consecutive aneurysms treated by endovascular approach
TRANSCRIPT
Consecutive aneurysms treated by endovascular approach- our experience
Talk at ISNR 2014 (annual conference of Indian Society of Neuroradiology, Delhi)
Vipul GuptaNeurointerventional Surgery(Interventional Neuroradiology)Institute of Neurosciences Medanta the Medicity

ANEURYSMS- basic facts
• Subarachnoid hemorrhage (SAH).• One in every 20 strokes , at the
prime of ones life (commonly between 40-50yrs).
• Up to 40-50% patients do not survive even for a month mostly because of the rerupture of the aneurysm
• With proper treatment up to 90% of patient who reach hospital before any major damage has happened will lead an independent and productive life
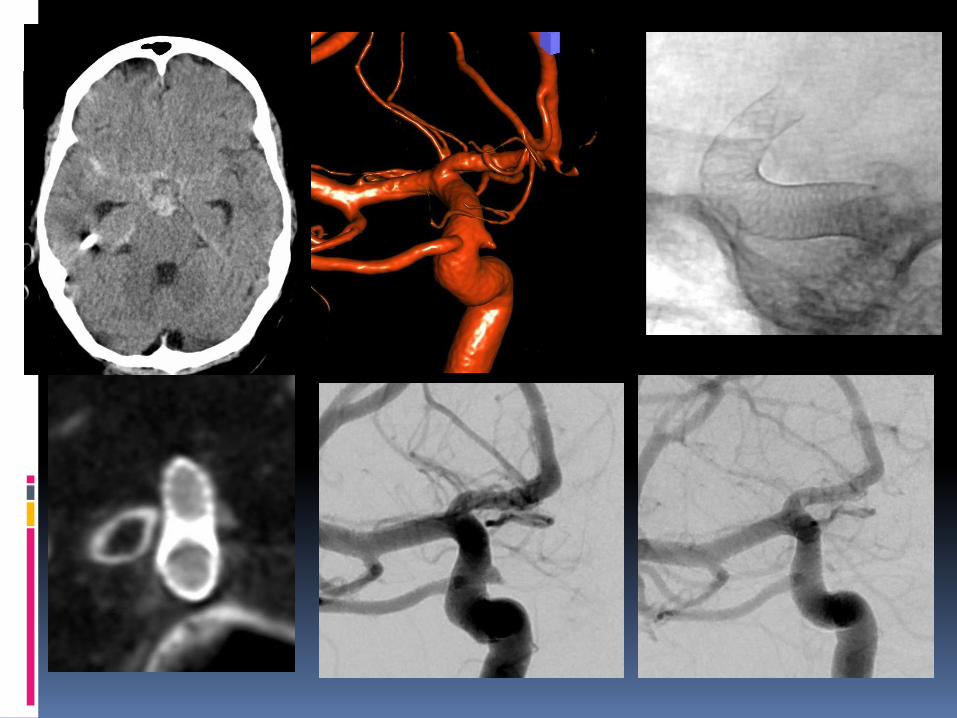
Initial CT Scan
Rebleeding after 1 day

ISAT Randomized, prospective, international trial
Clipping vs coiling 9559 patients screened,
2143 randomized at 1 year, the difference
in the risk of dependency or death between the two groups was 6.9% and the relative risk reduction was 22.6% (in the coiling group)
ISAT follow-up, Lancet 2009- death at 5 years lower
The Barrow Ruptured Aneurysm Trial
Compared clipping vs coiling in SAH patients. Poor outcome - 33.7% in clipping vs 23.2% in coiling
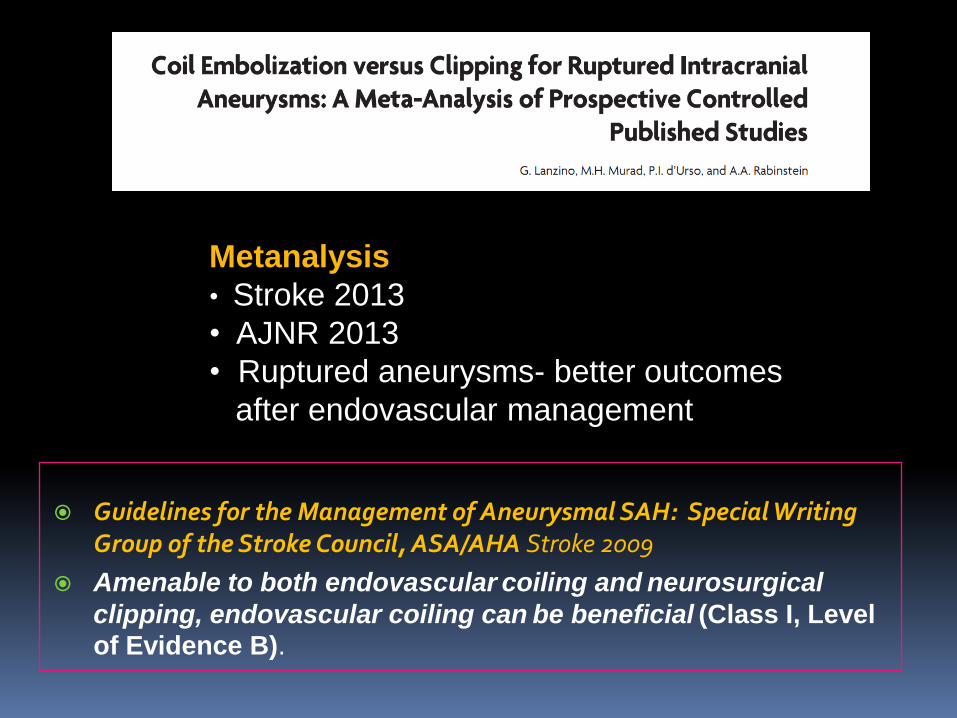
Guidelines for the Management of Aneurysmal SAH: Special Writing Group of the Stroke Council, ASA/AHA Stroke 2009
Amenable to both endovascular coiling and neurosurgical
clipping, endovascular coiling can be beneficial (Class I, Level
of Evidence B).
Metanalysis
• Stroke 2013
• AJNR 2013
• Ruptured aneurysms- better outcomes
after endovascular management

In the ISAT and BRAT trials only 39.8% and 62.3% percentage of patients respectively were treated by endovascular approach
• Image-guidance (3-D , Dyna-CT)
• Coil, catheter, balloons, stents
• Drugs- aspirin, clopidogrel, abciximab
• Appx. 90% by endovascular
• Intra-arterial vasospasm mgt.
• HELP and Cerecyte studies – mRS 0-2 in 87% (80% in ISAT)

Coiling as first choice…
Lubicz B et al of 167 patients treated by coiling as first intention, 87.3% coiled, surgery in 12.7% cases.
(Lubicz B, et alEndovascular treatment of intracranial aneurysms as the first thérapeutic option. J Neuroradiol. 2007; 34(4):250-9)
Clarity GDC study- 405 patients, 19 French centers, coilig- 402 cases, 3 – clipping
(Cognard C, et al, Clarity Study Group. Results of embolization used as the first treatment choice in a consecutive nonselected population of ruptured aneurysms: clinical results of the Clarity GDC study. Neurosurgery. 2011;69(4):837)
Multicentre series of 705 ruptured intracranial aneurysms, 96.9% feasibility of the endovascular technique was achieved.
(Sophie Gallas, et al. A Multicenter Study of 705 Ruptured Intracranial Aneurysms Treated with Guglielmi Detachable Coils. AJNR Am J Neuroradiol 2005; 26:17230

Our protocol
Interventionist part of neurosurgery team
DSA & if possible embolization Neuro lab with 3D, CT NS ICU monitoring (TCD/CTP). Vasospasm- IAVD N- 706 (Sept 2014) Data of consecutive patients


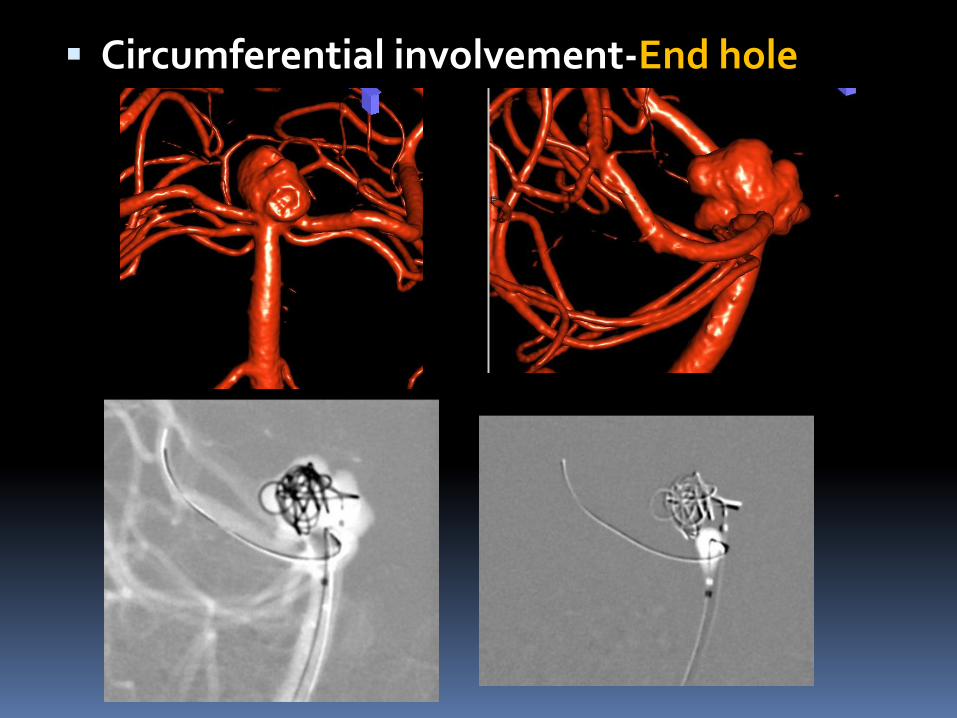
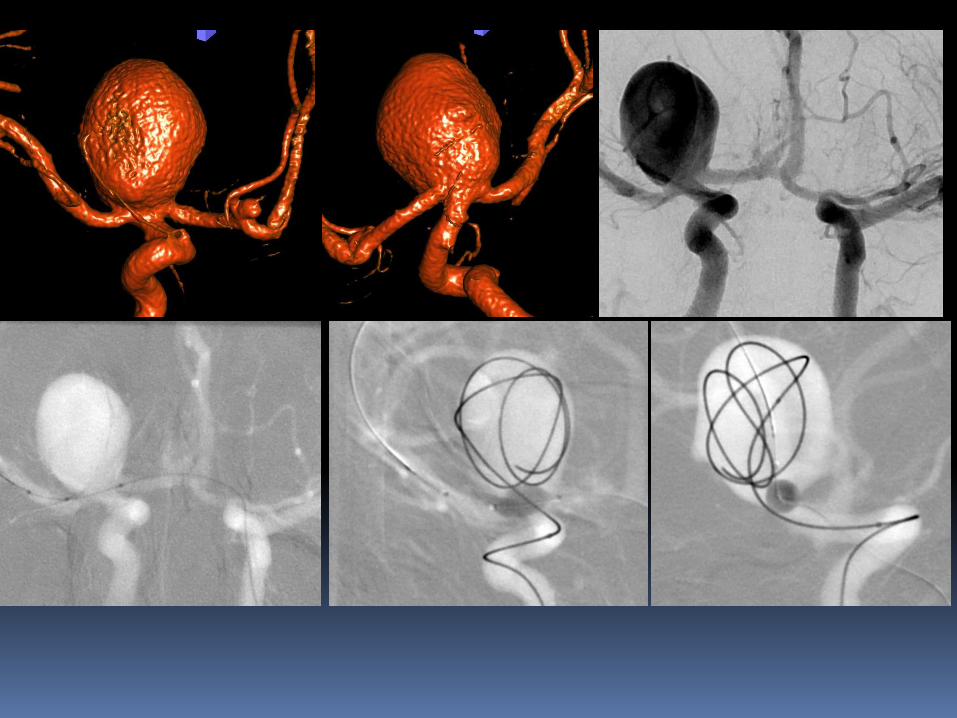
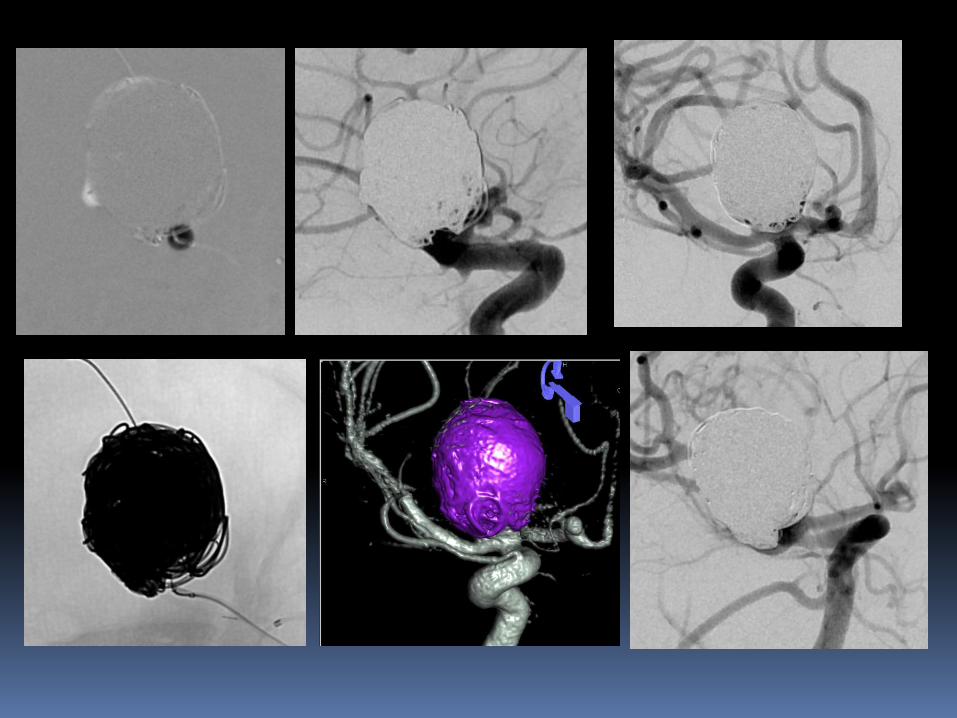
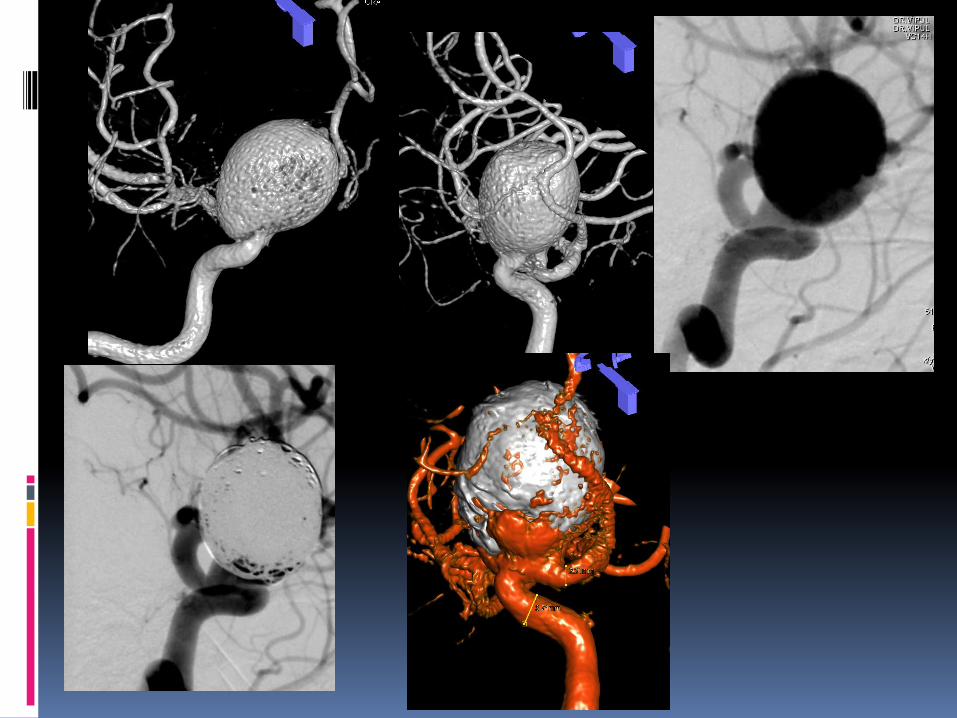
Circumferential involvement-End hole

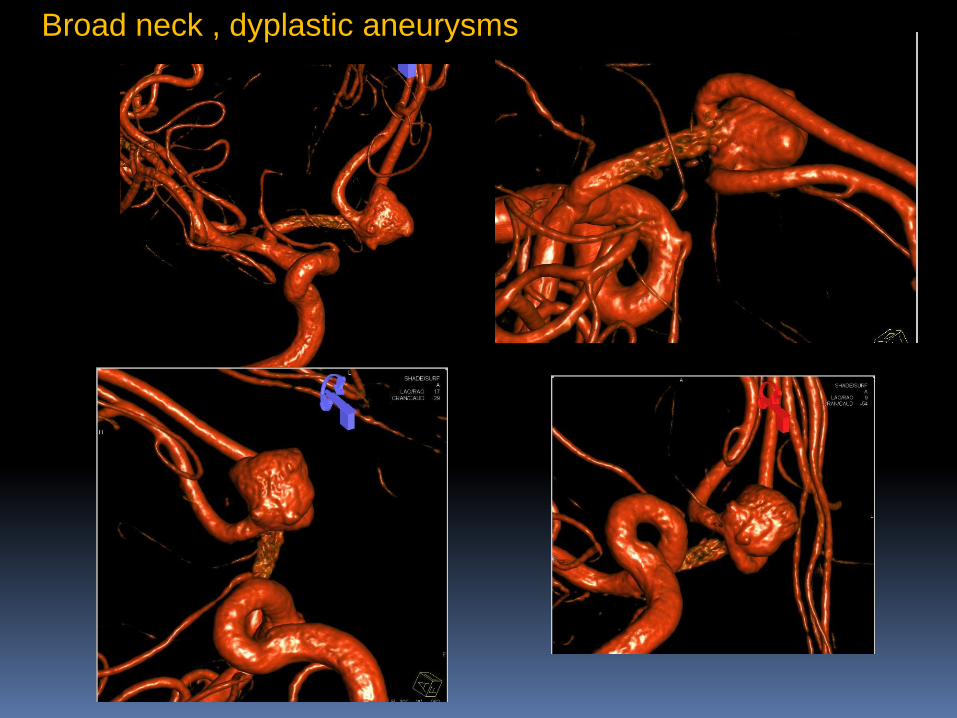
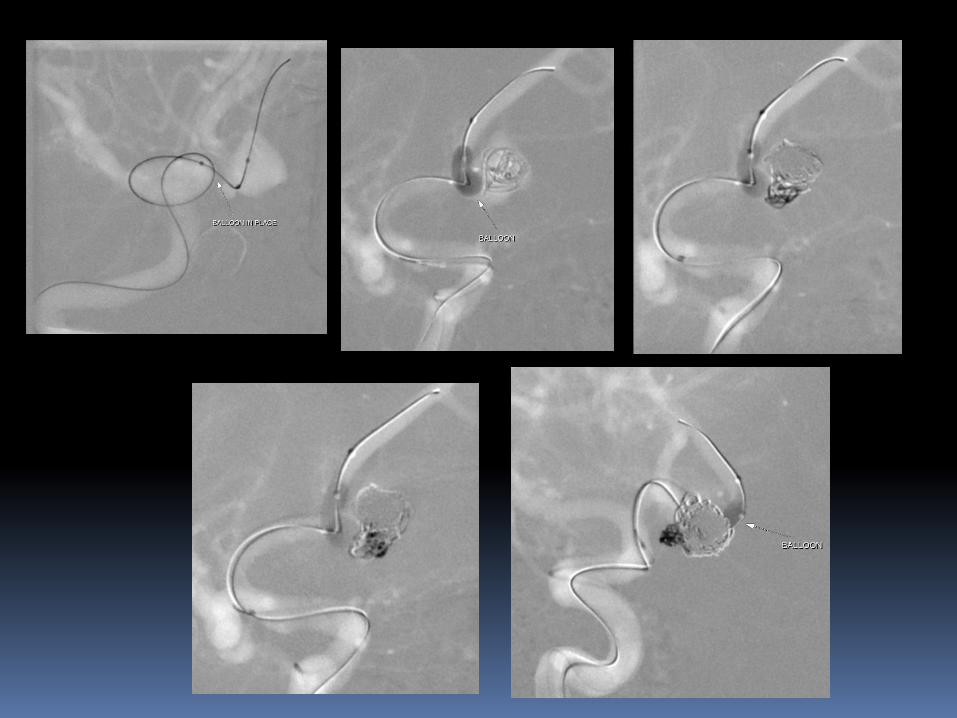
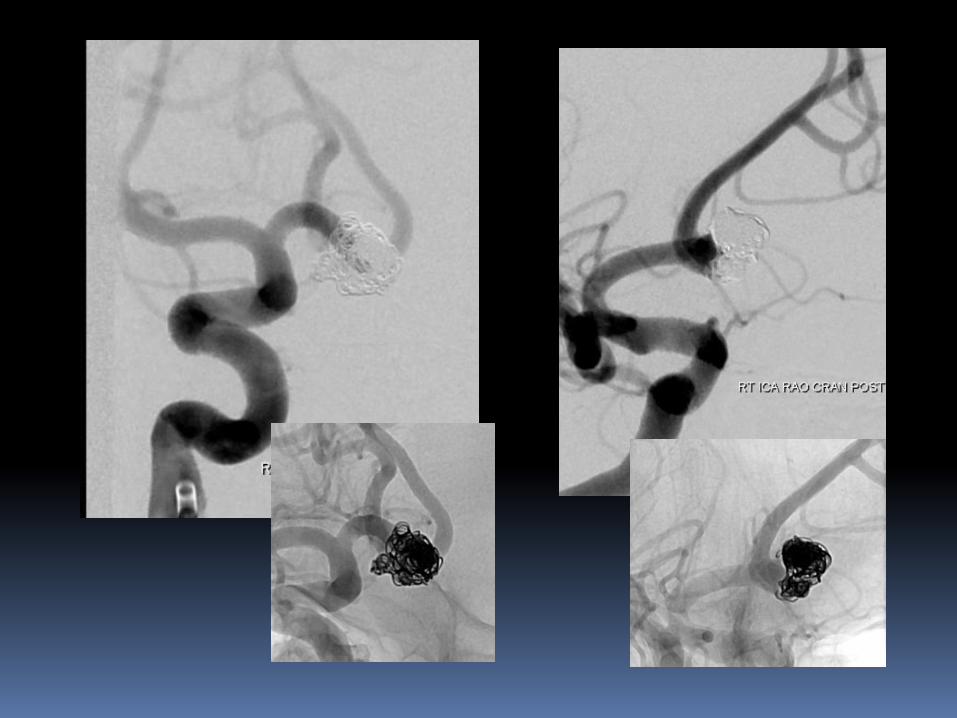
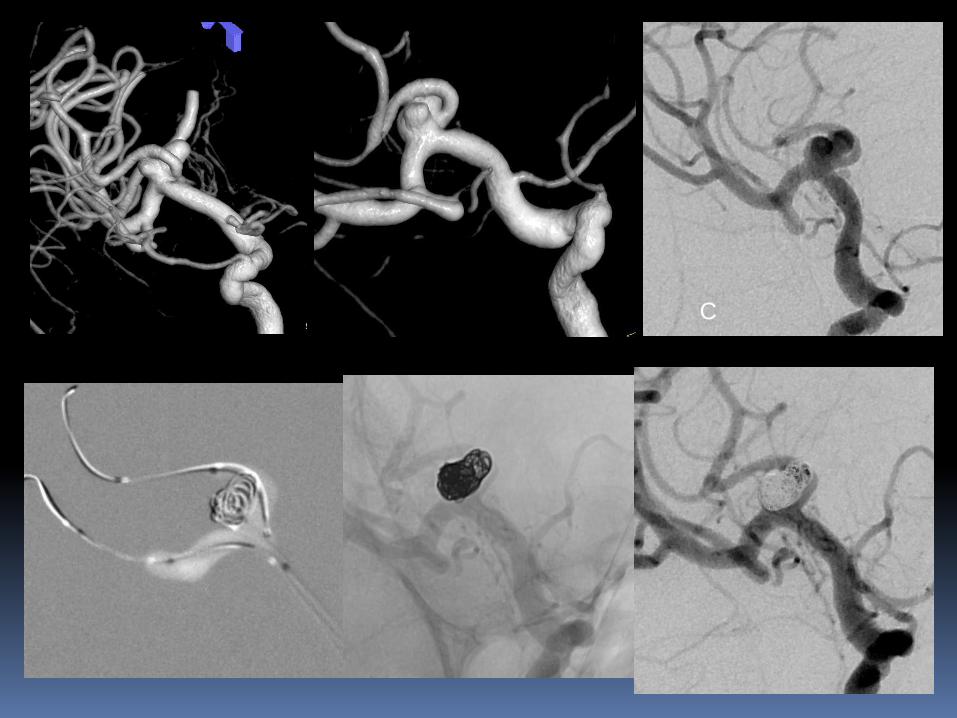
Broad neck , dyplastic aneurysms
A B C

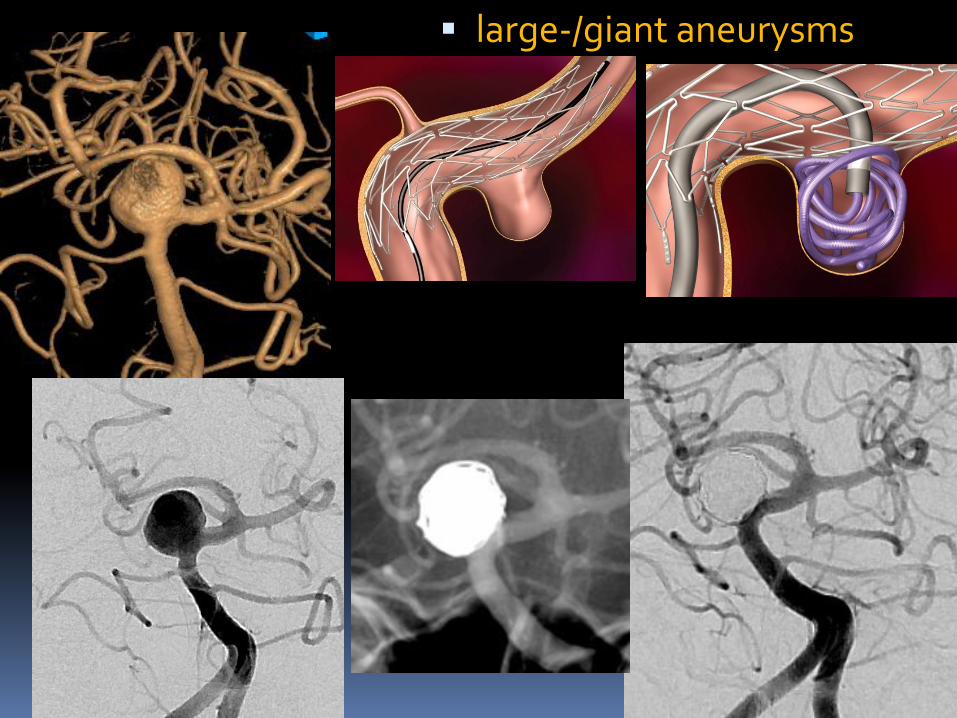
large-/giant aneurysms
Data
• Retrospective review of 548 intracranial aneurysms
• 35 aneurysms in 33 patients -F- 19, M-14; 30-68 yrs
• Fisher grade III SAH - 22 (66.6%)
• H& H grade- I-III - 27 (81.8%)• EVD/ Lumbar drainage - 8 (24.2%)
• <14 days of SAH - 26(78.7%)
•
• Wide Neck aneurysms - 16
• Dissecting and/or blister aneurysms - 19
• Single (28) or double overlapping (5) stents with additional coil placement in 26 aneurysms.

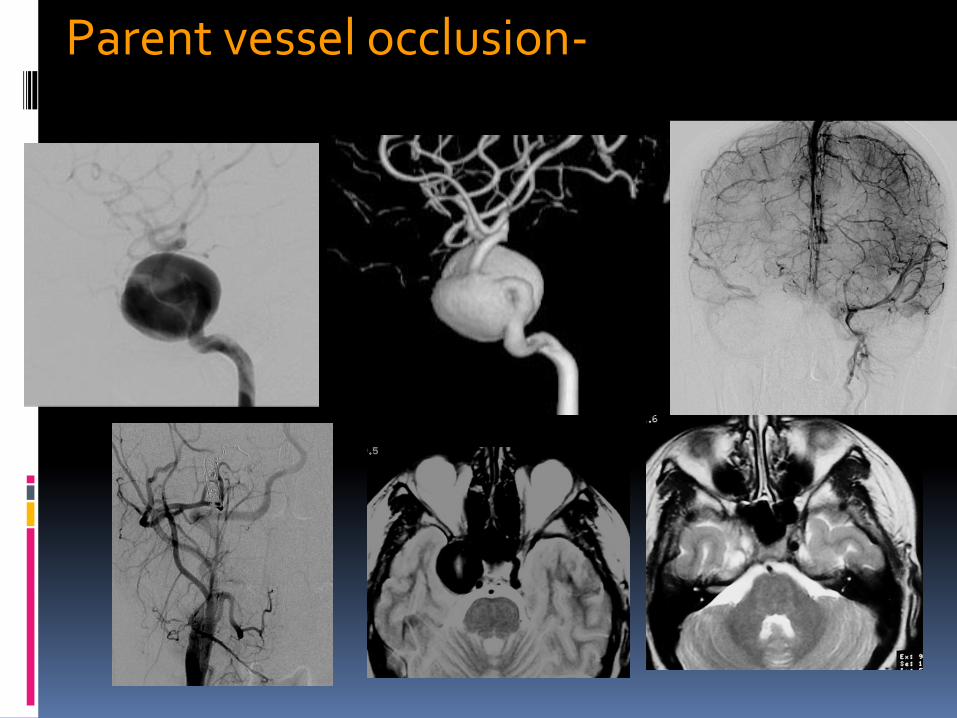
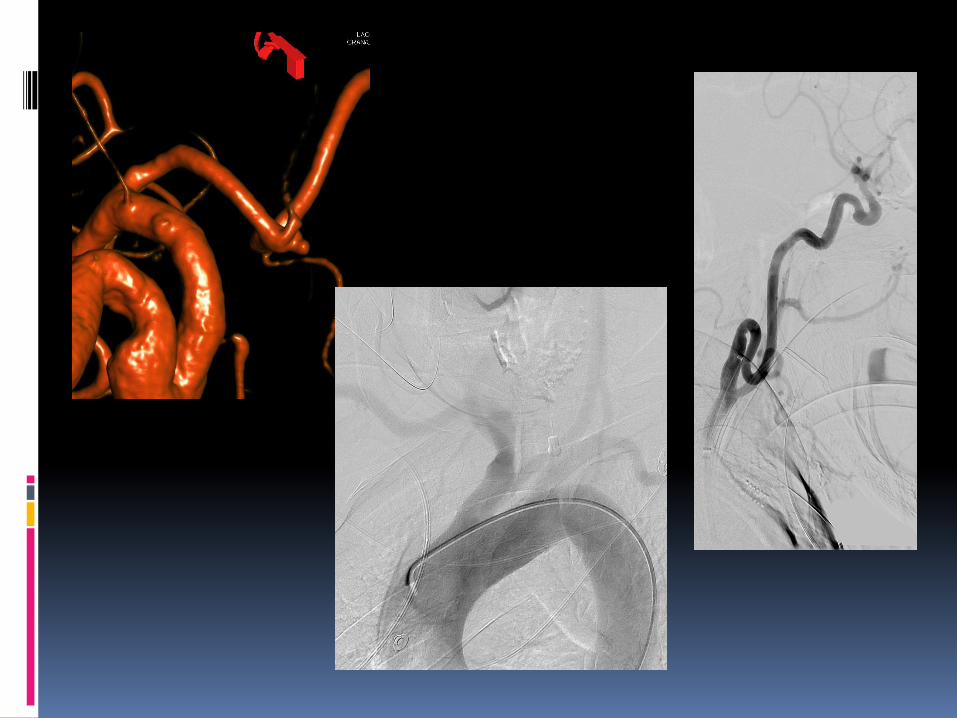
Parent vessel occlusion- Cavernous ICA,
dissecting (VA), small peripheral

Fusiform, dissecting aneurysm

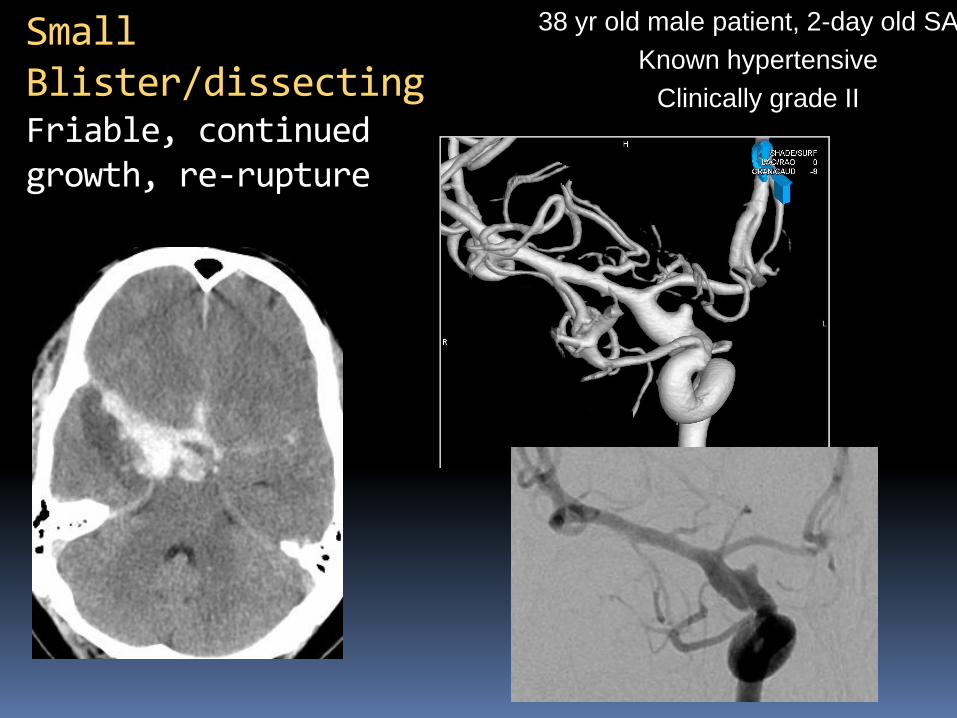
38 yr old male patient, 2-day old SAH
Known hypertensive
Clinically grade II
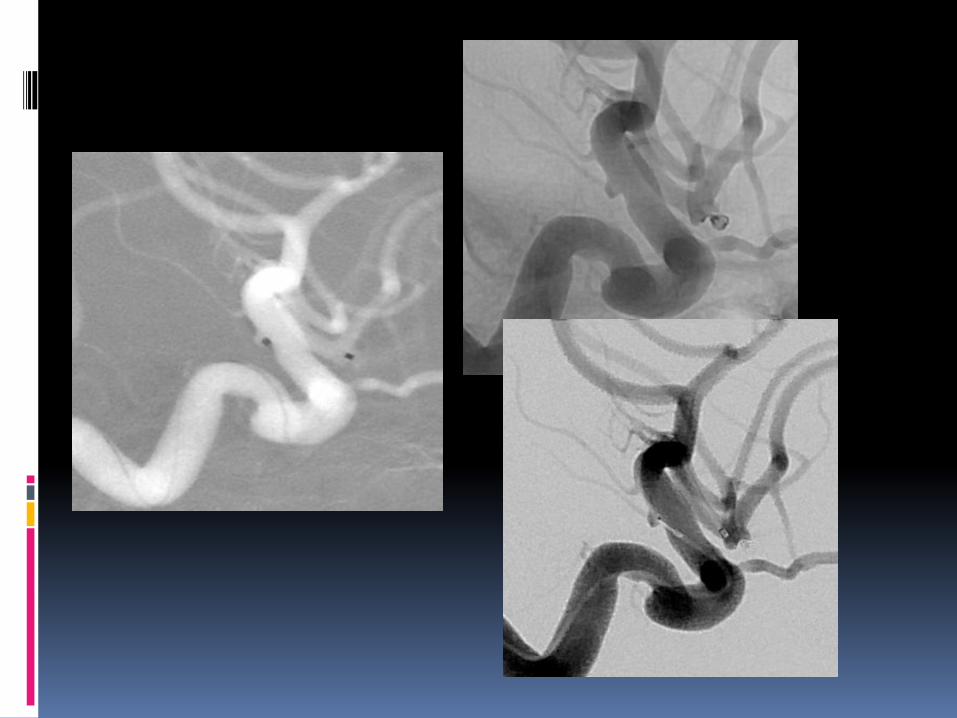
Small Blister/dissecting Friable, continued growth, re-rupture

Classical blister aneurysm
34-year M, SAH

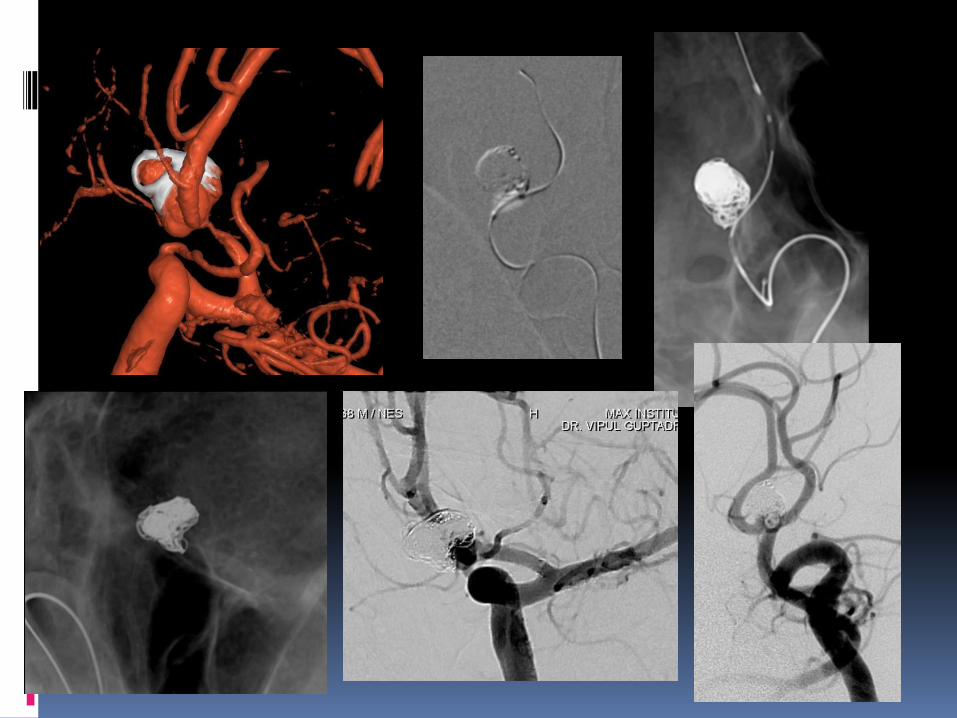
Very small aneurysms
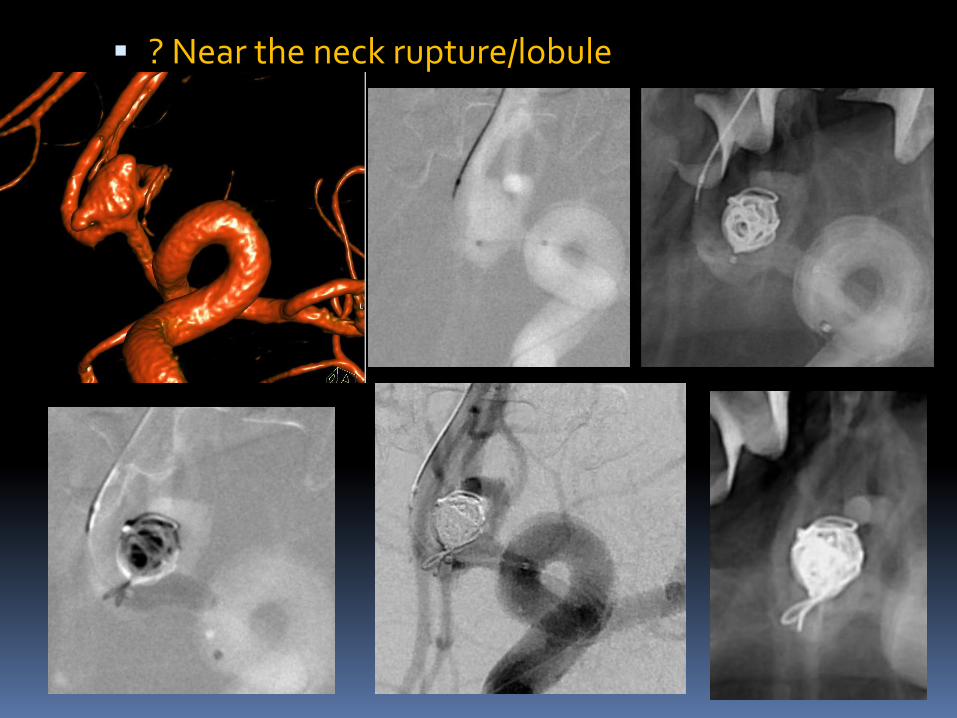
? Near the neck rupture/lobule
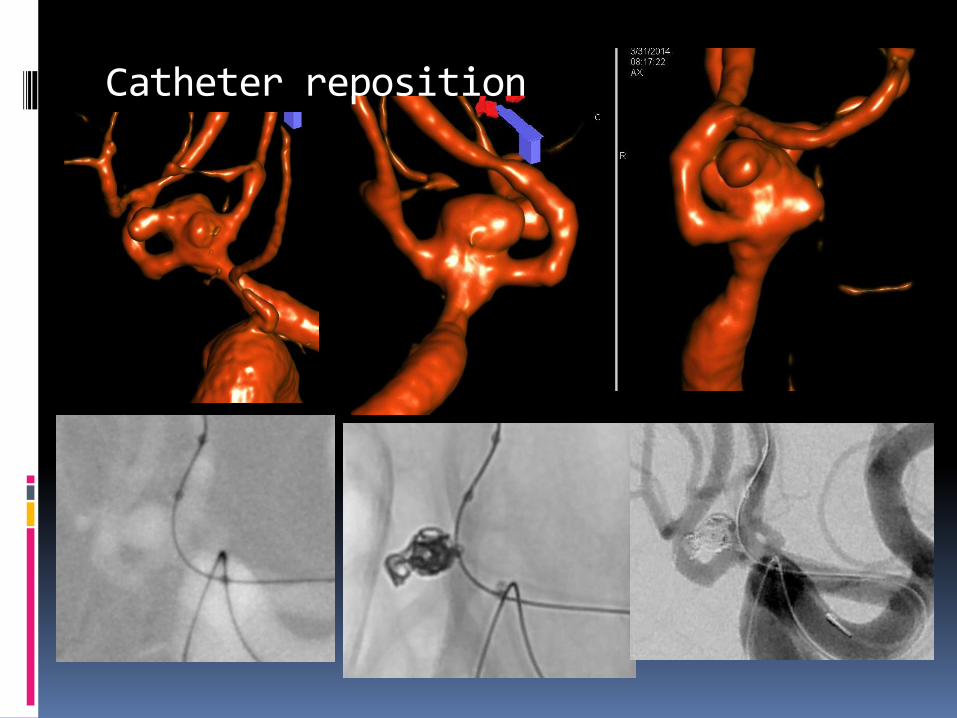
Catheter reposition
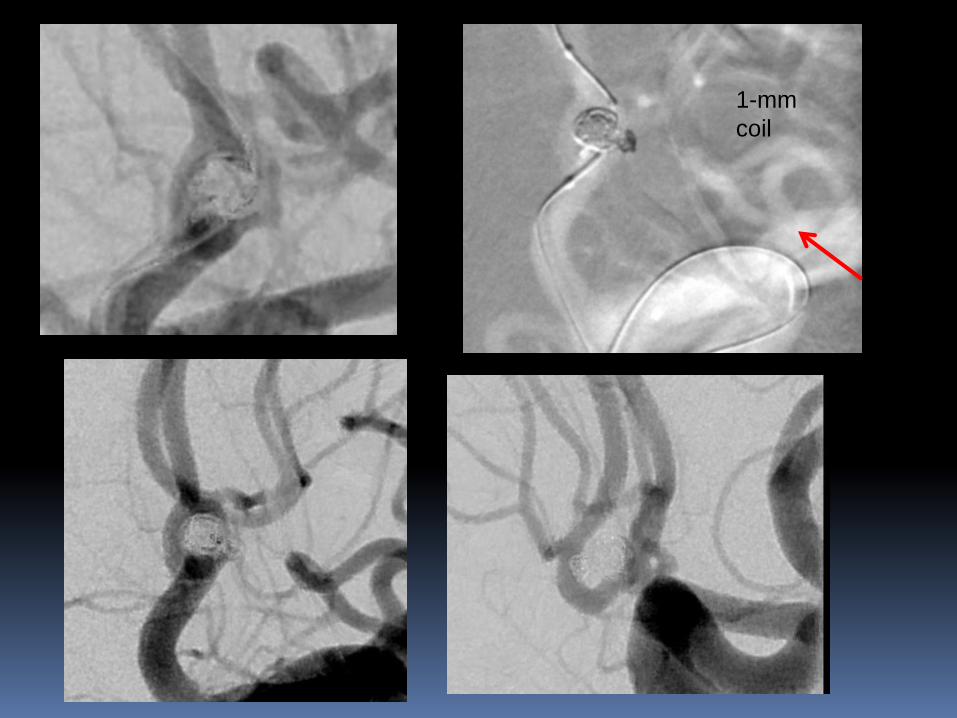
1-mm
coil

Branch from aneurysm- Overinflation technique
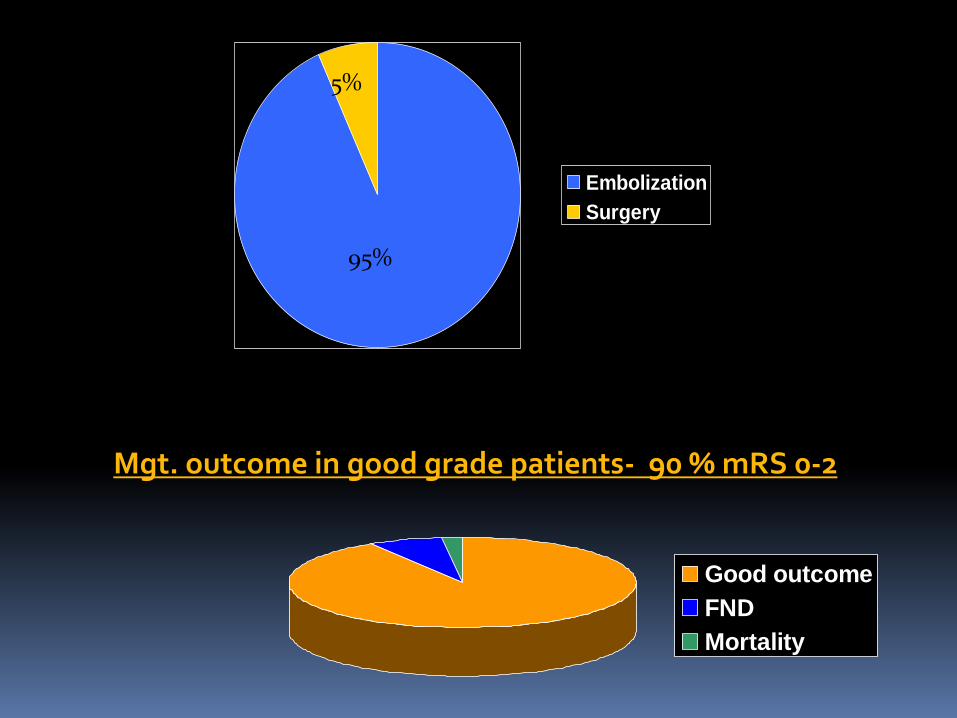
Embolization
Surgery
95%
5%
Good outcome
FND
Mortality
Mgt. outcome in good grade patients- 90 % mRS 0-2

The ISAT revealed a complete occlusion rate of 66% (584 of 988) in the coiled patients, whereas other case series of ruptured coiled aneurysms revealed complete occlusion rates ranging from 33% to 81%
Occlussion rate…
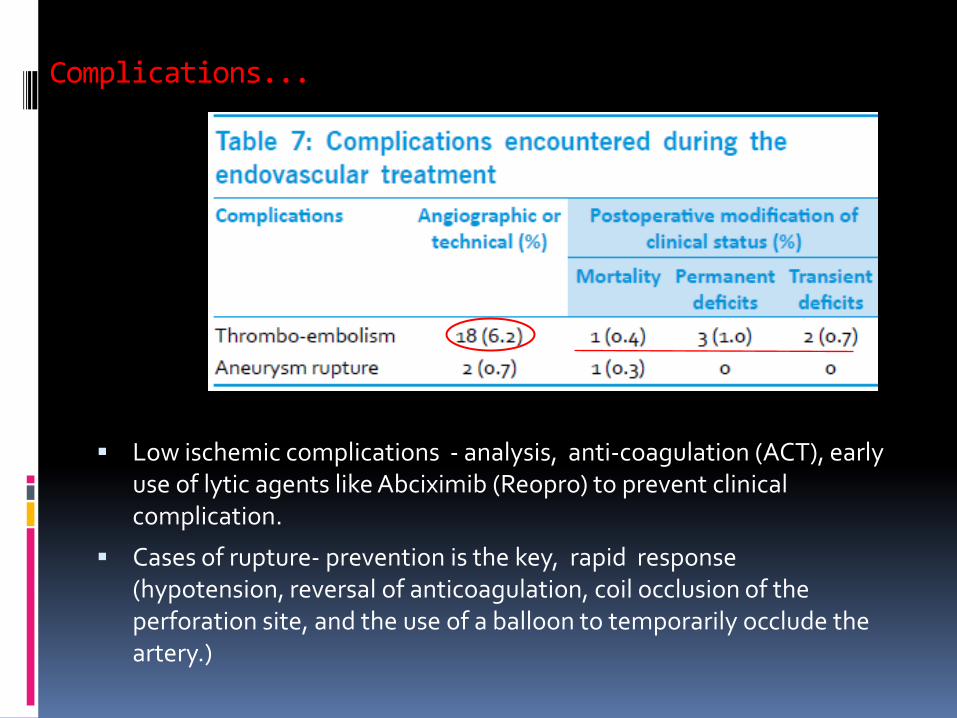
Complications...
Low ischemic complications - analysis, anti-coagulation (ACT), early use of lytic agents like Abciximib (Reopro) to prevent clinical complication.
Cases of rupture- prevention is the key, rapid response (hypotension, reversal of anticoagulation, coil occlusion of the perforation site, and the use of a balloon to temporarily occlude the artery.)
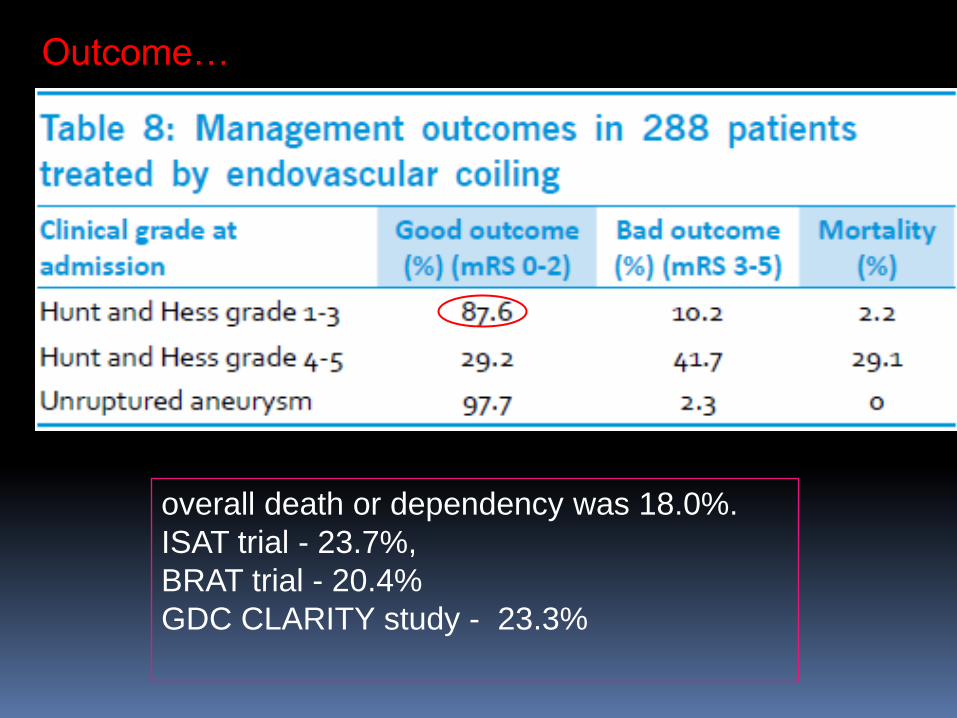
overall death or dependency was 18.0%.
ISAT trial - 23.7%,
BRAT trial - 20.4%
GDC CLARITY study - 23.3%
Outcome…

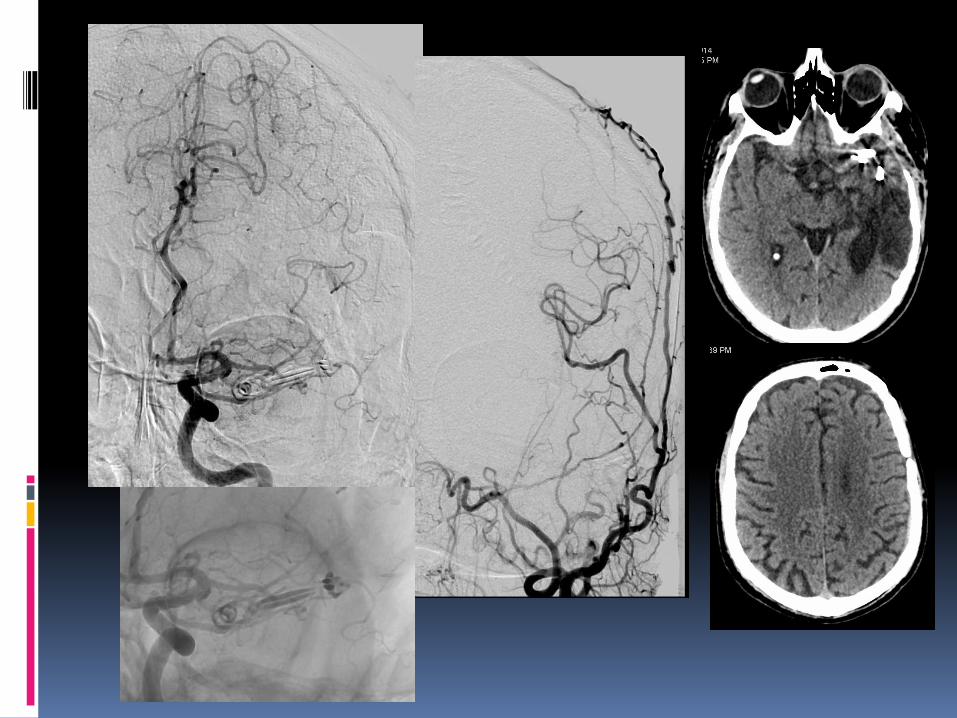
56 yr old, ischaemic stroke
CONCLUSION
>90-95%, with good outcomes – 87.6% ( Good grade),
Team work (NS, INR, critical care)
Meticulous technique with protocols
Imaging, technological advances in material, team work, management of SAH related complication such as vasospasm
Limitation - these are the initial management outcomes only

Thank you