convegno regionale aiom liguria genova, 21 settembre 2019
TRANSCRIPT

Novità nel trattamento
del tumore polmonare
Francesco Grossi
UOC Oncologia Medica
Fondazione IRCCS Ca’ Granda
Ospedale Maggiore Policlinico
Milano
Convegno Regionale AIOM Liguria
Genova, 21 Settembre 2019

Agenda
Immunotherapy in advanced and locally
advanced NSCLC and SCLC: focus on standard
of care and future combinations
Beyond EGFR, ALK and ROS-1: the new
targets BRAF, MET, RET, NTRK
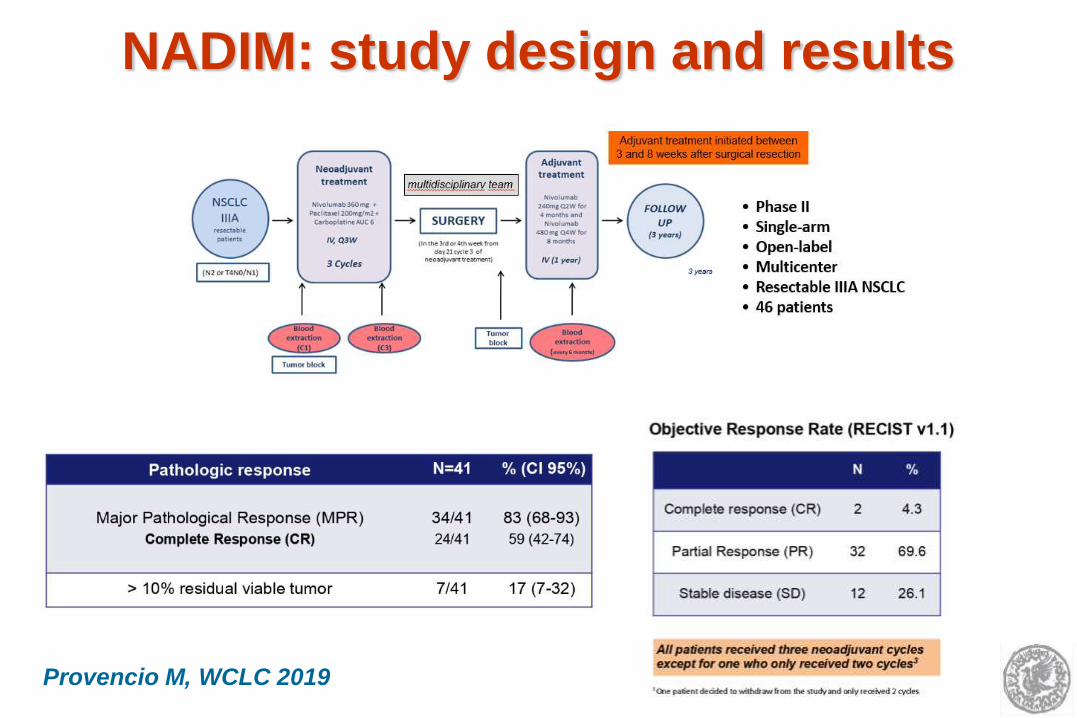
NADIM: study design and results
Provencio M, WCLC 2019

NADIM: PFS and OS (ITT)
Provencio M, WCLC 2019

Summary of neoadjuvant I/O trials
Lee JM, ASCO 2019

PACIFIC: durvalumab after concomitant
CT/RT in stage III NSCLC
Paz Ares L, ESMO 2017

PACIFIC: updated PFS and OS
Antonia S, NEJM 2018

IMpower133: atezolizumab+CBDCA+
etoposide in 1L ES-SCLC
a Only patients with treated brain metastases were eligible. ECOG PS, Eastern Cooperative Oncology Group Performance Status; IV, intravenous; PCI, prophylactic cranial irradiation; PD, progressive disease; PFS, progression-free survival; R, randomized; RECIST, Response Evaluation Criteria In Solid Tumors.
Horn L, NEJM 2018

IMpower133 - atezolizumab+CBDCA+
etoposide in 1L ES-SCLC: OS
Horn L, NEJM 2018

CASPIAN: study design
Paz-Ares L, WCLC 2019
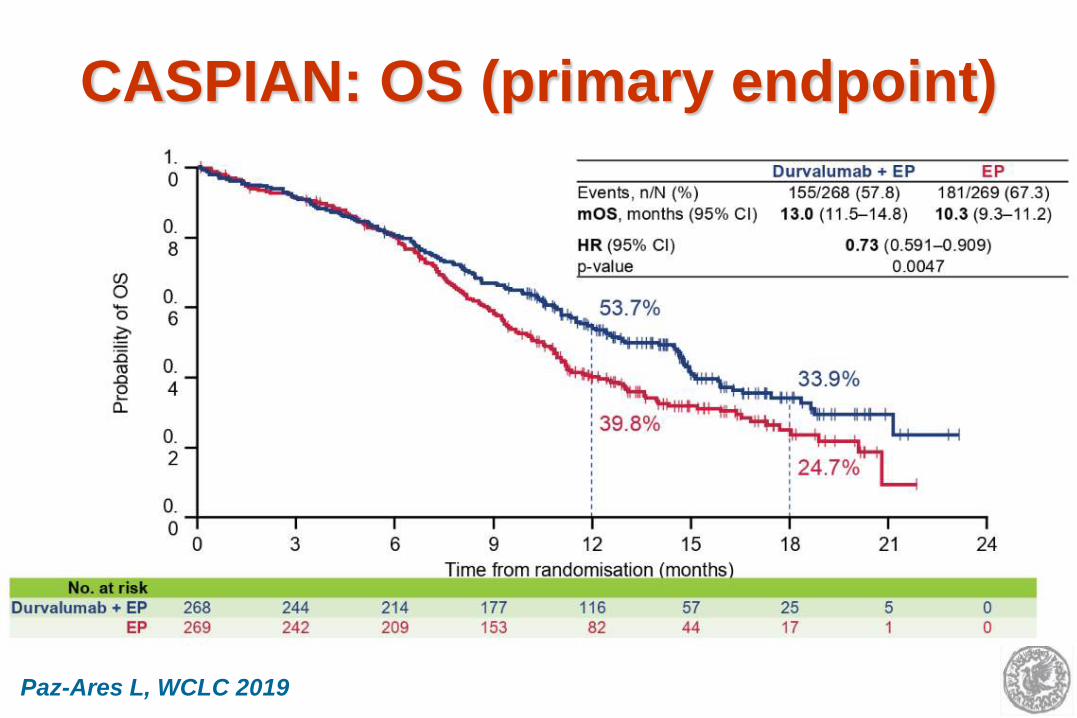
CASPIAN: OS (primary endpoint)
Paz-Ares L, WCLC 2019

CA209-003: 5-Year Overall Survival
Gettinger S, JCO 2018

5-year OS for pts with advanced NSCLC
treated with pembrolizumab
Garon EB, ASCO 2019
15.9%
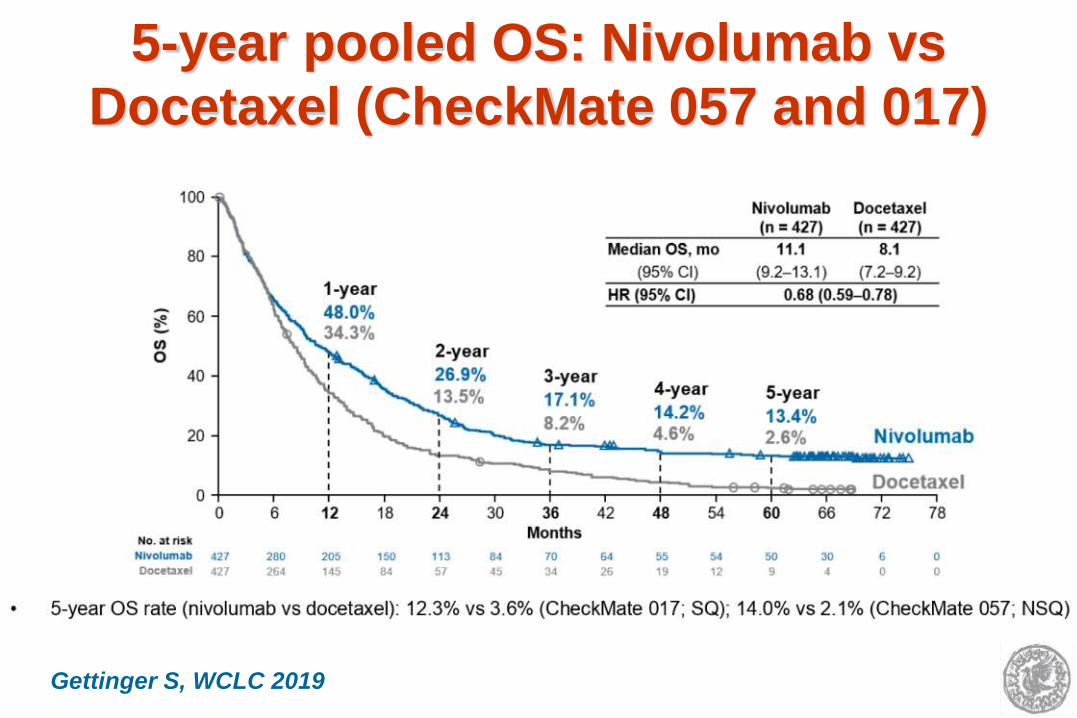
5-year pooled OS: Nivolumab vs
Docetaxel (CheckMate 057 and 017)
Gettinger S, WCLC 2019

KEYNOTE-024: studies design
Reck M, NEJM 2016
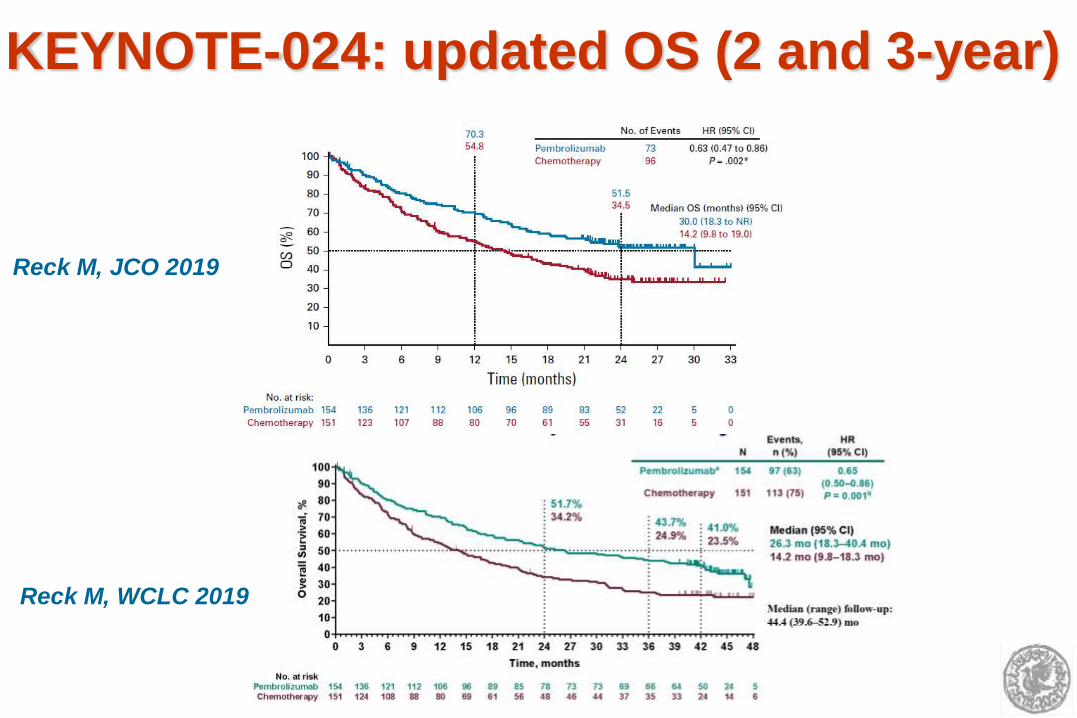
KEYNOTE-024: updated OS (2 and 3-year)
Reck M, JCO 2019
Reck M, WCLC 2019

First-line Pembrolizumab and a PD-L1
TPS of 50-74% vs 75-100%
Aguilar EJ, WCLC 2018
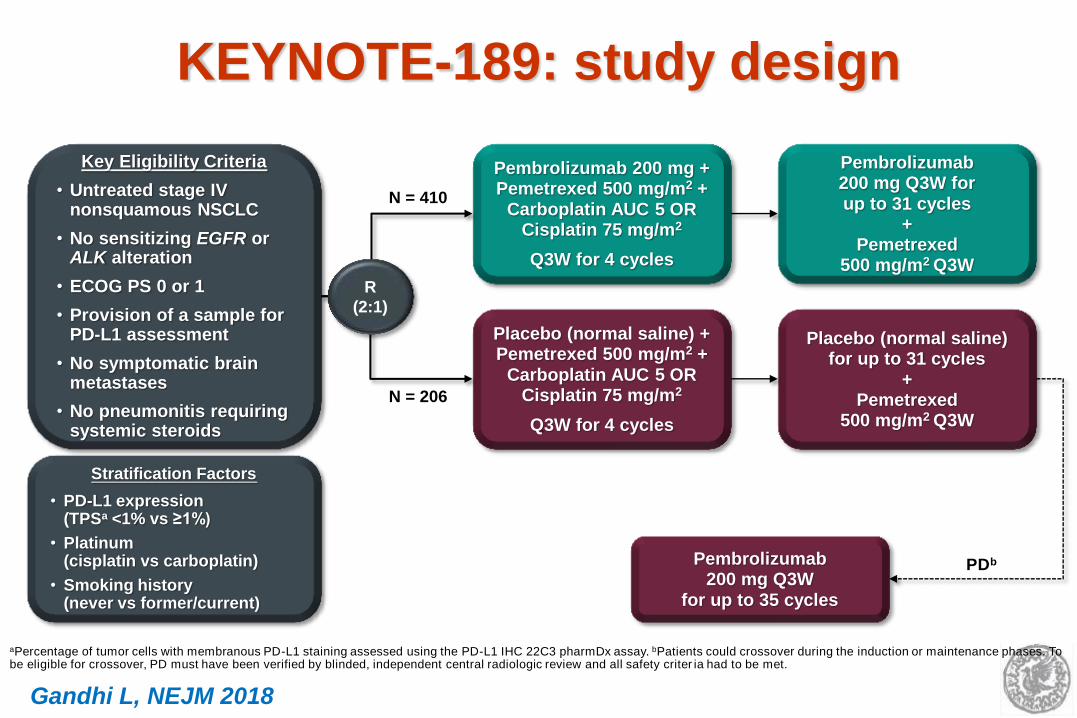
KEYNOTE-189: study design
Key Eligibility Criteria
• Untreated stage IV nonsquamous NSCLC
• No sensitizing EGFR or ALK alteration
• ECOG PS 0 or 1
• Provision of a sample for PD-L1 assessment
• No symptomatic brain metastases
• No pneumonitis requiring systemic steroids
Pembrolizumab 200 mg + Pemetrexed 500 mg/m2 +
Carboplatin AUC 5 OR Cisplatin 75 mg/m2
Q3W for 4 cycles
Placebo (normal saline) + Pemetrexed 500 mg/m2 +
Carboplatin AUC 5 OR Cisplatin 75 mg/m2
Q3W for 4 cycles
R
(2:1)
N = 410
N = 206
Pembrolizumab 200 mg Q3W for up to 31 cycles
+ Pemetrexed
500 mg/m2 Q3W
Placebo (normal saline) for up to 31 cycles
+ Pemetrexed
500 mg/m2 Q3W
Stratification Factors
• PD-L1 expression (TPSa <1% vs ≥1%)
• Platinum (cisplatin vs carboplatin)
• Smoking history (never vs former/current)
Pembrolizumab 200 mg Q3W
for up to 35 cycles
PDb
aPercentage of tumor cells with membranous PD-L1 staining assessed using the PD-L1 IHC 22C3 pharmDx assay. bPatients could crossover during the induction or maintenance phases. To be eligible for crossover, PD must have been verified by blinded, independent central radiologic review and all safety criter ia had to be met.
Gandhi L, NEJM 2018

ASCO 2019 update: Overall Survival
Gadgeel SM, ASCO 2019

IMpower150: PFS and OS (arm B vs C)
Socinski M, NEJM 2018

KEYNOTE-407: study design and OS
Paz-Ares L, NEJM 2018
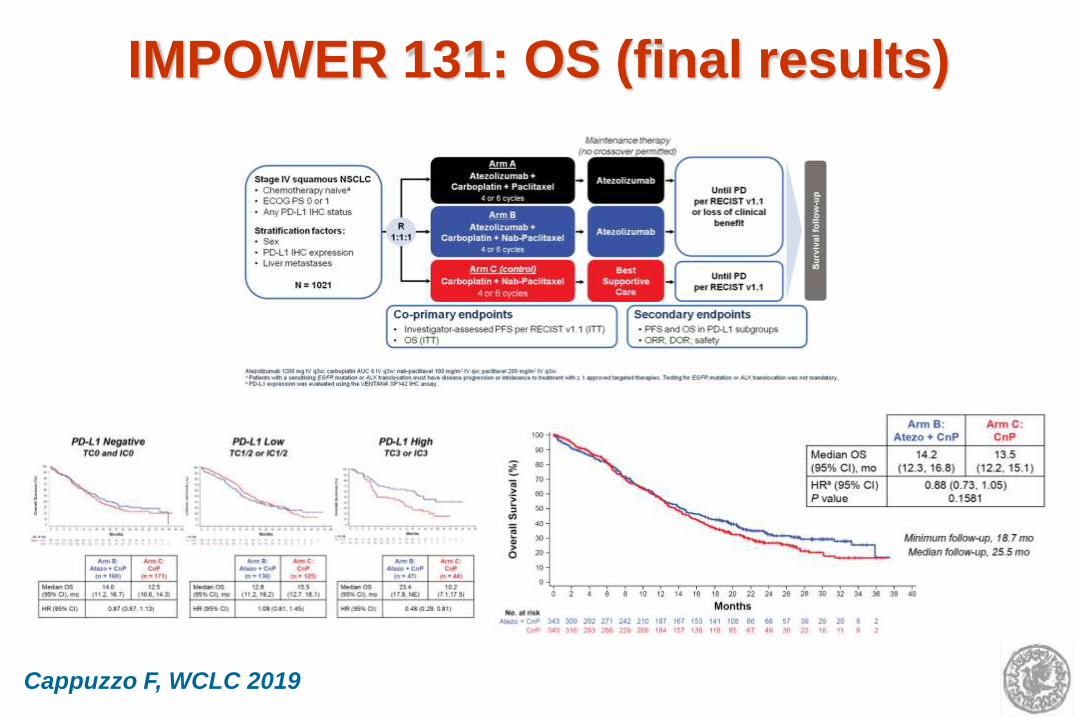
IMPOWER 131: OS (final results)
Cappuzzo F, WCLC 2019

Pooled Analysis of KN021G, KN189 and
KN407: OS in patients with PD-L1<1%)
Data cutoff dates: KN021G, December 1, 2017; KN189, September 21, 2018; KN407, April 3, 2018.
Events, n HR (95% CI)
Pembrolizumab + Chemotherapy
112 0.56 (0.43‒0.73)
Chemotherapy 110
Median (95% CI) OS
19.0 (15.2‒24.0) mo
11.0 (9.2‒13.5) mo
0 3 6 9 12 15 18 21 24 27 30 33
0
10
20
30
40
50
60
70
80
90
100
Time, months
OS
, %
No. at risk
Pembrolizumab +chemotherapy
Chemotherapy alone
221243 186 153 117 92 79 49 29 13 2 0
165185 127 83 56 34 26 16 7 5 4 1
66%
47%
52%
29%
Borghaei H, WCLC 2019

STK11 and KEAP-1 genomic alterations
are associated with inferior clinical
outcomes with CT-I/O in ns-NSCLC
Skoulidis F,
WCLC 2019

Overall Survival and prevalence of
patients with POLE/POLD1 mutations
Wang F, Jama Oncol 2019

Agenda
Immunotherapy in advanced NSCLC: focus on
standard of care and future combinations
Beyond EGFR, ALK and ROS-1: the new
targets BRAF, MET, RET, NTRK

Antitumor activity of TAK-788 in NSCLC
with EGFR exon 20 insertions
Janne PA, ASCO 2019

BRAF V600E mutation: responses
with Dabrafenib +Trametinib
Planchard D, Lancet Oncology 2016

Efficacy of Larotrectinib in TRK fusion–
positive cancers in adults and children
Drilon A, NEJM 2018

Larotrectinib is active in TRK fusion lung cancer
Farago AF, WCLC 2019

Capmatinib in MET ex14-mutated
advanced NSCLC: phase II GEOMETRY
trial (naive & pretrated)
Wolf J, ASCO 2019

Phase II study of tepotinib in NSCLC
patients with METex14 mutations
Paik PK, ASCO 2019

BLU-667 demonstrates substantial antitumor
activity in RET fusion+ advanced NSCLC
Gainor JF, ASCO 2019
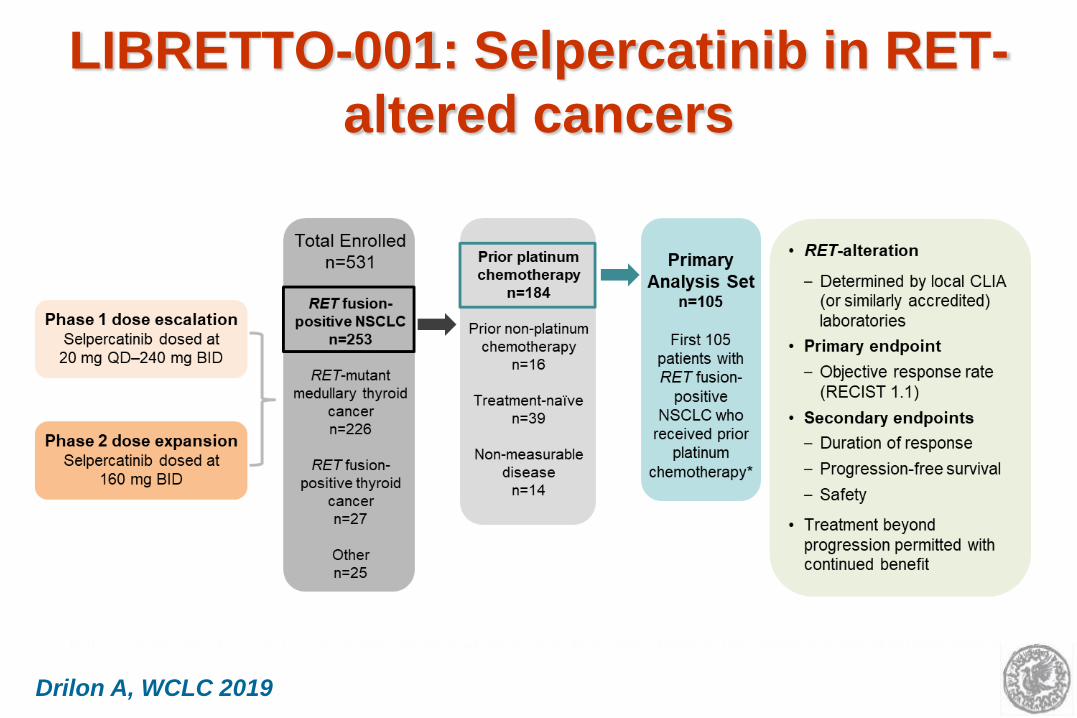
LIBRETTO-001: Selpercatinib in RET-
altered cancers
Drilon A, WCLC 2019

Efficacy of Selpercatinib
Drilon A, WCLC 2019

Phase 1, Multicenter, Open-label Study – Dose Escalation
AMG 510 First-in-Human Study Design
Key Eligibility
– Locally advanced or
metastatic malignancy
– Received prior
standard therapies
– KRAS G12C mutation as
assessed by molecular
testing of tumor biopsies
– No active brain
metastases Cohort 1
180 mg
Cohort 2
360 mg
Cohort 3
720 mg
Cohort 4
960 mg
– 2–4 patients enrolled in
each cohort
– Intra-patient dose
escalation allowed
– Additional patients
may be added to any
dose deemed safe
Safe
ty F
ollo
w-u
p &
Lo
ng
-term
Fo
llo
w-u
pa
a30 (+7) days after end of treatment for safety follow-up; every 12 weeks for long-term follow-up. PK: pharmacokinetics; PFS: progression-free survival.
– Repeated oral daily
dosing with 21-day cycles
– Treatment until disease
progression, intolerance,
or consent withdrawal
– Radiographic scan every
6 weeks
Primary endpoints: dose-limiting toxicities; safety
Key secondary endpoints: PK; objective response rate; duration of response; disease control rate; PFS; duration of stable disease
Scre
en
ing
/ E
nro
llm
en
t Dose Expansion
Expansion dose
determined
Scre
en
ing
/ E
nro
llm
en
t
Patients with
KRASG12C mutant
advanced tumors
N = ~20
(max 60)
Safe
ty F
ollo
w-u
p &
Lo
ng
-term
Fo
llo
w-u
pa
4
AMG 510 a Novel KRASG12C inhibitor:
study design
Govindan R, WCLC 2019

960 mg 720 mg
360 mg 180 mg Planned dose:
% C
han
ge F
rom
Baselin
e
in
Su
m o
f L
on
gest
Dia
mete
r
Evaluable NSCLC Patients With Available Post-baseline Tumor Data, (N = 22)a
Best Tumor Response and Change in Tumor Burden From Baseline
Efficacy outcomes
All evaluable
patients
N = 23
Evaluable patients
treated with 960mg
N = 13
Best overall response
Partial response – n (%)
Stable disease – n (%)
Progressive disease – n (%)
11 (48)
11 (48)
1 (4)a
7 (54)
6 (46)
0 (0)
Objective response rate – % 48 54
Disease control rateb – % 96 100
aOne patient discontinued study due to PD prior to the 1st assessment, and the post-baseline tumor burden data are missing. bPR or SD at week 6. cPatient had complete response to the target lesions. Evaluable patients: patients
who had the first 6-week scan or early PD; NSCLC: non-small cell lung cancer; PR: partial response; SD: stable disease; PD: progressive disease.
SD SD SD SD# SD#
SD# SD# SD# SD#
SD#
SD#
PR PR# PR# * PR# PR#
PR* PR PR# *
PR# * PR#
PR# * c –100
–80
–60
–40
–20
0
20
40
60
80
100
10
# Study ongoing
* Confirmed response
Govindan R, WCLC 2019
AMG 510: best tumor response and
change in tumor burden from baseline

Next Generation Sequencing (NGS)
in NSCLC

2018: The year of Lung Cancer
