congenital, inflammatory and infectious diseases of the lung
TRANSCRIPT
Congenital, inflammatory and infectious diseases of the lung
Most congenital diseases of the lung are recognized when respiratory symptoms develop in the newborn or infant.
Prenatal diagnosis
Asymptomatic child, incidental radiograph of the chest
Older child during evaluation for a respiratory tract infection
Disease range: Simple abnormal bronchus ..... Complete absence of one lung
Radiologic evaluation :chest X-ray, ultrasonography, computed tomography
Embryologic development of the lungs: 4 stages
Embryologic phase (26th day – 5th week) : lung bud disease: tracheo-esophageal fistula, bronchopulmonary foregut malformations, tracheobronchial atresia, tracheal bronchial diverticule
Pseudoglandular phase (5th week – 16 th week) : disease: congenital cystic adenomatoid malformation
Canalicular phase (16th week – 25th week) : Terminal saccule (alveolar period) (25th week – 40th
week) : saccular proliferation and progressive vascularization. Disease: extreme proliferation and no vascularization: congenital lobar emphysema

TRACHEO-BRONCHIAL ANOMALIES - I Tracheal Agenesia – Atresia: Fatal. Maternal
polyhidramnios and prematurity. Scream when born, then progressive cyanosis, bradycardia, arrest. ETcan not pass byond vocal cords. Esophageal entubation (TEF).
Tracheal Malacia: elastic and connective tissue degeneration. Structural deformation of the cartilage. Tracheal wall collapse during inspiration. Cyanotic spells in newborn, stridor. Recuurent pneumonia attacks. Asso. With esophageal atresia and TEF. Dianosis: bronchoscopy, CT, Virtual bronchoscopy and MRI.Conservative treatment, surgery, intraluminal absorbable stents
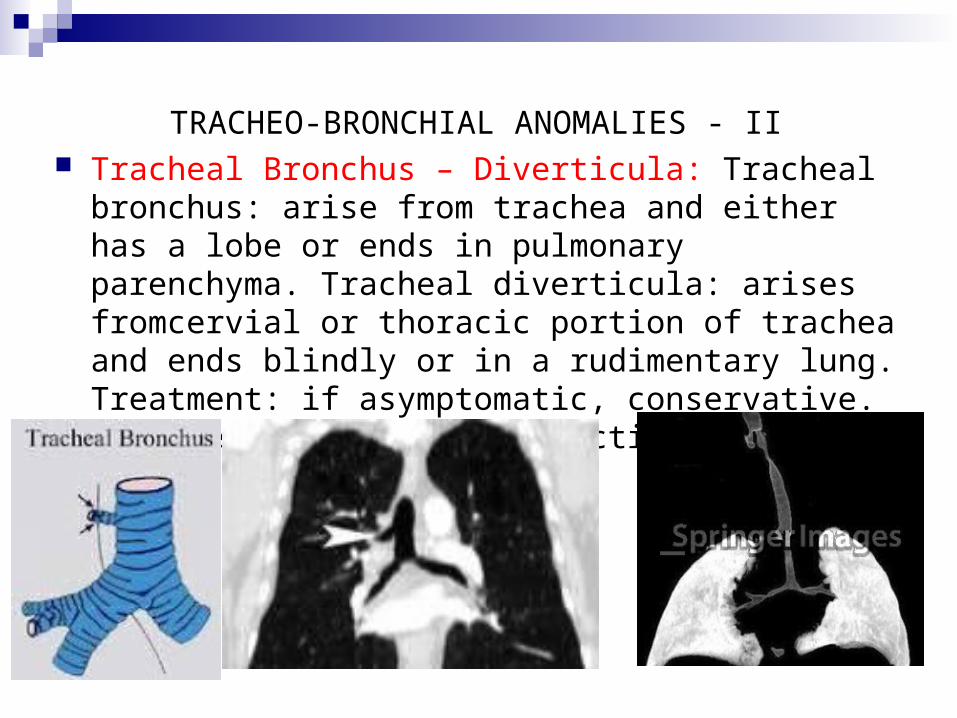
TRACHEO-BRONCHIAL ANOMALIES - II Tracheal Bronchus – Diverticula: Tracheal bronchus:
arise from trachea and either has a lobe or ends in pulmonary parenchyma. Tracheal diverticula: arises fromcervial or thoracic portion of trachea and ends blindly or in a rudimentary lung. Treatment: if asymptomatic, conservative. Recurrent infections: resection

TRACHEO-BRONCHIAL ANOMALIES - II
Laryngo-tracheo-esophageal Cleft: Fatal. Aspiration of the ingested food. Chooking while feeding. Surgery.
TRACHEO-BRONCHIAL ANOMALIES - III Bronchial Atresia: ends blindly in lung tissue. At birth,
portion of lung adjacent to atretic bronchus is filled with fluid. Fluid is absorbed. Retained secretions result in a mucocele. Obstructive emphysema occurs. Recurrent episodes of infection. Differential diagnosis: Congenital lobar emphysema and bronchogenic cysts. Bronchoscopy and CT. Surgery.
Anomalous Bronchi: most common communication between trachea and another foregut derivative is tracheoesophageal fistula. Pneumonia attacks
Tracheobiliary and bronchobiliary Fistula: bile-stained secretions, respiratory distress. Bronchoscopy and fistulography.
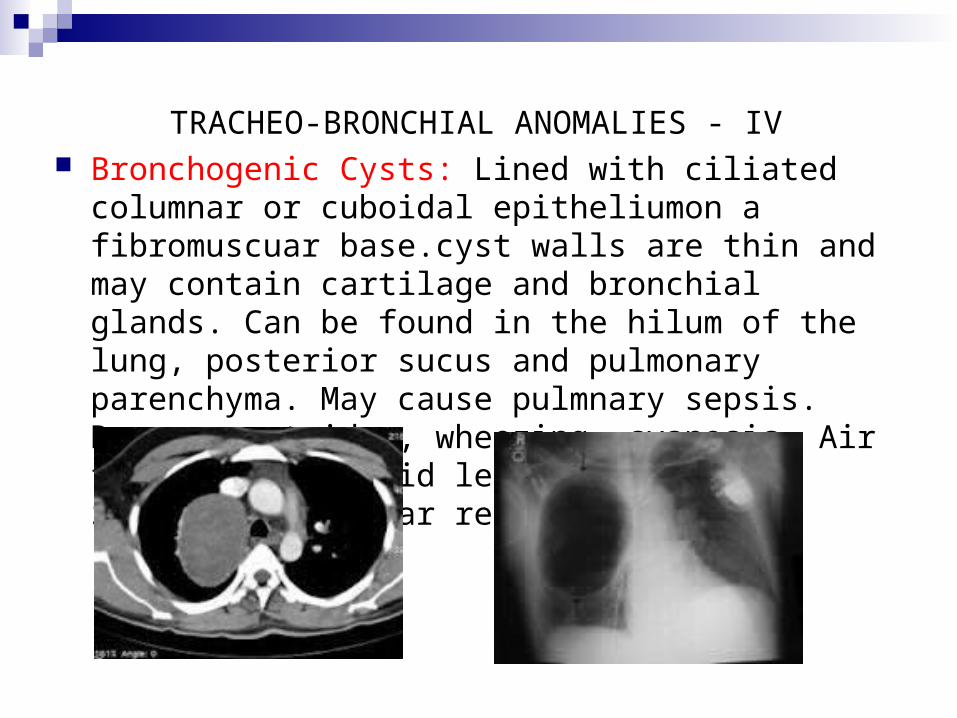
TRACHEO-BRONCHIAL ANOMALIES - IV Bronchogenic Cysts: Lined with ciliated columnar or
cuboidal epitheliumon a fibromuscuar base.cyst walls are thin and may contain cartilage and bronchial glands. Can be found in the hilum of the lung, posterior sucus and pulmonary parenchyma. May cause pulmnary sepsis. Dyspnea, stridor, wheezing, cyanosis. Air filled , air-fluid level. Surgery. Segmental or lobar resection.
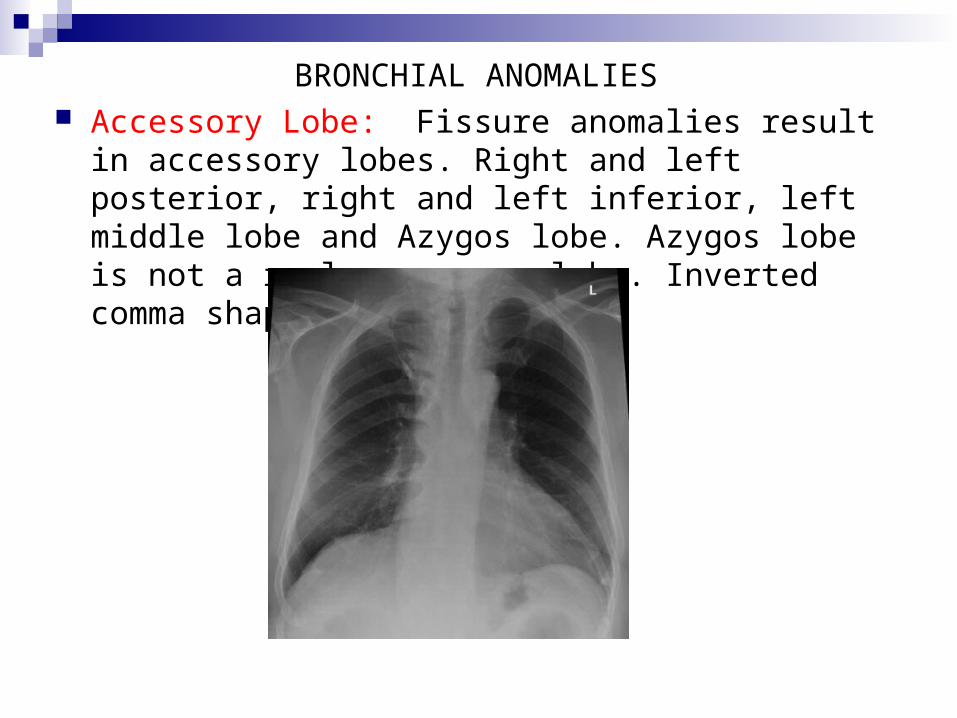
BRONCHIAL ANOMALIES Accessory Lobe: Fissure anomalies result in accessory
lobes. Right and left posterior, right and left inferior, left middle lobe and Azygos lobe. Azygos lobe is not a real accessory lobe. Inverted comma shape.
BRONCHIAL ANOMALIES Pulmonary Agenesia – Aplasia - Hypoplasia: Range from
single hypoplasia of a segment or lobe to double lung absence. Agenesia: absence of a structure. Aplasia: defective development. Primary hypoplasia and secondary hypoplasia (intrauterine
intrathoracic space problems: congenital diaphragmatic hernia, congenital cystic adenomatoid malformation, hydrops fetalis with pleural effusion, mediastinal neoplasms, cystic hygroma; Chest wall anomalies resulting in thoracic volume decrement: thoracic dystrohies (Jarco-Levin and Jeune synd), osteogenesis imperfecta; oligohydramnios syndrome (uterine distress over the fetus)
BRONCHIAL ANOMALIES Pulmonary Sequestration:
Most common developmental lung disease A segment or lobe of the lung tissue has no bronchial
communication with the normal tracheobronchial tree. Arterial blood supply is from a systemic artery. This vessel arises from abdominal aorta. Venous return is to systemic (azygos) or pulmonary veins.
Extralobar sequestration: (25%) seperate from normal lung and has its own visseral pleura. 90% on left side.
Intralobar sequestration: Within normal lung parenchyma. Abscess formation
CT – angio and MRI Surgery

BRONCHIAL ANOMALIES Pulmonary Sequestration:
BRONCHIAL ANOMALIES Congenital Lobar Emphysema:
isolated hyperinflation of a lobe in the absence of extrinsic bronchial obstruction.
Left upper lobe most commonly, second right middle lobe. Defective cartilage structure results in bronchial wall weakness,
collapse of the bronchus during expiration and air-trap Differential diagnosis: pneumothorax, tension cyst, congenital
diaphragm hernia and foreign body aspiration Tachypnea, retraction of the chest wall, wheezing since birth Tracheal and mediastinal shift to the contralateral hemithorax Breath sounds are decreased on the affected side, hyperresonance X-ray: hyperaeration of the affected lobe with atelectasis of the
adjacent lobes and a mediastinal shift CT: hyperlucent expanded lobe Surgery

BRONCHIAL ANOMALIES Congenital Lobar Emphysema:
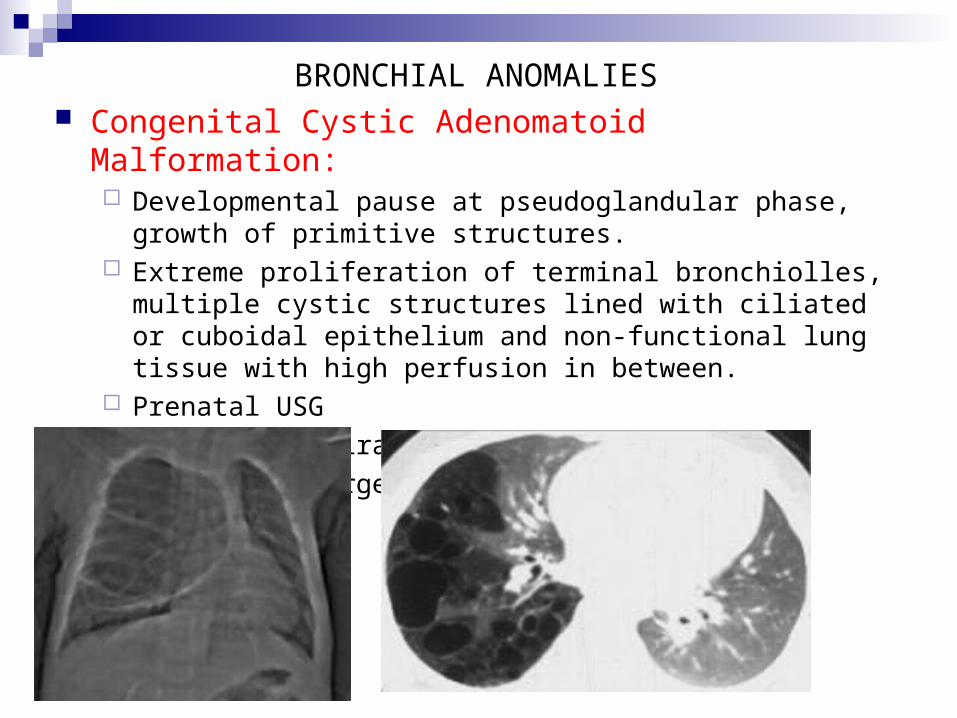
BRONCHIAL ANOMALIES Congenital Cystic Adenomatoid Malformation:
Developmental pause at pseudoglandular phase, growth of primitive structures.
Extreme proliferation of terminal bronchiolles, multiple cystic structures lined with ciliated or cuboidal epithelium and non-functional lung tissue with high perfusion in between.
Prenatal USG Neonatal respiratory distress Emergency, Surgery
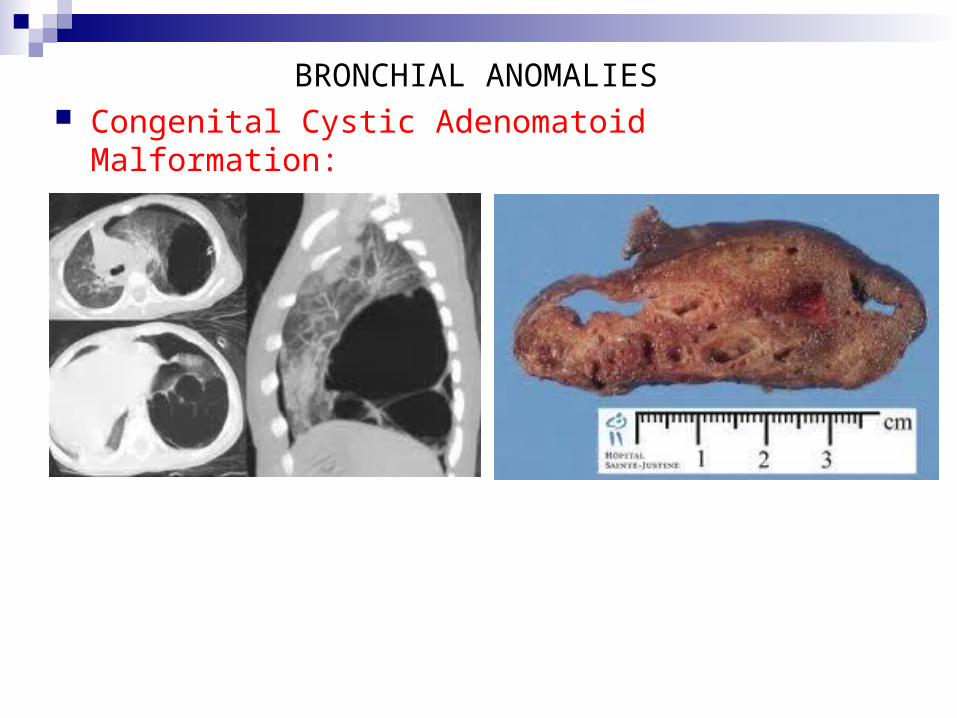
BRONCHIAL ANOMALIES Congenital Cystic Adenomatoid Malformation:
CONGENITAL VASCULAR LESIONS Agenesis and Stenosis of the pulmonary artery:
Die at early age from right-sided ventricular failure and hypertension in the pulmonary artery of the unaffected side
Pulmonary Arteriovenous Fistulas Most common anomaly of pulmonary vascular tree Hereditary hemorrhagic telangiectasia (Rendu-Osler-Weber
syndrome Exertional dypsnea, palpitations, easy fatigability Hypoxia, blood gas analysis CT-Angio Surgery, embolic obliteration
Pulmonary artery Aneurysms Abnormal pulmonary venous connection Lymphangiectasia
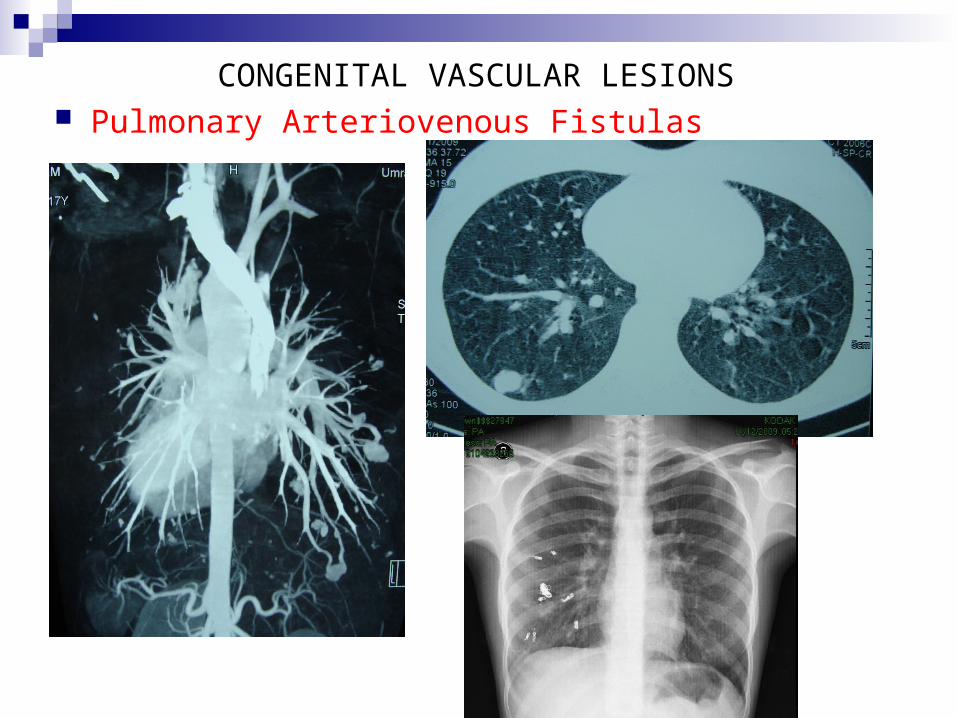
CONGENITAL VASCULAR LESIONS Pulmonary Arteriovenous Fistulas
INFLAMMATORY AND INFECTIOUS DISEASES Cystic Fibrosis Bronchiectasis Lung Abscess Right Middle Lobe Syndrome Broncholithiasis Pulmonary Tuberculosis Mycotic and Actinomycetic Infections Hydatid Disease of the lung
INFLAMMATORY AND INFECTIOUS DISEASES Cystic Fibrosis
AR disease, mutations in a single gene that encodes CF transmembrane conductance regulator (CFTR) protein
CF gene on long arm of chr 7 Chronic sinopulmonary infections, impaired exocrine pancreatic
function, elevated sweat chloride, male infertility Most common lethal genetic disease in whites Median predicted survival 36.5 years X-ray: hyperinflation with flattening of domes of diapragm,
increase in postero-anterior diameter of chest Diffuse cystic interstitial process Surgery for pulmonary complicatios (pneumothorax, hemoptysis) Lung transplantation

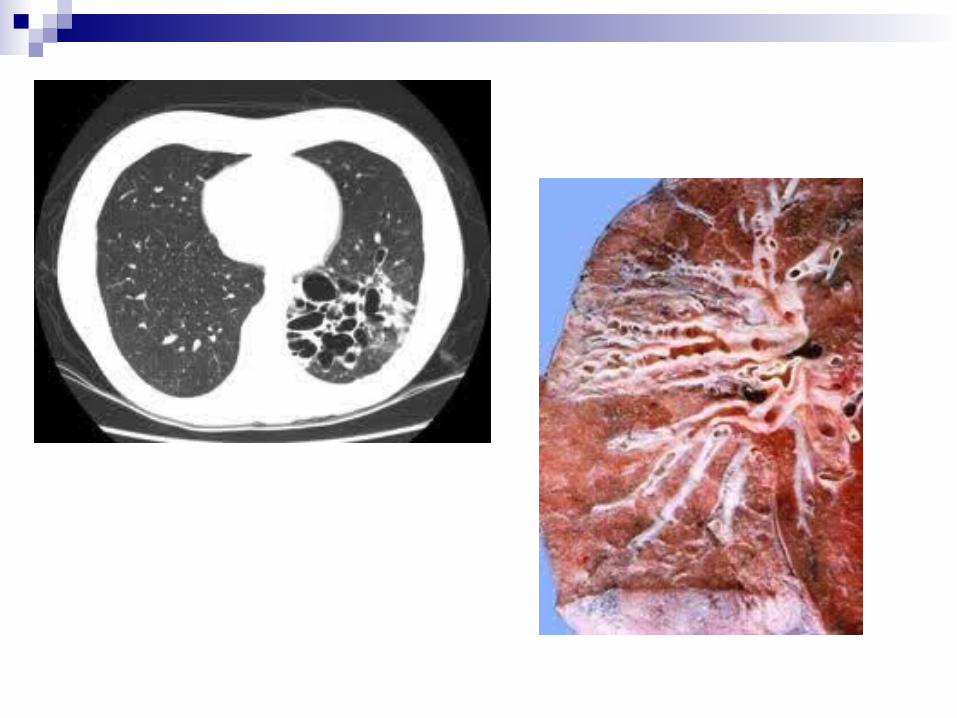
INFLAMMATORY AND INFECTIOUS DISEASES Bronchiectasis
Abnormal permanent dilatation of subsegmental airways Etiology:
Congenital Congenital cystic bronchiectasis Selective immunoglobulin A deficiency Cystic fibrosis (most common) Alpha-1 antitrypsin deficiency Kartagener’s syndrome (most common)
Acquired Infection (most common) Bronchial obstruction Middle lobe syndrome Scarring secondary to tuberculosis

INFLAMMATORY AND INFECTIOUS DISEASES Bronchiectasis
Classification: Saccular (follows a major pulmonary infection or results from foreign
body or bronchial stricture and is the principal type of surgical importance)
Cylindrical (consists of bronchi that do not end blindly but communicate with lung parenchyma. Frequently asso. with tuberculosisi and immune disorders)
Pseudobronchiectasis (cylindrical dilatation of a bronchus after an acute pneumonic process that is temporary and disapperas in weeks)
Posttuberculous bronchiectasis
INFLAMMATORY AND INFECTIOUS DISEASES Bronchiectasis
Frequency of Distribution of bronchiectasis: Left lung more often than right lung Left lower lobe: most frequently involved Right middle lobe and lingula: next most frequently involved Total left bronchiectasis, fourth most commonly involved Right lower and total right are less often involved Right upper lobe is involved more than left upper lobe (4:1)
HRCT Treatment:
Medical: preventive and control, antibiotics, postural drainage Surgical:
Unilateral, segmental or lobar distribution Persistent, recurrent symptoms when medication is discontinued Recurrent infection and hemoptysis Transplantation

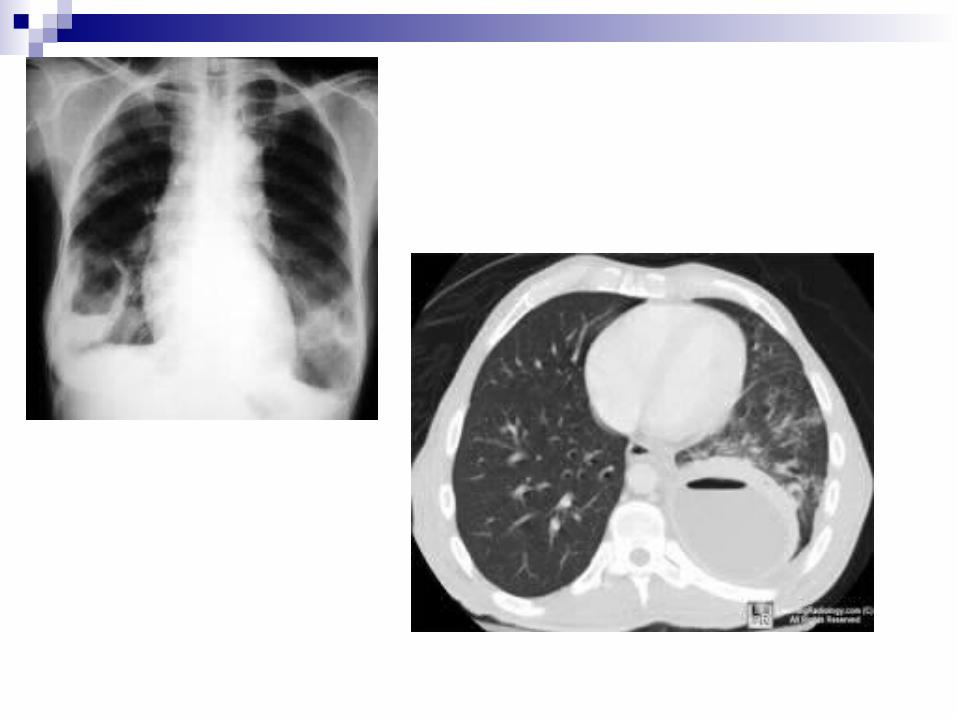
INFLAMMATORY AND INFECTIOUS DISEASES Lung Abscess
Subacute pulmonary infection in which chest radiograph shows a cavity within the pulmonary parenchyma
Localised collection of pus contained within pulmonary parenchyma An abscess is defined as acute when duration of symtoms is <6 weeks Classification :
Primary lung abscess (acute or chronic) Related to anaerobic aspiration Related to specific pneumonia
Secondary lung abscess With existing lung disease Metastatic from extrathoracic source Obstructing bronchial carcinoma Bronchoesophageal fistula Foreign body aspiration Pulmonary infarction Bullous emphysema
INFLAMMATORY AND INFECTIOUS DISEASES Lung Abscess
Most frequent anaerobic cause: Bacteroides Most frequent aerobic cause: staphylococcus aureus and
streptococcus pneumoniae Diagnostic techniques: H, PE, fever, purulent foul smelling-
sputum, FOB, CT Differential Diagnosis:
Cavitating carcinoma Tuberculous or other fungal diseases Pyogenic lung abscess Empyema with bronchopleural fistula

INFLAMMATORY AND INFECTIOUS DISEASES Lung Abscess
Principles of Therapy: Identification of etiologic organism Prolonged antimicrobial treatment Adequate drainage in acute stage Chest physiotherapy Bronchoscopy Percutaneous catheter drainage Emergency surgical treatment
INFLAMMATORY AND INFECTIOUS DISEASES Lung Abscess
Indications for Surgery: Acute Stage (emergency)
Complications Bronchopleural fistula Empyema Bleeding
Chronic Stage Persistent symptoms and signs Recurrent complications (empyema, fistula) Suspicion of carcinoma Persistence of lung abscess larger than 6 cm after 8 weeks of
treatment

INFLAMMATORY AND INFECTIOUS DISEASES Right Middle Lobe Syndrome
Episodes of hemoptysis, chronic cough and repeated pulmonary infections, atelectasis of right middle lobe
Bronchial obstruction CT
Broncholithiasis Isolated area of bronchial compressive disease, calcified lymph node
eroded into the lumen of a bronchus, distortion or partial obstruction of the tracheobronchial tree by calcified peribronchial lymph nodes
Pathogenesis is caused by tissue response to a healing granulomatous inflammation. Most frequent involved diseases are histoplasmosis and tuberculosis
CT, FOB Indications for surgery: intractable cough, recurrent hemoptysis, chronic
infection resulting from bronchostenosis or a secondary esophagobronchial fistula
INFLAMMATORY AND INFECTIOUS DISEASES Pulmonary Tuberculosis
Patients with lungs destroyed by MDR TB or cavitary disease with or without positive sputum smears will require resection
Decortication alone for a trapped lung Other patients who require surgical intervention are those with
bronchopleural fistulas, massive hemoptysis (>600ml in 24 hours), bronchostenosis or in whom there is a need to rule out cancer
INFLAMMATORY AND INFECTIOUS DISEASES Hydatid Disease of the lung
Endemic areas Middle East, Mediterranean countries, South America, Australia, New Zealand, Central Asia, China, Alaska and East Africa
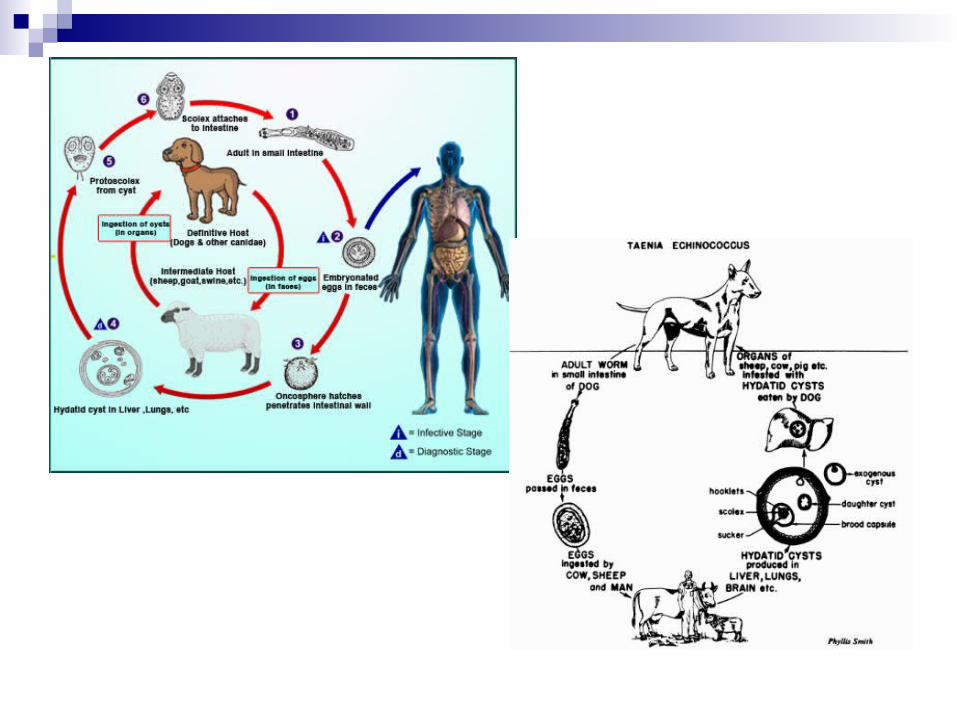
Caused by Echinococcus granulosus Primary host: Canidae family, dogs, wolves, coyotes. They contract echinococcosis by ingesting mature, productive
echinococcal cysts in the viscera of an intermediate host (sheep, goats, cattle, deer)
In the intestines of primary host, cyst develops into worm containing 400 to 800 ova. Ova are released in the feces of the primary host, introduced into intermediate hosts by ingestion of contaminated grass, water, vegetables.
In GI tract of intermediate host ovum develops into embryo, with hooklets penetrates mucosa od duodenum and jejenum, enters mesenteric venules, proceeds to portal vein and liver.
INFLAMMATORY AND INFECTIOUS DISEASES Hydatid Disease of the lung
Embryos <0.3 mm pass through snus capillaries of liver and by hepatic veins and vena cava proceed to right side of heart and pulmonary capillaries.
Alternative way: embryos enter lymphatics of small intestine, proceed to thoracic duct, to central venous system, to right side of heart and to lungs.
Another way: venovenous anastomosis in the liver Most common infected organ : LIVER (60-80%) Lung (10-30%) Hydatid cyst : wall + hydatid fluid Wall has 3 layers: outer laminated membrane and inner
germinative membrane derive from parasite and pericyst or adventitia (ectocyst) is produced by host.

INFLAMMATORY AND INFECTIOUS DISEASES Hydatid Disease of the lung
Germinative membrane is the living part. Hydatid fluid: odorless, colorless, sterile, crystal-clear water. Cyst may rupture during the growth period. Rupture of germinative membrane toward the interior of the cyst
result in formation of daughter cysts. Clinical presentation depends on whether cyst is intact or
ruptured. Intact cyst : no symptom, cough, hemoptysis, pain Ruptured: expectoration of salty sputum Rupture into pleural cavity. 5% X-ray: homogeneous spherical opacity with definite edges. Change from spherical to an oval shape only during inhalation
(Escudero-Nemerow sign)
INFLAMMATORY AND INFECTIOUS DISEASES Hydatid Disease of the lung
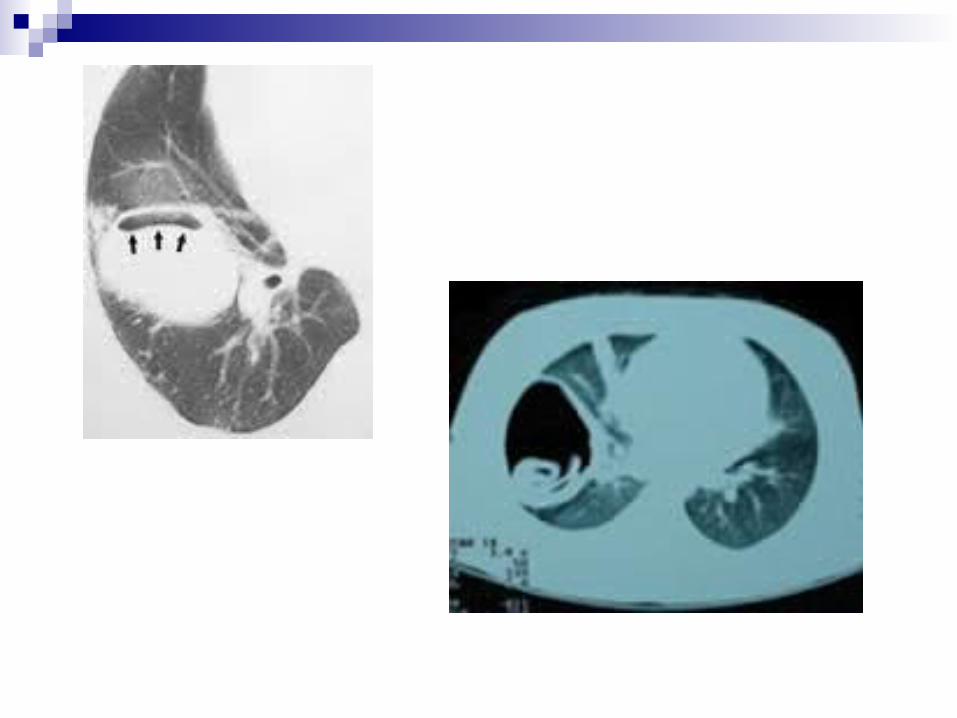
Crescent sign, moon sign, meniscus sign: clear crescent shadow on the top or on one side: first sign of rupture
Double domed arch sign: small additional air enters in. Camalote sign, water lily sign: enterance of free air into cyst after
complete rupture of the membrane. Floating membrane of the cyst.
CT, MRI, USG, ECHO Eosinophilia IHA: 80-94% in liver, 65% in lung Treatment:Albendazle, mebendazole: who cannot tolarate
surgery, numerous cysts, when complete removal is impossible., postoperative.
Surgery is the mainstay
INFLAMMATORY AND INFECTIOUS DISEASES Hydatid Disease of the lung
SURGERY: lung-sparing surgery Enucleation (Barret) Pericystectomy +/- capitonnage (Perez-Fontana) Cystotomy + capitonnage Segmentectomy/lobectomy/pneumonectomy
Bilateral: larger cyst or multiple cystic side, intact cyst
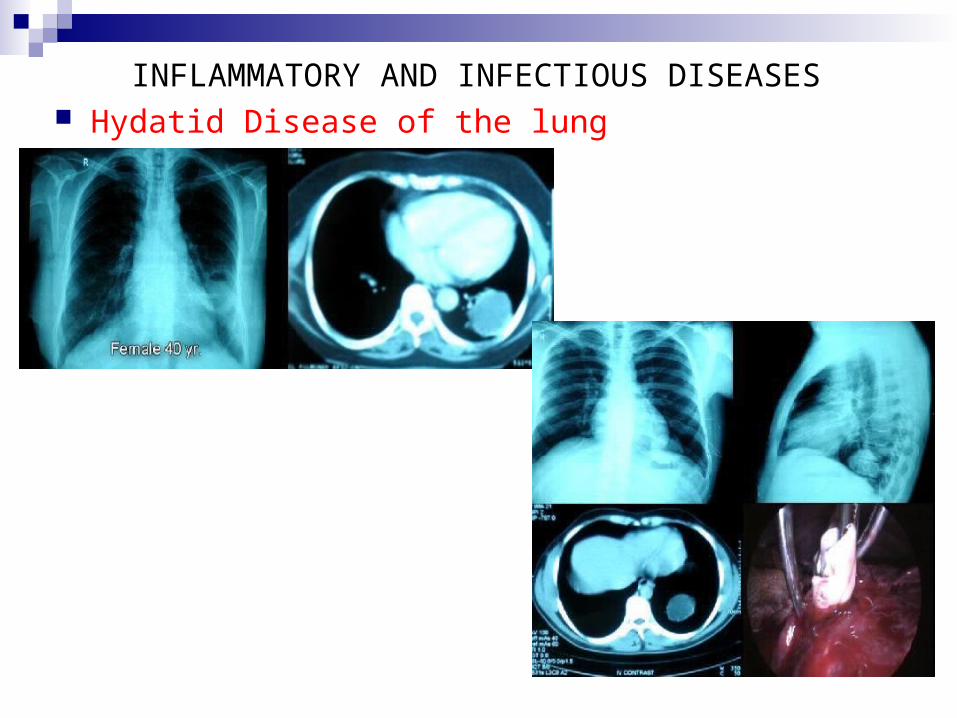
INFLAMMATORY AND INFECTIOUS DISEASES Hydatid Disease of the lung

INFLAMMATORY AND INFECTIOUS DISEASES Hydatid Disease of the lung
