conférence etudiant jeudi le 3 septembre 2015 jonathan gravel hassan khanafer
TRANSCRIPT

Conférence Etudiant Jeudi le 3 septembre 2015
Jonathan Gravel
Hassan Khanafer

Objectives• Describe the relevant findings on
history, physical examination, laboratory tests and diagnostic imaging used in evaluations of amenorrhea, and how they point to the etiology of amenorrhea
• Formulate a differential diagnosis of amenorrhea
• Describe the pharmacologic, non-pharmacologic and the surgical treatment options for amenorrhea

CaseA 17 yo nulliparous female complains that she has not yet started menstruating. She denies weight loss or excessive exercise. Each of her sisters achieved menarche by age 13 years. The patient’s mother recalls a doctor mentioning that her daughter had a missing right kidney on an abdominal x-ray film. On examination, she is 5 feet 6 inches ( cm) and weigh 65 kg. Her blood pressure is 110/60. Her thyroid gland is normal on palpation. She has Tanner stage IV breast development and female external genitalia. She has Tanner stage IV axillary and pubic hair. There are no skin lesions.

• ID: 17 year old nulliparous female
• CC: not yet started menstruating
• Present Illness:i. No weight lossii. No excessive exercise
• Family History: two sisters who achieved menarche by age 13 years
History

Physical Exam
• She is 5 feet 6 inches tall and weighs 65 kg
• Blood pressure is 110/60
• Thyroid gland is normal on palpation
• Breast Development: Tanner stage IV• Female external genitalia: Tanner
stage IV• Axillary and pubic hair: Tanner stage
IV
• No skin lesions



Diagnostic Imaging
• X-Ray film: may only have one kidney!• What is associated with renal
anomalies?
We don’t have any more information!

Primary Amenorrhea
• No menses by age 13 and absence of secondary sexual characteristics, such as breast development
OR
• No menses by age 15 in the presence of normal growth and secondary sexual characteristics • Our patient!
UpToDate

Diagnostic Approach: Primary Amenorrhea
• Step 1: History
• Step 2: Physical examination
• Step 3: Laboratory testing / Imaging

Step 1: History
UpToDate
•Other stages of puberty?•Family history of delayed or absent puberty?•Woman's height relative to family members? •Neonatal and childhood? •Symptoms of virilization : voice, hirsutism? •Stress, change in weight, diet, or exercise habits, or illness•Drugs (heroin and methadone)?•Galactorrhea?•Headaches, fatigue, or polyuria and polydipsia?

Step 2: Physical examination• Pubertal development (height, weight)?• Breast development (Tanner staging)?• Genital examination :• clitoral size• pubertal hair development• intactness of the hymen• depth of the vagina, and presence of a
cervix, uterus, and ovaries• Skin examination: hirsutism, acne,
increased pigmentation, and vitiligo• Evaluation for Turner syndrome such (low
hair line, web neck, shield chest, and widely spaced nipples) UpToDa
te

Step 3: Laboratory testing / Imaging
• Rule out pregnancy!!!!!! (bHCG)
UpToDate & Toronto Notes

DDx Primary Amenorrhea
Toronto Notes

So?
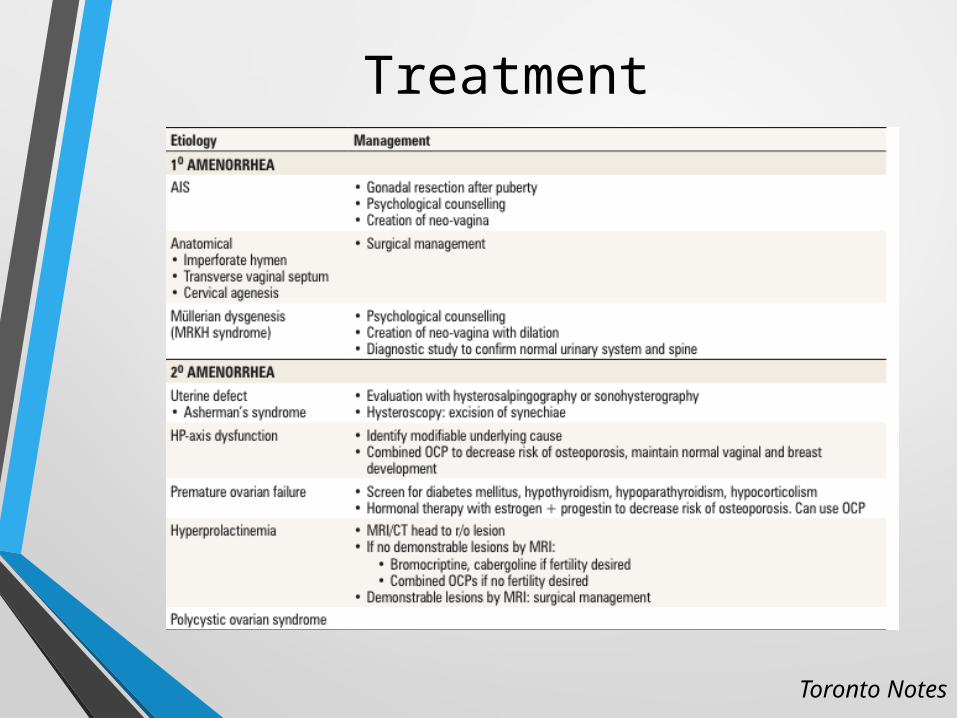
Treatment
Toronto Notes

Recap
• A pregnancy test should be the first test for any female with amenorrhea
• The two most common causes of primary amenorrhea in a woman with normal breast development are androgen insensitivity and müllerian agenesis
• Scant axillary and pubic hair suggest androgen insensitivity.
• A karyotype and testosterone level help to differentiate between müllerian agenesis and androgen insensitivity
• Renal anomalies are common with müllerian abnormalities

Secondary Amenorrhea
• Absence of menses for more than 3 consecutive months in girls or women who previously had regular menstrual cycles
OR
• Absence of menses for more than 6 consecutive months in girls or women who had irregular menses
UpToDate

Diagnostic Approach: Secondary Amenorrhea
• Step 1: Rule out pregnancy (bHCG)Pregnant until proven otherwise!
• Step 2: History
• Step 3: Physical examination
• Step 4: Laboratory testing / Imaging
UpToDate

Step 2: History
UpToDate
• Stress, change in weight, diet or exercise habits, or illness?
• Any drugs: OCP, metoclopramide?• Acne, hirsutism, or deepening of the
voice?• Hot flashes, vaginal dryness, poor sleep,
or decreased libido?• Is there galactorrhea?• Severe bleeding, dilatation and
curettage, or endometritis or other infection that might have caused scarring of the endometrial lining (Asherman syndrome)?

Step 3: Physical examination
• Height, weight: BMI ?• Skin examination: hirsutism, acne, striae,
acanthosis nigricans, vitiligo and easy bruisability.
• Evaluation for Turner syndrome such (low hair line, web neck, shield chest, and widely spaced nipples …).
• Breast examination for galactorrhea?• Vulvovaginal examination for estrogen
deficiency?• Parotid gland swelling and/or erosion of
dental enamel (eating disorder)?UpToDate

Step 4: Laboratory testing / Imaging
Depending on the findings of the bHCG, History and physical examination: • PL• Progestin challenge• FSH/LH• TSH• Total testosterone
UpToDate & Toronto Notes

DDx Secondary Amenorrhea
Toronto Notes

Treatment
Toronto Notes

MERCI!