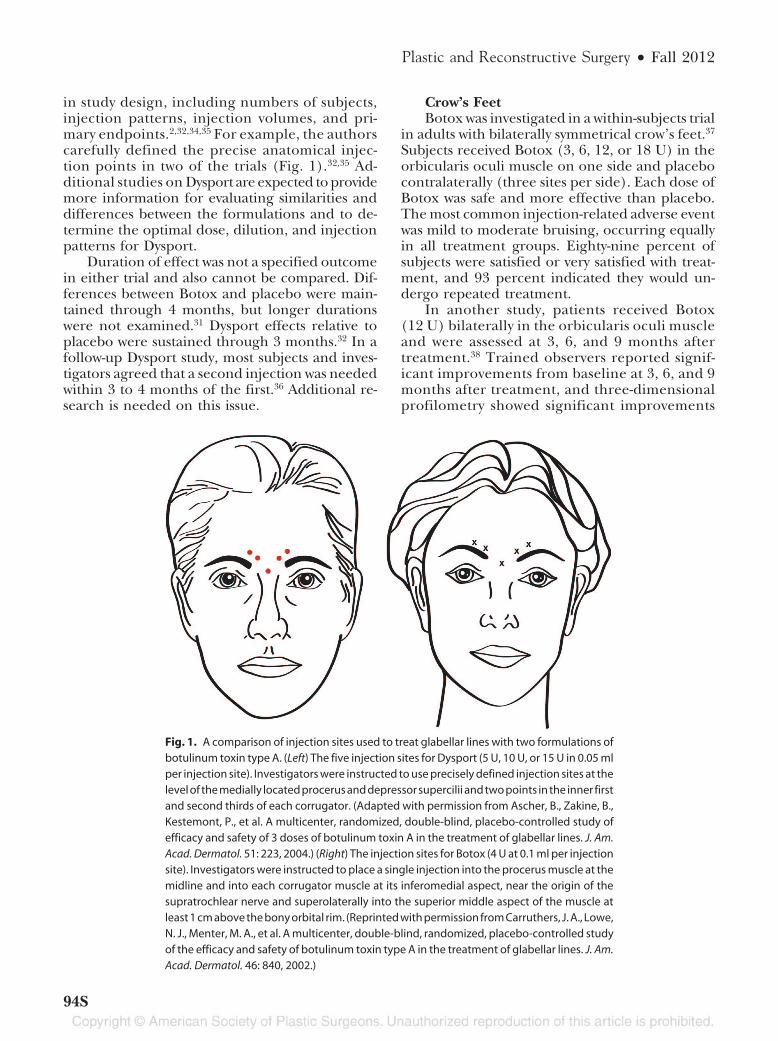
in study design, including numbers of subjects,injection patterns, injection volumes, and pri-mary endpoints.2,32,34,35 For example, the authorscarefully defined the precise anatomical injec-tion points in two of the trials (Fig. 1).32,35 Ad-ditional studies on Dysport are expected to providemore information for evaluating similarities anddifferences between the formulations and to de-termine the optimal dose, dilution, and injectionpatterns for Dysport.
Duration of effect was not a specified outcomein either trial and also cannot be compared. Dif-ferences between Botox and placebo were main-tained through 4 months, but longer durationswere not examined.31 Dysport effects relative toplacebo were sustained through 3 months.32 In afollow-up Dysport study, most subjects and inves-tigators agreed that a second injection was neededwithin 3 to 4 months of the first.36 Additional re-search is needed on this issue.
Crow’s FeetBotox was investigated in a within-subjects trial
in adults with bilaterally symmetrical crow’s feet.37
Subjects received Botox (3, 6, 12, or 18 U) in theorbicularis oculi muscle on one side and placebocontralaterally (three sites per side). Each dose ofBotox was safe and more effective than placebo.The most common injection-related adverse eventwas mild to moderate bruising, occurring equallyin all treatment groups. Eighty-nine percent ofsubjects were satisfied or very satisfied with treat-ment, and 93 percent indicated they would un-dergo repeated treatment.
In another study, patients received Botox(12 U) bilaterally in the orbicularis oculi muscleand were assessed at 3, 6, and 9 months aftertreatment.38 Trained observers reported signif-icant improvements from baseline at 3, 6, and 9months after treatment, and three-dimensionalprofilometry showed significant improvements
Fig. 1. A comparison of injection sites used to treat glabellar lines with two formulations ofbotulinum toxin type A. (Left) The five injection sites for Dysport (5 U, 10 U, or 15 U in 0.05 mlper injection site). Investigators were instructed to use precisely defined injection sites at thelevel of the medially located procerus and depressor supercilii and two points in the inner firstand second thirds of each corrugator. (Adapted with permission from Ascher, B., Zakine, B.,Kestemont, P., et al. A multicenter, randomized, double-blind, placebo-controlled study ofefficacy and safety of 3 doses of botulinum toxin A in the treatment of glabellar lines. J. Am.Acad. Dermatol. 51: 223, 2004.) (Right) The injection sites for Botox (4 U at 0.1 ml per injectionsite). Investigators were instructed to place a single injection into the procerus muscle at themidline and into each corrugator muscle at its inferomedial aspect, near the origin of thesupratrochlear nerve and superolaterally into the superior middle aspect of the muscle atleast 1 cm above the bony orbital rim. (Reprinted with permission from Carruthers, J. A., Lowe,N. J., Menter, M. A., et al. A multicenter, double-blind, randomized, placebo-controlled studyof the efficacy and safety of botulinum toxin type A in the treatment of glabellar lines. J. Am.Acad. Dermatol. 46: 840, 2002.)
Plastic and Reconstructive Surgery • Fall 2012
94S

at 3 and 6 months. Both of these measures in-dicate a long duration of effect when Botox isused to treat crow’s feet.
Lower FaceThe major aesthetic uses of botulinum neu-
rotoxins are for the upper face, although the safetyand effectiveness of Botox for treating moderatechin rhytides have been shown in a controlledstudy.30 Experienced practitioners also have foundBotox to be useful for treating the perioral area,chin, and platysmal bands.2,29,30,39 Recommenda-tions for the use of Botox, but not for other bot-ulinum neurotoxin preparations, in the lower faceand neck have been published, including experi-ence in more than 1500 patients treated with Bo-tox for platysmal bands.2,39
Comparative TrialsComparative trials of botulinum neurotoxins
demonstrate their noninterchangeability, consis-tent with approved prescribing information forthe various products.4,5,7 The data for Botox andDysport reveal tradeoffs between efficacy and tol-erability at various dosage ratios.
Upper FaceThe safety and efficacy of Botox and Dysport
were compared in a 20-week, double-blind, ran-domized, parallel-group study in subjects with gla-bellar lines of at least moderate severity at maxi-mum contraction.40 Each subject received fiveinjections of either 20 U of Botox or 50 U ofDysport, based on manufacturer recommenda-tions and published literature.4,32,40 The incidence
of responders (glabellar line severity of none ormild posttreatment) at week 2 was 53 percent foreach treatment group (Fig. 2).40 At week 12, 47percent of the Botox-treated versus 21 percent ofthe Dysport-treated subjects were responders. Agreater proportion of Botox-treated subjects re-mained relapse-free throughout the study. Subjectsatisfaction was significantly greater with Botoxtreatment at week 12: 64 percent of Botox-treatedversus 33 percent of the Dysport-treated subjectsreported at least 50 percent improvement. No sub-ject experienced ptosis of the brow or upper eyelidand one Botox-treated subject reported bruising.The investigators concluded that at a ratio of 2.5:1(Dysport to Botox), the Botox formulation of bot-ulinum neurotoxin type A afforded more pro-longed efficacy in diminishing glabellar lines andthat both formulations were well tolerated.
Various Facial RhytidesDysport and Botox were compared in an open-
label study of 20 Korean subjects who receivedtreatments in the lateral canthal area, glabellararea, nasal area, dorsum, or nasolabial fold.41 Sixsubjects received Dysport (20 U/0.1 ml) and 14received Botox (5 U/0.1 ml; a ratio of 4:1). Totaldoses were based on wrinkle severity, and mostsubjects received injections in more than one area.Efficacy was similar for each treatment group, buttransient adverse events occurred approximatelythree times more frequently in Dysport-treatedsubjects (six of six) than in Botox-treated subjects[five of 14 (35 percent)] (p � 0.05). No ptosisoccurred. Limitations of the study include smallsample size, lack of controls, and variability in
Fig. 2. Percentage of responders as determined by photographic examination at maximum frown.(Reprinted with permission from Lowe, P. L., Patnaik, R., and Lowe, N. J. A comparison of two bot-ulinum type A toxin preparations for the treatment of glabellar lines: Double-blind, randomized,pilot study. Dermatol. Surg. 31: 1651, 2005.)
Volume 130, Number 5S-3 • Comparisons among Botulinum Toxins
95S

treatment areas and doses. Nevertheless, the re-sults suggest that the efficacy of the two formula-tions of botulinum neurotoxin type A is similar ata 4:1 ratio (Dysport to Botox), but that Botox isassociated with significantly fewer complications.
Other Comparative Studies: TherapeuticIndications
Therapeutic trials for blepharospasm andhemifacial spasm, which also involve small facialmuscles, furnish additional insight into the rel-ative clinical performance of Botox and Dysport.With other trials on cervical dystonia and palmarhyperhidrosis, these studies provide data on therelative efficacy and safety of Botox and Dysportacross a range of dose ratios and indications(Table 4).26,42– 46 These data demonstrate thatalthough both products are efficacious in theseindications, the two formulations are not inter-changeable at any one fixed dose ratio and thattheir risk-to-benefit profiles differ, with Dysporttending to result in a greater number of adverseevents as shown in four of the six studies sum-marized. At least some of these adverse eventsmay represent unwanted diffusion from the in-jection site. In blepharospasm, for example, pto-sis occurred in 6.6 percent of patients duringDysport treatment and 1.4 percent of the samepatients during Botox treatment (p � 0.01).42 Inanother study, seven instances of ptosis and fourof double vision were reported across all indi-cations in Dysport treatment versus none duringBotox treatment.26 The results of a small studyin palmar hyperhidrosis also demonstrated thatpotentially small, not significant gains in efficacywere offset by a higher incidence of adverseevents such as thumb-index finger pinch weak-ness in four patients on palms treated with Dys-port versus two cases when palms were treatedwith Botox.45 Another patient reported right up-per limb heaviness lasting 8 days on the sideinjected with Dysport.
A closer look at dose ratios. The retrospective,multinational Real Dose Study examined real-world dosage use of Botox and Dysport in cer-vical dystonia and blepharospasm.47 Patients(n � 114) who had received either neurotoxinfor at least two consecutive treatments and werethen switched to the other neurotoxin for atleast 1 additional year were eligible. The major-ity of patients (88 percent) received a ratio ofgreater than 3:1 (Dysport to Botox), regardlessof the direction of the switch (Fig. 3).47 Theoverall mean dose ratio was 4.48:1 (Dysport toBotox). Of the 106 total adverse events re-ported, 71 percent occurred during Dysport Ta
ble
4.
Co
mp
arat
ive
Ther
apeu
tic
Tria
lso
fDys
po
rtan
dB
oto
x
Stud
yan
dD
esig
nT
hera
peut
icA
rea
Mea
nD
ose
Rat
io(D
yspo
rtto
Bot
ox)
Key
Find
ings
Eff
icac
ySa
fety
Bih
ari,
2005
26B
leph
aros
pasm
(n�
27)
4:1;
5:1
Bot
ox¡
grea
ter
dura
tion
ofef
fect
(ble
phar
ospa
sm,
p�
0.00
1;ce
rvic
aldy
ston
ia,
p�
0.01
4;h
emif
acia
lsp
asm
,p
�0.
014)
Dys
port
,23
in19
pati
ents
;B
otox
,0
Cer
vica
ldy
ston
ia(n
�12
)H
emif
acia
lsp
asm
(n�
9)
Nus
sgen
san
dR
ogge
nka
mpe
r,19
9742
;cr
osso
ver
stud
yB
leph
aros
pasm
(n�
212)
4:1
Equ
ival
ent
(dur
atio
n)
All
adve
rse
even
ts:
Dys
port
,24
%;
Bot
ox,
17%
;p
�0.
05Pt
osis
:D
yspo
rt,
6.6%
;B
otox
,1.
4%;
p�
0.01
Ode
rgre
net
al.,
1998
43;
para
llel
grou
pC
ervi
cal
dyst
onia
Bot
ox(n
�35
)3:
1E
quiv
alen
tef
fica
cyE
quiv
alen
tfr
eque
ncy
ofad
vers
eev
ents
Dys
port
(n�
38)
Ran
oux
etal
.,20
0244
;cr
osso
ver
stud
yC
ervi
cal
dyst
onia
(n�
54)
3:1;
4:1
Dys
port
effi
cacy
�B
otox
(p�
0.02
)D
yspo
rtad
vers
eev
ents
�B
otox
atbo
thdo
sera
tios
(p�
0.01
)Si
mon
etta
Mor
eau
etal
.,20
03;
wit
hin
-sub
ject
,do
uble
-blin
d45Pa
lmar
hyp
erh
idro
sis
(n�
8)4:
1E
quiv
alen
tef
fica
cyin
redu
ctio
nof
swea
tin
g;si
mila
rdu
rati
onof
effe
ctD
yspo
rtad
vers
eev
ents
�B
otox
Van
den
Ber
ghan
dL
ison
,19
9846
Hem
ifac
ial
spas
m(n
�10
)2.
33:1
Equ
ival
ent
effi
cacy
inbo
thin
dica
tion
sE
quiv
alen
t,n
ody
sph
agia
Cer
vica
ldy
ston
ia(n
�10
)2.
49:1
Plastic and Reconstructive Surgery • Fall 2012
96S
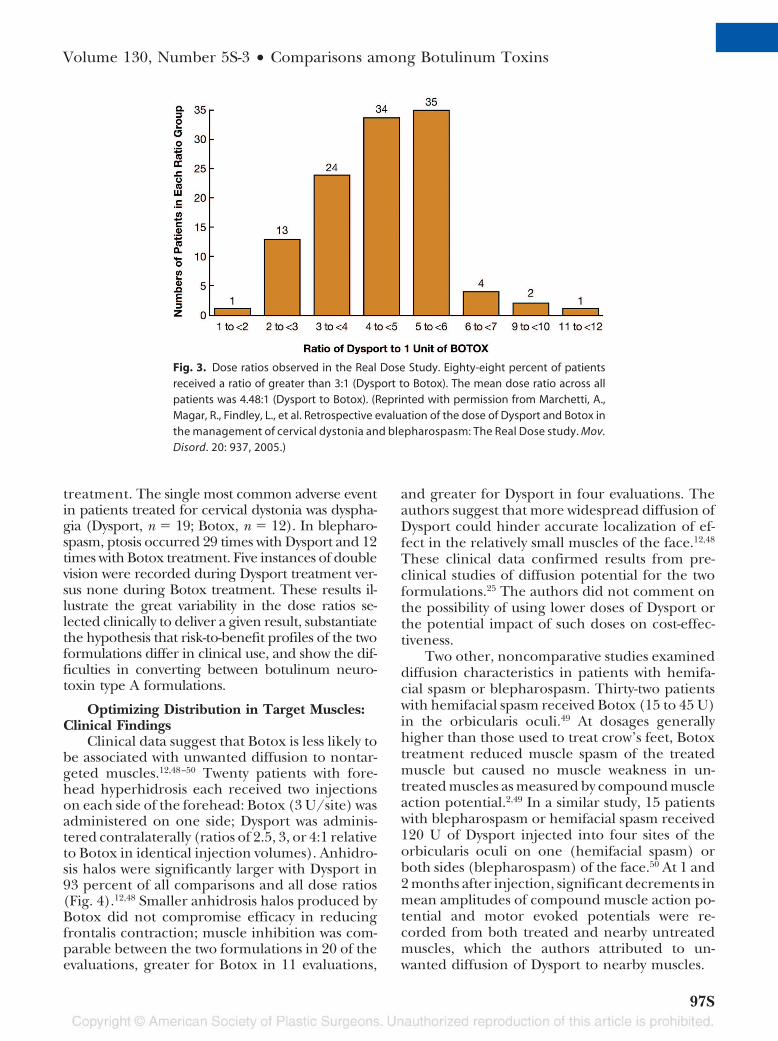
treatment. The single most common adverse eventin patients treated for cervical dystonia was dyspha-gia (Dysport, n � 19; Botox, n � 12). In blepharo-spasm, ptosis occurred 29 times with Dysport and 12times with Botox treatment. Five instances of doublevision were recorded during Dysport treatment ver-sus none during Botox treatment. These results il-lustrate the great variability in the dose ratios se-lected clinically to deliver a given result, substantiatethe hypothesis that risk-to-benefit profiles of the twoformulations differ in clinical use, and show the dif-ficulties in converting between botulinum neuro-toxin type A formulations.
Optimizing Distribution in Target Muscles:Clinical Findings
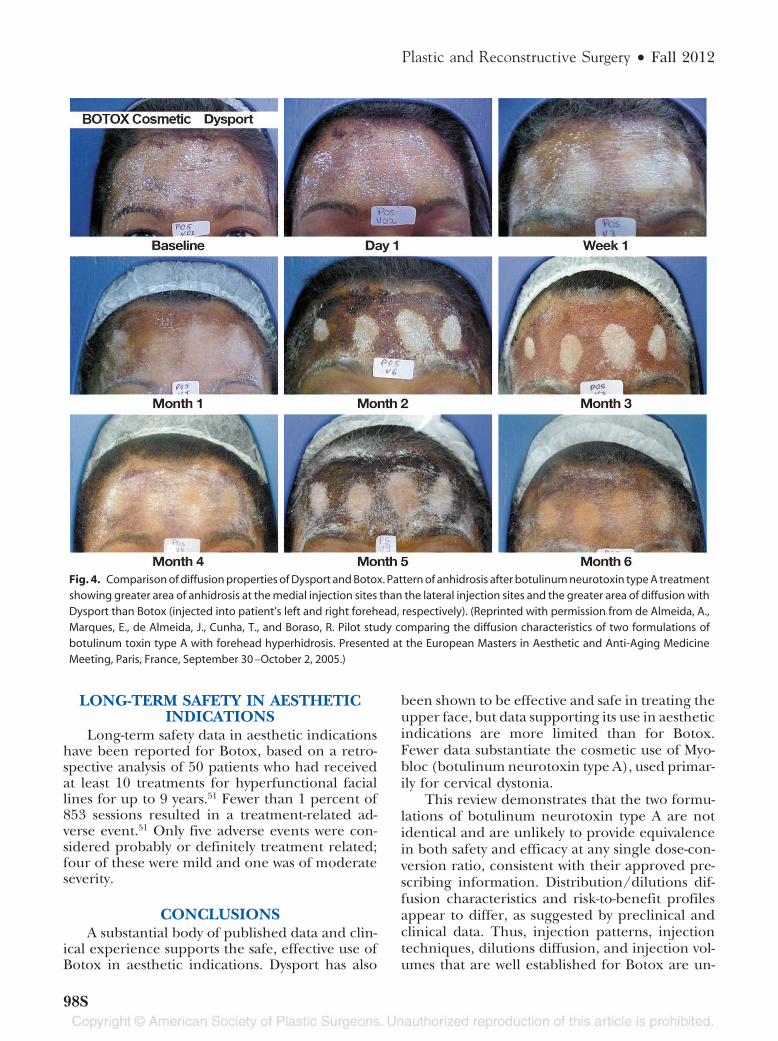
Clinical data suggest that Botox is less likely tobe associated with unwanted diffusion to nontar-geted muscles.12,48–50 Twenty patients with fore-head hyperhidrosis each received two injectionson each side of the forehead: Botox (3 U/site) wasadministered on one side; Dysport was adminis-tered contralaterally (ratios of 2.5, 3, or 4:1 relativeto Botox in identical injection volumes). Anhidro-sis halos were significantly larger with Dysport in93 percent of all comparisons and all dose ratios(Fig. 4).12,48 Smaller anhidrosis halos produced byBotox did not compromise efficacy in reducingfrontalis contraction; muscle inhibition was com-parable between the two formulations in 20 of theevaluations, greater for Botox in 11 evaluations,
and greater for Dysport in four evaluations. Theauthors suggest that more widespread diffusion ofDysport could hinder accurate localization of ef-fect in the relatively small muscles of the face.12,48
These clinical data confirmed results from pre-clinical studies of diffusion potential for the twoformulations.25 The authors did not comment onthe possibility of using lower doses of Dysport orthe potential impact of such doses on cost-effec-tiveness.
Two other, noncomparative studies examineddiffusion characteristics in patients with hemifa-cial spasm or blepharospasm. Thirty-two patientswith hemifacial spasm received Botox (15 to 45 U)in the orbicularis oculi.49 At dosages generallyhigher than those used to treat crow’s feet, Botoxtreatment reduced muscle spasm of the treatedmuscle but caused no muscle weakness in un-treated muscles as measured by compound muscleaction potential.2,49 In a similar study, 15 patientswith blepharospasm or hemifacial spasm received120 U of Dysport injected into four sites of theorbicularis oculi on one (hemifacial spasm) orboth sides (blepharospasm) of the face.50 At 1 and2 months after injection, significant decrements inmean amplitudes of compound muscle action po-tential and motor evoked potentials were re-corded from both treated and nearby untreatedmuscles, which the authors attributed to un-wanted diffusion of Dysport to nearby muscles.
Fig. 3. Dose ratios observed in the Real Dose Study. Eighty-eight percent of patientsreceived a ratio of greater than 3:1 (Dysport to Botox). The mean dose ratio across allpatients was 4.48:1 (Dysport to Botox). (Reprinted with permission from Marchetti, A.,Magar, R., Findley, L., et al. Retrospective evaluation of the dose of Dysport and Botox inthe management of cervical dystonia and blepharospasm: The Real Dose study. Mov.Disord. 20: 937, 2005.)
Volume 130, Number 5S-3 • Comparisons among Botulinum Toxins
97S
LONG-TERM SAFETY IN AESTHETICINDICATIONS
Long-term safety data in aesthetic indicationshave been reported for Botox, based on a retro-spective analysis of 50 patients who had receivedat least 10 treatments for hyperfunctional faciallines for up to 9 years.51 Fewer than 1 percent of853 sessions resulted in a treatment-related ad-verse event.51 Only five adverse events were con-sidered probably or definitely treatment related;four of these were mild and one was of moderateseverity.
CONCLUSIONSA substantial body of published data and clin-
ical experience supports the safe, effective use ofBotox in aesthetic indications. Dysport has also
been shown to be effective and safe in treating theupper face, but data supporting its use in aestheticindications are more limited than for Botox.Fewer data substantiate the cosmetic use of Myo-bloc (botulinum neurotoxin type A), used primar-ily for cervical dystonia.
This review demonstrates that the two formu-lations of botulinum neurotoxin type A are notidentical and are unlikely to provide equivalencein both safety and efficacy at any single dose-con-version ratio, consistent with their approved pre-scribing information. Distribution/dilutions dif-fusion characteristics and risk-to-benefit profilesappear to differ, as suggested by preclinical andclinical data. Thus, injection patterns, injectiontechniques, dilutions diffusion, and injection vol-umes that are well established for Botox are un-
Fig. 4. Comparison of diffusion properties of Dysport and Botox. Pattern of anhidrosis after botulinum neurotoxin type A treatmentshowing greater area of anhidrosis at the medial injection sites than the lateral injection sites and the greater area of diffusion withDysport than Botox (injected into patient’s left and right forehead, respectively). (Reprinted with permission from de Almeida, A.,Marques, E., de Almeida, J., Cunha, T., and Boraso, R. Pilot study comparing the diffusion characteristics of two formulations ofbotulinum toxin type A with forehead hyperhidrosis. Presented at the European Masters in Aesthetic and Anti-Aging MedicineMeeting, Paris, France, September 30 –October 2, 2005.)
Plastic and Reconstructive Surgery • Fall 2012
98S
likely to be applicable to Dysport. Additional aes-thetic studies on Dysport are needed to establishoptimal procedures and treatment recommenda-tions. With additional clinical studies and moreclinical experience with Dysport, improved tech-niques may be developed for optimal use of theproduct. At this time, the wealth of clinical expe-rience with Botox and its well-documented safetyand efficacy can help ensure that aesthetic treat-ments provide physicians with the tools to delivera natural, relaxed look that satisfies individualneeds and goals.
Arnold W. Klein, M.D.435 North Roxbury Drive, Suite 204
Beverly Hills, Calif. [email protected]
REFERENCES1. Fagien S. Botulinum toxin type A for facial aesthetic en-
hancement: Role in facial shaping. Plast Reconstr Surg. 2003;112(Suppl.):6S.
2. Carruthers J, Fagien S, Matarasso SL. Consensus recommen-dations on the use of botulinum toxin type A in facial aes-thetics. Plast Reconstr Surg. 2004;114(Suppl.):1S.
3. Klein AW. The clinical use of botulinum toxin. Dermatol Clin.2004;22:ix.
4. Botox Cosmetic. Package insert. Irvine, Calif.: Allergan, Inc.,2005.
5. Dysport. Package insert. Berkshire, U.K.: Ipsen Ltd., 2001.6. Xeomin. Package insert. Frankfurt, Germany: Merz Pharma-
ceuticals GmbH, 2006.7. Myobloc. Package insert. South San Francisco, Calif.: Solstice
Neurosciences, Inc., 2004.8. Aoki KR. A comparison of the safety margins of botulinum
neurotoxin serotypes A, B, and F in mice. Toxicon. 2001;39:1815.
9. Bellew SG, Carroll KC, Weiss MA, Weiss RA. Sterility of storednonanimal, stabilized hyaluronic acid gel syringes after pa-tient injection. J Am Acad Dermatol. 2005;52:988.
10. Aoki KR, Guyer B. Botulinum toxin type A and other botu-linum toxin serotypes: A comparative review of biochemicaland pharmacological actions. Eur J Neurol. 2001;8(Suppl.5):21.
11. Jankovic J, Vuong KD, Ahsan J. Comparison of efficacy andimmunogenicity of original versus current botulinum toxinin cervical dystonia. Neurology 2003;60:1186.
12. Trindade de Almeida AR, Marques E, de Almeida J, CunhaT, Boraso R. Pilot study comparing the diffusion of twoformulations of botulinum toxin type a in patients with fore-head hyperhidrosis. Dermatol Surg. 2007;33:S37.
13. Aoki KR. Botulinum neurotoxin serotypes A and B prepa-rations have different safety margins in preclinical models ofmuscle weakening efficacy and systemic safety. Toxicon. 2002;40:923.
14. Hambleton P, Capel B, Bailey N. Production, purificationand toxoiding of Clostridium botulinum type A toxin. In P. S.Angel and G. E. Lewis (Eds.), Biomedical Aspects of Botulism.New York: Academic Press, 1981.
15. Aoki KR. Pharmacology and immunology of botulinum toxintype A. Clin Dermatol. 2003;21:476.
16. Markey AC. Dysport. Dermatol Clin. 200422:213.
17. Inoue K, Fujinaga Y, Watanabe T. Molecular composition ofClostridium botulinum type A progenitor toxins. Infect Immun.1996;64:1589.
18. Friday D, Bigalke H, Frevert J. In vitro stability of botulinumtoxin complex preparations at physiological pH and tem-perature (Abstract). Naunyn Schmiedebergs Arch Pharmacol.2002;365:R20.
19. Schantz EJ, Johnson EA. Properties and use of botulinumtoxin and other microbial neurotoxins in medicine. MicrobiolRev. 1992;56:80.
20. Benecke R, Jost WH, Kanovsky P. A new botulinum toxin typeA free of complexing proteins for treatment of cervical dysto-nia. Neurology 2005;64:1949.
21. Jost WH, Kohl A, Brinkmann S, Comes G. Efficacy and tol-erability of a botulinum toxin type A free of complexingproteins (NT 201) compared with commercially availablebotulinum toxin type A (Botox) in healthy volunteers. J Neu-ral Transm. 2005;112:905.
22. Borodic G. Therapeutic botulinum toxin. Lancet 1994;344:1370.
23. Borodic GE, Ferrante RJ, Pearce LB, Alderson K. Pharma-cology and histology of the therapeutic application of bot-ulinum toxins. In J. Jankovic and M. Hallett (Eds.), Therapywith Botulinum Toxin. New York: Marcel Dekker, 1994.
24. Aoki R. Preclinical update on Botox (botulinum toxin typeA)-purified neurotoxin complex relative to other botulinumneurotoxin preparations. Eur J Neurol. 1999;6:S3.
25. Aoki KR, Satorius A, Ardila C. Pharmacology of Botox, Dys-port, Myobloc and BTX-A in animal models of efficacy andsafety. Abstract presented at the International Conferenceon Basic and Therapeutic Aspects of Botulinum and TetanusToxins, Denver, Colorado, June 23–25, 2005.
26. Bihari K. Safety, effectiveness, and duration of effect of Botoxafter switching from Dysport for blepharospasm, cervicaldystonia, and hemifacial spasm. Curr Med Res Opin. 2005;21:433.
27. Blitzer A, Brin MF, Keen MS, Aviv JE. Botulinum toxin for thetreatment of hyperfunctional lines of the face. Arch Otolar-yngol Head Neck Surg. 1993;119:1018.
28. Carruthers A, Carruthers J. The treatment of glabellar furrowwith botulinum A exotoxin (Abstract). J Dermatol Surg Oncol.1990;16:83.
29. Kane MA. Nonsurgical treatment of platysmal bands withinjection of botulinum toxin A. Plast Reconstr Surg. 1999;103:656.
30. Beer K, Yohn M, Closter J. A double-blinded, placebo-con-trolled study of Botox for the treatment of subjects with chinrhytids. J Drugs Dermatol. 2005;4:417.
31. Carruthers A, Carruthers J, Lowe NJ. One-year, randomised,multicenter, two-period study of the safety and efficacy ofrepeated treatments with botulinum toxin type A in patientswith glabellar lines. J Clin Res. 2004;7:1.
32. Ascher B, Zakine B, Kestemont P. A multicenter, random-ized, double-blind, placebo-controlled study of efficacy andsafety of 3 doses of botulinum toxin A in the treatment ofglabellar lines. J Am Acad Dermatol. 2004;51:223.
33. Monheit G, Carruthers A, Brandt F, Rand R. A randomized,double-blind, placebo-controlled study of botulinum toxintype a for the treatment of glabellar lines: Determination ofoptimal dose. Dermatol Surg. 2007;33:S51.
34. Fagien S. Double-blind, placebo-controlled study of thesafety and efficacy of botulinum toxin type A for patients withglabellar lines. Plast Reconstr Surg. 2003;112:31S.
35. Carruthers JA, Lowe NJ, Menter, MA. A multicenter, double-blind, randomized, placebo-controlled study of the efficacy
Volume 130, Number 5S-3 • Comparisons among Botulinum Toxins
99S

and safety of botulinum toxin type A in the treatment ofglabellar lines. J Am Acad Dermatol. 2002;46:840.
36. Ascher B, Zakine B, Kestemont P. Botulinum toxin A in thetreatment of glabellar lines: Scheduling the next injection.Aesthetic Surg J. 2005;25:365.
37. Lowe NJ, Lask G, Yamauchi P, Moore D. Bilateral, double-blind, randomized comparison of 3 doses of botulinum toxintype A and placebo in patients with crow’s feet. J Am AcadDermatol. 2002;47:834.
38. Levy JL, Servant JJ, Jouve E. Botulinum toxin A: A 9-monthclinical and 3D in vivo profilometric crow’s feet wrinkleformation study. J Cosmet Laser Ther. 2004;6:16.
39. Matarasso A, Matarasso SL, Brandt FS, Bellman B. BotulinumA exotoxin for the management of platysma bands. PlastReconstr Surg. 1999;103:645.
40. Lowe PL, Patnaik R, Lowe NJ. A comparison of two botuli-num type a toxin preparations for the treatment of glabellarlines: Double-blind, randomized, pilot study. Dermatol Surg.2005;31:1651.
41. Lew H, Yun YS, Lee SY, Kim SJ. Effect of botulinum toxinA on facial wrinkle lines in Koreans. Ophthalmologica 2002;216:50.
42. N¨ussgens Z, Roggenkamper P. Comparison of two botuli-num-toxin preparations in the treatment of essential bleph-arospasm. Graefes Arch Clin Exp Ophthalmol. 1997;235:197.
43. Odergren T, Hjaltason H, Kaakkola S. A double blind, ran-domised, parallel group study to investigate the dose equiv-alence of Dysport and Botox in the treatment of cervicaldystonia. J Neurol Neurosurg Psychiatry 1998;64:6.
44. Ranoux D, Gury C, Fondarai J, Mas JL, Zuber M. Respectivepotencies of Botox and Dysport: A double blind, ran-
domised, crossover study in cervical dystonia. J Neurol Neu-rosurg Psychiatry 2002;72:459.
45. Simonetta Moreau M, Cauhepe C, Magues JP, Senard, JM. Adouble-blind, randomized, comparative study of Dysport vs.Botox in primary palmar hyperhidrosis. Br J Dermatol. 2003;149:1041.
46. Van den Bergh PY, Lison DF. Dose standardization of bot-ulinum toxin. Adv Neurol. 1998;78:231.
47. Marchetti A, Magar R, Findley L. Retrospective evaluation ofthe dose of Dysport and Botox in the management of cervicaldystonia and blepharospasm: The Real Dose study. Mov Dis-ord. 2005;20:937.
48. de Almeida A, Marques E, de Almeida J, Cunha T, Boraso R.Pilot study comparing the diffusion characteristics of twoformulations of botulinum toxin type A with forehead hy-perhidrosis. Presented at the European Masters in Aestheticand Anti-Aging Medicine Meeting, Paris, France, September30–October 2, 2005.
49. Cinzia L, Francesca G, Sergio B, Alfredo B. Diffusion ofbotulinum toxin in facial muscles in patients with hemifacialspasm (Abstract). Mov Disord. 2005;20:S175.
50. Eleopra R, Tugnoli V, Caniatti L, DeGrandis D. Botulinumtoxin treatment in the facial muscles of humans: Evidence ofan action in untreated near muscles by peripheral local dif-fusion. Neurology 1996;46:1158.
51. Carruthers A, Carruthers J. Long-term safety review of sub-jects treated with botulinum toxin type A for cosmetic use.Poster presented at the 13th Congress of the European Acad-emy of Dermatology & Venereology, Florence, Italy, Novem-ber 17–21, 2004.
Plastic and Reconstructive Surgery • Fall 2012
100S